Jennifer K. Sun,
Joan W. Miller,
Lloyd P. Aiello
INTRODUCTION AND DEFINITION
With the introduction of insulin in the 1930s, diabetes mellitus rapidly ceased to be a fatal disease of young people, with coma as a cause of death falling from 60-4%.[1] The medical care of diabetic patients instead shifted to the management of vascular complications, including cardiac disease, renal failure, and diabetic retinopathy. In the 1970s, it was well demonstrated that laser photocoagulation could substantially reduce visual loss and blindness from diabetic retinopathy.[2,3] Advances in vitreoretinal surgery have made a further impact on severe proliferative diabetic retinopathy (PDR). Even so, diabetic eye disease remains a severe medical and social problem afflicting individuals during their productive years. The prevalence of diabetes and its associated micro and macrovascular complications is steadily increasing. Currently, at least 177 million people suffer from diabetes worldwide. It is estimated that by the year 2030, this number will increase to approximately 370 million individuals.[3a] Diabetic retinopathy is responsible for at least 12% of the new cases of blindness each year in the United States.[4] In the United States alone approximately 700 000 persons have PDR. The health care costs of retinopathy-associated disorders exceeds $620 million in the US each year.[4a]
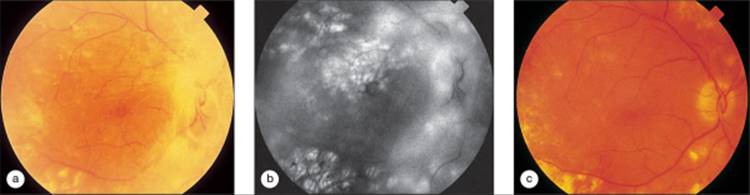
PDR is characterized by new vessels arising from the surface of the retina. New vessels may grow from the vessels on the surface of the optic disk (neovascularization at the disk (NVD)). They may also originate from the retinal vascular arcades elsewhere (neovascularization elsewhere in the retina (NVE)) and grow along the partially detached posterior hyaloid, also termed the 'posterior vitreous face' (Fig. 135.1). Fibroblasts and glial elements accompany the new vessels, and proliferation of this fibroglial tissue can become the predominant feature of the retinopathy. PDR also includes rubeosis iridis or new vessels on the surface of the iris or in the anterior chamber angle.
|
|
|
|
FIGURE 135.1 Proliferative diabetic retinopathy (PDR). (a) Neovascularization at the disk (NVD) a fan-shaped configuration of new vessels branching out from the optic nerve head. Additional findings include extensive vascular caliber changes, intraretinal hemorrhages and microaneurysms and cotton wool spots. (b), Neovascularization elsewhere in the retina (NVE) new vessels along the superotemporal arcade with associated preretinal hemorrhage. |
PATHOGENESIS
Early functional changes have been observed in diabetes, including alterations in retinal blood flow[4b] and a breakdown in the blood-retinal barrier, which is demonstrated by increased leakage from retinal blood vessels measured by vitreous fluorophotometry.[5-7] Recent evidence suggests that angiogenic factors may play a role in these early changes as well.[8,9] Morphologic changes in nonproliferative diabetic eye disease include microaneurysms, blot and dot hemorrhages, cotton-wool spots, venous caliber abnormalities, intraretinal microvascular abnormalities (IRMAs), hard exudates, and macular edema. Microaneurysms appear in clusters and surround areas of capillary closure. IRMAs are also found adjacent to areas of capillary closure. Controversy has existed as to whether IRMAs represented dilated and abnormal retinal capillaries or early intraretinal neovascularization.[6] However, recent evidence has demonstrated the continuity of intraretinal microvascular changes and preretinal neovascularization.[10] In a retrospective study of serial photographs of NVE, Chang and associates found that NVE originated at the same location as an earlier IRMA in 40 of 57 locations (70.2%), and the average time span between the appearance of IRMA and that of NVE was 3 years.[11]
As more advanced retinopathy develops, retinal neovascularization occurs. NVE develops from retinal vessels and tends to appear adjacent to regions of nonperfusion. NVD originates from vessels on the disk and appears coincident with significant areas of nonperfusion in the midperiphery. The exact pathogenesis of retinal neovascularization remains to be elucidated. Retinal neovascularization is not a response limited to diabetes but is probably a programmed response to retinal ischemia. In 1948, Michaelson hypothesized that a diffusible factor was released from ischemic retina that stimulated the development of embryonic vasculature.12 Ashton proposed that oxygen deprivation stimulated the production of an angiogenic factor in both development and retinopathy of prematurity.[13] Wise expanded the idea of an angiogenic factor to explain a number of adult retinopathies, including diabetic retinopathy, and the clinical correlation of retinal ischemia and retinal neovascularization has been well established.[2,14-16] These angiogenic factors are released from ischemic retina and stimulate new vessel growth from susceptible vessels both locally and at distant locations in the eye (Fig. 135.2).
|
|
|
|
FIGURE 135.2 Severe retinal ischemia with rubeosis. (a) The right eye of a 27-year old diabetic man who presented with rubeosis and neovascular glaucoma in each eye. There is NVD, and visual acuity is 20/200. (b) View of the inferotemporal arcade with numerous intraretinal hemorrhages and subtle intraretinal whitening. (c) Fluorescein angiogram documents severe capillary nonperfusion of the entire temporal macula and beyond. There is also hyperfluorescence indicating NVD. (d) Inferior view shows nearly complete absence of capillary perfusion outside the peripapillary area. |
Angiogenic factors have been isolated from ocular and other tissues and studied in clinical specimens and experimental models of neovascularization. Whereas the number of known angiogenic factors continues to increase, growth factors and signaling molecules that appear to have particular relevance to diabetic retinopathy include basic fibroblast growth factor (bFGF), insulin-like growth factor (IGF), vascular endothelial growth factor (VEGF), and the beta isoform of protein kinase c (PKC).
bFGF is the best characterized of the fibroblast growth factors (FGFs) and the one-most strongly implicated in the angiogenic process. bFGF stimulates endothelial cell proliferation and migration, induces protease production by endothelial cells, and stimulates endothelial cells to migrate into 3-dimensional collagen matrices to form capillary-like tubes.[17-19] bFGF stimulates angiogenesis in vivo in the chick chorioallantoic membrane and corneal micropocket, in concentrations as low as 100 ng.[20-22] bFGF has been isolated from corpus luteum, adrenal gland, kidney, and retina, and it has been implicated in tumor-mediated angiogenesis.[17,23]
When considering the FGFs as ocular angiogenic factors, one perplexing attribute of both acidic fibroblast growth factor (aFGF) and bFGF is their lack of a consensus signal peptide for secretion.[24] As a result, demonstration of aFGF[25,26] and bFGF[27] in the retina does not necessarily mean that the factors are exerting any action at that moment. bFGF related messenger RNA (mRNA) and protein levels have been reported to be elevated in a number of experimental systems and clinical settings, including the retinas of newborn mice exposed to hyperoxia,[28] the retinal pigment epithelium (RPE) after krypton laser injury,[29] and ocular fluids from individuals with PDR.[30] However, FGF has not been shown to have a causal role. The FGFs have a high affinity for heparin and heparin sulfate, and a significant proportion remains associated with the cell matrix.[31] This has led to the concept of matrix-associated FGF as a stored growth factor. Intracellular FGF may be secreted via alternate pathways, possibly in response to sublethal injury.[32]
The IGFs (IGF-I and IGF-II) are growth-promoting peptides with multiple biologic effects.[33] IGF-I was initially identified as a circulating factor that appeared to mediate the effects of growth hormone.[34] The role of this growth factor and its associated factors in ocular neovascularization was first suggested by the clinical observation of regression of PDR after infarction of the pituitary during pregnancy.[35] IGF-I stimulates migration and proliferation of endothelial cells[36] and has been demonstrated to be angiogenic in vivo at high doses.[37] Grant and colleagues demonstrated increased levels of IGF-I in the vitreous of patients with PDR compared with controls.[38]
VEGF was first identified in tumor and developmental systems as a vasopermeability factor and angiogenesis factor, which was upregulated by hypoxia, a component of ischemia.[39] VEGF and mRNA and protein were shown to be elevated in several experimental systems, including a model of retinal ischemia and iris neovascularization in the monkey and retinopathy of prematurity in the mouse and the rat.[40-43] Various strategies to inhibit VEGF either completely prevented or greatly reduced neovascularization in these models.[44,45] VEGF protein levels were found to be increased in the ocular fluids of patients with PDR or ischemic retinal vein occlusion and decreased after successful laser retinal ablation.[46,47] Surgical specimens from eyes with PDR consistently demonstrated VEGF expression, in contrast to other growth factors.[48] Finally, VEGF has been demonstrated to be sufficient to produce neovascularization, by injecting VEGF into normal animal eyes[49] or by means of a transgenic mouse model.[50]
Recent work has further suggested that the serine/threonine kinase PKC also appears to play a role in the development of diabetes-associated neovascularization, primarily through its influence on the activity of growth factors such as VEGF.[50a] In human vascular smooth muscle cells, hyperglycemia-induced expression of VEGF is prevented by administration of PKC inhibitors.[50b] Inhibition of PKC? by the selective inhibitor ruboxistaurin blocks VEGF's proliferative, angiogenic, and pro-permeability effects.[50c,50d] Using a model of ischemia-induced proliferative retinopathy, there is a significant increase in VEGF-mediated retinal neovascularization in transgenic mice, overexpressing the PKC?[2] isoform, and a corresponding decrease in angiogenic activity in PKC? isoform null mice.[50e]
Besides acting as a reservoir for growth factors, the vitreous may exert a mechanical effect in the development of proliferative tissue. Retrospective studies have shown that, whereas a complete posterior vitreous detachment (PVD) occurs in diabetes as a function of aging, partial PVD is seen in diabetics with PDR far more commonly than in individuals without diabetes or in diabetics with background retinopathy.[51] The posterior vitreous face remains attached to the retinal vessels at the sites of proliferation and provides a scaffold along which the new vessels and fibrous tissue can grow. The resulting tractional forces can lead to the development of traction retinal detachment. Precocious PVD, before the development of proliferative retinopathy, appears to protect patients from traction retinal detachments.[52]
EPIDEMIOLOGY
Epidemiologic studies are important in elucidating the systemic, ocular, and genetic factors associated with the development and progression of diabetic retinopathy. Understanding these factors gives insight into the pathophysiology of the disease, as well as indicating where treatment should be directed, in individual patients, and in the healthcare system as a whole.
The Wisconsin Epidemiologic Study of Diabetic Retinopathy (WESDR) is a large population-based study of 2366 subjects divided into two groups: the younger-onset group, or those diagnosed with diabetes before age 30 years, and the older-onset group, or those diagnosed with diabetes after age 30 years.[53,54] The older-onset group was subdivided into those taking insulin and those who did not. In the younger-onset group, the prevalence of any retinopathy was closely related to duration of diabetes, ranging from 2% in subjects with diabetes for less than 2 years to 98% in subjects with diabetes for 15 years or more.[53] The severity of retinopathy in this group also increased with duration of diabetes: the prevalence of PDR ranged from 0% in subjects with diabetes for less than 5 years to 25% in subjects with diabetes for 15 years and 56% in subjects with diabetes for 20 years or more. In the younger-onset group, macular edema is rare before diabetes has been present for 10 years, but the incidence reaches 21% after 20 or more years of disease. In a population examined at the Joslin Clinic, macular edema was more common in the older-onset group; and in patients under the age of 50 years, it was associated with preproliferative or proliferative retinopathy.[55]
In contrast to the younger-onset group, the older-onset group was more likely to have retinopathy present at the time diabetes was diagnosed. The prevalence of any retinopathy in this group in the WESDR was 30% in insulin-taking subjects and 23% in those not taking insulin who had diabetes for less than 2 years.[54] This increased to 85% in the group taking insulin and 58% in the group not taking insulin after 15 years or more of diabetes. After 15 years or more of diabetes, the prevalence of PDR was 20% in those taking insulin and 4% in those not taking insulin.
Incidence and progression of retinopathy were also studied in the WESDR. The younger-onset group had the highest 4 year incidence of any retinopathy (59%), as well as progression (41%), and progression to PDR (10.5%).[53] Older-onset patients taking insulin had a 47% 4 year incidence of any retinopathy, 34% incidence of progression, and 7% incidence of progression to PDR.[54] In those not using insulin, these numbers were all lower, with only a 34% incidence of any retinopathy. The incidence of legal blindness was 3% over 4 years in the older-onset group on insulin versus 1.5% in the younger-onset group.
Various investigators have attempted to determine the characteristics associated with the severity or progression of retinopathy. As already evidenced, the duration of diabetes is important in all patients. The WESDR also found that elevated glycosylated hemoglobin levels were associated with more severe retinopathy in all groups. Proteinuria was associated with severe retinopathy in younger-onset subjects who had diabetes for 10 years or more, as well as in the older-onset group. Elevated diastolic blood pressure and male sex were associated with more severe retinopathy in the younger-onset group and with elevated systolic blood pressure in the older-onset group.[53,54]
A prospective study was carried out at the Joslin Clinic in 153 patients with long-standing diabetes, 90% of whom were in the early-onset category.[56] The risk of progression to preproliferative or proliferative retinopathy increased in the presence of background retinopathy, even if it was slight. The risk of progression increased exponentially with increasing hemoglobin A1c. Diastolic blood pressure less than 70 mmHg, and increasing age were protective factors. Since the study involved patients with long-standing diabetes (duration 16-60 years), the results may not apply to patients in the early course of the disease.
Genetic factors have been investigated, particularly the histocompatibility antigens (human leukocyte antigen (HLA)) with varying findings.[57] Baker and Rand and associates reported that patients with HLA-DR phenotypes 4/0, 3/0, and X/X (neither 3 nor 4) had three to four times the risk of proliferative retinopathy of that found in patients with the HLA-DR phenotypes usually associated with diabetes (HLA-DR 3/4, 3/X, 4/X). In patients with myopia (2 D or greater), this risk was not evident.[57,58]
Several studies have reported significant mortality associated with PDR. In a cohort study at the Joslin Clinic, Rand and colleagues demonstrated that the risk of death was not attributable to PDR itself.[59]The increased risk of death was found only in PDR patients with diabetic nephropathy as evidenced by persistent proteinuria.
