Helen Hatcher
Case history
A 19-year-old woman presented with a fracture of the left femur (Fig. 24.1), sustained after a football tackle during a summer camp overseas. The femur was pinned, but because of abnormalities seen during surgery, samples of bone were sent for histopathological examination, which confirmed a diagnosis of osteosarcoma.

Fig. 24.1
Questions
1. What is the relevance of the fracture, and what impact does it have on the prognosis of osteosarcoma?
2. What further investigations are recommended?
3. What treatment should be recommended next?
4. What is the role of radiotherapy in this case?
Answers
1. What is the relevance of the fracture, and what impact does it have on the prognosis of osteosarcoma?
Pathological fracture in osteosarcoma is associated with a worse prognosis, especially if the lesion is pinned, due to potential dissemination of tumour along the bone marrow and into the blood stream. In one study, osteosarcoma patients with pathological fracture had lower 10-year overall survival than those without (34% versus 58%, P < 0.01) (Bramer et al. 2007).
2. What further investigations are recommended?
Staging and investigations at diagnosis include MRI of the primary and the joints on either side to examine the extent of disease and to detect skip lesions. CT of the chest is needed to exclude lung metastases and bone scan to rule out bone metastases. Investigations which will be required prior to starting systemic treatment include echocardiogram, nuclear medicine evaluation of renal function (GFR), FBC, biochemistry, coagulation screen, and placement of a central venous catheter to administer chemotherapy.
Staging in this patient confirmed that the left femur was the only site of disease.
3. What treatment should be recommended next?
Ideally, the pathological fracture should not have been pinned but stabilized by brace, case, or external fixation following a biopsy. Chemotherapy is the primary treatment in patients with pathological fracture, followed by limb-salvage surgery if possible.
Since this patient had a pinning of the pathological fracture, which carries a high risk of disseminated micrometastases, the priority at this stage is to give systemic treatment with combination chemotherapy. There is no worldwide consensus on the standard chemotherapy. The current UK recommendation is a combination of cisplatin given with doxorubicin and high-dose methotrexate (the MAP regimen). A recent meta-analysis showed that the MAP regimen gives a significantly better outcome than a combination of cisplatin and adriamycin (Anninga et al. 2011).
The abnormal bone should be resected after two cycles of MAP, preferably with an endoprosthetic replacement. (The EURAMOS trial (<http://www.ctu.mrc.ac.uk/euramos/euramos_i_trial.asp>) has been set up to evaluate the role of changing chemotherapy if a poor response is seen at the time of surgery and to evaluate the benefit of the addition of biological agents such as interferon, but has completed recruitment.) Outside a trial, four more cycles of MAP are given post-operatively. In patients over the age of 40, high-dose methotrexate is unlikely to be safely tolerated so these patients are treated with cisplatin and doxorubicin alone. There is controversial evidence about the use of another biological agent, mifamurtide (a liposomal formulation of the immune stimulant muramyl tripeptide phosphatidylethanolamine), which can be given postoperatively with MAP chemotherapy. In selected cases, it can improve 6-year overall survival by an additional 8% (78% versus 70%). This is licensed for the treatment in resectable osteosarcoma, and the evidence should therefore be discussed with the patient.
4. What is the role of radiotherapy in this case?
Radiotherapy is not routinely given in osteosarcoma as this is a relatively radioresistant disease. However, in selected cases, such as pathological fracture, tumour crossing the cortex, and poor margins at surgery, radiotherapy may be given to improve local control.
She completed treatment and went onto regular follow-up with chest X-ray and X-ray of the left femur every 3 months. The chest X-ray taken 9 months after completion of treatment is shown in Fig. 24.2.
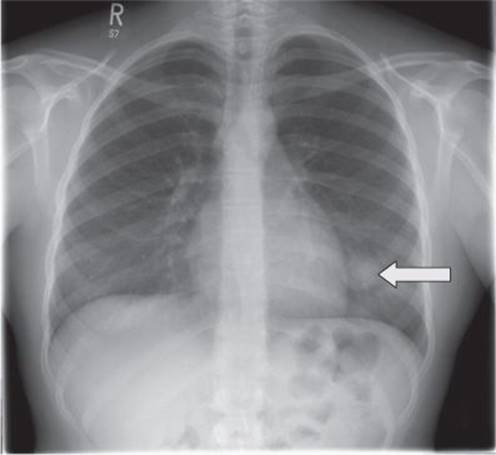
Fig. 24.2
Questions
5. What does the chest X-ray in Fig. 24.2 show?
6. How do you investigate?
7. What are the treatment options and what is the role of chemotherapy?
8. What is the prognosis?
Answers
5. What does the chest X-ray in Fig. 24.2 show?
The chest X-ray shows a solitary round lesion in the left chest close to the heart border. Given the relatively short time since completion of treatment for osteosarcoma, this is likely to represent a lung metastasis.
