MORBIDITY AND MORTALITY
![]() The leading cause of death in children under 1 year of age is grouped under the term perinatal conditions, which include:
The leading cause of death in children under 1 year of age is grouped under the term perinatal conditions, which include:
![]() Congenital malformation, deformations, and chromosomal abnormalities (number one cause).
Congenital malformation, deformations, and chromosomal abnormalities (number one cause).
![]() Low birth weight.
Low birth weight.
![]() Sudden infant death syndrome (SIDS).
Sudden infant death syndrome (SIDS).
![]() Respiratory distress syndrome.
Respiratory distress syndrome.
![]() Complications of pregnancy.
Complications of pregnancy.
![]() Perinatal infections.
Perinatal infections.
![]() Intrauterine or birth hypoxia.
Intrauterine or birth hypoxia.
![]() From 1 year to 24 years of age, the leading cause of death is injury (unintentional injuries).
From 1 year to 24 years of age, the leading cause of death is injury (unintentional injuries).
PREVENTION
Prevention is of primary importance in caring for the pediatric patient and is promoted through:
![]() Parental guidance (anticipatory guidance and counseling).
Parental guidance (anticipatory guidance and counseling).
![]() Screening tests.
Screening tests.
![]() Immunization.
Immunization.
PARENTAL GUIDANCE
Age-appropriate anticipatory guidance is provided to parents at various well-child visits.
1 Week–1 Month
![]()
A 1-month-old infant is brought to the ED with poor feeding, weak suck, drooling, constipation, and ![]() spontaneous movements. He is exclusively breast-fed, and his mother has been giving him home remedy for “colic”. Physical exam is positive for hypotonia. Think: Botulism and its relationship with some home remedies prepared with honey. Treatment is with human botulism immune globulin (BIG-IV).
spontaneous movements. He is exclusively breast-fed, and his mother has been giving him home remedy for “colic”. Physical exam is positive for hypotonia. Think: Botulism and its relationship with some home remedies prepared with honey. Treatment is with human botulism immune globulin (BIG-IV).
![]() Place infant to sleep on back to prevent sudden infant death syndrome (SIDS).
Place infant to sleep on back to prevent sudden infant death syndrome (SIDS).
![]() Use a car seat.
Use a car seat.
![]() Know signs of an illness.
Know signs of an illness.
![]() Maintain a smoke-free environment (associated with SIDS and ear infections).
Maintain a smoke-free environment (associated with SIDS and ear infections).
![]() Maintain water temperature at < 120°F (48.8°C).
Maintain water temperature at < 120°F (48.8°C).
![]() Do not give honey to a child under 1 year of age (risk for botulism).
Do not give honey to a child under 1 year of age (risk for botulism).
![]() Discuss normal crying behavior and give some suggestions for how to calm the infant.
Discuss normal crying behavior and give some suggestions for how to calm the infant.

Be informed of social services and financial assistance available to parents and patients.
2 Months–1 Year
![]() Childproof home to keep children safe from poisons, household cleaners, medications, buckets and tubs filled with water, plastic bags, electrical outlet covers, hot liquids, matches, small and sharp objects, guns, and knives.
Childproof home to keep children safe from poisons, household cleaners, medications, buckets and tubs filled with water, plastic bags, electrical outlet covers, hot liquids, matches, small and sharp objects, guns, and knives.
![]()
Any child with a rectal temperature > 100.4°F (38°C) in the first 3 months of life should be seen immediately.
![]() The American Academy of Pediatrics (AAP) does not recommend syrup of ipecac anymore. Explain proper use of syrup of ipecac for poisonings, and give telephone number to local poison control hotline.
The American Academy of Pediatrics (AAP) does not recommend syrup of ipecac anymore. Explain proper use of syrup of ipecac for poisonings, and give telephone number to local poison control hotline.
![]() No solid food until 4–6 months.
No solid food until 4–6 months.
![]() Avoid baby walkers.
Avoid baby walkers.
![]() Do not put baby to bed with bottle, as it can cause dental caries.
Do not put baby to bed with bottle, as it can cause dental caries.
![]() Breast-feed or give iron-fortified formula, but no whole milk until after 1 year of age.
Breast-feed or give iron-fortified formula, but no whole milk until after 1 year of age.
![]() Avoid choking hazards such as coins, peanuts, popcorn, carrot sticks, hard candy, whole grapes, and hot dogs.
Avoid choking hazards such as coins, peanuts, popcorn, carrot sticks, hard candy, whole grapes, and hot dogs.
![]() May start using cup at 6–9 months.
May start using cup at 6–9 months.
![]()
Falls and drowning are major risks of injury and death in toddlers.
1–5 Years
![]() Use toddler car seat (ages 1–4) and booster seat (ages 4–8) if proper weight and height.
Use toddler car seat (ages 1–4) and booster seat (ages 4–8) if proper weight and height.
![]() Brush teeth, see dentist.
Brush teeth, see dentist.
![]() Wean from bottle (start by 9 months of age with the introduction of cup).
Wean from bottle (start by 9 months of age with the introduction of cup).
![]() Make sure home is childproof again.
Make sure home is childproof again.
![]()
Most infants drown in their own bathtub.
![]() Restrict child’s access to stairs.
Restrict child’s access to stairs.
![]() Allow child to eat with hands or utensils.
Allow child to eat with hands or utensils.
![]() Use sunscreen.
Use sunscreen.
![]() Wear properly fitting bicycle helmet.
Wear properly fitting bicycle helmet.
![]() Provide close supervision, especially near dogs, driveways, streets, and lawnmowers.
Provide close supervision, especially near dogs, driveways, streets, and lawnmowers.
![]() Make appointment with dentist by 1 year of age.
Make appointment with dentist by 1 year of age.
![]() Ensure that child is supervised when near water; build fence around swimming pool with latched gate.
Ensure that child is supervised when near water; build fence around swimming pool with latched gate.
![]() Screen for amblyopia, strabismus, and visual acuity in all children younger than 5 years.
Screen for amblyopia, strabismus, and visual acuity in all children younger than 5 years.
![]() Strabismus: Cover test or Hirschberg light reflex test in children < 3 years.
Strabismus: Cover test or Hirschberg light reflex test in children < 3 years.
![]() Visual acuity: > 3 years and screen every 1–2 years throughout childhood.
Visual acuity: > 3 years and screen every 1–2 years throughout childhood.
Temperature of the water heater should be kept below 120°F (49°C) to prevent accidental scalding injuries.
6–10 Years
![]() Reinforce personal hygiene.
Reinforce personal hygiene.
![]() Teach stranger safety.
Teach stranger safety.
![]() Provide healthy meals and snacks.
Provide healthy meals and snacks.
![]() Keep matches and guns out of children’s reach.
Keep matches and guns out of children’s reach.
![]() Use seat belt always, and booster seat until 4 feet 9 inches in height.
Use seat belt always, and booster seat until 4 feet 9 inches in height.
11–21 Years
![]() Continue to support a healthy diet and exercise.
Continue to support a healthy diet and exercise.
![]() Wear appropriate protective sports gear.
Wear appropriate protective sports gear.
![]() Counsel on safe sex and avoiding alcohol and drugs.
Counsel on safe sex and avoiding alcohol and drugs.
![]() Promote a healthy social life, balanced diet, and at least 30 minutes of exercise every day.
Promote a healthy social life, balanced diet, and at least 30 minutes of exercise every day.
![]() Ask about mood or eating disorders (see below).
Ask about mood or eating disorders (see below).
SCREENING
Blood Pressure
![]() Routine monitoring of blood pressure should begin at age 3 years.
Routine monitoring of blood pressure should begin at age 3 years.
![]() Most common cause of high blood pressure reading in children is inappropriate cuff size.
Most common cause of high blood pressure reading in children is inappropriate cuff size.
Metabolic Screening
In the first month of life, the neonate should receive screening for various metabolic disorders including hypothyroidism, phenylketonuria (PKU), sickle cell disease, and adrenal cortex abnormalities.
Metabolic screening may vary from state to state in the United States.
Lead Screening
![]() Exposure is
Exposure is ![]() by:
by:
![]() Living in or visiting a house built before 1960 with peeling or chipped paint.
Living in or visiting a house built before 1960 with peeling or chipped paint.
![]() Plumbing with lead pipes or lead solder joints.
