Approach to the Problem
Hand swelling can be a result of pathology in the bones, joints, tendons, blood vessels, or soft tissues. Many systemic diseases, such as Kawasaki disease, sickle cell disease (SCD), juvenile idiopathic arthritis (JIA), viral arthritides, and serum sickness, can produce hand swelling. In these cases, hand involvement tends to be symmetric, and other constitutional symptoms lend important clues to the etiology. More localized causes of hand swelling include osteomyelitis, septic arthritis, tenosynovitis, cellulitis, trauma, and soft-tissue tumors. Careful examination of the hand, paying close attention to joint motion, range of motion, and areas of tenderness, swelling, or erythema, can narrow the differential diagnosis based on the anatomic structures involved.
Key Points in the History
• Osteomyelitis in the hands can result from hematogenous spread of infection, direct inoculation as seen with a puncture wound, or contiguous spread from adjacent structures as may be seen with septic arthritis. In infants, osteomyelitis commonly causes swelling of adjacent soft tissues.
• Septic arthritis, most commonly caused by Staphylococcus aureus, is usually monoarticular and associated with swelling, erythema, and pain on movement.
• Cellulitis may occur at the site of minor trauma. Patients may also report a “spider bite” that becomes larger and more erythematous, as the initial papular lesion often resembles an insect bite.
• JIA has a variety of manifestations. Of the seven subtypes of JIA, polyarticular rheumatoid factor positive (2%–7% of JIA), systemic (4%–17%), and psoriatic (2%–11%) are most likely to have hand involvement.
• Dactylitis associated with SCD presents with tender, erythematous, and edematous hands or feet in patients. It is frequently the presenting sign, occurring in 25% of affected individuals by 1 year of age and in 40% by 2 years of age. The pathophysiology is thought to be similar to other vasoocclusive crises.
• Clenched fist injuries are caused by the closed fist striking the teeth during a fight. These are not often recognized as bite injuries, but can become infected with mouth flora. They also have a high rate of extensor tendon and joint capsule injuries.
• A boxer’s fracture is a fracture of the fourth or fifth metacarpal neck. The mechanism is usually a closed fist striking a hard, immobile object such as a wall.
Key Points in the Physical Examination
• The extremity changes associated with Kawasaki disease (one of the five principal features, in addition to fever) typically manifest initially in the hands as swelling and palmar erythema. The palms may progress to painful induration within the acute phase. Desquamation of the fingertips appears in the convalescent phase, usually as the fever resolves (commonly at 10–14 days, if untreated).
• A sensitive screening examination showing arthritis in the metacarpophalangeal (MCP), proximal interphalangeal, and/or distal interphalangeal joints is the inability to make a completely clenched fist; that is, the fingertips do not meet the palm.
• Psoriatic arthritis is often accompanied by a psoriatic rash; if the rash is absent, arthritis must be accompanied by two of the following criteria: family history of psoriasis in a first-degree relative, dactylitis, and nail pitting. The typical scaly rash of psoriasis is most often found on the elbows, knees, and extensor surfaces.
• In a displaced boxer’s fracture, the fourth or fifth knuckle (MCP joint) will appear depressed when examining the partially closed fist. Even when nondisplaced, edema, discoloration, and point tenderness are usually present.
|
PHOTOGRAPHS OF SELECTED DIAGNOSES |

Figure 42-1 Kawasaki disease. The hands of this 4-year-old with 5 days of high fever show diffuse erythema and swelling. (Courtesy of Mark A. Ward, MD.)

Figure 42-2 Osteomyelitis. Soft-tissue swelling, joint involvement, and fistulous tracts complicate the finger osteomyelitis seen in this 12-year-old female. (Courtesy of Mary L. Brandt, MD.)

Figure 42-3 Juvenile rheumatoid arthritis. Flexion contractures complicate the polyarticular JIA seen in this 5-year-old. Also, note the swelling of the wrists and the fingers. (Courtesy of Shriners Hospitals for Children, Houston, Texas.)

Figure 42-4 Dactylitis. Painful sausage-shaped fingers and symmetrical swelling of the hands characterize the onset of dactylitis in this infant with SCD. (Courtesy of Tom Thatcher, MD.)

