Most chronic, recurrent headaches represent a benign headache syndrome; however, headache may also be a symptom of serious CNS or systemic disease. Therefore, the differentiation of primary from secondary headache is an important goal of evaluation.
Primary Headache Disorders
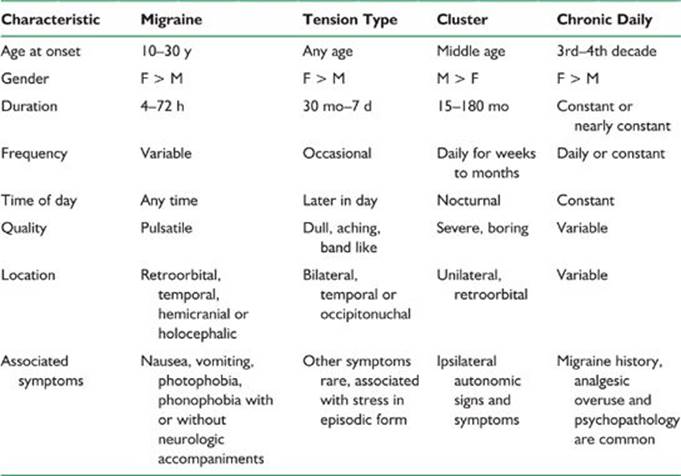
Migraine, tension-type headache, cluster headache, and chronic daily headache represent the overwhelming majority of headaches seen in primary care. Chronic daily headache is more common in referral-based practices specializing in headache. The International Headache Society (IHS) revised its classification system in 2004 and defines headache syndromes on the basis of signs and symptoms. The characteristics of the primary recurrent headaches are described below and in Table 21.1.
I. MIGRAINE
Migraine is now thought to be due to the disturbed function of the trigeminovascular system rather than a primary abnormality of blood vessels. Therefore, the IHS classification no longer refers to migraine as “migraine headache of the vascular type.”
A. The clinical characteristics of migraine are outlined as follows in the IHS criteria.
1. Duration of untreated or unsuccessfully treated headache is 4 to 72 hours.
2. The quality of the pain fulfills at least two of the following: unilaterality, pulsatility, moderate to severe intensity, and aggravation by routine physical activity.
3. At least one of the following is present: nausea or vomiting, photophobia and phonophobia.
4. The diagnosis of migraine and other benign headache syndromes requires the exclusion of organic disease.
5. There should be at least five such episodes if there is no aura or at least two if an aura is present.
B. Migraine with aura (formerly classical migraine) is associated with focal neurologic symptoms and signs. It is a manifestation of cortical spreading depression. Typical migraine auras include homonymous visual disturbance, unilateral paresthesia or numbness, unilateral weakness, aphasia, or unclassifiable speech disturbance. Sensory auras typically have a cheiro-oral distribution and “march” from one body part to another. By definition, the aura meets at least three of the following criteria:
1. It consists of one or more fully reversible positive or negative symptoms of focal cerebral or brainstem dysfunction.
2. One aura symptom develops gradually over 5 or more minutes. If two or more symptoms occur, they do so in succession.
3. No aura symptom lasts more than 60 minutes, or proportionately longer if there is more than one.
4. Headache follows within 1 hour of the aura, precedes the aura, or occurs simultaneously with it. An aura need not begin before the headache.
C. Migraine auras may be prolonged or permanent. Migraine with persistent aura occurs in patients when one aura symptom persists for more than 7 days and neuroimaging studies remain normal. Migrainous infarction is defined as a complication of migraine in which aura does not completely resolve within 7 days and there is evidence of infarction on imaging.
TABLE 21.1 Characteristics of Benign Recurrent Headache Disorders
D. Migraine aura without headache (migraine equivalent) occurs when the aura occurs without headache.
E. Migraine may be triggered by specific endogenous or environmental factors, including ingestion of tyramine-containing foods or alcohol, changes in sleep pattern, and emotional stress. There is also a relation with hormonal factors. Migraine is more frequent in women after menarche. For most women, it is more frequent or severe at or around menses, and the headaches often improve after menopause.
F. The new classification system recognizes a subgroup with chronic migraine that has more than 15 headache days per month or 180 per year.
II. TENSION-TYPE HEADACHE
Tension-type headache replaces the terms “tension” or “muscle contraction” headache because of evidence that muscle tension is not the underlying mechanism of pain.
A. Clinical characteristics of tension-type headache include the following:
1. Headache duration is 30 minutes to 7 days.
2. The pain meets two of the following criteria: pressing or tightening quality, nonpulsatility, mild to moderate intensity, bilaterality, and lack of aggravation by routine physical activity.
3. Absence of nausea or vomiting, although anorexia does occur. Photophobia or phonophobia may occur but not simultaneously.
4. No evidence of organic disease.
5. There may or may not be tenderness of pericranial muscles to palpation.
6. A history of 10 similar headaches.
B. Tension-type headache is episodic when there are fewer than 15 headache days per month or 180 days per year for at least 6 months and chronic when headache frequency exceeds these limits.
