Kenneth Crump
Key Points
· Risks of accidental exposure to cytotoxic drugs
· The greatest risks are during preparation and administration.
· Compounding pharmacies are often contracted to prepare drugs for administration.
· Equipment and supplies for the preparation of chemotherapy drugs
· Closed-system devices or medication containment devices like PhaSeal® and Onguard® are now available.
· Workspace preparation for the preparation of chemotherapy drugs
· The minimum requirement is a clean workspace in a small area with good ventilation and minimal traffic.
· Minimizing errors to protect your cancer patients
· Six steps to increase awareness and protect patients from chemotherapy-related errors
· Equipment and supplies for the administration of chemotherapy drugs
· Choosing the right catheter for the job
· Workspace preparation for the administration of chemotherapy drugs
· Overcoming accidents and errors often related to the workspace layout and common distractions
Introduction
It is common for members of a veterinary healthcare team to regard themselves as immune from any harm arising from their work. As a result, many of us inadvertently expose ourselves and others to hazardous substances while practicing every precaution to ensure that the substances themselves are protected from contamination. However, even inadvertent exposure to cytotoxic chemotherapy drugs can have very real consequences.
Cytotoxic means toxic to cells. Treating cancer cells with a cytotoxic compound can result in a variety of cell fates. The cells may lose cell membrane integrity, rupture, and die rapidly. The cells might just stop actively growing and dividing, or the compounds may force them to activate a program of controlled cell death, called apoptosis. In all of these cases, the cytotoxic chemotherapy compounds cannot tell the difference between the harmful cancer cells and the cells of normal healthy tissue. Normal tissues accidentally exposed to these substances could, over time, suffer any of these cell fates.
Nurses working in human cancer wards can sometimes experience many of the chemotherapy side effects noted by their patients. These may include nausea, dizziness, chronic headaches, hair loss, and dermatitis. More significant side effects like menstrual cycle irregularities, liver damage, infertility, and even miscarriage have also been reported. These side effects can all arise through careless handling and administration of the chemotherapy drugs.
An oncology nurse working in a human cancer ward was accidentally exposed to a solution of the chemotherapy drug carmustine. When the tubing system fell out of an infusion bottle of carmustine, all of the solution poured down her right arm and leg, and onto the floor. Although she wore gloves, her right forearm was unprotected. The solution also penetrated her clothing and stockings. She immediately washed her arm and leg with soap and water, but did not change her clothes. A few hours later, she began to experience minor abdominal distress and profuse belching. That was followed by intermittent episodes of diarrhea with cramping abdominal pain. Profuse vomiting followed, and then she felt better. Carmustine is known to cause gastric upset, and her symptoms were attributed to systemic absorption of the drug through her skin.
The risk of accidental exposure to chemotherapy agents is greatest during drug preparation and administration. The primary routes of exposure are by inhalation, direct contact, and ingestion of improperly handled drugs. The purpose of this chapter is to provide an overview of the equipment and supplies necessary to safely prepare and administer chemotherapy in a veterinary setting. Additionally, we will examine ways to prepare your workspace in order to minimize the risk of accidental exposure.
Drug Preparation
According to the National Institute for Occupational Safety and Health (NIOSH), all chemotherapy drugs should be drawn up, reconstituted, crushed, or otherwise prepared inside a biological safety cabinet (BSC) or in a negative pressure total exhaust compounding aseptic containment isolator. A BSC has vertical airflow that moves away from the worker, as opposed to horizontal airflow that moves air away from the product and toward the worker. Vertical airflow protects the worker, while horizontal airflow is designed to protect the sterile product from contamination. Air leaving a BSC is filtered and vented to the outdoors. An “isolator” is basically a glove box with external venting (see Chapter 4).
However, for many veterinary practices, such specialized equipment is cost prohibitive. Compounding cytotoxic chemotherapy drugs is especially hazardous if done without proper safety equipment. Furthermore, the drug preparation may be complex and requires special equipment or supplies that are not readily available in most veterinary clinics. For these reasons, compounding pharmacies are often contracted to prepare these drugs for administration and/or to dispense prescriptions for at-home administration by the client.
