Donald J. D'Amico
Giant tears defied as tears extending 90° or more around the circumference of the globe, deserve separate consideration in retinal detachment surgery for several reasons: (1) They often require highly specialized techniques for repair, (2) they may be bilateral, (3) they occur in association with several ocular and systemic conditions, and (4) they have a strong association with the development of proliferative vitreoretinopathy (PVR). Giant tears were first extracted as a specific group by Schepens and associates[1] in 1962, and these authors provided the initial defiition, classification into subgroups, and results with a specialized surgical technique. Since that report, refiements in the defiition have been suggested by others. For example, Norton and colleagues[2] noted that not all 90° or greater tears have a poor prognosis, whereas smaller tears may carry an extremely poor prognosis. They suggested modifying the defiition such that a giant tear was a tear greater than 90° with more than 50% above the horizontal meridian - based on the poorer prognosis with superiorly located giant retinal tears at the time - but this suggested change was not widely adopted. However, many surgeons shared the careful distinction between giant tears and giant dialyses enumerated by Scott.[3] Giant dialyses are a retinal disinsertion at the ora serrata with 90° or more of circumferential extent. These entities differ markedly in pathogenesis, vitreoretinal relationships, and surgical prognosis, and this distinction, undoubtedly obscured in many reports, must be carefully preserved. Similarly, giant tears must be distinguished from giant retinotomies, defied as surgically created retinal incisions extending 90° or greater in circumference.[4] Therefore, giant retinal tears are defied as tears (not dialyses or retinotomies) 90° or greater in circumference. Although the defiition includes several distinct clinical presentations with varied prognosis, it has proved useful because it unites specific surgical challenges and operative techniques.
Giant tears may be considered in relation to their size, location within the eye, configuration, presence of PVR, and cause (Table 185.1 and Figs 185.1 to 185.6). These characteristics have a direct relation to surgical technique for repair as well as visual prognosis. Size is denoted by either degrees of circumferential extent or clock hours, with each clock hour being 30°. Location refers to the primary quadrant or quadrants involved; that is, superior, inferior, temporal, and nasal. Configuration is extremely important and includes the contour of the posterior edge (flat, rolled, or inverted) and the presence of any radial rips-posterior extensions of the tear (see Fig. 185.4), which typically occur at the margins of the tear. Flat giant tears may occur without retinal detachment, and these usually indicate recent origin, whereas posterior rolling or inversion of the posterior aspect of the tear is typical in the later evolution of giant tear detachment. In this regard, distinction from a giant dialysis is crucial.
In a dialysis, vitreous remains attached to the posterior (as well as anterior) aspect of the retinal break, and a posterior vitreous detachment is usually absent. Consequently, the posterior margin of a giant dialysis is restrained by the attachment to the vitreous and prevented from inversion. This anatomy undoubtedly contributes to the excellent prognosis for giant dialyses, which are frequently amenable to buckling or even peripheral cryotherapy or laser alone. Conversely, in a giant tear, the vitreous remains strongly attached to the anterior margin or flap of the tear in a manner analogous to that of a horseshoe tear, and a posterior vitreous detachment is present. The posterior margin of the giant tear, unencumbered by vitreous attachments, is free to move and typically curls toward the disk owing to gravity, intrinsic retinal elasticity, and later development of epiretinal membranes. This results in the characteristic inverted posterior flap of a giant tear. Radial rips may occur at the margins or within the tear and, if substantial in size, may present great difficulties in surgical repair. Finally, a very significant feature is the degree of preoperative PVR that, if present to a substantial degree, has important implications for surgical approach and prognosis (see Fig. 185.6).
TABLE 185.1 -- Classification of Giant Retinal Breaks
|
Giant retinal tear (90° or more) |
|
Extent in degrees (90-360) or clock hours (3-12) |
|
Location (superior, temporal, nasal, inferior) |
|
Configuration |
|
Giant tear without detachment |
|
Giant tear with detachment with |
|
Flat or undisplaced posterior flap |
|
Rolled posterior flap |
|
Inverted posterior flap |
|
Associated with posterior extensions (radial rips) at or within the tear margins |
|
Associated proliferative vitreoretinopathy (absent to severe) |
|
Cause (e.g., spontaneous, trauma, postoperative, systemic syndrome) |
|
Giant dialysis |
|
Giant retinotomy |
|
|
|
|
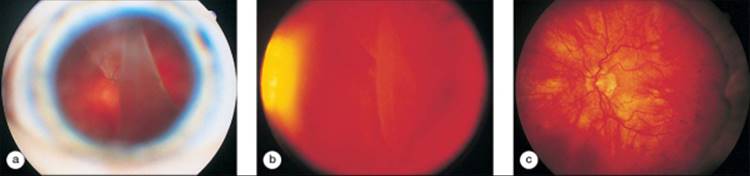
FIGURE 185.1 (a) Wide-angle fundus photograph of a 150° superotemporal giant retinal tear with an inverted posterior edge in the left eye. (b) Posterior pole view of the same eye shows the inverted posterior edge. The macula is shallowly detached, and the visual acuity is counting-figers at 1 ft. (c) After vitrectomy, scleral buckling, and prone air-fluid exchange on a giant tear table, the retina is reattached and acuity is recovered to 20/70. |
|
|
|
|
FIGURE 185.2 (a) Slit-lamp photograph of an aphakic left eye with a 180° giant retinal tear with the posterior edge visible through the pupil. (b) Wide-angle fundus photograph of the same eye. Visual acuity is hand motions. (c) Postoperative photograph after vitrectomy, scleral buckling, and prone air-fluid exchange on a giant tear table. The retina is attached, and visual acuity is 20/100. |
|
|
|
|
FIGURE 185.3 (a) Fundus photograph of a spontaneous 360° giant retinal tear in the left eye of an extremely myopic 13-year-old girl. The inverted retina remains attached only at the disk, and bare retinal pigment epithelium is visible superiorly and at the lower left of the photograph. Visual acuity is hand motions. (b) Fundus photograph of the same eye after two procedures, including an initial vitrectomy, lensectomy, liquid perfluorochemical exchange, and endolaser. The patient developed PVR postoperatively and underwent additional vitrectomy with membrane peeling, retinotomy, and silicone oil exchange. The posterior island of retina is attached, with the margin of endolaser visible just temporal to the macula. Visual acuity is hand motions. (c) Final appearance after one more surgery for epimacular membranes. The retina remains attached, but with severe vascular and optic disk atrophy, and visual acuity remains hand motions. |
|
|
|
|
FIGURE 185.4 Fundus photograph shows a radial rip at the margin of a 120° temporal giant retinal tear. |
|
|
|
|
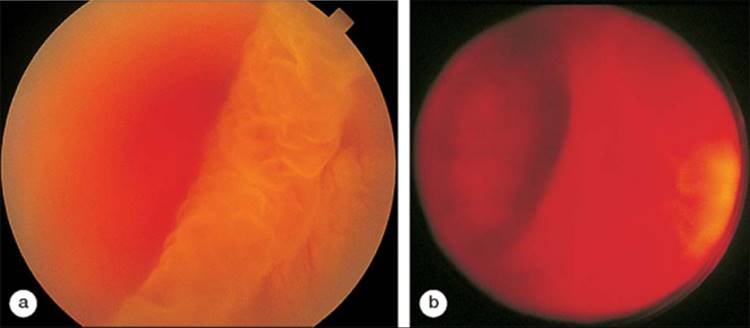
FIGURE 185.5 (a) Fundus photograph of a 150° temporal giant retinal tear in a right eye shows rolling, but not inversion, of the posterior edge. Visual acuity is 20/20. (b) Postoperative view of the same eye after vitrectomy, scleral buckling, liquid perfluorochemical exchange, cryotherapy, endolaser, and sulfur hexafluoride exchange. The lens was not removed; however, cataract developed 1½ years postoperatively. (c) Final postoperative view of the same eye, with the macula remaining attached and visual acuity of 20/20. |
|
|
|
|
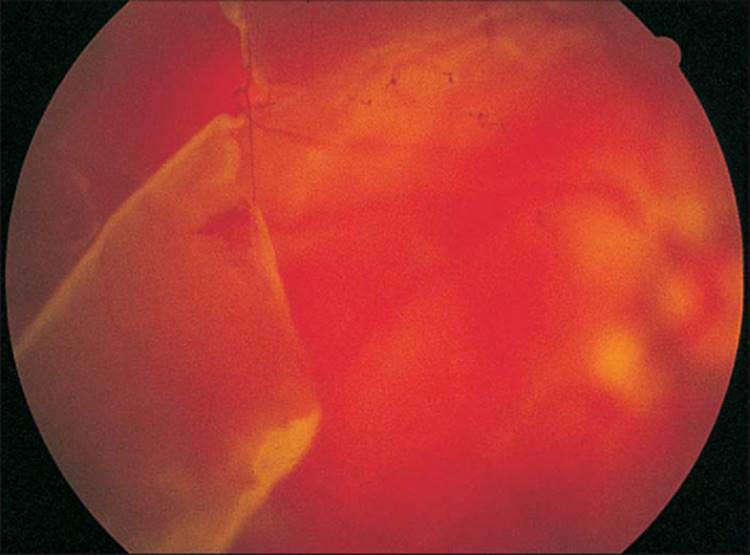
FIGURE 185.6 (a) Fundus photograph a right eye with a 150° giant retinal tear with severe PVR at the initial presentation. The tightly curled posterior edge with membrane-induced folds is shown. (b) Wide-angle view of the same eye displays the giant tear as well as the star folds present in the nasal retina. |
CAUSE
In their initial report, Schepens and associates[1] divided giant tears into four subgroups: traumatic, idiopathic, associated with extensive lattice-like degeneration, and associated with previous heavy treatment with diathermy or photocoagulation. In this series of 125 eyes of 122 patients, 27 eyes (21.6%) were traumatic, 83 (66.4%) idiopathic, 11 (8.8%) were lattice-associated, and 4 (3.2%) were retinopexy-associated. The traumatic category, in retrospect, was enlarged by the inclusion of dialyses as well as giant retinal tears in association with (typically superonasal) vitreous base avulsions. Indeed, a later series of 78 eyes of 66 patients by Schepens and Freeman[5] confirmed the preponderance of idiopathic cases (increased to 78%), males (85%), and younger age at onset (average 35 years). Lattice-associated giant tears were again noted in 10% of eyes, but no retinopexy-associated giant tears were found, perhaps as a result of refiements in the use of barrier diathermy and photocoagulation in retinal surgery. Myopia of any degree was present in approximately one-third of eyes in the later series, indicating a limited role in the pathogenesis of most giant tears.
