This chapter focuses on primary sleep disorders described in the second edition of the International Classification of Sleep Disorders (ICSD). The greatest difficulties in approaching patients with sleep disorders often relates to an incomplete sleep history, as only a few diagnoses require formal polysomnography (PSG). Nevertheless, the patient usually cannot recall a pathologic event that occurs during sleep, and as such, an attempt to substantiate the sleep history with a bed partner, family member, or close associate should be made.
I. GENERAL APPROACH
A. The sleep history. What is the sleeping environment and bedtime routine? When is bedtime (regular or irregular)? What is the sleep latency (the time to fall asleep “after the head hits the pillow”)? What is the sleep quality? Is it restful or restless and, if restless, why? How many arousals occur per night and for what reasons? What is the final awakening time? Is assistance in waking necessary? How does the patient feel on waking? How many hours of sleep are needed for refreshment? Does the patient nap, and, if so, how often, how long, and how does the person feel after the nap (refreshed, unchanged, and worse)? Does the patient experience excessive daytime sleepiness (EDS) or frank sleep attacks? A 2-week sleep diary, started prior to the initial clinic appointment, can diagnose disorders like inadequate sleep hygiene; a problem in 1% to 2% of adolescents and young adults, and in up to 10% of the sleep-clinic population that presents with insomnia (Fig. 9.1).
1. The degree of sleepiness can rate the severity of any sleep disorder through operational definitions: mild—sleepiness that impairs social or occupational performance during activities that require little attention (reading or watching television); moderate—sleepiness that impairs performance during activities that require some attention (meetings and concerts); and severe—sleepiness that impairs performance during activities that require active attention (conversing or driving).
2. Subjective measure scales, such as the Epworth Sleepiness Scale, can be used to qualify, quantify, and follow problems with sleepiness (Fig. 9.2). Chronically sleep-deprived persons can underestimate their sleepiness. Over time they lose the reference point from which to make comparisons and forget what it feels like to be fully rested. In such cases, excessive sleepiness can be reported as memory loss, slow mentation, and amnestic periods with automatic behavior.
B. The wake history. A history of insomnia and EDS can lead to, exacerbate, or result from a variety of medical and mental disorders, and from drug or substance use/abuse.
II. TYPES OF SLEEP DISORDERS
A. Insomnia. The ICSD criteria demand a history of difficulty initiating or maintaining sleep, or of waking up too early, or sleep that is chronically nonrestorative or poor in quality, and that the problem occurs despite adequate opportunity and circumstances for sleep. It also requires subsequent daytime impairment evidenced by at least one of the following: sleepiness, fatigue, malaise, impaired attention, concentration, or memory, social, vocational, or school dysfunction, tension, mood disturbance, reduced motivation, energy, or initiative reduction, errors or accidents at work or driving, headache, or gastrointestinal symptoms.
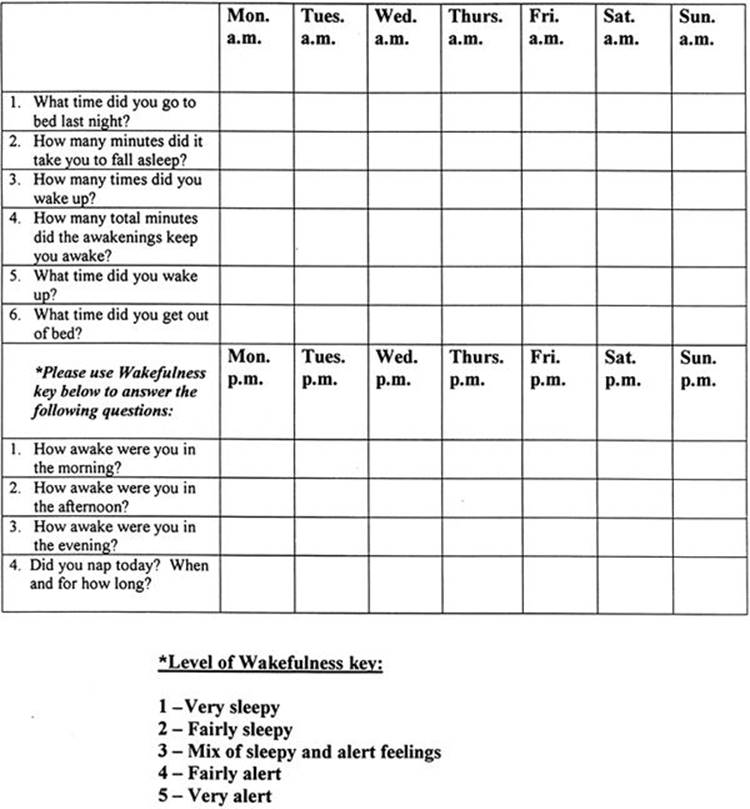
FIGURE 9.1 Example of a typical week-at-a-glance sleep diary.
1. Adjustment (acute) insomnia. This occurs in response to a clearly identifiable stressor and is expected to resolve when the stress ends or the patient adapts. Adjustment insomnia is often associated with anxiety and depression related to the specific stressor. The 1-year prevalence in adults is 15% to 20%, it is more common in women and older adults, and it may predispose to maladaptive behaviors and more persistent forms of insomnia.
2. Psychophysiological insomnia. This is a conditioned insomnia due to learned, sleep-preventing associations. It can represent persistent adjustment insomnia, where an external (or internal) stressor leads to a state of arousal “racing mind” in association with bedtime at home (patients often sleep better in the sleep lab; the “reverse first-night effect”). This affects 1% to 2% of the general population, is more frequent in women and adolescents, and is rare in children.
3. Paradoxical insomnia. Patients complain of severe insomnia with no objective evidence of disturbed sleep or daytime impairment. PSG studies show that these individuals overestimate their sleep latencies and underestimate their sleep times. Patient concerns are not alleviated when they are presented with these objective findings. High-frequency activity on EEG power-density measures may alter sleep perception in this patient population. Paradoxical insomnia occurs in <5% of insomniacs, is more common in women and young to middle-aged adults, and may be associated with neuroticism and depressive traits.