III. BENIGN RECURRENT HEADACHE
Migraine without aura and episodic tension-type headache may be difficult to differentiate in some patients because both can be bilateral, nonthrobbing, moderately severe, and associated with anorexia, photophobia, or phonophobia without violating IHS criteria. Some patients may have mixed headaches with features of both or have both types independently. It has been postulated that migraine and tension-type headache are phenotypic expressions of a common abnormality of serotoninergic nociceptive mechanisms referred to as benign recurrent headache. As headache frequency increases, the severity and association with autonomic and neurologic symptoms decrease.
IV. TRIGEMINAL AUTONOMIC CEPHALGIAS
This is a family of disorders manifested by brief, intense, unilateral headaches associated with signs of parasympathetic hyperactivity. The most frequent is cluster headache. Trigeminal autonomic cephalgias are associated with activation of the inferior posterior hypothalamus.
A. Cluster headache. The clinical manifestations of cluster headache are quite characteristic, and the disorder is readily diagnosed from the history and physical examination.
1. A diagnosis can be made using IHS criteria after five or more attacks with the following features:
a. Severe unilateral orbital, supraorbital, or temporal pain lasting 15 to 180 minutes. The pain is usually described as boring.
b. Patients invariably have at least one ipsilateral autonomic sign, including conjunctival injection, eyelid edema, lacrimation, nasal congestion or rhinorrhea, forehead and facial sweating, miosis, or ptosis and agitation.
c. Attacks occur from once every other day to eight times a day. There is a tendency for attacks to occur at the same time each day or to awaken the patient from sleep, usually in the early morning during rapid eye movement sleep.
2. The typical episodic pattern consists of periods of headache lasting 1 week to 1 year separated by remissions of at least 2 weeks. Chronic cluster occurs when headaches persist for at least 1 year without interruption or if remission lasts <2 weeks. Secondary chronic cluster headache occurs if chronic cluster develops after a period of typical episodic headaches.
3. During cluster periods, headache may be precipitated by alcohol, nitrates, and histamine.
B. Cluster headache variants. Several headache disorders, some of which are of mostly historical significance, are thought to represent cluster headache. Raeder originally described a parasellar syndrome of trigeminal pain, oculosympathetic paresis, and cranial nerve dysfunction. The term Raeder’s syndrome came to be used for non-neuralgic head pain and oculosympathetic paresis without other cranial nerve palsies. “Lower-half headaches” such as Sluder’s syndrome, sphenopalatine neuralgia, vidian neuralgia, and greater superficial petrosal neuralgia, which manifest as facial pain and ipsilateral nasal congestion or rhinorrhea may also represent cluster headache.
C. Chronic paroxysmal hemicrania is an unusual disorder mainly affecting women with multiple, brief, unilateral, cluster-like headaches occurring at least five times a day and absolute responsiveness to indomethacin. The pain is generally severe and lasts <30 minutes. There is at least one ipsilateral autonomic symptom during the headache including conjunctival injection, lacrimation, rhinorrhea, nasal congestion, eyelid edema, or oculosympathetic paresis.
D. Short-lasting unilateral neuralgiform cephalgia with conjunctival injection and tearing (SUNCT) is the rarest of the trigeminal autonomic cephalgias. The headaches are more frequent than in the other syndromes, are briefer and less severe, and autonomic involvement generally consists of ipsilateral lacrimation and conjunctival injection. The pain is sharp or pulsating and lasts <4 minutes. There may be as many as 200 attacks a day. Patients without conjunctival injection or lacrimation but with other autonomic symptoms may have a subgroup of this disorder.
V. OTHER PRIMARY HEADACHE DISORDERS
A. Hemicrania continua is a type of chronic daily headache that is strictly unilateral, constant, moderately severe, and usually associated with autonomic signs such as lacrimation, conjunctival injection, rhinorrhea or nasal congestion, ptosis or miosis, and completely responsive to indomethacin.
B. Idiopathic stabbing headache has previously been referred to as jabs and jolts or ice pick pains. It is frequently associated with other primary headaches such as migraine or cluster headache. The clinical pattern is distinctive and diagnosed as follows:
1. Pain is localized to the head, mainly to the distribution of the ophthalmic division of the trigeminal nerve.
2. The pain is stabbing in quality, lasts for a fraction of a second, and may occur singly or in series.
3. Headache recurs at irregular intervals of hours to days.
4. There are no structural changes at the site of the pain or in the distribution of the affected nerve.
C. Primary cough headache. This is a bilateral headache precipitated by Valsalva. Some patients with cough headache have posterior fossa mass lesions or cranio-vertebral junction abnormalities.
VI. CHRONIC DAILY HEADACHE
A. Chronic daily headache is a primary headache disorder in which headaches occur at least 15 days per month. The new IHS classification system recognizes chronic forms of migraine and tension-type headache.
B. Most patients with chronic daily headache evolve from a pattern of episodic migraine.
C. New daily persistent headache is a form of chronic daily headache, which arises acutely without antecedent migraine or tension-type headache and remains constant and unremitting from onset. Most patients can specifically identify the time of onset. The pain is bilateral, nonpulsatile, moderately severe, and unaffected by routine exertion. There may be mild nausea, photophobia, or phonophobia.
