This section contains differential diagnosesA (DDx) grouped either by signs and symptoms (see below), or by location/finding (starting on page 1209). DDx that are better covered elsewhere in a section devoted primarily to that topic are listed in Table 35-1.
A. in general usage, the term differential diagnosis sometimes refers to conditions that may mimic the one under consideration, however, it may also denote possible etiologies of a particular condition or finding. No attempt is made herein to consistently distinguish between these two similar usages of the term, although whenever possible, the word etiologies is employed where appropriate
Table 35-1 Differential diagnoses covered outside this chapter (followed by page number where the item may be found)
|
abducens palsy - 836 anisocoria - 831 ankylosing spondylitis - 502 bladder dysfunction - 117 brachial plexopathy - 794 carpal tunnel syndrome - 809 cervical stenosis - see below & 489 chordomas - 676 coma - 280 Creutzfeldt-Jakob disease - 363 dementia - 56 diabetes insipidus - 15 dizziness - 840 extra-axial fluid (peds) - 904 facial nerve palsy (Bell’s palsy) - 844 giant cell arteritis - 74 Guillain-Barré - 68 |
gyral enhancement - 1013 hydrocephalus - 311 internuclear ophthalmoplegia - 834 lateral disc herniation - 454 Meniere’s disease - 842 meralgia paresthetica - 819 multiple sclerosis - 62 ophthalmoplegia painful - 836 painless - 837 papilledema - 829 Parinaud’s syndrome - 114 Parkinson’s disease - 60 pineal region tumors - 691 pneumocephalus - 890 prolactin elevation - 644 pseudotumor cerebri - 716 |
retinal hemorrhage - 919 sarcoidosis - 72 seizures new onset, adult - 396 new onset, peds - 397 nonepileptic - 400 status epilepticus - 403 schizencephaly - 243 spinal cord tumors - 728 spinal epidural abscess - 377 spinal stenosis lumbar - 478 synovial cyst (spinal) - 456 thoracic outlet syndrome - 823 torticollis - 541 trigeminal neuralgia - 552 urinary retention - 118 vertigo - 840 |
35.1. Differential diagnosis (DDx) by signs and symptoms
35.1.1. Myelopathy
Items marked with a dagger (†) may present as a spinal epidural mass.
1. congenital
A. (Arnold)-Chiari malformation: Type I often presents in early adulthood (see page 488)
B. tethered cord: often may not present until after some trauma
C. syringomyelia: may be congenital or post-traumatic in quadriplegics, usually presents with a central cord syndrome (see Syringomyelia, page 510) or progressive myelopathy
D. neurenteric cyst: see page 227
E. cord compression that occurs with some mucopolysaccharidoses: e.g. Morquio syndrome (due to atlanto-axial subluxation), Hurler syndrome
F. hereditary spastic paraplegia: family history is key. Diagnosis of exclusion1
2. acquired
A. cervical or thoracic spinal stenosis: often degenerative disease superimposed on congenitally narrow canal (congenital narrowing is frequent in achondroplastic dwarfs)
B. traumatic: including spinal shock, hematomyelia, spinal epidural hematoma (see vascular below), barotrauma, electrical injuries, compression by bone fracture†. May follow minor trauma in the setting of spinal stenosis
C. herniated intervertebral disc†: myelopathy more common in thoracic region, radiculopathy more common in cervical region (long tract signs are rare with herniated cervical disc)
D. kyphosis
E. extramedullary hematopoeisis†: hypertrophy of marrow → cord compression. Primarily in chronic anemias (e.g. thalassemia major) (see page 43)
F. bony compression secondary to incompetence of odontoid process or transverse atlantal ligament†. May be congenital, traumatic (see page 963), neo-plastic, or inflammatory (especially rheumatoid arthritis)
G. epidural lipomatosis†: hypertrophy of epidural fat most often due to years of exogenous steroid therapy2 - see page 516
H. ossification of the posterior longitudinal ligament (OPLL)3 (see page 504)
I. arachnoiditis ossificans: a rare condition (only ≈ 43 case reports4) involving calcification of the arachnoid membrane. In the T-spine, may occur as ossified plaques or in a cylindrical form surrounding the spinal cord. May be difficult to detect on MRI and myelography. Plain unenhanced CT may be optimal for diagnosis
J. vertebral Paget’s disease† (see page 500)
K. idiopathic spinal cord herniation5, 6: rare. Thoracic spinal cord herniates through an anterior dural defect frequently producing a Brown-Séquard syndrome or spastic paraparesis (see page 514)
3. neoplastic
A. spine/spinal cord tumors (see page 728 for details)†
1. extradural (55%):
a. primary tumors (rare) include: neurofibromas, chordomas, osteoid osteoma, aneurysmal bone cyst, vertebral hemangioma7
b. if age > 40 yrs, suspect extradural lymphoma (primary or secondary) or leukemic deposits (chloroma), especially with pre-existing diagnosis of hematopoietic or lymphatic disorder
c. epidural metastases become increasingly common after age 50 yrs. Occurs in up to 10% of cancer patients. 5-10% of malignancies present initially with cord compression (see page 742)
2. intradural-extramedullary (40%): meningiomas, neurofibromas
3. intradural-intramedullary: primary cord tumors (ependymoma, astrocytoma) and rarely intramedullary mets (see page 730)
B. carcinomatous meningitis: neurologic deficit usually cannot be localized to a single level (see page 711)
C. paraneoplastic syndrome: including effects on spinal cord or on peripheral nerves
4. vascular
A. hematoma/hemorrhage
1. spinal epidural hematoma†: usually associated with anticoagulation therapy8 (see page 515 and page 39)
a. traumatic: following LP or epidural anesthesia (see page 39)
b. spontaneous9: rare. Includes hemorrhage from spinal cord AVM (see page 507) or from vertebral hemangioma (see page 738)
2. spinal subarachnoid hemorrhage: as in spinal epidural hematoma (see above), this may also be post-traumatic (e.g. following LP10, 11) or secondary to spinal cord AVM
3. spinal subdural hematoma
4. hematomyelia
B. spinal cord infarction: uncommon with the elimination of syphilitic endarteritis. Most often in the territory of the anterior spinal artery, sparing posterior columns. Most commonly ≈ T4 level (watershed zone)
1. atherosclerosis of radicular artery in elderly patient with hypotension is now the major cause of this rare condition
2. clamping aorta during surgery (e.g. for abdominal aortic aneurysm)
3. hypotension (relative or absolute) during surgery in the sitting position in the presence of spinal stenosis12. May be improved by avoiding absolute hypotension, using awake fiber-optic intubation and positioning, intraoperative SSEP monitoring and inducing hypertension if changes occur with positioning, avoidance of sitting position, and avoiding hyperflexion, hyperextension and traction
4. aortic dissection
5. embolization of spinal arteries
C. spinal cord vascular malformations (see page 507)†: 10-20% present as sudden onset of myelopathy usually in patients < 30 yrs13, myelopathy may be secondary to:
1. mass effect from AVM: spinal AVMs account for < 5% of lesions presenting as cord “tumors”
2. rupture → SAH, hematomyelia, or epidural hematoma
3. watershed infarction due to “steal”
4. spontaneous thrombosis (necrotizing myelopathy of Foix-Alajoua-nine disease14): presents as spastic → flaccid paraplegia, with ascending sensory level
D. radiation myelopathy: due to microvascular occlusion (see page 772)
E. secondary to iodinated contrast material used for mesenteric or aortic angiography. Especially when angiogrammed in presence of hypotension, where cardiac output is shunted away from viscera and into spinal radicular arteries. Treatment: place patient sitting, remove ≥ 100 ml of CSF via LP and replace with equal amount of saline over 30 mins15
5. autoimmune
A. post-viral (or post-vaccination): may be etiology of autoimmune process (i.e. transverse myelitis). Viral prodrome present in ≈ 37% of cases of ATM. Viral infection is usually most damaging to gray matter (e.g. poliomyelitis)
6. demyelinating
A. acute (idiopathic) transverse myelitis (ATM) (see page 69). Peak incidence during first 2 decades of life. Abrupt onset of LE weakness, sensory loss, back pain, and sphincter disturbance indistinguishable from spinal cord compression. Thoracic region most common. CT and myelogram are normal. MRI may demonstrate. CSF → pleocytosis and hyperproteinemia
B. multiple sclerosis (MS): diagnosed in only 7% of patients presenting as acute transverse myelopathy. Although more common in young adults, MS can occur at any time in life. Myelopathy of MS is usually insidious, and is usually incomplete (i.e. some sparing). Affects myelin, thus sparing gray matter. Abdominal cutaneous reflexes are almost always absent in MS
C. Devic syndrome (neuromyelitis optica (NMO)): a variant of MS characterized by acute bilateral optic neuritis and transverse myelitis (extending ≥ 3 levels16, often causing cervical myelopathy). Spinal cord edema may become so severe as to cause complete block on myelography. More common in Asia and India than U.S. or Europe. Compared to classic MS: the myelopathy tends to be more severe (pathology: more necrosis as opposed to incomplete demyelination) and with less chance of recovery. Distinct serum IgG antibodies (NMO-IgG) may help differentiate from MS17
7. metabolic/toxic
A. (subacute) combined system disease (CSD) (AKA subacute combined columnal degeneration): due to vitamin B12 (cyanocobalamin) deficiency.
1. etiologies:
a. dietary deficiency of B12
b. pernicious anemia: malabsorption of B12 in the distal ileum due to lack of secretion of intrinsic factor (a small polypeptide) by gastric parietal cells18)
c. other gastric disorders: low gastric pH e.g. in Zollinger-Ellison syndrome can inhibit attachment of intrinsic factor to ileal receptors
2. clinical: onset is gradual and uniform. Begins with symmetrical paresthesias in feet or hands (posterior column involvement) → leg stiffness, weakness, and proprioceptive deficits with unsteadiness that is worse in the dark → spasticity → paraplegia → bowel and bladder dysfunction. Dementia (confusion, memory impairment, irritability…) occurs in advanced cases due to cerebral white matter changes. Visual disturbances with or without optic atrophy may be due to optic nerve demyelination
3. labs:
a. serum B12: the most sensitive test. However, normal B12 levels do not R/O B12 deficiency. If there are neurologic symptoms then check malonic acid or other markers of B12 deficiency such as methylmalonic acid (also check homocysteine to R/O folate deficiency)
b. CBC: most (but not all) patients will have a macrocytic anemia (folic acid deficiency also produces megaloblastic anemia. Folic acid corrects the anemia, even with CSD, but not the neurologic deficits which may actually worsen)
c. Schilling test: determines the cause of the B12 deficiency even if B12 injections have already been given
4. imaging: T2WI MRI may demonstrate increased signal within the white matter of the spinal cord, predominantly in the posterior columns but may also be seen in spinothalamic tracts
5. treatment: B12 injections or large doses of oral preparations19
B. toxins: local anesthetics used for spinal anesthesia rarely cause myelopathy
8. infectious
A. (para) spinal abscess (AKA spinal epidural abscess) or epidural empyema†: often history of staphylococcus infection, usually a skin furuncle. Vertebral osteomyelitis often accompanies20. Produces local tenderness, back pain, fever, elevated ESR (see page 376)
B. vertebral osteitis/osteomyelitis† (see page 380)
C. pyogenic discitis†: spontaneous or following procedures (see page 383)
D. HIV or AIDS related myelopathy: similar to B12 deficiency. Spastic weakness & ataxia. Can cause vacuolization of spinal cord. “Tropical (spastic) paraparesis of AIDS” also seen in HTLV-I infection21
E. tuberculosis: Pott’s disease, see Tuberculous vertebral osteomyelitis, page 381
F. spinal meningitis with pachymeningitis
G. viral:
1. herpes varicella-zoster: rarely causes necrotizing myelopathy
2. Herpes simplex type 2: may cause ascending myelitis
3. cytomegalovirus: may cause transverse myelitis
H. syphilitic involvement: may cause tabes dorsalis, syphilitic meningomyelitis, or spinal vascular syphilis. Diagnosed by serum and CSF serology
I. parasitic cysts†
J. some forms of Creutzfeldt-Jakob disease (CJD) with predominant initial muscle wasting may mimic spinal cord disease or ALS (see page 362)
9. peripheral neuromuscular disorder
A. Guillain-Barré syndrome (GBS): rapidly ascending weakness (mimics cord compression) with areflexia and near normal sensation (see page 66)
B. chronic dysimmune neuropathies: presumed to be immune mediated22
1. chronic immune demyelinating polyradiculoneuropathy (CIDP): similar to GBS but can progress over a longer period of time (see page 68)
2. multifocal motor neuropathy (MMN): characterized by asymmetric muscle wasting, cramping & LE twitching. May mimic ALS, but is treatable (with IVIg or immunosuppression)
C. myopathies: including steroid myopathy (usually affects proximal > distal muscles)
10. motor neuron diseases
A. amyotrophic lateral sclerosis (ALS): upper and lower motor neuron disease. Slight spasticity of LEs (extreme spasticity is rare), atrophic weakness of the hands and forearms, fasciculations in the UEs, absence of sensory changes (including lack of pain), sphincter control usually preserved (see page 65)
B. primary lateral sclerosis: age > 50. No LMN signs. Slower progression than ALS (yrs to decades). Pseudobulbar palsy is common23 (see page 65)
† items with dagger may also present as a spinal epidural mass
35.1.2. Sciatica
Definition: pain in the distribution of the sciatic nerve. The sciatic nerve is comprised of components of nerve roots of L4-S3. The nerve passes out of the pelvis through the greater sciatic foramen along the back of the thigh. In the lower third of the thigh it divides into the tibial and common peroneal nerves.
The most common cause of sciatica is radiculopathy due to a herniated lumbar disc24. The differential diagnosis is similar to that for myelopathy (see above) but also includes:
1. congenital
A. meningeal cyst (perineural cyst) (see Spinal meningeal cysts, page 509)
B. conjoined nerve root: (see page 256) initially dismissed as a possible cause of radiculopathy, but current thinking recognizes that these may be symptomatic possibly by tethering
2. acquired
A. spinal stenosis/spondylosis/spondylolysis/spondylolisthesis
B. juxtafacet cyst: includes synovial cyst and ganglion cyst25: detection is increasing with the use of MRI (see page 456)
C. nerve root sheath cyst: may arise near axilla of nerve root and cause compression of adjacent roots. Treatment: excise cyst and oversew the ostium
D. arachnoiditis ossificans: rare (see page 1186). In the lumbar region may occur as columnar, cylindrical, or irregularly shaped masses26. May produce low back pain, radiculopathy, or cauda equina syndrome
E. heterotopic ossification around the hip27
F. injection injuries from misplaced IM injections
G. compartment syndrome of the posterior thigh
H. injury complicating total hip arthroplasty28
I. radiation injury following treatment of nearby tumors
3. infectious
A. discitis: usually causes excruciating pain with any movement (see page 383)
B. Lyme disease: see page 368
C. herpes zoster: a rare cause of radiculopathy29. Lumbosacral dermatomes are involved in ≈ 10-15% of zoster cases. Pain is usually independent of position. Typical herpetic skin lesions usually follow onset of pain by 3-5 days. 1-5% develop motor weakness (usually in arms or trunk). Sacral zoster can cause detrusor paralysis, producing urinary retention. 55% of those with motor symptoms have good recovery, 30% have fair to good recovery
4. neoplastic:
A. spine tumors: multiple myeloma (see page 740), metastases (see page 742)…
B. bone or soft-tissue tumors along the course of the sciatic nerve: may result in erroneous laminectomy for herniated lumbar disc30. Pain is usually insidious in onset, and not positional (see below)
1. intraabdominal or pelvic neoplasm
2. tumors of the thigh
3. tumors in the popliteal fossa or calf
5. inflammatory:
A. trochanteric bursitis: may produce pseudoradiculopathy. Rarely extends to the posterior thigh or as far distally as the knee (see page 479)
B. myositis ossificans of the biceps femoris muscle31
6. vascular:
A. sciatica may be mimicked by intermittent (i.e. vascular) claudication
B. psoas hematoma: usually in patient on anticoagulant. Sometimes drainage is required
7. referred pain of nonspinal origin: not dermatomal. Nerve root tensions signs (see page 443) are usually negative. Includes:
A. pyelonephritis
B. renolithiasis including ureteral obstruction
C. cholecystitis
D. appendicitis
E. endometritis/endometriosis
F. posterior perforating duodenal ulcer
G. inguinal hernia, especially if incarcerated
H. aortic dissection: see page 1192
8. piriformis syndrome (PS): controversial. Piriformis muscle originates on anterior S2-4 VBs, sacrotuberous ligament and passes through the greater sciatic notch to attach to the greater trochanter of the femur. It is innervated by L5-S1. It is the principle external rotator of the extended hip. It may irritate or compress the sciatic nerve (AKA pseudosciatica, can mimic symptoms of a herniated disc). The superior gluteal nerve is spared as it has a take-off proximal to the muscle. Conversely, PS may occur secondary to lower lumbar radiculopathy. Produces pain in the sciatic distribution and weakness of external rotation and abduction of the hip. Signs: Freiberg test (pain with forced internal rotation of the hip with thigh extension) or the Pace test (pain on resisted abduction/external rotation of the hip). No well designed studies of treatments. Advocated therapies include: PT, stretching, injection of the muscle localized by digital rectal exam taking care not to inject the sciatic nerve itself & piriformis muscle section. Sometimes long-lasting relief can follow injection with local anesthetic. Use of botulinum toxin (Botox®) injections has been described
9. more peripheral involvement (i.e. neuropathy) that may be confused with radiculopathy. Including:
A. femoral neuropathy mistaken for L4 radiculopathy (see below)
B. proximal sacral plexus lesion mistaken for S1 radiculopathy (see below)
C. diabetic neuropathy (see page 796) including diabetic amyotrophy
D. tumors (see below)
EXTRASPINAL TUMORS CAUSING SCIATICA
![]() Pain characteristics: pain is almost always insidious in onset30. It may be intermittent initially, but eventually all patients develop pain that is constant, progressive and unaffected by position or rest30. Significant night pain is described in ≈ 80%.
Pain characteristics: pain is almost always insidious in onset30. It may be intermittent initially, but eventually all patients develop pain that is constant, progressive and unaffected by position or rest30. Significant night pain is described in ≈ 80%.
Straight leg raising was positive in most, but in more than half the pain was localized to a specific point along the course of the nerve, distal to the sciatic notch30. Conservative treatment brings either no or only temporary relief.
Approximately 20% will have a previous history of tumor (usually neurofibromatosis or previous malignancy). Malignancies include30: metastatic lesions, primary bone sarcomas (chondrosarcoma…), soft-tissue sarcomas (liposarcoma…). Benign tumors include: lipoma, neurofibroma, schwannoma, aneurysmal bone cyst of the sacrum, giant cell tumor of the sacrum (see page 742), tenosynovial giant cell tumor.
In two-thirds of cases, a detailed medical history and physical exam allowed localization and even determining the nature (bone tumor vs. soft-tissue) of the lesion30. Radiographs that show the entire pelvis and the proximal femur will demonstrate almost all tumors in these locations30, 32.
FEATURES DIFFERENTIATING RADICULOPATHY IN SCIATICA
Sciatica may result from nerve root involvement within the spinal canal (e.g. with lumbar disc herniation). Clinically this produces a nerve root syndrome (see Nerve root syndromes, page 445). Spinal imaging studies (MRI, myelogram/CT) will usually detect nerve root compression here. More peripheral involvement may be difficult to image.
L4 involvement
Femoral neuropathy is often mistakenly identified as an L4 radiculopathy. Distinguishing features are shown in Table 35-2.
L5 involvement
Peroneal nerve palsy may be mistaken for L5 radiculopathy (see Foot drop, page 1194).
S1 involvement
Outside the spinal canal, S1 can also be involved as it enters the sacral plexus, e.g. by a pelvic tumor. In plexus lesions, EMG will show sparing of the paraspinal muscles (these nerves exit in the region of the neural foramen) and the gluteus maximus and medius (superior and inferior gluteal nerves take-off just distal to the paraspinal nerves).
Table 35-2 Distinguishing femoral neuropathy from L4 radiculopathy
|
Feature |
Femoral neuropathy |
L4 radiculopathy |
|
Sensory loss |
||
|
distribution (see Figure 5-13, page 94) |
anterior thigh |
dermatome from ≈ knee to medial malleolus, spares anterior thigh |
|
Muscle weakness |
||
|
iliopsoas |
weak |
normal |
|
thigh adductors |
normal (innervated by obturator nerve) |
may be weak |
|
quadriceps |
weak |
weak |
35.1.3. Acute paraplegia or quadriplegia
Entities causing spinal cord compression usually present as: paraplegia or - paresis (or quadriplegia/paresis), urinary retention (may require checking post-void residual to detect), and impaired sensation below level of compression. May develop over hours or days. Reflexes may be hyper- or hypoactive. There may or may not be a Babinski sign. Excluding trauma, the most common cause is compression by tumor or bone.