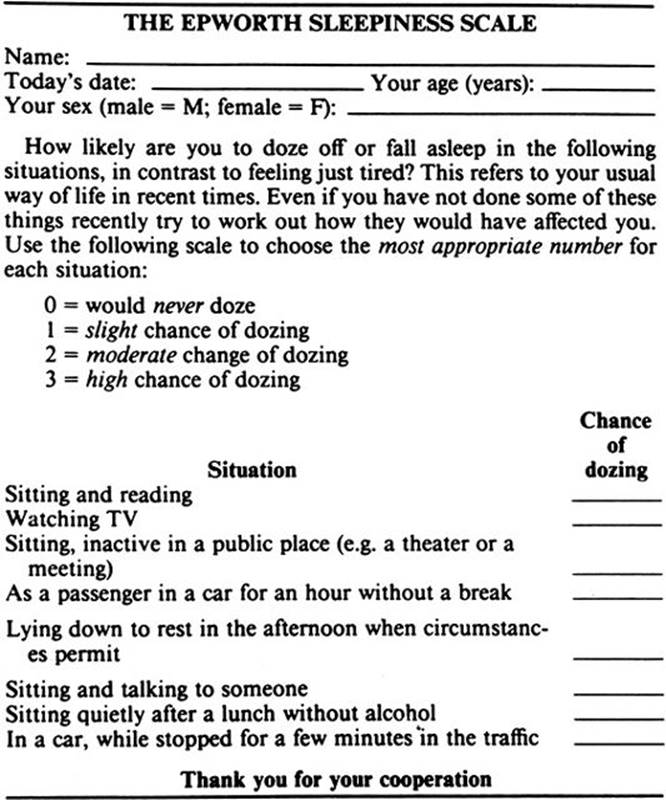
FIGURE 9.2 The Epworth sleepiness scale. A score of 10 or greater suggests excessive daytime sleepiness. (With permission from Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14:540–545.)
4. Idiopathic insomnia. This lifelong disorder is reported in 1% of young adults, begins in infancy or early childhood. It has no known precipitators or major psychological concomitants, but may be associated with attention deficit hyperactivity disorder (ADHD) and dyslexia. A genetic abnormality in sleep/wake mechanisms is suspected. PSG often shows reduced body movements despite severely disturbed sleep.
5. Insomnia due to mental disorder, not due to substance or known physiological condition. In this diagnosis, insomnia is a symptom of a mental disorder, but its severity demands treatment as a distinct problem, which often improves the underlying mental disorder. Major depression is frequently associated with insomnia and reduced rapid eye movement (REM) sleep latency, but PSG is not needed for diagnosis.
6. Inadequate sleep hygiene. This presents as a primary or secondary diagnosis in over 30% of sleep-clinic patients. It involves two categories of habits inconsistent with good sleep: practices that produce increased arousal (e.g., caffeine and nicotine use) and practices that are inconsistent with the principles of sleep organization (variable bedtime and awakening times). Important factors can include engaging in mentally or physically stimulating activities too close to bedtime and failure to maintain a comfortable sleeping environment.
7. Behavioral insomnia of childhood. There are 2 types seen in up to 30% of children (possibly more frequent in boys) after 6 months of age. Sleep-onset association type occurs with dependency on a specific stimulation, object, or setting for sleep. Sleep-onset associations are extremely prevalent and are only a disorder if highly problematic. Limit-setting type occurs with bedtime stalling, or refusal in toddlers and preschoolers. This problem is often due to poor practices of the caregiver.
8. Insomnia due to drug or substance. This is suppression or disruption of sleep during consumption; or exposure to a drug, food, or toxin; or upon its discontinuation. This affects 0.2% of the general population and 3.5% of those presenting to formal sleep-clinics. The PSG in chronic alcohol withdrawal can reveal light and fragmented sleep that may persist for years.
9. Insomnia due to medical condition and physiological (organic) insomnia. Disorders that cause discomfort (comfort is necessary for normal sleep) and neurodegenerative problems (with disruption of normal central sleep/wake mechanisms; poorly formed or absent sleep spindles are common) are representative of many possible etiologies. This diagnosis should only be considered when insomnia causes marked distress and warrants specific attention.
B. Sleep-related breathing disorders (SRBDs). In addition to the wake/sleep history, PSG is required in diagnosing SRBDs. PSG is the combined sleep monitoring of EEG, electromyography (EMG), electrooculography (EOG), and physiologic measures that include airflow, respiratory effort, and oxygen saturation (SaO2). PSG differentiates four sleep stages—non-REM (NREM) stages N1, N2, and N3, and REM (stage R). An obstructive apnea is a drop in airflow by ≥90%, in association with continued inspiratory effort, for ≥10 seconds in adults, or the duration of 2 baseline breaths in children. A central apnea is an absence of inspiratory effort for ≥10 seconds in adults, or, in children, for 20 seconds, or the duration of 2 baseline breaths in association with an arousal, awakening, or a ≥3% SaO2 reduction. A mixed apnea occurs when there is initially absent inspiratory effort, followed by resumption of inspiratory effort in the second part of the event. Hypopneas in adults occur with a ≥10 second period of reduced airflow of ≥30% or ≥50%, with respective SaO2 reductions of ≥4% or ≥3% (or an associated arousal). In children, a hypopnea requires a ≥50% fall in airflow for a duration of 2 baseline breaths, in association with an arousal, awakening, or ≥3% SaO2 reduction. Severity of a SRBD is suggested by the apnea–hypopnea index ([AHI]; the average number of apneas and hypopneas per hour of sleep). In adults, an AHI of 5 to 15 is considered mild; 15 to 30, moderate; and >30, severe.