D. Analgesic rebound headache. Rebound or withdrawal headache related to overuse of narcotics, butalbital-containing analgesics, ergotamine, or over-the-counter pain medications is frequently a factor in chronic daily headache. These patients have a rhythmic cycle of headache and medication use. The patient awakens with early morning headache resulting from medication withdrawal, and the headache is relieved only by the next dose of medication. Patients may begin to use analgesics in anticipation of pain. Other symptoms of medication withdrawal include irritability, asthenia, and insomnia.
Secondary Headache Disorders
Headache may be a symptom of a variety of disorders of the nervous system.
I. TUMOR
A. Head pain among patients with brain tumors arises from traction or pressure on pain-sensitive intracranial structures or from production of increased intracranial pressure (ICP).
B. There is nothing pathognomonic about headache associated with brain tumor. In most cases, headache is dull, aching, or pressure-like in quality. The headache is intermittent and moderately severe in most patients. Bending or Valsalva may aggravate the pain. Headache from brain tumor rarely mimics migraine.
C. The “typical” history of severe headache worse in the morning and associated with nausea or vomiting or a history of postural, cough, or exertional headache is relatively infrequent.
D. Unilateral headache usually is on the side of the lesion. Bilateral headache usually is due to increased ICP or either midline or bilateral tumor.
E. Supratentorial tumors generally produce frontal or bifrontal headache. Infratentorial tumors generally cause occipital pain.
F. Increased ICP produces severe headache in the frontal area, vertex, or neck with nausea and vomiting.
G. Involvement of the dura or skull may produce localized pain.
II. CEREBROVASCULAR DISEASE
A. Intracranial hemorrhage. Headache, nausea, and vomiting are more commonly associated with intracranial hemorrhage than with ischemic stroke. In some patients, recurrent subarachnoid hemorrhage (SAH) may resemble migraine. Patients with aneurysmal SAH often have a warning leak or sentinel headache several days to months before substantial hemorrhage occurs.
B. Unruptured aneurysms. It is controversial how often unruptured aneurysms cause recurrent headache. In some patients, sudden onset of an intense headache with normal imaging and spinal fluid, referred to as thunderclap headache, simulates SAH. Unruptured aneurysms and segmental vascular narrowing have been reported in patients with thunderclap headache. Data suggest that in most of these cases the aneurysm is incidental. Prospective data demonstrate that SAH is rare in patients with recurrent primary thunderclap headache.
C. Arteriovenous malformation (AVM). Chronic headache occurs in approximately 15% of patients with AVMs. These headaches may be clinically indistinguishable from migraine. This relation may be coincidental because migraine is common in the general population and AVMs are rare in large series of patients with migraine who undergo imaging studies.
D. Ischemic stroke. Headache occurs in 30% to 40% of patients with cerebral infarction and 25% to 40% of those with transient ischemia. It is usually nonthrobbing, ipsilateral to the infarct, and self-limited. In patients with chronic or recurrent headache associated with stroke, the following differential diagnoses should be considered.
1. Cervicocephalic dissection. An ipsilateral throbbing or steady headache, with or without neck or jaw pain, frequently accompanies carotid artery dissections. Dissection may produce fixed or reversible neurologic deficits. Oculosympathetic paresis, visual scintillations, and dysgeusia are also clues to this diagnosis. Dissections may be overlooked when they occur without a previous history of trauma or after relatively trivial injuries.
2. Migrainous stroke and late-life migraine accompaniments. When headache recurs in association with focal neurologic deficit, it may be challenging to distinguish between migrainous accompaniments from atherosclerotic cerebrovascular disease, especially in elderly patients with stroke risk factors. There need not be a preexisting history of migraine or a severe headache during the episode. Fisher suggested the following criteria for late-life migraine accompaniments.
a. Scintillations or other typical visual displays that may expand or “build up” after onset.
b. A sensory “march” from one body part to another or spread to the opposite side of the body.
c. Progression from one accompaniment to another without delay.
d. Episodes may be stereotyped, which should be less common with embolism.
e. Headache is frequently associated with the episode.
f. The attacks occur in characteristic flurries during mid- or late-life and have a benign course.
g. Exclusion of other causes of focal deficit, including atherosclerosis.
E. Sinovenous thrombosis. Occlusion of a major dural sinus frequently produces headache and papilledema indistinguishable from pseudotumor cerebri. Sinovenous occlusion should be suspected whenever acute or subacute neurologic dysfunction manifests as altered consciousness, focal deficits, seizures, or evidence of an increased ICP.
III. HEADACHES RESULTING FROM DISORDERS OF ICP
A. Idiopathic intracranial hypertension (benign intracranial hypertension and pseudotumor cerebri).
1. The primary features of this disorder are headache and visual disturbance (enlargement of the blind spot, transient visual obscurations, and progressive visual loss) resulting from elevated ICP. There may also be pulsatile tinnitus, dizziness, and nausea.
2. Idiopathic intracranial hypertension occurs most often in women and is frequently associated with obesity and menstrual irregularities.
3. Physical findings are limited to papilledema and abducens nerve palsies. Papilledema may be unilateral, asymmetric, or absent.
