Diana V. Do,
Quan Dong Nguyen,
Julia A. Haller
Aneurysmal alterations of the retinal vasculature are a frequent finding in clinical ophthalmic practice. These changes most commonly involve the retinal veins or capillaries and are usually seen as a sequel to diabetes mellitus, venous occlusive disease, sickle-cell disease, or radiation retinopathy. Less commonly, larger aneurysms arise directly from the major retinal arteries. Although mentioned sporadically in the earlier literature,[1,2] the entity currently known as retinal arterial macroaneurysms was formally described in 1973 by Robertson.[2]
DEFINITION AND DESCRIPTION
Retinal arterial macroaneurysms may be defined as fusiform or saccular dilatations of the retinal arteries, usually arising within the first three orders of bifurcation. Their diameter exceeds 100 ?m (arbitrarily the upper limit of typical microaneurysms) but generally is not greater than ?250 ?m. Although most cases are unilateral, 10% of patients have bilateral disease. Multiple aneurysms occur in ?20% of affected eyes and usually involve different arteries in the same eye. Patients may also present with multiple aneurysms along the same artery. The most commonly reported site of involvement is along the superotemporal arcade because individuals with aneurysms at this location are more likely to have visual symptoms.[2a] Rarely, macroaneurysms can occur directly on the optic nervehead[3-5] or arise from a cilioretinal artery.[6,7] They often occur at bifurcation sites and at arteriovenous crossings and have been seen to develop in vessels with a documented history of embolic damage.[7-9] Approximately 10% of macroaneurysms are pulsatile on initial presentation, but the literature is discordant as to whether this is a sign of impending rupture.[10-12]
EPIDEMIOLOGY
The typical patient presenting with a macroaneurysm is a woman, greater than 60 years of age, with an established history of systemic hypertension. The female preponderance is on the order of 3:1.[2,10,11]Approximately 75% of patients have a history of hypertension. Hypertension and arteriosclerotic vascular disease are the only consistent disease associations in patients harboring macroaneurysms.
FUNDUS APPEARANCE
The presentation of a patient with a macroaneurysm is variable. Retinal arterial macroaneurysms can be found on routine examination in asymptomatic patients. Sudden, severe visual loss may result from rupture of the aneurysm and resultant hemorrhage into the subretinal space, the subinternal limiting membrane space, the retrohyaloid space, or the vitreous (Fig. 138.1). Hemorrhage can also occur within the retina. Often a typical 'hourglass hemorrhage' occurs, consisting of simultaneous subretinal and preretinal collections of blood. Serous fluid can collect within the retina, producing diffuse, focal, or cystoid macular edema, or it can accumulate in the subretinal space, detaching the macula and producing a gradual diminution in visual acuity. Lipid exudates can also cause a gradual decrease in vision by migrating into the macula (Fig. 138.2).
|
|
|
|
FIGURE 138.1 Large hemorrhage obscures the macroaneurysm. |
|
|
|
|
FIGURE 138.2 (a and b) Peripherally located aneurysm with lipid exudate involving the fovea. |
Secondary epiretinal membranes may form as subhyaloid or subinternal limiting membrane hemorrhage resorbs, and these can cause persistent decreased visual acuity even after the macroaneurysm itself and bleeding/exudate caused by it have resolved. If the macroaneurysm is large and occurs at an arteriovenous crossing, a branch retinal vein occlusion may be produced secondarily, and symptoms may result from manifestations of the vein occlusion or from the macroaneurysm, or both.
ANGIOGRAPHIC FINDINGS
The most common fluorescein angiographic appearance of a macroaneurysm is uniform filling during the early arterial phase of the angiogram. Partial filling may occur if the aneurysm is spontaneously involuting or is partially thrombosed (Fig. 138.3). The late phase of the fluorescein angiogram may reveal leakage from the macroaneurysm or staining of the vessel wall. The involved artery is typically patent but may be narrowed proximal and distal to the macroaneurysm, although obliteration of the distal portion of the artery has been reported.[13] The area surrounding the macroaneurysm often shows capillary microaneurysms and nonperfusion, intraretinal microvascular abnormalities, telangiectasis, and fluorescein dye leakage.