1. Central sleep apnea (CSA) syndromes.
a. Primary CSA. This idiopathic disorder is more frequent in middle aged to elderly males, associated with low normal waking PaCO2 (<40 mm Hg), and high chemoresponsiveness (evidenced as central apneas) to the normal rise in PaCO2 that occurs in sleep. It is significant when there are complaints of EDS, insomnia, or arousals with shortness of breath, and the PSG shows an AHI ≥ 5.
b. Cheyne–Stokes’ breathing pattern (CSBP). PSG defines CSBP as at least 3 consecutive cycles of a cyclic crescendo and decrescendo change in breathing amplitude, with a central AHI of ≥5 and/or a cyclic crescendo and decrescendo change of ≥10 consecutive minutes. CSBP is most prominent in NREM sleep (usually absent or attenuated in REM). It occurs predominately in men >60 years of age, with a prevalence up to 45% in the congestive heart failure (CHF) population, and in 10% of strokes. CHF (a poor prognostic sign), stroke, and possibly renal failure are the most important precipitating factors.
c. High-altitude periodic breathing. This is an acute response to a relatively rapid ascent to altitudes ≥4,000 m, where (usually the first night) there are recurrent central apneas in NREM sleep that alternate with hyperpneas in cycles of 12 to 34 seconds (often leading to frequent arousals with shortness of breath and EDS). This is considered a normal, and transient, adaptive phase to higher altitudes.
d. CSA due to medical condition (not Cheyne–Stokes) and due to drug or substance. A majority of the medical conditions with CSA are associated with brainstem lesions, cardiac, or renal disorders. Regular use (>2 months) of long-acting opioids (methadone, time-release morphine, and hydrocodone), can lead to CSA (often in association with obstruction, hypoventilation, and periodic breathing). The presumed etiology is from an effect on μ-receptors on the ventral surface of the medulla.
e. Primary sleep apnea of infancy (apnea of prematurity <37 weeks conceptual age, apnea of infancy ≥37 weeks, ≤1 year conceptual age). Central, mixed, obstructive apneas or hypopneas (most notably in active/REM sleep) associate with signs of physiologic compromise (hypoxemia, bradycardia, the need for resuscitative measures), but progressively decrease as the patient matures during the early weeks of life. The prevalence varies inversely with conceptual age (in 84% of infants <1,000 g, and <0.5% of full-term newborns), as it is related to developmental immaturity of brainstem respiratory centers. This has not been established as an independent risk factor for sudden infant death syndrome.
2. Obstructive sleep apnea (OSA) syndromes. OSA is associated with repeated episodes of upper airway obstruction. From 30 to 60 years of age, the prevalence ranges from 9% to 24% for men and 4% to 9% for women. Obstructions often result in oxygen desaturation, elevation in PaCO2, and arousals, which disrupt sleep continuity and can lead to EDS. This syndrome often occurs among sleepy, middle-aged, overweight men with insomnia who snore. Premenopausal women are less commonly affected. This disorder also has been associated with systemic and pulmonary hypertension, nocturnal cardiac arrhythmia and angina, gastroesophageal reflux, nocturia, and an overall reduction in quality of life. Predisposing factors include familial tendencies, redundant pharyngeal tissue (e.g., adenotonsillar hypertrophy), craniofacial disorders (e.g., micrognathia, retrognathia, and nasal obstruction), endocrinopathy (e.g., acromegaly and hypothyroidism with myxedema), and neurologic disease.
a. OSA, adult.
(1) History. The patient or bed partner often reports restless, unrefreshing sleep and sleep maintenance insomnia with arousals associated with gasping, choking, or heroic snoring, possibly exacerbated by fatigue, alcohol, weight gain, or the supine sleeping position. Snoring may force the person to sleep alone and persist even when sitting. Although patients may not report daytime sleepiness, problems with fatigue, memory, and concentration are frequent. A family history of similar problems should be carefully sought.
(2) Examination. The blood pressure, body mass index (BMI = weight in kilograms per square meter of height) and neck and waist circumference should be documented, as hypertension and obesity may relate to OSA. Of general concern (following western standards) are a BMI ≥30 kg per m2, a neck circumference of >40 cm, and a waist circumference (often measured at the iliac crest) >102 cm in men, and >88 cm in women. These are frequent signs in OSA that may predict comorbidities in the metabolic syndrome, heart disease, and stroke. Oral and nasopharyngeal patency and abnormalities of the tonsils, adenoids, tongue, soft and hard palate, uvula, nasal septum, turbinates, and temporomandibular joint as well as fatty infiltration of soft tissues in the upper airways should be documented.
(3) PSG. Recurrent obstructions often result in microarousals/arousals, which contribute to EDS (however, the frequency of events correlates poorly with sleepiness severity). Events generally appear worse in the supine position and during REM sleep. Tachy-brady cardiac arrhythmias and asystole may be documented. The diagnosis of OSA is considered with an AHI ≥5, when there is at least one symptom that may include EDS, insomnia, arousals with shortness of breath or choking, and witnessed loud snoring or apneas. The diagnosis can also be given with an AHI ≥15 in the absence of symptoms.
(4) Differential diagnosis. Loud snoring and respiratory effort related arousals (RERA), as part of the upper airway resistance syndrome (UARS), can lead to EDS with no PSG evidence of OSA (as RERA are pathophysiologically similar to obstructions). During PSG, defining RERA requires esophageal balloon (or nasal pressure/inductance plethysmography) monitoring that reveals ≥10 second episodes of, respectively, increasing negative pressure, or flattening of nasal pressure waveforms (that correspond to increased respiratory effort), which terminate with arousal.
(5) Other tests. In severe cases, an interdisciplinary approach may necessitate ECG, chest radiography, echocardiography, and pulmonary function tests (addressing pulmonary hypertension and right ventricular hypertrophy), cephalometric evaluations of the upper airways, and extensive cerebrovascular assessments.
b. OSA, pediatric. The prevalence of OSA is 2% in the general pediatric population, with girls and boys being affected equally, but with a higher prevalence in African American relative to Caucasian children. Some children may have OSA breathing patterns similar to adults, nevertheless, younger children may be prone to obstructive hypoventilation (long periods of persistent partial upper airway obstruction).
(1) History. Snoring and difficulty breathing are common; often with reports of associated neck hyperextension and diaphoresis. Cognitive and behavioral complications (ADHD) are frequent, with EDS being reported especially in older children.
