Kenneth Crump and Douglas H. Thamm
Key points
· Use a consistent, organized system for obtaining a patient history to ensure nothing is overlooked.
· Ask open-ended questions that are nonjudgmental.
· The veterinary medical record is a legal document and should be written with utmost care and precision.
· Prior to administering chemotherapy, ensure that the patient shows no significant changes since the last recheck.
· The temperature, pulse, and respiration (TPR) is the foundation of a good physical examination.
· Rectal temperature measurement is optimal.
· Heart rate and pulse rate may share the same numeric value, but they are not the same piece of information.
· Animals displaying normal respiratory effort appear comfortable and lack any abdominal effort.
· Never estimate a cancer patient’s weight.
· Calipers are critical to accurately measure tumor size.
· Most commonly, the longest dimension of a tumor is measured.
· A complete blood count (CBC) is performed immediately prior to each chemotherapy treatment.
· White blood cells called neutrophils are most likely impacted by chemotherapy.
· Most chemotherapy drugs do not affect platelets.
· Anemia is rarely a clinical problem in dogs and cats receiving chemotherapy.
· Serum biochemistry profiles and urinalyses are performed before starting chemotherapy on a new patient.
· Additional imaging tests (e.g., radiographs, ultrasound) may be used to determine how well a treatment is working.
· Imaging is not performed at every visit but may be assessed periodically.
· Response to therapy is assessed by comparing tumor measurements over time.
· Complete response (CR) is the disappearance of all evidence of cancer.
· Partial response (PR) is significant tumor shrinkage, but not CR.
· Stable disease (SD) means the disease has not improved, nor has it worsened.
· Progressive disease (PD) means the disease has gotten “significantly” worse.
Introduction
The veterinary technician who can obtain a complete and accurate patient history and can perform a quality physical examination plays a critical role in a busy veterinary practice. As you become more proficient at gathering important information about a cancer patient’s history and current physical status, you free your veterinarians to complete other necessary work. The time it takes to do these tasks well increases the efficiency of the entire team. However, inaccurate or incomplete information can be worse than no information at all. Faulty information regarding a patient’s history or physical parameters can lead to unnecessary tests, useless treatments, and the loss of trust by your clients and your veterinarians.
Patient History
Despite its importance, obtaining a thorough history is often overlooked by veterinarians as well as veterinary technicians. Obtaining a thorough patient history in a clear and organized manner can sometimes be challenging. For example, there are owners who either talk too little or talk incessantly about unrelated issues. The process can be time-consuming, and sometimes even the most efficient people feel as if they are running behind schedule. Remember though, one of the biggest enemies of good time management is poor planning. The more rushed you feel, the less thorough you will be. The more frantic you are, the less accurate you will be. Using a consistent, organized system for obtaining a patient history is important to ensure that nothing is overlooked. The goal of this section is to describe an organized approach for obtaining a complete and accurate patient history. Although this is presented for the cancer patient and addresses specifically tailored cancer-related questions, this method can serve as a foundation upon which more general questions can be added.
The Introduction
The first step in obtaining a medical history is to introduce yourself to the client and to explain what you are doing. Mentioning your name, even to a client you have seen many times before, relieves the client of the responsibility of remembering your name from one visit to the next. This can be particularly important in a larger practice, where clients may see one of several different team members on any given visit.
Always be certain to have reviewed the patient’s record and that you know the client’s name, and the pet’s name and sex before you begin your interview, to prevent awkward mistakes when referring to the client or the pet. In situations where the pet has been taken away from the client before obtaining a history (e.g., taken to the treatment area during an emergency), it is essential to reassure the owner about the pet’s status before beginning the interview. If the client is worried that his or her pet is in danger, he or she may not be able to focus on your questions nor provide you with the information you need.
Asking Questions
The most important aspect of acquiring a history is to recognize the pet owner’s level of understanding and to respect it. The majority of owners do not understand medical jargon. Many can become confused by the acronyms and medical terminologies you use daily; so you must carefully strike a language balance that is appropriate for each client, one that neither confuses them nor insults their intelligence. For instance, while the term PU/PD may have meaning to you, it is likely to be unfamiliar to a client, yet asking if their pet “makes tinkle a lot” may seem an offensively juvenile way to speak to an adult.