OCULAR AND SYSTEMIC RISK FACTORS FOR PROGRESSION TO PDR
GLUCOSE CONTROL
With the introduction of insulin arose the question, is there a level of glycemic control that will prevent the secondary complications of diabetes? If there is such a level, at what point in the course of the disease must the intervention be made? Most clinical studies have shown an association between poor control of blood glucose and increased severity of retinopathy.[53,54,56,58,60] In the WESDR, an elevated glycosylated hemoglobin was associated with more severe retinopathy in the younger-onset and older-onset diabetics.[53,54] In a series at the Joslin Clinic, the risk of PDR in long-standing diabetes was related to elevated glycosylated hemoglobin levels.[56,58] Several prospective studies have begun placing diabetic patients on continuous subcutaneous insulin infusion (CSII) systems or multidose (three to four doses per day) insulin treatment regimens with home glucose monitoring.[61-63]
The Kroc Collaborative Study involved 70 patients with diabetes and nonproliferative retinopathy who were randomized to CSII or conventional injection treatment.[61] Over 8 months, glycosylated hemoglobin and blood glucose levels reached near-normal levels in the treatment group. The level of retinopathy progressed in both groups but was worse in the treatment group, with increased cotton-wool spots and IRMA. After 2 years of follow-up, however, little difference was found in the rates of progression between the two groups. The Oslo group, studying 45 patients randomized to CSII, multidose insulin, or conventional insulin therapy, also reported an initial worsening of retinopathy, with microaneurysms and IRMA.[62] One patient experienced severe preproliferative retinopathy in both eyes after 3 months of CSII and was followed up without laser intervention but continued on CSII with regression of the retinopathy after several months.[64] After 2 years of follow-up, patients receiving CSII or multiple injections had a lower rate of progression of retinopathy, as measured by number of microaneurysms and hemorrhages, than did the conventionally treated group. Both studies, as well as other case reports,[65]suggest that rapid achievement of good glycemic control in diabetics with previously poor metabolic control may be detrimental, particularly in patients with preproliferative or proliferative retinopathy.
These trials are limited because of their small study population, short duration, and patient makeup, with varying degrees of retinopathy. The Diabetes Control and Complications Trial (DCCT) was a large, randomized, controlled trial, involving 1441 insulin-dependent subjects, designed to study both primary prevention and secondary intervention.[63,66,67] Patients were randomized to standard therapy or intensive therapy of multidose insulin injections or CSII. The primary prevention study involved 726 subjects who had diabetes for 1-5 years and lacked retinopathy or evidence of renal disease. The secondary intervention study involved 715 subjects who had diabetes for 1-15 years, with minimal background retinopathy and minimal diabetic nephropathy. Retinopathy was the principal outcome in the DCCT. The primary prevention cohort was followed up to determine whether intensive therapy could prevent the development of retinopathy, and the secondary intervention cohort was followed up to determine whether intensive therapy could delay the progression of retinopathy. Patients in the primary cohort were followed up for an average of 6.0 years, and those in the secondary intervention cohort were followed-up for 7.0 years. In the primary prevention cohort, both treatment groups showed a steady rise in the cumulative incidence of any retinopathy (defined as ?1 microaneurysm in two consecutive 6 month sets of photographs), reaching 90% in the conventional group and 70% in the intensive treatment group. Intensive treatment slowed the development of retinopathy over the 9 years of follow-up, with an average risk reduction of 27%, but did not prevent its onset.[68] Using a more conservative outcome of at least three microaneurysms at two consecutive visits, the size of the risk reduction with intensive retreatment increased to 63%. Intensive therapy was more effective when initiated early in the course of insulin-dependent diabetes.
In the secondary intervention cohort, the 9 year cumulative incidence of three or more steps of progression, was 56% in patients who received intensive treatment versus 78% in patients treated conventionally. The incidence of severe nonproliferative retinopathy was 9.2% versus 26%, and the incidence of neovascularization was 8% versus 24%. For macular edema, the cumulative incidence was 27% versus 44%. Although all levels of retinopathy included in the study benefited from intensive therapy, the effects were less marked in eyes with more advanced retinopathy. Since the DCCT did not include patients with truly advanced retinopathy, it does not address the question of whether these eyes would benefit from intensive therapy. All of the observed risk reductions reflected an initial period of 2 years or more in which there was no benefit from intensive treatment, averaged against a period beyond 3 years in which intensive therapy showed increasing reductions in risk.
OCULAR SURGERY
Cataracts occur commonly in diabetic patients and may require surgical intervention for both visual rehabilitation and visualization of the fundus. Cataract surgery in diabetics may be more complicated than in the general population, however, with poorer postoperative results, including an increased incidence of cystoid macular edema, an increased risk of progression of the retinopathy, and an increased risk of anterior segment neovascularization. The outcome of cataract surgery in individuals with diabetes has been studied by a number of investigators.
Visual outcome in cataract surgery appears to be affected by the presence or absence of retinopathy preoperatively. In a series of 28 eyes of patients with diabetes, but without retinopathy undergoing extracapsular surgery with lens implantation, the corrected visual acuity achieved 12 months postoperatively was 20/40 or better in 88% of the patients.[69] These results compare favorably with those in nondiabetic individuals. Conversely, patients with retinopathy preoperatively had a poorer visual outcome, with one-third of the 18 eyes achieving a postoperative visual acuity less than 20/200. Eight out of the 18 eyes developed cystoid macular edema. Severe exudative maculopathy has been described after cataract extraction in patients with preoperative background diabetic retinopathy.[70] Postoperative visual acuity may be worse, despite medical treatment and macular laser photocoagulation.
In another retrospective series, Benson and associates studied the visual acuity results in diabetic patients undergoing extracapsular cataract extraction with placement of a posterior chamber lens.[71] They found that in this referral population, the final visual acuity was 20/40 or better in 48% of eyes, and that 28% had 20/200 or worse visual acuity. Sixty-five percent had an improvement in visual acuity of two or more Snellen lines. Interestingly, they found that age was a predictor of final visual acuity, patients aged 63 years or younger were more likely to achieve improved visual acuity. The poorer results in the older patients were due to complications of macular edema. Neovascularization of the iris developed in 6% of patients, and the risk of iris neovascularization in their study population was not increased by posterior capsulotomy.
Studies of the risk of progression of diabetic retinopathy, apart from macular edema, have reached differing conclusions. Sebestyen studied 74 patients with, either no background diabetic retinopathy, or mild background diabetic retinopathy, who were undergoing cataract extraction with lens implantation. He found a similar risk of progression between the operated and the unoperated eyes.[72] In another study comparing extracapsular and intracapsular techniques, Alpar found the lowest incidence of progression of retinopathy in the group undergoing extracapsular extraction.[73] However, he did not differentiate on the basis of preoperative retinopathy, which appears from other studies to be an important factor.
Aiello and co-workers retrospectively studied 154 diabetic patients, who had undergone routine intracapsular cataract extraction in one eye only.[74] The second eye served as a control, and neither eye received laser photocoagulation before surgery or during the first year after surgery. Although most of the eyes had either no diabetic retinopathy or background retinopathy, eyes were included with both quiescent PDR and active PDR. In all patients, regardless of the degree of preoperative retinopathy, there was a statistically significant increased risk of rubeosis iridis and neovascular glaucoma (8% vs 0%). In patients with active PDR, preoperatively the risk was even higher (40% vs 0%). There was also an increased risk of vitreous hemorrhage after surgery, but this was significant only for the group with no background retinopathy or mild background retinopathy preoperatively, and not for those with proliferative retinopathy, probably because of the small number of patients in this group.
Hykin and colleagues retrospectively compared visual acuity results in 90 patients with PDR or background retinopathy undergoing extracapsular cataract extraction with lens implantation.[75] They found that final visual acuity was better in eyes with background retinopathy (67% ? 20/40) compared with eyes with PDR (21% ? 20/40). Eyes with quiescent PDR and lacking maculopathy did somewhat better, with 52% achieving 20/40 or better. Deterioration of retinopathy occurred postoperatively, in 50% of eyes with active PDR preoperatively, and immediate postoperative fibrinous anterior uveitis preventing early panretinal photocoagulation occurred in over half the patients with active proliferative retinopathy. Eyes with active proliferative retinopathy and cataract are better treated with combined cataract removal and pars plana vitrectomy with intraoperative endolaser.
Given the increased risks associated with cataract surgery in patients with diabetic retinopathy, special consideration should be made, both preoperatively and postoperatively. The preoperative assessment of the visual impairment caused by cataract may be more difficult in the diabetic patient, and use of blue-field entoptoscope and potential acuity meter may be helpful.[76] Even in cases where the retina appears unremarkable, patients should be cautioned that there may be progression of diabetic changes postoperatively, with resultant poorer visual acuity. When a cataract is developing in a diabetic patient, effort should be made to perform indicated laser photocoagulation, particularly panretinal photocoagulation for active PDR, before the density of the cataract precludes treatment.
Surgery should be directed toward maintaining an adequate aperture for viewing (and possibly treating) the fundus; and phacoemulsification or extracapsular technique with 'in the bag' placement of an intraocular lens is preferred. Because of the increased rate of macular edema postoperatively in diabetic patients, it may be worth considering topical or oral nonsteroidal antiinflammatory agents as well as topical or depot steroids. Wounds should be sutured well to allow laser photocoagulation with a contact lens within 2-3 weeks of surgery if this proves necessary. If yttrium-aluminum-garnet (YAG) capsulotomy is indicated postoperatively, again the aperture should allow visualization of the retina to the equator. Close follow-up postoperatively is essential, with examination of the iris for neovascularization, and a dilated examination of the fundus for macular edema or progression of retinopathy, with consideration of focal or scatter photocoagulation, as indicated.
PREGNANCY
The role of pregnancy in the progression of diabetic retinopathy remains somewhat controversial. In his 1950 report, Beetham found that disease in pregnant diabetic patients without retinopathy did not progress during the pregnancy.[77] However, patients with evidence of proliferative retinopathy at the onset of pregnancy did so poorly, that he recommended them not to undertake pregnancy. In a study by Rodman and associates in 1979, 8% of 201 pregnant diabetic women, with no background retinopathy, or mild background retinopathy at the onset of pregnancy, had progression of their retinopathy during pregnancy.[78] In 127 women with proliferative disease, 25% had retinopathy progress during pregnancy. Laatikainen and colleagues prospectively studied 73 consecutive pregnant patients and noted no significant progression of retinopathy in patients who lacked or had minimal retinopathy at the beginning of pregnancy.[79] However, 13 of the 20 patients (65%) with frank retinopathy in the first trimester were observed to progress during pregnancy.
Klein and co-workers reported on a prospective case-control study comparing pregnant and nonpregnant insulin-taking diabetic women.[80] Risk factors that were evaluated for the progression of retinopathy included glycosylated hemoglobin, duration of diabetes, current age, diastolic blood pressure, number of past pregnancies, and current pregnancy. Women with evidence of proliferative retinopathy or evidence of previous panretinal photocoagulation were not considered to be at risk for progression, and their data were not included in evaluating risk factors for progression. After correcting for glycosylated hemoglobin level, current pregnancy was found significantly associated with progression, with an adjusted odds ratio of 2:3. Diastolic blood pressure had a smaller effect on progression. Pregnant women were significantly more likely to have a decrease in visual acuity, although this was only a mean difference of less than 1 Snellen letter poorer. Klein and co-workers noted that the metabolic control of the pregnant group was markedly better than that of the nonpregnant group.[80] This is probably because of the current obstetric practice of attempting tighter metabolic control during pregnancy. It has been postulated that progression of retinopathy during pregnancy may be at least partly related to the rapid tightening of metabolic control. Laatikainen and associates studied 40 pregnant patients randomized at the end of their first trimester to conventional insulin therapy and CSII.[81] They found that the risk of progression of retinopathy was the same. However, two of the patients in the CSII group progressed from background to proliferative retinopathy. Both patients had a rapid decrease in their glycosylated hemoglobin level as they entered CSII treatment. None of the patients in the conventional therapy group developed proliferative changes.
Diabetic retinopathy may also be a predictor of pregnancy outcome. Diabetic patients taking insulin are known to be at increased risk of an adverse pregnancy outcome, including abortion, perinatal death, and severe congenital anomalies. Klein and colleagues evaluated various risk factors as predictors for adverse outcome and found that the severity of retinopathy was the only variable to significantly predict an adverse outcome.[82]
Pregnancy in diabetic patients is a crucial time for coordinated care by ophthalmologists, obstetricians, and internists. Guidelines for patient care should be understood by all members of the team. Pregnant diabetic patients should be seen during the first month of the pregnancy. If no retinopathy is found, follow-up in each trimester is sufficient unless the patient becomes symptomatic. An exception is made if the patient is being brought under tighter metabolic control, which could increase the risk of progression of the retinopathy. Improvement in metabolic control should be gradual. Patients with preproliferative or proliferative disease should be followed up every 1-2 months. Laser photocoagulation should be considered earlier in pregnant diabetics than in nonpregnant diabetics, when there is evidence of early proliferative or active preproliferative retinopathy. These findings will be revealed by careful ophthalmoscopic and biomicroscopic examination, and fluorescein angiography can usually be avoided in the assessment of the pregnant diabetic patient. Although there are no firm data on the risk of vitreous hemorrhage in patients with proliferative retinopathy, PDR is not an indication for cesarean section.
HYPERTENSION
The relationship between hypertension and the development of diabetic retinopathy is not clear. In the WESDR, the presence and severity of retinopathy were associated, with elevated diastolic blood pressure in younger-onset diabetics after 10 years or more of diabetes, and with elevated systolic blood pressure in the older-onset diabetics.[53,54] In a case-control study at the Joslin Clinic, Rand and co-workers found that hypertension was associated with proliferative retinopathy in patients who had had diabetes for 15 years or more.[58] This association remained significant even if cases with renal disease were excluded. In a prospective study at the Joslin Clinic, Janka and associates found different rates of progression of severe retinopathy in patients with diastolic blood pressures less than or greater than 70 mmHg.[56,83] Chase and colleagues also found that elevated diastolic blood pressure, even just to 'high-normal' values, carried an increased risk of retinopathy in young diabetics.[84] Since hypertension is a known risk factor for stroke and myocardial infarction, it is important that elevated blood pressure be treated in the diabetic patient, regardless of its effect on retinopathy.
