Introduction
Major depression is one of the most common psychiatric disorders. At any given moment, about 3-5% of the population is depressed (point prevalence), and an estimated 10% of people may become depressed during their lives (lifetime prevalence). The symptoms of depression are often subtle and unrecognized both by patients and by physicians. Patients with vague complaints that resist explanation as manifestations of somatic disorders and those who might be simplistically described as "neurotic" should be suspected of being depressed.
Depression is a heterogeneous disorder that has been characterized and classified in a variety of ways. According to the American Psychiatric Association's modified fourth edition (2000) of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR), several diagnoses of affective disorders are possible. Major depression and dysthymia (minor) are pure depressive syndromes, whereas bipolar disorder and cyclothymic disorder signify depression in association with mania. A simplified classification based on presumed origin is as follows: (1) brief reactive or secondary depression (most common), occurring in response to real stimuli such as grief, illness, etc; (2) melancholic and recurrent depression, a genetically determined biochemical disorder manifested by an inability to experience ordinary pleasure or to cope with ordinary life events; and (3) depression associated with bipolar affective (manic-depressive) disorder. Because safe antidepressants are now available, almost any individual with several symptoms of depression that persist beyond a few weeks is a candidate for pharmacologic treatment. Intensive efforts to formalize guidelines for the treatment of depression have been pursued for more than a decade, resulting in guidelines from the American Psychiatric Association, the Agency for Health Care Policy and Research, and the World Federation of Societies of Biological Psychiatry. Pharmacologic treatment is emphasized, although a continuing role for electroconvulsive therapy for delusional or severe forms of life-threatening depression is also noted.
*Deceased.
The Pathogenesis of Major Depression: The Amine Hypothesis and Subsequent Developments
Soon after the introduction of reserpine in the early 1950s, it became apparent that the drug could induce depression. Studies revealed that the principal mechanism of action of reserpine was to inhibit the neuronal storage of amine neurotransmitters such as serotonin and norepinephrine. Reserpine induced depression and depleted stores of amine neurotransmitters; therefore, it was reasoned, depression must be associated with decreased functional amine-dependent synaptic transmission. This idea provided the basis for what became known as the amine hypothesis of depression. By extension, drugs that increased amine function in appropriate synaptic areas would relieve depression. A major puzzle in applying this hypothesis was the fact that although the pharmacologic actions of both tricyclic and monoamine oxidase (MAO) inhibitor classes of antidepressants are prompt, the clinical effects require weeks to become manifest. Attempts have been made to explain this observation by invoking slow compensatory responses to the initial blockade of amine reuptake or MAO inhibition (see below).
Current brain imaging and biochemical studies in patients do not support a single biologic abnormality as common to most depressions. Rather, prevailing hypotheses emphasize an underlying role for several brain circuits that have a propensity to become dysfunctional, especially following certain stressors, in individuals with a range of genetic predispositions. It is likely that several pathophysiologic processes will ultimately be identified to account for the presentation of what is now termed major depression.
Nevertheless, the amine hypothesis has provided the major experimental models for the discovery of new antidepressant drugs. As a result, all currently available antidepressants, except bupropion, are classified as having their primary actions on the metabolism, reuptake, or selective receptor antagonism of serotonin, norepinephrine, or both.
I. BASIC PHARMACOLOGY OF ANTIDEPRESSANTS
Chemistry
A variety of chemical structures have been found to have antidepressant activity. With the exception of bupropion, however, the core antidepressant action of even the newest agents derives from mechanisms proposed for antidepressants that were introduced four decades ago.
A. TRICYCLIC ANTIDEPRESSANTS (TCAS)
Tricyclic antidepressants¾so called because of the characteristic three-ring nucleus (Figure 30-1)¾have been used clinically for four decades. They closely resemble the phenothiazines chemically and, to a lesser extent, pharmacologically. Like the phenothiazines, tricyclics were first thought to be useful as antihistamines with sedative properties. The discovery of their antidepressant properties was a fortuitous clinical observation. Imipramine and amitriptyline are the prototypical drugs of the class as mixed norepinephrine and serotonin uptake inhibitors, although they also have several other effects.
B. SECOND-GENERATION AND SUBSEQUENT AGENTS
Between 1980 and 2005, thirteen structurally unique antidepressants and one isomeric variation were introduced. The agents classified as second generation and available for clinical use in the USA are shown in Figure 30-2. Amoxapine and maprotiline resemble the structure of the tricyclic agents, whereas trazodone and bupropion are distinctive. Newer, third generation drugs include venlafaxine, mirtazapine, nefazodone, and duloxetine. The structures of these compounds are shown in Figure 30-3. Six additional agents that work mainly through serotonin uptake inhibition are classified together in the following section.