|
|
|
|
FIGURE 138.3 Fluorescein angiogram shows rapid, incomplete filling of the macroaneurysm, which is consistent with partial thrombosis. |
Occasionally, fluorescein angiography may not demonstrate a macroaneurysm because of blockage by overlying hemorrhage. A high index of suspicion combined with serial examinations and angiography as the hemorrhage clears will result in an accurate diagnosis. When hemorrhage prevents view of underlying structures, indocyanine green angiography may be useful in viewing the macroaneurysm because the absorption and emission spectra of indocyanine green are in the near-infrared range, and the dye can often be seen through hemorrhage, allowing views of structures that would otherwise be obscured. A retrospective case series using indocyanine green angiography in eyes with dense preretinal and subretinal hemorrhages demonstrated that indocyanine green angiography could correctly diagnose retinal macroaneurysms as the cause of hemorrhage when fluorescein angiography was inconclusive.[13a]
PATHOGENESIS AND PATHOLOGIC APPEARANCE
The exact pathogenetic mechanism of macroaneurysm formation is uncertain. However, several observations and associations have led investigators to at least three hypotheses - focal damage to the blood vessel wall, chronic hypertensive vascular damage, and inherent structural defects in blood vessels.
Lewis and colleagues[9] observed a patient who developed macroaneurysm at the site of a documented incomplete embolic occlusion of a retinal artery. The authors postulated that embolic injury results in focal damage to the blood vessel wall, causing weakening of the wall and subsequent aneurysm formation. Wiznia[7] reported a macroaneurysm occurring in a cilioretinal artery after an embolic occlusion of the artery. Ohga and associates[14] described a case of a macroaneurysm in an artery that crossed over a toxoplasmosis scar. Periarteritis from the toxoplasmic inflammation may have caused structural damage that weakened the arterial wall and caused an aneurysm to form. The role of previous vascular damage was also suggested by the study of Panton and co-workers.[14a] They noted a high concordance rate between the location of macroaneurysms and that of branch retinal vein occlusions when these occurred in the same eye. Macroaneurysms occurred 12 times more often in the quadrant served by the affected vein than elsewhere. In two eyes, the branch vein occlusion was known to have preceded development of the macroaneurysm.
Retinal arterial macroaneurysms have been noted to be similar to intracerebral miliary aneurysms seen in elderly hypertensive patients, especially women.[2,11] Since hypertension is commonly associated with retinal arterial macroaneurysms, it is believed that chronic vascular wall damage caused by hypertension and associated arteriosclerotic changes predispose the vessels to focal dilatation in the presence of continued increased intraluminal pressure.
Lavin and colleagues[11] noted that at the point of arteriovenous crossing, there is no adventitia and the two blood vessels share a common coat. The arterial wall thus has less support at these locations, and with increased intraluminal pressure in the hypertensive patient, ectasia of the arterial wall may result.
After development of the macroaneurysm, symptoms are produced by leakage through the thinned wall of the lesion as well as from the surrounding microvascular alterations that are usually present. Histopathologically, actual aneurysmal sites show thickening of the arterial walls secondary to a fibrin-laminated clot accompanied by hypertrophy of the muscular layer. A thrombus will often partially or entirely fill the macroaneurysm. Thickened, hyalinized arterial walls are common in adjacent arterioles. The areas surrounding the macroaneurysm, clinically noted to show microvascular changes such as capillary loss, telangiectasias, and products of vascular leakage, typically show corroborating histologic findings including dilatation of the capillary bed, hemorrhage, lipid, edema, and photoreceptor degeneration.[14b]
NATURAL HISTORY
The natural history of macroaneurysms varies and is dependent on the clinical presentation. In some patients with hemorrhage and no involvement of the macula, the visual acuity is not affected and the hemorrhage can resolve without any adverse effects (Fig. 138.4).
|
|
|
|
FIGURE 138.4 (a) Subretinal hemorrhage not involving the fovea. (b) Same eye as in (a) 6 weeks later without treatment. |
Abdel-Khalek and Richardson[10] reported the natural history of 18 cases of macroaneurysm, segregating them by clinical presentation into acute and chronic decompensation. Acute decompensation was typified by hemorrhage into the retina, subretinal space, subhyaloid space, or vitreous, and it produced sudden visual loss. Chronic decompensation was characterized by more gradual visual loss from the accumulation of macular edema and lipid exudate.
