13.1. Brain death in adults
Most states accept some form of “brain death” as a valid determination of death. The President’s Commission provides the following guidelines1:
1. the diagnosis of death requires both cessation of function and irreversibility of cessation of either cardiopulmonary system or entire brain (including brainstem)
2. for age < 5 years, see Brain death in children, page 292
3. with no “complicating conditions” listed below, there are “…no cases of brain functions returning following a 6 hr cessation, documented by clinical examination and confirmatory EEG”A
4. with conditions such as massive intracerebral tumor with herniation or gunshot wound to the head, it is possible to pronounce death sooner with more certainty than, e.g. with post cardiac-arrest anoxia or following a coma of unknown etiology
5. when death results from criminal assault, or there is the possibility of litigation regarding the death, extra care must be taken and legal counsel may be advisable before making the determination of brain death
Table 13-1 Summary of findings in brain death (see text for details)
|
1. absence of brainstem reflexes A. fixed pupils (no response to light) B. absent corneal reflexes C. absent oculovestibular reflex (calorics) D. absent oculocephalic reflex (doll’s eyes) E. absent gag & cough reflex 2. apnea with arterial pCO2 > 60 mm Hg 3. no response to deep central pain 4. vital signs & general criteria A. core temp > 32.2° C (90° F) B. SBP ≥ 90 mm Hg C. no drugs that could simulate brain death |
BRAIN DEATH CRITERIA
Recommendations1, 2 (see Table 13-1 for summary):
A. absence of brainstem reflexes:
1. ocular examination:
A. fixed pupils: no response to bright light (caution after resuscitation: see below). The size of the pupils is unimportant (they are usually midposition (4-6 mm) but may vary to dilated rangeB (9 mm))
B. absent corneal reflexesC
C. absent oculocephalic (doll’s eyes) reflex (contraindicated if C-spine not cleared): see page 283
D. absent oculovestibular reflex (cold water calorics): instill 60-100 ml ice water into one ear (do not do if TM perforated) with HOB at 30°. Brain death is excluded if any eye movement (see page 283). Wait at least 1 minute for response, and ≥ 5 min before testing the opposite side
2. absent oropharyngeal reflex (gag) to stimulation of posterior pharynx
3. no cough response to bronchial suctioning
B. apnea test AKA apnea challenge: no spontaneous respirationsD after disconnection from ventilator (assesses function of medulla). Since elevating PaCO2 increases ICP which could precipitate herniation and vasomotor instability, this test should be reserved for last and only used when the diagnosis of brain death is reasonably certain. Guidelines4, 5
1. apnea for > 2 minutes with PaCO2 > 60 mm Hg or PaCO2 > 20 mm Hg over base-line or pH < 7.3 (CO2 is the most potent stimulus for respirations). If patient does not breathe by this point, they won’t breathe at a higher PaCO2. Not valid with severe COPD or CHF
2. to prevent hypoxemia during the test (with the danger of cardiac arrhythmia or myocardial infarction):
• precede the test with 15 minutes of ventilation with 100% FIO2 (preoxygenation)
• prior to the test, adjust the ventilator to bring the PaCO2 ≈ 40 mm Hg (to shorten the test time and thus reduce the risk of hypoxemia)
• during the test, have passive O2 flow administered at 6 L/min through either a pediatric oxygen cannula or a No. 14 French tracheal suction catheter (with the side port covered with adhesive tape) passed to the estimated level of the carina
3. starting from normocapnea, the average time to reach PaCO2 = 60 mm Hg is 6 minutes (classic teaching is that PaCO2 rises 3 mm Hg/min, but in actuality this varies widely, with an average 3.7 ± 2.34; or 5.1 mm Hg/min if starting at normocarbia5). Sometimes as long as 12 minutes may be necessary
4. the test is aborted prematurely if:
• the patient breathes: incompatible with brain death
• significant hypotension occurs
• if O2 saturation drops below 80% (on pulse oximeter)
• significant cardiac arrhythmias occur
5. if patient does not breathe, send ABG at regular intervals and at the completion of test regardless of reason for termination. If the patient does not breathe for at least 2 minutes after a PaCO2 > 60 mm Hg is documented, then the test is valid and is compatible with brain death (if the patient is stable and ABGs results are available within a few minutes, the apnea challenge may be continued while waiting for results in case the PaCO2 is < 60)