4. CSF is acellular with elevated pressure. The protein may be low.
5. Imaging may show slit-like ventricle, acquired tonsillar ectopia, or an empty sella, but no mass lesion.
6. Most cases are idiopathic but potential etiologies include vitamin A intoxication, steroid withdrawal, hypoparathyroidism, systemic lupus erythematosus (SLE), or medications (tetracycline and nalidixic acid). In some patients, imaging reveals superior sagittal or lateral sinus thrombosis. Sinovenous occlusion associated with ear infection has been referred to by the misnomer “otitic hydrocephalus.”
7. Idiopathic intracranial hypertension without papilledema should be considered in the differential of chronic daily headache.
B. Hydrocephalus.
1. Headache is not usually a feature of communicating hydrocephalus.
2. Headache is common with obstructive hydrocephalus. It is usually occipital and may be associated with neck pain or stiffness, vomiting, or visual abnormalities. The headache may be present on awakening and more severe in the morning. Obstructive hydrocephalus resulting from intraventricular tumors may cause positional headache and life-threatening increases in ICP.
C. Intracranial hypotension. The typical history includes postural headache with or without nausea and dizziness, which is worsened or initiated by standing and relieved by recumbency. The diagnosis is obvious when there is a history of a preceding lumbar puncture (LP).
1. Post-LP headache may occasionally be protracted or complicate evaluation of patients with chronic or recurrent headaches from other causes. Demographic features associated with post-LP headache are youth, female gender, and low body mass index. Technical aspects affecting the risk of post-LP headache include needle diameter, use of cutting (Quincke) needles, and orientation of the bevel but not duration of recumbency after the procedure or hydration.
2. CSF hypotension may also occur as a result of CSF leaks from head trauma, Valsalva’s maneuver, or nerve-root avulsion.
3. The diagnosis may be confirmed by low-CSF pressure on repeat LP. MRI demonstrates diffuse dural enhancement, descent of the cerebellar tonsils, and subdural fluid collections.
IV. PHEOCHROMOCYTOMA
Approximately 10% of patients with pheochromocytoma present with headache and paroxysmal hypertension. The headache is usually bifrontal, severe, and throbbing. It may be exacerbated by coughing, bending, straining, or lying flat.
V. HEADACHE OF RHINOSINUSITIS
A. Current criteria require that headache of rhinosinusitis be associated with acute or acute on chronic sinus infection demonstrated by objective means such as nasal endoscopy or facial CT, a temporal relationship with onset of sinusitis and resolution after successful treatment of the sinus infection.
B. Chronic changes such as mucoperiosteal thickening are not associated with headache.
C. Most patients with self-reported sinus headaches meet IHS criteria for migraine or respond to triptans.
VI. INFLAMMATORY DISORDERS
A. Giant cell arteritis.
1. This disorder is rare before age 50 but increases in incidence with advancing age.
2. Headache is almost invariably present. Pain is often localized to the temple and is sharp, throbbing, or boring in quality. There may be constitutional symptoms, joint complaints (polymyalgia rheumatica), or jaw claudication. Blindness from ischemic optic neuropathy is the most feared complication. Diplopia may arise from ischemia of oculomotor nerves or extraocular muscles.
3. Physical findings include a tender, nodular, nonpulsatile, thickened superficial temporal artery.
4. Diagnosis. The Westergren erythrocyte sedimentation rate (ESR) is elevated in approximately 85% of patients. Other common laboratory abnormalities include elevated C-reactive protein, thrombocytosis, and anemia. Definitive diagnosis requires superficial temporal artery biopsy, but the biopsy may be negative because of patchy involvement (skip lesions).
B. SLE.
1. Migrainous headaches, often with focal auras, occur frequently in patients with systemic lupus. Visual scintillations have been reported anecdotally as the presenting symptom of lupus. In a case-controlled prospective study of patients with SLE, there was a higher incidence of migraine, a higher percentage of migraine with aura, and later age of migraine onset than in controls. There was also a tendency for headaches to parallel the activity of the lupus and sometimes to respond to steroids or immunosuppressants.
2. There is no proven association of antiphospholipid antibodies to migraine in SLE patients.
VII. POST-TRAUMATIC HEADACHES
A. Postconcussion syndrome is a distinct clinical entity following relatively minor head injuries that is manifested by recurrent headache, memory disturbances, irritability, difficulty concentrating, dizziness, and depressive symptoms. Symptoms usually resolve within 6 months.
B. Chronic subdural hematoma may present with headache, seizures, or focal neurologic deficits.
C. Occipital neuralgia. The occipital nerve may be traumatized directly or compressed by spasm of the trapezius or semispinalis capitis muscle. There is usually a lancinating, neuralgic component to the pain, a Tinel’s sign over the occipital condyle and decreased sensation over the ipsilateral occipital scalp.
D. Post-traumatic migraine and tension-type headaches. In some patients, head trauma may precipitate headaches identical in quality to migraine or tension-type headache or aggravate preexisting ones. Post-traumatic cluster headache has also been reported. In some patients, headache is associated with scarring at the site of a scalp laceration and is relieved by infiltration of a local anesthetic.
E. Post-traumatic dysautonomic cephalalgia. Throbbing headaches associated with nausea, photophobia, and signs of ipsilateral sympathetic overactivity, such as sweating and mydriasis, occur as delayed sequelae of penetrating neck injuries that damage the sympathetic fibers in the carotid sheath. This disorder should not be confused with cluster headache, which it superficially resembles.