It is also important to ask open-ended questions rather than leading questions. An open-ended question is one that requires the client to fill in the information themselves. A leading question is one that can usually be answered with a “yes” or “no” and seems to guide the client to an appropriate answer. For example, if you are trying to determine the activity level of a patient since its last chemotherapy treatment, it is better to ask the client to “Describe any changes in Fluffy’s activity level since your last visit,” rather than asking “Has Fluffy been acting more tired and lethargic since your last visit?” When leading questions are asked, clients sense which response the interviewer prefers, and they are likely to give it. Pet owners are anxious to help resolve their animal’s problems. Although you are trying to gather accurate information about their pet, they may feel it helpful to try to guess the right answers to your questions.
Another pitfall in interviewing clients is asking questions that seem judgmental of their care or their management of their pet’s disease. Questions that suggest a judgment can cause them to feel uncomfortable about giving truthful answers. For instance, when questioning an owner about their pet’s continued vomiting and diarrhea, it would not be helpful to ask, “You didn’t forget to give Fluffy her medicine, did you?” Faced with that question, an owner is very likely to respond, “No, of course not,” even if the medication had been forgotten. It would be better to ask, “How often do you give Fluffy her medicine?” or “What times of day does Fluffy receive her medication?” Allowing clients to feel comfortable with their answers will improve the chances that you receive accurate information.
The key to history taking is to obtain accurate information by asking enough of the right questions. In asking questions, be aware of your own assumptions. For instance, an owner may tell you that their dog does not have diarrhea, when in fact they do not normally observe their dog defecating. At times, it may be better to ask more than one question: “Do you observe your dog when it defecates?” and if so, “Does your dog have diarrhea?”
In a classic scene from a 1960s Pink Panther movie, the bumbling Inspector Clouseau notices a small dog in the lobby of a hotel. He asks the clerk, “Does your dog bite?” The clerk responds, “No.” However, when Clouseau reaches to pet the dog, the little dog tears into his hand. Astonished, Clouseau says, “I thought you said your dog does not bite!” The clerk looks up from what he is reading and says, “That’s not my dog.”
The Information
Medical information is useless unless it is written carefully, neatly, and accurately in a structured medical record form. A standardized history form allows efficient recording of the information gathered from your interview. Additionally, forms that prompt you remind you to obtain key pieces of information. Record the information in real time and directly into the medical record to prevent any subsequent misunderstandings. Write legibly, in an organized manner, using appropriate medical terminology. Keep in mind that although veterinary medical records are not subject to the federal and state regulations that are seen in the human medical field, the veterinary medical record is still a legal document, and, as such, should be written with utmost care and precision. The medical history provides a reference for the veterinary healthcare team as it implements and revises its treatment plans for the patient. The history form used at the pet’s initial presentation differs from a recheck history form. Upon initial presentation, you gather more extensive background information about the pet’s overall health, diet, behaviors, and living conditions. It also includes any pertinent medical history, such as vaccinations, allergies, and previous surgeries. A recheck history form is more focused and generally gathers information from one appointment to the next. Whatever intake history form you currently use in your practice will suffice at initial presentation of a cancer patient. An example of a useful patient history form for recheck appointments of cancer patients can be found in Appendix 4.1.
The following provides a general list of important information to obtain at each visit from a chemotherapy patient. After you introduce yourself, it is useful to begin with a broad, open-ended question that allows the client to voice any general concerns they have. For instance, “How have things been going since the last treatment?”
Once you have noted their response, go more specifically through the patient’s behavior. Ask questions about:
· appetite
· attitude
· activity level
· any nausea/vomiting/diarrhea
· anything else
o breathing problems
o lameness
o changes to injection site of previous treatments
o other pertinent information.
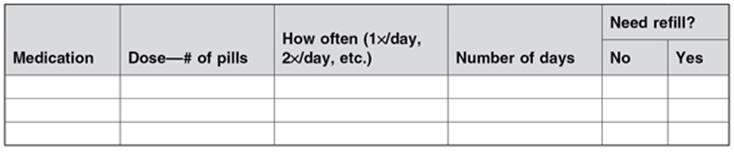
These questions can then be followed by questions about medications:
· What medications is the pet currently taking?
· Do they need any refills?
Finally, confirm with the client what will happen at this visit:
· tests that will be performed,
· drugs that will be administered,
· how long it is all likely to take, and
· discuss the owner’s plan for pickup.
o Will they stop back? At what time?
o Do they expect a call when the treatment is complete?