6. if PaCO2 stabilizes below 60 mm Hg and the pO2 remains adequate, try reducing the passive O2 flow rate slightly (O2 flow may be washing out CO2)
C. no motor function
1. no response to deep central pain
2. true decerebrate or decorticate posturing or seizures are incompatible with the diagnosis of brain death
3. spinal cord mediated reflex movements (including flexor plantar reflexes, flexor withdrawal, muscle stretch reflexes6, and even abdominal and cremasteric reflexes) can be compatible with brain death, and may occasionally consist of complex movements7, including bringing one or both arms up to the face8, or sitting up (the “Lazarus” sign9) especially with hypoxemia (thought to be due to spinal cord ischemia stimulating surviving motor neurons in the upper cervical cord). If complex integrated motor movements occur, it is recommended that confirmatory testing be performed prior to pronouncement of brain death10
D. absence of complicating conditions (that could simulate brain death on exam):
1. hypothermia: core temp should be > 32.2° C (90° F). Below this temp, pupils may be fixed and dilated11, respirations may be difficult to detect, and recovery is possible12
2. no evidence of remediable exogenous or endogenous intoxication, including drug or metabolic (barbiturates, benzodiazepines, meprobamate, methaqualone, trichloroethylene, paralytics, hepatic encephalopathy, hyperosmolar coma…). If there is doubt, depending on circumstances, lab tests including drug levels (serum and urine) may be sent. Pseudocholinesterase deficiency is present in 1/3000 patients which can cause succinycholine to last up to 8 hours (instead of 5 mins). A twitch monitor can rule-out NMB (place the electrodes immediately behind the eye or across the zygomatic arch)
3. shock (SBP should be ≥ 90 mm Hg) and anoxia. Loss of > 45% of circulating blood volume can produce lethargy
4. immediately post-resuscitation: shock or anoxia may cause fixed and dilated pupils. Atropine may cause slight dilatation but not unreactivity (see page 292). Neuromuscular blockage (e.g. for intubation) does not affect pupils because the iris lacks nicotinic receptors
5. patients coming out of pentobarbital coma (wait until level ≈ ≤ 10 mcg/ml)
E. confirmation of brain death by use of Clinical confirmatory tests (EEG, angiography, CRAG, BAER…, see below) is not required, but may be used as determined by judgement of attending or consulting physician
F. recommended observation periods during which time the patient fulfills criteria of clinical brain death before the patient may be pronounced dead:
1. in situation where overwhelming brain damage from an irreversible condition is well established (e.g. massive intracerebral hemorrhage), some experts will pronounce death following a single valid brain death exam in conjunction with a clinical confirmatory test
2. if an irreversible condition is well established, and clinical confirmatory tests are used: 6 hours
3. if an irreversible condition is well established and no clinical confirmatory tests are used: 12 hours
4. if diagnosis is uncertain and no clinical confirmatory tests: 12-24 hours
5. if anoxic injury is the cause of brain death: 24 hours (may be shortened if cessation of CBF is demonstrated)
A. note: EEG is not mandatory, see recommended observation periods…, page 291
B. cervical sympathetic pathways may remain intact
C. corneal reflex: eye closing to corneal (not scleral) stimulation
D. respirations are defined as abdominal or chest excursions that produce adequate tidal volumes; if there is any question, a spirometer may be connected to the patient3
CLINICAL CONFIRMATORY TESTS
CEREBRAL ANGIOGRAPHY
Criteria: absence of intracranial flow at the level of the carotid bifurcation or circle of Willis2). Filling of the superior sagittal sinus may occur in a delayed fashion. Interobserver validity has not been studied. Not routinely used in the diagnosis of brain death, but may be employed in difficult situations.
EEG
Can be done at bedside. Requires experienced interpreter. Does not detect brainstem activity, and electrocerebral silence (ECS) does not exclude the possibility of reversible coma. Thus, at least 6 hoursobservation is recommended in conjunction with ECS. Using ECS as a clinical confirmatory test should be done only in patients without drug intoxication, hypothermia, or shock.