RENAL DISEASE
Approximately one-third of juvenile-onset insulin-dependent diabetics experience diabetic nephropathy, with the highest risk in the second decade of diabetes.[85] Several risk factors may be involved in the development of diabetic nephropathy, including genetic predisposition, hypertension, and poor glycemic control. Severe retinopathy is more likely to be found in patients with renal insufficiency. In the WESDR, proteinuria was strongly associated with severe retinopathy in the younger-onset diabetics with 10 years or more of diabetes.[53] Older-onset diabetics with proteinuria were also more likely to have proliferative retinopathy.[54] Renal retinopathy will overlie diabetic retinopathy in uremic patients and consists of a hypertensive component and a uremic component.12 The hypertensive changes include nerve fiber layer hemorrhages, cotton-wool spots, and a narrowing and irregular caliber of the retinal arterioles. The uremic changes include disk edema and diffuse retinal edema, which may lead to massive macular edema. Treatment of the renal failure, with diuretics, dialysis, or renal transplantation, may result in decreased retinal and macular edema. Laser photocoagulation is not very effective in this group of patients; it is important to consider laser photocoagulation treatment for preproliferative retinopathy or early proliferative changes in the diabetic patient experiencing renal failure.
The treatment of renal failure may result in a different set of ocular problems. Patients on hemodialysis are at increased risk of developing elevated intraocular pressure, particularly in eyes that have undergone vitrectomy. Renal transplant patients are at an increased risk of acquiring cataract from chronic corticosteroid treatment or cytomegalovirus retinitis from chronic immunosuppression.[86]
PANCREAS TRANSPLANTATION
Pancreas transplantation, alone or in combination with renal transplantation, is a relatively new and risky procedure performed on diabetic patients with advanced diabetic nephropathy in conjunction with renal transplantation. Several investigators have begun to examine the effect of transplantation on diabetic retinopathy, although all the studies to date have been limited by low numbers and short follow-up. Petersen and Vine reported on eight patients who underwent combined pancreas and renal transplantation from cadaver donors.[87] Four patients successfully retained functioning pancreas transplants for at least 12 months, whereas four patients with failed pancreas transplants but functioning renal transplants served as the controls. Successful pancreas transplantation led to a euglycemic state, with normal fasting blood glucose, and glycosylated hemoglobin levels. However, the progression of retinopathy appeared unaffected. Three of the study group eyes had an increase in capillary closure versus no increase in the control eyes. Four of the study group eyes versus two of the control eyes had an increase in preretinal gliosis. One eye in each group had worsening of proliferative retinopathy. Comparison of the variables of visual acuity, macular edema, capillary closure, NVD, preretinal neovascularization, preretinal gliosis, and severity of retinopathy showed no statistically significant difference between the two groups.
Ramsay and co-workers reported on the ophthalmic outcomes of pancreas transplant recipients, again comparing successful and unsuccessful transplantations.[88] Twenty-two patients were in the successful transplantation group and 16 in the control group, with follow-up averaging 24 months. Although the investigators noted no substantial difference in the progression of retinopathy in the two groups after 2 years, they observed a trend toward less progression of retinopathy in the treated group after 3 years. In order to adequately study the ophthalmic outcomes of pancreas transplant recipients, it will probably be necessary to pool the patients in transplantation centers across the United States under a common protocol.
Pancreas transplantation still carries significant morbidity and mortality and requires chronic immunosuppression. As a result, the procedure has been limited to patients with end-stage nephropathy, which is a group with a high incidence of advanced retinopathy, many of whom have already received panretinal photocoagulation. It may be difficult to show an effect of pancreas transplantation and normoglycemia on this advanced and already treated eye disease.
OCULAR CONSEQUENCES OF NEOVASCULAR PROLIFERATION
NVD AND NVE
Neovascularization occurs most frequently in the posterior pole or within 45° of the optic disk.[89] It is very commonly observed on the disk itself. New vessels on the disk can be easily overlooked in their early stages, beginning as fine loops or networks of vessels. The vessels gradually increase in caliber from one-eighth to one-quarter the diameter of a retinal vein at the optic disk. The vessels often form a cartwheel configuration with vessels radiating out from the center to a circumferential peripheral vessel (Fig. 135.1a). Occasionally, new vessels will appear similar to normal retinal vessels, with a large caliber and extending across the retina without forming networks. However, these vessels can be distinguished from normal retinal vasculature by the fact that they cross both arterioles and venules. NVD is best identified using a magnified stereoscopic view, either by contact or precorneal lens or with stereoscopic photography.
NVE is best detected by a thorough fundus examination, with binocular indirect ophthalmoscopy combined with biomicroscopy using a lens. Fundus photographs are also helpful in detecting early NVE. Neovascularization typically occurs adjacent to areas of capillary closure, marked by cotton-wool spots and hemorrhagic microaneurysms (Fig. 135.1b). IRMA may be difficult to differentiate from early NVE. IRMA is used to describe irregular, segmental dilatation of intraretinal capillaries, representing early neovascular changes or shunt vessels. On fluorescein angiography, IRMA typically does not leak as profusely as do new vessels (Fig. 135.3).
|
|
|
|
FIGURE 135.3 Fluorescein angiography of neovascularization. (a) NVE along the vascular arcade. (b) Early fluorescein transit defines NVE. (c) Late transit shows continued leakage from NVE. |
VITREOUS AND PRERETINAL HEMORRHAGE
While the posterior hyaloid remains attached, neovascular proliferations appear to be on or slightly anterior to the retina, and are usually asymptomatic. Small hemorrhages may occur near the growing tips of the vessels, but these usually remain subhyaloid. As the posterior hyaloid detaches, hemorrhages become less confined and visual acuity may diminish in proportion to the extent and diffusion of the hemorrhage (Fig. 135.4). Vitreous detachment usually begins in the posterior pole on either side of the vascular arcades, over the fovea, or temporal to the macula. Progression of detachment of the vitreous is halted whenever a tuft of neovascularization or a particularly strong attachment to a retinal vessel is encountered. The tuft may be pulled forward as the vitreous contracts, with or without detachment of the underlying retina. The vitreous detachment will continue to the periphery, at which point the vitreous is permanently attached to the vitreous base. The vitreous usually remains attached at the disk if fibrovascular proliferations are present.
|
|
|
|
FIGURE 135.4 A complication of neovascularization. Vitreous hemorrhage from NVD. |
This process leads to a variety of complex patterns of partial vitreous detachment. In general, however, the pathophysiology of partial vitreous detachment favors attachment of the vitreous to neovascularization, major retinal vessels, the disk, and obligatorily, the peripheral vitreous base. The outer contour of the partially detached vitreous has been termed the 'vitreous cone', with the widest aspect of the cone anteriorly and a variable stem of the cone oriented at the posterior pole. The posterior vitreous face and its attachments in a given eye are critical to the understanding of the surgical approaches in PDR (Fig. 135.5). The posterior vitreous face serves as a surface that may loculate hemorrhage. In addition, it may also have perforations, which at times may cause it to be confused with an epiretinal membrane or even a macular hole.
|
|
|
|
FIGURE 135.5 Posterior hyaloid (posterior vitreous face) configurations in PDR. (a) The posterior hyaloid is attached across the macula, at the disc, and just beyond each arcade. Outside of these areas, the vitreous is detached. In this eye, the posterior hyaloid is fibrotic and slightly separated from the surface of the macula, rendering it visible. The underlying retina is totally attached and the visual acuity is 20/30. (b) Posterior hyaloid with a large hole centrally, simulating an epiretinal membrane with hole. The residual attachment points of the posterior hyaloid at the disk in superior, inferior, and inferotemporal locations may be seen. The retina is attached, and visual acuity is 20/30. (c) Ultrasound demonstrates traction retinal detachment and vitreous attachments (vitreous cone). (d) Intraoperative view of vitreous surgery with creation of an opening in the detached peripheral vitreous with the vitrectomy instrument. The membranous character of this tissue is shown. |
Vitreous hemorrhage may occur as a result of vitreous traction on new vessels. Contraction of the vitreous or fibrovascular proliferation can lead to avulsion of a retinal vessel, usually a vein, and vitreous hemorrhage. Hemorrhage may also be associated with Valsalva's maneuvers related to coughing or vomiting or occasionally is associated with insulin reactions.[90] Most of the time, it occurs during sleep and is unrelated to any obvious factor. Results of the Early Treatment Diabetic Retinopathy Study (ETDRS) indicate that aspirin use does not increase the risk of vitreous hemorrhage.[91]
Blood in the fluid vitreous behind the detached posterior vitreous face remains red until it is absorbed, which usually occurs over weeks to months. Hemorrhage into the formed vitreous tends to turn white over time and may require months to clear.
FIBROUS PROLIFERATION AND RETINAL TRACTION
Early in the course of neovascularization, the new vessels appear bare, but as they develop, delicate white fibrous tissue can be seen adjacent to the vessels. This tissue increases as the vessels develop, and it may subsequently contract. Distortion and disruption of the normal retinal tissue may result in conjunction with the process of vitreous detachment (Fig. 135.6).
|
|
|
|
FIGURE 135.6 Very severe neovascularization with vascular overgrowth obscuring the retina and traction retinal detachment. |
Contraction of the posterior vitreous face and fibrovascular proliferation may lead to tractional retinal detachment. Since fibrous proliferation usually progresses along the temporal arcades, the retina along the temporal arcades is usually the first to detach. Progression of the detachment can then extend centrally and peripherally. The rate of progression of an extramacular tractional detachment to involve the macula may be as low as 15% in a single year.[92] In contrast to rhegmatogenous retinal detachments, tractional detachments are typically concave, are localized, and do not extend to the ora serrata. Tractional retinal detachments in PDR have many configurations, depending on the location, number, and severity of attachments of the posterior vitreous face to neovascularization and its associated fibrovascular tissue. The activity of the neovascularization also plays a role. Configurations of tractional detachments may range from an isolated tractional detachment outside the arcades associated with an area of NVE that has regressed, to a tractional detachment of the entire posterior retina with extensive contact of the retina, neovascular tissue, and the posterior vitreous face. The various configurations have implications for the indications for surgical intervention and for the prognosis for successful reattachment. Tractional retinal detachments may also develop retinal breaks, either atrophic or tractional. The resulting combined tractional-rhegmatogenous detachment typically progresses, although in some cases the detachment may remain stable despite the break, particularly in an eye with extensive panretinal photocoagulation (Fig. 135.7). Detachments involving the fovea have obvious impact on vision. However, in other cases, the fibrovascular tissue may overgrow and obscure the fovea, reducing vision without actual foveal detachment. Contraction of fibrovascular tissue can also lead to distortion or horizontal displacement of the macula (tangential traction). Visual acuity may be reduced in this condition owing to striae in the macula, and surgery may result in visual improvement.[93]
|
|
|
|
FIGURE 135.7 Posterior break in tractional retinal detachment. (a) Tractional detachment along the superior arcade with a retinal break just inferior to the neovascular stalk. (b) Confluent laser applied to surround the detachment. (c) Four months later, the detachment is unchanged and visual acuity remains 20/20. The detachment has remained stable over the subsequent 2.5 years of observation. |
RUBEOSIS
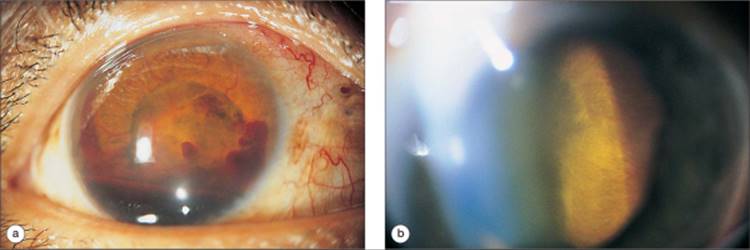
Iris neovascularization or rubeosis is a complication of proliferative retinopathy. Rubeosis is characterized by the networks of branching vessels over the surface of the iris, with vessels crossing the scleral spur on gonioscopy. Usually, the new vessels are apparent on clinical examination, but fluorescein angiography is occasionally helpful in demonstrating leakage from the new vessels. Rubeosis is observed in the setting of proliferative changes and retinal ischemia and also in long-standing retinal detachment related to diabetic retinopathy. It is most dramatically evident in eyes with retinal detachment after unsuccessful vitrectomy. In this setting, rubeosis will develop in almost all cases and will progress rapidly if the underlying detachment is not repaired.
INVOLUTIONAL PROLIFERATIVE DIABETIC RETINOPATHY
All diabetic retinopathy eventually reaches an involutional stage. The visual outcome is variable and depends on the degree of structural alteration in the posterior pole. Vitreous detachment is completed, except in the areas where fibrovascular proliferations prevent complete separation, and fibrovascular proliferation ceases. In an untreated eye, there is usually some element of tractional detachment by the time this phase is reached, and it typically involves the macula. The optic nerve develops some pallor, and the retinal arterioles become attenuated. Retinal hemorrhages and microaneurysms are rare, and pigmentary changes in the RPE may be seen. Fibrous tissue may be thinner and translucent, with the appearance of vitreous veils in contact with diaphanous retina. Visual loss at the involutional phase may relate to macular detachment, macular ischemia, long-standing macular edema, or optic nerve disease (Fig. 135.8).
|
|
|
|
FIGURE 135.8 Macular ischemia in a 21-year-old man with PDR. (a) Intraretinal hemorrhages and cotton-wool spots. Visual acuity is 20/30. (b) Fluorescein angiogram demonstrates macular capillary nonperfusion and early disk neovascularization. (c) Late phase of the angiogram shows continued ischemia with diffuse leakage in the macula. (d) Six months later, the cotton-wool spots have increased and visual acuity is 20/50. (e) Fluorescein angiogram now displays extensive capillary nonperfusion, most prominent in the temporal macula. NVD has increased, and visual acuity is 20/50. (f) Eight years later, after extensive panretinal photocoagulation and also a vitrectomy for vitreous hemorrhage, regressed proliferative changes are noted. Sclerotic vessels are seen temporally, and visual acuity is 20/80. (g) Fluorescein angiogram shows delayed filling of temporal vessels and a greatly increased foveal avascular zone. (h) Late phase of the angiogram shows continued ischemia, vascular wall leakage in the temporal vessels, and macular edema due to intraretinal vascular abnormalities. |
TREATMENT OF PROLIFERATIVE DIABETIC RETINOPATHY
PITUITARY ABLATION
Some of the earliest attempts at treating PDR involved pituitary ablation. However, this treatment modality has subsequently been supplanted by other procedures that are more effective and that have fewer complications, including laser photocoagulation and vitrectomy. Thus, the technique of pituitary ablation is of primarily historical interest today.