Before ending the patient history interview, be sure to ask the client if there are any questions or concerns they would like to discuss with the doctor at this visit. If the client has concerns to be discussed, explain to the client whether those concerns will be discussed before or after the treatment.
Physical Examination
Prior to administering chemotherapy, it is critical to ensure that the patient’s overall health is good and that there have been no significant changes since the last recheck. Although a thorough physical examination is always performed by a veterinarian, some of the most critical pieces of the physical examination are often performed by the technical staff, and it is important that abnormalities be pointed out to the veterinarian prior to chemotherapy administration.
Temperature, Pulse, and Respiration (TPR)
The TPR is the foundation of a good physical examination. These values provide a quick reference to a substantial amount of information about the patient. Different parts of the TPR may be altered in a chemotherapy patient, depending on the drugs they received and when, as well as their underlying disease. See Table 4.1 for the normal TPR values for the dog and cat.
Table 4.1 Normal TPR values for the dog and cat
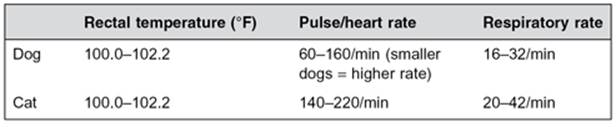
Temperature
Rectal temperature measurement is optimal; however, an axillary (armpit) or aural (ear) temperature may be used in patients with swelling or pain in the rectum or surrounding anatomy. These sites are less accurate than a rectal measurement and should only be used when absolutely necessary.
Neutropenia (a low white blood cell count) can sometimes be observed following chemotherapy administration (see below). If the neutrophil count falls too low (typically at 1 week following treatment), the patient becomes at increased risk for infection and may run a fever. Although some dogs present with elevated temperatures as a result of stress or excitement, a temperature above 103°F might suggest an infection. Some dogs with very serious infections can have a normal or low body temperature, so the absence of a fever does not completely rule out infection. See Chapter 7 for additional information about side effects.
Pulse Rate and Heart Rate
In a normal healthy animal, the pulse rate and heart rate are the same number. Although they may share the same numeric value, they are not the same piece of information. Much can be determined with a stethoscope in the ears of a highly trained medical professional, but a patient’s pulse rate and subjective pulse quality are not among them. Those values are best determined with your fingers.
Palpate the peripheral pulses on every patient to determine the pulse rate and pulse quality. The femoral arteries are generally palpated for this and are located high on the medial thigh of dogs and cats. Finding and using the femoral arteries to determine a patient’s pulse rate and quality is a learned skill, and requires practice to gain proficiency. Practice on every patient you see (Figure 4.1). Apply pressure over the femoral arteries using your fingertips. Some degree of pressure is required to feel the pulse; however, excessive pressure could compress the artery, occluding the blood flow. Count the number of pulses you feel for 15 seconds and then multiply that number by 4 in order to calculate the pulse rate per minute.
Figure 4.1 Obtaining a femoral pulse. Apply light pressure over the femoral arteries using your fingertips.

It is also important to auscultate (listen to) the heart while palpating pulses (Figure 4.2). It may be difficult to coordinate holding a stethoscope over the heart of a dog or cat while trying to palpate its pulses at the same time (especially if the pet loses interest), so you may want to take and record the pet’s pulse before you try this. The heart rate and the pulse rate should be identical, and there should be a pulse of near equal quality produced by every heartbeat. The absence of a palpable pulse (or significant change in pulse quality) with an audible heartbeat is called a pulse deficit. Pulse deficits usually indicate a cardiac abnormality and should be brought to the attention of a veterinarian.
Figure 4.2 Palpating the pulse and auscultating the heart simultaneously. It is important to auscultate the heart while palpating the pulses. There should be a detectable pulse for each heartbeat.

Tachycardia (high heart rate) can be a sign of anemia, excitement, pain/discomfort, or other illness. An irregular heart rate can be a sign of disturbed electrical activity in the heart. Certain drugs, such as doxorubicin, should not be given to dogs with some kinds of heart disease, and thus, additional tests might be necessary to further investigate an abnormal heart rhythm prior to chemotherapy.
Respiratory Rate/Effort
Respiratory rate and effort should be noted in all patients. Rate is generally done visually first, and then by auscultation to actually hear the lung sounds. The determination of respiratory effort is more subjective. Animals displaying normal effort appear comfortable and lack any abdominal effort.