C. SELECTIVE SEROTONIN REUPTAKE INHIBITORS (SSRIS)
Search for molecules with greater selectivity for the serotonin transporter led to the introduction of fluoxetine¾an effective and more selective antidepressant with minimal autonomic toxicity. Since that time, four more SSRIs have been introduced as well as the active enantiomeric form of one, (S)-citalopram. All are structurally distinct from the tricyclic molecules (Figure 30-4). These drugs have fewer adverse effects than the tricyclics and have become very popular.
D. MONOAMINE OXIDASE (MAO) INHIBITORS
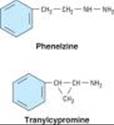
MAO inhibitors may be classified as hydrazides, exemplified by the C-N-N moiety, as is the case with phenelzine and isocarboxazid (no longer marketed); or nonhydrazides, which lack such a moiety, as with tranylcypromine (Figure 30-5).
Tranylcypromine closely resembles dextroamphetamine, which is itself a weak inhibitor of MAO. Tranylcypromine retains some of the sympathomimetic characteristics of the amphetamines. The hydrazides appear to combine irreversibly with the enzyme, whereas tranylcypromine has a prolonged duration of effect even though it is not bound irreversibly. These older MAO inhibitors are nonselective inhibitors of both MAO-A and MAO-B. Selegiline, an MAO inhibitor used in Parkinson's disease that is selective for MAO-B at low doses but less selective at higher doses, has been approved for the treatment of major depression.
|
|
Figure 30-1. Structural relationships between various tricyclic antidepressants (TCAs). |
|
|
|
Figure 30-2. Second-generation antidepressants. |
|
|
|
Figure 30-3. Newer (third-generation) antidepressants. |
||
|
|
Figure 30-4. Selective serotonin reuptake inhibitors (SSRIs). |
||
|
|
Figure 30-5. Some monoamine oxidase inhibitors. Phenelzine is the hydrazide of phenylethylamine (see Figure 9-3), whereas tranylcypromine has a cyclopropyl amine side chain and closely resembles dextroamphetamine (see Figure 9-4). These agents are unselective and produce an extremely long-lasting inhibition of the enzyme. Selegiline, which is partially selective for MAO-B, is shown in Figure 28-2. |
Pharmacokinetics
A. TRICYCLIC ANTIDEPRESSANTS
Most tricyclics are incompletely absorbed and undergo significant first-pass metabolism. As a result of high tissue protein binding and relatively high lipid solubility, volumes of distribution tend to be very large. Tricyclics are metabolized by two major routes: transformation of the tricyclic nucleus and alteration of the aliphatic side chain. Monodemethylation of tertiary amines leads to active metabolites such as desipramine and nortriptyline (which are themselves available as drugs; Figure 30-1). The pharmacokinetic parameters of various antidepressants are summarized in Table 30-1.
B. SECOND-GENERATION AND SUBSEQUENT ANTIDEPRESSANTS
The pharmacokinetics of these drugs are similar to those of the TCAs (Table 30-1). Some have active metabolites. Trazodone and venlafaxine have short plasma half-lives, which mandates divided doses during the day when beginning treatment, although once-a-day dosing may be possible later. Extended-release forms of bupropion and venlafaxine allow for once-a-day dosing in some patients from the outset.
C. SELECTIVE SEROTONIN REUPTAKE INHIBITORS
The pharmacokinetic parameters of these drugs are summarized in Table 30-1. Fluoxetine is notable for the long half-life of its active metabolite, norfluoxetine (7-9 days at steady state). This long t1/2 has allowed the introduction of a formulation for once-weekly dosing. Sertraline and paroxetine have pharmacokinetic parameters similar to those of tricyclics. Citalopram and fluvoxamine resemble fluoxetine.
D. MAO INHIBITORS
The monoamine oxidase inhibitors (MAOIs) are readily absorbed from the gastrointestinal tract. The hydrazide inhibitor phenelzine is acetylated in the liver and manifests differences in elimination, depending on the acetylation phenotype of the individual (see Chapter 4). However, inhibition of MAO persists even after these drugs (including selegiline) are no longer detectable in plasma. Therefore, conventional pharmacokinetic parameters (half-life, etc) are not very helpful in governing dosage. It is prudent to assume that the drug effect will persist for 7 days (tranylcypromine) to 2 or 3 weeks (phenelzine, selegiline) after discontinuance of the drug.
Pharmacodynamics
A. ACTIONS OF ANTIDEPRESSANTS ON AMINE NEUROTRANSMITTERS
The amine hypothesis was buttressed by studies on the mechanism of action of various types of antidepressant drugs. Tricyclics block the amine transporters (uptake pumps; Figure 30-6) known as the norepinephrine and serotonin transporters, NET and SERT, respectively. These transporters terminate amine neurotransmission (see Table 30-2 and Chapter 6). Blockade of these transporters presumably permits a longer sojourn of neurotransmitter in the intrasynaptic space at the receptor site. MAO inhibitors block a major intraneuronal degradative pathway for the amine neurotransmitters, which permits more amines to accumulate in presynaptic stores (Figure 30-6) and more to be released. Some of the second-generation antidepressants have similar strong effects on amine transporters, whereas others have only moderate or minimal effects on reuptake or metabolism. Countering this simple model of increased synaptic activity is increasing evidence of alterations in presynaptic regulation of neurotransmitter release. Presynaptic autoreceptors respond to increased synaptic transmitter by down-regulating transmitter synthesis and release. Furthermore, some (but not all) of these regulatory receptors may themselves be down-regulated. These changes occur on a slower time scale more in keeping with the clinically observed effects.
