Approach to the Problem
The pattern of a rash can be quite helpful in identifying its etiology. Linear patterns of rashes may be seen in many conditions. In particular, linear red rashes are commonly seen in infectious and inflammatory conditions. They may also be the result of other systemic processes.
Key Points in the History
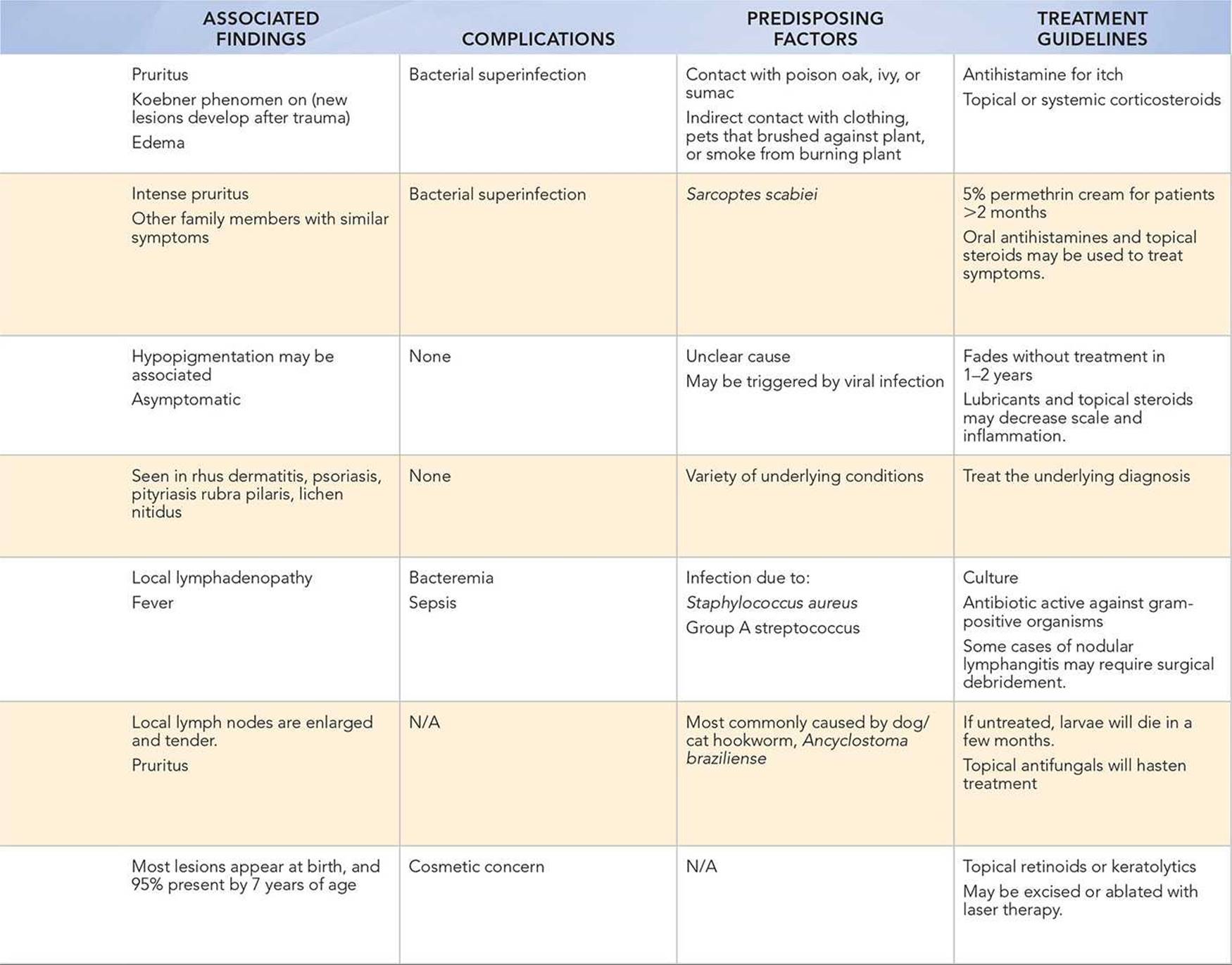
• A linear red rash that develops after outdoor activity should raise the suspicion of rhus dermatitis due to the exposure to poison ivy, oak, or sumac.
• Rhus dermatitis, scabies, and cutaneous larva migrans are intensely pruritic lesions.
• Children with scabies may have a close contact, who also has an itchy rash. It is helpful to inquire if the parent or another household contact also has a rash, particularly if they share a sleeping surface or bed with the child.
• Lichen striatus may start as a small area of papules that then spreads into a linear distribution.
• Lichen striatus is twice as common in girls than in boys.
• Outdoor exposure to soil or sand that is shared with dogs or cats (e.g., sandboxes) is often a predisposing factor in patients affected with cutaneous larva migrans.
• Linear epidermal nevus, which is not typically pruritic, appears at birth or shortly thereafter.
• Lymphangitis is the secondary manifestation of infection at a distal site. Systemic symptoms of fever, chills, and malaise are often present.
Key Points in the Physical Examination
• Rhus dermatitis is seen on exposed skin, particularly the areas that were exposed while outdoors.
• Excoriation surrounding a linear rash suggests pruritus and scratching, which may lead to bacterial superinfection.
• Red rashes may not be as apparent in individuals with darker skin; therefore, it is important to assess patients in adequate lighting.
• Lichen striatus may appear to be mildly hypopigmented or flesh-colored.
• Infants with scabies often have a generalized rash that includes the soles of their feet. In young children, the rash of scabies is typically seen in the axilla and groin. Older children will often have lesions in the web spaces of their fingers and toes.
• An advancing serpiginous eruption in the skin that is intensely pruritic is virtually pathognomonic for cutaneous larva migrans.
• The Koebner phenomenon is commonly seen in linear rashes such as rhus dermatitis, linear psoriasis, and lichen planus.
|
PHOTOGRAPHS OF SELECTED DIAGNOSES |