In a recent series[6] of 162 eyes in 161 patients, most eyes with giant tears had no identifiable predisposition, 25.3% had a history of trauma, and 12.3% were highly myopic. Males represented 76.5% of patients, and 80 patients (49.4%) had undergone previous cataract extraction. Given the recent nature of this series and the typical implantation of a posterior chamber intraocular lens in modern cataract surgery, the fact that 40 (50%) of these patients were aphakic and another 11 had anterior chamber intraocular lenses, it is interesting to speculate that vitreous loss, lens nucleus dislocation, or other complications of cataract surgery may have been predisposing factors accounting for such a high percentage of post-cataract extraction patients in this series. Indeed, attempts to retrieve posteriorly dislocated lens fragments by limbal approaches with forceps, copious irrigation, or deep phacoemulsification at the time of cataract surgery have been recently identified as a predisposing factor for the development of giant retinal tears.[7]
Giant tears have been noted in association with several ocular and systemic conditions. Invariably, these associations worsen the difficulties in diagnosis and repair. Stickler's syndrome, an autosomal dominant connective tissue disease with variable penetrance, includes a marked predisposition to giant retinal breaks and retinal detachment.[8-11] Breaks may occur in posterior or irregular locations. Other ocular features include congenital and progressive high myopia that is typically axial in nature (and is often associated with other features of high myopia, such as fundus hypopigmentation and myopic conus), cataracts in ?50% of patients, anterior chamber and angle abnormalities, and vitreous liquefaction. Systemic manifestations are extensive and include joint, dental, palatal, craniofacial, and hearing abnormalities. Giant retinal tears (including a 360° tear) have been documented in four eyes of three children with aniridia, a spontaneous or autosomal dominant condition associated with cataract, glaucoma, foveal hypoplasia, and other ocular and systemic abnormalities including Wilms' tumor.[12] All eyes were buphthalmic, and although lens subluxation was present in all of these eyes, there was no history of previous ocular surgery, indicating a primary association with aniridia. Eight cases of bilateral giant retinal tear and retinal detachment associated with nasal lens coloboma have been reported.[13] In these eyes, the giant tear was usually in the nasal quadrants, and the retina was successfully reattached in only four of 16 eyes. Other authors have noted giant retinal tears in children with buphthalmos,[14]congenital megalophthalmos syndrome,[15] myopia,[16] and congenital cataract.[17] Reports of retinal detachment in patients with retinitis pigmentosa are rare, but isolated cases with giant retinal tear have been documented.[18, 19]
Marfan's syndrome is a hereditary disorder of connective tissue with autosomal dominant transmission in a majority of cases.[20, 21] Many cases have been found to have a point mutation in the fibrillin gene located in chromosome 15.[21] Patients display a typical marfanoid habitus, in which skeletal and joint abnormalities include arachnodactyly, joint laxity, pectus excavatum, and scoliosis. Cardiovascular system abnormalities include dilatation of the aortic root, with possibly fatal involvement by aortic aneurysm dissection. Ocular manifestations are prominent and include ectopia lentis, myopia, rhegmatogenous retinal detachment, glaucoma, and cataract.[21-23] In a recent series of 18 eyes in Marfan's patients undergoing surgery for retinal detachment, three were noted to have giant retinal tears and were managed with vitrectomy, scleral buckling, cryopexy, and intraocular tamponade with silicone oil or gas.[23] One eye redetached with advanced PVR and lost all light perception, a second had partial redetachment but retained macular attachment with 20/300 acuity, and the fial case was completely reattached with 20/200 acuity after two additional surgeries.
In patients with giant retinal tear, the fellow eye is at considerable risk of retinal breaks, giant breaks, and detachment.[17, 24] In a study of 226 patients with giant tears, 51% developed retinal breaks in the fellow eye, including 13% who developed giant tears.[17] In a subsequent study, pretear changes in the periphery of fellow eyes were noted.[24] These included vitreous condensation, transvitreal membranes, and increasing white with pressure with a sharp posterior border. These fidings led the authors to recommend prophylactic measures such as an encircling scleral buckle and retinopexy for fellow eyes displaying prebreak characteristics. A more recent study has retrospectively evaluated the course of 48 fellow eyes after treatment with 360° cryotherapy to the posterior edge of the vitreous base in association with giant tear surgery in the opposite eye.[25] These 48 eyes were followed for 7 years on average, and displayed an 8% incidence of retinal tears or detachments, typically occurring 18 ± 9 months after cryo prophylaxis. The authors acknowledge the lack of controls in this study, but state that this incidence compares quite favorably with other reports suggesting a considerably worse natural history for fellow eyes. Although the precise indications and benefits of such potential aggressive prophylaxis remain arguable, the need for careful and continued surveillance of the fellow eye is unquestioned.
SURGICAL MANAGEMENT
PREOPERATIVE EVALUATION
The preoperative examination of a patient with giant tear does not depart from the established guidelines for the preoperative evaluation of any patient with a retinal detachment - namely, careful ocular examination with dilated indirect ophthalmoscopy with scleral depression. Notation is made of the extent of the tear, the extent of associated detachment, the mobility of the tear, the degree of inversion of the posterior flap, any radial rips, any additional breaks or areas of lattice, the presence or absence of posterior vitreous detachment, the status of the lens and anterior segment, and most importantly, the presence and degree of PVR. Associated ocular and systemic features are noted, and examination of the fellow eye (and possibly family members as well) is performed. Preoperative studies of giant tear movement with various positions and head movements may in fact cause extension of the tear and have been abandoned.
SURGERY
The elements of giant retinal tear surgery are listed in Table 185.2. As is the case in every area of surgery, many techniqueshave been successfully employed, and the surgical approach for a given case will always contain aspects of an individual surgeon's preference. Nevertheless, it is possible to consider these surgical elements in relation to several distinct giant tear presentations, in some cases guided by detailed, but not randomized, clinical studies.