(2) Examination. Children with OSA generally have relatively large tonsils and adenoids, and obesity is becoming more common. Pectus excavatum may result from chronic paradoxical respirations. Patients with craniofacial abnormalities, Down’s syndrome, neuromuscular diseases, cerebral palsy, gastroesophageal reflux (with upper airway edema), mucopolysaccharidosis, sickle cell disease, or who are post cleft palate repair may be prone to OSA.
(3) PSG. Even relatively short obstructions may lead to severe hypoxemia as children have faster respiratory rates with lower functional residual capacities than adults. OSA in children is defined by an AHI ≥1.
(4) Differential diagnosis. In children UARS and RERA can be diagnosed when snoring (or noisy breathing, elevated end-tidal CO2/transcutaneous PCO2, or increased work of breathing) is associated with esophageal pressure monitoring that shows a progressive increased inspiratory effort, or the nasal pressure sensor amplitude falls <50% of baseline with waveform flattening, for a duration of at least 2 baseline breaths.
c. Sleep-related hypoventilation/hypoxemia syndromes. These syndromes often coexist with elements of OSA and CSA.
(1) PSG. Hypoventilation appears as prolonged periods (often several minutes or longer) of reduced respiratory effort (shallow breathing) associated with sustained SaO2 desaturations, with a ≥10 mm Hg increase in PaCO2(with an absolute value that is often >45 mm Hg) in comparison to awake supine values, in the relative absence of obstructive and central events. An arterial blood gas (ABG) that reveals an elevated PaCO2 immediately upon awakening is suggestive of hypoventilation. Alternatives are being investigated as clinically it is impractical to obtain ABGs during sleep. Although there is presently insufficient evidence to allow specification of sensors, both end-tidal and transcutaneous CO2 monitors can be used for surrogate measures of PaCO2 if there is demonstration of reliability and validity within the testing laboratory.
(a) Sleep related nonobstructive alveolar hypoventilation, idiopathic. Sleep related nonobstructive alveolar hypoventilation, idiopathic is postulated to result from a lesion of medullary chemoreceptors, leading to periods (often worse in REM sleep) of decreased tidal volume lasting several minutes with sustained SaO2 desaturations and elevated carbon dioxide levels. This often presents in adolescents or young adults.
(b) Congenital central alveolar hypoventilation syndrome. Similar to sleep related nonobstructive alveolar hypoventilation, idiopathic, the congenital central alveolar hypoventilation syndrome can lead to polycythemia, pulmonary hypertension, heart failure and death. It is a rare congenital genetic disease (most cases due to de novo mutations in the PHOX2B gene) associated with failure of automatic central control of breathing, usually evident at birth, and requiring intubation. Patients may progress to adequate waking breathing, although some need continuous ventilatory support. The congenital central alveolar hypoventilation is often associated with Hirschsprung’s disease, autonomic dysfunction, neural tumors, dysphagia, and hypoventilation that may appear worse during slow wave (stage N3) sleep.
(c) Sleep-related hypoventilation/hypoxemia due to pulmonary parenchymal or vascular pathology. This occurs when disease has been documented using pulmonary function tests, radiography, echocardiography, pulmonary artery catheter measurements, and hemoglobin studies. Associated diseases include interstitial lung diseases, pulmonary hypertension, sickle cell anemia, and cystic fibrosis. Worse pulmonary function and a lower waking SaO2 increases the risk for sleep hypoventilation/hypoxemia, and subsequent polycythemia and cardiac dysrhythmias. PSG findings are generally worse in REM sleep, and include an SaO2 <90% for >30% of the total sleep time.
(d) Sleep-related hypoventilation/hypoxemia due to lower airways obstruction. This occurs in disorders with obstruction or increased airflow resistance below the larynx, such as chronic obstructive pulmonary disease ([COPD]; chronic bronchitis and emphysema), bronchiectasis, cystic fibrosis, and α-1 antitrypsin deficiency. The greatest risk factor for COPD (the third leading cause of death in the United States) is cigarette smoking. Patients with COPD and significant sleep hypoxemia have increased pulmonary hypertension and mortality. Lower airway obstructive disease is evidenced by a forced expiratory volume exhaled in 1-second per forced vital capacity ratio <70% of predicted values.
(e) Sleep-related hypoventilation/hypoxemia due to neuromuscular and chest wall disorders. Hypoventilation can occur from reduced contractility of the ventilatory musculature (intercostals, accessory muscles, and diaphragm) or due to anatomic distortion of the chest wall (which causes inefficient breathing). This often affects patients with obesity, amyotrophic lateral sclerosis, myasthenia gravis, muscular dystrophies, kyphoscoliosis, postpolio syndrome, and spinal cord injuries with diaphragmatic paralysis. The course of the breathing disturbance approximates the severity of the underlying condition and can put the patient at risk for pulmonary hypertension, cor pulmonale, and cognitive dysfunction.
C. Hypersomnias of central origin. These disorders involve dysfunction of the normal central wake/sleep centers. The ascending reticular activating system (ARAS) of the brainstem promotes wakefulness through two pathways, leading to diffuse cortical projections. A ventral hypothalamic system excites the lateral nucleus (LN) and tuberomammillary nucleus of the hypothalamus, which relays to cholinergic basal forebrain cells, whereas a dorsal thalamic route stimulates nonspecific midline and intralaminar nuclei, while inhibiting the reticular nucleus of the thalamus. The central sleep-onset system has a hypothalamic “sleep switch” in the preoptic area of the hypothalamus (the ventrolateral and median preoptic nuclei). These nuclei have reciprocal inhibitory relays with multiple waking centers.