Etiologies
Some overlap with myelopathy. For items with asterisk, see Myelopathy, page 1185:
1. in infancy (may produce “floppy infant syndrome”)
A. spinal muscular atrophy (the most severe form is called Werdnig-Hoffmann disease and is usually fatal within months): autosomal recessive congenital disease of childhood with degeneration of anterior horn cells. Only rarely evident at birth (where it presents as a paucity of movement), produces weakness, areflexia, muscle and tongue fasciculations with normal sensation. Severe cases progress over the first year or two to quadriplegia
B. spinal cord injury during parturition: a rare sequela of breech delivery
C. congenital myopathies: e.g. infantile acid maltase deficiency (Pompe disease)
D. infantile botulism: ileus, hypotonia, weakness, mydriasis, Claustridium botulinum bacteria and toxin in feces
2. traumatic spinal cord injury
A. major trauma: diagnosis is usually evident
B. minor trauma: may cause cord injury in setting of spinal stenosis, may → central cord syndrome (see Central cord syndrome, page 948)
C. atlantoaxial dislocation: from major trauma or due to instability from tumor or rheumatoid arthritis (see page 495)
3. congenital
A. extradural spinal cord compression by bone secondary to cervical hemivertebra (symptoms not present at birth, may develop decades later, occasionally after minor trauma)
B. cervical stenosis (usually with superimposed spondylosis): quadriplegia or central cord syndrome may follow minor trauma (see page 948)
C. achondroplastic dwarfism: spinal stenosis (animal model: dachshund)
D. syringomyelia: usually presents with central cord syndrome
4. metabolic
A. combined system disease*: see page 1187
B. thallium poisoning: usually causes sensory and autonomic symptoms, quadriplegia and dysarthria may be seen in severe cases
C. central pontine myelinolysis: see page 11
5. infectious
A. epidural spinal infection (abscess or empyema)*
B. post-viral (or post-vaccination): may be a transverse myelitis*
6. peripheral neuromuscular disorder*
A. Guillain-Barré syndrome: classically an ascending paralysis (see page 66), but paraparesis mimicking a spinal cord lesion is an unusual variant33
B. myopathies
7. neoplastic*: spinal cord tumors
8. autoimmune*
9. vascular
A. acute pontomedullary infarction: age usually > 50 yrs. Patient is quadriplegic, alert, with bulbar palsies (eye movement abnormalities, impaired gag and speech)
B. spinal cord infarction*: including AVM, radiation myelopathy…
10. miscellaneous compressive*: including epidural hematoma, bony compression, epidural lipomatosis
11. functional: hysteria, malingering
12. bilateral cerebral hemisphere lesion (involving both motor strips): e.g. post-cerebral irradiation or parasagittal lesion. Will not have sensory level
* for items with asterisk, see Myelopathy, page 1185 for details
35.1.4. Hemiparesis or hemiplegia
May be produced by anything that interrupts the corticospinal tract from its origin in the pyramidal cells of Betz in the motor strip down to the cervical spine. This results an upper motor neuron paralysis (see Table 24-3, page 786) which should also produce long tract findings, including Babinski sign ipsilateral to hemiplegia. Etiologies include:
1. lesions of the cerebral hemisphere in the region of the contralateral motor strip. Large lesions may also involve sensory cortex producing reduced sensation ipsilateral to the hemiparesis
A. tumor (neoplasm): primary or metastatic
B. traumatic: epidural or subdural hematoma, hemorrhagic contusion of the brain, compression by depressed skull fracture
C. vascular:
1. infarction
a. ischemic: embolic, low flow (due to atherosclerosis, arterial dissection…)
b. hemorrhagic: intracerebral hemorrhage, aneurysmal SAH…
2. TIA (see page 1010)
D. infection: cerebritis, abscess
2. lesions of the contralateral internal capsule: produces pure motor hemiplegia without sensory loss. Most common etiology is ischemic lacunar infarct
3. lesions of the brainstem: ischemic infarct, hemorrhage, tumor
4. lesions of cervicomedullary junction: foramen magnum lesions (see page 1212)
5. unilateral spinal cord lesions above ≈ C5 ipsilateral to the weakness producing a Brown-Séquard syndrome with contralateral sensory loss to pain and temperature (see page 950). For etiologies, see page 951
6. hypoglycemia can sometimes be associated with hemiparesis that clears after administration of glucose
 In a patient with unexplained hemiparesis/hemiplegia, especially after trauma, consider carotid dissection.
In a patient with unexplained hemiparesis/hemiplegia, especially after trauma, consider carotid dissection.
35.1.5. Low back pain
The following considers primarily low back pain (LBP) without radiculopathy or myelopathy, although some overlap occurs. Trauma is usually obvious and is not discussed. See Sciatica on page 1188 for differential diagnosis of that and also Low back pain and radiculopathy on page 428 for evaluation.
ACUTE LOW BACK PAIN
Similar to list for myelopathy (see page 1185). Most cases are non-specific (e.g. lumbosacral sprain), only 10-20% can be given a precise pathoanatomical diagnosis34:
1. patients writhing in pain should be evaluated for an intraabdominal or vascular condition (e.g. pain of aortic dissection is typically described as a “tearing” pain): patients with neurogenic LBP tend to remain as still as possible, possibly needing to change positions at intervals
2. unrelenting pain at rest:
A. spinal tumor (intradural or extradural) (see page 728)
1. primary or metastatic spine tumor: suspected in patients with pain duration > 1 month, unrelieved by bed rest, failure to improve with conservative therapy, unexplained weight loss, age > 50 yrs35
2. nocturnal back pain relieved by aspirin is suggestive of osteoid osteoma or benign osteoblastoma36 (see page 736)
B. infection (especially in IV drug abusers, diabetics, post spinal surgery, immunosuppressed patients, or those with pyelonephritis or UTI post-GU surgery). Fever is somewhat insensitive for spinal infections. Spine tenderness to percussion has 86% sensitivity with bacterial infections, but a low specificity of 60%35. Types of infections include:
1. discitis
2. spinal epidural abscess: should be considered in patients with back pain, fever, spine tenderness, or skin infection (furuncle)
3. vertebral osteomyelitis
C. inflammatory:
D. sacroiliitis: may produce pain and tenderness over one or both SI joints
1. pelvic x-rays may show sclerosis of one or both sacroiliac joints
a. bilateral & symmetric
i. ankylosing spondylitis (see page 502): morning back stiffness, no relief at rest, improvement with exercise37. Usually seen in males with symptom onset before age 40 yrs. Positive Patrick’s test (see page 444) and pain on compressing the pelvis with the patient in the lateral decubitus position
ii. Reiter syndrome: a reactive arthritis (usually 1-3 weeks following certain bacterial infections) with involvement of at least one other non-joint area (urethritis, uveitis/conjunctivitis, skin lesions, mucosal ulcerations…). 75% are HLA-B27 positive
iii. may occur in Crohn’s disease
b. bilateral & asymmetric
i. psoriatic arthritis
ii. rheumatoid arthritis: adult & juvenile forms
c. unilateral
i. gout
ii. osteoarthritis
iii. infection
3. evolving neurologic deficit (cauda equina syndrome: perineal anesthesia, urinary incontinence or urgency or retention, progressive weakness) all require emergent diagnostic evaluation to rule-out treatable conditions such as:
A. spinal epidural abscess: see page 376
B. spinal epidural hematoma: see page 515
C. spinal tumor (intradural or extradural): see page 728
D. massive central disc herniation: see page 446
4. pathologic fracture: acute pain in patients at risk for osteoporosis or with known Ca should prompt evaluation for pathologic fractures
A. lumbar compression fracture: see Osteoporotic spine fractures, page 992
B. sacral insufficiency fracture38: especially in rheumatoid arthritis patients on chronic steroids, often with no antecedent history of trauma. May cause back pain and/or radiculopathy. Often missed on plain films, best seen on CT, but may also be detected on bone scan
5. coccydynia: pain and tenderness around the coccyx (see page 516)
6. tears in the anulus fibrosus (“anular tears”)39 (NB: also present in 40% of asymptomatic patients between 50-60 yrs age, and 75% between 60-70 yrs40)
7. rarely following subarachnoid hemorrhage (SAH) due to irritation of lumbar nerve roots and dura: usually accompanied by other signs of SAH (see page 1035)
8. myalgia: may be a side-effect of “statins” (drugs used to lower serum concentration of LDL cholesterol), sometimes with accompanying weakness and rarely with severe rhabdomyolysis and myoglobinuria leading to renal failure (risk may be increased with renal or hepatic dysfunction, advanced age, hypothyroidism, or serious infection)41
9. drug induced
A. statins: see above under myalgia
B. phosphodiesterase type 5 (PDE5) inhibitors used for erectile dysfunction: all may be associated with LBP, but the incidence is higher with tadalafil42, etiology unknown. Usually occurs 12-24 hours post-dose and resolves by 48 hours. Most respond to simple analgesics
SUBACUTE LOW BACK PAIN
10% have LBP that persists > 6 weeks.
Differential diagnosis
Includes causes of acute LBP (above) and also:
1. continued pain at rest should prompt evaluation for spinal osteomyelitis (especially with fever and elevated ESR) or neoplasm if not already done
2. plain spine x-rays may show possibly causative conditions, although many or all of the following may also be seen in asymptomatic patients
A. spondylolisthesis (see page 475)
B. spinal osteophytes
C. lumbar stenosis
D. Schmorl’s node or nodule: disc herniation through cartilaginous end-plate into vertebral body (NB: may also be seen in 19% of asymptomatic patients43) (see page 455)
CHRONIC LOW BACK PAIN
After 3 months, only ≈ 5% of patients will continue to have persistent symptoms. A structural diagnosis is possible in only ≈ 50% of these patients. These patients account for 85% of the cost in lost work and compensation34. Differential diagnosis includes causes of acute and subacute LBP listed above, as well as:
1. degenerative conditions
A. degenerative spondylolisthesis (see page 475)
B. spinal stenosis (affecting the spinal canal)
C. lateral recess syndrome
2. spondyloarthropathies
A. ankylosing spondylitis: look for erosive changes adjacent to SI joint and positive test for HLA-B27 antigen
B. Paget’s disease of the spine: vertebral involvement is very common in a patients with Paget’s disease
3. osteitis condensans ilii: increased density in ilium, usually asymptomatic (incidental) finding. Occasionally may produce low back pain or tenderness. Usually found in women who have been pregnant
4. psychological overlay: including secondary gain (financial, emotional…)
35.1.6. Foot drop
![]() Key concepts:
Key concepts:
• weak anterior tibialis (foot extension) innervated by deep peroneal nerve (L4, 5)
• most common etiologies: L4/L5 radiculopathy, common peroneal nerve palsy
• in a patient with foot drop, check posterior tibialis (foot inversion) and gluteus medius (internal rotation of flexed hip) - both are spared in peroneal nerve palsy and both should be involved with L4/5 radiculopathy
• EMG can assist in localization and prognostication
Definition: weakness of anterior tibialis (primarily L4 and to a lesser extent L5), often accompanied by a weak extensor digitorum longus and extensor hallicus longus (primarily L5 with some S1 contribution), all of which are innervated by the deep peroneal nerve.
With common peroneal nerve (CPN) palsy, there is sparing of posterior tibialis (foot inversion, innervated by posterior tibial nerve) and gluteus medius (internal rotation of the thigh with the hip flexed, innervated by superior gluteal nerve, primarily L5 with some L4, the takeoff is shortly after the roots exit from neural foramen). With L4 or L5 root lesions these muscles will also be weak, see Table 35-4. Flail foot results from paralysis of dorsiflexors plus plantarflexors, e.g. in sciatic nerve dysfunction as can occur during surgery for hip fracture/dislocation44 or injection injuries (IM injections should be give superiorly and laterally to a line drawn between the posterior superior iliac spine and the greater trochanter of the hip). NB: the pero-neal division of the sciatic nerve tends to be more vulnerable to injury than the tibial division.


Abbreviations
CPN = common peroneal nerve
DPN = deep peroneal nerve
IGN = inferior gluteal nerve
SGN = superior gluteal nerve
Etiologies of foot drop:
Three major categories: 1) muscular, 2) neurologic, 3) anatomic.
1. peripheral nerve palsies (more common) (see Table 35-3 and Table 35-4)
A. peroneal nerve injury (also, see Common peroneal nerve palsy, page 820 for details including etiologies). Branches that may be involved:
1. deep peroneal nerve: isolated foot drop with minimal sensory loss (except possibly in great toe web space)
2. superficial peroneal nerve: weakness of peroneus longus and brevis (foot eversion) with no foot drop. Sensory loss: lateral aspect of lower half of leg and foot
3. common peroneal nerve: combination of above (i.e. foot drop + weak foot eversion, with sparing of tibialis posterior (foot inversion). Sensory loss: lateral aspect of lower half of leg and foot)
B. L5 radiculopathy: (or, less commonly, L4). The most common cause is HLD at L4-5, other etiologies include: lumbar spinal stenosis at L4-5, sacral ala fracture (see page 997)
![]() results in pain and/or sensory changes in L5 (or L4) dermatome
results in pain and/or sensory changes in L5 (or L4) dermatome
![]() weakness with radiculopathy tends to be more pronounced in distal muscles (e.g. anterior tibialis) than in proximal (e.g. gluteus maximus)
weakness with radiculopathy tends to be more pronounced in distal muscles (e.g. anterior tibialis) than in proximal (e.g. gluteus maximus)
![]() painless foot drop is unlikely to be due to radiculopathy; consider peroneal neuropathy, diabetic neuropathy, lesion anywhere along pyramidal tract, motor neuron disease…
painless foot drop is unlikely to be due to radiculopathy; consider peroneal neuropathy, diabetic neuropathy, lesion anywhere along pyramidal tract, motor neuron disease…
C. lumbar plexus injury
D. lumbosacral plexus neuropathy: see page 795
E. injury to lateral trunk of sciatic nerve
F. peripheral neuropathy: weakness tends to be greater distally, producing wrist or foot drop. Classic example: Charcot-Marie-Tooth (see page 793), findings tend to be rather dramatic in spite of the fact that it often doesn’t seem to bother the patient very much
G. early in the course of motor neuron disease (ALS)
H. heavy metal poisoning
2. central nervous system causes (foot drop here is usually painless)
A. cortical lesion (UMN): parasagittal lesions in region of motor strip (sensation will be spared if the lesion does not extend posteriorly to the sensory cortex)45. There may be a Babinski sign or hyperactive Achilles reflex (so-called “spastic foot drop”). Usually painless
B. spinal cord injury: including cervical spinal myelopathy
3. non-neurogenic causes
A. muscular dystrophy
B. lead toxicity: in children may cause foot drop with no sensory loss
C. anterior compartment syndrome
Clinical
Loss of dorsiflexion causes foot slap with the front of the foot when the heel strikes the ground while walking. Also during the swing phase of gait the front of the foot may snag the ground (especially on uneven surfaces) which may cause tripping; thus patients develop steppage gait (exaggerated thigh & knee flexion) on the affected side. Associated weakness of tibialis posterior, when present (e.g. with L5 radiculopathy) destabilizes the ankle permitting eversion which also predisposes to falls and to ankle fractures. Chronic foot drop may produce achilles tendon contracture with talipes equinus.
Wasting of the extensor digitorum brevis may be seen.
Laboratory evaluation
1. bloodwork: glucose, ESR
2. EMG: can help differentiate L5 radiculopathy from peroneal nerve palsy, plexus lesion (see Table 35-4) or motor neuron disease (see page 821 for details)
35.1.7. Weakness/atrophy of the hands/UEs
Hand/UE weakness or atrophy with relatively preserved function in the LEs.
1. cervical spondylosis: often causes sensory disturbance (see page 485)
2. cervical radiculopathy: see page 461
3. amyotrophic lateral sclerosis (ALS): no sensory involvement. One of the few causes of clinically prominent fasciculations (see page 65 for details of ALS, see page 1188 for other distinguishing features, see page 786 for fibrillations)
4. spinal cord pathology
A. central cord syndrome: typically causes more involvement (weakness, sensory disturbance) in the UE than the LE (see page 948)
B. syringomyelia: usually burning dysesthesias of the hands with dissociated sensory loss (see page 510)
5. brachial plexus injury: see page 801
6. brachial plexus neuropathy (includes Parsonage-Turner syndrome): see page 794
7. peripheral nerve problems, including
A. carpal tunnel syndrome: see page 808
B. ulnar neuropathy: see page 812
C. other peripheral nerve entrapment syndromes: see page 804
8. foramen magnum lesions (see page 1212): can cause (Bell’s) cruciate paralysis46 due to compression above the pyramidal decussation which produces bilateral UE weakness and possibly atrophy of the hands with sparing of the LEs47 (in the differential diagnosis for central cord syndrome). Compression on one side may produce the similarly named but clinically different hemiplegia cruciata (spastic palsy of one UE and the contralateral LE)47
9. thoracic outlet syndrome: see page 822
10. botulism: see page 1202
11. pharyngeal-cervical-brachial variant of Guillain-Barré syndrome: see page 68
ATROPHY OF THE FIRST DORSAL INTEROSSEOUS MUSCLE
Etiologies: either C8/T1 nerve root or ulnar nerve involvement (either may be focal or diffuse). There are 4 main differential diagnoses:
1. ulnar neuropathy: check median nerve to see if findings extend to a nearby but separate nerve
A. at the elbow: see page 813
B. at Guyon’s canal: see page 816
2. nerve root involvement:
A. cervical radiculopathy: C8 or T1
B. nerve root avulsion: weakness + sensory loss with normal SNAP on EMG (see page 270) usually with a history of precipitating trauma
3. lower brachial plexus involvement
A. thoracic outlet syndrome: see page 822
B. Pancoast tumor: see page 794
4. neurodegenerative disorders
A. amyotrophic lateral sclerosis (ALS): see page 65
B. multifocal motor neuropathy (MMN): a chronic dysimmune neuropathy with asymmetric muscle wasting, cramping & LE twitching (see page 1188)
35.1.8. Radiculopathy, upper extremity (cervical)
See Weakness/atrophy of the hands/UEs above. In addition to those items:
1. primary shoulder pathology: characteristically, pain is aggravated by active and/or passive shoulder movement. In general, shoulder pathology does not produce pain referred to the neck
A. rotator cuff tear
B. bicipital tendonitis: tenderness over biceps tendon
C. subacromial bursitis: there may be tenderness over the AC joint
D. adhesive capsulitis
E. impingement syndrome: the “empty can test” is usually positive (each arm held out in front, 30° lateral to straight forward, thumbs pointing down, as in emptying out a soda can. Examiner pushes down on the patient’s hands while the patient resists. Test is positive if it reproduces pain)
2. shoulder pain is very common in polymyalgia rheumatica (see page 77), typically worsens with movement
3. interscapular pain: a common location for referred pain with cervical radiculopathy, may also occur with cholecystitis or some shoulder pathologies
4. MI: some cases of cervical radiculopathy (especially left C6) may present with symptoms that are suggestive of an acute myocardial infarction
5. complex regional pain syndrome AKA reflex sympathetic dystrophy: may be difficult to distinguish from cervical radiculopathy. Stellate ganglion blocks may help48. Also see page 576
35.1.9. Neck pain (cervical pain)
This section deals primarily with axial neck-pain without radicular features. For radicular features, see Radiculopathy, upper extremity (cervical) above.
1. cervical spondylosis (including facet arthritis)
2. cervical sprain: including whiplash associated disorder
3. fracture of the cervical spine: with upper cervical spine fractures (e.g. odontoid), patients characteristically hold their head in their hands, especially when going from recumbent to upright position
A. traumatic
B. pathologic (tumor invasion, rheumatoid arthritis)
4. occipital neuralgia: see page 804
5. herniated cervical disc:
A. lateral herniated disc: if symptomatic, tends to produce more radicular symptoms in the UE than actual neck pain
B. central disc herniation: if symptomatic, tends to produce myelopathy, does not produce any neck pain whatsoever in many cases
6. abnormalities of the craniocervical junction:
A. Chiari 1 malformation: see page 233
B. atlantoaxial subluxation
7. fibromyalgia: idiopathic chronic pain syndrome characterized by widespread nonarticular musculoskeletal pain, nodularity and stiffness49, 50 without pathologic inflammation. Possible link to neuroendocrine dysfunction51. Afflicts 2% of the population50, female:male ratio is 7:1. No diagnostic laboratory study. May be associated with psychiatric illness and multiple non-specific somatic complaints including malaise, fatigue, impaired sleep, GI complaints and cognitive impairment
8. Eagle’s syndrome: elongation of the styloid process. Surgical resection can ameliorate the pain. Two variants:
A. typical variant: history of tonsillectomy. Pharyngeal pain, dysphagia and otalgia
B. second variant: AKA carotid artery-styloid process syndrome. Carotidynia radiating into ipsilateral eye and vertex
35.1.10. Burning hands/feet
1. spinal cord syndromes:
A. central cord syndrome (CCS): see page 948
B. burning hands syndrome: a possible variant of CCS, described in football-related cervical spine injury (see page 980)
C. numb-clumsy hand syndrome: seen in cervical myelopathy (see page 488)
2. complex regional pain syndrome (CRPS) AKA reflex sympathetic dystrophy: see page 576
3. peripheral neuropathy
A. diabetic amyotrophy AKA Bruns-Garland syndrome: see page 796
4. erythermalgia AKA erythromelalgia: rare disorder characterized by erythema, edema, increased skin temperature, and burning pain of the hands and/or feet. Usually refractory to medical management, some success reported with epidural bipuvicaine52, lidocaine patches53, or cold soaks
A. primary erythermalgia: etiology is idiopathic
B. secondary erythermalgia: associated with autoimmune and rheumatologic factors
5. vascular:
A. occlusive arterial disease: atherosclerosis, Raynaud’s syndrome
B. venous insufficiency
35.1.11. Muscle pain/tenderness
1. fibromyalgia: see above
2. myopathy
3. “statin” myopathy
4. diffuse severe sensitivity to light touch is a marker of nonorganic pain54
35.1.12. Lhermitte’s sign
Really a symptom. Electrical shock-like sensation radiating down the spine usually provoked by neck flexion (shocks radiating up the spine are sometimes referred to as reverse Lhermitte’s sign). Classically attributed to MS, but may occur in any process involving primarily the posterior columns.