Houssay first noted that hypophysectomy reduced the severity of diabetes in pancreatectomized dogs in 1930.[94] Interest was further generated by a report by Poulsen in 1953 of remission of diabetic retinopathy in a woman with Sheehan's syndrome, or postpartum anterior pituitary insufficiency.[35] Luft and co-workers introduced the technique in humans in the 1950s.[95] Various techniques of pituitary ablation were tried, including surgical hypophysectomy, transsphenoidal hypophysectomy, yttrium-90 implantation, x-irradiation, proton beam irradiation, and stereotactic hypophysectomy using radiofrequency coagulation.
Both short- and long-term follow-up of patients undergoing pituitary ablation demonstrated a stabilization of visual acuity in survivors, an improvement in both disk and peripheral neovascularization, and a reduction in exudates, microaneurysms, and hemorrhages.[12,35,96] However, the complications of treatment were frequent and significant. As reported by Sharp and colleagues, they included debilitating postural hypotension and asymptomatic hypoglycemia, with several related deaths. Osteoporosis and avascular necrosis of the hip were reported and were related to steroid replacement. Sterility led to episodes of severe depression in several patients and suicide in at least one case. In the group from London treated with yttrium-90, the 5 year mortality rate was 18% and the 10 year rate was 51%.[96]
BEETHAM'S OBSERVATIONS LEADING TO RATIONALE FOR LASER THERAPY
Early investigators observed that certain ocular conditions seemed to prevent severe diabetic retinopathy. Eyes with chorioretinal scarring, optic atrophy, retinitis pigmentosa, and high myopia were protected from severe proliferative retinopathy.[97] Beetham, studying patients at the Joslin Clinic, described spontaneous resolution of PDR in approximately 10% of patients.[98] The fundus picture in these patients consisted of lacy, reticulated proliferative tissue; attenuated arterioles, and obliterated vessels appearing as white lines. The fundus picture resembled that of the ocular conditions described earlier, as well as the fundus picture that developed after successful hypophysectomy for PDR. Over a period of time, it was recognized that this appearance and the subsequent possibility of inducing regression of PDR with preserved visual acuity could be achieved with laser photocoagulation.
EARLY LASER TRIALS (DIRECT ABLATION)
Meyer-Schwickerath and Schott first used light photocoagulation to treat diabetic retinopathy in 1955.99 The xenon arc they used produced white light emitting multiple wavelengths. Lesions of moderate therapeutic intensity were full-thickness retinal burns histologically, with destruction of inner retina, explaining the frequent occurrence of visual-field defects. With the xenon arc, one could obliterate vessels directly, treating flat neovascular patches, dilated retinal capillaries, microaneurysms, and edematous retina. Treating elevated vessels required increased power and resulted in extensive retinal destruction. The best results were obtained by Meyer-Schwickerath and Schott in patients with nonproliferative and early PDR.99 Several months to years after treatment with the xenon arc, flat neovascular patches remained scarred and atrophic, there was a decrease in exudates, retinal edema, and venous dilatation. New retinal vessels disappeared even if not treated directly. Atrophic changes progressed over 4-8 years. Of 73 patients with nonproliferative diabetic retinopathy treated with the xenon arc and followed up for 1-9 years, only one patient developed PDR. However, diffuse treatments of the retina resulted in large visual-field defects, hemorrhage, and fibrous proliferation and traction.
Aiello and co-workers, postulated that in order to reproduce the involutional fundus picture, one needed to be able to produce multiple small 'harmless' chorioretinal scars in the posterior pole.[100] Clearly, this was not possible with the xenon arc. However, with the development of the ruby laser, this treatment approach became possible. The ruby laser emits monochromatic energy at 694.3 nm, a wavelength transmitted through ocular media and absorbed well by the RPE and choroid. It transmits fairly well through blood, permitting treatment through mild vitreous hemorrhage but also making the laser less effective in treating vessels directly. The laser emits energy for less than 1 ms. In experimental studies by Campbell and associates, the thermal changes were smaller and more narrowly confined than those found with the xenon arc. In 1965, Campbell and associates reported the results of treating 220 patients for a variety of conditions, including retinal tears, retinoschisis, retinal detachment, angiomas, and chorioretinitis.[101]
Beetham and colleagues began using the ruby laser to treat patients with diabetic retinopathy in 1967. By 1969, they had treated 329 patients with various degrees of proliferating retinopathy, treating one eye and using the second eye as a control, in patients in whom the degree of retinopathy was approximately the same.[97] Most of the patients treated had flat neovascularization of the retina, or early NVD plus or minus NVE. Patients were medically evaluated and followed up by complete ocular examinations, including refraction, field examination, fundus photography, and fluorescein angiography. The ruby laser was used at a 2.5° aperture to produce 750 individual chorioretinal lesions of grade I or II intensity. Applications were placed in all areas of the posterior pole, avoiding the disk, macula, and papillomacular bundle.
With 1-2 years of follow-up, there was regression of neovascularization in the treated eyes that was statistically significant.[97] Eighty percent of the treated eyes showed some regression, and 54% had complete disappearance of neovascularization, with the control eyes remaining unchanged or worsening. Aiello and co-workers also noted a decrease in the diffuse angiopathy of the posterior pole, even in the untreated area of the papillomacular bundle.[100] Results in patients with more severe proliferative retinopathy were more disappointing, although with fewer patients falling into these groups so that statistical comparisons could not be made. Of seven patients with elevated disk neovascularization who were treated with ruby laser, two patients showed improvement, three patients suffered severe vitreous hemorrhage with one developing severe fibrous proliferation after the hemorrhage, and two patients remained stable. None of the treated patients in any group developed sector visual-field defects, and there was no related vitreous traction, iritis, cataracts, or elevated intraocular pressure.
Aiello and Beetham and their associates noted the following results after treatment: neovascular nets disappeared or became nonfilling, diffuse angiopathy improved, dot-blot hemorrhages decreased, retinal edema decreased, the disk became paler, there was no change in fibrous proliferation, and the retinal veins were noted to be less 'leaky' by fluorescein.[97,100] The pathophysiologic mechanism by which the laser treatment worked was unclear, possibly involving the reduction in metabolic demand by destroying functioning retinal tissue, or altering the hemodynamic statues of the retinal-choroid layer. Several decades later, the issue is still not completely resolved, although alterations in the levels of various modulators of angiogenesis, such as VEGF, likely play a role.[46,47] Aiello and Beetham and their associates believed that a 'green' laser might be useful to directly treat elevated vessels prone to hemorrhage because there would be greater absorption by the blood column. They also believed that their results warranted a large, long-term, controlled study.
DIABETIC RETINOPATHY STUDY AND MODERN PANRETINAL PHOTOCOAGULATION (PRP)
Indications
The early studies of Beetham and Aiello and associates suggested a beneficial effect of laser photocoagulation in controlling PDR. DRS was a multicentric randomized prospective study designed to determine whether laser treatment in diabetics prevented severe visual loss. It proved very quickly that severe visual loss (visual acuity < 5/200) occurred ?60% less frequently in eyes treated with photocoagulation than in eyes assigned to no treatment.[2,3] The study was also able to identify certain high-risk characteristics in subgroups of patients that led to poor outcome without treatment and in which treatment clearly was of benefit.[102] After 4 years, the study was changed to allow treatment of previously untreated eyes that developed these high-risk characteristics.
The high risk characteristics demonstrated by the DRS are:
|
. |
moderate to severe NVD (greater than standard photograph 10A), |
|
|
. |
any NVD with vitreous or preretinal hemorrhage, and moderate to severe NVE with vitreous or preretinal hemorrhage. |
Other indications, although not clearly demonstrated by the study, are also widely employed, and these are summarized in Table 135.1. These include widespread capillary dropout, moderate to severe NVE alone, and rubeosis with or without neovascular glaucoma. Special consideration should also be given to the history, compliance, medical complications precluding follow-up, and other clinical aspects seen in the patient. For instance, it may be argued that a juvenile diabetic with visual loss caused by severe proliferative retinopathy in one eye should be treated in the second eye when any degree of proliferative retinopathy, preproliferative retinopathy, or increasing retinal ischemia is documented. Similarly a pregnant woman with proliferative changes may be treated sooner because of the possibility of rapid progression of the retinopathy, particularly if tight metabolic control is instituted.
TABLE 135.1 -- Indications for Panretinal Photocoagulation for Proliferative Diabetic Retinopathy
|
DRS High-Risk Characteristics |
|
NVD of moderate to severe degree (greater than standard photo 10A) |
|
NVD of any degree if associated with preretinal or vitreous hemorrhage |
|
NVE of moderate to severe degree if associated with preretinal or vitreous hemorrhage |
|
Additional Indications Widely Employed |
|
Rubeosis with or without neovascular glaucoma |
|
Moderate to severe NVE alone, particularly in juvenile diabetic patients |
|
Widespread retinal ischemia and capillary drop-out on fluorescein angiography |
|
Special Situations for Consideration of Panretinal Photocoagulation |
|
PDR developing in pregnancy, particularly with the institution of tight metabolic control |
|
Preproliferative retinopathy in the second eye of a juvenile diabetic patient with severe PDR in the other eye |
|
Abbreviations: DRS, Diabetic Retinopathy Study; NVD, neovascularization at the disc; NVE, neovascularization elsewhere in the retina; PDR, proliferative diabetic retinopathy. |
Technique
Laser photocoagulation has effectively replaced the xenon arc photocoagulator as the instrument of choice. Multiple wavelengths and instruments are available and effective. Argon green (514 nm) is most commonly employed, and the energy is well absorbed by blood-filled vessels and by pigment in the RPE. Argon blue-green (488 nm) is rarely used, although it was the standard of therapy for the DRS. It is more widely scattered by media and may lead to long-term retinal toxicity in the treating physician. Dye yellow (577 nm) is well absorbed by blood and may permit direct treatment of new vessels in certain instances, such as NVE persisting after panretinal photocoagulation. Krypton red (647 nm) offers better penetration through nuclear sclerotic cataracts and, to a lesser extent, vitreous hemorrhage than does the argon green wavelength. Improved penetration to the choroid may make this wavelength more painful to the patient. More recently, solid-state diode lasers emitting wavelengths between 780 and 850 nm have become available for medical use. They offer the advantage of small size and portability, as well as low power requirements. The longer wavelengths can penetrate media opacity, but they do require more power to produce equivalent retinal lesions, and they may be associated with more patient discomfort.
Laser photocoagulation can be delivered through a slit-lamp system, an indirect ophthalmoscope, or an endolaser probe. Transpupillary slit-lamp delivery is the most common delivery system for the treatment of adults. The indirect ophthalmoscope laser is available with argon, krypton, or diode lasers and permits panretinal photocoagulation in patients under general anesthesia or in a recumbent position. The endolaser, argon, krypton, or diode is restricted to be used at vitrectomy.
Topical anesthesia is usually adequate, although retrobulbar or peribulbar anesthesia may be needed for re-treatments, or for treatment with longer wavelengths, or for indirect ophthalmoscope delivery. Oral diazepam supplementation can also be useful in a patient who is very nervous. The lenses used for slit-lamp delivery include the Rodenstock panfunduscopic lens, the Volk quadraspheric lens, and the Goldmann three-mirror lens. The Rodenstock and Volk lenses allow one to view a large area of the fundus during treatment and are popular for the performance of panretinal photocoagulation. With these lenses, the image is inverted and far peripheral burns are more difficult to place than with the Goldmann lens. The Rodenstock and Volk lenses magnify the spot size, and relatively more power is required for these lenses. The Goldmann lens allows placement of far peripheral burns, but it provides a view of only a small area of the retina.