Plumbing with lead pipes or lead solder joints.
![]() Living near a major highway where soil may be contaminated with lead.
Living near a major highway where soil may be contaminated with lead.
![]() Contact with someone who works with lead.
Contact with someone who works with lead.
![]() Living near an industrial site that may release lead into the environment.
Living near an industrial site that may release lead into the environment.
![]() Taking home remedies that may contain lead.
Taking home remedies that may contain lead.
![]() Having friends/relatives who have had lead poisoning.
Having friends/relatives who have had lead poisoning.
![]() Screen for lead levels at age 12 months.
Screen for lead levels at age 12 months.
Hematocrit
![]() Screen for anemia at 9–12 months of age where certification is needed for WIC (Women, Infants, and Children) or if the appropriate risk factors are present.
Screen for anemia at 9–12 months of age where certification is needed for WIC (Women, Infants, and Children) or if the appropriate risk factors are present.
![]() Second test 6 months later in high-risk communities for iron deficiency.
Second test 6 months later in high-risk communities for iron deficiency.
![]() Anemia: Hemoglobin levels < 11 g/dL.
Anemia: Hemoglobin levels < 11 g/dL.
Hyperlipidemia
![]() Screen for hyperlipidemia in children older than 2 years with appropriate risk factors:
Screen for hyperlipidemia in children older than 2 years with appropriate risk factors:
![]() Family history of coronary or peripheral vascular disease before the age of 55 years in parents or grandparents.
Family history of coronary or peripheral vascular disease before the age of 55 years in parents or grandparents.
![]() Parent with a total serum cholesterol level > 240 mg/dL.
Parent with a total serum cholesterol level > 240 mg/dL.
![]() Obesity.
Obesity.
![]() Hypertension.
Hypertension.
![]() Diabetes mellitus.
Diabetes mellitus.
![]() Screening may also be considered in children with inactivity; also in adolescents who smoke.
Screening may also be considered in children with inactivity; also in adolescents who smoke.
![]() Risk factors for anemia include low socioeconomic status, birth weight under 1500 g, whole milk received before 6 months of age, low-iron formula given, low intake of iron-rich foods.
Risk factors for anemia include low socioeconomic status, birth weight under 1500 g, whole milk received before 6 months of age, low-iron formula given, low intake of iron-rich foods.
Vision and Hearing
![]() A hearing screen is recommended shortly after birth.
A hearing screen is recommended shortly after birth.
![]() Vision screening may begin at age 3 years, sooner if concerns.
Vision screening may begin at age 3 years, sooner if concerns.
![]() Suspect hearing loss earlier if child’s speech is not developing appropriately.
Suspect hearing loss earlier if child’s speech is not developing appropriately.
![]() A child’s cooperation is essential to obtaining an accurate result (~3 years).
A child’s cooperation is essential to obtaining an accurate result (~3 years).
CAR SEATS
![]() Car seats should be used for travel in automobiles for children from birth until the child reaches at least 40 pounds.
Car seats should be used for travel in automobiles for children from birth until the child reaches at least 40 pounds.
![]() Children under 20 pounds should be in an infant car seat, which belongs in the back seat and is rear-facing.
Children under 20 pounds should be in an infant car seat, which belongs in the back seat and is rear-facing.
![]() Children from 20 pounds to 40 pounds belong in a car seat that is in the back seat but may be forward facing.
Children from 20 pounds to 40 pounds belong in a car seat that is in the back seat but may be forward facing.
![]() Never place a car seat in front of an air bag (front passenger-side and side-impact air bags). The safest place for the infant is the middle portion of the rear seat.
Never place a car seat in front of an air bag (front passenger-side and side-impact air bags). The safest place for the infant is the middle portion of the rear seat.
![]() Make sure parents understand the proper use of car seats.
Make sure parents understand the proper use of car seats.
![]() Booster seats should be used until the child is 4 feet 9 inches tall (generally ages 4–8).
Booster seats should be used until the child is 4 feet 9 inches tall (generally ages 4–8).
Newborns should not leave the hospital without a car seat.
VACCINES
![]() See page 13.
See page 13.
![]() Site of injection:
Site of injection:
![]() Infants: Anterolateral thigh.
Infants: Anterolateral thigh.
![]() Children: Deltoid.
Children: Deltoid.
Hepatitis B
![]()
A 25-year-old female who is hepatitis B surface antigen positive is about to deliver a baby and she asks what is the best way to prevent the baby from having hepatitis B. Think: Prevention.
Babies born to women who are hepatitis B surface antigen positive receive hepatitis B immunoglobulin and hepatitis B vaccine shortly after birth, and 1–2 months after completing three doses of hepatitis B vaccine, they should be tested for hepatitis B surface antigen as well as the antibody.
![]() First given intramuscularly (IM) at birth or within first 2 months of life.
First given intramuscularly (IM) at birth or within first 2 months of life.
![]() Second dose given 1 month after first dose.
Second dose given 1 month after first dose.
![]() Third dose given 4 months after first dose and 2 months after second dose, but not before 6 months of age.
Third dose given 4 months after first dose and 2 months after second dose, but not before 6 months of age.
![]() Must give at birth along with hepatitis B immune globulin (HBIG) if baby is exposed transplacentally or if maternal status is unknown.
Must give at birth along with hepatitis B immune globulin (HBIG) if baby is exposed transplacentally or if maternal status is unknown.
![]() Infants born to HBsAg-positive mothers should be tested for HBsAg and antibody to HBsAg 1–2 months after completion of at least three doses of the HepB vaccine, at age 9–18 months.
Infants born to HBsAg-positive mothers should be tested for HBsAg and antibody to HBsAg 1–2 months after completion of at least three doses of the HepB vaccine, at age 9–18 months.
Fever is not a contraindication to receiving immunization. Moderate/severe illness is a contraindication. This holds true for all vaccines.
CONTENT
Adsorbed recombinant hepatitis B surface antigen proteins.
SIDE EFFECTS
![]() Pain at injection site.
Pain at injection site.
![]() Fever > 99.9°F (37.7°C) in 1–6%.
Fever > 99.9°F (37.7°C) in 1–6%.
CONTRAINDICATIONS
Anaphylactic reaction to vaccine, yeast, or another vaccine constituent.
![]()
DTaP is preferred for children under 7 years of age. Td or Tdap is given after 7 years of age.
Diphtheria, Tetanus, and Acellular Pertussis (DTaP)
![]() Minimum age: 6 weeks.
Minimum age: 6 weeks.
![]() Given IM at 2, 4, and 6 months of age, then another between 12 and 18 months of age.
Given IM at 2, 4, and 6 months of age, then another between 12 and 18 months of age.
![]() The fourth dose may be administered as early as age 12 months; must allow 6 months between third and fourth doses.
The fourth dose may be administered as early as age 12 months; must allow 6 months between third and fourth doses.
![]() Administer the final dose at age 4–6 years.
Administer the final dose at age 4–6 years.
![]()
DTP has greater risks of side effects than DTaP.
CONTENT
![]() DTaP is diphtheria and tetanus toxoids with acellular pertussis.
DTaP is diphtheria and tetanus toxoids with acellular pertussis.
![]() DTP contains a whole-cell pertussis.
DTP contains a whole-cell pertussis.
![]()
DTaP is not a substitute for DTP if a contraindication to pertussis exists.
SIDE EFFECTS
![]() Erythema, pain, and swelling at injection site.
Erythema, pain, and swelling at injection site.
![]() Fever > 100.9°F (38.3°C) in 3–5%.
Fever > 100.9°F (38.3°C) in 3–5%.
![]() Anaphylaxis in 1/50,000.
Anaphylaxis in 1/50,000.
CONTRAINDICATIONS
![]() Anaphylactic reaction to vaccine or another vaccine constituent.
Anaphylactic reaction to vaccine or another vaccine constituent.
![]() Encephalopathy not attributable to another cause within 7 days of a prior dose of pertussis vaccine.
Encephalopathy not attributable to another cause within 7 days of a prior dose of pertussis vaccine.
Haemophilus influenzae Type B (Hib)
![]() Minimum age: 6 weeks.
Minimum age: 6 weeks.
![]() Given IM at 2, 4, and 6 months of age, then again between 12 and 15 months of age.
