Wade R. Smith, MD, FACS
Philip F. Stahel, MD, FACS
Takashi Suzuki, MD
Gabrielle Peacher, MD
THE HIGH COST OF MUSCULOSKELETAL TRAUMA
Injury has become a major cause of death and disability globally. Trauma is the leading cause of death for people age 1–34 years of all races and socioeconomic levels and the third leading cause of death for all age groups. Traumatic motor vehicle accidents (MVAs) are the leading cause of traumatic death. Approximately 1.3 million people die on the world’s roads every year. Over 20 million people sustain nonfatal injuries. In 2010, death from road traffic accidents was the ninth cause of all deaths; it is estimated to be the fifth leading cause of death by 2030, resulting in 2.4 million fatalities per year. The economic impact of MVAs is approximately $230 billion in the United States and €180 billion in the European Union. The global losses due to road traffic injuries are estimated to be $518 billion, and these injuries cost governments between 1 and 3% of their gross national product. Low-income and middle-income countries account for $65 billion, which is more than they receive in development assistance.
Gunshot injuries are the third cause of all injury-related deaths in the United States. There are 60,000–80,000 nonfatal gunshot wounds annually in the United States. In 2006, 30,896 persons died from firearm injuries in the United States, with estimated lifetime medical costs over $2 billion.
Trauma is the leading cause of death and disability in children, accounting for some 11 million hospitalizations, 150,000 disabilities, and 15,000 deaths every year in the United States. Although direct costs of pediatric trauma exceed $8 billion per year, indirect costs to families and society are impossible to estimate but undoubtedly substantial.
With an unprecedented increase in population and life expectancy, age-related musculoskeletal conditions such as fragility fractures and sports-related ligamentous injuries are now more common than ever, even in the elderly population. Approximately 1.6 million hip fractures occur worldwide each year. By 2050, this number is expected to increase three- or fourfold. In 2005 in the United States, over 2 million osteoporotic fractures cost $17 billion.
Both natural and man-made disasters have caused hundreds of thousands of deaths and disabilities in the past 20 years, and the World Health Organization estimates an overall increase over the next two decades. Although true mass casualty situations are rare, the earthquake in Haiti in 2010 left 300,000 injured behind. These situations require highly organized trauma systems for optimal outcomes.
While considering the cost of musculoskeletal injuries, effects on the patient, the family, and society in general should be considered. Practitioners should keep in mind that there are direct expenditures for diagnosis, treatment, and rehabilitation, and also indirect economic costs associated with lost labor and diminished productivity.
Dougherty PJ, Vaidya R, Silverton CD, Bartlett C, Najibi S: Joint and long-bone gunshot injuries. J Bone Joint Surg Am 2009;91:980-997. [PMID: 20415399]
Galano GJ, Vitale MA, Kessler MW, Hyman JE, Vitale MG: The most frequent traumatic orthopaedic injuries from a national pediatric inpatient population. J Pediatr Orthop 2005;25:39-44. [PMID: 15614057]
Gullberg B, Johnell O, Kanis JA: World-wide projections for hip fracture. Osteoporos Int 1997;7:407-413. [PMID: 9425497]
Heron M, Hoyert DL, Murphy SL, Xu J, Kochanek KD, Tejada-Vera B: Deaths: final data for 2006. Natl Vital Stat Rep 2009;57:1-134. [PMID: 19788058]
Mathers CD, Loncar D: Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med 2006;3:e442. [PMID: 17132052]
Peden M, Scurfield R, Sleet D, et al: World Report on Road Traffic Injury Prevention. Geneva, Switzerland: World Health Organization; 2004.
THE HEALING PROCESS
![]() Bone Healing
Bone Healing
Bone is a unique tissue among all musculoskeletal tissues because it heals by the formation of normal bone, as opposed to scar tissue. In fact, it is considered a nonunion when a bone heals by a fibroblastic response instead of by bone formation.
Fracture healing can be divided into primary and secondary healing. In primary healing, the cortex attempts to reestablish itself without the formation of callus (osteonal or haversian healing). This occurs when the fracture is anatomically reduced, the blood supply is preserved, and the fracture is rigidly stabilized by internal fixation. Secondary fracture healing results in the formation of callus and involves the participation of the periosteum and external soft tissues. This fracture healing response is enhanced by motion and is inhibited by rigid fixation.
Fracture healing can be conveniently divided, based on the biologic events taking place, into the following four stages:
1. Hematoma formation (inflammation) and angiogenesis
2. Cartilage formation with subsequent calcification
3. Cartilage removal and bone formation
4. Bone remodeling
Initially, there is hematoma formation followed by an inflammatory phase characterized by an accumulation of mesenchymal cells around the fracture site. These mesenchymal cells differentiate into chondrocytes or osteoblasts. Growth factors and cytokines derived mainly from platelets are essential for angiogenesis, cellular chemotaxis, proliferation, and differentiation. Growth factors induce mesenchymal cells and osteoblasts to produce type II collagen and proteoglycans. Platelet-derived growth factor (PDGF) recruits inflammatory cells at the fracture site. Bone morphogenetic proteins (BMPs) are osteoinductive mediators inducing metaplasia of mesenchymal cells into osteoblasts. Interleukin (IL)-1 and IL-6 recruit inflammatory cells to the fracture site. Periosteum is the main source of mesenchymal cells. In high-energy fractures where the periosteum has been compromised, stem cells originate from the circulation and the surrounding soft tissues.
Low oxygen tension, low pH, and movement favor the differentiation into chondrocytes; high oxygen tension, high pH, and stability predispose toward osteoblast stimulation. In the presence of mechanical instability, fractures heal by the process of endochondral ossification—bony callus formation is preceded by a cartilaginous template.
Chondrocytes and fibroblasts produce a semirigid soft callus that is able to provide a mechanical support to the fracture, as well as act as a template for the bony callus that will later supersede it. The most active stage of osteogenesis, also known as primary bone formation, is characterized by high levels of osteoblast activity and the formation of mineralized bone matrix, which arises directly in the peripheral callus in areas of stability. Mineralization causes chondrocyte degeneration, hypertrophy, and finally apoptosis. The phase of mineralized callus leads to a state in which the fracture site is enveloped in a polymorphous mass of mineralized tissues consisting of calcified cartilage, woven bone made from cartilage, and woven bone formed directly. The woven-bone mineralized callus has to be replaced by lamellar bone arranged in osteonal systems to allow the bone to resume its normal function. In order for bridging new hard callus to form, the insecure soft callus is gradually removed, concomitant with revascularization. The new bone is known as hard callus, and it is typically irregular and underremodeled.
The final stage of fracture repair, also referred to as secondary bone formation, encompasses the remodeling of the woven bone hard callus into the original cortical and/or trabecular bone configuration. The key cell type involved with the resorption of mineralized bone is the osteoclast, which is a large, multinucleated cell formed by fusion of monocytes. Osteoblasts are mononuclear and are responsible for the accretion of bone.
Macrophage colony-stimulating factor (M-CSF) and receptor activator of nuclear factor-κB ligand (RANKL) are two principal cytokines secreted by osteoblasts that are critical for the induction, survival, and competency of osteoclasts.
![]() Cartilage Healing
Cartilage Healing
Articular cartilage consists of extracellular matrix (ECM) and chondrocytes. The ECM is formed by water (65–80%), collagen (95% type II), and proteoglycans (chondroitin sulfate and keratan sulfate). Collagen in the ECM provides form and tensile strength. Proteoglycans and water give the cartilage stiffness, resilience, and endurance.
Chondrocytes are sparse in the adult cartilage, which is not a vascularized tissue. Their nutrition comes from the synovial fluid, and adequate circulation of the fluid through the spongelike cartilage matrix is crucial. The low baseline metabolic rate and small cell-to-matrix ratio of chondrocytes also diminish the reparative capacity of articular cartilage. Motion of the joint is responsible for most of the circulation. Rigid internal fixation of articular fractures and early weight bearing of immobilized joints allow cyclical compression of the cartilage and circulation of the synovial fluid. If the defect in the cartilage does not go through the calcified plate, the body attempts repair with hyaline cartilage. This may be seen at superficial articular cartilage lesions. Chondral fissures, flap tears, and chondral defects are loss of segmental cartilage. They have a limited, short chondrocytic reparative response. If the calcified plate is violated, as in osteochondral lesions, the subchondral capillaries bring an inflammatory reaction, which fills the defect with granulation tissue and, eventually, fibrocartilage. The quality of this fibrocartilage can be improved by passive or active motion of the joint. Basic and clinical research has shown the potential of artificial matrices, growth factors, perichondrium, periosteum, transplanted chondrocytes, and mesenchymal stem cells to stimulate the formation of cartilage in articular defects.
![]() Tendon Healing
Tendon Healing
Tendons are specialized structures that allow muscles to extend their contractile action. Tendons consist of long bundles of collagen scattered with relatively inactive fibrocytes. These cells are nourished by the synovial fluid secreted by the one-cell-thick synovial membrane that covers the tendon (endotenon) and the parietal surface of the sheath (epitenon). The flexor tendons are covered by a richly vascularized adventitia (paratenon).
![]() Muscle Healing
Muscle Healing
Type 1 fiber, known as slow twitch, slow oxidative, or red muscle, has a slow speed of contraction and the greatest strength of contraction. It functions aerobically and, therefore, is fatigue-resistant. Type 2 fiber, known as fast twitchor white muscle, is subdivided into two types, according to metabolic activity level: fiber that functions by oxidative and glycolytic metabolism (type 2A) and fiber that is largely glycolytic (type 2B). Both subtypes of white fast-twitch muscles are fatigable but have high strength of contraction and high speed of contraction. Traumatic injury to muscle can occur from a variety of mechanisms, including blunt trauma (muscle contusion), laceration, and strains resulting from excessive stretching or ischemia. Recovery occurs through a process of degeneration and regeneration, with new muscle cells arising from undifferentiated cells. In addition to muscle regeneration, laceration repair requires reinnervation of denervated muscle areas. Muscle contusion frequently results in hematoma. The normal repair process includes an inflammatory reaction, formation of connective tissue, and muscle regeneration. Blunt trauma may result in myositis ossificans and may cause decreased function.
Orthopedic surgeons should be aware of atrophy of muscle tissue due to immobilization and lack of activity. Loss of muscle weight initially occurs rapidly and then tends to stabilize, and loss of strength occurs simultaneously. Resistance to fatigue diminishes rapidly.
![]() Nerve Healing
Nerve Healing
Multiple nerve fibers combine to form a fascicle surrounded by perineurium. Multiple fascicles are surrounded by epineurium. Nerves fall into patterns of monofascicular, oligofascicular, and polyfascicular structures. The size and distribution of fascicles change as a function of length, reflecting greater or lesser nerve fibers in each fascicle. Increasing distance from the nerve injury to the distal point of inner-vation reduces the likelihood of recovery. Other factors include the length of the damage to the nerve, the technical ability of the surgeon, and the length of time prior to repair. Nerves can be damaged in many ways, including stretching, and ischemic damage may occur at elongation of 15%. Nerve injuries are rated from 1 to 5 degrees; however, Mackinnon introduced a sixth-degree injury to describe a mixed nerve injury that combines the other degrees of injury. First-degree injury is the least severe and equivalent to neurapraxia. Second-degree injury is equivalent to axonotmesis, with degeneration of the axon; recovery is complete. Third-degree injury is the same as second-degree injury with the addition of loss of continuity of the endoneurial tube. Despite the continuity of the nerve trunk, because of extensive degeneration of the fascicles, fourth-degree injuries may require excision of the damaged segment, with reapproximation or grafting of the nerve ends to achieve a functional outcome. Fifth-degree injury involves complete loss of continuity of the nerve trunk. Surgical repair is required to achieve restoration of function.
The outcome of recovery is much more optimistic for children than adults, and the prognosis diminishes with age.
Browne JE, Branch TP: Surgical alternatives for treatment of articular cartilage lesions. J Am Acad Orthop Surg 2000;8:180. [PMID: 10874225]
Buckwalter JA: Articular cartilage injuries. Clin Orthop Relat Res 2002;402:21-37. [PMID: 14620787]
Jackson DW, Scheer MJ, Simon TM: Cartilage substitutes: overview of basic science and treatment options. J Am Acad Orthop Surg 2001;9:37. [PMID: 11174162]
Lee SK, Wolfe SW: Peripheral nerve injury and repair. J Am Acad Orthop Surg 2000;8:243. [PMID: 10951113]
Mackinnon SE, Dellon AL: Surgery of the Peripheral Nerve. New York: Thieme; 1988.
Robinson LR: Role of neurophysiologic evaluation in diagnosis. J Am Acad Orthop Surg 2000;8:190. [PMID: 10874226]
ORTHOPEDIC ASSESSMENT AND MANAGEMENT OF MULTIPLY INJURED PATIENTS
A thorough understanding of the pathophysiology of trauma is essential for prompt diagnosis and timely treatment of musculoskeletal injuries. Sound therapeutic principles improve the overall outcome for the patient and optimize the utilization of limited health care resources.
![]() Life-Threatening Conditions: The ABCs of Trauma Care
Life-Threatening Conditions: The ABCs of Trauma Care
A systematic approach is required in all cases. The patient is assessed, and treatment priorities are established according to the type of injury, stability of vital signs, and mechanism of injury. In a severely injured patient, treatment priorities are dictated by the patient’s overall condition, with the first goal being to save life and preserve the major functions of the body. Assessment consists of four overlapping phases:
1. Primary survey (ABCDE)
2. Resuscitation
3. Secondary survey (head-to-toe evaluation and history)
4. Definitive care
This process identifies and treats life-threatening conditions and can be remembered as follows:
Airway maintenance (with cervical spine protection)
Breathing and ventilation
Circulation (with hemorrhage control)
Disability (neurologic status)
Exposure and environmental control (undress the patient but prevent hypothermia)
A brief overview of the treatment of polytrauma patients, with special emphasis on the orthopedic aspects, follows.
A. Airway
Great care should be taken while assessing the airway. The cervical spine should be carefully protected at all times and not be hyperextended, hyperflexed, or rotated to obtain a patent airway. Any patient with a blunt injury above the clavicle should be considered at risk for cervical spine injury. The airway should be rapidly assessed for signs of obstruction, foreign bodies, and facial, mandibular, or tracheal/laryngeal fractures. A chin lift or jaw thrust maneuver should be used to establish an airway. A Glasgow Coma Score of 8 or less, decreased mental status, severe pulmonary injury, facial fracture, or laryngeal injury is an indication for the placement of a definitive airway.
B. Breathing
The trauma surgeon should evaluate the patient’s chest. Adequate ventilation requires not only airway patency but also adequate oxygenation and carbon dioxide elimination. Remember that the following four conditions, if present, must be addressed emergently:
1. Tension pneumothorax
2. Flail chest with pulmonary contusion
3. Open pneumothorax
4. Massive hemothorax
C. Circulation
Hemorrhage is the principal cause of preventable postinjury death. Postinjury hypotension is considered hypovolemic in origin until proven otherwise. Level of consciousness, skin color, and pulses are simple to assess and reliably mirror the hemodynamic status of the patient, especially if recorded serially. Fractures of the femur or pelvis can cause major blood loss, which can severely compromise survival. (See sections on pelvic and femoral fracture.)
D. Disability (Neurologic Status)
The Glasgow Coma Score (see Chapter 12, “Rehabilitation”) should be used to assess neurologic status; it is quick, simple, and predictive of patient outcome. An even simpler way to monitor central neurologic status is to remember the mnemonic AVPU and check if the patient is Alert and oriented, or responds to Vocal stimuli, or responds only to Painful stimuli, or is Unresponsive.
E. Exposure and Environmental Control
For a thorough examination of lacerations, contusions, abrasions, swelling, and deformities, the patient should be completely disrobed. This also prevents further displacement of fractures and minimizes the risk of overlooking significant problems. Hypothermia must be avoided because cardiac function may be affected, especially when there is decreased blood volume.
F. Care of Patient Before Hospitalization
As a general rule, the following measures should be taken for patients with fractures:
1. The joints above and below the fracture should be mobilized and adequate immobilization of the cervical spine should be obtained to prevent further damage to the neurovascular elements and limit hemorrhage.
2. Splints can be improvised with pillows, blankets, or clothing.
3. Immobilization does not need to be absolutely rigid.
4. Apply gentle in-line traction to realign the extremity when there is severe angulation.
5. Overt bleeding should be tamponaded with available dressings and firm pressure.
6. Tourniquets should be avoided, unless the patient’s life is in danger from extremity bleeding.
![]() Orthopedic Examination
Orthopedic Examination
A. History
An adequate assessment of the conditions in which the injury was sustained is crucial. Information from paramedics, patient relatives, and bystanders should be recorded. Obtain the following information according to injury mechanism:
1. MVA: speed; direction (T bone, rollover, etc.); patient location in the vehicle, impact location, postimpact location of the patient (if ejection, determine distance); internal and external damage to the vehicle; restraint use and type.
2. Falls: distance of the fall; landing position.
3. Crush: weight of the object, site of the injury, duration of weight application.
4. Explosion: blast magnitude; patient distance from the blast: primary blast injury (force of the blast wave); secondary blast injury (projectiles).
5. Vehicle-pedestrian: type of vehicle, site of collision, speed.
Environmental exposure, comorbidity (diabetes, coronary artery disease, etc.), use of steroids, prehospital care, and observations at the accident scene should be determined. Estimated bleeding, open wounds, deformity, motor and sensory function, and delays in extrication or transport are recorded.
B. General Examination
The clinical orthopedic examination requires assessment of the axial skeleton, pelvis, and extremities. The extent of this examination depends on the patient’s overall central neurologic status. Swelling, hematomas, and open wounds are assessed visually in the undressed patient. It is obligatory to palpate the entire spine, pelvis, and each joint. Examination soon after trauma may precede telltale swelling in joint or long bone injuries. In the unresponsive patient, only crepitation and false motion may be discerned. The pelvic examination is important; however, if the patient is hemo-dynamically unstable, manipulation of the pelvis should be avoided in order to prevent increased bleeding.
C. Neurologic Examination
The neurologic examination of the extremities should be documented to the fullest extent possible, in light of the patient’s mental status, because it is central to subsequent decision making. This examination includes delineation of sensory function in the major nerves and dermatomes in the upper and lower extremities. Perianal sensation is also important. A normal neurologic examination does not rule out cervical spine injuries; it only makes them less likely. Particularly important when there is spinal cord injury or suspected injury are the reflexes of the anal “wink” and bulbocavernosus muscle. Other spinal reflexes (ie, of the biceps and triceps muscles, of the knee and ankle, and the Babinski reflex) are important in “fine-tuning” the neurologic examination. (These are discussed more fully in Chapter 4, “Disorders, Diseases, and Injuries of the Spine.”)
D. Muscle Examination
Motor examination can be difficult because of pain or impaired mental status, but even in such cases, useful and relatively complete information can be obtained. One must be sure to evaluate all upper and lower extremity motion. Hematoma, ecchymosis, and dermabrasions should be noted for an underlying muscle injury. Muscle strength grading is desirable, but demonstration of a minimum of volitional control (even if withdrawal to painful stimuli) is important in verifying the presence of intact central sensory-motor integration.
![]() Imaging Studies
Imaging Studies
Radiologic assessment follows the same general hierarchy as the clinical assessment. The severely injured polytrauma patient requires plain films of the chest, abdomen, and pelvis to indicate sources of respiratory and circulatory compromise. The second level of examination requires the cervical spine cross-table lateral view. The information obtained from this film dictates treatment and the need for any further evaluation of the cervical spine. In the hemodynamically unstable patient, the anteroposterior (AP) pelvis film is sufficient to make immediate treatment decisions. Complementary pelvis films can be obtained later.
Subsequent evaluation is dependent on clinical findings. Any long bone or joint with a laceration, hematoma, angulation, or swelling must undergo roentgenographic evaluation. Any long bone fracture requires complete evaluation of the joints proximal and distal to the fracture. At the minimum, two views of the extremities are needed, usually the AP and lateral views. The use of focused assessment sonography in trauma (FAST) has also become an extension of the physical examination of the trauma patient. Coordination of more sophisticated studies with other trauma specialties (eg, neurosurgery or urology) is necessary to allow cardiorespiratory monitoring of the patient while efficiently performing these studies.
![]() “Clearing” the Cervical Spine
“Clearing” the Cervical Spine
The ATLS (Advanced Trauma Life Support) protocol mandates that all patients are presumed to have a cervical spine injury until proven otherwise. The objective of cervical spine clearance is to establish that an injury does not exist. If there is a change in orientation from one cervical spine level to another, then cervical fracture, jumped facets, or dislocation should be suspected. Immobilization in a cervical collar should be initiated until the secondary evaluation has been made. In the conscious and responsive patient, swelling or tenderness on physical examination of the cervical spine is readily apparent. In the unconscious patient, cervical spine injuries can go undetected, and a careful physical examination must be performed with heavy reliance on radiographic evaluation.
The essential radiographs for evaluation of the cervical spine include AP views, lateral views, and an open-mouth odontoid view. It is essential to be able to see to the top of T1. If this level is not visualized through these conventional views, the inclusion of oblique view and swimmer’s view, which is a lateral cervical spine radiograph with the arm abducted and elevated, only slightly improves the sensitivity and, therefore, has been deemed cost-inefficient.
On the open-mouth view, the lateral masses of C1 should line up with the body of C2. The amount of total overhang of C1 over C2 should be less than 7 mm. On the lateral view, the anterior border of the bodies of the cervical segments should be an arc. The distance from the basion to the posterior arch of C1 divided by the distance from the opisthion to the anterior arch of C1 should be less than 1 (Powers ratio) (Figure 2–1). A basion to odontoid tip distance greater than 10 mm in children and 5 mm in adults indicates craniocervical dislocation, a potentially fatal injury. The posterior border of the anterior arch of C1 should be within 2–3 mm of the anterior border of C2. There should be no diastasis of the spinous processes, and the joints and facet joints should all be visible. In the obtunded patient, computed tomography (CT) and/or magnetic resonance imaging (MRI) scan is necessary to delineate soft-tissue injuries. Although CT is sensitive in the identification of osseous abnormalities, it has not been shown to have the same level of accuracy as MRI in detecting an isolated ligamentous injury. MRI is not indicated for primary cervical spine clearance imaging procedures. MRI requires extensive time to perform, interferes with the patient’s monitoring equipment, and is expensive. MRI is most useful in the patient for whom other imaging modalities are not consistent with the neurologic presentation.

![]() Figure 2–1. Powers ratio: a – anterior arch of atlas, b – basion, p – posterior arch of atlas, o – opisthion. The ratio of bp:oa should be approximately 0.77 in the normal population. Anterior occipitoatlantal dislocation is present when the Powers ratio is greater than 1.15.
Figure 2–1. Powers ratio: a – anterior arch of atlas, b – basion, p – posterior arch of atlas, o – opisthion. The ratio of bp:oa should be approximately 0.77 in the normal population. Anterior occipitoatlantal dislocation is present when the Powers ratio is greater than 1.15.
In the case of neurologic deficit, careful evaluation of the neurologic status is important, and immediate decompression-stabilization must be considered.
![]() Immediate Management of Musculoskeletal Trauma
Immediate Management of Musculoskeletal Trauma
The orthopedic injuries in the polytrauma patient are seldom truly emergency situations, except for those involving neural or vascular compromise. For example, fracture-dislocation of the ankle or knee resulting in distal ischemia justifies immediate attempts at reduction to minimize the sequelae of ischemia. A more subtle situation requiring emergent treatment would be dislocation of the hip in which vascular compromise of the femoral head, avascular necrosis, may result. Arterial bleeding from an open fracture should be treated immediately with pressure to minimize blood loss. Other bone and joint injuries, although urgent, may be approached in a more deliberate manner.
Orthopedic surgeons must be aware that management of traumatic injuries requires consideration of the entire patient as well as the entire extremity.
![]() Complications
Complications
There is ample evidence to indicate that the early treatment of fractures in a multiply injured patient has a significant effect on the risk of the subsequent development of respiratory complications. Traumatic injury leads to systemic inflammation as a normal response to injury. Extent of injury, hypoxia, consequent surgeries, and blood loss may impair the balance existing between the beneficial effects of inflammation and the potential for the process itself to cause and aggravate tissue injury, leading to acute respiratory distress syndrome (ARDS) and multiple organ failure (MOF). Early fracture fixation allows early mobilization, which is beneficial to prevent pulmonary complications. Definitive or lengthy surgery, however, causes further complications.
A. Acute Respiratory Distress Syndrome and Multiple Organ Failure
ARDS is used to describe the respiratory failure associated with evidence of multiple organ dysfunction, which occurs in patients after high-energy injury. The lung is prominently targeted in the early stages, but if the patient survives, features of cardiac, gastrointestinal, renal, hepatic, hematologic, and cerebral failure become apparent as part of the syndrome of MOF. Massive tissue injury activates the immunologic system and releases inflammatory mediators, with subsequent disruption of the microvasculature of the pulmonary system. Some acute orthopedic procedures have been shown to similarly activate the immune system. The incidence of ARDS after major trauma is probably between 5 and 8%, with mortality between 3 and 40% of cases. Postinjury MOF is the most significant cause of late trauma mortality.
Fat embolism syndrome (FES) is a unique manifestation of ARDS caused by the release of marrow fat into the circulation. Embolism occurs in over 95% of patients after fracture and invariably during reamed nailing of fractures. However, only 1–5% of patients develop severe pulmonary compromise and FES. This syndrome may also occur in nonfracture situations involving pressurization of the medullary canal of long bones. Cardinal pulmonary signs of ARDS and FES are refractory hypoxemia, not correctable by high-dose oxygen therapy (60–100%), associated with the development of a characteristic “snowstorm” appearance in both lung fields on chest radiography. A characteristic petechial rash is found in 60% of patients with FES, and neurologic features are encountered in over 80%, including the development of an acute confusional state or a focal neurologic deficit.
B. Atelectasis
Atelectasis, or localized collapse of alveoli, is a frequent postoperative complication because of patient immobilization. Combined with respiratory depression due to analgesia, significant hypoxemia can result, and onset may be relatively rapid. This may be a source of postoperative fever in the early recovery phase. Occasionally, radiograph examination, showing collapse of areas of the lung, will confirm the diagnosis. By encouraging coughing and deep breathing, using incentive spirometry, and, in resistant cases, using respiratory therapy, resolution can be expected.
C. Pulmonary Embolism and Deep Venous Thrombosis
Pulmonary embolism (PE) is the third most common cause of death in trauma patients who survive after the first day. The trauma patient is at a 13-fold increased risk of venous thromboembolism (VTE). There are several factors associated with increased risk of VTE in a trauma patient (Table 2–1). Patients at high risk for PE are those with deep venous thrombosis (DVT) in the lower extremities and pelvic veins. Clinically significant PE usually arises from the large veins proximal to the knee. Prevention of DVT in the venous system in this area reduces the risk of PE. Various strategies used to accomplish this include drug therapy with low-dose heparin, low-molecular-weight heparin, pentasaccharide, or sodium warfarin and mechanical prophylaxis with intermittent pneumatic compression devices or inferior vena cava filters in high-risk patients with contraindications to pharmacologic prophylaxis.
Table 2–1. Factors that increase the risk for developing venous thromboembolism (VTE) in trauma patients.

Clinical diagnosis of DVT is unreliable. Definitive diagnosis is made with venography, duplex ultrasound scanning, impedance plethysmography, or CT or MRI venography. Prevention appears to be the best strategy because even routine surveillance screening in a trauma population is cost-ineffective and does not appear to lower the overall rate of PE.
PE is suspected in the orthopedic patient suffering an onset of tachypnea and dyspnea usually more than 5 days after an inciting event. The patient frequently reports chest pain and can often point to the painful area. On physical examination, tachycardia, cyanosis, and pleural friction rub can be noted. Arterial blood gas studies demonstrate hypoxemia, although this is a nonspecific finding. Use of the D-dimer is unreliable in the early trauma patient but may be useful later in the recovery period. Definitive diagnosis is best made with CT angiogram. Perfusion ventilation scanning is less invasive and may help determine whether there is a high or low probability of PE. Single-slice spiral CT has become the reference standard for imaging acute PE in clinical practice. The negative predictive value of a normal spiral CT approaches 98%.
Treatment involves pulmonary support and heparin therapy. The natural history of treated PE is gradual lysis of the emboli, with the return of flow through the pulmonary arterial tree. The natural history of proximal DVT involves recanalization and arborization to bypass the clot. Patients may suffer from postphlebitic syndrome characterized by chronically painful swelling in the extremity.
D. Compartment Syndrome
The term compartment syndrome refers to pathologic developments in a closed space in the body caused by buildup of pressure. Most commonly, such compartments are circumscribed by fascia and incorporate one or more bones. Pressure rises from edema or bleeding within the compartment, compromising circulation to the contents of the compartment over a period, and can result in necrosis of muscle and damage to nerves.
Compartment syndrome may result from a fracture; a soft-tissue injury; a vascular injury causing ischemia, necrosis, and edema; or a burn. Failure to redistribute pressure through postural changes results in ischemia of the area under pressure because of collapse of capillaries.
The diagnosis of compartment syndrome must be considered in the postoperative or posttrauma patient who has pain out of proportion to that expected from the inciting injury. As the pain worsens, it can become totally unresponsive to narcotic medication. Subsequent to fracture or injury, pain with passive stretching of involved muscles is also a subjective finding and must be differentiated from pain arising from the original injury.
The five P’s (pulselessness, paresthesia, paresis, pain, and pressure) characteristic of compartment syndrome are helpful, but not diagnostic. Pulses are poor indicators of compartment syndrome as they generally remain intact until late.
Patients with equivocal clinical findings or those at high risk but without a reliable clinical examination (eg, those who are comatose, have psychiatric problems, or are under the influence of narcotics) should have compartmental pressure measurements.
Intracompartmental pressure readings within 30 mm Hg or less of the diastolic blood pressure are indications for fasciotomy. Prior to fasciotomy, circular dressings, including casts, should be removed, and the patient should be observed for a short period for signs of improvement. Positive clinical findings may justify fasciotomy despite normal pressures. Late fasciotomy may result in muscle damage or possible necrosis, with resulting risk of infection.
Although compartment syndrome can occur in almost any portion of the body, young patients who have a tibia fracture or patients with a high-energy forearm fracture are at particular risk. In the forearm, an extensile volar incision to permit complete release, including the carpal tunnel distally and the lacertus fibrosus proximally, is necessary. Dorsally, a longitudinal incision is used. In the calf, two incisions are used to release the four compartments of the leg. The anterior and lateral compartments are decompressed using a longitudinal incision approximately over the anterior intermuscular septum. Posteromedially, a second incision is used to approach the superficial and deep posterior compartments. While single and limited incision approaches have been described, these may be unreliable and have a higher incidence of iatrogenic nerve injury in trauma patients.
E. Heterotopic Bone Formation
Clinically significant heterotopic ossification occurs as a consequence of trauma in perhaps 10% of cases and may cause pain or joint motion restriction even to the point of ankylosis. Trauma patients without head injuries frequently manifest heterotopic ossification on radiograph 1–2 months following trauma; if the ossification is clinically significant, resection may be indicated when the bone has matured as indicated by radiographs and bone scan. This can take up to 18 months to achieve.
Resection is accomplished by removing the entire piece of heterotopic bone. Selected patients may benefit from low-dose radiation (7 Gy) and oral indomethacin for 3–6 weeks. In acetabular fractures, a focused single dose of radiation may be better than oral indomethacin. Heterotopic bone is a much more common occurrence in patients with head injuries. This is believed to result from release of humeral modulators that have not yet been characterized. Further discussion of this topic can be found in Chapter 12, “Rehabilitation.”
![]() Classification of Open Fractures: Gustilo and Anderson Classification
Classification of Open Fractures: Gustilo and Anderson Classification
The Gustilo and Anderson classification, the most popular and generally accepted classification of open fractures, uses three grades and divides the third most severe grade into three subtypes (Table 2–2). The prevalence of wound infection increases with the increase in grade of open injury. Open fractures resulting from natural disasters, highly contaminated or comminuted, independent of wound size, are automatically classified as grade III open fractures.
Table 2–2. Gustilo-Anderson classification for open fractures.

The magnitude of soft-tissue and bony injuries complicates the decision making between immediate amputation and reconstruction in the lower extremity. Despite the advent of microvascular surgery, prosthetic replacements are a viable alternative to a poorly functioning, insensate lower extremity. Long years of reconstruction to achieve union without infection, multiple operations, and emotional trauma should be considered in the decision making of salvage versus amputation.
![]() Early Total Care
Early Total Care
The desirability of early fracture stabilization in multiply injured patients has become well established. Benefits of timely and aggressive treatment include decreased rates of mortality, primarily due to reductions in ARDS and MOF. In a classic study by Bone et al, 178 patients with femoral fractures were entered into an early fixation group (treatment within 24 hours) or a delayed fixation group (treatment after 48 hours). The incidence of pulmonary complications, such as ARDS, fat embolism, or pneumonia, was higher, the hospital stay was longer, and the intensive care unit requirements increased when femoral fixation was delayed. A follow-up, retrospective, multicenter study of 676 patients who had an Injury Severity Score greater than 18 and major pelvic or long-bone injuries treated with early fixation within 48 hours revealed a lower mortality rate for patients whose fractures were stabilized early.
![]() Damage Control Orthopedics
Damage Control Orthopedics
Controversy exists regarding the appropriate timing of orthopedic intervention for specific subsets of severely injured patients, particularly those with head injury or systemic hypotension. Long bone fracture fixation with reamed intramedullary rods, in particular, may cause intra-operative hypotension or an increased release of inflammatory mediators with deleterious results in specific patients.
The multiply injured patient’s immunologic system is stimulated or primed after trauma (first event). Subsequent resuscitation, hemorrhage, blood products, hypotension, and surgery (second event) may produce an exaggerated systemic inflammatory response syndrome (SIRS), potentially leading to ARDS or MOF. Activated neutrophils are the principal effector of the inflammatory response, releasing active oxygen species, which damage the vascular endothelium. Bone marrow contents pushed to the systemic circulation during reaming and nailing can activate neutrophils, leading to SIRS in polytrauma patients, particularly during the first 96 hours after trauma. Damage control orthopedics (DCO) aims to decrease the additional surgical trauma through external fixation and secondary definitive surgery. Several studies demonstrated that conversion of an external fixator to a reamed intramedullary nail is safe and effective if performed within 2 weeks. Alternatives to modify the inflammatory response are currently under investigation. Tuttle et al showed that DCO is a safer initial approach that helps to reduce blood loss and significantly decrease the initial operative exposure. Additionally, in 2008, Parekh et al demonstrated that temporary bridging fixation and planned conversion to internal fixation of periarticular knee fractures resulting from high-energy injury avoid the risk of potential local soft-tissue damage of early internal fixation.
![]() Soft-Tissue Injuries and Traumatic Arthrotomies
Soft-Tissue Injuries and Traumatic Arthrotomies
Lacerations of the extremities can result in neural or vascular compromise to an extremity and may also cause traumatic arthrotomies. Compromise of the sterility of any joint requires surgical debridement of that joint. For many joints, arthroscopic irrigation and debridement will minimize trauma and improve the return to function. All complete tendon lacerations of the hand, except for those of the palmaris longus, should be repaired. In the foot, extrinsic tendons are repaired to prevent late imbalance or loss of function. Muscle belly injuries generally require surgical debridement because their subfascial location makes simple irrigation difficult. Laceration involving only the muscle belly usually requires no surgical repair. Frequently, however, muscle belly laceration involves the continuation of the origin or the insertion tendon of the muscle. In this case, optimal function is obtained by reattaching the lacerated ends.
In most cases, immediate treatment of open fractures and lacerations consists of surgical debridement. Debridement removes nonviable tissue. Generally, care should be taken to remove only tissue that is necrotic. Skin edges should be debrided, as should dead muscle and the surface of any contaminated fat or fascia. Soft-tissue attachments to bone should be maintained whenever possible. Fragments of bone, particularly cortical bone, without attachment, should be removed from the wound. Prior to formal debridement, it is appropriate to splint fractures and cover open wounds with sterile wet dressings. Antibiotic therapy is begun immediately, usually with a cephalosporin bactericidal antibiotic. Tetanus prophylaxis is administered if needed. Antibiotic therapy is continued based on the clinical course.
Although it is acceptable practice to leave any wound open, grade I wounds may be closed completely. Following effective operative debridement, grade II wounds may be treated in a similar fashion, with close initial follow-up. Primary closure of grade III wounds is rarely performed. Patients with massive wounds should be returned to the operating room within 48 hours and then every 48 hours until the wound is completely clean and granulating. Smaller wounds that are left open may be closed safely at 3–5 days.
![]() Flaps and Soft-Tissue Coverage for Open Trauma
Flaps and Soft-Tissue Coverage for Open Trauma
Because of extensive soft-tissue damage involved, type IIIB and IIIC open fractures require aggressive surgical management for wound coverage. These wounds may be treated by regional or free flap reconstruction. With the advent of microsurgical techniques for skin, muscle, and fascia transplantation, the treatment of large soft-tissue trauma has changed, and local rotational flaps, fasciocutaneous flaps, or free tissue transfer can be used successfully. Despite the classic study by Godina favoring immediate free flap reconstruction within the first 48 hours after trauma, controversy still exists for the timing for reconstruction. The requirement for this procedure is radical debridement of the zone of injury, similar to the way one would resect a tumor.
If radical debridement is not performed, then flap reconstruction should be delayed until soft tissues have healed at the margins and there is no sign of infection. The use of free flaps gives an overall improved outcome by bringing a new source of vascularity to a compromised extremity, preventing infection and simultaneously providing soft-tissue coverage.
There are many sites that can be harvested for flaps. The most common and hardiest flaps include fasciocutaneous flaps from the latissimus dorsi, gracilis, serratus anterior, and rectus abdominis muscles. These are suitable for medium- to large-size wounds in a variety of locations. Additionally, there are a host of smaller tissue transfers designed for more specific uses that have advantages in the matching of defect to donor and minimizing problems at the donor site.
A recent innovation in wound management is vacuum-assisted closure (VAC) therapy. The VAC system exposes the wound bed to negative pressure in a closed system. The stretching stimulus is transformed into microchemical forces that promote wound healing through increased cell division and proliferation, angiogenesis stimulation, and local increase of growth factors. Also, edema fluid is removed from the extravascular space, eliminating the extrinsic cause of microcirculatory alteration and improving local blood supply. Although this device does not replace the need for surgical debridement, it may avoid the need for a free tissue transfer in patients with large traumatic wounds. Additional orthopedic indications include the treatment of infected wounds after debridement, war wounds, and fasciotomy closures.
![]() Gunshot Wounds
Gunshot Wounds
Gunshot wounds to the musculoskeletal system result in complex soft-tissue lesions, fractures that are often comminuted, and related nerve, artery, and tendon involvement. A gunshot wound near a major joint should also be suspected of penetrating the joint. Optimum treatment of fractures caused by gunshots relies on an appreciation of the kinetic energy of injury, direction, caliber, and distance. Differences between high-velocity (>2000 ft/s) and low-velocity (<2000 ft/s) weapons and civilian and military settings for these wounds are also important. Additional characteristics are the efficiency of energy transfer, including deformation and fragmentation, kinetic energy, stability, profile of entrance, path through the body, and biologic characteristics of the tissues. In general, kinetic energy associated with an injury is calculated by the formula, E = M/2 × V2, where M equals mass and V equals velocity. Along with the characteristics of the tissue penetrated, velocity and missile mass are the determinants of resultant type and amount of tissue damage. Velocity is more important than mass, doubling the velocity quadruples the kinetic energy. Shotguns are technically low-velocity weapons, but shotgun injuries are different from single gunshot wounds, because the weight of the shot causes an increase in the kinetic energy, resulting in a more severe injury.
In gunshot wounds and high-velocity missiles, shock waves, laceration and crushing, and cavitation result in tissue damage. Shock waves can produce injury in areas that are relatively distant from the direct path of the missile. Cavitation is an important mechanism of tissue damage in high-velocity injuries. The subatmospheric pressure in the cavity sucks contaminants in from both ends. Missile wound tracks close to a major vessel may be associated with occult vascular injury despite normal pulses. Doppler ultrasound is indicated when a vascular injury is suspected. Retained bullet or a fragment in the synovial fluid within a joint can cause lead toxicity.
The majority of low-velocity gunshot wounds can be managed with local wound care and outpatient treatment. The wound should be left open for drainage. If the fracture requires surgical treatment, antibiotic prophylaxis is recommended.
The use of immediate fixation by either internal or external fixator means is controversial. On the one hand, the danger of treatment of these open fractures with foreign material is a deterrent for immediate stabilization. However, in grossly unstable injuries, treatment that would be used for other open fractures appears to be reasonable in selected cases. The use of temporary external fixation as a bridge from the injury to definitive fracture stabilization has become a popular means of initially stabilizing the fracture.
High-velocity and shotgun fractures require surgical irrigation, appropriate debridement, and at least 24–48 hours of intravenous antibiotic treatment. Vascular injuries should be explored and repaired after prompt fracture stabilization. Distal neurologic deficit alone is not an indication for exploration, as it often resolves without surgical intervention and is due to a blast neurapraxia.
![]() Multiple Trauma Patient Scoring Systems
Multiple Trauma Patient Scoring Systems
Several classification systems have been used to try to stratify multiple injured patients and to determine severity of injuries. The classification systems serve as a guide for both patient treatment and eventual outcomes. The Revised Trauma Score (RTS) was developed to help with patient triage. The scores for systolic blood pressure and respiratory rate are separated into five domains with each assigned a point value from 0 to 4. These scores are added to the Glasgow Coma Score (GCS) to yield an RTS. The GCS is the most accepted score for traumatic brain injury. This scale ranges from 3 to 15, with 15 being normal. Evaluation is based on three sections: eye movement, verbal response, and motor response. In the United States, the American College of Surgeons’ guidelines direct patients with a GCS of 11 or less to a designated trauma center.
The Abbreviated Injury Scale (AIS) divides injuries into nine body regions and stratifies the injuries from minor to fatal on a 6-point scale. These scores take into account life-threatening aspects of injuries, anticipated permanent impairment, treatment, and injury pattern.
The Injury Severity Score (ISS) is the sum of the squares of the highest AIS scores in the three most severely injured body regions, which are chosen from head or neck, face, chest, abdomen, extremities or pelvic girdle, and external (skin). Multiple-trauma patients are defined as patients with an ISS greater than or equal to 14. A good prognosis is associated with an ISS of less than 30, whereas an ISS greater than 60 is usually fatal.
Factors at the time of injury that have a bearing on the decision to amputate include status of the opposite leg, the time of limb ischemia, and the age of the patient. Many of these factors have been accounted for by Johansen et al, who have defined a Mangled Extremity Severity Score (MESS). The MESS was previously used as a predictor of eventual amputation; however, recent studies have shown the MESS and other scoring systems to be inaccurate in predicting the functional outcome for mangled limb patients (Table 2–3).
Table 2–3. Factors in evaluation of the mangled extremity severity score (MESS) variables.

