This chapter is designed to be a very brief reference for common neurologic emergencies. In general, we presume an accurate diagnosis has been made and mainly concentrate on acute therapy. Although not comprehensive, this guide should allow you to care for a patient with the following problems for the first few hours.
I. ELEVATED INTRACRANIAL PRESSURE
A. Thirty degrees head-up neutral position.
B. Correction of factors exacerbating intracranial pressure (ICP).
1. Hypercarbia.
2. Hypoxia.
3. Hyperthermia.
4. Acidemia.
5. Hypotension.
6. Hypervolemia.
C. Avoid hypotonic solutions.
D. If ICP monitor has been placed, maintain cerebral perfusion pressure at 70 mm Hg.
E. Goal is euvolemia with elevation of osmolality.
F. Mannitol (20% solution) 1.0 g per kg intravenous (IV) as a bolus followed by 0.25 to 0.5 g per kg every 4 to 6 hours, depending on clinical status, serum osmolality (target 310 to 320 mOsm per kg), volume status, and ICP measurements.
G. Consider hypertonic saline 3% solution or 23.4% solution (0.5 to 2.0 cc per kg) through a central line in therapy-resistant elevation of ICP (target serum sodium of 145 to 155 mEq per L).
H. Dexamethasone (if vasogenic edema).
I. Hyperventilation to PaCO2 of 30 to 35 mm Hg (temporizing measure).
1. Typically, it loses effectiveness in 24 to 48 hours.
2. Four percent change in cerebral blood flow for every 1 mm Hg change in PaCO2.
J. Sedation and paralysis if necessary.
K. CSF drainage if necessary.
L. Barbiturates.
M. Hypothermia.
N. Surgical decompression (see Chapter 36).
II. COMA
A. Thorough general and neurologic examination.
B. ABCs: airway, breathing, and circulation.
C. IV fluids: normal saline.
D. Manage hypoglycemia with 50 ml of 50% glucose IV. Consider thiamine 100 mg IV before glucose.
E. Consider naloxone 0.4 to 2.0 mg IV for opioid overdose.
F. Consider flumazenil 0.2 mg IV for benzodiazepine overdose.
G. Arterial blood gases, glucose, electrolytes, calcium, magnesium, phosphorus, blood urea nitrogen, creatinine, liver enzymes, ammonia, CBC, urinalysis, blood and urine toxicology screens, and TSH.
H. If focal neurologic signs, or history of head trauma, consider therapy for elevated ICP with hyperventilation and osmotherapy.
I. Emergency brain imaging: typically unenhanced head CT.
J. Consider lumbar puncture (LP) if suspected CNS infection or suspected subarachnoid hemorrhage (SAH) with normal findings on head CT.
K. EEG.
III. STATUS EPILEPTICUS (GENERALIZED TONIC–CLONIC STATUS EPILEPTICUS)
A. ABCs: airway, breathing, and circulation.
B. IV line with normal saline.
C. Reduce temperatures >39°C with cooling blankets.
D. Consider 100 mg thiamine IV.
E. Consider 50 ml of 50% glucose IV.
F. Lorazepam 0.1 mg per kg IV at 2 mg per minute, maximum of 8 mg in adults or diazepam 0.2 mg per kg IV at 5 mg per minute up to a total dose of 20 mg.
G. Phenytoin 20 mg per kg IV (at <150 mg per minute in adults) or fosphenytoin 20 mg per kg IV (up to 150 mg phenytoin equivalent per minute).
H. If seizures continue, give additional bolus of phenytoin 10 mg per kg or fosphenytoin 10 mg per kg (to a maximum of 30 mg per kg).
I. Intubation, airway protection, and possibly ventilatory support.
J. If seizures persist, administer one of the following IV:
1. Midazolam (Load 0.2 mg per kg; repeat 0.2 to 0.4 mg per kg boluses every 5 minutes until seizure stops. Maximum loading dose 2 mg per kg.)
2. Propofol (Load 1 mg per kg; repeat 1 to 2 mg per kg boluses every 3 to 5 minute until seizures stop. Maximum loading dose 10 mg per kg.)