Trazodone, nefazodone, and mirtazapine stand out as agents in which antagonism of subtypes of serotonin receptors (5-HT2A or 5-HT2C) may be important in their action. Mirtazapine is unique in including antagonism of a2 norepinephrine receptors as presumably contributing to its therapeutic effects. Bupropion has been found to alter the output of norepinephrine in humans following chronic administration through some as yet unidentified primary mechanism as well as occupying about 25% of dopamine uptake transporters (DAT) in the brain as revealed by positron emission tomography. (Since it has been shown that effective doses of SSRIs occupy 80% of serotonin uptake sites, the clinical relevance of 25% DAT occupancy is uncertain.) Thus, even the newest antidepressants can still be categorized as possibly working through serotonergic and noradrenergic effects with the additional possibility of a role for dopamine. Increased synaptic dopamine has often been invoked as relevant to the efficacy of MAOIs.
B. RECEPTOR AND POSTRECEPTOR EFFECTS
Considerable attention has been paid to the long-term postsynaptic effects of increased neurotransmitters in the synapses. In tests of postsynaptic effects, especially of the tricyclics, cAMP concentrations have consistently decreased rather than increased. In addition, the number of receptors for the neurotransmitters can decrease over the same time course as clinical improvement in patients. Thus, the initial increase in neurotransmitter seen with some antidepressants appears to produce, over time, a compensatory decrease in receptor activity, ie, down-regulation of certain postsynaptic as well as presynaptic receptors.
It has long been thought that enhanced serotonergic transmission, albeit mediated through diverse mechanisms, might be a common effect of antidepressants even without an increase in synaptic serotonin. Moreover, selective antagonism of either norepinephrine or serotonin receptors as opposed to that of the 5-HT transporter may lead to enhanced extracellular serotonin due to the complex manner in which these neurotransmitters are regulated.
Most recently, long-term intracellular changes involving phosphorylation of various regulatory elements, including those within the nucleus, have been implicated as relevant to antidepressant action. It is possible that effects on certain neurotrophic factors¾factors critical to sustained survival and function of neurons in the adult nervous system¾may be central to the actions of antidepressants.
Clinical studies have indirectly tested the relevance of findings from animals for norepinephrine or serotonin function. The approach has been to reduce the amino acid precursor of serotonin, tryptophan, in the diet and, by implication, the amount of available neurotransmitter in the brain, since tryptophan availability can be rate-limiting in the formation of serotonin. Severely tryptophan-depleted diets reduce plasma tryptophan and acutely reverse antidepressant responses to SSRIs but not to NET inhibitors. Similarly, depletion of the norepinephrine amino acid precursor tyrosine can reverse antidepressant effects of the relatively selective NET inhibitor, desipramine. These findings support the hypothesis that enhanced serotonin and norepinephrine throughput is necessary for the antidepressant actions of the respective transporter inhibitors. However, tryptophan depletion does not consistently worsen the condition of unmedicated depressed patients. Thus, there is still no clear relationship between serotonin and depression or antidepressant mechanisms in general.
C. EFFECTS OF SPECIFIC ANTIDEPRESSANTS
1. Tricyclics¾ The first-generation antidepressants demonstrate varying degrees of selectivity for the reuptake pumps for norepinephrine and serotonin (Table 30-2) but selectivity is much lower than for the SSRIs. They also have numerous autonomic actions, as described below under Adverse Effects.
2. Second-generation agents¾ Amoxapine is a metabolite of the antipsychotic drug loxapine and retains some of its antipsychotic action and dopamine receptor antagonism (see Chapter 29). A combination of antidepressant and antipsychotic actions might make it a suitable drug for depression in psychotic patients. However, the dopamine antagonism may cause akathisia, parkinsonism, amenorrhea-galactorrhea syndrome, and perhaps tardive dyskinesia.
Maprotiline (a tetracyclic drug) is most like desipramine in terms of its potent norepinephrine uptake inhibition. Like desipramine, it has fewer sedative and antimuscarinic actions than the older tricyclics.
Clinical experience with trazodone has indicated unpredictable efficacy for depression, although it has proved very useful as a hypnotic, sometimes being combined with MAOIs, which disturb sleep.
