Claudia U. Richter
INTRODUCTION
Laser trabeculoplasty became an important tool in the management of open-angle glaucoma when Wise and Witter[1] found that intraocular pressure (IOP) could be reduced reliably and predictably by evenly spaced burns around the circumference of the trabecular meshwork. This technique did not attempt to penetrate through the trabecular meshwork into Schlemm's canal and the spacing between burns did not result in worsening or induced glaucoma as seen with confluently placed laser burns. Since the introduction of laser trabeculoplasty, the procedure has been refined by variations in the extent of the trabecular meshwork treated, power, and medications to minimize postlaser IOP elevations. Finally, there are several choices in laser wavelengths that have been demonstrated to be effective: argon, diode, and Q-switched, frequency-doubled 532-nm Nd:YAG (selective, SLT) laser.
|
Key Features |
||||||||||||
|
PATHOPHYSIOLOGY
The IOP reduction after laser trabeculoplasty is caused by an increase in aqueous outflow facility. The mechanism for this increased outflow resistance has variously been explained mechanically by a shrinkage of the inner trabecular ring and by a biologic response of the trabecular cells.
Wise initially proposed that laser trabeculoplasty caused shrinkage of the inner trabecular ring, resulting in separation of the trabecular sheets and opening of the aqueous channels in the trabecular meshwork.[2] According to this hypothesis, multiple burns would displace the entire inner portion of the meshwork toward the anterior chamber. Schlemm's canal would be prevented from collapsing. However, in studies of 23 pairs of enucleated eyes examined equidistant between argon laser trabeculoplasty burns, no effect could be demonstrated on the cross-sectional area of Schlemm's canal or the development of its collapse.[3]
Van Buskirk et al[3] suggested that the increased facility of outflow and reduced IOP after laser trabeculoplasty is due to a biologic response by the trabecular endothelial cells. Trabecular meshwork preserved in organ culture and treated with laser trabeculoplasty had an alteration in the turnover or synthesis of glycosaminoglycans. In addition, increased trabecular cell division and migration from distant areas of the meshwork were demonstrated using organ culture trabecular meshwork exposed to tritiated thymidine after 180° argon laser trabeculoplasty. Nonburned areas of the trabecular meshwork showed a marked incorporation of thymidine into trabecular cell DNA 2 days after laser trabeculoplasty.[4] The cell division indicated by this thymidine incorporation occurred predominantly in the anterior, nonfiltering region of the trabecular meshwork where it inserts into the cornea beneath Schwalbe's line. Two weeks after trabeculoplasty, the labeled cells became concentrated in the burn sites. Based on these observations, the authors suggested that the laser burns are repopulated by dividing trabecular cells and that these cells have migrated into the burn sites from a distant site, primarily the region of Schwalbe's line. The exact mechanism by which these changes result in improved outflow facility is still unclear.
The mechanism for reduced IOP by SLT is also unclear. The laser may stimulate an intrinsic system to remodel the trabecular meshwork without causing the thermal damage of the argon and diode lasers or the postlaser inflammatory response may stimulate antiinflammatory cells to clean up the entire trabecular meshwork and increase outflow. Latina found notable reductions in IOP in the contralateral eyes of SLT-treated patients which suggests a biologic effect on the trabecular meshwork.[5]
HISTOLOGY
The morphologic changes in the trabecular meshwork immediately after laser trabeculoplasty have been studied in nonglaucomatous Cynomolgus monkeys and in human specimens obtained at trabeculectomy. In monkey eyes, Melamed and colleagues[6] found coagulative necrosis of treated trabecular meshwork 1 h after treatment, with disruption of trabecular beams and fragmented cells and fibrocellular tissue debris in the juxtacanalicular meshwork (Figs 218.1 and 218.2). Many endothelial cells were rounded up and some were actively phagocytic. Four weeks after treatment, the treated spots were detected as regions of flattened and collapsed beams covered by a cellular sheet extending from the corneal endothelium (Fig. 218.3).[7] The inner wall of Schlemm's canal beneath these regions was flat, with no vacuoles. Adjacent nonlasered spots had wide open intertrabecular spaces with herniations of juxtacanalicular trabecular meshwork and of inner wall endothelium into and across the lumen of Schlemm's canal. The herniations contained chronic inflammatory cells and large vacuoles.