Definition of electrocerebral silence on EEG: no electrical activity > 2 μV with the following requirements:
• recording from scalp or referential electrode pairs ≥ 10 cm apart
• 8 scalp electrodes and ear lobe reference electrodes
• inter-electrode resistance < 10,000 Ω (or impedance < 6,000 Ω) but over 100 Ω
• sensitivity of 2 μV/mm
• time constants 0.3-0.4 sec for part of recording
• no response to stimuli (pain, noise, light)
• record > 30 mins
• repeat EEG in doubtful cases
• qualified technologist and electroencephalographer with ICU EEG experience
• telephone transmission not permissible
CEREBRAL RADIONUCLIDE ANGIOGRAM (CRAG)
Can be performed at the bedside with a general purpose scintillation camera with a low energy collimatorA. May not detect minimal blood flow to the brain, especially brainstem, therefore 6 hours observation in conjunction with CRAG is recommended unless there is a clear etiology of overwhelming brain injury (e.g. massive hemorrhage or GSW).
A. portable scintillation cameras are becoming increasingly scarce
May be useful to confirm clinical brain death in the following settings:
1. where complicating conditions are present, e.g. hypothermia, hypotension (shock), drug intoxication
2. severe facial trauma where ocular findings may be difficult or confusing
3. in patients with severe COPD or CHF where apnea testing may not be valid
4. to shorten the observation period, especially when organ donation is a possibility
Technique
1. scintillation camera is positioned for an AP head and neck view
2. inject 20-30 mCi of 99mTc-labeled serum albumin or pertechnetate in a volume of 0.5-1.5 ml into a proximal IV port, or a central line, followed by a 30 ml NS flush
3. perform serial dynamic images at 2 second intervals for ≈ 60 seconds
4. then, obtain static images with 400,000 counts in AP and then lateral views at 5, 15 & 30 minutes after injection
5. if a study needs to be repeated because of a previous non-diagnostic study or a previous exam incompatible with brain death, a period of 12 hours should lapse
Findings
No uptake in brain parenchyma = “hollow skull phenomenon” (see Figure 13-1). Termination of carotid circulation at the skull base, and lack of uptake in the ACA and MCA distributions (absent “candelabra effect”). There may be delayed or faint visualization of dural venous sinuses even with brain death13 due to connections between the extracranial circulation and the venous system.
TRANSCRANIAL DOPPLER3
1. small peaks in early systole without diastolic flow or reverberating flow (indicative of significantly increased ICP)
2. initial absence of doppler signals cannot be used as criteria for brain death since 10% of patients do not have temporal insonation windows
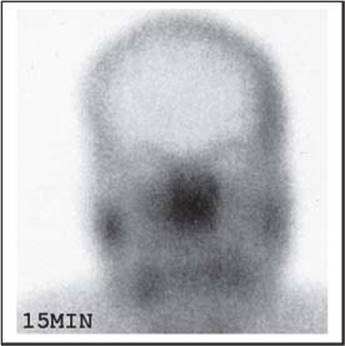
Figure 13-1 “Hollow-skull” sign on CRAG (static AP view taken15 minutes after injection)
SSEPS
Bilateral absence of N20-P22 response with median nerve stimulation.
ATROPINE
In brain death, 1 amp of atropine (1 mg) IV should not affect the heart rate due to the absence of vagal tone (the normal response to atropine of increased heart rate rules out brain death, but absence of the response is not helpful since some conditions such as Guillain-Barre may blunt the response).
Systemic atropine in usual doses causes slight pupillary dilatation14, 15, but does not eliminate reaction to light (therefore, to eliminate uncertainty, it is prudent to examine the pupils before giving the atropine).