Etiologies:
1. multiple sclerosis (MS): see page 61
2. cervical spondylosis
3. subacute combined degeneration: check for vitamin B12 deficiency (see page 1187)
4. cervical cord tumor
5. cervical disc herniation
6. radiation myelopathy: see page 772
7. Chiari type I malformation: see page 233
8. central cord syndrome: see page 948
9. SCIWORA (spinal cord injury without radiographic abnormality): see page 974
35.1.13. Encephalopathy
Many etiologies are similar to that for coma (see page 280). EEG may be helpful in distinguishing some etiologies (see page 266).
1. a rare cause may be (spontaneous) intracranial hypotension (see page 305)
2. hypertensive encephalopathy from malignant hypertension
35.1.14. Syncope and apoplexy
Syncope may be defined as one or more episodes of brief loss of consciousness (LOC) with prompt recovery (this term is considered by many to signify a vasovagal episode). The uncommonly used term lipothymia may be less likely to imply an etiology. Prevalence may be as high as ≈ 50% (higher in the elderly). Apoplexy is traditionally considered a form of hemorrhage, usually intracerebral. The recovery from apoplexy would therefore usually be slower than for syncope.
Etiologies (adapted55, 56)
1. vascular: a few myotonic jerks may be seen in cerebral ischemia
A. cerebrovascular
1. subarachnoid hemorrhage (most commonly aneurysmal)
2. intracerebral hemorrhage
3. brain stem infarction
4. pituitary apoplexy (rare): see page 635
5. vertebrobasilar insufficiency (VBI): see page 1158
6. rarely with migraine
B. cardiovascular
1. Stokes-Adams attacks: disorder of AV-node conduction in the heart resulting in syncope with bradycardia
2. carotid sinus syncope: minimal stimulation (e.g. tight shirt collar, syncope while shaving…) causes reflex bradycardia with hypotension, more common in patients with carotid vascular disease. Bedside carotid massage with ECG and BP monitor may diagnose56
3. cardiac standstill: seen rarely in patients with glossopharyngeal neuralgia (see page 563)
4. vasodepressor syncope (the common faint), AKA vasovagal response, and recently AKA neurocardiogenic syncope57: the most common cause of transient LOC. Hypotension usually with any of the following autonomic manifestations: pallor, nausea, heavy perspiration, pupillary dilatation, bradycardia, hyperventilation, salivation. Usually benign. Most common in age < 35 yrs
5. orthostatic hypotension: drop in SBP ≥ 25 mm Hg on standing
6. triggered syncope: includes micturition, tussive syncope, weight lifting syncope… (most involve elevation of intrathoracic pressure)
2. infectious
A. meningitis
B. encephalitis
3. seizure: in general, there are involuntary movements and confusion afterwards, lasts at least several minutes. Todd’s paralysis may follow and usually resolves slowly over a period of a few hours (see page 396). There may be irritative specialsense phenomena (visual, auditory, or olfactory hallucinations)
A. generalized
B. complex partial
C. akinetic seizure
D. drop attack (loss of posture without LOC): seen in Lennox-Gastaut
4. metabolic: hypoglycemia (may produce seizure, usually generalized)
5. miscellaneous
A. intermittent ventricular obstruction: the classic example is a colloid cyst of the third ventricle, but this mechanism is questionable (see page 665)
B. narcoleptic cataplexy: narcolepsy is characterized by somnolence and sudden attacks of weakness (cataplexy) when awake. Easy arousal and lack of post-ictal drowsiness distinguishes cataplexy from a seizure
C. psychogenic
6. intracranial hypotension: usually with CSF shunt when upright (see page 325)
7. unknown: in ≈ 40% of cases no cause can be diagnosed
Practical approach to syncope
The core of diagnosis and management are the H&P, orthostatic vital signs, and the ECG, with a combined diagnostic yield of 50%58 covering:
1. reflex mediated such as vasovagal or valsalva/stress-induced: 36 -62%
2. cardiac valvular etiology or arrhythmia: 10-30%
3. orthostatic due to autonomic dysregulation, dehydration or polypharmacy: 2-24%
4. cerebrovascular due to stroke: ≈ 1%
5. seizure
Evaluation:
1. history: includes
A. medication list: look for drugs that may cause orthostatic hypotension, especially blood pressure medication, beta blockers
B. precipitating factors: e.g. change in position, sensitivity to tight collars…
C. premonitory factors: e.g. sweating and tremulousness may signify hypoglycemia, bradycardia is associated with vasovagal events, tonic-clonic movements may occur with a seizure
D. post-ictal emergence: usually rapid after a simple faint, slower after seizure which may also exhibit Todd’s paralysis (see page 396)
2. cardiovascular etiologies: Testing is also guided by H&P, vital signs & ECG:
A. cardiac arrhythmia evaluation: 12-lead ECG & 24-hour Holter monitor, and may lead to electrophysiologic (EP) testing/intervention58, 59
B. abnormal orthostatics warrants a formal tilt-table test
C. history of cardiomyopathy or CAD merits an echocardiogram and formal stress testing. These results determine the need for cardiac catheterization
3. neurologic etiologies: comprise < 1% of cases60. In the absence of clinical evidence of a neurologic etiology, neurodiagnostic testing (EEG, CT scan, MRI/MRA, carotid doppler) have a diagnostic yield of 2-6%. ![]() These tests are warranted only when clinically indicated59 (seizures, altered consciousness, gradually resolving Todd’s paralysis, known history of cerebrovascular compromise). Tests include:
These tests are warranted only when clinically indicated59 (seizures, altered consciousness, gradually resolving Todd’s paralysis, known history of cerebrovascular compromise). Tests include:
A. unenhanced brain CT: rules out most acute neurosurgical etiologies (bleed, hydrocephalus, edema which may be associated with tumor)
B. MRI without and with enhancement in cases with unexplained CT findings, or with a negative CT but high suspicion of a CNS etiology
C. seizure evaluation: when symptoms suggest possible seizure:
1. EEG: usually a sleep deprived EEG. Not very sensitive
2. 24 hour video EEG monitoring: in cases with high index of suspicion of seizures or nonepileptic seizures
Management: Admission and inpatient management is warranted for patients with diagnosed cardiac or neurologic syncope, either by suggestive history (family history of sudden death, syncope during exertion, witnessed seizure) or diagnostic testing (arrhythmia, severe orthostatic changes, hemodynamic instability)58, 61.
35.1.15. Transient neurologic deficit
For apoplexy, etc., see Syncope and apoplexy, page 1199.
The first three etiologies listed below cover most cases of transient neurologic deficit:
1. transient ischemic attack (TIA): temporary neurologic dysfunction as a result of ischemia. Maximum deficit usually at onset. Most resolve in < 20 mins (see page 1010)
2. migraine: unlike TIA, tends to progress in a march-like fashion over several minutes. May or may not be followed by headache (see Migraine, page 57)
3. seizure: may be followed by a Todd’s paralysis (see page 396)
4. TIA-like syndrome
A. “tumor TIA”: a transient deficit in a patient with a tumor, may be clinically indistinguishable from an ischemic TIA
B. TIA-like symptoms may occur as a prodrome to a lobar intracerebral hemorrhage62, 63 in cases of cerebral amyloid angiopathy (CAA). Unlike typical TIAs, these usually consist of numbness, tingling or weakness that gradually spreads in a manner reminiscent of a Jacksonian-march and may cross-over vascular territories (see page 1124). Caution: antiplatelet drugs and anticoagulation may increase the risk of hemorrhage in patients with CAA (see page 1122)
C. chronic subdural hematoma: may cause recurrent TIA-like symptoms of the involved hemisphere64 (including transient aphasia, hemisensory or motor abnormalities). The duration of symptoms tends to be longer than the typical TIA64. Postulated mechanisms include:
1. electrical basis: the possibility of epileptic activity due has not been supported in the literature; however, spreading depression of Leao has been considered65
2. impairment of venous outflow by compression of surface veins
3. compromised regional cerebral perfusion by indirect shifting of the anterior and posterior cerebral arteries66
4. transient ICP elevations → variations in cerebral perfusion pressure
35.1.16. Ataxia/balance difficulties
1. cerebellar origin: usually with involvement of UEs in addition to LEs
A. cerebellar tumors
B. cerebellar hemorrhage
C. acute cerebellar ataxia: usually follows viral infection in a child < 3 years. Usually self-limited with good prognosis for complete recovery
2. spinal cord: usually worse with eyes closed (loss of proprioceptive input)
A. spinal stenosis
B. neoplastic cord compression
C. syringomyelia (may be part of Chiari malformation)
3. degenerative
A. ataxia-telangiectasia syndrome
B. ataxia oculomotor apraxia
C. Friedreich’s ataxia
D. spinocerebellar degeneration
4. metabolic/nutritional
A. vitamin B12 deficiency
B. drugs
1. AEDs (especially phenytoin or carbamazepine)
2. alcohol: acutely with intoxication and chronic
3. heavy metal poisoning
5. conditions that may mimic ataxia
A. weakness
B. peripheral neuropathy
C. dizziness: including orthostatic hypotension (see Dizziness and vertigo, page 840)
6. peripheral neuropathy:
A. ataxia can occur with Guillain-Barré syndrome (see page 66), especially Miller Fisher variant (see page 68)
B. balance difficulties are common with chronic immune demyelinating polyradiculoneuropathy (CIDP) (see page 68)
35.1.17. Diplopia
1. cranial nerve palsy of any one or combination of III, IV (rare), or VI
A. for multiple cranial nerve palsies, see Multiple cranial nerve palsies (cranial neuropathies) below
B. VI palsy: can occur with increased intracranial pressure, e.g. in idiopathic intracranial hypertension (pseudotumor cerebri) (see page 713), sphenoid sinusitis… (see page 836 for other causes of abducens palsy)
C. isolated muscle paresis of III suggests nuclear lesion or myasthenia gravis
2. intraorbital mass compressing extraocular muscles
A. orbital pseudotumor: see page 837
B. meningioma
3. Graves’ disease: hyperthyroidism + ophthalmopathy (see page 1219)
4. myasthenia gravis
5. giant cell arteritis: see page 74
6. botulism: due to toxin from Claustridium botulinum (in adults: ingested or in wound). N/V, abdominal cramps, and diarrhea often precede neurologic symptoms. Neurologic involvement is typically symmetric. Dry mouth & cranial nerves palsies (diplopia, ptosis, loss of accommodation and pupillary light reflex) are followed by descending weakness. Bulbar paresis (dysarthria, dysphagia, dysphonia, flaccid facial muscles) follows. Muscles of the trunk/extremities and respiration progressively weaken in a descending fashion. Sensory disturbances are absent. Sensorium usually remains clear
7. following head trauma: includes injury to EOMs, orbital hematoma, VI palsy from increased ICP
35.1.18. Anosmia
1. abrupt onset of anosmia
A. severe upper respiratory infection with damage to the neuroepithelium: the most common cause
B. head trauma: second most common cause. Anosmia occurs in 7-15% of patients with significant head trauma
2. gradual onset of anosmia
A. allergic rhinitis and sinus disease67: third most common cause of anosmia (anosmia in this setting may be intermittent)
B. intracranial neoplasms: olfactory groove meningioma (see Foster Kennedy syndrome, page 112), esthesioneuroblastoma (see page 1230)
C. may also be associated with Alzheimer’s disease
D. olfactory sense diminishes with age: ≈ 50% of patients 65-85 years of age have some loss of sense of smell
E. metabolic abnormalities: vitamin deficiency
F. physical blockage of nasal passages: nasal polyps…
G. endocrine abnormalities: diabetes…
H. chemical: alcohol abuse, exposure to solvents68, cocaine (ischemic infarction of olfactory mucosa from vasoconstriction)
3. congenital anosmia: Kallmann syndrome (anosmia with hypogonadotrophic hypogonadism69)
35.1.19. Multiple cranial nerve palsies (cranial neuropathies)
The differential diagnosis is legion. The following is a framework (modified70):
1. congenital
A. Möbius syndrome: AKA congenital facial diplegia. Facial plegia is complete in ≈ 35% (in rest, affects upper face more than lower face, unlike central or peripheral facial palsy), associated with abducens palsy in 70%, external ophthalmoplegia in 25%, ptosis in 10%, lingual palsy in 18%
B. congenital facial diplegia may be part of facioscapulohumeral or myotonic muscular dystrophy
2. infectious
A. chronic meningitis:
1. spirochetal, fungal, mycoplasma, viral (including AIDS)
2. mycobacterial AKA tuberculous (TB) meningitis: 6th nerve involved first and most frequently. CSF shows lymphocytic pleocytosis and hypoglycorrhachia. Smears are usually negative and multiple cultures are needed to diagnose
B. stage II Lyme disease: see page 368. Facial nerve weakness is common, sometimes bilateral (Lyme disease is the most common cause of facial diplegia in endemic areas). Other cranial nerve involvement is rare
C. neurosyphilis: rare nowadays except with AIDS. Diagnosed by serologic testing
D. fungal infection
1. cryptococcal meningitis: CSF analysis for cryptococcal antigen and India ink prep can detect (see page 374)
2. aspergillosis: may extend to the orbit from sinuses and involve cranial nerves
3. mucormycosis (phycomycosis): produces cavernous sinus syndrome, usually occurs in diabetics (see page 836)
E. cysticercosis: especially with basal form (see Neurocysticercosis, page 370)
3. traumatic: especially with basal skull fractures. Lower cranial nerve palsies may occur (sometimes delayed in onset) with occipital condyle fractures (see page 954) or atlanto-occipital dislocation (see page 952)
4. neoplastic (brain stem compression and intrinsic lesions usually also produce long tract findings early). Also see Jugular foramen syndromes, page 115
A. chordoma: see page 676
B. sphenoid-ridge meningioma
C. neoplasms of the temporal bone (often in conjunction with chronic otitis media and otalgia): adenoid cystic carcinoma, adenocarcinoma, mucoepidermoid carcinoma
D. glomus jugulare tumors: often affects nerves IX, X, and XI. May cause pulsatile tinnitus (see Paraganglioma, page 678)
E. carcinomatous or lymphomatous meningitis: CSF pleocytosis and elevated protein. Palsies are painless or associated with diffuse headache. Sensory palsies are common, resulting in deafness and blindness (see page 711)
F. invasive pituitary adenomas involving the cavernous sinus (see page 637): extraocular cranial neuropathies tend to develop after visual field deficits in these tumors, and are less common when compared to other intracavernous solid tumors71
G. primary CNS lymphoma: see page 672
H. multiple myeloma involving the skull base: see page 740
I. intrinsic brain stem tumors: gliomas, ependymoma, metastases…
5. vascular
A. aneurysm: intracranial or cavernous sinus (see page 1056)
B. brain stem CVA: usually also produces long tract findings (see page 114):
1. Weber’s syndrome: Cr N III (usually pupil sparing) + contralateral hemiparesis
2. Millard-Gubler syndrome: Cr N VI + VII + contralateral hemiparesis
C. vasculitis: Wegener’s granulomatosis usually affects eighth nerve in addition to others
6. granulomatous
A. sarcoidosis: ≈ 5% have CNS involvement, usually as fluctuating single or multiple cranial neuropathies (facial nerve is most common, and may be indistinguishable from Bell’s palsy). CSF pleocytosis is common (see page 71)
7. inflammatory
8. neuropathies
A. Guillain-Barré syndrome (GBS): cranial nerve involvement includes facial diplegia, oropharyngeal paresis. Peripheral neuropathy usually presents with ascending weakness, proximal muscle weakness > distal, and absent deep tendon reflexes (see page 66)
B. Miller-Fisher variant GBS: ataxia, areflexia & ophthalmoplegia. Serum marker: anti-GQ1b antibodies
C. idiopathic cranial polyneuropathy: subacute onset of constant facial pain, usually retro-orbital. Frequently precedes sudden onset of cranial-nerve palsies usually involving III, IV & VI, less frequently V, VII, and lower nerves (IX through XII). Olfactory and auditory nerves usually spared. Acute and chronic inflammation of unknown etiology similar to Tolosa-Hunt and orbital pseudotumor. Steroids reduce pain and expedite recovery
9. entrapment in abnormal bone
A. hyperostosis cranialis interna: a rare autosomal dominant abnormality of the bone of the base of the skull causing recurrent facial palsy and other cranial nerve palsies72
B. osteopetrosis: see below
C. Paget’s disease (see page 498) involving the skull: 8th nerve involvement (deafness) is most common. Optic nerve atrophy, and palsies of oculomotor, facial, IX, XI, olfactory nerves and others may also occur73
D. fibrous dysplasia: see page 701
FACIAL DIPLEGIA
Items culled from the above list that have facial diplegia as a prominent finding:
1. congenital: Möbius syndrome, congenital facial diplegia
2. infectious: Lyme disease
3. neuropathies: Guillain-Barré syndrome
4. isolated 4th ventricle (see page 309): compression at the facial colliculus
5. granulomatous: sarcoidosis:
CAVERNOUS SINUS SYNDROME
Multiple cranial nerve palsies (involving any of the cavernous sinus cranial nerves: III, IV, V1, V2, VI) which primarily produce diplopia (due to ophthalmoplegia). Classically the third nerve palsy (e.g. from an enlarging cavernous carotid artery aneurysm) will not produce a dilated pupil because the sympathetics which dilate the pupil are also paralyzed74 (p 1492). Facial pain or altered facial sensation may occur.
For a list of lesions that may produce cavernous sinus syndrome, see page 1219.
OSTEOPETROSIS
AKA “marble bone disease” (there may be confusion with the term osteosclerosis; osteosclerosis fragilis generalisata is the obsolete term for osteopetrosis). A rare group of genetic disorders of defective osteoclastic resorption of bone resulting in increased bone density, may be transmitted either as autosomal dominant or recessive75. The dominant form is usually benign and is seen in adults and adolescents. The recessive (“malignant”) form is often associated with consanguinity, and is similar to hyperostosis cranialis interna (see above), but in addition to the proclivity for the skull, also involves ribs, clavicles, long bones, and pelvis (long-bone involvement results in destruction of marrow and subsequent anemia). Cranial nerves involved primarily include optic (optic atrophy and blindness are the most common neurologic manifestation), facial, and vestibulo-acoustic (with deafness), trigeminal nerve may also be involved. There may also be extensive intracranial calcifications, hydrocephalus, intracranial hemorrhage and seizures.
Bilateral optic nerve decompression via a supraorbital approach may improve or stabilize vision75.
35.1.20. Binocular blindness
1. bilateral occipital lobe dysfunction
A. bilateral posterior cerebral artery flow impairment
1. top of the basilar syndrome
2. increased intracranial pressure
a. hydrocephalus with shunt malfunction
b. pseudotumor cerebri (idiopathic intracranial hypertension): see page 713 c. cryptococcal meningitis: decreased visual acuity (see page 374)
B. trauma: bilateral occipital lobe injury (e.g. contrecoup injury)
2. seizures: epileptic blindness
3. migraine: cortical spreading depression
4. posterior ischemic optic neuropathy: usually in the setting of shock
5. bilateral vitreous hemorrhage: e.g. with SAH (Terson’s syndrome)
6. functional: conversion reaction, hysterical blindness…
35.1.21. Monocular blindness
Due to a lesion anterior to the optic chiasm.
1. Amaurosis fugax: often described as a “shade coming down” over one eye
A. TIA: usually due to occlusion of the retinal artery (see page 1144)
B. giant cell arteritis (GCA): usually due to ischemia of optic nerve or tracts (less commonly due to retinal artery occlusion)76 (see page 75)
2. trauma: optic nerve injury
3. ruptured carotid cavernous aneurysm: resultant carotid cavernous fistula increases intraocular pressure by impeding venous return
4. intraorbital pathology: tumors
5. injury within the globe: retinal detachment, ocular trauma
6. unilateral vitreous hemorrhage: e.g. with SAH (Terson’s syndrome)
35.1.22. Exophthalmos
Alt. spelling: exophthalmus. Definition: abnormal protrusion of the eyeball. Some authors reserve the term exophthalmos for cases due to endocrinopathies and use proptosis (of the eye) for other causes, but these terms are widely used interchangeably.
Criteria: different criteria are proposed. Anterior displacement of 18 mm (Hertal exophthalmometry can be used to measure clinically - requires intact lateral orbital bone). CT criteria: for most accurate results, the patient’s should have their eyes open and fixated on a point in the primary gaze position. position of equator of the globe (widest part) is distal to a line drawn from lateral orbit to medial canthus, > 2/3 of the globe anterior to this line.
