Douglas C. Bauer, MD, & Stephen J. McPhee, MD
The thyroid gland synthesizes the hormones thyroxine (T4) and triiodothyronine (T3), iodine-containing amino acids that regulate the body’s metabolic rate. Adequate levels of thyroid hormone are necessary in infants for normal development of the CNS, in children for normal skeletal growth and maturation, and in adults for normal function of multiple organ systems. Thyroid dysfunction is one of the most common endocrine disorders encountered in clinical practice. Although abnormally high or low levels of thyroid hormones may be tolerated for long periods of time, usually there are symptoms and signs of overt thyroid dysfunction.
NORMAL STRUCTURE & FUNCTION
ANATOMY
The normal thyroid gland is a firm, reddish brown, smooth gland consisting of two lateral lobes and a connecting central isthmus (Figure 20-1). A pyramidal lobe of variable size may extend upward from the isthmus. The normal weight of the thyroid ranges from 30–40 g. It is surrounded by an adherent fibrous capsule from which multiple fibrous projections extend deeply into its structure, dividing it into many small lobules. The thyroid is highly vascular and has one of the highest rates of blood flow per gram of tissue of any organ.
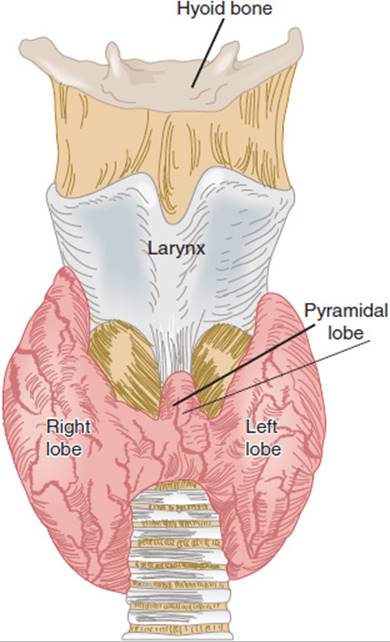
FIGURE 20-1 The human thyroid. (Redrawn, with permission, from Barrett KE et al, eds. Ganong’s Review of Medical Physiology, 24th ed. McGraw-Hill, 2012.)
HISTOLOGY
Histologically, the thyroid gland consists of many closely packed acini, called follicles, each surrounded by capillaries and stroma. Each follicle is roughly spherical, lined by a single layer of cuboidal epithelial cells and filled with colloid, a proteinaceous material composed mainly of thyroglobulin and stored thyroid hormones. When the gland is inactive, the follicles are large, the lining cells are flat, and the colloid is abundant. When the gland is active, the follicles are small, the lining cells are cuboidal or columnar, the colloid is scanty, and its edges are scalloped, forming reabsorption lacunae (Figure 20-2). Scattered between follicles are the parafollicular cells (C cells), which secrete calcitonin, a hormone that inhibits bone resorption and lowers the plasma calcium level (see Chapter 17).
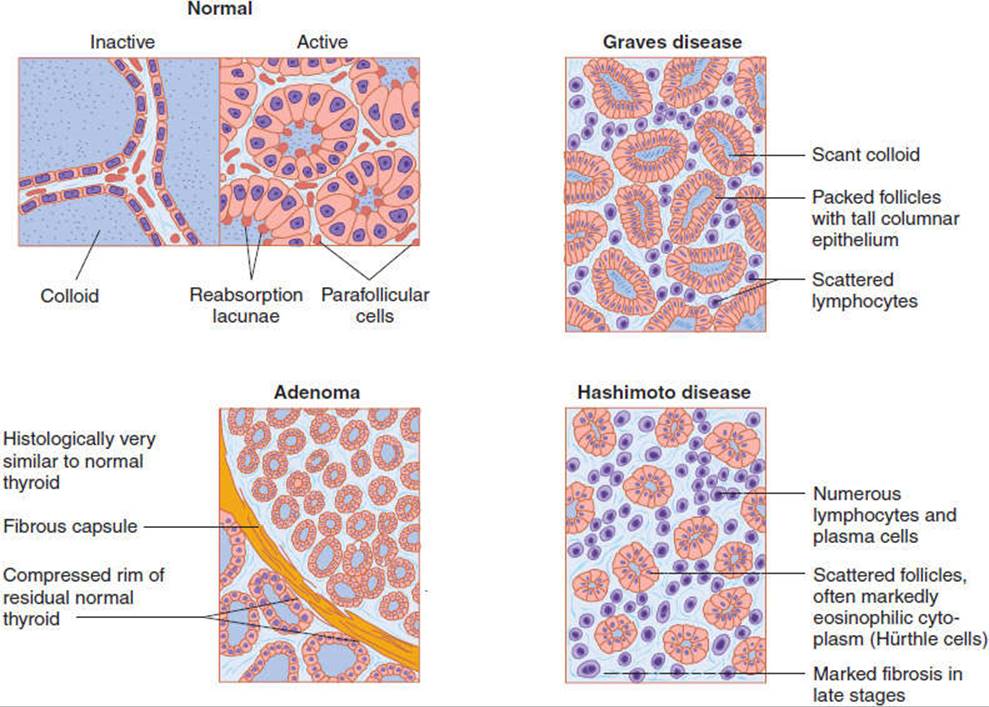
FIGURE 20-2 Normal and abnormal thyroid histology. (Redrawn, with permission, from Barrett KE et al, eds. Ganong’s Review of Medical Physiology, 24th ed. McGraw-Hill, 2012; Chandrasoma P et al, eds. Concise Pathology, 3rd ed. Originally published by Appleton & Lange. Copyright © by The McGraw-Hill Companies, Inc.; Gardner DG et al, eds. Greenspan’s Basic and Clinical Endocrinology, 9th ed. McGraw-Hill, 2011.)
The ultrastructure of a follicular epithelial cell is diagrammed in Figure 20-3. The cells vary in appearance with the degree of gland activity. The follicular cell rests on a basal lamina. The nucleus is round and centrally located. The cytoplasm contains mitochondria, rough endoplasmic reticulum, and ribosomes. The apex has a discrete Golgi apparatus, small secretory granules containing thyroglobulin, and abundant lysosomes and phagosomes. At the apex, the cell membrane is folded into microvilli.
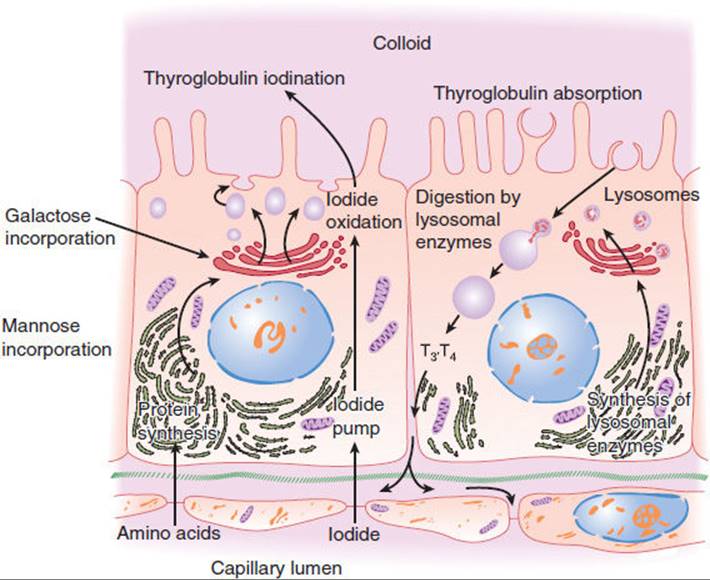
FIGURE 20-3 Thyroid cell ultrastructure (schematic). The processes of synthesis and iodination of thyroglobulin are shown on the left and its reabsorption and digestion on the right. (Redrawn, with permission, from Junqueira LC et al, eds. Basic Histology, 9th ed. Originally published by Appleton & Lange. Copyright © 1998 by The McGraw-Hill Companies, Inc.)