Spot size depends on the lens selected, usually 500 ?m for the Goldmann lens and 200 ?m for the Rodenstock lens, to achieve ?500 ?m burn. Occasionally, larger lesions are employed for heavy therapy (e.g., when treating rubeosis). The duration is typically 0.1-0.2 s. Longer durations can be used in patients with media opacity, as well as for treatment with longer wavelengths. The power should be titrated to produce a gray-white burn. Treatment should begin at 100 mW with the Goldmann lens or 150 mW with the Rodenstock or Volk lens, although a heavily pigmented fundus in an aphakic or pseudophakic eye suggests an even lower initial setting. The number of spots is less critical than the response to therapy and follow-up. The DRS protocol specified 800-1600 spots 500 ?m in size. The burns should be placed 1-1.5 burn widths apart, with focal confluent bombardment of the NVE. If possible, the treatment inferiorly should be heavier than the treatment superiorly to preserve downgaze field. In treating the temporal raphe, a barrier line should be placed 2.5 disk diameters temporal to the center of the macula, with treatment extending distal to the barrier. Panretinal treatments are usually divided over two to three sessions, but they may be given in a single session if required. One study found no significant long-term differences in single-session versus multiple-session treatment, but fewer transient choroidal and exudative retinal detachments were observed in the multiple-session group.[103]
Results
The DRS clearly demonstrated that photocoagulation in selected diabetics reduced the risk of severe visual loss. Eligible patients for the DRS had proliferative retinopathy in at least one eye or severe nonproliferative retinopathy in two eyes, and visual acuity of 20/100 or better in each eye. One eye was randomly assigned to treatment, and treatment was randomized between argon laser and xenon arc photocoagulation. The rate of severe visual loss (visual acuity < 5/200) was reduced by treatment from 16% in nontreated eyes over 2 years to 6% in treated eyes, a reduction of 57%.[2,3,104] The DRS identified certain subgroups, based on severity of the retinopathy, for which the treatment effect outweighed any harmful effect. Severe visual loss in patients with these retinopathy gradings (called 'high-risk characteristics' and discussed earlier) fell from 26% in nontreated eyes to 11% in treated eyes.[3,102,104] Harmful effects of treatment were also identified and were somewhat greater in the xenon-treated group of the DRS. Estimates of persistent visual acuity loss attributable to treatment in the xenon-treated eyes were 19% with loss of one line of visual acuity and 11% with loss of two lines.[104,105] In the argon-treated group, these numbers were 11% and 3%, respectively. Twenty-five percent of the xenon-treated eyes demonstrated a modest loss of visual field, and an additional 25% had more severe field loss. Five percent of the argon group showed some constriction in visual field. It was felt that some adverse treatment effects were related to focal treatment of NVD and elevated NVE, and this aspect of treatment was abandoned.[104] Other studies comparing the use of xenon arc and laser photocoagulation failed to demonstrate any significant difference in the two modalities, either in effectiveness or in the rate of visual loss related to treatment.[106,107] However, they did confirm the greater risk of field loss occurring after xenon arc treatment, which probably correlates with the inner retinal damage with a xenon arc burn evident on histopathology.[108]
Regression of neovascularization occurs in 30-55% of eyes after laser photocoagulation using various treatment approaches and may correlate with visual prognosis (Fig. 135.9). The DRS found complete regression of NVD in 29.8% and partial regression in 24.5% of eyes 12 months after treatment.[2] Blankenship compared central and peripheral photocoagulation and found a trend toward decreased visual loss (related to treatment) in the peripheral distribution group and a slightly smaller loss of visual field. Regression of NVD was similar in both groups, with 47% complete regression in the peripheral distribution group versus 40% in the central distribution group. In both groups, 33% of patients had partial regression of NVD after photocoagulation.[108] Regression of NVD should be assessed several weeks after photocoagulation as a prognostic indicator and to determine whether additional treatment is necessary. Doft and Blankenship have shown that regression of neovascularization 3 weeks after treatment is a good indicator of longer-term visual results.[109] Vine suggested that eyes be assessed 6-8 weeks after laser treatment and that treatment be augmented if high-risk characteristics persist.[110]He described a group of 'nonresponders' who continued to have high-risk characteristics despite augmented PRP averaging 3000 Goldman burns. Approximately 50% of these 'nonresponders' did respond to additional low-intensity, but extensive, photocoagulation, reaching an average of 7550 Goldman burns, with preservation of visual acuity.
|
|
|
|
FIGURE 135.9 Progression of PDR despite panretinal photocoagulation. (a) A 29-year-old man with preproliferative changes in the right eye. Vascular dilatation, cotton-wool spots, and intraretinal hemorrhages are seen. Visual acuity is 20/25. (b) Superior retina with similar preproliferative changes. (c) Fluorescein angiogram shows numerous microaneurysms with leakage and an enlarged foveal avascular zone. (d) Superior retina with capillary nonperfusion and leakage into the vascular walls. (e) Patient was lost to follow-up for 1.5 years and presented with severe NVD. Visual acuity is 20/25. (f) Fluorescein angiogram shows marked progression of ischemic changes in association with prominent leakage from NVD. (g) Angiogram of the superior retina shows greatly increased ischemia compared with the previous angiogram. (h) Angiogram of the nasal retina documents almost total closure of the capillary bed in association with areas of neovascularization. (i) Six months later, NVD progressed despite extensive and repeated panretinal photocoagulation. (j) After an additional 10 months, a traction retinal detachment involving the fovea developed. The retina was obscured by neovascular tissue, and visual acuity is counting fingers at 1 ft. (k), One year after vitrectomy and endolaser treatment, the retina is attached but displays vascular and optic atrophy, and visual acuity is 20/200. |
Although the DRS used blue-green argon wavelengths or xenon arc for photocoagulation, other wavelengths are employed by treating ophthalmologists. Argon green has replaced argon blue-green to avoid long-term retinal toxicity in the treating physician. Dye yellow, krypton red, and diodes emitting in the near-infrared have all been utilized for PRP. Studies have compared the effectiveness of certain wavelengths but not all. Krypton red photocoagulation was demonstrated to be as effective as argon blue-green for the treatment of PDR, comparing visual outcome, regression of vessels, and incidence of complications.[111]
There is some controversy regarding photocoagulation in the presence of tractional retinal detachment. If the tractional retinal detachment involves the fovea, vitrectomy is indicated. However, concerns are often expressed that photocoagulation in patients with extrafoveal tractional detachments will lead to worsening of the detachment and involvement of the fovea. The DRS found that harmful treatment effects, including decreased visual acuity, were associated with preexisting fibrous proliferations and localized retinal detachments, particularly in the xenon-treated group.[105] However, the report also confirmed that those patients with severe proliferative retinopathy still benefited from argon laser treatment. Some authors have suggested 'prophylactic vitrectomy' for traction retinal detachments 'threatening' the macula.[112] This approach may unnecessarily subject some patients to the risks of vitrectomy surgery. One study investigating argon laser photocoagulation in patients with severe proliferative retinopathy and posterior extrafoveal traction detachments found that detachments rarely progress after treatment to involve the fovea.[113] In this study, the area of detachment was avoided with otherwise standard photocoagulation techniques and without any effort to wall off the detachment.[113] PRP with careful follow-up should be the first line of therapy in patients with proliferative retinopathy and traction retinal detachments not involving the fovea.
The DRS found that eyes with high-risk characteristics have a 2 year risk of severe visual loss of 25%. Scatter photocoagulation reduces the risk of severe visual loss by 50% or more. Eyes with severe nonproliferative retinopathy or proliferative retinopathy without high-risk characteristics have a 2 year risk of severe visual loss of 3-7%. Thus, the risk of visual-acuity loss relating to treatment assumes greater relative importance.[104] The DRS was unable to determine whether deferral of treatment with observation in this group was better than early treatment. The Early Treatment of Diabetic Retinopathy Study was designed in part to determine the optimal timing of photocoagulation. Early treatment for nonproliferative retinopathy was compared with deferral of photocoagulation until high-risk characteristics developed. There was a small reduction in the rate of severe visual loss with early treatment, but the rates of severe visual loss were low in both groups (2.6% for the early treatment group, and 3.7% for the deferral group).[114] Therefore, the study group initially recommended that as long as careful follow-up can be provided for the patient, PRP is not recommended for eyes with mild or moderate nonproliferative retinopathy. It is important to note that the data was subsequently re-analyzed taking into account the type of diabetes, type 1 or type 2. In this analysis, there was an advantage in treating severe nonproliferative or early PDR with PRP in patients with type 2 diabetes.[115] The physician must also incorporate clinical judgment, including assessment of the fellow eye, progression of lens opacities, and other conditions.
Complications
Laser photocoagulation is clearly an effective treatment but can result in complications (Table 135.2). These complications may occur during treatment in the immediate postoperative period or present as long-term problems (Fig. 135.10). Pain during treatment is usually transient but may require retrobulbar anesthesia for completion of the session. Increased intraocular pressure can occur, particularly after heavy treatment, because of choroidal swelling and angle shallowing, but it usually resolves after 48 h.[116] It can usually be avoided with divided sessions or lighter treatment. The cornea in diabetic patients is very sensitive to contact lens trauma, and corneal abrasion during treatment may result in a persistent epithelial defect. The cornea should be inspected after treatment and any abrasions treated appropriately. Mydriasis is the result of laser damage to nerves in the uveal tract and is permanent. Paralysis of accommodation can occur but is usually transient.[117]
TABLE 135.2 -- Complications of Panretinal Photocoagulation
|
Foveal burn |
|
Optic disc damage |
|
Macular edema |
|
Choroidal hemorrhage |
|
Choroidal neovascularization |
|
Choroidal detachment |
|
Exudative retinal detachment |
|
Vitreous hemorrhage |
|
Pain during treatment |
|
Increased intraocular pressure |
|
Corneal abrasion |
|
Mydriasis and paresis of accommodation |
|
Loss of visual field |
|
Loss of dark adaptation |
|
Lens opacities |
|
Increase in traction detachments |
|
|
|
|
FIGURE 135.10 Panretinal photocoagulation and complications. (a) Wide-angle photograph of a typical panretinal photocoagulation pattern. (b) Choroidal and exudative retinal detachment after extensive photocoagulation for rubeosis. (c) Macular edema 2 weeks after panretinal photocoagulation. Visual acuity is at the counting fingers at 2 ft level, and was 20/30 before laser. (d) Fluorescein angiogram documents cystoid edema. Edema resolved in 1 month with visual recovery. |
Macular edema and visual acuity loss of one to three lines can occur and are more common in patients with perifoveal capillary nonperfusion. Maximum macular edema after panretinal photocoagulation can occur anywhere from 4 to 7 weeks after the initial laser treatment. However, visual recovery is usually good.[117a] Visual-field loss secondary to photocoagulation was documented in the DRS and is related to the extent of treatment;[104] loss of dark adaptation can also occur after PRP.[118] Choroidal detachment and exudative retinal detachment are usually the result of very heavy PRP and generally resolve spontaneously.[119] Choroidal hemorrhage can occur with a very heavy burn, particularly with longer wavelengths, but is usually limited and resolves spontaneously. Subretinal neovascularization has been reported and should be treated if it is macular.[120] Foveal burns are the result of the surgeon's disorientation or unfortunate ocular movement and result in permanent loss of central acuity, but there may be some improvement after the initial loss. Vision loss has also been reported in association with peripapillary treatment.[121] Vitreous hemorrhage can result from rupture of neovascular vessels during treatment (rarely) or from shrinkage and regression of neovascular tissue after treatment (commonly). Hemorrhage that occurs after panretinal photocoagulation usually resolves with time but may occasionally require vitrectomy. Direct treatment of elevated neovascularization with green (514 nm) or yellow (577 nm) wavelengths has a limited role and is restricted to eyes with recurrent vitreous hemorrhage and persistent neovascularization despite complete PRP.
Lens opacities can occur with high energy and misfocusing, particularly with the panfundus-style lenses, and are usually permanent but nonprogressive.[122,123] Vascular occlusion can result from placement of burns over a vessel. Frequently, the vessel will again become patent. Although heavy treatment with the xenon arc photocoagulator in eyes with active vitreoretinal traction can lead to progression of an extrafoveal tractional retinal detachment into the fovea in certain cases, data indicate that argon laser therapy may be safely performed in these eyes.[113] Care should be taken to avoid heavy treatment near areas of vitreoretinal traction.
THE ROLE OF VITRECTOMY FOR PROLIFERATIVE DIABETIC RETINOPATHY
Indications
Laser photocoagulation allows effective treatment of moderate to severe PDR. However, although treatment substantially reduces the risk of severe visual loss, PDR in a certain number of eyes progresses to tractional retinal detachment and vision loss. Standard laser cannot be performed in eyes with vitreous hemorrhage precluding visualization of the retina. Vitrectomy was first introduced by Machemer in the 1970s as a method of removing nonclearing vitreous hemorrhage.[124] As techniques and instrumentation have improved, its indications have broadened (Table 135.3).[125,126]
TABLE 135.3 -- Indications for Vitrectomy in Proliferative Diabetic Retinopathy
|
Vitreous hemorrhage |
|
Nonclearing, based on duration and visual need |
|
To permit photocoagulation of active retinopathy |
|
Traction retinal detachment involving the fovea |
|
Visual loss owing to macular striae or distortion (tangential traction) |
|
Combined traction-rhegmatogenous retinal detachment |
|
Rubeosis with media opacity precluding panretinal photocoagulation |
|
Visual loss owing to epiretinal membrane or opacified posterior vitreous face |
|
Progressive neovascularization unresponsive to retinal ablation |
Removing dense, nonclearing vitreous hemorrhage remains an important indication for vitrectomy in diabetics. The Diabetic Vitrectomy Study Group studied the timing of vitrectomy and its effect on visual outcome and complications.[127,128] They included patients with severe vitreous hemorrhage (visual acuity < 5/200) and compared early vitrectomy (after 1 month) with deferred vitrectomy (after 1 year). In patients with type 1 diabetes, early vitrectomy offered a greater chance of visual recovery. In type 2 diabetics and mixed type, the visual results were essentially the same whether vitrectomy was performed early or after 1 year. However, the study was performed without standardized photocoagulation management in the deferred vitrectomy group and without the use of endolaser photocoagulation in diabetic vitrectomy in either group, and the validity of its conclusions may be questioned. Nevertheless, early vitrectomy offers the chance for prompt recovery of vision, which is of greatest importance to patients who do not have useful vision in the fellow eye.[126]
Progressive fibrovascular proliferation in diabetes can lead to tractional retinal detachment. Posterior tractional detachments not involving the fovea may remain stable and should be observed.[92,113,126]However, once the fovea is involved, vitrectomy is indicated. Surgery should be performed promptly because degenerative changes in the detached retina will prevent visual recovery after reattachment (Fig. 135.11). The combination of vitreous traction and membrane contraction can lead to retinal holes and combined traction-rhegmatogenous retinal detachments, which need to be approached via pars plana vitrectomy.
|
|
|
|
FIGURE 135.11 Tractional retinal detachment involving the fovea. (a) Preoperative photograph illustrates extensive neovascularization emanating from the disk with tractional detachment. Visual acuity is 20/400. (b) Postoperative photograph after vitrectomy shows retinal reattachment and removal of neovascular tissue. Visual acuity is 20/40. |
Some patients will present with cataract and proliferative disease. If adequate PRP cannot be performed because of media opacity, there are several management options. Cataract surgery can be performed using extracapsular or phacoemulsification techniques, with PRP performed within a few days of surgery. It should be kept in mind that proliferation may progress rapidly after cataract extraction. Alternatively, pars plana vitrectomy and the endolaser can be performed in conjunction with cataract removal, either pars plana lensectomy or phacoemulsification via a limbal approach, with intraocular lens placement.[92,126,129,130] Lensectomy can be performed with preservation of the anterior capsule and sulcus fixation of a posterior chamber intraocular lens after completion of the vitrectomy. Alternatively, phacoemulsification may be performed, with placement of the intraocular lens in the capsular bag either preceding pars plana vitrectomy or after its completion. The advantage to placement of the intraocular lens after the vitrectomy is improved visualization of the retina during vitrectomy. A combined surgical approach may be most useful in cases when the cataract is visually significant and would prevent visualization of the fundus during vitrectomy and when the anticipated retinal surgery is not unduly complicated.