Figure 42-5 Blistering distal dactylitis. A superficial blister with an erythematous base covers the entire distal volar fat pad of this 5-year-old, also extending to the base of the digit. (Courtesy of Mark A. Ward, MD.)
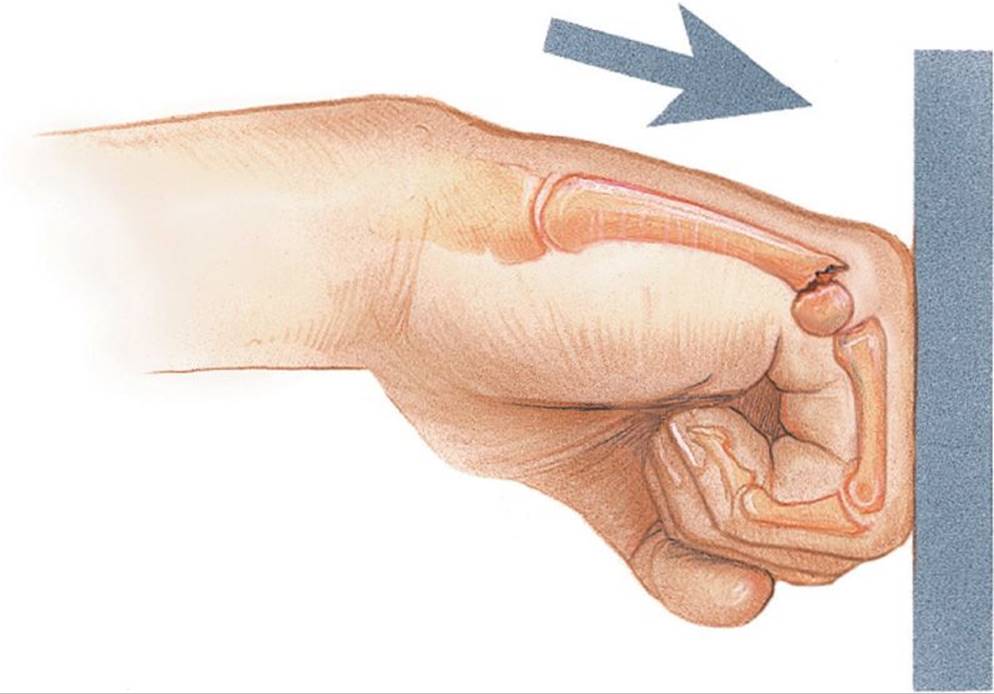
Figure 42-6 Boxer’s fracture. The neck of the fourth or fifth metacarpal snaps when a closed fist strikes a hard immobile object. (Used with permission from the Anatomical Chart Company. ACC Systems and Structures Chart Images, p. 2.)
DIFFERENTIAL DIAGNOSIS


Other Diagnoses to Consider
• Henoch–Schönlein purpura
• Lysosomal storage disease (Farber disease, also known as ceramidase deficiency)
• Pachydermodactyly (superficial dermal fibromatosis)
• Soft-tissue tumors
• Serum sickness
• Tuberculous dactylitis
When to Consider Further Evaluation or Treatment
• Orthopedic or plastic surgery consultation should be obtained for significant soft-tissue infections of the hand, particularly with abscess, as tenosynovitis and other deeper involvement can cause permanent functional deficits.
• A hand fracture with any adjacent break in the skin should be treated emergently as an open fracture, requiring orthopedic surgery consultation.
• If septic arthritis is suspected, joint aspiration and irrigation should be performed. Most infections should be treated by arthrotomy (or sometimes arthroscopy) and a surgical washout, in order to minimize the potential for cartilage destruction and subsequent arthritis.
• Dactylitis associated with SCD should be treated like other vaso-occlusive crises with hydration and analgesics.
• Patients with four of five principal features of Kawasaki disease may be treated with IVIG and aspirin after 4 days of fever. Patients with 5 days of fever and suspected Kawasaki disease, but fewer than four features, should have an echocardiogram and additional laboratory testing, and may be treated for incomplete or atypical Kawasaki disease if results support the diagnosis.
SUGGESTED READINGS
Faust SN, Clark J, Pallett A, et al. Managing bone and joint infection in children. Arch Dis Child. 2012;97:545–553.
McCavit TL. Sickle cell disease. Pediatr Rev. 2012;33(5):195–206. Erratum in. Pediatr Rev. 2012;33:375.
Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement of the Council on Cardiovascular Disease in the Young, American Heart Association. Pediatrics. 2004;114(6):1708–1733. Erratum in. Pediatrics. 2005;115(4):1118.
Ravelli A, Martini A. Juvenile idiopathic arthritis. Lancet. 2007;369:767–778.