PHYSIOLOGY
Formation & Secretion of Thyroid Hormones
A. T4, T3, and Thyroglobulin
Thyroid follicular cells have three functions: (1) collect and transport iodine to the colloid; (2) synthesize thyroglobulin, a 660,000-Da glycoprotein made up of two subunits and containing many tyrosine residues, and secrete it into the colloid; and (3) release thyroid hormones from thyroglobulin and secrete them into the circulation. The structures of the two thyroid hormones, T3 and T4, are shown in Figure 20-4. T3 and T4 are synthesized in the colloid by iodination and condensation of tyrosine molecules bound together in thyroglobulin.
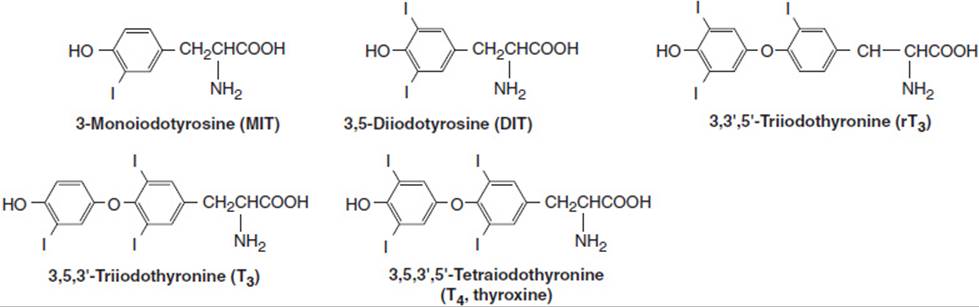
FIGURE 20-4 MIT, DIT, T3, T4, and rT3.
B. Iodine Metabolism and Trapping
For normal thyroid hormone synthesis, an adult requires a minimum daily intake of 150 μg of iodine. In the United States, the average intake is about 500 μg/d. Iodine ingested in food is first converted to iodide, which is absorbed and taken up by the thyroid. The follicular cells transport iodide from the circulation to the colloid (“iodide trapping” or “iodide pump”). The sodium-iodide symporter is a 65-kDa cell membrane protein. This iodide transport is an example of secondary active transport dependent on Na+-K+ adenosine triphosphatase (ATPase) for energy; it is stimulated by thyroid-stimulating hormone(TSH, thyrotropin). At the normal rate of thyroid hormone synthesis, about 120 μg/d of iodide enters the thyroid. About 80 μg/d is secreted in T3 and T4, and the rest diffuses into the extracellular fluid and is excreted in the urine.
C. Thyroid Hormone Synthesis and Secretion
Thyroid hormones are synthesized in the colloid, near the apical cell membrane of the follicular cells. Catalyzed by the enzyme thyroidal peroxidase, iodide in the thyroid cell is oxidized to iodine. The iodine enters the colloid and is rapidly bound at the 3 position (Figure 20-4) to tyrosine molecules attached to thyroglobulin, forming monoiodotyrosine (MIT). MIT is next iodinated at the 5 position, forming diiodotyrosine (DIT). Two DIT molecules then condense in an oxidative process (“coupling reaction”) catalyzed by thyroperoxidase to form one thyroxine (T4) molecule. Some T3 is probably formed within the thyroid gland by condensation of MIT with DIT. A small amount of reverse T3 (rT3) is also formed. Figure 20-4 shows the structures of MIT, DIT, T4, T3, and reverse T3. In the normal thyroid, the average distribution of iodinated compounds is 23% MIT, 33% DIT, 35% T4, 7% T3, and 2% reverse T3.
The thyroid secretes about 80 μg (103 nmol) of T4 and 4 μg (7 nmol) of T3 per day. The folds of the apical cell membrane (lamellipodia) encircle bits of colloid and bring them into the cytoplasm by endocytosis, forming endosomes. This process is accelerated by TSH. The endosomes fuse with lysosomes containing proteases that break peptide bonds between the iodinated residues and thyroglobulin, releasing T4, T3, DIT, and MIT into the cytoplasm. The free T4 and T3 then cross the cell membrane and enter adjacent capillaries. The MIT and DIT are enzymatically degraded in the cell by thyroid deiodinase (iodotyrosine dehalogenase) to iodine and tyrosine, which are reused in colloid synthesis.
D. Thyroid Hormone Transport and Metabolism
The normal plasma level of T4 is approximately 8 μg/dL (103 nmol/L) (range: 5–12 μg/dL or 65–156 nmol/L), and the normal plasma level of T3 is approximately 0.15 μg/dL (2.3 nmol/L) (range: 0.08–0.22 μg/dL or 1.2–3.3 nmol/L). Both hormones are bound to plasma proteins, including albumin, transthyretin (formerly called thyroxine-binding prealbumin [TBPA]), and thyroxine-binding globulin (TBG). The thyroid hormone-binding proteins serve mainly to transport T4 and T3 in the serum and to facilitate uniform distribution of hormones within tissues.
Physiologically, it is the free (unbound) T4 and T3 in plasma that are active and inhibit pituitary secretion of TSH. The free T4 and T3 are in equilibrium with the protein-bound hormones in plasma and tissue and circulate in much lower concentrations. Tissue uptake of the free hormones is proportionate to their plasma concentrations.
Almost all (99.98%) of the circulating T4 is bound to thyroxine-binding globulin (TBG) and other plasma proteins, so that the free T4 level is approximately 2 ng/dL. The biologic half-life of T4 is long (about 6–7 days). Somewhat less T3 (99.8%) is protein bound. Therefore, compared with T4, T3 acts more rapidly and has a shorter half-life (about 30 hours). It is also three to five times more potent on a molar basis.
T4 and T3 are metabolized in the liver, kidneys, and many other tissues by deiodination and by conjugation to glucuronides. Normally, one-third of circulating T4 is converted to T3 by 5′-deiodination, and 45% is converted to the metabolically inert reverse triiodothyronine (rT3) by 5-deiodination. About 87% of circulating T3 derives from peripheral conversion of T4 to T3 and only 13% from thyroid secretion. Both T4 and T3 are conjugated to glucuronides in the liver and excreted into the bile. On passage into the intestine, the conjugates are hydrolyzed, and small amounts of T4 and T3 are reabsorbed (enterohepatic circulation). The rest is excreted in the stool.