|
|
|
|
FIGURE 218.1 Scanning electron micrograph of argon laser trabeculoplasty lesion immediately after treatment in a Cynomolgus monkey demonstrates coagulative damage with adjacent tears of the corneal endothelium. |
|
|
|
|
FIGURE 218.2 Transmission electron micrograph of argon laser trabeculoplasty lesion immediately after treatment in a Cynomolgus monkey demonstrates coagulative damage to the trabecular meshwork. |
|
|
|
|
FIGURE 218.3 Scanning electron micrograph of argon laser trabeculoplasty lesion 4 weeks after treatment in a Cynomolgus monkey demonstrates flattening of the trabecular meshwork with extension of the corneal endothelium over the scarred lasered region. |
Specimens of human trabecular meshwork after laser trabeculoplasty obtained at trabeculectomy demonstrate changes similar to those seen in monkey eyes.[8] Early changes consisted of disruption of the trabecular beams and accumulation of cellular and fibrinous debris. The corneal endothelial cells adjacent to the laser burn showed extension of cytoplasmic processes, cytoplasmic edema, and nuclear irregularity. One week after treatment, shrinkage of treated uveal and corneoscleral trabecular meshwork occurred in a 50- to 60-?m area, with nontreated areas appearing normal. After 6 months to 1 year, tissues demonstrated confluent areas of fibrosis and abnormally migrating corneal endothelial cells lining the uveal meshwork and occluding the trabecular spaces.
SLT selectively lyses intraocular melanosomes, leaving nonpigmented cells intact and not scarring the trabecular meshwork. The short pulse duration of the SLT (3 ns) limits the conversion of energy to heat, which also minimizes collateral tissue damage. Histologic studies of human cadaver eyes after SLT reveal no evidence of coagulative damage or distruption of the corneoscleral or uveal trabecular beam structure.[9]
INDICATIONS
Laser trabeculoplasty is an appropriate treatment to lower IOP in eyes with open-angle glaucoma that is uncontrolled by medical therapy; as the initial treatment of open-angle glaucoma; and for IOP control in patients noncompliant with medications (Table 218.1). Laser trabeculoplasty is often a useful treatment for IOP control in open-angle glaucoma before filtration surgery.
TABLE 218.1 -- Indications for Laser Trabeculoplasty
|
Uncontrolled open-angle glaucoma |
|
Noncompliance with medical therapy |
|
Initial therapy for open-angle glaucoma |
Open-angle glaucoma uncontrolled by medical therapy is the most common indication for laser trabeculoplasty. The number of medications that a patient has tried depends on the patient's compliance with a medication schedule, tolerance of medications, and side effects. The number of glaucoma medications available for treatment currently means that most patients would not be compliant with or tolerant of all classes of medications for treatment. Therefore, laser trabeculoplasty is often recommended when medical treatment with one or two medications has been ineffective.
Noncompliance with antiglaucoma medications can be an indication for laser trabeculoplasty. These patients may suffer optic nerve damage and visual-field loss because of uncontrolled IOP and trabeculoplasty may provide adequate IOP control to prevent this visual loss.
The success of laser trabeculoplasty in controlling IOP in open-angle glaucoma has inspired several studies of laser trabeculoplasty as a primary therapy in glaucoma treatment. The Glaucoma Laser Trial[10]is a multicenter, randomized clinical trial assessing the efficacy and safety of argon laser trabeculoplasty as an alternative to treatment with topical medications for uncontrolled IOP in patients with newly diagnosed, previously untreated primary open-angle glaucoma. After 2 years of follow-up, eyes treated with argon laser trabeculoplasty first and medications added as necessary had lower mean IOPs than did eyes treated with medications first. Additionally, eyes treated initially with laser trabeculoplasty required fewer medications for IOP control than did eyes treated initially with medications. The Glaucoma Laser Trial Follow-up Study[11] demonstrated in a randomized trial with up to 9 years of follow-up that eyes treated with laser trabeculoplasty prior to medical therapy had intraocular pressures an average of 1.2 mmHg lower than eyes that received medications first. In addition, the eyes that had laser trabeculoplasty first also had slightly better visual fields at the end of follow-up. This study provides good support for using laser trabeculoplasty as initial therapy in open-angle glaucoma.