1. Narcolepsy. Classically begins during puberty or young adulthood with excessive sleepiness. Sleep attacks can occur while driving, engaged in active conversation, or eating. Once sleepiness stabilizes, it generally does not progress, but the other symptoms associated with narcolepsy may come and go. Cataplexy, often precipitated by strong positive emotion, involves attacks that range from brief sensations of weakness to essential paralysis. The spells are transient and do not produce cognitive impairment. Hypnagogic (at sleep-onset) and hypnopompic (on awakening) hallucinations are generally frightening visual, auditory, or movement perceptions that essentially represent dreaming while awake. Sleep paralysis occurs during the transition from sleep to waking (or waking to sleep). The patient may experience brief paralysis (seconds to minutes) with the inability to speak. Other symptoms of narcolepsy can include insomnia, poor memory, depression, and automatic behaviors. Narcolepsy is associated with pathologic REM sleep mechanisms, clinically evidenced as sleepiness, cataplexy, sleep paralysis, and hypnagogic/hypnopompic hallucinations. These symptoms are due to a deficiency of wake-promoting neuropeptides (orexins/hypocretins) in the LN of the hypothalamus.
a. PSG and the multiple sleep latency test (MSLT). REM sleep is defined on PSG and MSLT as a “relatively low voltage, mixed frequency EEG” of alpha and theta waveforms, associated with “saw-tooth” waves, that occurs with an EOG that shows REMs and an EMG that documents atonia. In diagnosing narcolepsy, an MSLT should be performed approximately 2 hours after the patient awakens from an overnight PSG (which assures adequate sleep and a paucity of other sleep disorders). The MSLT is a series of five 20-minute attempts at napping (during the patient’s normal waking hours), which are separated by approximately 2-hour intervals. A mean sleep latency (the average time it takes the patient to fall asleep after the beginning of each individual nap period) ≤8 minutes and 2 or more naps during which REM sleep appears is classically associated with narcolepsy.
b. Split-screen, video-PSG studies. These studies, performed during cataplectic events precipitated by emotional provocation, have shown REM sleep patterns during periods when patients were able to give appropriate responses to detailed questioning. Similar results have been documented during episodes of sleep paralysis and hypnagogic hallucinations.
c. Genetics. Three percent of patients with idiopathic narcolepsy have a first-degree relative with excessive sleepiness and cataplexy, whereas 40% have at least 1 relative with excessive sleepiness. The major histocompatibility complex of chromosome 6 contains genetic markers for narcolepsy. In over 90% of patients with cataplexy, the mapping of specific human leukocyte class II antigens (DR2 and DQ1) reveal a subtype human leukocyte antigen allele DQB1*0602. The presence of the DQB1*0602 allele in only 40% of patients with 2 or more SOREMPS on MSLT indicates genetic testing alone is not sufficient for the diagnosis of narcolepsy.
d. Orexins/hypocretins. A paucity of these wake-promoting neuropeptides, located in the LN of the hypothalamus, may be the primary deficit in idiopathic narcolepsy. Low CSF levels (≤110 pg per ml or one-third of mean normal control values) are found in more than 90% of narcoleptics with cataplexy.
2. Recurrent hypersomnia.
a. Kleine–Levin’s syndrome (KLS). The KLS, classically more common in males, is characterized by periods of hypersomnia, hyperphagia, and encephalopathy that can last several weeks, recur up to 10 times a year, and generally improve over a 4-year period. The brain MRI is generally normal, but single photon emission computed tomography scans have shown reduced thalamic blood flow. Hypothalamic injury has been reported at autopsy and suggested by case reports associated with encephalitis, stroke, traumatic brain injury, and low CSF levels of orexin/hypocretin.
b. Menstrual-related hypersomnia (MRH). MRH is associated with recurrent hypersomnolent episodes occurring within the first months after menarche. Episodes routinely last 1 week and resolve quickly after menses. A reported elevation in 5-hydroxyindolacetic acid turnover suggests that MRH is related to a hormone imbalance.
3. Idiopathic hypersomnia (IH). The 2 variants of IH are either with or without long sleep time. Patients with long sleep time have prolonged, sustained nonrefreshing nocturnal sleep periods lasting 10 to 20 hours, whereas in IH without long sleep time, these periods are >6 hours, but <10 hours. An IH is a lifelong problem that begins early in life and has suspected genetic concomitants. This disorder is due to dysfunctional NREM sleep mechanisms, with NREM onset sleep periods, and difficulties in waking associated with sleep drunkenness. The autonomic concomitants implied by the frequency of associated migraine headaches, orthostasis, syncope, and Raynaud’s syndrome suggest hypothalamic dysfunction. Nevertheless, CSF studies have shown normal orexin/hypocretin levels, with histamine deficiency.
4. Behaviorally induced insufficient sleep syndrome. This is due to voluntary, but unintentional, chronic sleep deprivation. Patients are preoccupied with etiologies they presume are responsible for their sleepiness (causes other than a reduced total sleep time), and their symptoms, which may include irritability, malaise, and reduced concentration.
5. Hypersomnia due to a medical condition. The conditions that can cause hypersomnia through direct effects on wake/sleep mechanisms include neurodegenerative disorders, brain trauma and tumors, encephalitis, genetic disease, and stroke. The diagnosis of narcolepsy due to medical condition is given when these conditions lead to cataplexy.
a. Neurodegenerative disorders. These can include Parkinson’s disease, Alzheimer’s disease (AD), and frontotemporal and Lewy’s body dementia. In Parkinson’s disease, hypersomnia may result from degeneration of dopaminergic cells in the substantia nigra, and cholinergic neurons in the basal forebrain.
b. Post-traumatic hypersomnia. This type of hypersomnia has been reported even in mild head injury (without loss of consciousness) and also during recovery from post-traumatic coma (where early PSG return of sleep spindles and normal sleep–wake cycling is a positive prognostic sign).
c. Genetic disorders. Specific genetic disorders associated with hypersomnia include Norrie’s disease, Niemann–Pick’s type C disease, myotonic dystrophy, Prader–Willi’s syndrome, fragile X syndrome, and Moebius’ syndrome. In Niemann–Pick’s disease type C, accumulation of unesterified cholesterol and sphingolipids in the hypothalamus, with a subsequent reduction in orexin/hypocretin, may be a cause of sleepiness. In myotonic dystrophy, hypothalamic (orexin/hypocretin) dysfunction, and loss of serotonin in the dorsal raphe nucleus, may account for hypersomnolence.
d. Endocrine disorders. Hypersomnia secondary to endocrine disorder is typified by hypothyroidism. A significant reduction in slow wave activity can be induced by hypothyroidism.
e. Hypersomnia due to drug or substance. This includes use, abuse, and cessation of stimulants and sedative-hypnotic drugs.