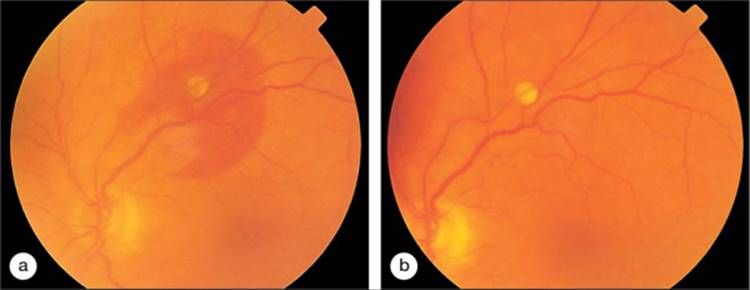
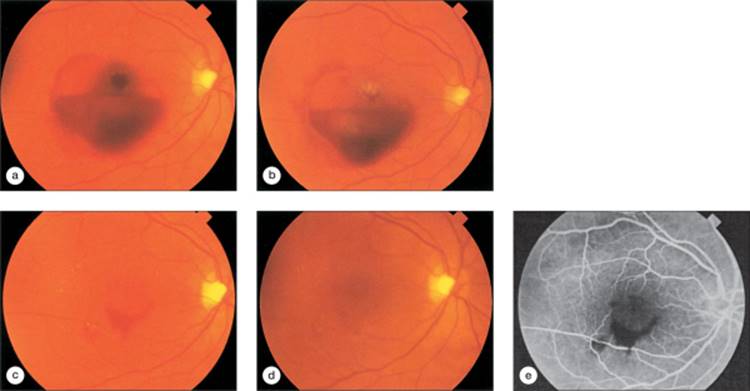
After presumed aneurysmal rupture associated with the acute decompensation category, several pathways were followed. In some subjects, the arterial perforation closed, leaving an intact aneurysm that could rebleed or continue to leak fluid and exudate. Other aneurysms spontaneously closed, forming Z-shaped kinks at the former aneurysm site (Fig. 138.5). Subjects with only an intraretinal hemorrhage often experienced a yellow-gray, saddle-shaped plaque centered on the macroaneurysm, with surrounding exudate. The involved arteriole often became heavily sheathed.
|
|
|
|
FIGURE 138.5 Spontaneous closure of the macroaneurysm seen in Figure 138.1. (a) At 6 days. (b) At 20 days. (c) At 42 days. (d) At close to 6 months after Figure 138.1. (e) Fluorescein angiogram shows kinks at the former aneurysm site. |
In the group of patients with chronic decompensation, several macroaneurysms were treated with photocoagulation because edema and lipid exudate had already involved the central macular area and caused decreased visual acuity. In five subjects in whom macular function was not threatened, no treatment was undertaken. None of these cases ever progressed to involve the macula, although only one spontaneously closed during the study.
After closure of these chronically decompensating aneurysms, either spontaneously or as a result of photocoagulation, kinking occurred at the aneurysmal site. Arteriolar constriction also occurred, usually proximal but occasionally distal to the macroaneurysm site. Arterial sheathing distal to the macroaneurysm was commonly seen, but distal arterial closure was rare, even after therapy.
These authors reported a relatively good visual prognosis with macroaneurysms presenting with acute hemorrhage, as have some other investigators.[11,12] Of the eight patients in this category, only two patients had a final visual acuity of 6/18 or worse.[10] The remaining six patients had visual acuity of 6/12 or better. Of the patients with chronic aneurysmal decompensation, one patient had visual acuity of 6/60, two patients had visual acuity of 6/36, and one patient had visual acuity of 6/18, with only six patients arriving at visual acuity of 6/12 or better. These authors concluded that acute hemorrhage infrequently leads to marked decreases in visual acuity, whereas chronic macular edema and exudate commonly lead to a poorer visual outcome.
Palestine and associates[12] investigated the natural course of macroaneurysms using a similar strategy. They divided their patients into three groups. Group A included eyes with hemorrhage, exudate, edema, or the macroaneurysm within the vascular arcades, accompanied by decreased visual acuity. Group B included eyes with hemorrhage, exudate, edema, or the macroaneurysm within the arcades, but without an effect on visual acuity. Group C included eyes in which all the pathologic features were peripheral to the vascular arcades. These investigators concluded that eyes in group A could do poorly and that the prognosis was variable. Eyes in group B did better but needed to be observed periodically to be certain they did not convert to the group A type of eyes. Group C eyes typically did well without therapy. These investigators also noted that eyes presenting with acute vitreous or subinternal limiting membrane hemorrhage tended to do well.
Cleary and co-workers[13] reviewed the natural history of macroaneurysms in 20 patients. They observed that the macroaneurysms almost always closed spontaneously after acute hemorrhage, whereas the lesions rarely did so when macular edema was the presenting pathologic condition. The authors concluded that the prognosis was good in patients presenting with hemorrhage and poorer in those presenting with macular edema. Both the degree of chronicity and the severity of the macular edema affected the prognosis.