Regulation of Thyroid Secretion
Thyroid hormone secretion is stimulated by pituitary thyroid-stimulating hormone (TSH, thyrotropin). Pituitary TSH secretion is, in turn, stimulated by thyrotropin-releasing hormone (TRH), a tripeptide secreted by the hypothalamus that also increases the biologic activity of TSH, by altering its glycosylation.
TSH is a two-subunit glycoprotein containing 211 amino acids. The α-subunit is identical to that of pituitary follicle-stimulating hormone (FSH), luteinizing hormone (LH), and placental human chorionic gonadotropin (hCG). The β-subunit confers the specific binding properties and biologic activity of TSH. The gene encoding the α-subunit is located on chromosome 6, and the gene for the β-subunit is on chromosome 1.
TSH has a biologic half-life of about 60 minutes. The average plasma level of TSH is 2 mU/L (normal range: 0.4–4.8 mU/L). When individuals with autoantibodies, goiter, or a family history of thyroid disease are excluded, the upper limit is somewhat lower, between 2.5–3.0 mU/L. Controversy exists over the effects of advanced age on the normal range for TSH. Several population-based studies have found that the upper limit of normal in healthy older individuals (older than 80 years) might be as high as 7.5 mU/L, but the clinical significance of using age-specific upper limit cut-points remains unclear. Although the phenomenon is not clinically important, normal TSH secretion exhibits a circadian pattern, rising in the afternoon and evening, peaking after midnight, and declining during the day.
Circulating free T4 and T3 inhibit TSH secretion by the pituitary both directly and indirectly by regulating biosynthesis of TRH in the hypothalamus. TSH secretion is inhibited by stress, perhaps via glucocorticoid inhibition of TRH secretion. In infants, but not in adults, TSH secretion is increased by cold and inhibited by warmth. Dopamine and somatostatin also inhibit pituitary secretion of TSH. In animals, there is a pituitary-specific form of the thyroid hormone receptor that may be selectively regulated by thyroid hormone. Figure 20-5 illustrates the hypothalamic-pituitary-thyroid axis and various stimulatory and inhibitory factors.
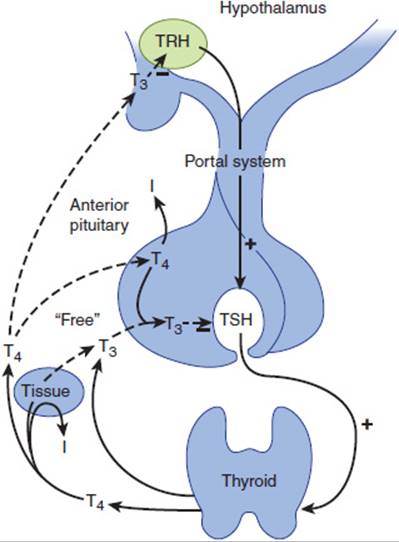
FIGURE 20-5 Hypothalamic-pituitary-thyroid axis. T4, thyroxine; T3, triiodothyronine; TRH, thyrotropin-releasing hormone; TSH, thyroid-stimulating hormone. (Redrawn and modified, with permission, from Gardner DG et al, eds. Greenspan’s Basic and Clinical Endocrinology, 9th ed. McGraw-Hill, 2011.)
When TSH is secreted or administered, it binds to a specific TSH receptor (TSH-R) in the thyroid cell membrane, activating the GTP-binding (Gs) protein-adenylyl cyclase-cyclic adenosine monophosphate (cAMP) cascade. The increase in intracellular cAMP mediates immediate increases in uptake and transport of iodide, iodination of thyroglobulin, and synthesis of iodotyrosines T3 and T4. Within a few hours, there is an increase in mRNA for thyroglobulin and thyroidal peroxidase, enhanced lysosomal activity, increased secretion of thyroglobulin into colloid, more endocytosis of colloid, and increased secretion of T4 and T3 from the gland. TSH receptor is also expressed in lymphocytes and other tissues, including the pituitary, thymus, kidney, testis, brain, adipocytes, and fibroblasts. TSH-R has also been detected on osteoblast precursors, suggesting that TSH may have a direct effect on bone resorption.
TSH binding to TSH receptor also stimulates membrane phospholipase C, which leads to thyroid cell hypertrophy. With chronic TSH stimulation, the entire gland hypertrophies, increases in vascularity, and becomes a goiter.
TSH receptor has been cloned. It is a single-chain glycoprotein composed of 744 amino acids. Two specific amino acid sequences are thought to represent different binding sites for TSH and for the TSH-R–stimulating antibody(TSH-R [stim] Ab) found in Graves disease (see later).
The amount of thyroid hormone needed to maintain normal organ system function in thyroidectomized individuals is defined as the amount necessary to maintain the plasma TSH within the normal range (0.4–4.8 mU/L). About 80% of orally administered levothyroxine is absorbed from the GI tract, and 100–125 μg/d usually maintains a normal plasma TSH in individuals of average size.
Mechanism of Action of Thyroid Hormones
Thyroid hormones exert their actions by two mechanisms: (1) genomic actions mediated by T3 interactions with its nuclear receptors, regulating gene activity; and (2) nongenomic actions effected by T3 and T4 interactions with specific enzymes (such as pyruvate kinase, adenylate cyclase, and calcium APTase), mitochondrial proteins, and glucose transporters. Thyroid hormones enter target tissue cells by either passive diffusion or specific transport carriers through the cell membrane and cytoplasm. Within the cell cytoplasm, most of the T4 is converted to T3. The nuclear receptor for T3 has been cloned and found to be similar to the nuclear receptors for glucocorticoids, mineralocorticoids, estrogens, progestins, vitamin D3, and retinoic acid. For reasons that are unclear, there are two different receptor (TR) genes in humans. Each gene (hTR-α and hTR-β) yields at least two differently spliced proteins: hTR-α (hTR-α1 and hTR α2) and hTR-β (hTR-β1 and hTR-β1). hTR-α2 may be biologically inactive. The TR gene for the alpha form is on chromosome 17 and for the beta form, on chromosome 3. The two different receptor forms may help to explain both the normal variation in thyroid hormone responsiveness of various organs and the selective tissue abnormalities found in various thyroid resistance syndromes. For example, the brain contains mostly α receptors, the liver contains mostly β receptors, and the heart contains both. Point mutations in the hTR-β1 gene result in abnormal T3 receptors and the syndrome of generalized resistance to thyroid hormone (Refetoff syndrome).
When the T3 receptor complex binds to DNA, it increases expression of specific genes, with the induction of related messenger RNAs. A wide variety of enzymes must be produced to account for the many effects of thyroid hormones on cell function.
Effects of Thyroid Hormones
The effects of thyroid hormones in various organs are summarized in Table 20-1. Thyroid hormones increase the activity of membrane-bound Na+-K+ ATPase, increase heat production, and stimulate oxygen consumption (calorigenesis). Thyroid hormones also affect tissue growth and maturation, help regulate lipid metabolism, increase cardiac contractility by stimulating the expression of myosin protein, and increase intestinal absorption of carbohydrates.
TABLE 20-1 Physiologic effects of thyroid hormones.