TABLE 185.2 -- Elements of Giant Retinal Surgery
|
Preoperative examination |
|
Retinopexy |
|
Lens removal in some cases |
|
Vitrectomy, possibly with membrane peeling and retinotomy |
|
Scleral buckling in some cases |
|
Unfolding and repositioning the inverted posterior retinal flap |
|
Tamponade |
|
Postoperative patient positioning and management |
The essence of giant retinal tear surgery is the continued evolution of techniques for unfolding the inverted retinal flap. Numerous surgical approaches have been employed. The original approach included forcible transscleral drainage with intentional retinal incarcerations to secure the flap in association with scleral buckling.[1] The use of an intravitreal air bubble, in association with patient positioning, was an important and relatively early advance.[2] Techniques were described in which the air bubble was used to unfold the break for retinopexy with cryotherapy or diathermy without scleral buckling, as well as injecting intravitreal air preoperatively, intraoperatively, and postoperatively in order to unfold the break onto a scleral buckle.[2, 5, 26-28] Preoperative head positioning and intraoperative jerking of the rectus sutures to rapidly uncurl the flap were also tried with occasional success.[1-3, 5] The introduction of pars plana vitrectomy was of extreme importance, as it not only permitted vastly superior mobilization of the tear but also provided for new and powerful means of direct manipulation and unfolding of the tear intraoperatively.[29, 30] Coupled with face-down positioning on specialized giant tear tables and the preretinal injection of air with the simultaneous removal of intraocular fluid, many retinal tears were able to be reapproximated to the retinal pigment epithelium intraoperatively (Fig. 185.7).
|
|
|
|
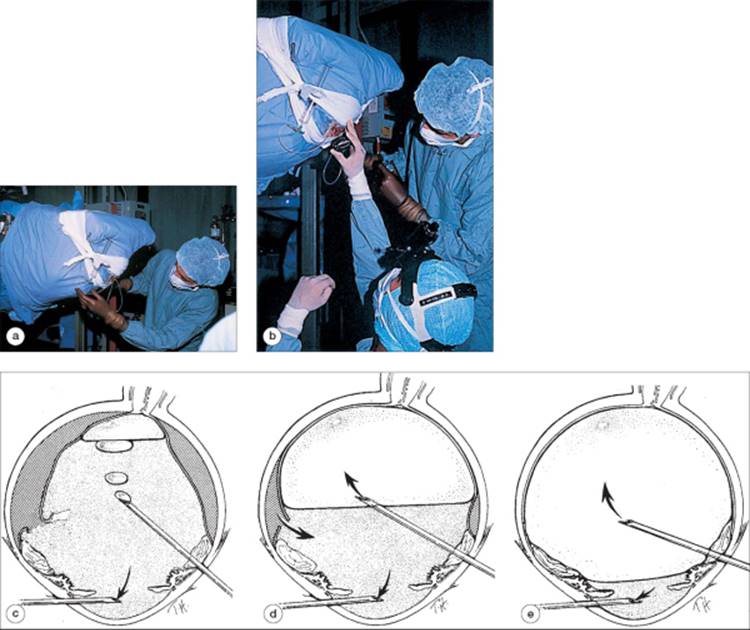
FIGURE 185.7 Prone air-fluid exchange on a specialized giant tear table. (a) Patient is inverted on the table after mobilization of the retina by vitrectomy. The infusion cannula is used for air infusion in this case and is located opposite the center of the tear. It is connected to an air syringe (shown). Alternatively, a needle introduced through the limbus or pars plana may be used. (b) The surgeon evaluates the effectiveness of the exchange in unfolding the inverted posterior retinal flap. (c-e) Schematic drawing of prone air-fluid exchange with air progressively introduced under the disk via the pars plana, with egress of fluid from a second needle in the anterior chamber. |
After the widespread development of vitreous surgery, later techniques attempted to unfold the retina in the supine position, preserving the vitrectomy approach and eliminating the need for specialized giant tear tables. Sutures were passed through the posterior retinal flap, for both mobilization and later securing of the tear to the eye wall.[31-34] Similarly, intraocular tacks were used to return and impale the retinal flap to the periphery.[35-38] Although described with initial enthusiasm, sutures and tacks proved to be cumbersome and unreliable, and they are seldom used now. Incarceration techniques, in which the margin of the posterior flap was fixed in an anterior sclerotomy, were refied by vitreous surgery to include direct grasping of the retinal flap[34] or attached vitreous[39] with intraocular instruments or sutures or incarceration by perforation of the eye wall with penetrating diathermy after reattaching the retina with vitrectomy and prone air-fluid exchange.[40] Hyaluronic acid was injected under the posterior flap after vitreous removal and was used successfully to unroll a 200° giant retinal tear, but the patient developed posterior migration of the tear and recurrent detachment.[41] Hyaluronic acid was tried by other surgeons for unrolling giant tears, but the migration of the substance into the subretinal space and its high cost dampened the initial enthusiasm. A vitrectomy technique employing simultaneous internal subretinal fluid removal and silicone oil injection via the pars plana permitted the intraoperative reattachment of 16 of 17 eyes with giant retinal tears up to 180°.[42] This technique successfully retained the supine position of vitreous surgery, but at some cost owing to long-term difficulties associated with silicone oil tamponade.[42-45]
The introduction of heavier-than-water liquid perfluorochemicals by Chang and co-workers supplanted all of the previous techniques for unrolling and repositioning inverted giant retinal tears (Fig. 185.8).[46]In liquid perfluorochemical technique, a vitrectomy is performed with additional mobilization of the retina by membrane removal if necessary.[6, 46-58] Liquid perfluorochemical (either perfluoro-N-octane or perfluoroperhydrophenanthrene) is then progressively injected through a cannula placed over the surface of the disk, and the flap of the giant tear is reapproximated to the retinal pigment epithelium by continued anterior displacement and removal of subretinal fluid. The reattached retina is then secured with retinopexy, tamponade, and possibly scleral buckling. The power of this elegant technique has greatly simplified giant retinal tear surgery to the point that most cases may be performed in the outpatient surgery suite with the patient under local anesthesia.
|
|
|
|
FIGURE 185.8 (a) Introduction of perfluorooctane into the vitreous cavity. Initial placement is directly above the optic nerve. The perfluorooctane-saline solution interface is easily seen. (b) With the patient in a supine position, gradual filling of the vitreous cavity with heavier-than-water perfluorooctane allows flattening of the detached retina. (c) Completion of the perfluorooctane fill into the vitreous cavity. The retina is completely flat, and the flap of the giant retinal tear is supported on the encircling element. (d) Endophotocoagulation is applied around the edges of the giant retinal tear to induce chorioretinal adhesion. The presence of an encircling element greatly facilitates laser photocoagulation after surgery. (e) Laser indirect ophthalmoscopy can also be used to photocoagulate the retina around the giant retinal tear during and after surgery. (f) A slow, deliberate removal of the perfluorooctane and saline solution is essential to prevent posterior slippage of the retina. |
GIANT TEAR WITHOUT PVR-REPRESENTATIVE TECHNIQUE
Retrobulbar (or, rarely, general) anesthesia is administered. The conjunctiva is opened for 360°, and bridle sutures are passed under the rectus muscles. The eye is reexamined by indirect ophthalmoscopy, and any changes from the preoperative examination are noted carefully. If retinopexy with cryopexy is to be performed, it is done at this time and care is taken to ensure adequate coverage beyond the margins of the tear as well as posteriorly, particularly at the center of the tear. If a scleral buckle is to be placed, sutures may be passed at this time or just after the vitrectomy. A pars plana infusion cannula is secured to the globe, and a pars plana vitrectomy is performed with careful trimming of the peripheral vitreous; this may require gentle indentation of the globe with a cotton-tipped applicator or muscle hook, and some surgeons prefer to do the entire case with a panoramic visualization system. Some surgeons also prefer to remove the lens. After vitreous removal, the giant tear will be fully mobile. If used, an encircling buckling element such as a band or smaller tire is threaded into the pre-placed sutures and tied permanently into position, including covering the buckle with Tenon's capsule if desired. Returning to vitreous surgery, liquid perfluorochemical is used to reattach the retina by instilling it slowly on the disk area while allowing fluid to exit the eye. Care is taken to remove subretinal fluid from under the most anterior margins of the tear, while preventing the liquid perfluorochemical from entering the subretinal space. With the retina held in place by the perfluorochemical, endolaser, indirect ophthalmoscopic laser, or additional cryopexy is applied. The liquid perfluorochemical is then exchanged for gas or silicone oil tamponade, and the case is closed.
GIANT TEAR WITH PVR-REPRESENTATIVE TECHNIQUE
These cases have many similarities to the technique just described, but several important features emerge: lens removal is almost always performed. A scleral buckle is also widely employed, although recent studies have shown success in such cases without routine buckling (this is discussed in a subsequent section). Membrane peeling from the retinal surfaces is the most critical component of surgery, and failure to reattach the retina during instillation of liquid perfluorochemical usually indicates the need to perform a relaxing retinotomy as well. Endolaser retinopexy is applied to the giant tear and any other breaks created or suspected, supplemented by indirect ophthalmoscopic laser or peripheral retinal cryopexy.