McCabe and associates reviewed 41 patients who presented with macular hemorrhage secondary to macroaneurysms and were managed with observation.[15] After an average follow-up of 15.7 months, a visual acuity of 20/40 was achieved in 37%, between 20/50 and 20/100 in 29%, and 20/200 or worse in 34%. Poorer visual acuity outcomes were associated with macular pigmentary changes after resorption of blood.
More recently, Yang and colleagues conducted a retrospective review of arterial macroaneurysms followed at their institution over a 17-year period.[16] The authors classified the 31 patients in their study as having either predominantly hemorrhagic or exudative macroaneurysms. Eyes with hemorrhagic lesions had a greater improvement in vision after resolution of the blood compared to eyes in the exudative cohort, and foveal exudate was a statistically significant risk factor for final visual acuity equal to or worse than 6/30.
Although arterial closure is not a common occurrence, some investigators have described a significant number in their case series. Panton and co-workers[14a] reported an 8% rate of branch retinal artery occlusion in untreated cases of macroaneurysm and a 16% incidence after treatment. There has been at least one other case report of spontaneous branch retinal artery occlusion.[17]
As already noted, a question has been raised in the literature regarding the significance of pulsation of the macroaneurysm. Some investigators consider this a sign of imminent rupture,[10,18,19] although others believe that it has no relationship to eventual rupture and that there are no reliable signs of impending rupture.[11]
DIFFERENTIAL DIAGNOSIS
In cases uncomplicated by a poor view of the fundus, the diagnosis of retinal arterial macroaneurysm is easily established. Often, however, the true nature of the pathologic condition is obscured by hemorrhage, whether in the vitreous, on the surface of the retina, or within the retina itself. A typical hourglass type of hemorrhage should alert the clinician to the possibility of a macroaneurysm. In addition, several entities closely resemble retinal arterial macroaneurysms and are not always easily distinguishable. Spalter[20] called retinal arterial macroaneurysms another 'masquerade' syndrome.
Microaneurysms such as those occurring secondary to diabetes mellitus, radiation retinopathy, sickle-cell disease, and branch retinal vein occlusion are usually not confused with retinal arterial macroaneurysms. They are smaller and the nature of the underlying disease is often well established.
Schulman and colleagues[21] described large capillary macroaneurysms occurring secondary to retinal venous obstructive disease. These were similar in size to macroaneurysms but originated from the venous side of the capillary bed. They caused decreased visual acuity as a result of macular edema and exudate as well as serous elevation of the macula, mechanisms shared in common with retinal arterial macroaneurysms. Parodi and co-workers[22] reported multiple 150-300 ?m capillary macroaneurysms in an eye with central retinal vein occlusion.
A variety of macroaneurysms has been reported after branch retinal vein occlusion.[23,24] Cousins and associates[24] reviewed the photographs and fluorescein angiograms of patients who participated in the Collaborative Branch Vein Occlusion Study through the Bascom Palmer Eye Institute. They noted that four types of macroaneurysm could be seen after branch retinal vein occlusion. Typical retinal arterial macroaneurysms, indistinguishable from the idiopathic variety, were common and occurred within the zone of the branch retinal vein occlusion. Venous macroaneurysms were similar in size but slower to fill angiographically because they occurred along the obstructed vein. Capillary aneurysms were also seen, similar to those reported by Schulman and colleagues.[21] Finally, they described a new type of macroaneurysm that they called the collateral-associated macroaneurysm. These were associated with clearly identifiable dilated collateral vessels on fluorescein angiography. All four types of these macroaneurysms were associated with intraretinal lipid or hemorrhagic exudation, often involving the macula. On fluorescein angiography, the macroaneurysms were typically found to be present in areas of capillary nonperfusion. Eighty-four percent of these eyes were classified as having severe nonperfusion according to the criteria of the Branch Vein Occlusion Study.
There has been one case report of a spontaneous venous macroaneurysm occurring without an antecedent vein occlusion. Brourman and colleagues[25] described a macroaneurysm of the proximal superotemporal vein in a patient with pericarditis. They suggested that increased venous pressure may have been a causative factor.
Branch retinal vein occlusions have been reported to masquerade as retinal arterial macroaneurysms; this is known as the Bonnet sign.[26] The classic Bonnet sign consists of intraretinal hemorrhage at an arteriovenous crossing simulating a macroaneurysm.