Anglen JO: Wound irrigation in musculoskeletal injury. J Am Acad Orthop Surg 2001;9:219. [PMID: 11476531]
Bartlett CS: Ballistic and gunshot wounds: effects on musculo-skeletal tissues. J Am Acad Orthop Surg 2000;8:21. [PMID: 10666650]
Biffl WL, Smith WR, Moore EE, et al: Evolution of a multidisciplinary clinical pathway for the management of unstable patients with pelvic fractures. Ann Surg 2001;233:843. [PMID: 11407336]
Bone LB, McNamara K, Shine B, Border J: Mortality in multiple trauma patients with fractures. J Trauma 1994;37:262. [PMID: 8064927]
Bosse MJ, Mackenzie EJ, Kellam JF, et al: A prospective evaluation of the clinical utility of the lower-extremity injury-severity scores. J Bone Joint Surg Am 2001;83-A:3-14. [PMID: 11205855]
Dickson K, Watson TS, Haddad C, Jenne J, Harris M: Outpatient management of low-velocity gunshot-induced fractures. Orthopedics 2001;24:951. [PMID: 11688773]
Giannoudis PV, Pountos I, Pape HC, Patel JV: Safety and efficacy of vena cava filters in trauma patients. Injury 2007;38:7-18. [PMID:17070525]
Godina M: The tailored latissimus dorsi free flap. Plast Reconstr Surg 1987;80:304. [PMID: 3602183]
Gustilo RB, Anderson JT: Prevention of infection in the treatment of 1025 open fractures of long bones. J Bone Joint Surg Am 1976;58:453. [PMID: 773941]
Hammert WC, Minarchek J, Trzeciak MA: Free-flap reconstruction of traumatic lower extremity wounds. Am J Orthop 2000;29:22. [PMID: 11011776]
Hildebrand F, Giannoudis P, Krettek C, Pape HC: Damage control: extremities. Injury 2004;35:678. [PMID: 15203308]
Johansen K, Daines M, Howey T, et al: Objective criteria accurately predict amputation following lower extremity trauma. J Trauma 1990;30:568. [PMID: 2342140]
Mendelson SA, Dominick TS, Tyler-Kabara E, et al: Early versus late femoral fracture stabilization in multiply injured pediatric patients with closed head injury. J Pediatr Orthop 2001;21:594. [PMID: 11521025]
Mullett H, Al-Abed K, Prasad CV, O’Sullivan M: Outcome of compartment syndrome following intramedullary nailing of tibial diaphyseal fractures. Injury 2001;32:411. [PMID: 11382428]
Pape HC, Tornetta P 3rd, Tarkin I, Tzioupis C, Sabeson V, Olson SA: Timing of fracture fixation in multitrauma patients: the role of early total care and damage control surgery. J Am Acad Orthop Surg2009;17:541-549. [PMID: 19726738]
Parekh AA, Smith WR, Silva S, et al: Treatment of distal femur and proximal tibia fractures with external fixation followed by planned conversion to internal fixation. J Trauma 2008;64: 736-739. [PMID: 18332816]
Perrier A, Howarth N, Didier D, et al: Performance of helical computed tomography in unselected outpatients with suspected pulmonary embolism. Ann Intern Med 2001;135:88. [PMID: 11453707]
Pierce TD, Tomaino MM: Use of the pedicled latissimus muscle flap for upper-extremity reconstruction. J Am Acad Orthop Surg 2000;8:324. [PMID: 11029560]
Schoepf UJ: Diagnosing pulmonary embolism: time to rewrite the textbooks. Int J Cardiovasc Imaging 2005;21:155-163. [PMID: 15915948]
Stannard JP, Riley RS, McClenney MD, et al: Mechanical prophylaxis against deep-vein thrombosis after pelvic and acetabular fractures. J Bone Joint Surg Am 2001;83-A:1047. [PMID: 11451974]
Tuttle MS, Smith WR, Williams AE, et al: Safety and efficacy of damage control external fixation versus early definitive stabilization for femoral shaft fractures in the multiple-injured patient. J Trauma2009;67:602-605. [PMID: 19741407]
Van Belle A, Büller HR, Huisman MV, et al: Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA2006;295:172. [PMID: 16403929]
PRINCIPLES OF OPERATIVE FRACTURE FIXATION
Fractures occur when one or more types of stress, in excess of failure strength, are applied to bones. Fractures may occur from axial loading (tension, compression), bending, torsion (a twisting force), or shearing. The type of failure and mechanism of injury may be helpful in determining fracture treatment. Examples of these are shown in Figure 2–2.

![]() Figure 2–2. Mechanisms of failure of bones.
Figure 2–2. Mechanisms of failure of bones.
![]() Biomaterials Used in Fracture Fixation
Biomaterials Used in Fracture Fixation
Operative fracture fixation requires strength and flexibility of the fixation materials. Metal implants made of stainless steel and titanium offer high stiffness and strength, good ductility, and are biologically well tolerated. Titanium alloy and stainless steel both may be contoured to fit irregularities without compromising stability in bone surfaces at the time of surgery. They provide adequate strength and fatigue resistance to permit fracture healing to occur. The elastic modulus of titanium is half that of stainless steel, resulting in half the flexural rigidity in plates of equal size. The modulus measures the material stiffness and its ability to resist deformation when a force is applied. Ductility is the property of a material that undergoes significant plastic deformation before failure. An example of a ductile material is stainless steel.
![]() Biomechanical Principles of Fracture Fixation
Biomechanical Principles of Fracture Fixation
Fracture healing requires specific sufficient biologic and mechanical conditions. This is provided by blood supply, mediator and hormonal stimuli, and a certain degree of immobilization. By compression of two anatomically reduced fracture fragments, absolute stability can be achieved. Lag screw, compression plate fixation, and tension band techniques are examples of absolute stability. If there is some motion between fracture fragments that is compatible with fracture healing, this is called relative stability and promotes indirect bone healing, resulting in callus. Motion should be below strain level of tissue repair. Intramedullary nails, bridge plates, and external fixators are examples of devices that provide indirect healing.
A. Screws
Screws are the most common and basic form of fixation. They are generally used to function as lag screws, locking or nonlocked plate screws, and positioning screws. They can be used alone or with a plate. The locking head screws have a head with a thread that engages with the reciprocal head of the plate hole. Lag screw technique is a powerful way to compress a fracture plane providing absolute stability. This can be achieved by fully or partially threaded screws. An example of a positioning screw is a screw placed between the tibia and fibula in the presence of a syndesmotic injury.
B. Titanium and Stainless Steel Rods
Regardless of the localization or the type of the fracture, the most important feature in application of an intramedullary nail is the entry point. Current literature supports “gentle” reaming to be superior and safe compared with unreamed technique. One must pay attention to the general condition of a patient especially with the multiply injured patients. Insertion of a femoral nail may exacerbate pulmonary injury in the polytrauma patient with chest injury. Many available nail options for the femur, tibia, and humerus are on the market. Current techniques recommend that all nails be statically locked.
C. Bone Plate
The placement of a plate on a bone has a significant bearing on its function. Optimal placement of a plate is on the tension side of the bone, so that the bone will be placed in compressive loading as a result of muscle action. This stimulates healing and minimizes the stresses on the plate.
The conventional plate and screw system requires substantial bone exposure for access for open reduction and internal fixation. The surgeon-contoured plate is compressed onto the bone with screws resulting in anatomic reduction and absolute stability. The compressive forces acting on the bone–plate interface can compromise the blood supply and hence the healing process. The low contact dynamic compression (LCDC) plate was developed to reduce the bone–plate contact surface area.
Locking plates or internal fixators use a system where the screw head threads into the plate hole, thereby locking the plate just above the bone to minimize contact surface area and compressive forces. The locked screws in the plate also act as a second bone cortex, and therefore self-tapping uni-cortical screws can be used. This achieves relative stability and therefore promotes callus formation at the fracture site. During fixation, the working length of the plate and screws should be kept in mind with the aim of increasing the working length of the plate and reducing the number of screws used in order to facilitate callus.
D. External Fixation
External fixation is an important treatment modality for musculoskeletal injuries. The basic principles are that pins are placed within the musculoskeletal system proximal and distal to the zone of injury. These pins are then placed on an external frame, a frame outside the confines of the bone and soft-tissue envelope, to stabilize fractures. These devices can be useful as temporary treatment for musculoskeletal injuries or as definitive treatment, depending on their location and the type of bone and soft-tissue trauma. In the upper extremity, they play a significant role in treating comminuted distal radius fractures.
For the pelvis, rapidly applied external fixation with compression for pelvic injuries can stabilize the pelvis, reduce blood loss, be of assistance in initial resuscitation, and in some cases provide definitive treatment of such injuries.
For femur and tibia fractures, external fixation may provide excellent and safe initial or provisional stabilization, which can then be converted to intramedullary fixation for definitive care.
External fixators are frequently used as provisional treatment for grade III open fractures with segmental bone loss and large soft-tissue injuries of the upper and lower extremity.
![]() Bone Substitutes Used in Fracture Fixation
Bone Substitutes Used in Fracture Fixation
A. Autogenous Bone Grafting
Autologous bone grafting is the gold standard for management of bone defects and nonunion due to a combination of osteogenic, osteoinductive, and osteoconductive properties. Different types of autologous bone grafts have variable properties associated with structural anatomy. Cancellous grafts are most commonly harvested from the iliac crest. These have a history of success despite variable complication rates. However, with the recently developed reamer-irrigator-aspirator (RIA) system, large quantities of autologous bone graft can be harvested from the femoral and tibial medullary cavities with minimal morbidity.
B. Osteoconductive Graft Substitutes
Hydroxyapatite and tricalcium phosphate are inorganic structural bone graft substitutes that are primarily osteo-conductive. They provide scaffold for new bony growth and do not stimulate bone formation. These materials can be injected into fracture sites, such as the distal radius and calcaneus, to provide stabilization from compressive loads. If they are combined with growth factors (eg, BMPs), they may also show osteoinductive and osteogenic properties.
C. Donor Bone Allografts
Allograft bone grafting, which is the transfer of bone between two genetically dissimilar individuals of same species, is used primarily to support mechanical loads and resist failure at sites where structural support is desired. The greatest concern with using allograft materials is the possibility of viral disease transmission. Several methods may be used to process allograft bone, including low-dose (<20 kGy) irradiation, physical debridement, ultrasonic or pulsatile water washes, ethanol treatment, and antibiotic soaking. Sterilization treatments, such as irradiation and ethylene oxide, are known to compromise these qualities to some extent, with ethylene oxide perhaps being worse than irradiation. Freeze-dried bone is convenient for storage at room temperature but must be sterilized secondarily with ethylene oxide. Because ethylene oxide is unable to penetrate to the depths of large pieces, secondary sterilization of large structural allografts is safer with radiation. The accepted dosage of gamma radiation is 2.5 mrad, but even this dose may not be sufficient to eradicate the human immunodeficiency virus. However, allograft bone usage with the current sterilization technique has been shown to be safe and effective for specific indications.
D. Osteoinductive Agents
BMPs have been identified as important components of musculoskeletal repair for bone and cartilage growth. With recent advances in molecular biology and recombinant DNA techniques, rhBMP-7 and rhBMP-2 have been used in clinical trials. These proteins can potentially be coupled with a collagen matrix and the addition of blood products from the patient to stimulate bone healing. Current usage includes spine fusion, tibial nonunions, and open tibia grafting.
Demineralized bone matrix (DBM) is another osteoinductive agent containing decalcified bone treated to reduce the potential for an immunogenic host reaction and transmission of infection. The resulting product is a biologic scaffold with some remaining growth factors (BMPs). This has the potential to impart a greater osteoconductive effect than standard allograft, as the growth factors have not been exposed by demineralization in the latter.
Belthur MV, Conway JD, Jindal G, et al: Bone graft harvest using a new intramedullary system. Clin Orthop Relat Res 2008;466:2973-2980. [PMID: 18841433]
Centers for Disease Control and Prevention: Update: allograft-associated bacterial infections—United States, 2002. MMWR Morb Mortal Wkly Rep 2002;51:207. [PMID: 11922189]
Cobos JA, Lindsey RW, Gugala Z: The cylindrical titanium mesh cage for treatment of a long bone segmental defect: description of a new technique and report of two cases. J Orthop Trauma 2000;14:54. [PMID: 10630804]
El Maraghy AW, El Maraghy MW, Nousiainen M, et al: Influence of the number of cortices on the stiffness of plate fixation of diaphyseal fractures. J Orthop Trauma 2001;15:186. [PMID: 11265009]
Kurdy NG: Serology of abnormal fracture healing: the role of PIIINP, PICP, and BsALP. J Orthop Trauma 2000;14:48. [PMID: 10630803]
Laurencin C, Khan Y, El-Amin SF: Bone graft substitutes. Expert Rev Med Devices 2006;3:49. [PMID: 16359252]
Radomisli TE, Moore DC, Barrach HJ, et al: Weight-bearing alters the expression of collagen types I and II, BMP 2/4 and osteocalcin in the early stages of distraction osteogenesis. J Orthop Res2001;19:1049. [PMID: 11781004]
Spinella-Jaegle S, Roman-Roman S, Faucheu C, et al: Opposite effects of bone morphogenetic protein-2 and transforming growth factor-beta I on osteoblast differentiation. Bone 2001;29:323. [PMID: 11595614]
Wagner M: General principles for the clinical use of the LCP. Injury 2003;34(Suppl 2):B31-B42. [PMID: 14580984]
Zlotolow DA, Vaccaro AR, Salamon ML, Albert TJ: The role of human bone morphogenetic proteins in spinal fusion. J Am Acad Orthop Surg 2000;8:3. [PMID: 10666648]
![]() I. TRAUMA TO THE UPPER EXTREMITY
I. TRAUMA TO THE UPPER EXTREMITY
SHOULDER AND ARM INJURIES
![]() Anatomy and Biomechanical Principles
Anatomy and Biomechanical Principles
A. Bony Anatomy
1. Humeral shaft— The humeral shaft extends from the level of the insertion of the pectoralis major muscle proximally to the supracondylar ridge distally. The upper portion of the shaft is cylindrical and then becomes more flattened in an anteroposterior direction as it proceeds distally. Medial and lateral intermuscular septae divide the arm into anterior and posterior compartments. In the anterior compartment reside the biceps brachii, coracobrachialis, and brachialis muscles, along with the neurovascular bundle coursing along the medial border of the biceps with the brachial artery and vein and the median, musculocutaneous, and ulnar nerves. In the posterior compartment reside the triceps brachii muscle and the radial nerve. Understanding the insertions of the muscle forces around the humerus helps explain the tendency for fractures to displace in predictable patterns, based on the influence of these muscles (Figure 2–3).

![]() Figure 2–3. A: Muscle insertions on humerus and fracture displacement. B: Neer four-part classification of displaced fractures. (Reproduced, with permission, from Rockwood CA, Green DP, Bucholz RW, et al, eds: Fractures in Adults, 4th ed. Philadelphia: Lippincott; 1996.)
Figure 2–3. A: Muscle insertions on humerus and fracture displacement. B: Neer four-part classification of displaced fractures. (Reproduced, with permission, from Rockwood CA, Green DP, Bucholz RW, et al, eds: Fractures in Adults, 4th ed. Philadelphia: Lippincott; 1996.)
2. Shoulder girdle—The shoulder girdle is a complex arrangement of bony and soft-tissue structures. The glenoid cavity is a shallow socket, approximately one third the size of the humeral head. Stability of the joint depends on capsule, ligament, and muscle. A redundant capsule allows for motion.
3. Proximal humerus—The proximal humerus contains the humeral head, lesser and greater tuberosities, bicipital groove, and proximal humeral shaft. The anatomic neck lies at the junction of the head and the tuberosities. The surgical neck lies below the greater and lesser tuberosities. The major blood supply to the humeral head is through the ascending branch of the anterior humeral circumflex artery, which penetrates the head at the bicipital groove and becomes the arcuate artery. Important structures that lie in the vicinity of the shoulder joint include the brachial plexus and axillary artery, which are anterior to the coracoid process of the scapula and humeral head. Nerves innervating muscles around the shoulder include the axillary, suprascapular, subscapular, and musculocutaneous nerves. Fractures of the anatomic neck have a poor prognosis because of complete disruption of the blood supply to the head. Surgical neck fractures are common, and with these, the blood supply to the head is preserved. Within the bicipital groove lies the biceps tendon, which is covered by the transverse humeral ligament. The greater tuberosity provides attachment for the supraspinatus, infraspinatus, and teres minor muscles. The lesser tuberosity contains the attachment of the subscapularis muscle. The neck-shaft angle measures an average of 135 degrees, and the humeral head is retroverted an average of 30 degrees.
The rotator cuff consists of four muscles: the subscapularis, supraspinatus, infraspinatus, and teres minor muscles. The teres major is not a rotator cuff muscle. The cuff muscles serve as depressors of the humeral head to allow the deltoid to efficiently abduct the humerus. The infraspinatus and teres minor are external rotators, while the subscapularis is an internal rotator of the humerus. Two other important muscles in this region are the deltoid and the pectoralis major muscles. These muscles, along with the rotator cuff, cause predictable displacement of fractures around the proximal humerus. Additionally, injury to the rotator cuff, independent of injuries to the insertion of the tuberosities, may be encountered and need to be considered when evaluating the shoulder.
B. Nerve Supply
Injuries to the nerves around the shoulders occur with fractures and dislocations. The brachial plexus and axillary artery can also be injured with anterior shoulder dislocations.
The most important evaluation consists of a neurovascular examination after injury around the arm and shoulder girdle. The radial nerve is commonly injured in humeral shaft fractures, particularly at the junction of the middle and distal third (Holstein-Lewis fracture). Careful evaluation of radial nerve sensory and motor function is critical. Evaluation should include sensation of the dorsal web space between the thumb and index finger, independent digital extension, and wrist extension.
Around the shoulder girdle, fractures of the proximal humerus and fracture-dislocations can on occasion result in axillary nerve and artery injuries. An axillary nerve injury from proximal humeral fracture or fracture-dislocation would result in paralysis of the deltoid muscle and anesthesia over the “badge” region at the lateral proximal arm.
FRACTURES AND DISLOCATIONS AROUND THE SHOULDER
• The second most common fractures of the upper extremity.
• Incidence sharply increases in the elderly.
• Eighty-five percent of fractures can be treated nonoperatively.
![]() Classification
Classification
An extension of Codman’s observations, Neer introduced the concept of “parts” based on the epiphyseal growth centers that collectively compose the proximal humerus. Displaced parts then include the anatomic neck, surgical neck, or tuberosities. Segments are considered to be displaced if they are separated by more than 1 cm or angled more than 45 degrees from the normal anatomic position. Other categories include fracture-dislocations and head-splitting injuries. The relationship of the humeral head to the displaced parts in the glenoid, as well as the blood supply, is also taken into consideration.
![]() Clinical Findings
Clinical Findings
Young people sustain these injuries in high-energy accidents, whereas fractures in older patients are usually from lower energy mechanisms. Clinical presentation is usually with pain, swelling, and ecchymosis.
Radiographic evaluation is a cornerstone for diagnosis and planning of treatment. The recommended series of radiographs is the so-called Neer trauma series, which consists of (1) an AP view, (2) a lateral view in the scapular plane, and (3) a Velpeau modified axillary view. The lateral radiograph in the scapular plane is the tangential Y-view of the scapula. The combination of three of these views allows evaluation of the shoulder joint in three separate perpendicular planes. The axillary view is important for evaluating the glenoid articular surface and the relationship of the humeral head anteriorly and posteriorly. On occasion, other studies, including CT scanning for detailing bony anatomy, may be necessary.
Rotator cuff injuries can be expected with fractures of the tuberosities, but can also result from strictly soft-tissue injuries such as shoulder dislocations. Evaluation of the integrity of the rotator cuff may be difficult in the acute setting. Ultrasound, MRI, arthrogram, or arthroscopy may be valuable in making this diagnosis.
Axillary artery injuries, although uncommon, generally result from fractures or fracture-dislocations in which a medial bone spike injures or penetrates the axillary artery. The index of suspicion is high if the arm shows significant color differences compared with the uninjured arm. Pulses should be palpated and evaluated by Doppler studies. In late diagnosis, the outcome is determined by the neurologic morbidity, even though the results of acute vascular reconstruction are good.
![]() Treatment
Treatment
A. Closed Treatment
Approximately 85% of proximal humerus fractures are minimally displaced or nondisplaced and can be treated nonoperatively with a sling for comfort and early motion exercises. The mainstay of closed treatment is initial immobilization and then early motion. Physical therapy or physician-directed exercises are essential and should be started at 7–10 days if possible. Monitoring of the exercises is important to prevent a program that is either too conservative (thus causing unnecessary contractures) or too aggressive (leading to displacement, with excessive pain and swelling).
B. Surgical Treatment
Techniques useful for the smaller percentage of fractures include closed reduction and percutaneous pinning, intramedullary nails, tension band, open reduction and internal fixation (ORIF) with either conventional plates or locking plates, and hemiarthroplasty. Locking plates provide angular stability and a favorable bone–implant interface for comminuted and osteoporotic fractures.
Hemiarthroplasty remains a useful option for older patients with anatomic neck and head-splitting fractures. Good bone quality and simple fracture patterns are essential to make use of the minimal soft-tissue dissection in the closed reduction and percutaneous pinning method. In younger patients, ORIF may be possible even in comminuted fractures.
The age of the patient, quality of the bone, fracture pattern, and amount of comminution are all important considerations in developing a treatment plan.
C. Two-Part Anatomic Neck Fractures (ICD-9:812.01)
Two-part anatomic neck fractures are rare. No single optimal method of management has been established. Closed reduction is difficult because controlling the articular fragment, which is usually rotated and angulated within the joint capsule, is difficult. The fragment can be preserved in a young patient (<40 years old) with ORIF with pins or interfragmentary screws. It may be difficult to obtain adequate screw purchase without violating the articular surface. Additionally, the prognosis for head survival is poor because the blood supply is usually completely disrupted. In general, prosthetic hemiarthroplasty provides the most predictable result in the elderly (>75 years old).
D. Two-Part Greater Tuberosity Fractures (ICD-9:812.03)
Greater tuberosity fractures generally displace posteriorly and superiorly because of traction by the supraspinatus muscle. This is often associated with anterior glenohumeral dislocation. It is appropriate to attempt closed reduction, which may result in an acceptable position for the greater tuberosity. Neer has reported that displacement of the fragment by more than 1 cm is pathognomonic of a rotator cuff defect. The result of fracture healing in this position is subacromial impingement, with limitation of forward elevation and external rotation. In one series, ORIF is recommended if displacement is greater than 5 mm with some references recommending ORIF with greater than 3 mm displacement in the high-performance athlete because impingement symptoms may develop. A variety of methods, including screws, pins, wires, and suture, can be used to repair the greater tuberosity. Treatment of this condition should be directed at rotator cuff repair as well as bony reconstruction. Percutaneous pinning tends to be inadequate for preventing redisplacement of greater tuberosity fractures.
E. Two-Part Lesser Tuberosity Fractures (ICD-812.00)
If the displaced fragment (usually medially by subscapularis) is small, closed reduction of this rare injury is satisfactory. This fracture may be associated with posterior dislocation and may be treated by closed reduction in the acute setting. The position of immobilization in this case would be either neutral or slight external rotation. Larger fragments may require internal fixation.
F. Two-Part Surgical Neck Fractures (ICD-9:812.01)
In these conditions, both tuberosities remain attached to the head, and the rotator cuff in general remains intact. The diaphysis is often displaced anteromedially by the pull of the pectoralis major muscle. Reduction may be blocked by interposition of the periosteum, biceps tendon, or deltoid muscle, or by buttonholing of the shaft in the deltoid, pectoralis major, or fascial elements. One attempt at closed reduction is advisable; if this fails, operative intervention is recommended. If, on the other hand, the reduction is successful, percutaneous pinning under fluoroscopic control may be an excellent choice for the reducible but unstable fracture (Figure 2–4). If open reduction is required to remove displaced soft tissues, internal fixation can be accomplished by means of percutaneous pinning or intramedullary fixation in conjunction with a tension band wiring technique. In the osteoporotic patient, wire or suture material for tension banding can be passed through the soft tissues and the rotator cuff, which may be superior to bone for fixation.

![]() Figure 2–4. Pinning of the unstable surgical neck fracture. AP, anteroposterior. (Reproduced, with permission, from Fu FH, Smith WR, eds: Percutaneous pinning of proximal humerus fractures. Oper Tech Orthop 2001;11:235.)
Figure 2–4. Pinning of the unstable surgical neck fracture. AP, anteroposterior. (Reproduced, with permission, from Fu FH, Smith WR, eds: Percutaneous pinning of proximal humerus fractures. Oper Tech Orthop 2001;11:235.)
Another technique for internal fixation uses intramedullary devices such as Enders nails or Rush rods, which can be inserted through a limited deltoid-splitting incision; however, the control of rotational alignment is poor. For elderly (>75 years old) or debilitated patients, this may be the best solution to achieve overall alignment with minimal surgical morbidity.
G. Three-Part and Four-Part Fractures (ICD-9:812.00)
Optimal treatment of three- and four-part fractures of the proximal part of the humerus in patients with poor bone quality is controversial. ORIF of these fractures has generally produced unsatisfactorily high rates of complications such as avascular necrosis and malunion. Avascular necrosis in three-part fractures has been reported to be as high as 27%. The Atlas Orthogonal (AO) buttress plate has had significant complications, including a high rate of avascular necrosis related in part to extension of soft-tissue displacement and dissection, superior placement of the plate with secondary impingement, loss of plate and screw fixation, malunion, and infections. Recent studies with locking plates show improved fracture stability and healing. Screws, which lock into the plate, may decrease pullout in osteoporotic fractures. In the less active or elderly (>75 years old) patient, the accepted method of treatment is hemiarthroplasty, particularly because the avascular necrosis rate may be as high as 90% and the bone is usually osteoporotic. Appropriate prosthesis level and humeral retroversion, as well as the attachment of greater and lesser tuberosities, are critical in achieving a good result. Repair of any rotator cuff defects is necessary to prevent proximal migration of the humeral component as well as loss of rotator cuff power. With postoperative rehabilitation, generally good pain relief can be expected; however, function is usually limited.
H. Fracture-Dislocations
Fracture-dislocations require reduction of the humeral head, and their management is generally based on the fracture pattern. These injuries usually produce impression defects or head-splitting fractures, with concomitant posterior dislocation. Management is determined by the size of the impression defect and the time of persistent locked dislocation. Fractures of less than 20% will generally be stable with closed reduction and can be treated with immobilization in external rotation for 6 weeks to restore long-term stability. If the defect is 20–50%, however, transfer of the lesser tuber-osity with the subscapularis tendon into the defect by open means is indicated. With impression fractures of greater than 50% or chronic dislocations, hemiarthroplasty may be the best treatment. If concomitant glenoid destruction is present, total shoulder arthroplasty may be required.
Eberson CP, Ng T, Green A: Contralateral intrathoracic displacement of the humeral head. J Bone Joint Surg Am 2000;82-A:105. [PMID: 10653090]
Helmy N, Hintermann B: New trends in the treatment of proximal humerus fractures. Clin Orthop Relat Res 2006;442:100. [PMID: 16394747]
Hintermann B, Trouillier HH, Schafer D: Rigid internal fixation of fractures of the proximal humerus in older patients. J Bone Joint Surg Br 2000;82-B:1107. [PMID: 11132267]
Naranja RJ, Iannotti JP: Displaced three- and four-part proximal humerus fractures: evaluation and management. J Am Acad Orthop Surg 2000;8:373. [PMID: 11104401]
Palvanen M, Kannus P, Niemi S, Parkkari J: Update on the epidemiology of proximal humerus fractures. Clin Orthop Relat Res 2006;442:87. [PMID: 16394745]
Ruch DS, Glisson RR, Marr AW, et al: Fixation of three-part proximal humeral fractures: a biomechanical evaluation. J Orthop Trauma 2000;14:36. [PMID: 10630801]
Steinmann SP, Moran EA: Axillary nerve injury: diagnosis and treatment. J Am Acad Orthop Surg 2001;9:328. [PMID: 11575912]
Thanasas C, Kontakis G, Angoules A, Limb D, Giannoudis P: Treatment of proximal humerus fractures with locking plates: a systematic review. J Shoulder Elbow Surg 2009;18:837-844. [PMID: 19748802]
HUMERAL SHAFT FRACTURE (ICD-9:812.21)
• Account for 3–5% of all fractures.
• More than 90% can be managed nonsurgically.
• Traumatic and/or iatrogenic radial nerve injury is common.
Fractures of the shaft of the humerus usually result from a direct blow, a fall, an automobile injury, or a crushing injury. Missiles from firearms or shell fragments may pierce the arm and cause an open fracture. Other indirect means of injury, such as a fall on an outstretched upper extremity or violent muscle contracture, can cause midshaft fractures.
![]() Classification
Classification
Fractures are classified according to whether they are open or closed and according to the level of the fracture in relation to the insertions of the pectoralis major and deltoid muscles. Characteristics of fracture and associated injury are also factors.
![]() Clinical Findings
Clinical Findings
Clinical signs and symptoms include a shortened extremity with crepitus and pain at the diaphysis of the humerus. Confirmation should be obtained by radiographs in two planes. Both the shoulder and elbow joints should be thoroughly evaluated, clinically and radiographically, as should the neurovascular status.
![]() Treatment
Treatment
A. Closed Treatment
The majority of these fractures do well with nonoperative methods with high union rates. Nonoperative methods include traction by hanging casts, functional bracing, Velpau dressings, and skeletal traction. Cast bracing appears to be the most effective closed treatment.
The musculature of the upper arm will accommodate 20 degrees of anterior angulation, 30 degrees of varus angulation, and 3 cm of shortening without apparent deformity and functional loss.
1. Hanging cast—Treatment with a hanging cast involves placement of the arm in a cast and correcting the fracture by the weight of cast. This treatment requires weekly radiographic evaluations. Patients with a large body habitus may develop more significant angulation at the time of healing with this technique, compared with slimmer patients. The vertical position must be maintained even at night. Spiral, comminuted, and oblique fractures have additional advantages of large fracture surfaces for ready healing. Transverse fractures may have more difficulty in healing. One risk of this treatment is distraction of the fracture site and eventual nonunion.
2. Coaptation splint—A TU-shaped coaptation splint with cuff and collar is another method for initial treatment of humerus fractures. It gives greater stabilization but less distraction than a hanging arm cast, so it is indicated for minimally shortened fractures and short oblique or transverse fractures that may displace in hanging cast.
3. Functional bracing—Functional cast braces are typically applied 2 weeks after the injury following the initial treatment with a hanging cast or a coaptation splint. During this period, swelling has subsided. The sleeve is ready-made or custom-made from thermoplastic splinting materials and fixed with Velcro straps that can be adjusted to achieve the appropriate level of compression. A collar and cuff may be used to support the forearm, but sling application may result in varus angulation. Repeat graphs are checked, and healing is expected in 8–12 weeks.
4. External fixation—External fixation is applicable to the humerus in the case of burns, gunshot wounds, or severe comminuted open injuries with defects of skin, bone, or soft tissue. Other indications may include osteitis and infected nonunion. Complications include pin tract infections, nonunion, and neurovascular injury.
B. Open Treatment
Special circumstances may merit ORIF. Selected segmental fractures, inadequate closed reduction, “floating” elbow, bilateral humeral fractures, open fractures, multiple trauma, pathologic fractures, and trauma with associated vascular injuries requiring exploration may benefit from internal fixation. Recent advances in internal fixation techniques and instrumentation have led to an expansion of surgical indications for such fractures. There are three general forms of internal fixation: (1) compression plate and screw fixation using the AO techniques, with posterior, modified lateral, and anterolateral surgical approaches; (2) intramedullary nailing, which is especially useful in osteopenic bone, segmental, and pathologic fractures; and (3) percutaneous humeral bridge plating with minimal incision as described by Livani and Belangero. In multiply injured patients, humeral stabilization, permitting mobilization, pulmonary toilet, and pain control may be beneficial. The incidence of radial nerve palsy with acute fracture is about 16%; however, current literature does not recommend operative fixation and nerve exploration in these injuries.
Blum J, Janzing H, Gahr R, et al: Clinical performance of a new medullary humeral nail: antegrade versus retrograde insertion. J Orthop Trauma 2001;15:342. [PMID:11433139]
Chapman JR, Henley MB, Agel J, et al: Randomized prospective study of humeral shaft fracture fixation: intramedullary nails versus plates. J Orthop Trauma 2000;14:162. [PMID: 10791665]
Cox MA, Dolan M, Synnott K, et al: Closed interlocking nailing of humeral shaft fractures with the Russell-Taylor nail. J Orthop Trauma 2000;14:349. [PMID: 10926243]
Livani B, Belangero WD: Bridging plate osteosynthesis of humeral shaft fractures. Injury 2004;35:587. [PMID: 15135278]
McCormack RG, Brien D, Buckley R, et al: Fixation of fractures of the shaft of the humerus by dynamic compression plate or intramedullary nail. J Bone Joint Surg Br 2000;82-B:336. [PMID: 10813165]
Orthoteers. Available at: http://www.orthoteers.co.uk/Nrujpbbij33lm/Orthcrps.htm
Pickering RM, Crenshaw AH Jr, Zinar DM: Intramedullary nailing of humeral shaft fractures. Instr Course Lect 2002;51:271. [PMID: 12064112]
Sarmiento A, Zagorski JB, Zych GA, et al: Functional bracing for the treatment of fractures of the humeral diaphysis. J Bone Joint Surg Am 2000;82:478. [PMID: 10761938]
Strothman D, Templeman DC, Varecka T, et al: Retrograde nailing of humeral shaft fractures: a biomechanical study of its effects on the strength of the distal humerus. J Orthop Trauma 2000;14:101. [PMID: 10716380]
Ziran BH, Belangero W, Livani B, Pesantez R: Percutaneous plating of the humerus with locked plating: technique and case report. J Trauma 2007;63:205. [PMID: 17622893]
INJURIES AROUND THE ELBOW
• Intercondylar fractures are the most common fracture pattern.
• CT scan with three-dimensional reconstruction is helpful for preoperative planning.
• ORIF is the choice of treatment in the majority of cases.
![]() Anatomy and Biomechanical Principles
Anatomy and Biomechanical Principles
On cross-section, the humerus is circular at the mid-shaft but flared and flattened at the distal end. The distal humerus consists of an arch formed by two condyles. Articular surface of the condyles: capitellum, on the lateral, and trochlea medial to it, articulates with radial head and proximal ulna, respectively. The ulnohumeral joint allows the flexion extension of the joint, and the radiocapitellar joint allows forearm rotation. The proximal ulna, which articulates with the trochlea, contains the olecranon process posteriorly, the coronoid process anteriorly, and the sigmoid or semilunar notch. The trochlea has a 300-degree arc of cartilage. The medial column diverges from the humeral shaft at a 45-degree angle, and the lateral column diverges at a 20-degree angle.
The triceps has a broad tendinous insertion into the olecranon posteriorly; anteriorly, the brachialis inserts on the coronoid process and the tuberosity of the ulna. The radial head lines up in its lesser sigmoid, or radial notch, with the annular ligament surrounding it. Medial to the trochlea, the medial epicondyle locates and the medial collateral ligament and flexor-pronator group of muscles attach here. The most important portion of the medial or ulnar collateral ligament is the anterior portion, which attaches to a small process on the medial surface of the coronoid. The supinator-extensor muscle group attaches to the lateral epicondyle, which is slightly proximal and lateral to the capitellum.
With the elbow in 90 degrees of flexion, the medial condyle, lateral condyle, and olecranon form a palpable triangle. These boney landmarks are important when assessing the elbow for fractures, dislocations, or effusions. Effusions can be discerned by swelling between the lateral epicondyle and the olecranon.
The ulnar nerve passes through the cubital tunnel at the medial column of the elbow and must be appropriately assessed following injury. The ulnar nerve enters the anterior forearm by traveling between the two heads of the flexor carpi ulnaris.
A complete neurovascular examination of the radial, median, ulnar, and anterior and posterior interosseous nerves should be done before and after treatment.
DISTAL HUMERUS FRACTURES
• Account for 30% of elbow fractures.
• Treatment similar to other intraarticular fractures.
1. Intercondylar-T or -Y Fractures (ICD-9:812.49)
Intercondylar humerus fractures are among the most challenging fractures treated by the orthopedic surgeon. The usual mechanism of injury is axial loading of the ulna in the trochlear groove. Studies have demonstrated increasing numbers of these injuries in the older (>60 years) population. It is critical to assess the integrity of the medial and lateral column for reconstructible bone fragments and the degree of comminution.
![]() Classification
Classification
Jupiter and Mehne classified distal humerus fractures into intraarticular and extraarticular patterns. Intraarticular fractures are divided into the following types:
1. Single column: Divided into medial or lateral
2. Bicolumnar: Divided into TT, TY, TH, lambda, or multiplane pattern
3. Capitellum fractures
4. Trochlea fractures
Extraarticular fractures are classified into intracapsular and extracapsular (Table 2–4).
Table 2–4. The Jupiter and Mehne classification of distal humerus fractures.