Iris neovascularization, with or without angle involvement and glaucoma, is conventionally treated with panretinal photocoagulation. In cases of rubeosis, vitrectomy with endolaser use, with or without lensectomy, is indicated in patients with media opacities such as cataract or vitreous hemorrhage or when retinal reattachment is also necessary.[126,131]
Epiretinal membranes develop in diabetes after premacular hemorrhages or after extensive photocoagulation. Vitrectomy is indicated when the patient's vision is compromised enough to warrant surgery.
Technique
The goals of vitrectomy in diabetic retinopathy are simple in concept. One major objective is to remove media opacities, either vitreous hemorrhage or cataract. The second objective is to relieve vitreous traction causing detachment, distortion, or displacement of the fovea, either transvitreal traction from anterior vitreous to posterior attachments or tangential traction from proliferative tissue adherent to the retinal surface. As dissection is performed, it is important to obtain hemostasis to preserve visualization and allow for effective endophotocoagulation. The final goal is to perform retinal ablation, usually by laser, to prevent subsequent neovascular proliferation.[126]
Two major differences in the technical approach to diabetic vitrectomy are (1) the segmentation technique, and (2) the delamination and en-bloc resection techniques. In all approaches, the anterior vitreous is removed to permit visualization and to create a fluid space posterior to the lens. In segmentation, an opening is made in the mid-peripheral detached vitreous where it is typically separated from the underlying retina.[124,126] This opening is extended 360° at the equator and eliminates anteroposterior traction. This 'truncation of the vitreous cone' separates the posterior vitreous face with its attachments to the retina from the vitreous base anteriorly. Segmentation then proceeds with dissection of the posterior vitreous face with vertical scissors cuts around each neovascular attachment of the posterior vitreous face to the underlying retina.[92,126] The end result is the segmentation of the posterior vitreous face into small islands of residual neovascular attachments, and this segmentation relieves contraction between these points and permits reattachment of the retina. These islands can then be trimmed with the vitrectomy instrument.
In delamination and en-bloc resection techniques, the anteroposterior traction is not relieved initially but is used to facilitate dissection of the posterior vitreous face in a horizontal fashion. In the delamination technique, an opening is created in the posterior vitreous face over the macula, gaining access to the surgical plane between the posterior vitreous face and the retina. Horizontal scissors transection across the neovascular attachments above the disk and major vascular arcades is performed radiating outward from the posterior pole, ultimately freeing the retina from the posterior vitreous face entirely.[92] In the conceptually similar en bloc technique, access to this same surgical plane is accomplished by creating an opening in the peripheral detached vitreous and then proceeding with horizontal scissors transection across the posterior pole.[132] In both techniques, the dissection is concluded by using the vitrectomy instrument to remove the now freed posterior vitreous face as it hangs supported by the remaining attachments to the anterior vitreous base.
It should be emphasized that each of the techniques mentioned previously has adherents and detractors. The segmentation technique is criticized for the incomplete removal of proliferative tissue from the retina with possible recurrent hemorrhage or membrane proliferation, and the horizontal dissection techniques are criticized because there is a greater frequency of retinal breaks and a possibility of increased intraocular hemorrhage from transection across the neovascular stalks. In actual practice, a combination of surgical approaches is frequently required in a given eye.
Diathermy is used as needed to obtain hemostasis, but most hemorrhages can be controlled by elevation of the infusion fluid height.[126] Airfluid exchange with internal drainage of subretinal fluid is used in cases of retinal detachment with a posterior retinal break. Panretinal endophotocoagulation is performed when there is active neovascularization or preoperative iris neovascularization or if panretinal photocoagulation has not been performed before surgery.[92,131] Endophotocoagulation is also used to treat iatrogenic retinal breaks. Trans-scleral cryopexy remains a useful tool when extensive retinal ablation is required or the fundus view is lost. Intraocular tamponade with air, long-acting gas, or silicone oil is used in cases of retinal detachment.
Results
The results of vitrectomy for PDR have improved steadily since the mid-1970s owing to increasing vitreoretinal surgical sophistication in general and the introduction of the endolaser and the continuing development of intraocular tamponade in particular. Surgical results in patients with vitreous hemorrhage alone suggest that 71-78% of patients will have improved vision 6 months after vitrectomy[133-135] and that 76% of patients will have visual acuity of 5/200 or better. For patients with traction retinal detachment involving the fovea, 57-75% of patients will have improved visual acuity,[136-141] with 20/200 or greater acuity at 6 months in 40-54% of patients (Fig. 135.12).[138,140,141] Anatomic reattachment of the macula can now be obtained intraoperatively in the great majority of cases,[137,138] but recurrent macular detachment (resulting from recurrent epiretinal tissue or rhegmatogenous detachment) occurs in 5-23% of cases.[137,140,141] For patients with combined tractional- rhegmatogenous retinal detachment who require vitrectomy for management, long-term macular re-attachment is obtained in 64% of cases, and improved visual acuity is observed in 53% of cases, with 55% of these patients having postoperative visual acuity greater than 5/200.[142] These results are an improvement over earlier series in which scleral buckling alone was available for repair, in which the retina was reattached in 46% of cases and 43% had improved visual acuity.[143] For patients with distortion of the macula from contraction of proliferative tissue (tangential traction syndrome), visual acuity was improved in four of four of patients in one report (Fig. 135.13).[93] In a large series, preoperative factors associated with a negative prognostic value for visual recovery include iris neovascularization, cataract, visual acuity less than 5/200, and retinal detachment.[144] Long-term studies indicate the stability of visual and anatomic results of vitreoretinal surgery for PDR.[145] However, postoperative complications such as rubeosis (with or without neovascular glaucoma), retinal detachment, recurrent vitreous hemorrhage, and anterior hyaloid fibrovascular proliferation are the chief causes of irreparable visual loss in these patients.[133-142,146,147]
|
|
|
|
FIGURE 135.12 Tractional retinal detachment involving the fovea. (a) Preoperative photograph shows severe neovascularization with detachment of the fovea. Visual acuity is 20/400. (b) Postoperative appearance after vitrectomy shows retinal reattachment with continued inferior distortion of the macula. Visual acuity is 20/200. |
|
|
|
|
FIGURE 135.13 Tangential traction on the fovea with decreased vision. (a) Preoperative appearance shows macular striae to regressed neovascular tissue to the disc. Visual acuity is 20/80. (b) Fluorescein angiogram documents extensive cystoid edema, primarily affecting the area of traction. (c) Postoperative photograph 2 months after vitrectomy and removal of posterior vitreous face. Traction is relieved and visual acuity is 20/70. |
Complications
Postoperative complications after vitrectomy can be early (within the first week) or late (weeks to months later). Early complications are frequent but can usually be treated successfully. The cornea of the diabetic individual is susceptible to injury at surgery, and epithelial defects may be difficult to heal, requiring pressure patching and, occasionally, bandage contact lens for resolution.[126] Cataract formation may occur from direct lens trauma at the time of vitrectomy or from exposure to intraocular gas postoperatively.[92,126] Lens removal should be performed, if visually significant, after the posterior segment is stable, or sooner if significant complications arise from lens-induced glaucoma or inflammation.
Postoperative hemorrhage usually resolves spontaneously over several weeks. If the fundus is obscured, ultrasound should be performed periodically to exclude retinal detachment.[92,126] If the blood does not clear within several weeks or if there is a concurrent retinal detachment, reoperation is indicated. Ghost cell glaucoma is an infrequent complication but usually requires a washout procedure to control the intraocular pressure.[92] Retinal detachment after vitrectomy may result from unrecognized retinal holes or traction and requires reoperation.[92,126] Endophthalmitis is rare and should be diagnosed and treated emergently. Glial recurrence occurs rarely, the glial tissue proliferates directly on the retinal surface and is managed surgically with a segmentation-delamination approach.[92]
Iris and angle neovascularization may develop after vitrectomy; it is usually related to rhegmatogenous retinal detachment or extensive retinal ischemia (Fig. 135.14a).[92,126] Surgery for the retinal detachment with extensive panretinal photocoagulation is indicated. Anterior hyaloidal fibrovascular proliferation is a serious complication of diabetic vitrectomy and is most commonly observed in juvenile diabetics with severe retinal ischemia undergoing vitrectomy without lens removal.[146,147] In this situation, extensive neovascularization develops posterior to the lens and along the anterior hyaloid (Fig. 135.14b). Unless surgical intervention, including lensectomy and extensive peripheral retinal ablation, is performed promptly, these eyes are invariably lost.
|
|
|
|
FIGURE 135.14 Complications of vitrectomy. (a) Rubeosis, hyphema, neovascular glaucoma, and recurrent detachment after failed vitrectomy for traction retinal detachment involving the fovea; visual acuity is at the no-light perception level. (b) Anterior hyaloid fibrovascular proliferation in a 22-year-old man after phakic diabetic vitrectomy. Visual acuity is at the seeing-hand motions level, and the eye was lost despite repeat surgery. |
INTRAVITREAL INJECTION OF ANTIANGIOGENIC AGENTS
Much recent attention has focused on the role of intravitreal injections of antiangiogenic agents in the treatment of a number of retinal conditions, including age-related macular degeneration, diabetic macular edema, and diabetic PDR. There are a number of potential complications of intraocular injections, including endophthalmitis, retinal tears/detachments, vitreous hemorrhage, cataract, hypotony, and glaucoma. In spite of these risks, however, a review of the literature indicates that the risk of a serious adverse event from an intravitreal injection is relatively low. Jager et al analyzed data from 14 866 intravitreal injections in 4382 eyes and found a prevalence of 0.2% per injection and 0.5% per eye of endophthalmitis after excluding cases reported specifically as pseudoendophthalmitis.[148] Guidelines for proper technique in intravitreous injections are still evolving,[149] although certain procedures, including the routine use of a wire lid speculum, sterile preparation with povidone iodine, and the avoidance of a paracentesis have gained widespread acceptance as means toward reducing the risk of endophthalmitis.
Intravitreal steroids have been used as adjuncts to both PRP and vitrectomy for PDR. Although there are no large-scale, randomized, placebo-controlled clinical trials in the literature to address the efficacy of intravitreal steroids for retinal neovascularization, the available case reports suggest that intraocular steroids are well tolerated at least in the short term.[150] Well-documented complications of long-term steroid administration include cataract and glaucoma. Although intraocular steroid often has a beneficial, if temporary effect on macular edema, its effects are less well-established regarding proliferative disease.[151] Some surgeons have advocated the intraoperative use of triamcinolone acetonide in order to improve staining and visualization of the vitreous to facilitate the identification and removal of the posterior hyaloid face.
Anti-VEGF agents that have been used in the treatment of PDR include the nonselective VEGF inhibitors ranibizumab and bevacizumab as well as pegaptanib sodium which is a targeted aptamer against the VEGF isoform 165. Although there is extensive data on these agents in the treatment of choroidal neovascularization from age-related macular degeneration, the literature on their use in treatment of PDR is limited to case reports and series. Nonetheless, the anecdotal evidence that exists suggests that anti-VEGF therapy is effective in at least some patients in regressing iris and retinal neovascularization and reducing vitreous hemorrhage.[152,153] The Macugen Diabetic Retinopathy Study Group reported that in patients with PDR who were enrolled in a study of pegaptanib sodium for diabetic macular edema, 62% (eight of 13) of patients treated with pegaptanib demonstrated regression of neovascularization on fundus photographs and/or decreased fluorescein leakage from their neovascularization. None of the fellow, nonstudy eyes or eyes randomized to sham injection showed a similar regression of neovascularization.[154]
REFERENCES
1. Waite J, Beetham W: The visual mechanism in diabetes mellitus: comparative study of 2002 diabetics and 457 non-diabetics for control. N Engl J Med 1935; 212:367-429.
2. The Diabetic Retinopthay Study Research Group : Photocoagulation treatment of proliferative diabetic retinopathy: the second report of Diabetic Retinopathy Study -ndings. Ophthalmology 1978; 85:82.
3. The Diabetic Retinopathy Study Group : Preliminary report on effects of photocoagulation therapy. Am J Ophthalmol 1976; 81:383-396.
3a. World Health Organization : Diabetes fact sheet. Available: http://www.who.int/hpr/NPH/docs/gs_diabetes.pdf#search=%22370%20million%20diabetes%20world%20health%20organization%22![]() 30 Sept 2006
30 Sept 2006
4. Klein R, Klein B: Vision disorders in diabetes. In: Harris M, Hamman R, ed. Diabetes Data Compiled 1984, p XIII, Washington, DC: US Government Printing Of-ce; 1985.
4a. Aiello LP: Angiogenic pathways in diabetic retinopathy. N Engl J Med 2005; 353:839-841.
4b. Bursell SE, Clermont AC, Kinsley BT, et al: Retinal blood flow changes in patients with insulin-dependent diabetes mellitus and no diabetic retinopathy. Invest Ophthalmol Vis Sci 1996; 37:886-897.
5. Michaelson IC: The mode of development of the vascular system of the retina, with some observations on its signi-cance for certain retinal disease. Trans Ophthalmol Soc UK 1948; 68:137-180.
5a. Plehwe W, Sleightholm M, Kohner E, et al: Does vitreous fluorophotometry reflect severity of early diabetic retinopathy. Br J Ophthalmol 1989; 73:225-260.
6. Frank R: Diabetic retinopathy: current concepts of evaluation and treatment. Clin Endocrinol Metab 1986; 15:933-969.
7. Aiello L, Li R, Sebestyen J, et al: The eyes and diabetes. In: Marble A, ed. Joslin's Diabetes Mellitus, 12th edn. Philadelphia: Lea & Febiger; 1985.