13.2. Brain death in children
Criteria for death: irreversible loss of cardiopulmonary or entire brain function (as in adult), but the (clinically unproven) assumption that a child’s brain is more resilient results in more difficult determination of brain death. The following guidelines are proposed for patients < 5 yrs age16:
• these recommendations are not applicable for the premature infant
• determination of proximate cause of coma should be made to ensure absence of remediable conditions: especially toxic and metabolic disorders, sedatives, paralytics, hypothermia, hypotension (for age), and surgically treatable conditions
• criteria:
A. coma and apnea must coexist: including complete loss of consciousness, vocalization and volitional activity
B. absence of brainstem function
1. midposition or fully dilated pupils, unresponsive to light (R/O drug effects)
2. EOM: absence of spontaneous, doll’s eyes and caloric movements of eyes
3. absence of bulbar musculature movement: including oropharyngeal and facial muscles; absence of corneal, gag, cough, suck, and rooting reflex
4. absence of respiratory movement (usually tested after other criteria met)
5. flaccid tone and absence of spontaneous or induced movements (spinal myoclonus and spinal cord movements, e.g. reflex withdrawal are not included)
6. examination results should remain consistent with brain death throughout observation period
• observation periods according to age:
A. in newborns born at or after term (> 38 wks): 7 days
B. age 7 days - 2 mos: 2 examinations and 2 EEGs 48 hrs apart (repeat exam unnecessary if cerebral radionuclide angiogram (CRAG) fails to visualize cerebral arteries)
C. age 2-12 mos: 2 examinations and 2 EEGs 24 hrs apart (repeat exam unnecessary if CRAG negative)
D. age > 12 mos: if irreversible condition exists, laboratory testing is not necessary, and 12 hrs observation is sufficient (unclear conditions, especially hypoxic-ischemic encephalopathy, are difficult to assess, and 24 hrs observation is suggested unless electrocerebral silence on EEG or a negative CRAG confirm diagnosis)
• confirmatory tests:
A. EEG: standard requirement for 10 cm electrode distance (see page 292) may be decreased in proportion to size of head
B. CRAG: applicability to patient < 2 mos age unproven
13.3. Organ and tissue donation
State and federal laws require families of individuals satisfying criteria for brain death to be approached about the possibility of organ donation. Facts that may be conveyed to family in order to help their understanding about organ procurement:
1. any or all suitable organs may be individually specified for donation or to be excluded from consideration for donation
2. organ procurement may be done in such a way as not to interfere with an open casket funeral (i.e. disfigurement can be avoided)
3. families can receive information as to the ultimate use of any recovered organs
13.3.1. Criteria for qualification for organ donation
General exclusionary criteria for organ donation (modified17)
1. infection
A. untreated septicemia
B. the following infections or conditions: AIDS, viral hepatitis, viral encephalitis, Guillain-Barré syndrome
C. current IV drug abuse
D. active TB
2. malignancy: brain tumors represent possible exceptions (see below)
3. relative exclusions: chronic untreated HTN, hypotension (desired SBP > 100 with normal CVP)
4. disease of the organs considered for donation
5. anencephalic newborns: recent consensus is that the functioning brainstem in these infants (e.g. spontaneous respirations) disqualifies them from the diagnosis of brain death (furthermore, few such organs would likely benefit others)18
Guidelines for inclusion (some recommendations from reference17 included)
These guidelines are constantly being revised, in part due to improved results with the use of cyclosporin in recipients. In general, consultation with a transplant coordinator is recommended to determine appropriateness of donation.
1. brain death or cardiac death19
2. organs:
A. kidneys: age > 6 mos (because of size). Normal blood pressure, BUN, serum creatinine & U/A. No SLE (because of possible lupus nephritis)
B. heart and heart/lung: age ideally < 40 years for males and < 45 for females (above these ages, a cardiac cath is usually performed) but up to 60 yrs may be used depending on condition of heart and potential recipients). Exam by cardiologist indicating no heart disease (cardiomyopathy, valve defect, reduced ejection fraction, severe ASHD, S/P CABG). No IDDM
C. liver: age > 1 mos. Normal hepatic function (normal or acceptable AST, ALT, LDH, bilirubin (direct, indirect & total) and normal clotting studies) with no history of liver disease
D. pancreas: age 15 - 40 yrs. No history of diabetes. Normal serum glucose and amylase
3. tissues:
A. corneas: age ≥ 1 yr. Neither cancer nor sepsis disqualifies (rabies and Creutzfeldt-Jakob disease are contraindications)
B. skin: age 15-65 yrs. Excluded if cancer
C. bone: age 15-65 yrs. Excluded if cancer
D. bone marrow: age ≤ 50 yrs
E. heart valves: age ≤ 55 yrs
13.3.2. Organ donation in patients with brain tumors
Among patients with a brain tumor:
1. those that are not candidates for organ donation:
A. metastatic tumors to the brain
B. brain tumors that have been manipulated (biopsied or excised)
C. patients with brain tumors who have been shunted
2. those that might be candidates, but considered high-risk donorsA include unmanipulated:
A. glioblastoma
B. anaplastic astrocytoma
C. medulloblastoma
3. unmanipulated tumors that might not be considered high risk
A. hemangioblastoma
B. meningioma
Optimally, if no metastases are seen on CT (chest, abdomen and pelvis) and no mets are found at time of organ procurement, a brain biopsy would be performed after the organs are procured at the same anesthetic and the organs would not be “released” until the biopsy proves which of the above categories applies.