Given IM at 2, 4, and 6 months of age, then again between 12 and 15 months of age.
CONTENT
Consists of a capsular polysaccharide antigen conjugated to a carrier.
SIDE EFFECTS
Erythema, pain, and swelling at injection site in 25%.
CONTRAINDICATIONS
Anaphylactic reaction to vaccine or vaccine constituent.
Measles, Mumps, and Rubella
![]()
A 12-month-old boy is due for his vaccines in the middle of October. His mother mentions that he developed a skin rash as well as some respiratory problems 1 month prior after she fed him eggs for the first time. He is due for MMR, varicella, and influenza vaccines. Think: Egg allergy and the vaccines that are contraindicated: Influenza vaccine, yellow fever vaccine. MMR can be given safely to children with egg allergy.
![]()
MMR is a live virus vaccine.
![]() Minimum age: 12 months.
Minimum age: 12 months.
![]() First dose given subcutaneously (SC) at 12–15 months of age, and second dose at 4–6 years of age.
First dose given subcutaneously (SC) at 12–15 months of age, and second dose at 4–6 years of age.
![]() Second dose may be given at any time after 4 weeks from first dose if necessary.
Second dose may be given at any time after 4 weeks from first dose if necessary.
![]() Must be at least 12 months old to ensure a sufficient response.
Must be at least 12 months old to ensure a sufficient response.
CONTENT
Composed of live attenuated viruses.
SIDE EFFECTS
![]() Fever > 102.9°F (39.4°C) 7–12 days after immunization in 10%.
Fever > 102.9°F (39.4°C) 7–12 days after immunization in 10%.
![]() Transient rash in 5%.
Transient rash in 5%.
![]() Febrile seizures and encephalopathy with MMR vaccine are rare. Transient thrombocytopenia may occur 2–3 weeks after vaccine in 1/40,000.
Febrile seizures and encephalopathy with MMR vaccine are rare. Transient thrombocytopenia may occur 2–3 weeks after vaccine in 1/40,000.
CONTRAINDICATIONS
![]() Anaphylactic reaction to prior vaccine.
Anaphylactic reaction to prior vaccine.
![]() Anaphylactic reaction to neomycin or gelatin.
Anaphylactic reaction to neomycin or gelatin.
![]() Immunocompromised states.
Immunocompromised states.
![]() Pregnant women.
Pregnant women.
![]() Recent intravenous immune globulin (IVIg) administration requires delaying vaccinations by 12 months.
Recent intravenous immune globulin (IVIg) administration requires delaying vaccinations by 12 months.
Inactivated Poliovirus Vaccine (IPV)
![]() Minimum age: 6 weeks.
Minimum age: 6 weeks.
![]() Given SC at 2 and 4 months, then again between 6 and 18 months, then a fourth between 4 and 6 years of age.
Given SC at 2 and 4 months, then again between 6 and 18 months, then a fourth between 4 and 6 years of age.
![]() The final dose should be administered on or after the fourth birthday and at least 6 months following the previous dose.
The final dose should be administered on or after the fourth birthday and at least 6 months following the previous dose.
![]() If four doses are administered prior to age 4 years, a fifth dose should be administered at age 4–6 years.
If four doses are administered prior to age 4 years, a fifth dose should be administered at age 4–6 years.
![]() OPV is given orally.
OPV is given orally.
CONTENT
![]() IPV contains inactivated poliovirus types 1, 2, and 3.
IPV contains inactivated poliovirus types 1, 2, and 3.
![]() Live oral poliovirus vaccine (OPV) contains live attenuated poliovirus types 1, 2, and 3.
Live oral poliovirus vaccine (OPV) contains live attenuated poliovirus types 1, 2, and 3.
SIDE EFFECTS
![]() Vaccine-associated paralytic polio (VAPP) with OPV in 1/760,000.
Vaccine-associated paralytic polio (VAPP) with OPV in 1/760,000.
![]() With prior IPV, risk is reduced by 75–90%.
With prior IPV, risk is reduced by 75–90%.
![]()
An all-IPV schedule is recommended in the United States to prevent VAPP (vaccine-associated paralytic polio). Under certain circumstances, OPV may be used.
CONTRAINDICATIONS
![]() Anaphylaxis to vaccine or vaccine constituent.
Anaphylaxis to vaccine or vaccine constituent.
![]() Anaphylaxis to streptomycin, polymixin B, or neomycin.
Anaphylaxis to streptomycin, polymixin B, or neomycin.
![]()
OPV is contraindicated in immunodeficiency disorders or when household contacts are immunocompromised.
Varicella
![]() Minimum age: 12 months.
Minimum age: 12 months.
![]() Given SC between 12 and 18 months of age; second dose between 4 and 6 years (may be administered before age 4, provided at least 3 months have elapsed since the first dose).
Given SC between 12 and 18 months of age; second dose between 4 and 6 years (may be administered before age 4, provided at least 3 months have elapsed since the first dose).
![]() Susceptible persons > 13 years of age must receive two doses at least 4 weeks apart.
Susceptible persons > 13 years of age must receive two doses at least 4 weeks apart.
![]()
Varicella vaccine contains live virus.
CONTENT
Cell-free live attenuated varicella virus.
SIDE EFFECTS
![]() Erythema and swelling in 20–35%.
Erythema and swelling in 20–35%.
![]() Fever in 10%.
Fever in 10%.
![]() Varicelliform rash in 1–4%.
Varicelliform rash in 1–4%.
CONTRAINDICATIONS
![]() Anaphylactic reaction to vaccine, neomycin, or gelatin.
Anaphylactic reaction to vaccine, neomycin, or gelatin.
![]() Patients with altered immunity, including corticosteroid use for > 14 days.
Patients with altered immunity, including corticosteroid use for > 14 days.
![]() Patients on salicylate therapy.
Patients on salicylate therapy.
![]() Pregnant women.
Pregnant women.
![]() Recent blood product or IG administration (defer at least 5 months).
Recent blood product or IG administration (defer at least 5 months).
Influenza Vaccine (Seasonal)
![]() Minimum age: 6 months (trivalent inactivated influenza vaccine [TIV]); 2 years (live attenuated influenza vaccine) [LAIV]).
Minimum age: 6 months (trivalent inactivated influenza vaccine [TIV]); 2 years (live attenuated influenza vaccine) [LAIV]).
![]() Given IM to children > 6 months of age yearly beginning in autumn, usually between October and mid-November (two doses 1 month apart for the first time).
Given IM to children > 6 months of age yearly beginning in autumn, usually between October and mid-November (two doses 1 month apart for the first time).
![]() All children should receive this vaccine, especially high-risk children.
All children should receive this vaccine, especially high-risk children.
![]() Caution! LAIV should not be given to children aged 2–4 years who have had wheezing in the past 12 months.
Caution! LAIV should not be given to children aged 2–4 years who have had wheezing in the past 12 months.
CONTENT
It is especially important to vaccinate for influenza those with asthma, chronic lung disease, cardiac defects, immunosuppressive disorders, sickle cell anemia, chronic renal disease, and chronic metabolic disease.
![]() Contains three virus strains, usually two type A and one type B, and can be an inactivated whole-virus vaccine or a “split” vaccine containing disrupted virus particles.
Contains three virus strains, usually two type A and one type B, and can be an inactivated whole-virus vaccine or a “split” vaccine containing disrupted virus particles.
![]() Children < 9 years of age should receive the “split” vaccine only.
Children < 9 years of age should receive the “split” vaccine only.
![]() Children without prior exposure to influenza vaccine should receive two vaccines 1 month apart in order to obtain a good response.
Children without prior exposure to influenza vaccine should receive two vaccines 1 month apart in order to obtain a good response.
SIDE EFFECTS
![]() Pain, swelling, and erythema at injection site.
Pain, swelling, and erythema at injection site.
![]() Fever may occur, especially in children < 24 months of age.
Fever may occur, especially in children < 24 months of age.
![]() In children > 13 years of age, fever may occur in up to 10%.
In children > 13 years of age, fever may occur in up to 10%.
CONTRAINDICATIONS
Children with anaphylactic reactions to chicken or egg protein.
H1N1 Vaccine
Influenza vaccine does not cause the disease. The vaccine has been associated with an ![]() risk of GuillainBarré syndrome (GBS) in older adults, but no such cases have been reported in children.
risk of GuillainBarré syndrome (GBS) in older adults, but no such cases have been reported in children.