![]() Treatment
Treatment
Treatment options include bracing, ORIF, total elbow arthroplasty (TEA), elbow arthrodesis, and distal humerus replacement. It is difficult to achieve and maintain the fracture reduction by casting, and prolonged immobilization leads to stiffness and ankylosis of the adult elbow joint. Nonsurgical management of distal humerus fractures is mainly reserved for medically unstable older patients, those with limited arm function (eg, paralysis), and some nondisplaced fractures.
With modern hardware and techniques, ORIF is preferred for most fractures. Surgical exposure is through a transolecranon approach (ie, either transverse osteotomy or chevron osteotomy). Triceps-sparing and triceps-splitting posterior approaches have also been shown to be effective.
The intraarticular fracture fragments should be anatomically restored with lag screw fixation of periarticular fragments and stable attachment of the metaphysis to the diaphysis with small fragment contoured plates. When possible, dual plate fixation should be used.
2. Fracture of the Humeral Condyles
Both medial and lateral condyles can be disrupted. These fractures can correspond with the ossification centers of the distal humerus.
![]() Lateral Condylar Fracture (ICD-9:812.42)
Lateral Condylar Fracture (ICD-9:812.42)
Lateral column fractures are single-column injuries and are divided into “low” and “high.” Low fractures have the lateral wall of the trochlea attached to the main mass of the humerus and are generally stable, whereas high fractures involve a majority of the trochlea and are unstable. “Low” and “high” correspond to Milch type I and II injuries, respectively. Stable internal fixation with early range of motion is generally recommended for displaced fractures.
![]() Medial Condylar Fracture (ICD-9: 812.43)
Medial Condylar Fracture (ICD-9: 812.43)
Medial condyle fractures are similarly single-column injuries with low fractures (Milch type I) involving a portion of the trochlea, with preservation of the trochlear ridge, and are generally stable. In high medial condyle fractures (Milch type II), the lateral trochlear ridge is included with the fracture portion.
Both fractures, if displaced, should be treated with ORIF and early range of motion.
3. Fracture of the Epicondyles (ICD-9:812.43)
Although lateral epicondylar fractures are rare, medial epicondylar fractures are fairly common, especially among children or adolescents. They commonly present as avulsion fractures. Treatment depends on the amount of displacement. If displacement is minimal, then closed reduction is appropriate. A displaced fracture may require percutaneous pinning or open reduction. Elbow instability is not generally a problem; however, irritation of the ulnar nerve can result. Early motion seems to be important for restoration and ultimate function. If a displaced fracture results in ulnar symptoms or is itself symptomatic, the fragment can be excised at a later date.
ELBOW DISLOCATION
• Posterior dislocation is the most common.
• Simple dislocations are those without fracture.
Dislocations of the elbow occur when loads are placed on the structures about the elbow that exceed the intrinsic stability provided by the anatomic shape of the joint surfaces and soft-tissue constraints. These are potentially limb-threatening, as vascular compromise is a possible sequela. Expeditious reduction of the elbow joint is the goal of treatment.
Elbow dislocations are characterized according to direction of the distal bone. Isolated radial head dislocation is rare; it is usually accompanied by an ulnar fracture (Monteggia fracture). When combinations of dislocations with concomitant fractures occur, treatment of the combined injury is usually dictated by the treated fracture. Adequate fracture care will usually cause secondary reduction of the dislocation.
![]() Posterior Elbow Dislocations (ICD-9:832.02)
Posterior Elbow Dislocations (ICD-9:832.02)
Posterior dislocations are the most common type (80%) of elbow dislocations, resulting from an axial force applied to the extended elbow. Both collateral ligaments are disrupted, whether the dislocation is posteromedial or posterolateral.
Diagnosis is made by clinical examination and verified by radiograph to rule out associated fractures. The extremity is typically shortened and the elbow held slightly flexed.
Treatment is initiated after documenting the neurovascular examination. Anesthesia, either injected locally into the joint or administered intravenously, is necessary. Traction on the extremity with correction of the medial or lateral displacement usually produces reduction with a “clunk.” The elbow is put through a range of motion to ensure that reduction has been obtained and that there is no soft-tissue or bony mechanical blockage to motion. The elbow is generally splinted in flexion and pronation to maintain stability. Postreduction radiographs are necessary to rule out occult fracture.
![]() Anterior Elbow Dislocations (ICD-9:832.01)
Anterior Elbow Dislocations (ICD-9:832.01)
Anterior dislocations are relatively rare. Soft-tissue damage is typically severe. Treatment is similar to that for posterior dislocations, except that the method of reduction is reversed.
![]() Medial and Lateral Elbow Dislocations (ICD-9:832.03 and 832.04)
Medial and Lateral Elbow Dislocations (ICD-9:832.03 and 832.04)
The radius and ulna may be displaced medially or laterally. Some semblance of joint motion may be present with lateral dislocations, as the ulna may be displaced into the groove between the trochlea and the capitellum. The anteroposterior radiograph is diagnostic. Medial or lateral force is used, after attempting to distract the joint surfaces, to reduce these dislocations.
![]() Isolated Ulnar Dislocations
Isolated Ulnar Dislocations
Isolated ulnar dislocations occur when the humerus pivots around the radial head, causing the coronoid process to be displaced posterior to the humerus or the olecranon anterior to the humerus. The more common injury is posterior dislocation, which causes cubitus varus deformity of the forearm. Traction in extension and supination reduces the ulna.
![]() General Treatment Procedures
General Treatment Procedures
A. Early Treatment
The elbow is tested for stability to varus and valgus stress and to pronation and supination. Stable dislocations are splinted for comfort at 90 degrees of flexion, and motion is instituted as soon as possible, generally within a few days. Maintenance of reduction is necessary, and radiographs should be taken periodically if any doubt exists. Immobilization does not guarantee maintenance of reduction. Unstable reductions are rare. Immobilization for longer periods may be necessary in these cases, as a stiff but stable elbow is preferable to an unstable elbow. The lateral ulnar collateral ligament injury is the cause of recurrent instability.
Uncomplicated elbow dislocations have a favorable long-term prognosis. A loss of extension of 5–10 degrees compared with the contralateral elbow can be expected following this injury. Posterolateral dislocation has been associated with persistent valgus instability in some patients, which is associated with a worse overall clinical result.
B. Delayed Treatment
Late reduction of elbow dislocations can be accomplished with closed techniques for up to several weeks from the time of injury. Dislocations left untreated for longer periods generally require open reduction techniques. Better function with less flexion contracture after open reduction of posterior dislocations is obtained by lengthening the triceps tendon.
C. Elbow Dislocation and Coronoid Fracture (ICD-9:813.12 for coronoid fracture)
An elbow dislocation and associated fracture of the coronoid process increase the risk of recurrent and chronic instability. The size of the coronoid fragment varies from a small marginal fragment (Reagan-Morrey type I) to a larger fragment (Reagan-Morrey type II), or includes the insertion of the anterior bundle of the medial collateral ligament (Reagan-Morrey type III). The decision to fix a coronoid fracture should be made based on elbow stability. Even small rim fractures may require surgical fixation if instability is present after repair of associated fractures. When there is greater than 50% loss of coronoid, fixation is mandatory according to the cadaver studies. Interfragmentary screws can be used to fix a large fragment. Otherwise, a pullout technique can be used.
D. Elbow Dislocation With Radial Head and Coronoid Fractures
Denominated the terrible triad of the elbow, these injuries are difficult to treat, and the reported results have been poor. The most common problems after these lesions are recurrent and chronic instability, stiffness, posttraumatic arthrosis, and pain. Appropriate treatment should include ORIF of the coronoid fracture and/or repair of the anterior capsule, ORIF or replacement of the radial head, and repair of the lateral ligament complex. Residual instability after treatment represents an indication for medial collateral ligament repair and/or application of a hinged external fixator.
Bailey CS, MacDermid J, Patterson SD, et al: Outcome of plate fixation of olecranon fractures. J Orthop Trauma 2001;15:542. [PMID: 11733669]
Eygendaal D, Verdegaal SH, Obermann WR, et al: Posterolateral dislocation of the elbow joint. J Bone Joint Surg Am 2000; 82-A:555. [PMID: 10761945]
Hak DJ, Golladay GJ: Olecranon fractures: treatment options. J Am Acad Orthop Surg 2000;8:266. [PMID: 10951115]
Mckee MD, Wilson T, Winston L, et al: Functional outcome following surgical treatment of intraarticular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82-A:1701. [PMID: 11130643]
Paramasivan ON, Younge DA, Pant R: Treatment of nonunion around the olecranon fossa of the humerus by intramedullary locked nailing. J Bone Joint Surg Br 2000;82-B:332. [PMID: 10813164]
Popovic N, Rodriguez A, Lemaire R: Fracture of the radial head with associated elbow dislocation: results of treatment using a floating radial head prosthesis. J Orthop Trauma 2000;14:171. [PMID: 10791667]
Pugh DMW, Wild LM, Schemitsch EH, et al: Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. J Bone Joint Surg Am 2004;86:1122. [PMID: 15173283]
Sanchez-Sotelo J, Romanillos O, Garay EG: Results of acute excision of the radial head in elbow radial head fracture-dislocations. J Orthop Trauma 2000;14:354. [PMID: 10926244]
Schneeberger AG, Sadowski MM, Jacob HA: Coronoid process and radial head as posterolateral rotatory stabilizers of the elbow. J Bone Joint Surg Am 2004;86-A:975. [PMID: 15118040]
Wainwright AM, Williams JR, Carr AJ: Interobserver and intraobserver variation in classification systems for fractures of the distal humerus. J Bone Joint Surg Br 2000;82-B:636. [PMID: 10963156]
FRACTURE OF THE RADIAL HEAD (ICD-9:813.05)
• Accounts for 15–25% of all elbow fractures.
• The radial head is the secondary restraint to valgus stability of elbow.
• Associated injuries are common.
The radial head is seated in the lesser sigmoid notch and has contact axially with the capitellum of the distal humerus. Radial head fractures are generally caused by longitudinal loading from a fall on an outstretched hand; dislocation of the elbow is another cause.
![]() Clinical Findings
Clinical Findings
One generally describes these fractures based on their location, percentage of articular involvement, and amount of displacement. Radiographs in the anteroposterior and lateral projections show the injury. The fat pad sign is usually present on the lateral projection (Figure 2–5).

![]() Figure 2–5. Positive fat pad sign on lateral radiograph of elbow. This finding indicates that fluid is in the elbow joint. In the acute setting, the fluid is blood, most commonly from a fracture.
Figure 2–5. Positive fat pad sign on lateral radiograph of elbow. This finding indicates that fluid is in the elbow joint. In the acute setting, the fluid is blood, most commonly from a fracture.
![]() Classification
Classification
Mason proposed a classification scheme for radial head fractures: Type I is a nondisplaced fracture; type II is a fracture that is displaced, usually involving a single large fragment; type III is a comminuted fracture; and type IV is a fracture associated with an elbow dislocation (Figure 2–6).

![]() Figure 2–6. Mason classification of radial head fractures. (Reproduced, with permission, from Browner BD, Levine A, Jupiter J, et al, eds: Skeletal Trauma, 2nd ed. New York: WB Saunders; 1998.)
Figure 2–6. Mason classification of radial head fractures. (Reproduced, with permission, from Browner BD, Levine A, Jupiter J, et al, eds: Skeletal Trauma, 2nd ed. New York: WB Saunders; 1998.)
![]() Treatment
Treatment
For type I fractures, nonoperative treatment with early motion can generally produce a good outcome.
The treatment of type II fractures is controversial. For fractures with near-normal motion, less than 2 mm step-off, and without associated injury, nonsurgical treatment is indicated.
Type II fractures with associated injuries that may compromise elbow stability or fractures with a mechanical block to full motion after injection of anesthetic into the elbow joint are indications for ORIF. ORIF can be performed with pins, articular screws, or Herbert screws. Implants should be placed into the nonarticular safe zone to avoid impingement on the sigmoid fossa of the ulna. The safe zone corresponds to the lateral 100-degree arc with the forearm in neutral rotation.
The result of ORIF is less predictable when there is more than one fragment in type II fractures, and limitation of forearm rotation not attributable to implant prominence can be expected.
Early excision with immediate motion is recommended for type III fractures with no associated elbow instability, coronoid fracture, wrist pain, or distal radioulnar joint injury. If any of these conditions exist, then current literature recommends placement of a metallic radial head prosthesis. Replacement of the radial head becomes most important when there is evidence of the Essex-Lopresti injury (longitudinal disruption of interosseous membrane, distal radioulnar joint injury, and radial head fracture/dislocation). Some suggest that replacement of the radial head should be considered in healthy, active patients even if the elbow and forearm are stable. Antuna et al showed that radial head resection in young patients with isolated fractures without instability yields satisfactory results in greater than 90% of cases after 15 years of follow-up. Broberg and Morrey noticed a 92% incidence of arthrosis 10 years after fracture-dislocation treatment without repair or replacement of the radial head.
1. Capitellar Fractures (ICD-9:812.44)
Capitellar fractures frequently accompany and result from the same mechanism that causes radial head fractures. The medial collateral ligament, the interosseous ligament, and the distal radioulnar joint may also be injured. Various levels of injury, from cartilage damage to large osteochondral portions of the capitellum, can occur from impaction of the radius against the capitellum. Low-grade radial head fractures create higher-grade cartilage lesions as the intact radial head can cause more damage to the capitellum. Shearing forces can result in more significant injuries: an osteochondral injury or complete fracture (type 1 or Hahn-Steinthal), an articular-cartilage-only injury (type 2 or Kocher-Lorenz), a comminuted fracture (type 3), or a fracture line extending into the trochlea (Hahn-Steinthal II). CT reconstructions are useful to further delineate the fracture and for surgical planning. Osteochondral pieces can be overlooked or confused with bone chips from radial head fractures.
![]() Treatment
Treatment
Today, anatomic reduction and early motion compose the standard treatment for these injuries, whether obtained by open or closed means. Open reduction is performed through a lateral approach between the anconeus and extensor carpi ulnaris.
OLECRANON FRACTURES (ICD-9:813.01)
• Tension band is the gold standard treatment for transverse fractures.
• Hardware-related problems are common.
Olecranon fractures compose approximately 10% of all fractures around the elbow. Fractures of the olecranon commonly occur with a direct blow, generally resulting in comminuted fractures, or as an avulsion injury with triceps contracture. Contraction of the triceps often results in transverse or short oblique types of fractures.
![]() Clinical Findings
Clinical Findings
Radiographic evaluation consists of a true lateral radiograph of the elbow, and classifications or descriptions generally analyze the fracture based on the percentage of articular surface involved in the fractured proximal fragment. This factor, the amount of comminution, the fracture angle, intraarticular step-off, the degree of displacement, and patient comorbidities and functional demands are all critical in evaluating the injury and selecting the appropriate treatment.
![]() Treatment
Treatment
Methods of treatment vary from closed treatment to ORIF. Nondisplaced fractures or fractures with less than 2 mm displacement and an intact extensor mechanism should be immobilized in a long arm cast with the elbow in 90 degrees of flexion.
Displaced transverse or short oblique fractures generally are best treated with ORIF. The optimal method for treating this fracture is tension banding with two longitudinal K-wires placed across the fracture site and stabilized with a figure-of-8 wire loop (Figure 2–7). More oblique fractures can be treated with interfragmentary screws with a neutralization plate. Wire protrusion and pain frequently result and may necessitate removal of the hardware.

![]() Figure 2–7. Tension band technique for fixation of olecranon fractures. (Reproduced, with permission, from Browner BD, Levine A, Jupiter J, et al, eds: Skeletal Trauma, 2nd ed. New York: WB Saunders; 1998.)
Figure 2–7. Tension band technique for fixation of olecranon fractures. (Reproduced, with permission, from Browner BD, Levine A, Jupiter J, et al, eds: Skeletal Trauma, 2nd ed. New York: WB Saunders; 1998.)
For the significantly comminuted fractures, or oblique fractures distal to the midpoint of the trochlear notch, a low-profile, limited contact compression plate can be applied to the dorsal surface of the ulna. Selected comminuted fractures may be treated by selective bony excision or complete excision of the fragment followed by reattachment of the triceps. All these treatments generally can be accompanied with early protected range-of-motion exercises.
FOREARM SHAFT FRACTURES (ICD-9:813)
• Incidence is greater in men than in women.
• Patients should be treated within intraarticular fracture principles.
• Volkmann ischemia and compartment syndrome are devastating complications.
In general, any fracture requires evaluation both clinically and radiographically of a joint above and joint below the fracture. It is not uncommon for fractures of the midshaft of the forearm to have significant consequences to either the wrist or elbow.
1. Isolated Fracture of the Ulna (Nightstick Fracture) (ICD-9:813.22)
The most common injury mechanism is from a direct blow. Isolated ulna fractures are commonly known as nightstick fractures as the arm is raised overhead to protect from injury. They may be classified as stable or unstable. Unstable fracture are those that have more than 50% displacement, more than 10 degrees of angulation, involve the proximal third, or have associated instability at the proximal or the distal radioulnar joint (DRUJ). The time to union is about 3 months, with union achieved with cast immobilization and early mobilization of the wrist and elbow. Excellent results have been achieved using a functional brace for isolated ulnar fractures. With displaced fractures, ORIF is the choice of treatment. Current recommendations include fixation with a 3.5-mm dynamic or limited contact compression plate with six to eight cortices of fixation proximal and distal to the fracture. Nonunion, delayed union, and radioulnar synostosis with or without operation are not rare complications. Loss of forearm rotation and refracture after hardware removal are other important complications.
2. Isolated Radial Shaft Fractures (ICD-9:813.21)
A fracture anywhere along the length of the radius with or without associated ulnar fracture with injury to the DRUJ is defined as a Galeazzi fracture. Injuries associated with the DRUJ include ulnar styloid fractures, radial shortening of more than 5 mm, and DRUJ dislocation.
![]() Treatment
Treatment
ORIF with plate fixation is recommended in adult patients to ensure a reasonable chance of restoration of the DRUJ. After ORIF of the radial shaft through a volar Henry approach using compression plating, the DRUJ should be carefully inspected. If it is unstable, pinning in a position of stability (usually full supination) is required. If it is frankly dislocated and cannot be reduced closed and maintained by closed or percutaneous means, then open stabilization with repair of associated ligaments or removal of interposed soft tissue is mandatory.
3. Monteggia Fracture (ICD-9:813.03)
![]() Classification of Fractures
Classification of Fractures
In 1814, Monteggia of Milan described an injury involving fracture of the proximal third of the ulna, with anterior dislocation of the radial head. This definition was extended by Bado to include the entire spectrum of these fractures with associated radial head dislocations, regardless of the direction of dislocation. They are classified in the following way:
Type 1: Fracture of the ulnar diaphysis with anterior angulation and anterior dislocation of the radial head (60% of cases)
Type 2: Fracture of the ulnar diaphysis with posterior angulation or posterior or posterolateral dislocation of the radial head (15% of cases)
Type 3: Fracture of the ulnar metaphysis, with lateral or anterolateral dislocation of the radial head (20% of cases)
Type 4: Fracture of the ulna and radius at the proximal third, with anterior dislocation of the radial head (5% of cases)
Other authors have noted that type 3 fractures may be more common than type 2 fractures, but all agree that type 1 lesions are the most common.
It is important to perform an adequate neurovascular examination at the time of evaluation. Albeit rare, the radial and/or median nerve and the posterior and/or anterior interosseous nerve can be injured in conjunction with Bado type 2 and 3 fractures. The index of suspicion must be high because radial head dislocation may be missed if appropriate radiographs are not obtained and scrutinized.
![]() Treatment
Treatment
Closed treatment is usually satisfactory for children, but ORIF is the treatment of choice for Monteggia lesions in an adult. Optimal results require early diagnosis, rigid internal fixation of the fractured ulna, complete reduction of the dislocated radial head, and immobilization for approximately 6 weeks to allow healing with sufficient stability. Internal fixation is best performed with a compression plate technique. The radial head can often be completely reduced by closed means once the ulnar fracture is reduced and rigidly fixed. If this is not possible, open reduction is required; attention should be paid to the relationship between the annular ligament, the lateral epicondyle, and the radial head. Entrapment of the soft tissues is the most common reason for inability to obtain concomitant closed radial head reduction at the time of ORIF of the ulna.
4. Fractures of Both the Radius and Ulna (ICD-9:813.23)
Fractures of both the radius and ulna (both-bones fractures) usually result from high-energy injuries. These fractures are usually displaced because of the force required to produce such an injury. Careful neurovascular examination and adequate radiographs to show both the wrist and the elbow are mandatory.
![]() Treatment
Treatment
Treatment of choice for both-bones fractures is ORIF. The volar Henry approach should be used for radius repair, between the flexor carpi radialis and brachioradialis, with the ulna approached subcutaneously. ORIF offers the best chance of restoring the normal positions of the radius and ulna, which is critical to forearm function and, in particular, pronation and supination. For fractures of the proximal half of the radius, the dorsal Thompson approach can be used; however, the risk of iatrogenic injury to the posterior interosseous nerve is increased. Technical points to be considered include minimal subperiosteal stripping only of the fracture site. The plates can be placed on top of the periosteum to preserve the blood supply as much as possible. A 3.5-mm dynamic compression plate or limited-contact compression plate can be used for AO/ASIF compression plating. The recent development and implementation of locked intramedullary nail systems provide an effective alternative to plating. Bone grafting can be used for severely comminuted fractures with significant bone loss. Only the skin is closed so as not to cause compartment syndrome or Volkmann contracture.
Many authors recommend plate fixation for Gustilo type I, II, and IIIA open both-bones fractures. Use of an external fixator is a viable alternative, however, particularly if severe open wounds are present with skin and soft-tissue loss as in Gustilo type IIIB and IIIC injuries.
Catalano LW 3rd, Barron OA, Glickel SZ: Assessment of articular displacement of distal radius fractures. Clin Orthop Relat Res 2004;423:79-84. [PMID: 15232430]
Chung KC, Spilson SV: The frequency and epidemiology of hand and forearm fractures in the United States. J Hand Surg Am 2001;26:908. [PMID: 11561245]
Dell’Oca AA, Tepic S, Frigg R, et al: Treating forearm fractures using an internal fixator. Clin Orthop Relat Res 2001;389:196. [PMID: 11501811]
Iqbal MJ, Abbas D: Distal radioulnar synostosis following K-wire fixation. Orthopedics 2001;24:61. [PMID: 11199355]
Qidwai SA: Treatment of diaphyseal forearm fractures in children by intramedullary Kirschner wires. J Trauma 2001;50:303. [PMID: 11242296]
Ruch DS, Vallee J, Poehling GG, Smith BP, Kuzma GR. Arthroscopic reduction versus fluoroscopic reduction in the management of intraarticular distal radius fractures. Arthroscopy 2004;20:225. [PMID: 15007310]
Wei SY, Born CT, Abene A, et al: Diaphyseal forearm fractures treated with and without bone graft. J Trauma 1999;46:1045. [PMID: 10372622]
FRACTURES AND DISLOCATIONS OF THE DISTAL AND MID-FOREARM
![]() Anatomy and Biomechanical Principles
Anatomy and Biomechanical Principles
The distal radius has three articular components (Figure 2–8): distally the scaphoid and lunate fossae, which allow articulation with the scaphoid and the lunate bones, respectively; the sigmoid notch, which allows articulation with the ulna medially. Between the scaphoid and the lunate fossa is a ridge that corresponds with the scapholunate interval. This entire surface is covered with articular cartilage. The radial styloid allows attachment of the brachioradialis tendon. Also, it is the origin of several important wrist ligaments, including the radial scapholunate and radial lunocapitate ligaments.

![]() Figure 2–8. Articular components of the distal radius. L, lunate articular surface; N, sigmoid notch; S, scaphoid articular surface. (Reproduced, with permission, from Green DP, Hotchkiss RN, Pederson WC, eds: Operative Hand Surgery, 4th ed. New York: WB Saunders; 1999.)
Figure 2–8. Articular components of the distal radius. L, lunate articular surface; N, sigmoid notch; S, scaphoid articular surface. (Reproduced, with permission, from Green DP, Hotchkiss RN, Pederson WC, eds: Operative Hand Surgery, 4th ed. New York: WB Saunders; 1999.)
The third articular component of the distal radius is the sigmoid notch. This convex structure allows the radius to rotate around the distal ulna. The distal ulna itself has an ulnar styloid, which contains attachments to the triangular fibrocartilage complex, including the meniscus homolog, the volar and dorsal ulnar carpal ligaments, and the ulnar collateral ligament at the wrist. The concave elliptical distal radius is oriented in the sagittal plane with an average of 11 degrees of volar tilt. In the frontal plane, the average radial inclination is 23 degrees. Radial length is measured from the tip of the radial styloid to the ulnar articular surface and averages 13 mm.
In addition to the bony surfaces, the articular cartilage, joint capsule, and wrist ligaments, there are other soft tissues within the distal forearm and wrist. On the dorsal surface, six dorsal compartments contain wrist and digital extensor tendons (Figure 2–9). On the volar surface reside the contents of the carpal tunnel, with nine flexor tendons and the median nerve. On the ulnar surface, the flexor carpi ulnaris tendon can be palpated near its insertion on the pisiform. The boundaries of the ulnar tunnel, or Guyon’s canal, are the volar carpal ligament and transverse carpal ligament, the hook of the hamate radially, and the pisiform ulnarly. Guyon’s canal contains the ulnar artery and nerve. The ulnar shaft remains fixed in its rotation at the ulnohumeral joint, and the radius rotates around the ulna in pronation and supination. The radius has a lateral bow that is crucial to the maintenance of full pronation and supination.
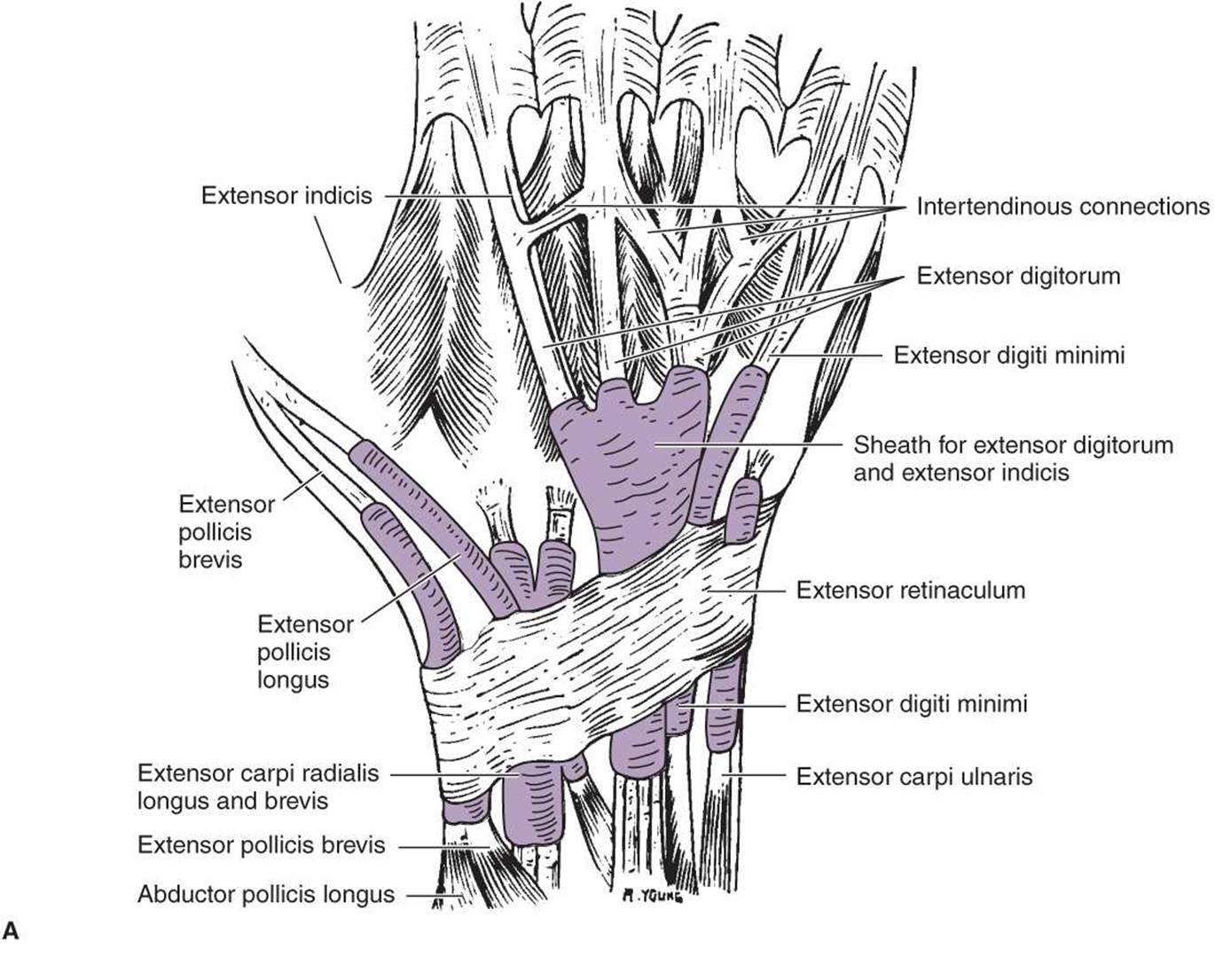

![]() Figure 2–9. A: Dorsal section of the wrist, showing the six dorsal compartments of the extensor tendons. B: Cross section of the wrist, showing the tendons, arteries, and nerves. (Reproduced, with permission, from Jenkins DB: Hollinshead’s Functional Anatomy of the Limbs and Back, 6th ed. New York: WB Saunders; 1991.)
Figure 2–9. A: Dorsal section of the wrist, showing the six dorsal compartments of the extensor tendons. B: Cross section of the wrist, showing the tendons, arteries, and nerves. (Reproduced, with permission, from Jenkins DB: Hollinshead’s Functional Anatomy of the Limbs and Back, 6th ed. New York: WB Saunders; 1991.)
The interosseous membrane in the interosseous space connects the shafts of the radius and ulna. The central portion is thickened and has been shown to be important in force transmission between the radius and ulna. Origins of flexor and extensor muscles are located along the anterior and posterior surfaces of the radius, ulna, and interosseous membrane.
Berger RA: The anatomy of the ligaments of the wrist and distal radioulnar joints. Clin Orthop Relat Res 2001;383:32. [PMID: 11210966]
Blazar PE, Chan PS, Kneeland JB, et al: The effect of observer experience on magnetic resonance imaging interpretation and localization of triangular fibrocartilage complex lesions. J Hand Surg Am2001;26:742. [PMID: 11466652]
Cober SR, Trumble TE: Arthroscopic repair of triangular fibro-cartilage complex injuries. Orthop Clin North Am 2001;32:279. [PMID: 11331541]
Freeland AE, Geissler WB: The arthroscopic management of intraarticular distal radius fractures. Hand Surg 2000;5:93. [PMID:11301502]
Gupta R, Bozenthka DJ, Osterman AL: Wrist arthroscopy: principles and clinical applications. J Am Acad Orthop Surg 2001;9:200. [PMID: 11421577]
Lindau T, Adlercreutz C, Aspenberg P: Peripheral tears of the triangular fibrocartilage complex cause distal radioulnar joint instability after distal radial fractures. J Hand Surg Am 2000;25:464. [PMID: 10811750]
McGinley JC, D’addessi L, Sadeghipour K, Kozin SH: Mechanics of the antebrachial interosseous membrane: response to shearing forces. J Hand Surg Am 2001;26:733. [PMID: 11466651]
Nakamura T, Takayama S, Horiuchi Y, Yabe Y: Origins and insertions of the triangular fibrocartilage complex: a histological study. J Hand Surg Br 2001;26:446. [PMID: 11560427]
Poitevin LA: Anatomy and biomechanics of the interosseous membrane: its importance in the longitudinal stability of the forearm. Hand Clin 2001;17:97. [PMID: 11280163]
DISLOCATION OF THE RADIOCARPAL JOINT
Dislocation of the radiocarpal joint is usually accompanied by significant carpal-ligamentous injury or fracture. Treatment of these injuries involves restoration of the bony architecture through immediate closed reduction, if possible; elective closed reduction; ORIF; or a combination of these procedures. Associated fractures, such as transscaphoid perilunate or distal radius fracture associated with carpal dislocation, should be treated with ORIF. Ligamentous repair should be performed at this time (see Chapter 9, “Hand Surgery”). Median nerve evaluation is mandatory, and surgical exploration is indicated if a dense neuropathy is present.
DISTAL RADIUS AND ULNA INJURIES
• Account for approximately 14% of all fractures.
• Most common osteoporotic upper extremity fracture.
• Fall on outstretched hand is the most common injury mechanism.
1. Distal Radius and Ulna Fracture (ICD-9:813.40)
In 1814, Abraham Colles described the distal radius fracture as a “silver fork deformity”—volarly angulated, dorsally displaced, with loss of radial inclination and resultant radial shortening. In contrast, the Smith fracture, or reverse Colles fracture, is a dorsally angulated fracture of the distal radius, with the hand and wrist displaced volarly with respect to the forearm. The fracture may be extraarticular, intraarticular, or a part of a fracture-dislocation involving the wrist. Barton fracture is a fracture-dislocation with an intraarticular fracture in which the carpus and a rim of the distal radius are displaced together (Figure 2–10). The Chauffeur’s fracture is a radial styloid fracture, described initially in car drivers operating automobiles, which required hand cranking to start. When the engine engaged, the crank would “kick back,” and the Chauffeur’s fracture would result.