3. Valproate (Load 40 mg per kg over 10 minute. If seizures persist, 20 mg per kg over 5 minute.)
4. Phenobarbital (load 20 mg per kg, at 50 to 100 mg per minute).
K. If seizures still continue, use IV pentobarbital.
1. Loading with 5 to 10 mg per kg IV. Rate 50 mg per minute. Maintenance 1 to 3 mg/kg/hour.
2. Goal is burst-suppression pattern on EEG.
L. Management of intercurrent medical complications.
IV. BACTERIAL MENINGITIS
A. Treat within 30 minutes of arrival for medical care.
B. Manage elevated ICP.
C. Control seizures.
D. Manage complications (subdural empyema, brain abscess, ventriculitis, acute hydrocephalus, vasculitis, vascular spasm, venous thrombosis, and hyponatremia due to SIADH) (Fig. 58.1).
E. No universally accepted standard for duration of treatment.
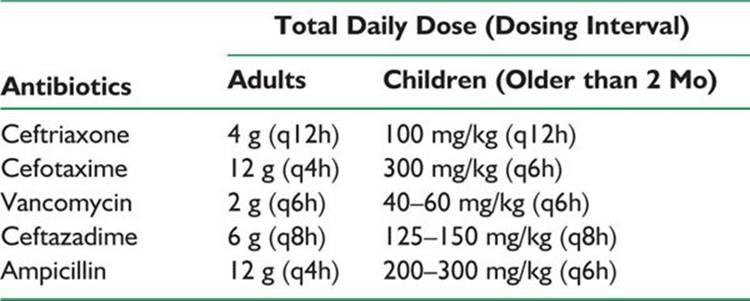
F. Empiric antibiotic treatment of immunocompetent patients with community-acquired meningitis: ceftriaxone or cefotaxime plus vancomycin plus dexamethasone 0.15 mg per kg IV every 6 hours for 4 days (American Academy of Pediatrics recommendation for infants and children—first dose to be given before or within 4 hours of antibiotic). See Table 58.1 for antibiotic doses.
G. Consider ceftazidime if Pseudomonas infection is suspected.
H. Consider ampicillin if Listeria infection is suspected, as in an immunocompromised host.
I. Consider doxycycline if Rickettsia, Anaplasma, Ehrlichia, or Coxiella burnetii is suspected.
J. Chemoprophylaxis of meningococcal and Haemophilus influenzae infection with rifampin.
V. HERPES SIMPLEX ENCEPHALITIS
A. Fluid and ICP management.
B. Seizure control.
C. Acyclovir IV 10 mg per kg every 8 hours for 14 to 21 days; adjust dose to patient’s renal function.
D. Untreated has a mortality rate of 70%.
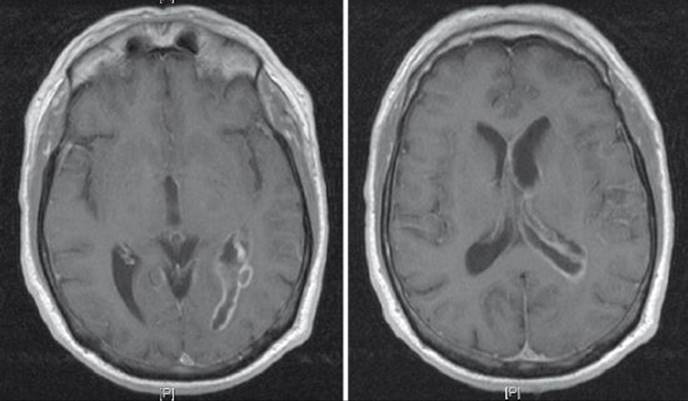
FIGURE 58.1 Axial T1-weighted MR images demonstrate diffuse abnormal enhancement extending along the ependymal surface of the left lateral ventricle and third ventricle consistent with ventriculitis/ependymitis in a 65-year-old man with Streptococcus constellatus meningitis.