![]() Two doses separated by 4 weeks in children under 10 years of age.
Two doses separated by 4 weeks in children under 10 years of age.
![]() Two preparations:
Two preparations:
![]() Inactivated vaccine (killed virus).
Inactivated vaccine (killed virus).
![]() Nasal spray vaccine (live attenuated) approved for children > 2 years old.
Nasal spray vaccine (live attenuated) approved for children > 2 years old.
![]() The following patients should receive priority:
The following patients should receive priority:
1. Pregnant women.
2. Caregivers for infants aged < 6 months.
3. Health care providers.
4. Children aged 6 months–4 years.
5. Children and adolescents aged 5–18 years with medical conditions.
CONTRAINDICATIONS
1. Children younger than 6 months of age.
2. Severe allergy to chicken eggs.
3. Severe reaction to an influenza vaccination.
4. People who developed GBS within 6 weeks of getting an influenza vaccine previously.
Chemoprophylaxis against influenza is recommended as an alternative means of protection in those who cannot be vaccinated.
Pneumococcus (Conjugate Vaccine)
![]() Minimum age: 6 weeks for pneumococcal conjugate vaccine (PCV), 2 years for pneumococcal polysaccharide vaccine (PPSV).
Minimum age: 6 weeks for pneumococcal conjugate vaccine (PCV), 2 years for pneumococcal polysaccharide vaccine (PPSV).
![]() Babies receive three doses (shots) 2 months apart starting at 2 months, and a fourth dose when they are 12–15 months old.
Babies receive three doses (shots) 2 months apart starting at 2 months, and a fourth dose when they are 12–15 months old.
![]() Also given to high-risk children ≤ 2 years of age.
Also given to high-risk children ≤ 2 years of age.
![]() PCV is recommended for all children aged younger than 5 years. Administer one dose of PCV to all healthy children aged 24–59 months who are not completely immunized for their age.
PCV is recommended for all children aged younger than 5 years. Administer one dose of PCV to all healthy children aged 24–59 months who are not completely immunized for their age.
![]() Administer PPSV ≤ 2 months after last dose of PCV to children aged 2 years or older with certain underlying medical conditions, including a cochlear implant.
Administer PPSV ≤ 2 months after last dose of PCV to children aged 2 years or older with certain underlying medical conditions, including a cochlear implant.
The pneumococcal vaccine helps to protect against meningitis, bacteremia, pneumonia, and otitis media caused by serotypes of Streptococcus pneumoniae.
CONTENT
![]() The older PPV-23 vaccine (not indicated under age 2) contains the purified capsular polysaccharide antigens of 23 pneumococcal serotypes. The PPV-23 is usually reserved for high-risk children.
The older PPV-23 vaccine (not indicated under age 2) contains the purified capsular polysaccharide antigens of 23 pneumococcal serotypes. The PPV-23 is usually reserved for high-risk children.
![]() The newer PCV-7 is the conjugate vaccine described above.
The newer PCV-7 is the conjugate vaccine described above.
SIDE EFFECTS
![]() Erythema and pain at injection site.
Erythema and pain at injection site.
![]() Anaphylaxis reported rarely.
Anaphylaxis reported rarely.
![]() Fever and myalgia are uncommon.
Fever and myalgia are uncommon.
CONTRAINDICATIONS
Usually deferred during pregnancy.
Hepatitis A Vaccine
![]() Minimum age: 12 months.
Minimum age: 12 months.
![]() Administer to all children aged 1 year (12–23 months).
Administer to all children aged 1 year (12–23 months).
![]() Administer two doses at least 6 months apart.
Administer two doses at least 6 months apart.
![]() Recommended for older children who live in areas where vaccination programs target older children, who are at
Recommended for older children who live in areas where vaccination programs target older children, who are at ![]() risk for infection, or for whom immunity against hepatitis A is desired.
risk for infection, or for whom immunity against hepatitis A is desired.
Meningococcal Vaccine
![]() Minimum age: 2 years for meningococcal conjugate vaccine (MCV4) and meningococcal polysaccharide vaccine (MPSV4).
Minimum age: 2 years for meningococcal conjugate vaccine (MCV4) and meningococcal polysaccharide vaccine (MPSV4).
![]() Administer MCV4 to children aged 2–10 years with:
Administer MCV4 to children aged 2–10 years with:
![]() Persistent complement component deficiency.
Persistent complement component deficiency.
![]() Anatomic or functional asplenia.
Anatomic or functional asplenia.
![]()
Live attenuated vaccines include:
![]() MMR
MMR
![]() VZV
VZV
![]() Nasal influenza vaccine
Nasal influenza vaccine
![]() OPV
OPV
![]() Smallpox
Smallpox
![]() Typhoid
Typhoid
These should be avoided in the immunocompromised.
Rotavirus Vaccine
![]() Minimum age: 6 weeks.
Minimum age: 6 weeks.
![]() Administer the first dose at age 6–14 weeks (maximum age: 14 weeks 6 days). Vaccination should not be initiated for infants aged 15 weeks 0 days or older.
Administer the first dose at age 6–14 weeks (maximum age: 14 weeks 6 days). Vaccination should not be initiated for infants aged 15 weeks 0 days or older.
![]() The maximum age for the final dose in the series is 8 months 0 days.
The maximum age for the final dose in the series is 8 months 0 days.
![]() If Rotarix rotavirus vaccine is administered at ages 2 and 4 months, a dose at 6 months is not indicated.
If Rotarix rotavirus vaccine is administered at ages 2 and 4 months, a dose at 6 months is not indicated.
Respiratory Syncytial Virus (RSV)
![]() Palivizumab (synagis) is a monoclonal antibody used for prophylaxis against infections with RSV.
Palivizumab (synagis) is a monoclonal antibody used for prophylaxis against infections with RSV.
![]() Given IM once a month at the beginning of RSV season, usually beginning in October and ending in March.
Given IM once a month at the beginning of RSV season, usually beginning in October and ending in March.
![]() Children < 2 years of age with chronic lung disease who have required medical therapy 6 months before the anticipated RSV season should receive the vaccine.
Children < 2 years of age with chronic lung disease who have required medical therapy 6 months before the anticipated RSV season should receive the vaccine.
![]() Children born at 32 weeks’ gestation or earlier with other risk factors for lung disease should receive the vaccine.
Children born at 32 weeks’ gestation or earlier with other risk factors for lung disease should receive the vaccine.
CONTENT
RSV immune globulin intravenous (RSV-IGIV) consists of RSV-neutralizing antibodies collected from donors selected for high serum titers.
Tuberculosis (TB)
The Mantoux test contains five tuberculin units of purified protein derivative (PPD).
SCREENING
![]() Asymptomatic children at high risk for tuberculosis should be screened with a PPD test annually.
Asymptomatic children at high risk for tuberculosis should be screened with a PPD test annually.
![]() The test is placed intradermally in:
The test is placed intradermally in:
![]() Children having contact with persons with confirmed or suspected disease.
Children having contact with persons with confirmed or suspected disease.
![]() Children with radiographic or clinical findings of TB.
Children with radiographic or clinical findings of TB.
![]() Children from medically underserved populations (eg, low income, homeless, injection drug users).
Children from medically underserved populations (eg, low income, homeless, injection drug users).
![]() Children with travel history to endemic countries.
Children with travel history to endemic countries.
![]() Children with HIV.
Children with HIV.
![]() Children with clinical conditions that make them high risk.
Children with clinical conditions that make them high risk.
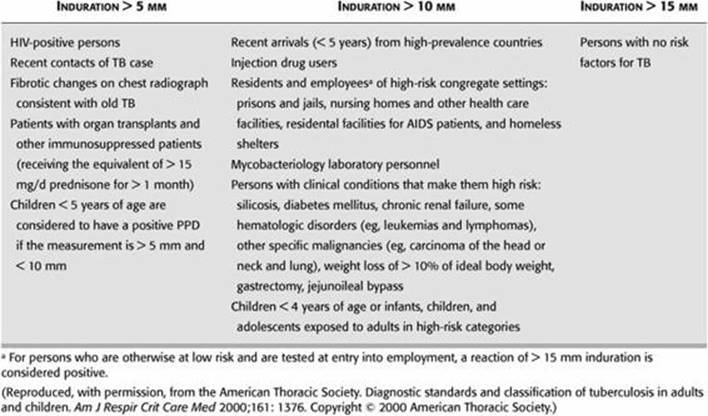
![]() Interpretation: See Table 6.1.