The contraindications to laser trabeculoplasty are few (Table 218.2). The two absolute contraindications are total angle closure and hazy media precluding visualization of the angle structures. Laser trabeculoplasty may be difficult or impossible in an uncooperative patient, but this situation is uncommon and retrobulbar anesthesia may allow safe treatment. Secondary open-angle glaucomas that are infrequently improved by laser trabeculoplasty, such as the inflammatory glaucomas, are a contraindication. A serious complication from laser trabeculoplasty in one eye, such as a marked IOP elevation, may constitute a contraindication to treatment in the fellow eye. Finally, laser trabeculoplasty should be used cautiously in eyes that need urgent IOP control to preserve vision. Since the results of trabeculoplasty are not immediate and not always predictable, these eyes may be better treated with glaucoma surgery than laser trabeculoplasty.
TABLE 218.2 -- Contraindications to Laser Trabeculoplasty
|
Angle closure glaucoma, primary or secondary |
|
Hazy media precluding visualization of the trabecular meshwork |
|
Urgent necessity for IOP control |
|
LTP complication in other eye (especially high IOP) |
TECHNIQUE
Laser trabeculoplasty is an outpatient procedure that is usually well tolerated by the patient. Preoperative preparations include obtaining informed consent, prophylactic treatment for postlaser IOP elevations, topical anesthesia, and patient positioning to maximize the patient's comfort. Prelaser instillation of an alpha-adrenergic agonist helps decrease postlaser IOP spikes, but other antiglaucomatous topical medications may be used if necessary. Topical anesthesia with 0.5% proparacaine hydrochloride is usually adequate. In rare circumstances, poor patient cooperation or nystagmus may require either peribulbar or retrobulbar anesthesia. The laser energy is delivered to the trabecular meshwork through a mirrored contact lens that has been filled with methylcellulose and placed on the cornea. The dome-shaped mirror angled at 59° on the Goldmann three-mirror lens, the Ritch trabeculoplasty lens, or the Latina SLT lens may be used.
The initial laser settings for the different types of lasers are listed in Table 218.3. The desired reaction to the laser treatment with the argon and diode laser is a blanching of the trabecular meshwork with or without minimal bubble formation (Fig. 218.4). The power setting is adjusted between 700 and 1200 mW to achieve this response. Large bubble formation and pigment scattering indicate that the power is too high and should be lowered. Occasionally the trabecular meshwork is pale, and even 1200-mW power with the argon laser causes no discernible tissue reaction. In this situation, the trabeculoplasty session should be completed with the 1200-mW power. In selective laser trabeculoplasty, the endpoint is small champagne bubbles and power is reduced if large bubbles form or there is tissue blanching. During a treatment session, the power may need to be adjusted because the trabecular meshwork pigmentation can vary over its circumference.
TABLE 218.3 -- Technique of Laser Trabeculoplasty
|
Argon Laser |
Diode Laser |
SLT |
|
|
Laser power |
700-1200 mW |
700-1400 mW |
0.8 mJ |
|
Duration |
0.1 s |
0.2 s |
|
|
Spot size |
50 mm |
100 mm |
|
|
Placement |
Anterior TM |
Anterior TM |
Pigmented TM |
|
Number of burns |
50 over 180° of TM |
50 over 180° of TM |
50 over 180° of TM |
|
|
|
|
FIGURE 218.4 The desired tissue reaction is blanching of the trabecular meshwork, with or without minimal bubble formation, demonstrated on the left. The right laser burn demonstrates excessive pigment scattering; the power should be reduced. |
The argon or diode laser burns are placed at the anterior half of the trabecular meshwork, straddling the junction of the pigmented and nonpigmented trabecular meshwork (Fig. 218.5). Placement of burns in the anterior region of the trabecular meshwork minimizes both the postlaser IOP rise and the postlaser formation of peripheral anterior synechiae. With the SLT, the aiming beam is focused on the pigmented trabecular meshwork. Approximately 50 laser burns are typically placed over 180° of the trabecular meshwork per session with the argon, diode or SLT lasers. With the argon and diode lasers the burns are equally spaced approximately three burn widths apart (150 ?m); with the SLT laser the burns are placed confluently without overlapping. While 180° of the angle is usually treated, the optimal extent of angle treatment has not been identified.
