Sofia Androudi,
Eugene W.M. Ng,
Alexandros N. Stangos,
Donald J. D'Amico,
Periklis D. Brazitikos
Infectious endophthalmitis is an intraocular inflammation process generally due to an infection with either bacteria or fungi. Infectious endophthalmitis has been subgrouped into several categories based on the time of onset and events leading to the infection. This distinction is important in predicting the causative organisms and guiding therapeutic decisions prior to the definitive microbiologic diagnosis. The broad categories of endophthalmitis include: acute postoperative, delayed onset postoperative, that associated with conjunctival filtering-bleb, posttraumatic, endogenous, and the more recently recognized category of postintravitreal injection endophthalmitis. Endophthalmitis can be a rare but potentially devastating complication of intraocular surgery. In recent years, refinements in the diagnosis and treatment of this sight-threatening condition have led to significant improvement in visual prognosis. Indeed, with prompt medical and surgical intervention, up to 74% of patients attain visual-acuity outcomes of 20/100 or better (Table 184.1).[1-8] Nevertheless, a significant proportion of patients still suffer severe visual loss.
TABLE 184.1 -- Visual Recovery in Treated Endophthalmitis[*]
|
Culture Positive |
|||||||
|
Authorst[?] |
Culture Negative |
Staphylococcus epidermidis |
Other Gram-Positive[?] |
Gram-Negative |
Fungi |
Mixed |
Total[§] |
|
EVS Group[1] |
80% (98/123) |
84% (157/187) |
43% (24/56) |
56% (9/16) |
42% (5/12) |
74% (293/394) |
|
|
Pavan et al[2] |
100% (15/15) |
75% (3/4) |
88% (7/8) |
80% (4/5) |
91% (29/32) |
||
|
Weber et al[3] |
53% (8/15) |
50% (5/10) |
100% (1/1) |
100% (4/4) |
60% (18/30) |
||
|
Driebe et al[4] |
94% (15/16) |
78% (14/18) |
56% (9/16) |
40% (4/10) |
60% (3/5) |
63% (32/51) |
|
|
Bohigian and Olk[5] |
61% (19/31) |
87% (13/15) |
21% (5/24) |
11% (1/9) |
33% (1/3) |
39% (20/51) |
|
|
Rowsey et al[6] |
53% (8/15) |
75% (12/16) |
23% (5/22) |
25% (2/8) |
75% (3/4) |
0% (0/5) |
40% (22/55) |
|
Puliafito et al[7] |
75% (12/16) |
22% (2/9) |
20% (1/5) |
0% (0/1) |
0% (0/5) |
42% (15/36) |
|
|
Diamond[8] |
80% (8/10) |
70% (7/10) |
67% (2/3) |
67% (2/3) |
73% (19/26) |
||
|
* |
Visual recovery defined as 20/100 or better visual acuity in the EVS. Visual recovery defined as 20/400 or better visual acuity in all other studies. |
|
? |
Studies listed in descending chronologic order according to date of patient enrollment (EVS most recent). |
|
? |
Includes all grampositive isolates except Staphylococcus epidermidis. |
|
§ |
Includes two miscellaneous cases in which the organism cannot be determined from the published data. |
INCIDENCE AND EPIDEMIOLOGY OF POSTOPERATIVE ENDOPHTHALMITIS
Bacterial endophthalmitis occurs in a number of clinical settings. Compilation of large reported series (Table 184.2) suggests the following distribution of cases: 62% occur after intraocular surgery, 20% after penetrating trauma, 10% after planned or inadvertent filtering blebs, and 8% as a result of metastatic infection.[5-10]
TABLE 184.2 -- Clinical Setting in Endophthalmitis
|
Authors |
Total |
Postoperative |
Trauma |
Bleb |
Metastatic |
|
Bohigian and Olk[5] |
82 |
55 (67%) |
16 (20%) |
5 (6%) |
6 (7%) |
|
Diamond[8] |
22 |
16 (73%) |
5 (23%) |
1 (4%) |
|
|
Forster et al[9] |
140 |
69 (49%) |
31 (22%) |
25 (18%) |
15 (11%) |
|
Nelsen et al[10] |
55 |
42 (76%) |
9 (16%) |
4 (7%) |
|
|
Puliafito et al[7] |
36 |
24 (66%) |
6 (17%) |
4 (11%) |
2 (6%) |
|
Rowsey et al[6] |
54 |
34 (63%) |
12 (22%) |
8 (15%) |
A 10-year review from 1984 to 1994 of over 58123 intraocular surgeries at three US centers estimated the incidence of postoperative endophthalmitis at 0.093%.[11] The incidence of endophthalmitis based on 36 000 consecutive cataract operations performed at the Massachusetts Eye and Ear Infirmary was evaluated by Allen and Mangiaracine in 1974, and was found to be 0.086%.[12] A 5-year review from 1984 to 1989 of 30002 intraocular surgical procedures at Bascom Palmer Eye Institute demonstrates incidences ranging from 0.051% for pars plana vitrectomy up to 0.30% for secondary intraocular lens (IOL) implantation.[13] Another retrospective study at Bascom Palmer from 1995 to 2001 examining 35 916 intraocular procedures found the incidence of postoperative endophthalmitis among all procedures studied to be 0.05%.[14] Javitt and colleagues reviewed 338 141 cataract surgical procedures and found that the risk of rehospitalization for endophthalmitis in the year after surgery was 0.17% for intracapsular cataract extraction, 0.12% for extracapsular cataract extraction, and 0.12% for phacoemulsification.[15] A cross-sectional, large-scale survey in Germany examining 340633 cataract procedures in 1996 found a mean responder-specific postoperative endophthalmitis rate of 0.148%.[16] Finally, a large retrospective study in the US examining 9.079 cases who underwent a phacoemulsification procedure at a single setting between 1997 and 2001 found an incidence of 0.286%, despite fluoroquinolone prophylaxis.[17]
Recent findings have suggested that postcataract endophthalmitis rates may be on the rise.[18] West et al[19] from a 5% sampling of Medicare beneficiary data files revealed an increase in the rate of endophthalmitis from the time period 1994-97 when compared with 1998-2001. The pooled rate over the entire 8-year period (which corresponds to the rise in clear corneal cataract surgery) was also high at 2.15 per 1000 surgeries (0.2%). The authors hypothesize that clear corneal incisions may be playing a role. This is supported by the fact that the clear corneal technique has had an increase in use by cataract surgeons. The rate of surgeons using this technique had increased from 30% in 1997 to 47% in 2000.[19] Although this independent trend is intriguing, the authors correctly state that no factor can be definitively identified to explain this increase from the information available. Taban et al[20] performed a systematic review of the English literature and concluded that endophthalmitis rates are rising. Using a regression analysis model and excluding case reports, the authors found the rate of pooled endophthalmitis to be 2.65 per 1000 surgeries (0.265%) from 2000 to 2003. This was significantly higher than the rate of less than one per 1000 surgeries (0.087%) in the 1990s. This leads many thoughtful researchers to perform and publish studies to help evaluate current practices that may impact our endophthalmitis rates and outcomes. A majority of these studies are retrospective or case series that constitute level-3 evidence-based data. This is good evidence, however, for this condition. Cost restraints and time make a prospective, epidemiologic study of endophthalmitis incidence an impractical task. Therefore, frequent reporting and publishing of large numbers of patients will probably be the best way to come to a consensus regarding preventative measures, surgery types and techniques, and postoperative approaches to infection risk reduction.
RISK FACTORS
A number of studies have supported the hypothesis that the most common source of postoperative endophthalmitis is the patient's external flora, i.e., organisms colonizing the conjunctival surface and periocular tissues, such as the eyelid and nose.[21] We have summarized in a box the factors increasing the likelihood of microbial pathogens entering the eye, thus increasing the risk of endophthalmitis.
Ocular conditions such as bacterial blepharitis and nasolacrimal duct infections increase the risk of intraocular infection by allowing pathogenic organisms to be present in the operative field.[22-24] Morris and co-workers described a case of postoperative endophthalmitis resulting from bacterial contamination of the contralateral prosthesis in a monocular patient.[25] Patients with the previously mentioned conditions should be excluded from surgery until they have been appropriately treated. In monocular patients, ocular prostheses should be removed before surgery and treatment of the anophthalmic socket and conjunctiva with topical povidone iodine and antibiotics should be performed. Systemic conditions predisposing to endophthalmitis include active infection, ranging from upper respiratory tract infections to sepsis elsewhere in the body.[22-24] The risk of intraocular infection is also increased in diabetic[1, 13, 26, 27] and immunocompromized patients.[28]
A number of surgical factors may increase the risk of endophthalmitis. Some studies have found that bacterial contamination of the anterior chamber occurs in 5-43% of patients during routine cataract surgery.[29-36] Significantly less aqueous contamination occurs with phacoemulsification than with extracapsular cataract surgery, presumably because of the use of smaller incisions and self-sealing wounds.[37] However, the low incidence of postoperative endophthalmitis that occurs despite such relatively high contamination rates suggests that the anterior chamber is able to successfully eradicate low levels of bacterial contamination, a hypothesis that has been supported by animal studies.[38] Consequently, the potential benefit of small incision surgery in decreasing the incidence of endophthalmitis remains unproved.
Cataract surgery incision type has been put into question as a risk factor for postoperative endophthalmitis, following reports of increased incidence associated with clear corneal surgery. In a survey of 340633 cataract cases in Germany, a multivariate analysis identified clear corneal incisions as a risk factor for postoperative endophthalmitis compared to corneoscleral incisions.[16] Other studies also supported this finding. Colleaux et al[39] in a study of 13 886 cataract reported an incidence for endophthalmitis of 0.129% for clear corneal incisions as compared with 0.050% for scleral tunnel incisions. Cooper and associates[40] found that clear corneal incisions were associated with a threefold greater risk of endophthalmitis than was scleral tunnel incision. A subgroup analysis revealed that the presence or absence of a suture was not significant.
IOL materials may influence bacterial adherence and, thus, the risk of prosthetic infection. Menikoff and associates found that IOLs with polypropylene (Prolene) haptics increase the risk of endophthalmitis by a factor of 4.5.[41] Subsequent in vitro studies demonstrated preferential bacterial adherence to the polypropylene haptic portions of these IOLs.[42] In a study of 46 292 cataract cases, by Wedge et al,[37]silicone IOLs carried a higher risk than heparin surface modified polymethylmethacrylate (PMMA) implants. The use of silk suture for wound closure may also increase the risk of endophthalmitis.[43]
Prolonged and complicated surgery increases the risk of endophthalmitis. Additionally, vitreous loss, posterior capsular tears, and surgery in which communication with the vitreous cavity occurs (e.g., intracapsular cataract extraction) increases the risk by nearly 14-fold.[4, 41] The posterior lens capsule serves as a barrier preventing bacterial entry into the vitreous cavity. Primate studies have demonstrated that eyes challenged with intracameral injections of bacteria after cataract extraction were more likely to develop endophthalmitis if posterior capsulectomy had also been performed, compared with eyes with intact posterior capsules.[44] The vitreous provides a milieu that promotes bacterial proliferation. In 1955, Maylath and Leopold showed that inoculation of bacteria into the anterior chamber of phakic rabbit eyes was less effective in causing endophthalmitis than was intravitreal inoculation.[38]
Organisms may be introduced into the eye during the postoperative period. Wound abnormalities, such as vitreous wicks, wound leaks, infected wound margins, and inadvertent filtering blebs, have been found in up to 22% of patients with postoperative endophthalmitis.[4] Cases of endophthalmitis after penetrating keratoplasty,[45] strabismus surgery,[46] scleral buckling, and even suture removal[47] have been described.[13] These findings highlight the importance of meticulous surgical technique, wound closure, and postoperative care.
Concerns regarding the risk of endophthalmitis after sutureless cataract surgery have arisen in the light of several reported cases.[48, 49] Interestingly, the practice of clear corneal temporal incisions has been associated with an increased risk of postoperative endophthalmitis.[50] In the same study the IOL material did not seem to affect the incidence of the infection.
Wound abnormalities such as wound gape and inadvertent filtering blebs have been implicated as contributing factors in these cases. With the current paucity of data, it remains unclear whether self-sealing sutureless wounds carry an inherently higher risk of infection. Nevertheless, it seems clear that the integrity of the surgical closure, whether achieved by sutures or sutureless techniques, is of critical importance in the prevention of postoperative infection.
CLINICAL PRESENTATION
The diagnostic features of infectious endophthalmitis can be broken down into two aspects: clinical recognition and microbiologic confirmation. The accurate diagnosis of postoperative endophthalmitis requires careful assessment of symptoms and signs, in addition to appropriately selected laboratory tests. The earliest symptom of endophthalmitis is usually ocular discomfort or deep pain, although rapid improvement in postoperative visual acuity with IOL implantation has increased the proportion of patients reporting decreased vision as the initial symptom. Other symptoms include complaints of lid swelling, a red eye, photophobia, and discharge.
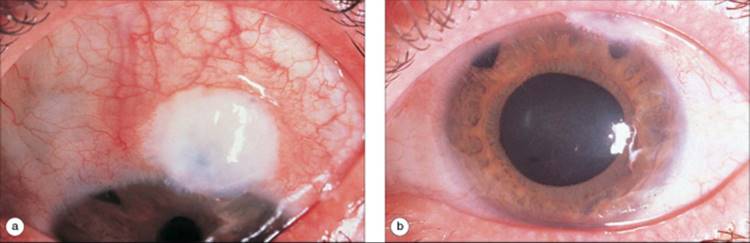
Signs of endophthalmitis include conjunctival hyperemia, chemosis, discharge, corneal edema, increased anterior chamber reaction (cells and flare, fibrin, hypopyon), and membrane formation on the IOL (Figs 184.1 to 184.3). In the posterior segment, vitritis, scattered retinal hemorrhages, and loss of the red reflex are observed. Retinal periphlebitis may be seen as an early sign of bacterial endophthalmitis (Fig. 184.4).[51] Severe cases may cause corneal opacification, corneal ring ulcer or infiltrate, and a systemic response (fever, leukocytosis). Although pain and hypopyon constitute the classic presentation of bacterial endophthalmitis, these findings are absent in a significant proportion of patients with culture-positive endophthalmitis, particularly when the organisms implicated are gram-positive coagulase-negative micrococci (coagulase-negative staphylococci and Micrococcus species), of which Staphylococcus epidermidis is the most common.[1, 52]
|
|
|
|
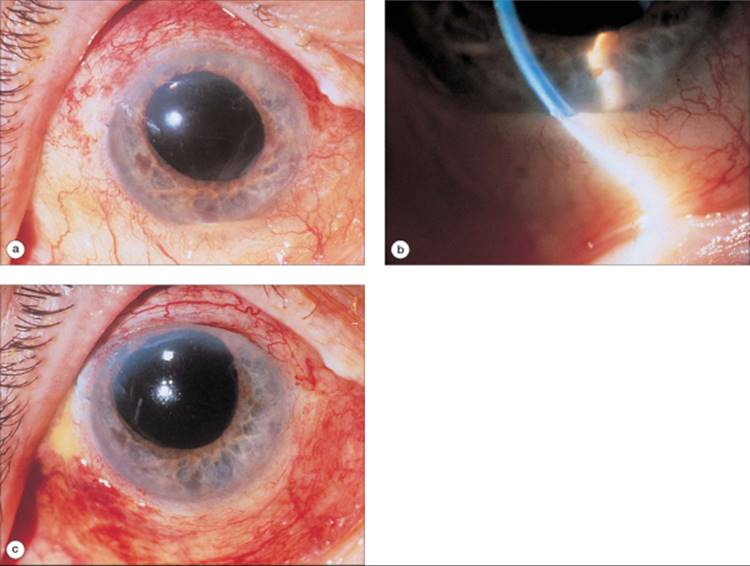
FIGURE 184.1 (a) Postoperative endophthalmitis due to Staphylococcus epidermidis presenting 6 days after extracapsular cataract extraction with posterior chamber lens implantation. Visual acuity was at hand-motions level, and conjunctival hyperemia, hypopyon, and inflammatory membrane on the IOL are seen. (b) Slit-lamp photograph of hypopyon in the patient. (c) Visual acuity improved to 20/500 (limited by preexisting macular degeneration) 2 weeks later after vitrectomy with intravitreal administration of vancomycin (1 mg), amikacin (400 ?g), and dexamethasone (200 ?g). The inflammatory membrane on the IOL was removed at surgery (see text). The IOL was not removed. |
|
|
|
|
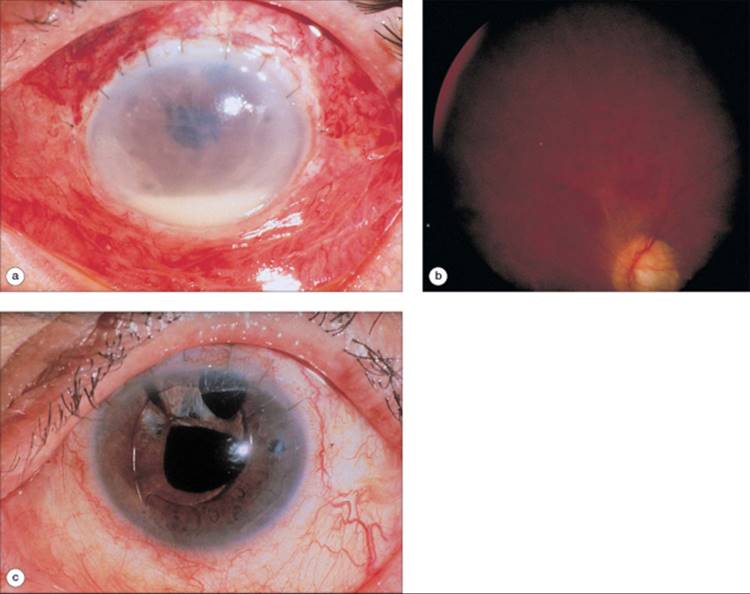
FIGURE 184.2 (a) Postoperative endophthalmitis due to S. epidermidis presenting 4 days after extracapsular cataract extraction complicated by vitreous loss, with anterior chamber lens implantation. Visual acuity is at light-perception level, and conjunctival hyperemia, mild corneal edema, hypopyon, and inflammatory membranes on the iris and both surfaces of the IOL are evident. (b) Fundus photograph after vitrectomy documents petechial retinal hemorrhages frequently observed in association with active endophthalmitis. (c) Two months after vitrectomy with intravitreal administration of cefazolin (2.25 mg), amikacin (400 ?g), and dexamethasone (200 ?g), visual acuity has improved to 20/300. The IOL is preserved after intraoperative removal of the inflammatory membranes noted preoperatively. |
|
|
|
|
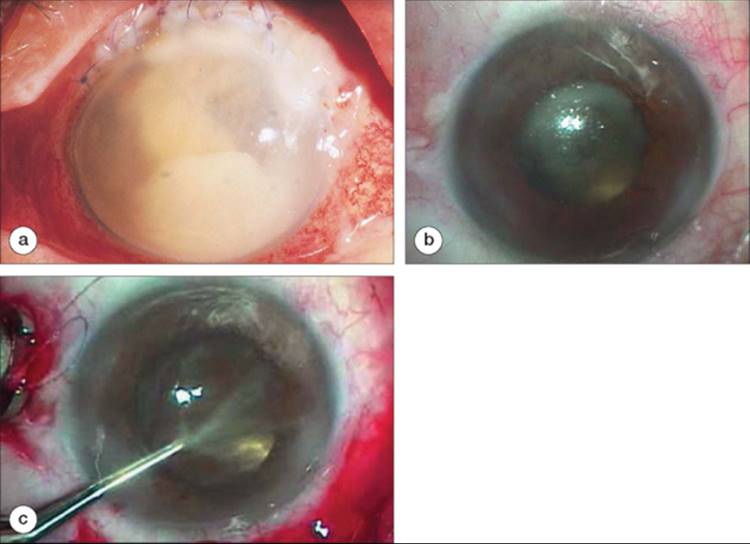
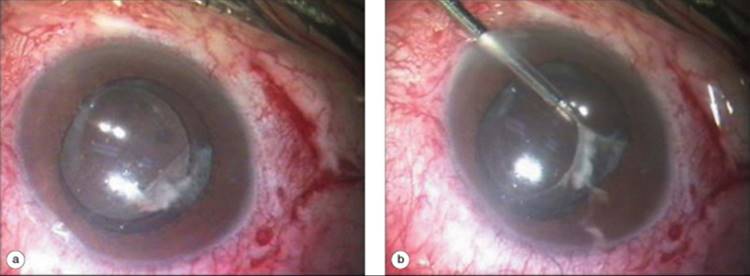
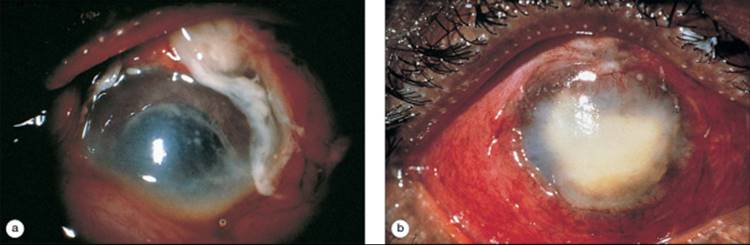
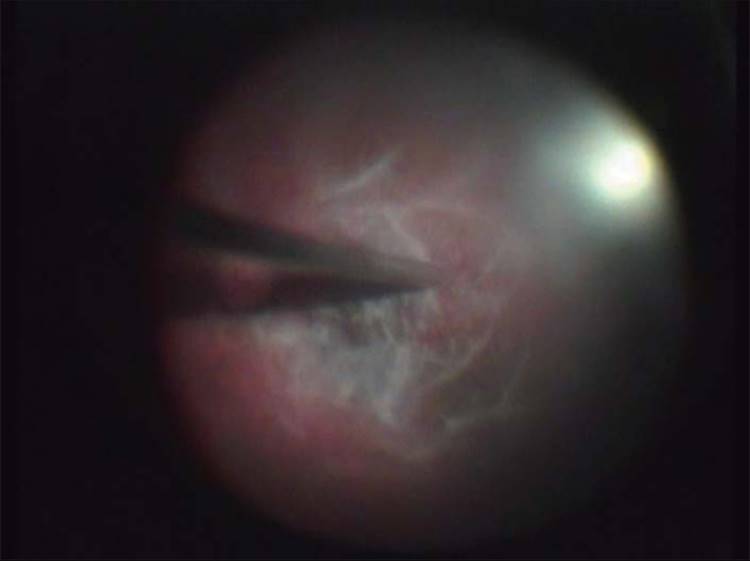