VIII. TEMPOROMANDIBULAR JOINT DYSFUNCTION
Temporomandibular joint (TMJ) dysfunction is believed to be a myofascial syndrome related to dental malocclusion or bruxism. It may cause recurrent preauricular or temporal pain radiating into the neck. The pain is typically aggravated by chewing and is frequently worse in the morning. Physical findings include lateral jaw deviation and crepitus of the joint on opening the mouth and tenderness or spasm of the masticatory muscles.
IX. TRIGEMINAL NEURALGIA
Trigeminal neuralgia is often mentioned in the differential diagnosis of cluster headache, although typical trigeminal neuralgia is rarely confused with other entities. Onset usually occurs late in life except when it is a manifestation of multiple sclerosis.
A. The IHS defines trigeminal neuralgia as follows:
1. Paroxysmal attacks of facial or frontal pain lasting a few seconds to <1 minute.
2. The attacks have at least four of the following characteristics:
a. Distribution along one or more divisions of the trigeminal nerve.
b. Sudden, intense, sharp, superficial, stabbing or burning quality.
c. Severe intensity.
d. Precipitation by stimulation of trigger areas or by daily activities such as eating, talking, washing the face, or cleaning the teeth.
e. The patient is asymptomatic between the paroxysms.
f. Absence of neurologic deficit.
g. Attacks are stereotyped.
3. Most cases result from microvascular compression of the trigeminal nerve, but secondary causes include cerebellopontine angle tumors and vascular malformations.
Clinical Assessment
I. HISTORY
The history is the most important factor in the accurate diagnosis of headache. It is usually helpful to ask the patient to describe a typical headache from its onset. As many as 30% to 40% of headache patients have more than one headache type, and an accurate description of each type should be obtained. Disorders of structures in or near the head may be perceived as headache. Therefore, the physician must inquire about general symptoms and signs of nervous system dysfunction in addition to a detailed medical history. The headache history should specifically include questions regarding the following areas.
A. Age of onset. Most benign headache syndromes start early in life, usually between childhood and the third decade, although tension-type headache may begin at any time. Late onset may suggest a more serious condition.
B. Localization of pain. The location of headache may help in determining its etiology. Migraine is frequently unilateral, alternates sides, and involves the temple or retro-orbital area. Tension-type headache is usually bilateral, frontal, or occipital, and radiates into the neck and shoulders. Brief attacks of strictly unilateral orbital pain suggest cluster headache or chronic paroxysmal hemicrania. Dental, ocular, and sinus disorders often produce frontal pain. The site of headache may be of localizing value in patients with mass lesions.
C. Temporal pattern. Headache syndromes may have characteristic patterns of duration and frequency. In general, longer-lasting headaches tend to be benign, particularly when headache is constant over more than several months without change in character or new signs. Headache resulting from meningitis may be constant, but not usually over a prolonged duration. Benign headache syndromes typically produce episodic headache. For instance, migraine usually lasts several hours and occurs several times a month. Cluster headache has a characteristic periodicity. Acute tension-type headache is usually brief and associated with emotional stress, but in its chronic form, tension-type headache becomes more frequent, prolonged, or constant and loses its association with psychosocial stressors. The mode of onset may also be helpful. Does the headache begin gradually or start suddenly? Sudden onset of headache is of greater concern because it may indicate intraparenchymal or SAH.
D. Quality and severity of pain. These may be difficult for patients to verbalize and the interviewer may need to offer guidance to elicit the history. Migraine and headache associated with fever are usually throbbing and pulsatile, for instance. Tension-type headache is usually described as dull and nagging, tight and constricting, or bandlike. Tumor and meningitis typically produce a steady, aching pain. Severity of pain can be ranked on a scale of 1 to 10. An indirect indicator of severity is interference with work and social activities.
E. Prodromal and associated symptoms. Symptoms that precede or coincide with headache may be clues to the nature of the underlying headache. The patient with migraine may have premonitory mood or behavioral changes for several days prior to onset. Visual scintillations and fortification spectra are typical migraine prodromes, but visual symptoms may also be associated with carotid dissections and occipital AVMs. Ipsilateral autonomic features are almost always present in cluster headache, the paroxysmal hemicranias, hemicrania continua, and SUNCT.
F. Precipitating factors. Provoking factors may suggest the diagnosis. Examples include precipitation of an attack of trigeminal neuralgia by cutaneous stimulation or of migraine by ingestion of certain foods or alcohol, stressful life events, glare, hypoglycemia, or sleep deprivation. Chewing may trigger pain in patients with TMJ dysfunction or giant cell arteritis. Avoidance of triggers may also be helpful in treatment.
G. Sleep onset. Migraine, hypnic, and cluster headaches may awaken patients from sleep. Tension-type headache rarely does. Headaches are generally worse in the mornings in patients with sleep apnea and increased ICP.
H. Relieving or exacerbating factors. Patients with migraine typically report exacerbation with movement, bending, straining, and coughing and relief with lying flat, avoiding bright light and sometimes by pressure over the superficial temporal artery or after vomiting. Post-LP headache is characteristically modified by posture.
I. Family history. About 20% to 60% of patients with migraine report at least one affected family member. However, this is not unexpected because 6% of men and 18% of women in the general population have migraine.