|
|
|
|
FIGURE 218.5 The laser burns are placed at the anterior half of the trabecular meshwork, straddling the junction of the pigmented and nonpigmented meshwork. The appropriate spacing between laser burns and the effect of trabecular meshwork pigmentation on tissue reaction are also demonstrated. |
Adequate visualization of the angle structures and precise focusing of the laser during the procedure are important. If the angle is narrow and visualization is difficult, pilocarpine may adequately open the angle, or a laser iridectomy can be performed to deepen the angle and facilitate the trabeculoplasty. A properly focused beam appears perfectly round.
After laser trabeculoplasty, an alpha-adrenergic agonist or other antiglaucomatous medication is administered. The IOP is monitored for 1-3 h. Any IOP elevations are treated as necessary to protect the optic nerve and visual field. The patient's preoperative glaucoma medications are continued and topical steroids may be prescribed four times daily for 3-5 days. The IOP is measured at 1 h, 1 week and again at 4-6 weeks, or sooner if the severity of the glaucoma requires it.
COMPLICATIONS OF LASER TRABECULOPLASTY
Complications of laser trabeculoplasty are fortunately relatively uncommon and usually transient (Table 218.4). The most serious postlaser complication is elevated IOP, which may cause optic nerve damage or visual field loss, or both. Other complications include decreased vision, pain, hemorrhage, peripheral anterior synechiae, iritis, and a possible adverse effect on filtration surgery.
TABLE 218.4 -- Complications of Laser Trabeculoplasty
|
Elevated IOP |
|
Decreased visual acuity |
|
Discomfort |
|
Hemorrhage |
|
Peripheral anterior synechiae |
|
Iritis |
Some level of IOP elevation commonly occurs after laser trabeculoplasty with any type of laser. In the Glaucoma Laser Trial, 34% of eyes had an IOP increase of more than 5 mmHg and 12% had an increase of more than 10 mmHg.[12] Most of these increases were detectable 1 h after treatment, but a small percentage of eyes had IOP increases greater than 5 mmHg at 4 h despite no such elevation at 1 h.
The magnitude and frequency of elevated IOP seems to be related to the amount of treatment administered, the amount of pigmentation in the trabecular meshwork, the laser power, and placement of the laser burns. Weinreb and colleagues[13] demonstrated that the incidence as well as the magnitude of the postoperative rise in pressure were significantly greater in eyes that had received 100 laser burns over 360° compared with 50 laser burns over 180°. The Glaucoma Laser Trial found that moderate or heavy pigmentation of the trabecular meshwork was the strongest risk factor for pressure increases after argon laser trabeculoplasty. Elevations of more than 10 mmHg were observed in 19% of eyes with moderate or heavy pigmentation in comparison with 5% in eyes with no pigmentation and 8% in eyes with mild pigmentation. Postlaser IOP spikes also occur with selective laser trabeculoplasty and may be more marked with heavily pigmented trabecular meshwork.
Histopathologic examination of eyes with persistent, medically unresponsive elevation of IOP after argon laser trabeculoplasty has revealed an inflammatory response that is essentially confined to the trabecular meshwork.[14] The IOP increase may have resulted from inflammatory cells and debris obstructing the trabecular meshwork and reducing aqueous outflow facility.