When a compounding pharmacist prepares chemotherapy for you, ask that a material safety data sheet (MSDS) and the drug package insert accompany the prescription. The MSDS provides you with procedures for handling the drug in a safe manner. The MSDS, the package insert, and the pharmacist are all valuable resources of information regarding emergency procedures in the event of accidental exposure to the drug, as well as the potential side effects, drug interactions, precautions, or contraindications associated with a particular drug.
While preparing a vincristine prescription, a pharmacy technician accidentally inhaled an aerosolized mist of the solution. His reaction included sneezing, hot flashes, swollen eyelids, shortness of breath, chest tightness, and congestion. He immediately sought medical attention in the emergency room. He was treated, and by the following morning, all of his symptoms were gone.
Preparing chemotherapy drugs in your practice is a procedure not to be taken lightly. Fortunately, new cost-effective equipment and supplies provide a satisfactory level of safety when used properly. Closed-system devices or medication containment devices like PhaSeal® (Baxa Corporation, Englewood, CO) and Onguard® (B. Braun Medical Inc., Bethlehem, PA) are now available in the United States. They consist of several components that trap drug aerosols, prevent leakage when withdrawing drugs from a vial, allow leak-free drug transfers, and provide for a “dry spike” of an intravenous (IV) bag. Studies have demonstrated the effectiveness of these devices in reducing surface and personnel contaminations.
Equipment and Supplies
Standard Operating Procedure (SOP) Manual
An SOP manual is used to ensure safety and consistency in the performance of repetitive tasks. Although it may contain seemingly redundant checks and rechecks of details like the patient’s name and the drug’s name and dose, the safety of your team and your patient is more important than efficiency. A good list of operating procedures for the preparation and administration of chemotherapy is thorough, understandable, and can be followed by any qualified member of your team. When preparing a chemotherapy SOP, consider the following:
· A good chemotherapy SOP is written with careful consideration by a knowledgeable individual or committee.
· It is concise. Use a step-by-step, bulleted approach rather than a running narrative.
· It is explicit, including every detail necessary to complete the task in your specific practice.
· It includes a flowchart or checklist as a visual picture of the steps and how they relate to one another.
· A good chemotherapy SOP is reviewed and rehearsed before it is put into practice.
Personal Protective Equipment (PPE)
Imagine the consequences to a professional football player who neglects to wear a helmet, pads, or other PPE. The PPE required for preparing and administering cytotoxic drugs in our profession includes the following:
· gown—disposable, made of fabric that has a low permeability, with a closed front and elastic cuffs;
· gloves—powder free; made of latex, nitrile, or neoprene; double glove or use gloves labeled and tested for use with chemotherapy drugs;
· face and eye protection when splashing is possible; and
· a respirator when there is a risk of inhaling drug aerosols.
Drug Preparation Supplies
The supplies for cytotoxic drug preparation are as follows:
· absorbent pad with nonporous backing
· labels
· appropriate reagents for dilution or reconstitution
o see drug package insert
· Luer lock syringes and needles
o Luer lock fittings securely joined by means of a tabbed hub on the female fitting, which screws into threads in a sleeve on the male fitting
· PhaSeal or Onguard (or similar) chemotherapy preparation supplies
· Chemo-spill kit (see below)
· sealable transfer bag
o a bag to transfer the drug from where it is prepared to where it is to be administered
o an appropriately labeled “ziplock” freezer bag
· appropriate chemo-waste disposal container
o see Chapter 4.
Prepare Your Workspace
The optimum place to prepare chemotherapy drugs is inside a BSC or a negative pressure total exhaust compounding aseptic containment isolator. In the absence of either a BSC or an isolator, designate a specific area within your hospital for this task. All that is required is a clean workspace like a countertop in a small area with good ventilation (but no drafts) and minimal traffic. Since one of the primary routes of exposure is ingestion, eating, drinking, chewing gum, and storing food are all prohibited in the preparation area. Many practices use their small animal isolation ward as their designated area for preparing chemotherapy drugs. It is usually a small area, away from the general flow of traffic through the clinic, and most of the PPE for isolation is similar to that used for chemotherapy preparation. Post signs to protect your colleagues when you are preparing cytotoxic drugs and to eliminate traffic through your work area.