FIGURE 184.3 (a) Severe postoperative endophthalmitis due to Streptococcus pneumoniae seen 12 days after extracapsular cataract extraction with posterior chamber lens implantation. Visual acuity was light-perception only. Dense hypopyon, intense conjunctival hyperemia, and purulent exudate are evident, precluding visualization of the iris and fundus. Vitrectomy with intravitreal injection of cefazolin (2.25 mg), amikacin (400 ?g), and dexamethasone (200 ?g) was performed. The IOL was removed intraoperatively to aid visualization during vitrectomy. The patient's eye progressed to phthisis despite treatment and was eventually enucleated. (b) Case of low-grade chronic postsurgical endophthalmitis (postphacoemulsification). Marked absence of conjunctival inflammation is noted. The inflammation of the vitreous is readily apparent. (c) Removal of papillary membrane to improve visualization during vitrectomy. |
|
|
|
|
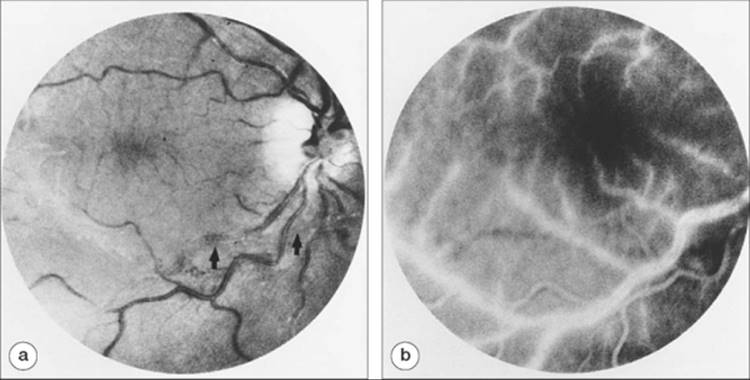
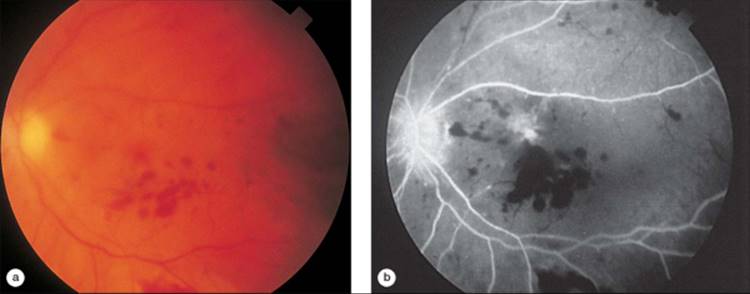
FIGURE 184.4 (a) Fundus photograph of retinal periphlebitis seen early in bacterial endophthalmitis. The patient had Terson's syndrome (vitreous and subarachnoid hemorrhage) and had undergone vitrectomy and excision of a detached internal limiting membrane. Arrows delineate the edge of the trimmed membrane. One day after surgery, the patient complained of ocular discomfort. Visual acuity was 20/80, and anterior chamber cells were noted. Fundus examination revealed prominent venous sheathing just outside the major arcades and extending peripherally. On the following day, visual acuity declined to the hand-motions level, and hypopyon developed. The fundus could no longer be visualized. Bacterial endophthalmitis was confirmed by vitreous culture. (b) Fluorescein angiogram of the same eye demonstrates venous staining and sheathing. |
Typically, nearly two-thirds of patients present within 1 week of cataract surgery, with ?25% of patients presenting within 3 days of the initiating procedure.[1] However, infection caused by less virulent organisms may delay the clinical presentation for up to 2 weeks or longer. Indeed, ?20% of patients may present 2-6 weeks after surgery.[1] The use of topical corticosteroid therapy postoperatively may suppress symptoms and signs of inflammation, such as hyperemia and hypopyon formation, thus delaying presentation. In some instances, months or years may elapse before endophthalmitis presents. In these cases, infection is generally acquired at the time of surgery with indolent organisms such as Propionibacterium species,[53-60] although they may also occur as a result of traumatic wound dehiscence, a neglected inadvertent bleb, or metastatic infection.
Johnson and co-workers examined patients in the Endophthalmitis Vitrectomy Study (EVS) to determine whether specific features of their clinical presentation were predictive of microbiologic culture result. Not surprisingly, it was found that infection with highly virulent organisms was associated with greater clinical severity.[61] Eyes in which symptoms developed within 2 days postoperatively had a higher yield of both gram-negative organisms and gram-positive organisms other than gram-positive coagulase-negative micrococci (referred to as 'other' gram-positive), pathogens considered to be of greater virulence in the EVS. Complaint of eyelid swelling also predicted a higher rate of other gram-positive isolates. Of note, pain was not a predictor for the type of organism implicated. With regard to examination findings, initial light-perception-only visual acuity, an afferent pupillary defect, corneal infiltrates (with or without ring ulcer), large hypopyon, cataract wound abnormalities, and loss of red reflex predicted a higher incidence of gram-negative or other gram-positive organisms. In addition to these individual presenting features, the combination of loss of red reflex and onset of symptoms within 2 days predicted a 50% or greater chance of infection by more virulent bacteria. The most discriminating feature at presentation allowing specific prediction of culture results was the ability to visualize a retinal blood vessel by indirect ophthalmoscopy. Gram-negative organisms did not grow in any eyes in which retinal vessels could be visualized, with nearly two-thirds of these eyes being culture-negative.
Occasionally, an exaggerated postoperative sterile inflammatory response may cause symptoms and signs mimicking infectious endophthalmitis. Such reactions have been described with retained lens material, phacoanaphylaxis,[62, 63] excessive surgical trauma, virgin silk sutures in the cataract wound,[64] vitreous manipulation, incarceration of vitreous or iris, intraocular blood, and reaction to the IOL and associated materials.[65-68] A diagnosis of bacterial endophthalmitis should be suspected on the basis of inflammation that is disproportionate to the clinical setting, although it is apparent that there may be considerable overlap between infectious endophthalmitis and noninfectious inflammatory reactions in the postoperative patient. In addition, systemic diseases with secondary ocular inflammation may also present in the postoperative patient and contribute to diagnostic uncertainty. For example, a case of luetic retinitis and vitritis presenting several weeks after cataract surgery is shown in Figure 184.5. In certain cases, ultrasound examination may be helpful in the diagnosis. The combination of thickening of the retinochoroid layer and echoes in the anterior or posterior vitreous, or both, supports the diagnosis of endophthalmitis.[69]
|
|
|
|
FIGURE 184.5 Luetic retinitis and vitritis presenting in the postoperative period, masquerading as bacterial endophthalmitis. The patient presented with a 5-week history of decreasing visual acuity bilaterally 6 weeks after uncomplicated extracapsular cataract extraction and posterior chamber lens implantation in the left eye. Ocular examination revealed bilateral panuveitis. (a) Fundus photograph of the left eye demonstrates extensive vitritis with associated multiple yellow-white chorioretinal infiltrates inferotemporally. Disk edema with overlying disk hemorrhage and vascular sheathing are also evident. Visual acuity was at hand-motions level. (b) Fundus photograph of the right eye demonstrates dense vitritis obscuring features of the posterior pole. Visual acuity was 5/200. On further questioning, the patient admitted to a previous high-risk sexual encounter, and syphilis was confirmed by strongly positive serum and cerebrospinal fluid serology. After 2 weeks of intravenous penicillin, retinitis and vitritis resolved in both eyes. (c) Fluorescein angiogram of the left eye demonstrates leakage from the optic disk, mottled choroidal fluorescence, and pigmentary changes throughout the posterior pole. (d) Fundus photograph of the left eye after 2 weeks of therapy demonstrates residual disc pallor and edema. Vascular attenuation and sclerosis are also seen. Visual acuity improved to 20/50. |
Accurate diagnosis ultimately rests with the demonstration of microbial pathogens within the eye by appropriate stains and cultures. Given the speed with which endophthalmitis can progress to irreversible visual loss, prompt procurement of microbiologic specimens in all suspected cases is an essential part of management.
LABORATORY INVESTIGATIONS
Approximately two-thirds of eyes with a clinical diagnosis of infectious endophthalmitis will have a positive culture result (Table 184.3).[1, 4-6, 9, 10] Obtaining microbiologic specimens for culture not only is important in directing antibiotic therapy but also predicts visual outcome. Negative culture results are associated with greatly improved visual prognosis, with up to 94% of pseudophakic eyes achieving 20/400 or better visual acuity in one study (Table 184.4).[55]
TABLE 184.3 -- Incidence of a Positive Culture Result in Suspected Infectious Endophthalmitis
|
Author |
Positive Culture Result (%) |
Positive Culture Result/Total Number of Cases |
|
Bohigian and Olk[5] |
62.1 |
51/82 |
|
Driebe et al[4][*] |
74.7 |
62/83 |
|
EVS[1] |
69.3 |
291/420 |
|
Forster et al[9][*] |
55.7 |
78/140 |
|
Nelsen et al[10] |
54.5 |
30/55 |
|
Rowsey et al[6] |
77.15 |
4/70 |
|
EPSWA[169] |
58.5 |
114/195 |
|
* |
These two series from the same institution partially overlap. |
TABLE 184.4 -- Classification of Isolates in Culture Positive Postoperative Endophthalmitis
|
Coagulase Negative Staphylococci/ |
||||||
|
Author |
Staphylococcus epidermidis |
Staphylococcus aureus |
Streptococcus species |
Other Gram Positive |
Gram Negative |
Fungal |
|
Driebe et al[4][*] |
38% (24/63) |
21% (13/63) |
11% (7/63) |
6% (4/63) |
16% (10/63) |
8 (5/63) |
|
EVS[1][?] |
70% (226/323) |
10% (32/323) |
9% (29/323) |
5% (17/323) |
6% (19/323) |
|
|
Forster et al[9][*] |
18% (14/78) |
9% (7/78) |
21% (16/78) |
10% (8/78) |
29% (23/78) |
13% (10/78) |
|
Olson et al[77] |
38% (11/29) |
24% (7/29) |
17% (5/29) |
10% (3/29) |
7% (2/29) |
4% (1/29) |
|
Pavan et al[2][?] |
49% (19/39) |
5% (2/39) |
13% (5/39) |
13% (5/39) |
21% (8/39) |
|
|
Puliafito et al[7] |
39% (20/51) |
4% (2/51) |
10% (5/51) |
16% (8/51) |
29% (15/51) |
2% (1/51) |
|
Rowsey et al[6] |
28% (17/61) |
15% (9/61) |
3% (2/61) |
31% (19/61) |
15% (9/61) |
8% (5/61) |
|
EPSWA[169] |
61/113 |
24/113 |
25/113 |
3/113 |
16/131 |
2/131 |
|
* |
Enterococcus species classified as Streptococcus species in the study. |
|
? |
Bacterial endophthalmitis cases only were included in the study. |
Samples for culture should be obtained from the anterior chamber and vitreous cavity. Vitreous samples are most important, as it has been demonstrated that the vitreous is more readily infected than the anterior chamber.[38] Aqueous samples may be useful, but are often negative despite positive vitreous cultures.[4, 9, 70] Uncommonly, a negative vitreous culture result may be accompanied by a positive anterior chamber culture; therefore, both anterior chamber and vitreous cultures should always be performed.[4, 5]
Table 184.5 summarizes the microbiologic investigations that should be performed in suspected endophthalmitis. Gram-stained smears of ocular specimens may provide rapid diagnostic information, but may be inappropriately negative or inconsistent with culture results in approximately one-third of cases.[6, 71] As such, the usefulness of the Gram stain in directing therapy is limited. In suspected fungal endophthalmitis, evaluation by calcofluor white or other stains may allow rapid identification of fungal elements.[72]
TABLE 184.5 -- Microbiologic Investigations in Suspected Endophthalmitis
|
Specimen Collection |
||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||
|
Microbial Detection |
||||||||||||||||||||||||||||||||||||||||||||||||
|
Specimens should be cultured on a variety of media as indicated in Table 184.5. Anaerobic organisms are very sensitive to refrigeration and, therefore, samples with suspected anaerobes should be kept at room temperature before plating.[73] Large-volume vitrectomy specimens are passed through membrane filter systems to concentrate and collect organisms, thus increasing culture yield. A simplified culture technique involving the direct inoculation of vitreous specimens into blood culture bottles has demonstrated a very high rate of recovery of organisms, and compares favorably with the more definitive membrane filter technique.[74] This technique may be particularly useful in patient care settings with limited microbiologic laboratory support.
Data from the EVS have raised new questions about the role and costs of aqueous and vitreous cultures in the management of postoperative endophthalmitis. In this series of 420 patients, carefully defined as postcataract or postsecondary IOL implantation endophthalmitis with symptoms and signs presenting within 6 weeks of surgery, treatment was assigned and administered before culture results were available, and no additional treatment modifications were made in 91% of patients.[1] In fact, the actual number managed without regard to culture results was even higher, although these data have not yet been released. In many of the remaining 9% who had an additional procedure performed (e.g., reculture, repeat intravitreal injection, vitrectomy), the management step was also independent of the culture result, and was based on worsening clinical condition, media reopacification, and other symptoms and signs. Finally, it is not clear how many of the culture-informed additional treatment decisions resulted in successful clinical outcomes, raising further questions about the usefulness of intraocular cultures.
Despite these considerations, more compelling arguments may be made to retain the practice of obtaining pretreatment aqueous and vitreous cultures. They are easily performed with low morbidity, establish a definitive diagnosis, allow epidemiologic study of postoperative infection, and permit ongoing microbiologic evaluation of specific pathogens and drug sensitivities. All of these factors will improve patient outcomes with further study. Consequently, routine intraocular cultures should be included in the management of postcataract endophthalmitis until this information is stabilized or exhausted.
Conjunctival and eyelid cultures have limited utility because, although they often yield the same organism as that within the eye, they may sometimes be falsely negative or positive with an unrelated organism. However, because of ease of obtaining such specimens, they may be carried out as a supplement to intraocular cultures. In patients with blepharitis, wound dehiscence, or filtration bleb endophthalmitis with prominent exudate, the concordance of positive conjunctival and lid cultures with intraocular cultures lends support to the suspected route of infection and may indicate the need for external therapy. This may be particularly important if the fellow eye is in jeopardy (e.g., presence of a filtration bleb) or is to be considered for intraocular surgery at a later date.
The use of other techniques such as immunocytochemistry and electron microscopy for the rapid identification of microbial pathogens in endophthalmitis has been met with limited success.[73] Difficulty with these approaches has been due to subectivity in interpreting results. Molecular biologic techniques, such as in situ hybridization and polymerase chain reaction, may provide future advances in the rapid laboratory diagnosis of infectious endophthalmitis.[75] Rickman and associates reported a case of chronic uveitis due to the Whipple disease bacillus (Tropheryma whippelii) that was diagnosed on the basis of light and electron microscopy of vitreous specimens.[76] Polymerase chain reaction detection of T. whippelii 16S ribosomal RNA gene sequences in the vitreous confirmed the diagnosis and suggested that ocular involvement was due to local bacterial infection rather than immune-mediated processes. Undoubtedly, more cases of infectious endophthalmitis masquerading as uveitis will be diagnosed in the future by these methods.
MICROBIOLOGIC SPECTRUM
Review of large clinical series indicates that 56-90% of isolates in postoperative endophthalmitis are gram-positive, 7-29% are gram-negative, and 3-13% are fungal (see Table 184.4).[4, 6, 7, 9, 77] In general, postoperative infections involve a single organism, although an incidence of mixed infection as high as 33% has been reported.[7] Of gram-positive isolates, 30-74% are coagulase-negative staphylococci (S. epidermidis), 6-30% are Staphylococcus aureus, and 10-30% are Streptococcus species. Of gram-negative isolates, ?30-40% are Proteus species, 20% are Pseudomonas aeruginosa, and 20% are Haemophilus species. Microbiologic results of the EVS, the largest endophthalmitis clinical study to date, indicated that 94% of isolates were due to gram-positive organisms, and 70% of isolates were due S. epidermidis alone.[1]
The microbiologic spectrum differs in other clinical categories of endophthalmitis. H. influenzae, rarely seen in postcataract infection, is frequently implicated in late bleb-associated endophthalmitis, as are streptococci.[78-80] Bacillus species are one of the most frequently encountered pathogens in endophthalmitis after penetrating trauma, being implicated in 26-46% of patients.[81-84] Cases have also been reported after sepsis with this organism.[85, 86] Bacillus species are not seen in the postoperative setting.