ANESTHESIA
Experience has shown that most giant tear surgeries may be comfortably performed within the framework of retrobulbar anesthesia, particularly when supplemented by intravenous sedation and monitoring. In addition, this form of anesthesia has many advantages:
|
1. |
It permits gas kinetics to remain unaltered. |
|
|
2. |
Patient cooperation for postoperative (or even intraoperative) positioning is enhanced. |
|
|
3. |
It produces less postoperative nausea and recovery difficulties. |
|
|
4. |
It may permit surgery in patients who are otherwise prohibited from general anesthesia. |
For these reasons, general anesthesia is reserved for patients who are children, mentally impaired, or prohibited from successful retrobulbar anesthesia by some obvious limitation.
RETINOPEXY
Permanent closure of the giant retinal break is achieved with one or more modes of retinopexy, including cryotherapy, laser photocoagulation, or diathermy. Most authors recommend extending the treatment a full clock hour beyond the margins of the tear into normal retina, as well as treating any additional breaks or radial rips. The selection of retinopexy modality is guided by surgeon's preference and ease of use within a given surgical situation, as there are no randomized data to support claims of superior results with the use of one or the avoidance of another modality. In actual practice, it is common to combine modalities. Endolaser may be used to treat the posterior aspect of the retinal flap, and transscleral cryotherapy to supplement the more anterior periphery, although others would shift to indirect ophthalmoscopic laser for the latter.
Transscleral cryotherapy may be used alone or as a supplement to laser or diathermy. A popular technique for giant tears without PVR involves performing transscleral cryotherapy to the retinal pigment epithelium in the intended bed of the tear, as well as desired treatment beyond the clock hours of the tear, before retinal reattachment.[58] In this technique, it is particularly important to treat somewhat more posteriorly in the very middle of the tear, as this is the area where posterior slippage may occur, and an extra margin of posterior treatment in this area may preserve surgical success despite posterior slippage of the break. Later in the case when the retina has been reattached, cryotherapy may be applied if insufficient or inaccurate coverage is noted. In cases associated with PVR, although cryotherapy might be used in similar ways, in practice it is difficult to gauge the fial appearance and location of the retina distorted by membranes, and possibly requiring retinotomy for reattachment. Therefore, cryotherapy is less often used in the beginning of cases with PVR, and endolaser after retinal reattachment is the dominant retinopexy, with cryotherapy or indirect ophthalmoscopic laser assuming a supplementary role.
It has become popular in recent years to denounce cryotherapy, but it thrives owing to its many advantages. It may be placed with ease in the far periphery, avoiding the lens and permitting thorough treatment of the critical vitreous base area. It may be performed in the face of moderate or severe limitation of the ocular media and is consistent in reaction despite variations in residual subretinal fluid under the margins of the tear or ocular pigmentation. It may be applied to the bed of the tear before or subsequent to retinal reattachment. Its disadvantages include the need for access to the sclera (precluding treatment through existing scleral buckles), the greater degree of breakdown of the blood-vitreous barrier,[59] dispersion of retinal pigment epithelial cells and debris,[60, 61] and the perceived greater risk of PVR as a consequence of these latter two effects. If cryotherapy is used intraoperatively, many surgeons prefer to perform transscleral cryotherapy before vitrectomy.[62] Experimental studies have demonstrated dispersion of numerous viable pigment epithelial cells during cryotherapy,[59] and it has been suggested that the subsequent vitrectomy portion of the procedure will remove these cells and debris and may reduce the incidence of postoperative PVR.[62] This rationale has support from animal experiments and is widely quoted, and it has led some authors to even question the use of cryotherapy in any retinal procedure. Nevertheless, it remains completely conjectural within the clinical confies of giant retinal tear surgery, and it is entirely possible that the many advantages of cryotherapy outweigh its disadvantages; and in aggregate, it might even prove to be superior to other modes of retinopexy.
Endolaser photocoagulation is performed while the retina is held in position by the liquid perfluorochemical, and two or three rows of spots serve as a barrier around the break margins. Newer laser systems permit continuous application ('painting'), and this is a very effective and efficient technique as long as care is taken to avoid overtreating in extent or intensity. Laser lesions have a moderate degree of immediate adhesion owing to the coagulum of tissue that is induced, but these adhesions may be dislodged by forcible movement of the retina with air-fluid exchanges and the like. Permanent adhesion requires a cellular response and develops over several weeks. Laser application requires retinal apposition to the retinal pigment epithelium with minimal or no residual fluid, and variations in subretinal fluid as well as ocular pigmentation will cause considerable variation in lesion intensity. In important areas where adequate treatment intensity is not achieved, careful inspection for persistent detachment is mandatory. In some cases, only additional subretinal fluid removal will be needed to permit endolaser application, and in other eyes, the persistent detachment will indicate the need for additional membrane peeling, retinotomy, or scleral buckling. Also, if it can be determined that the inability to achieve laser lesions in a necessary area is due merely to residual subretinal fluid and that additional retinal mobilization is not required, the area may also be treated with cryotherapy or laser photocoagulation in the postoperative period when the subretinal fluid has reabsorbed under the tamponade. Similar considerations apply to indirect ophthalmoscopic laser, which has the added advantage that it may be applied to the anterior periphery without disturbing the lens or requiring ocular contact and the added disadvantage that it requires clear media for application.
Diathermy, once as popular as retinopexy in detachment surgery, is now used principally as a coagulator. It is used in scleral dissection technique and has received little attention in modern series. Transscleral diode laser application or diopexy is a new technique that combines the surgical approach of cryotherapy with a versatile laser technology, and preliminary studies indicate that it creates an effective chorioretinal adhesion.[63]
LENS REMOVAL
The exact role of lens removal in giant tear surgery has come under reexamination in recent years. Although cases of successful giant tear repair without lens removal were reported early on, the use of prone positioning technique before the introduction of liquid perfluorochemical technique increasingly incorporated lens removal, principally for the need to perform fluid-air exchanges completely in a one-compartment eye. Lens removal has numerous advantages in giant tear surgery:
|
1. |
It provides the best access to the vitreous base area for thorough vitreous removal. |
|
|
2. |
It simplifies fluid-air exchanges and offers contact lens-less optics for surgery under air. |
|
|
3. |
It increases the options, volume, and duration of tamponades without the development of postoperative cataract. |
|
|
4. |
It provides surgical access to the pupil and anterior chamber. |
|
|
5. |
It further clears the media. |
Its disadvantages include: (1) the quality of postoperative vision, (2) the necessity for optical correction for postoperative acuity, and (3) the relative difficulty of implanting an intraocular lens after certain lensectomy techniques.
At the present time, lens or intraocular lens removal is performed in virtually all cases of giant retinal tear associated with PVR.[6, 46, 51, 53, 55, 64] This is done principally because of the need to aggressively dissect the vitreous base tissues as well as the need for extended tamponade with longer-acting gas or silicone oil tamponades that will almost certainly cause postoperative cataract. It is in the consideration of tears unassociated with PVR that a new trend toward preservation of the lens has emerged with perfluorochemical technique.
In the subgroup of eight phakic eyes in the original report on perfluorochemical technique, two eyes required later lensectomy as part of subsequent surgery for PVR, and one eye required surgery for nuclear sclerotic cataract, but five eyes (62%) remained phakic.[46] Although the authors found that preservation of the lens did not adversely affect outcome in their initial series, the variations of other surgical elements such as buckling and the rapid evolution of their overall technique prevented precise comparisons to other studies. In another series of 25 giant tears unassociated with PVR, primary lensectomy was performed in 11 (69%) of the 16 phakic eyes, and a secondary lensectomy was performed in one eye as part of subsequent vitreous surgery for PVR. Therefore, four of 16 phakic eyes (25%) remained phakic.[56] In a study focused on the effects of a lens-sparing perfluorochemical technique and gas tamponade in a consecutive series of 34 eyes, all eyes had intraoperative reattachment and 67% maintained attachment with a single procedure.[57] However, 59% of eyes developed cataract postoperatively. The authors concluded that lens-sparing technique did not diminish the prospect of successful initial surgery or subsequent visual rehabilitation with conventional cataract surgery. In a multicenter case series of 162 eyes with giant tears treated with the use of perfluoroperhydrophenanthrene (Vitreon), the lens was primarily removed in 31 (37.8%) of 82 eyes that were phakic in order to perform vitreous base dissection.[6] Cataract subsequently developed in 20 (39.2%) of the 51 eyes in which the lens was retained. However, it is important to note that this percentage must certainly be amplified by the fact that 80 eyes (49.4%) developed recurrent detachment and many received complicated additional vitreoretinal surgery that included lensectomy, although the number is not available in the printed report. The authors found no evidence that lens removal was a significant predictive factor for visual or anatomic outcome. In a multicenter trial of perfluoro-N-octane, clear lenses were removed in 47% of phakic eyes, and cataract developed in 57% of eyes in which the lens was retained.[64]
In summary, although it is clear that with liquid perfluorochemicals the lens may be preserved in cases of giant retinal tear without PVR, its retention must be tempered by the need to perform a thorough dissection of the vitreous base and by the fact that a majority of retained lenses will eventually require removal for cataract or as part of a subsequent retinal procedure. Although secondary cataract surgery with intraocular lens implantation has many advantages, secondary intraocular lens implantation and contact lenses are also visually successful. It appears reasonable to conclude that the surgeon should not compromise the initial surgery for giant retinal tear by diminishing other surgical goals to preserve the lens.