Many attempts have been made to prevent the immediate rise in postoperative IOP. Alpha-adrenergic agonists (brimonidine or apraclonidine) administered either 1 h before and immediately after or only immediately after laser reduce IOP increases. If an a-adrenergic agonist is contraindicated, other antiglaucomatous medications may be used. In a prospective, randomized, investigator-masked study the frequency of pressure elevation with 1% apraclonidine was 3%, with acetazolamide 39%, with dipivefrin 38%, with 4% pilocarpine 33%, and with 0.5% timolol 32%.[15] Treatment with topical steroids or topical nonsteroidal antiinflammatory agents does not affect the postlaser IOP elevation.
Decreased visual acuity is usually a transient problem after laser trabeculoplasty and is usually caused by the goniosolution and laser flash. Occasionally, hemorrhage into the anterior chamber and iritis can be significant enough to cause decreased vision until they resolve. Visual acuity or visual field, or both, may be permanently lost by significantly elevated IOP after laser trabeculoplasty.
Discomfort is usually minimal during and after laser trabeculoplasty. Topical anesthesia with 0.5% proparacaine is nearly always adequate anesthesia during the procedure. Marked iritis may cause postlaser ocular discomfort.
Hemorrhage into the anterior chamber uncommonly occurs during laser trabeculoplasty (Fig. 218.6). Bleeding may result from reflux of blood from Schlemm's canal or inadvertent photocoagulation of an iris root vessel or a circumferential ciliary vessel. Any bleeding is usually easily controlled by increasing pressure on the contact lens. Low-power photocoagulation (200 mW, 200 ?m, 0.2 s) can be used to control bleeding from an identifiable site.
|
|
|
|
FIGURE 218.6 Hyphema after argon laser trabeculoplasty. |
Peripheral anterior synechiae can be identified in as many as 46% of eyes treated with laser trabeculoplasty.[12] The peripheral anterior synechiae are characteristically small and peaked and may reach to the ciliary body band, scleral spur, or the trabecular meshwork (Fig. 218.7). Formation of peripheral anterior synechiae has been associated with posterior laser burns, higher-power burns, and brown eyes.
|
|
|
|
FIGURE 218.7 Small, peaked peripheral anterior synechiae can complicate laser trabeculoplasty. |
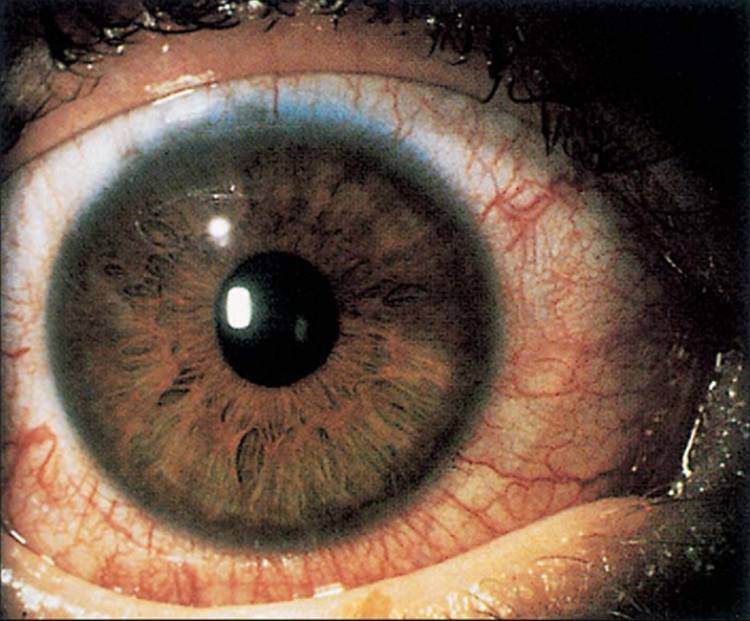
Anterior iritis is common after laser trabeculoplasty (Fig. 218.8), and patients are frequently treated with topical corticosteroids for 3-5 days. The iritis is usually mild and clears rapidly. Occasionally, the inflammation may be prolonged and may be associated with elevated IOP.