MEDICAL THERAPY
Medical intervention is the mainstay of endophthalmitis therapy. Table 184.6 summarizes recommended drugs and dosages for medical therapy, and practical management guidelines are suggested in Table 184.7.
TABLE 184.6 -- Postoperative Endophthalmitis: Suggested Doses for Medical Therapy
|
Suspected Bacterial Cases |
|
Intravitreal Injection* |
|
Vancomycin 1.0 mg |
|
Subconjunctival injection |
|
Vancomycin 25 mg |
|
Dexamethasone 2-24 mg |
|
Topical therapy |
|
Vancomycin 50 mg/mL, q 1-4 h, staggered with |
|
Systemic therapy? |
|
Vancomycin 1.0 g IV q 12 h |
|
or |
|
Suspected Fungal Cases |
|
Intravitreal Injection |
|
Amphotericin B 5-10 mg |
|
Systemic therapy[§] |
|
Ketoconazole 400-600 mg daily PO |
|
* |
Intravitreal injections are not repeated unless repeat smear or culture demonstrates persisting organisms or profound clinical deterioration occurs despite initial injections. |
|
? |
Intravitreal dexamethasone may be considered in all cases but is of particular benefit in cases with more severe inflammation. Its use remains experimental. |
|
? |
Systemic antibiotic therapy, if administered, should be given for 5-7 days. |
|
§ |
Systemic amphotericin is associated with a high incidence of side effects. Ketoconazole and fluconazole appear to be safer alternatives for cases in which systemic therapy is desired.[226,230] Some studies suggest that successful therapy of postoperative fungal endophthalmitis may be accomplished without systemic administration of antifungal agents. |
TABLE 184.7 -- Postoperative Endophthalmitis: Suggested Guidelines for Therapy
|
1. Aqueous and vitreous specimens should be obtained for culture in all suspected cases. |
|
2. For suspected fungal endophthalmitis, calcofluor white technique should be performed on fresh vitreous specimens for evaluation of fungal elements. |
|
3. Medical therapy should be promptly administered in all cases, as suggested in Table 184-6. |
|
4. For postcataract endophthalmitis, immediate vitrectomy should be performed in eyes with light-perception - only vision at the initial visit. Routine immediate vitrectomy is not necessary in eyes presenting with better than light-perception vision. Limited vitrectomy should also be performed for failure of initial therapy, blebassociated endophthalmitis, chronic endophthalmitis, and fungal endophthalmitis. |
|
5. An intraocular lens should be retained except in infection with filamentous fungi. |
|
6. Patients should be monitored for toxicity owing to systemic antimicrobial therapy. |
ANTIBIOTIC THERAPY
Intravitreal Therapy
Intravitreal antibiotic injection is the principal element of endophthalmitis treatment. In 1944, von Sallmann and colleagues demonstrated that intravitreal injection of penicillin successfully treated S. aureus endophthalmitis in the rabbit.[87] Their study represented a major turning point in the therapeutic approach to endophthalmitis. Intravitreal antibiotic therapy has subsequently been an area of extensive research, resulting in dramatic improvements in the possibility for salvaging vision in endophthalmitis.[9, 38, 88-110]
The ideal antibiotic for intravitreal injection (1) is efficacious against offending organisms, (2) is nontoxic to the retina and other ocular structures at bactericidal doses, and (3) has an appropriate half-life within the vitreous to be therapeutic. Antibiotics should ideally be injected before irreversible destruction of the retina and other ocular tissues occurs. In order to facilitate prompt therapy, and because of known inaccuracies in Gram's stain evaluation of vitreous samples,[6, 71] agents must be selected before culture results are obtained, and coverage with a combination of antibiotics directed against both gram-positive and gram-negative organisms is required. Consideration of the clinical setting (e.g., postoperative, penetrating trauma) provides an indication of probable causative organisms.
Given the microbiologic spectrum encountered with postcataract endophthalmitis, antibiotic coverage of staphylococci is critical. With methicillin and cephalosporin resistance being common among staphylococci, particularly in the nosocomial setting,[111-113] vancomycin is currently the intravitreal agent of choice for gram-positive coverage.[1, 77, 81, 103, 108, 114] Studies in the rabbit demonstrate no evidence of retinal toxicity at the dose (1.0 mg) recommended for intravitreal use in patients.[101, 103, 110] The recent emergence of vancomycin resistance among enterococci and reports of resistance in staphylococci[115] indicate the need for ongoing evaluation of recommended drugs as bacterial sensitivity and resistance patterns inevitably change over time.
Aminoglycosides continue to be efficacious against the majority of gram-negative organisms. Concerns about the retinal toxicity of these agents have made them the subject of considerable study.[90-92, 95-97, 102, 104, 105,116-119] A 100-?g dose of gentamicin has not been reported to produce toxicity in the rabbit, but outer retinal toxicity consisting of alterations in the retinal pigment epithelium and photoreceptor layers has been noted with a 200-?g dose.[96, 105] Higher doses produce extensive disruption of the retinal pigment epithelium-photoreceptor layers, and full-thickness retinal necrosis is observed with intravitreal doses greater than 1.0 mg. Studies in the primate suggest that a 500-?gdose of gentamicin does not produce retinal alterations.[102, 116] With increasing gentamicin resistance among ocular isolates,[111, 120] amikacin has now become the aminoglycoside of choice.[104, 121] Studies suggest that retinal toxicity occurs at a threshold dose of 750 ?g for this drug.[97]
In the mid-1980s, there appeared reports of pronounced retinal toxicity due to inadvertent intravitreal injection of large doses (up to 40 mg) of gentamicin intended for subconjunctival injection at the end of cataract surgery.[117] This condition of macular infarction, characterized by macular edema and extensive capillary nonperfusion, results in permanent loss of central vision in nearly all patients. Because of growing concern regarding the safety of aminoglycoside administration, Campochiaro and Conway reviewed 93 cases of aminoglycoside-related macular infarction (Fig. 184.6).[118, 122] Approximately two-thirds of these cases occurred in eyes that had undergone treatment for endophthalmitis, and 23 cases occurred with prophylactic subconjunctival antibiotic injection after routine ocular surgery. Although gentamicin was implicated in most patients, cases of infarction were also observed with tobramycin and amikacin. Most cases of macular infarction after intravitreal gentamicin administration occurred in eyes that received 400 ?g aftervitrectomy, but a significant number may have occurred after injection of doses intended to contain 100 or 200 ?g, doses preiously considered safe.[123] Similarly, cases in eyes supposedly receiving 400 ?g of amikacin were observed, although the retinal toxicity of this agent is purported to be less.[86]
|
|
|
|
FIGURE 184.6 (a) Fundus photograph of macular infarction syndrome occurring after subconjunctival gentamicin injection. Optic disk pallor, vascular attenuation, whitening and swelling of the retina in the macular area, and scattered intraretinal hemorrhages are seen. (b) Fluorescein angiogram of the same eye demonstrates abrupt nonperfusion of first-order arterioles and capillaries in the macular area and blocking defects secondary to intraretinal hemorrhages. |
These data have led some clinicians to question the use of any dose of intravitreal aminoglycoside, but such an interpretation must be balanced with available information. In a study by Narvaez and co-workers[124] in which pharmacists, ophthalmologists, and assistant personnel were asked to prepare aminoglycoside dilutions by a variety of methods, only pharmacist-prepared solutions achieved target concentrations on final analysis. Ophthalmologists in the study achieved wide variations in dosage (many in the clearly toxic range) when diluting the drug according to self-devised calculations, but were able to follow with acceptable accuracy an established dilution scheme with instructions prepared by a pharmacist. However, the authors documented that none of the assistant personnel ever achieved accurate doses, regardless of the degree of written instruction provided, with doses routinely miscalculated into the highly toxic range. These data suggest that ancillary personnel should not prepare drugs for intraocular injection, and that some cases of reported aminoglycoside toxicity with 'safe' doses may in fact be dosage errors. The EVS group found that of the 420 postcataract endophthalmitis patients enrolled in the study, only one case of macular infarction was reported despite all patients having received intravitreal amikacin as part of their treatment regimen.[1]
Ceftazidime is a third-generation cephalosporin that displays excellent activity against almost all gram-negative ocular isolates.[125] Microbiologic analysis of gram-negative endophthalmitis suggests that the coverage provided by ceftazidime is equivalent to that of aminoglycosides.[125, 126] However, ceftazidime has limited activity against gram-positive organisms, particularly staphylococci. Resistant gram-positive organisms include Enterococcus faecalis.[127] Studies in the monkey demonstrate that an intravitreal dose of 2.25 mg (recommended for use in patients) does not appear to be toxic to the retina.[128]Animal studies have confirmed the efficacy of intravitreal ceftazidime, and reports of its use in patients with bacterial endophthalmitis have been encouraging.[129-131]
At the present time, concerns regarding the intraocular safety of aminoglycosides have led some clinicians to advocate the substitution of intravitreal ceftazidime for gram-negative coverage.[128-130] Others maintain that the theoretical advantages of aminoglycosides over ceftazidime (e.g., concentration-dependent killing, synergy with vancomycin against enterococci, streptococci, and staphylococci) and broader clinical experience with these agents support the continued use of amikacin.[132] Current experience suggests that either drug can be used efficaciously and safely with appropriate preparation.
In the EVS population, carefully defined to include postcataract and postsecondary IOL cases only, the incidence of gram-negative pathogens was remarkably low (4.1% of cases) compared with previous series.[1] This has raised the possibility of eliminating gram-negative intraocular coverage entirely or restricting it to a subgroup if defining features are present at outset. In the EVS, no patient with retinal vessels visible by ophthalmoscopy at presentation was found to have infection with a gram-negative organism. Johnson and co-workers suggest that the use of these data to guide empirical antibiotic therapy is not recommended, as the predictive value of presenting clinical features are not sufficiently strong.[61] For example, gram-negative endophthalmitis may present early, before the development of significant media opacification. In addition, the relative intraocular safety and potential therapeutic synergy between agents such as vancomycin and an aminoglycoside suggest that administration of initial broad-spectrum coverage in the absence of microbiologic data should still occur.
Antibiotics injected intravitreally diffuse quickly throughout the vitreous cavity, rapidly achieving therapeutic levels.[133] Clearance of drug from the vitreous occurs either anteriorly through aqueous outflow channels (vancomycin and aminoglycosides) or posteriorly across the retina (cefazolin and clindamycin).[134, 135] Third-generation cephalosporins (ceftazidime) may be eliminated by both routes.[136] Drugs cleared anteriorly have half-lives that are generally longer than that of drugs cleared posteriorly.[134-137] Antibiotic clearance is significantly increased in aphakic or vitrectomized eyes.[136, 138-141] Intraocular inflammation may increase or decrease clearance depending on the primary route of drug elimination.[135-141]
In rabbit models, the half-life of intravitreal vancomycin in the uninflamed phakic eye is 25.1 h, and is reduced to 9.0 h in the uninflamed aphakic-vitrectomized eye.[141] The half-life of amikacin is 25.5 h in the uninflamed phakic eye, and decreases to 7.9 h in the aphakic-vitrectomized eye.[139] Ceftazidime has a half-life of 13.8 h in the uninflamed phakic eye, and this is reduced to 4.7 h in the aphakic-vitrectomized eye.[140] Modest reductions in the half-lives of vancomycin[141] and amikacin,[139] but not that of ceftazidime,[140] are noted with coexisting inflammation (in addition to aphakia and vitrectomy). These data collectively suggest that drug clearance is greatest in aphakic-vitrectomized eyes, and that the half-lives of antibiotics in this setting cluster around values of 5-8 h. Extrapolation of these data to humans suggests that most intravitreal antibiotics may be maintained at potentially effective concentrations for ?48 h after initial injection.[142, 143]
Although a single dose of intravitreal antibiotic is usually successful in sterilizing the eye, several studies have shown that infection may persist in some patients.[4, 77, 107, 125, 143-145] Persistent infection may occur with virulent organisms, such as streptococci and gram-negative bacteria (e.g., Pseudomonas), or with slowly replicating organisms, such as Propionibacterium acnes and fungi. Failure of therapy may also occur if organisms are not sensitive to the antibiotics chosen. Shaarawy and associates reviewed patients with persistently culture-positive endophthalmitis and found that these eyes had worse visual outcome compared with eyes that were culture-negative on repeat sampling.[143] The results of this study may, however, be limited by its small sample size and retrospective nature. With clinical and experimental data to suggest that a single injection of antibiotics is not uniformly effective, some clinicians have suggested that a second intravitreal injection may be valuable at 48 h after the initial dose in certain cases (e.g., poor clinical response, virulent organism isolated).
Oum and colleagues examined the safety of repeated injections of vancomycin-aminoglycoside combinations in the rabbit.[146, 147] The authors demonstrated no toxicity with a single injection, but repeated injections at intervals of 48 h were associated with increasing degrees of retinal toxicity. Stern reinjected rabbit eyes with only one antibiotic (vancomycin or an aminoglycoside) and found that toxicity still occurred.[148] Thus, although the value of repeated intravitreal injections is unknown, toxicity data suggest that this practice should be discouraged and may minimize potential antibiotic toxicity in eyes that do not require any additional therapy. The role of systemic antibiotics or corticosteroids in improving outcome in persistent infection deserves further examination, and these may prove to be safer alternatives.
Systemic Therapy
The penetration of systemically delivered antibiotics into the vitreous cavity is impeded by the blood-eye barrier.[134, 149] Consequently, vitreous levels after systemic antibiotic administration are usually extremely low in eyes with intact blood-eye barriers and normal vitreous. Intravitreal penetration is enhanced by inflammation, which causes breakdown of the blood-eye barrier, and also by vitrectomy.[136, 150-153] Moreover, repeated administration may result in progressive accumulation of antibiotic in the vitreous and even higher levels compared with a single dose.[151-153]
Studies in the rabbit have demonstrated that inflammation, removal of the lens, and vitrectomy significantly increase the penetration of cefazolin,[153] ceftazidime,[151] and vancomycin[152] into the vitreous. Levels above the minimal inhibitory concentration (MIC) for target organisms can be achieved, particularly in aphakic-vitrectomized eyes. Quinolones, such as ciprofloxacin and ofloxacin, also achieve intraocular levels above the MIC of many ocular pathogens, even in the absence of inflammation or vitrectomy.[154-163] These agents have become attractive to clinicians because they may achieve significant levels after intravenous or oral administration. In contrast, human and animal studies demonstrate that systemically administered gentamicin and amikacin do not reach therapeutic levels, even in conditions optimized to enhance intraocular penetration.[150, 163-165]
As previously mentioned, antibiotic concentrations in the vitreous cavity may fall below therapeutic levels by ?48 h after initial intravitreal injection, and endophthalmitis caused by virulent organisms may occasionally not be sterilized by a single injection of antibiotic. For these reasons, many clinicians advocate the use of 5-10 days of adjunctive systemic antibiotics as part of their treatment regimen. It should be noted that patients on systemic therapy require monitoring for drug side effects, particularly renal toxicity resulting from vancomycin or aminoglycoside administration.
Concerns regarding the efficacy, cost (including prolonged hospitalization),[166] and side effects of systemic antibiotics resulted in the evaluation of this mode of therapy in the EVS.[1] This randomized prospective clinical trial evaluated the role of systemic antibiotics in patients with postcataract endophthalmitis and found that adjunctive intravenous amikacin and ceftazidime did not improve the outcome of therapy (ciprofloxacin was substituted for penicillin-allergic patients unable to receive ceftazidime). As such, it was concluded that systemic antibiotics were unnecessary in the management of postcataract endophthalmitis. These data and the EVS systemic antibiotic protocol have been criticized at length.[142, 167, 168] The systemic agents chosen in the EVS were presumably optimized for vitreous penetration, based on previous studies, but were not selected for optimal gram-positive coverage. As postoperative endophthalmitis is overwhelmingly a gram-positive disease, the antibiotic selection in the study is open to question. For patients with satisfactory results and good visual outcomes, it is clear that the simplest treatment regimens are preferred and that any additional therapeutic elements, including systemic antibiotics, are irrelevant if results are excellent without them. However, for patients with unsatisfactory results and poor visual outcomes, the EVS data establish only that treatment with these questionably chosen antibiotics was as ineffective as omitting them. The Endophthalmitis Population Study of Western Australia (EPSWA)'s Fifth Report,[169] a retrospective, 21-year period study, of 213 cases showed that treatment with oral antibiotics was associated with improved visual acuity outcome. The authors comment that a variety of ocular antibiotics were used in the study and do not specify which one was found to be probably more potent.
Although data regarding laboratory sensitivities of study organisms have been offered for hypothetical analysis in an attempt to defend the relevance of the systemic treatment data, it is clear that the many factors involved in translating laboratory sensitivities and drug penetration to clinical treatment render this analysis problematic. Therefore, the possibility remains that more appropriate systemic antibiotics may improve outcomes in certain subgroups of patients now or in the future, and clinicians are encouraged to utilize ongoing judgment in the administration or avoidance of systemic antibiotics in subgroups with poor outcomes. Further evaluation of agents (e.g., vancomycin, quinolones) that better penetrate the vitreous cavity and that are more effective against gram-positive organisms appears warranted. Finally, clinicians should be wary of extrapolating the EVS results to other clinical settings, such as bleb-associated and posttraumatic endophthalmitis. These forms of endophthalmitis were not evaluated in the study, and as such, the role of systemic antibiotics in these cases remains undetermined.
Local Therapy
Topical and subconjunctival antibiotics are also usually administered during endophthalmitis therapy. Although these routes of administration achieve therapeutic levels in the anterior chamber, penetration of antibiotic into the vitreous is negligible.[158, 170, 171]
CORTICOSTEROID THERAPY
Intraocular, periocular, and systemic corticosteroids have been increasingly used to ameliorate inflammation and intraocular tissue damage in endophthalmitis. Although the rationale for antiinflammatory therapy is to preserve retinal tissue and function by decreasing inflammatory tissue destruction, there has been concern that adjunctive corticosteroids may impair bacterial eradication. As such, it remains unclear whether this modality is to be reserved for infections caused by more virulent organisms (in which the inflammatory response is more severe), or whether it may be employed more widely.