There is one report of a retinal arterial macroaneurysm presenting as a mass lesion of the optic nerve; only with serial follow-up was the proper diagnosis ultimately made.[3] There has been one case report of Valsalva's retinopathy occurring as the result of a ruptured retinal arterial macroaneurysm.[27]
Before retinal arterial macroaneurysms became a familiar clinical entity, they were commonly confused with retinal telangiectasis, Leber's miliary aneurysms, or Coats' disease. These patients have unilateral disease consisting of multiple telangiectatic vessels in the midperiphery, predominantly on the venous side of the circulation and usually present in childhood, often with massive exudation including exudative retinal detachment.
von Hippel's angiomatosis usually shows a distinct genetic component. When small, the angiomas may be confused with macroaneurysms, but when well developed, they are typically much larger and accompanied by large, tortuous feeder and draining vessels. Similar-sized retinal angiomas may occur unassociated with von Hippel's disease; they do not have prominent feeder and drainage vessels unless the tumors become quite large.
A common presenting situation is that of an elderly patient with an acute subretinal hemorrhage in the macula. There is often a surrounding area of subretinal lipid exudate, and the appearance can closely mimic neovascular age-related macular degeneration. The macroaneurysm may be obscured by the retinal hemorrhage. A high index of suspicion and careful examination of the fellow eye, coupled with indocyanine green angiography may lead to the proper diagnosis, confirmed after hemorrhage resolution.
Since ?10% of retinal arterial macroaneurysms present with vitreous hemorrhage, this diagnosis must be suspected when no retinal detachment, retinal tear, or avulsed retinal vessel is found after the vitreous hemorrhage clears. The retinal arterial macroaneurysm may involute before adequate fundus viewing and leave only subtle telltale signs of its presence as the cause of the vitreous hemorrhage.
If large subretinal or subretinal pigment epithelial hemorrhage occurs, this presentation may be mistaken for a choroidal melanoma (Fig. 138.6).
|
|
|
|
FIGURE 138.6 Patient with a large subretinal and subpigment epithelial hemorrhage referred to as a choroidal melanoma. (a) At presentation. (b) Fluorescein angiogram at presentation. (c) Appearance 5 months later. |
MANAGEMENT
Although there have been no prospective, randomized clinical trials involving laser photocoagulation treatment of retinal arterial macroaneurysms, empirical treatment guidelines have been established by numerous investigators. Many investigators apply laser photocoagulation directly to macroaneurysms associated with exudates, macular edema, and visual acuity decrease. Although advances in vitreous surgery and the development of adjunctive pharmacologic agents have made the removal of submacular hemorrhage technically feasible, and good results with this strategy have been reported, the usefulness of surgical intervention has not been established as yet. Natural history studies suggest that spontaneous resorption of blood usually occurs with relatively good visual outcomes.[28-33]
Most authorities agree that a quiet macroaneurysm that is asymptomatic without visible leakage should not be treated but should continue to be monitored until spontaneous fibrosis occurs. Ghost macroaneurysms (i.e., those that are already spontaneously fibrosed and show the kinked-vessel Z-sign or the saddle-shaped plaque) also should not be treated, as they have run their natural course and will remain quiescent. Similarly, macroaneurysms that have ruptured and bled acutely rarely rebleed,[34] so observation is adequate in these cases. Aneurysms that leak fluid or exudate, or both, and threaten to involve or already involve the central macula should be considered for therapy (Fig. 138.7). Treatment has been shown to shorten the duration of macroaneurysm patency.[11] The duration of the hemorrhage and exudate as well as its severity will determine the ultimate visual outcome.
|
|
|
|
FIGURE 138.7 Treatment algorithm for retinal arterial macroaneurysm. |
Abdel-Khalek and Richardson[10] treated macroaneurysms with direct photocoagulation using the argon laser and xenon arc. Two of their patients also received perianeurysmal treatment preceding the direct treatment. No bleeding or complications occurred from the direct therapy. The macroaneurysms were closed in all cases. Some investigators recommend treatment to be undertaken early in the course of the disease because the longer the edema and exudate are present, the less the chance of improving the visual acuity and preventing permanent macular damage. Closure of the macroaneurysm has been shown to enhance the rate of resorption of retinal exudate,[9] although the exudate may initially appear to worsen or increase because of more rapid and selective resorption of retinal edema fluid, which may cause further precipitation of lipid exudate.
Palestine and associates[12] treated several eyes with macroaneurysms that had produced macular edema and exudate. They specifically advised against treating the aneurysm or the artery directly because of the possibility of rupture of the aneurysm, although they acknowledged that this complication had not been reported. These investigators, as did Lewis and colleagues,[9] treated the area of the microvascular changes surrounding the aneurysm and found that this predictably produced involution of the aneurysm. They also noted an early increase in lipid exudation, as less protein-rich fluid was initially resorbed. Complete resolution of the exudate took several months.