Chemo-spill kit
Keep a clearly labeled chemo-spill kit near the site where chemotherapy drugs are mixed and where they are administered. Chemotherapy spill kits are commercially available or are easy to assemble and maintain on your own. Each spill kit contains at least the following:
· a respirator or heavy-duty mask
· eye protection
· two pairs of gloves
o powder free; made of latex, nitrile, or neoprene
· gown
o disposable, made of fabric that has low permeability, with closed front and elastic cuffs
· absorbent pads
o disposable diapers work well
· two large ziplock chemo-waste disposal bags.
When a spill occurs, contain and absorb the spilled liquid with absorbent pads or kitty litter. While wearing gloves, absorb the remaining liquid with paper towels. Place the paper towels and all other contaminated materials in an appropriate chemo-waste receptacle. Then, clean the contaminated area with water and detergent.
Drug Administration
Experts estimate that as many as 98,000 people die in any given year from medical errors that occur in hospitals. That is the equivalent of a jumbo jet airliner crashing each and every day of the year, which is more than the number of people who die annually from motor vehicle accidents, breast cancer, or AIDS.
Although there are no studies regarding the number of animals who die in any given year from medical errors, the statistics on human medical errors underscore the need for personal attention to details. When each member of a medical team takes personal responsibility for the welfare of each patient, then any single member of the team can protect a pet from being harmed by a medical accident.
A technician with more than a decade of experience in a large multidoctor referral practice gathered supplies to administer chemotherapy to a canine patient. The day was hectic and she had begun to fall behind schedule. When she received the patient’s chemotherapy from the in-house pharmacy, the technician rechecked the patient’s name and dose on the chemotherapy bag. Both were accurate. Finally, she confirmed with the doctor that she should begin administration. Afterward, when the technician updated the patient’s record, she realized that the dog should not have received chemotherapy on that visit. He was scheduled only for a blood test. The “system” had failed that patient in several ways. However, if the technician had simply reviewed the patient’s record before administering chemotherapy, she could have prevented significant risk to the dog’s health.
As an integral part of a veterinary healthcare team, the veterinary technician stands as the last line of defense between what could happen to a patient and what does happen to a patient in the hospital. Here are some simple steps you can take to increase your awareness and to protect your patients from being harmed by a chemotherapy-related error.
(1) Review the patient’s record.
· Try to review your patient’s record before its appointment, and definitely before you begin a treatment. Things to look for in the record:
o What disease does this patient have?
o Why is the pet here today?
o What other therapy is the pet receiving?
o Does the owner have any specific concerns?
o Is there anything about this case that you do not understand?
(2) Recheck the patient’s blood test results.
· There are more than 50 chemotherapy drugs available to treat cancer, and many of them interfere with the body’s ability to make white blood cells.
· Neutrophils (also called “segs”) are the most abundant of the white blood cells and form an integral part of the immune system
· An insufficient number of neutrophils could be a cause to postpone a chemotherapy treatment. Your clinic will establish a minimum acceptable number of neutrophils for treatment. Be sure you know that number.
(3) Recheck the drug name and dose.
· After reviewing the record, be sure the drug name and the dose you are about to administer make sense to you. If you discover an inconsistency, or something you do not understand, ask the doctor for clarification.
(4) Recheck the dose calculation.
· Math errors are the most frequent and are often the most dangerous of medical errors. They are also the most preventable. Take a moment and recalculate your patient’s chemotherapy dose. If your answer does not match someone else’s answer, stop everything until the error is found.