Interpretation: See Table 6.1.
TABLE 6-1. Guidelines for Determining a Positive Tuberculin Skin Test Reaction
![]() The QuantiFERON®-TB Gold test (QFT-G) is a newer alternative for detection of TB, approved by the U.S. Food and Drug Administration (FDA) in 2005.
The QuantiFERON®-TB Gold test (QFT-G) is a newer alternative for detection of TB, approved by the U.S. Food and Drug Administration (FDA) in 2005.
![]() Advantages:
Advantages:
![]() Requires a single patient visit to draw a blood sample.
Requires a single patient visit to draw a blood sample.
![]() Results can be available within 24 hours.
Results can be available within 24 hours.
![]() Does not boost responses measured by subsequent test, which can happen with tuberculin skin tests (TSTs).
Does not boost responses measured by subsequent test, which can happen with tuberculin skin tests (TSTs).
![]() Is not subject to reader bias that can occur with TSTs.
Is not subject to reader bias that can occur with TSTs.
![]() Is not affected by prior BCG (bacille Calmette-Guerin) vaccination.
Is not affected by prior BCG (bacille Calmette-Guerin) vaccination.
![]() Disadvantages:
Disadvantages:
![]() Blood samples must be processed within 12 hours after collection while white blood cells are still viable.
Blood samples must be processed within 12 hours after collection while white blood cells are still viable.
![]() Limited data in children < 17 years of age, among persons recently exposed to Mycobacterium tuberculosis, and in immunocompromised persons.
Limited data in children < 17 years of age, among persons recently exposed to Mycobacterium tuberculosis, and in immunocompromised persons.
![]() Errors in collecting or transporting blood specimens or in running and interpreting the assay can
Errors in collecting or transporting blood specimens or in running and interpreting the assay can ![]() the accuracy of QFT-G.
the accuracy of QFT-G.
![]() Limited data on the use of QFT-G to determine who is at risk for developing TB disease.
Limited data on the use of QFT-G to determine who is at risk for developing TB disease.
MEDICATIONS
Only 25% of Food and Drug Administration (FDA)-approved drugs have been approved for pediatric use.
Differences Between Children and Adults
ABSORPTION
![]() Infants have thinner skin; therefore, topical substances can more likely cause systemic toxicity.
Infants have thinner skin; therefore, topical substances can more likely cause systemic toxicity.
![]() Children do not have the stomach acidity of adults until age 2, and gastric emptying time is slower and less predictable,
Children do not have the stomach acidity of adults until age 2, and gastric emptying time is slower and less predictable, ![]()
![]() absorption of some medications.
absorption of some medications.
Controls with Candida, measles, or diphtheria can be placed along with the PPD to test for anergy, although opinion may vary in practice.
DISTRIBUTION
![]() Less predictable in children.
Less predictable in children.
![]() Total body water
Total body water ![]() from 90% in infants to 60% in adults.
from 90% in infants to 60% in adults.
![]() Fat stores are similar to adults in term infants, but much less in preterm infants.
Fat stores are similar to adults in term infants, but much less in preterm infants.
![]() Newborns have smaller protein concentration, therefore less binding of substances in the blood.
Newborns have smaller protein concentration, therefore less binding of substances in the blood.
![]() Infants have an immature blood–brain barrier.
Infants have an immature blood–brain barrier.
METABOLISM
Infants metabolize some drugs more slowly or rapidly than adults and may create a different proportion of active metabolites.
ELIMINATION
Kidney function ![]() with age, so younger children may clear drugs less efficiently.
with age, so younger children may clear drugs less efficiently.
DOSAGE
Pediatric medications are generally dosed by milligrams per kilogram (mg/kg).
POISONING
EPIDEMIOLOGY
More often accidental in younger children and suicide gestures or attempts in older children/adolescents.
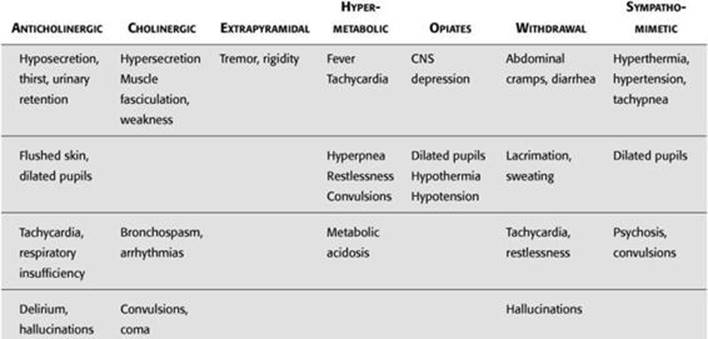
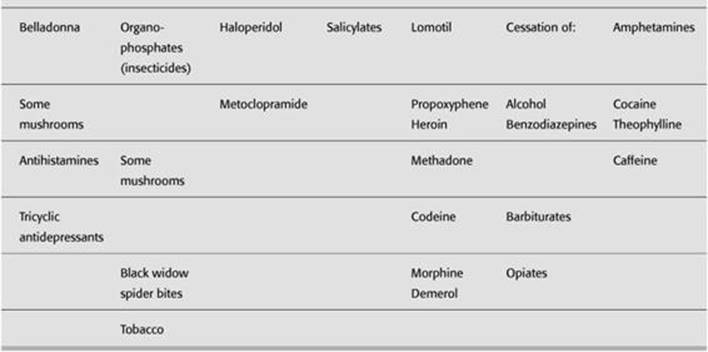
SIGNS AND SYMPTOMS
See Table 6-2.
PREVENTION
![]() Childproof home, including cabinets and containers.
Childproof home, including cabinets and containers.
![]() Store toxic substances in their original containers and out of children’s reach.
Store toxic substances in their original containers and out of children’s reach.
![]() Supervise children appropriately.
Supervise children appropriately.
![]() Have poison control center number easily accessible.
Have poison control center number easily accessible.
MANAGEMENT
![]() Frequently, ingested substances are nontoxic, but if symptoms arise or there is any question, a poison control center should be contacted.
Frequently, ingested substances are nontoxic, but if symptoms arise or there is any question, a poison control center should be contacted.
![]() History:
History:
![]() Precise name of product (generic, brand, chemical—bring container or extra substance/pills).
Precise name of product (generic, brand, chemical—bring container or extra substance/pills).
![]() Estimate amount of exposure, time of exposure.
Estimate amount of exposure, time of exposure.
![]() Progression of symptoms.
Progression of symptoms.
![]() Other medical conditions (eg, pregnancy, seizure disorder).
Other medical conditions (eg, pregnancy, seizure disorder).
![]() Gastric decontamination: Emesis (induced by syrup of ipecac) and gastric lavage remove only one third of stomach contents and are not generally recommended, though the combination of the latter with activated charcoal may be most effective.
Gastric decontamination: Emesis (induced by syrup of ipecac) and gastric lavage remove only one third of stomach contents and are not generally recommended, though the combination of the latter with activated charcoal may be most effective.
![]() Activated charcoal is effective for absorbing many drugs and chemicals, though it does not bind heavy metals, iron, lithium alcohols, hydrocarbons, cyanide. It may be used in conjunction with cathartics such as sorbitol or magnesium sulfate.
Activated charcoal is effective for absorbing many drugs and chemicals, though it does not bind heavy metals, iron, lithium alcohols, hydrocarbons, cyanide. It may be used in conjunction with cathartics such as sorbitol or magnesium sulfate.
![]() Dilution of stomach contents with milk has limited value except in the case of ingestion of caustic materials.
Dilution of stomach contents with milk has limited value except in the case of ingestion of caustic materials.
![]() Skin decontamination: Remove clothing, use gloves, flood area with water for 15 minutes, use other mild material such as petroleum or alcohol to remove substances not removed by water.
Skin decontamination: Remove clothing, use gloves, flood area with water for 15 minutes, use other mild material such as petroleum or alcohol to remove substances not removed by water.
![]() Ocular decontamination: Rinse eyes with water, saline, or lactated Ringer’s for > 15 minutes; consider emergency ophthalmologic exam.