6. Hypersomnia not due to substance or known physiological condition. These are related to psychiatric conditions that include adjustment, personality, schizoaffective, mood, and seasonal affective disorders. Subtypes include hypersomnia associated with a major depressive episode (atypical depression and bipolar type II disorder) and conversion disorder (or as an undifferentiated somatoform disorder).
D. Circadian rhythm sleep disorders (CRSDs). A CRSD occurs when there are incongruities between the sleep–wake schedule demanded by society and the intrinsic sleep–wake pattern of the patient (determined in large part by the circadian pacemaker—the suprachiasmatic nuclei of the anterior hypothalamus). When not extrinsic or self-imposed (“jet lag” or shift work), these problems are believed to result from abnormal intrinsic physiologic responses to environmental time cues (Zeitgebers) such as sunlight (which exerts its effects through retinal–hypothalamic pathways). The patient’s state of sleepiness or arousal subsequently is out of synchrony with that of the general population. The result is alternating sleepiness and insomnia when the patient tries to follow a normal schedule.
1. History. In many cases, a sleep log can be diagnostic. The accurate, 1- to 2-month documentation of all bedtimes, final awakening times, and nap times, can help differentiate a circadian rhythm disorder from poor sleep hygiene. The log should be filled out during a vacation or “free” time so as to avoid societal constraints that prevent the patient from following their intrinsic sleep–wake pattern.
2. Other tests. Actigraphy is a method for recording limb movement using a devise (usually placed on the wrist) that records movement. Digitized data are downloaded to a computer, and computer algorithms are used to approximate wake and sleep periods over prolonged periods of time. The American Academy of Sleep Medicine (AASM) indicates actigraphy is reliable and valid for detecting sleep in healthy populations and useful in the routine evaluation of CRSDs, insomnia, and EDS. In addition, some sleep disorder centers can monitor hormonal rhythms (such as dim-light melatonin onset) and 24-hour body temperature fluctuations, which can lose normal circadian fluctuations and amplitudes in CRSDs.
a. CRSD, delayed sleep phase type. This occurs with a prevalence rate up to 16%, and is primarily noted in adolescents and young adults, and individuals with evening type personalities (as defined by the Horne–Ostberg’s questionnaire). There is an association with polymorphisms in the circadian clock gene hPer3, with a positive family history in 40%. Patients report chronically late bedtimes with late final awakening times (delayed over 2 hours relative to societal norms), which can be confirmed with a sleep logs and actigraphy (over at least 7 days). These individuals do not report sleepiness unless they attempt to follow the normal societal sleep–wake schedule.
b. CRSD, advanced sleep phase type. Persons with this syndrome go to sleep very early in relation to the setting of the sun, arise very early in relation to sunrise, and do not report excessive sleepiness during their “normal” waking hours. This tendency increases with age, and has a prevalence of 1% in middle-aged and older adults. Almost all patients are considered morning type personalities. In younger patients genetic factors may be involved, possibly with an autosomal dominant inheritance pattern, in association with a mutation in the circadian clock gene hPer2. This CRSD is generally addressed only if it impairs the quality of the patient’s work, social, or family life.
c. CRSD, irregular sleep–wake type. In this disorder, there is no definitive sleep–wake rhythm. Patients subsequently have intermittent nocturnal insomnia and variable periods of daytime sleepiness, which generally result in 3 or more irregularly timed naps during a 24-hour period. The total sleep time during a 24-hour is normal, but the timing of sleep is not predictable. This disorder is can be seen in the institutionalized elderly, in association with dementia, and in children with intellectual disabilities.
d. CRSD, free-running type. Also known as hypernychthemeral syndrome, these patients have an inability to synchronize (entrain) the physiologic desire for a sleep–wake schedule that is greater than 24 hours with a normal 24-hour day. Subsequently these patients continually “phase delay” and on a day-to-day basis show a progressive 1 to 2 hour delay of bedtime and final awakening times. When they attempt to keep regular sleep–wake schedules (fixed bedtime and final awakening times), they experience recurrent periods without sleep problems (when their intrinsic schedules match society’s), which are then followed by the gradual onset of periods associated with sleep-onset insomnia, difficulty waking in the morning, and daytime sleepiness (when their intrinsic schedules are out of synchrony with society’s). These patients are often blind and the disorder has been reported with intellectual disability, schizophrenia, and rarely in the otherwise normal population. Upon diagnosis, imaging studies of the brain can be considered, as this disorder has been associated with suprasellar lesions.
e. CRSD, shift work type. In this disorder, insomnia and EDS result when the patient works during the normal physiologic sleep period. The prevalence of shift work in industrialized countries is 20% and the estimated prevalence of insomnia/EDS due to shift work is 2% to 5%. This disorder may complicate gastrointestinal and cardiovascular disorders, cause social difficulties, or lead to drug dependency in attempts to improve sleep, and presents work-related safety concerns.
f. CRSD, due to medical condition. Degenerative diseases (including Parkinson’s and AD), blindness, and hepatic encephalopathy can alter the function of the biologic clock and lead to insomnia and EDS. Sleep-related problems can then influence the severity of the underlying condition (e.g., “sun downing” and nocturnal wandering in dementia).
E. Parasomnias. These are undesired sleep-related physical events, associated with semi-purposeful behaviors and elevated autonomic activity. Of the parasomnias, only the REM sleep behavior disorder (RBD) requires PSG for diagnosis.