Lavin and colleagues[11] treated hemorrhagic and exudative macroaneurysms when the macula was involved, with a combination of direct and perianeurysmal techniques using the argon laser. They achieved closure of the macroaneurysms without complications and again noted that the visual prognosis depended on the degree of intraretinal hemorrhage and exudate in the central macula.
Joondeph and co-workers[35] treated macroaneurysms using the yellow dye laser. They used a technique of partially overlapping burns applied to just the peripheral margin of the macroaneurysm, sparing the feeding and draining arterioles. They successfully closed all the macroaneurysms in one treatment and reported no complications of therapy.
Mainster and Whitacre[36] also used the yellow dye laser with a similar technique to successfully close five macroaneurysms. They also reported no complications. However, Russell and Folk,[37] after having successfully treated 15 macroaneurysms with the argon laser, used the yellow dye laser on one patient and immediately produced a branch retinal artery occlusion after applying only four burns to the macroaneurysm. Their treatment technique was not well described but appeared to involve a more direct treatment to the macroaneurysm than did either of the previous two reports involving the yellow dye laser.
Recent work by Brown and associates[38] suggested that direct laser treatment of macroaneurysms may be harmful and, in their study, it involved a significant risk factor for poor visual outcome. In a retrospective study, they compared the long-term visual outcome between patients treated with direct laser photocoagulation and untreated patients. They treated eight eyes with argon green and eight eyes with yellow dye lasers. Even when statistically controlling for the effect of subfoveal hemorrhage and subfoveal lipid, laser photocoagulation remained the strongest predictor for final visual acuity of less than 20/80. They noted four cases of branch retinal artery occlusion, at least two of which led to further foveal capillary dropout and subsequent decreased visual acuity. They suggested that indirect treatment may lower the complication rate and show better results.
Panton and co-workers[14a] observed a 16% rate of branch retinal artery occlusion after laser photocoagulation, but noted that none occurred with exclusively perianeurysmal treatment. They also acknowledged that other investigators believed that direct treatment was riskier and more likely to cause arterial closure than were indirect techniques.
Chaum and colleagues reported the development of retinochoroidal anastomoses and choroidal neovascularization (CNV) in one patient after applying laser photocoagulation directly to a macroaneurysm.[38a] Although the CNV was not located directly beneath the site of the photocoagulation, the authors hypothesize that the laser treatment induced changes in the blood flow in the macula which induced retinochoroidal anastomoses formation and CNV.
These aforementioned treatment techniques are routinely used for managing the vision-threatening consequences of macroaneurysms. Ancillary techniques have been reported. Tassignon and colleagues[39]used a Q-switched neodymium:yttrium- aluminum garnet laser to release a retrohyaloid hemorrhage resulting from a ruptured macroaneurysm, thus facilitating more rapid resorption of the blood than would have occurred spontaneously. Raymond[40] reported two cases in which subinternal limiting membrane hemorrhage from macroaneurysms was liberated into the vitreous with the same type of laser.
Subfoveal hemorrhage, whether from a macroaneurysm or associated with other pathology, has traditionally been believed to have a uniformly poor prognosis for visual acuity. Advances in vitrectomy surgery have attempted to address this problem. Hanscom and Diddie[28] first reported drainage of submacular hemorrhage resulting from ruptured retinal arterial macroaneurysms in 1987. There have been numerous subsequent reports, some of which described the adjunctive use of tissue plasminogen activator to evacuate submacular hemorrhage in this situation.[29-33] None of these reports described more than four eyes with subfoveal hemorrhage. Patients showed improvement from their preoperative visual acuities, but it has yet to be determined whether this aggressive approach improves on the natural history, even for this serious presentation of macroaneurysms. There can be significant and sometimes marked improvement in vision even without treatment, although natural history data are scant. Berrocal and associates[41] studied variations in the clinical course of subfoveal hemorrhages. Two of their patients had hemorrhage due to macroaneurysms. One did poorly, but the other recovered to 20/30 from an initial vision of 5/200. The authors recently observed a case of subretinal hemorrhage extending beneath the fovea to cause counting fingers visual acuity with eventual spontaneous recovery to 20/40 (Fig. 138.8).