Pulsatile
1. carotid cavernous fistula (CCF) (see page 1113)
2. transmitted intracranial pulsation due to defect in orbital roof
A. seen unilaterally e.g. in neurofibromatosis type 1 (see page 723)
B. post-op following procedures that remove orbital roof or wall
3. vascular tumors
Non-pulsatile
1. tumor
A. intraorbital tumor: may be due to mass effect from tumor or to compromised venous drainage from the orbit
1. optic glioma (see page 606)
2. optic sheath neuroma
3. lymphoma
4. optic sheath meningioma77
5. orbital involvement with multiple myeloma: see page 740
6. orbital invasion by invasive pituitary adenoma: see page 637
7. in peds: metastatic neuroblastoma
B. due to hyperostosis from a sphenoid ridge meningioma
2. Graves’ disease (hyperthyroidism + exophthalmos): even though the exophthalmos is usually bilateral with this (80% - see page 1219), thyroid disease is still the most common cause of unilateralproptosis78
3. enlargement of periorbital fat79
4. infection: orbital cellulitis (usually has concomitant sinusitis)
5. inflammatory: orbital pseudotumor. Usually unilateral (see page 837)
6. hemorrhage
A. traumatic
B. spontaneous
7. 3rd nerve palsy: up to 3 mm proptosis from relaxation of the rectus muscles
8. cavernous sinus occlusion (may affect both eyes)
A. cavernous sinus thrombosis (see page 1167)
B. cavernous sinus tumor obstructing venous outflow
9. pseudo-exophthalmos
A. congenital macrophthalmos (bull’s eye)
B. lid retraction: e.g. in Graves’ disease (see page 1219)
C. coronal craniosynostosis can cause a “relative” proptosis (see page 230)
35.1.23. Ptosis
AKA blepharoptosis. Drooping of the upper eyelid.
Distinguished from pseudoptosis (lid droop not resulting from weakness of levator palpebrae superioris (LPS)) which can be due to enophthalmos (globe displaced posteriorly, e.g. with orbital floor blow-out fracture), microphthalmia, blepharospasm, Duane syndrome.
Etiologies of ptosis:
1. congenital: most are simple (autosomal dominant inheritance), complicated ptosis is associated with other findings (e.g. ptosis with ophthalmoplegia)
2. traumatic: injury to eyelid, orbital roof fracture…
3. neurogenic:
A. third nerve palsy (see page 834)
1. involvement of main trunk of third nerve: can occur intradurally or within cavernous sinus. Ptosis may be an early sign of pituitary tumor expansion (apoplexy) (see page 635)
2. involvement of the superior division of the third nerve within the orbit
B. Horner’s syndrome (see page 833): ptosis here is partial (may be a pseudoptosis since weakness is in tarsal muscles, not LPS), and the lower eyelid will higher than the uninvolved contralateral lower eyelid
4. myogenic ptosis
A. botulinum toxin injection (e.g. Botox®)
B. myasthenia gravis
5. mechanical ptosis
A. tumors: neurofibroma, hemangioma, malignant melanoma, mets…
B. extension of mucocele of frontal sinus
6. pharmacologic (drugs). Partial list:
A. corticosteroids: including topical
B. alcohol
C. opium
35.1.24. Pathologic lid retraction
1. hyperthyroidism: see page 1219
2. psychiatric: schizophrenia…
3. steroids
4. Parinaud’s syndrome: see page 114
35.1.25. Macrocephaly
Macrocephaly means increased size of the head80. Although sometimes used synonymously, some contend that the term macrocrania by convention refers to a head circumference > 98th percentile81 (pp 203). Also, not to be confused with macrencephaly AKA megalencephaly (see below). In a pediatric practice the 3 most common etiologies in decreasing order of frequency: familial (parents have big heads), benign subdural fluid collections of infancy (see page 904), and hydrocephalus.
1. with ventricular enlargement
A. (hydrostatic) hydrocephalus (HCP) (see page 311 for etiologies)
1. communicating
2. obstructive
B. hydranencephaly: see page 244
C. constitutional ventriculomegaly: ventricular enlargement of no known etiology with normal neurologic function
D. hydrocephalus ex vacuo: loss of cerebral tissue (more often associated with microcephaly, e.g. with TORCH infections)
E. vein of Galen aneurysms: see below
2. with normal or mildly enlarged ventricles
A. “external hydrocephalus”: prominent subarachnoid spaces and basal cisterns (see External hydrocephalus (AKA benign external hydrocephalus), page 307)
B. subdural fluid
1. hematoma
2. hygroma
3. effusion benign and symptomatic
4. benign subdural collections of infancy (see page 904)
C. cerebral edema: some consider this to be a form of pseudotumor cerebri80
1. toxic: e.g. lead encephalopathy (from chronic lead poisoning)
2. endocrine: hypoparathyroidism, galactosemia, hypophosphatasia, hypervitaminosis A, adrenal insufficiency…
D. familial (hereditary) macrocrania: parents also have large heads, the brains eventually “catch up”
E. idiopathic
F. megalencephaly (AKA macrencephaly): an enlarged brain (see page 245)
G. neurocutaneous syndromes: usually due to increased volume of brain tissue (megalencephaly, see above)80. Seen especially in neurofibromatosis and congenital hypermelanosis (Ito’s syndrome). Less common in tuberous sclerosis and Sturge-Weber. Also seen in the rare hemimegalencephaly syndrome
H. arachnoid cyst (AKA subependymal or subarachnoid cyst)80: a duplication of the ependyma or arachnoid layer filled with CSF. Usually reach maximal size by 1 month of age and do not enlarge further. Treatment is required in ≈ 30% due to rapid enlargement or growth beyond first month. Cyst may be shunted or fenestrated. Prognosis with true arachnoid cyst is generally good (unlike porencephalic cyst) if no increased ICP or progressive macro-cephaly during 1st year of life
I. arteriovenous malformation: especially vein of Galen “aneurysm” (see page 1112). Auscultate for cranial bruit. With vein of Galen aneurysms, macro-cephaly may be due to HCP from obstruction of the sylvian aqueduct80. With other malformations, macrocrania may be due to increased pressure in venous system without HCP
J. brain tumors without hydrocephalus: brain tumors are rare in infancy, and most cause obstructive HCP. Tumors that occasionally present without HCP includes astrocytomas. May also be seen in the rare diencephalic syndrome (tumor of anterior hypothalamus, see page 606)
K. “gigantism syndromes”
1. Soto’s syndrome: associated with advanced bone age on x-ray, and multiple dysplastic features of face, skin and bones
2. exomphalomacroglossia-gigantism (EMG) syndrome: hypoglycemia (from abnormalities in islets of Langerhans), large birth weight, large umbilicus or umbilical hernia and macroglossia
L. “craniocerebral disproportion”80 (see page 904): may be the same as benign extra-axial fluid of infancy
M. achondroplastic dwarf: cranial structures are enlarged but the skull base is small, giving rise to a prominent forehead and an OFC ≥ 97th percentile for age
N. Canavan’s disease: AKA spongy degeneration of the brain, an autosomal recessive disease of infancy prevalent among Ashkenazi Jews. Produces symmetrical low attenuation of hemispheric white matter on CT82 and macrocephaly
O. neurometabolic diseases: usually due to deposition of metabolic substances in the brain. Seen in Tay-Sachs gangliosidosis, Krabbe disease…
3. due to thickening of the skull
A. anemia: e.g. thalassemia
B. skull dysplasia: e.g. osteopetrosis (see page 1204)
35.1.26. Tinnitus
May be either subjective (heard only by patient) or objective (e.g. cranial bruit, can be heard by examiner as well, usually with a stethoscope). Objective tinnitus is almost always due to vascular turbulence (from increased flow or partial obstruction).
Pulsatile tinnitus
Most cases are due to vascular lesions.
1. pulse synchronous:
A. carotid cavernous fistula (see page 1113)
B. AVM:
1. cerebral (pial) AVM
2. dural AVM: see page 1109
C. glomus jugulare tumor: see page 680
D. cerebral aneurysm: (rare) possibly with turbulent flow in giant aneurysm
E. hypertension
F. hyperthyroidism
G. idiopathic intracranial hypertension (pseudotumor cerebri): see page 713
H. transmitted bruit: from heart (e.g. aortic stenosis), carotid artery stenosis (especially external carotid)
I. dehiscent jugular bulb or high riding jugular bulb: normal venous variant
J. rarely with posterior fossa tumors: CP-angle tumors e.g. vestibular schwannoma or meningioma, vascular intraparenchymal tumors e.g. hemangioblastoma (especially in CPA)
K. lesions that can present with a red tympanic membrane
1. aberrant carotid artery in middle ear
2. persistent stapedial artery: rare. Arises from aberrant ICA or from junction of horizontal and vertical petrous ICA. Foramen spinosum is absent on the affected side. Enlargement of anterior tympanic segment of seventh nerve canal
3. glomus tympanicum tumor: see page 680
2. non pulse-synchronous: asymmetrical enlargement of sigmoid sinus and jugular vein may produce a low grade hum
Workup for pulsatile tinnitus:
1. MRI without and with enhancement: to look for tumors, e.g. glomus jugulare
2. angiogram: include internal and external carotid injections
3. tests that are usually not helpful and should not be ordered routinely
A. carotid ultrasound: nonspecific, not sensitive
B. MRI/MRV: may miss small dural fistulas and do not give details needed for treatment for large ones
Non-pulsatile tinnitus
1. occlusion of external ear: cerumen, foreign body
2. middle ear infection (otitis media)
3. otosclerosis
4. stapedial muscle spasms: as occurs in hemifacial spasm
5. CP-angle tumors: including vestibular schwannoma (see page 620)
6. Meniere’s disease: see page 842
7. labyrinthitis
8. endolymphatic sac tumors: e.g as in von Hippel-Lindau disease (see page 668)
9. drugs
A. salicylates: aspirin, bismuth subsalicylate (Pepto Bismol®)
B. quinine
C. aminoglycoside toxicity: streptomycin, tobramicin (tinnitus precedes hearing loss)
35.1.27. Facial sensory changes
1. circumoral paresthesias
A. hypocalcemia
B. syringobulbia
2. unilateral facial sensory changes
A. large vestibular schwannoma
B. trigeminal nerve neuroma
C. compression of the spinal trigeminal tract (large compressive lesions may cause bilateral alteration of facial sensation) that chiefly manifests in diminution of pain and temperature sense with little effect on touch sense83. The tract usually extends as far down as ≈ C2 (although it may occasionally extend down to C4)
35.1.28. Language disturbance
1. aphasia:
A. injury to speech areas of brain
1. Wernicke’s aphasia: classically produces fluent aphasia (normal sentence length & intonation, devoid of meaning) (see page 114)
2. Broca’s aphasia: faltering, dysarthric (see page 114)
3. conduction aphasia: fluent spontaneous speech and paraphasias, but patients understand spoken or written words, and are aware of their deficit (see page 114)
B. transitory aphasia following a seizure (see Todd’s paralysis, page 396)
C. primary progressive aphasia of adulthood: idiopathic & degenerative
2. akinetic mutism: seen with bilateral frontal lobe dysfunction (e.g. with bilateral ACA distribution infarction due to vasospasm from a-comm aneurysm rupture or with large bilateral frontal lesions; may actually be abulia) or with bilateral cingulate gyrus lesions
3. muteness of cerebellar origin84, 85
4. following transcallosal surgery: as a result of bilateral cingulate gyrus retraction or thalamic injury together with section of the midportion of the corpus callosum86
35.1.29. Swallowing difficulties
1. mechanical: the term globus describes a sensation of a lump in the throat
A. ossification of the anterior longitudinal ligament (OALL): see page 506
1. as part of diffuse idiopathic skeletal hyperostosis (DISH): see page 506
B. post-op following ACDF
1. it is normal to have a little swelling and fullness early post-op
2. may be increased with multiple levels and with anterior plating
3. as a complication from post-op hematoma
2. neurologic
35.2. Differential diagnosis (DDx) by location
35.2.1. Posterior fossa lesions
35.2.1.1. Cerebellar lesions
The following addresses intra-axial p-fossa abnormalities (for extra-axial lesions, see Cerebellopontine angle (CPA) lesions below).
ADULT
Single lesion
Rule of thumb: “the differential diagnosis of a solitary intraparenchymal lesion in an adult p-fossa is metastasis, metastasis, metastasis, until proven otherwise”.
1. tumors:
A. metastasis
B. hemangioblastoma: (see page 667) the most common PRIMARY intra-axial p-fossa tumor in adults (7-12% of p-fossa tumors). Very vascular nodule, often has cyst. Almost all p-fossa tumors are relatively avascular on angiography except these (look for serpentine signal voids especially in the periphery of the lesion on MRI87, much less common in cavernous hemangioma)
C. pilocytic astrocytoma: solid or cystic, tends to occur in younger adults (see page 604)
D. brainstem glioma: an isolated glioblastoma in the posterior fossa of an adult is a reportable rarity
E. choroid plexus tumor: usually infratentorial in adults (see page 695)
F. cerebellar liponeurocytoma: see page 613
2. infectious: abscess
3. vascular
A. cavernous hemangioma
B. hemorrhage
C. infarction: cerebellar CVA may be associated with H/A and/or pain in sub-occipital region or upper neck
1. embolic
2. thrombotic/plaque related
3. vertebral artery dissection: much less common than carotid dissection (see page 1163)
4. vertebrobasilar hypoplasia: see page 1160
4. Lhermitte-Duclos: see page 593. Focal or diffuse. Nonenhancing. Characteristic tiger stripes. Widens folia (c.f. most neoplasms which destroy folial pattern)
Multiple lesions
1. metastases
2. hemangioblastoma (possibly as part of von Hippel-Lindau): see page 667
3. abscesses
4. cavernous hemangiomas
PEDIATRIC
Also see Pediatric brain tumors, page 697.
Currently: p-fossa tumors comprise 54-60% of childhood brain tumors (breakdown listed below). 4 types account for ≈ 95% of infratentorial tumors in patients ≤ 18 yrs age88. The 3 most common are equal in incidence81:
1. PNET (including medulloblastoma): 27% (see page 686)
A. most start in roof of 4th ventricle (fastigium), and most are solid
B. differentiating medulloblastoma (MB) from ependymoma:
1. 4th ventricle drapes around medulloblastoma (“banana sign”) from the anterior aspect, c.f. ependymoma which tends to grow into 4th ventricle from floor. Ependymoma may grow through foramen of Luschka and/or Magendie
2. ependymomas tend to be inhomogeneous on T1WI MRI (unlike MB)
3. the exophytic component of ependymomas tends to be high signal on T2WI MRI (with MB this is only mildly hyperintense)
4. calcifications: common in ependymomas, but only in < 10% of MB
2. cerebellar (pilocytic) astrocytoma: 27%. Most start in cerebellar hemisphere. Often cystic with enhancing mural nodule (see page 604)
3. brainstem gliomas: 28%. Usually present with multiple cranial nerve palsies and long tract findings (see page 607)
4. ependymoma: usually arise in floor of 4th ventricle (see page 683)
5. choroid plexus papilloma: majority of patients are < 2 yrs old (see page 695)
6. atypical teratoid/rhabdoid tumor (AT/RT): see page 688
7. metastasis: neuroblastoma, rhabdomyosarcoma, Wilm’s tumor…
8. PHACES syndrome: acronym for a group of findings including Posterior fossa malformations, cervicofacial Hemangioma, Arterial anomalies of the head and neck, Coarctation of the aorta and cardiac defects, Eye anomalies and Sternal cleft. Ratio girls:boys = 9:1. Thought to begin during gestation weeks 8-10
35.2.1.2. Cerebellopontine angle (CPA) lesions
Vestibular schwannoma, meningioma, and epidermoid account for most. For those lesions that may be cystic, see below.
1. vestibular schwannoma: 80-90% of CPA lesions } see below to differentiate these two lesions
2. meningioma: (5-10%) } see below to differentiate these two lesions
3. ectodermal inclusion tumors (see page 688)
A. epidermoid (cholesteatoma): 5-7%. High signal on DWMRI (see page 689). Tumor passing from the posterior fossa to the middle fossa though the incisura is highly suggestive of epidermoid
B. dermoid
4. metastases
5. neuroma from cranial nerves other than VIII (also see below)
A. trigeminal neuroma: expands towards Meckel’s cave
B. facial nerve neuroma89: may arise in any portion of the VII nerve, with a predilection for the geniculate ganglion90. Hearing loss may be sensorineural from VIII nerve compression from tumors arising in the proximal portion of VII (cisternal or internal auditory canal (IAC) segment), or it may be conductive from erosion of the ossicles by tumors arising in the second (tympanic, or horizontal) segment of VII. Facial palsy (peripheral) may also develop, usually late89 (see page 845)
C. neurinoma of lowest 4 cranial nerves (IX, X, XI, XII)
6. arachnoid cyst: see page 222
7. neurenteric cyst: rare91 (see page 227). May secrete mucin
8. cholesterol granuloma (distinct from epidermoid): see page 689
9. lipoma
10. aneurysm: PICA, AICA, vertebrobasilar
11. dolichobasilar ectasia
12. cysticercosis
13. extensions of:
A. brain stem or cerebellar glioma
B. pituitary adenoma
C. craniopharyngioma
D. chordoma & tumors of skull base
E. fourth ventricle tumors (ependymoma, medulloblastoma)
F. choroid plexus papilloma: from 4th ventricle through foramen of Luschka
G. glomus tumor
1. glomus jugulare
2. glomus tympanicum
H. primary tumors of temporal bone (e.g. sarcoma or carcinoma)
Cystic lesions of the CPA
CPA lesions from the above list that may be cystic or have a cystic component91:
1. arachnoid cyst: same intensity as CSF on all MRI sequences, homogeneous
2. epidermoid cyst: ![]() high signal on DWMRI differentiates this from arachnoid cyst (see page 690)
high signal on DWMRI differentiates this from arachnoid cyst (see page 690)
3. dermoid cyst: high intensity areas on T1WI similar to fat; usually midline
4. cystic schwannoma
5. cholesterol granuloma: ![]() ≈ only lesion that is high signal on T1WIA (due to blood breakdown products). Also high signal on T2WI. Usually extradural, especially near petrous apex. Bone destruction is common
≈ only lesion that is high signal on T1WIA (due to blood breakdown products). Also high signal on T2WI. Usually extradural, especially near petrous apex. Bone destruction is common
6. neurenteric cyst: nonenhancing. Low intensity on DWMRI
7. choroidal cyst
8. cysticercosis: enhancing nodule (scolex)
A. exception: the rare “white” epidermoid
Differentiating neuromas of V, VII and VIII cranial nerves
All 3 may present in the CPA and may cross from posterior fossa to middle fossa, but they do so in different manners. Vestibular schwannomas show “transhiatal” extension by passing through the tentorial hiatus medially. Most trigeminal neuromas show “transapicopetrosal” extension by crossing into the middle fossa via the petrous apex (although some show transhiatal extension). When facial neuromas cross, they tend to spread across the midpetrosal bone, which is characteristic for facial neuromas89. When a facial neuroma enlarges the IAC, unlike a vestibular schwannoma, it tends to erode the anterosuperior aspect of the IAC.
Differentiating vestibular schwannoma from CPA meningioma
• vestibular schwannoma (VS) (AKA acoustic neuroma):
A. clinical: progressive unilateral hearing loss, usually with tinnitus. Progression results in unsteadiness, with true vertigo being rare. The facial nerve is more resistant to stretching, thus facial nerve signs and symptoms occur late. Trigeminal nerve involvement may occur with tumors > 3 cm (check corneal reflex), with tic douloureux-like symptoms being unusual
B. imaging: often heterogeneous signal and nonuniform enhancement. Rarely calcified. Except for very small tumors, IAC is frequently enlarged. Look for an acute angle between the tumor and the petrous bone, (meningiomas usually have an obtuse angle)
• meningiomas: may mimic VSs with these differences:
A. clinical: since they often arise from the superior anterior edge of the IAC, early facial nerve involvement is more common, and hearing loss is usually late. Trigeminal neuralgia-like pain is more common than with VSs
B. imaging: homogeneous signal and enhancement. IAC usually not enlarged. Calcification, and bony hypertrophy may occur (which occasionally narrows the IAC)
35.2.1.3. Petrous apex lesions
1. infection/inflammatory:
A. osteomyelitis: may produce Gradenigo’s syndrome (see page 838)
B. cholesterol granuloma (bright on T1WI epidermoid cyst are bright on DWI, neither enhance)
2. vascular lesions: aneurysm
3. neoplastic:
A. squamous cell cancer
B. glomus tumor
C. chondrosarcoma: will displace the carotid from medial to lateral (almost every other tumor in this region encases the carotid)
35.2.1.4. Foramen magnum lesions
1. extra-axial tumors: for more details of tumors (i.e. neoplasms only) see page 711
A. meningioma
B. chordoma: a mass behind the dens compressing the spinal cord is a chordoma until proven otherwise (see page 675)
C. neurilemmoma
D. epidermoid
E. chondroma
F. chondrosarcoma
G. metastases
2. non-neoplastic
A. aneurysms or ectasia of the vertebral artery
B. odontoid process in cases of basilar invagination (see page 138)
C. pannus from involvement of the odontoid with rheumatoid arthritis or old nonunion of fracture
D. synovial cyst of the quadrate ligament of the odontoid92
35.2.2. Multiple intracranial lesions on CT or MRI
1. neoplastic
A. primary
1. multicentric gliomas (≈ 6% of gliomas are multicentric, more common in neurofibromatosis, see Multiple gliomas, page 597)
2. tuberous sclerosis (including giant cell astrocytomas); (usually periventricular)
3. multiple meningiomas
4. lymphoma
5. PNET
6. multiple neuromas (usually in neurofibromatosis, including bilateral vestibular schwannomas)
B. metastatic: usually cortical or subcortical, surrounded by prominent vasogenic edema. See page 702. More common tumors include:
1. lung
2. breast
3. melanoma: may be higher density than brain on unenhanced CT
4. renal cell
5. gastrointestinal tumors
6. genitourinary tract tumors
7. choriocarcinoma
8. testicular
9. atrial myxoma
10. leukemia
2. infection: mostly abscess or cerebritis. Most commonly due to:
A. pyogenic bacteria
B. toxoplasmosis: common in AIDS patients (see page 364)
C. fungal
1. cryptococcus
2. mycoplasma
3. coccidiomycosis
4. aspergillosis
5. candidiasis
D. echinococcus
E. schistosomiasis
F. paragonimiasis
G. herpes simplex encephalitis (HSE): usually temporal lobe (see page 358)
3. inflammatory
A. demyelinating disease
1. MS: usually in white matter, periventricular, with little mass effect, margins are usually very sharp. Ring enhancing lesions can occur with tumefactive demyelinating lesions (see page 64)
2. progressive multifocal leukoencephalopathy (PML): primarily in white matter. No enhancement. Patients are usually very sick
B. gummas
C. granulomas
D. amyloidosis
E. sarcoidosis
F. vasculitis or arteritis
G. collagen vascular disease, including:
1. periarteritis nodosa (PAN) (see page 77)
2. systemic lupus erythematosus (SLE)
3. granulomatous arteritis
4. vascular
A. multiple aneurysms (congenital or atherosclerotic)
B. multiple hemorrhages, e.g. associated with DIC or other coagulopathies (including anticoagulant therapy)
C. venous infarctions (especially in dural sinus thrombosis, see page 1166)
D. moyamoya disease (see page 1170)
E. subacute hypertension (as in malignant HTN, eclampsia…) → symmetric confluent lesions with mild mass effect and patchy enhancement usually in occipital subcortical white matter (see page 73)
F. multiple strokes
1. lacunar strokes (l’etat lacunaire)
2. multiple emboli (e.g. in atrial fibrillation, mitral valve prolapse, SBE, air emboli)
3. sickle cell disease
4. vasculitis
5. intravascular lymphomatosis: see page 674
5. hematomas and contusions
A. traumatic (multiple hemorrhagic contusions, multiple SDH)
B. multiple “hypertensive” hemorrhages (amyloid angiopathy, etc.)
6. intracranial calcifications (see page 1223)
7. miscellaneous
A. radiation necrosis
B. foreign bodies (e.g. post gunshot wound)
C. periventricular low densities
1. Binswanger’s disease
2. transependymal absorption of CSF (e.g. in active hydrocephalus)
EVALUATION
Deciding which of the following tests are needed to evaluate a patient with multiple intracranial lesions must be individualized for the appropriate clinical setting.