8. Tolentino MJ, Miller JW, Gragoudas ES, et al: Intravitreous injections of vascular endothelial growth factor produce retinal ischemia and microangiopathy in an adult primate. Ophthalmology 1996; 103:1820-1828.
9. Amin R, Frank R, Kennedy A, et al: Vascular endothelial growth factor is present in glial cells of the retina and optic nerve of human subjects with nonproliferative diabetic retinopathy. Invest Ophthalmol Vis Sci 1997; 38:36-47.
10. Pascal DI, Bindley CO, Wallow IHL: Clinicopathologic correlation of intraretinal microvascular abnormalities. Retina 1997; 17:321-329.
11. Chang S, Leonard-Martin T, Feman S: Relationship between IRMA and diabetic neovascularization. Invest Ophthalmol Vis Sci 1995; 36:S483.
13. Ashton N: Retinal vascularization in health and disease. Am J Ophthalmol 1957; 44:7-24.
14. Kohner E, Schilling J, Hamileton A: The role of avascular retina in new vessel formation. Metab Ophthalmol 1976; 1:15.
15. Wise G: Retinal neovascularization. Trans Am Ophthalmol Soc 1956; 54:729-826.
16. Branch Vein Occlusion Study Group : Argon laser scatter photocoagulation for prevention of neovascularization and vitreous hemorrhage in branch vein occlusion. Arch Ophthalmol 1986; 104:34-41.
17. Baird A, Böhlen P: Fibroblast growth factors. In: Roberts AB, Sporn MB, ed. Handbook of Experimental Pharmacology: Peptide Growth Factors and Their Receptors, Berlin: Springer-Verlag; 1990:369-418.
18. Mignatti P, Tsuboi R, Robbins E, et al: In vitro angiogenesis on the human amniotic membrane: requirement for basic -broblast growth factor-induced proteinases. J Cell Biol 1989; 108:671-682.
19. Montesano R, Vassali JD, Baird A, et al: Basic -broblast growth factor induces angiogenesis in vitro. Proc Natl Acad Sci USA 1986; 83:7297-7301.
20. Lobb RR, Alderman EM, Fett JW: Induction of angiogenesis by bovine brain derived class I heparin-binding growth factor. Biochemistry 1985; 24:4969-4973.
21. Shing Y, Folkman J, Haudenschild C, et al: Angiogenesis is stimulated by a tumor-derived endothelial cell growth factor. J Cell Biochem 1985; 29:275-287.
22. Esch F, Ueno N, Baird A, et al: Primary structure of bovine brain acidic -broblast growth factor. Biochem Biophys Res Commun 1986; 133:554-562.
23. Gospodarowicz D: Fibroblast growth factors. In: Pimental E, Perucho M, ed. Critical Reviews in Oncogenesis, Boca Raton, FL: CRC; 1989:1-26.
24. Abraham JA, Mergia A, Whang JL, et al: Nucleotide sequence of a bovine clone encoding the angiogenic protein, basic -broblast growth factor. Science 1986; 233:545-548.
25. D'Amore PA, Klagsbrun M: Endothelial mitogens derived from retina and hypothalamus: Biological and biochemical similarities. J Cell Biol 1984; 99:1545-1549.
26. Caruelle D, Groux MB, Gaudric A, et al: Immunological study of acidic -broblast growth factor (aFGF) distribution in the eye. J Cell Biochem 1989; 39:117-128.
27. Gao H, Holly-eld JG: Basic -broblast growth factor (bFGF) immunolocalization in the rodent outer retina demonstrated with an anti-rodent bFGF antibody. Brain Res 1992; 585:355-360.
28. Nyberg F, Hahnenberger R, Jakobson AM, et al: Enhancement of FGF-like polypeptides in the retinae of newborn mice exposed to hyperoxia. FEBS Lett 1990; 267:75-77.
29. Zhang NL, Samadani EE, Frank RN: Mitogenesis and retinal pigment epithelial cell antigen expression in the rat after krypton laser photocoagulation. Invest Ophthalmol Vis Sci 1993; 34:2412-2424.
30. Sivalingam A, Kenney J, Brown GC, et al: Basic -broblast growth factor levels in the vitreous of patients with proliferative diabetic retinopathy. Arch Ophthalmol 1990; 108:869-872.
31. Vlodavsky I, Folkman J, Sullivan R, et al: Endothelial cell-derived basic -broblast growth factor: Synthesis and deposition into subendothelial extracellular matrix. Proc Natl Acad Sci USA 1987; 84:2292-2296.
32. McNeil PL, Muthukrishnan L, Warder E, et al: Growth factors are released by mechanically wounded endothelial cells. J Cell Biol 1989; 109:811-822.
33. LeRoith D, Roberts Jr CT: Insulin-like growth factors. Ann N Y Acad Sci 1993; 692:1-9.
34. Salmon Jr WD, Daughaday WH: A hormonally controlled serum factor which stimulates sulfate incorporation by cartilage in vitro. J Lab Clin Med 1957; 49:825-836.
35. Poulsen JE: The Houssay phenomenon in man. Recovery from retinopathy in a case of diabetes with Simmonds' disease. Diabetes 1953; 2:7-12.
36. Grant M, Jerdan J, Merimee TJ: Insulin-like growth factor-I modulates endothelial cell chemotaxis. J Clin Endocrinol Metab 1987; 65:370-371.
37. Grant MB, Mames RN, Fitgerald C, et al: Insulin-like growth factor I as an angiogenic agent. In vivo and in vitro studies. Ann N Y Acad Sci 1993; 692:230-242.
38. Grant M, Russell B, Fitgerald C, et al: Insulin-like growth factors in vitreous. Studies in control and diabetic subjects with neovascularization. Diabetes 1986; 35:416-420.
39. Miller J, Adamis A, Aiello L: Vascular endothelial growth factor in ocular neovascularization and proliferative diabetic retinopathy. Diabetes Metab Rev 1997; 13:37-50.
40. Miller JW, Adamis AP, Shima D, et al: Vascular endothelial growth factor/vascular permeability factor is temporally and spatially correlated with ocular angiogenesis in a primate model. Am J Pathol 1994; 145:574-584.
41. Pierce EA, Avery R, Foley E, et al: Vascular endothelial growth factor/vascular permeability factor expression in a mouse model of retinal neovascularization. Proc Natl Acad Sci USA 1995; 92:905-909.
42. Dorey C, Aouididi S, Reynaud X, et al: Correlation of vascular permeability factor/vascular endothelial growth factor with extraretinal neovascularization in the rat. Invest Ophthalmol Vis Sci 1996; 114:1210-1217.
43. Stone J, Chan-Ling T, Pe'er J, et al: Roles of vascular endothelial growth factor and astrocyte degeneration in the genesis of retinopathy of prematurity. Invest Ophthalmol Vis Sci 1996; 37:290-299.
44. Adamis A, Shima D, Tolentino M, et al: Inhibition of VEGF prevents ocular neovascularization in a non-human primate. Arch Ophthalmol 1996; 114:66-71.
45. Aiello L, Pierce E, Foley E, et al: Inhibition of vascular endothelial growth factor suppresses retinal neovascularization in vivo. Proc Natl Acad Sci USA 1995; 92:10457-10461.
46. Aiello L, Avery R, Arrigg P, et al: Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N Engl J Med 1994; 331:1480-1487.
47. Adamis AP, Miller JW, Bernal MT, et al: Elevated vascular permeability factor/vascular endothelial growth factor levels in the vitreous of eyes with proliferative diabetic retinopathy. Am J Ophthalmol 1994; 118:445-450.
48. Malecaze F, Clamens S, Simorre-Pinatel V, et al: Detection of vascular endothelial growth factor messenger RNA and vascular endothelial growth factor-like activity in proliferative diabetic retinopathy. Arch Ophthalmol 1994; 112:1476-1482.
49. Tolentino M, Miller J, Gragoudas E, et al: Vascular endothelial growth factor is suf-cient to produce iris neovascularization and neovascular glaucoma in a nonhuman primate. Arch Ophthalmol 1996; 114:964-970.
50. Okamoto N, Tobe T, Hackett S, et al: Transgenic mice with increased expression of vascular endothelial growth factor in the retina: a new model of intraretinal and subretinal neovascularization. Am J Pathol 1997; 151:281-291.
50a. Meier M, King GL: Protein kinase C activation and its pharmacological inhibition in vascular disease. Vascular Med 2000; 5:173-185.
50b. Williams B: Factors regulating the expression of vascular permeability/vascular endothelial growth factor by human vascular tissues. Diabetologia 1997; 40:S118-S120.
50c. Ishii H, Jirousek MR, Koya D, et al: Amerlioration of vascular dysfunctions in diabetic rats by an oral PKC inhibitor. Science 1996; 272:728-731.
50d. Aiello LP, Bursell SE, Clermont A, et al: Vascular endothelial growth factor-induced retinal permeability is mediated by protein kinase C in vivo and suppressed by an orally effective beta-isoform-selective inhibitor. Diabetes 1997; 46:1473-1480.
50e. Suzuma K, Takahara N, Suzuma I, et al: Characterization of protein kinase C isoform's action on retinoblastoma protein phosphorylation, vascular endothelial growth factor-induced endothelial cell proliferation, and retinal neovascularization. Proc Natl Acad Sci USA 2002; 99:721-726.
51. Tagawa H, McMeel J, Furukawa H, et al: Role of the vitreous in diabetic retinopathy. I. Vitreous changes in diabetic retinopathy and in physiologic aging. Ophthalmology 1986; 93:596-601.
52. Foos R, Kreiger A, Forsythe A, et al: Posterior vitreous detachment in diabetic subjects. Ophthalmology 1980; 87:122-128.
53. Klein R, Klein B, Moss S, et al: Diabetic retinopathy. II. Prevalence and risk of diabetic retinopathy when age at diagnosis is less than 30 years. Arch Ophthalmol 1984; 105:520-526.
54. Klein R, Klein B, Moss S, et al: The Wisconsin Epidemiologic Study of Diabetic Retinopathy. III. Prevalence and risk of diabetic retinopathy when age at diagnosis is 30 or more years. Arch Ophthalmol 1984; 102:527-532.
55. Aiello L, Rand L, Briones J, et al: Diabetic retinopathy in Joslin Clinic patients with adult-onset diabetes. Ophthalmology 1981; 88:619-623.
56. Janka H, Warram J, Rand L, et al: Risk factors for progression of background retinopathy in long-standing IDDM. Diabetes 1989; 38:460-464.
57. Baker R, Rand L, Krolewski A, et al: Influence of HLA-DR phenotype and myopia on the risk of nonproliferative and proliferative diabetic retinopathy. Am J Ophthalmol 1986; 102:693-700.
58. Rand L, Krolewski A, Aiello L, et al: Multiple factors in the prediction of risk of proliferative diabetic retinopathy. N Engl J Med 1985; 313:1433-1438.
59. Rand L, Krolewski A, Warram J: Late complications: The critical period. In: Friedman E, L'Esperance A, ed. Diabetic Renal-Retinal Syndrome, New York: Grune & Stratton; 1986:3.
60. Orchard T, Dorman J, Maser R, et al: Factors associated with avoidance of severe complications after 25 yr of IDDM. Pittsburgh Epidemiology of Diabetes Complications Study I. Diabetes Care 1990; 13:741-747.
61. Kroc Collaborative Study Group : Blood glucose control and the evolution of diabetic retinopathy and albuminuria: A preliminary multicenter trial. N Engl J Med 1984; 311:365-372.
62. Dahl-Jorgensen K, Brinchmann-Hanses O, Hanssen K, et al: Effect of near normoglycemia for two years on progression of early diabetic retinopathy, nephropathy, and neuropathy: The Oslo Study. BMJ 1986; 293:1195-1199.
63. The DCCT Research Group : Diabetes Control and Complications Trial (DCCT): Results of feasibility study. Diabetes Care 1987; 10:1-19.
64. Rosenlund E, Hasskens K, Brinchmann-Hanses O, et al: Transient proliferative diabetic retinopathy during intensi-ed insulin treatment. Am J Ophthalmol 1988; 105:618-625.
65. Dandona P, Bolger J, Boag F, et al: Rapid development and progression of proliferative retinopathy after strict diabetic control. BMJ 1985; 290:895-896.
66. Zinman B: The physiologic replacement of insulin, an elusive goal. N Engl J Med 1989; 321:363-370.
67. The Diabetes Control and Complications Trial Research Group : The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993; 329:977-986.
68. The Diabetes Control and Complications Trial Research Group : Progression of retinopathy with intensive versus conventional treatment in the Diabetes Control and Complications Trial. Ophthalmology 1995; 102:647-661.
69. Cheng H, Franklin S: Treatment of cataract in diabetics with and without retinopathy. Eye 1988; 2:607-614.
70. Jaffe G, Burton T: Progression of nonproliferative diabetic retinopathy following cataract extraction. Arch Ophthalmol 1988; 106:745-749.
71. Benson W, Brown G, Tasman W, et al: Extracapsular cataract extraction with placement of a posterior chamber lens in patients with diabetic retinopathy. Ophthalmology 1993; 100:730-738.
72. Sebestyen J: Introcular lenses and diabetes mellitus. Am J Ophthalmol 1986; 101:425-428.
73. Alpar J: Diabetes: Cataract extraction and intraocular lenses. J Cataract Refract Surg 1987; 13:43-46.
74. Aiello L, Wand M, Liang G: Neovascular glaucoma and vitreous hemorrhage following cataract surgery in patients with diabetes mellitus. Ophthalmology 1983; 90:814-820.
75. Hykin P, Gregson R, Stevens J, et al: Extracapsular cataract extraction in proliferative diabetic retinopathy. Ophthalmology 1993; 100:394-399.
76. Lischwe T, Ide C: Predicting visual acuity after cataract surgery using the blue -eld entoptoscope and projected slides. Ophthalmology 1988; 95:256-260.