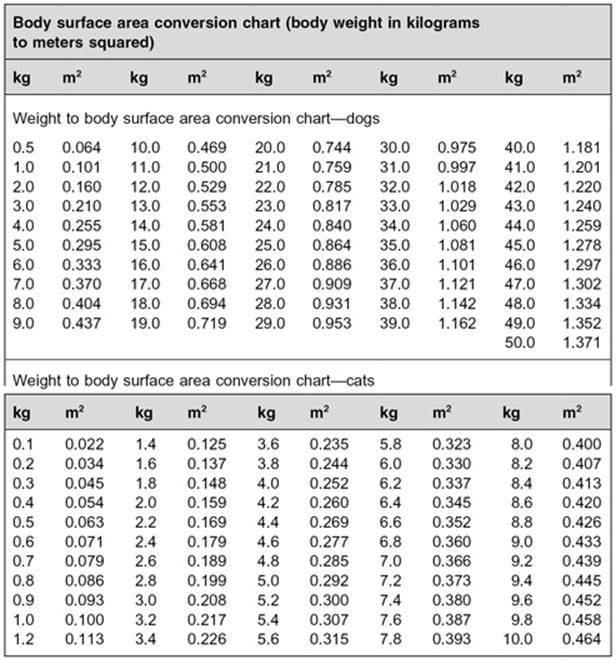
· Remember that most chemotherapy doses are calculated based on the patient’s body surface area, rather than its weight. Refer to the meter squared (m2) chart in Appendix 3.1 to convert pounds or kilograms to body surface area.
(5) Ask questions.
· Your knowledge and understanding are the two greatest assets you offer to your patients and to your veterinary practice. Still, we are likely to ask more questions when ordering a meal than we do during a busy day in the clinic. Asking questions may slow your efficient pace, but when you ask questions, you get answers that help you make better decisions. And better decisions mean better and safer quality of care for your patients. Use these quick tips to make it easier to A.S.K.
o Avoid beginning a question with the word “why.”
§ We all react defensively to questions that begin with “why.”
o Stay on topic.
§ Avoid vague open-ended questions. Make your questions specific and concise.
o Keep it simple.
§ Ask the question. Get the answer. Move on.
(6) Keep accurate records.
· The information in your patient’s record should be easy for everyone to understand and use. It must also be reliable, accurate, and consistent if the information that it supplies is to be relied on. Be clear. Be concise. Be accurate.
Body Surface Area
Body surface area is equivalent to the surface area of the skin. It is difficult to measure the surface area of the skin, so it is commonly estimated on the basis of formulas that use body weight as part of the equation. The most commonly used formula was published in 1916. The practice of using body surface area to calculate cytotoxic drug doses began in 1966 and has been handed down through generations of clinical oncologists. Why do we still use body surface area? Hippocrates instructed us to do no harm. It is extremely difficult to treat our patients using drugs that have such a narrow therapeutic index like anticancer drugs and still do no harm. Doses calculated on the basis of body surface area give us a greater sense of accuracy and safety. Use the chart in Appendix 3.1 to convert the body weight of dogs and cats from kilograms to their meter squared (m2) surface area. Remember that each kilogramequals 2.2 lb (lb ÷ 2.2 = kg).
Equipment and Supplies
Catheter Decision
We are all creatures of habit. Fortunately, committing some routine tasks to habit increases our efficiency. However, to protect the cancer patient receiving chemotherapy, more than any other patient you serve, it is important that you avoid reaching for the catheter you habitually use and take that extra moment to make a conscious decision to select the best catheter for the job.
Why is selecting the appropriate catheter so important to a patient receiving chemotherapy? Because many of the cytotoxic drugs used to treat cancer are vesicants. A vesicant is a substance that causes tissue blistering. Vesicants are highly reactive chemicals that combine with proteins, DNA, and other cellular components to result in destructive cellular changes. Vesicant drugs cause no damage to veins; however, when vesicant medications leak out of a vein and make contact with the surrounding tissue, the damage begins. The severity of the damage depends on the kind and the amount of drug that has leaked out of the vein. Tissue damage can range from mild skin irritation to gaping necrotic wounds, requiring multiple surgical repairs.
Catheters used in veterinary medicine for peripheral venipuncture come in two styles: butterfly catheters and over-the-needle catheters (Figure 3.1). Butterfly catheters have a steel needle attached to flexible plastic wings and a short piece of extension tubing. Butterfly catheters are usually not taped in place for longer-term infusions because the needle will lacerate the vein when the patient moves about. An over-the-needle catheter is used for longer infusions into peripheral veins. Unlike the butterfly catheter, after the needle of an over-the-needle catheter is inserted into a vein, the catheter is then slid over the needle into the vein and the needle is withdrawn.