![]() Figure 2–10. Schematic drawings of Colles fracture (A) and Smith and Barton fractures (B). AP, anteroposterior. (Reproduced, with permission, from Green DP, Hotchkiss RN, Pederson WC, eds: Operative Hand Surgery, 4th ed. New York: WB Saunders; 1999.)
Figure 2–10. Schematic drawings of Colles fracture (A) and Smith and Barton fractures (B). AP, anteroposterior. (Reproduced, with permission, from Green DP, Hotchkiss RN, Pederson WC, eds: Operative Hand Surgery, 4th ed. New York: WB Saunders; 1999.)
![]() Fracture Classification
Fracture Classification
In modern day fracture care, the emphasis has shifted from “named” fractures to anatomic descriptions of the injury.
No one fracture classification system is comprehensive in describing all important variables of distal radius fractures.
The Frykman classification categorizes fractures by the presence or absence of an ulnar styloid fracture and by whether fracture lines are extraarticular, intraarticular involving the radiocarpal joint, intraarticular involving the DRUJ, or intraarticular involving both the radiocarpal joint and DRUJ (Figure 2–11).

![]() Figure 2–11. Classification of distal radius fractures according to Frykman. (Reproduced, with permission, from Green DP, Hotchkiss RN, Pederson WC, eds: Operative Hand Surgery, 4th ed. New York: WB Saunders; 1999.)
Figure 2–11. Classification of distal radius fractures according to Frykman. (Reproduced, with permission, from Green DP, Hotchkiss RN, Pederson WC, eds: Operative Hand Surgery, 4th ed. New York: WB Saunders; 1999.)
The AO classification and its derivative, the OTA fracture classification system, are the most comprehensive systems currently used to classify distal radius fractures. Broadly, distal radius fractures are separated into three groups: extraarticular (type A), partial articular (type B), and complete articular (type C). Within these are subclassifications that relate to the particular amount of displacement and comminution (Figure 2–12). These subclassifications are primarily used for research.

![]() Figure 2–12. AO classification of distal radius fractures. A: Extraarticular metaphyseal fracture. Junction of the metaphysis and diaphysis is identified by the “square” or T method (greatest width on frontal plane of distal forearm; illustrated in A1). A1: Isolated fracture of distal ulna. A2: Simple radial fracture. A3: Radial fracture with metaphyseal impaction. B: Intraarticular rim fracture (preserving the continuity of the epiphysis and metaphysis). B1: Fracture of radial styloid. B2: Dorsal rim fracture (dorsal Barton fracture). B3: Volar rim fracture (reverse Barton 5 Goyrand-Smith type 2, Letenneur). C:Complex intraarticular fracture (disrupting the continuity of the epiphysis and metaphysis). C1: Radiocarpal joint congruity preserved; metaphysis fractured. C2: Articular displacement. C3: Diaphyseal-metaphyseal involvement. It should be considered that injury of the distal radioulnar joint is possible in any of these fractures. (Reproduced, with permission, from Green DP, Hotchkiss RN, Pederson WC, eds: Operative Hand Surgery, 4th ed. New York: WB Saunders; 1999.)
Figure 2–12. AO classification of distal radius fractures. A: Extraarticular metaphyseal fracture. Junction of the metaphysis and diaphysis is identified by the “square” or T method (greatest width on frontal plane of distal forearm; illustrated in A1). A1: Isolated fracture of distal ulna. A2: Simple radial fracture. A3: Radial fracture with metaphyseal impaction. B: Intraarticular rim fracture (preserving the continuity of the epiphysis and metaphysis). B1: Fracture of radial styloid. B2: Dorsal rim fracture (dorsal Barton fracture). B3: Volar rim fracture (reverse Barton 5 Goyrand-Smith type 2, Letenneur). C:Complex intraarticular fracture (disrupting the continuity of the epiphysis and metaphysis). C1: Radiocarpal joint congruity preserved; metaphysis fractured. C2: Articular displacement. C3: Diaphyseal-metaphyseal involvement. It should be considered that injury of the distal radioulnar joint is possible in any of these fractures. (Reproduced, with permission, from Green DP, Hotchkiss RN, Pederson WC, eds: Operative Hand Surgery, 4th ed. New York: WB Saunders; 1999.)
Another useful classification that addresses intraarticular fractures is that popularized by Melone (Figure 2–13). The Melone classification describes four major fracture components including the shaft, radial styloid, and dorsal and volar medial fragments. Often, the lunate fossa is fractured into dorsal and volar components, with the scaphoid fossa a separate component. Four-part articular fractures can have varying degrees of displacement and comminution.

![]() Figure 2–13. Intraarticular fracture classification of Melone. (Reproduced, with permission, from Green DP, Hotchkiss RN, Pederson WC, eds: Operative Hand Surgery, 4th ed. New York: WB Saunders; 1999.)
Figure 2–13. Intraarticular fracture classification of Melone. (Reproduced, with permission, from Green DP, Hotchkiss RN, Pederson WC, eds: Operative Hand Surgery, 4th ed. New York: WB Saunders; 1999.)
![]() Treatment
Treatment
Treatment of distal radius fractures should be influenced by fracture pattern and bone quality with a goal of restoring normal alignment and articular congruity. Patients’ activity level and comorbidities must be taken into account. Most distal radius fractures can be assessed through high-quality posteroanterior (PA), oblique, and lateral radiographs. The normal alignments as measured in the AP and lateral radiographs of the wrist are as follows: radial inclination, 22 degrees; volar tilt, 11–12 degrees; and radial length, 11–12 mm. Additional factors to consider are fracture displacement, intraarticular components, angulation, and degree of comminution; age of the patient; and functional level. Additional imaging techniques can be used to assess complex fracture patterns, including CT scan for preoperative planning of intraarticular fractures and MRI to rule out injuries to the carpal ligaments (eg, lunotriquetral and scapholunate ligament) or to the triangular fibrocartilage complex.
Surgery is indicated in patients with an open fracture or those with an inherently unstable fracture pattern (generally defined by at least three of the following criteria as discussed by Lafontaine et al: initial dorsal angulation of more than 20 degrees, initial shortening of more than 5 mm, more than 50% dorsal comminution, an intraarticular fracture, or an age of more than 60 years with an associated ulnar fracture), a shear fracture, or a fracture dislocation of the wrist.
A. Extraarticular Nondisplaced Fractures
Extraarticular nondisplaced fractures can be treated with cast immobilization for 4–6 weeks until fracture healing occurs, followed by mobilization with an off-the-shelf brace. Radial length and angulation are generally not fully restored with closed reduction techniques. Small amounts of radial shortening can lead to increased load in the lunate fossa, distal ulna, and triangular fibrocartilage. In most low-demand patients, however, this treatment can be successful, and functional wrist motion can be obtained. If shortening is significant, midcarpal instability may occur. Another potential problem is DRUJ arthrosis and ulnar carpal abutment, which may necessitate later reconstruction. In minimally displaced fractures, a rapid cast conversion to a supportive splint (2 or 3 weeks) and early mobilization can be safely done and may yield improved outcomes.
B. Extraarticular Displaced Fractures
Closed reduction should be attempted on extraarticular displaced fractures. If radial length and volar tilt are restored, then a sugar tong splint or long arm cast can be effective in holding the reduction. If the reduction is not adequate by closed means, then an external fixator (for ligamentotaxis) and percutaneous pins (to manipulate the fracture) may be necessary. Although current trends are toward plating via a volar approach with specialized locking plates, new low-profile plate designs make the dorsal approach a reliable option. Major drawbacks of dorsal plating are tendon irritation and joint stiffness. Recent studies indicate that locked plates and early postoperative range of motion may provide improved long-term results.
Percutaneous pin fixation can be an effective adjunct to cast treatment or external fixation. It can be intrafocal or interfragmentry. Arthroscopically assisted reduction can be a useful tool for assessing articular reduction. Loss of reduction is a potential complication in older patients. Also, granuloma formation around the pin can be seen.
External fixation is an effective way to handle distal radius fractures. With external fixation, there is the additional advantage of not devascularizing bony fragments and not creating a surgical wound. Use of indirect traction on fracture fragments, taking advantage of “ligamentotaxis” via the fixator pins, can be effective. In cases of open fractures, an external fixator can facilitate wound care. External fixation is effective in preventing loss of reduction and length in situations where there is comminution of bone. Complications with external fixation include pin tract infection, superficial radial nerve neuropathy, pin loosening, and stiffness.
C. Intraarticular Fractures
The treatment of intraarticular fractures aims to restore the congruity of the articular surface and the anatomic axis of the distal radius in order to improve the outcome. ORIF is the treatment of choice. For volar Barton fractures, the treatment of choice is the volar buttress plate. The only contraindications to this treatment are cases with excessive comminution such that ORIF will fail to achieve a stable bony construct. In these situations, use of an external fixator as a distractor and neutralization device is generally indicated. Using a fluoros-copy unit to visualize the fracture will help ascertain that both articular alignment and overall radial length have been adequately restored with external fixation. Minor adjustments as necessary can be effectively done with adjunct percutaneous pins. These maneuvers may fail to achieve the appropriate articular alignment, particularly if some healing has already occurred or if the displacement is severe. In this case, ORIF should be performed. Justification for aggressive treatment of distal radius fractures in young patients (<60 years) comes from several studies. The goal should be articular step-off less than 2 mm, radial shortening less than 4 mm, dorsal tilt less than 15 degrees, volar tilt less than 20 degrees, and loss of radial inclination less than 10 degrees. Arthroscopically assisted repair of distal radius fractures has been advocated. Intraarticular step-off and associated injuries such as triangular fibrocartilage, scapholunate, and lunotriquetral tears, as well as osteochondral lesions, can be accurately assessed. Some authors advocate bone grafting in the acute treatment of comminuted fractures. In intraarticular fractures, external fixation can be used, but reductions are difficult to maintain without percutaneous pins or internal fixation.
2. Distal Radioulnar Joint Dislocation (ICD-9:833.01)
The distal ulna transmits significant loads to the forearm through the distal ulna via the triangular fibrocartilage complex. Even minor disruptions of the precise anatomic relationships between the distal radius and ulna and ulnar carpus result in pain syndromes. The DRUJ can be dislocated by a variety of mechanisms, including low- and high-energy trauma. These are associated with disruption of the ulnar soft-tissue triangular fibrocartilage complex, including the articular disk and associated ligaments. There should be a high index of suspicion in order to diagnose this lesion because radiographs that are not taken in the perfect lateral orientation will tend to look relatively normal. A displaced fracture at the ulnar styloid base indicates a high risk of distal radioulnar instability. In the presence of forearm and elbow fracture-dislocations, further evaluation of the radioulnar joint is mandatory.
![]() Clinical Findings
Clinical Findings
The clinical examination is key, with identification of the DRUJ surface anatomy and clinical evaluation of the joint. The amount of stability should be carefully assessed and compared with that of the opposite wrist. The patient should position the wrist to reproduce the pain. With the hand pronated, the examiner tries to displace the ulnar head, applying a dorsal to volar load 4 cm proximal to the DRUJ (“piano key test”). Little resistance to ballottement and volar movement of the ulna head corresponds to a positive piano key test. Subluxation is much more common than anterior or posterior dislocation. Limitation of pronation and supination, or pain associated with such motion, would be expected in such a situation. Palpation of the sixth extensor compartment during resisted pronation is useful to identify any subluxation. The other common cause of DRUJ problems is rheumatoid arthritis.
![]() Treatment
Treatment
Dorsal dislocation, or subluxation, should be treated by reduction of the ulnar head into the sigmoid fossa and placement of the forearm in full supination. The arm should be immobilized in supination, which requires a long arm cast or splint. Volar dislocation is relatively rare and is usually stable after reduction. If dorsal or volar dislocation or subluxation of the distal ulna cannot be reduced with manipulation in the outpatient setting, closed treatment can be attempted under anesthesia. If this fails, open reduction and soft-tissue reconstruction may be necessary. If this is performed, a retinacular flap may be used to transpose the extensor carpi ulnaris to a more dorsal position to stabilize the distal ulna, as has been described for Darrach reconstruction of the joint.
3. Malunion of Distal Radius
Malunion of the distal radius can have a variety of negative consequences. Alteration of the biomechanical function of the wrist may lead to weakness, limitation of motion, and midcarpal instability. Associated DRUJ arthrosis may be present, as well as ulnocarpal abutment. Also, rotational deformity is common with angulated malunions. CT of both wrists can be used to identify and measure malrotation preoperatively.
![]() Treatment
Treatment
The treatment of choice in such a situation, if conservative treatment fails, is reconstructive surgery. Fernandez has elegantly described the strategy. An osteotomy of the radius with iliac crest bone grafting and plate fixation is performed (Figure 2–14).

![]() Figure 2–14. Open wedge osteotomy of the distal radius with iliac crest bone graft and plate fixation. (Reproduced, with permission, from Green DP, Hotchkiss RN, Pederson WC, eds: Operative Hand Surgery, 4th ed. New York: WB Saunders; 1999.)
Figure 2–14. Open wedge osteotomy of the distal radius with iliac crest bone graft and plate fixation. (Reproduced, with permission, from Green DP, Hotchkiss RN, Pederson WC, eds: Operative Hand Surgery, 4th ed. New York: WB Saunders; 1999.)
The DRUJ must be addressed and, depending on the degree of subluxation or arthrosis, may require closed reduction, open reduction, or reconstruction using the Darrach or Sauve-Kapandji procedure (Figure 2–15). In the Sauve-Kapandji procedure, instead of distal ulnar resection as in the Darrach procedure, transverse segmental resection of the ulnar metaphysis is followed by creation of an arthrodesis of the distal ulna to the radius, using the resected bone as grafting material. Forearm rotation occurs through the ulnar metaphyseal pseudoarthrosis. Additionally, restoration of the radial length may be difficult with manipulation alone. Useful adjuncts to achieve restoration of appropriate length and orientation in severe malunion include use of laminar spreaders to distract the proximal and distal fragments of the radius after osteotomy. Alternatively, an external fixator may prove useful in helping to achieve appropriate length after osteotomy.

![]() Figure 2–15. Suave-Kapandji reconstruction of the distal radioulnar joint. (Reproduced, with permission, from Green DP, Hotchkiss RN, Pederson WC, eds: Operative Hand Surgery, 4th ed. New York: WB Saunders; 1999.)
Figure 2–15. Suave-Kapandji reconstruction of the distal radioulnar joint. (Reproduced, with permission, from Green DP, Hotchkiss RN, Pederson WC, eds: Operative Hand Surgery, 4th ed. New York: WB Saunders; 1999.)
If the distal radius has settled into a position of shortening and significant angulatory deformity but the fracture is not yet fully healed, osteotomy for early or “nascent” malunion is justified. The advantage of taking down a nascent malunion is that the operation is technically simpler to perform, shortens the time of disability, and leads to better long-term results. Additionally, the DRUJ can be restored more reliably in these early reconstructions than when osteotomy is required for established malunion. The latter often requires adjunctive DRUJ reconstruction with Darrach resection, Sauve-Kapandji procedure, hemiresection, or matched resection arthroplasty.
Abboudi J, Culp RW: Treating fractures of the distal radius with arthroscopic assistance. Orthop Clin North Am 2001;32:307. [PMID: 11331543]
Antuña SA, Sánchez-Márquez JM, Barco R: Long-term results of radial head resection following isolated radial head fractures in patients younger than forty years old. J Bone Joint Surg Am 2010;92:558. [PMID: 20194313]
Carter PB, Stuart PR: The Sauve-Kapandji procedure for post-traumatic disorders of the distal radio-ulnar joint. J Bone Joint Surg Br 2000;82:1013. [PMID: 11041592]
Chhabra A, Hale JE, Milbrandt TA, et al: Biomechanical efficacy of an internal fixator for treatment of distal radius fractures. Clin Orthop Relat Res 2001;393:318. [PMID: 11764365]
Jakob M, Rikli A, Regazzoni P: Fractures of the distal radius treated by internal fixation and early function. J Bone Joint Surg Br 2000;82-B:341. [PMID: 10813166]
Ladd AL, Pliam NB: The role of bone graft and alternatives in unstable distal radius fracture treatment. Orthop Clin North Am 2001;32:337. [PMID: 11331546]
Lafontaine M, Hardy D, Delince P: Stability assessment of distal radius fractures. Injury 1989;20:208. [PMID: 2592094]
Margaliot Z, Haase SC, Kotsis SV, et al: A meta-analysis of outcomes of external fixation versus plate osteosynthesis for unstable distal radius fractures. J Hand Surg 2005;30:1185. [PMID: 16344176]
May MM, Lawton JN, Blazar PE: Ulnar styloid fractures associated with distal radius fractures: incidence and implications for distal radioulnar joint instability. J Hand Surg Am 2002;27:965. [PMID: 12457345]
Medoff RJ: Essential radiographic evaluation for distal radius fractures. Hand Clin 2005;21:279. [PMID: 16039439]
Nalbantoglu U, Gereli A, Kocaoglu B, Aktas S, Turkmen M: Capitellar cartilage injuries concomitant with radial head fractures. J Hand Surg Am 2008;33:1602. [PMID: 18984344]
Orbay JL, Fernandez DL: Volar fixed-angle plate fixation for unstable distal radius fractures in the elderly patient. J Hand Surg Am 2004;29:96. [PMID: 14751111]
Penzkofer R, Hungerer S, Wipf F, von Oldenburg G, Augat P: Anatomical plate configuration affects mechanical performance in distal humerus fractures. Clin Biomech 2010;25:972. [PMID: 20696508]
Rogachefsky RA, Lipson SR, Applegate B, et al: Treatment of severely comminuted intraarticular fractures of the distal end of the radius by open reduction and combined internal and external fixation. J Bone Joint Surg Am2001;83-A:509. [PMID: 11315779]
Schneeberger AG, Ip W, Poon T, et al: Open reduction and plate fixation of displaced AO type C3 fractures of the distal radius: restoration of articular congruity in eighteen cases. J Orthop Trauma2001;15:350. [PMID: 11433140]
Simic PM, Robison J, Gardner MJ, Gelberman RH, Weiland AJ, Boyer MI: Treatment of distal radius fractures with a low-profile dorsal plating system: an outcomes assessment. J Hand Surg Am2006;31:382. [PMID: 16516731]
Stoffel K, Cunneen S, Morgan R, Nicholls R, Stachowiak G: Comparative stability of perpendicular versus parallel double-locking plating systems in osteoporotic comminuted distal humerus fractures. J Orthop Res 2008;26:778. [PMID: 18203185]
Viso R, Wegener EE, Freeland AE: Use of a closing wedge osteotomy to correct malunion of dorsally displaced extraarticular distal radius fractures. Orthopedics 2000;23:721. [PMID: 10917249]
![]() II. TRAUMA TO THE LOWER EXTREMITY
II. TRAUMA TO THE LOWER EXTREMITY
PELVIC FRACTURES AND DISLOCATIONS
• Pelvic fractures are potentially life-threatening injuries with high mortality rates.
• Most are caused by MVAs and falls from height.
• A multidisciplinary approach is necessary to reduce mortality and disability.
• Pelvic ring fractures account for 3% of all fractures.
![]() Mechanism of Injury
Mechanism of Injury
Four patterns of injury are responsible for pelvic fractures. Anteroposterior compression results in external rotation of the hemipelvis and rupture of the pelvic floor and anterior sacroiliac ligaments. Lateral compression creates compression fractures of the sacrum and disruption of the posterior sacroiliac ligament complex. The sacrospinous and sacrotuberous ligaments remain intact, limiting the instability. In high-energy lateral compression injuries, the contralateral hemipelvis can be pushed in external rotation, as seen in rollover or crush injuries. Combined external rotation-abduction is common in motorcycle accidents, and the deforming forces are transmitted through the femur. The fourth pattern is a shear force vector resulting from fall from heights, where the grade of translational instability is variable.
![]() Clinical Findings
Clinical Findings
Knowledge of the injury mechanism is of prime importance to estimate the outcomes; the physical examination includes inspection of the skin, perineum, and rectum. Closed degloving injuries (Morel-Lavallée) should be properly identified. Palpation of the pelvic bony landmarks, including posterior palpation of the sacrum and sacroiliac joint, should be done, but anteroposterior and lateral iliac wing compression maneuvers to assess stability should be performed only once or avoided in hemodynamically unstable patients because excessive manipulation can increase bleeding by mobilizing the initial clotting. Rectovaginal examination is mandatory in all cases to identify open fractures. Bony spikes protruding through the mucosa contaminate the fracture hematoma. Associated injuries should also be systematically sought: lower urinary tract injuries, distal vascular status, and a thorough recorded neurologic examination.
An initial AP pelvic radiograph as per ATLS protocol is examined to evaluate the pelvic ring as a possible cause of shock. Following successful resuscitation, AP pelvis radiography should be obtained. When the patient is hemodynamically stabilized, inlet and outlet views and, if acetabular fractures are suspected, obturator or iliac oblique views should be ordered. Actual displacement of the symphysis pubis can also be evaluated by stress views under general anesthesia. CT scan is essential to further define the fracture pattern. Vascular and urologic imaging may also be required.
![]() Treatment
Treatment
Most pelvis fractures treated by orthopedic surgeons are stable injuries, and management of these low-energy fractures generally requires nonsurgical treatment. On the contrary, management of unstable pelvic injuries requires a systemic approach in a multidisciplinary manner. Thus, in the hemo-dynamically unstable patient, the ATLS protocol should be followed. Hemorrhage and shock are the primary causes of death due to pelvic fracture. The cornerstones of successful treatment include identification of a significant pelvic injury; rapid resuscitation; hemorrhage control (using angiography or pelvic packing); assessment and treatment of associated injuries; and mechanical stabilization in selected cases. Initial resuscitation started with 2 L of crystalloid should be followed by packed blood cells, fresh frozen plasma, and platelets in a 1:1:4 ratio. A pelvic binder or sheet can be used to stabilize the unstable pelvis temporarily. After ruling out other sources of bleeding by chest and spine radiography and focused abdominal sonography for trauma (FAST), an external fixation device (pelvic clamp and/or anterior external fixator) should be applied. Pelvic packing and/or arterial angiography should be executed according to the protocol of the trauma center. If the patient’s hemodynamic status stabilizes, the need for definitive versus temporizing mechanical fixation of the pelvis should be determined. Anterior fixation may involve anterior plating of the pubic symphysis or maintaining the external fixation device in place, which does not provide posterior stability and can potentially increase displacement of the fractured pelvis in vertical unstable fracture configuration. It usually resists stresses imposed by sitting but not those from weight bearing, and further internal fixation is often required at a later stage. Posterior fixation (either surgical or CT-guided percutaneous fixation) is usually deferred until a later time.
In open pelvic fractures, which account for 2–4% of all pelvic fractures, early surgical intervention using a multi-disciplinary approach should be undertaken. Seventy-two percent of open pelvic fractures are grade III open wounds and should be appropriately treated. The definitive method of stabilization of open pelvic fractures remains controversial. Internal fixation can be done when no gross contamination is present. Otherwise, external fixation is preferred when fecal or environmental contamination is present. If the fecal content contacts the open wound, colostomy is indicated.
A. Associated Injuries
1. Hemorrhage—Most of the bleeding associated with pelvic ring fractures usually comes from the small to mediumsized veins in the surrounding soft tissues and from the bone itself. Arterial injuries causing significant bleeding occur only in about 10% of pelvic fractures. After blunt trauma, the most common pelvic arteries injured are the superior gluteal and internal pudendal arteries. CT scans can be used to detect arterial bleeding before angiography but should be postponed until the patient is hemodynamically stable for transfer. Embolization can be used to prevent arterial bleeding. Pelvic packing helps tamponade the bleeding by increasing the intrapelvic pressure. Surgery for repair or bypass is urgently required if there is a distal ischemia.
2. Thrombosis—Pelvic fractures increase the risk of venous thromboembolic problems in trauma patients. DVT is seen not only in distal calf veins, but also in pelvic venous plexus. Magnetic venous venography is more advantageous than duplex color ultrasound to detect pelvic thrombosis. Guidelines for prophylaxis are controversial, and one should consider the benefits, risks, and cost of different treatment options. Early administration of low-molecular-weight heparin (LMWH) may decrease the incidence of symptomatic pulmonary emboli. More trauma centers now use intermittent pneumatic compression after trauma and temporary vena cava filters in severely traumatized patients with contradictions to pharmacologic prophylaxis (heparin, warfarin, or LMWH).
3. Neurologic injury—Neurologic injuries are common, and the frequency increases with complexity of the fractures. Up to 40% of unstable pelvic injuries may have neurologic injuries. After unstable vertical shear sacral fractures, the incidence rises to 50%. L5 and S1 are the most common affected roots. It is of paramount importance that a thorough neurologic examination is performed and recorded as soon as possible, searching for sensory or motor deficits in the distribution of sciatic, femoral, obturator, pudendal, or superior gluteal nerves. Peripheral nerve injuries have, overall, a better prognosis than root injuries. Partial nerve injuries also have a better outcome than complete ones. Most of the lesions are of the neurapraxia type, with favorable outcome. It is still accepted that nearly 10% have clinically significant permanent neurologic sequelae.
4. Urogenital injuries—Urogenital injuries are common and occur in as many as 24% of adults with pelvic fractures. Males have twice the urethral injury incidence than females because of the anatomic disadvantage. In males, these injuries should be suspected in a patient who is unable to void, who has gross hematuria at the meatus, swelling or hematoma of the perineum or penis, or a “high-riding” or “floating” prostate at digital rectal examination.
Additionally in female patients, vaginal bleeding, labial edema, blood at the meatus, and urinary leak per rectum can be clinical signs of possible urethral injury. Blind insertion of a Foley catheter may cause extension of a partial tear into a complete tear, may increase the extent of a hemorrhage, or may introduce an infectious agent into a previously sterile hematoma, so a retrograde (ascending) urethrogram should be obtained before insertion. When a partial or complete urethral disruption is diagnosed, a suprapubic cystotomy should be performed.
1. Injuries to the Pelvic Ring (ICD-9:808.41-42-43-49, 808-2)
Injuries that are stable do not deform under normal physiologic forces, whereas unstable injuries are characterized by their type of displacement, such as vertically unstable or horizontally unstable.
From the anatomic standpoint, the posterior sacroiliac ligamentous complex is the single most important structure for pelvic stability. Injuries involving the pelvic ring in two or more sites create an unstable segment. The integrity of the posterior sacroiliac ligamentous complex will determine the degree of instability. Inlet and outlet views and CT scanning are necessary imaging techniques to make this determination. When intact, the hemipelvis will be rotationally unstable but vertically stable. When disrupted, the hemipelvis will be both rotationally and vertically unstable.
![]() Classification and Treatment
Classification and Treatment
Tile devised a dynamic classification system based on the mechanism of injury and residual instability (Table 2–5).
Table 2–5. The Tile classification of pelvic ring disruptions.