Animal studies have variably supported the efficacy of adjunctive corticosteroid therapy,[38, 109, 172-177] and clinical success in association with intravitreal antibiotic injection and vitrectomy has also been reported.[178] In 1955, Maylath and Leopold demonstrated that the combination of antibiotics and corticosteroids was better than antibiotics alone in decreasing inflammation in a rabbit model of S. aureus endophthalmitis.[38] Later, Graham and Peyman showed that intravitreal dexamethasone and gentamicin, if administered within 5 h of infection, resulted in decreased inflammation and faster clearing of media in a rabbit model of P. aeruginosa endophthalmitis.[172] Experimental studies using animal models of S. epidermidis endophthalmitis have found adjunctive corticosteroids to be beneficial.[173-175]Meredith and co-workers found the combination of vitrectomy, intraocular antibiotics, and corticosteroids to be the most successful regimen for decreasing inflammation.[175] Park and associates demonstrated that intravitreal vancomycin and dexamethasone resulted in significantly less intraocular inflammation and greater retinal tissue preservation compared with vancomycin alone in a rabbit model of Streptococcus pneumoniae endophthalmitis.[176] Stern quantitatively examined the effect of corticosteroids on microbial eradication in a rabbit model of S. aureus endophthalmitis and demonstrated that the addition of intravitreal dexamethasone to intravitreal vancomycin therapy had no effect on bacterial killing.[148]
Graham and Peyman first noted that 400 ?g of dexamethasone injected intravitreally did not produce retinal toxicity on ophthalmoscopy, electroretinography, or light microscopy.[172] This was confirmed by Kwak and D'Amico, who found that a 440-?g dose of intravitreal dexamethasone only caused a transient and reversible increase in Müller cell staining.[179] Doses of 800 ?g and higher caused increasing retinal disorganization.
Clinical studies examining the efficacy of corticosteroids and comparing routes of administration have yet to be performed. Nonetheless, the use of adjunctive intraocular corticosteroids continues to gain acceptance, with some clinicians recommending it routinely as part of initial endophthalmitis therapy. Further studies are required to define the role of this promising modality.
VITRECTOMY
The role of vitrectomy in the treatment of endophthalmitis has been examined in animal studies and clinical series. Potential benefits of vitrectomy include obtaining a better vitreous sample for culture, more rapid restoration of media clarity, more rapid and complete sterilization of the vitreous cavity, removal of toxic bacterial products and products of inflammation, and enhancement of systemic antimicrobial penetration into the eye. Disadvantages of vitrectomy may include the possibility of treatment delays associated with surgery, increased risk of iatrogenic complications (e.g., retinal hole, retinal detachment, choroidal hemorrhage), and reduction in the half-life of intravitreally administered antibiotics.
The benefits of vitrectomy have been generally supported in a number of experimental studies. Cottingham and Forster evaluated a phakic rabbit model of S. aureus endophthalmitis and found that intravitreal antibiotics alone were curative only when injections were given within the first 24 h of infection.[180] In eyes with more established disease (treated between 25 and 31 h and between 40 and 49 h after infection), the addition of vitrectomy to intravitreal antibiotic therapy significantly raised the rate of treatment success, as determined by posttreatment culture results. These findings have been confirmed by Stern.[148] Talley and colleagues examined the role of vitrectomy in an aphakic rabbit model of S. aureus endophthalmitis.[181] The authors showed that intravitreal antibiotics alone were as successful as a combination of vitrectomy and intravitreal antibiotics in sterilizing the eye, but media clarity was significantly improved at 14 days in eyes receiving vitrectomy. Aguilar and co-workers also compared treatment strategies for experimental S. aureus endophthalmitis in the aphakic rabbit eye and found that the combination of vitrectomy and intravitreal antibiotics was more effective than injection of antibiotics alone in reducing clinical inflammation scores and reducing positive culture results.[177] Similarly, Meredith and co-workers demonstrated that the addition of vitrectomy to medical therapy improved inflammatory scores in an aphakic rabbit model of S. epidermidis endophthalmitis.[175]
Until recently, clinical series examining the role of vitrectomy in endophthalmitis were limited by their retrospective nature. In addition, vitrectomy was invariably offered in cases that appeared more advanced on initial presentation, with an expected bias toward the poorer prognosis observed in these eyes. As a result, some clinical series reported worse visual outcomes in eyes treated with vitrectomy while others reported better outcomes in similarly treated eyes.[4, 8, 9, 77, 125, 182]
The role of vitrectomy in the therapy of postoperative endophthalmitis was therefore examined in the EVS, a randomized, prospective, multicenter clinical trial.[1] In the study, 420 patients with clinical features of bacterial endophthalmitis developing within 6 weeks after cataract surgery or secondary lens implantation were randomized to receive either immediate pars plana vitrectomy or vitreous tap-biopsy as part of their management. Treatment outcome was evaluated by determining visual acuity and media clarity at 9 months. In patients whose visual acuity at presentation was hand motions or better, no improvement in visual acuity was provided by vitrectomy, compared with vitreous tap or biopsy. Over 60% of such eyes achieved 20/40 or better visual acuity regardless of whether vitrectomy was performed, and less than 5% suffered severe visual loss (5/200 or worse visual acuity). However, in patients with initial light-perception-only vision, immediate vitrectomy provided a threefold increase in the frequency of achieving 20/40 or better visual acuity, a twofold increase in the frequency of achieving 20/100 or better visual acuity, and half the frequency of severe visual loss. Vitrectomy also offered more rapid clearing of media, although this was not associated with a concomitant rapid improvement in visual acuity. The results of the EVS therefore suggest no benefit from routine immediate vitrectomy in postcataract endophthalmitis patients presenting with better than light-perception vision. In patients presenting with light-perception-only vision, immediate pars plana vitrectomy significantly increases the likelihood of improved visual outcome. The role of therapeutic vitrectomy in other clinical settings (e.g., bleb-associated and chronic endophthalmitis) has not been fully defined and therefore continues to be an important part of management in these cases.
Until recently, studies[183, 184] have suggested a higher complication rate associated with vitrectomy than with vitreous tap, with retinal detachment occurring in up to 21% of vitrectomized eyes in one series.[183] However, selection bias may have been responsible for these results. In the EVS, retinal detachment occurred in only 20 of 420 patients (5%). In fact, the frequency of retinal detachment was significantly lower in eyes receiving vitrectomy (6 of 218 patients) compared with eyes receiving vitreous tap (14 of 202 patients).[1] A study by Kaynak et al[185] compared the vitrectomy for endophthalmitis as an initial procedure according to the EVS study to a more radical approach of vitrectomy combined with an encircling band, silicone tamponade and endolaser. The authors found a significant better anatomic and visual outcome in the group of patients that were treated more radically.
A recent study examined if the EVS - published in 1995 - changed significantly the diagnosis and management of postoperative endophthalmitis.[169] In a 21-year period, and 213 cases of endophthalmitis, the authors reported a significant increase in anterior chamber and vitreous sampling. The overall use of vitrectomy was also reported to have an increasing tendency, but no difference according to presenting visual acuity was observed. The role of intravitreal antibiotics increased significantly, whereas the use of both subconjunctival and IV antibiotics decreased. Vitrectomy in all patients increased marginally, but there was no difference in its use, according to the presenting visual acuity. The study reported a halving of enucleation or evisceration since 1995 and concludes that vitrectomy has provided a better overall cosmetic outcome by reducing chronic inflammation and limiting globe shrinkage. The authors conclude that although a noticeable change in the diagnosis and management of endophthalmitis was observed since the EVS report, the visual outcomes have not improved and still remain poor.
PROGNOSIS
The visual outcome of infected eyes may be predicted by a number of variables. Presenting visual acuity appears to be the most important prognostic indicator, with poor initial vision being associated with a decreased final visual acuity.[1, 5, 186] The species of organism implicated is also associated with visual prognosis. Data from the EVS confirm that infection with more virulent organisms, in particular noncoagulase-negative staphylococci (i.e., S. aureus), streptococci, enterococci, and gram-negative species (particularly Pseudomonas), portends a poorer visual prognosis.[186] The EVS group found that presenting visual acuity was more powerful than microbiologic factors in predicting visual outcome and response to vitrectomy.[186] However, the two factors are interrelated, as organisms of higher virulence tend to be clustered in cases presenting with poor initial vision. The EPSWA's Fifth Report[169] found no correlation between admission and final visual acuity but instead reported that discharge visual acuity was a significant predictor of long-term acuity. It is possible that discharge visual acuity is a de facto indicator of the success and timing of treatment and the virulence of the underlying infective process. Other factors such as culture positivity, Gram-stain positivity, delays before instituting therapy, concomitant ocular disease (e.g., rubeosis, retinal detachment), and concurrent diabetes are also prognostic risk factors.[1, 4, 7, 186] In addition, corneal infiltrate or ring ulcer, an open posterior capsule, and absence of the red reflex predict a decreased visual outcome.[1]
PROPHYLAXIS
Prophylactic measures in ocular surgery are intended to sterilize the ocular surface and periocular tissues and to exclude pathogenic organisms from entering the surgical field. Important steps in endophthalmitis prophylaxis are summarized in Table 184.8.
TABLE 184.8 -- Recommendations for Prophylaxis of Postoperative Endophthalmitis
|
Preoperative |
|||||||||||||||||||||
|
|||||||||||||||||||||
|
Intraoperative |
|||||||||||||||||||||
|
|||||||||||||||||||||
|
Postoperative |
|||||||||||||||||||||
|
DRAPING
The routine use of drapes is to exclude the eyelids and lashes from the operative field. These sites represent a rich source of potential ocular pathogens.
TOPICAL POVIDONE IODINE
Field sterilization has become a priority in preventive measures. The use of topical antiseptic agents such as povidone iodine (Betadine) is routine for skin preparation prior to surgery. Studies conducted in the 1980s demonstrated the bacterial efficacy of topical povidone iodine on the ocular surface.[187, 188] Povidone iodine is minimally toxic, is inexpensive, and has a broad spectrum of activity, making it an ideal agent for preparation of the ocular surface and surrounding tissues before surgery. By the early 1990s, use of topical povidone iodine in preoperative conjunctival and eyelid preparation gained popularity following demonstration of superiority to silver protein solution in reducing the risk of postoperative endophthalmitis. A variety of bacterial endophthalmitis prophylaxis measures were reviewed and preoperative povidone iodine preparation was found to be the only recommended technique based on the current clinical evidence.[189] Isenberg and associates demonstrated that a single application of topical 5% povidone iodine solution has a bactericidal effect that is equivalent to a 3-day course of topical antibiotics.[187] Apt and colleagues found that its efficacy is further enhanced by concurrent use of topical antibiotics, with 83% of conjunctival cultures being negative after combination therapy.[188]
Subsequently, Speaker and Menikoff conducted a controlled, nonrandomized trial to determine the efficacy of povidone iodine in decreasing the incidence of postoperative endophthalmitis.[190] Their study found that preoperative administration of topical 5% povidone iodine solution into the conjunctival sac significantly reduced the incidence of culture-positive endophthalmitis compared with silver protein solution. Moreover, no adverse reactions were reported with its use.
Recently, Isenberg and co-workers demonstrated that povidone iodine solution applied to the eye at the conclusion of surgery was as effective as topical antibiotics in reducing the conjunctival bacterial flora during the first postoperative week.[191] The efficacy of this and other modes of postoperative prophylaxis in reducing the incidence of endophthalmitis is uncertain and requires further study.
ANTIBIOTIC PROPHYLAXIS
Preoperative Antibiotic Prophylaxis
Antibiotic prophylaxis of endophthalmitis is widely employed, but difficulties in rationalizing certain practices exist owing to the low incidence of this complication, a lack of controlled trials in contemporary surgical settings, and the medicolegal climate surrounding the potentially catastrophic outcome of this disease. Evidence to date suggests that the use of antibiotic prophylaxis reduces the incidence of postoperative endophthalmitis. However, the appropriate routes of delivery, timing, antibiotic choices, and dose regimens are less clear, based on available data. Studies in general surgery and ophthalmology currently indicate that the administration of antibiotic prophylaxis has greatest efficacy during the preoperative and intraoperative stage, rather than in the postoperative period.[12, 192]
Preoperative topical antibiotics effectively reduce bacterial counts on the ocular surface and decrease the incidence of postoperative endophthalmitis.[193-195] In addition, some agents, such as ofloxacin and levofloxacin, are capable of penetrating the cornea to achieve significant intraocular concentrations.[196]
However, sterilization of the ocular surface is not invariably achieved, as infection still occurs, often by organisms sensitive to the agents used.[195, 197] Topical antibiotic agents currently used include aminoglycosides, polymyxin B-trimethoprim, and fluoroquinolones. Aminoglycosides display a broad spectrum of coverage. With increasing resistance to gentamicin among coagulase-negative staphylococci, tobramycin has become the aminoglycoside of choice.[112] The combination of polymyxin B and trimethoprim acts synergistically to provide broad-spectrum coverage and demonstrates efficacy similar to that of tobramycin in reducing the ocular surface flora.[198] Fluoroquinolones such as ciprofloxacin and ofloxacin have recently become available for topical use. These potent new agents display tremendous activity against most aerobic organisms, including methicillin-resistant staphylococci, and display greater in vitro activity against ocular bacterial isolates compared with aminoglycosides and polymyxin B. Ofloxacin has been shown to be as effective as tobramycin in sterilizing the lids and ocular surface preoperatively.[199]
Currently, there is a lack of comparative data regarding the effectiveness of these agents in preventing endophthalmitis. Despite decades of routine use of topical antibiotics, studies supporting this prophylactic measure for risk reduction[12] have been criticized for methodological flaws.[200] Schmitz et al[16] reported an increased risk of postoperative endophthalmitis associated with preoperative topical antibiotics. There is concern among clinicians that the indiscriminant use of newer agents, such as quinolones, may facilitate the emergence of bacterial resistance. Nonetheless, preoperative topical antibiotics, in particular fluoroquinolones, continue to be widely used in the prevention of postoperative endophthalmitis[201, 202] and are generally believed to contribute beneficially to risk reduction.[200]Further studies are required to assist in rationalizing the use of antibiotics for endophthalmitis prophylaxis.
The timing and frequency of topical antibiotic administration has also been studied. Ta et al in a prospective, randomized study, compared the administration of topical ofloxacin 1 h prior to surgery to q.i.d. administration for 3 days prior to surgery. The authors reported a statistically significant reduction in positive conjunctival cultures both immediately before and after the surgery when ofloxacin was administered 3 days prior to surgery.[203]
The use of antibiotics in infusion solutions has been suggested. The efficacy of this mode of prophylaxis has not been supported by currently available data.[204, 205] Concerns regarding inadequate contact time with bacteria, the risk of retinal toxicity, effects on the buffering capabilities and chemical composition of infusion fluids, and the emergence of bacterial resistance have prompted many clinicians to reconsider this mode of prophylaxis. Similar concerns exist regarding the injection of antibiotics into the peri-IOL space for prophylaxis. Additional studies are required to address these issues. According to the Guilla et al review published in 2002,[200] none of these methods have been proven to impact the postoperative endophthalmitis risk. In the recently published ESCRS study of 13 698 cataract surgery patients,[206] the incidence rate of postoperative endophthalmitis in patients that did not receive intracameral cefuroxime 1 mg was almost five times as high as that in the group receiving this treatment. Perioperative levofloxacin eyedrops as prophylaxis was also associated with a reduction in the observed incidence rate of endophthalmitis, although this result was not statistically significant.
Collagen shields placed on the eye before or after surgery are a novel device used for the delivery of drugs into the anterior segment. Antibiotic-soaked collagen shields provide an alternative to eye drops or subconjunctival injections, in order to avoid the inconveniences and risks of these current modes of prophylaxis. Animal studies have demonstrated that antibiotic delivery to the anterior chamber is at least comparable with, if not superior to, that achieved by eye drops or subconjuctival injection.[207-210] The use of this device is not without risks, with a case of macular infarction syndrome reported with the use of a gentamicin-soaked collagen shield.[211] Corneal epithelial defects, poorly closed incisions, sutureless scleral tunnels, or clear corneal incision may permit unintentionally high doses of antibiotic to directly enter the eye, with potentially toxic effects. Further studies are required to fully define the role of this device.
Postoperative Antibiotic Prophylaxis
Postoperative antibiotics are commonly administered via a number of routes: subconjunctival, intracameral, and topical. A number of studies have examined the potential benefit of postoperative subconjunctival and intracameral antibiotics. Although various findings have in general demonstrated a possible benefit, results have not necessarily achieved statistical significance.
The role of subconjunctival antibiotics at the conclusion of surgery continues to be unclear. Although animal studies have shown that subconjunctival injection of ceftazidime, gentamicin, and ciprofloxacin is efficacious in preventing postcataract endophthalmitis,[211-213] the results of human studies have not been as compelling. Several clinical studies have found no decrease in the incidence of endophthalmitis with the addition of postoperative subconjunctival antibiotics, although these studies have been small or have been performed in Third World settings.[214-216] Human and animal data demonstrate that vitreous levels of antibiotic after this mode of delivery are very low.[158, 170, 194, 217] In a prospective case-controlled study of 214 cases of presumed endophthalmitis, subconjunctival antibiotics at the end of surgery and face mask wearing by the scrubing nurse were found to have a protective role against postoperative infection.[218] In a German survey of 340 633 cases,[216] a periocular injection of antibiotics at the end of the surgery was associated with a trend towards reducing the incidence of postoperative infection. Concerns have also arisen regarding the safety of subconjunctival antibiotics, particularly with aminoglycosides, which are the most frequent agents employed. Campochiaro and Conway reviewed 23 cases of macular infarction syndrome after postoperative subconjunctival aminoglycoside injection and found that most occurred after inadvertent penetration of the globe during injection (see Fig. 184.6).[122] Of added concern is the fact that some cases appeared to have occurred after uncomplicated injection. The use of other antibiotics, such as vancomycin and quinolones, has also been questioned, not only because of safety concerns in the event of inadvertent intraocular injection but mainly because of the risk of emergence of antibiotic resistance in ocular isolates.
Systemic administration of most antibiotic agents achieves concentrations in the aqueous and vitreous humor that are subtherapeutic. Some of the antibiotics used can achieve anterior chamber levels sufficient to suppress infective pathogen growth. Thus, degree of ocular penetration has become an important issue in agent selection. Agents displaying better ocular penetration are vancomycin,[152]cefazolin,[153] ceftazidime,[151] and quinolones.[154-162]
Fluoroquinolones are a class of synthetic antibacterial agents that were approved for ocular therapy in 1991 and have become popular therapy for the treatment and prevention of various ocular infections. These agents are synthetic, broad-spectrum, rapidly bactericidal, and have good penetration into ocular tissues. Their main mechanism of action is the inhibition of bacterial enzymes needed for bacterial DNA synthesis. Because fluoroquinolones, owning to their broad-spectrum activity and favorable pharmacokinetic and safety profiles, are the most popular topical agents used for prophylaxis, a number of studies have compared ocular penetration rates among different agents. Studies comparing topical norfloxacin, ciprofloxacin, ofloxacin, and levofloxacin have consistently demonstrated that all agents are capable of achieving aqueous humor (AH) concentrations above the MIC[90] of common susceptible organisms, although ofloxacin and levofloxacin exhibit significantly higher concentrations than norfloxacin or ciprofloxacin.[219-221] However, antibiotic resistance occurred swiftly to the earlier fluoroquinolones and better fluoroquinolones were needed. The fourth-generation fluoroquinolones, such as moxifloxacin and gatifloxacin, have enhanced activity against gram-positive bacteria while retaining potent activity against most gram-negative bacteria. These fourth-generation fluoroquinolones have improved penetration into the anterior chamber and have also demonstrated increased in vivo efficacy in several animal models of ocular infections. In addition, topical ophthalmic antibiotic products can deliver antibiotic concentrations directly to the eye that are thousands of times higher than their MICs.