3. Subsequent non-SSRI agents¾ Four antidepressants¾nefazodone, venlafaxine, duloxetine, and mirtazapine¾are all related to earlier agents in either structure or mechanism of action. Nefazodone is closely related to trazodone but is less sedating. It produces fewer adverse sexual effects than the SSRIs (see below) but is a potent inhibitor of CYP3A4. (Fluvoxamine causes the same inhibition of CYP3A4.)
Venlafaxine is a potent inhibitor of serotonin transport and a weaker inhibitor of norepinephrine transport. At lower therapeutic doses, venlafaxine behaves like an SSRI. At high doses (more than 225 mg/d), it produces mild to moderate increases of heart rate and blood pressure attributable to norepinephrine transporter inhibition. Doses in the range of 225 mg/d or more may confer broader therapeutic effects than SSRIs, but titration up to these doses is needed to control adverse effects.
Mirtazapine is a potent antihistaminic with greater sedating effects than the other second- and third-generation antidepressants. Its use is also more likely to be associated with weight gain. The hypothesized mechanism of action of mirtazapine combines 5-HT2 receptor and a-adrenoceptor antagonism and, if established in humans, would be unique among available drugs. Thus, mirtazapine may prove beneficial in patients who can tolerate its sedative effects and do not respond well to SSRIs or cannot tolerate their sexual adverse effects.
4. Selective serotonin reuptake inhibitors¾ These drugs achieve high ratios of SERT versus NET inhibition of 300 to 7000 (Table 30-2). Fluoxetine was the first SSRI to reach general clinical use. Paroxetine and sertraline differ mainly in having shorter half-lives and different potencies as inhibitors of specific P450 isoenzymes. Racemic citalopram and (S)-citalopram (escitalopram), the most selective SSRIs of all, have achieved very widespread use. Although the SSRIs have not been shown to be more effective overall than prior drugs, they lack many of the toxicities of the tricyclic and heterocyclic antidepressants. Thus, patient acceptance has been high despite their own adverse effects.
5. MAO inhibitors¾ MAO-A (isoform A) is the amine oxidase primarily responsible for norepinephrine, serotonin, and tyramine metabolism. MAO-B is more selective for dopamine. The irreversible inhibitors available in the USA are nonselective and at the doses used block both forms of the enzyme. Irreversible block of MAO, characteristic of the older MAO inhibitors, allows significant accumulation of tyramine and loss of the first-pass metabolism that protects against tyramine in foods (see Adverse Effects). Because they result in replacement of the normal transmitter (norepinephrine) stored in noradrenergic nerve terminal vesicles with a false transmitter (octopamine), they may cause significant hypotension.
|
|
Figure 30-6. Schematic diagram showing some of the potential sites of action of antidepressant drugs. The primary neuron is shown as releasing a transmitter amine (NT). A modulating neuron may release a second transmitter (NTx), regulating the activity of the primary neuron. The most consistent observed effect of the antidepressants (other than MAO inhibitors) is inhibition of the reuptake transporters (T) for norepinephrine or serotonin. The MAO inhibitors increase the vesicular stores of both NE and 5-HT. Other direct or indirect effects include initial increase in activation of pre- and postsynaptic receptors and subsequent desensitization or down-regulation of transmitter synthesis from an amino acid (AA), receptor numbers, or postreceptor mechanisms. Desensitization resulting from antidepressant use has been reported for a2, b, and 5-HT1A systems (color). VAT denotes a vesicle-associated transporter. |
II. CLINICAL PHARMACOLOGY OF ANTIDEPRESSANTS
Clinical Indications
The major indication for antidepressant drugs is to treat depression, but a number of other uses have been established by clinical experience and controlled trials.
A. DEPRESSION
This indication has been kept broad deliberately, even though evidence from clinical studies strongly suggests that the drugs are specifically useful only in major depressive episodes. Major depressive episodes are diagnosed primarily on the basis of the persistent degree and quality of depressed mood or loss of interest and pleasure in most activities, usually accompanied by disturbances of sleep, appetite, sexual drive, activity, or ability to concentrate. The diagnosis of major depression may be uncertain in individual patients, so that on balance this condition is underdiagnosed and undertreated. The depressed phase of bipolar illness definitely requires pharmacologic treatment given the high rate of suicide in persons with this disorder. Standard antidepressants are usually added to lithium or another antimanic agent; SSRIs are less likely to induce mania than the older tricyclic agents. There are, however, few controlled studies on their relative efficacy or proper duration of use. Finally, recent controlled studies support the additional labeling of the anticonvulsant lamotrigine for maintenance and prophylaxis of the depressed phase of bipolar illness.