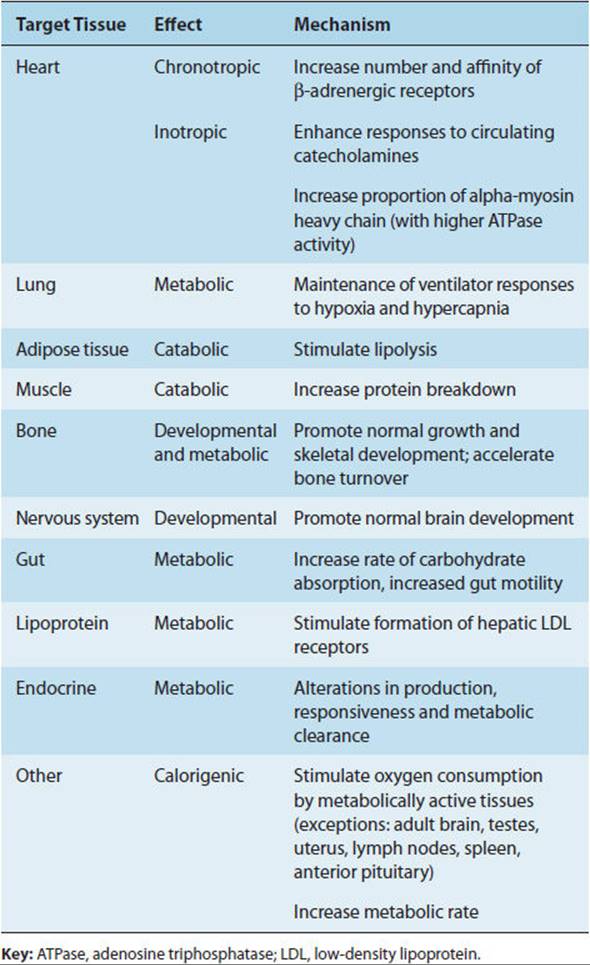
The effects of T4 and T3 and the catecholamines epinephrine and norepinephrine are closely interrelated. Both increase the metabolic rate and stimulate the nervous system and heart. In humans, the transcriptional effects of T3include production of increased numbers of (and perhaps sensitivity to) β-adrenergic receptors in the heart, skeletal muscle, adipose tissue, and lymphocytes.
CHECKPOINT
1. Describe a thyroid follicle and its change with activity versus inactivity of the gland.
2. What forms of thyroid hormone does the thyroid gland secrete? What are the normal proportions of the different forms? What are the relative potencies of each hormone?
3. To what is thyroid hormone bound during its transport in plasma?
4. How are thyroid hormone levels regulated?
5. What is the mechanism of action of thyroid hormone?
6. What are the most prominent organ system–specific effects of thyroid hormone?
OVERVIEW OF THYROID DISEASE
The symptoms and signs of thyroid disease in humans are predictable consequences of the physiologic effects of thyroid hormones discussed previously. The clinician commonly encounters patients with one of five types of thyroid dysfunction: (1) hyperthyroidism (thyrotoxicosis), caused by an excess of thyroid hormones; (2) hypothyroidism (myxedema), caused by a deficiency of thyroid hormones; (3) goiter, a diffuse enlargement of the thyroid gland, caused by prolonged elevation of TSH; (4) thyroid nodule, a focal enlargement of a portion of the gland, caused by a benign or malignant neoplasm; and (5) abnormal thyroid function tests in a clinically euthyroid patient.
Several laboratory tests are useful in the initial evaluation of patients suspected of having thyroid dysfunction. The first is plasma TSH measured by a sensitive assay (usually defined by a lower detection limit of 0.1 mU/L or less). TSH is below normal in hyperthyroidism and above normal in hypothyroidism (except in the rare instances of pituitary or hypothalamic disease). The second useful laboratory test is measurement of non-protein-bound thyroxine. Most clinical laboratories are now able to accurately measure free thyroxine (FT4) directly. Although rarely used today, an estimate of non-protein-bound thyroxine is provided by the free thyroxine index (FT4I), the product of the total plasma thyroxine (TT4) and the T4 resin uptake (RT4U) (ie, FT4I = TT4 × RT4U). The TT4 by itself often reflects the functional state of the thyroid hormone–binding proteins. The RT4U is an indicator of thyroid-binding globulin and serves to correct for alterations in the concentration of binding protein. Some laboratories instead measure T3 resin uptake (RT3U).
Although total and free T3 levels can be measured, they have a short half-life and are technically difficult assays. Under most circumstances, circulating levels of T3 correlate less well with clinical hyperthyroidism or hypothyroidism.
A variety of thyroid autoantibodies are detectable in patients with thyroid dysfunction, including (1) thyroidal peroxidase antibody (TPO Ab), formerly termed antimicrosomal antibody; (2) thyroglobulin antibody (Tg Ab); and (3) TSH receptor antibody, either stimulating (TSH-R [stim] Ab) or blocking (TSH-R [block] Ab). Thyroglobulin and thyroidal peroxidase antibodies are commonly found in hypothyroidism resulting from Hashimoto thyroiditis and occasionally in hyperthyroidism from Graves disease (see later). TSH-R [stim] Ab is present in individuals with hyperthyroidism caused by Graves disease. Detection of TSH-R [block] Ab in maternal serum is predictive of congenital hypothyroidism in newborns of mothers with autoimmune thyroid disease.
Other procedures such as thyroid scans and the thyrotropin-releasing hormone (TRH) test are discussed later.
PATHOPHYSIOLOGY OF SELECTED THYROID DISEASES
The pathogenesis of the most common thyroid diseases probably involves an autoimmune process with sensitization of the host’s own lymphocytes to various thyroidal antigens. Three major thyroidal antigens have been documented: thyroglobulin (Tg), thyroidal peroxidase (TPO), and the TSH receptor. Both environmental factors (eg, viral or bacterial infection or high iodine intake) and genetic factors (eg, defect in suppressor T lymphocytes) may be responsible for initiating autoimmune thyroid disease.
HYPERTHYROIDISM
Etiology
The causes of hyperthyroidism are listed in Table 20-2. Most commonly, thyroid hormone overproduction is due to Graves disease. In Graves disease, the TSH receptor autoantibody TSH-R [stim] Ab stimulates the thyroid follicular cells to produce excessive amounts of T4 and T3. Less commonly, patients with multinodular goiter may become thyrotoxic without circulating antibodies if given inorganic iodine (eg, potassium iodide) or organic iodine compounds (eg, the antiarrhythmic drug amiodarone, which contains 37% iodine by weight). Multinodular goiters may also develop one or more nodules that become autonomous from TSH regulation and secrete excessive quantities of T4 or T3. Patients from regions where goiter is endemic may develop thyrotoxicosis when given iodine supplementation (jodbasedow phenomenon). Large follicular adenomas (>3 cm in diameter) may produce excessive thyroid hormone.
TABLE 20-2 Hyperthyroidism: causes and pathogenetic mechanisms.

Occasionally, TSH overproduction (eg, from a pituitary adenoma) or hypothalamic disease may cause excessive thyroid hormone production. The diagnosis is suggested by clinically evident hyperthyroidism with elevated serum T4and T3 and elevated serum TSH levels. Neuroradiologic procedures such as computed tomography (CT) scans or magnetic resonance imaging (MRI) of the sella turcica confirm the presence of a pituitary tumor. Even more rarely, hyperthyroidism results from TSH overproduction caused by pituitary (but not peripheral tissue) resistance to the suppressive effects of T4 and T3. The diagnosis is suggested by finding elevated serum T4 and T3 levels with an inappropriately normal serum TSH level.