1. Disorders of arousal (from NREM sleep). Confusional arousals, sleepwalking, and sleep terrors are closely related parasomnias that can occur in a familial pattern, primarily among children, and generally begin in slow-wave (stage N3) sleep during the first third of the night. The spells are associated with general lack of environmental responsiveness, automatic actions, confusion, disorientation, and occasional injuries. After these events, from which the patient is generally unarousable, there usually is amnesia without dream recall.
a. Confusional arousals. These are prevalent in children (17.3% in children 3 to 13 years of age) and adults <35 years of age. Young children may sleepwalk when they become adolescents. Adolescents and adults can have the variants; severe morning sleep inertia, and sleep-related abnormal sexual behaviors. Severe morning sleep inertia is a persistent problem that can lead to sleep-related injury (risk of motor vehicle accidents), violent behavior, poor work performance, and social problems. Sleep-related abnormal sexual behaviors can lead to assaultive behaviors followed by morning amnesia.
b. Sleepwalking. This occurs with a prevalence up to 17% in children (peaking by 8 to 12 years of age) and in up to 4% of adults (with associated violent behaviors occurring more frequently in men). The rate of familial sleepwalking is 60% when both parents are affected. Childhood sleepwalking can lead to injury, but usually resolves by puberty.
c. Sleep terrors. These occur with a prevalence rate up to 6.5% in children and in 2.2% of adults. Adults may have associated bipolar, depressive, or anxiety disorders. The onset is usually between 4 and 12 years with resolution often during puberty. During the spell, the patient often appears frightened, with tachycardia, tachypnea, diaphoresis, and inconsolable screaming and crying that can last from a few seconds to 20 minutes.
2. Parasomnias usually associated with REM sleep.
a. REM sleep behavior disorder. This disorder is associated with violent behavior during sleep that reflects dream enactment. Events begin during REM (“dreaming” or “paralyzed”) sleep and are followed, after arousal, by reports of dream imagery compatible with the actions observed during the spell. This disorder generally appears after the age of 50 years, in elderly men, with a prevalence of 0.5% to 0.8% in the elderly population. It is often associated with synucleinopathies (neurodegenerative disorders like Parkinson’s disease and Lewy’s body dementia, which are associated with neuronal lesions from aggregates of insoluble α-synuclein protein), being reported in one-third of patients with newly diagnosed Parkinson’s disease, and in 90% of patients with multiple system atrophy (MSA). The patients have histories of potentially harmful sleep-related body movements associated with dreaming. Patients frequently report sleep-related injuries, which include bruises, lacerations, dislocations, fractures, and subdural hemorrhage. The pathophysiology may be degeneration of REM-atonia pathways. The PSG shows that during REM sleep, muscle tone generally is elevated. Periodic limb movements during sleep (PLMS) are seen in 75% of patients during NREM sleep. Behaviors appearing as dream enactment may be appreciated during REM sleep.
(1) Subtypes. Preclinical RBD (“REM without atonia”) may develop into clinical RBD in 25% of cases. Parasomnia overlap disorder occurs when RBD occurs with sleepwalking and/or sleep terrors. Status dissociatus is diagnosed when the PSG has no discernable sleep stages, but behaviors that resemble sleep and suggest dreaming and RBD. This can be seen with the prion disease fatal familial insomnia, with parkinsonism, dementia, and MSA.
F. Sleep-related movement disorders.
1. Restless legs syndrome (RLS). RLS is clinically diagnosed by symptoms which form the acronym URGE; an urge to move the limbs (usually the legs), that is worse at rest, improves with movement (going), and is most evident in the evening (often when attempting to go to sleep). In children, there may be an association with ADHD. This symptom complex affects up to 10% of the general adult population, 30% of patients with rheumatoid arthritis, and up to 20% of patients with uremia (up to 62% of those on hemodialysis). It is reported almost twice as often in women, possibly related to the 11% to 20% prevalence recognized after the 20th week of pregnancy. There are early and late onset types of RLS. The early form begins <45 years of age, is slowly progressive, with 50% reporting an AD familial pattern of inheritance (risk for RLS is up to 6 times greater in first degree relatives), with a major susceptibility locus on chromosome 12q. The late onset may have symptoms that either remain stable after onset, or that rapidly progress over a 5-year period. Etiologic factors may relate to physiologic mechanisms associated with relative central dopamine and iron deficiencies (serum ferritin <18 to 50 µg per liter, iron-saturation <16% to 20%).
2. Periodic limb movement disorder (PLMD). PLMS are reported in 80% to 90% of patients with RLS, in up to 34% of patients >60 years of age, and in up to 15% of insomniacs. When PLMS are significantly elevated and they have an adverse effect on sleep or daytime functioning, the diagnosis of PLMD is made. PLMD can be exacerbated by tricyclic antidepressants, monoamine oxidase inhibitors, and hypnotics, and during withdrawal from benzodiazepines, barbiturates, and anticonvulsants. On PSG, the PLMS appear as elevated, predominantly 50 to 150 Hz, EMG activity from the tibialis anterior muscle, which persists for 0.5 to 5.0 seconds and coincides with episodes of repetitive, stereotypic extensions of the large toe with ankle, knee, and hip flexion. Consecutive movements have an intermovement interval ≥5 seconds and ≤90 seconds (generally 20 to 40 seconds), and occur primarily in stage N2 sleep. PLMS are considered significant when the PLM index (the average number of PLMS per hour of sleep) is >5 in children, and >15 in adults. New actigraphic monitors with high sampling rates can adequately detect PLMS and promise to be a powerful research tool to study the known night-to-night variability of PLMS.
3. Rhythmic movement disorder (RMD). RMD primarily affects children. The movements are sleep-related, stereotypical, repetitive movements of the head, neck, or large muscle groups and often are associated with rhythmic vocalization that includes head banging, body rocking, and leg banging. Rhythmic body movements often begin in normal children between 8 and 18 months of age and rarely lead to injury. These movements generally resolve by 5 years of age, although persistence may be associated with stress, stimulus deprivation, or CNS lesions. Family members generally are concerned about the noise and sometimes violent nature of these behaviors. PSG studies have shown that rhythmic movements tend to arise from stage N1 or N2 sleep and occur with a frequency of 0.5 to 2 Hz. A series of movements generally lasts <15 minutes.