TABLE 58.1 Antibiotic Therapy for Bacterial Meningitis
VI. BRAIN ABSCESS
A. If there is no clear etiologic factor, administer ceftriaxone (Table 58.1) plus vancomycin (Table 58.1) plus metronidazole 500 mg every 6 hours in adults and 7.5 mg per kg every 8 hours in children.
B. Sulfa drugs for Nocardial infection.
C. Ceftazidime if Gram-negative aerobes are suspected.
D. Surgical treatment.
VII. CEREBRAL TOXOPLASMOSIS
A. Usually CD4 counts <200 cells per mm3.
B. Pyrimethamine: loading dose of 100 to 200 mg then 75 to 100 mg per day plus folinic acid 10 to 15 mg per day plus sulfadiazine 6 to 8 mg per day.
C. If patient is allergic to sulfa drugs, substitute clindamycin 2,400 to 4,800 mg per day.
VIII. ISCHEMIC STROKE: WITHIN 3 HOURS OF ONSET
A. Unenhanced head CT does not show intracranial hemorrhage.
B. IV t-PA (Alteplase) 0.9 mg per kg, maximum dose of 90 mg. Ten percent of dose as initial bolus over 1 minute, and rest of dose infused over 60 minutes.
C. Exclusion criteria.
1. Minor or rapidly improving neurologic deficits (relative contraindication).
2. Seizure at the onset of symptoms (if residual impairments are postictal).
3. Symptoms suggestive of SAH.
4. Systolic blood pressure ≥185 mm Hg or diastolic blood pressure ≥110 mm Hg after two attempts to reduce blood pressure.
5. Stroke or serious head trauma in the previous 3 months.
6. Major surgery in the previous 14 days.
7. History of intracranial hemorrhage.
8. Gastrointestinal or genitourinary bleeding in the last 21 days.
9. Arterial puncture at a noncompressible site in the previous 7 days.
10. Received heparin therapy within the preceding 48 hours, and the aPTT is elevated.
11. INR >1.7 or prothrombin time (PT) >15 seconds.
12. Platelet count <100,000 per μl.
13. Glucose level <50 mg per dl (<2.7 mmol per L).
14. Myocardial infarction in the previous 3 months.
D. No antiplatelet agents or anticoagulants within first 24 hours of treatment.
E. Blood pressure must be maintained <180 per 105 mm Hg during and after treatment with tPA.
IX. ISCHEMIC STROKE 3 TO 4.5 HOURS FROM SYMPTOM ONSET
A. Exclusion criteria.
1. In addition to above (VIII C.) exclusion criteria:
a. >80 years old.
b. NIHSS >25.
c. Combination of previous stroke and diabetes mellitus.
d. On anticoagulant therapy regardless of INR.
e. CT scan with low attenuation area of >one-third of the middle cerebral artery territory.
X. PERIOPERATIVE ACUTE ISCHEMIC STROKE WITHIN 14 DAYS OF SURGICAL PROCEDURE
A. IV thrombolysis contraindicated.
B. No CT exclusion.
C. Six hours in carotid artery territory.
D. Twelve hours or more in basilar artery occlusive disease.
E. Consider intra-arterial thrombolysis. IA tPA 1 to 5 mg bolus followed by 0.1 to 0.2 mg/kg/hour for 1 to 2 hours.
F. Consider mechanical clot disruption in high-risk surgery patients.
XI. MANAGEMENT OF INTRACRANIAL BLEEDING AFTER THROMBOLYTIC THERAPY
A. Stop infusion of thrombolytic.
B. Hematocrit, hemoglobin, PT/INR, aPTT, platelet count, fibrinogen, and type and cross match.
C. Emergency unenhanced head CT.
D. Ten units of cryoprecipitate containing factor VIII.
E. Six to eight units of platelets.
F. Hematology and neurosurgery consultations.
G. Surgery only after stabilization of intracranial bleeding.
XII. MANAGEMENT OF INTRACRANIAL BLEEDING ASSOCIATED WITH WARFARIN
A. Discontinue warfarin (Fig. 58.2).
B. Vitamin K1 10 mg subcutaneously or 10 to 20 mg slow IV injection.
C. Fresh frozen plasma 10 to 15 ml per kg or prothrombin complex concentrate (15 to 50 units of factor IX per kg body weight) containing high concentrations of the vitamin K-dependent coagulation factors II, VII, IX, and X.