Hyperthyroidism may be precipitated by germ cell tumors (choriocarcinoma and hydatidiform mole), which secrete large quantities of human chorionic gonadotropin (hCG). The large quantities of hCG secreted by these tumors bind to the follicular cell TSH receptor and stimulate overproduction of thyroid hormone. Rarely, hyperthyroidism can be produced by ovarian teratomas containing thyroid tissue (struma ovarii). Hyperthyroidism results when this ectopic thyroid tissue begins to function autonomously. Patients with large metastases from follicular thyroid carcinomas may produce excess thyroid hormone, particularly after iodide administration.
Transient hyperthyroidism is occasionally observed in patients with lymphocytic or granulomatous (subacute) thyroiditis (Hashimoto thyroiditis). In such cases, the hyperthyroidism is due to destruction of the thyroid with release of stored hormone.
Finally, patients who consume excessive amounts of exogenous thyroid hormone (accidentally or deliberately) and those treated with amiodarone or interferon alpha may present with symptoms, signs, and laboratory findings of hyperthyroidism.
Pathogenesis
Whatever the cause of hyperthyroidism, serum thyroid hormones are elevated. Both the free thyroxine (FT4) and the free thyroxine index (FT4I) are elevated. In 5–10% of patients, T4 secretion is normal while T3 levels are high (so-called T3 toxicosis). Total serum T4 and T3 levels are not always definitive because of variations in concentrations of thyroid hormone–binding proteins.
Hyperthyroidism resulting from Graves disease is characterized by a suppressed serum TSH level as determined by sensitive immunoenzymometric or immunoradiometric assays. However, TSH levels may also be suppressed in some acute psychiatric and other nonthyroidal illnesses. In the rare TSH-secreting pituitary adenomas (so-called secondary hyperthyroidism) and in hypothalamic disease with excessive TRH production (so-called tertiary hyperthyroidism), hyperthyroidism is accompanied by elevated plasma TSH.
The radioactive iodine (RAI) uptake of the thyroid gland at 4, 6, or 24 hours is increased when the gland produces an excess of hormone (eg, Graves disease); it is decreased when the gland is leaking stored hormone (eg, thyroiditis), when hormone is produced elsewhere (eg, struma ovarii), and when excessive exogenous thyroid hormone is being ingested (eg, factitious hyperthyroidism). Technetium 99m scanning can provide information similar to that obtained with RAI and is quicker and entails less radiation exposure.
The TRH test is sometimes helpful in diagnosis when patients have confusing results of thyroid function tests. In normal individuals, administration of TRH (500 μg intravenously) produces an increase in serum TSH of at least 6 mU/L within 15–30 minutes. In primary hyperthyroidism, TSH levels are low and TRH administration induces little or no rise in the TSH level.
Graves Disease
A. Pathology
Graves disease is the most common cause of hyperthyroidism. In this condition, the thyroid gland is symmetrically enlarged and its vascularity markedly increased. The gland may double or triple in weight. Microscopically, the follicular epithelial cells are columnar in appearance and increased in number and size (Figure 20-2). The follicles are small and closely packed together. The colloid is scanty; the edges are scalloped in appearance secondary to the rapid proteolysis of thyroglobulin. The gland’s interstitium is diffusely infiltrated with lymphocytes and may contain lymphoid follicles with germinal centers.
B. Pathogenesis
The serum of more than 90% of patients with Graves disease contains TSH-R [stim] antibody, directed against the TSH receptor site in the thyroid follicular epithelial membrane. This antibody, formerly called long-acting thyroid stimulator (LATS), is now also called thyroid-stimulating immunoglobulin (TSI). When it binds to the cell membrane TSH receptors, TSH-R [stim] Ab stimulates hormone synthesis and secretion in somewhat the same way as TSH. Although serum levels of TSH-R [stim] Ab correlate poorly with disease severity, its presence can be helpful diagnostically and perhaps prognostically. After discontinuation of antithyroid drug treatment, about 30–50% of patients with Graves hyperthyroidism relapse. There seems to be a greatly increased recurrence risk if the TSH-R [stim] Ab is still found in plasma at the time of discontinuation of the antithyroid drug treatment, so this test can perhaps be used to predict likely relapse.
The genesis of TSH-R [stim] Ab in patients with Graves disease is uncertain. However, Graves disease is familial. A genetic contribution to the development of Graves disease is suggested by the finding of much higher concordance rates in monozygotic same-sex twin pairs (0.35) than in dizygotic pairs (0.03). In Caucasians, it is associated with the HLA-B8 and HLA-DR3 histocompatibility antigens; in Asians, with HLA-Bw46 and HLA-B5; and in blacks, with HLA-B17. Furthermore, patients with Graves disease frequently suffer from other autoimmune disorders (Table 20-3). The precipitating cause of this antibody production is unknown, but an immune response against a viral antigen that shares homology with TSH receptor may be responsible. Another theory of the pathogenesis of Graves disease is a defect of suppressor T lymphocytes, which allows helper T lymphocytes to stimulate B lymphocytes to secrete antibodies directed against follicular cell membrane antigens, including the TSH receptor (Figure 20-6).
TABLE 20-3 Autoimmune disorders associated with Graves disease and Hashimoto thyroiditis.
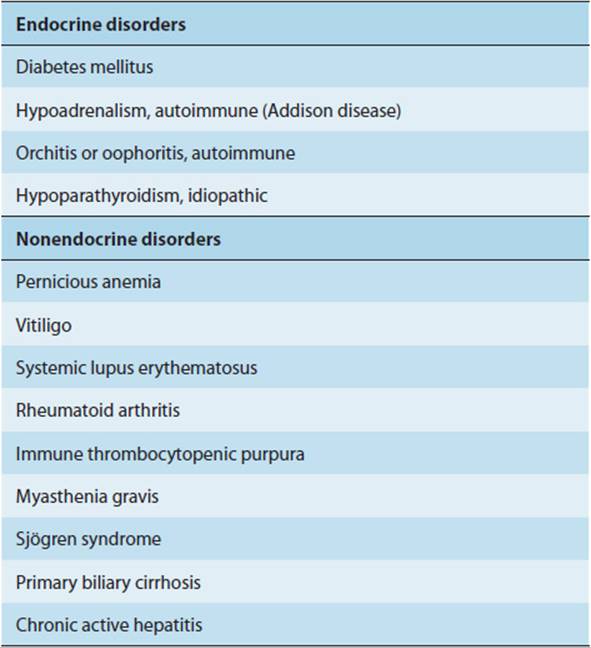

FIGURE 20-6 Proposed pathogenesis of Graves disease. A defect in suppressor T lymphocytes (Ts) allows helper T lymphocytes (TH) to stimulate B lymphocytes (B) to synthesize thyroid autoantibodies. The thyroid receptor–stimulating antibody (TSH-R [stim] Ab) is the driving force for thyrotoxicosis. Inflammation of the orbital muscles may be due to sensitization of cytotoxic T lymphocytes (Tc), or killer cells, to orbital antigens linked to an antigen in the thyroid. What triggers this immunologic cascade is not known. Ag, antigen; P Ab, peroxidase or microsomal antibody; Tg Ab, thyroglobulin antibody. (Redrawn, with permission, from Gardner DG et al, eds. Greenspan’s Basic and Clinical Endocrinology, 9th ed. McGraw-Hill, 2011.)