Figure 3.1 Butterfly catheter (left) and over-the-needle catheter (right).
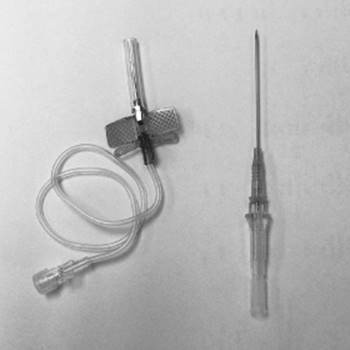
Although not all chemotherapy drugs are vesicants, there is wisdom in treating them all as though they were. The style of catheter you choose for chemotherapy administration is determined, in large part, by the volume of drug you intend to administer. For volumes less than 1 mL (cc), a butterfly catheter is appropriate. For a drug volume more than 1 mL (cc), a securely placed over-the-needle catheter will significantly reduce the risk of injury to the patient.
When selecting an over-the-needle catheter, it is easy to be lured into a false sense of confidence by selecting a smaller gauge catheter. Unfortunately, though it may seem easier to place a smaller gauge catheter into a vein, it is more difficult to keep one there. Smaller gauge catheters (22 gauge and smaller) come in very short lengths—usually less than an inch. Animal skin is very elastic, and as an animal patient moves, that elastic skin could pull a shorter catheter out of the vein, leaving it to lie alongside the vein, just beneath the skin. Infusing a vesicant drug through such a dislodged catheter is an invitation to injury. Remember, when it comes to over-the-needle catheters, length does matter.
Supplies for Chemotherapy Administration
The following are the supplies needed for chemotherapy administration:
· catheter setup (Figure 3.2)
o butterfly catheter (21 gauge or 23 gauge) or over-the-needle catheter (18 gauge or 20 gauge, 2 in)
o PhaSeal or Onguard injection adapter
o two syringes of normal saline
o 4 × 4 gauze sponges
o tape
o antiseptic cotton balls
o surgical prep
o gloves
· PPE
o see the section on “Personal Protective Equipment (PPE)” on page 26 for details
· an absorbent pad
o place a disposable plastic-backed absorbent liner under the connection site during chemotherapy administration.
· appropriate chemo-disposal bag
o see Chapter 4
· Chemo-spill kit
o Keep a clearly labeled chemo-spill kit near the site where chemotherapy drugs are mixed and where they are administered.
Figure 3.2 Over-the-needle catheter setup.

Prepare Your Workspace
Opportunities for accidents and errors are often related to the workspace layout and common distractions. These opportunities can be overcome with careful attention to your workspace design, your process design, and the development of SOPs for the administration of chemotherapy drugs in your practice. Listed below are some steps to take to prepare an appropriate workspace to administer chemotherapy:
· A busy treatment room is the least suitable place for a chemotherapy treatment. Administer chemotherapy in a room that is away from the flow of traffic and where it is easy to regulate personnel in and out of the room.
· Install an eyewash station where cytotoxic drugs are handled or administered.
o Affordable eyewash nozzles can be attached to most industrial faucets.
· Post signs to inform your colleagues that you are administering cytotoxic drugs.
· Restrict unnecessary personnel from the immediate vicinity where chemotherapy is being administered.
o Clients often wish to “help” or watch a chemotherapy treatment. For the safety of the client, the patient, and the staff, it should not be allowed.
· Protect your team and animal care staff from inadvertent exposure to chemotherapy drugs and metabolites excreted in the urine, stool, and blood, or into the beddings of cancer patients by labeling the patient’s cage.
o Instruct staff members to wear PPE when cleaning potentially contaminated cages.