D. Neurosurgery consultation.
E. Recombinant FVIIa not routinely recommended.
XIII. MANAGEMENT OF INTRACRANIAL BLEEDING ASSOCIATED WITH HEPARIN
A. Discontinue heparin.
B. Protamine sulfate for every 1 mg/100/U of heparin administered in the preceding 4 hours.
C. Dose adjustment according to elapsed time from last heparin dose.
1. 20 to 60 minutes: 0.5 to 0.75 mg per 100 U of heparin.
2. 60 to 120 minutes: 0.375 to 0.5 mg per 100 U of heparin.
3. >120 minutes: 0.25 to 0.375 mg per 100 U of heparin.
D. Slow IV infusion; not to exceed 50 mg per 10 minute.
XIV. SUBARACHNOID HEMORRHAGE
A. Unenhanced head CT.
B. LP, if head CT is normal.
C. Four-vessel catheter cerebral angiography or CT angiography (less invasive alternative).
If renal insufficiency:
1. Normal saline 1 ml/kg/hour before and after angiography.
2. Acetylcisteine 600 mg orally twice daily for 2 days.
D. Blood pressure management (avoid nitroprusside/nitroglycerin; may use labetalol); maintain normotensive range.
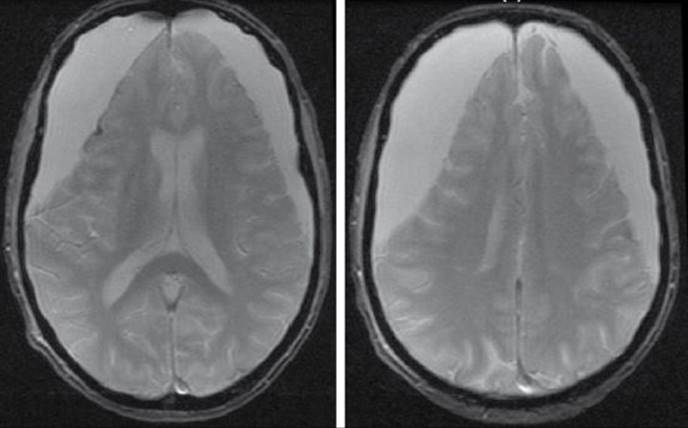
FIGURE 58.2 Axial gradient echo MRI shows large bilateral chronic subdural hematomas (SDH). The right-sided SDH is slightly larger than the left. There is approximately a 2 mm of right-to-left subfalcine shift. There is also evidence of previous hemorrhage along the lateral cortical surface of the right frontal lobe. The patient was an 83-year-old man with atrial fibrillation, on warfarin, who reported a subacute history of memory loss. INR on admission was 2.4.
E. Avoid hypotension and hypovolemia.
F. Nimodipine 60 mg every 4 hours by mouth or NG tube for 21 days.
G. Sedation, bedrest, analgesics, and stool softeners.
H. Prophylactic antiepileptic drugs (debatable).
I. Management of elevated ICP.
J. DVT prophylaxis.
1. Pneumatic compression boots.
2. May use subcutaneous UFH 5,000 units three times daily once aneurysm clipped.
K. Management of complications (rebleeding, hydrocephalus, vasospasm, and hyponatremia due to cerebral salt wasting or SIADH).
L. Antifibrinolytic therapy (epsilon aminocaproic acid or tranexamic acid) reduces risk of rebleeding but increases risk of cerebral ischemia.