6. How do you investigate?
A CT scan of the chest should be done to rule out multiple metastases and define in more detail the lesion seen on the chest X-ray. A bone scan should also be done to rule out bone metastases. The CT scan showed a single lesion in the left lower lobe (Fig. 24.3).
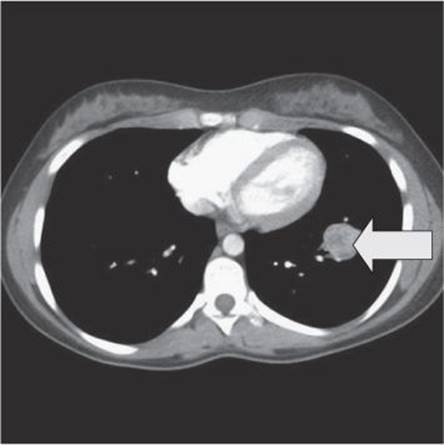
Fig. 24.3
7. What are the treatment options and what is the role of chemotherapy?
The treatment options include removal of the metastasis by wedge resection or lobectomy and further chemotherapy. Ideally, surgery, which removes the lesion with a safe margin but with the lowest impact on lung function (wedge resection), should be performed if possible. There are no randomized trials examining the role of chemotherapy before or after surgery. However, relapse in a site that had no previous lung nodule within less than a year is a poor prognostic sign and many clinicians would advocate chemotherapy with a drug that is known to be active in osteosarcoma and that was not used in the neoadjuvant or adjuvant setting. In this situation, ifosfamide with etoposide or high-dose ifosfamide may be considered. This can be given pre- and post-operatively—giving some pre-operatively allows for systemic treatment upfront without a post-operative delay if the recovery period is prolonged.
8. What is the prognosis?
In this specific patient the prognosis is guarded because relapse has occurred within less than a year, but long-term survival is still possible in 10–15% of patients. Factors which predict for a poorer outcome in this situation include the short time between the end of treatment and relapse, suggesting a rapidly growing tumour.
After further treatment, the patient remained well for 23 months but was found to have an abnormal chest X-ray at follow-up. CT staging is shown in Fig. 24.4.
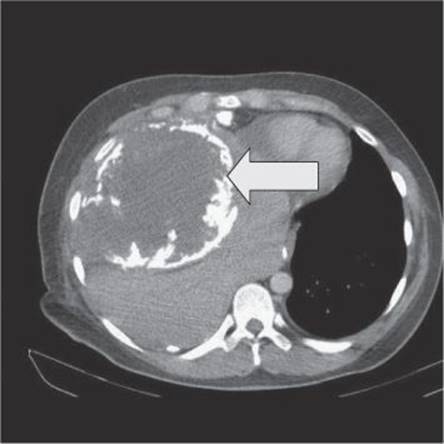
Fig. 24.4
Question
9. What options does she have now and what is her prognosis?
Answer
9. What options does she have now and what is her prognosis?
The CT scan (Fig. 24.4) shows an extensive lesion with calcification. In view of the large size of the recurrence there is no realistic curative treatment option. Palliative options, if the patient chooses to opt for palliative chemotherapy, could include gemcitabine with docetaxel or oral etoposide. Opting for supportive care only would also be an option if the patient chooses. Her prognosis is now severely limited due to the rapid occurrence (between 3-monthly chest X-rays) of a large tumour bulk. Palliative care services should be involved from an early stage.
Further reading
Anninga JK, Gelderblom H, Fiocco M, et al. Chemotherapeutic adjuvant treatment for osteosarcoma: where do we stand? European Journal of Cancer 2011; 47: 2431–2445.
Bramer JA, Abudu AA, Grimer RJ, Carter SR, Tillman RM. Do pathological fractures influence survival and local recurrence rate in bony sarcomas? European Journal of Cancer 2007; 43: 1944–1951.
DeLaney TF, Park L, Goldberg SI, et al. Radiotherapy for local control of osteosarcoma. International Journal of Radiation Oncology Biology Physics 2005; 61: 492–498.
Meyers PA, Schwartz CL, Krailo MD, et al. Osteosarcoma: the addition of muramyl tripeptide to chemotherapy improves overall survival-a report from the Children’s Oncology Group. Journal of Clinical Oncology 2008; 26: 633–638.