|
|
|
|
FIGURE 138.8 Patient with subretinal hemorrhage extending into the fovea. (a) Vision is counting fingers. (b) Early resorption of hemorrhage. (c) Vision is 20/40 10 weeks after (a). |
Although vitreous hemorrhage from macroaneurysms typically clears rapidly, pars plana vitrectomy surgery is effective for the occasional case of dense, nonclearing vitreous hemorrhage.[33]
SUMMARY
Retinal arterial macroaneurysms are a well-defined retinal vascular disorder consisting of saccular or fusiform dilatations of the major retinal arterioles, usually within the first three orders of bifurcation. They usually occur in older, hypertensive women. Diagnosis can sometimes be difficult, and a high index of suspicion is required. Indocyanine green angiography may be helpful in cases where hemorrhage obscures the macroaneurysm. Their natural history is often benign, with many progressing to spontaneous fibrosis and involution with retention of good visual acuity. The visual acuity is decreased as the result of macular involvement with hemorrhage, exudate, edema, or serous detachment or from vitreous or preretinal hemorrhage. Selected patients may be successfully treated using laser photocoagulation, but the visual prognosis cannot be reliably predicted in individual cases.
|
Key Features |
|||||||||||||||
|
REFERENCES
1. Rabb MF, Gagliano DA, Teske MP: Retinal arterial macroaneurysms. Surv Ophthalmol 1988; 33:73.
2. Robertson DM: Macroaneurysms of the retinal arteries. Trans Am Acad Ophthalmol Otolaryngol 1973; 77:OP55.
2a. Moosavi RA, Fong KCS, Chopdar A: Retinal artery macroaneurysms: clinical and fluorescein angiographic features in 34 patients. Eye 2006; 20:1011-1020.
3. Brown GC, Weinstock F: Arterial macroaneurysm on the optic disc presenting as a mass lesion. Ann Ophthalmol 1985; 17:519.
4. Kowal L, Steiner H: Arterial macroaneurysm of the optic disc. Aust N Z J Ophthalmol 1991; 19:75.
5. Iwasawa A, Majima A, Shirai S, et al: Bilateral prepapillary macroaneurysm. Report of a case. Jpn J Ophthalmol 1989; 43:619.
6. Giuffre G, Montalto FP, Amodei G: Development of an isolated retinal macroaneurysm of the cilioretinal artery. Br J Ophthalmol 1987; 71:445.
7. Wiznia RA: Development of a retinal artery macroaneurysm at the site of a previously detected retinal artery embolus. Am J Ophthalmol 1982; 114:642.
8. El-Asrar AMA, Awad A, Tabbara KF: Retinal artery macroaneurysm in a patient with congenital heart disease. Br J Ophthalmol 1993; 77:606.
9. Lewis RA, Norton MH, Wise GN: Acquired arterial macroaneurysms of the retina. Br J Ophthalmol 1976; 60:21.
10. Abdel-Khalek MN, Richardson J: Retinal macroaneurysm: natural history and guidelines for treatment. Br J Ophthalmol 1986; 70:2.
11. Lavin MJ, Marsh RJ, Peart S, et al: Retinal arterial macroaneurysms: a retrospective study of 40 patients. Br J Ophthalmol 1987; 71:817.
12. Palestine AG, Robertson DM, Goldstein BG: Macroaneurysms of the retinal arteries. Am J Ophthalmol 1982; 93:164.
13. Cleary PE, Kohner EM, Hamilton AM, et al: Retinal macroaneurysms. Br J Ophthalmol 1975; 59:355.
13a. Townsend-Pico WA, Meyers SM, Lewis H: Indocyanine green angiography in the diagnosis of retinal arterial macroaneurysms associated with submacular and preretinal hemorrhages: a case series. Am J Ophthalmol 2000; 129:33-37.
14. Ohga H, Egi K, Katayama T, et al: A case of retinal macroaneurysm with congenital ocular toxoplasmosis. Folia Ophthalmol Jpn 1990; 41:898.
14a. Panton RW, Goldberg MF, Farber MD: Retinal arterial macroaneurysms: risk factors and natural history. Br J Ophthalmol 1990; 74:595.
14b. Fichte C, Streeten BW, Friedman AH: A histopathologic study of retinal arterial aneurysms. Am J Ophthalmol 1978; 85:509.
15. McCabe C, Flynn HW, McLean WC, et al: Nonsurgical management of macular hemorrhage secondary to retinal artery macroaneurysms. Arch Ophthalmol 2000; 118:780-785.
16. Yang CS, Tsai DC, Lee FL, Hsu WM: Retinal arterial maacroaneurysms: risk factors of poor visual outcome. Ophthalmologica 2005; 219:366-372.