|
|
|
|
FIGURE 218.8 Inflammation after laser trabeculoplasty to the inferior 180° of the trabecular meshwork. |
One of the concerns about argon laser trabeculoplasty and the inflammation of the trabecular meshwork that it produces has been that the procedure could adversely affect glaucoma filtering surgery. While some reports found that the formation of encapsulated blebs after filtration surgery was associated with prior argon laser trabeculoplasty,[16,17] other studies did not confirm that this effect was statistically significant.[18]
RESULTS OF LASER TRABECULOPLASTY
IOP reduction does not usually occur immediately after laser trabeculoplasty but evolves over several days and weeks. The IOP reduction that may be present at 24 h is frequently accompanied by iritis; this inflammation may contribute to the initial hypotensive effect. By 4-6 weeks, however, the iritis is usually resolved and any IOP reduction caused by the procedure is apparent.
The success of laser trabeculoplasty in controlling IOP has variously been reported to range from 65% to 75% at 1 year, 59% at 3 years, 52% at 4 years, 46% at 5 years, and 32% at 10 years.[2,19-22] The short-term results are similar for all types of laser trabeculoplasty (LTP). The long-term results with argon and diode lasers are similar and are still being determined with the SLT.
Predictors of successful laser trabeculoplasty (LTP) results include type of glaucoma, prelaser IOP, lens status, and age of the patient. LTP is frequently successful in reducing IOP in primary open-angle glaucoma, glaucoma with the exfoliation syndrome, and pigmentary glaucoma.[23,24] The technique has also been shown to be effective when an eye has had prior glaucoma surgery that is failing. Glaucoma associated with uveitis, angle-recession glaucoma, glaucoma associated with the Sturge-Weber syndrome, congenital glaucoma, trabeculodysgenesis, and glaucoma in the iridocorneal endothelial syndrome are not usually successfully managed with LTP.
The absolute amount of IOP reduction by laser trabeculoplasty is frequently directly related to the prelaser IOP. Eyes with higher initial IOPs often have a greater absolute decrease in IOP. Eyes with prelaser IOPs exceeding 30 mmHg have shown reductions of 39-50%, while eyes with pretreatment IOP less than 20 had a mean decline of 3-4%.[25,26] However, AGIS demonstrated that higher prelaser IOP is associated with a higher failure rate.[27]
Phakic eyes respond to laser trabeculoplasty better than do aphakic eyes. Thomas and colleagues[28] demonstrated a mean decrease of 2 mmHg in aphakic eyes with open-angle glaucoma and a mean decrease of 7 mmHg in phakic eyes. Pseudophakic eyes also have better responses than aphakic eyes, and eyes that have had extracapsular surgery respond better than following intracapsular cataract surgery.[29]
The age of the patient affects the results of laser trabeculoplasty. Patients older than 40 years of age respond much more favorably than do younger patients, with success rates reported near 90% compared with 40% in patients less than 40 years.[27,28,30] Race does not appear to affect the short-term efficacy of laser trabeculoplasty[31] but may affect the long-term efficacy,[19] with African-American patients having a lower long-term success rate than white patients. Indian[32] and Japanese patients respond to laser trabeculoplasty similarly to white patients.
EFFICACY OF RETREATMENT
Retreatment with laser trabeculoplasty means additional laser therapy to the trabecular meshwork after the entire circumference of trabecular meshwork has been treated, whether in one or two sessions. If only one-half of the trabecular meshwork has been treated and the glaucoma again becomes uncontrolled, additional therapy to the untreated meshwork is indicated and is frequently effective in lowering IOP,[25,28,33,31] but it is not referred to as re-treatment. The results of studies of the efficacy of laser trabeculoplasty re-treatment when the entire trabecular meshwork circumference has been previously treated are variable.
In studies of eyes that had initially successful glaucoma control by laser trabeculoplasty but had a return of elevated IOP, Messner and colleagues[34] reported 36% of eyes had a 15% reduction in IOP at 6 weeks, but only 21% had such a reduction at 6 months. Brown and colleagues[35] reported a 38% success rate in glaucoma control with argon laser trabeculoplasty re-treatment, but 12% of the treated eyes had IOP increases 10 mmHg or greater, necessitating urgent surgical intervention. Richter and colleagues[36] reported that 32% of eyes re-treated were successfully controlled. Feldman and colleagues[37]determined that re-treatment was successful in 35% at 6 months, 21% at 12 months, 11% at 24 months, and 5% at 48 months.