Type A: Fractures that involve the pelvic ring in only one place and are stable.
Type A1: Avulsion fractures of the pelvis that usually occur at muscle origins (eg, the anterosuperior iliac spine [sartorius], anteroinferior iliac spine [direct head of the rectus femoris], and ischial apophysis [hamstring muscles]). These fractures occur most often in the adolescent, and conservative treatment is usually sufficient. On rare occasions, symptomatic nonunion occurs and is best dealt with surgically.
Type A2: Stable fractures with minimal displacement. Isolated fractures of the iliac wing without intraarticular extension usually result from direct trauma. Even with significant displacement, bony healing is to be expected, and therefore, treatment is symptomatic. On rare occasions, the soft-tissue injury and accompanying hematoma may heal with significant heterotopic ossification.
Type A3: Obturator fractures. Isolated fractures of the pubic or ischial rami are usually minimally displaced. The posterior sacroiliac complex is intact, and the pelvis is stable. Treatment is symptomatic, with bed rest and analgesia, early ambulation, and weight bearing as tolerated.
Type B: Fractures that involve the pelvic ring in two or more sites. They create a segment that is rotationally unstable but vertically stable.
Type B1: Open-book fractures occur from anteroposterior compression. Unless the anterior separation of the pubic symphysis is severe (>6 cm), the posterior sacroiliac complex is usually intact and the pelvis relatively stable. Significant injury to perineal and urogenital structures is often present and should always be looked for. One should remember that fragment displacement at the time of injury might have been significantly more than what is apparent on radiograph. For minimally displaced symphysis injuries, only symptomatic treatment is needed. The same applies for the so-called straddle (four rami) fracture. For more displaced fracture-dislocations, reduction is done by lateral compression using the intact posterior sacroiliac complex as the hinge on which “the book is closed.” Reduction can be maintained by external or internal fixation. “Closing the book” decreases the space available for hemorrhage. It also increases patient comfort, facilitates nursing care, and allows earlier mobilization, which is beneficial to the polytrauma patient.
Type B2 and B3: Lateral compression fractures. A lateral force applied to the pelvis causes inward displacement of the hemipelvis through the sacroiliac complex and the ipsilateral (B2) or, more often, contralateral pubic rami (B3, bucket-handle type). The degree of involvement of the posterior sacroiliac ligaments will determine the degree of instability. The posterior lesion may be impacted in its displaced portion, affording some relative stability. The hemipelvis is infolded, with overlapping of the symphysis. Major displacement requires manipulation under general anesthesia. This should be done soon after injury because disimpaction becomes difficult and hazardous after the first few days. Reduction can be maintained with external or internal fixation, or both. External fixation alone decreases pain and makes nursing care easier but is not strong enough for ambulation if the fracture is unstable posteriorly.
Type C: Fractures that are both rotationally and vertically unstable. They often result from a vertical shear mechanism, like a fall from a height. Anteriorly, the injury may fracture the pubic rami or disrupt the symphysis pubis. Posteriorly, the sacroiliac joint may be dislocated, or there may be a fracture in the sacrum or in the ilium immediately adjacent to the sacroiliac joint, but there is always loss of the functional integrity of the posterior sacroiliac ligamentous complex. The hemipelvis is completely unstable. Three-dimensional displacement is possible, particularly proximal migration. Massive hemorrhage and injury to the lumbosacral nerve plexus are common. Indirect radiologic clues of pelvic instability should be looked for such as avulsion of the sciatic spine or fracture of the ipsilateral L5 transverse process. Reduction is relatively easy, with longitudinal skeletal traction through the distal femur or the proximal tibia. If chosen as definitive treatment, traction should be maintained for 8–12 weeks. Bony injuries heal quicker than ligamentous injuries. External fixation alone is insufficient to maintain reduction in highly unstable fractures, but it may help control bleeding and eases nursing care. ORIF is often required. The surgical technique is demanding, and there is a significant risk of complications. It is best left to experienced pelvic surgeons.
![]() Complications
Complications
Long-term complications of unstable pelvic ring disruptions are more frequent and disabling than once thought. If anatomic restoration of anatomic bony alignment cannot be achieved and maintained, complications such as pain, leg-length discrepancy, and residual gait abnormalities can be seen. The overall nonunion rate is around 3%. Chronic low back pain and sacroiliac pain are frequent and seen in up to 50% of cases on long-term follow-up. Changes in voiding pattern, altered defecation, and sexual dysfunction are common after sacral fractures or sacroiliac dislocations.
2. Fractures of the Acetabulum (ICD-9:808.0)
The acetabulum results from the closure of the Y or triradiate cartilage and is covered with hyaline cartilage.
Fractures of the acetabulum occur through direct trauma on the trochanteric region or indirect axial loading through the lower limb. The position of the limb at the time of impact (rotation, flexion, abduction, or adduction) will determine the pattern of injury. Comminution is common.
![]() Anatomy
Anatomy
The acetabulum appears to be contained within an arch. It is supported by the confluence of two columns and enhanced by two walls. The posterior column is the strongest one and where more space is available for fixation. It begins at the dense bone of the greater sciatic notch and extends distally through the center of the acetabulum to include the ischial spine and ischial tuberosity. The inner surface forms the posterior wall, and the anterior surface forms the posterior articular surface of the acetabulum. The anterior column extends from the iliac crest to the symphysis pubis. The anterior column rotates 90 degrees just above the acetabulum as it descends. The medial part of the anterior column is the true pelvic brim. The quadrilateral plate is the medial structure preventing medial displacement of the hip and is an independent structure between the two columns. The acetabular dome or weight-bearing area extends from the bone posterior to the anterior inferior iliac spine to the posterior column.
![]() Classification
Classification
Letournel has classified acetabular fractures based on the involved column. Fractures may involve one or both columns in a simple or complex pattern.
Proper fracture classification requires good-quality radiographs. Two oblique views (Judet views) taken 45 degrees toward and away from the involved side complement the standard AP view of the pelvis. The obturator (internal) oblique view is obtained by elevating the fractured hip 45 degrees from the horizontal. This view shows the anterior column (iliopectineal line) and the posterior lip of the acetabulum, and the iliac wing is perpendicular to its broad surface. In this view, the spur sign can be identified in 95% of cases of both-column fractures (type C), and it corresponds to the area of the iliac wing above the acetabular roof. The iliac (external) oblique view is obtained by elevating the nonfractured hip 45 degrees. This view best shows the posterior column (ilioischial line), including the ischial spine, the anterior wall of the acetabulum, and the full expanse of the iliac wing. In addition, inlet and outlet pelvic views can be complementary if any doubt about pelvic ring compromise is present.
CT scanning gives further information on the fracture pattern, the presence of free intraarticular fragments, and the status of the femoral head and the rest of the pelvic ring.
Letournel has classified acetabular fractures into 10 different types: five simple patterns (one fracture line) and five complex patterns (the association of two or more simple patterns) (Figure 2–16). This is the most widely used classification system, as it allows the surgeon to choose the appropriate surgical approach.
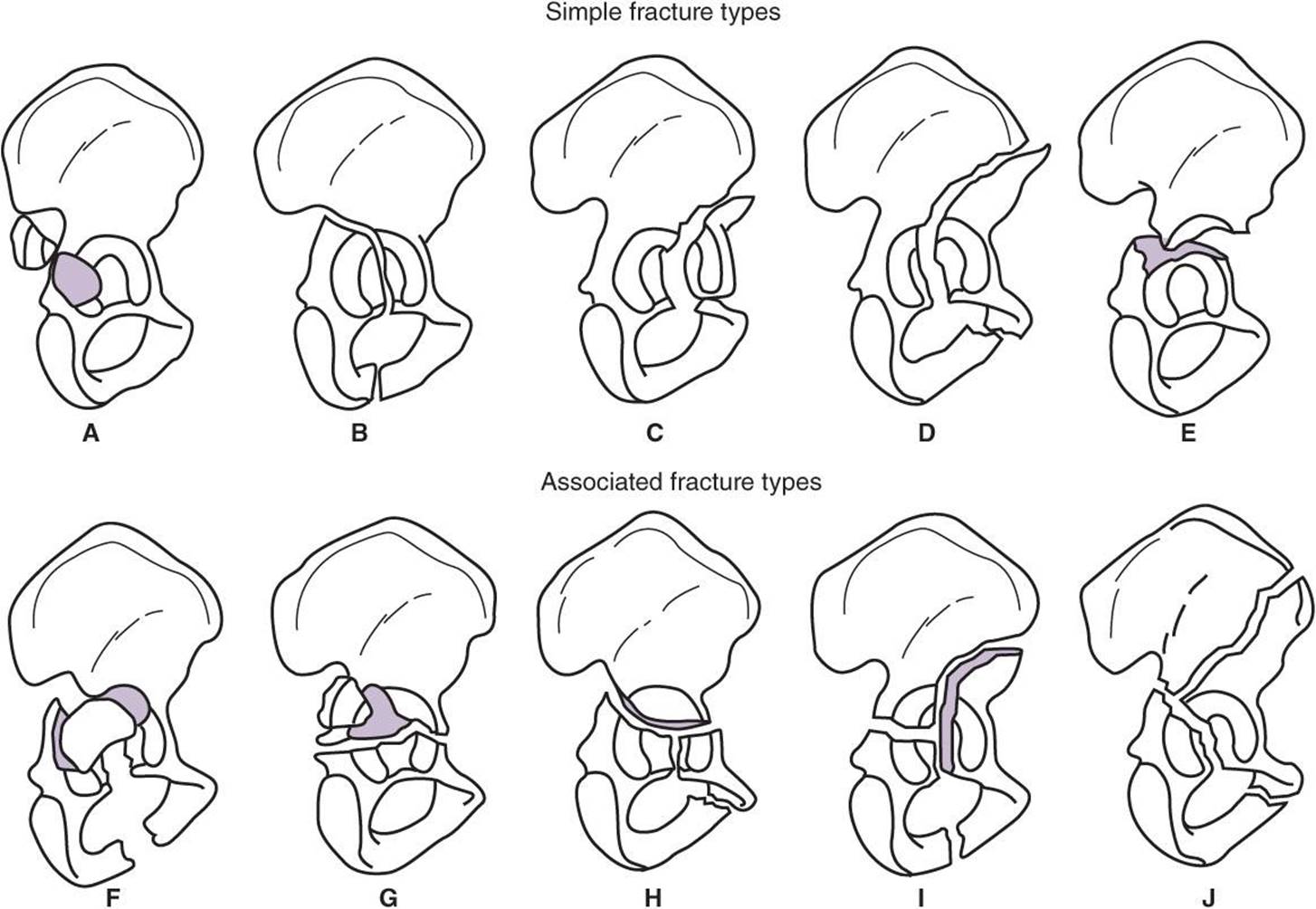
![]() Figure 2–16. Letournel classification of acetabular fractures. (Reproduced, with permission, from Canale ST, ed: Campbell’s Operative Orthopaedics, 9th ed. Philadelphia: Lippincott; 1998.)
Figure 2–16. Letournel classification of acetabular fractures. (Reproduced, with permission, from Canale ST, ed: Campbell’s Operative Orthopaedics, 9th ed. Philadelphia: Lippincott; 1998.)
![]() Treatment
Treatment
The goal of treatment is to attain a spherical congruency between the femoral head and the weight-bearing acetabular dome and to maintain it until bones are healed. As with other pelvic fractures, acetabular fractures are frequently associated with abdominal, urogenital, and neurologic injuries, which should be systematically sought and treated. Significant bleeding can be present and should be addressed as soon as possible. Examination of the knee ligaments and vascular status of the extremities is mandatory. A careful neurologic examination is necessary. Sciatic nerve compromise occurs in 20% of cases. The peroneal branch is often involved. The femoral nerve and superior gluteal nerve are also susceptible to injury during trauma or surgery. Prophylaxis and surveillance for DVT should be started soon after trauma.
The stabilized patient should be put in longitudinal skeletal traction through a distal femoral or proximal tibial pin pulling axially in neutral position. A trochanteric screw for lateral traction is contraindicated, because it will create a contaminated pin tract and thus preclude possible further surgical treatment. Postreduction radiographs are obtained. In general, a displaced acetabular fracture is rarely reduced adequately by closed methods. If the reduction is judged acceptable, traction is maintained for 6–8 weeks until bone healing is evident. Another 6–8 weeks is necessary before full weight bearing can be attempted. Surgical indications include intraarticular displacement of 2 mm or more, an incongruous hip reduction, marginal impaction of more than 2 mm, or intraarticular debris. The choice of approach is of primary importance, and sometimes more than one approach will prove necessary. Acetabular surgery uses extensile approaches and sophisticated reduction and fixation techniques and is best performed by trained pelvic surgeons. Other surgical indications include free osteochondral fragments, femoral head fractures, irreducible dislocations, or unstable reductions.
![]() Complications
Complications
Complications inherent to the injury include posttraumatic degenerative joint disease, heterotopic ossification, femoral head osteonecrosis, DVT, and other complications related to conservative treatment. Surgery is performed to prevent or delay osteoarthritis but increases the possibility of complications such as infection, iatrogenic neurovascular injury, and heterotopic ossification. When the reduction is stable and fixation is solid, the patient can be mobilized after a few days with non–weight-bearing ambulation, and weight bearing may begin as early as 6 weeks. Most pelvic surgeons now routinely use postoperative prophylactic anticoagulation and heterotopic bone formation prophylaxis with irradiation or indomethacin, or both.
American College of Surgeons, Committee on Trauma: Advanced Trauma Life Support for Doctors: Student Course Manual, 7th ed. Chicago: American College of Surgeons; 2008.
Bellabarba C, Ricci WM, Bolhofner BR: Distraction external fixation in lateral compression pelvic fractures. J Orthop Trauma 2000;14:475. [PMID: 11083609]
Carlson DA, Scheid DK, Maar DC, et al: Safe placement of S1 and S2 iliosacral screws: the vestibule concept. J Orthop Trauma 2000;14:264. [PMID: 10898199]
Grotz MRW, Allami MK, Harwood P, Pape HC, Kretekk C, Giannoudis PV: Open pelvic fractures: epidemiology, current concepts of management and outcome. Injury 2005;1:1. [PMID: 15589906]
Hak DJ, Smith WR, Suzuki T: Management of hemorrhage in life-threatening pelvic fracture. J Am Acad Orthop Surg 2009;17:447. [PMID: 19571300]
McCormick JP, Morgan SJ, Smith WR: Clinical effectiveness of the physical examination in diagnosis of posterior pelvic ring injuries. J Orthop Trauma 2003;17:257. [PMID: 12679685]
Saterbak AM, Marsh JL, Nepola JV, et al: Clinical failure after posterior wall acetabular fractures: the influence of initial fracture patterns. J Orthop Trauma 2000;14:230. [PMID: 10898194]
Slobogean GP, Lefaivre KA, Nicolaou S, O’Brien PJ: A systematic review of thromboprophylaxis for pelvic and acetabular fractures. J Orthop Trauma 2009;23:379. [PMID: 19390367]
Switzer JA, Nork SE, Routt ML: Comminuted fractures of the iliac wing. J Orthop Trauma 2000;14:270. [PMID: 10898200]
Tornetta P: Displaced acetabular fractures: indications for operative and nonoperative management. J Am Acad Orthop Surg 2001;9:18. [PMID: 11174160]
Tötterman A, Glott T, Madsen JE, RØise O: Unstable sacral fractures: associated injuries and morbidity at 1 year. Spine 2006;31:E628. [PMID: 17545913]
HIP FRACTURES AND DISLOCATIONS
• Globally, 6.3 million hip fractures are estimated by year 2050.
• Primarily occur in older patients over 55 years.
• Fall from standing height is the main cause of injury.
• Almost all hip fractures are treated surgically.
• One-year mortality after femoral neck and intertrochanteric fracture exceeds 14–36%.
![]() Anatomy and Biomechanical Principles
Anatomy and Biomechanical Principles
The hip joint is the articulation between the acetabulum and the femoral head. The trabecular pattern of the femoral head and neck, and that of the acetabulum, is oriented to optimally accept the forces crossing the joint. Calcar femorale is the dense bone oriented in posteromedial portion of the femoral shaft under the lesser trochanter that supports the force transfer from the neck to the shaft.
The total force acting across the joint is 2.5 times body weight when standing on one leg and five times body weight when running. Using a cane in the opposite hand reduces the force to body weight when standing on that leg.
1. Femoral Neck Fractures (ICD-9:820.0)
Femoral neck fractures occur in the intracapsular region between the trochanters distally and the head proximally. Main arterial blood supply of the neck comes from an extra-capsular ring of vessels formed by the ascending branch of the lateral circumflex artery anteriorly and medial circumflex artery posteriorly. These fractures are classified as subcapital, transcervical, and basicervical. The latter acts more like an intertrochanteric fracture. These fractures are generally low-energy injuries in the elderly population; however, they are more often seen as high-energy injuries at young ages. The typical patient is a female who had a falling incident and presents with a painful hip, with shortened and externally rotated extremity on physical examination. Stress fractures of the femoral neck can also occur and should be excluded in young athletes. These fractures may be difficult to diagnose. Physical examination, as well as the initial radiographs, may be normal. Repeat radiographs, radionuclide imaging, and MRI may be necessary to confirm the diagnosis. Plain AP view and a cross-table lateral view of the involved hip are indicated to diagnose and classify the fracture. Bone scans can be false negative in the acute phase.
![]() Classification
Classification
The Garden classification for acute fractures is the most widely used system:
Type 1: Valgus impaction of the femoral head
Type 2: Complete but nondisplaced
Type 3: Complete fracture, displaced less than 50%
Type 4: Complete fracture displaced more than 50%
This classification is of prognostic value for the incidence of avascular necrosis: The higher the Garden number, the higher the incidence. The benefits of either skeletal or skin traction are unclear prior to definitive treatment. Traction may offer comfort in some patients but does not improve overall outcome.
![]() Stable Femoral Neck Fractures
Stable Femoral Neck Fractures
These include stress fractures and Garden type 1 and 2 fractures. Nonsurgical treatment should be reserved for patients with extreme medical risks for surgery.
The Garden type 1 fracture is impacted in valgus position and is usually stable. Impaction must be demonstrated on both AP and lateral views. The risk of displacement is nevertheless significant; most surgeons recommend prophylactic internal fixation with screws or sliding hip screw to maintain reduction and allow earlier ambulation and weight bearing.
![]() Unstable Femoral Neck Fractures
Unstable Femoral Neck Fractures
Treatment is directed toward preservation of life and restoration of hip function, with early mobilization. This is best attained by rigid internal fixation or primary arthroplasty as soon as the patient is medically prepared for surgery. In general, the younger the patient, the greater the effort is justified to save the femoral head. More studies are in favor of an urgent intervention in a young patient to protect the head viability. Necessity of a capsulotomy to decompress the joint is controversial. In the elderly patient, surgical options are either ORIF or primary arthroplasty. Gjertsen et al showed that hemiarthoplasty for displaced femoral neck fractures in the elderly resulted in fewer reoperations, less pain, and higher satisfaction rates than internal screw fixation in 4335 patients from the Norwegian Hip Fracture Register.
![]() Treatment
Treatment
A. Internal Fixation
The fracture is reduced under fluoroscopic imaging as anatomically accurately as possible. Gentle manipulation is usually sufficient. Rarely, open reduction may be necessary before fixation. Open reduction, if performed, should be approached anteriorly because this results in less disruption of blood supply than a posterior approach. The most accepted method is fixation with three screws (in an inverted triangle manner with one screw in the posteroinferior of the neck). Sliding hip screw or plate should be placed with center-apex distance within 25 mm. An additional screw is inserted superior or posteroinferior in order to control the rotational forces. The patient can usually be mobilized the following day, and weight bearing is allowed according to the stability of the construct.
B. Primary Arthroplasty
Arthroplasty is reserved for elderly displaced fractures, particularly for Garden type 4 fractures, in which avascular necrosis is highly probable, and for Garden type 3 fractures that cannot be satisfactorily reduced or for femoral heads with preexisting disease. Recent studies indicate that a lower rate of reoperations and better outcomes are expected after total hip arthroplasty versus hemiarthroplasty.
![]() Complications
Complications
The most common sequelae of femoral neck fractures are loss of reduction with or without hardware failure, nonunions or malunions, and avascular necrosis of the femoral head. This latter complication can appear as late as 2 years after injury. According to different series, the incidence of avascular necrosis varies from 0 to 15% for Garden type 1 fractures, 10 to 25% for type 2 fractures, 25 to 50% for type 3 fractures, and 50 to 100% for type 4 fractures. Secondary degenerative joint disease appears somewhat later. The most disabling complication, infection, is fortunately rare.
2. Trochanteric Fractures (ICD-9:820.2)
![]() Lesser Trochanter Fracture (ICD-9:820.20)
Lesser Trochanter Fracture (ICD-9:820.20)
Isolated fracture of the lesser trochanter is rare. When it occurs, it is the result of the avulsion force of the iliopsoas muscle. Rarely, a symptomatic nonunion may require fragment fixation or excision.
![]() Greater Trochanter Fracture (ICD-9:820.20)
Greater Trochanter Fracture (ICD-9:820.20)
Isolated fracture of the greater trochanter may be caused by direct injury or may occur indirectly as a result of the activity of the gluteus medius and gluteus minimus muscles. It occurs most commonly as a component of intertrochanteric fracture.
If displacement of the isolated fracture fragment is less than 1 cm and there is no tendency to further displacement (as determined by repeated radiographic examinations), treatment may be bed rest until acute pain subsides. As rapidly as symptoms permit, activity can increase gradually to protected weight bearing with crutches. Full weight bearing is permitted as soon as healing is apparent, usually in 6–8 weeks. If displacement is greater than 1 cm and increases on adduction of the thigh, extensive tearing of surrounding soft tissues may be assumed, and ORIF is indicated. Tension band wiring is the preferred technique.
![]() Intertrochanteric Fractures (ICD-9:820.21)
Intertrochanteric Fractures (ICD-9:820.21)
• Approximately 50% of all hip fractures.
• Older age, female gender, osteoporosis, history of fall, and gait abnormalities are risk factors.
By definition, these fractures usually occur along a line between the greater and the lesser trochanter. They typically occur at a later age than do femoral neck fractures. They are most often extracapsular and occur through cancellous bone. Bone healing within 8–12 weeks is the usual outcome, regardless of the treatment. Nonunion and avascular necroses of the femoral head are not significant problems.
Clinically, the involved extremity is usually shortened and can be internally or externally rotated. If there is comminution in the calcar (posteromedial cortex) or the fracture line extends through the subtrochanteric region, the fracture is considered unstable. Reverse oblique fractures, where the course fracture line is proximal-medial to distal-lateral, are extremely unstable. A wide spectrum of fracture patterns is possible, from the nondisplaced fissure fracture to the highly comminuted fracture with four major fragments (head and neck, greater trochanter, lesser trochanter, and femoral shaft). The Muller/AO system is useful in classifying intertrochanteric femur fractures and has gained more popularity in recent years (Figure 2–17).

![]() Figure 2–17. Muller/AO system for intertrochanteric femur fracture classification. (Reproduced, with permission, from Browner BD, Levine A, Jupiter J, et al, eds: Skeletal Trauma, 2nd ed. New York: WB Saunders; 1998.)
Figure 2–17. Muller/AO system for intertrochanteric femur fracture classification. (Reproduced, with permission, from Browner BD, Levine A, Jupiter J, et al, eds: Skeletal Trauma, 2nd ed. New York: WB Saunders; 1998.)
The selection of definitive treatment depends on the general condition of the patient and the fracture pattern. Rates of illness and death are lower when the fracture is internally fixed, allowing early mobilization. Operative treatment is indicated as soon as the patient is medically able to tolerate surgery. Overall mortality decreases if surgery can be performed within 48 hours. Initial treatment in the hospital should be by gentle skin traction to minimize pain and further displacement. Skeletal traction as the definitive treatment is rarely indicated and is fraught with complications such as pressure sores, DVT and PE, deterioration of mental status, and varus malunion. When surgery is contraindicated, it may be preferable to mobilize the patient as soon as pain permits and accept the eventual malunion or nonunion.
The great majority of these fractures are amenable to surgery. The goal is to obtain a fixation secure enough to allow early mobilization and provide an environment for sound fracture healing in a good position. Reduction of the fracture is usually accomplished by closed methods, using traction on the fracture table, and monitored using fluoroscopic imaging. Internal fixation can be obtained by dynamic hip screw (DHS), intramedullary (IM) nail, and side plate. Fixation with IM nail has biomechanical advantages over DHS, especially for the unstable fracture patterns. Early full weight bearing, return to preinjury activity, decrease in blood loss, insertion through small incision, and shorter surgery time also make IM nailing favorable. While inserting the hip screw, the screw should be centrally positioned in the head, and the distance of the lag screw to the apex of the femoral head on both AP and lateral radiographic views should be within 25 mm. Reverse oblique fractures should be treated as subtrochanteric fractures. Although generally it is not the primary option for fixation, calcar replacement arthroplasty may be an option for patients with preexisting arthritic change who have poor bone quality or for salvage procedures. General complications include infection, hardware failure, loss of reduction, nonunion, irritation bursitis over the tip of the sliding screw, and dislocation for prosthetic implants.
3. Traumatic Dislocation of the Hip Joint
• Usually results from a high-energy trauma.
• Occurs with or without acetabular fracture.
• Eighty-five percent are posterior dislocations.
• Concomitant femur, knee, and patella fractures are common.
![]() Posterior Hip Dislocation (ICD-9:835.01)
Posterior Hip Dislocation (ICD-9:835.01)
Usually the head of the femur is dislocated posterior to the acetabulum when the thigh is flexed, for example, as may occur in a head-on automobile collision when the knee is driven violently against the dashboard. Posterior dislocation is also a complication of hip arthroplasty, especially with the posterior approach.
The significant clinical findings are shortening, adduction, and internal rotation of the extremity. Anteroposterior, lateral, and, if fracture of the acetabulum is demonstrated, oblique radiographic projections (Judet views) are required. Common associated injuries include fractures of the acetabulum or the femoral head or shaft and sciatic nerve injury. The head of the femur may be displaced through a tear in the posterior hip joint capsule. The short external rotator muscles of the femur are commonly lacerated. Fracture of the posterior margin of the acetabulum can create instability.
If the acetabulum is not fractured or if the fragment is small, reduction by closed manipulation is indicated. Reduction should be achieved as soon as possible, under general anesthesia with maximum muscle relaxation, preferably within the first few hours after injury. The incidence of avascular necrosis of the femoral head increases with time until reduction. The main feature of reduction is traction in the line of deformity followed by gentle flexion of the hip to 90 degrees with stabilization of the pelvis by an assistant. While manual traction is continued, the hip is gently rotated into internal and then external rotation to obtain reduction (Allis method).
The stability of the reduction is evaluated clinically by ranging the extended hip in abduction and adduction and internal and external rotation. If stable, the same movements are repeated in 90 degrees of hip flexion. The point of redis-location is noted, the hip is reduced, and an AP radiograph of the pelvis is obtained. Soft-tissue or bone fragment interposition will be manifested by widening of the joint space as compared to the contralateral side. Irreducible dislocations, nonconcentric reductions, open dislocations, dislocations with ipsilateral femoral neck fractures, and dislocations that redislocate after reduction despite hip extension and external rotation (usually because of associated posterior wall fracture of the acetabulum) are indications for immediate ORIF if necessary. Most authors agree that a widened joint space on radiograph, despite a stable reduction, is also an indication for immediate arthrotomy. Others prefer obtaining a CT scan first to further delineate the incarcerated fragments and associated injuries before surgery. Recent studies support the use of hip arthroscopy as a safer alternative to arthrotomy for managing loose bodies.
Minor fragments of the posterior margin of the acetabulum may be disregarded, but larger displaced fragments are not usually successfully reduced by closed methods. ORIF with screws or plates is indicated.
Postreduction treatment will vary according to the type of initial surgery and the extent of the injury. Some period of skin or skeletal traction may be beneficial after strictly soft-tissue injury with a stable concentric reduction. Gradual weight bearing starting with crutch ambulation follows this period, progressing to full weight bearing at 6 weeks. Securely fixed fractures are treated as soft-tissue injuries, but weight bearing is allowed when radiologic signs of bone healing are present. When fixation is tenuous, skeletal traction for 4–6 weeks or hip spica immobilization may be necessary.
Complications include infection, avascular necrosis of the femoral head, malunion, posttraumatic degenerative joint disease, recurrent dislocation, and sciatic nerve injury. Avascular necrosis occurs because of the disruption of the retinacular arteries providing blood to the femoral head. Its incidence increases with the duration of the dislocation. It can occur as late as 2 years after the injury. MRI studies enabling early diagnosis and protected weight bearing until revascularization has occurred are recommended. Sciatic nerve injury is present in 10–20% of patients with posterior hip dislocation. Although usually of the neurapraxia type, these lesions leave permanent sequelae in about 20% of cases. The rare patient who is neurologically intact before reduction but has a deficit after reduction should be explored surgically to see if the nerve has been entrapped in the joint. Associated injuries also, on rare occasions, include fracture of the femoral head. Small fragments or those involving the non–weight-bearing surface should be ignored if they do not disturb hip mechanics; otherwise, they should be excised. Large fragments of the weight-bearing portion of the femoral head should be reduced and fixed if at all possible.
![]() Anterior Hip Dislocation (ICD-9:835.03)
Anterior Hip Dislocation (ICD-9:835.03)
• Accounts for 10–15% of hip fracture dislocations.
• Occurs when the hip is extended and externally rotated at the time of impact.
Usually, the femoral head remains lateral to the obturator externus muscle but can be found rarely beneath it (obturator dislocation) or under the iliopsoas muscle in contact with the superior pubic ramus (pubic dislocation).
The hip is classically flexed, abducted, and externally rotated. The femoral head is palpable anteriorly below the inguinal flexion crease. AP and transpelvic lateral radiographic projections are usually diagnostic.
Closed reduction under general anesthesia is generally successful. Here also the surgeon must ensure a concentric reduction, comparing both hip joints on the postreduction AP radiograph. The patient starts mobilization within a few days when pain is tolerable. Active and passive hip motion, excluding external rotation, is encouraged, and the patient is usually fully weight bearing by 4–6 weeks. Skeletal traction or spica casting may rarely be useful for uncooperative patients.
4. Rehabilitation of Hip Fracture Patients
There has been an increased interest in the psychosocial outcomes of patients with hip fractures. The goal of rehabilitation after hip injuries is to return the patient as rapidly as possible to the preinjury functional level. Factors influencing rehabilitation potential include age, mental status, associated injuries, previous medical status, myocardial function, upper extremity strength, balance, and motivation.
For the rare patient treated conservatively, rehabilitation focuses early on preventing stiffness and weakness of the other extremities and, eventually, on mobilizing the patient out of bed when pain is tolerable. Because the great majority of these injuries are now treated with internal fixation or prosthetic replacement, rehabilitation efforts are focused toward early range of motion, muscle strengthening, and weight bearing. Early full weight bearing as tolerated is encouraged for patients with prosthetic replacements, cemented or not, and for patients with stable fixation of an intertrochanteric fracture to allow compression of the fracture fragments. Most authors now agree that the same applies for femoral neck fractures with stable internal fixation, although some still prefer partial weight bearing until radiologic evidence of bone healing is present to prevent hardware failure. When internal fixation does not provide stable fixation of the fracture fragments, supplemental protection may be added with a spica cast or brace; however, it is highly undesirable in elderly patients. Otherwise, restricted range of motion or weight bearing may be allowed according to the surgeon’s specifications.
Ahn J, Bernstein J: Fractures in brief: intertrochanteric hip fractures. Clin Orthop Relat Res 2010;468:1450. [PMID: 20195807]
Bernstein J, Ahn J: In brief: fractures in brief: femoral neck fractures. Clin Orthop Relat Res 2010;468:1713. [PMID: 20224957]
Conn KS, Parker MJ: Undisplaced intracapsular hip fractures: results of internal fixation in 375 patients. Clin Orthop Relat Res 2004;421:249. [PMID 15123955]
Cooper C, Campion G, Melton LJ 3rd: Hip fractures in the elderly: a world-wide projection. Osteoporos Int 1992;2:285. [PMID: 1421796]
Foulk DM, Mullis BH. Hip dislocation: evaluation and management. J Am Acad Orthop Surg 2010;18:199. [PMID: 20357229]
Gjertsen JE, Vinje T, Engesaeter LB, et al: Internal screw fixation compared with bipolar hemiarthroplasty for treatment of displaced femoral neck fractures in elderly patients. J Bone Joint Surg Am2010;92:619. [PMID: 20194320]
Gotfried Y: Percutaneous compression plating of intertrochanteric hip fractures. J Orthop Trauma 2000;14:490. [PMID: 11083611]
Gruson K, Aharonoff GB, Egol KA, et al: The relationship between admission hemoglobin level and outcome after hip fracture. J Orthop Trauma 2002;15:39. [PMID: 11782632]
Jaglal S, Lakhani Z, Schatzker J: Reliability, validity and responsiveness of the lower extremity measure for patients with a hip fracture. J Bone Joint Surg Am 2000;82-A:955. [PMID: 10901310]
Kaplan K, Miyamoto R, Levine BR, Egol KA, Zuckerman JD: Surgical management of hip fractures: an evidence-based review of the literature. II: intertrochanteric fractures. J Am Acad Orthop Surg2008;16:665. [PMID:18978289]
Kenny AM, Joseph C, Taxel P, Prestwood KM: Osteoporosis in older men and women. Conn Med 2003;67:481. [PMID: 14587128]
Miyamoto RG, Kaplan KM, Levine BR, Egol KA, Zuckerman JD: Surgical management of hip fractures: an evidence-based review of the literature. I: femoral neck fractures. J Am Acad Orthop Surg2008;16:596. [PMID: 18832603]
Parker MJ, Handoll HH: Pre-operative traction for fractures of the proximal femur. Cochrane Database Syst Rev 2001;3:CD000168. [PMID 11686954]
Parker MJ, Handoll HH, Bhargara A: Conservative versus operative treatment for hip fractures. Cochrane Database Syst Rev 2000;4:CD000337. [PMID 11034683]
Rosen JE, Chen FS, Hiebert R, Koval KJ: Efficacy of preoperative skin traction in hip fracture patients: a prospective randomized study. J Orthop Trauma 2001;15:81. [PMID: 11232658]
Sahin V, Karaka![]() ES, Aksu S, Atlihan D, Turk CY, Halici M: Traumatic dislocation and fracture-dislocation of the hip: a long-term follow-up study. J Trauma 2003;54:520. [PMID: 12634533]
ES, Aksu S, Atlihan D, Turk CY, Halici M: Traumatic dislocation and fracture-dislocation of the hip: a long-term follow-up study. J Trauma 2003;54:520. [PMID: 12634533]
FEMORAL SHAFT FRACTURES
• Fractures between 5 cm distal to the lesser trochanter and 5 cm proximal to the adductor tubercle.
• Closed intramedullary nailing is the standard of care for most of the fractures.
• Associated orthopedic injuries are common.
1. Diaphyseal Fractures (ICD-9:813.20)
Fracture of the shaft of the femur usually occurs as a result of severe trauma. Indirect force, especially torsional stress, is likely to cause spiral fractures that extend proximally or, more commonly, distally into the metaphyseal regions. Most are closed fractures; open fracture is often the result of compounding from within.
![]() Clinical Findings
Clinical Findings
Extensive soft-tissue injury, bleeding, and shock are commonly present with diaphyseal fractures. The most significant features are severe pain in the thigh and deformity of the lower extremity. Hemorrhagic shock may be present, as multiple units of blood may be lost into the thigh, though only moderate swelling may be apparent. Careful radiographic examination in at least two planes is necessary to determine the exact site and configuration of the fracture pattern. The hip and knee should be examined and radiographs obtained to rule out associated injury. Concomitant ipsilateral femoral neck fractures may occur up to 9% of patients and must be suspected and evaluated as ipsilateral ligamentous and meniscal injury of the knee.
Injuries to the sciatic nerve and the superficial femoral artery and vein are uncommon but must be recognized promptly. Hemorrhagic shock and secondary anemia are the most important early complications. Later complications include those of prolonged recumbency, joint stiffness, malunion, nonunion, leg-length discrepancy, and infection.
![]() Classification
Classification
Classically, the fracture is described according to its location, pattern, and comminution. Winquist has proposed a comminution classification that is now widely used.
Type 1: Minimal or no comminution at the fracture site, stable after intramedullary nailing
Type 2: Fracture with comminution leaving at least 50% of the circumference of the two major fragments intact
Type 3: Fracture with comminution of 50–100% of the circumference of the major fragments; nonlocked intramedullary nails do not afford stable fixation
Type 4: Fracture with completely comminuted segmental pattern with no intrinsic stability
![]() Treatment
Treatment
Treatment depends on the age and medical status of the patient as well as the site and configuration of the fracture.
A. Closed Treatment
This remains a treatment option for some skeletally immature patients. Depending on the age of the pediatric patient and the amount of initial displacement at the fracture site, treatment may consist of immediate immobilization in a hip spica cast. In the adult, closed treatment of femoral shaft fractures is rarely indicated. Malalignment and joint stiffness are frequent. Other rare complications are pressure sores due to prolonged recumbency and DVT.
B. Operative Treatment
Reamed, locked, antegrade intramedullary nailing through the piriformis fossa is the gold standard for the treatment for most of the cases. Intramedullary fixation of femoral shaft fractures allows early mobilization of the patient (within 24–48 hours if the fracture fixation is stable), which is of particular benefit to the polytraumatized patient; more anatomic alignment; improved knee and hip function by decreasing the time spent in traction; and a marked decrease in the cost of hospitalization.
Although open nailing procedures have been described, intramedullary fixation is routinely performed closed. Utilization of the novel fluted reamer designs and use of sharp reamers help to avoid thermal necrosis and excessive fat embolization. Despite the theoretic damaging effect of reaming on the fracture healing, reaming allows use of a larger diameter and stronger implant, improves rotational control, and has been shown to reduce the rate of nonunion.
Closed nailing decreases the chance of infection by decreasing the amount of soft-tissue dissection necessary. In most cases, static interlocking should be used to provide rotational control and to prevent shortening of the bone at the fracture site. Dynamic interlocking screws are used at only one end of the nail, and this allows axial compression at the fracture site. Reamed interlocked nailing is recommended for most grade 1, 2, and 3a open fractures. Temporary bony stability may be achieved with external fixation devices when there is extensive soft-tissue loss associated, as in grade 3b and 3c open fractures.
Because of technical problems (eg, choice of a rod length) during the surgery, complications like malalignment or shortening may occur. Nonunions are rare, and one should always suspect deep infections if considered. Infections, leg-length discrepancy, and heterotrophic ossification are other complications after this procedure. The rod may be removed after healing is complete, usually at 12–16 months. Retrograde nailing may be beneficial in some multiply injured trauma patients and morbidly obese and pregnant patients.
Flexible intramedullary rods of the Ender type do not provide sufficient stability in the adult; however, they are routinely used in the pediatric population. Plates and screws require significant soft-tissue dissection and opening of the fracture hematoma and are usually reserved for special cases such as ipsilateral femoral neck and diaphy-seal fractures. External fixation remains indicated in some open fractures. In polytrauma patients, initial external fixation may be indicated when early intramedullary nailing (first 24 hours after trauma) might be potentially hazardous due to hemodynamic instability or head or chest trauma. It has also recently gained acceptance as treatment for closed femoral shaft fractures in children to allow earlier mobilization and decreased hospital stays. The distal fragment pins should always be inserted with the knee in flexion to avoid quadriceps tenodesis that will prevent knee flexion. Superficial pin tract infection is common but rarely involves the bone.
2. Subtrochanteric Fractures (ICD-9:822.22)
• Between lesser trochanter and a point 5 cm distal to the lesser trochanter.
• Frequent site of pathologic fracture.
Subtrochanteric fractures occur below the level of the lesser trochanter and are usually the result of high-energy trauma in young to middle-aged adults. They are often comminuted, with distal or proximal extension toward the greater trochanter. The patient usually presents with a swollen painful proximal thigh with or without shortening or mal-rotation. If the lesser trochanter is intact, the proximal fragment will tend to displace in flexion, external rotation, and abduction because of the unopposed pull of the iliopsoas and abductor muscles.
Recent reports suggest there may be a correlation between bisphosphonate use and low-energy subtrochanteric fractures that radiographically present atypically as transverse or slightly oblique, with medial beaking and marked thickening of the lateral cortex. These fractures typically heal late and necessitate surgical intervention.
The Russell and Taylor classification (Figure 2–18) is a treatment-based classification system that incorporates involvement of the piriformis fossa. Type Ia Russell-Taylor fractures do not involve the piriformis fossa, with the lesser trochanter attached to the proximal fragment. These fractures may be treated with a first-generation intramedullary nail. Type Ib fractures do not involve the piriformis fossa; however, the lesser trochanter is detached from the proximal fragment. These fractures require a second-generation nail, with screw fixation into the head and neck. Type II fractures have fracture extension into the piriformis fossa and are best treated with a sliding hip screw or fixed angle plate.

![]() Figure 2–18. Russell and Taylor classification of subtrochanteric femur fractures. (Reproduced, with permission, from Browner BD, Levine A, Jupiter J, et al, eds: Skeletal Trauma, 2nd ed. New York: WB Saunders; 1998.)
Figure 2–18. Russell and Taylor classification of subtrochanteric femur fractures. (Reproduced, with permission, from Browner BD, Levine A, Jupiter J, et al, eds: Skeletal Trauma, 2nd ed. New York: WB Saunders; 1998.)
In the vast majority of cases, internal fixation (by closed or open methods) is now widely favored. Temporary skeletal traction will maintain femoral length until the definitive surgical procedure can be performed. A variety of devices are available.
Fixation can be obtained with first-generation intramedullary nails, “gamma nails,” intramedullary hip screws, or a variety of cephalomedullary nails or blades and long side plates based on the fracture pattern.
Postoperative activity depends on the adequacy of internal fixation. If fixation is solid, an agile cooperative patient can be out of bed within a few days after surgery and ambulating on crutches with toe-touch weight bearing on the affected side. The fracture is usually healed at 3–4 months, but delayed union and nonunion are not uncommon. Hardware failure is not uncommon. Repeat internal fixation with autogenous bone grafting is then the treatment of choice.
Black DM, Kelly MP, Genant HK, et al: Bisphosphonates and fractures of the subtrochanteric or diaphyseal femur. N Engl J Med 2010;362:1761. [PMID: 20335571]
Brumback RJ, Virkus WW: Intramedullary nailing of the femur: reamed versus nonreamed. J Am Acad Orthop Surg 2000;8:83. [PMID: 10799093]
Das De S, Setiobudi T, Shen L, Das De S: A rational approach to management of alendronate-related subtrochanteric fractures. J Bone Joint Surg Br 2010;92-B:679. [PMID: 20436006]
Dora C, Leunig M, Beck M, et al: Entry point soft tissue damage in antegrade femoral nailing: a cadaver study. J Orthop Trauma 2001;15:488. [PMID: 11602831]
Giannoudis PV, MacDonald DA, Matthews SJ, et al: Nonunion of the femoral diaphysis. J Bone Joint Surg Br 2000;82-B:655. [PMID: 10963160]
Herscovici D, Ricci WM, McAndrews P, et al: Treatment of femoral shaft fracture using unreamed interlocked nails. J Orthop Trauma 2000;14:10. [PMID: 10630796]
Nowotarski PJ, Turen CH, Brumback RJ, et al: Conversion of external fixation to intramedullary nailing for fractures of the shaft of the femur in multiply injured patients. J Bone Joint Surg Am 2000;82-A:2000. [PMID: 1085909]
Ostrum RF, Agarwal A, Lakatos R, et al: Prospective comparison of retrograde and antegrade femoral intramedullary nailing. J Orthop Trauma 2000;14:496. [PMID: 11083612]
Patton JT, Cook RE, Adams CI, et al: Late fracture of the hip after reamed intramedullary nailing of the femur. J Bone Joint Surg Br 2000;82-B:967. [PMID: 11041583]
Ricci WM, Bellabarba C, Lewis R, et al: Angular malalignment after intramedullary nailing of femoral shaft fractures. J Orthop Trauma 2001;15:90. [PMID: 11232660]
Ricci WM, Bellabarba C, Evanoff B, et al: Retrograde versus antegrade nailing of femoral shaft fractures. J Orthop Trauma 2001;15:161. [PMID: 11265005]
Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: damage control orthopedics. J Orthop Trauma 2004;18(8 Suppl):S2. [PMID: 15472561]
Shepherd LE, Shean CJ, Gelalis ID, et al: Prospective randomized study of reamed versus undreamed femoral intramedullary nailing: an assessment of procedures. J Orthop Trauma 2001;15:28. [PMID: 11147684]
Tornetta P, Tiburzi D: Antegrade or retrograde reamed femoral nailing. J Bone Joint Surg Br 2000;82-B:652. [PMID: 10963159]
Tornetta P, Tiburzi D: Reamed versus nonreamed anterograde femoral nailing. J Orthop Trauma 2000;14:15. [PMID: 10630797]
Tornetta P 3rd, Kain MS, Creevy WR: Diagnosis of femoral neck fractures in patients with a femoral shaft fracture. Improvement with a standard protocol. J Bone Joint Surg Am 2007;89:39. [PMID: 17200308]
PATELLAR INJURIES
• Largest sesamoid bone in the body.
• Straight leg test is mandatory to assess extensor mechanism.
• Severe hemarthrosis is common.
1. Transverse Patellar Fracture (ICD-9:822.0)
Transverse fractures of the patella (Figure 2–19) are the result of an indirect force, usually with the knee in flexion. Fracture may be caused by sudden voluntary contraction of the quadriceps muscle or sudden forced flexion of the leg with the quadriceps contracted. The level of fracture is commonly in the middle. Associated tearing of the patellar retinacula depends on the force of the initiating injury. The activity of the quadriceps muscle causes upward displacement of the proximal fragment, the magnitude of which depends on the extent of the retinacular tear.