VITRECTOMY
Selected giant retinal tears unassociated with substantial PVR have been repaired without vitrectomy. Numerous techniques have been described, including buckling after positioning the posterior flap with an intravitreal gas bubble,[2, 27, 65] intravitreal gas bubbles with retinopexy but without buckling,[2, 28] and forced retinal incarceration in the bed of a scleral buckle.[1, 5] Whereas some of these techniques may fid occasional use in selected cases, the overwhelming majority of giant retinal tears will benefit from the additional effectiveness that a vitrectomy approach provides. It should be mentioned that giant dialyses, owing to different vitreo-retinal relationships, may be successfully repaired with primary buckling or even outpatient retinopexy and gas procedures, and for these cases vitrectomy appears much less necessary.
Vitrectomy is employed in giant tear surgery for several related goals. Removing the vitreous gel mobilizes the retina, permits safer intraocular instrumentation in a gel-free environment, creates space for subsequent intraocular tamponade, softens the eye for scleral buckle placement without external drainage, and removes blood, liberated retinal pigment epithelial cells, and other debris. Surprisingly, the vitrectomy portion of the surgery for giant tears unassociated with PVR is frequently straightforward, with the greatest complexity in the removal of the anterior, peripheral vitreous. As mentioned, this may be facilitated by gentle scleral indentation, wide-angle viewing systems, lens removal, and scleral buckling, although one or more measures usually suffice.
In cases with PVR, the removal of the lens, intraocular lens, or pupillary membranes is crucial to the adequacy of removal of vitreous base gel and membranes. In such cases, the surgeon may prefer that the sequence of elements may be arranged so that lens removal and vitreous base dissection precede fial placement or revision of the scleral buckle or may perform this dissection after buckle tightening has brought the periphery into closer view. Meticulous examination of the retinal surfaces and fixed folds is continued with removal of membranes in an effort to restore as much mobility as possible. Notation is made of (and possibly marking diathermy applied to) any additional retinal breaks created during this portion of the surgery, but the primacy of retinal mobilization over break avoidance is stressed. If it becomes clear during the perfluorochemical exchange or later that insufficient mobility has been restored to reattach the retina to the eye wall, then additional membrane removal, retinotomy, or additional scleral buckling must be pursued, or the operation will fail.
SCLERAL BUCKLING
Placing the question of scleral buckling for giant retinal tears in the context of modern vitrectomy and liquid perfluorochemical surgical techniques requires separate consideration for tears unassociated with PVR as well as those in which PVR is present. For giant tears unassociated with PVR and treated with perfluorochemical technique, the use of a scleral buckle, like the performance of lensectomy, has also undergone reevaluation. Like lensectomy, previous studies have been reported to specifically address the necessity of scleral buckling, but the conclusions remain limited by the overall evolution of surgical technique and by their small size, retrospective character, and nonrandomized design.[54, 66] As mentioned previously, giant tears were repaired with some success by buckling without vitrectomy or by gas without buckling very early in the history of giant tear surgery, thereby proving that buckling was unnecessary in some cases.[2]
After the introduction of vitreous surgery but before the development of liquid perfluorochemical technique, vitrectomy without scleral buckling was used to reattach six of six consecutive eyes having giant tears without PVR.[66] The technique included preoperative photocoagulation to the attached periphery, intraoperative cryopexy to the bed of the tear, vitrectomy, intravitreal injection of 1.2 cm3 of pure C3F8, postoperative positioning with bubble expansion, and postoperative photocoagulation to the reattached retina.
For giant tears without PVR, the initial report of 17 cases managed with liquid perfluorochemicals documented successful repair of five eyes (all with tears 180° or greater) of seven attempted without scleral buckling; the two failures later required buckling for localized detachment opposite the original tear and recurrent detachment with PVR.[46] The authors concluded that the presence of a buckle was disadvantageous in some situations, generating redundant radial retinal folds and limiting the use of cryopexy. A specific study of 11 eyes with giant tears without PVR managed without scleral buckling with perfluorochemical technique, including radical dissection of the vitreous base, documented that all eyes were reattached at the fial evaluation and that nine eyes had 5/200 or better acuity.[54] However, this study has been criticized for the number of reoperations required (nine of the 11 study eyes required some additional surgery, and seven of these eyes required eight additional major surgical procedures), and for the use of silicone oil as a tamponade in five eyes, necessitating subsequent removal.[67] In addition, the lens was removed in five of six phakic eyes in this series, confounding the analysis of the relative contributions of lens removal versus scleral buckling. In a series of 162 eyes (including 52 eyes (32.1%) with grade C or D PVR) managed with perfluoroperhydrophenanthrene, an encircling buckle was placed in 100 eyes (62.5%).[6] Statistical evaluation showed no correlation with the presence of a scleral buckle and fial visual acuity or reattachment. A study of 25 consecutive cases managed by surgeons with a preference for including scleral buckling routinely when possible (23 eyes or 92% of cases) noted that only seven eyes (28%) required additional surgery consisting of nine varied reoperations and that all retinas were reattached at fial follow-up.[56] Final visual acuity was 20/80 or better in 72% of patients and 20/200 or better in 84%. These authors also performed lens removal in 69% of phakic eyes. They concluded that scleral buckling has clear advantages, including easier access and visualization of the peripheral retina as well as mechanical support to counteract traction at the vitreous base.
Most recently, in a preliminary communication regarding a multicenter trial of perfluoro-N-octane for the repair of giant retinal tears, ?90% reattachment rate was noted for 76 primary tears without PVR. There was no significant difference in reattachment between the 55 tears whose treatment included scleral buckling and the 21 without buckling.[64] However, in the subgroup of 89 eyes with PVR in this same study, reattachment was achieved in 71.8% of the 71 eyes in which buckling was included versus 61.1% of 18 eyes without scleral buckling. A later report of the fial 212 eyes in this multicenter study documented that 62% of eyes had scleral buckling as part of study surgery.[68] Evaluating all eyes combined, regardless of PVR, the report noted that lack of scleral buckle placement (either before study surgery or during study surgery) was significantly associated with a risk of recurrent retinal detachment. Although these latter data suggest that buckling should be routinely included in cases with PVR, the number of possibly confounding variables (size of tears, degree of preoperative PVR, number of reoperations required, lens status, and most importantly, fial visual acuity) suggests some caution in concluding that scleral buckling is superior in cases with PVR. Indeed, recent reports suggest a trend away from scleral buckling in contemporary surgery. Ambresin and associates[69] treated 17 eyes with representative giant tears, including eight eyes with grade B PVR and three eyes with grade C without scleral buckling, favoring a vitrectomy and perfluorochemical technique followed by silicone oil exchange, and most significantly, the application of 360° photocoagulation to the peripheral retina with the indirect ophthalmoscopic laser. The retina was reattached with the initial surgery in 16 eyes, and with a mean follow-up of over 2 years, the retina was reattached in 17 of the 18 eyes (94.4%) at the fial exam. This silicone oil technique with its high reattachment rate may have entailed some compromise of the crystalline lens. Of the eleven eyes that were phakic at the start, the lens was removed intraoperatively in three, and an additional five developed postoperative cataract. Nevertheless, this study suggests that the evolving sophistication in the use of aggressive membrane peeling, vitreous base gel removal, retinotomy, tamponade, and retinopexy may permit improved reattachment without scleral buckling even in cases with PVR.