II. PHYSICAL EXAMINATION
In addition to a thorough general and neurologic examination, certain areas require special attention.
A. Vital signs should be checked for fever and hypertension.
B. Inspection, palpation, and percussion of the skull should be performed to check for tenderness or scarring, which may be signs of trauma. There may be tenderness at the site of a skull neoplasm. Percussion over the site of a tumor or subdural hematoma may also produce pain. In children, head circumference should always be measured.
C. Assessment of the ears, tympanic membranes, and mastoids may reveal evidence of otitis or mastoiditis.
D. Evaluation of the TMJs. There may be local tenderness, crepitus or lateral jaw deviation with mouth opening or closing. This can be felt externally or with the examiner’s fingers in the external auditory canals. When TMJ dysfunction results from muscle spasm, the joint is tender to direct palpation but not to palpation through the ear canal.
E. Palpation of glandular and lymphatic tissues. Examination of the soft tissues of the neck may reveal evidence of infection or malignancy, sarcoidosis, or Behçet’s syndrome.
F. Inspection of the teeth and oropharynx. In some patients, headache may be referred from dental disease, although headache rarely occurs without concomitant tooth pain. Percussion of the teeth and inspection for caries and periodontal disease may reveal a dental origin of pain. Percussion of the maxillary teeth may also hint at maxillary sinusitis, which can arise from dental root infection.
G. Assessment of the nose and paranasal sinuses. The nasal mucosa should be examined for polyps, septal deviation, and secretions. The maxillary and frontal sinuses may be palpated or percussed. The sinuses can also be transilluminated with a flashlight in a darkened room. The ethmoid and sphenoid sinuses cannot be adequately evaluated at the bedside.
H. Assessment of the eyes. Ocular causes of headache are uncommon but patients frequently consult an ophthalmologist or optometrist before seeking a neurologic opinion. Eye strain and refractive errors rarely prove to be the cause of chronic headache. Nevertheless, examination of the eyes may reveal papilledema or abducens palsy resulting from increased ICP, optic disc pallor from a compressive lesion, or ischemic optic neuropathy associated with giant cell arteritis. Acute glaucoma may sometimes present primarily with head pain.
I. Assessment of the extracranial vasculature is especially important in cases of suspected giant cell or temporal arteritis, in which the superficial temporal artery may be tender, nodular, and nonpulsatile. Bruits may result from arterial stenosis or increased venous outflow in patients with AVMs. Increased collateral flow may be a source of headache when there is extracranial vascular disease. In patients with migraine, compression of the superficial temporal artery may temporarily relieve the pain.
J. Palpation of the scalp and neck musculature and neck mobility. Tenderness of the pericranial muscles and limited or painful range of motion of the neck may suggest tension-type headache or spinal pathology. Spinal disease may cause headache referred to the frontal area. Resistance to passive anteroposterior neck movement, Kernig’s and Brudzinski’s signs are indications of meningeal irritation due to CNS infection or subarachnoid bleeding.
K. A low hairline may be a clue to craniovertebral junction abnormalities such as a Chiari’s malformation, basilar impression, or basilar invagination.
Clues to Structural Disease
I. INDICATORS OF STRUCTURAL DISEASE
Recurrent attacks of an acute recurrent headache are usually migraine. Chronic nonprogressive headache usually represents analgesic overuse, benign intracranial hypertension, or chronic tension-type headache. Features that suggest structural disorders are discussed in this section:
A. Altered consciousness or behavior. Although loss of consciousness during headache may result from vasovagal syncope or basilar migraine, in most cases it is a sign of increased ICP, seizure activity, or ischemia. Sudden headache with altered consciousness may represent SAH. Changes in cognitive function may also accompany structural lesions.
B. Neurologic deficit developing simultaneously with or following the onset of headache. Migraine auras usually precede the headache, although this is not required by definition. For the other benign headache disorders except cluster headache, nonspecific subjective neurologic symptoms occur more often than objective signs of neurologic dysfunction. When a neurologic deficit develops at or after onset of headache, differential considerations include tumor, stroke, and abscess.
C. Headache associated with fever or meningeal signs should always suggest infection. Recurrent meningitis may occur in patients with anatomic defects, after splenectomy, or immune compromise. Noninfectious causes of recurrent meningitis include craniopharyngiomas, dermoid cysts, sarcoidosis, Behçet’s syndrome, and Vogt–Koyanagi–Harada’s syndrome. Recurrent aseptic meningitis associated with large mononuclear endothelial cells is referred to as Mollaret’s meningitis. It has been associated with Herpes simplex infection. Tuberculous and fungal meningitides are likely to present chronically. SAH may also produce meningismus and low-grade fever. Fever and headache may accompany sinusitis or dental abscess, but the physician should keep in mind the possibility of intracranial complications of extracranial infections of the head and neck, including sinovenous thrombosis and brain abscess.
D. Headache occurring exclusively on one side over time is referred to as side-locking. It has traditionally been described as a sign of structural disease, particularly vascular abnormalities. In reality, benign headache syndromes such as migraine, cluster headache, and atypical facial pain may consistently affect one side of the head.
E. Onset after age 50. Benign headache syndromes generally begin early in life. Exceptions are cluster headache, which usually begins in middle age, and hypnic” headache.