13.3.3. Management after brain death for organ donation
Note: once brain death occurs, cardiovascular instability eventually ensues, generally within 3-5 days, and management with pressors is usually required. Fluid and electrolyte imbalances from loss of hypothalamic regulation must be normalized. In some instances a beating-heart cadaver can be maintained for months20.
1. consent: must be obtained from donor’s legal guardian. NB: must also be obtained from medical examiner or coroner’s office for all cases under their jurisdiction (in most states, death resulting from accident, within 24 hrs of hospitalization, etc.)
2. signed note in chart stating date and time patient pronounced brain dead
3. contact transplant coordinator at earliest possible time
4. wean from vasopressors if possible. Control hypotension through volume expansion whenever possible (after brain death, ADH production ceases, producing diabetes insipidus with high urine output, thus copious fluid administration is anticipated (> 250-500 ml/hr is common). Most centers prefer AVOIDING exogenous ADH (vasopressin (Pitressin®)) if possible since the risk of renal shutdown increases in brain-death
A. start with crystalloid (D5 1/4 NS + 20 mEq KCl/L is generally a good choice since it replaces free water), replace urine cc for cc plus 100 cc/hr maintenance
B. use colloid (FFP, albumin…) if unable to maintain BP by replacement
A. high-risk organs may be considered e.g. for liver transplants in patients who are very low on the list due to age or hepatocellular cancer
C. use vasopressors if still hypotensive. Start with low dose dopamine, increase up to ≈ 10 μg/kg/min, add dobutamine if still hypotensive at this dosage
D. if UO is still > 300 ml/hr after above measures, use ADH analog (aqueous vasopressin (Pitressin®) is preferred over DDAVP to avoid renal shutdown)
5. thyroglobulin given IV converts some cells from anaerobic to aerobic metabolism which may help stave off cardiovascular collapse
LABORATORY EVALUATION17
General initial labs
1. serology: VDRL or RPR, HBsAg, HIV, CMV, ABO blood group, HLA tissue type
2. chemistry: electrolytes, glucose, BUN, creatinine, calcium, phosphate, liver function tests, U/A (urine analysis)
3. hematology: CBC, PT/PTT
4. microbiology: blood, urine and sputum cultures; sputum Gram stain
Kidney donor
1. in addition to general labs (see above), check BUN & creatinine ≈ q day
2. check electrolytes ≈ q 12 hrs (modify as appropriate)
Liver donor
1. in addition to general labs (see above), check LDH, AST, ALT, bilirubin (direct, indirect, and total)
Heart donor
1. all require an echocardiogram prior to donation
13.3.4. Organ donation after cardiac death
![]() Key concepts:
Key concepts:
• candidates: ventilator dependent patients (typically with brain or spinal cord injury) who are so near death that further care is futile
• consent from legal next of kin for: organ donation, heparin, and femoral lines
• clearance from medical examiner when applicable (usually unnatural death)
• counsel the family that the procedure cannot be done in ≈ 20%. They are to be notified immediately if this happens and end-of-life care resumes
• transplant team cannot participate in end-of-life care, declaration of death, and should not be in O.R. until after cardiad death is declared
Covered in this section because of relevance to organ donation.
Candidates for organ donation after cardiac death are typically ventilator dependent patients with brain or spinal cord injuries who are so near death that further treatment is futile, but who do not meet brain death criteria. Organs typically recovered in this manner: kidneys, liver, pancreas, lungs, and rarely the heart19.
Ethical concerns related to this practice have been raised21.
Cardiology consultation may help determine the likelihood that cardiac death will follow extubation in a timeframe consistent with organ procurement.
Consent
Consent for withdrawal of care and procurement of organs must be obtained from the legal next of kin (which may be a family member, designated health care representative or health care surrogate). Consent must also be obtained for any donation-related procedures prior to death (which typically includes heparin infusion to prolong organ viability22 and the possibility of femoral catheters).