B. ANXIETY DISORDERS: PANIC, GENERALIZED ANXIETY, AND SOCIAL PHOBIA
Imipramine was first shown in 1962 to have a beneficial effect in the acute episodes of anxiety that have come to be known as panic attacks. It has also been demonstrated that SSRIs, venlafaxine, and duloxetine are effective in panic, generalized anxiety disorder (GAD), and social phobia, but they require 6-8 weeks of treatment. Since there is considerable comorbidity between depression and anxiety disorders, it is advantageous for many patients to use a treatment that is helpful for both conditions. In some instances, because they are well tolerated and their clinical effects become evident promptly, benzodiazepines remain the preferred drugs for anxiety disorders despite the physiologic dependence associated with long-term use.
C. OBSESSIVE-COMPULSIVE DISORDERS
Potent SSRIs are uniquely effective for treating these disorders. Recent studies have focused on fluoxetine and other SSRIs, although clomipramine, the most potent mixed serotonin and norepinephrine transporter inhibitor, may be especially effective. Fluvoxamine is marketed exclusively for this disorder in the United States.
D. ENURESIS
Enuresis is an established indication for tricyclics. Proof of efficacy for this indication is substantial, but drug therapy is not the preferred approach, especially given the risks of cardiovascular effects and the dangers from overdoses.
E. CHRONIC PAIN
Clinicians in pain clinics have found tricyclics to be useful for treating a variety of chronically painful states that often cannot be definitively diagnosed. It is likely that tricyclics and other combined serotonin-norepinephrine transporter inhibitors work directly on pain pathways and do not work simply on depressive equivalents secondary to chronic pain.
In addition to TCAs, controlled studies of higher doses of venlafaxine show efficacy in pain. Duloxetine has similar effects at doses closer to standard antidepressant doses. SSRIs, however, are not effective for chronic pain.
F. OTHER INDICATIONS
Certain antidepressants have been shown to be effective for eating disorders, especially bulimia (fluoxetine), premenstrual dysphoric disorder (fluoxetine), and attention deficit hyperkinetic disorder (imipramine, desipramine). Atomoxetine was recently introduced for the treatment of attention deficit hyperactivity disorder (ADHD). This selective NET inhibitor does not appear to have the abuse liability of the standard drugs for this condition (methylphenidate and amphetamine; see Chapter 9).
Drug Choice
Controlled comparisons of the available antidepressants have usually led to the conclusion that they are roughly equivalent in efficacy. Although this may be true for groups of patients, individual patients may respond better to one drug than to another. European studies show that patients depressed enough to be hospitalized respond better to classic tricyclics than to monotherapy with SSRIs. Meta-analyses of outpatient studies also show a greater efficacy of tricyclics over SSRIs in patients who complete trials. The greater tolerability of the SSRIs, however, makes them the preferred agent for most patients. At high doses (> 225 mg), venlafaxine also shows greater efficacy than the SSRIs. Thus, finding the right drug and the right dose for the individual patient must be accomplished empirically. The history of the patient's drug experience is the most valuable guide.
Tricyclics and the second- and third-generation agents differ mainly in the degree of sedation they produce (greatest with amitriptyline, doxepin, trazodone, and mirtazapine) and their antimuscarinic effects (greatest with amitriptyline and doxepin; Table 30-2). SSRIs are generally free of sedative effects and safe in overdose. Combined with their mild adverse effects, these qualities account for the popularity of SSRIs as the most widely prescribed antidepressants.
In contrast, amoxapine and maprotiline seem to have as many sedative and autonomic actions as most tricyclics; more recently introduced antidepressants such as bupropion, venlafaxine, and duloxetine are, like SSRIs, mostly free of such effects, whereas nefazodone and mirtazapine are very sedating. Amoxapine and maprotiline are at least as dangerous as the tricyclics when taken in overdose; the other newer agents seem to be safer.
No special indications for particular types of depression have been found for SSRIs or other newer antidepressants. The popularity of these drugs, despite their higher cost, is due principally to their greater acceptance by patients. A provocative clinical report that fluoxetine use increased suicidal or aggressive ideation was not supported by subsequent analyses of massive databases. In 2004, however, because of an apparent increase in suicidal thoughts and behaviors in children on SSRIs, the FDA issued a general warning about increased risk of suicide with newer antidepressants. Studies of concurrent epidemiologic data involving much larger numbers than the trials cited by the FDA came to the opposite conclusion¾any increase in suicide risk is seen only with older antidepressants (primarily tricyclics).
Clinical reports, prescription databases, and a few trials support the use of SSRIs in combination with the older tricyclics, especially desipramine; with bupropion; and, most recently, with mirtazapine in patients who do not show an adequate response to a single agent.
MAO inhibitors remain helpful despite their adverse effects but are reserved for patients who have failed to respond to at least two courses of monotherapy or combination treatment with different classes of antidepressants.
Lithium, a mood stabilizer (see Chapter 29), in combination with an antidepressant may achieve a favorable response not obtained by the antidepressant alone.