1. cardiac echo: to R/O SBE that could shed septic emboli
2. “metastatic workup” (see Metastatic work-up, page 706) including:
A. chest x-ray: to R/O primary bronchogenic Ca or pulmonary metastases of another Ca, but also to R/O pulmonary abscess that could shed septic emboli. Chest CT may be needed in cases of positive CXR or if CXR is negative and there is high suspicion of lungs as source of primary
B. abdominal CT: has largely replaced lower GI (barium enema) and IVP
C. mammogram in women
35.2.3. Ring-enhancing lesions on CT/MRI
Abscess vs. tumor: (see Figure 35-1 and Figure 35-2) Tumor: the enhancing ring may be incomplete and irregular. Abscess: ring is usually complete, often thinner and smoother than with tumor. Abscess: usually brighter than tumor on DWI MRI.
Multiple lesions: metastases or abscess are much more likely than astrocytoma.
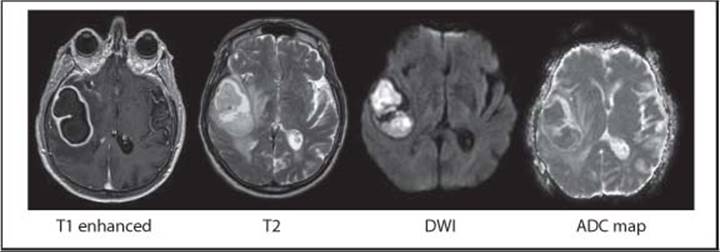
Figure 35-1 MRI of right hemispheric cerebral abscess (bright on DWI)

Figure 35-2 MRI of right hemispheric glioblastoma (dark on DWI)
Bold entries account for most cases in adults. Also consider lymphoma.
1. astrocytoma: usually malignant astrocytoma, viz. glioblastoma multiforme
2. metastases: (see page 702) especially lung
3. abscess: see page 350
A. may see visible growth over several days on serial imaging
B. pyogenic abscesses are often (but not always) associated with fever and rapidly progressing neurologic deficit
C. Nocardia abscesses are often multiloculated (see page 356) and are usually associated with a lung lesion
4. others
A. lymphoma (primary brain lymphoma or metastatic systemic lymphoma): wall is thicker than abscess93. Incidence is increasing (see page 672)
B. radiation necrosis
C. resolving intracerebral hematoma: on T1 gradient echo sequence, a continuous ring suggests hematoma, an interrupted ring suggests malignancy
D. cystic lesions with enhancing wall:
1. cysticercosis cyst (see Neurocysticercosis, page 370)
E. trauma
F. recent infarct
G. thrombosed giant aneurysm
35.2.4. White matter lesions
LEUKOENCEPHALOPATHY
Disease largely confined to the white matter. Demyelinating disease cause most.
Appear as white matter low density on CT or low signal on T1WI MRI, and high-intensity on T2WI. Usually does not enhance. Unlike a CVA, changes tend to spare the cortex. Conditions such as metabolic derangements, leuko-araiosis, etc. tend to produce fairly symmetric findings.
Differential diagnosis:
1. anoxia/ischemia
2. demyelinating disease
A. MS
B. ADEM
3. intoxication: cyanide, organic solvents, carbon monoxide
4. vitamin deficiencies: B12 with subacute combined degeneration
5. infectious, especially viral:
A. progressive multifocal leukoencephalopathy (PML) (see page 364)
B. herpes varicella-zoster leukoencephalitis (see page 360)
C. HIV infection (AIDS): perivascular pattern of demyelination
D. cytomegalovirus infection
E. Creutzfeldt-Jakob disease: small and perivascular demyelination
6. metabolic derangements: hyponatremia, excessively rapid correction of hyponatremia (causing osmotic myelinolysis, see page 11)
7. hereditary: metachromatic leukodystrophy, adult-onset Schilder’s disease
8. leuko-araiosis (see page 1227)
9. multiple myeloma (see page 740)
10. low grade (WHO grade II infiltrating) glioma (see page 595)
35.2.5. Corpus callosum lesions
1. lymphoma
2. MS plaque
3. tumefactive demyelinating lesions: see page 64
4. lipoma
35.2.6. Sellar, suprasellar and parasellar lesions
May enlarge, erode or destroy the sella turcica. Considerations in adults (adenoma is the most common enhancing pituitary lesion) are different than for children (adenomas are rare, craniopharyngioma and germinoma are more common). Includes (modified94):
1. tumors/pseudotumors
A. tumors having epicenter within the sella
1. pituitary tumor
a. adenohypophyseal tumors
i. adenoma
1. microadenoma: < 1 cm diameter (see page 634)
2. macroadenoma: ≥ 1 cm diameter
3. invasive adenoma: see page 637. Includes aggressive tumors of Nelson’s syndrome (see page 639)
ii. pituitary carcinoma or carcinosarcoma: see page 634
b. neurohypophyseal tumors
i. metastases: the most common tumor found in the posterior pituitary (presumably due to rich blood supply): breast and lung are most common primaries95
ii. pituicytoma: the most common tumor arising from neurohypophysis/pituitary stalk (i.e. primary) (see page 641)
iii. astrocytoma: arising from stalk or posterior pituitary
2. pituitary “pseudotumor”:
a. hyperplasia (enlargement)
i. thyrotroph hyperplasia due to primary hypothyroidism96 causing chronic pituitary stimulation by TRH see page 645. Typically: free T4 low or normal, TSH ↑↑, symmetrical sellar mass on MRI
ii. gonadotroph hyperplasia: due to primary hypogonadism
iii. somatotroph hyperplasia: due to ectopic GH-RH secretion
iv. lactotroph hyperplasia: in pregnancy
b. pituitary enlargement may occur in intracranial hypotension (see page 305)
c. the pituitary gland of young women of childbearing potential is normally slightly enlarged
B. juxtasellar or suprasellar tumors or masses: any of these lesions may extend into the sella
1. craniopharyngioma: in this region, these account for 20% of tumors in adult, 54% in peds (see page 663)
2. Rathke cleft cyst: see page 665
3. meningioma (parasellar, tuberculum sellae, or diaphragma sellae): to differentiate tuber-culum sellae meningioma from pituitary macroadenoma on MRI (see Figure 35-3), 3 characteristics of meningioma are: 1) bright homogeneous enhancement with gadolinium (c.f. heterogeneous, poor enhancement with macroadenoma), 2) suprasellar epicenter (vs. sellar), 3) tapered extension of intracranial dural base97(dural tail). Also, the sella is usually not enlarged, and even large suprasellar meningiomas rarely produce endocrine disturbances98. The pituitary stalk is sometimes seen being pushed posteriorly by a meningioma. Tuberculum sellae meningiomas may be associated with sphenoid pneumosinus dilatans99 (enlargement of the underlying sphenoid sinus without bone erosion)
4. pituitary tumor (mostly adenomas) with extrasellar extension: tends to push carotids laterally (unlike meningioma which may encase carotid), more symmetric than meningioma
5. germ cell tumors (GCT): (see page 692) choriocarcinoma, germinoma, teratoma, embryonal carcinoma, endodermal sinus tumor. In females, suprasellar GCTs are more common; in males pineal region is more common
a. suprasellar GCT: triad of diabetes insipidus, visual deficit and panhypopituitarism100. May also present with obstructive hydrocephalus
b. simultaneous suprasellar and pineal lesions is diagnostic of GCT (so-called synchronous germ cell tumors - see page 692)
6. glioma
a. hypothalamic glioma
b. optic nerve or chiasm (optic glioma): see page 606
7. metastasis
8. chordoma
9. parasitic infections: cysticercosis
10. epidermoid cyst
11. suprasellar arachnoid cyst: see Arachnoid cysts, page 222
12. sarcoidosis: (see page 71) hypothalamic involvement is a more likely site as a cause of anterior and/or posterior pituitary insufficiency
13. bone abnormalities
a. giant cell tumor: see page 742
b. chondromyxoid fibroma
c. brown tumor of hyperparathyroidism
d. bone spur
e. extramedullary hematopoiesis101
2. vascular lesions
A. aneurysm: ACoA, ICA (cavernous carotid or suprasellar variant of superior hypophyseal artery aneurysm, see page 1070), ophthalmic, basilar bifurcation. Giant aneurysms may produce mass effect
B. carotid cavernous fistula (CCF): see page 1113
3. inflammatory:
A. (autoimmune) hypophysitis (see below):
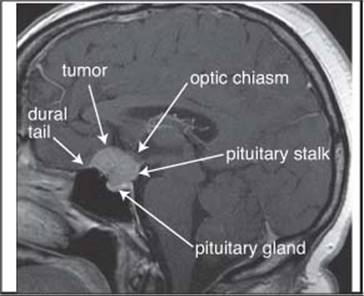
Figure 35-3 Tuberculum sellae meningioma that could be mistaken for a pituitary adenoma. Contrast enhanced T1WI sagittal MRI
1. distinguishing imaging characteristics are shown in Table 35-5
2. the most important clinical feature: pregnancy
3. the most important laboratory feature: diabetes insipidus (if DI is present, it is unlikely to be an adenoma)
B. pituitary granuloma102
4. empty sella syndrome:
A. primary: see page 719
B. secondary: following pituitary tumor resection (see page 719)
Table 35-5 Imaging characteristics of hypophysitis vs. adenoma103
|
Feature |
Hypophysitis |
Adenoma |
|
Enlargement |
symmetric |
asymmetric |
|
Pituitary stalk |
thickened, nontapering |
not thickened, -tapering, deviated |
|
Sellar floor* |
spared |
may be eroded |
|
Enhancement |
intense, may be heterogeneous |
less intense, usually homogeneous |
|
Mean size at time of presentation |
3 cm3 |
10 cm3 |
|
Posterior pituitary bright spot† |
lost |
preserved in 97% |
* on CT scan
† the normal hyperintensity of the posterior pituitary on T1WI MRI104 (see page 648)
HYPOPHYSITIS
AKA autoimmune hypophysitis (AH) Two main forms:
1. lymphocytic (adeno)hypophysitis 103: the more commonly encountered form. Inflammation of the pituitary stalk with lymphocytic infiltrate. Well established autoimmune etiology, although the antigens have not been identified. Primarily affects women in late pregnancy or early postpartum period
2. granulomatous hypophysitis: more aggressive. No gender bias. No association with pregnancy. May be autoimmune, but pathogenesis not definitely known
Because AH often mimics a nonsecretory pituitary macroadenoma (enhancing sellar mass on imaging, with negative endocrine tests), these lesions often undergo surgical resection instead of what may be more appropriate medical therapy (e.g. steroids105, or discontinuing possible offending agents such as ipilimumab106).
For distinguishing imaging characteristics, see Table 35-5.
35.2.7. Intracranial cysts
Modified107:
1. arachnoid cysts: see page 222. Typically lined with meningothelial cells
2. suprasellar cyst from dilated third ventricle
3. interhemispheric cyst from porencephaly
4. neuroectodermal cysts (glioependymal cysts): intraparenchymal, located near ventricles
5. old infarct: if it communicates with ventricle it is called a porencephalic cyst
6. tumor cysts (the solid portion may sometimes be isodense to brain on CT):
A. ganglioglioma: usually solid but may appear cystic on CT (see page 677)
B. pilocytic astrocytoma (see page 603): usually has enhancing mural nodule
C. neurilemmomas may be cystic
D. supratentorial ependymomas are often cystic: see page 683
7. infectious
A. abscess
B. cysticercosis: see Neurocysticercosis, page 370
C. hydatid cyst: see Echinococcosis, page 373
8. pineal cysts: see page 691
9. colloid cyst: see page 665
10. Rathke’s cleft cyst: see page 665
11. giant aneurysm
12. on CT, a low density non-enhancing tumor can mimic a cyst
13. chronic subdural hematoma or hygroma may mimic a cyst
14. posterior fossa: (for cysts of the CPA see page 1211). Includes:
A. cyst associated with Dandy-Walker malformation (see page 240)
B. epidermoid: see page 689
C. enlarged cisterna magna may mimic a cyst
D. cerebellar hemangioblastoma: often has an enhancing mural nodule (see page 667)
E. arachnoid cyst of posterior fossa
F. neurenteric cyst: see page 227
G. pilocytic astrocytoma of the cerebellum (see page 604): usually has an enhancing mural nodule
MIDLINE CAVITIES
Three potential supratentorial midline cavities in the center of the brain and differentiating features are shown in Table 35-6.

Cavum septum pellucidum (CSP)
AKA fifth ventricle, among others. A variable slit-like fluid-filled space between the leaflets of the left and right septum pellucidum. The compartment is usually isolated, although some communicate with third ventricle. The CSP is part of normal development, and persists until shortly after birth. Thus, it is present in ≈ all preemies. It is found in ≈ 10% of the adult population, usually representing an asymptomatic developmental anomaly. However, it is also commonly seen in boxers suffering from chronic traumatic encephalopathy (see page 911).
35.2.8. Orbital lesions
4 compartments of the orbit: 1) ocular (AKA globe, AKA bulbar), 2) optic nerve sheath, 3) intraconal, and 4) extraconal. CT remains a strong imaging modality within the orbit (less susceptible to motion artifact than MRI, images bony structures to good advantage). For pediatrics, see below.
Orbital lesions in adults: Orbital pseudotumor is the most common.
1. neoplastic
A. cavernous hemangioma: the most common benign primary intra-orbital neoplasm. Choroidal hemangioma is seen in Sturge-Weber syndrome } discrete tumors that may occur adjacent to but not envelope the optic nerve sheath
B. fibrohistiocytoma } discrete tumors that may occur adjacent to but not envelope the optic nerve sheath
C. hemangiopericytoma } discrete tumors that may occur adjacent to but not envelope the optic nerve sheath
D. capillary hemangioma: produces infantile proptosis. Regresses spontaneously
E. lymphangioma: produces infantile proptosis. Does not regress
F. melanoma: the most common primary ocular malignancy of adulthood
G. retinoblastoma: congenital, malignant primary retinal tumor. 40% are bilateral, 90% are calcified (often a key differentiating feature; does not portend benignity as with other lesions). CT may show retinal detachment
H. lymphoma of the orbit: causes painless proptosis. The 3rd most common cause of proptosis
I. intraorbital meningioma
J. primary optic nerve tumors
1. optic glioma
2. optic nerve sheath tumor (schwannoma)
2. congenital
A. Coats disease: telangiectatic vascular malformation of retina which leaks a lipid exudate causing retinal detachment. May mimic retinoblastoma. Vitreous is hyperintense on MRI on both T1WI and T2WI due to lipid
B. persistent hyperplastic primary vitreous
C. retinopathy of prematurity (retrolental fibroplasia)
3. infectious
A. toxocara endophthalmitis
4. inflammatory/collagen vascular disease: usually bilateral
A. scleritis
B. pseudotumor of the orbit: the most common intraconal lesion. Usually uni-lateral (see page 837)
C. sarcoidosis: usually affects the conjunctiva and lacrimal gland and spares connective tissues and intraorbital muscles
D. Sjögren’s syndrome
5. vascular
A. enlargement of the superior orbital vein: may occur in thrombosis of cavernous sinus or in carotid-cavernous fistula
B. dural AVM
6. miscellaneous
A. drusen: degenerated retinal pigment cells in the posterior globe that may resemble calcified masses on CT
B. thyroid ophthalmopathy: Graves’ disease (hyperthyroidism & swelling of EOMs → painless proptosis). 80% of cases are bilateral. The ophthalmopathy is independent of the level of thyroid hormone (possibly an autoimmune process). NB: a swollen inferior rectus muscle may resemble an orbital tumor if seen only on lower CT cut through the orbit
C. EOM enlargement with steroid use or occasionally with obesity
D. fibrous dysplasia
Orbital tumors in pediatrics:
1. dermoid cyst: 37%. The most common lesion in children
2. hemangioma: 12%. Most regress spontaneously without surgery
3. rhabdomyosarcoma: 9%. The most common malignant tumor of the orbit
4. optic nerve glioma: 6%
5. lymphangioma: < 7%. Imaging resembles hemangioma. But will not regress spontaneously, requires surgery. Proptosis may worsen after a URI. May bleed into itself (chocolate cysts)
35.2.9. Cavernous sinus lesions
Modified109:
1. primary tumors (rare)
A. meningiomas110
B. neurinomas
2. tumors from adjacent areas that may extend into cavernous sinus (head and neck cancers may track intracranially along cranial nerves, especially V):
A. meningiomas
B. neurinomas
C. chordomas
D. chondromas
E. chondrosarcomas
F. pituitary tumors111
G. nasopharyngeal carcinomas
H. esthesioneuroblastomas
I. nasopharyngeal angiofibromas
J. metastatic tumors
3. inflammation: e.g. Tolosa-Hunt (see page 837)
4. infection: mucormycosis (phycomycosis). Usually in diabetics (see page 836)
5. vascular
A. cavernous carotid aneurysm
B. carotid-cavernous fistula (see page 1113)
C. cavernous sinus thrombosis
35.2.10. Skull lesions
The most common benign tumors of skull are osteoma and hemangioma. Osteogenic sarcoma is the most common malignancy. See page 698 for specific skull tumors.
EVALUATING ROENTGENOGRAPHIC SKULL LUCENCIES
There is enough overlap of features to prevent any systematic means of determining the etiology of all or even most radiographic skull lucencies. The following features should be noted for any lucency, some are more helpful than others (modified112):
1. multiplicity (single or multiple?): except for multiple venous lakes, the presence of 6 or more defects is usually indicative of a malignancy
2. origin (intradiploic, full thickness, inner or outer table only):
A. most vault lesions originate intradiploically, so limitation to this space may merely signify early recognition of a lesion
B. expansion of the diploë with bulging of one or both tables almost always signifies a benign lesion
C. full thickness lesions affecting both tables congruently usually indicates malignancy, whereas non-congruent erosion is more common with benign lesions
3. edges (smooth or ragged):
A. smooth edges, whether regular, distinct or indistinct: no predictive value
B. irregular margins (especially ragged undermined edges): more suggestive of infection (osteomyelitis) or malignancy
C. sharply demarcated, full thickness punched out defects: suggest myeloma
4. presence of peripheral sclerosis: circumferential bony sclerosis suggests benignity (may indicate slow expansion and longstanding nature). The ring of sclerosis is generally narrow except in fibrous dysplasia
5. presence or absence of peripheral vascular channels: presence is highly suggestive of benign lesions (seen in ≈ 66% of venous lakes and ≈ 50% of hemangiomas)
6. pattern within the lucency:
A. ![]() hemangiomas classically show honeycomb or trabecular pattern (seen in ≈ 50% of cases) or sunburst pattern (seen in ≈ 11% of cases)
hemangiomas classically show honeycomb or trabecular pattern (seen in ≈ 50% of cases) or sunburst pattern (seen in ≈ 11% of cases)
B. fibrous dysplasia may show well defined islands of bone, or a grossly mottled appearance with randomly arranged cystic and dense areas
7. location on the cranial vault (high vs. low): poor correlation with benign vs. malignant lesions
8. pain: eosinophilic granulomas are often tender
Remember: skull lesions may have an intracranial component. CT scanning is good for assessing bone (MRI is poor for this), however, CT may miss small intracranial lesions tucked within the convexity of the calvaria due to bone hardening artifact (MRI has better sensitivity in this setting).