In particular the fourth generation fluoroquinolones (moxifloxacin and gatifloxacin) were compared in many recent studies with the older generation antibiotics. McCulley et al[222] found that topical preoperative application of both fourth-generation fluoroquinolones achieved a greater AH concentration after four times daily dosing relative to prior-generation fluoroquinolones. Moxifloxacin 0.5% ophthalmic solution achieved a twofold higher AH concentration than gatifloxacin 0.3% ophthalmic solution. The superior penetration of moxifloxacin into the AH was attributed partially to its high degree of lipophilicity, greater solubility at neutral pH, and higher concentration in the commercial formulation. Moreover, the topical application of moxiflocaxin and gatifloxacin was found to penetrate the vitreous in the uninflamed eye, but the vitreous concentrations attained were all lower than the 90% minimum inhibitory concentration for the commonest bacterial pathogens causing acute postoperative endophthalmitis.[223]
Oral administration of both moxifloxacin and gatifloxacin was found to achieve therapeutic levels in the noninflamed human eye, and the activity spectra of both moxifloxacin and gatifloxacin appropriately encompass the bacterial species most frequently involved in the various causes of endophthalmitis.[224, 225]
Emerging Resistance
An issue worthy of consideration regarding antibiotic prophylaxis and agent selection is bacterial coverage and emerging resistance. Although fluoroquinolones have traditionally been chosen for topical prophylaxis against the pathogens of postoperative endophthalmitis because of their broad spectrum of activity, resistance has been emerging to this class of antibacterials, particularly among gram-positive organisms. Goldstein et al[226] reported significant increases in resistance to ciprofloxacin and ofloxacin from 1993 to 1997 among S. aureus, coagulase-negative Staphylococcus species, and Streptococcus species, approaching 50% of isolates examined, for some species. Another study reported a threefold increase in fluoroquinolone resistance among S. aureus isolates,[227] whereas resistance to fluoroquinolones among gram-negative organisms has also been documented.[189] Inappropriate sublethal dosing, which has induced mutagenesis in once susceptible pathogens was thought to trigger the resistance among older fluoroquinolones.[201] The fourth-generation fluoroquinolones offered a possible alternative to postoperative endophthalmitis prophylaxis in an era of emerging resistance. These agents confer a dual-binding mechanism of action in gram-positive organisms, inhibiting both DNA gyrase and topoisomerase IV, which is believed to expand their spectrum of activity to inhibit bacterial strains otherwise resistant to older fluoroquinolones.[228-230] Fung-Tomc et al studied the susceptibility to gatifloxacin of ofloxacin nonsusceptible Streptococcus pneumoniae and methicillin-resitant S. aureusstrains. The study results demonstrated that gatifloxacin did not select for the less susceptible variants of pneumococci and MRSA strains as compared with the 10-100-fold higher selection frequencies with ciprofloxacin and ofloxacin. The authors hypothesized that gatifloxacin may prevent the development of fluoroquinolone resistance in gram-positive bacteria.[231] Yet, in another publication by Marangon et al the levofloxacin resistance among methicillin-sensitive S. aureus corneal and conjunctival isolates was found to be increasing.[232]
In a study by Iihara et al,[233] the authors suggest that application of high-concentration fluoroquinolone ophthalmic solutions selects for isolates presenting such mutations, which may result in a high level of resistance to fluoroquinolones. Recchia et al[234] have recently reported on the longitudinal resistance patterns in endophthalmitis isolates from 1989 to 2000. Comparing the time periods 1989-94 and 1995-2000, the authors found a significant increase in resistant bacteria (20 compared with 37%) to ciprofloxacin (third-generation). Additionally, coagulase negative Staphylococcus had increased resistance to cefazolin (19 compared with 40%). The authors demonstrated that both empiric endophthalmitis treatment and general use of these antibiotic agents could lead to infecting bacteria with more resistance. Although a direct comparison cannot be made, fourth-generation fluoroquinolones may suffer a similar fate if not used judiciously.
SPECIAL CONSIDERATIONS
THE INTRAOCULAR LENS
Postoperative endophthalmitis is most frequently encountered in the pseudophakic eye. Prosthetic infections elsewhere in the body usually require removal of the prosthesis to facilitate sterilization; however, pseudophakic endophthalmitis appears to be an exception to this rule.[235] Intraocular infection can usually be eradicated while retaining an IOL. Inflammatory membranes are frequently present on the anterior and posterior surfaces of an IOL, and removal of the IOL is most commonly performed in order to facilitate visualization for vitrectomy. However, it is often possible to incise and débride such lenticular membranes with a 25-gauge needle. It is also often possible to aspirate a dense hypopyon from the surface of the IOL and iris by introducing a vitrectomy instrument into the anterior chamber. These techniques usually allow for preservation of an IOL. Given the preference of most surgeons for a 'core' vitrectomy in endophthalmitis, it appears that removal of an IOL to permit far-peripheral vitrectomy or to peel inflammatory membranes from the retina is, perhaps, unwarranted. However, these considerations are altered in endophthalmitis resulting from filamentous fungi, as these organisms tenaciously adhere to the IOL. Removal of the IOL is advocated to facilitate sterilization, although information is limited regarding these difficult cases.[4]
DELAYED-ONSET (CHRONIC) POSTOPERATIVE ENDOPHTHALMITIS
An unusual subgroup of postoperative endophthalmitis is that caused by indolent organisms, such as P. acnes.[53-60, 236] Typically, these patients present with a chronic, recurrent, steroid-responsive uveitis occurring months or even years after otherwise successful extracapsular cataract extraction with posterior chamber IOL implantation. Patients complain of decreased vision and pain, although some patients may have minimal discomfort. Signs include conjunctival hyperemia, keratic precipitates, a variable anterior chamber reaction (that may include hypopyon and beaded fibrin strands extending across the anterior chamber), vitritis, and sometimes loss of the red reflex. In addition, these eyes very typically display a white plaque within the equator of the remaining lens capsule (Fig. 184.7) or on the posterior surface of the IOL. The peripheral plaque may be mistaken for a Soemmering ring and is best visualized in a widely dilated pupil.
|
|
|
|
FIGURE 184.7 (a) White peripheral capsular plaque in a patient wih propionibacterium acnes endophthalmitis, (b) intraoperative photography of plaque removal. |
Patients are often initially diagnosed with idiopathic uveitis and are often treated with topical steroids, with subsequent clinical improvement. However, after several relapses, the possibility of infection is considered and the diagnosis is established by intraocular cultures. In chronic endophthalmitis, samples obtained from sites of maximal inflammatory involvement may increase the likelihood of isolating an organism. This may include aspirating fluid from the capsular bag[237] or excising involved portions of the lens capsule. Proper handling of material for anaerobic culture is critical, and cultures must be maintained for at least 14 days to maximize the recovery of these organisms.
The most common cause of chronic endophthalmitis is P. acnes.[59, 238] S. epidermidis, Propionibacterium granulosum, Achromobacter, Corynebacterium, and fungi have also been reported.[239]
The optimal therapeutic approach for P. acnes endophthalmitis is unclear. Early reports suggested intravitreal injection of vancomycin alone, although recurrences are common with this regimen. Current recommendations for initial therapy include vitrectomy with posterior capsulectomy and intravitreal injection of vancomycin. Cases that recur despite this are further treated with removal of the IOL, residual lens capsule, and equatorial material, as well as a repeat injection of intravitreal vancomycin (and possible reimplantation of an IOL). Excising infected portions of the lens capsule not only may provide material for culture but also may allow the removal of sequestered organisms from the eye.[58, 236] Several cases have been reported of successful treatment of chronic low-grade postcataract endophthalmitis by antibiotic irrigation of the capsular bag without vitrectomy, thus allowing IOL retention.[240]
Most patients infected with P. acnes enjoy relatively good outcomes after treatment, with the majority of eyes achieving 20/60 visual acuity or better.[58, 59] It is probable that a significant number of 'sterile' postoperative endophthalmitis cases in the past were improperly cultured infections caused by these indolent organisms and that increasing awareness of this clinical entity will further refine therapy.
ENDOPHTHALMITIS AFTER GLAUCOMA-FILTERING SURGERY
As a subgroup, bleb-associated endophthalmitis (Fig. 184.8) portends a dismal prognosis despite maximal medical and surgical intervention, with 33.3-72.7% of patients achieving a final visual acuity of less than 20/400.[78, 79, 241-243] Many eyes deteriorate to phthisis. Patients typically present with sudden-onset pain, redness, and decreased vision, and the clinical course is rapidly progressive. Bleb-associated endophthalmitis requires differentiation from blebitis, a term describing localized infection of the conjunctival bleb without vitreal involvement (Fig. 184.9).
|
|
|
|
FIGURE 184.8 (a) Streptococcal endophthalmitis in an eye with a long-standing filtering bleb. Photograph displays purulent discharge, opacification of the bleb, anterior chamber cell, hypopyon, and loss of red reflex. (b) Rapid clinical deterioration occurred over the subsequent 2 weeks despite immediate and repeated therapy, including intravitreal antibiotics and vitrectomies. The eye lost all light perception. |
|
|
|
|
FIGURE 184.9 (a) Blebitis (localized infection of a conjunctival bleb) due to S. epidermidis presenting in a patient with previous trabeculectomy. A milky-white appearance of the bleb and intense conjunctival injection are seen. The patient was treated with an intensive course of topical antibiotics and close observation. (b) Examination after 1 week of therapy shows resolution of the infection. |
Early bleb-associated endophthalmitis occurring in the early postoperative period has a spectrum of organisms similar to that of postcataract endophthalmitis. Late bleb-associated endophthalmitis occurs months or even years after surgery. Bacterial entry into the eye presumably occurs by migration through intact conjunctiva. In most cases, blebs are biomicroscopically intact and demonstrate a negative Seidel test. Streptococcus species and gram-negative organisms, particularly H. influenzae, are most commonly implicated.[78, 79, 243, 244] The poor response to therapy associated with this condition may be partially explained by the liberation of exotoxins and enzymes by these highly virulent bacteria.
The risk of bleb-associated endophthalmitis appears to be higher in eyes with thin-walled cystic blebs.[241, 245, 246] This is evidenced by the higher rate of endophthalmitis in eyes with full-thickness procedures[241, 247] and guarded filtration procedures with adjunctive antimetabolite therapy (5-fluorouracil and mitomycin C),[248-252] compared with trabeculectomy without antifibrotic agents. Moreover, the risk of infection is further increased in inferior trabeculectomy.[251, 252] This may be due to repeated mechanical abrasion with lower eyelid blinking and chronic exposure to bacteria residing in the tear pool and eyelid margin. Other risk factors include recent conjunctivitis or upper respiratory tract infection, a leaking bleb, and contact lens use.[245, 253] Patients should be educated as to the importance of prompt medical attention should any symptoms of infection develop.
The management of bleb-associated endophthalmitis includes obtaining conjunctival, aqueous, and vitreous cultures. Intraocular, subconjunctival, topical, and systemic antibiotic therapy covering streptococci and H. influenzae should be instituted promptly. Vancomycin, in combination with amikacin or ceftazidime, is a suitable choice for intravitreal injection. Initial systemic administration of intravenous vancomycin and ceftazidime, followed later by an oral quinolone such as ofloxacin, may be appropriate. The roles of initial pars plana vitrectomy and intravitreal corticosteroid therapy are uncertain, although they appear warranted in most cases. In a recent series, Kangas and associates found a trend toward improved outcome with vitrectomy and intraocular steroid injection, although a larger study is required to confirm these results statistically.[243] The possibility that the prognosis may be improved by surgically obliterating the sclerotomy also requires further study. Surgeons have been understandably reluctant to close a functioning filter, but the dismal prognosis in such cases suggests a departure from previous methods of therapy.
THE OPEN EYE
Bacterial endophthalmitis may occur late after cataract surgery owing to perforation of a corneal ulcer that has arisen either spontaneously or secondary to extended contact lens use as correction for aphakia. Data are limited regarding the treatment of endophthalmitis in the open eye, and unique challenges are posed for successful management.[254, 255] There is usually a need for débridement and possible patch grafting, gluing, or keratoplasty. In addition, the open eye frequently has extensive choroidal detachment, with attendant difficulties in the approach to the posterior segment. No data are available regarding the retinal toxicity of antibiotics when injected into an eye with greatly reduced vitreous volume. Nevertheless, an anterior approach with débridement of infected tissue, vitrectomy, and antibiotic and corticosteroid administration by intraocular, periocular, and systemic routes at standard dosages is currently advocated for these severe cases.
POST-OPERATIVE FUNGAL ENDOPHTHALMITIS
Fungi are infrequent causes of postoperative endophthalmitis, with Candida species predominating in reported cases. In a series of 62 culture-positive cases of pseudophakic endophthalmitis, fungi were isolated in five patients, of whom three achieved 20/400 or better visual acuity after therapy.[4] Cases associated with contaminated intraocular irrigating solutions[256] and infected donor corneas[257] have been reported. There have also been reports of epidemics after cataract surgery.[256, 258]
Most cases of fungal endophthalmitis present in a subacute or chronic manner. The use of cellufluor and calcofluor white techniques for the identification of fungal elements in fresh vitreous smears represents a significant advance in the rapid diagnosis of fungal endophthalmitis.[72] As this is a rare condition, the appropriate therapeutic approaches remain unclear. Intravitreal amphotericin B and vitrectomy are advocated. The role of systemic antifungal therapy remains unclear, and the high incidence of complications with systemic amphotericin B (particularly nephrotoxicity)[259] indicates the need for careful surveillance during its use. Some clinicians now advocate systemic imidazoles, such as ketoconazole and fluconazole, as alternatives.[260-265] Suggested removal of the IOL in the treatment of endophthalmitis owing to filamentous fungi has been previously discussed. Candida endophthalmitis does not routinely require IOL removal for successful sterilization, although recurrences may occur.[266]
POST-INTRAVITREAL INJECTION AND INTRAOCULAR DEVICE-RELATED ENDOPHTHALMITIS
The use of intravitreal injections of either triamcinolone acetonide or anti-vascular endothelial growth factors (anti-VEGF) have exponentially increased in frequency within the last years for therapy of macular and other diseases. Intravitreal injections of anti-VEGF agents have been proposed for treating choroidal neovascularization. Most of these injections are office-based procedures and therefore questions and concerns are raised regarding the safety and possible complications.
However, there are lingering questions about the rate of infectious endophthalmitis after intravitreal injections of triamcinolone and many cases are still presumed sterile inflammatory reactions to the vehicle, endotoxin, or other contaminants. Endophthalmitis associated with intravitreal triamcinolone acetonide use presents with less pain and delayed onset of symptoms (median 10 days) compared to endophthalmitis not associated with intravitreal triamcinolone use. Westfall et al[267] reported on an interventional, consecutive case series of 1006 eyes receiving intravitreal triamcinolone acetonide. The authors consistently performed these injections with the use of both povidone iodine and a lid speculum. One patient was treated for endophthalmitis with the notable absence of either pain or hypopyon. They concluded that a rate of 0.1% for postinjection endophthalmitis is favorable when considering the risk/benefit for the patient.
Moshfeghi et al[268] reported eight cases of culture-positive, acute postinjection endophthalmitis in a total of 922 injections of triamcinolone acetonide (overall risk of endophthalmitis 0.3%, similar to the risk of endophthalmitis reported for ganciclovir[269]). All patients presented at approximately the same time (median, 7.5 days) in the postinjection period with characteristic signs of infection: hypopyon, pain, red eye, vitritis and decreased vision. Injection from a multiuse triamcinolone acetonide bottle, diabetes mellitus, and filtering blebs seems to be important risk factors for postinjection endophthalmitis.[268] Jonas et al[270] reported an endophthalmitis rate of 1:1000 injections of intravitreal triamcinolone, if the solvent agent is removed. Gragoudas et al[271] reported an endophthalmitis rate of 1.3% for pegaptanib sodium intraocular injections.
The reported endophthalmitis rate of RETISERT in a multicentered study is 0.4%.[272] The cases do not typically occur soon after the surgery but with a median time to occurrence of 37 weeks. The majority of patients who experienced endophthalmitis had wound problems, i.e., exposed sutures, wound leak, or extruding implant.
The increased risk of endophthalmitis after steroid injection or RETISERT implant may be secondary to multiple issues that include (MW Johnson, Infectious complications of intravitreal steroids. Proceedings of 34th Aspen retinal detachment society meeting, 2006:28-29):
|
. |
Wound problems: vitreous wick upon needle withdrawal, steroid-associated inhibition of wound healing following RETISERT implantation or exposed sutures |
|
|
. |
Multidose vials susceptible to contamination |
|
|
. |
Susceptibility to endophthalmitis increased by corticosteroid induced ocular immunosuppression. |
It has been demonstrated that eyes with injection of both triamcinolone acetonide and bacteria were 12.2 times more likely to develop culture positive endophthalmitis than eyes with the same dose of bacteria alone (MW Johnson, Infectious complications of intravitreal steroids. Proceedings of 34th Aspen retinal detachment society meeting, 2006:28-29). The presence of triamcinolone acetonide may therefore turn a subthreshold inoculum into a threshold inoculum resulting in endophthalmitis. For this reason, it may be recommended to avoid injection of intravitreal triamcinolone at the end of or prior to intraocular surgery as bacteria are commonly introduced into the eye during surgery, and this may be even more common with sutureless techniques.
Based on the current literature,[268] prudent but not-concensus opinions with regard to intravitreal injections include: pre- and postinjection topical antibiotics, the use of sterile gloves and adhesive drape, and displacement of the conjunctiva to avoid externalized vitreous wick. All patients should be followed-up in the immediate postinjection period (1-7 days). In the first sign of a visual disturbance or pain, prompt intervention, including vitreous specimen for cultures and intraocular antibiotics are highly recommended.
RARE CAUSES OF ENDOPHTHALMITIS
Endophthalmitis after pars plana vitrectomy is a rare occurrence. Diabetic patients appear to have a greater predilection for postvitrectomy endophthalmitis.[266, 273] This may be due to the complicated surgical procedures that these patients often receive, as well as to host immunocompromise. Historically, visual acuity outcomes in patients with endophthalmitis after vitrectomy are poor. Cohen and colleagues found that over half of eyes infected with coagulase-negative staphylococci achieved final visual acuities of 20/50 or better, whereas eyes harboring all other organisms were left with final visual acuities of hand motions to no-light perception.[273] Several of these eyes required enucleation or evisceration. Eifrig et al[274] reported four of six patients with a final visual acuity of light perception or worse. Visual acuity outcomes have been reported to be better with less virulent organisms such as coagulase-negative Staphylococcus and Propionibacterium acnes.[273]
More recently the advent of transconjunctival 25-gauge vitrectomy has changed the general perception of vitrectomy approach. The large-scale studies on the long-term complication of this technique are lacking for the moment. In a recently published study of 140 cases, no cases of endophthalmitis were observed.[275] Further long-term, large-scale studies are needed to actually appreciate any possible differences in endophthalmitis rates between the classic and the 25-gauge technique.