Laser trabeculoplasty by the SLT is theoretically repeatable because it does not produce significant alterations in the trabecular meshwork. SLT has been show to reduce IOP after failed argon LTP and had the same success rate as those with SLT initial treatment.[5,38] Information on re-treatment with SLT of eyes that failed previous SLT is limited.
These studies demonstrate that laser trabeculoplasty re-treatment can lower IOP and provide glaucoma control for some patients, but the results are more variable and less predictable than with initial treatment. Consequently, re-treatment should be performed cautiously. Patients who need urgent IOP control to prevent visual loss may need glaucoma surgery rather than laser trabeculoplasty re-treatment.
REFERENCES
1. Wise JB, Witter SL: Argon laser therapy for open angle glaucoma: a pilot study. Arch Ophthalmol 1979; 97:319-322.
2. Wise JB: Long-term control of adult open angle glaucoma by argon laser treatment. Ophthalmology 1981; 88:197-202.
3. Van Buskirk EM, Pond V, Rosenquist RC, et al: Argon laser trabeculoplasty: studies on mechanism of action. Ophthalmology 1984; 91:1005-1110.
4. Acott TS, Samples JR, Bradley JMB, et al: Trabecular repopulation by anterior trabecularmeshwork cells after laser trabeculoplasty. Am J Ophthalmol 1989; 107:1-6.
5. Latina MA, Sibayan SA, Shin DH, et al: Q-switched 532-nm Nd:YAG laser trabeculoplasty (Selective Laser Trabeculoplasty). Ophthalmology 1998; 105:2082-2090.
6. Melamed S, Pei J, Epstein DL: Short-term effect of argon laser trabeculoplasty in monkeys. Arch Ophthalmol 1985; 103:1546-1552.
7. Melamed S, Pei J, Epstein DL: Delayed response to argon laser trabeculoplasty in monkeys. Arch Ophthalmol 1986; 104:1078-1083.
8. Rodrigues MM, Spaeth GL, Donahoo P: Electron microscopy of argon laser therapy in phakic open-angle glaucoma. Ophthalmology 1982; 89:198-210.
9. Kramer TR, Noecker RJ: Comparison of the morphologic changes after selective laser trabeculoplasty and argon laser trabeculoplasty in human eye bank eyes. Ophthalmology 2001; 108:773-779.
10. Glaucoma Laser Trial Research Group: The glaucoma laser trial (GLT). 2: results of argon laser trabeculoplasty versus topical medicines. Ophthalmology 1990; 97:1403-1413.
11. Glaucoma Laser Trial Research Group: The glaucoma laser trial (GLT) and glaucoma laser trial follow-up study,7: results. Am J Ophthalmol 1995; 120:718-731.
12. Glaucoma Laser Trial Research Group: The glaucoma laser trial. I. Acute effects of argon laser trabeculoplasty on intraocular pressure. Arch Ophthalmol 1989; 107:1135-1142.
13. Weinreb RN, Ruderman J, Juster R, et al: Influence of the number of laser burns administered on the early results of argon laser trabeculoplasty. Am J Ophthalmol 1983; 95:287-292.
14. Greenidge KC, Rodrigues MM, Spaeth GL, et al: Acute intraocular pressure elevation after argon laser trabeculoplsty and iridectomy: a clinicopathologic study. Ophthalmic Surg 1984; 15:105-110.
15. Robin AL: Argon laser trabeculoplasty medical therapy to prevent the intraocular pressure rise associated with argon laser trabeculoplasty. Ophthalmic Surg 1991; 22:31-37.
16. Richter CU, Shingleton BJ, Bellows AR, et al: The development of encapsulated filtering blebs. Ophthalmology 1988; 95:1163-1168.