17. Oo A, Saito Y, Okamoto S, et al: Retinal macroaneurysm and branched retinal artery occlusion. Ther Res 1989; 10:11.
18. Psinakis A, Kokolakis PG, Theodossiadis C, et al: Pulsatile retinal arterial macroaneurysm: treatment with argon laser photocoagulation. J Fr Ophtalmol 1989; 12:673.
19. Yokoi N, Tohsaka S, Yamamoto T: A case of pulsating retinal arterial macroaneurysm. Folia Ophthalmol Jpn 1990; 41:584.
20. Spalter HF: Retinal macroaneurysms: a new masquerade syndrome. Trans Am Ophthalmol Soc 1982; 80:113.
21. Schulman J, Jampol LM, Goldberg MF: Large capillary aneurysms secondary to retinal venous obstruction. Br J Ophthalmol 1981; 65:36.
22. Parodi MB, Bondel E, Ravalico G: Capillary macroaneurysms in central retinal vein occlusion. Ophthalmologica 1995; 209:248.
23. Sanborn GE, Magargal LE: Venous macroaneurysm associated with branch retinal vein obstruction. Ann Ophthalmol 1984; 16:464.
24. Cousins SW, Flynn HW, Clarkson JG: Macroaneurysms associated with retinal branch vein occlusion. Am J Ophthalmol 1990; 109:567.
25. Brourman ND, Goldberg RE, Augsburger JJ, et al: Isolated venous macroaneurysm. Ophthalmic Surg 1990; 21:646.
26. Kimmel AS, Magargal LE, Morrison DL, et al: Temporal branch retinal vein obstruction masquerading as a retinal arterial macroaneurysm: the Bonnet sign. Ann Ophthalmol 1989; 21:251.
27. Avins LR, Krummenacher TK: Valsalva maculopathy due to a retinal arterial macroaneurysm. Ann Ophthalmol 1983; 15:421.
28. Hanscom TA, Diddie KR: Early surgical drainage of macular subretinal hemorrhage. Arch Ophthalmol 1987; 105:1722.
29. Peyman GA, Nelson NC, Alturki W, et al: Tissue plasminogen activating factor assisted removal of subretinal hemorrhage. Ophthalmic Surg 1991; 22:575.
30. Moriarty AP, McAllister IL, Constable IJ: Initial clinical experience with tissue plasminogen activator (tPA) assisted removal of submacular hemorrhage. Eye 1995; 9:582.
31. Lim JI, Drews-Botsch C, Sternberg P, et al: Submacular hemorrhage removal. Ophthalmology 1995; 102:1393.
32. Ibanez HE, Williams DF, Thomas MA, et al: Surgical management of subretinal hemorrhage: a series of 47 consecutive cases. Arch Ophthalmol 1995; 113:62.
33. Brent BD, Gonce M, Diamond JG: Pars plana vitrectomy for complications of retinal arterial macroaneurysms - a case series. Ophthalmic Surg 1993; 24:534.
34. Nadel AJ, Gupta KK: Macroaneurysms of the retinal arteries. Arch Ophthalmol 1976; 94:1092.
35. Joondeph BC, Joondeph HC, Blair NP: Retinal macroaneurysms treated with the yellow dye laser. Retina 1989; 9:187.
36. Mainster MA, Whitacre MM: Dye yellow photocoagulation of retinal arterial macroaneurysms. Am J Ophthalmol 1988; 105:97.
37. Russell SR, Folk JR: Branch retinal artery occlusion after dye yellow photocoagulation of an arterial macroaneurysm. Am J Ophthalmol 1987; 104:186.
38. Brown DM, Sobol WM, Folk JC, et al: Retinal arteriolar macroaneurysms: long term visual outcome. Br J Ophthalmol 1994; 78:534.
38a. Chaum E, Greenwald MA: Retinochoroidal anastomoses and a choroidal neovascular membrane in a macular exudate following treatment for retinal macroaneurysms. Retina 2002; 22:363-366.
39. Tassignon MJ, Stempels N, Van Mulders L: Retrohyaloid premacular hemorrhage treated by q-switched Nd-YAG laser. Graefes Arch Clin Exp Ophthalmol 1989; 227:440.
40. Raymond LA: Neodymium:YAG laser treatment for hemorrhages under the internal limiting membrane and posterior hyaloid face in the macula. Ophthalmology 1995; 102:406.
41. Berrocal MH, Lewis ML, Flynn HW: Variations in the clinical course of submacular hemorrhage. Am J Ophthalmol 1996; 122:486.