M. Neurosurgery consultation (clipping versus coiling).
XV. CEREBELLAR HEMORRHAGE
A. ABCs: airway, breathing, and circulation.
B. Neurosurgery consultation (Fig. 58.3).
C. Ventriculostomy for acute hydrocephalus.
D. Consider craniotomy with removal of hemorrhage.
XVI. METASTATIC EPIDURAL SPINAL CORD COMPRESSION
A. Emergency MRI.
B. If MRI not available or contraindicated—CT myelography.
C. Dexamethasone: optimal dose uncertain (16 to 100 mg).
D. Radiation therapy (within 24 hours).
E. Consider surgical intervention:

FIGURE 58.3 CT head without contrast demonstrates acute intraparenchymal hemorrhage of the left cerebellar hemisphere with effacement of the fourth ventricle and subsequent hydrocephalus of the third and lateral ventricles. The patient underwent placement of a right frontal external ventricular drain and a suboccipital craniotomy with bilateral decompression and removal of intracerebellar clot.
1. If worsening deficits during or following radiotherapy.
2. If radioresistant tumor.
3. If spinal instability.
F. Pain control with opioids.
G. Venous thromboembolism prophylaxis for nonambulatory patients.
H. Bowel program.
XVII. CENTRAL CORD SYNDROME
A. Hyperextension traumatic injury in patients with longstanding cervical spondylosis.
B. Other associations.
1. Cervical spine fracture dislocations.
2. Congenital or acquired cervical canal stenosis.
3. Central spinal cord bleeding.
C. Disproportionate upper motor neuron pattern of weakness—upper limbs >> lower limbs.
D. Muscle stretch reflexes initially absent.
E. Bladder dysfunction.
F. Variable sensory loss below injury level.
G. IV methylprednisolone.
H. Surgery rarely indicated.
I. Favorable prognosis.
XVIII. GUILLAIN–BARRÉ SYNDROME
A. Nerve conduction studies including F waves.
B. CSF for albuminocytologic dissociation.
C. Endotracheal intubation if respiratory compromise: forced vital capacity (FVC) <15 ml per kg.
D. Monitoring for autonomic disturbances.
E. Plasma exchange: total 200 to 250 ml per kg over 1 to 2 weeks or immunoglobulin 0.4 g per kg IV per day for 5 days.
XIX. MYASTHENIC CRISIS
A. Careful monitoring of airway, swallowing, and respiration.
B. Intubation when FVC <15 ml per kg.
C. Optimize anticholinesterase dose.
1. If there is concern about anticholinesterase toxicity, stop anticholinesterase.
D. Manage concurrent infections.
E. Plasma exchange or immunoglobulin 0.4 g per kg IV a day for 5 days.
XX. ACUTE DYSTONIC REACTION
A. Stop causative agent.
B. Diphenhydramine 50 mg IV.
C. Benztropine 1 to 2 mg IV.
D. Typically follow with oral anticholinergic agent for 2 weeks, especially if long-acting dopamine receptor blocking agent was causative agent.
XXI. NEUROLEPTIC MALIGNANT SYNDROME
A. Immediate withdrawal of all neuroleptics or dopamine-depleting agents or reinstitution of previously withdrawn dopaminergic therapy.
B. Hydration and maintenance of adequate urine flow.
C. Alkalinization of urine if myoglobinuria.
D. Lowering of elevated body temperature.
E. Bromocriptine 2.5 to 5.0 mg four times a day, increase four times a day dose until response occurs (maximum 50 mg per day).
F. Dantrolene 1 to 10 mg per kg a day in divided doses.
G. Other possible agents for treatment include amantadine and carbamazepine.
H. For severe psychosis during treatment, consider electroconvulsive therapy.
I. Monitoring for complications.
XXII. ACUTE SEROTONIN SYNDROME
A. Discontinue all serotonergic drugs.
B. Benzodiazepines—especially for agitation.
C. Cyproheptadine 12 to 32 mg per day. Consider initial dose in adults of 12 mg and maintenance dose of 8 mg every 6 hours.
D. Other possible treatments include propranolol, chlorpromazine, and methysergide (not available in the United States).
E. Monitoring for complications.
XXIII. GIANT CELL ARTERITIS, TEMPORAL ARTERITIS
A. STAT erythrocyte sedimentation rate.
B. Oral prednisone 1 to 2 mg per kg every day or 1 g per day methylprednisolone IV for 3 days followed by oral prednisone 1 mg per kg a day, especially if there are visual symptoms or visual loss.