UNFOLDING AND REPOSITIONING THE INVERTED POSTERIOR RETINAL FLAP
As mentioned previously, numerous methods have been employed to unfold the inverted posterior retinal flap in giant tear surgery. Forcible incarcerations of the retina during transscleral drainage, positioning with small gas bubbles, prone air-fluid exchange, vitreous incarceration, sutures, tacks, silicone oil exchange, and many other techniques have been used with success, but all have been surpassed by the use of liquid perfluorochemicals.[6, 46-58, 64] In perfluorochemical technique, after the vitreous has been removed and the retina mobilized by membrane peeling if necessary, liquid perfluorochemical is placed on the optic disk area and gradually increased as subretinal and vitreous cavity fluid is displaced anteriorly and out of the eye. The egress for fluid may simply be the pars plana sclerotomy site, or a special double-barreled cannula may be used, simultaneously permitting perfluorochemical injection and fluid egress into a second port a few millimeters above the tip with an exit channel outside the eye. With the tear fully reattached, and after any additional endolaser or cryopexy, the perfluorochemical is removed and replaced with gas or silicone oil. This may be done in a single step or may be performed after an initial air-perfluorochemical exchange removes all perfluorochemical from the eye. One advantage of performing this air exchange before instilling the tamponade gas or oil is that, during the period of air insufflation of the globe, residual droplets of perfluoro-N-octane in the vitreous cavity will evaporate owing to the high vapor pressure of this substance. Perfluoroperhydrophenanthrene, however, is much less volatile and requires manual removal.
Care must be taken to meticulously remove fluid under the most anterior aspect of the flap as the exchange nears completion; otherwise the most anterior margin of the flap will remain elevated. If unrecognized, this anterior residual fluid will be driven posteriorly under the retina in subsequent gas-or oil-perfluorochemical exchange and produce posterior slippage. Similarly, care must be taken to avoid the subretinal passage of perfluorochemical. This typically occurs when perfluorochemical exchange is performed before sufficiently mobilizing the posterior flap in cases with PVR. Because the tear cannot fully unfold in such a situation, as the perfluorochemical bubble is increased it migrates over the rigid edge of the flap and into the subretinal space. Subretinal perfluorochemical migration may also occur in cases with radial rips or with irregular retinotomies. Histologic studies in animals have shown that liquid perfluorochemicals are well tolerated within the eye, but retinal changes have been noted with large volumes of perfluorochemical placed in the vitreous cavity for more than 1 week.[70, 71] Consequently, efforts are made to prevent migration of these liquids into the subretinal space where removal is more difficult.
INTRAOCULAR TAMPONADE
Prolonged postoperative retinal reapposition and giant tear closure are maintained by the use of long-acting gas or silicone oil in almost all contemporary surgical techniques for giant tear repair. In giant tear surgery, if the lens has been preserved, sulfur hexafluoride gas, air, perfluoroethane, or low concentrations of perfluoropropane gas (10% or less) will be selected owing to the formation of cataract with other tamponades. In aphakic or pseudophakic patients, perfluoropropane gas and silicone oil are the tamponades of choice for most patients. A recent study has suggested equal outcomes in a randomized trial between silicone oil and perfluoropropane tamponade in the management of giant retinal tears complicated by PVR.[72]
An interesting new technique is the use of perfluorochemicals as a short-term postoperative tamponade. Sirimaharaj and co-workers[73] reported the maintenance of perfluoro-n-octane for 5-14 days (mean 7.5 days) postoperatively in 62 eyes of 61 patients undergoing vitreoretinal surgery for a wide variety of giant tears. Patients were positioned in an appropriate fashion to tamponade the break with this heavier-than-water material. This short tamponade was followed by a second procedure to remove the perfluorochemical and replace it with gas or oil. With a mean follow-up of 2 years, 58 of 62 eyes (93.5%) were reattached, and there was no residual perfluorochemical in any eye. Glaucoma developed in three eyes, and was medically controlled. Final visual acuity was 20/40 or better in 27 eyes (46.5%), 20/200 or better in 51 eyes (82.3%), and worse that 20/200 in 11 eyes. Rofail and associates[74] used similar postoperative tamponade for a mean of 16.4 days (range 6-50 days) in 16 eyes with giant tear without significant PVR. In their cases, all treated without scleral buckling, 15 eyes were reattached (93.7%), and no complications attributable to the perfluorochemical were noted. While the results of these two studies are impressive, it remains to be seen whether such a technique - with its attendant additional surgery - is required in the majority of cases, given the overall evolution in technique. Nevertheless, when confronted with slippage or patient positioning difficulties, a brief postoperative perfluorchemical tamponade should be considered.
POSTOPERATIVE PATIENT POSITIONING AND MANAGEMENT
In many patients, postoperative management is quite simple and is limited to appropriate positioning with intraocular tamponade, topical medications including cycloplegic, steroid, and antibiotic, and monitoring for increased intraocular pressure or other complications. In the first few days after surgery, it is helpful to have the patient positioned in a manner that encourages the maximal unrolling of the giant tear. This is accomplished by sequentially moving into position by turning the body in a specified direction. As an example, a description is given for a patient with a 5-clock-hour tear in the temporal periphery of the right eye. To begin a period of positioning after a free period, the patient would be instructed to first rest for a moment on the back with face up, then turn on to the right side (rolling the tear to ground), then continuing to face down, and fially coming to rest on the left side with the tamponade closing the tear. This movement encourages the expression of subretinal fluid and the unrolling of the tear and will minimize the possibility of posterior slippage postoperatively until the retinopexy begins its effect.
A few surgeons perform supplemental photocoagulation or cryopexy routinely, whereas others reserve these treatments for posterior slippage of the tear or missed areas at surgery; but the need for postoperative retinopexy can be minimized by careful intraoperative technique. In an occasional case, retinopexy can be combined with the rolling maneuver described previously, possibly with additional gas injection, in an attempt to salvage an early postoperative redetachment.
RESULTS
Anatomic and functional results have improved dramatically compared with the earliest series. In a recent multicenter series of 162 eyes managed with liquid perfluorochemical technique, preoperative factors associated with a poorer visual outcome included higher-grade PVR, giant tear greater than 180°, poor visual acuity, a history of cataract extraction, hypotony, and macular detachment.[6] In this series, in which almost one-third of eyes had grade C or D PVR and one-quarter had tears 180° or greater, the retina was reattached at the most recent follow-up examination in 90.7%, and visual acuity was 20/80 or better in 29% of eyes and 20/200 or better in 43.2% of eyes. These results were obtained despite a sobering 49.4% redetachment rate after the initial procedure as well as one or more additional procedures in 58.6% of eyes, indicating the need for persistence in management. In another multicenter series[68] of 212 eyes managed with liquid perfluorochemical technique, 167 eyes (79%) were reattached at fial follow-up median 3.5 months. Although this follow-up for the entire study population was rather short, the 6 month prespecified endpoint included 141 eyes of which a similar proportion, i.e., 76% (108 eyes) were reattached. Visual acuity at last follow-up was 20/80 or better in 35% and 20/200 or better in 50%.
In a series of 34 eyes that excluded cases with significant PVR, retinal reattachment was ultimately achieved in 100% of eyes, and 88.2% had visual acuity of 20/200 or better.[57] Redetachment had occurred after the initial procedure and was repaired in 33% of eyes, and the majority of these redetachments were due to the development of PVR. In another series excluding cases with PVR, 100% of 25 eyes were similarly reattached at fial follow-up, with 20/80 or better acuity in 72% and 20/200 or better acuity in 84% of eyes.[56] Additional procedures were performed in 28% of eyes. However, it is interesting to note that redetachment occurred in only 12% of the 25 eyes in this series, compared with the 33% of cases in the previous series mentioned, and it is possible that this is related to the much greater use of buckling and lensectomy in the latter series.
Finally, in a series of 10 complicated eyes with giant tears greater than 180° and PVR grade D1 or worse, 90% were ultimately reattached with 20/80 or better visual acuity in 40% and 20/200 or better in 60% of eyes.[51] Reoperations were performed in five of the 10 eyes, principally for removal of epiretinal membranes.