![]() Figure 2–19. Transverse fracture of the patella. (Reprinted from Canale ST, ed: Campbells Operative Orthopaedics, 9th ed. Vol. 3. Copyright 1998, Mosby, with permission from Elsevier.)
Figure 2–19. Transverse fracture of the patella. (Reprinted from Canale ST, ed: Campbells Operative Orthopaedics, 9th ed. Vol. 3. Copyright 1998, Mosby, with permission from Elsevier.)
![]() Clinical Findings
Clinical Findings
Swelling of the anterior knee region is caused by hemarthrosis and hemorrhage into the soft tissues overlying the joint. If displacement is present, the defect in the patella can be palpated, and active extension of the knee is lost. A straight leg raise may be preserved if the retinaculum is intact.
![]() Treatment
Treatment
Nondisplaced fractures can be treated with a walking cylinder cast or brace for 6–8 weeks followed by knee rehabilitation. Open reduction is indicated if the fragments are displaced more than 3 mm or if articular step-off is more than 2 mm. The fragments must be accurately repositioned to prevent early posttraumatic arthritis of the patellofemoral joint. If the minor fragment is small (no more than 1 cm in length) or severely comminuted, it may be excised and the quadriceps or patellar tendon (depending on which pole of the patella is involved) sutured directly to the major fragment. Whenever possible, internal fixation of anatomically reduced fragments should be done, allowing early motion of the knee joint. This is best achieved by figure-of-8 tension banding over two longitudinal parallel K-wires or cannulated screws. Accurate reduction of the articular surface must be confirmed by lateral radiographs taken intraoperatively.
2. Comminuted Patellar Fracture (ICD-9:822.0)
Comminuted fractures of the patella are usually caused by a direct force. Severe injury may cause extensive destruction of the articular surface of both the patella and the opposing femur.
If comminution is not severe and displacement is insignificant, immobilization for 8 weeks in a cylinder extending from the groin to the supramalleolar region is sufficient.
Severe comminution can often be treated with ORIF with addition of a cerclage wire, but on rare occasions, excision of the patella with repair of the defect by imbrication of the quadriceps expansion is the only viable alternative. Excision of the patella can result in decreased strength, pain in the knee, and general restriction of activity. No matter what the treatment, high-energy injuries are frequently complicated by chondromalacia patella and patellofemoral arthritis.
3. Patellar Dislocation (ICD-9:836.3)
Acute traumatic dislocation of the patella should be differentiated from episodic recurrent dislocation, because the latter condition is likely to be associated with occult organic lesions. When dislocation of the patella occurs alone, it may be caused by a direct force or activity of the quadriceps, and the direction of dislocation of the patella is almost always lateral. Spontaneous reduction is apt to occur if the knee joint is extended. If so, the clinical findings may consist merely of hemarthrosis and localized tenderness over the medial patellar retinaculum. Gross instability of the patella, which can be demonstrated by physical examination, indicates that injury to the soft tissues of the medial aspect of the knee has been extensive. Balcarek et al found that 98.6% of the patients who had lateral patella dislocations also had medial patellofemoral ligament injuries, with a complete tear in 51.4% of cases and injuries most frequently localized at the femoral attachment site.
Reduction is maintained in a brace or cylinder cast with the knee in extension for 2–3 weeks. Isometric quadriceps exercises are encouraged. Physical therapy should be initiated to maximize the strength of the vastus medialis. Dynamic bracing may be helpful. Recurrent episodes require operative repair for effective treatment.
4. Tear of the Quadriceps Tendon (ICD-9:727.65)
Tear of the quadriceps tendon occurs most often in patients over the age of 40. Apparent tears that represent avulsions from the patella occur in patients with renal osteodystrophy or hyperparathyroidism. Preexisting attritional disease of the tendon is apt to be present, and the causative injury may be minor.
Swelling is caused by hemarthrosis and extravasation of blood into the soft tissues. The patient is unable to extend the knee completely. Radiographs may show a bony avulsion from the superior pole of the patella if a small flake of bone is avulsed from the superior pole of the patella.
Operative repair is recommended for complete tear. Postoperative immobilization should be encouraged in a walking cylinder cast or brace for 6 weeks, at which time knee mobilization is started.
5. Tear of the Patellar Tendon (ICD-9:727.66)
The same mechanism that causes tears of the quadriceps tendon, transverse fracture of the patella, or avulsion of the tibial tuberosity may also cause the patellar ligament to tear. The characteristic finding is proximal displacement of the patella. A bony avulsion may be present adjacent to the lower pole of the patella if the tear takes place in the proximal patellar tendon.
Operative treatment is necessary for a complete tear. The ligament is resutured to the patella, and any tear in the quadriceps mechanism is repaired. The extremity should be immobilized for 6–8 weeks in a cylinder cast extending from the groin to the supramalleolar region. Guarded exercises may then be started.
Balcarek P, Ammon J, Frosch S, et al: Magnetic resonance imaging characteristics of the medial patellofemoral ligament lesion in acute lateral patellar dislocations considering trochlear dysplasia, patella alta, and tibial tuberosity-trochlear groove distance. Arthroscopy 2010;26:926. [PMID: 20620792]
Jutson JJ, Zych GA: Treatment of comminuted intraarticular distal femur fractures with limited internal and external tensioned wire fixation. J Orthop Trauma 2000;14:405. [PMID: 1100141])
Meyer RW, Plaxton NA, Postak PD, et al: Mechanical comparison of a distal femoral side plate and a retrograde intramedullary nail. J Orthop Trauma 2000;14:398. [PMID: 11001413]
Stahelin T, Hardegger F, Ward JC: Supracondylar osteotomy of the femur with use of compression. J Bone Joint Surg 2000; 82-A:712. [PMID: 10819282]
Woo SL, Vogrin TM, Abramowitch SD: Healing and repair of ligament injuries in the knee. J Am Acad Orthop Surg 2000;8:364. [PMID: 11104400]
DISTAL FEMUR FRACTURES (ICD-9:821.23)
• Account for 7% of all femur fractures.
• Important to distinguish between supracondylar and articular fractures.
• Increasingly seen as periprosthetic fractures.
These fractures involve the distal 10–15 cm of the femur and are usually seen as low-energy fractures in the elderly and high-energy fractures in young patients. The distal fragment is usually rotated into extension from traction by the gastrocnemius muscle. The distal end of the proximal fragment is apt to perforate the overlying quadriceps and may penetrate the suprapatellar pouch, causing hemarthrosis. The distal fragment may impinge on the popliteal neurovascular bundle, and an immediate thorough neurovascular examination is mandatory. Absence or marked decrease of pedal pulsations is an indication for immediate reduction. If this fails to restore adequate circulation, an arteriogram should be obtained immediately and the vascular lesion repaired as indicated. Injuries to the tibial or peroneal nerves are less frequent. Treatment should be aimed at restoring the mechanical axis, anatomic reduction of the articular surface, and early knee range of motion.
A temporary spanning external fixation can be used to stabilize the fracture in polytrauma patients. Two pins can be rapidly allocated in the femoral shaft and two additional pins in the tibial shaft. ORIF can be safely done in the first 2 weeks when the patient has been hemodynamically stabilized without increasing the risk of infection, provided that no infection at the pin sites has occurred. Complex trauma of the knee encompasses a distal supra- or intercondylar femoral fracture combined with a proximal tibial fracture (floating knee); a supra- or intercondylar femoral fracture with a second- or third-degree closed or open injury; or a complete knee dislocation and possible associated neurovascular injuries. Because of the complexity of injury and multidisciplinary team approach, this subset of patients is better treated in level 1 trauma centers.
Most extraarticular fractures are best treated with internal fixation: fixed-angle plates, locking plates using minimally invasive percutaneous plate osteosynthesis (MIPPO) techniques, or retrograde intramedullary nailing. Skeletal traction treatment is reserved for patients for whom surgery is contraindicated.
As for any intraarticular fracture, maximal functional recovery of the knee joint requires anatomic reduction of the articular components and restitution of the mechanical axis. Closed reduction of displaced fragments is almost never successful. Displaced intraarticular fractures usually require ORIF with a variety of methods including dynamic compression screws, AO buttress plating, and less invasive stabilization system (LISS), with or without MIPPO.
According to the configuration of the articular fragments, displaced T- or Y-type fractures of the distal femoral epiphysis are best treated by open reduction. Even if the fracture heals in anatomic position, joint stiffness, pain, and posttraumatic arthritis are not uncommon outcomes.
Isolated fractures of the lateral or medial femoral condyles are rare and usually associated with ligament injury. They usually result from varus or valgus stress to the knee joint. Fractures of the posterior portion of one or the other condyle in the frontal plane can also be seen (Hoffa fracture).
ORIF is usually indicated and requires anteroposterior lag screws. Associated ligamentous ruptures are repaired as needed. If fixation is solid, postoperative immobilization is kept at a minimum, and the patient can start moving the knee joint early. Weight bearing is usually allowed at 3 months when clinical and radiologic evidence of bone healing is present.
INJURIES AROUND THE KNEE
![]() Anatomy and Biomechanical Principles
Anatomy and Biomechanical Principles
The knee is a modified synovial hinge joint formed by three bones: the distal femur, the proximal tibia, and the patella. It is often divided into three compartments: medial, lateral, and patellofemoral.
The distal femoral diaphysis broadens into two curved condyles at the metaphyseal junction. Each condyle is convex and articulates distally with its corresponding tibial plateau. Their articular surfaces join anteriorly to articulate with the patella. Posteriorly, they remain separate to form the intercondylar notch. The lateral condyle is wider in the sagittal plane (preventing lateral patella displacement) and extends further proximally. The medial condyle is narrower but extends further distally. This difference in length of both condyles allows for the distance between both knees, when weight bearing, to be smaller than the distance between both hips. Both condylar surfaces form a horizontal plane parallel to the ground and create an anatomic angle (physiologic valgus position) of 5–7 degrees with the femoral shaft. Normally, the centers of the hip, knee, and ankle joints are all aligned to form a mechanical angle of 0 degrees. The supracondylar area of the femur is defined as the distal 9 cm. Fractures proximal to this are considered femoral shaft fractures and carry a different prognosis.
As for the distal femur, the proximal tibia widens proximally at the diaphyseal-metaphyseal junction to form the medial and lateral tibial plateaus (condyles). There is a 7- to 10-degree slope from anterior to posterior of the tibial plateaus. The tibial eminence, with its medial and lateral spines, separates both compartments and is the attachment for the cruciate ligaments and the menisci. Distal to the joint itself, the tibia has two prominences: the tibial tubercle anteriorly, where the patellar tendon attaches, and Gerdy’s tubercle anterolaterally, where the iliotibial band inserts. Posterolaterally, the under surface of the tibial condyle articulates with the fibular head to form the proximal tibiofibular joint.
The patella is the biggest sesamoid bone in the body. It lies within the substance of the quadriceps tendon. The distal third of the under surface is nonarticular and provides attachment for the patellar tendon. The proximal two thirds articulates with the anterior surface of the femoral condyles and is divided into medial and lateral facets by a longitudinal ridge. The area of contact at the patellofemoral joint varies according to the degree of knee flexion. On each side of the patella are the medial and lateral retinacular expansions formed by fibers of the vastus medialis and vastus late-ralis muscles. These expansions bypass the patella to insert directly on the tibia. When intact, they can allow active knee extension even in the presence of a fractured patella. The blood supply to the patella is derived from anastomosis of the genicular vessels from the distal pole proximally. Avascular necrosis of a proximal fracture fragment is not uncommon.
The main plane of motion of the knee is flexion and extension, but physiologically, internal and external rotation, abduction and adduction (varus and valgus), and anterior and posterior translations also occur. The intrinsic bony configuration of the joint affords little stability. A complex soft-tissue network provides joint stability under physiologic loading. It includes passive stabilizers, such as medial and lateral collateral ligaments, medial and lateral menisci, anterior and posterior cruciate ligaments, and joint capsule, and active stabilizers, such as the extensor mechanism, the popliteus muscle, and the hamstrings with their capsular expansions. All these soft-tissue components work together in an extremely complex and finely tuned way to prevent excessive displacement of the joint surfaces throughout the full arc of motion under physiologic loading. When abnormal stresses that exceed the soft tissues’ ability to resist them are transmitted across the joint, an infinite range of injuries can occur. These may be isolated or combined, partial or complete, and may or may not be associated with bony injuries. An accurate diagnosis, although sometimes difficult, is essential before the appropriate treatment can be decided upon.
LIGAMENTOUS INJURIES
• Associated injuries to bone, cartilage, and menisci are common.
• Knowledge of the mechanism of injury is of paramount importance, as certain injury patterns may be anticipated.
• Grade 1 and 2 medial collateral injuries can be treated conservatively.
An efficient clinical examination is sometimes difficult, because patients guard examinations due to pain in the acute phase and these are generally young muscular athletes with a large lower extremity, but clinical examination is essential and will usually provide key diagnostic information.
Plain radiographs are of limited benefit. They will show fractures, bony avulsions at ligament attachment sites, or capsular avulsions.
MRI is now by far the imaging tool of choice for ligamentous injuries of the knee, with an accuracy rate above 95%. Diagnostic arthroscopy is now reserved for cases when MRI is inconclusive or the surgeon is fairly sure that surgical treatment of a lesion will be necessary.
1. Medial (Tibial) Collateral Ligament Injury (ICD-9:844.1)
This ligament normally resists valgus angulation at the knee joint. It is the most commonly seen isolated ligament injury and generally seen in the young athletic population. A history of abduction injury, often with an external torsional component, is usually obtained. Examination reveals tenderness over the site of the lesion and often some knee effusion. When compared with the contralateral knee, valgus stressing with the knee flexed at 20–30 degrees will show exaggerated laxity at the joint line, signaling a complete tear. The subjective gapping on the medial joint line during valgus applied force at 30 degrees of knee flexion is used for grading these injuries (Table 2–6). Stress radiographs can, on rare occasions, be useful in confirming the diagnosis.
Table 2–6. Subjective gapping of the medial joint line during valgus applied force at 30 degrees of knee flexion.

Grade 1 and 2 sprains (incomplete) are treated with protective weight bearing in a hinged brace or cast to prevent further injury while healing progresses. Grade 3 sprains (complete) are rarely isolated. Known associated injuries, such as medial meniscus damage, anterior cruciate ligament (ACL) tear, or lateral tibial plateau fractures, should be systematically ruled out. Most surgeons now favor conservative treatment of isolated grade 3 medial collateral ligament tears in a long leg hinged-knee brace for 4–6 weeks. Concomitant ACL injuries determine the success of treatment for these injuries.
2. Lateral (Fibular) Collateral Ligament Injury (ICD-9:844.0)
This ligament originates from the lateral femoral condyle and inserts on the fibular head. It is the primary static varus stabilizer of the knee joint. Isolated injuries are extremely rare. Most often, there is a combination of varying degrees of injury to the posterolateral corner (PLC), which includes the biceps tendon, posterolateral capsule, popliteus tendon, and iliotibial band. Associated ACL and posterior cruciate ligament injuries are more common than isolated injuries. Injury to the peroneal nerve can be seen. Pain and tenderness are present over the lateral aspect of the knee, usually with some intraarticular effusion. A through physical examination combined with plain x-ray and MRI is paramount for diagnosis. ACL and posterior cruciate ligament reconstructions often fail in the presence of an unrecognized fibular collateral or PLC injury. Varus stress radiographs are useful for detecting these injuries. In severe injuries, there is abnormal laxity on varus stressing at 0 and 30 degrees of flexion, compared with the other knee.
When there is an avulsion of the fibular head and this fragment is of sufficient size, internal fixation with a screw gives excellent results. Most injuries require operative treatment. Immediate repair or primary reconstruction in the acute setting gives better results than late reconstruction.
3. Anterior Cruciate Ligament Injury (ICD-9:844.2)
This ligament originates at the posteromedial aspect of the lateral femoral condyle and inserts near the medial tibial spine. Because it is composed of at least two distinct fiber bundles, part of it remains taut throughout the normal flexion-extension arc of motion. It prevents anterior translation (gliding) of the tibia under the femoral condyles. Isolated injuries are frequent, especially with hyperextension mechanism, as seen in skiers, volleyball players, or basketball players. Valgus, flexion, external rotation injury results in damage to the medial collateral ligament, medial meniscus, and ACL (the terrible triad). When the tear is complete, it most often occurs within the substance of its fibers. Rarely, bony avulsion at the femoral or tibial attachment will be seen on plain radiograms. Associated medial collateral ligament, medial meniscus, posteromedial capsule, and even posterior cruciate ligament injuries are more common.
![]() Clinical Findings
Clinical Findings
The patient usually recalls the mechanism of injury and classically feels a popping or snapping sensation in the knee. A moderate effusion usually accumulates during the first few hours. The only clinical finding in acute ACL deficiency may be a positive Lachman test, which is the anterior drawer test performed with 20–30 degrees of knee flexion. The classic drawer test, done with the knee flexed at 90 degrees and the foot resting on the table, is not as reliable. The injured knee should always be compared with the uninjured contralateral knee. In chronic ACL deficiency, secondary restraints have stretched out and other clinical signs, such as the pivot shift and the active drawer sign, become more apparent.
![]() Treatment
Treatment
Despite the fact that ACL reconstruction does not prevent osteoarthritis, ACL deficiency causes knee pain, functional impairment, and an increased risk of meniscus tear and early knee osteoarthritis. Although surgical reconstruction is indicated in most instances, functionally stable knees can be managed conservatively with rehabilitation therapy and bracing. Patients who remain unacceptably unstable after conservative treatment can still benefit from delayed reconstructive surgery. When bony avulsions from the femur or tibia are present, surgical repair is indicated, as bone-to-bone healing and good long-term results have been demonstrated. Primary repair of the ligament stumps without reconstruction is likely to fail. Arthroscopically assisted reconstruction with the middle third of the patellar tendon or harvest of an autogenous hamstrings graft gives excellent results. Recently, there has been a trend to perform anatomic double-bundle repairs and single-bundle reconstruction through an anteromedial portal.
4. Posterior Cruciate Ligament Injury (ICD-9:844.2)
The posterior cruciate ligament is a broad thick ligament that extends from the lateral aspect of the medial femoral condyle posteriorly and inserts extraarticularly over the back of the tibial plateau approximately 1 cm below the joint line. It resists posterior translation (gliding) of the tibia under the femoral condyle. It usually ruptures after a posteriorly directed force on the proximal tibia as is sometimes seen in dashboard injuries. Posterior cruciate ligament ruptures can also occur as the end stage of severe hyperextension injuries.
![]() Clinical Findings
Clinical Findings
The posterior drawer test will be positive, as will the sag test, showing posterior sagging of the tibia with the knee flexed to 90 degrees compared with the opposite side. As for the ACL, the rupture may be at the bone–ligament junction or more often in the middle substance of the ligament.
![]() Treatment
Treatment
Most isolated posterior cruciate ligament tears can be treated successfully with conservative treatment with rehabilitation (ie, reducing inflammation, strengthening extensor mechanism, regaining knee motion, and gradual return to sports within 3–6 weeks). If the posterior tibial translation compared with that of the contralateral knee is over 10 mm, there is associated PLC injury and surgical treatment is recommended.
5. Meniscal Injury (ICD-9:836.0, 1, 2)
The meniscus is a fibrocartilage that allows a more congruous fit between the convex femoral condyle and the flat tibial plateau. Both medial and lateral menisci are attached peripherally and have a central free border. They are wedge-shaped and thicker at the periphery. The medial meniscus is C-shaped, and the lateral meniscus is O-shaped, with both anterior and posterior horns almost touching medially. They are vascularized only at their peripheral third. Tears involving that vascularized portion have a better repair potential. The menisci spread the load more uniformly on the underlying cartilage, thus minimizing point contact and wear. They are secondary knee stabilizers but are more important in the ligament-deficient knee.
![]() Clinical Findings
Clinical Findings
Tears can be secondary to trauma or attrition. The medial meniscus is more often involved. Symptoms include pain, swelling, a popping sensation, and occasionally locking and giving way. Examination usually reveals nonspecific medial or lateral joint-line pain, and occasionally grinding or snapping can be felt with tibial torsion and the knee flexed to 90 degrees (McMurray sign). Radiographs are of minimal value but may rule out other disorders; MRI has replaced contrast arthrography as the diagnostic tool of choice.
![]() Treatment
Treatment
Initial conservative management with immobilization, bracing, protective weight bearing, and exercises can give good results. Arthroscopic evaluation and treatment are recommended for recurrent or persistent locking, recurrent effusion, or disabling pain. If the tear is large enough and in the vascularized portion, repair should be attempted. For other tears, the affected area should be removed, leaving as much as possible of the healthy meniscus. Routine total meniscectomy has been abandoned because of the high incidence of subsequent arthritis.
6. Chondral and Osteochondral Injuries (ICD-9:733.92)
The hyaline articular cartilage is avascular and has no intrinsic capability to repair superficial lacerations. Deep injuries involve the bone in the subchondral plate, and extrinsic repair occurs first with a fibrin clot replaced by granulation tissue, which is then transformed to fibrocartilage. Repetitive injury can cause abnormal motion with shearing stresses that can loosen chondral or osteochondral fragments. Compression injuries to the cartilage can lead to posttraumatic chondromalacia.
![]() Clinical Findings
Clinical Findings
Chondral injuries usually give nonspecific symptoms that mimic meniscal injury. Plain radiographs will often reveal a loose body if the osteochondral fragment is big enough. Tunnel views and patellar tangential views can be helpful in visualizing fragments. Although it can miss the delaminating injuries, superficial flap tears, and surface fibrillations, MRI is the optimal diagnostic tool for articular lesions. However, arthroscopy remains the most accurate diagnostic procedure.
![]() Treatment
Treatment
Debridement, fixation of the osteochondral fragment, bone marrow stimulation, which is excision of the free fragment, debridement of the donor site, microfracture or drilling of the underlying subchondral bone to promote fibrin clot formation, mosaicplasty, and autologous chondrocyte implantation with or without using a scaffold are the most common treatment options. Selection of the treatment depends on the age of the patient, size of the defect, skeletal maturity, and presence of adequate subchondral bone. After the surgery, gaining preoperative function usually takes months depending on the extent of the articular damage.
7. Knee Dislocation (ICD-9:836.5)
Traumatic dislocation of the knee is a rare injury that often results from high-energy trauma but may occur from low-energy injuries in the elderly. It is classified according to the direction of displacement of the tibia: anterior, posterior, lateral, medial, or rotatory. Complete dislocation can occur only after extensive tearing of the supporting ligaments and soft tissues. Injury to the neighboring neurovascular bundle is common and should be looked for systematically.
![]() Treatment
Treatment
Knee dislocations require prompt reduction. This is most easily accomplished in the emergency room by applying axial traction on the leg. Rarely, reduction can only be obtained under general anesthesia. The role of angiography is controversial. If pulses and ankle-brachial pressure index are normal, the limb is closely observed. Studies have shown that the isolated presence of abnormal foot pulses is not sensitive enough to detect a surgical vascular injury. Furthermore, one study demonstrated no vascular injury in any of their traumatic knee dislocations with initial normal vascular examination. Angiograms can be useful in the limb with obvious vascular injury but should not delay treatment. Any vascular injury should be repaired as soon as possible. Ischemia of more than 4 hours implies a poor prognosis for salvage of a functional limb. Prophylactic fasciotomies should be performed at the time of vascular repair to prevent compartment syndrome caused by postrevascularization edema.
Most authors now agree that surgical repair of all ligaments is indicated in relatively young (<50 years) active patients. Early reconstructions yield better results. Open dislocations, irreducible dislocations, and popliteal artery damage necessitate immediate surgical treatment.
Intensive quadriceps and hamstring rehabilitation is necessary to minimize functional loss. The need for a brace for strenuous activities may be permanent.
PROXIMAL TIBIA FRACTURES (ICD-9:823.0)
1. Tibial Plateau Fractures (ICD-9:823.00)
• Tibia plateau represents a spectrum of intraarticular injuries with a wide variety of injury patterns.
• Regardless of the treatment choice, posttraumatic osteoarthritic changes are common.
Proximal tibia plateau fractures account for 1% of all fractures. Lateral tibial plateau fractures account for 60% of plateau fractures. Like other metaphyseal fractures, impaction injury creates a void of structural bone loss. These fractures commonly result from axial loading, combined with varus and valgus force. Associated meniscal and ligamentous injuries are common. Using MRI, Gardner et al showed that 91% of patients had evidence of lateral meniscus pathology, 44% had medial tears, 57% had ACL injuries, and 68% had pathology in the posterolateral corner. A thorough neurovascular evaluation should also be recorded as high-energy fractures and fracture-dislocations can be associated with a popliteal artery injury.
![]() Classification
Classification
Many different classification systems have been proposed, none with universal acceptance. The most widely used system is the Schatzker classification: type I, split fracture of the lateral plateau; type II, split-depression of the lateral plateau; type III, depression of the lateral plateau; type IV, medial plateau fracture; type V, bicondylar fracture; and type VI, a fracture with metaphyseal-diaphyseal dissociation (Figure 2–20). Proper classification is based on quality radiographs, including oblique views if necessary. CT and three-dimensional CT have become an important adjuvant for preoperative planning and evaluating postoperative reductions. MRI is useful for the identification of associated soft-tissue injuries.