Moderate titers of other autoantibodies (thyroidal peroxidase antibody and TSH-R [block] Ab) can be found in patients with Graves disease. Their significance is uncertain. In some cases, TSH-R [block] Ab appears after 131I radioiodine therapy of Graves disease.
Patients with hyperthyroidism from Graves disease may later develop hypothyroidism by one of several mechanisms: (1) thyroid ablation by surgery or 131I radiation treatment; (2) autoimmune thyroiditis, leading to thyroid destruction; and (3) development of antibodies that block TSH stimulation (TSH-R [block] Ab).
After radioactive iodine therapy, there is often a lag in recovery of thyrotropin (TSH) responsiveness that may last 60–90 days or longer. During this period, decisions regarding further therapy must be based on the patient’s clinical status as well as on the serum levels of TSH and thyroid hormones.
CHECKPOINT
7. What are the five categories of thyroid dysfunction most commonly observed in patients?
8. What are seven different pathophysiologic mechanisms by which a patient might develop hyperthyroidism?
9. What is the most useful initial test of thyroid function in hyperthyroidism? What results would you expect compared with normal?
10. How can thyroid scanning help confirm the suspected cause of hyperthyroidism?
11. Describe the mechanism of hyperthyroidism in Graves disease.
Clinical Manifestations
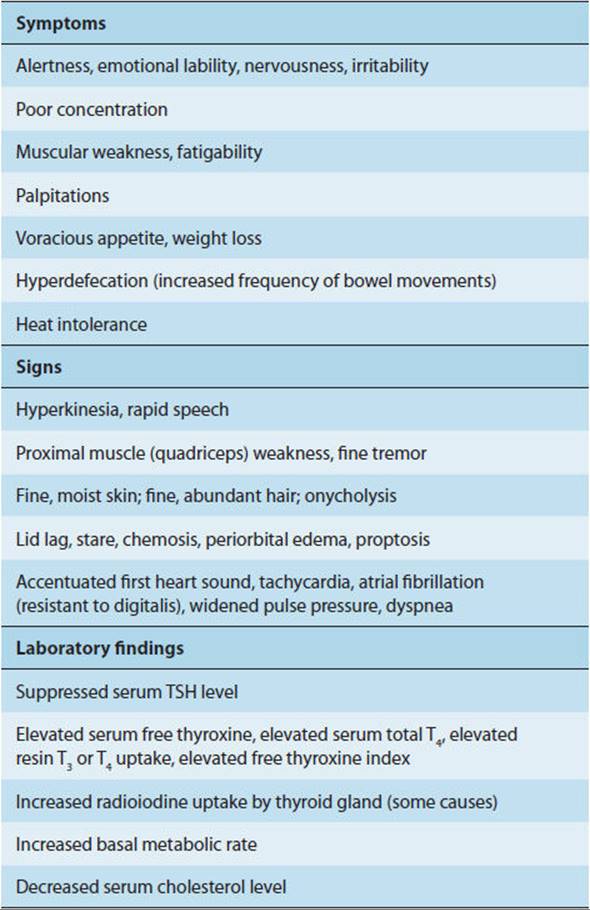
The clinical consequences of thyroid hormone excess (Table 20-4) are exaggerated expressions of the physiologic activity of T3 and T4.
TABLE 20-4 Clinical findings in hyperthyroidism (thyrotoxicosis).
An excess of thyroid hormone causes enough extra heat production to result in a slight rise in body temperature and to activate heat-dissipating mechanisms, including cutaneous vasodilation and a decrease in peripheral vascular resistance and increased sweating. The increased basal metabolic rate leads to weight loss, especially in older patients with poor appetite. In younger patients, food intake typically increases, and some patients have seemingly insatiable appetites.
The apparent increased catecholamine effect of hyperthyroidism is probably multifactorial in origin. Thyroid hormones increase β-adrenergic receptors in many tissues, including heart muscle, skeletal muscle, adipose tissue, and lymphocytes. They also decrease α-adrenergic receptors in heart muscle and may amplify catecholamine action at a postreceptor site. Thus, thyrotoxicosis is characterized by an increased metabolic and hemodynamic sensitivity of the tissues to catecholamines. However, circulating catecholamine levels are normal. Drugs that block β-adrenergic receptors reduce or eliminate the tachycardia, arrhythmias, sweating, and tremor of hyperthyroidism. When β blockers are used in the treatment of hyperthyroidism, it appears that “nonselective” β blockers (such as propranolol), which block both β1 and β2 receptors, have an advantage over “selective” β1 blockers (such as metoprolol). The “nonselective” agents appear to reduce the metabolic rate significantly, whereas the “selective” β1 blockers do not reduce oxygen consumption and provide only symptomatic relief related to the normalization of heart rate.
Thyroid hormone excess causes rapid mentation, nervousness, irritability, emotional lability, restlessness, and even mania and psychosis. Patients complain of poor concentration and reduced performance at work or in school. Tremor is common and deep tendon reflexes are brisk, with a rapid relaxation phase. Muscle weakness and atrophy (thyrotoxic myopathy) commonly develop in hyperthyroidism, particularly if severe and prolonged. Proximal muscle weakness may interfere with walking, climbing, rising from a deep knee bend, or weight lifting. Such muscle weakness may be due to increased protein catabolism and muscle wasting, decreased muscle efficiency, or changes in myosin. Despite an increased number of β-adrenergic receptors in muscle, the increased proteolysis is apparently not mediated by β receptors, and muscle weakness and wasting are not affected by β-adrenergic blockers. Myasthenia gravis or periodic paralysis may accompany hyperthyroidism.
Vital capacity and respiratory muscle strength are reduced. Extreme muscle weakness may cause respiratory failure.
In hyperthyroidism, cardiac output is increased as a result of increased heart rate and contractility and reduced peripheral vascular resistance. Pulse pressure is increased, and circulation time is shortened in the hyperthyroid state. Tachycardia, usually supraventricular, is frequent and thought to be related to the direct effects of thyroid hormone on the cardiac conducting system. Atrial fibrillation may occur, particularly in elderly patients. Continuous 24-hour electrocardiographic monitoring of thyrotoxic patients shows persistent tachycardia but preservation of the normal circadian rhythm of the heart rate, suggesting that normal adrenergic responsiveness persists. Myocardial calcium uptake is increased in thyrotoxic rats; in humans, calcium channel–blocking agents (eg, diltiazem) can decrease heart rate, number of premature ventricular beats, and number of bouts of supraventricular tachycardia, paroxysmal atrial fibrillation, and ventricular tachycardia. Patients with hyperthyroidism may manifest acute heart failure as a result of left ventricular dysfunction with segmental wall motion abnormalities; its rapid reversibility with treatment suggests that it may be due to myocardial “stunning.” Long-standing hyperthyroidism may lead to cardiomegaly and a “high-output” heart failure. Flow murmurs are common and extracardiac sounds occur, generated by the hyperdynamic heart.