COMPLICATIONS
The complications that may be encountered in giant retinal tear surgery are numerous and, in general, may be considered in relation to the major elements of surgery, e.g., those related to vitrectomy, scleral buckle, tamponade, and liquid perfluorochemical. Beyond the extensive list of possible complications noted previously, several specific complications deserve consideration. Preoperatively, extension of a giant tear, possibly with the creation of radial rips, may occur with violent head movement, and patients should not be subjected to extensive manipulation or physical activity. Intraoperatively, posterior slippage of a giant tear after previous successful reapproximation to the periphery usually indicates residual subretinal fluid at the very margin of the tear, and if the slippage is substantial, a repeat perfluorochemical exchange with careful anterior drainage will be required. In two large multicenter trials of liquid perfluorochemical technique, intraoperative slippage of the tear was noted in 4.9-10.7% of cases.[6, 64] Postoperative slippage may also occur and was noted in 1.5% of cases (Fig. 185.9).[64] Its effect may be controlled by careful, sequential positioning to enhance repositioning of the tear as described previously, as well as by including some additional posterior coverage with retinopexy during the surgery as a matter of course, or postoperatively with laser if a deficiency in the retinopexy coverage is recognized.
|
|
|
|
FIGURE 185.9 Posterior slippage of a giant retinal tear. (a) Preoperative photograph of a 180° superior giant retinal tear with a rolled posterior edge. (b) Postoperative view with posterior slippage of the tear visible as a redundant retinal fold posterior to the buckle. (c) Posterior pole view of the same eye. The macula remains attached despite substantial posterior slippage of the tear. |
Retention of liquid perfluorochemical in the vitreous cavity or in the subretinal space may also occur. Although experimental studies have shown retinal changes after 1 week with large vitreous volumes of perfluoro-N-octane,[70, 71] in clinical practice tiny residual intravitreal or anterior chamber droplets appear to be well tolerated; subretinal droplets may cause scotomas. In the multicenter experience in 207 eyes managed with perfluoro-N-octane, retention was noted in 7.9% of eyes overall and 3.0% of eyes had retained perfluorochemical in the subretinal space.[64] Removal of liquid perfluoro-N-octane from the vitreous cavity is simplified by allowing the eye to remain air filled with air insufflation for ?5 min after removal of visible droplets. The high vapor pressure of this substance allows for evaporation from the retinal surface. Recently, the performance of a 15-30 cm3saline rinse after bulk perfluorochemical removal was also found to minimize unwanted retention.[75] However, perfluorochemical migration into the subretinal space is to be avoided by monitoring the anterior margin of the tear during the perfluorochemical exchange. If the tear remains elevated by membranes and perfluorochemical migrates into the subretinal space, it will become trapped within the subretinal space as the subsequent air-fluid exchange occurs. When recognized, subretinal perfluorochemical can usually be removed by expression with additional perfluorochemical instilled into the vitreous cavity or removed with a flexible cannula or even a small retinotomy.
The most important postoperative complication in giant retinal surgery is recurrent detachment, which is principally due to the development of PVR (Fig. 185.10). This complication developed in 49.4% and 31.5% of patients in the two large multicenter series mentioned previously, respectively.[6, 64] Also, visually significant postoperative epimacular membranes developed in 7.4% and 15% of patients in these series, respectively, and are a frequent cause of reoperation in patients after otherwise successful repair of a giant retinal tear.[6, 64] Although many cases that develop the various manifestations of PVR can now be salvaged with additional surgery, efforts to understand and control this process as described in Chapter 183, would have their greatest benefit in the management of patients with giant retinal tear.
|
|
|
|
FIGURE 185.10 PVR after giant retinal tear. (a) Fundus photograph of the right eye with a 150° temporal giant retinal tear that developed after initial scleral buckling for a smaller tear. The inverted posterior edge is visible temporally, and the scleral buckle can be seen nasally. Visual acuity is hand motions. (b) Postoperative photograph 3 weeks after vitrectomy and prone air-fluid exchange. Extensive PVR is displayed, with recurrent detachment and visual acuity of counting-figers at 6 ft. (c) Fundus photograph 6 months after additional vitrectomy and membrane peeling for PVR. The retina is attached, but visual acuity remains limited to counting figers owing to subretinal membranes distorting the macula. |
REFERENCES
1. Schepens CL, Dobbie JG, McMeel JW: Retinal detachments with giant breaks: preliminary report. Trans Am Acad Ophthalmol Otolaryngol 1962; 66:471-479.
2. Norton EWD, Aaberg T, Fung W, Curtin VT: Giant retinal tears. I. Clinical management with intravitreal air. Am J Ophthalmol 1969; 68:1011-1021.
3. Scott JD: Giant tear of the retina. Trans Ophthalmol Soc UK 1975; 95:142-144.
4. Machemer R: Retinotomy. Am J Ophthalmol 1981; 92:768-774.
5. Schepens CL, Freeman HM: Current management of giant retinal breaks. Trans Am Acad Ophthalmol Otolaryngol 1967; 71:487.
6. Kertes PJ, Wafapoor H, Peyman GA, et al: The management of giant retinal tears using perfluoroperhydrophenanthrene: a multicenter case series. Ophthalmology 1997; 104:1159-1165.
7. Aaberg Jr TM, Rubsamen PE, Flynn Jr HW, et al: Giant retinal tear as a complication of attempted removal of intravitreal lensfragments. Am J Ophthalmol 1997; 124:222-226.
8. Stickler GB, Belau PG, Farrell FJ, et al: Hereditary progressive arthro-ophthalmopathy. Mayo Clin Proc 1965; 40:433-455.
9. Langmann A, Langmann G, Kainer U, Faulborn J: Vitreoretinale Veränderungen bei den Geschwistern der Patienten mit Stickler-syndrom. Ophthalmologe 1993; 90:506-509.
10. Watanabe Y, Ueda M, Adachi-Usami E: Retinal detachment in identical twins with Stickler syndrome type 1. Br J Ophthalmol 1996; 80:976-981.
11. Ahmad NN, Dimascio J, Knowlton RG, Tasman WS: Stickler syndrome: a mutation in the nonhelical 3' end of type II procollagen gene. Arch Ophthalmol 1995; 113:1454-1457.
12. Dowler JGF, Lyons CJ, Cooling RJ: Retinal detachment and giant retinal tears in aniridia. Eye 1995; 9:268-270.
13. Hovland KR, Schepens CL, Freeman HM: Developmental giant retinal tears associated with lens coloboma. Arch Ophthalmol 1968; 80:325-331.
14. Cooling RJ, Rice NSC, McLeod D: Retinal detachment in congenital glaucoma. Br J Ophthalmol 1980; 64:417-421.
15. Scott JD: Congenital myopia and retinal detachment. Trans Ophthalmol Soc UK 1980; 100:69-71.
16. Daniel R, Kanski JJ, Glasspool MG: Retinal detachments in children. Trans Ophthalmol Soc UK 1974; 94:325-334.
17. Freeman HM: Fellow eyes of giant retinal breaks. Trans Am Ophthalmol Soc 1978; 76:343-382.
18. Edwards RS, Calder IG, Crews SJ: Retinal detachment in retinitis pigmentosa. Trans Ophthalmol Soc UK 1985; 104:315-318.
19. Johnston ME, Gonder JR: Giant retinal tears, retinal detachment, and retinitis pigmentosa. Can J Ophthalmol 1985; 20:16-18.
20. Pyeritz RE, McKusick VA: The Marfan syndrome: diagnosis and management. N Engl J Med 1979; 300:772-777.
21. Kainulainen K, Karttunnen L, Puhakka L, et al: Mutations in the fibrillin gene responsible for dominant ectopia lentis and neonatal Marfan syndrome. Nat Genet 1994; 6:64-69.
22. Maumenee IH: The eye in the Marfan syndrome. Trans Am Ophthalmol Soc 1981; 79:684-733.
23. Dotrelova D, Karel I, Clupkova E: Retinal detachment in Marfan's syndrome: characteristics and surgical results. Retina 1997; 17:390-396.
24. Freeman HM, Castillejos ME: Current management of giant retinal breaks: results with vitrectomy and total air-fluid exchange in 95 cases. Trans Am Ophthalmol Soc 1981; 79:89-102.
25. Wolfensberger TJ, Aylward GW, leaver PK: Prophylactic 360° cryotherapy in fellow eyes of patients with spontaneous giant retinal breaks. Ophthalmology 2003; 110:1175-1177.
26. Lincoff H, Kreissig I, LaFranco F: Mechanisms of failure in the repair of large retinal tears. Am J Ophthalmol 1977; 84:501-507.
27. Lincoff H: A small bubble technique for manipulating giant retinal tears. Ann Ophthalmol 1981; 13:241-243.
28. Kreissig I, Stanowsky A, Lincoff H, Richard G: The treatment of difficult retinal detachments with an expanding gas bubble without vitrectomy. Graefes Arch Clin Exp Ophthalmol 1986; 224:51-54.
29. Machemer R, Allen AW: Retinal tears 180° and greater: management with vitrectomy and intravitreal gas. Arch Ophthalmol 1976; 94:1340-1346.