F. Change in character of preexisting headache or response to treatment. A patient with chronic recurrent headache can develop a second disorder. Therefore, the clinician should carefully approach the patient with a change in the pattern or quality of chronic headaches.
G. Vomiting preceding headache by days to weeks, with or without preceding nausea, may be a sign of increased ICP.
H. Headache associated with paroxysmal hypertension. Pheochromocytomas cause headache, tachycardia, tremor, nausea, or diaphoresis. When the tumor is located in the bladder, symptoms may follow urination.
I. Associated endocrine changes. The association of subacute or chronic headache with signs of secondary hypothyroidism, galactorrhea, hypo- or hypercortisolism, or other evidence of pituitary dysfunction raises suspicions of a sellar lesion such as a pituitary adenoma. Hypopituitarism may also occur with craniopharyngiomas.
J. Headache precipitated by rapid changes in head position or head movement. Rapid changes in head position may produce pain when there is an intracranial mass. Intraventricular lesions such as colloid cysts of the third ventricle may cause obstructive hydrocephalus with a change in posture.
K. Headache initiated by Valsalva’s maneuver or associated with exercise or sexual activity. Although migraine is often exacerbated by Valsalva’s maneuver, the onset of headache with Valsalva’s maneuver is more ominous. About 10% of patients with exertional or cough headache have an underlying structural abnormality such as a craniocervical junction abnormality, posterior fossa mass, or pituitary tumor. These patients should always have MRI scans. Some patients with exertional headache have a benign disorder that is usually considered a form of migraine. The headaches are often self-limited and respond to indomethacin. Coital headache is usually bilateral, throbbing, and intense. It is more common in men than in women and usually occurs just prior to orgasm. The major differential diagnosis is SAH.
L. Headache not conforming to known functional headache patterns.
Diagnostic Studies
I. LABORATORY STUDIES
In many patients, a diagnosis can be made on clinical grounds alone and treatment can be initiated without further testing. Headache is rarely the sole symptom of serious nervous system disorders. Patients with any of the historical factors discussed in the preceding section or with fever, focal signs, changes in cognition or consciousness, or stiff neck on examination should be evaluated more extensively.
II. BLOOD WORK
Occasionally, routine blood work may provide evidence of infection, anemia, or electrolyte or hormonal abnormalities that are related to headache. The ESR should be checked in all elderly patients with headache due to the possibility of giant cell arteritis. When the ESR is not elevated, other acute phase reactants such as C-reactive protein, haptoglobin, or the platelet count may be increased.
III. IMAGING
Imaging studies are indicated when the clinical pattern suggests the presence of a secondary cause of headache.
A. Uninfused CT is commonly performed with the intent of excluding acute hemorrhage. It is faster than MRI, less expensive and less sensitive to movement artifact. MRI sequences showing susceptibility artifact, such as gradient echo imaging, are also sensitive for acute blood. Catheter angiography is still the gold standard for identifying aneurysms but MR angiography and CT angiography are alternative modalities.
B. MRI is preferable to CT for imaging some lesions in headache patients such as Chiari’s malformations, neoplasm, and sinovenous thrombosis. Radiographic contrast increases the yield of CT in patients with tumor, vascular lesions, inflammatory disorders, and infection. However, there is insufficient evidence that this superiority of MRI is of clinical importance in patients with chronic recurrent headaches.
C. Imaging is unlikely to uncover a significant abnormality in patients with nonacute headache but CT or MRI may reveal abnormalities that are unrelated to the headaches. In a recent meta-analysis of individuals without neurologic symptoms undergoing brain MRI, almost 3% had incidental abnormalities. Evidence-based guidelines suggest that imaging should be considered when there is an unexplained abnormality on physical examination, if the headache is atypical or does not meet criteria for a primary headache disorder or if there is an additional risk factor such as immune deficiency.
D. A history consistent with migraine reduces the risk of abnormal imaging. In Frishberg’s retrospective and prospective review of CT or MRI studies, only 0.4% of patients with migraine and a normal exam had abnormal imaging compared with 2.4% in patients with nonmigrainous headache. White matter changes are relatively common in migraineurs but if extensive, they may raise suspicion of a secondary migraine syndrome such as cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy or a mitochondrial disorder.
E. There are no evidence-based guidelines on the role of imaging in chronic nonmigrainous or tension-type headaches.
IV. LUMBAR PUNCTURE
A. Exclusion of SAH. CT is very sensitive to the presence of subarachnoid blood but the presence of CSF blood or xanthochromia may be diagnostic in patients with a high degree of suspicion and a negative CT.
B. Diagnosis of CNS infection. In patients with suspected encephalitis or meningitis, LP may indicate the presence of CSF pleocytosis. Patients should have an imaging procedure prior to undergoing LP except when bacterial meningitis is strongly suspected, in which case LP should be done immediately to prevent a potentially life-threatening delay in antibiotic therapy.
C. Measurement of CSF pressure. For the patient with chronic headache and signs of increased ICP, such as papilledema or small ventricles, especially in young obese women, idiopathic intracranial hypertension should always be included in the differential diagnosis. When imaging studies exclude a mass lesion, LP should be performed to confirm an elevation of CSF pressure.