Conclusions
The reality of chemotherapy for animal cancer patients is much different from that for human cancer patients. For animals receiving chemotherapy, quality of life for the patient is a primary concern. Doses of drugs and treatment schedules are calculated to minimize the discomfort to the patient while providing the most effective defense against the disease. Cytotoxic drugs can be lifesaving for patients with cancer, but they can also be dangerous to the staff members who handle and administer them. The risk of accidental exposure is greatest during drug preparation and administration, with the primary routes being inhalation, direct contact, and ingestion of improperly handled drugs. Two other routes of exposure important to a veterinary team and their clients include handling discarded items that have come in contact with chemotherapy (syringes, catheters, gloves, etc.) and contact with urine and feces from patients recently treated.
Each member of a veterinary healthcare team stands between what could happen to a patient and what does happen. It takes more time to prepare and follow clinical safety policies, and it can sometimes be inconvenient to slow down and recheck our work. The goal of veterinary oncology is to provide for the medical and nonmedical needs of the cancer patient and the client, and to improve the quality of life for both. Protecting the patient, client, hospital staff, and yourself from accidents and errors are quality steps toward that goal. Remember, none of us is medically bulletproof. Doing more things faster is no substitute for doing the right things.
Appendix 3.1 Body Surface Area Conversion Chart
Additional Reading
Aboumatar HJ, Winner L, Davis R, Peterson A, Hill R, Frank S, Almuete V, Leung TV, Trovitch P, Farmer D. 2010. Applying Lean Sigma solutions to mistake-proof the chemotherapy preparation process. Jt Comm J Qual Patient Saf 36(2):79–86.
Connor TH, Anderson RW, Sessink PJ, Spivey SM. 2002. Effectiveness of a closed-system device in containing surface contamination with cyclophosphamide and ifosfamide in an I.V. admixture area. Am J Health Syst Pharm59:68–72.
Du Bois D, Du Bois EF. 1916. A formula to estimate the approximate surface area if height and weight be known. Arch Intern Med 17:863–71.
Freireich EJ, Gehan EA, Rall DP, Schmidt LH, Skipper HE. 1966. Quantitative comparison of toxicity of anticancer agents in mouse, rat, hamster, dog, monkey, and man. Cancer Chemother Rep 50:219–31.
Kohn LT, Corrigan JM, Donaldson, MS. 2000. To Err Is Human: Building a Safer Health System. Washington, DC: The National Academy Press.
Labuhn K, Valanis B, Schoeny R, Loveday K, Vollmer WM. 1998. Nurses’ and pharmacists’ exposure to antineoplastic drugs: Findings from industrial hygiene scans and urine mutagenicity tests. Cancer Nursing 21(2):79–89.
McDiarmid M, Egan T. 1988. Acute occupational exposure to antineoplastic agents. J Occup Med 30(12):984–7.
NIOSH. 2004. NIOSH Alert: Preventing occupational exposure to antineoplastic and other hazardous drugs in healthcare settings. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health. [http://www.cdc. gov/niosh/docs/2004-165/].
Skov T, Lynge E, Maarup B, Olsen J, Rørth M, Winthereik H. 1990. Risk for physicians handling antineoplastic drugs. Lancet 336:1446.
Skov T, Maarup B, Olsen J, Rørth M, Winthereik H, Lynge E. 1992. Leukaemia and reproductive outcome among nurses handling antineoplastic drugs. Br J Ind Med 49:855–61.
Sotaniemi EA, Sutinen S, Arranto AJ, Sutinen S, Sotaniemi, KA. 1983. Liver damage in nurses handling cytotoxic agents. Acta Med Scand 214(3):181–9.
Valanis BG, Vollmer WM, Labuhn K, Glass A. 1997. Occupational exposure to antineoplastic agents and self-reported infertility among nurses and pharmacists. J Occup Environ Med 39:574–80.
Valanis BG, Vollmer WM, Steele P. 1999. Occupational exposure to antineoplastic agents: Self-reported miscarriages and stillbirths among nurses and pharmacists. J Occup Environ Med 41:632–8.
Vandenbroucke J, Robays H. 2001. How to protect environment and employees against cytotoxic agents, the UZ Ghent experience. J Oncol Pharm Pract 6(4):146–52.
Wick C, Slawson MH, Jorgenson JA, Tyler LS. 2003. Using a closed-system protective device to reduce personnel to antineoplastic agents. Am J Health Syst Pharm 60:2314–20.