Depending on the type of tumor a pet has, an increase in respiratory rate or effort could be a sign of tumor spread to the lungs. This could indicate additional tests (e.g., X-rays of the chest), or a change in treatment might be necessary. An abnormal respiratory rate or effort should be brought to the attention of the veterinarian.
Weight
A cancer patient’s weight must never be estimated, and must be measured and recorded at every visit. An accurate body weight is critical for accurate chemotherapy dosing. A small inaccuracy in weight measurement can result in a higher risk of toxicity or reduced effectiveness of treatment. For clarity, it is a good idea to measure a cancer patient’s weight in both pounds and kilograms, and to clearly label both in the patient’s record. Most American veterinary practices are accustomed to weighing patients in pounds; however, many cancer-related medications are dosed using weight measured in kilograms. Remember also that most chemotherapy doses are calculated based on the patient’s body surface area, rather than its weight. Refer to the meter squared (m2) chart in Chapter 2 to convert weight in kilograms to body surface area.
How has the weight changed since the last visit? Weight loss might indicate poor appetite and decreased food intake, and changes in nutrition might be indicated. If weight is very different from the previous visit, this could indicate an inaccuracy in weighing, and the patient should be weighed again.
Tumor Measurements
Although often performed by a veterinarian, sometimes tumor measurements are performed by the technical staff as well. This is the main way to tell whether treatments are working or not. What is expected will depend on the tumor type you are treating. Sometimes, complete disappearance of all measurable disease is expected. For other tumor types, partial shrinkage or absence of any growth is a very acceptable outcome. Investment in calipers (Figure 4.3) is critical for accurate assessment of tumor size. These can be purchased at most hardware stores, as well as from various veterinary/surgical supply vendors.
Figure 4.3 Different styles of calipers. Calipers can be purchased at most hardware stores, as well as from veterinary or surgical supply vendors.

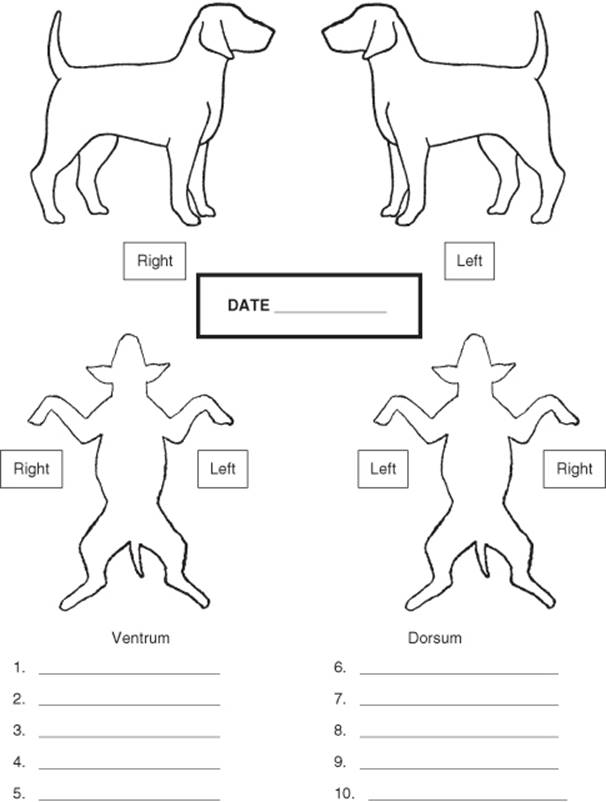
Most commonly, the longest dimension of a tumor is measured (e.g., if the tumor is longer than it is wide or deep, then the length is recorded). Sometimes, tumors are measured in two or three dimensions. It is helpful to have a separate sheet that keeps track of tumor measurements over time to make comparisons easier. In animals with multiple masses, it can be helpful to keep track of mass locations and sizes on a body map: An example of such a map is included in Appendix 4.2.
Laboratory Tests
While blood tests are an important part of the management of the chemotherapy patient, they are rarely used in animals to determine if the treatment is working: This is usually determined with tumor measurements. However, blood tests are critical to establish that chemotherapy is safe to administer. Blood from patients undergoing chemotherapy is almost always drawn from the jugular vein, rather than from a peripheral vein. This preserves the peripheral veins for chemotherapy administration and reduces the likelihood of chemotherapy being extravasated from a prior venipuncture site.