Nuclear bone scan may be a helpful adjunctive test (see specific lesion for findings).
Biopsy: indicated for questionable skull lesions. If the bone has not been destroyed by soft tissue, biopsy may be accomplished with a Craig needle, and the specimen may need decalcification by the pathologist before histologic evaluation can be completed.
RADIOLUCENT LESION OR BONE DEFECT IN SKULL (AKA LYTIC LESIONS)
• congenital or developmental
A. epidermoid (cholesteatoma): sclerotic edge
B. congenital: encephalocele, meningoencephalocele, dermal sinus
C. fibrous dysplasia: see page 701. A benign condition in which normal bone is replaced by fibrous connective tissue. Tends to occur higher in calvaria. 3 types:
1. cystic: widening of the diplöe usually with thinning of the outer table and little involvement of the inner table. Typically involves calvaria
2. sclerotic: usually involves skull base (especially sphenoid bone) and facial bones
3. mixed: appearance is similar to cystic type with patches of increased density within the lucent lesions
D. hemangioma or AVM of bone or scalp
E. pacchionian depression: arachnoid granulations (older terms: Pacchioni’s granulation or pacchionian bodies) resorb CSF into vascular system and occasionally cause a bony lucency, usually near the superior sagittal sinus
F. Albright’s syndrome
G. congenital foramina: “holes” in skull traversed by emissary veins
H. parietal thinning: usually a bilateral process
I. frontal fenestrae
J. venous lakes
K. cerebral herniations: AKA occipital pacchionian granulations
• traumatic
A. surgical defect: burr hole, craniectomy
B. fracture
C. post-traumatic leptomeningeal cyst (see page 892)
D. following trauma in children113
• inflammatory
A. osteomyelitis: including tuberculosis114
B. sarcoidosis
C. syphilis
• neoplastic
A. hemangioma: fine, honeycombed matrix. Classic x-ray finding: “starburst” appearance due to radiating bone spicules (may occur in as few as ≈ 11% of cases112)
B. intracranial tumor with erosion
C. lymphoma, leukemia
D. meningioma
E. metastasis: usually hot on bone scan
F. multiple myeloma, plasmacytoma: see page 740. Usually cool on bone scan
G. sarcoma or fibrosarcoma of bone
H. skin tumor with invasion (rodent ulcer)
I. neuroblastoma
J. lipoma
K. epidermoid (may also be considered congenital, thus also see above)
• miscellaneous
A. histiocytosis X (eosinophilic granuloma is the mildest form): perfectly round non-sclerotic punched out lesion, generally multiple, tender (see page 699)
B. Paget’s disease (when seen as a zone of osteolysis without osteoblastic sclerosis on skull films, this is defined as osteoporosis circumscripta). Usually “hot” on bone scan
C. aneurysmal bone cyst: rare. Arises in diploë and expands both tables which become thin but remain intact
D. brown tumor of hyperparathyroidism
DIFFUSE DEMINERALIZATION OR DESTRUCTION OF THE SKULL
(including “salt and pepper skull”)
• common
1. hyperparathyroidism, primary or secondary
2. metastatic carcinoma or neuroblastoma
3. multiple myeloma
4. osteoporosis
• uncommon
1. Paget’s disease (osteoporosis circumscripta)
DIFFUSE INCREASED DENSITY, HYPEROSTOSIS, OR CALVARIAL THICKENING
• common
1. anemia (sickle cell, iron deficiency, thalassemia, hereditary spherocytosis)
2. fibrous dysplasia
A. leontiasis ossea (“lion-like facies”): a form of polyostotic fibrous dysplasia
3. hyperostosis interna generalisata
4. osteoblastic metastases (especially prostate, breast)
5. Paget’s disease (begins with lytic zone and diploic thickening)
6. treated hydrocephalus
• uncommon
1. chronic phenytoin therapy
2. Engelman’s disease (progressive diaphyseal dysplasia)
3. fluorosis
4. hypervitaminosis D
5. hypoparathyroidism, pseudohypoparathyroidism
6. meningioma
7. osteogenesis imperfecta
8. osteopetrosis (see page 1204)
9. secondary polycythemia
10. syphilitic osteitis
11. tuberous sclerosis
“HAIR-ON-END” APPEARANCE IN SKULL
• common
1. congenital hemolytic anemia (e.g. thalassemia, sickle cell, hereditary spherocytosis, pyruvate kinase deficiency)
• uncommon
1. hemangioma
2. cyanotic congenital heart disease (with secondary polycythemia)
3. iron deficiency anemia
4. metastases: especially neuroblastoma, thyroid carcinoma
5. multiple myeloma
6. meningioma
7. osteosarcoma
8. polycythemia vera
FOCAL INCREASED DENSITY OF SKULL BASE
• common
1. fibrous dysplasia
2. meningioma
• uncommon
1. mastoiditis
2. nasopharyngeal carcinoma
3. osteoblastic metastasis
4. osteoma of the outer table or diploe
5. chondroma
6. sarcoma of bone (e.g. osteosarcoma, chondrosarcoma)
7. sphenoid sinusitis
GENERALIZED INCREASED DENSITY OF SKULL BASE
• common
1. fibrous dysplasia
2. Paget’s disease
• uncommon
1. severe anemia (e.g. thalassemia, sickle cell)
2. Engelman’s disease (progressive diaphyseal dysplasia)
3. fluorosis
4. hyperparathyroidism, primary or secondary (treated)
5. hypervitaminosis D
6. idiopathic hypercalcemia
7. meningioma
8. osteopetrosis (see page 1204)
LOCALIZED INCREASED DENSITY OR HYPEROSTOSIS OF THE CALVARIA
• common
1. anatomic variation (e.g. sutural sclerosis)
2. fibrous dysplasia
3. osteoma (see page 698)
4. meningioma
5. hyperostosis frontalis interna (see page 700)
6. osteoblastic metastases (especially: prostate, breast)
7. Paget’s disease (begins with lytic zone and diploic thickening)
8. cephalhematoma
9. depressed skull fracture
• uncommon
1. osteosarcoma
2. chronic osteomyelitis, tuberculosis
3. tuberous sclerosis
4. osteoid osteomas: radiolucent nidus with surrounding zone of dense sclerosis
5. osteoblastoma:
6. ossifying fibromas: predilection for frontotemporal region
7. radiation necrosis
PNEUMOCELE
Pneumocele: enlargement of an air sinus often with bone erosion. Pneumosinus dilatans generally denotes enlargement of an air sinus without bone erosion, as may occur with tuberculum sellae or planum sphenoidale meningiomas (see page 1216).
Pneumoceles occur primarily in the maxillary antrum. Involvement of frontal sinus. usually involves pneumosinus dilatans. Etiology is unknown, and may involve a trap-valve mechanism, ruptured mucocele, or possibly congenital. May occur with fibrous dysplasia.
Presentation of pneumocele or pneumosinus dilatans:
1. headache
2. neuralgia
3. facial asymmetry
4. frontal bossing (with frontal pneumosinus dilatans)
5. exophthalmous
6. CSF fistula (leak)
35.2.11. Combined intracranial/extracranial lesions
Lesion causing mass outside skull with intracranial component.
1. intra-axial: rule of thumb - “there is no intra-axial lesion that grows out of skull”
2. extra-axial:
A. meningioma
1. may arise in diploe, grows outward and inward
2. intracranial meningioma can grow through bone by destroying it
3. intracranial meningioma can induce hyperostosis that causes extracranial mass
B. metastatic disease (e.g. GI carcinoma, and especially prostate Ca)
C. bone (skull) lesion:
1. hemangioma
2. epidermoid
3. fibrous dysplasia (rare)
4. giant cell tumor (rare)
5. Ewing’s sarcoma (rare in skull)
6. aneurysmal bone cyst (5% occur in skull, occipital bone most common)
35.2.12. Intracranial calcifications
Often due to deposition of calcium in the media of medium-sized blood vessels without compromise of the lumen. Usually asymptomatic. Considered abnormal when present to a significant enough degree to be visible on plain x-ray in a young person.
SINGLE INTRACRANIAL CALCIFICATIONS
1. physiologic
A. choroid plexus: calcifications usually bilateral (see below)
B. arachnoid granulation
C. diaphragma sellae
D. dural (falcine, tentorial, sagittal sinus)
E. habenular commissure
F. petroclinoid or interclinoid ligaments
G. pineal: 55% of patients > 20 yrs age have a calcified pineal gland visible on plain skull x-ray
2. infection
A. cysticercosis cyst: single or multiple (see Neurocysticercosis, page 370)
B. encephalitis, meningitis, cerebral abscess (acute and healed)
C. granuloma (torulosis and other fungi)
D. hydatid cyst
E. tuberculoma
F. paragonimiasis
G. rubella
H. syphilitic gumma
3. vascular
A. aneurysm, including:
1. vein of Galen aneurysm
2. giant aneurysm
B. arteriosclerosis (especially carotid artery in siphon region)
C. hemangioma, AVM, Sturge-Weber syndrome
4. neoplastic: calcifications usually suggest a more benign process
A. meningioma (see page 613)
B. craniopharyngioma
C. choroid plexus papilloma
D. ependymoma
E. glioma (especially oligodendroglioma, also astrocytoma)
F. ganglioglioma
G. lipoma of corpus callosum
H. pinealoma
I. hamartoma of tuber cinerium
5. miscellaneous
A. hematoma: ICH, EDH or SDH. Calcifications usually only when chronic
B. idiopathic
C. tuberous sclerosis (see page 725)
MULTIPLE INTRACRANIAL CALCIFICATIONS
• common
A. choroid plexus: the most common site for physiologic calcification (in lateral ventricles where it is usually bilateral and symmetric; rare in 3rd & 4th ventricles). Increases in frequency and extent with age (prevalence: 75% by 5th decade). Rare under age 3. Under age 10, consider possible choroid plexus papilloma. Involvement in the temporal horns is often associated with neurofibromatosis
B. basal ganglia (BG): slight bilateral BG calcifications on CT are common, especially in the elderly. Considered a normal radiographic variant by some. They may be idiopathic, secondary to conditions such as hypoparathyroidism or long-term anticonvulsant use, or part of rare conditions such as Fahr’s disease (see below). BG calcifications > 0.5 cm dia are possibly association with cognitive impairment and a high prevalence of psychiatric symptoms115
• uncommon
A. Fahr’s disease: progressive idiopathic calcification of medial portions of basal ganglia, sulcal depths of cerebral cortex, and dentate nuclei116
B. hemangioma, AVM, Sturge-Weber syndrome, von Hippel-Lindau disease
C. basal cell nevus syndrome (falx, tentorium)
D. Gorlin’s syndrome. Associated findings: mandibular cysts, rib and vertebral deformities, short metacarpals. Medulloblastoma seen in several patients
E. cytomegalic inclusion disease
F. encephalitis (e.g. measles, chickenpox, neonatal herpes simplex)
G. hematomas (SDH or EDH, chronic)
H. neurofibromatosis (choroid plexi)
I. toxoplasmosis
J. tuberculomas; tuberculous meningitis (treated)
K. tuberous sclerosis
L. hypoparathyroidism (including post-thyroidectomy cases117) and pseudohypoparathyroidism
M. multiple tumors (e.g. meningiomas, gliomas, metastases)
N. cysticercosis cyst: may be single or multiple (see Neurocysticercosis, page 370)
35.2.13. Intraventricular lesions
Intraventricular tumors represent only ≈ 10% of CNS neoplasms. A clue to differentiating a tumor located within the ventricle from an intraparenchymal tumor invaginating into the ventricle is a “cap” of CSF surrounding an intraventricular tumor on CT or MRI. Differential diagnosis (percentages quoted are from a series of 73 patients with an intraventricular lesion on CT seen at UCSF118).
1. astrocytoma: (20%) the most common lesion. Hydrocephalus (HCP) is present in 73%. Hyperdense on non-contrast CT (NCCT) in 77%.
Locations in descending order of frequency:
• frontal horn
• third ventricle
• atrium (AKA trigone)
• fourth ventricle
2. colloid cyst: (14%) essentially seen only in anterior third ventricle at foramen of MonroA. 50% are hyperdense on NCCT. MRI appearance is variable, and may occasionally be missed. Little or no enhancement on CT/MRI (see page 665). DDx includes xanthogranuloma
3. meningioma: (12%) most in atrium, rarely in frontal horn. All hyperdense with dense uniform enhancement. May be calcified. Most have dense tumor blush on angiogram, most supplied from anterior choroidal artery, posterior choroidal less common. Thought to arise from arachnoidal cells within the choroid plexus
4. ependymoma: (10%) most in 4th ventricle, may occur in body of lateral ventricle. Often hyperdense on CT because of high cellularity
5. craniopharyngioma: (7%) primarily in 3rd ventricle. Most have punctate calcification. Squamous epithelial rests in region of lamina terminalis are felt to give rise to this uncommon variety of craniopharyngioma
6. medulloblastoma: (5%) often fill 4th ventricle. Hyperdense on CT with homogeneous enhancement
7. cysticercosis: (5%) may involve any ventricle or may be panventricular (NB: incidence related to geographic location), see page 370
8. choroid plexus papilloma: (5%) most common in lateral ventricle (may be bilateral), but also may be seen in 4th and occasionally in 3rd. Non-obstructive HCP may occur (possible CSF overproduction). Intense blush on angiogram
9. epidermoid: (4%) mostly in 4th ventricle. Hypodense on CT with no enhancement (tend to follow CSF signal). The most common 4th ventricular low density lesion in the U.S.
10. dermoid: (3%) common in 4th ventricle. May see free floating fat in ventricles suggestive of cyst rupture. Tendency to form in midline
11. choroid plexus carcinoma: (3%) common in atrium of lateral ventricle. May extended into adjacent brain parenchyma with edema and shift. Intense blush on angio. NB: very rare lesion
12. subependymoma: (3%) 4th ventricle or frontal horn. Typically isodense on CT with minimal enhancement. May have calcification or cystic degeneration (more common in ependymoma). Most commonly in floor of 4th ventricle near obex
13. ependymal cyst: (3%) common in lateral ventricle. Absence of communication demonstrated by water soluble contrast cisternography
14. arachnoid cyst: (1%) lateral ventricle. Absence of communication demonstrated by water soluble contrast cisternography
15. arteriovenous malformation (AVM): (3%)
16. teratoma: (1%) Located in anterior 3rd ventricle. Partially calcified with foci of fat density. Marked enhancement
17. central neurocytoma: see page 612
18. metastases: breast and lung reported119
19. chordoid glioma of the 3rd ventricle120
A. other sites have been described but are exceedingly rare
FEATURES TO HELP IDENTIFY TYPE OF INTRAVENTRICULAR LESIONS
By location within ventricular system
Table 35-7 shows the breakdown of lesion type by location within the ventricular system.

By location and age within lateral ventricle121
See Table 35-8. This study excluded tumors that were clearly arising in the third ventricle or were predominantly parenchymal with intraventricular extension.
The teratoma and both PNETs occurred in age < 1 year, and all showed calcifications. Only one CPP occurred above age 5 years.
In adults > 30 years age, the only tumors found in the trigone were meningiomas. Subependymomas were the only nonenhancing tumor in this age group.

By location within third ventricle
• anterior third ventricle
1. colloid cyst
2. sellar mass
3. sarcoidosis
4. aneurysm
5. hypothalamic glioma
6. histiocytosis
7. meningioma
8. optic glioma
• posterior third ventricle
1. pinealoma (dysgerminoma)
2. meningioma
3. arachnoid cyst
4. vein of Galen aneurysm
By enhancement
All lesions enhanced except: cysts (ependymal and arachnoid), dermoids and epidermoids. There are differences of opinion of the tendency for subependymomas to enhance, Jelinek et al.121 found that they did not.
By multiplicity
Multiple lesions are more suggestive of: neurocysticercosis, metastases, a ruptured epidermoid cyst.
35.2.14. Periventricular lesions
Periventricular solid enhancing lesions on CT (in decreasing frequency)
1. lymphoma (CNS involvement from systemic, or rarely primary brain): must be included in differential diagnosis of any solid enhancing periventricular brain tumor (see page 672). Very radiosensitive
2. ependymoma (usually invaginates)
3. metastatic Ca: especially malignant melanoma or choriocarcinoma
4. ventriculitis
5. medulloblastoma (in peds), AKA cerebellar sarcoma in adults
6. pineal tumor (dysgerminoma type): usually midline, young patient
7. occasionally, glioblastoma can present like this
Periventricular low density on CT, or high signal on T2WI MRI
1. increased extracellular or intracellular water content (edema)
A. in hydrocephalus: transependymal CSF absorption (see footnote page 310)
B. necrosis from infarction
C. edema from tumor
2. uncommon late variants of adrenoleukodystrophy
3. vascular disorders
A. subacute arteriosclerotic encephalopathy (Binswanger’s disease)122, 123
B. cerebral embolism
C. vasculitis
D. amyloid angiopathy
E. low flow states
4. demyelination: including multiple sclerosis
5. leukoaraiosis 124: white matter disease with symmetric (or nearly so) periventricular white matter changes on CT or MRI. May be asymptomatic or may present with findings including dementia. May be related to:
A. Binswanger’s encephalopathy
B. watershed infarction125
C. normal aging126: increases each decade after age 60, usually patchy
D. hypoxia
E. hypoglycemia127
6. heterotopias: islands of grey matter in abnormal locations
7. following radiation therapy (XRT)
35.2.15. Meningeal thickening/enhancement
Two main categories of enhancement128:
1. dural enhancement: visible beneath the inner table of the skull. Does not follow the gyral convolutions. May be either:
A. focal
1. adjacent to meningioma: so called “dural tail”
2. pleomorphic xanthoastrocytoma: also can have “dural tail”
B. diffuse dural enhancement129: associated with extraaxial neoplastic processes in ≈ 65%. Clinically: H/A, multiple cranial nerve palsies, seizures; may be indistinguishable from leptomeningeal metastases
1. intracranial hypotension: diffuse pachymeningeal enhancement on cerebral MRI (see page 305)
2. bacterial meningitis
3. primary CNS tumors: medulloblastoma, malignant meningioma
4. sarcoidosis
5. following craniotomy
6. metastases (mostly carcinomas):
a. bony mets to skull: present in 10 of 13 patients
b. dural metastases
c. leptomeningeal
7. following subdural hemorrhage130
2. leptomeningeal: may be either:
A. thin linear enhancement that closely follows the gyri
B. small nodules attached to the brain
35.2.16. Ependymal and subependymal enhancement
Some overlap with periventricular enhancement. Ependymal enhancement often heralds a serious condition131. Main DDx is tumor vs. infectious process.
1. ventriculitis or ependymitis: ependymal enhancement occurs in 64% of cases of pyogenic ventriculitis132. Infection may occur in the following settings
A. following shunt surgery
B. after intraventricular surgery
C. with indwelling prosthetic devices (e.g. Ommaya reservoir)
D. with use of intrathecal chemotherapy
E. with meningitis
F. with viral ependymitis
G. in some cases of CMV encephalitis in immunocompromised patients
H. granulomatous involvement: esp. in immunocompromised patients; e.g. tuberculosis, mycobacterium, syphilis
2. lymphoproliferative disorders
A. CNS lymphoma: see page 672
B. leukemia
3. metastasis
4. carcinomatous meningitis: typically also produces meningeal enhancement (see page 711)
5. multiple sclerosis: usually more peri ventricular (in the white matter)
6. transient enhancement reported in a child with ependymoma in the absence of tumor spread133
7. tuberous sclerosis: subependymal hamartomas appear as nodules which occasionally enhance (see page 725). These gradually calcify with age
Immunocompromised patients: DDX is mainly lymphoma vs. viral ependymitis131. The enhancement pattern is helpful131:
1. thin linear enhancement: suggests virus (CMV or varicella-zoster)
2. nodular enhancement: suggests CNS lymphoma
3. band enhancement: less specific (may occur with virus, lymphoma, or TB)
Immune competent patients131:
1. infection
A. bacterial (pyogenic) ventriculitis
B. tuberculous ventriculitis
C. cystic lesions suggest cysticercosis
2. in the absence of constitutional symptoms
A. lymphoma
B. ependymoma
C. germ cell tumor
D. metastases
3. in the presence of appropriate constitutional symptoms: linear enhancement is rarely due to neurosarcoidosis or Whipple’s disease, metastatic multiple myeloma (usually nodular)
35.2.17. Intraventricular hemorrhage
Etiologies:
1. most occur as a result of extension of intraparenchymal hemorrhages
A. in the adult:
1. spontaneous ICH: especially thalamic or putaminal (see page 1118)
2. associated with AVM
B. in newborns: extension of subependymal hemorrhage (see page 1131)
2. pure intraventricular hemorrhage (IVH) is usually the result of a rupture of
A. aneurysm: accounts for ≈ 25% of IVH in adults, and is second only to extension of intracerebral hemorrhage as the most common cause. IVH occurs in 13-28% of ruptured aneurysms in clinical series134. More common with the following aneurysms: a-comm, distal basilar artery or carotid terminus, VA or distal PICA (see page 1056 for patterns)
B. vertebral artery dissection (or dissecting aneurysms): see page 1163
C. intraventricular AVM
D. intraventricular tumor
35.2.18. Medial temporal lobe lesions
May be responsible for seizures, especially “uncal fits” (temporal lobe seizures).