Patients who have undergone pars plana vitrectomy for advanced posterior segment disease (diabetic retinopathy, retinal detachment with proliferative vitreoretinopathy) often have conjunctival injection, reduced vision and discomfort postoperatively, which may delay the diagnosis of endophthalmitis; adjunctive techniques such as panretinal endolaser photocoagulation, cryoretinopexy, or retinal tamponade with gas or silicone oil can make the clinical diagnosis of endophthalmitis even more challenging as these manipulations may induce a plasmoid or fibrin response in the anterior or posterior segment (Fig. 184.10), which usually responds well to topical corticosteroids. The presence of a hypopyon or fluctuating inflammation on topical corticosteroids should raise the index of suspicion for infection. Treatment of postvitrectomy endophthalmitis is similar to treatment of other types of postoperative endophthalmitis (anterior chamber and vitreous cultures, and injection of intraocular and subconjunctival antibiotics). The best treatment option for a gas-filled eye with postvitrectomy endophthalmitis is not known. Intravitreal antibiotics are generally recommended in such eyes but the dosage and specific drug may vary. The standard dosage of intravitreal antibiotics could be used even in a 50% gas-filled eye. To reduce the risk of retinal toxicity from intraocular antibiotics, reduced dosages of the medications could be injected into a 50% gas-filled eye. Another option used by the authors is to inject vancomycin alone (1 mg) into a gas-filled vitreous cavity and to administer an oral fourth-generation fluoroquinolone.[225] Finally, an option for patients with endophthalmitis in the setting of concurrent retinal detachment is to add antibiotics to the vitrectomy infusion fluid after intraocular cultures have been obtained and before the fluid-gas exchange is performed.[276]
|
|
|
|
FIGURE 184.10 Shield-like fibrin membrane overlying a silicone oil bubble 6 days after complicated vitreoretinal surgery for recurrent retinal detachment with proliferative vitreoretinopathy (PVR) in a lensectomized eye. During surgery, pars plana vitrectomy, epiretinal membrane peeling, extensive endolaser, and silicone oil exchange had been performed. The patient had a history of macular hole surgery complicated by retinal detachment and PVR, necessitating multiple vitreoretinal procedures. The membrane resolved with topical corticosteroids. |
In addition to intravitreal antibiotic therapy, systemic antibiotics may be beneficial in these patients because of the shorter half-life of intraocular antibiotics[136, 138-141] and greater penetration of systemic agents in inflamed vitrectomized eyes.[149, 151-153]
Endophthalmitis after pediatric intraocular surgery has a dismal prognosis, with up to 60% of eyes being left with a finalvisual acuity of no-light perception despite aggressive treatment.[277, 278] Lacrimal duct obstruction and upper respiratory tract infections are likely sources of infection in these patients.[277, 278] The incidence of pediatric postoperative endophthalmitis is estimated to be 0.071-0.45%,[277, 278]thereby prompting some clinicians to caution against the practice of simultaneous bilateral surgery for pediatric cataracts and glaucoma. Endophthalmitis after strabismus surgery[46] or intraocular foreign body has also been reported[5-10] (Fig 184.11).
|
|
|
|
FIGURE 184.11 Severe endophthalmitis secondary to an intraocular foreign body. |
Despite the fact that yttrium-aluminum garnet (YAG) laser posterior capsulotomy does not breach the ocular integrity, case reports of acute endophthalmitis after this procedure have been published.[279, 280]The organisms implicated in these cases were S. epidermidis and P. acnes, and these are known to cause a chronic indolent endophthalmitis in which clinical signs of inflammation may be minimal. The organisms were presumably sequestered in the capsular bag at surgery and were released into the vitreous cavity after laser capsulotomy, resulting in the development of acute signs of infection after the procedure. Clinicians should be aware of this entity, so that patients with unusual symptoms after YAG laser posterior capsulotomy may receive appropriate evaluation.
With the increase in keratorefractive surgery have come reports of bacterial endophthalmitis after some of these procedures.[281-284] S. epidermidis has been most commonly implicated. These cases serve to emphasize that infective surgical complications can occur regardless of how minimally invasive a procedure may appear.
Finally, outbreaks of endophthalmitis have occurred as a result of contaminated intraoperative irrigation solutions, IOLs, and donor corneas for penetrating keratoplasties.[256, 257, 285] These isolated events serve to highlight the importance of exacting sterilization procedures and appropriate methods of donor tissue storage. Taban et al[286] also performed a systematic review of the literature regarding the rate of endophthalmitis following penetrating keratoplasty. The authors' methodology was similar to their study[286] that suggested an increasing incidence in postcataract endophthalmitis. In endophthalmitis after penetrating keratoplasty, the authors reported declining endophthalmitis rates compared with prior decades. The endophthalmitis rate has dropped from 0.45% in the 1990s to 0.2% in the 2002-2003 period. Theories on the reduced rate included povidone iodine use of the donor cornea at the time of harvesting.
|
Key Features: Risk Factors for Postoperative Endophthalmitis |
||||||||||||||||||||||||||||||||||||||||||||||||
|
REFERENCES
1. Endophthalmitis Vitrectomy Study Group: Results of the endophthalmitis vitrectomy study: a randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Arch Ophthalmol 1995; 113:1479-1496.
2. Pavan PR, Oteiza EE, Hughes BA, Avni A: Exogenous endophthalmitis initially treated without systemic antibiotics. Ophthalmology 1994; 101:1289-1296.
3. Weber DJ, Hoffman KL, Thoft RA, Baker AS: Endophthalmitis following intraocular lens implantation: report of 30 cases and review of the literature. Rev Infect Dis 1986; 8:12-20.
4. Driebe Jr WT, Mandelbaum S, Forster RK, et al: Pseudophakic endophthalmitis: diagnosis and management. Ophthalmology 1986; 93:442-448.
5. Bohigian GM, Olk RJ: Factors associated with a poor visual result in endophthalmitis. Am J Ophthalmol 1986; 101:332-334.
6. Rowsey JJ, Newsom DL, Sexton DJ, Harms WK: Endophthalmitis: current approaches. Ophthalmology 1986; 89:1055-10661982.
7. Puliafito CA, Baker AS, Haaf J, Foster CS: Infectious endophthalmitis. Ophthalmology 1982; 89:921-929.
8. Diamond JG: Intraocular management of endophthalmitis. Arch Ophthalmol 1981; 99:96-99.
9. Forster RK, Abbott RL, Gelender H: Management of infectious endophthalmitis. Ophthalmology 1980; 87:313-319.
10. Nelsen PT, Marcus DA, Bovino JA: Retinal detachment following endophthalmitis. Ophthalmology 1985; 92:1112-1117.
11. Aaberg TM, Flynn Jr HW, Schiffman J, Newton J: Nosocomial acute-onset postoperative endophthalmitis survey. A 10-year review of incidence and outcomes. Ophthalmology 1998; 105:1004-1010.
12. Allen HF, Mangiaracine AB: Bacterial endophthalmitis after cataract extraction. II. Incidence in 36,000 consecutive operations with special reference to preoperative topical antibiotics. Arch Ophthalmol 1974; 91:3-7.
13. Kattan HM, Flynn HW Jr, Pflugfelder S, et al: Nosocomial endophthalmitis survey: current incidence of infection after intraocular surgery. Ophthalmology 1991; 98:227-238.
14. Eifrig CW, Flynn Jr HW, Scott IU, Newton J: Acute onset postoperative endophthalmitis: review of incidence and visual outcomes (1995-2001). Ophthalmic Surg Lasers 2002; 33:378-388.
15. Javitt JC, Vitale S, Canner JK, et al: National outcomes of cataract extraction: endophthalmitis following inpatient surgery. Arch Ophthalmol 1991; 109:1085-1089.
16. Schmitz S, Dick HB, Krummenauer F, Pfeiffer N: Endophthalmitis in cataract surgery: results of a German survey. Ophthalmology 1999; 106:1869-1877.
17. Jensen MK, Fiscella RG, Crandall AS, et al: Retrospective study of endophthalmitis rates comparing quinolone antibiotics. Am J Ophthalmol 2005; 139:141-148.
18. Busbee BG: Endophthalmitis: a reappraisal of incidence and treatment. Curr Opin Ophthalmol 2006; 17:286-291.
19. West ES, Behrens A, McDonnell PJ, et al: The incidence of endophthalmitis after cataract surgery among the US. Medicare population increased between 1994 and 2001. Ophthalmology 2005; 112:1388-1394.
20. Taban M, Behrens A, Newcomb RL, et al: Acute endophthalmitis following cataract surgery: a systematic review of the literature. Arch Ophthalmol 2005; 123:613-620.
21. Speaker MG, Milch FA, Shah MK, et al: Role of external bacterial flora in the pathogenesis of acute postoperative endophthalmitis. Ophthalmology 1991; 98:639-650.
22. Flynn Jr HW, Pflugfelder SC, Culbertson WW, Davis JL: Recognition, treatment, and prevention of endophthalmitis. Semin Ophthalmol 1989; 4:69-83.
23. Pflugfelder SC, Flynn HW Jr, Kattan H: Recent developments in prevention, diagnosis and treatment of endophthalmitis. Ophthalmol Clin North Am 1990; 3:475-485.
24. Pflugfelder SC, Flynn Jr HW: Infectious endophthalmitis. Infect Dis Clin North Am 1992; 6:859-873.
25. Morris R, Camesasca FI, Byrne J, John G: Postoperative endophthalmitis resulting from prosthesis contamination in a monocular patient. Am J Ophthalmol 1993; 116:346-349.
26. Fisch A, Salvanet A, Prazuck T, et al: Epidemiology of infective endophthalmitis in France. Lancet 1991; 338:1373-1376.
27. Phillips WB, Tasman WS: Postoperative endophthalmitis in association with diabetes mellitus. Ophthalmology 1994; 101:508-518.
28. Wilson FM: Causes and prevention of endophthalmitis. Int Ophthalmol Clin 1987; 27:67-73.
29. Ferro JF, De-Pablos M, Logrono MJ, et al: Postoperative contamination after using vancomycin and gentamicin during phacoemulsification. Arch Ophthalmol 1997; 115:165-170.
30. Manners TD, Chitkara DK, Marsh PJ, Stoddart MG: Anterior chamber aspirate cultures in small incision cataract surgery. Br J Ophthalmol 1995; 79:878-880.
31. Samad A, Solomon LD, Miller MA, Mendelson J: Anterior chamber contamination after uncomplicated phacoemulsification and intraocular lens implantation. Am J Ophthalmol 1995; 120:143-150.
32. Sherwood DR, Rich WJ, Jacob SJ, et al: Bacterial contamination of intraocular and extraocular fluids during cataract extraction. Eye 1989; 3:308-312.
33. Dickey JB, Thompson KD, Jay WM: Anterior chamber aspirate cultures after uncomplicated cataract surgery. Am J Ophthalmol 1991; 112:278-282.
34. Egger SF, Huber-Spitz V, Scholda C, et al: Bacterial contamination during extracapsular surgery. Prospective study on 200 consecutive patients. Ophthalmologica 1984; 208:77-81.
35. Egger SF, Huber-Spitz V, Skorpik C, et al: Different techniques of extracapsular cataract extraction: bacterial contamination during surgery. Prospective study on 230 consecutive patients. Graefes Arch Clin Exp Ophthalmol 1984; 232:308-3111994.
36. Chitkara DK, Manners T, Chapman F, et al: Lack of effect of preoperative norfloxacinon bacterial contamination of anterior chamber aspirates after cataract surgery. Br J Ophthalmol 1994; 78:772-774.
37. Wejde G, Salomon B, Seregard S, et al: Risk factors for endophthalmitis following cataract surgery: a retrospective case-control study. J Hosp Infect 2005; 61:251-256.
38. Maylath FR, Leopold IH: Study of experimental intraocular infection. I. The recoverability of organisms inoculated into the ocular tissues and fluids. II. The influence of antibiotics and cortisone, alone and combined, in intraocular growth of these organisms. Am J Ophthalmol 1955; 40:86-101.
39. Colleaux KM, Hamilton WK: Effect of prophylactic antibiotics and incision type on the incidence of endophthalmitis after cataract surgery. Can J Ophthalmol 2000; 35:373-378.
40. Cooper BA, Holekamp NM, Bohigian G, Thompson PA: Case-control study of endophthalmitis after cataract surgery comparing scleral tunnel and clear corneal wounds. Am J Ophthalmol 2003; 137:598-599.
41. Menikoff JA, Speaker MG, Marmor M, Raskin EM: A case-control study of risk factors for post-operative endophthalmitis. Ophthalmology 1991; 98:1761-1768.
42. Raskin EM, Speaker MG, McCormick SA, et al: Influence of haptic materials on the adherence of staphylococci to intraocular lenses. Arch Ophthalmol 1993; 111:250-253.
43. Parkkari M, Paivarinta H, Salminen L: The treatment of endophthalmitis after cataract surgery: review of 26 cases. J Ocul Pharmacol Ther 1995; 11:349-359.
44. Beyer TL, O'Donnell FE, Goncalves V, Singh R: Role of the posterior capsule in the prevention of postoperative bacterial endophthalmitis: experimental primate studies and clinical implications. Br J Ophthalmol 1985; 69:841-846.
45. Confino J, Brown SI: Bacterial endophthalmitis associated with exposed monofilament sutures following corneal transplantation. Am J Ophthalmol 1985; 99:111-113.
46. Salamon SM, Friberg TR, Luxenberg MN: Endophthalmitis after strabismus surgery. Am J Ophthalmol 1982; 93:39-41.
47. Gelender H: Bacterial endophthalmitis following cutting of sutures after cataract surgery. Am J Ophthalmol 1982; 93:323-326.
48. Miller KM, Glasgow BJ: Bacterial endophthalmitis following sutureless cataract surgery. Arch Ophthalmol 1993; 111:377-379.
49. Stonecipher KG, Parmley VC, Jensen H, Rowsey JJ: Infectious endophthalmitis following sutureless cataract surgery. Arch Ophthalmol 1991; 109:1562-1563.
50. Nagaki Y, Hayasaka S, Kadoi C, et al: Bacterial endophthalmitis after small-incision cataract surgery. Effect of incision placement and intraocular lens type. J Cataract Refract Surg 2003; 29:20-26.
51. Packer AJ, Weingeist TA, Abrams GW: Retinal periphlebitis as an early sign of bacterial endophthalmitis. Am J Ophthalmol 1983; 96:66-71.
52. Deutsch TA, Goldberg MF: Painless endophthalmitis after cataract surgery. Ophthalmic Surg 1984; 15:837-840.
53. Jaffe GJ, Whitcher JP, Biswell R, Irvine AR: Propionibacterium acnes endophthalmitis seven months after extracapsular cataract extraction and intraocular lens implantation. Ophthalmic Surg 1986; 17:791-793.
54. Meisler DM, Palestine AG, Vastine DW, et al: Chronic Propionibacterium endophthalmitis after extracapsular cataract extraction and intraocular lens implantation. Am J Ophthalmol 1986; 102:733-739.
55. Ormerod LD, Paton BG, Haaf J, et al: Anaerobic bacterial endophthalmitis. Ophthalmology 1987; 94:799-808.
56. Friberg TR, Kuzman PM: Propionibacterium acnes endophthalmitis two years after extracapsular cataract extraction. Am J Ophthalmol 1990; 109:609-610.
57. Walker J, Dangel ME, Makley TA, Opremcak EM: Postoperative Propionibacterium granulosum endophthalmitis. Arch Ophthalmol 1990; 108:1073-1074.
58. Zambrano W, Flynn HW Jr, Pflugfelder SC, et al: Management options for Propionibacterium acnes endophthalmitis. Ophthalmology 1989; 96:1100-1105.
59. Meisler DM, Mandelbaum S: Propionibacterium-associated endophthalmitis after extracapsular cataract extraction: review of reported cases. Ophthalmology 1989; 96:54-61.
60. Ficker L, Meredith TA, Wilson LA, et al: Chronic bacterial endophthalmitis. Am J Ophthalmol 1987; 103:745-748.
61. Johnson MW, Doft BH, Kelsey SF, et al: The Endophthalmitis Vitrectomy Study: relationship between clinical presentation and microbiological spectrum. Ophthalmology 1997; 104:261-272.
62. Apple DJ, Mamalis N, Steinmetz RL, et al: Phacoanaphylactic endophthalmitis associated with extracapsular cataract extraction and posterior chamber intraocular lens. Arch Ophthalmol 1984; 102:1528-1532.
63. McMahon MS, Weiss JS, Riedel KG, Albert DM: Clinically unsuspected phacoanaphylaxis after extracapsular cataract extraction with intraocular lens implantation. Br J Ophthalmol 1985; 69:836-840.
64. Soong HK, Kenyon KR: Adverse reactions to virgin silk sutures in cataract surgery. Ophthalmology 1984; 91:479-483.
65. Meltzer DW: Sterile hypopyon following intraocular lens surgery. Arch Ophthalmol 1980; 98:100-104.
66. Stark WJ, Rosenblum P, Maumenee AE, Cowan CL: Postoperative inflammatory reactions to intraocular lenses sterilized with ethylene-oxide. Ophthalmology 1980; 87:385-389.
67. Allen HR, Grove AS: Early acute aseptic iritis after cataract extraction. Trans Am Acad Ophthalmol Otolaryngol 1976; 81:145-150.
68. McDonnell PJ, Green WR, Maumenee AE, Iliff WJ: Pathology of intraocular lenses in 33 eyes examined postmortem. Ophthalmology 1983; 90:386-403.
69. Chan IM, Jalkh AE, Trempe CL, Tolentino FI: Ultrasonographic findings in endophthalmitis. Ann Ophthalmol 1984; 16:778-784.
70. Forster RK: Etiology and diagnosis of bacterial postoperative endophthalmitis. Ophthalmology 1978; 85:320-326.
71. Durfee K, Smith JP: Use of Gram stain to predict vitreous fluid infection. Am J Med Technol 1982; 48:525-529.
72. Sutphin JE, Robinson NM, Wilhelmus KR, Osato MS: Improved detection of oculomycoses using induced fluorescence with cellufluor. Ophthalmology 1986; 93:416-417.
73. Kinnear FB, Kirkness CM: Advances in rapid laboratory diagnosis of infectious endophthalmitis. J Hosp Infect 1995; 30:253-261.
74. Joondeph B, Flynn Jr HW, Miller DM, Joondeph HC: A new culture method for infectious endophthalmitis. Arch Ophthalmol 1989; 107:1334-1337.
75. Hykin PG, Tobal K, Mcintyre G, et al: The diagnosis of delayed postoperative endophthalmitis by polymerase chain reaction recovery of bacterial 16s rDNA. J Med Microbiol 1994; 40:408-415.
76. Rickman LS, Freeman WR, Green WR, et al: Brief report: uveitis caused by Tropheryma whippelii (Whipple's bacillus). N Engl J Med 1995; 332:363-366.
77. Olson JC, Flynn Jr HW, Forster RK, Culbertson WW: Results in the treatment of postoperative endophthalmitis. Ophthalmology 1983; 90:692-699.
78. Mandelbaum S, Forster RK, Gelender H, Culbertson WW: Late-onset endophthalmitis associated with filtering blebs. Ophthalmology 1985; 92:964-972.
79. Phillips WB, Wong TP, Bergren RL, et al: Late onset endophthalmitis associated with filtering blebs. Ophthalmic Surg 1994; 25:88-91.
80. Greenfield DS, Suner IJ, Miller MP, et al: Endophthalmitis after filtering surgery with mitomycin. Arch Ophthalmol 1996; 114:943-949.
81. Levin MR, D'Amico DJ: Diagnosis and management of traumatic endophthalmitis. In: Shingleton B, Hersh P, Kenyon K, ed. Ocular trauma, St. Louis: Mosby-Year Book; 1991:242-252.