Complete Blood Count (CBC)
A CBC is almost always performed immediately before each and every chemotherapy treatment, and sometimes in between treatments as well. While it is optimal to have a CBC performed in-house on the same day as the chemotherapy, it is acceptable to have a CBC performed the day before (not earlier) if the test needs to be sent out to a referral laboratory. If a CBC is performed any earlier than the day before treatment, the results may not be reliable as values may have changed enough to impact treatment decisions.
White Blood Cells
Of all the cells that are evaluated on a CBC, the one most likely to be impacted by chemotherapy is a subset of the white blood cells called neutrophils. Neutrophils are the body’s first line of defense against bacteria, and a decreased number of neutrophils increase the patient’s risk of bacterial infection (see Chapter 7 for more information). It is very important that treatment decisions be based on the absolute neutrophil count rather than on the total white blood cell count or the percentage of neutrophils. Most drugs can be administered safely if the patient has at least 2000–2500 neutrophils/µL. Dogs with fewer neutrophils may need to have their treatment delayed for a few days. If the neutrophil count is low but greater than 1000/µL, the risk of infection is small. However, if the neutrophil count is less than 1000/µL, the risk of infection is higher, and careful monitoring at home, as well as oral antibiotics, is typically recommended until the neutrophil count recovers.
It is important to let owners know that if the neutrophil count is low, it typically recovers quickly. Also, inform owners that delaying a treatment for a few days until the neutrophil count is acceptable for chemotherapy is not likely to decrease the effectiveness of treatment.
Platelets
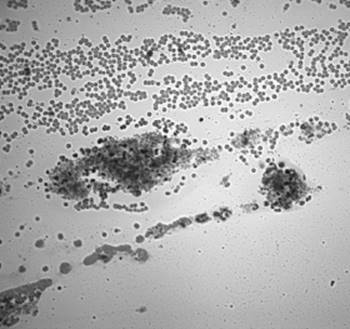
While there are a few cancer drugs that can cause a decrease in the number of platelets (usually with long-term use), most do not. Thus, severely low platelets are not often encountered in animals receiving chemotherapy. However, a treatment delay and additional tests may be required in animals with less than 50–75,000 platelets/µL. For this reason, it is important that a manual platelet count, not just a platelet estimate, be obtained. One of the most common reasons for a platelet count to be reported as decreased is due to platelet clumping (Figure 4.4). Platelet clumping can be assessed as the cause for a low platelet count by scanning the blood smear, looking for clumps. The risk of clumping can be reduced if the blood sample is obtained via a clean jugular stick with a relatively large-gauge needle.
Figure 4.4 Platelet clumps on the feathered edge of a blood smear. Numerous or large platelet clumps can artificially lower the platelet count.
Red Blood Cells
Unlike in human cancer patients, anemia is rarely a clinical problem in dogs and cats receiving chemotherapy. Mild, cumulative anemia can be observed, but it is extremely rare for it to be severe enough to require intervention. If a large or sudden drop in red blood cells is noted, it could indicate a different serious problem that requires attention (internal bleeding, ulcer, etc.).
Biochemistry and Urinalysis
Serum biochemistry profiles and urinalyses are almost always performed before starting chemotherapy on a new patient, to ensure that organ function is adequate to tolerate chemotherapy and to rule out any other serious medical problems that might be just as important to treat as the cancer is. Occasionally, biochemistry profiles or individual tests may be performed throughout treatment, depending on the disease and the chemotherapy being received.
Calcium
In dogs that present with a high blood calcium (also called paraneoplastic hypercalcemia or hypercalcemia of malignancy), periodic rechecks of calcium can indicate how well the cancer treatment is working. Calcium will usually return to normal in patients whose disease is removed surgically, or those in which complete remission is induced with chemotherapy. Conversely, a rise in blood calcium levels may indicate a relapse of the patient’s disease.
Liver Values
Some chemotherapy drugs, specifically lomustine, can cause elevations in liver values with chronic use. Thus, in addition to a CBC, liver values (especially alanine aminotransferase [ALT]) are usually checked before each treatment in dogs and cats receiving lomustine.
Kidney Values/Urine Specific Gravity
Some drugs, specifically cisplatin in dogs and doxorubicin in cats, as well as nonsteroidal anti-inflammatory drugs like piroxicam, are capable of causing kidney toxicity. For this reason, kidney values (blood urea nitrogen and creatinine), as well as urine specific gravity, are usually checked before administration of these agents. Sterile urine is not required for urine specific gravity and can be performed on a free-catch sample.