77. Beetham W: Diabetic retinopathy in pregnancy. Trans Ophthalmol Soc UK 1950; 48:205-216.
78. Rodman H, Singerman LJ, Aiello L, et al: Diabetic retinopathy and its relationship to pregnancy. In: Merkaty T, Adams P, ed. The Diabetic Pregnancy: A Perinatal Perspective, New York: Grune & Stratton; 1979.
79. Laatikainen L, Larinkari J, Teramo K, et al: Occurrence and prognostic signi-cance of retinopathy in diabetic pregnancy. Metab Pediatr Ophthalmol 1980; 4:191-195.
80. Klein B, Moss S, Klein R: Effect of pregnancy on progression of diabetic retinopathy. Diabetes Care 1990; 13:34-40.
81. Laatikainen L, Teramo K, Hieta-Heikeraninen , et al: A controlled study of the influence of continuous subcutaneous insulin infusion treatment on diabetic retinopathy during pregnancy. Acta Med Scand 1987; 221:367-376.
82. Klein B, Klein R, Meur S, et al: Does the severity of diabetic retinopathy predict pregnancy outcome. J Diabetes Complications 1988; 2:179-184.
83. Janka H, Ziegler A, Valsania P, et al: Impact of blood pressure on diabetic retinopathy. Diabetes Metab 1989; 15:333-337.
84. Chase H, Garg S, Jackson W, et al: Blood pressure and retinopathy in type I diabetes. Ophthalmology 1990; 97:155-159.
85. Krolewski A, Canessa M, Warram J, et al: Predisposition to hypertension and susceptibility to renal disease in insulin-dependent diabetes mellitus. N Engl J Med 1988; 318:140-145.
86. Klein R: Recent developments in the understanding and management of diabetic retinopathy. Med Clin North Am 1988; 72:1415-1437.
87. Petersen M, Vine A: The University of Michigan Pancreas Transplant Evaluation Committee: Progression of diabetic retinopathy after pancreas transplantation. Ophthalmology 1990; 97:496-500.
88. Ramsay R, Goetz F, Sutherland D, et al: Progression of diabetic retinopathy after pancreas transplantation for insulin-dependent diabetes mellitus. N Engl J Med 1988; 318:208-214.
89. The Diabetic Retinopathy Study Research Group : Design, methods, and baseline results. Invest Ophthalmol Vis Sci 1981; 21:149-226.
90. Davis M: Proliferative diabetic retinopathy. In: Ryan S, ed. Retina, St Louis: Mosby; 1989:367-402.
91. Early Treatment of Diabetic Retinopathy Study Group : Effects of aspirin treatment on diabetic retinopathy. Ophthalmology 1991; 98:107-120.
92. Charles S: Vitreous microsurgery, Baltimore: Williams & Wilkins; 1981:107-120.
93. Packer A: Vitrectomy for progressive macular traction associated with proliferative diabetic retinopathy. Arch Ophthalmol 1987; 105:1679-1682.
94. Poulsen J: Diabetes and anterior pituitary insuf-ciency. Final course and postmortem study of a diabetic patient with Sheehan's syndrome. Diabetes 1966; 15:73-77.
95. Luft R, Olivecrona H, Ikkos D, et al: Hypophysectomy in man: further experiences in severe diabetes mellitus. BMJ 1955; 2:752-756.
96. Sharp P, Fallon T, Brazier O, et al: Long-term follow-up of patients who underwent yttrium-90 pituitary implantation for treatment of proliferative diabetic retinopathy. Diabetologia 1987; 30:199-207.
97. Beetham W, Aiello L, Balodimos M, et al: Ruby laser photocoagulation of early diabetic neovascular retinopathy. Arch Ophthalmol 1970; 83:261-272.
98. Beetham W: Visual prognosis of proliferating diabetic retinopathy. Br J Ophthalmol 1963; 47:611-619.
98a. Meyer-Schwickerath G, Schott K: Diabetic retinopathy and photocoagulation. Am J Ophthalmol 1968; 66:597-603.
100. Aiello L, Beetham W, Balodimos M, et al: Ruby laser photocoagulation in treatment of diabetic proliferating retinopathy: Preliminary report. In: Goldberg M, Fine S, ed. Symposium on the Treatment of Diabetic Retinopathy, Washington, DC: Public Health Service; 1969:437.
101. Campbell C, Koester C, Curtice V, et al: Clinical studies in laser photocoagulation. Arch Ophthalmol 1965; 74:57-65.
102. The Diabetic Retinopathy Study Research Group : Four risk factors for severe visual loss in diabetic retinopathy. The third report from the DRS. Arch Ophthalmol 1979; 97:654-655.
103. Doft B, Blankenship G: Single versus multiple treatment sessions of argon laser panretinal photocoagulation for proliferative diabetic retinopathy. Ophthalmology 1982; 89:772-779.
104. The Diabetic Retinopathy Study Research Group : Photocoagulation treatment of proliferative diabetic retinopathy. Clinical application of DRS -ndings. Ophthalmology 1981; 88:583-600.
105. The Diabetic Retinopathy Study Research Group : Photocoagulation treatment of proliferative diabetic retinopathy: Relationship of adverse treatment effects to retinopathy severity. Dev Ophthalmol 1981; 2:248-261.
106. Okun E, Johnston G, Boniuk I, et al: Xenon arc photocoagulation of proliferative diabetic retinopathy. a review of 2688 consecutive eyes in the format of the Diabetic Retinopathy Study. Ophthalmology 1984; 91:1458-1463.
107. Plumb A, Swan A, Chignell A, et al: A comparative trial of xenon arc and argon laser photocoagulation in the treatment of proliferative diabetic retinopathy. Br J Ophthalmol 1982; 66:213-218.
108. Blankenship G: A clinical comparison of central and peripheral argon laser panretinal photocoagulation for proliferative diabetic retinopathy. Ophthalmology 1988; 95:170-177.
109. Doft B, Blankenship G: Retinopathy risk factor regression after laser panretinal photocoagulation for proliferative diabetic retinopathy. Ophthalmology 1984; 91:1453-1457.
110. Vine A: The ef-cacy of additional argon laser photocoagulation for persistent, severe proliferative diabetic retinopathy. Ophthalmology 1985; 92:1532-1537.
111. Blankenship G: Red-krypton and blue-green argon panretinal laser photocoagulation for proliferative diabetic retinopathy: A laboratory and clinical comparison. Trans Ophthalmol Soc UK 1986; 134:967-1003.
112. Shea M: Early vitrectomy in proliferative diabetic retinopathy. Arch Ophthalmol 1983; 101:1204-1205.
113. D'Amico D: Diabetic traction retinal detachments threatening the fovea and panretinal argon laser photocoagulation. Semin Ophthalmol 1991; 6:11-18.
114. Early Treatment Diabetic Retinopathy Study Group : Early photocoagulation for diabetic retinopathy. Ophthalmology 1991; 98:766-785.
115. Ferris F: Effect of Scatter Photocoagulation: Type I vs. Type II Diabetes. Vitreoretinal Frontiers. 21st Century, San Francisco: American Academy of Ophthalmology; 1996:93.
116. Blondeau P, Pavan P, Phelps C: Acute pressure elevation following panretinal photocoagulation. Arch Ophthalmol 1981; 99:1239-1241.
117. Lobes L, Bourgon P: Pupillary abnormalities induced by argon laser photocoagulation. Ophthalmology 1985; 92:234-236.
117a. Shimura M, Yasuda K, Nakazawa T, et al: Quantifying alterations of macular thickness before and after panretinal photocoagulation in patients with severe diabetic retinopathy and good vision. Ophthalmology 2003; 110:2386-2394.
118. Pender P, Benson W, Compton H, et al: The effects of panretinal photocoagulation on dark adaptation in diabetics with proliferative retinopathy. Ophthalmology 1981; 88:635-638.
119. Kleiner R, Elman M, Murphy R, et al: Transient severe visual loss after panretinal photocoagulation. Am J Ophthalmol 1988; 106:298-306.
120. Wallow I, Johns K, Barry P, et al: Chorioretinal and choriovitreal neovascularization after photocoagulation for proliferative diabetic retinopathy. Ophthalmology 1985; 92:523-532.
121. Swartz M, Apple D, Creel D: Sudden severe visual loss associated with peripapillary burns during panretinal argon photocoagulation. Br J Ophthalmol 1983; 67:517-519.
122. McCanna R, Chandra S, Stevens T, et al: Argon laser-induced cataract as a complication of retinal photocoagulation. Arch Ophthalmol 1982; 100:1071-1073.
123. Lakhanpal V, Schocket S, Richards R, et al: Photocoagulation-induced lens opacity. Arch Ophthalmol 1982; 100:1068-1070.
124. Machemer R: Vitrectomy: A Pars Plana Approach, New York, Grune & Stratton, 1975.
125. Aaberg T, Abrams G: Changing indications and techniques for vitrectomy in management of complications of diabetic retinopathy. Ophthalmology 1987; 94:775-779.
126. Michels R: Proliferative diabetic retinopathy: pathophysiology of extraretinal complications and principles of vitreous surgery. Retina 1981; 1:1-17.
127. The Diabetic Retinopathy Vitrectomy Study Research Group : Early vitrectomy for severe vitreous hemorrhage in diabetic retinopathy. Arch Ophthalmol 1985; 103:1644-1652.
128. The Diabetic Retinopathy Vitrectomy Study Group : Two-year course of visual acuity in severe proliferative diabetic retinopathy with conventional management. Ophthalmology 1985; 92:492-502.
129. Koenig S, Mieler W, Han D, et al: Combined phacoemulsi-cation, pars plana vitrectomy, and posterior chamber intraocular lens insertion. Arch Ophthalmol 1992; 110:1101-1104.
130. Senn P, Schipper I, Perren B: Combined pars plana vitrectomy, phacoemulsi-cation, and intraocular lens implantation in the capsular bag: a comparison to vitrectomy and subsequent cataract surgery as a two-step procedure. Ophthalmic Surg Lasers 1995; 26:420-428.
131. McCuen BD, Rinkoff J: Silicone oil for progressive ocular neovascularization after failed diabetic vitrectomy. Arch Ophthalmol 1989; 107:677-682.
132. Abrams G, Williams G: 'En bloc' excision of diabetic membranes. Am J Ophthalmol 1987; 103:302-308.
133. Mandelcorn M, Blankenship G, Machemer R: Pars plana vitrectomy for the management of severe diabetic retinopathy. Am J Ophthalmol 1976; 81:561-570.
134. Michels R, Rice T, Tice E: Vitrectomy for diabetic vitreous hemorrhage. Am J Ophthalmol 1983; 95:12-21.
135. Peyman G, Raichand M, Huamonte F, et al: Vitrectomy in 125 eyes with diabetic vitreous hemorrhage. Br J Ophthalmol 1976; 60:752-755.
136. Barrie T, Feretis E, Leaver P, et al: Closed microsurgery for diabetic traction macular detachment. Br J Ophthalmol 1982; 66:754-758.
137. Williams D, Williams G, Hartz A, et al: Results of vitrectomy for diabetic traction retinal detachments using the en bloc excision technique. Ophthalmology 1989; 96:752-758.
138. Aaberg T: Clinical results in vitrectomy for diabetic traction retinal detachment. Am J Ophthalmol 1979; 88:246-253.
139. Hutton W, Bernstein I, Fuller D: Diabetic traction retinal detachment: Factors influencing -nal visual acuity. Ophthalmology 1980; 87:1071-1077.
140. Tolentino F, Freeman H, Tolentino F: Closed vitrectomy in the management of diabetic traction retinal detachment. Ophthalmology 1980; 87:1078-1089.
141. Rice T, Michels R, Rice E: Vitrectomy for diabetic traction retinal detachment involving the macula. Am J Ophthalmol 1983; 95:22-33.
142. Rice T, Michels R, Rice E: Vitrectomy for diabetic rhegmatogenous retinal detachment. Am J Ophthalmol 1983; 95:34-44.
143. Miller S, Shafrin G, Bresnick G, et al: Scleral buckling for diabetic retinal detachments secondary to proliferative diabetic retinopathy. Am J Ophthalmol 1980; 89:103-112.
144. Thompson J, Auer C, de Bustros S, et al: Prognostic indicators of success and failure in vitrectomy for diabetic retinopathy. Ophthalmology 1986; 93:290-295.
145. Blankenship G, Machemer R: Long-term diabetic vitrectomy results: Report of 10-year follow-up. Ophthalmology 1985; 92:503-506.
146. Lewis H, Abrams G, Williams G: Anterior hyaoidal -brovascular proliferation after diabetic vitrectomy. Am J Ophthalmol 1987; 104:607-613.
147. Lewis H, Abrams G, Foos R: Clinicopathologic -ndings in anterior hyaloidal -brovascular proliferation after diabetic vitrectomy. Am J Ophthalmol 1987; 104:614-618.
148. Jager RD, Aiello LP, Patel SC, et al: Risks of intravitreous injection: a comprehensive review. Retina 2004; 24:676-698.
149. Aiello LP, Brucker AJ, Chang S, et al: Evolving guidelines for intravitreous injections. Retina 2004; 24:S3-S19.
150. Bandello F, Polito A, Pognuz DR, et al: Triamcinolone as adjunctive treatment to laser panretinal photocoagulation for proliferative diabetic retinopathy. Arch Ophthalmol 2006; 124:643-650.
151. Jonas JB, Sofker A, Degenring R: Intravitreal triamcinolone acetonide as an additional tool in pars plana vitrectomy for proliferative diabetic retinopathy. Eur J Ophthalmol 2003; 13:468-473.
152. Oshima Y, Sakaguchi H, Gomi F, et al: Regression of iris neovascularization after intravitreal injection of bevacizumab in patients with proliferative diabetic retinopathy. Am J Ophthalmol 2006; 142:155-158.
153. Spaide RF, Fisher YL: Intravitreal bevacizumab (Avastin) treatment of proliferative diabetic retinopathy complicated by vitreous hemorrhage. Retina 2006; 26:275-278.
154. Adamis AP, Altaweel M, Bressler NM, et al: Macugen Diabetic Retinopathy Study Group, Changes in retinal neovascularization after pegaptanib (Macugen) therapy in diabetic individuals. Ophthalmology 2006; 113:23-28.