82. Affeldt JC, Flynn HW Jr, Forster RK, et al: Microbial endophthalmitis resulting from ocular trauma. Ophthalmology 1987; 94:407-413.
83. Brinton GS, Topping TM, Hyndiuk RA, et al: Posttraumatic endophthalmitis. Arch Ophthalmol 1984; 102:547-550.
84. Schemmer GB, Driebe Jr WT: Posttraumatic Bacillus cereus endophthalmitis. Arch Ophthalmol 1987; 105:342-344.
85. Bouza E, Grant S, Jordan C, et al: Bacillus cereus endogenous panophthalmitis. Arch Ophthalmol 1979; 97:498-499.
86. Grossniklaus H, Bruner WE, Frank KE, Purnell EW: Bacillus cereus endophthalmitis appearing as acute glaucoma in a drug addict. Am J Ophthalmol 1985; 100:334-335.
87. von Sallmann L, Meyer K, DiGrandi J: Experimental study on penicillin treatment of ectogenous infection of vitreous. Arch Ophthalmol 1944; 32:179-189.
88. Duguid JP, Ginsberg M, Fraser IC, et al: Experimental observation on the intravitreal use of penicillin and other drugs. Br J Ophthalmol 1947; 31:193-211.
89. Sorsby A, Ungar J: Intravitreal injection of penicillin. Study of the levels of concentration reached and therapeutic efficacy. Br J Ophthalmol 1948; 32:857-864.
90. Peyman GA, Herbst R: Bacterial endophthalmitis: treatment with intraocular injection of gentamicin and dexamethasone. Arch Ophthalmol 1974; 91:416-418.
91. Peyman GA, May DR, Ericson ES, Apple D: Intraocular injection of gentamicin: toxic effects and clearance. Arch Ophthalmol 1974; 92:42-47.
92. Peyman GA, Paque JT, Meisels HI, Bennett TO: Postoperative endophthalmitis: a comparison of methods for treatment and prophylaxis with gentamicin. Ophthalmic Surg 1975; 6:45-55.
93. Forster RK: Endophthalmitis: diagnostic cultures and visual results. Arch Ophthalmol 1974; 92:387-392.
94. Forster RK, Zachary IG, Cottingham AH, Norton EWD: Further observation on the diagnosis, cause, and treatment of endophthalmitis. Am J Ophthalmol 1976; 81:52-56.
95. Cobo LM, Forster RK: The clearance of intravitreal gentamicin. Am J Ophthalmol 1981; 92:59-62.
96. D'Amico DJ, Libert J, Kenyon KR, et al: Retinal toxicity of intravitreal gentamicin: an electron microscopic study. Invest Ophthalmol Vis Sci 1984; 25:564-572.
97. D'Amico DJ, Caspers-Velu L, Libert J, et al: Comparative toxicity of intravitreal aminoglycoside antibiotics. Am J Ophthalmol 1985; 100:264-275.
98. Fett DR, Silverman CA, Yoshizumi MO: Moxalactam retinal toxicity. Arch Ophthalmol 1984; 102:435-438.
99. Fisher JP, Civiletto SE, Forster RK: Toxicity, efficacy, and clearance of intravitreally injected cefazolin. Arch Ophthalmol 1982; 100:650-652.
100. Graham RO, Peyman GA: Intravitreal injection of dexamethasone: treatment of experimentally induced endophthalmitis. Arch Ophthalmol 1974; 92:149-154.
101. Homer P, Peyman GA, Koziol J, Sanders D: Intravitreal injection of vancomycin in experimental staphylococcal endophthalmitis. Acta Ophthalmol 1975; 53:311-320.
102. Ling CH, Peyman GA, Raichand M: Electron microscopic study of toxicity of intravitreal injections of gentamicin in primates. Can J Ophthalmol 1985; 20:179-183.
103. Smith MA, Sorenson JA, Lowy FD, et al: Treatment of experimental methicillin-resistant Staphylococcus epidermidis endophthalmitis with intravitreal vancomycin. Ophthalmology 1986; 93:1328-1335.
104. Talamo JH, D'Amico DJ, Kenyon KR: Intravitreal amikacin in the treatment of bacterial endophthalmitis. Arch Ophthalmol 1986; 104:1483-1485.
105. Zachary IG, Forster RK: Experimental intravitreal gentamicin. Am J Ophthalmol 1976; 82:604-611.
106. Baum J, Peyman GA, Barza M: Intravitreal administration of antibiotic in the treatment of bacterial endophthalmitis. III. Consensus. Surv Ophthalmol 1982; 26:204-206.
107. Stern GA, Engel HM, Driebe Jr WT: The treatment of postoperative endophthalmitis. Results of differing approaches to treatment. Ophthalmology 1989; 96:62-67.
108. Choi S, Hahn TW, Osterhout G, O'Brien TP: Comparative intravitreal antibiotic therapy for experimental Enterococcus faecalis endophthalmitis. Arch Ophthalmol 1996; 114:61-65.
109. Jett BD, Jensen HG, Atkuri RV, Gilmore MS: Evaluation of therapeutic measures for treating endophthalmitis caused by isogenic toxin-producing and toxin-nonproducing Enterococcus faecalis strains. Invest Ophthalmol Vis Sci 1995; 36:9-15.
110. Pflugfelder SC, Hernandez E, Fliesler SJ, et al: Intravitreal vancomycin: retinal toxicity, clearance and interaction with gentamicin. Arch Ophthalmol 1987; 105:831-837.
111. Lambert SR, Stern WH: Methicillin- and gentamicin-resistant Staphylococcus epidermidis endophthalmitis after intraocular surgery. Am J Ophthalmol 1985; 99:725-726.
112. Davis JL, Koidou-Tsiligianni A, Pflugfelder SC, et al: Coagulase-negative staphylococcal endophthalmitis: increase in antimicrobial resistance. Ophthalmology 1988; 95:1404-1410.
113. Flynn Jr HW, Pulido JS, Pflugfelder SC, et al: Endophthalmitis therapy: changing antibiotic sensitivity patterns and current therapeutic recommendations. Arch Ophthalmol 1991; 109:175-176.
114. Kervick GN, Flynn Jr HW, Alfonso E, Miller D: Antibiotic therapy for Bacillus species infections. Am J Ophthalmol 1990; 110:683-687.
115. Schwalbe RS, Stapleton JT, Gilligan PH: Emergence of vancomycin resistance in coagulase-negative staphylococci. N Engl J Med 1987; 316:927-931.
116. Bennett TO, Peyman GA: Toxicity of intravitreal aminoglycosides in primates. Can J Ophthalmol 1974; 9:475-478.
117. McDonald HR, Schatz H, Allen AW, et al: Retinal toxicity secondary to intraocular gentamicin injection. Ophthalmology 1986; 93:871-877.
118. Conway BP, Campochiaro PA: Macular infarction after endophthalmitis treated with vitrectomy and intravitreal gentamicin. Arch Ophthalmol 1986; 104:367-371.
119. Brown GC, Eagle RC, Shakin EP, et al: Retinal toxicity of intravitreal gentamicin. Arch Ophthalmol 1990; 108:1740-1744.
120. Insler MS, Cavanaugh HD, Wilson WA: Gentamicin-resistant Pseudomonas endophthalmitis after penetrating keratoplasty. Br J Ophthalmol 1985; 69:189-191.
121. Majerovics A, Tanenbaum HL: Endophthalmitis and pars plana vitrectomy. Can J Ophthalmol 1984; 19:25-28.
122. Campochiaro PA, Conway BP: Aminoglycoside toxicity: a survey of retinal specialists; implications for ocular use. Arch Ophthalmol 1991; 109:964-1050.
123. Campochiaro PA, Lim JI, Bloome MA, et al: Aminoglycoside toxicity in the treatment of endophthalmitis. Arch Ophthalmol 1994; 112:48-53.
124. Narvaez J, Wessels IF, Mattheis JK, Beierle F: Intravitreal antibiotics: accuracy of dilution by pharmacists, ophthalmologists, and ophthalmic assistants using three protocols. Ophthalmic Surg 1992; 23:265-268.
125. Irvine WD, Flynn HW Jr, Miller D, et al: Endophthalmitis caused by gram-negative organisms. Arch Ophthalmol 1992; 110:1450-1454.
126. Rowsey JJ, Stonecipher KG, Jensen H, et al: Culture and sensitivities of infectious endophthalmitis: a microbiological analysis of 302 intravitreal biopsies. Invest Ophthalmol Vis Sci 1992; 33(Suppl):745.
127. Donowitz GR: Third generation cephalosporins. Infect Dis Clin North Am 1989; 3:595-612.
128. Campochiaro PA, Green WR: Toxicity of intravitreous ceftazidime in primate retina. Arch Ophthalmol 1992; 110:1625-1629.
129. Lim JI, Campochiaro PA: Successful treatment of gram-negative endophthalmitis with intravitreous ceftazidime. Arch Ophthalmol 1992; 110:1686.
130. Aaberg Jr TM, Flynn HW Jr, Murray TG: Intraocular ceftazidime as an alternative to the aminoglycosides in the treatment of endophthalmitis. Arch Ophthalmol 1994; 112:18-19.
131. Stonecipher KG, Parmley VC, Jensen H, Rowsey JJ: Infectious endophthalmitis following sutureless cataract surgery. Arch Ophthalmol 1991; 109:1562-1563.
132. Doft BH, Barza M: Ceftazidime or amikacin: choice of intravitreal antimicrobials in the treatment of postoperative endophthalmitis. Arch Ophthalmol 1994; 112:17-18.
133. Ben-Nun J, Joyce DA, Cooper RL, et al: Pharmacokinetics of intravitreal injection: assessment of a gentamicin model by ocular dialysis. Invest Ophthalmol Vis Sci 1989; 30:1055-1061.
134. Maurice DM, Mishima S: Ocular pharmacokinetics. In: Sears ML, ed. Pharmacology of the eye, New York: Springer-Verlag; 1984:19-116.
135. Barza M: Antibacterial agents in the treatment of ocular infections. Infect Dis Clin North Am 1989; 3:533-551.
136. Meredith TA: Antimicrobial pharmacokinetics in endophthalmitis treatment: studies of ceftazidime. Trans Am Ophthalmol Soc 1993; 91:653-699.
137. Maurice DM: Injection of drugs into the vitreous body. In: Leopold IJ, Burns RP, ed. Symposium on ocular therapy, New York: Wiley; 1976:59-72.
138. Ficker LA, Meredith TA, Gardner SK, Wilson LA: Cefazolin levels after intravitreal injection: effects of inflammation and surgery. Invest Ophthalmol Vis Sci 1990; 31:502-505.
139. Mandell TA, Meredith TA, Aguilar EA, et al: Effects of inflammation and surgery on amikacin levels in the vitreous cavity. Am J Ophthalmol 1993; 115:770-774.
140. Shaarawy A, Meredith TA, Kincaid M, et al: Intraocular injection of ceftazidime. Effects of inflammation and surgery. Retina 1995; 15:433-438.
141. Aguilar HE, Meredith TA, el-Massry A, et al: Vancomycin levels after intravitreal injection. Effects of inflammation and surgery. Retina 1995; 15:428-432.
142. Flynn Jr HW, Meredith TA: The Endophthalmitis Vitrectomy Study [letter]. Arch Ophthalmol 1996; 114:1027-1028.
143. Shaarawy A, Grand MG, Meredith TA, Ibanez H: Persistent infection after intravitreal antimicrobial therapy. Ophthalmology 1995; 102:382-387.
144. Stern GA, Engel HM, Driebe Jr WT: Recurrent postoperative endophthalmitis. Cornea 1990; 9:102-107.
145. Mao LK, Flynn Jr HW, Miller D, Pflugfelder SC: Endophthalmitis caused by streptococcal species. Arch Ophthalmol 1992; 110:798-801.
146. Oum BS, D'Amico DJ, Wong KW: Intravitreal antibiotic therapy with vancomycin and aminoglycoside. An experimental study of combination and repetitive injections. Arch Ophthalmol 1989; 107:1055-1060.
147. Oum BS, D'Amico DJ, Kwak HW, Wong KW: Intravitreal antibiotic therapy with vancomycin and aminoglycoside: examination of the retinal toxicity of repetitive injections after vitreous and lens surgery. Graefes Arch Clin Exp Ophthalmol 1992; 230:56-61.
148. Stern GA: Factors affecting the efficacy of antibiotics in the treatment of experimental postoperative endophthalmitis. Trans Am Ophthalmol Soc 1993; 91:775-844.
149. Barza M: Factors affecting the intraocular penetration of antibiotics: the influence of route, inflammation, animal species and tissue pigmentation. Scand J Infect Dis 1978; 11(Suppl):151-159.
150. El-Massry A, Meredith TA, Aguilar HE, et al: Aminoglycoside levels in the rabbit vitreous cavity after intravenous administration. Am J Ophthalmol 1996; 122:684-689.
151. Aguilar HE, Meredith TA, Shaarawy A, et al: Vitreous cavity penetration of ceftazidime after intravenous administration. Retina 1995; 15:154-159.
152. Meredith TA, Aguilar HE, Shaarawy A, et al: Vancomycin levels in the vitreous cavity after intravenous administration. Am J Ophthalmol 1995; 119:774-778.
153. Martin DF, Ficker LA, Aguilar HA, et al: Vitreous cefazolin levels after intravenous injection: effects of inflammation, repeated antibiotic doses, and surgery. Arch Ophthalmol 1990; 108:411-414.
154. Lesk MR, Ammann H, Marcil G, et al: The penetration of oral ciprofloxacin into the aqueous humor, vitreous, and subretinal fluid of humans. Am J Ophthalmol 1993; 115:623-628.
155. Keren U, Alhalel A, Bartov E, et al: The intravitreal penetration of orally administered ciprofloxacin in humans. Invest Ophthalmol Vis Sci 1991; 32:2388-2392.
156. El Baba FZ, Trousdale MD, Gauderman WJ, et al: Intravitreal penetration of oral ciprofloxacin in humans. Ophthalmology 1992; 99:483-486.
157. Skoutelis AT, Gartaganis SP, Chrysanthopoulos CJ, et al: Aqueous humor penetration of ciprofloxacin in the human eye. Arch Ophthalmol 1988; 106:404-405.
158. Behrens-Baumann W, Martell J: Ciprofloxacin concentration in the rabbit aqueous humor and vitreous following intravenous and subconjunctival administration. Infection 1988; 16:54-57.
159. Kowalski RP, Karenchak LM, Eller AW: The role of ciprofloxacin in endophthalmitis therapy. Am J Ophthalmol 1993; 116:695-699.
160. Gatti G, Panozzo G: Effect of inflammation on intraocular penetration of intravenous ofloxacin in albino rabbits. Antimicrob Agents Chemother 1995; 39:549-552.
161. Von Gunten S, Lew D, Paccolat F, et al: Aqueous humor penetration of ofloxacin given by various routes. Am J Ophthalmol 1994; 117:87-89.
162. Donnenfeld ED, Perry HD, Snyder RW, et al: Intracorneal, aqueous humor, and vitreous humor penetration of topical and oral ofloxacin. Arch Ophthalmol 1997; 115:173-176.
163. Verbraeken H, Verstraete A, Van de Velde E, Verschraegen G: Penetration of gentamicin and ofloxacin in human vitreous after systemic administration. Graefes Arch Clin Exp Ophthalmol 1996; 234:S59-S65.
164. Barza M, Kane A, Baum J: Comparison of the effects of continuous and intermittent systemic administration on the penetration of gentamicin into infected rabbit eyes. J Infect Dis 1983; 147:144-148.
165. Rubenstein E, Goldfarb J, Keren G, et al: The penetration of gentamicin into the vitreous humor in man. Invest Ophthalmol Vis Sci 1983; 24:637-639.
166. Wisniewski SR, Hammer ME, Grizzard WS, et al: An investigation of the hospital charges related to the treatment of endophthalmitis in the Endophthalmitis Vitrectomy Study. Ophthalmology 1997; 104:739-745.
167. Baker AS, Durand M: The Endophthalmitis Vitrectomy Study [letter]. Arch Ophthalmol 1996; 114:1025-1026.
168. Haimann MH, Weiss H, Miller J: The Endophthalmitis Vitrectomy Study [letter]. Arch Ophthalmol 1996; 114:1025.
169. Ng JQ, Morlet N, Pearman JW, et al: Management and outcomes of postoperative endophthalmitis since the Endophthalmitis Vitrectomy Study: the Endophthalmitis Population Study of Western Australia's (EPSWA) fifth report. Ophthalmology 2005; 112:1199-1206.
170. Barza M, Doft B, Lynch E: Ocular penetration of ceftriaxone, ceftazidime, and vancomycin after subconjunctival injection in humans. Arch Ophthalmol 1993; 111:492-494.
171. Barza M, Kane A, Baum J: Intraocular penetration of gentamicin after subconjunctival and retrobulbar injection. Ophthalmology 1978; 85:541-547.
172. Graham RO, Peyman GA: Intravitreal injection of dexamethasone: treatment of experimentally-induced endophthalmitis. Arch Ophthalmol 1974; 92:149-154.
173. Smith MA, Sorenson JA, D'Aversa G, et al: Treatment of experimental methicillin-resistant Staphylococcus epidermidis endophthalmitis with intravitreal vancomycin and intravitreal dexamethasone. J Infect Dis 1997; 175:462-466.
174. Maxwell DP, Brent BD, Diamond JG, et al: Effect of intravitreal dexamethasone on ocular histopathology in a rabbit model of endophthalmitis. Ophthalmology 1991; 98:1370-1375.
175. Meredith TA, Aguilar HE, Miller MJ, et al: Comparative treatment of experimental Staphylococcus epidermidis endophthalmitis. Arch Ophthalmol 1990; 108:857-860.
176. Park SS, Samiy N, Ruoff K, et al: Effect of intravitreal dexamethasone in treatment of pneumococcal endophthalmitis in rabbits. Arch Ophthalmol 1995; 113:1324-1329.
177. Aguilar HE, Meredith TA, Drews C, et al: Comparative treatment of experimental Staphylococcus aureus endophthalmitis. Am J Ophthalmol 1996; 121:310-317.
178. Schulman JA, Peyman GA: Intravitreal corticosteroids as an adjunct in the treatment of bacterial and fungal endophthalmitis. A review. Retina 1992; 12:336-340.
179. Kwak HW, D'Amico DJ: Evaluation of the retinal toxicity and pharmacokinetics of dexamethasone after intravitreal injection. Arch Ophthalmol 1992; 110:259-266.
180. Cottingham AJ, Forster RK: Vitrectomy in endophthalmitis: results of a study using vitrectomy, intraocular antibiotics, or a combination of both. Arch Ophthalmol 1976; 94:2078-2081.
181. Talley AR, D'Amico DJ, Talamo JH, et al: The role of vitrectomy in the treatment of post-operative bacterial endophthalmitis. Arch Ophthalmol 1987; 105:1699-1702.
182. Bode DD, Gelender H, Forster RK: A retrospective review of endophthalmitis due to coagulase-negative staphylococci. Br J Ophthalmol 1985; 69:915-919.
183. Nelsen PT, Marcus DA, Bovino JA: Retinal detachment following endophthalmitis. Ophthalmology 1986; 92:1112-1117.
184. Ficker LA, Meredith TA, Wilson LA, Kaplan HJ: Role of vitrectomy in Staphylococcus epidermidis endophthalmitis. Br J Ophthalmol 1988; 72:386-389.