30. Freeman HM: Current management of giant retinal breaks with an inverted retinal flap. In: Neetens A, ed. Modern concepts in vitreo-retinal diseases. Proceedings of the vitreoretinal conference, University of Antwerp, 1985, Antwer: UIA Press; 1985:183-194.
31. Usui M, Hamazaki S, Takano S, Matsuo H: A new surgical technique for the treatment of giant tear: transvitreoretinal fixation. Jpn J Ophthalmol 1979; 23:206-215.
32. Federman JL, Shakin JL, Lanning RC: The microsurgical management of giant retinal tears with trans-scleral sutures. Ophthalmology 1982; 89:832-839.
33. Nishi O, Ideta H: A new suturing method for the treatment of giant retinal tear. Ophthalmic Surg 1987; 18:359-362.
34. Michels RG, Rice TA, Blankenship G: Surgical techniques for selected giant retinal tears. Retina 1983; 3:139-153.
35. Ando F, Kondo J: A plastic tack for the treatment of retinal detachment with giant tear. Am J Ophthalmol 1983; 95:260-261.
36. Ando F, Kondo J: Surgical techniques for giant retinal tears with retinal tacks. Ophthalmol Surg 1986; 17:408-411.
37. deJuan Jr E, Hickingbotham D, Machemer R: Retinal tacks. Am J Ophthalmol 1985; 99:272-274.
38. Algvere P, Stenkula S, Crafoord S, et al: Sealing of retinal breaks with metal tacks: evaluation of a new procedure in retinal re-attachment surgery. Acta Ophthalmol 1986; 64:421-424.
39. Fung WE, Hall DL, Cleasby GW: Combined technique for a 355° traumatic giant retinal break: a case report. Arch Ophthalmol 1975; 93:264-266.
40. Peyman GA, Rednam KRV, Seetner AA: Retinal microincarceration with penetrating diathermy in the management of giant retinal tears. Arch Ophthalmol 1984; 102:562-565.
41. Fitzgerald CR: The use of Healon in a case of rolled-over retina. Retina 1981; 1:227-231.
42. Leaver PK, Lean JS: Management of giant retinal tears using vitrectomy and silicone oil/fluid exchange: a preliminary report. Trans Ophthalmol Soc UK 1981; 101:189-191.
43. Leaver PK, Cooling RJ, Feretis EB, et al: Vitrectomy and fluid/silicone-oil exchange for giant retinal tears: results at six months. Br J Ophthalmol 1984; 68:432-438.
44. Billington BM, Leaver PK: Vitrectomy and fluid/silicone-oil exchange for giant retinal tears: results at 18 months. Graefes Arch Clin Exp Ophthalmol 1986; 224:7-10.
45. Leaver PK: Vitrectomy and fluid/silicone-oil exchange for giant retinal tears: 10-year follow-up. Ger J Ophthalmol 1993; 2:20-23.
46. Chang S, Lincoff H, Zimmerman NJ, Fuchs W: Giant retinal tears: surgical techniques and results using perfluorocarbon liquids. Arch Ophthalmol 1989; 107:761-766.
47. Dralands L, Leys A, Missotten L: Decollement dur dechirure geante. Bull Soc Belge Ophtalmol 1989; 235:43-55.
48. Claes C, Zivojnovic R: The use of perfluorocarbon liquids in vitreous surgery. Bull Soc Belge Ophtalmol 1990; 238:145-150.
49. Le Mer Y, Kroll P: Flüssiges Perfluorocarbon bei der Behandlung von Riesenrissen. Klin Monatsbl Augenheilkd 1991; 198:256-258.
50. Le Mer Y, Kroll P: Die Anwendung von flüssigem Perfluorocarbon bei Riesenrissen; erste Ergebnisse. Klin Monatsbl Augenheilkd 1991; 198:264-267.
51. Glaser BM, Carter JB, Kupperman BD, Michels RG: Perfluoro-octane in the treatment of giant retinal tears with proliferative vitreoretinopathy. Ophthalmology 1991; 98:1613-1621.
52. Fritsch D, Aouizerate F: Utilisations originales des perfluorocarbones liquides. J Fr Ophtalmol 1992; 15:415-418.
53. Millsap CM, Peyman GA, Mehta NJ, et al: Perfluoroperhydrophenanthrene (Vitreon) in the management of giant retinal tears: results of a collaborative study. Ophthalmic Surg 1993; 24:759-763.
54. Kreiger AE, Lewis H: Management of giant retinal tears without scleral buckling: use of radical dissection of the vitreous base and perfluoro-octane and intraocular tamponade. Ophthalmology 1992; 99:491-497.
55. Larricart P, Le Mer Y, Petit E, et al: Les perfluorocarbones liquides dans le traitement chirurgical des décollement de rétine par inversion rétinienne. J Fr Ophtalmol 1993; 16:673-678.
56. Ie D, Glaser BM, Sjaarda RN, et al: The use of perfluoro-octane in the management of giant retinal tears without proliferative vitreoretinopathy. Retina 1994; 14:323-328.
57. Verstraeten T, Williams GW, Chang S, et al: Lens-sparing vitrectomy with perfluorocarbon liquid for the primary treatment of giant retinal tears. Ophthalmology 1995; 102:17-20.
58. Bourke RD, Cooling RJ: Perfluorocarbon heavy liquids. Aust N Z J Ophthalmol 1995; 23:165-171.
59. Vidaurri-Leal J, de Bustros S, Michels RG: Surgical treatment of giant retinal tears with inverted posterior retinal flaps. Am J Ophthalmol 1984; 98:463-466.
60. Jaccoma EH, Conway BP, Campochiaro PA: Cryotherapy causes extensive breakdown of the blood-retinal barrier: a comparison with argon laser photocoagulation. Arch Ophthalmol 1985; 103:1728-1730.
61. Campochiaro PA, Kaden IH, Vidaurri-Leal J, Glaser BM: Cryotherapy enhances intravitreal dispersion of viable retinal pigment epithelial cells. Arch Ophthalmol 1985; 103:434-436.
62. Singh AK, Michels RG, Glaser BM: Scleral indentation following cryotherapy and repeat cryotherapy enhance release of viable retinal pigment epithelial cells. Retina 1986; 6:176-178.
63. Haller JA, Lim JI, Goldberg MF: Pilot trial of transscleral diode laser retinopexy in retinal detachment surgery. Arch Ophthalmol 1993; 111:952-956.
64. Freeman HM: Giant retinal tears: 207 cases from the Perfluoron study [abstract]. Am Acad Ophthalmol Vitreoretinal Update 1997.168-171.
65. Ando F, Hirose H, Nagasaka T, et al: Treatment of retinal detachment with giant tear by pneumatic retinopexy. Eur J Ophthalmol 1993; 3:201-206.
66. Hoffman ME, Sorr EM: Management of giant retinal tears without scleral buckling. Retina 1986; 6:197-204.
67. McCuen BW: Discussion of Kreiger AE, Lewis H: management of giant retinal tears without scleral buckling: use of radical dissection of the vitreous base and perfluoro-octane and intraocular tamponade. Ophthalmology 1992; 99:497.
68. Scott IU, Murray TG, Flynn Jr HW, et al: Outcomes and complications associated with giant retinal tear management using perfluoro-n-octane. Ophthalmology 2002; 109:1828-1833.
69. Ambresin A, Wolfensberger TJ, Bovey EH: Management of giant retinal tears with vitrectomy, internal tamponade, and peripheral 360° retinal photocoagulation. Retina 2003; 23:622-628.
70. Chang S, Sparrow JR, Iwamoto T, et al: Experimental studies of tolerance to intravitreal perfluoro-N-octane liquid. Retina 1991; 11:367-374.
71. Eckardt C, Nicolai U, Winter M, Knop E: Experimental intraocular tolerance to liquid perfluorooctane and perfluoropolyether. Retina 1991; 11:375-384.
72. Batman C, Cekic O: Vitrectomy with silicone oil or long-acting gas in eyes with giant retinal tears; long-term follow-up of a randomized clinical trial. Retina 1999; 19:188-192.
73. Sirimaharaj M, Balachandran C, Chan WC, et al: Vitrectomy with short term postoperative tamponade using perfluorocarbon liquid for giant retinal tears. Br J Ophthalmol 2005; 89:1176-1179.
74. Rofail M, Lee LR: Perfluoro-n-octane as a postoperative vitreoretinal tamponade in the management of giant retinal tears. Retina 2005; 25:897-901.
75. Garcia-Valenzuela E, Ito Y, Abrams GW: Risk factors for retention of subretinal perfluorocarbon liquid in vitreoretinal surgery. Retina 2004; 24:746-752.