Imaging
In some cases, additional imaging tests (e.g., radiographs, ultrasound) may be used to determine how well the treatment is working. Imaging is usually not performed at every visit due to cost considerations but may be assessed periodically.
If the only measurable disease happens to be inside a body cavity, sometimes repeated imaging to evaluate the size and number of lesions is the only way to know whether a treatment is effective or not. When being used to assess response, imaging is often repeated after two treatments with a given drug (approximately 6 weeks, for most drugs), and then at approximately the same intervals thereafter. Sometimes imaging is performed to ensure that the disease has not spread to another part of the body, especially with tumors at high risk for spread following surgery. Examples of tumors that fall into this category include melanoma, hemangiosarcoma, osteosarcoma, anal sac carcinoma, and mammary gland carcinoma. In these situations, imaging may be repeated every 2–3 months after surgery to make sure that the disease remains under control.
Radiographs (X-Rays)
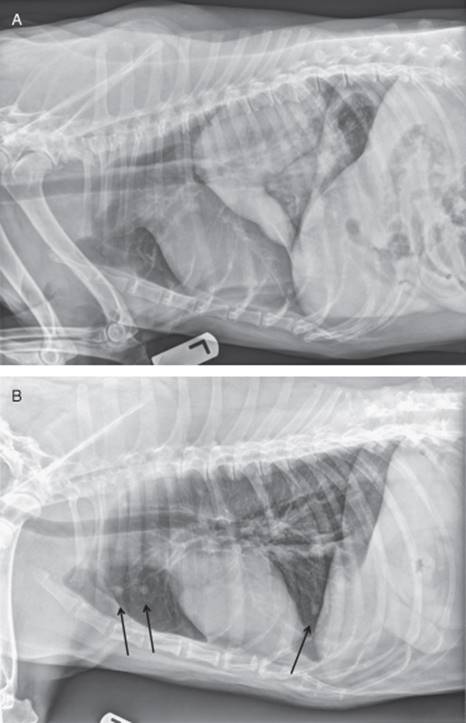
Radiographs are commonly used to assess changes in the lungs and the surrounding structures in cancer patients (Figure 4.5). Most of the time, tumors in the lungs are easy to measure with calipers, much in the same way as tumors on the outside of the body can be measured. Radiographs can also be used to assess changes in bones. Radiographs are less sensitive for looking at or measuring disease in the abdomen.
Figure 4.5 (A) Thoracic radiograph from a 10-year-old male castrated springer spaniel with a primary lung tumor. Changes in size of this tumor can be measured serially to assess response to therapy. (B) Thoracic radiograph from a 7-year- old spayed female Labrador retriever with lung metastases from a bone tumor (osteosarcoma). Arrows indicate pulmonary nodules suggesting metastasis. These metastases developed 10 months after amputation, and chemotherapy was performed.
Ultrasound
Ultrasound is an excellent test for evaluating and measuring tumors in the abdomen (Figure 4.6). It is commonly used to look at tumors in organs like the bladder, liver, spleen, and abdominal lymph nodes. Most ultrasound machines have measurement devices built into them so that abnormal structures can be measured digitally.
Figure 4.6 (A) A dog in dorsal recumbency undergoing an ultrasound examination of the abdomen. (B) A splenic mass in an 8-year-old male castrated golden retriever. Measurements can be obtained digitally on the images collected. (C) A bladder mass in an 11-year-old female spayed Scottish terrier. Changes in the size of this mass can be assessed over time as an indication of how well treatment is working.

Computed Tomography (CT) and Magnetic Resonance Imaging (MRI)
Advanced imaging tests such as CT and MRI can be very useful for the initial diagnosis and treatment planning for certain tumors, such as those of the nasal cavity and brain. CT and MRI are rarely used for the serial assessment of tumor response due to their high expense and the need for general anesthesia or heavy sedation.
Assessment of Tumor Response
Although it is primarily the job of the veterinarian to determine how well the treatment is working, it sometimes falls to the staff to interpret for the client what the veterinarian means by terms such as “partial response” or “stable disease.” An understanding of how treatment response is assessed can help owners interpret how the treatment is working.
In general, responses to therapy are assessed by comparing the tumor measurements you or the veterinarians make over time. This can be done by comparing either the maximum tumor diameters or the tumor volumes, calculated by multiplying measurements in two or three different dimensions.