185. Kaynak S, Oner FH, Kocak N, Cingil G: Surgical management of postoperative endophthalmitis: comparison of 2 techniques. J Cataract Refract Surg 2003; 29:966-969.
186. The Endophthalmitis Vitrectomy Study Group: Microbiologic factors and visual outcome in the Endophthalmitis Vitrectomy Study. Am J Ophthalmol 1996; 122:830-846.
187. Isenberg SJ, Apt L, Yoshimori R, Khwarg S: Chemical preparation of the eye in ophthalmic surgery. IV. Comparison of povidone-iodine on the conjunctiva with a prophylactic antibiotic. Arch Ophthalmol 1985; 103:1340-1342.
188. Apt L, Isenberg SJ, Yoshimori R, Spierer A: Outpatient topical use of povidone-iodine in preparing the eye for surgery. Ophthalmology 1989; 96:289-292.
189. Chaudry NA, Flynn HW, Murray TG: Emerging ciprofloxacin-resistant Pseudomonas aeruginosa. Am J Ophthalmol 1999; 128:509-510.
190. Speaker MG, Menikoff JA: Prophylaxis of endophthalmitis with topical povidone-iodine. Ophthalmology 1991; 98:1769-1775.
191. Isenberg SJ, Apt L, Yoshimori R, et al: Efficacy of topical povidone-iodine during the first week after ophthalmic surgery. Am J Ophthalmol 1997; 124:31-35.
192. Classen DC, Evans RS, Pestotnik SL, et al: The timing of prophylactic administration of antibiotics and the risk of surgical wound infection. N Engl J Med 1992; 326:281-286.
193. Burns RP, Hansen T, Faunfelder FT, et al: An experimental model for evaluation of human conjunctivitis and topical antibiotic therapy: Comparison of gentamicin and neomycin. Can J Ophthalmol 1968; 3:132-137.
194. Burns RP, Oden M: Antibiotic prophylaxis in cataract surgery. Trans Am Ophthalmol Soc 1972; 70:43-57.
195. Fahmy JA: Bacterial flora in relation to cataract extraction. V. Effects of topical antibiotics on the preoperative conjunctival flora. Acta Ophthalmol (Copenh) 1980; 58:567-575.
196. Kobayakawa S, Tochikubo T, Tsuji A: Penetration of levofloxacin into human aqueous humor. Ophthalmic Res 2003; 35:97-101.
197. Ormerod LD, Ho DD, Becker LE, et al: Endophthalmitis caused by the coagulase-negative staphylococci. 1. Disease spectrum and outcome. Ophthalmology 1993; 100:715-723.
198. Osher RH, Amdahl LD, Cheetham JK: Antimicrobial efficacy and aqueous humor concentration of preoperative and postoperative topical trimethoprim/polymyxin B sulfate versus tobramycin. J Cataract Refract Surg 1994; 20:3-8.
199. Kirsch LS, Jackson WB, Goldstein DA, Discepola MJ: Perioperative ofloxacin versus tobramycin: efficacy in external ocular adnexal sterilization and anterior chamber penetration. Can J Ophthalmol 1995; 30:11-20.
200. Guilla TA, Starr MB, Masket S: Bacterial endophthalmitis prophylaxis for cataract surgery: an evidence-based update. Ophthalmology 2002; 109:13-26.
201. Liesegang TJ: Use of antimicrobials to prevent postoperative infection in patients with cataracts. Curr Opin Ophthalmol 2001; 12:68-74.
202. Masket S: Preventing, diagnosing and treating endophthalmitis. J Cataract Refract Surg 1998; 24:725-726.
203. Ta CN, Egberg PR, Singh K, et al: Prospective randomized comparison of 3-day versus 1-hour preoperative ofloxacin prophylaxis for cataract surgery. Ophthalmology 2002; 109:2036-2041.
204. Gritz DC, Cevallos AV, Smolin G, Whitcher JP: Antibiotic supplementation of intraocular irrigating solutions: an in vitro model of antibacterial action. Ophthalmology 1996; 103:1204-1209.
205. Henry JC, Rozas D, Bryant E, Memphis W: Bacterial growth from anterior chamber fluid aspirates using different irrigating solutions in phacoemulsification. Invest Ophthalmol Vis Sci 1993; 34(Suppl):884.
206. ESCRS Endophthalmitis Study Group: ESCRS study of prophylaxis of postoperative endophthalmitis after cataract surgery. Preliminary report of principal results from a European multicenter study. J Cataract Refract Surg 2006; 32:407-410.
207. Alaranta S, Oksala O, Mahlberg K, et al: Drug delivery into the rabbit eye: collagen shields soaked with gentamicin compared with subconjunctival injections. Invest Ophthalmol Vis Sci 1993; 34(Suppl):1488.
208. Milani JK, Verbukh I, Pleyer V, et al: Collagen shields impregnated with gentamicin-dexamethasone as a potential drug delivery device. Am J Ophthalmol 1993; 166:622-627.
209. Phinney RB, Schwartz SD, Lee DA, Mondino BJ: Collagen shield delivery of gentamicin and vancomycin. Arch Ophthalmol 1988; 106:1599-1604.
210. Renard G, Bennami N, Lutaj P, et al: Comparative study of a collagen corneal shield and subconjunctival injection at the end of cataract surgery. J Cataract Refract Surg 1993; 19:48-51.
211. Shockley RK, Fishman P, Aziz M, et al: Subconjunctival administration of ceftazidime in pigmented rabbit eyes. Arch Ophthalmol 1986; 104:266-268.
212. Elliot RD, Katz HR: Inhibition of pseudophakic endophthalmitis in a rabbit model. Ophthalmic Surg 1987; 18:538-541.
213. Parks DJ, Cyryin AS, Sarfarazi FA, Katz HR: Subconjunctival ciprofloxacin inhibits pseudophakic endophthalmitis in a rabbit model. Invest Ophthalmol Vis Sci 1991; 34(Suppl):706.
214. Kolker AE, Freeman MI, Pettit TH: Prophylactic antibiotics and postoperative endophthalmitis. Am J Ophthalmol 1967; 63:434-439.
215. Christy NE, Lall P: Postoperative endophthalmitis following cataract surgery. Arch Ophthalmol 1973; 90:361-366.
216. Chalkley THF, Shoch D: An evaluation of prophylactic subconjunctival antibiotic injection in cataract surgery. Am J Ophthalmol 1967; 64:1084-1087.
217. Rubenstein E, Triester G, Auni I, Schwartzkopf R: The intravitreal penetration of cefotaxime in man following systemic and subconjunctival administration. Ophthalmology 1987; 94:30-34.
218. Kamalarajah S, Ling R, Silvestri G, et al: Presumed infectious endophthalmitis following cataract surgery in the UK: a case-control study of risk factors. Eye 2006.7.Epub ahead of print.
219. Kobayakawa S, Tochikubo T, Tsuji A: Penetration of levofloxacin into human aqueous humor. Ophthalmic Res 2003; 65:97-101.
220. Yalvac IS, Basci NE, Bozkurt A, Duman S: Penetration of topically applied ciprofloxacin and ofloxacin into the aqueous humor and vitreous. J Cataract Refract Surg 2003; 29:487-491.
221. Yamada M, Mochizuki H, Yamada R: Aqueous humor levels of topically applied levofloxacin in human eyes. Curr Eye Res 2002; 24:403-406.
222. McCulley JP, Caudle D, Aronowicz JD, Shine WE: Fourth-generation fluoroquinolone penetration into the aqueous humor in humans. Ophthalmology 2006; 113:955-959.
223. Costello P, Bakri SJ, Beer PM, et al: Vitreous penetration of topical moxifloxacin and gatifloxacin in humans. Retina 2006; 26:191-195.
224. Hariprasad SM, Shah GK, Mieler WF, et al: Vitreous and aqueous penetration of orally administered moxifloxacin in humans. Arch Ophthalmol 2006; 124:178-182.
225. Hariprasad SM, Mieler WF, Holz ER: Vitreous and aqueous penetration of orally administered gatifloxacin in humans. Arch Ophthalmol 2004; 122:1408-1409.
226. Goldstein MH, Kowalski RP, Gordon J: Emerging flouroquinolone resistance in bacterial keratitis: a 5-year review. Ophthalmology 1999; 106:1313-1318.
227. Alexandrakis G, Alfonso EC, Miller D: Shifting trends in bacterial keratitis in South Florida and emerging resistance to fluoroquinolones. Ophthalmology 2000; 107:1497-1502.
228. Olson RJ: Reducing the risk of postoperative endophthalmitis. Surv Ophthalmol 2004; 49:S55-S61.
229. Fukuda H, Kishii R, Takei M, Hosaka M: Contributions of the 8-methoxy group pf gatifloxacin to resistance selectivity, target preference, and antibacterial activity against Streptococcus pneumoniae. Antimicrob Agents Chemother 2001; 45:1649-1653.
230. Mather R, Karenchak LM, Romanowski EG, Kowalski RP: Fourth generation fluoroquinolones: new weapons in the arsenal of ophthalmic antibiotics. Am J Ophthalmol 2002; 133:463-466.
231. Fung-Tomc J, Gradelski E, Huczko E: Activity of gatifloxacin against strains resistant to ofloxacin and ciprofloxacin and its ability to select for less susceptible bacterial variants. Int J Antimicrob Agents 2001; 18:77-80.
232. Marangon FB, Miller D, Muallem MS, et al: Ciprofloxacin and levofloxacin resistance among methicillin-sensitive Staphylococcus aureus isolates from keratitis and conjunctivitis. Am J Ophthalmol 2004; 137:453-458.
233. Iihara H, Suzuki T, Kawamura Y, et al: Emerging multiple mutations and high-level fluoroquinolone resistance in methicillin-resistant Staphylococcus aureus isolated from ocular infections. Diagn Microbiol Infect Dis 2006.10.Epub ahead of print.
234. Recchia FM, Busbee BG, Pearlman RB, et al: Changing trends in the microbiologic apsects of postcataract endophthalmitis. Arch Ophthalmol 2005; 123:341-346.
235. Hopen G, Mondino BJ, Kozy D, Lipkowitz J: Intraocular lenses and experimental bacterial endophthalmitis. Am J Ophthalmol 1982; 94:402-407.
236. Fox GM, Joohdeph BC, Flynn Jr HW, et al: Delayed-onset pseudophakic endophthalmitis. Am J Ophthalmol 1991; 111:163-173.
237. Owens SL, Lam S, Tessler HH, Deutsch TA: Preliminary study of a new intraocular method in the diagnosis and treatment of Propionibacterium acnes endophthalmitis following cataract extraction. Ophthalmic Surg 1993; 24:268-272.
238. Mandelbaum S, Meisler DM: Postoperative chronic microbial endophthalmitis. Int Ophthalmol Clin 1993; 33:71-79.
239. Theodore FH: Etiology and diagnosis of fungal postoperative endophthalmitis. Ophthalmology 1978; 85:327-340.
240. Busin M: Antibiotic irrigation of the capsular bag to resolve low-grade endophthalmitis. J Cataract Refract Surg 1996; 22:385-389.
241. Hattenhauer JM, Lipsich MP: Late endophthalmitis after filtering surgery. Am J Ophthalmol 1971; 72:1097-1101.
242. Katz LJ, Cantor LB, Spaeth GL: Early and late bacterial endophthalmitis following glaucoma filtering surgery. Ophthalmology 1985; 92:959-963.
243. Kangas TA, Greenfield DS, Flynn Jr HW, et al: Delayed-onset endophthalmitis associated with conjunctival filtering blebs. Ophthalmology 1997; 104:746-752.
244. Ciulla TA, Baker AS: Endophthalmitis following glaucoma filtering surgery. Int Ophthalmol Clin 1996; 36:87-96.
245. Ashkenazi I, Melamed S, Avni I, et al: Risk factors associated with late infection of filtering blebs and endophthalmitis. Ophthalmic Surg 1991; 22:570-574.
246. Sugar HS, Zekman T: Late infection of filtering conjunctival scars. Am J Ophthalmol 1958; 46:155-170.
247. Lamping KA, Bellows AR, Hutchinson BT, Afran SI: Long-term evaluation of initial filtration surgery. Ophthalmology 1986; 93:91-101.
248. Ticho U, Ophir A: Late complications after glaucoma filtering surgery with adjunctive 5-fluorouracil. Am J Ophthalmol 1993; 115:506-510.
249. The Fluorouracil Filtering Surgery Study Group: Three-year follow-up of the Fluorouracil Filtering Surgery Study Group. Am J Ophthalmol 1993; 115:82-92.
250. Rockwood EJ, Parrish RK II, Heuer DK, et al: Glaucoma filtering surgery with 5-fluorouracil. Ophthalmology 1987; 94:1071-1078.
251. Wolner B, Liebmann JM, Sassani JW, et al: Late bleb-associated endophthalmitis after trabeculectomy with adjunctive 5-fluorouracil. Ophthalmology 1991; 98:1053-1060.
252. Greenfield DS, Suner IJ, Miller MP, et al: Endophthalmitis after filtering surgery with mitomycin. Arch Ophthalmol 1996; 114:943-949.
253. Bellows AR, McCulley JP: Endophthalmitis in aphakic patients with unplanned filtering blebs wearing contact lenses. Ophthalmology 1981; 88:839-943.
254. Kozarsky AM, Stulting RD, Waring GO, et al: Penetrating keratoplasty for exogenous Paecilomyces keratitis followed by postoperative endophthalmitis. Am J Ophthalmol 1984; 98:552-557.
255. Weiss I: Pseudomonas orbital cellulitis. Am J Ophthalmol 1979; 87:368-370.
256. Stern WH, Tamura E, Jacobs RA, et al: Epidemic postsurgical Candida parapsilosis endophthalmitis: clinical findings and management of 15 consecutive cases. Ophthalmology 1985; 92:1701-1709.
257. Cameron JA, Antonios SR, Cotter JB, Habash NR: Endophthalmitis from contaminated donor corneas following penetrating keratoplasty. Arch Ophthalmol 1991; 109:54-59.
258. Pettit TH, Olson RJ, Foos RY, et al: Fungal endophthalmitis following intraocular lens implantation. Arch Ophthalmol 1980; 98:1025-1039.
259. Medoff G, Kobayashi GS: Strategies in the treatment of systemic fungal infections. N Engl J Med 1980; 302:145-155.
260. Pflugfelder SC, Flynn HW Jr, Zwickey TA, et al: Exogenous fungal endophthalmitis. Ophthalmology 1988; 95:19-30.
261. Park SS, D'Amico DJ, Paton B, Baker AS: Treatment of exogenous Candida endophthalmitis in rabbits with oral fluconazole. Antimicrob Agents Chemother 1995; 39:958-963.
262. Savani DV, Perfect JR, Cobo LM, et al: Penetration of new azole compounds into the eye and efficacy in experimental Candida endophthalmitis. Antimicrob Agents Chemother 1987; 31:6-10.
263. Urbank SF, Degn T: Fluconazole in the treatment of Candida albicans endophthalmitis. Acta Ophthalmol 1992; 70:528-529.
264. Luttrull JK, Wan WL, Kubak BM, et al: Treatment of ocular fungal infections with oral fluconazole. Am J Ophthalmol 1995; 119:477-481.
265. Akler ME, Vellend H, McNeely DM, et al: Use of fluconazole in the treatment of candidal endophthalmitis. Clin Infect Dis 1995; 20:657-664.
266. Ho PC, Tolentino FI: Bacterial endophthalmitis after closed vitrectomy. Arch Ophthalmol 1984; 102:207-210.
267. Westfall AC, Osborn A, Kuhl D, et al: Acute endophthalmitis incidence: intravitreal triamcinolone. Arch Ophthalmol 2005; 123:1075-1077.
268. Moshfeghi DM, Kaiser PK, Scott IU, et al: Acute endophthalmitis following intravitreal triamcinolone acetonide injection. Am J Ophthalmol 2003; 136:791-796.
269. Engstrom Jr RE, Holland GN: Local therapy for cytomegalovirus retinopathy. Am J Ophthalmol 1995; 120:376-385.
270. Jonas JB, Kreissig I, Spandau UH, Harder B: Infectious and non-infectious endophthalmitis after intravitreal high-dosage triamcinolone acetonide. Am J Ophthalmol 2006; 141:579-580.
271. Gragoudas ES, Adamis AP, Cunningham ET, et al: Pegaptanib for neovascular age-related macular degeneration. N Engl J Med 2004; 351:2805-2816.
272. Jaffe GD, Martin D, Callanan D, et al: Fluocinolone acetonide implant (Retisert) for noninfectious posterior uveitis: thirty-four-week results of a multicenter randomized clinical study. Ophthalmology 2006; 113:1020-1027.
273. Cohen SM, Flynn HW Jr, Murray TG, et al: Endophthalmitis after pars plana vitrectomy. Ophthalmology 1995; 102:705-712.
274. Eifrig CWG, Scott IU, Flynn HW, et al: Endophthalmitis after pars-plana vitrectomy: incidence, causative organisms, and visual acuity outcomes. Am J Ophthalmalol 2004; 138:799-802.
275. Lakhanpal RR, Humayun MS, deJuan Jr E, et al: Outcomes of 140 consecutive cases of 25-gauge transconjunctival surgery for posterior segment disease. Ophthalmology 2005; 112:817-824.
276. Morgan BS, Larson B, Peyman GA, West CS: Toxicity of antibiotic combinations for vitrectomy infusion fluid. Ophthalmic Surg 1979; 10:74-77.
277. Good WV, Hing S, Irvine AR, et al: Postoperative endophthalmitis in children following cataract surgery. J Pediatr Ophthalmol Strabismus 1990; 27:283-285.
278. Wheeler DT, Stager DR, Weakley Jr DR: Endophthalmitis following pediatric intraocular surgery for congenital cataracts and congenital glaucoma. J Pediatr Ophthalmol Strabismus 1992; 29:139-141.
279. Carlson AN, Koch DD: Endophthalmitis following Nd:YAG laser posterior capsulotomy. Ophthalmic Surg 1988; 19:168-170.
280. Neutenboom GHG, De Vries-Knoppert WAEJ: Endophthalmitis after Nd:YAG laser capsulotomy. Doc Ophthalmol 1988; 70:175-178.
281. Gelender H, Flynn HW Jr, Mandelbaum SH: Bacterial endophthalmitis resulting from radial keratotomy. Am J Ophthalmol 1982; 93:323-326.
282. Barak MH, Shapiro MB: Bacterial endophthalmitis following postkeratoplasty relaxing incisions. Refract Corneal Surg 1990; 6:271-272.
283. Rosecan LR: Endophthalmitis and cystoid macular edema after astigmatic keratotomy. Ophthalmic Surg 1994; 25:481-482.
284. McLeod SD, Flowers CW, Lopez PF, et al: Endophthalmitis and orbital cellulitis after radial keratotomy. Ophthalmology 1995; 102:1902-1907.
285. Gerding DN, Poley BJ, Hall WH, et al: Treatment of Pseudomonas endophthalmitis associated with prosthetic intraocular lens implantation. Am J Ophthalmol 1991; 109:54-59.
286. Taban M, Behrens A, Newcomb RL, et al: Incidence of acute endophthalmitis following penetrating keratoplasty: a systematic review. Arch Ophthalmol 2005; 123:605-609.