(Clin Infect Dis 2006;43:1089)
Epidemiology
• Most common vector born dz in U S, ↑ trend; peak incidence in summer, incubation period (for early localized disease) 2–31 d, mean 11
• Endemic areas include Northeast, Great Lakes, mid-Atlantic regions, usually in rural, wooded areas (for local prevalences: American Lyme disease foundation: http://www.aldf.com/usmap.shtml)
• Most prevalent in children 2–15 yo (Pediatrics 1998;102:905)
Microbiology
• Spirochete Borrelia burgdorferi spread by tick (Ixodes scapularis) on deer and mice
• Coinfection w/ Babesia, and other rickettsial species not uncommon (up to 10%), may contribute to prolonged sx despite Rx for Lyme
• Infection usually requires tick attachment >36 hr
Clinical Manifestations
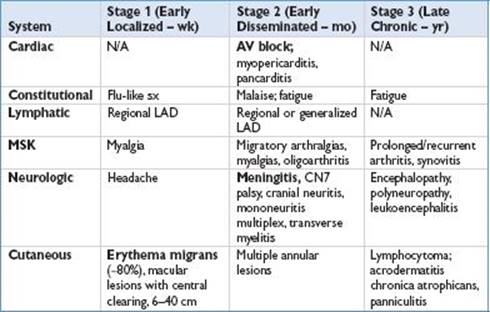
From: N Engl J Med 2001;345:115; Lancet 2003;362:1639; Ann Intern Med 2002;136:421.
Diagnostic Studies
• Clinical dx during early stages (erythema migrans), Ab against B. burgdorferi not detectable w/i first few wks after infection
• In early disseminated or late dz, dx based on clinical findings and serologic tests
• 2-step approach: 1st, screening test for serum Ab’s (IFA or EIA)
• If +, then standardized Western blot (False +’s 2/2 EBV, other spirochete, HIV, SLE)
• Early dz, IgG and IgM; late dz, IgG (lots of IgM false +)
• A + IgM test needs 2 of 3 bands (Ab’s). A + IgG test requires 5 of 10 bands
• Note: Rx’d individuals early in course of infection might not develop Ab’s
• Consider PCR in joint fluid, and serologies in CSF. Culture is not recommended
Treatment
• Prophylaxis: RCT (>12 yr) w/ efficacy doxycycline 200 mg × 1 w/i 72 hr of tick bite (must have seen and removed tick) to prevent Lyme dz (N Engl J Med 2001;345:79)
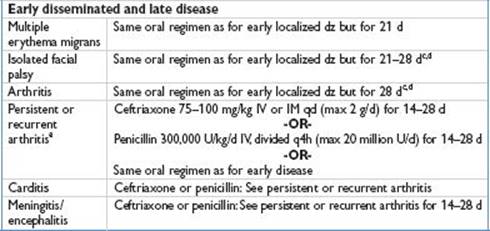
• Recommended treatment of Lyme disease in children (Lyme Disease. Red Book 2009)
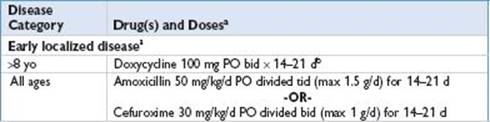
aFor pts who are allergic to PCN, cefuroxime, and erythromycin are alternative drugs.
bTetracyclines contraindicated in pregnancy.
cCorticosteroids should not be given.
dRx has no effect on the resolution of facial nerve palsy; its purpose is to prevent late disease.
eArthritis not considered persistent or recurrent unless objective evidence of synovitis exists at least 2 mo after Rx initiated. Some experts administer 2nd course of oral agent before using IV antimicrobial agent.