1. hamartoma
2. mesial temporal sclerosis: should see atrophy of the parenchyma in this area with dilatation of the temporal horn of the lateral ventricle (see page 395)
3. glioma: may be low grade. Look for mass effect and possibly enhancement
35.2.19. Basal ganglion abnormalities
1. generally symmetric abnormalities
A. calcification: see page 1224
B. Wilson’s disease (hepatolenticular degeneration): autosomal recessive disease causing accumulation of copper in tissues
C. Huntington’s disease (or chorea): caused by > 40 trinucelotide CAG repeats in the Huntington gene (4p16.3) which leads to the production of the protein huntingtin. Cell loss in caudate nucleus can be seen on CT or MRI
D. manganese: symmetrical high signal abnormalities on T1WI primarily in the globus pallidus with essentially no findings on T2WI or GRASS (almost pathognomonic) - see page 60
E. globus pallidus (low density on CT):
1. severe carbon monoxide intoxication
2. cyanide poisoning
3. hypoxia
F. putamen
1. hypoglycemia: affects corpus striatum (caudate and putamen)
2. stroke
35.2.20. Thalamic lesions
Astrocytomas are the most common tumors.
1. common neoplasms
|
Adults |
Pediatrics |
|
A. anaplastic astrocytoma |
anaplastic astrocytoma |
|
B. glioblastoma multiforme |
astrocytoma (WHO grade II) |
|
C. metastasis |
glioblastoma multiforme |
|
D. primary CNS lymphoma |
pilocytic astrocytoma |
2. uncommon neoplasms
|
Adults |
Pediatrics |
|
A. astrocytoma (WHO grade II) |
germinoma |
|
B. neurocytoma |
glioblastoma multiforme |
|
C. oligodendroglioma |
PNET |
|
D. pilocytic astrocytoma |
subependymal giant cell tumor |
|
E. hamartoma |
3. non-neoplastic (pediatric and adult)
A. cavernous angioma
B. granuloma
C. heterotopias
D. AVM
E. infarct
35.2.21. Intranasal/intracranial lesions
Lesions within the nose that may communicate with the intracranial cavity:
1. infectious
A. tuberculosis
B. syphilis
C. Hansen’s disease (leprosy)
D. fungal infections, especially:
1. aspergillosis
2. mucormycosis: seen primarily in diabetics or immunocompromised patients (see page 836)
3. Sporothrix schenckii
4. Coccidioides
E. Wegener’s granulomatosis: (see page 78) necrotizing granulomatous vasculitis of the upper and lower respiratory tracts with glomerulonephritis and nasal destruction135
F. lethal midline granuloma: (see page 78) a locally destructive lymphomatoid infiltrative disease that may not have true granulomas, and may also cause local nasal destruction. However, renal and tracheal involvement do not occur as in Wegener’s granulomatosis
G. polymorphic reticulosis: may be a nasal lymphoma. Possibly the same disease as lethal midline granuloma (see above)
2. mucocele: a retention cyst of an air sinus that results from an occluded ostium and may cause expansive erosion of the involved sinus. Often enhances with IV contrast (MRI or CT), and may contain mucus or pus
3. neoplasms
A. carcinoma of the nasal sinus
1. squamous cell
2. glandular
3. nasopharyngeal carcinomas: may be related to Epstein-Barr Virus (EBV) infection
4. sinonasal undifferentiated carcinoma (SNUC)136: distinct from lymphoepithelioma (less keratinizing). Rare, aggressive carcinoma (more lethal variant of squamous cell carcinoma) with poor prognosis. Incidence may be higher with prior XRT and in woodworkers and nickel factory workers. May invade adjacent structures, those relevant to neurosurgeons: frontal fossa, and cavernous sinus. No relation to EBV. Treatment: tri-modal therapy (XRT, chemotherapy and salvage surgery)
B. esthesioneuroblastoma 137 or aesthesioneuroblastoma AKA olfactory neuroblastoma: named for the stem cell of the olfactory epithelium (esthesioneuroblast). A malignant tumor arising from crest cells of the nasal vault, often with intracranial invasion. Very rare (≈ 200 reported cases). Presents with epistaxis (76%), nasal obstruction (71%), tearing (14%), pain (11%), diplopia, proptosis, anosmia and endocrinopathies138. Treatment: surgical resection followed by XRT, ± chemotherapy
C. metastatic tumors: very rare, possibly with renal cell carcinoma
D. benign tumors
1. frontal meningioma: rarely erodes into nasal cavity
2. rhabdomyoma
3. benign hemangiopericytoma
4. cholesteatoma
5. chordoma
4. congenital lesions
A. encephalocele (see page 232): a nasal polypoid mass in a newborn should be considered an encephalocele until proven otherwise. Classifications:
1. cranial vault
2. frontal ethmoidal
3. basal
4. posterior fossa
B. nasal glioma: non-neo-plastic glial tissue located within the nose, often conceptually and diagnostically confused with an encephalocele (see Table 35-9). The term “glioma” is a misnomer, and nasal glial heterotopia is preferred. Does not communicate with the subarachnoid space
Table 35-9 Encephalocele vs. nasal glioma
|
Finding |
Encephalocele |
Nasal glioma |
|
pulsatile? |
frequently (may not be if small) |
no |
|
changes with Valsalva maneuver |
swells (Furstenberg sign) |
no change |
|
presence of hypertelorism |
suggests encephalocele |
does not correlate |
|
attachment to CNS |
stalk |
none, or minimal |
|
probe |
can be passed lateral |
cannot be passed lateral |
35.2.22. Spine
35.2.22.1. Atlantoaxial subluxation
1. incompetence of the transverse atlantal ligament (TAL): results in increased atlanto-dental interval (ADI) (see page 136)
A. rheumatoid arthritis: erosion of insertion points of the TAL (see page 495)
B. traumatic (see page 957)
1. disruption (tear) of the TAL (rare)
2. avulsion of the insertion points of the TAL (as in comminuted C1 fx)
C. congenital laxity of the TAL:
1. Down syndrome: 20% incidence139 (see page 498)
2. may be associated with neurofibromatosis
D. retropharyngeal infections: chronic tonsillitis, Grisel syndrome (see page 956)
E. chronic steroid use
2. incompetence of the odontoid process: ADI is normal
A. odontoid fractures: see page 963
B. os odontoideum: see page 966
C. erosion of the odontoid due to rheumatoid arthritis (RA): see page 495
D. neoplastic erosion of the odontoid:
1. metastases to the upper cervical spine (see page 743)
2. other tumors of the axis (see below)
E. Morquio syndrome: hypoplasia of the dens (see page 494)
F. congenital absence/dysplasia of the odontoid
G. following transoral odontoidectomy: (see page 176)
H. local infection
Chronic AAS seen in conditions such as rheumatoid arthritis or Down syndrome may be significant yet asymptomatic. Treatment decisions in this group are difficult. Acute AAS is more commonly symptomatic and may be life threatening.
35.2.22.2. Abnormalities in vertebral bodies
For lesions unique to the craniocervical junction & upper cervical spine, see page 494. For abnormalities unique to the axis (C2), see below.
1. neoplasms (for more extensive list, see page 728)
A. metastases: prostate, breast, lung, renal cell, thyroid, lymphoma & myeloma commonly go to bone. Four patterns (≈ all are low intensity on T1WI):
1. focal lytic (most common): T1WI = hypointense, T2WI = hyperintense
2. focal sclerotic: hypointense on T1WI and T2WI
3. diffuse homogeneous: T1WI = hypointense, T2WI = hyperintense or heterogeneous
4. diffuse heterogeneous: mixed signal intensities on T1WI & T2WI
B. primary bone tumors (see page 736 for more extensive discussion)
1. vertebral hemangioma
2. osteoblastoma
2. infection: osteomyelitis/discitis
3. fatty infiltrate or replacement of bone marrow: with age, hematopoietic red marrow of VBs is gradually replaced by yellow marrow in a splotchy pattern at a slower rate than in many other locations, e.g. distal appendicular bones140. T1WI: yellow marrow (MRI characteristics similar to subcutaneous fat) is hyperintense to red marrow (caution: bright areas on T1WI may be fat, or may be a normal area next to a low intensity met). T2WI: yellow marrow is bright
4. degenerative changes (Modic changes): see page 430
5. metabolic
A. Paget’s disease: plain x-rays → enlargement of VBs with cortical thickening usually involving several contiguous levels (see page 499)
B. osteoporosis: reduced bone density. Vertebral compression fractures may be seen
C. ankylosing spondylitis: osteoporotic VBs, calcified intervertebral discs (sparing the nucleus pulposus), and ossified ligaments, → square VBs with bridging syndesmophytes (“bamboo spine”) (see page 502). Starts in sacroiliac joints & lumbar spine
35.2.22.3. Axis (C2) vertebra lesions
1. tumors: rare. Possibilities include those that involve the spine at any location (see page 728). Some factors pertinent to this location141:
A. primary bone
1. chondroma
2. chondrosarcoma: rare in the craniovertebral junction. Lobulated tumors with calcified areas
3. chordoma: slow-growing radioresistant malignancy (see page 675)
4. osteochondroma (chondroma)
5. osteoblastoma: see page 736
6. osteoid osteoma (see page 736): more common in posterior elements than VB142
7. giant-cell tumors of bone: typically arise in adolescence. Lytic with bony collapse143
B. metastatic: including
1. typical metastases that spread hematogenously to bone, including:
a. breast cancer
b. prostate cancer
c. malignant melanoma
d. paraganglioma
e. renal cell carcinoma
2. extension of regional tumors
a. nasopharyngeal tumors
b. craniopharyngioma
C. miscellaneous
1. plasmacytoma
2. multiple myeloma
3. eosinophilic granuloma: osteolytic defect with progressive vertebral collapse. Occasionally occur in C2144
4. Ewing’s sarcoma: malignant. Peak incidence during 2nd decade of life
5. aneurysmal bone cyst145
2. infection: osteomyelitis of the axis
3. pannus from old nonunion of fracture or from rheumatoid arthritis (RA)
4. erosive changes in the odontoid process with RA (see page 495)
35.2.22.4. Pathologic fractures of the spine
Fractures due to metastatic involvement are hypointense on T1WI and hyperintense on T2WI. Benign VB collapse should be isointense to normal VBs on all sequences146, 147 and the VB should look homogeneous. On T2WI or STIR images, the cortex of the VB (which should be dark border around the VB due to low water content of cortical bone) should be intact.
Etiologies:
1. osteoporosis
2. neoplasm: short list (see page 736 for the long list)
A. metastases: common sources of spine mets: lung, breast, prostate, myeloma
B. eosinophilic granuloma (see page 729): may cause vertebra plana (see below)
C. lymphoma
D. hemangioma: see page 738
3. infection
4. avascular necrosis of the vertebral body
A. Calve-Kummel-Verneuil disease (see below)
B. with steroid use
Vertebra plana
Criteria:
1. uniform collapse of vertebral body into flat thin disc
2. increased density of vertebra
3. spares neural arches
4. normal disc and intervertebral disc space
5. intervertebral vacuum cleft sign (pathognomonic)
6. no kyphosis
Etiologies include:
1. eosinophilic granuloma
2. Calve-Kummel-Verneuil disease: avascular necrosis of the vertebral body. Occurs in 2-15 year olds
3. hemangioma
35.2.22.5. Spinal epidural masses
See items marked with a dagger (†) under Myelopathy on page 1185.
35.2.22.6. Destructive lesions of the spine
1. neoplastic (see Differential diagnosis: spine & spinal cord tumors, page 728 for more):
A. metastatic tumors with a predilection for bone: prostate, breast, renal cell, lymphoma, thyroid, lung… (see Spinal epidural metastases, page 742)
B. primary bone tumors: chordomas (see page 675), osteoid osteoma (see page 736), hemangioma (see page 738)
2. infection:
A. vertebral osteomyelitis: occurs mostly in IV drug abusers, patients with diabetes mellitus, and hemodialysis patients. May have associated spinal epidural abscess. Also see Vertebral osteomyelitis, page 380
B. discitis (see Discitis, page 383)
3. chronic renal failure: some patients develop a destructive spondyloarthropathy that resembles infection148, 149
4. ankylosing spondylitis: bamboo spine (square VBs with bridging syndesmophytes) - see page 502
5. lesions producing posterior scalloping of VB (mnemonic: AMEN)
A acromegaly or achondroplasia
M Marfan syndrome or mucopolysaccharidosis E Ehlers-Danlos
N neurofibromatosis
• also: dural ectasia
6. lesions producing anterior scalloping of VB
A. aortic aneurysm
B. lymphoma
C. spinal TB
DIFFERENTIATING FACTORS
Of the many lytic or destructive lesions that involve the vertebra, destruction of the disc space is highly suggestive of infection which often involves at least two adjacent vertebral levels. Although tumors may involve adjacent vertebral levels and cause collapse of disc height, the disc space is usually not destroyed150 (possible exceptions include: some vertebral plasmacytomas, a reported metastatic cervical carcinoma, and there may occasionally be destruction of the disc in ankylosing spondylitis151). Unlike pyogenic infections, the disc may be relatively resistant to tuberculous involvement in Pott’s disease152. Also, since metastatic tumor involvement usually produces widespread bony involvement, it is less likely with involvement of a single bone.
35.2.22.7. Vertebral hyperostosis
1. Paget’s disease: classic “ivory bone” with cortical thickening (“picture frame” appearance on plain x-rays). Consider Paget’s with a dense vertebra on x-ray in an older patient, commonly involving several contiguous vertebrae (see page 498)
2. osteoblastic metastases
A. in men: prostate
B. in women: breast
C. lymphoma
35.2.22.8. Sacral lesions
1. tumors
A. metastases: the most common sacral neoplasm
B. primary neoplasms of the sacrum are uncommon and include:
1. giant cell tumor: see page 742
2. chordoma
3. teratoma:
a. adults: pre-sacral or sacro-coccygeal teratomas may arise from cells sequestered from Hensen’s node in the caudal embryo. Rarely cause neurologic involvement (distinguishing this from chordoma). Sacrum may be normal in up to 50% (abnormal in almost all chordomas). Treatment is complete removal usually by general surgeon
b. peds: malignant pre-sacral teratoma is a rare tumor seen primarily in female children
2. infection: most infections of the sacrum or sacroiliac joint are due to contiguous spread from a suppurative focus
3. arthritic disorders
A. ankylosing spondylitis: (see page 502) involves SI joint almost by definition
B. osteoarthritis
4. sacral fractures: may be due to
A. trauma
B. repetitive stress
C. sacral insufficiency: see page 1193
5. congenital
A. sacral agenesis (caudal regression syndrome): rare (prevalence: 0.005-0.01%; higher (0.1-0.2%) in children of diabetic mothers (16-20% of children with sacral agenesis have diabetic mothers)). Increased incidence of associated spinal abnormalities including: syrinx, tethered cord, lipoma, and lipomyelomeningocele.
1. Four types:
Type 1: partial unilateral agenesis, localized to the sacrum or coccyx
Type 2: partial bilaterally symmetric defects in the sacrum. Iliac bones articulate with S1, and distal segments of the sacrum and coccyx fail to develop
Type 3: total sacral agenesis + iliac bones articulate with the lowest segment of the lumbar spine present
Type 4: total sacral agenesis + iliac bones fused posteriorly along the midline
2. in cases of total sacral agenesis (types 3 & 4), MR findings include: absence of the sacrum and coccyx and variable absence of a portion of the lumbar spine, with a characteristic club-shaped configuration of the conus medullaris
6. miscellaneous
A. osteitis condensans ilii: increased density in ilium, usually asymptomatic (incidental) finding. Occasionally may produce low back pain or tenderness
35.2.22.9. Enhancing nerve roots
1. tumor
A. meningeal carcinomatosis
B. lymphoma
2. infection: especially CMV (often seen in AIDS patients)
3. inflammatory
A. Guillain-Barre
B. arachnoiditis
C. sarcoid
35.2.22.10. Nodular enhancing lesions in the spinal canal
1. neurofibromatosis (NFT)
2. tumor
A. drop mets
B. neurofibroma
C. schwannoma
35.2.22.11. Intraspinal cysts
1. spinal meningeal cysts: see page 509
2. cystic neurofibroma:
3. ependymoma: may be cystic. In filum terminale: myxopapillary ependymoma (see page 731)
4. syringomyelia: see page 510
5. dilated central canal: see page 510
35.2.22.12. Diffuse enhancement of nerve roots/cauda equina
(As distinct from nodular enhancement, see above)
1. Guillain-Barre (see page 66)
2. meningitis
3. cytomegalovirus (CMV) (especially in AIDS)
4. lymphoma
5. sarcoid (look for hilar adenopathy)
35.3. References
1. Ungar-Sargon J Y, Lovelace R E, Brust J C: Spastic paraplegia-paraparesis: A reappraisal. J Neurol Sci 46: 1-12, 1980.
2. George W E, Wilmot M, Greenhouse A, et al.: Medical management of steroid-induced epidural lipomatosis. N Engl J Med 308: 316-9, 1983.
3. Nagashima C: Cervical myelopathy due to ossification of the posterior longitudinal ligament. J Neurosurg 37: 653-60, 1972.
4. Lucchesi A C, White W L, Heiserman J E, et al.: Review of arachnoiditis ossificans with a case report. BNI Quarterly 14: 4-9, 1998.
5. Marshman L A G, Hardwidge C, Ford-Dunn S Z, et al.: Idiopathic spinal cord herniation: Case report and review of the literature. Neurosurgery 44: 1129-33, 1999.
6. Darbar A, Krishnamurthy S, Holsapple J W, et al.: Ventral thoracic spinal cord herniation: Frequently misdiagnosed entity. Spine 31 (17): E600-5, 2006.
7. Fox M W, Onofrio B M: The natural history and management of symptomatic and asymptomatic vertebral hemangiomas. J Neurosurg 78: 36-45, 1993.
8. Harik S I, Raichle M E, Reis D J: Spontaneous remitting spinal epidural hematoma in a patient on anticoagulants. N Engl J Med 284: 1355-7, 1971.
9. Packer N P, Cummins B H: Spontaneous epidural hemorrhage: A surgical emergency. Lancet 1: 356-8, 1978.
10. Brem S S, Hafler D A, Van Uitert R L, et al.: Spinal subarachnoid hematoma: A hazard of lumbar puncture resulting in reversible paraplegia. N Engl J Med 303: 1020-1, 1981.
11. Rengachary S S, Murphy D: Subarachnoid hematoma following lumbar puncture causing compression of the cauda equina. J Neurosurg 41: 252-4, 1974.
12. Epstein N E, Danto J, Nardi D: Evaluation of intraoperative somatosensory-evoked potential monitoring during 100 cervical operations. Spine 18: 737-47, 1993.
13. Tobin W D, Layton D D: The diagnosis and natural history of spinal cord arteriovenous malformations. Mayo Clin Proc 51: 637-46, 1976.
14. Wirth F P, Post K D, Di Chiro G, et al.: Foix-Alajouanine disease. Spontaneous thrombosis of a spinal cord arteriovenous malformation: A case report. Neurology 20: 1114-8, 1970.
15. Rothman R H, Simeone F A, (eds.): The spine. 2nd ed., W.B. Saunders, Philadelphia, 1982.
16. Wingerchuk D M, Lennon V A, Pittock S J, et al.: Revised diagnostic criteria for neuromyelitis optica. Neurology 66: 1485-9, 2006.
17. Lennon V A, Wingerchuk D M, Kryzer T J: A serum autoantibody marker of neuromyelitis optica: Distinction from multiple sclerosis. Lancet 364 (9451): 2106-12, 2004.
18. Pruthi R K, Tefferi A: Pernicious anemia revisited. Mayo Clin Proc 69: 144-50, 1994.
19. Elia M: Oral or parental therapy for B12 deficiency. Lancet 352: 1721-2, 1998 (commentary).
20. Altrocchi P H: Acute spinal epidural abscess vs acute transverse myelopathy: A plea for neurosurgical caution. Arch Neurol 9: 17-25, 1963.
21. Sheremata W A, Berger J R, Harrington W J, et al.: Human T lymphotropic virus type I-associated myelopathy: A report of 10 patients born in the United States. Arch Neurol 49: 1113-8, 1992.
22. Busby M, Donaghy M: Chronic dysimmune neuropathy. A subclassification based upon the clinical features of 102 patients. J Neurol 250 (6): J Neurol: 714-24, 2003.
23. Rowland L P: Diagnosis of amyotrophic lateral sclerosis. J Neurol Sci 160: S6-24, 1998.
24. Deen H G: Diagnosis and management of lumbar disk disease. Mayo Clin Proc 71: 283-7, 1996.
25. Gritza T, Taylor T K F: A ganglion arising from a lumbar articular facet associated with low back pain and sciatica. J Bone Joint Surg 52: 528-31, 1970.
26. Kitigawa H, Kanamori M, Tatezaki S, et al.: Multiple spinal ossified arachnoiditis. A case report. Spine 15: 1236-8, 1990.
27. Thakkar D H, Porter R W: Heterotopic ossification enveloping the sciatic nerve following posterior fracture-dislocation of the hip: A case report. Injury 13: 207-9, 1981.