Dosages
The usual daily dose ranges of antidepressants are shown in Table 30-3. Doses are almost always determined empirically; the patient's acceptance of adverse effects is the usual limiting factor. Tolerance to some of the objectionable effects may develop, so that the usual pattern of treatment has been to start with small doses, increasing either to a predetermined daily dose, or to one that produces relief of depression, or to the maximum tolerated dose (except in the case of nortriptyline, which loses efficacy at plasma concentrations over 150 ng/mL).
MAO inhibitors, bupropion, fluoxetine, sertraline, paroxetine, citalopram, and venlafaxine are customarily given early in the day when initiating treatment, because they can be somewhat stimulating and may cause insomnia if given late. After a few weeks on the drug, however, any such effects should disappear, and time of day administered is rarely important. Virtually all the other antidepressants have varying degrees of sedative effects and are best given near bedtime. Autonomic adverse effects also tend to be less troublesome if the dose is given late.
Maintenance Treatment
Whether or not to undertake long-term maintenance treatment of a depressed patient depends entirely on the actual history of the disorder in that individual. If the depressive episode was the patient's first and if the patient responded quickly and satisfactorily to drug therapy, it is reasonable to gradually withdraw treatment over a period of a few weeks after treating for 6-9 months. If relapse does not occur, drug treatment can be stopped until another episode occurs, which is unpredictable but highly probable. Pooled data from randomized trials covering 6-36 months reveal a more than 50% reduction in relapses or recurrences if patients are maintained on an antidepressant. Thus, a patient who has had previous episodes of depression¾especially if each succeeding one was more severe and more difficult to treat¾is a candidate for maintenance therapy. Maintenance therapy requires the full dosage used to obtain the initial response. The duration of treatment varies, though many patients require maintenance treatment indefinitely.
Unresponsive Patients
One third or more of patients do not respond (defined as 50% or more improvement) to treatment, and almost two thirds fail to achieve or maintain full remission on any single regimen. In evaluating any patient's limited response to a treatment, one should consider the five D's: diagnosis, drug, dose, duration of treatment, and different treatment.
Diagnosis might be reassessed if the patient shows little response over a period of 2-3 weeks of adequate dosage or plasma concentrations. Whether or not the patient is bipolar, lithium might be added (see Chapter 29); if psychotic, treatment might be augmented with an antipsychotic agent. Combination of an SSRI with desipramine, bupropion, or mirtazapine is safe and effective for some patients. There is no good pharmacologic rationale for combining venlafaxine or duloxetine with SSRIs because they are full serotonin reuptake inhibitors at doses that inhibit norepinephrine uptake; rather, they might be combined with bupropion or mirtazapine. At least 6-8 weeks should be tried before giving up on a drug or combination as long as there is some evidence of improvement by 3-4 weeks.
One strategy is to begin treatment with an SSRI in mild to moderate outpatient depression and then augment by adding a drug of a different class for more impaired patients. Otherwise, switch to a drug of a different class. Most experts would move through various antidepressant drug classes in the search for the right drug rather than through various drugs within a class.
Dose and duration of treatment for depression must be considered. Many treatment failures are due to inadequate dosage, which should be pushed to the limits of the patient's tolerance in refractory cases. Duration of treatment is even more important. In over 50% of patients, full response does not occur until there has been at least 8 weeks of treatment.
Finally, some patients may need a completely different type of treatment, such as electroconvulsive therapy (ECT). ECT is often viewed as a treatment of last resort, but it should not be withheld from patients with depression who cannot be helped by drug therapy. For patients with psychotic depression, ECT may be a treatment of first choice.
Noncompliance is an important cause of lack of response to drugs. Patients should be warned also that noticeable improvement may be slow, with the first clear signs taking perhaps 3 weeks or more. Inability to tolerate adverse effects and discouragement with treatment are two major causes for noncompliance and for failure of antidepressants to show efficacy.
Adverse Effects
Adverse effects of various antidepressants are summarized in Table 30-4. Most common unwanted effects are minor, but they may seriously affect patient compliance. Seriously depressed patients, however, can tolerate unwanted effects, perhaps because they are too depressed to care. In healthy volunteers, even moderate doses of the tricyclics¾amitriptyline, imipramine, clomipramine, and doxepin¾are poorly tolerated. With the SSRIs, transient nausea is the most frequent complaint, and decreased libido and sexual dysfunction create the greatest concerns in patients during maintenance treatment. Concerns about teratogenic potential recently led to revised labeling of paroxetine.
Among the major drawbacks of most first-generation antidepressants are their many "irrelevant" pharmacologic actions, a trait inherited from the phenothiazine antipsychotic agents. It appears that the antimuscarinic, antihistaminic, and a-adrenoceptor-blocking actions of tricyclic antidepressants contribute only to the undesirable effects of these agents. Blurred vision, dry mouth, urinary hesitancy or retention, and constipation represent the most common antimuscarinic complaints. Postural hypotension is a significant and potentially dangerous manifestation of the a-blocking action, especially in the elderly.