Complete Response (CR)
CR means the complete disappearance of all evidence of cancer: Obviously, this is the “Holy Grail” for cancer treatment. In addition to all the measurable disease going away, all clinical signs associated with disease are expected to resolve as well. While this is great news for any client, it is important for owners to know that this does not necessarily mean “cure.” There are some cancers, such as lymphoma, in which we can induce CR in 75–90% of patients; however, in all but 5% of the cases, the disease eventually comes back.
Cure is hard to define in veterinary oncology. For many types of cancer in humans, “cure” means being disease free for longer than 5 or 10 years. Our patients are typically older at the time of diagnosis and would usually have other age-related problems before reaching the 5- or 10-year mark. So, for our patients, cure may mean that the cancer stays away long enough for the patient to die of an unrelated problem.
Partial Response (PR)
PR means that we see “significant” tumor shrinkage but not complete disappearance of all disease. Technically, this term means that all measurable disease decreases by more than 50% in volume or more than 30% in maximum diameter and without the development of any new lesions. This is the next best thing to seeing a CR.
Stable Disease (SD)
SD means that the disease has not improved significantly but also has not worsened. In other words, tumors have shrunk by less than 50% in volume or less than 30% in maximum diameter, but have grown by less than 25% in volume or less than 20% in maximum diameter, and no new lesions have appeared. As mentioned above, we certainly strive for tumor shrinkage or even complete tumor disappearance, but there are many types of cancer for which “not growing” is a very acceptable outcome. If we can give a treatment that is well tolerated and preserves an excellent quality of life, and if we can make tumors stop growing, then that can be a very good outcome for the pet and the client, and a very rewarding outcome for the veterinary team.
Progressive Disease (PD)
PD means that the disease has gotten “significantly” worse. Technically, this means that all measurable disease has increased by more than 25% in volume or more than 20% in maximum diameter, or that new lesions that have not been previously seen, have appeared. In most cases, this is an indication to either discontinue the treatment or try something different, depending on the alternatives, the quality of life of the patient, and the owner’s interest in continuing treatment.
Additional Reading
Bassert JM, McCurnin DM. 2009. McCurnin’s Clinical Textbook for Veterinary Technicians (7th Ed.). Philadelphia: Saunders.
Ogilvie GS, Moore AS. 2001. Feline Oncology. Yardley, PA: Veterinary Learning Systems.
Ogilvie GS, Moore AS. 2006. Managing the Canine Cancer Patient: A Practical Guide to Compassionate Care. Yardley, PA: Veterinary Learning Systems.
Withrow SJ, Vail DM. 2007. Withrow and MacEwen’s Small Animal Clinical Oncology (4th Ed.). Philadelphia: Saunders.
Appendix 4.1 Oncology Patient Recheck History Form
PLEASE ANSWER ALL QUESTIONS
|
Date: _____________ |
Patient: _________________________ |
When will you return to pick up your pet?
12–1 PM ![]() 1–3 PM
1–3 PM ![]() 3–5 PM
3–5 PM ![]() 5–8 PM
5–8 PM ![]() 8–10 PM
8–10 PM ![]()
Telephone # where you can be reached ( ) ![]() Work
Work ![]() Home
Home ![]() Cell
Cell
Which best describes your pet’s health since last visit?
Excellent ![]() Good
Good ![]() Fair
Fair ![]() Poor
Poor ![]()
Please describe each item according to your dog’s behavior since the last appointment.
|
Appetite |
Comparison of appetite compared to the last appointment. |
|
|
|
|
Sleeping |
Amount of time that your dog spends sleeping, compared to the last appointment. |
|
|
|
|
Activity |
Current activity level compared to the last appointment. |
|
|
|
|
Playfulness |
Playfulness compared to the last appointment. |
|
|
|
|
Accidents |
Number of urinary or fecal accidents in the house compared to the last appointment. |
|
|
|
|
Panting |
Amount of panting compared to the last appointment. |
|
|
|
|
Response |
General responsiveness compared to the last appointment. |
|
|
|
|
Health |
General health compared to the last appointment. |
|
|
|
|
Overall |
General health compared to before your dog’s diagnosis of cancer. |
|
|
Describe any concerns you have about your pet since last visit (i.e., loss of appetite, vomiting, diarrhea, cough).
When did these problems occur? Have the problems resolved?
______________________________________________________________________________
______________________________________________________________________________
What questions or concerns you would like to discuss with your pet’s doctor?
______________________________________________________________________________
______________________________________________________________________________
What medications have you given since your pet’s last visit?
Appendix 4.2 Oncology Body Map