Clearance from the medical examiner must be obtained in applicable cases (including deaths due to accident, homicide, suicide…).
Procedure
Life sustaining measures are then discontinued (typically consisting of extubation) usually in the operating room. Death is pronounced typically ≈ 2 minutes after cardiac activity becomes insufficient to generate a pulse, because limited data indicates that circulation will not spontaneously return23 (NB: EKG activity does not need to cease). After declaration of death, cold perfusion of organs is performed and they are procured.
To avoid potential conflicts of interest, no member of the transplant team can participate in end-of-life care nor the declaration of death19. About 20% of the time, the progression to cardiac death does not occur in a timeframe that permits organ retrieval. In these cases, organ donation is cancelled, the family must be immediately notified, and end-of-life care continues.
13.4. References
1. President’s Commission for the Study of Ethical Problems in Medicine: Guidelines for the determination of death. JAMA 246: 2184-6, 1981.
2. Quality Standards Subcommittee of the American Academy of Neurology: Practice parameters for determining brain death in adults (summary statement). Neurology 45: 1012-4, 1995.
3. Widjicks E F: Determining brain death in adults. Neurology 45: 1003-11, 1995.
4. Benzel E C, Gross C D, Hadden T A, et al.: The apnea test for the determination of brain death. J Neurosurg 71: 191-4, 1989.
5. Benzel E C, Mashburn J P, Conrad S, et al.: Apnea testing for the determination of brain death: A modified protocol. J Neurosurg 76: 1029-31, 1992.
6. Ivan L P: Spinal reflexes in cerebral death. Neurology 23: 650-2, 1973.
7. Turmel A, Roux A, Bojanowski M W: Spinal man after declaration of brain death. Neurosurgery 28: 298-302, 1991.
8. Heytens L, Verlooy J, Gheuens J, et al.: Lazarus sign and extensor posturing in a brain-dead patient. J Neurosurg 71: 449-51, 1989 (case report).
9. Ropper A H: Unusual spontaneous movements in brain-dead patients. Neurology 34: 1089-92, 1984.
10. Jastremski M S, Powner D, Snyder J, et al.: Spontaneous decerebrate movement after declaration of brain death. Neurosurgery 29: 479-80, 1991 (letter).
11. Treatment of hypothermia. Med Letter 36: 116-7, 1994.
12. Antretter H, Dapunt O E, Mueller L C: Survival after prolonged hypothermia. N Engl J Med 330: 219, 1994.
13. Goodman J M, Heck L L, Moore B D: Confirmation of brain death with portable isotope angiography: A review of 204 consecutive cases. Neurosurgery 16: 492-7, 1985.
14. Greenan J, Prasad J: Comparison of the ocular effects of atropine and glycopyrrolate with two IV induction agents. Br J Anaesth 57: 180-3, 1985.
15. Goetting M G, Contreras E: Systemic atropine administration during cardiac arrest does not cause fixed and dilated pupils. Ann Emerg Med 20: 55-7, 1991.
16. Task Force for the Determination of Brain Death in Children: Guidelines for the determination of brain death in children. Arch Neurol 44: 587-8, 1987.
17. Darby J M, Stein K, Grenvik A, et al.: Approach to management of the heartbeating “brain dead” organ donor. JAMA 261: 2222-8, 1989.
18. Shewmon D A, Capron A M, Peacock W J, et al.: The use of anencephalic infants as organ sources: A critique. JAMA 261: 1773-81, 1989.
19. Steinbrook R: Organ donation after cardiac death. N Engl J Med 357 (3): N Engl J Med: 209-13, 2007.
20. Bernstein I M, Watson M, Simmons G M, et al.: Maternal brain death and prolonged fetal survival. Obstet Gynecol 74: 434-7, 1989.
21. DuBois J M, DeVita M: Donation after cardiac death in the United States: How to move forward. Crit Care Med 34 (12): Crit Care Med: 3045-7, 2006.
22. Bernat J L, D’Alessandro A M, Port F K, et al.: Report of a national conference on donation after cardiac death. Am J Transplant 6 (2): Am J Transplant: 281-91, 2006.
23. DeVita M A: The death watch: Certifying death using cardiac criteria. Prog Transplant 11 (1): Prog Transplant: 58-66, 2001.