Drug Interactions
A. PHARMACODYNAMIC INTERACTIONS
The pharmacodynamic interactions of antidepressants with other drugs depend on their class. Those with sedative effects may be additive with other sedatives, especially alcohol. Patients taking tricyclics or mirtazapine should be warned that use of alcohol may lead to greater than expected impairment of driving ability. MAO inhibitors, by increasing stores of catecholamines, sensitize the patient to indirectly acting sympathomimetics such as tyramine, which is found in some fermented foods and beverages, and to sympathomimetic drugs such as diethylpropion, phenylpropanolamine, or botanicals containing ephedrine. Such sensitization can result in dangerous and¾rarely¾fatal hypertensive reactions. A pharmacodynamic interaction may occur when fluoxetine or another SSRI is used in the presence of an MAO inhibitor. The combination of increased stores of 5-HT plus inhibition of reuptake after release is thought to result in a marked increase of serotonin in the synapses, leading to a serotonin syndrome. This sometimes fatal syndrome includes hyperthermia, muscle rigidity, myoclonus, and rapid changes in mental status and vital signs (see Chapter 16).
B. PHARMACOKINETIC INTERACTIONS
The most likely pharmacokinetic interactions are between the potent inhibitors of P450 2D6, paroxetine and fluoxetine, and those drugs highly dependent on this pathway for clearance (eg, desipramine, nortriptyline, flecainide; see also Chapter 4). Actual instances of clinically significant interactions are extremely rare, and there are only a handful of case reports after cumulative exposure of more than 50 million patients to these SSRI drugs. Inhibition of P450 3A4 could possibly occur at high concentrations of nefazodone and fluvoxamine and block the metabolism of the many substrates of this isoform.
Overdoses
A. TRICYCLICS
Tricyclics are extremely dangerous when taken in overdose quantities, and depressed patients are more likely than others to be suicidal. Prescriptions should therefore be limited to amounts less than 1.25 g, or 50 dose units of 25 mg, on a "no refill" basis. If suicide is a serious possibility, the tablets should be entrusted to a family member. The drugs must be kept away from children. Both accidental and deliberate overdoses continue to occur and are serious medical emergencies. Major effects and management of overdosage are discussed in Chapter 59.
B. SECOND- AND THIRD-GENERATION DRUGS
Overdoses of amoxapine are characterized by severe neurotoxicity, with seizures that are difficult to control. Overdoses of maprotiline also have a tendency to cause seizures as well as cardiotoxicity. Overdoses of the other heterocyclic drugs appear to create only minor problems and can usually be managed with purely supportive measures.
C. MAO INHIBITORS
Intoxication with MAO inhibitors is unusual. Agitation, delirium, and neuromuscular excitability are followed by obtunded consciousness, seizures, shock, and hyperthermia. Supportive treatment is usually all that is required, though sedative phenothiazines with a-adrenoceptor-blocking action, such as chlorpromazine, may be useful.
D. SELECTIVE SEROTONIN REUPTAKE INHIBITORS
A few deaths have occurred during overdosage of SSRIs when other drugs were also being taken. The likelihood of fatalities from SSRI overdoses is extremely low. In case of overdose, only supportive treatment can be offered, since the high volume of distribution, as with other antidepressants, rules out removal of drug by dialysis. As much as 2.6 g of sertraline has been taken with survival. Overdoses of paroxetine are relatively benign: Up to 850 mg has been taken with no evidence of cardiotoxicity.
PREPARATIONS AVAILABLE
TRICYCLICS
Amitriptyline (generic, Elavil)
Oral: 10, 25, 50, 75, 100, 150 mg tablets
Parenteral: 10 mg/mL for IM injection
Amoxapine (generic)
Oral: 25, 50, 100, 150 mg tablets
Clomipramine (generic, Anafranil; labeled only for obsessive-compulsive disorder)
Oral: 25, 50, 75 mg capsules
Desipramine (generic, Norpramin)
Oral: 10, 25, 50, 75, 100, 150 mg tablets
Doxepin (generic, Sinequan)
Oral: 10, 25, 50, 75, 100, 150 mg capsules; 10 mg/mL concentrate
Imipramine (generic, Tofranil)
Oral: 10, 25, 50 mg tablets (as hydrochloride); 75, 100, 125, 150 mg capsules (as pamoate)