C. Long segment superficial temporal artery biopsy.
XXIV. CENTRAL RETINAL ARTERY OCCLUSION
A. Ocular massage.
B. Breathing 95% oxygen and 5% carbon dioxide.
C. Lowering of intraocular pressure with acetazolamide intravenously or orally.
D. Anterior chamber paracentesis.
E. Aspirin.
F. Consider intraarterial thrombolysis (<12 hours).
XXV. WERNICKE’S ENCEPHALOPATHY
A. Thiamine deficiency state—chronic alcoholism, hyperemesis gravidarum, starvation, gastrointestinal malignancies, pyloric stenosis, anorexia nervosa, inappropriate parenteral nutrition, digitalis intoxication, chronic hemodialysis, drug therapy for obesity, and thyrotoxicosis.
B. Global confusional state.
C. Ataxic gait.
D. Ocular abnormalities.
1. Nystagmus.
2. CN VI palsy.
3. Gaze palsy.
4. Vestibular paresis.
E. 100 mg thiamine IV.
F. Bed rest.
G. Nutritional supplements.
H. Avoid glucose without thiamine.
![]()
Recommended Readings
Adams HP Jr, del Zoppo G, Alberts MJ, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. American Heart Association/American Stroke Association Stroke Council; American Heart Association/American Stroke Association Clinical Cardiology Council; American Heart Association/American Stroke Association Cardiovascular Radiology, and Intervention Council; Atherosclerotic Peripheral Vascular Disease Working Group; Quality of Care Outcomes in Research Interdisciplinary Working Group. Stroke. 2007;38(5):1655–1711.
Benderson JB,Connolly ES Jr, Batjer HH, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke. 2009;40(3):994–1025.
Biller J, Chair. Asconapé J, Kase CS, et al. Iatrogenic neurology. Continuum. 2001;7:1–224.
Caroff SN, Campbell EC, Sullivan KA. Neuroleptic malignant syndrome in elderly patients. Expert Rev Neurotherapeutics. 2007;7(4):423–431.
Chamberlain MC, Kornanik PA. Epidural spinal cord compression: a single institution’s retrospective experience. Neuro-oncology. 2000;192:120–123.
Diringer MN, Zazulia AR. Osmotic therapy: fact and fiction. Neurocrit Care. 2004;1:219–233.
Johnson RT, Griffin JW, eds. Current Therapy in Neurologic Disease. 5th ed. St Louis, MO: Mosby; 1997.
Morgenstern LB, Hemphill JC III, Anderson C, et al. Guidelines for the management of spontaneous intracerebral hemorrhage: a guideline for health professionals from the American Heart Association/American Stroke Association. Stroke. 2010;41:2108–2129.
Qureshi Al, Thurim S, Broderick JP, et al. Spontaneous intracerebral hemorrhage. N Engl J Med. 2001;344:1450–1460.
Rabinstein AA, Wijdicks E. Tough Calls in Acute Neurology. Boston, MA: Butterworth-Heinemann; 2004.
Roos K, ed. Central Nervous System Infectious Diseases and Therapy. New York, NY: Marcel Dekker; 1997.
Ropper AH, ed. Neurological and Neurosurgical Intensive Care. 3rd ed. New York, NY: Raven Press; 1993.
Rosovsky RP, Crowther MA. What is the evidence for the off-label use of recombinant Factor VIIIa (rFVIIa) in the acute reversal of warfarin? ASH evidence-based review 2008. Hematology Am Soc Hematol Educ Program. 2008:36–38.
Stochetti N, Maas AL, Chieregato A, van der Plas AA. Hyperventilation in head injury: a review. Chest. 2005;127:1812–1827.
Wasterlain CG, Treiman DM, eds. Status Epileptic Mechanisms and Management. Cambridge, MA: MIT Press;2006.
Wijdicks E. Neurologic Catastrophes in the Emergency Department. Boston, MA: Butterworth-Heineman; 2000.