Figure 65-1 Rhus dermatitis. Linear papules and vesicles following exposure to poison ivy. (Courtesy of George A. Datto, III, MD.)

Figure 65-2 Lichen striatus. Small, shiny, hypopigmented papules in a linear distribution on the posterior thigh. (Courtesy of George A. Datto, III, MD.)

Figure 65-3 Scabies. This close-up view shows a burrow (arrow) on the palm. (From Goodheart HP, MD. Goodheart’s Photoguide of Common Skin Disorders. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003.)

Figure 65-4 Koebner phenomenon. Papulovesicular eruption in a linear distribution on the forearm of a child with an Id reaction (autosensitization dermatitis) associated with tinea capitis. (Courtesy of George A. Datto, III, MD.)

Figure 65-5 Lymphangitis. Linear red streak proximal to skin infection. (Courtesy of Paul S. Matz, MD.)

Figure 65-6 Cutaneous larva migrans. Serpiginous red streaks on sole of foot. (Used with permission from Goodheart HP. Goodheart’s Photoguide of Common Skin Disorders. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:315.)

Figure 65-7 Linear epidermal nevus. Warty, linear lesions on face. (Used with permission from Goodheart HP. Goodheart’s Photoguide of Common Skin Disorders. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:9.)
DIFFERENTIAL DIAGNOSIS

Other Diagnoses to Consider
• Striae
• Contact dermatitis
• Linear psoriasis
• Linear morphea (localized scleroderma)
When to Consider Further Evaluation or Treatment
• Rhus dermatitis may be treated with systemic corticosteroids when severe or extensive in distribution. If systemic steroids are used, start with a 48-hour course of steroids, followed by a 2- to 3-week taper.
• Scabies should be treated with 5% permethrin if the patient is older than 2 months. The lotion should be applied from head to toe, and then washed off 8 to 14 hours later. Treatment may need to be repeated 1 week later if symptoms worsen. Treatment is recommended for all household contacts, when possible.
• Resistant scabies is increasing in prevalence; therefore, if there is no improvement after two treatments with permethrin, another treatment such as ivermectin, precipitated sulphur, or benzyl benzoate should be considered.
• For scabies, all bedding, clothing, towels and stuffed animals that the person has touched during the 3 days prior to treatment should be laundered in a washer with hot water. Mites do not survive more than 3 days in the absence of skin contact, so items that cannot be washed can be placed in a plastic bag for at least 3 days.
• Itching associated with scabies may last for several weeks after mites are eliminated. Steroid creams or oral steroids may be necessary if itching is severe.
• If desired by the patient for cosmetic reasons, linear epidermal nevus may be treated with topical retinoids or keratolytics. If these agents are unsuccessful, the lesion can be excised or ablated by laser therapy.
• If lymphangitis is suspected, appropriate antibiotic coverage should be initiated and the source of infection should be investigated.
SUGGESTED READINGS
American Academy of Pediatrics. Red Book: 2012 Report of the Committee on Infectious Diseases. In: Pickering LK, ed. 29th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2012:298–299, 641–643.
Cohen BA. Pediatric Dermatology. 3rd ed. Baltimore, MD: Elsevier Mosby; 2005.
Goodheart HP. Goodheart’s Photoguide to Common Skin Disorders. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008:11, 361–362.
Paller AS, Mancini AJ, eds. Hurwitz Clinical Pediatric Dermatology: A Textbook of Skin Disorders of Childhood and Adolescence. 4th ed. Philadelphia, PA: Elsevier Saunders; 2011.
Weston WL, Lane AT, Morelli JG. eds. Color Textbook of Pediatric Dermatology. 4th ed. St. Louis, MO: Mosby; 2007.
Zitelli BJ, McIntire SC, Nowalk AJ. eds. Zitelli and Davis’s Atlas of Pediatric Physical Diagnosis. 6th ed. Philadelphia, PA: Mosby; 2012.