Nortriptyline (generic, Aventyl, Pamelor)
Oral: 10, 25, 50, 75 mg capsules; 10 mg/5 mL solution
Protriptyline (generic, Vivactil)
Oral: 5, 10 mg tablets
Trimipramine (Surmontil)
Oral: 25, 50, 100 mg capsules
SECOND-GENERATION & SUBSEQUENT DRUGS
Amoxapine (generic, Asendin)
Oral: 25, 50, 100, 150 mg tablets
Bupropion (generic, Wellbutrin)
Oral: 75, 100 mg tablets; 100, 150, 200 mg 12-hour sustained-release tablets; 150, 300 mg 24-hour sustained-release tablets
Duloxetine (Cymbalta)
Oral: 20, 30, 50 mg capsules
Maprotiline (generic)
Oral: 25, 50, 75 mg tablets
Mirtazapine (generic, Remeron)
Oral: 7.5, 15, 30, 45 mg tablets; 15, 30, 45 mg disintegrating tablets
Nefazodone (Serzone)
Oral: 50, 100, 150, 200, 250 mg tablets
Trazodone (generic, Desyrel)
Oral: 50, 100, 150, 300 mg tablets
Venlafaxine (Effexor)
Oral: 25, 37.5, 50, 75, 100 mg tablets; 37.5, 75, 150 mg extended-release capsules
SELECTIVE SEROTONIN REUPTAKE INHIBITORS
Citalopram (generic, Celexa)
Oral: 10, 20, 40 mg tablets; 10 mg/5 mL solution
Escitalopram (Lexapro)
Oral: 5, 10, 20 mg tablets; 5 mg/5 mL solution
Fluoxetine (generic, Prozac)
Oral: 10, 20, 40 mg capsules; 10, 20 mg tablets; 20 mg/5 mL liquid
Oral delayed-release (Prozac Weekly): 90 mg capsules
Fluvoxamine (generic, labeled only for obsessive-compulsive disorder)
Oral: 25, 50, 100 mg tablets
Paroxetine (generic, Paxil)
Oral: 10, 20, 30, 40 mg tablets; 10 mg/5 mL suspension; 12.5, 25, 37.5 mg controlled-release tablets
Sertraline (Zoloft)
Oral: 25, 50, 100 mg tablets; 20 mg/mL oral concentrate
MONOAMINE OXIDASE INHIBITORS
Phenelzine (Nardil)
Oral: 15 mg tablets
Tranylcypromine (Parnate)
Oral: 10 mg tablets
OTHER
Atomoxetine (Strattera)
Oral: 10, 18, 25, 40, 60 mg capsules
REFERENCES
American Psychiatric Association: DSM-IV-TR (Diagnostic and Statistical Manual of Mental Disorders, 4th ed). American Psychiatric Association, 1994, modified 2000.
American Psychiatric Association: APA practice guideline for major depressive disorder in adults (revision). Am J Psychiatry 2000;157:1.
Anderson IM, Tomenson BM: Selective serotonin reuptake inhibitors versus tricyclic antidepressants: A meta-analysis of efficacy and tolerability. J Affect Disord 2000;58:19.
Berton O, Nestler EJ: New approaches to antidepressant drug discovery: Beyond monoamines. Nat Rev Neurosci 2006;7:137.
Bradberry SM et al: Management of the cardiovascular complications of tricyclic antidepressant poisoning: Role of sodium bicarbonate. Toxicol Rev 2005;24:195.
Briley M: New hope in the treatment of painful symptoms in depression. Curr Opin Investig Drugs 2003;4:42.
Duman RS, Heninger G, Nestler E: A molecular and cellular theory of depression. Arch Gen Psychiatry 1997;54:597.
Ernst CL, Goldberg JF: Antidepressant properties of anticonvulsant drugs for bipolar disorder. J Clin Psychopharmacol 2003;23:182.
Esposito E: Serotonin-dopamine interaction as a focus of novel antidepressant drugs. Curr Drug Targets 2006;7:177.
Geddes JR et al: Relapse prevention with antidepressant drug treatment in depressive disorders: A systematic review. Lancet 2003;361:653.
Harvey AT et al: Evidence of the dual mechanisms of action of venlafaxine. Arch Gen Psychiatry 2000;57:503.
Merikangas KR et al: Workgroup Reports: NIMH Strategic Plan for Mood Disorders Research, Future of Genetics of Mood Disorders Research. Biol Psychiatry 2002;52:457.
Meyer JH et al: Occupancy of serotonin transporters by paroxetine and citalopram during treatment of depression: A [(11)C]DASB PET imaging study. Am J Psychiatry 2001;158:1843.
Mottram P, Wilson K, Strobl J: Antidepressants for depressed elderly. Cochrane Database Syst Rev 2006;CD003491.
Nestler EJ et al: Preclinical models: Status of basic research in depression. Biol Psychiatry 2002;52:503.
Potter WZ: Adrenoceptors and serotonin receptor function: Relevance to antidepressant mechanisms of action. J Clin Psychiatry 1996;57(Suppl 4):4.
Rush JA, Ryan ND: Current and emerging therapeutics for depression. In: Davis KL et al (editors): Neuropsychopharmacology: The Fifth Generation of Progress. Lippincott Williams & Wilkins, 2002.
Schatzberg I et al: Molecular and cellular mechanisms in depression. In: Davis KL et al (editors): Neuropsychopharmacology. The Fifth Generation of Progress. Lippincott Williams & Wilkins, 2002.