Ocular decontamination: Rinse eyes with water, saline, or lactated Ringer’s for > 15 minutes; consider emergency ophthalmologic exam.
TABLE 6-2. “Toxidromes,” Symptoms, and Some Causes
![]() Respiratory decontamination: Move to fresh air; bronchodilators may be effective, inhaled dilute sodium bicarbonate may help acid or chlorine inhalation.
Respiratory decontamination: Move to fresh air; bronchodilators may be effective, inhaled dilute sodium bicarbonate may help acid or chlorine inhalation.
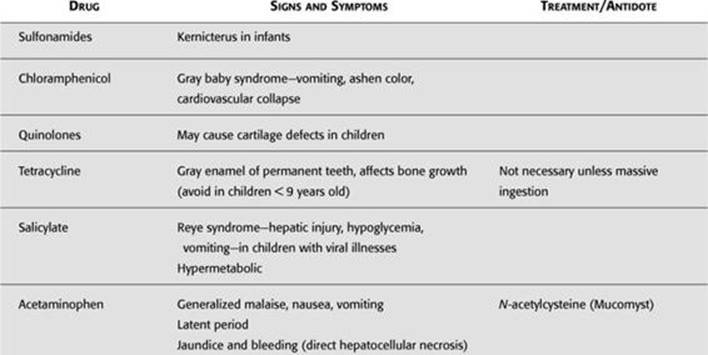
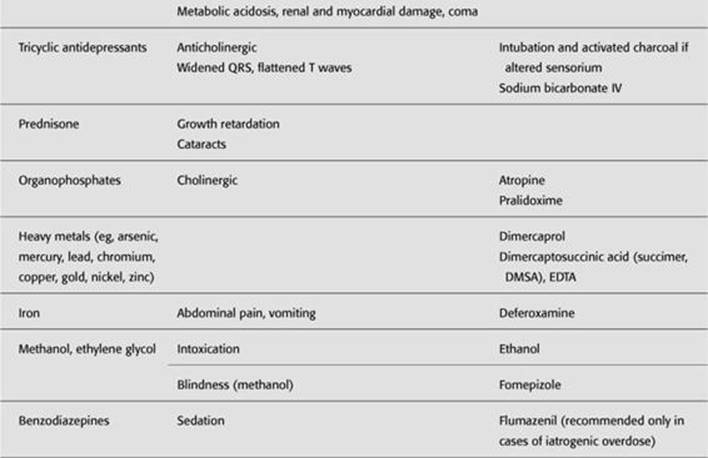
![]() Antidotes: See Table 6-3.
Antidotes: See Table 6-3.
![]() Treat seizures, respiratory distress/depression, hemodynamics, and electrolyte disturbances as they arise.
Treat seizures, respiratory distress/depression, hemodynamics, and electrolyte disturbances as they arise.
TABLE 6-3. Drug Toxicities

ADOLESCENCE
![]() Adolescence comprises the ages between 10 and 21 years.
Adolescence comprises the ages between 10 and 21 years.
![]() The most common health problems seen in this age group include unintended pregnancies, sexually transmitted diseases (STDs), mental health disorders, physical injuries, and substance abuse.
The most common health problems seen in this age group include unintended pregnancies, sexually transmitted diseases (STDs), mental health disorders, physical injuries, and substance abuse.
![]()
The leading causes of death for adolescents are accidents, homicide, and suicide.
PREVENTION
![]() Be on the lookout for adolescents at high risk for health problems, including physical, mental, and emotional health.
Be on the lookout for adolescents at high risk for health problems, including physical, mental, and emotional health.
![]() Screen for depression. Suicide is the third leading cause of death in adolescents. Depression in the adolescent can manifest as irritability, anger, new drug use, and drop-off in school performance.
Screen for depression. Suicide is the third leading cause of death in adolescents. Depression in the adolescent can manifest as irritability, anger, new drug use, and drop-off in school performance.
![]() Look for:
Look for:
![]() Decline in school performance, excessive school absences, cutting class.
Decline in school performance, excessive school absences, cutting class.
![]() Frequent psychosomatic complaints.
Frequent psychosomatic complaints.
![]() Changes in sleeping or eating habits.
Changes in sleeping or eating habits.
![]() Difficulty in concentrating.
Difficulty in concentrating.
![]() Signs of depression, stress, or anxiety.
Signs of depression, stress, or anxiety.
![]() Conflict with parents.
Conflict with parents.
![]() Social withdrawal.
Social withdrawal.
![]() Sexual acting-out.
Sexual acting-out.
![]() Conflicts with the law.
Conflicts with the law.
![]() Suicidal thoughts, preoccupation with death.
Suicidal thoughts, preoccupation with death.
![]() Substance abuse.
Substance abuse.
![]()
One percent of adolescents have made at least one suicide gesture.
SCREENING
![]() Routine health care should involve audiometry and vision screening, blood pressure checks, exams for scoliosis.
Routine health care should involve audiometry and vision screening, blood pressure checks, exams for scoliosis.
![]() Breast and pelvic exams in females may also be necessary, and self-exams should be emphasized.
Breast and pelvic exams in females may also be necessary, and self-exams should be emphasized.
![]() Likewise, examination for scrotal masses is necessary in males with emphasis on self-examination.
Likewise, examination for scrotal masses is necessary in males with emphasis on self-examination.
![]() STDs (gonorrhea and chlamydia), including HIV should be considered in those adolescents with high-risk behaviors. Counsel sexually active adolescents on contraception and protection against STDs.
STDs (gonorrhea and chlamydia), including HIV should be considered in those adolescents with high-risk behaviors. Counsel sexually active adolescents on contraception and protection against STDs.
![]() Screen with Pap smears within 3 years of the onset of sexual activity or at 21 years of age.
Screen with Pap smears within 3 years of the onset of sexual activity or at 21 years of age.
![]() Adolescents who are engaged in one risk-taking activity such as smoking cigarettes are at greater risk for experimenting with drugs and alcohol.
Adolescents who are engaged in one risk-taking activity such as smoking cigarettes are at greater risk for experimenting with drugs and alcohol.
PHYSICAL EXAM
Sexual maturity should be assessed at each visit.
![]()
An ![]() in the number of years of schooling for a woman delays the age at which a woman marries and has her first child.
in the number of years of schooling for a woman delays the age at which a woman marries and has her first child.
Pregnancy
EPIDEMIOLOGY
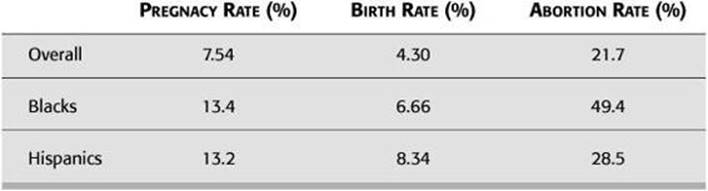
![]() Over 750,000 teenage girls become pregnant in the United States each year (see Table 6-4).
Over 750,000 teenage girls become pregnant in the United States each year (see Table 6-4).
![]() One fifth of all sexually active girls become pregnant each year.
One fifth of all sexually active girls become pregnant each year.
Contraception
EPIDEMIOLOGY
![]() According to a 2004 Centers for Disease Control and Prevention (CDC) report, 62% of high school seniors report having ever had intercourse.
According to a 2004 Centers for Disease Control and Prevention (CDC) report, 62% of high school seniors report having ever had intercourse.
![]() Ninety-eight percent of sexually active teens report using at least one form of birth control.
Ninety-eight percent of sexually active teens report using at least one form of birth control.
![]() Thirty-three percent of ninth graders report having had sex.
Thirty-three percent of ninth graders report having had sex.
![]() Most common contraceptions methods are condoms (94%) and oral contraceptives (61%).
Most common contraceptions methods are condoms (94%) and oral contraceptives (61%).
RISK FACTORS
Factors associated with early sexual activity include poor academic performance, lower expectations for education, poor perception of life options, low school grades, and involvement in other high-risk behaviors such as substance abuse.
FORMS OF CONTRACEPTION
![]() Abstinence, condoms (male and female), diaphragm, cervical cap, spermicides, or some combination of these.
Abstinence, condoms (male and female), diaphragm, cervical cap, spermicides, or some combination of these.