![]() Figure 2–20. Schatzker classification of tibial plateau fractures: A, type I: lateral split; B, type II: lateral split depression; C, type III: lateral depression; D, type IV: medial plateau; E, type V: bicondylar; F, type VI: bicondylar with separation of metaphysis from diaphysis. (Reproduced, with permission, from Rockwood CA, Green DP, Bucholz RW, et al, eds: Fractures in Adults, 4th ed. Philadelphia: Lippincott; 1996.)
Figure 2–20. Schatzker classification of tibial plateau fractures: A, type I: lateral split; B, type II: lateral split depression; C, type III: lateral depression; D, type IV: medial plateau; E, type V: bicondylar; F, type VI: bicondylar with separation of metaphysis from diaphysis. (Reproduced, with permission, from Rockwood CA, Green DP, Bucholz RW, et al, eds: Fractures in Adults, 4th ed. Philadelphia: Lippincott; 1996.)
![]() Treatment
Treatment
The goal of treatment is to restore the anatomic contours of the articular surface, facilitate soft-tissue healing, and prevent knee stiffness. Both closed and open treatment can achieve these goals. The choice will depend on multiple factors, including the patient’s age and general medical condition, the degree of displacement and comminution of the fracture, associated local soft-tissue and bony injuries, local skin condition, residual knee stability, and fracture configuration.
Closed treatment with a functional brace is appropriate for minimally displaced fractures with stable ligaments. Varus and valgus laxity at full extension is a poor prognostic sign for closed treatment. Articular step-offs of 3 mm or less and condylar widening of 5 mm or less can be treated conservatively. Lateral or valgus tilt up to 5 degrees is well tolerated. Medial plateau fractures with any significant displacement should be surgically stabilized due to the propensity for further displacement. Bicondylar fractures with any medial displacement, valgus tilt of more than 5 degrees, or significant articular step-off should be surgically stabilized. Immediate range of motion is usually encouraged with protected weight bearing at 8–12 weeks. Noncomminuted fractures can undergo closed reduction with fluoroscopic imaging and percutaneous screw placement.
ORIF with plates and screws remains an effective operative treatment. Reduction should be as anatomically precise as possible, and fixation should be solid enough to allow early mobilization. More recently, minimally invasive plate osteosynthesis (MIPO) is being used in the treatment of these injuries. Bone defects should be grafted with auto-graft, allograft, or structural graft substitutes. Early range of motion is allowed according to the stability of the construct. Open surgery should only be undertaken when the soft tissues are minimally swollen; for unstable fractures, temporary external fixation with delayed definitive surgery has been shown to be safe and effective.
External monolateral or ring fixator can be used for provisional and definitive treatment depending on the clinical situation and experience of the surgical team. The proximal pin in the tibia must be no closer than 14 mm to the joint line to prevent septic arthritis. Hybrid and ring external fixators have been found to be useful for bicondylar injuries with severe soft-tissue trauma.
Bai B, Kummer FJ, Sala DA, et al: Effect of articular step-off and meniscectomy on joint alignment and contact pressures for fractures of the lateral tibial plateau. J Orthop Trauma 2001;15:101. [PMID: 11232647]
Bedi A, Feeley BT, Williams RJ 3rd: Management of articular cartilage defects of the knee. J Bone Joint Surg Am 2010;92:994. [PMID: 20360528]
Cain EL, Clancy WG: Treatment algorithm for osteochondral injuries of the knee. Clin Sports Med 2001;20:321. [PMID: 11398361]
Chen FS, Rokito AS, Pitman MI: Acute and chronic posterolateral rotatory instability of the knee. J Am Acad Orthop Surg 2000;8:97. [PMID: 1075373]
Collinge CA, Sanders RW: Percutaneous plating in the lower extremity. J Am Acad Orthop Surg 2000;8:211. [PMID: 10951109]
Fanelli GC, Stannard JP, Stuart MJ, et al: Management of complex knee ligament injuries. J Bone Joint Surg Am 2010;92:2235. [PMID: 20844167]
Gardner MJ, Yacoubian S, Geller D, et al: The incidence of soft tissue injury in operative tibial plateau fractures: a magnetic resonance imaging analysis of 103 patients. J Orthop Trauma 2005;19:79. [PMID: 15677922]
Geller J, Tornetta P 3rd, Tiburzi D, et al: Tension wire position for hybrid external fixation of the proximal tibia. J Orthop Trauma 2000;14:502. [PMID: 11083613]
Griffin LY, Agel J, Albohm MJ, et al: Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies. J Am Acad Orthop Surg 2000;8:141. [PMID: 10874221]
Kumar A, Whittle AP: Treatment of complex (Schatzker type VI) fractures of the tibial plateau with circular wire external fixation: a retrospective case review. J Orthop Trauma 2000;14:339. [PMID: 10926241]
Larsson S, Bauer TW: Use of injectable calcium phosphate cement for fracture fixation: a review. Clin Orthop Relat Res 2002;395:23. [PMID: 11937863]
Levy BA, Dajani KA, Whelan DB, et al: Decision making in the multiligament-injured knee: an evidence-based systematic review. Arthroscopy 2009;25:430. [PMID: 19341932]
Lundy DW, Johnson KD: “Floating knee” injuries: ipsilateral fractures of the femur and tibia. J Am Acad Orthop Surg 2001;9:238. [PMID: 11476533]
Matava MJ, Ellis E, Gruber B: Surgical treatment of posterior cruciate ligament tears: an evolving technique. J Am Acad Orthop Surg 2009;17:435. [PMID: 19571299]
Ranawat A, Baker CL 3rd, Henry S, Harner CD: Posterolateral corner injury of the knee: evaluation and management. J Am Acad Orthop Surg 2008;16:506. [PMID: 18768708]
Stevens DG, Beharry R, McKee MD, et al: The long-term functional outcome of operatively treated tibial plateau fractures. J Orthop Trauma 2001;15:312. [PMID: 11433134]
Wijdicks CA, Griffith CJ, Johansen S, Engebretsen L, LaPrade RF: Injuries to the medial collateral ligament and associated medial structures of the knee. J Bone Joint Surg Am 2010;92:1266. [PMID: 20439679]
Yacoubian SV, Nevins R, Sallis J, et al: Impact of MRI on treatment plan and fracture classification of tibial plateau fractures. J Orthop Trauma 2002;16:632. [PMID 12368643]
![]() Complications
Complications
Early complications of tibia plateau fracture management include infection, DVT, compartment syndrome, loss of reduction, and hardware failure. Late complications include residual instability and posttraumatic degenerative joint disease that may require total knee replacement arthroplasty or arthrodesis.
2. Tibial Tuberosity Fracture (ICD-9:823-02)
Tibial tuberosity fractures can occur with a violent quadriceps muscle contraction causing avulsion of the tibial tuberosity. When the fracture is complete, the extensor mechanism is disrupted and active knee extension is impossible.
Although conservative treatment of a nondisplaced avulsion fracture with a cylinder cast in extension for 6–8 weeks will allow it to heal, rigid screw fixation permits earlier knee mobilization. Closed or open reduction with internal fixation is recommended for all fractures displaced by 5 mm or more.
3. Tibial Eminence (Spine) Fracture (ICD-9:823.80)
A tibial eminence fracture occurs as an isolated injury or as part of the comminution of tibial plateau fractures. The isolated type of injury occurs mostly in the pediatric population. Meniscal, capsular, or collateral ligament or osteochondral injuries are seen in up to 40% of patients.
Meyers has classified this lesion into three types. Nondisplaced type 1 can be treated nonsurgically with a cylinder cast with the knee in extension for 6 weeks. Type 2 is displaced in the anterior margin and can be treated nonsurgically if anatomic reduction is achieved with a cast. Type 3 fractures should be surgically fixed. Permanent or absorbable sutures, K-wire, or screws can be used for fixation. When associated with other fractures of the tibial plateau, the tibial eminence fragment usually keeps its attachment to the anterior cruciate ligament, and anatomic reduction with rigid fixation should be obtained.
TIBIA AND FIBULA INJURIES
• Tibia fracture is the most common long bone fracture.
• Due to the subcutaneous location of the anteromedial tibia, open fractures occur in high incidence.
• The treating physician must be aware of the clinical signs of compartment syndrome.
![]() Anatomy
Anatomy
The tibial diaphysis is straight and triangular in cross-section. Its anteromedial border and anterior crest are palpable throughout the entire length of the bone and are useful landmarks for closed reduction techniques and cast molding with pressure relief, as are the palpable fibular head, distal third of the fibula, medial malleolus, and patellar tendon. The distal half of the leg has more tendons and less muscle than the proximal half, and thus soft-tissue coverage and blood supply of the distal tibia are more precarious than in the proximal portion. The fibula transmits approximately one sixth of the axial load from the knee to the foot and the tibia five sixths.
From a surgical standpoint, the leg is divided into four fascial compartments. A compartment is defined by the unyielding boundaries, such as bone and fascia, enclosing a group of muscles. The anterior compartment is limited medially by the tibia, posteriorly by the interosseous membrane, laterally by the fibula, and anteriorly by the crural fascia. The anterior compartment contains the tibialis anterior, extensor hallucis longus, extensor digitorum longus, and peroneus tertius muscles, responsible for ankle and toe extension, as well as the anterior tibial artery and the deep branch of the peroneal nerve. The lateral compartment contains the peroneus brevis and longus muscles responsible for ankle flexion and foot eversion and the superficial branch of the peroneal nerve. The superficial posterior compartment contains the gastrocnemius, soleus, plantaris, and popliteus muscles and the sural nerve. The deep posterior compartment is enclosed by the tibia, the interosseous membrane, and the deep transverse fascia and contains the tibialis posterior, flexor hallucis longus, flexor digitorum longus muscles, and posterior tibial and peroneal arteries and the tibial nerve.
1. Tib-Fib Fractures (ICD-9:823.22)
Fractures of the tibial or fibular diaphysis are the result of direct or indirect trauma, with some of these injuries being open fractures. A thorough assessment of the surrounding soft tissues is mandatory. One must remember that the size of the skin wound does not necessarily correlate with the amount of underlying soft-tissue damage. A 1-cm skin laceration can be associated with an extensive muscle and periosteal injury, making the fracture a Gustilo grade III instead of I, with a much poorer prognosis. Also, closed tibia fractures can be associated with significant soft-tissue injury. In 1982, Tscherne and Oestern classified the soft-tissue injury in ascending order of severity (grades 0–3):
Grade 0: Soft-tissue damage is absent or negligible.
Grade 1: There is a superficial abrasion or contusion caused by fragment pressure from within.
Grade 2: A deep contaminated abrasion is present associated with localized skin or muscle contusion from direct trauma. Impending compartment syndrome is included in this category.
Grade 3: The skin is extensively contused or crushed, and muscular damage may be severe. Subcutaneous avulsions, compartment syndrome, and rupture of a major blood vessel associated with a closed fracture are additional criteria.
When the fracture is displaced, the clinical diagnosis is usually evident. All compartments should be palpated, and a thorough distal neurovascular examination should be recorded.
Radiographs in the AP and lateral projections are taken of the entire leg, including the knee and ankle joints. Oblique views are sometimes necessary. Fractures of the distal end of the tibia (pilon or plafond fractures) can be better visualized with CT scanning.
![]() Fibula Diaphysis Fractures (ICD-9:823.21)
Fibula Diaphysis Fractures (ICD-9:823.21)
Isolated fibula fractures can be associated with other injuries of the leg, such as fracture of the tibia or fracture-dislocation of the ankle joint. One should pay particular attention to the medial malleolus to rule out deltoid ligament rupture or medial malleolus fracture. Isolated fibula fracture can be the result of a direct blow; however, it can also coincide with syndesmosis disruption. If reduction of the mortise is congruent, radiographic follow-up is needed to ensure maintenance of reduction.
![]() Tibia Diaphyseal Fractures (ICD-9:823.20)
Tibia Diaphyseal Fractures (ICD-9:823.20)
Isolated fractures of the tibial diaphysis are usually the result of torsional stress. There is a tendency for the tibia to displace into varus angulation because of an intact fibula.
Fractures of both the tibia and fibula are more unstable, and displacement can recur after reduction. The fibular fracture usually heals independently of the reduction achieved. The same does not apply to the tibia. There is some controversy as to what is an acceptable reduction of a tibial shaft fracture in the adult. The following criteria are generally accepted: apposition of 50% or more of the diameter of the bone in both AP and lateral projections, no more than 5 degrees of varus or valgus angulation, 5 degrees of angulation in the anteroposterior plane, 10 degrees of rotation, and 1 cm of shortening. It is assumed that fracture healing in an unacceptable position (ie, malunion) will affect the mechanics of the knee or ankle joint and possibly lead to premature degenerative joint disease.
Acceptable reduction can be obtained in one of many ways, and this is another area of ongoing controversy: closed versus open treatment. The goal of any treatment is to allow the fracture to heal in an acceptable position with minimal negative effect on the surrounding tissues or joints. Closed reduction is obtained under general anesthesia if necessary, and the patient is immobilized in a long leg non–weight-bearing cast. If radiographs at 2 weeks show acceptable alignment, the patient can be transitioned to a Sarmiento type fracture brace with full weight bearing.
If acceptable and stable reduction cannot be obtained by closed means, common options for surgical treatment include early definitive fixation or delayed stabilization after provisional splinting or external fixation. A reamed intramedullary nail is the recommended treatment for most displaced closed and Gustilo type I–IIIA fractures. External fixation is used as temporary fixation until soft-tissue management permits definitive nailing. Intramedullary nails are placed percutaneously under fluoroscopic control without opening the fracture site. Dynamic or static interlocking can be achieved with transfixing screws on both ends of the nail, and this maintains length and provides rotational control.
ORIF with plates and screws is rarely performed for tibial shaft fracture. MIPPO may be used as if there is distal or proximal fracture extension prohibiting nailing. This technique avoids exposure of the fracture and decreases soft-tissue dissection, devascularization of the bone, risk of infection, and delayed union.
![]() Fracture of the Distal End of the Tibia (ICD-9:823.80, 823.82)
Fracture of the Distal End of the Tibia (ICD-9:823.80, 823.82)
• Protecting the soft-tissue envelope while restoring the articular surface and the alignment of the tibia are the primary goals of the treatment.
• Postoperative complications are common.
Also referred to as pilon or plafond fractures, these fractures involve the distal articular surface of the tibia at the tibiotalar joint. As for any intraarticular fracture, the goal of treatment is to restore an anatomic articular surface. This can be difficult and sometimes impossible. Closed reduction of displaced fractures is almost never successful, and external fixation spanning the injury, with or without ORIF of the fibula, can be initially performed. Once soft-tissue swelling subsides, ORIF can be safely undertaken. Bone graft can be added to metaphyseal defects to support the articular surface. When the fracture is so comminuted that internal fixation is impossible, an attempt at indirect reduction by ligamentotaxis should be done, with or without an ORIF of the fibular fracture to restore length, closed reduction, and external fixation of the tibia. This can usually restore normal contours and alignment of the distal leg and make an eventual tibiotalar fusion easier should disabling posttraumatic arthritis occur. Primary ankle fusion is an alternative for severely comminuted fractures.
Surgical incisions through hemorrhagic blisters should be avoided. Healing is likely to be slow, and weight bearing should be carefully started only when radiologic evidence of bone healing is present. Postoperative pain, stiffness, and swelling can be seen in almost 25% of patients. Failure of healing is higher than 5% after primary procedures.
![]() Compartment Syndrome (ICD-9:958.62)
Compartment Syndrome (ICD-9:958.62)
Compartment syndrome is a frequent concern in tibia fractures and is caused by increased pressure in any of the four closed osteofascial spaces, compromising circulation and perfusion of the tissues within the involved compartment. Nerves and muscle tissue are particularly susceptible. Compartment syndrome can occur in crush injuries without fractures and in open fractures. The hallmark of compartment syndrome is severe pain out of proportion to the injury. The pain is increased with passive stretch to the leg muscles.
Fasciotomies should be performed emergently and are performed through lateral and medial incisions in the skin and fascia of all four compartments. Compartment pressure measurements may be used preoperatively but are not mandatory if the diagnosis is clear. Debridement of all necrotic tissue is imperative. The wounds are left open, possibly with a wound VAC system, and then treated by delayed primary closure or split-thickness skin grafting within 5 days. Delaying treatment of any compartment syndrome by more than 6–8 hours can lead to irreversible nerve and muscle damage.
![]() Complications
Complications
Complications are common after tibia and fibula fractures and include infection, malunion, nonunion, muscle contractions, and chronic pain.
A. Delayed Union or Nonunion
The tibia, particularly its distal third, is prone to delayed union or nonunion due to lower blood flow and muscle coverage. This occurs more frequently in high-energy, open, and segmental fractures. Pain and motion at the fracture are noted to be present more than 6 months after injury. Radiographs show the persistence of the fracture line with or without callus. Sclerosis and flaring of the bone ends characterize the hypertrophic nonunion, whereas osteopenia and thinning of the fragments are seen in atrophic nonunions. Early weight bearing is thought to stimulate bone healing. If nonunion develops, rigid fixation with or without bone grafting (atrophic nonunion) will be required to achieve healing. Electrical stimulation, ultrasound, and shock waves have limited efficacy but may achieve union in selected cases.
B. Malunion
Malunion may lead to premature degenerative joint disease. Corrective osteotomies may be required. When associated with shortening, multiple-plane correction and lengthening can be obtained after corticotomy and external fixation with ring-type fixation devices, which allow progressive correction of the deformity.
C. Infection
Infection of the tibia following open fracture or surgical treatment remains the most severe complication, especially when associated with nonunion. Perioperative prophylactic antibiotic therapy and adequate debridement and irrigation of open fractures are not always successful in preventing this complication. Aggressive utilization of early muscle transfers to increase the local blood supply has significantly improved the overall results of treatment. However, amputation may be required and is a viable functional alternative.
D. Complex Regional Pain Syndrome (Reflex Sympathetic Dystrophy) (ICD-9:337.20)
Complex regional pain syndrome is a fortunately rare complication of unknown cause. It is characterized by pain out of proportion to the original injury. Swelling, pain, and vasomotor disturbances are the hallmarks of this syndrome. Gradual increase in weight bearing and early joint mobilization will minimize the occurrence of this complication. Chemical or surgical sympathetic blockade may be helpful for the more severe forms of this disease.
E. Other Complications
Posttraumatic arthritis is a frequent occurrence after pilon fractures or as a complication of tibial shaft malunion. Joint stiffness and ankylosis may occur after prolonged immobilization. Soft-tissue injuries, including those of nerve, vessels, or muscles, have been discussed in the compartment syndrome section. Sequelae may include dropfoot and claw toe deformities and may require further soft-tissue or bone procedures.
Blauth M, Bastian L, Krettek C, et al: Surgical options for the treatment of severe tibial pilon fractures: a study of three techniques. J Orthop Trauma 2001;15:153. [PMID: 11265004]
Bozic V, Thordarson DB, Hertz J: Ankle fusion for definitive management of non-reconstructable pilon fractures. Foot Ankle Int 2008;29:914. [PMID: 18778670]
Finkemeier CG, Schmidt AH, Kyle RF, et al: A prospective, randomized study of intramedullary nails inserted with and without reaming for the treatment of open and closed fractures of the tibial shaft. J Orthop Trauma2000;14:187. [PMID: 10791670]
Fulkerson EW, Egol KA: Timing issues in fracture management: a review of current concepts. Bull NYU Hosp Jt Dis 2009;67:58. [PMID: 19302059]
Gopal S, Majumder S, Batchelor AG, et al: Fix and flap: the radical orthopaedic and plastic treatment of severe open fractures of the tibia. J Bone Joint Surg Br 2000;82-B:959. [PMID: 11041582]
Hernigou P, Cohen D: Proximal entry for intramedullary nailing of the tibia. J Bone Joint Surg Br 2000;82-B:33. [PMID: 10697311]
Keating JF, Blachut PA, O’Brien PJ, et al: Reamed nailing of Gustilo grade-IIIB tibial fractures. J Bone Joint Surg Br 2000;82-B: 1113. [PMID: 11132268]
Larsen LB, Madsen JE, Hoiness PR, Ovre S: Should insertion of intramedullary nails for tibial fractures be with or without reaming? A prospective, randomized study with 3.8 years’ follow-up. J Orthop Trauma 2004;18:144. [PMID: 15091267]
LeBus GF, Collinge C: Vascular abnormalities as assessed with CT angiography in high-energy tibial plafond fractures. J Orthop Trauma 2008;22:16. [PMID: 18176160]
Lin J, Hou SM: Unreamed locked tight-fitting nailing for acute tibial fractures. J Orthop Trauma 2001;15:40. [PMID: 11132268]
Nassif JM, Gorczyca JT, Cole JK, et al: Effect of acute reamed versus unreamed intramedullary nailing on compartment pressure when treating closed tibial shaft fractures: a randomized prospective study. J Orthop Trauma2000;14:554. [PMID: 11149501]
Tscherne H, Lobenhoffer P: A new classification of soft-tissue damage in open and closed fractures. Unfallheilkunde 1982;85:111. [No PMID]
Samuelson MA, McPherson EJ, Norris L: Anatomic assessment of the proper insertion site for a tibial intramedullary nail. J Orthop Trauma 2002;16:23. [PMID: 11782628]
Sarmiento A, Latta LL: 450 closed fractures of the distal third of the tibia treated with a functional brace. Clin Orthop Relat Res 2004;428:261. [PMID: 15534552]
Thordarson DB: Complications after treatment of tibial pilon fractures: prevention and management strategies. J Am Acad Orthop Surg 2000;8:253. [PMID: 10951114]
Vives MJ, Abidi NA, Ishikawa SN, et al: Soft tissue injuries with the use of safe corridors for transfixion wire placement during external fixation of distal tibia fractures: an anatomic study. J Orthop Trauma2001;15:555. [PMID: 11733671]
Zelle BA, Bhandari M, Espiritu M, et al: Treatment of distal tibia fractures without articular involvement: a systematic review of 1125 fractures. J Orthop Trauma 2006;20:76. [PMID: 16424818]
Ziran BH, Darowish M, Klatt BA, Agudelo JF, Smith WR: Intramedullary nailing in open tibia fractures: a comparison of two techniques. Int Orthop 2004;28:235. [PMID: 15160254]
FOOT AND ANKLE INJURIES
A thorough physical examination should compare the injured extremity to the uninjured contralateral side (looking for ecchymosis, swelling, or deformity), palpating carefully all points of tenderness, stressing the different joints when indicated, and assessing the neurovascular status. Associated injuries and certain systemic disorders (particularly diabetes and peripheral vascular disease) should be identified. An appropriate radiographic evaluation is mandatory. AP and lateral views are standard. Oblique and special views are requested according to clinical suspicion. Although some fracture patterns are still best delineated by conventional tomography, CT scanning with three-dimensional rendering has recently proved to be valuable, especially for ankle and calcaneal fractures. Radionuclide imaging is helpful to identify occult injuries and stress fractures. MRI is gaining popularity and is particularly helpful in diagnosing soft-tissue damage to the tibialis posterior tendon or gastrocnemius muscle, osteochondral fractures, and avascular necrosis.
ANATOMY AND BIOMECHANICAL PRINCIPLES
The foot is a complex, highly specialized structure that permits weight bearing in a smooth, energy-conserving pattern; thus, when planning treatment of an injured foot, delicate balance between soft tissues and bones should be addressed. High-energy injuries, such as crush injuries, generally have a poorer prognosis, even if the bones are anatomically reduced. Scarring of soft tissues, particularly specialized tissues like the heel fat pad or the plantar fascia, prevents normal function and is often painful.
Embryologically, the foot develops from proximal to distal into three functional segments: the tarsus, metatarsus, and phalanges. Anatomically, it is divided into the hindfoot (talus and calcaneus), the midfoot (navicular, cuboid, and three cuneiforms), and the forefoot (five metatarsals and 14 phalanges). Besides skin, vessels, and nerves, the soft tissues include extrinsic tendons, intrinsic musculotendinous units, a complex network of capsuloligamentous structures, and some uniquely specialized tissues such as fat pads.
The bones, ligaments, and muscles of the foot actively maintain the integrity of the three arches of the foot. The two longitudinal arches aid in weight bearing and absorbing the forces during motion. The transverse arch helps with the movements of the foot. The plantar aspect of the foot is divided into four layers, each containing different muscles and tendons, from superficial to deep.
These 28 bones, 57 articulations, and extrinsic and intrinsic soft tissues work harmoniously as a unit resembling functionally a ball and socket to allow walking, running, jumping, and accommodation of irregular surfaces with a minimal expense of energy.
Restoration of the complex relationship between bone and soft-tissue structures is often challenging, but is the goal of treatment of foot injuries.
FRACTURES COMMON TO ALL PARTS OF THE FOOT
1. Stress Fractures
Also known as fatigue or march fractures, stress fractures are commonly seen in young active adults involved in vigorous and excessive exercise. These are fractures of bones due to repetitive loading rather than a single traumatic event. Fracture occurs when damage from cyclical loading of a bone overwhelms its physiologic repair capacity. A high longitudinal arch and excessive forefoot varus are intrinsic precipitating factors. Sites of fracture are most frequently the metatarsals and the calcaneus, but fatigue fractures can be found anywhere.
![]() Clinical Findings
Clinical Findings
Incipient pain of varying intensity at rest is then accentuated by walking. Swelling and point tenderness are likely to be present. Depending on the stage of progress, radiographs may be normal or may show an incomplete or complete fracture line or only extracortical callus formation that can be mistaken for osteogenic sarcoma. Radionuclide imaging, CT, and MRI can be helpful for occult fractures. CT is also helpful to differentiate incomplete and complete fractures. Persistent unprotected weight bearing may cause arrest of bone healing and even displacement of the fracture fragment.
![]() Treatment
Treatment
Treatment is by protection in a short leg cast, walking boot, or a heavy stiff-soled shoe. Weight bearing is restricted until pain has subsided and restoration of bone continuity is confirmed radiographically, usually within 3–4 weeks. Because of the high risk of displacement and nonunion, early surgical management is proposed for high-risk stress fractures in the elite athlete.
2. Multiple High-Energy Injuries
Violent forces applied to the foot may cause more extensive damage than initially appreciated. High-energy fractures are often open, and the basic principles of open fracture management should be applied.
![]() Treatment
Treatment
The objectives of treatment are to preserve circulation and sensation (particularly of the plantar region), maintain a plantigrade position of the foot, prevent or control infection, preserve plantar skin and fat pads, preserve gross motion of the different joints (both actively and passively), achieve bone union, and, ultimately, preserve fine motion. Fasciotomies of the severely injured foot may be necessary to avoid compartment syndromes and their serious sequelae.
Early stabilization of multiple fractures and dislocations will simplify wound management. This can be accomplished through external fixation or internal fixation with K-wires, plates, or screws. Early soft-tissue coverage with local or free flaps is also beneficial.
3. Neuropathic Joint Injuries and Fractures
Fractures and other foot disorders often present in the patient with Charcot arthropathy. Neuropathic fractures are frequently seen with diabetes. Other rare causes are tabes dorsalis, syringomyelia, peripheral nerve injury, and leprosy.
The potential for bone healing is normal if no other comorbidities exist. It has been found, however, that healing of fractures is often delayed in this patient group. Protection, rest, and elevation can result in union without deformity. ORIF is sometimes necessary. Rarely, arthrodesis is indicated; however, the rate of nonunion is higher than for normal joints.
ANKLE FRACTURES AND DISLOCATIONS
• Among the most common injuries treated by orthopedic surgeons.
• Recognizing and treating syndesmotic injury are important for a successful outcome.
![]() Anatomy and Biomechanical Principles
Anatomy and Biomechanical Principles
The ankle joint itself is limited to one plane of motion: plantarflexion and dorsiflexion in the sagittal plane. With incorporation of the motion of the subtalar joint (which allows for inversion and eversion in the coronal plane), the foot is able to move in a complex and varied arc in relationship to the leg.
The inner and distal articular surfaces of the distal tibia and fibula form the ankle mortise (a uniplanar hinge joint). The ankle mortise serves as the “roof” over the talus. The articular portions of the lateral and medial malleoli serve as constraining buttresses to allow for controlled plantarflexion and dorsiflexion in the ankle mortise. This geometric configuration resists rotation of the talus in the ankle mortise. Further constraint and stability are provided by ligaments and the soft tissue surrounding the ankle joint. The syndesmotic ligament is composed of four ligaments of which the posterior inferior tibiofibular ligament is the thickest and strongest and connects the tibia to the fibula at the level of the tibial plafond. The bony architecture of the mortise also provides some constraint to posterior subluxation of the talus. This is provided by the cup-shaped tibial plafond and the slightly increased width of the talar dome anteriorly as compared with posteriorly.
The distal tibia also serves to absorb the compressive loads and stress placed on the ankle. The internal trabecular pattern of the bone helps transmit, diffuse, and resorb the compressive forces. Cross-sectional studies have shown that reduced activity and old age lead to resorption of cancellous bone, thereby decreasing the compressive resistance of the distal tibia.
Fracture-dislocations of the ankle are frequently referred to as bimalleolar (fractures of the medial and lateral malleoli) or trimalleolar (fractures of the medial, lateral, and posterior malleoli). Fracture of the lateral malleolus with complete rupture of the deltoid ligament or fracture of the medial malleolus with complete disruption of the syndesmosis and a proximal fibular shaft fracture (Maisonneuve fracture) are also considered bimalleolar fractures on a functional basis.
![]() Classification
Classification
The purpose of any classification scheme is to provide a means to better understand the extent of injury, describe an injury, and determine a treatment plan. Presently, the two most widely used classification schemes for describing ankle fractures are the Lauge-Hansen and Weber-Danis classifications.
In 1950, Lauge-Hansen described a classification system based on mechanism of injury that described over 95% of all ankle fractures (Figure 2–21 shows a comparison of the Weber-Danis and Lauge-Hansen schemes). By stressing freshly amputated limbs in combinations of supination, pro-nation, adduction, abduction, and external rotation, he was able to describe nearly all fracture patterns. Pronation and supination refer to the position of the patient’s foot at the instance of injury, while adduction, abduction, and external rotation refer to the vector of the force that is applied. Thus, four mechanisms of injury were described for ankle fractures: (1) supination adduction, (2) supination-external rotation, (3) pronation abduction, and (4) pronation-external rotation. Lauge-Hansen later added a fifth type of injury, the pronation dorsiflexion injury, in order to include a mechanism for tibial plafond fractures. This fifth type is caused by a compression-type axial loading injury.

![]() Figure 2–21. Comparison of Lauge-Hansen and Weber-Danis ankle classifications. (Reproduced, with permission, from Browner BD, Levine A, Jupiter J, et al, eds: Skeletal Trauma, 2nd ed. New York: WB Saunders; 1998.)
Figure 2–21. Comparison of Lauge-Hansen and Weber-Danis ankle classifications. (Reproduced, with permission, from Browner BD, Levine A, Jupiter J, et al, eds: Skeletal Trauma, 2nd ed. New York: WB Saunders; 1998.)
The Weber-Danis classification is much simpler and is based on anatomy rather than mechanism as it relates to the level at which the fibular fracture occurs.
Type A: Fracture in which the fibula is avulsed distal to the joint line. The syndesmotic ligament is left intact, and the medial malleolus is either undamaged or is fractured in a shear-type pattern.
Type B: Spiral fracture of the fibula beginning at or near the level of the joint line and extending in a proximal-posterior direction up the shaft of the fibula. Parts of the syndesmotic ligament complex can be torn, but the large interosseous ligament is usually left intact so that no widening of the distal tibiofibular articulation occurs. Complete syndesmotic disruptions, however, can result from this fracture pattern. The medial malleolus can either be left intact or sustain a transverse avulsion fracture. If the medial malleolus is left intact, there can be a tear of the deltoid ligament. Avulsion fracture of the posterior lip of the tibia (posterior malleolus) can also occur.
Type C: Fracture of the fibula proximal to the syndesmotic ligament complex, with consequent disruption of the syndesmosis. Medial malleolar avulsion fracture or deltoid ligament rupture is also present. Posterior malleolar avulsion fracture can also occur.
The AO classification represents an alpha-numeric system based on the Weber-Danis classification.
![]() Treatment
Treatment
Four criteria should be met for the optimal treatment of ankle fractures: (1) dislocations and fractures should be reduced as soon as possible; (2) all joint surfaces must be precisely restored; (3) the fracture must be held in a reduced position during the period of bony healing; and (4) joint motion should be initiated as early as possible. If these treatment goals are met, a good outcome can be expected, keeping in mind that disruption of the articular cartilage results in permanent damage.
Previous studies have demonstrated that the ankle has the thinnest articular cartilage but the highest ratio of joint congruence to articular cartilage thickness of any of the large joints. This suggests that loss in congruity of the ankle joint following fracture will be poorly tolerated and lead to post-traumatic arthritic changes. Thus, it is important to obtain anatomic reduction of the articular surfaces of the ankle after a fracture. A lateral talar shift of as little as 1 mm will decrease surface contact at the tibiotalar joint by 40%.
Initial treatment of ankle fractures should include immediate closed reduction and splinting, with the joint held in the most normal position possible to prevent neurovascular compromise of the foot. An ankle joint should never be left in a dislocated position. If the fracture is open, the patient should be given appropriate intravenous antibiotics and taken to the operating room on an urgent basis for irrigation and debridement of the wound, fracture site, and ankle joint. The fracture should also be appropriately stabilized at this time.
When performing ORIF of ankle fractures, several principles must be followed. It is important to gently handle the soft tissues about the ankle so as to minimize the risks of infection and wound-healing problems. In the treatment of bimalleolar and trimalleolar fractures, the lateral malleolus should usually be reduced and fixed first. This has two benefits: (1) it helps to correctly restore the original limb length, and (2) because of the strong ligamentous connections between the lateral malleolus and talus (anterior and posterior talofibular ligaments), initial fixation of the lateral malleolus will correctly position the talus in the mortise. When performing ORIF of the medial malleolus, it is important to remove any soft tissue or periosteum interposed in the fracture site. It is also preferable to fix the medial malleolus with either two cancellous-type lag screws or by tension banding principles to achieve interfragmentary compression.
The necessity for fixation of the posterior malleolar fragment is dependent on several factors. After the lateral and medial malleolar fractures have been internally fixed, ligamentotaxis often will anatomically reduce the posterior malleolar fragment. If this fragment represents less than 25% of the articular surface of the tibial plafond and there is less than 2 mm of displacement, internal fixation is not always required. If the fragment does not reduce on the intraoperative radiograph with ligamentotaxis, or if the fragment represents more than 25% of the articular surface, most authors agree that it should be internally fixed. Several methods have been described for this, using either direct fixation posteriorly via the posterolateral approach or by lag screw from anterior to posterior.
Following surgery, the limb is placed in a bulky sterile dressing with plaster splints from the ball of the foot to the proximal calf to allow for wound healing. The ankle is kept in neutral position to prevent equinus deformity. After the sutures are removed at 2 weeks, the surgeon must decide whether to begin early mobilization of the ankle joint. If the patient is reliable and stable fixation was achieved at the time of surgery, then early range of motion may be initiated, keeping the patient on crutches and not allowing weight bearing. If there is a question about patient reliability or stability of fixation, the limb can be placed in a short leg cast for added protection. Usually at 6 weeks, all immobilization is discontinued and weight bearing is slowly advanced. Physical therapy often helps promote ankle motion, strengthening, and regained ankle proprioception.
Brockwell J, Yeung Y, Griffith JF: Stress fractures of the foot and ankle. Sports Med Arthrosc 2009;17:149. [PMID: 19680111]
Egol KA, Dolan R, Koval KJ: Functional outcome of surgery for fractures of the ankle. J Bone Joint Surg Br 2000;82-B:246. [PMID: 10755435]
Egol KA, Pahk B, Walsh M, Tejwani NC, Davidovitch RI, Koval KJ: Outcome after unstable ankle fracture: effect of syndesmotic stabilization. J Orthop Trauma 2010;24:7. [PMID: 20035171]
Hess F, Sommer C: Minimally invasive plate osteosynthesis of the distal fibula with the locking compression plate: first experience of 20 cases. J Orthop Trauma 2011;25:110. [PMID: 21245715]
Horisberger M, Valderrabano V, Hintermann B: Posttraumatic ankle osteoarthritis after ankle-related fractures. J Orthop Trauma 2009;23:60. [PMID: 19104305]
Manjoo A, Sanders DW, Tieszer C, MacLeod MD: Functional and radiographic results of patients with syndesmotic screw fixation: implications for screw removal. J Orthop Trauma 2010;24:2. [PMID: 20035170]
Miller AN, Paul O, Boraiah S, Parker RJ, Helfet DL, Lorich DG: Functional outcomes after syndesmotic screw fixation and removal. J Orthop Trauma 2010;24:12. [PMID: 20035172]
Moore JA Jr, Shank JR, Morgan SJ, Smith WR: Syndesmosis fixation: a comparison of three and four cortices of screw fixation without hardware removal. Foot Ankle Int 2006;27:567. [PMID: 1691920]
Stark E, Tornetta P 3rd, Creevy WR: Syndesmotic instability in Weber B ankle fractures: a clinical evaluation. J Orthop Trauma 2007;21:643. [PMID: 17921840]
Tornetta P: Competence of the deltoid ligament in bimalleolar ankle fractures after medial malleolar fixation. J Bone Joint Surg 2000;82-A:843. [PMID: 10859104]
WikerØy AK, HØiness PR, Andreassen GS, Hellund JC, Madsen JE: No difference in functional and radiographic results 8.4 years after quadricortical compared with tricortical syndesmosis fixation in ankle fractures. J Orthop Trauma 2010;24:17. [PMID: 20035173]
HINDFOOT FRACTURES AND DISLOCATIONS
1. Talus Fractures (ICD-9:825.21)
• Second in frequency among all tarsal fractures after calcaneus fractures.
• Sixty percent of the talus is covered with articular cartilage.
Fractures of the talus commonly occur either through the body or the neck. Talar neck fractures represent almost 50% of all talus fractures. The blood supply enters the talar neck area and is tenuous. Fractures and dislocations may disrupt this vascularization, causing delayed healing or avascular necrosis. CT is essential for exact assessment and classification of the fracture and preoperative planning for every talus fracture.
![]() Fractures of the Neck of the Talus
Fractures of the Neck of the Talus
The most common mechanism of talar neck fracture is hyperdorsiflexion with an axial load causing impingement between the talar neck and tibia. The most widely used classification, which relies on the degree of initial dislocation and number of affected joints, has been described by Hawkins:
Type 1: Nondisplaced vertical fracture
Type 2: Displaced and dislocation or subluxation at the subtalar joint
Type 3: Displaced and dislocation or subluxation at the subtalar and tibiotalar joints
Type 4: Essentially type 3 injuries with talonavicular subluxation or dislocation (Figure 2–22)

![]() Figure 2–22. Hawkins classification of talar neck fractures. (Reproduced, with permission, from Coughlin MJ, Mann RA, eds: Surgery of the Foot and Ankle, 7th ed. New York: WB Saunders; 1999.)
Figure 2–22. Hawkins classification of talar neck fractures. (Reproduced, with permission, from Coughlin MJ, Mann RA, eds: Surgery of the Foot and Ankle, 7th ed. New York: WB Saunders; 1999.)
This classification is of prognostic value for avascular necrosis of the body: 0–13% for type 1 fractures, 25–50% for type 2 fractures, 80–100% for type 3 fractures, and 100% for type 4 fractures.
Complications of talar neck fractures include infection, delayed union or nonunion, malunion, and osteoarthritis of the tibiotalar and subtalar joints.
Treatment of talar fractures is aimed at minimizing the occurrence of these complications. Type 1 fractures are best treated with a non–weight-bearing below-knee cast for 6–8 weeks until clinical and radiologic signs of healing are present. Closed reduction is first attempted for type 2 fractures, and if this is successful in attaining anatomic alignment, treatment is as for a type 1 fracture. In about 50% of cases, closed reduction is unsuccessful, and ORIF with K-wires, pins, or screws is indicated. Closed reduction of type 3 and 4 fractures is almost never successful; ORIF is the rule. The postoperative regimen is the same as above. Progressive weight bearing will be allowed after fracture union if there is no avascular necrosis of the body. Within 6–8 weeks, a subchondral lucency seen in the dome of the talus (“Hawkins sign”) is possible only if the talar body is vascularized. The absence of the Hawkins sign, however, does not predict the occurrence of avascular necrosis in histologic and MRI-based studies.
![]() Fractures of the Body of the Talus
Fractures of the Body of the Talus
Talus body fractures occur mainly due to shear and axial compression forces, and they are intraarticular and involve the surfaces of both the tibiotalar and subtalar joints.
Fractures of the body of the talus are generally categorized as follows:
Type 1: Osteochondral fracture
Type 2: Coronal, sagittal, or horizontal fracture
Type 3: Posterior process fracture
Type 4: Lateral process fracture
Type 5: Crush fracture of the body
Treatment of talar body fractures is based on restoring joint integrity of both the tibiotalar and subtalar joints. Minimally displaced fractures of the talar body are not likely to cause disability if immobilization is continued until union is restored. Associated fractures of the malleoli, talar neck, and calcaneus occur frequently. AP, mortise, lateral, and Broden (45 degrees internal oblique) views aid radiographic assessment of the injury and enable the quantification of articular surface involvement and displacement. CT is recommended in all talar body fractures to assess comminution and associated fractures.
Open anatomic reduction and internal fixation via a twoincision approach, lateral and medial, should be the choice of treatment. Fixation may also allow earlier motion. Medial malleolar osteotomy can be performed over the more comminuted side of the talar body side to allow direct access to the fracture fragments. If reduction is not anatomic, delayed healing of the fracture may follow, and posttraumatic arthritis is a likely sequela. If this occurs, arthrodesis of the ankle or subtalar joints may be necessary to relieve painful symptoms in the long term.
![]() Osteochondral Fractures of the Talar Dome
Osteochondral Fractures of the Talar Dome
Any chronic pain after ankle sprain should raise the suspicion of osteochondral lesions. A history of trauma may not always be present.
Initial radiograph evaluation often does not demonstrate these lesions. CT and MRI have been used successfully as imaging modalities, but they are not as sensitive and specific as arthroscopy.
Classic staging performed by Berndt and Harty is based on the appearance on the plain radiographs:
Stage 1: Localized compression
Stage 2: Incomplete separation of the fragment
Stage 3: Completely detached but nondisplaced fragment
Stage 4: Completely detached, displaced fracture
Others proposed classification systems are based on MRI, CT, and existence of a cystic component. A cyst around the lesion is accepted as a bad prognostic factor.
Symptomatic stage 1, 2, and 3 lesions are usually initially treated conservatively with immobilization and restricted weight bearing. Healing is monitored radiographically with AP and mortise views. Lesions that fail conservative treatment and all stage 4 lesions require surgical treatment. Reduction and pinning or fixation with screws and excision with or without drilling have been recommended. Arthroscopic management seems to give as good a result as arthrotomy, with fewer complications. Degenerative disease of the tibiotalar joint is a frequent long-term complication.
![]() Subtalar Dislocation (ICD-9:837)
Subtalar Dislocation (ICD-9:837)
Subtalar dislocation, also called peritalar dislocation, is the simultaneous dislocation of the talocalcaneal and talonavicular joints. Inversion injuries result in medial dislocations (85%), whereas eversion injuries result in lateral dislocations (15%). Anterior and posterior dislocations are rare.
Prompt, gentle, closed reduction under sedation is usually successful. Immobilization in a non–weight-bearing short leg cast for 6 weeks is usually satisfactory. Soft-tissue interposition, particularly of the posterior tibial tendon, may prevent closed reduction. Open reduction, with or without internal fixation, is then indicated.
![]() Total Dislocation of the Talus (Extrusion Injury)
Total Dislocation of the Talus (Extrusion Injury)
This injury usually results from high-energy trauma, and most dislocations are open dislocations. Despite adequate prompt reduction and thorough wound debridement, the complication rate is extremely high, including persistent infection and avascular necrosis.
2. Calcaneus Fractures (ICD-9:825.0)
• The most common tarsal fracture.
• Approximately 75% involve an intraarticular component.
• Wound dehiscence and infection are the most common postoperative complications.
The most common mechanism of fracture is high-energy axial loading driving the talus downward. Ten percent of calcaneal fractures are associated with compression fractures of the thoracic or lumbar spine, and 5% are bilateral. Comminution and impaction are common features.
![]() Clinical Findings
Clinical Findings
A. Symptoms and Signs
Pain is usually significant but may be masked by associated injuries. Swelling, deformity, and blistering of the skin occur frequently during the first 36 hours as a result of the severe damage to surrounding soft tissues. The heel pad in particular is a highly specialized fatty structure that acts as a hydraulic cushion. Major disruptions of the heel pad lead to persistent pain and deformity and can produce poor functional results despite adequate bony healing.
B. Imaging Studies
Initial radiographs include three views: anteroposterior, lateral, and axial projection (Harris view). Disruption of Böhler’s angle and the angle of Gissane can be determined from initial radiographs (Figure 2–23). Oblique and Broden views are useful to demonstrate subtalar joint incongruity. CT scanning is the diagnostic tool of choice and will further delineate fracture patterns and occult injuries.

![]() Figure 2–23. Böhler angle (A) and Gissane angle (B), indicating normal anatomic landmarks. (Reproduced, with permission, from Coughlin MJ, Mann RA, eds: Surgery of the Foot and Ankle, 7th ed. New York: WB Saunders; 1999.)
Figure 2–23. Böhler angle (A) and Gissane angle (B), indicating normal anatomic landmarks. (Reproduced, with permission, from Coughlin MJ, Mann RA, eds: Surgery of the Foot and Ankle, 7th ed. New York: WB Saunders; 1999.)
C. Classification
Various classification systems for calcaneus fractures have been advocated. In general, calcaneus fractures can be divided into intraarticular and extraarticular fractures. Intraarticular fractures are frequently (80%) associated with worse outcomes than extraarticular fractures. Sanders has developed a classification system for intraarticular fractures based on coronal CT images (Figure 2–24). This classification has been found to be useful in both treatment and prognosis. Type I fractures are nondisplaced articular fractures. Type II fractures are two-part fractures of the posterior facet and are divided into A, B, and C based on the location of the fracture line. Type III fractures are three-part fractures with a centrally depressed fragment, also divided into A, B, and C. Type IV fractures are four-part articular fractures with extensive comminution. The Essex-Lopresti classification describes the “joint depression–type” and the “tongue-type” fractures.

![]() Figure 2–24. Sanders computed tomography classification of calcaneus fractures. Sust, sustentaculum. (Reproduced, with permission, from Coughlin MJ, Mann RA, eds: Surgery of the Foot and Ankle, 7th ed. New York: WB Saunders; 1999.)
Figure 2–24. Sanders computed tomography classification of calcaneus fractures. Sust, sustentaculum. (Reproduced, with permission, from Coughlin MJ, Mann RA, eds: Surgery of the Foot and Ankle, 7th ed. New York: WB Saunders; 1999.)
1. Nondisplaced fractures—These fractures (eg, Sanders type I) are successfully treated by nonoperative management with protected weight bearing for 6–8 weeks, until clinical and radiographic signs of healing are present.
2. Tongue-type fractures—This fracture pattern (Figure 2–25) splits the tuber in the axial plane and involves the subtalar joint. The pull of the achilles tendon displaces the dorsal fragment cranially.

![]() Figure 2–25. Tongue-type fracture of the calcaneus showing involvement of the subtalar joint.
Figure 2–25. Tongue-type fracture of the calcaneus showing involvement of the subtalar joint.
3. Joint depression—This fracture pattern (Figure 2–26) creates a separate fragment of the posterior facet with joint incongruity.