III. OTHER INVESTIGATIONAL TOOLS AND OPTIONS
A. The maintenance of wakefulness test (MWT). The MWT is a MSLT variant that is performed while the patient attempts to maintain wakefulness in an environment conducive to sleep (a warm, dark room, while lying in a semireclining position). The sleepiness documented utilizing an MWT may more accurately translate to a work situation when compared with the MSLT. The AASM Standards of Practice Committee recommends the MWT begin 2 hours after awakening from overnight sleep. It consists of 4, 40-minute naps; each nap separated from the next by a 2-hour interval. A mean sleep latency <8 minutes is abnormal, whereas values between 8 and 40 minutes are of uncertain value. The use of an MWT has been approved in some occupations where sleepiness is hazardous, to justify a change in employment, and to support disability. No sleep is the strongest evidence for the ability to maintain wakefulness, but does not guarantee safety in regard to hypersomnolence.
B. Brain imaging and electroencephalography. In some hypersomnias due to a medical condition, imaging of the brain and routine EEG may be of prognosticating value. In post-traumatic coma with hypersomnolence, radiographic evidence of hydrocephalus predicts poor treatment response. In AD, clinical progression, secondary to degeneration of cholinergic neurons in the basal forebrain, often correlates with EEG loss of sleep spindles, slow waves, and REM sleep patterns. The use of extended PSG montages, which have extra channels, can allow more thorough assessment of variables such as the EEG (for nocturnal seizures) and EMG (for sleep-related movement and behavior disorders). Daytime provocative studies can be used to appropriately characterize phenomena such as cataplexy.
C. Others. Routine laboratory studies may be needed to rule out anemia, hypoxemia, infection, and metabolic and endocrinologic abnormalities. A Minnesota Multiphasic Personality Inventory with an interview by a neuropsychologist or psychiatrist familiar with sleep disorders can be helpful in cases in which an affective disorder is suspected. There is promise that for a number of intrinsic sleep disorders, such as narcolepsy, genetic testing may help to confirm the diagnosis.
D. Referral to a sleep disorder center. When sleep problems persist, greatly impair quality of life, or necessitate formal sleep studies for diagnosis or therapy (as SRBDs and narcolepsy), referral to a reputable sleep disorder center should be considered.
IV. SUMMARY
The general approach to the patient with a sleep disorder should always begin with the sleep history. The many specific questions necessary for diagnosing a variety of unique sleep disorders are neatly summarized in the ICSDs. The use of PSG is essential in the diagnosing SRBDs, hypersomnias of central origin, and the RBD. The MSLT can delineate the types of pathologic sleepiness specific to narcolepsy and idiopathic hypersomnolence, whereas the MWT has been used assess treatment efficacy and job suitability. In certain cases, basic metabolic panels, drug screens, genetic testing, and a variety of laboratory studies, including ABGs, complete blood counts, and renal function tests are of value. Occasionally, brain imaging, to address potential lesions affecting the ARAS and specific wake/sleep CNS centers is important. An approach that properly combines clinical acumen with the appropriate diagnostic tools generally leads to a solid diagnosis, which allows successful therapeutic interventions.
![]()
Recommended Readings
American Academy of Sleep Medicine. International Classification of Sleep Disorders: Diagnostic and Coding Manual. 2nd ed. Westchester, IL: American Academy of Sleep Medicine; 2005.
Dyken ME. Cerebrovascular disease and sleep apnea. In: Lenfant C, Bradley TD, Floras JS, eds. Sleep Apnea: Implications in Cardiovascular and Cerebrovascular Disease. New York, NY: Marcel Dekker; 2000:285–306.
Dyken ME, Lin-Dyken DC, Poulton S, et al. Prospective polysomnographic analysis of obstructive sleep apnea in Down syndrome. Arch Pediatr Adolesc Med. 2003;157:655–660.
Dyken ME, Lin-Dyken DC, Seaba P, et al. Violent sleep related behavior leading to subdural hemorrhage: polysomnographically documented REM sleep behavior disorder with split-screen electroencephalographic-video analysis. Arch Neurol. 1995;52:318–321.
Dyken M, Lin-Dyken, Yamada T. Diagnosing rhythmic movement disorder with video-polysomnography. Pediatr Neurol. 1997;16:37–41.
Dyken ME, Rodnitzky R. Periodic, aperiodic and rhythmic motor disorders of sleep. Neurology. 1992;42:68–74.
Dyken ME, Somers VK, Yamada T, et al. Investigating the relationship between stroke and obstructive sleep apnea. Stroke. 1996;27:401–407.
Dyken ME, Yamada T, Glenn CL, et al. Obstructive apnea associated with cerebral hypoxemia and death. Neurology 2004;62:491–493.
Dyken ME, Yamada T, Lin-Dyken DC. Polysomnographic assessment of spells in sleep; nocturnal seizures versus parasomnias. Semin Neurol. 2001;21(4):377–390.
Dyken ME, Yamada T, Lin-Dyken DC, et al. Diagnosing narcolepsy through the simultaneous clinical and electrophysiologic analysis of cataplexy. Arch Neurol. 1996;53:456–460.
Iber C, Ancoli-Israel S, Chesson A, Quan SF; for the American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. 1st ed. Westchester, IL: American Academy of Sleep Medicine; 2007.
Kushida CA, Littner MR, Morgenthaler T, et al. Practice Parameters for the Indication for Polysomnography and Related Procedures: An Update for 2005. Sleep 2005;28(4):499–521.
Littner MR, Kushida C, Wise M, et al. Practice Parameters for Clinical Use of Multiple Sleep Latency Test and the Maintenance of Wakefulness Test. Sleep 2005;28(1):113–121.
Practice parameters for clinical use of multiple sleep latency test and the maintenance of wakefulness test. Sleep. 28(1):113–121.
Arand D, Bonnet M, Hurwitz T, et al. The clinical use of the MSLT and MWT. Sleep 2005;28(1):123–144.
Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. Sleep. 1999;22(5):667–689.
Young T, Palta M, Dempsey J, et al. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328:1230–1235.
Young T, Peppard P, Palta M, et al. Population-based study of sleep-disordered breathing as a risk factor for hypertension. Arch Intern Med. 1997;157:1746–1752.