TABLE 6-4. 2002 Teenage Statistics
![]() Hormonal methods include oral contraceptive pills and injectable or implantable hormones, and hormone patches.
Hormonal methods include oral contraceptive pills and injectable or implantable hormones, and hormone patches.
![]() Intrauterine devices are not recommended for adolescents because of the
Intrauterine devices are not recommended for adolescents because of the ![]() risk of sexually transmitted infections.
risk of sexually transmitted infections.
COMBINATION ORAL CONTRACEPTIVES
Usually consist of either 50, 35, 30, or 20 μg of an estrogenic substance such as mestranol or ethinyl estradiol plus a progestin.
Adolescents who smoke may ![]() their risk for side effects from oral contraceptives.
their risk for side effects from oral contraceptives.
SIDE EFFECTS
![]() Short-term effects may include nausea and weight gain.
Short-term effects may include nausea and weight gain.
![]() Other possible effects include thrombophlebitis, hepatic adenomas, myocardial infarction, and carbohydrate intolerance.
Other possible effects include thrombophlebitis, hepatic adenomas, myocardial infarction, and carbohydrate intolerance.
POTENTIAL BENEFITS
Long-range benefits may include ![]() risks of benign breast disease and ovarian disease.
risks of benign breast disease and ovarian disease.
HIV/AIDS
See the Infectious Disease chapter.
EPIDEMIOLOGY
![]() HIV/AIDS is the sixth leading cause of death among adolescents aged 15–24 years.
HIV/AIDS is the sixth leading cause of death among adolescents aged 15–24 years.
![]() One half of all new infections in the United States occur in people younger than 25 years of age.
One half of all new infections in the United States occur in people younger than 25 years of age.
SCREENING
Screening should include adolescents with risk factors such as previous STD, unprotected sex, practicing insertive or receptive anal sex, trading sex for money or drugs, homelessness, intravenous drug or crack cocaine use, being the victim of sexual abuse.
CHILD ABUSE
DEFINITION
Child maltreatment encompasses a spectrum of abusive actions, and lack of action, that result in morbidity or death. Forms of child abuse include:
![]() Physical abuse
Physical abuse
![]() Sexual abuse
Sexual abuse
![]() Neglect
Neglect
If the story doesn’t make sense, suspect abuse.
RISK FACTORS
![]() Parental risk factors:
Parental risk factors:
![]() Low socioeconomic status.
Low socioeconomic status.
![]() Mother’s age (young).
Mother’s age (young).
![]() History of being abused as a child.
History of being abused as a child.
![]() Alcoholism, substance abuse, psychosis.
Alcoholism, substance abuse, psychosis.
![]() Social isolation.
Social isolation.
Mongolian spots can be confused with bruises.
![]() Child risk factors:
Child risk factors:
![]()
A baby should never be shaken for any reason.
![]() Children with special needs, handicapped children (chronic illness, congenital malformation, mental retardation).
Children with special needs, handicapped children (chronic illness, congenital malformation, mental retardation).
![]() Prematurity.
Prematurity.
![]() Age < 3 years.
Age < 3 years.
![]() Nonbiologic relationship to the caretaker.
Nonbiologic relationship to the caretaker.
![]() “Difficult” children.
“Difficult” children.
![]() Family and environmental factors:
Family and environmental factors:
![]() Unemployment.
Unemployment.
![]() Intimate partner violence.
Intimate partner violence.
![]() Poverty.
Poverty.
![]()
The most common reason for shaking a baby is inconsolable crying.
Physical Abuse
Suspect if:
![]() Injury is unexplained or unexplainable.
Injury is unexplained or unexplainable.
![]() Injury is inconsistent with mechanism suggested by history.
Injury is inconsistent with mechanism suggested by history.
![]() History changes each time it is told.
History changes each time it is told.
![]() There are repeated “accidents.”
There are repeated “accidents.”
![]() There is a delay in seeking care.
There is a delay in seeking care.
Sometimes abusive parents “punish” their children for enuresis or resistance to toilet training by forcibly immersing their buttocks in hot water.
SKIN MANIFESTATIONS
Bruises
![]() Most common manifestation of physical abuse
Most common manifestation of physical abuse
![]() Suspicious if:
Suspicious if:
![]() Seen on nonambulatory infants.
Seen on nonambulatory infants.
![]() Have geometric pattern (belt buckles, looped-cord marks).
Have geometric pattern (belt buckles, looped-cord marks).
Burns
![]() Suspicious if:
Suspicious if:
![]() Involve both hands or feet in stocking-glove distribution or buttocks with sharp demarcation line (forced immersion in hot water).
Involve both hands or feet in stocking-glove distribution or buttocks with sharp demarcation line (forced immersion in hot water).
![]() Cigarette burns—if nonaccidental, usually full-thickness, sharply circumscribed.
Cigarette burns—if nonaccidental, usually full-thickness, sharply circumscribed.
![]() “Branding” injuries (inflicted by hot iron, radiator cover, etc).
“Branding” injuries (inflicted by hot iron, radiator cover, etc).
![]()
Skeletal injuries suspicious of abuse: “Some Parents Are Maliciously Mean” (or Parents Should Manage Anger)
SKELETAL INJURIES
Suspicious if:
![]() Spiral fractures of lower extremities in nonambulatory children (see Figure 6-1A and B).
Spiral fractures of lower extremities in nonambulatory children (see Figure 6-1A and B).
![]() Posterior rib fractures (usually caused by squeezing the chest).
Posterior rib fractures (usually caused by squeezing the chest).
![]() Fractures of different Ages.
Fractures of different Ages.
![]() Metaphyseal “chip” fractures (usually caused by wrenching).
Metaphyseal “chip” fractures (usually caused by wrenching).
![]() Multiple fractures.
Multiple fractures.
![]() Scapular and clavicle fractures.
Scapular and clavicle fractures.
![]()
CNS injuries suspicious of abuse: “Mothers, Refuse Shaking!” (Metaphyseal fractures, Retinal hemorrhages, Subdural hematoma)
CENTRAL NERVOUS SYSTEM (CNS) INJURIES
![]() Most common cause of death in child abuse: “Shaken baby syndrome.”
Most common cause of death in child abuse: “Shaken baby syndrome.”
![]() Occurs due to violent shakes and slamming against mattress or wall while an infant is held by the trunk or upper extremities.
Occurs due to violent shakes and slamming against mattress or wall while an infant is held by the trunk or upper extremities.
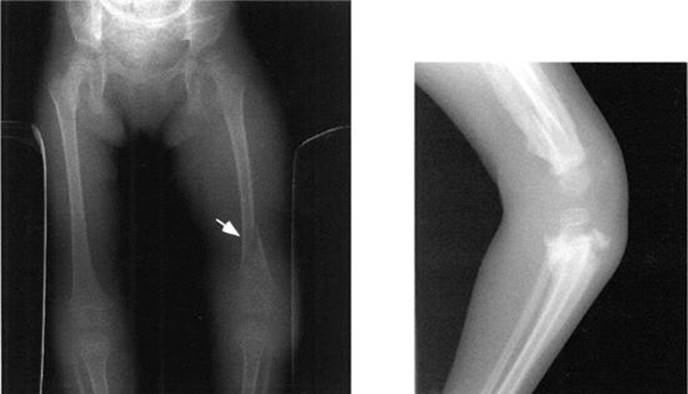
FIGURE 6-1. A. Spiral fracture (arrow) of the femur in a nonambulatory child, consistent with nonaccidental trauma. B. Same child 2 months later. Note the exuberant callus formation at all the fracture sites in the femur and proximal tibia and fibula.
![]() Findings include:
Findings include:
![]() Retinal hemorrhages.
Retinal hemorrhages.
![]() Subdural hematoma (from rupturing of bridging veins between dura mater and brain cortex).
Subdural hematoma (from rupturing of bridging veins between dura mater and brain cortex).
![]() Symptoms include:
Symptoms include:
![]() Lethargy or irritability
Lethargy or irritability
![]() Vomiting
Vomiting
![]() Seizures
Seizures
![]() Bulging fontanelle
Bulging fontanelle
Epiphyseal-metaphyseal injury is virtually diagnostic of physical abuse in an infant, since an infant cannot generate enough force to fracture a bone at the epiphysis.
Abdominal Injuries
![]() Second most common cause of death in child abuse.