D. Diagnosis of carcinomatous meningitis.
E. Cisternal taps. Cisternal puncture may increase the likelihood of diagnosing fungal or tuberculous meningitis, which may primarily affect basal meninges.
V. BIOPSY OF PATHOLOGIC MATERIAL IS INDICATED UNDER CERTAIN CIRCUMSTANCES
A. Diagnosis of giant cell arteritis. Temporal artery biopsy is still the gold standard for diagnosing cranial arteritis. A specimen of adequate length is necessary to avoid sampling error because of skip lesions. The risk of blindness in untreated patients is sufficient to warrant initiation of steroids when the diagnosis is considered. The incidence of positive biopsy results falls dramatically after short trials of steroids, so moving to biopsy rapidly is recommended. There is a modest increase in diagnostic yield by biopsying the contralateral temporal artery if the initial biopsy specimen is negative. Biopsy may be of value in diagnosing other arteritides, such as polyarteritis nodosa, which may involve the temporal artery. Preoperative angiography or ultrasound to select a biopsy site is rarely beneficial because arteriosclerotic changes are common in this age group and can be mistaken for arteritis.
B. Meningeal Biopsy. In patients with chronic meningitis, meningeal biopsy may help establish diagnoses such as granulomatous angiitis, sarcoidosis, or meningeal carcinomatosis.
VI. EEG
EEG is not recommended for routine evaluation of patients with headache, unless associated symptoms suggest a seizure.
![]()
Recommended Readings
Allison MC, Gallagher PJ. Temporal artery biopsy and corticosteroid treatment. Ann Rheum Dis. 1984;43:416–417.
Boes CJ, Matharu MS, Goadsby PJ. Benign cough headache. Cephalalgia. 2002;22:772–779.
Boyev LR, Miller NR, Green WR. Efficacy of unilateral versus bilateral temporal artery biopsies for the diagnosis of giant cell arteritis. Am J Ophthalmol. 1999;128:211–215.
Brightbill TC, Goodwin RS, Ford RG. Magnetic resonance imaging of intracranial hypotension syndrome with pathological correlation. Headache. 2000;40:292–299.
Clarke CE, Edwards J, Nicholt DJ, et al. Imaging results in a consecutive series of 530 new patients in the Birmingham Headache Service. J Neurol. 2010;257:1274–1278.
Dodick DW. Thunderclap headache. J Neurol Neurosurg Psychiatry. 2002;72:6–111.
Evans RW, Armon C, Frohman EM, et al. Assessment: prevention of post-lumbar puncture headaches—report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2000;55:909–914.
Fisher CM. Late-life migraine accompaniments as a cause of unexplained transient ischemic attacks. Can J Neurol Sci. 1980;7:9–17.
Forsyth PA, Posner JB. Headaches in patients with brain tumors: a study of 111 patients. Neurology. 1993;43:1678–1683.
Frishberg BM. The utility of neuroimaging in the evaluation of headache in patients with normal neurologic examinations. Neurology. 1994;44:1191–1197.
Gorelick PB, Hier DB, Caplan LR, et al. Headache in acute cerebrovascular disease. Neurology. 1986;36:1445–1450.
Headache Classification Committee of the International Headache Society. The international classification of headache disorders. Cephalalgia. 2004;24(suppl 1):9–160.
Marcelis J, Silberstein SD. Idiopathic intracranial hypertension without papilledema. Arch Neurol. 1991;48:392–399.
Mathew NT, Ravishankar K, Sanin LC. Coexistence of migraine and idiopathic intracranial hypertension without papilledema. Neurology. 1996;46:1226–1230.
May A, Jurgens TP. Trigeminal-autonomic headaches in daily clinical practice. Expert Rev Neurother. 2006;6:1531–1543.
Medina JL, Diamond S. Cluster headache variant: spectrum of a new headache syndrome. Arch Neurol. 1981;38:705–709.
Mitchell C, Osborn RE, Grosskreutz SR. Computed tomography in the headache patient: is routine evaluation really necessary? Headache. 1993;33:82–86.
Morris Z, Whitely WN, Longstreth WT, et al. Incidental findings on brain magnetic resonance imaging: systematic review and meta-analysis. BMJ. 2009;339:b3016.
Pless M, Rizzo JF 3rd, Lamkin JC, et al. Concordance of bilateral temporal artery biopsy in giant cell arteritis. J Neuroophthalmol. 2000;20:216–218.
Quality Standards Subcommittee of the American Academy of Neurology. Practice parameter: the electroencephalogram in the evaluation of headache. Neurology. 1995;45:1411–1413.
Silberstein SD, Lipton RB, Sliwinski M. Classification of daily and near-daily headaches: proposed revision to the IHS criteria. Headache. 1994;34:1–7.
Silberstein SD for the U.S. Headache Consortium. Practice parameter: evidence-based guidelines for migraine headache (an evidence based review). Neurology. 2000;55:754–762.
Tsushima Y, Endo K. MR imaging in the evaluation of chronic or recurrent headache. Radiology. 2005;235(2):575–579.
Vijayan N, Dreyfus PM. Post-traumatic cephalalgia. Arch Neurol. 1975;32:649–652.
Vijayan N, Watson C. Pericarotid syndrome. Headache. 1978;18:244–254.