Hyperthyroidism leads to increased hepatic gluconeogenesis, enhanced carbohydrate absorption, and increased insulin degradation. In nondiabetic patients, after ingestion of carbohydrate, the blood glucose rises rapidly, sometimes causing glycosuria, and then falls rapidly. There may be an adaptive increase in insulin secretion, perhaps explaining the normal glycemic, glycogenolytic, glycolytic, and ketogenic sensitivity to epinephrine. Diabetic patients have an increased insulin requirement in the hyperthyroid state.
Metabolically, the total plasma cholesterol is usually low, related to an increase in the number of hepatic low-density lipoprotein (LDL) receptors. Lipolysis is increased, and adipocytes show an increase in β-adrenergic receptor density and increased responsiveness to catecholamines. With the rise in metabolic rate, there is also an increased need for vitamins; if dietary sources are inadequate, vitamin deficiency syndromes may occur. Normally, thyroid hormone stimulates osteoblastic production of insulin-like growth factor-I (IGF-I), clearly important for the anabolic effects of thyroid hormone on bone. In hyperthyroid patients, levels of serum IGF-I and several binding proteins (IGFBP-3 and IGFBP-4) are significantly increased before treatment and return to normal after antithyroid drug treatment. In addition, because of enhanced osteoblastic and osteoclastic activity, overtly hyperthyroid patients frequently exhibit accelerated bone turnover and negative calcium and phosphorus balance, resulting in low bone mineral density and increased skeletal fragility. Hypercalciuria and sometimes hypercalcemia can occur. Normalization of thyroid function is associated with a significant attenuation of increased bone turnover followed by an increase in bone mineral density.
There is an increase in frequency of bowel movements (hyperdefecation) as a result of increased GI motility. Accelerated small bowel transit may be caused by increased frequency of bowel contractions and of giant migrating contractions. In severe thyrotoxicosis, abnormal liver function tests may be observed, reflecting malnutrition. Anorexia in untreated hyperthyroidism is associated with older age, anxiety, and abnormal liver function but not with hypercalcemia.
In women, hyperthyroidism may lead to oligomenorrhea and decreased fertility. In the follicular phase of the menstrual cycle, there is an increased basal plasma LH and an increased LH and FSH response to GnRH (Chapter 22). There is an increase in sex hormone–binding globulin, leading to increased levels of total estradiol. In men, hyperthyroidism may cause decreased fertility and impotence from altered steroid hormone metabolism. Serum levels of total testosterone, total estradiol, sex hormone–binding globulin, LH, and FSH and gonadotropin response to GnRH are significantly greater than normal. However, the ratio of free testosterone to free estradiol is lower than normal. Mean sperm counts are normal, but the percentage of forward progressive sperm motility is lower than normal (Chapter 23). These hormone and semen abnormalities are reversible with successful treatment of the hyperthyroidism. Gynecomastia may occur despite high normal serum testosterone levels secondary to increased peripheral conversion of androgens to estrogens (Chapter 23).
There is an increased plasma concentration of atrial natriuretic peptide (ANP) and its precursors. The plasma ANP concentration correlates with the serum thyroxine level and heart rate and decreases to normal with successful antithyroid therapy.
The wide-eyed stare of hyperthyroid patients may be due to increased sympathetic tone. In addition, proptosis develops in 25–50% of patients with Graves disease as a result of infiltration of orbital soft tissues and extraocular muscles with lymphocytes, mucopolysaccharides, and edema fluid (Figure 20-7). This may lead to fibrosis of the extraocular muscles, restricted ocular motility, and diplopia. In severe Graves ophthalmopathy, pressure on the optic nerve or keratitis from corneal exposure may lead to blindness. In patients with Graves disease, it is clear that thyroid-stimulating antibody is related to Graves ophthalmopathy. In addition, autoantibodies against G2s, a 55-kDa protein found in both thyroid and eye muscle tissue, are definitely associated with Graves ophthalmopathy. For instance, antibodies reactive with G2s are identified in significantly more patients with active thyroid ophthalmopathy than in patients with Graves disease without ophthalmopathy, those with Hashimoto thyroiditis or nonimmunologic thyroid disorders, and those without thyroid disease. The pathogenesis of Graves ophthalmopathy may involve cytotoxic lymphocytes (killer cells) and cytotoxic antibodies to an antigen common to orbital fibroblasts, orbital muscle, and thyroid tissue (Figure 20-6). It is postulated that cytokines released from these sensitized lymphocytes cause inflammation of orbital tissues, resulting in the proptosis, diplopia, and edema. For unknown reasons, Graves ophthalmopathy is worse in smokers and may be exacerbated by radioiodine therapy.
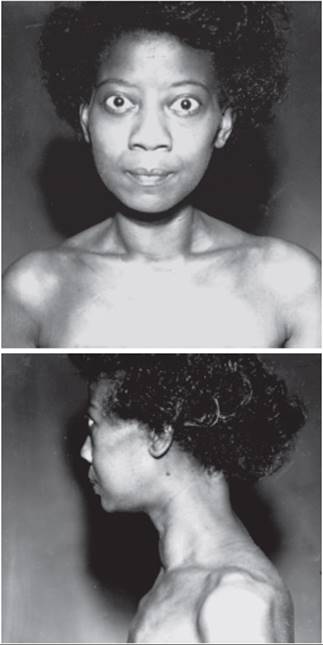
FIGURE 20-7 Graves disease. (Reproduced, with permission, of PH Forsham.)
The skin is warm, sweaty, and velvety in texture. Hyperpigmentation can be seen on the lower extremities, most strikingly on the shins, the backs of the feet, and the nail beds. The hyperpigmentation is due to basal melanosis and heavy deposition of hemosiderin around dermal capillaries and sweat glands. Its distribution, hemosiderin deposition, and poor response to treatment distinguish it from the hyperpigmentation seen with Addison disease. There may be onycholysis (ie, retraction of the nail from the nail plate). In Graves disease, the pretibial skin may become thickened, resembling an orange peel (pretibial myxedema or thyrotoxic dermopathy). The dermopathy is usually a late manifestation of Graves disease, and affected patients invariably have ophthalmopathy. The most common form of the dermopathy is nonpitting edema, but nodular, plaque-like, and even polypoid forms also occur. The pathogenesis of thyroid dermopathy may also involve lymphocyte cytokine stimulation of fibroblasts. Thyroid dermopathy is associated with a very high serum titer of TSH-R [stim] Ab.
Untreated hyperthyroidism may decompensate into a state called thyroid storm. Patients so affected have tachycardia, fever, agitation, nausea, vomiting, diarrhea, and restlessness or psychosis. The condition is usually precipitated by an intercurrent illness or by a surgical emergency.