Second most common cause of death in child abuse.
![]() Usually no external marks. Most commonly, liver or spleen is ruptured.
Usually no external marks. Most commonly, liver or spleen is ruptured.
![]() Symptoms include vomiting, abdominal pain or distention, shock.
Symptoms include vomiting, abdominal pain or distention, shock.
Shaken baby syndrome can mimic meningitis or sepsis.
Sexual Abuse
![]() Includes genital, anal, oral contact; fondling; and involvement in pornography.
Includes genital, anal, oral contact; fondling; and involvement in pornography.
![]() Most common perpetrators—fathers, stepfathers, mother’s boyfriend(s) (adults known to child).
Most common perpetrators—fathers, stepfathers, mother’s boyfriend(s) (adults known to child).
![]() Suspect if:
Suspect if:
![]() Genital trauma.
Genital trauma.
![]() STDs in small children.
STDs in small children.
![]() Sexualized behavior toward adults or children.
Sexualized behavior toward adults or children.
![]() Unexplained decline in school performance.
Unexplained decline in school performance.
![]() Runaway.
Runaway.
![]() Chronic somatic complaints (abdominal pain, headaches).
Chronic somatic complaints (abdominal pain, headaches).
![]() Symptoms include:
Symptoms include:
![]() May be totally absent.
May be totally absent.
![]() Tears/bleeding in female or male genitalia.
Tears/bleeding in female or male genitalia.
![]() Anal tears or hymenal tears (not very reliable symptoms).
Anal tears or hymenal tears (not very reliable symptoms).
Children too young to talk about what has happened to them (generally younger than 2) should have a complete skeletal survey if you suspect abuse.
Evaluation of Suspected Abuse
PHYSICAL ABUSE
![]() Bleeding disorders must be ruled out in case of multiple bruises.
Bleeding disorders must be ruled out in case of multiple bruises.
![]() X-ray skeletal survey (skull, chest, long bones) in children < 2 years of age (to look for old/new fractures).
X-ray skeletal survey (skull, chest, long bones) in children < 2 years of age (to look for old/new fractures).
![]() Computed tomographic (CT) scans of the head/abdomen as indicated.
Computed tomographic (CT) scans of the head/abdomen as indicated.
![]() Ophthalmology consult.
Ophthalmology consult.
A child who presents with multiple fractures at multiple sites and in various stages of healing should be considered abused until proven otherwise.
SEXUAL ABUSE
![]() Sexual abuse includes any sexual activity (nonconsensual and consensual) between an adult and a child.
Sexual abuse includes any sexual activity (nonconsensual and consensual) between an adult and a child.
![]() Cultures for STDs, test for presence of sperm, if indicated (usually within 72 hours of assault).
Cultures for STDs, test for presence of sperm, if indicated (usually within 72 hours of assault).
MANAGEMENT
![]() If abuse is suspected, it must be reported to child protective services (CPS) (after medical stabilization, if needed).
If abuse is suspected, it must be reported to child protective services (CPS) (after medical stabilization, if needed).
![]() All siblings need to be evaluated for abuse, too (up to 20% of them might have signs of abuse).
All siblings need to be evaluated for abuse, too (up to 20% of them might have signs of abuse).
![]() Disposition of the child (ie, whether to discharge the patient back to parents or to a CPS worker if medically cleared) has to be decided by CPS in conjunction with treating physician.
Disposition of the child (ie, whether to discharge the patient back to parents or to a CPS worker if medically cleared) has to be decided by CPS in conjunction with treating physician.
![]() Family must receive intensive intervention by social services and, if needed, legal authorities.
Family must receive intensive intervention by social services and, if needed, legal authorities.
![]() Remember: If sent back to abusive family without intervention, up to 5% of children can be killed and up to 25% seriously reinjured.
Remember: If sent back to abusive family without intervention, up to 5% of children can be killed and up to 25% seriously reinjured.
Management of abuse:
Suspect
![]()
Report
![]()
Disposition
![]()
Family counseling
Neglect
DEFINITION
![]() Neglect is the most common form of reported abuse.
Neglect is the most common form of reported abuse.
![]() Neglect to meet nutritional, medical, and/or developmental needs of a child can present as:
Neglect to meet nutritional, medical, and/or developmental needs of a child can present as:
![]() Failure to thrive.
Failure to thrive.
![]() Poor hygiene (severe diaper rash, unwashed clothing, uncut nails).
Poor hygiene (severe diaper rash, unwashed clothing, uncut nails).
![]() Developmental/speech delay.
Developmental/speech delay.
![]() Delayed immunizations.
Delayed immunizations.
![]() Not giving treatment for chronic conditions.
Not giving treatment for chronic conditions.
MANAGEMENT
If nonorganic (ie, due to insufficient feeding) failure to thrive is suspected:
![]() Patient should be hospitalized and given unlimited feedings for 1 week; 2 oz/24 hours of weight gain is expected.
Patient should be hospitalized and given unlimited feedings for 1 week; 2 oz/24 hours of weight gain is expected.
![]() All suspected cases of neglect must be reported to CPS.
All suspected cases of neglect must be reported to CPS.
Munchausen Syndrome by Proxy
DEFINITION
![]() Parent/caregiver either simulates illness, exaggerates actual illness, or induces illness in a child.
Parent/caregiver either simulates illness, exaggerates actual illness, or induces illness in a child.
![]() Psychiatrically disturbed parent(s) gain satisfaction from attention and empathy from hospital personnel or their own family because of problems created.
Psychiatrically disturbed parent(s) gain satisfaction from attention and empathy from hospital personnel or their own family because of problems created.
![]()
Baron von Munchausen was an 18th-century nobleman who became famous because of his incredible stories, which included travel to the moon and flying atop a cannonball over Constantinople, as well as visiting an island made of cheese. His name became a synonym for gross confabulations.
EPIDEMIOLOGY
![]() Affected children are usually < 6 years old.
Affected children are usually < 6 years old.
![]() Parent (usually mother) has some medical knowledge.
Parent (usually mother) has some medical knowledge.
SIGNS AND SYMPTOMS
![]() Vomiting (induced by ipecac).
Vomiting (induced by ipecac).
![]() Chronic diarrhea (from laxatives).
Chronic diarrhea (from laxatives).
![]() Recurrent abscesses or sepsis (usually polymicrobial, from injecting contaminated fluids).
Recurrent abscesses or sepsis (usually polymicrobial, from injecting contaminated fluids).
![]() Apnea (from choking the child).
Apnea (from choking the child).
![]() Fever (from heating thermometers).
Fever (from heating thermometers).
![]() Bloody vomiting or diarrhea (from adding blood to urine or stool specimens).
Bloody vomiting or diarrhea (from adding blood to urine or stool specimens).
DIAGNOSIS
Diagnosis is difficult, but is initiated by removing child from parent via hospitilization. Usually, child without access to parent will have all/most symptoms resolved; testing will also usually be normal.
MANAGEMENT
![]() Admission to the hospital for observation, possibly using hidden video cameras.
Admission to the hospital for observation, possibly using hidden video cameras.
![]() All cases of suspected Munchausen syndrome by proxy must be reported to CPS.
All cases of suspected Munchausen syndrome by proxy must be reported to CPS.
Sudden Infant Death Syndrome (SIDS)
DEFINITION
![]() Sudden death of an infant (< 1 year old) that remains unexplained after thorough case investigation, autopsy, and review of the clinical history.
Sudden death of an infant (< 1 year old) that remains unexplained after thorough case investigation, autopsy, and review of the clinical history.
![]() SIDS is one of the leading causes of death of infants.
SIDS is one of the leading causes of death of infants.
ETIOLOGY
Apnea hypothesis.
DIAGNOSIS
Difficult to differentiate from intentional harm.
PREVENTION
![]() There has been a vast
There has been a vast ![]() in the number of cases since the trend of having infants sleep on their backs (supine).
in the number of cases since the trend of having infants sleep on their backs (supine).
![]() The number one preventive measure to date is parental education, though the use of cardiorespiratory monitoring in the home is being debated.
The number one preventive measure to date is parental education, though the use of cardiorespiratory monitoring in the home is being debated.
![]() Limiting passive smoke exposure.
Limiting passive smoke exposure.
Infants unable to roll over should be placed on the back while sleeping.