17. Feldman RM, Gross RL, Spaeth GL, et al: Risk factors for the development of Tenon's capsule after trabeculectomy. Ophthalmology 1989; 96:336-341.
18. Schwartz AL, Van Veldhuisen PC, Gaasterland DE, et al: The advanced glaucoma intervention study (AGIS):5. encapsulated bleb after initial trabeculectomy. Am J Ophthalmol 1999; 127:8-19.
19. Schwartz AL, Love DC, Schwartz MA: Long-term follow-up of argon laser trabeculoplasty for uncontrolled open angle glaucoma. Arch Ophthalmol 1985; 103:1482-1484.
20. Grinich NP, Van Buskirk EM, Samples JR: Three-year efficacy of argon laser trabeculoplasty. Ophthalmology 1987; 94:858-861.
21. Shingleton BJ, Richter CU, Bellows AR, et al: Long-term efficacy of argon laser trabeculoplasty. Ophthalmology 1987; 94:1513-1518.
22. Shingleton BJ, Richter CU, Dharma SK, et al: Long-term efficacy of argon laser trabeculoplasty: a 10-year follow-up study. Ophthalmology 1993; 100:1324-1329.
23. Lieberman MF, Hoskins HD, Hetherington Jr J: Laser trabeculoplasty and the glaucomas. Ophthalmology 1983; 90:790-795.
24. Robin AL, Pollack IP: Argon laser trabeculoplasty in secondary forms of open angle glaucoma. Arch Ophthalmol 1983; 101:382-384.
25. Horns DJ, Bellows AR, Hutchinson BT, et al: Argon laser trabeculoplasty for open-angle glaucoma: a retrospective study of 380 eyes. Trans Ophthalmol Soc UK 1983; 103:288-296.
26. Schwartz AL, Whitter ME, Bleiman B, et al: Argon laser trabecular surgery in uncontrolled phakic open angle glaucoma. Ophthalmology 1981; 88:203-212.
27. The Advanced Glaucoma Intervention Study (AGIS):11. risk factors for failure of trabeculectomy and argon laser trabeculoplasty. Am J Ophthalmol 2002; 134:481-498.
28. Thomas JV, Simmons RJ, Belcher CD: Argon laser trabeculoplasty in the pre-surgical glaucoma patient. Ophthalmology 1982; 89:187-197.
29. Schwartz AL, Wilson MC, Schwartz LW: Efficacy of argon laser trabeculoplasty in aphakic and pseudophakic eyes. Ophthalmic Surg Lasers 1997; 28:215-218.
30. Safran MJ, Robin AL, Pollack IP: Argon laser trabeculoplasty in younger patients with primary open angle glaucoma. Am J Ophthalmol 1984; 97:292-295.
31. Krupin T, Patkin R, Kurata FK, et al: Argon laser trabeculoplasty in black and white patients with primary open-angle glaucoma. Ophthalmology 1986; 93:811-816.
32. Singh M, Kaur B: Argon laser trabeculoplasty in Asian eyes. Int Ophthalmol 1987; 10:161-165.
33. Klein HZ, Shields MB, Ernest JT: Two-stage argon laser trabeculoplasty in open angle glaucoma. Am J Ophthalmol 1985; 99:392-395.
34. Messner D, Siegel LI, Kass MA, et al: Repeat argon laser trabeculoplasty. Am J Ophthalmol 1987; 103:113-115.
35. Brown SVL, Thomas JV, Simmons RJ: Laser trabeculoplasty re-treatment. Am J Ophthalmol 1985; 99:8-10.
36. Richter CU, Shingleton BJ, Bellows AR, et al: Retreatment with argon laser trabeculoplasty. Ophthalmology 1987; 94:1085-1089.
37. Feldman RM, Katz LJ, Spaeth GL, et al: Long-term efficacy of repeat argon laser trabeculoplasty. Ophthalmology 1991; 98:1061-1065.
38. Latina MA, Gulati V: Selective laser trabeculoplasty: stimulating the meshwork to mend its way. Int Ophthalmol Clin 2004; 44:93-103.