![]() Figure 2–26. Joint depression-type fracture of the calcaneus. The posterior facet is a separate fragment.
Figure 2–26. Joint depression-type fracture of the calcaneus. The posterior facet is a separate fragment.
4. Comminuted fractures—Some fracture patterns create such comminution and impaction that they defy classification. They all have in common significant soft-tissue injury and subtalar joint incongruity.
![]() Treatment
Treatment
Treatment of displaced intraarticular fractures remains controversial. As already stated, the final outcome can depend on soft-tissue as well as bony healing.
Prospective large-scale studies out of Canada have revealed excellent clinical outcomes by conservative treatment even for displaced intraarticular fractures. Heavy smoking, severe peripheral vascular disease, and poorly controlled diabetes are considered to be relative contraindications for surgery. The extent of varus displacement in the axial plane (Harris heel view) appears to guide operative management more than the extent of joint depression in the posterior facet.
Some surgeons advocate early closed manipulation of displaced intraarticular fractures to at least partially restore the external anatomic configuration of the heel region. Internal fixation with percutaneous pins may be performed. This is particularly successful for noncomminuted tongue-type fracture patterns. An axial pin is inserted in the tongue fragment, which is then disimpacted and reduced. The pin is then pushed further to stabilize the fracture (Essex-Lopresti technique). ORIF with pins, screws, or plates, with or without bone grafting, has gained acceptance. The aim of ORIF is to restore Böhler’s angle and improve heel alignment out of varus through stable fixation. Immediate surgery is associated with a high incidence of wound healing complications. Therefore, a 10- to 14-day delay in surgical fixation is recommended to decrease the risk of wound breakdown and infection. The “wrinkle test” should be positive prior to surgery. More recently, concerns surrounding the complications of wound healing have encouraged the use of minimally invasive approaches. Few authors advocate primary subtalar arthrodesis for severely comminuted fractures.
Fractures of the sustentaculum represent rare injuries that are usually caused by a high-energy trauma. This fracture should be suspected in patients with a history of eversion injury and pain below the medial malleolus. The injury is mainly diagnosed by CT scan. Displaced sustentaculum fractures may require surgical fixation through a medial approach.
Fractures of the anterior process are usually caused by forced inversion of the foot and must be differentiated from midtarsal and ankle sprains. The firmly attached bifurcate ligament avulses a bony flake from the anterior process. Maximal tenderness and swelling occur midway between the tip of the lateral malleolus and the base of the fifth metatarsal. A lateral oblique radiograph will demonstrate the fracture line.
Fractures of the medial process give origin to the abductor hallucis and part of the flexor digitorum brevis muscle and can be avulsed in eversion-abduction injuries.
![]() Complications
Complications
The most significant complications are postoperative wound breakdown and infection. Posttraumatic degenerative arthritis is a relatively common long-term complication requiring subtalar fusion or triple arthrodesis. The rate of wound complications after ORIF has been reported to be as high as 30–50%. Other complications include compartment syndrome, nerve entrapment syndromes (medial or lateral plantar branches and sural nerve, either from posttraumatic or postsurgical scarring), peroneal tendon injury, heel pad pain, exostosis, and malunion. Compartment syndrome is present in 10% of patients and should be excluded during the examination.
Allmacher DH, Galles KS, Marsh JL: Intra-articular calcaneal fractures treated nonoperatively and followed sequentially for 2 decades. J Orthop Trauma 2006;20:464. [PMID: 16891937]
Attiah M, Sanders DW, Valdivia G, et al: Comminuted talar neck fractures: a mechanical comparison of fixation techniques. J Orthop Trauma 2007;21:47. [PMID: 17211269]
Benirschke S: Calcaneal fractures: to fix or not to fix. Opinion: open reduction internal fixation. J Orthop Trauma 2005;19:356. [PMID: 15891548]
Buckley R: Calcaneal fractures: to fix or not to fix. Opinion: nonoperative approach. J Orthop Trauma 2005;19:357. [PMID: 15891549]
Buckley RE: Evidence for the best treatment for displaced intra-articular calcaneal fractures. Acta Chir Orthop Traumatol Cech 2010;77:179. [PMID: 20619108]
Buckley RE, Tough S: Displaced intra-articular calcaneal fractures. J Am Acad Orthop Surg 2004;12:172. [PMID: 15161170]
Della Rocca GJ, Nork SE, Barei DP, Taitsman LA, Benirschke SK: Fractures of the sustentaculum tali: injury characteristics and surgical technique for reduction. Foot Ankle Int 2009;30:1037. [PMID: 19912711]
Early JS: Talus fracture management. Foot Ankle Clin 2008;13:635. [PMID: 19013400]
Gardner MJ, Nork SE, Barei DP, Kramer PA, Sangeorzan BJ, Benirschke SK: Secondary soft tissue compromise in tongue-type calcaneus fractures. J Orthop Trauma 2008;22:439. [PMID: 18670282]
Lim EV, Leung JP: Complications of intraarticular calcaneal fractures. Clin Orthop Relat Res 2001;391:7. [PMID: 11603691]
Longino D, Buckley RE: Bone graft in the operative treatment of displaced intraarticular calcaneal fractures: is it helpful? J Orthop Trauma 2001;15:280. [PMID: 11371794]
Marsh JL, Saltzman CL, Iverson M, Shapiro DS: Major open injuries of the talus. J Orthop Trauma 1995;9:371. [PMID: 8537838]
McGahan PJ, Pinney SJ: Current concept review: osteochondral lesions of the talus. Foot Ankle Int 2010;31:90. [PMID: 2006772]
Rammelt S, Zwipp H: Calcaneus fractures: facts, controversies and recent developments. Injury 2004;35:443. [PMID: 15081321]
Rammelt S, Zwipp H: Talar neck and body fractures. Injury 2009;40:120. [PMID: 18439608]
Sanders DW, Busam M, Hattwick E, Edwards JR, McAndrew MP, Johnson KD: Functional outcomes following displaced talar neck fractures. J Orthop Trauma 2004;18:265. [PMID: 15105747]
Swanson SA, Clare MP, Sanders RW: Management of intra-articular fractures of the calcaneus. Foot Ankle Clin 2008;13:659. [PMID: 19013401]
Tezval M, Dumont C, Sturmer KM: Prognostic reliability of the Hawkins sign in fractures of the talus. J Orthop Trauma 2007;21:538. [PMID: 17805020]
Verhagen RA, Maas M, Dijkgraaf MG, Tol JL, Krips R, van Dijk CN: Prospective study on diagnostic strategies in osteochondral lesions of the talus. Is MRI superior to helical CT? J Bone Joint Surg Br2005;87:41. [PMID: 15686236]
MIDFOOT FRACTURES AND DISLOCATIONS
1. Navicular Fractures (ICD-9:825.22)
![]() Avulsion Fractures
Avulsion Fractures
Avulsion fractures of the tarsal navicular may occur as a result of severe midtarsal sprain and require neither reduction nor elaborate treatment. Avulsion fracture of the tuberosity near the insertion of the posterior tibialis tendon is uncommon and must be differentiated from a persistent ununited apophysis (accessory navicular) from the supernumerary sesamoid bone, or os tibiale externum. Dorsal lip avulsions also occur.
![]() Body Fractures
Body Fractures
Body fractures occur either centrally in a horizontal plane or, more rarely, in a vertical plane. They are occasionally characterized by impaction. Noncomminuted fractures with displacement of the dorsal fragment can be reduced. Closed manipulation by strong traction on the forefoot and simultaneous digital pressure over the displaced fragment can restore normal position. If a tendency to redisplace is apparent, this can be counteracted by temporary fixation with a percutaneously inserted Kirschner wire. Non–weight-bearing immobilization in a cast or splint is required for a minimum of 6 weeks. Comminuted and impacted fractures cannot be anatomically reduced in a closed manner. Where fragments involve more than 25% of the bone, ORIF may be required to prevent dorsal subluxation of the navicular fragment. Bone graft may be used for depressed areas. Some authorities offer a pessimistic prognosis for comminuted or impacted fractures. It is their contention that even though partial reduction has been achieved, posttraumatic arthritis supervenes, and that arthrodesis of the talonavicular and naviculocuneiform joints will be ultimately necessary to relieve painful symptoms.
![]() Stress Fractures (ICD-9:733.95)
Stress Fractures (ICD-9:733.95)
The navicular is also a frequent site of fatigue fracture in runners. CT or radionuclide imaging is often necessary to make the diagnosis. Six weeks in a non–weight-bearing short leg cast is usually required for fracture healing.
2. Cuneiform and Cuboid Bone Fractures (ICD-9:825.23, 825.24)
Because of their relatively protected position in the midtarsus, isolated fractures of the cuboid and cuneiform bones are rarely encountered. Avulsion fractures occur as a component of severe midtarsal sprains. Extensive fractures usually occur in association with other injuries of the foot and often are caused by severe crushing. A “nutcracker” fracture is a compression fracture of the cuboid and, when associated with lateral column shortening, can be treated by lateral column lengthening, ORIF, and bone grafting.
3. Midtarsal Dislocations (ICD-9:838.12)
Midtarsal dislocation through the naviculocuneiform and calcaneocuboid joints, or more proximally through the talonavicular and calcaneocuboid joints (Chopart’s joint), may occur as a result of a twisting injury to the forefoot. Fractures of varying extent of adjacent bones are frequently associated.
When acute treatment is administered, closed reduction by traction on the forefoot and manipulation is generally effective. If reduction is unstable and displacement tends to recur upon release of traction, stabilization for 4 weeks by percutaneously inserted Kirschner wires is recommended.
FOREFOOT FRACTURES AND DISLOCATIONS
1. Metatarsal Fractures and Dislocations
Fracture of the metatarsals and dislocation of the tarsometatarsals are frequently caused by a direct crushing or indirect twisting injury to the forefoot. With severe trauma, circulation may be compromised from injury to the dorsalis pedis artery, which passes between the first and second metatarsals.
![]() Metatarsal Shaft Fractures (ICD-9:825.25)
Metatarsal Shaft Fractures (ICD-9:825.25)
Undisplaced fractures of the metatarsal shafts cause only temporary disability, unless failure of bone healing occurs. Displacement is rarely significant when the first and fifth metatarsals are not involved because they act as internal splints. These fractures can be treated with a hard-soled shoe with partial weight bearing or, if pain is marked, a short leg walking cast.
For displaced fractures of the shaft, it is of paramount importance to correct angulation in the longitudinal axis of the shaft. Residual dorsal angulation causes prominence of the metatarsal head on the plantar surface. The concentrated local pressure may produce a painful skin callus. Residual plantar angulation of the first metatarsal will transfer weight to the heads of the second and third metatarsals. After reduction of angular deformity, a cast should be well molded to the plantar surface to minimize recurrence of deformity and support the transverse and longitudinal arches. If significant angulation or intraarticular displacement persists, open or closed reduction and internal fixation should be considered.
![]() Metatarsal Neck and Head Fractures (ICD-9:825.25)
Metatarsal Neck and Head Fractures (ICD-9:825.25)
Fractures of the metatarsal “neck” are close to the head but remain extraarticular. Dorsal angulation is common and should be reduced to avoid reactive skin callus formation from pressure on the plantar skin. Intraarticular fractures of the metatarsal heads are rare. Even when they heal in a displaced position, some remodeling occurs and the functional outcome is surprisingly good. The indications for open reduction with or without internal fixation remain controversial.
Closed reduction of metatarsal fractures is best achieved by applying traction (Chinese finger traps) to the involved toes. Reduction is evaluated with intraoperative radiographs, and if judged unacceptable, ORIF with K-wires or plates and screws is indicated. Unstable reductions should also undergo percutaneous pinning under fluoroscopic imaging.
![]() Tarsometatarsal (Lisfranc) Dislocations (ICD-9:838.25)
Tarsometatarsal (Lisfranc) Dislocations (ICD-9:838.25)
Lisfranc injuries have traditionally been associated with high-energy trauma such as motor vehicle collisions and industrial accidents, but recently there is an increased incidence of such energy resulting from low-energy trauma such as athletic activity. These injuries are often overlooked following an athletic injury or in a polytrauma patient, so a high index of suspicion is necessary for proper diagnosis.
The base of the second metatarsal is recessed proximally to the base of the other metatarsals in a cleft between the first and third cuneiforms, thus “locking” the joint. Whereas primary stabilization is provided by bony skeleton, the strong ligamentous attachments provide substantial stability to the Lisfranc joint. The ligament structures are divided into plantar, dorsal, and interosseous components, with plantar being the strongest. The medial border of the fourth metatarsal and the cuboid should align on the 30-degree oblique view, and on the lateral view, the superior border of the metatarsal base should be aligned with the superior border of the medial cuneiform. For subtle injuries, MRI, CT, or stress x-rays may be useful.
Three commonly occurring patterns of this injury are identified: total incongruity, partial incongruity, and divergent (Figure 2–27).

![]() Figure 2–27. Classification of Lisfranc injuries. (Reproduced, with permission, from Coughlin MJ, Mann RA, eds: Surgery of the Foot and Ankle, 7th ed. New York: WB Saunders; 1999.)
Figure 2–27. Classification of Lisfranc injuries. (Reproduced, with permission, from Coughlin MJ, Mann RA, eds: Surgery of the Foot and Ankle, 7th ed. New York: WB Saunders; 1999.)
With nondisplaced injuries, cast immobilization with limited weight bearing can be used. Generally a short-leg cast for 6 weeks is followed by 6 weeks in a walking cast until the pain and tenderness subside.
More than 2 mm of displacement between the first and second metatarsal bases compared with the contralateral foot is indication for operative treatment. Achieving anatomic reduction is the key to successful treatment, and if this cannot be achieved by closed means, open reduction is indicated. Reduction can be secured with screws, bioabsorbable screws, plates, or a suture endobutton, which has recently gained popularity.
Failure to diagnose the injury or malreduction may cause posttraumatic arthritis, which is the most common complication after Lisfranc injuries. Other common complications are complex regional pain syndrome, symptomatic hardware, and incomplete reduction or loss of reduction.
![]() Fracture of the Base of the Fifth Metatarsal (ICD-9:825.25)
Fracture of the Base of the Fifth Metatarsal (ICD-9:825.25)
This is the most common of all metatarsal fractures. Three distinct patterns occur: (1) avulsion fracture of a variably sized portion of the tuberosity (styloid process) that may, on rare occasions, involve the joint between the cuboid and the fifth metatarsal; (2) acute Jones fracture involving the intermetatarsal joint (located at the metaphyseal-diaphyseal junction); and (3) transverse fracture of the proximal meta-tarsal diaphysis.
Avulsion fractures usually occur after adduction injury to the forefoot. The peroneus brevis muscle may pull and displace the fractured fragment proximally. A hard-soled shoe, cast brace, or elastic wrapping for 3 weeks is often successful for treatment, and bony healing rarely fails to occur. Symptomatic nonunions, displacement of more than 2 mm, and more than 30% involvement of the cubometatarsal joint should be treated surgically. Symptomatic small fragments can be excised.
Acute Jones fractures are best treated in a non–weight-bearing cast for 6–8 weeks. Some authors recommend acute ORIF of Jones fractures in the high-performance athlete. Proximal diaphyseal fractures, or “chronic Jones fractures,” are most probably secondary to fatigue failure. Again, conservative treatment in a non–weight-bearing short leg cast for 6 weeks will usually bring healing of the fracture. Nonunions do occur (due to the poor inherent blood supply) and are often symptomatic. If there is no evidence of bone healing at 12 weeks, internal fixation and bone grafting are recommended. Treatment of proximal metatarsal shaft fractures is similar to that for Jones fractures.
2. Fractures and Dislocations of the Phalanges of the Toes
Fractures of the phalanges of the toes are most commonly caused by a direct force such as a crush injury. Spiral or oblique fractures of the shaft of the proximal phalanges of the lesser toes may occur as a result of an indirect twisting injury. The injury should be assessed in terms of deformity, soft-tissue injury, and neurovascular status and also radiographically.
![]() Treatment
Treatment
Comminuted fracture of the proximal phalanx of the great toe, alone or in combination with fracture of the distal phalanx, is a disabling injury. Because wide displacement of fragments is not likely, correction of angulation and support by a splint usually suffice. A weight-bearing removable cast boot may be useful for relief of symptoms arising from associated soft-tissue injury. Spiral or oblique fracture of the proximal or middle phalanges of the lesser toes can be treated adequately by binding the involved toe to the adjacent uninjured toe (buddy taping). Comminuted fractures of the distal phalanx are treated as soft-tissue injuries.
Dislocation of the metatarsophalangeal joints and dislocation of the proximal interphalangeal joints usually can be reduced by closed manipulation. These dislocations are rarely isolated and usually occur in combination with other injuries to the forefoot.
3. Fracture of the Sesamoids of the Great Toe (ICD-9:825.20)
Fractures of the sesamoid bones of the great toe are rare but may occur as a result of a crushing injury. These injuries must be differentiated from a bipartite sesamoid by comparing radiographs of the contralateral uninvolved foot.
![]() Treatment
Treatment
Undisplaced fractures require no treatment other than a hard-soled shoe or metatarsal bar. Displaced fractures may require immobilization in a walking boot or cast, with the toe strapped in flexion. Persistent delay of bone healing may cause disabling pain arising from arthritis of the articulation between the sesamoid and the head of the first metatarsal. If conservative modalities have been exhausted, excision of the sesamoid may be necessary; however, this should be a last resort treatment.
Brin YS, Nyska M, Kish B: Lisfranc injury repair with the TightRope device: a short-term case series. Foot Ankle Int 2010;31:624. [PMID: 20663431]
Chuckpaiwong B, Queen RM, Easley ME, Nunley JA: Distinguishing Jones and proximal diaphyseal fractures of the fifth metatarsal. Clin Orthop Relat Res 2008;466:1966. [PMID: 18363075]
DeOrio M, Erickson M, Usuelli FG, Easley M: Lisfranc injuries in sport. Foot Ankle Clin 2009;14:169. [PMID: 19501801]
Desmond EA, Chou LB: Current concepts review: Lisfranc injuries. Foot Ankle Int 2006;27:653. [PMID: 16919225]
Haapamaki V, Kiuru M, Koskinen S: Lisfranc fracture-dislocation in patients with multiple trauma: diagnosis with multidetector computed tomography. Foot Ankle Int 2004;25:614. [PMID: 15563381]
Porter DA, Duncan M, Meyer SJ: Fifth metatarsal Jones fracture fixation with a 4.5-mm cannulated stainless steel screw in the competitive and recreational athlete: a clinical and radiographic evaluation. Am J Sports Med2005;33:726. [PMID: 1572227]
Richter M, Wippermann B, Krettek C, et al: Fractures and fracture dislocations of the midfoot: occurrence, causes and long-term results. Foot Ankle Int 2001;22:392. [PMID: 11428757]
Vorlat P, Achtergael W, Haentjens P: Predictors of outcome of non-displaced fractures of the base of the fifth metatarsal. Int Orthop 2007;31:5. [PMID: 16721621]
Zwitser EW, Breederveld RS: Fractures of the fifth metatarsal; diagnosis and treatment. Injury 2010;41:555. [PMID:19570536]
![]() Complex Regional Pain Syndrome (CRPS) (ICD-9:337.20)
Complex Regional Pain Syndrome (CRPS) (ICD-9:337.20)
This is defined as an abnormal reaction to injury characterized by burning pain, mechanical and thermal allodynia (pain caused by a stimulus that is normally not painful), hyperalgesia, stiffness, vasomotor changes, swelling, and osteoporosis of the affected limb. It is classified into two types depending on the presence of nerve lesion following the injury. Type 1 (formerly reflex sympathetic dystrophy) is associated with pain out of proportion to the initial injury, hyperesthesia, restricted mobility and movement disorder, skin changes (color, texture, and temperature), edema, patchy osteoporosis, and spreading symptoms to become more diffuse. Type 2 (formerly causalgia) includes the features of type 1 with an identified nerve lesion. CRPS can be precipitated by trauma, infection, myocardial infarction, stroke, surgery, and spinal cord disorders or sometimes without obvious cause. The pathophysiology is not fully understood, but damage to the nervous control of the affected part has been speculated. There is an increased incidence in people aged 40–60 years. Women are affected three times more often than men. Early diagnosis is the key to try to prevent chronic changes (muscle wasting and contractures) and can be made based on history and examination. Investigations include x-rays, bone scans, nerve conduction studies, and thermography. The cause, if identified, should be treated.
Clinically, reflex sympathetic dystrophy has three stages that are not completely distinct from one another. During the first, or early, stage, a burning or aching pain may be present and may be increased by external stimuli. Vasospasm that affects the color and temperature of the skin may also occur. The second stage generally develops at approximately 3 months. Pain is more severe, and this stage is characterized by significant edema, cold glossy skin, and joint limitations. Radiographs may reveal diffuse osteopenia. The third, or atrophic, stage is marked by progressive atrophy of skin and muscle and significant joint contractures.
Sudeck atrophy is a radiographic term that is extended to a clinical condition. Spotty rarefaction is distinguished from generalized diffuse atrophy of bone and may occur 6–8 weeks after the onset of symptoms. Shoulder-hand syndrome is a variation of this phenomenon that often occurs with upper extremity disorders. Stiffness is characteristic, both at the shoulder and at the wrist and hand level.
Because the cause is unclear, the recommended treatment is an aggressive program of physical therapy modalities to help with soft-tissue sensitivity; prevention or treatment of joint contractures can also be useful. Progressive loading of the extremity and progressive resistance-type exercises can also be of benefit in the appropriate setting.
FAILURE OF FRACTURE HEALING
There are many reasons why a fracture might not heal. The optimal time for healing depends on the bone in question, location of the fracture, the nature of the injury, and the quality of the soft tissues.
Generally, a fracture has united when there is radiographic evidence of bony bridging of the fracture on at least three cortices on orthogonal projections. Clinical criteria, such as absence of motion and resolution of pain at the fracture site, while helpful, are much less sensitive in confirming that a fracture has healed.
![]() Nonunion of Fracture (ICD-9:733.82)
Nonunion of Fracture (ICD-9:733.82)
According to the Food and Drug Administration, delayed union of a long bone is defined as a fracture that has not gone on to full bony union after 6 months. Delayed union is represented by evident cessation of periosteal new bone formation before union has been achieved.
Nonunion is less well defined. Clearly, a fracture that fails to show progressive evidence of healing over a 4- to 6-month period can be considered a nonunion. One can immediately declare a fracture with a 2-in bony defect, for example, a nonunion, as one knows that bony reconstitution will not occur spontaneously if this fracture is simply left immobilized.
Nonunion corresponds to scar formation in which the rate of endosteal and periosteal osteogenesis is zero or low and outweighed by bone resorption, with sclerosis of the medullary canal at the fracture surfaces. If the periosteum is active and there is no bridging despite new bone formation, the result is hypertrophic nonunion. If no new bone formation is taking place, the morphology will be atrophic.
A. Reasons for Nonunion
The two most common reasons are lack of adequate blood supply at the fracture site and inadequate stabilization of the fracture. Soft-tissue interposition at the fracture site, fractures stabilized in an unacceptable amount of distraction, metabolic abnormalities, initial displacement of fracture fragments, whether the fracture is open or closed, the patient’s age, comorbidities and nutritional status, medication use (eg, steroids, anticoagulants), smoking, and infection are other variables affecting fracture healing. Infection at the fracture site does not in and of itself preclude a fracture from healing, but it can be a contributing cause to the development of nonunion. Rosen has outlined the known causes of nonunion (Table 2–7).
Table 2–7. Causes of nonunion.
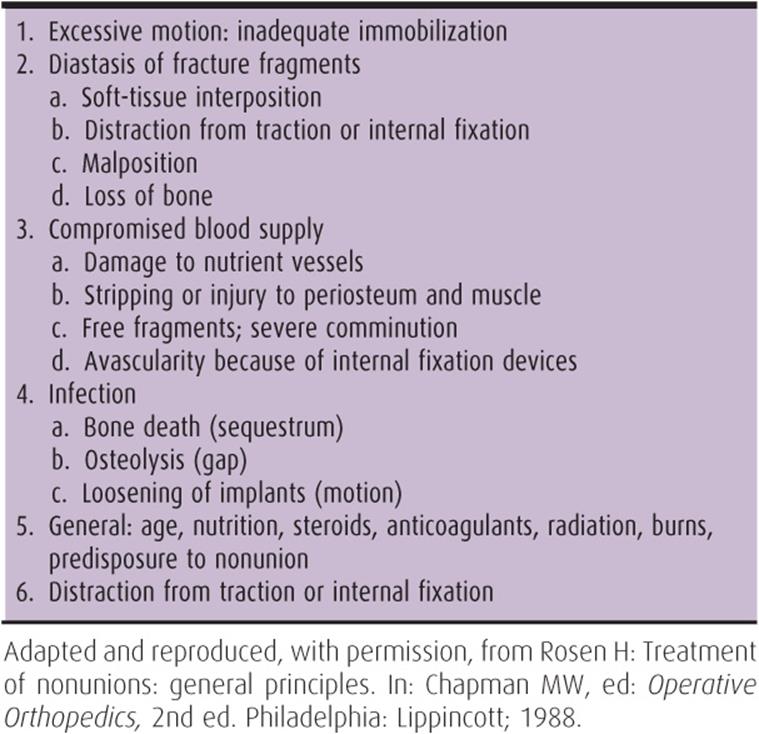
Certain areas of the skeleton (distal tibial diaphysis, scaphoid, subtrochanteric femoral region, and proximal diaphysis of the fifth metatarsal) are more prone to developing nonunion, even when appropriate treatment is rendered. Fracture pattern also plays a role in the development of nonunion. Segmental fractures of long bones are much more prone to nonunion, as are fractures with large “butterfly” fragments, because of devascularization of the intermediary segment.
B. Classification of Nonunions
Nonunions have been classified according to their radiologic characteristics. The most widely used classification is that developed by Weber and Cech, who classified nonunion of long bones as being either hypertrophic or atrophic. They used standard radiographs and strontium isotope studies to differentiate these two categories. Hypertrophic nonunions have viable bone ends, whereas atrophic nonunions have nonviable bone ends. This differentiation has importance both in prognosis and in determining appropriate treatment. They further subdivided hypertrophic nonunions into “elephant’s foot type,” “horse’s foot type,” and oligotrophic nonunions (Figure 2–28). As a generalization, those nonunions with better blood supply and some degree of micromotion at the fracture site develop more callus, while those with no motion, excess motion, or distraction and a less rich blood supply produce less callus.
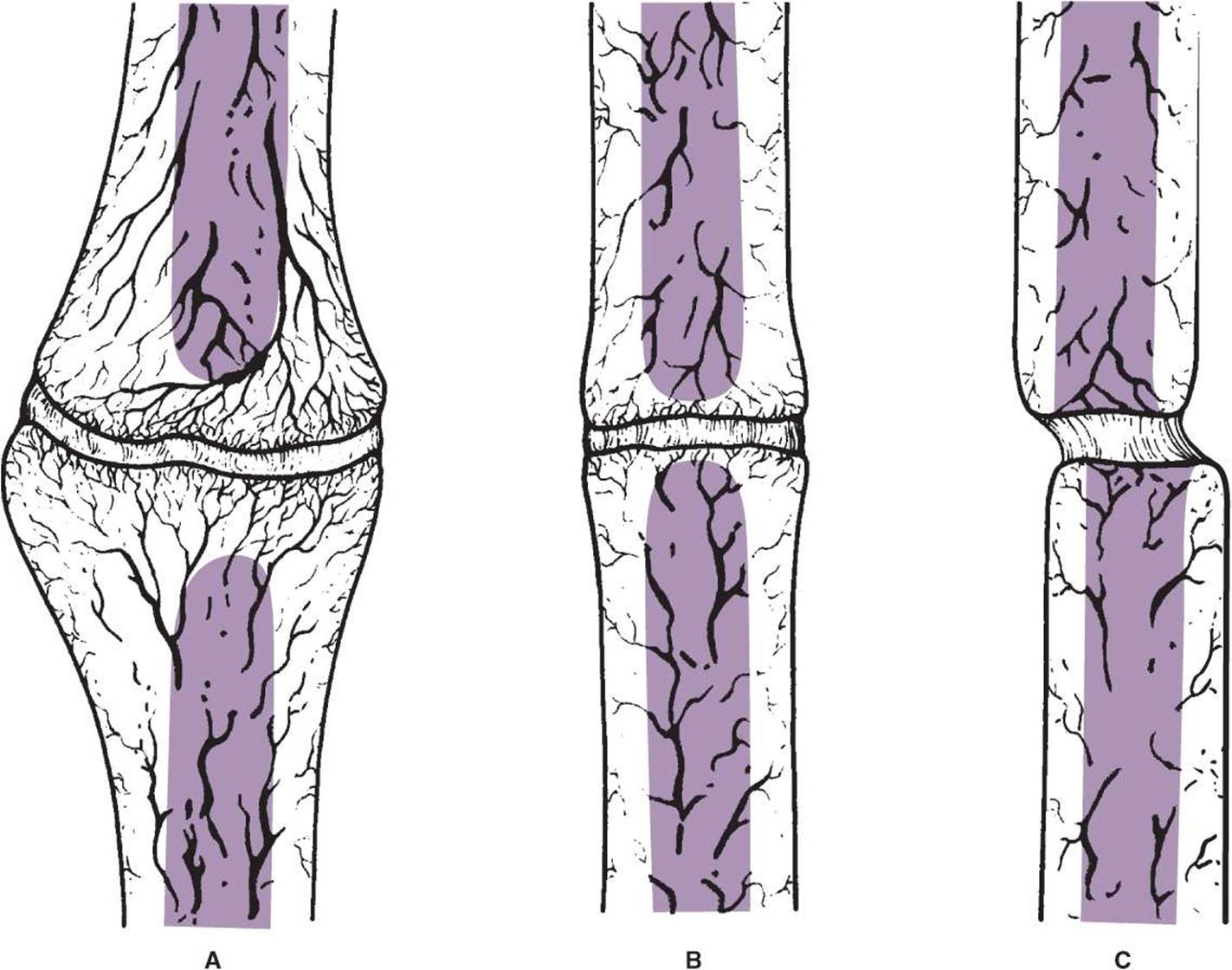
![]() Figure 2–28. Weber and Cech’s subclassification of hypertrophic nonunions: elephant’s foot (A); horse’s foot (B); and oligotrophic (C). (This can often resemble atrophic nonunion and is hard to distinguish.) (Reprinted, with permission, from Browner BD, Levine A, Jupiter J, et al, eds: Skeletal Trauma, 2nd ed. New York: WB Saunders; 1998.)
Figure 2–28. Weber and Cech’s subclassification of hypertrophic nonunions: elephant’s foot (A); horse’s foot (B); and oligotrophic (C). (This can often resemble atrophic nonunion and is hard to distinguish.) (Reprinted, with permission, from Browner BD, Levine A, Jupiter J, et al, eds: Skeletal Trauma, 2nd ed. New York: WB Saunders; 1998.)
C. Complications of Nonunion
Grossly mobile hypertrophic or atrophic nonunions that are left untreated for an extended period often develop into a pseudarthrosis (false joint) (Figure 2–29). There is an actual synovial-lined capsule enveloping the bone ends. Synovial fluid is present in the cleft. As a joint now exists between the ununited bone ends, surgical intervention is the only treatment option available.

![]() Figure 2–29. Fourteen-year-old distal humeral pseudarthrosis left untreated in an 89-year-old woman. All motion about the elbow is occurring through the pseudarthrosis, as the elbow is ankylosed.
Figure 2–29. Fourteen-year-old distal humeral pseudarthrosis left untreated in an 89-year-old woman. All motion about the elbow is occurring through the pseudarthrosis, as the elbow is ankylosed.
D. Treatment
The degree of shortening or deformity of the affected limb and the joints above and below the nonunion must be evaluated to determine their function and motion. One must also determine the general health of the patient as well as the degree of functional impairment the patient is actually experiencing. This is especially important because some patients are actually asymptomatic and therefore do not warrant treatment. Treatment must also be tailored in the sick or elderly (>70 years) because these patients may not be able to safely tolerate surgical intervention.
1. Stimulation of osteogenesis by external forces—It is now known that several pathways exist to stimulate healing of nonunion. The pathways can be divided into the type of force required to stimulate osteogenesis. These inductive forces can be categorized as mechanical, electrical, and chemical and can be applied with varying success both operatively and nonoperatively.
A. MECHANICAL FORCES—Cyclic mechanical force of ambulation while the fracture reduction is maintained with an external support is the presumed mechanism with which fracture healing is achieved without surgical intervention. Sarmiento has shown that the use of functional bracing incorporated with weight bearing can lead to union of documented tibial nonunions.
Mechanical forces can also be generated by surgical means. Mechanical stabilization of a long bone nonunion can be achieved either by placement of an intramedullary rod or compression plating. The rod works by providing mechanical stabilization of the fracture, hence allowing for cyclic axial loading of the limb without shearing forces caused by weight bearing. The compression plate provides stability as well as immediate rigid compression across the fracture fragments. These forms of treatment are often all that is necessary in elephant’s foot-type nonunions.
B. ELECTRICAL STIMULATION—Studies generated by Fukada and Yasuda led to the development of electrical bone growth stimulators for clinical application in the treatment of delayed union and nonunion. Electrical fields have been shown to stimulate the inactive chondrocytes and mesenchymal cells in the nonunion site to “turn on” and produce bone that results in healing. Surgically implanted devices have the disadvantage of implantation, removal, and infection, so shorter application time would be advantageous. Current opinion is to use combined magnetic fields applied over fracture sites.
c. Biologic enhancement—Chemical modulators also play an important role in promoting nonunion healing. Application of autogenous cancellous bone graft (most frequently obtained from the iliac crest) is a potent stimulator of fracture healing. Because a rigid nonunion will heal with autogenous bone grafting alone and no internal fixation, it is apparent that chemical modulators from the grafted cancellous bone are responsible for stimulating the healing response. There has been recent intense interest in determining the growth factors present in this cancellous bone responsible for “turning on” the healing process. Some surgeons have even reported success by obtaining bone marrow via a large-bore needle from the iliac crest and injecting this into the nonunion site. In the future, it is likely that the humoral modulator responsible will be isolated, synthesized in sufficient quantities by genetic engineering techniques, and simply injected into nonunion clefts to attain union.
2. Atrophic nonunions—Atrophic nonunions are not as easily treated as hypertrophic nonunions, and fewer treatment options are available. Electrical stimulation and nonoperative treatment methods have not been effective. The treatment most commonly used, and most successfully, is “freshening up” of the avascular bone ends, combined with rigid internal fixation and autogenous bone grafting. This same procedure is used in treating pseudarthroses.
The Ilizarov method has also shown great success in the treatment of complex hypertrophic and atrophic nonunions, sometimes in combination with autogenous bone grafting. This method allows not only for achievement of bony union but also for treatment of any accompanying deformity, segmental bone loss, or shortening that may be present.
![]() Malunion of Fracture (ICD-9:733.81)
Malunion of Fracture (ICD-9:733.81)
A fracture that has healed with an unacceptable amount of angulation, rotation, or overriding that has resulted in shortening of the limb is defined as malunion. Shortening is better tolerated in the upper than the lower extremity, and angulatory deformities are better tolerated in bones such as the humerus than in the femur or tibia. Hence, no absolute guidelines can be given as to an acceptable versus an unacceptable malunion. Generally, shortening greater than 1 in is poorly tolerated in the lower extremity. Smaller discrepancies, however, are well treated with just a shoe lift in most situations. When the degree of deformity is sufficient to cause pain (eg, caused by walking on the side of the foot secondary to varus malunion of the distal tibia) or impair normal function, surgical correction of the malunion is indicated.
When correction of malunion is undertaken, proper preoperative planning is imperative. Determination of the true plane of deformity is essential in planning for the surgical correction. One must determine the true mechanical axis of the limb to determine the actual site of deformity. If an osteotomy is performed, the surgeon must decide whether to use a closing wedge (where a wedge of bone is removed) or an opening wedge (where a wedge of autogenous or allograft bone is added). This is important, as it will alter the limb length. If the limb is already short, the surgery should also include a limb-lengthening procedure. Proper fixation and often autogenous cancellous bone grafting should be incorporated to ensure that the osteotomy heals, because converting a malunion to a nonunion is only worsening an already bad situation. Special care must be paid to treatment of the soft tissues to prevent wound breakdown and infection.
![]() Ilizarov Method
Ilizarov Method
Since its introduction in Kurgan, Siberia, in 1951 by Gavril A. Ilizarov, the Ilizarov apparatus and the concepts of distraction osteogenesis have dramatically revolutionized the application of the principles of external fixation in the management of bony defects, nonunions, malunions, pseudarthroses, and osteomyelitis. Ilizarov realized that healing and neogenesis both required a dynamic state, which could occur in either controlled distraction or compression. This dogma is a function of many principles that Ilizarov classified into three categories: biologic, clinical, and technical. Important biologic concepts include preservation of endosteal and periosteal blood supply via low-energy corticotomy and stable fixation. A 5- to 7-day latency and a distraction rate of 1 mm/day in three or four divided increments follow the osteotomy. At the termination of distraction, neutral fixation is required to allow maturation, calcification, and strengthening of the new bone. In essence, the technique fools the body into believing it is a child again, with the corticotomy site acting as a physis. Ilizarov fixation prevents shearing forces but permits axial micromotion with postoperative weight bearing, which enhances bone formation. From a technical viewpoint, the Ilizarov method relies on the use of an extremely rigid (in all planes except the axial loading plane), extremely versatile external fixator, employing K-wire fixation under tension. It is this “tension stress” phenomenon of gradually controlled distraction of bone ends at the corticotomy site that makes possible the limb lengthening or osteogenesis required in bone transport. Neogenesis of the accompanying soft tissues, including vessels, nerves, muscle, and skin, also occurs. Likewise, because of the dynamic nature of the apparatus, constant high loads of compression can be maintained across fracture sites to help stimulate fracture healing. A hyperemic state exists during distraction osteogenesis, with abundant neovascularization in the distraction gap. The overall blood flow to the affected limb is also increased up to 40%.
The most important parts of circular fixators are rings and rods. Ring diameter and the distance between the rings affect the stability. Small-diameter rings are more stable; however, a general rule is to leave 2 cm of space between the ring and skin circumferentially to allow for possible limb swelling. Rings that are far apart and connected with long rods will be less stable. Ideally, four connecting rods between the rings and at least two points of fixation or wires per ring are required. Two diameters of wires are used: 1.5 mm in small children and in upper extremities in adults, and 1.8 mm (twice as stiff in bending) in lower extremities in adults and adolescents. Beaded wires (olive wires) are used for bony transport, as well as to provide for rigidity of fixation, to prevent unwanted translation of the bone on the frame. An appropriately applied frame on the lower extremity should allow full weight bearing on the limb, irrespective of the extent of the bony defect present. This cyclic axial loading of the affected limb is a crucial element of the Ilizarov method.
Clinical principles such as the geometry of the apparatus once it is constructed, adjustment of the rate of transport, and wound care directly affect the outcome of the procedure. The initial operation for the application of the apparatus is only one small part in the whole treatment scheme. The construct should be as safe and comfortable as possible because the apparatus is worn for an extended period of time. Pin tract infections are common and must be addressed aggressively with oral antibiotics and local pin care.
With the incorporation of hinges, plates, rods, and other elements, correction of a deformity can be accomplished in any plane. Hence, the apparatus has become an increasingly useful tool in the treatment of congenital, acquired, and posttraumatic limb deformities, as well as nonunion and malunion. What makes this treatment method unique is that all problems affecting a limb can be managed with the application of one apparatus.
Bhandari M, Guyatt GH, Tong D, et al: Reamed versus nonreamed intramedullary nailing of lower extremity long bone fractures: a systematic overview and meta-analysis. J Orthop Trauma 2000;14:2. [PMID: 10630795]
Einhorn TA, Lee CA: Bone regeneration: new findings and potential clinical applications. J Am Acad Orthop Surg 2001;9:157. [PMID: 11421573]
Goldstein C, Spraque S, Petrisor BA: Electrical stimulation for fracture healing: current evidence. J Orthop Trauma 2010; 24(Suppl 1): S62. [PMID: 20182239]
Hak DJ, Lee SS, Goulet JA: Success of exchange reamed intramedullary nailing for femoral shaft nonunion or delayed union. J Orthop Trauma 2000;14:178. [PMID: 10791668]
Henson P, Bruehl S: Complex regional pain syndrome: state of the art update. Curr Treat Options Cardiovasc Med 2010;12:156. [PMID: 20842553]
Hupel TM, Weinberg JA, Aksenov SA, Schemitsch EH: Effect of unreamed, limited reamed, and standard reamed intramedullary nailing on cortical bone porosity and new bone formation. J Orthop Trauma2001;15:18. [PMID: 11147683]
Ilizarov GA: The significance of the combination of optimal mechanical and biological factors in the regenerate process of transosseous synthesis. In: Abstracts of First International Symposium on Experimental, Theoretical, and Clinical Aspects of Transosseous Osteosynthesis Method Developed in Kniekot, Kurgan, USSR, September 20–23, 1983.
Ilizarov GA: Transosseous Osteosynthesis. New York: Springer-Verlag; 1992.
Katsenis D, Bhave A, Paley D, et al: Treatment of malunion and nonunion at the site of an ankle fusion with the Ilizarov apparatus. J Bone Joint Surg Am 2005;87:302. [PMID: 15687151]
Lowenberg DW, Randall RL: The Ilizarov method. In: Braverman MH, Tawes RL, eds: Surgical Technology International II. San Francisco: Surgical Technology International; 1993.
Marsh D: Concepts of fracture union, delayed union, and nonunion. Clin Orthop Relat Res 1998;355S:S22. [PMID: 9917623]
Paley D, Maar DC: Ilizarov bone transport treatment for tibial defects. J Orthop Trauma 2000;14:76. [PMID: 10716377]
Spiegelberg B, Parratt T, Dheerendra SK, Khan WS, Jennings R, Marsh DR: Ilizarov principles of deformity correction. Ann R Coll Surg Engl 2010;92:101. [PMID: 20353638]
Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nails for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335. [PMID: 11029556]