28. Johanson N A, Pellici P M, Tsairis P, et al.: Nerve injury in total hip arthroplasty. Clin Orthop 179: 214-22, 1983.
29. Burkman K A, Gaines R W, Kashani S R, et al.: Herpes zoster: A consideration in the differential diagnosis of radiculopathy. Arch Phys Med Rehabil 69: 132-4, 1988.
30. Bickels J, Kahanovitz N, Rupert C K, et al.: Extraspinal bone and soft-tissue tumors as a cause of sciatica. Clinical diagnosis and recommendations: Analysis of 32 cases. Spine 24: 1611-6, 1999.
31. Jones B V, Ward M W: Myositis ossificans in the biceps femoris muscles causing sciatic nerve palsy: A case report. J Bone Joint Surg 62B: 506-7, 1980.
32. Thompson R C, Berg T L: Primary bone tumors of pelvis presenting as spinal disease. Orthopedics 19: 1011-6, 1996.
33. Ropper A H: Unusual clinical variants and signs in Guillain-Barre syndrome. Arch Neurol 43 (11): 1150-2, 1986.
34. Frymoyer J W: Back pain and sciatica. N Engl J Med 318: 291-300, 1988.
35. Deyo R A, Rainville J, Kent D L: What can the history and physical examination tell us about low back pain? JAMA 268: 760-5, 1992.
36. Janin Y, Epstein J A, Carras R, et al.: Osteoid osteomas and osteoblastomas of the spine. Neurosurgery 8: 31-8, 1981.
37. Calin A, Porta J, Fries J F, et al.: Clinical history as a screening test for ankylosing spondylitis. JAMA 237: 2613-4, 1977.
38. Crayton H E, Bell C L, De Smet A A: Sacral insufficiency fractures. Sem Arth Rheum 20: 378-84, 1991.
39. McCarron R F, Wimpee M W, Hudkins P G, et al.: The inflammatory effect of nucleus pulposus: A possible element in the pathogenesis of low-back pain. Spine 12: 760-4, 1987.
40. Hirsch C, Schajowicz F: Studies on structural changes in the lumbar annulus fibrosus. Acta Orthop Scand 22: 184-231, 1952.
41. Choice of lipid-regulating drugs. Med Letter 43 (1105): 43-8, 2001.
42. Seftel A D, Farber J, Fletcher J, et al.: A three-part study to investigate the incidence and potential etiologies of tadalafil-associated back pain or myalgia. Int J Impot Res 17 (5): 455-61, 2005.
43. Jensen M C, Brant-Zawadzki M N, Obuchowski N, et al.: Magnetic resonance imaging of the lumbar spine in people without back pain. N Engl J Med 331: 69-73, 1994.
44. Bonney G: Iatrogenic injuries of nerves. J Bone Joint Surg 68B: 9-13, 1986.
45. Eskandary H, Hamzel A, Yasamy M T: Foot drop following brain lesion. Surg Neurol 43: 89-90, 1995.
46. Bell H S: Paralysis of both arms from injury of the upper portion of the pyramidal decussation: “cruciate paralysis”. J Neurosurg 33 (4): J Neurosurg: 376-80, 1970.
47. Yayama T, Uchida K, Kobayashi S, et al.: Cruciate paralysis and hemiplegia cruciata: Report of three cases. Spinal Cord 44 (6): Spinal Cord: 393-8, 2006.
48. Hawkins R J, Bilco T, Bonutti P: Cervical spine and shoulder pain. Clin Orthop Rel Res 258: 142-6, 1990.
49. Goldenberg D L: Fibromyalgia syndrome. JAMA 257: 2782-7, 1987.
50. Wolfe F, Smythe H A, Yunus M B, et al.: The American college of rheumatology 1990 criteria for the classification of fibromyalgia: Report of the multicenter criteria committee. Arthritis Rheum 33: 160-72, 1990.
51. Adler G K, Kinsley B T, Hurwitz S, et al.: Reduced hypothalamic-pituitary and sympathoadrenal responses to hypoglycemia in women with fibromyalgia syndrome. Am J Med 106: 534-43, 1999.
52. Stricker L J, Green C R: Resolution of refractory symptoms of secondary erythermalgia with intermittent epidural bupivacaine. Reg Anesth Pain Med 26: 488-90, 2001.
53. Davis M D, Sandroni P: Lidocaine patch for pain of erythromelalgia. Arch Dermatol 138: 17-9, 2002.
54. Sobel J B, Sollenberger P, Robinson R, et al.: Cervical nonorganic signs: A new clinical tool to assess abnormal illness behavior in neck pain patients. Arch Phys Med Rehabil 81: 170-5, 2000.
55. Cardoso E R, Peterson E W: Pituitary apoplexy: A review. Neurosurgery 14: 363-73, 1984.
56. Kapoor W N: Evaluation and management of the patient with syncope. JAMA 268: 2553-60, 1992.
57. Barron S A, Rogovski Z, Hemli Y: Vagal cardiovascular reflexes in young persons with syncope. Ann Intern Med 118: 943-6, 1993.
58. Miller T H, Kruse J E: Evaluation of syncope. Am Fam Physician 72 (8): Am Fam Physician: 1492-500, 2005.
59. Linzer M, Yang E H, Estes N A, 3rd, et al.: Diagnosing syncope. Part 1: Value of history, physical examination, and electrocardiography. Clinical efficacy assessment project of the American college of physicians. Ann Intern Med 126 (12): Ann Intern Med: 989-96, 1997.
60. Sarasin F P, Louis-Simonet M, Carballo D, et al.: Prospective evaluation of patients with syncope: A population-based study. Am J Med 111 (3): Am J Med: 177-84, 2001.
61. Brignole M, Alboni P, Benditt D, et al.: Guidelines on management (diagnosis and treatment) of syncope. Eur Heart J 22 (15): Eur Heart J: 1256-306, 2001.
62. Smith D B, Hitchcock M, Philpot P J: Cerebral amyloid angiopathy presenting as transient ischemic attacks: Case report. J Neurosurg 63: 963-4, 1985.
63. Greenberg S M, Vonsattel J P, Stakes J W, et al.: The clinical spectrum of cerebral amyloid angiopathy: Presentations without lobar hemorrhage. Neurology 43: 2073-9, 1993.
64. Kaminski H J, Hlavin M L, Likavec M J, et al.: Transient neurologic deficit caused by chronic subdural hematoma. Am J Med 92: 698-700, 1992.
65. Moster M, Johnston D, Reinmuth O: Chronic subdural hematoma with transient neurologic deficits: A review of 15 cases. Ann Neurol 14: 539-42, 1983.
66. McLaurin R: Contributions of angiography to the pathophysiology of subdural hematomas. Neurology 15: 866-73, 1965.
67. Apter A, Mott A, Frank M, et al.: Allergic rhinitis and olfactory loss. Ann Allergy Asthma Immunol 75: 311-6, 1995.
68. Emmett E: Parosmia and hyposmia induced by solvent exposure. Br J Ind Med 33: 196-, 1976.
69. Lieblich J M, Rogol A D, White B J, et al.: Syndrome of anosmia with hypogonadotropic hypogonadism (Kallmann syndrome): Clinical and laboratory studies in 23 cases. Am J Med 73 (4): Am J Med: 506-19, 1982.
70. Beal M F: Multiple cranial-nerve palsies - a diagnostic challenge. N Engl J Med 322: 461-3, 1990.
71. Krisht A F: Giant invasive pituitary adenomas. Contemp Neurosurg 21 (1): 1-6, 1999.
72. Manni J J, Scaf J J, Huygen P L M, et al.: Hyperostosis cranialis interna: A new hereditary syndrome with cranial-nerve entrapment. N Engl J Med 322: 450-4, 1990.
73. Chen J-R, Rhee R S C, Wallach S, et al.: Neurologic disturbances in Paget disease of bone: Response to calcitonin. Neurology 29: 448-57, 1979.
74. Wilkins R H, Rengachary S S, (eds.): Neurosurgery. McGraw-Hill, New York, 1985.
75. Al-Mefty O, Fox J L, Al-Rodhan N, et al.: Optic nerve decompression in osteopetrosis. J Neurosurg 68: 80-4, 1988.
76. Salvarani C, Cantini F, Boiardi L, et al.: Polymyalgia rheumatica and giant-cell arteritis. N Engl J Med 347: 261-71, 2002.
77. Clark W C, Theofilos C S, Fleming J C: Primary optic sheath meningiomas: Report of nine cases. J Neurosurg 70: 37-40, 1989.
78. Gibson R D: Measurement of proptosis (exophthalmos) by computerised tomography. Australas Radiol 28 (1): Australas Radiol: 9-11, 1984.
79. Peyster R G, Ginsberg F, Silber J H, et al.: Exophthalmos caused by excessive fat: CT volumetric analysis and differential diagnosis. AJR Am J Roentgenol 146 (3): AJR Am J Roentgenol: 459-64, 1986.
80. Strassburg H M: Macrocephaly is not always due to hydrocephalus. J Child Neurol 4 (Suppl): S32-40, 1989.
81. Section of Pediatric Neurosurgery of the American Association of Neurological Surgeons, (ed.) Pediatric neurosurgery. 1st ed., Grune and Stratton, New York, 1982.
82. Rushton A R, Shaywitz B A, Duncan C C, et al.: Computed tomography in the diagnosis of Canavan’s disease. Ann Neurol 10: 57-60, 1981.
83. Carpenter M B: Core text of neuroanatomy. 2nd ed. Williams and Wilkins, Baltimore, 1978.
84. Rekate H, Grubb R, Aram D, et al.: Muteness of cerebellar origin. Arch Neurol 42: 637-8, 1985.
85. Ammirati M, Mirzai S, Samii M: Transient mutism following removal of a cerebellar tumor: A case report and review of the literature. Childs Nerv Syst 5: 12-4, 1989.
86. Apuzzo M L J: Surgery of masses affecting the third ventricular chamber: Techniques and strategies. Clin Neurosurg 34: 499-522, 1988.
87. Ho V B, Smirniotopoulos J G, Murphy F M, et al.: Radiologic-pathologic correlation: Hemangioblastoma. AJNR 13: 1343-52, 1992.
88. Laurent J P, Cheek W R: Brain tumors in children. J Pediatr Neurosci 1: 15-32, 1985.
89. Inoue Y, Tabuchi T, Hakuba A, et al.: Facial nerve neuromas: CT findings. J Comput Assist Tomogr 11: 942-7, 1987.
90. Tew J M, Yeh H S, Miller G W, et al.: Intratemporal schwannoma of the facial nerve. Neurosurgery 13: 186-8, 1983.
91. Enyon-Lewis N J, Kitchen N, Scaravilli F, et al.: Neurenteric cyst of the cerebellopontine angle. Neurosurgery 42: 655-8, 1998.
92. Onofrio B M, Mih A D: Synovial cysts of the spine. Neurosurgery 22: 642-7, 1988.
93. O’Neill B P, Illig J J: Primary central nervous system lymphoma. Mayo Clin Proc 64: 1005-20, 1989.
94. Davis D O: Sellar and parasellar lesions. Clin Neurosurg 17: 160-88, 1970.
95. Kovacs K: Metastatic cancer of the pituitary gland. Oncology 27 (6): 533-42, 1973.
96. Atchison J A, Lee P A, Albright L: Reversible suprasellar pituitary mass secondary to hypothyroidism. JAMA 262: 3175-7, 1989.
97. Taylor S L, Barakos J A, Harsh G R, et al.: Magnetic resonance imaging of tuberculum sellae meningiomas: Preventing preoperative misdiagnosis as pituitary macroadenoma. Neurosurgery 31: 621-7, 1992.
98. Symon L, Rosenstein J: Surgical management of suprasellar meningioma. J Neurosurg 61: 633-41, 1984.
99. Mai A, Karis J, Sivakumar K: Meningioma with pneumosinus dilatans. Neurology 60 (11): Neurology: 1861, 2003.
100. Hoffman H J, Ostubo H, Hendrick E B, et al.: Intracranial germ-cell tumors in children. J Neurosurg 74: 545-51, 1991.
101. Aarabi B, Haghshenas M, Rakeii V: Visual failure caused by suprasellar extramedullary hematopoiesis in beta thalassemia: Case report. Neurosurgery 42 (4): 922-5; discussion 925-6, 1998.
102. Daniels D L, Williams A L, Thornton R S, et al.: Differential diagnosis of intrasellar tumors by computed tomography. Radiology 141: 697-701, 1981.
103. Gutenberg A, Larsen J, Lupi I, et al.: A radiologic score to distinguish autoimmune hypophysitis from nonsecreting pituitary adenoma preoperatively. AJNR Am J Neuroradiol 30 (9): AJNR Am J Neuroradiol: 1766-72, 2009.
104. Kucharczyk W, Davis D O, Kelly W M, et al.: Pituitary adenomas: High-resolution MR imaging at 1.5 T. Radiology 161: Radiology: 761-5, 1986.
105. Miyake I, Takeuchi Y, Kuramoto T, et al.: Autoimmune hypophysitis treated with intravenous glucocorticoid therapy. Intern Med 45: Intern Med: 1249-52, 2006.
106. Carpenter K J, Murtagh R D, Lilienfeld J, et al.: Ipilimumab-induced hypophysitis: MR imaging findings. AJNR 30 (9): AJNR: 1751-3, 2009.
107. Harsh G R, Edwards M S B, Wilson C B: Intracranial arachnoid cysts in children. J Neurosurg 64: 835-42, 1986.
108. Miller M E, Kido D, Horner F: Cavum vergae: Association with neurologic abnormality and diagnosis by magnetic resonance imaging. Arch Neurol 43: 821-3, 1986.
109. Sekhar L N, Moller A R: Operative management of tumors involving the cavernous sinus. J Neurosurg 64: 879-89, 1986.
110. Knosp E, Perneczky A, Koos W T, et al.: Meningiomas of the space of the cavernous sinus. Neurosurgery 38: 434-44, 1996.
111. Knosp E, Steiner E, Kitz K, et al.: Pituitary adenomas with invasion of the cavernous sinus space: A magnetic resonance imaging classification compared with surgical findings. Neurosurgery 33: 610-8, 1993.
112. Thomas J E, Baker H L: Assessment of roentgeno-graphic lucencies of the skull: A systematic approach. Neurology 25: 99-106, 1975.
113. Horning G W, Beatty R M: Osteolytic skull lesions secondary to trauma. J Neurosurg 72: 506-8, 1990.
114. Le Roux P D, Griffin G E, Marsh H T, et al.: Tuberculosis of the skull - a rare condition: Case report and review of the literature. Neurosurgery 26: 851-6, 1990.
115. Lopez-Villegas D, Kulisevsky J, Deus J, et al.: Neuropsychological alterations in patients with computed tomography-detected basal ganglia calcification. Arch Neurol 53: 251-6, 1996.
116. Ang L C, Alport E C, Tchang S: Fahr’s disease associated with astrocytic proliferation and astrocytoma. Surg Neurol 39: 365-9, 1993.
117. Bhimani S, Sarwar M, Virapongse C, et al.: Computed tomography of cerebrovascular calcifications in postsurgical hypoparathyroidism. J Comput Assist Tomogr 9: 121-4, 1985.
118. Morrison G, Sobel D F, Kelley W M, et al.: Intraventricular mass lesions. Radiology 153: 435-42, 1984.
119. D’Angelo V A, Galarza M, Catapano D, et al.: Lateral ventricle tumors: Surgical strategies according to tumor origin and development - a series of 72 cases. Neurosurgery 56: ONS36-45, 2005.
120. Brat D J, Scheithauer B W, Staugaitis S M, et al.: Third ventricular chordoid glioma: A distinct clinicopathologic entity. J Neuropathol Exp Neurol 57 (3): 283-90, 1998.
121. Jelinek J, Smirniotopoulos J G, Parisi J E, et al.: Lateral ventricular neoplasms of the brain: Differential diagnosis based on clinical, CT, and MR findings. AJNR 11: 567-74, 1990.
122. Kinkel W R, Jacobs L, Polachini I, et al.: Subcortical arteriosclerotic encephalopathy (Binswanger’s disease). Arch Neurol 42: 951-9, 1985.
123. Roman G C: Senile dementia of the Binswanger type: A vascular form of dementia in the elderly. JAMA 258: 1782-8, 1987.
124. Hachinski V C, Potter P, Merskey H: Leuko-araiosis. Arch Neurol 44: 21-3, 1987.
125. Steingart A, Hachinski V C, Lau C, et al.: Cognitive and neurologic findings in subjects with diffuse white matter lucencies on computed tomographic scan (leuko-araiosis). Arch Neurol 44: 32-5, 1987.
126. Zatz L M, Jernigan T L, Ahumada A J: White matter changes in cerebral computed tomography related to aging. J Comput Assist Tomogr 6: 19-23, 1982.
127. Janota I, Mirsen T R, Hachinski V C, et al.: Neuropathologic correlates of leuko-araiosis. Arch Neurol 46: 1124-8, 1989.
128. Paakko E, Patronas N J, Schellinger D: Meningeal gd-dtpa enhancement in patients with malignancies. J Comput Assist Tomogr 14 (4): 542-6, 1990.
129. River Y, Schwartz A, Gomori J M, et al.: Clinical significance of diffuse dural enhancement detected by magnetic resonance imaging. J Neurosurg 85 (5): 777-83, 1996.
130. Sze G, Soletsky S, Bronen R, et al.: MR imaging of the cranial meninges with emphasis on contrast enhancement and meningeal carcinomatosis. AJNR 10: 965-75, 1989.
131. Guerini H, Helie O, Leveque C, et al.: [diagnosis of periventricular ependymal enhancement in MRI in adults]. J Neuroradiol 30 (1): 46-56, 2003 (French).
132. Fukui M B, Williams R L, Mudigonda S: CT and MR imaging features of pyogenic ventriculitis. AJNR Am J Neuroradiol 22 (8): 1510-6, 2001.
133. Butler W E, Khan A, Khan S A: Posterior fossa ependymoma with intense but transient disseminated enhancement but not metastasis. Pediatr Neurosurg 37 (1): 27-31, 2002.
134. Mohr G, Ferguson G, Khan M, et al.: Intraventricular hemorrhage from ruptured aneurysm: Retrospective analysis of 91 cases. J Neurosurg 58: 482-7, 1983.
135. Brandwein S, Esdaile J, Danoff D, et al.: Wegener’s granulomatosis: Clinical features and outcome in 13 patients. Arch Intern Med 143: 476-9, 1983.
136. Jeng Y M, Sung M T, Fang C L, et al.: Sinonasal un-differentiated carcinoma and nasopharyngeal-type undifferentiated carcinoma: Two clinically, biologically, and histopathologically distinct entities. Am J Surg Pathol 26 (3): 371-6, 2002.
137. Morita A, Ebersold M J, Olsen K D, et al.: Esthesioneuroblastoma: Prognosis and management. Neurosurgery 32: 706-15, 1993.
138. Hlavac P J, Henson S L, Popp A J: Esthesioneuroblastoma: Advances in diagnosis and treatment. Contemp Neurosurg 20 (8): 1-5, 1998.
139. Martel W, Tishler J M: Observations on the spine in mongoloidism. Am J Roentgenol Radium Ther Nucl Med 97 (3): Am J Roentgenol Radium Ther Nucl Med: 630-8, 1966.
140. Lakhkar B, Aggarwal M, Jose J: Pictorial essay: MR appearances of osseous spine tumors. Indian J Radiol Imaging 12: 383-90, 2002.
141. Piper J G, Menezes A H: Management strategies for tumors of the axis vertebra. J Neurosurg 84: 543-51, 1996.
142. Molloy S, Saifuddin A, Allibone J, et al.: Excision of an osteoid osteoma from the body of the axis through an anterior approach. Eur Spine J 11 (6): 599-601, 2002.
143. Honma G, Murota K, Shiba R, et al.: Mandible and tongue-splitting approach for giant cell tumor of axis. Spine 14: 1204-10, 1989.
144. Osenbach R K, Youngblood L A, Menezes A H: Atlanto-axial instability secondary to solitary eosinophilic granuloma of C2 in a 12-year-old girl. Case report. J Spinal Disord 3: 408-12, 1990.
145. Verbiest H: Benign cervical spine tumors: Clinical experience. In The cervical spine, The Cervical Spine Research Society Editorial Committee, (ed.). J.B. Lippincott, Philadelphia, 2nd ed., 1989: pp 723-74.
146. Li K, Poon P: Sensitivity and specificity of MRI in detecting spinal cord compression and in distinguishing malignant from benign compression fractures of vertebrae. Magn Reson Imaging 6: 547-56, 1988.
147. Yuh W, Zachar C, Barloon T, et al.: Vertebral compression fractures: Distinction between benign and malignant causes with MR imaging Radiology 172: 215-8, 1989.
148. Kuntz D, Naveau B, Bardin T, et al.: Destructive spondyloarthropathy in hemodialyzed patients: A new syndrome. Arthritis Rheum 27: 369-75, 1984.
149. Alcalay M, Goupy M-C, Azais I, et al.: Hemodialysis is not essential for the development of destructive spondyloarthropathy in patients with chronic renal failure. Arthritis Rheum 30: 1182-6, 1987.
150. Borges L F: Case records of the Massachusetts General Hospital: Case 24-1989. N Engl J Med 320: 1610-8, 1989.
151. Cawley M D, Chalmers T M, Kellgren J H, et al.: Destructive lesions of vertebral bodies in ankylosing spondylitis. Ann Rheum Dis 31: 345-8, 1972.
152. Rothman R H, Simeone F A, (eds.): The Spine. 3rd ed., W.B. Saunders, Philadelphia, 1992.