CHECKPOINT
12. Describe the physiologic consequences of hyperthyroidism and identify their mechanism (as is best known) on the following systems:
Heart
Liver
Lungs
Gl tract
Kidney
Eyes
Skin
Brain
Bone
Reproductive system
HYPOTHYROIDISM
Etiology
The causes of hypothyroidism are listed in Table 20-5. The most common cause is Hashimoto thyroiditis, which results from an autoimmune destruction of the thyroid, although the precipitating cause and exact mechanism of the autoimmunity and subsequent destruction are unknown. Hypothyroidism may also be caused by lymphocytic thyroiditis after a transient period of hyperthyroidism. Thyroid ablation, whether by surgical resection or by therapeutic radiation, commonly results in hypothyroidism.
TABLE 20-5 Hypothyroidism: causes and pathogenetic mechanisms.
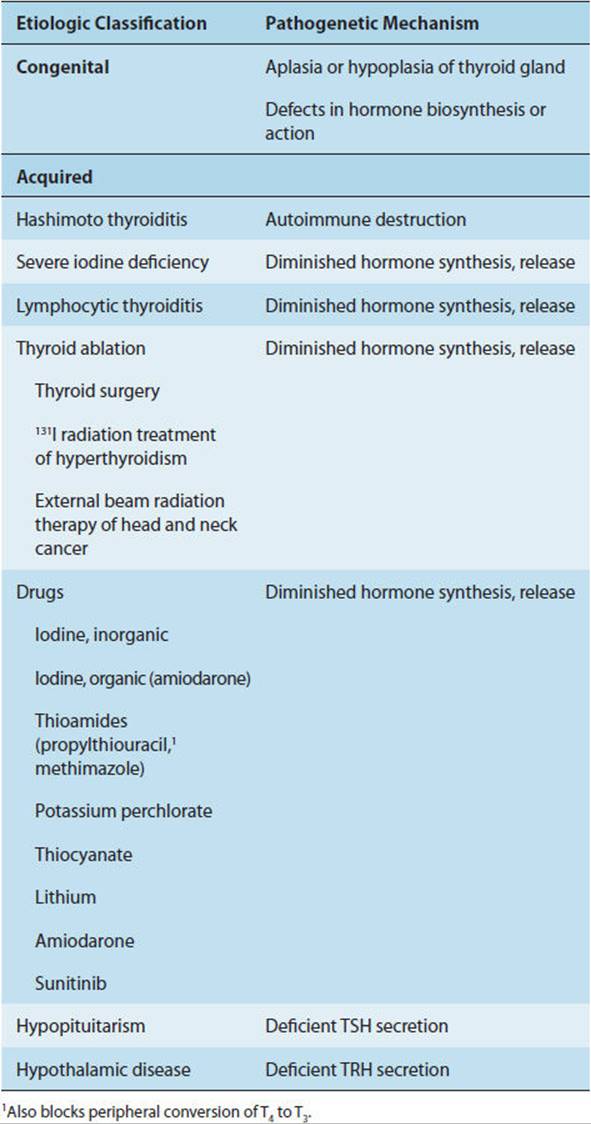
Congenital hypothyroidism, a preventable cause of mental retardation, occurs in approximately 1 in 4000 births; girls are affected about twice as often as boys. Most cases (85%) are sporadic in distribution, but 15% are hereditary. The most common cause of sporadic congenital hypothyroidism is thyroid dysgenesis, in which hypofunctioning ectopic thyroid tissue is more common than thyroid hypoplasia or aplasia. Although the pathogenesis of thyroid dysgenesis is largely unknown, some cases have been described as resulting from mutations in the transcription factors PAX-8 and TTF-2. The most common problems causing hereditary congenital hypothyroidism are inborn errors of thyroxine (T4) synthesis. Mutations have been described in the genes coding for the sodium iodide transporter, thyroid peroxidase (TPO), and thyroglobulin. Other cases of congenital hypothyroidism are caused by loss of function mutations in the TSH receptor. Finally, a transient form of familial congenital hypothyroidism is caused by transplacental passage of a maternal TSH receptor–blocking antibody (TSH-R [block] Ab).
Central hypothyroidism, characterized by insufficient TSH secretion in the presence of low levels of thyroid hormones, is a rare disorder. It is caused by diseases of the pituitary or hypothalamus that result in diminished or abnormal TSH secretion, such as tumors or infiltrative diseases of the hypothalamopituitary area, pituitary atrophy, and inactivating mutations in genes that code for the various proteins involved in regulation of the hypothalamic-pituitary-thyroid axis (Figure 20-5). For example, mutations have been identified in the genes for the TRH receptor, the transcription factors Pit-1 and PROP1, and the TSH β-subunit. Pituitary (“secondary”) hypothyroidism is characterized by a diminished number of functioning thyrotropes in the pituitary gland, accounting for a quantitative impairment of TSH secretion. Hypothalamic (“tertiary”) hypothyroidism is characterized by normal or sometimes even increased TSH concentrations but qualitative abnormalities of the TSH secreted. These abnormalities cause the circulating TSH to lack biologic activity and to exhibit impaired binding to its receptor. This defect can be reversed by administration of TRH. Thus, TRH may regulate not only the secretion of TSH but also the specific molecular and conformational features that enable it to act at its receptor.
Finally, a variety of drugs, including the thioamide antithyroid medications propylthiouracil and methimazole, may produce hypothyroidism. The thioamides inhibit thyroid peroxidase and block the synthesis of thyroid hormone. In addition, propylthiouracil, but not methimazole, blocks the peripheral conversion of T4 to T3. Deiodination of iodine-containing compounds such as amiodarone, releasing large amounts of iodide, may also cause hypothyroidism by blocking iodide organification, an effect known as the Wolff-Chaikoff block. Lithium is concentrated by the thyroid and inhibits the release of hormone from the gland. Most patients treated with lithium compensate by increasing TSH secretion, but some become hypothyroid. Lithium-associated clinical hypothyroidism occurs in about 10% of patients receiving the drug. It occurs more commonly in middle-aged women, particularly during the first 2 years of lithium treatment.
Pathogenesis
Hypothyroidism is characterized by abnormally low serum T4 and T3 levels. Free thyroxine levels are always depressed. The serum TSH level is elevated in hypothyroidism (except in cases of pituitary or hypothalamic disease). TSH is the most sensitive test for early hypothyroidism, and marked elevations of serum TSH (>20 mU/L) are found in frank hypothyroidism. Modest TSH elevations (5–20 mU/L) may be found in euthyroid individuals with normal serum T4 and T3 levels and indicate impaired thyroid reserve and incipient hypothyroidism (see Subclinical Thyroid Dysfunction below). In patients with primary hypothyroidism (end-organ failure), the nocturnal TSH surge is intact. In patients with central (pituitary or hypothalamic) hypothyroidism, the serum TSH level is low and the normal nocturnal TSH surge is absent.
In hypothyroidism resulting from thyroid gland failure, administration of TRH produces a prompt rise in the TSH level, the magnitude of which is proportionate to the baseline serum TSH level. The hypernormal response is caused by absence of feedback inhibition by T4 and T3. However, the TRH test is not usually performed in patients with primary hypothyroidism because the elevated basal serum TSH level suffices to make the diagnosis. The test may be useful in the clinically hypothyroid patient with an unexpectedly low serum TSH level in establishing a central (pituitary or hypothalamic) origin. Pituitary disease is suggested by the failure of TSH to rise after TRH administration; hypothalamic disease is suggested by a delayed TSH response (at 60–120 minutes rather than 15–30 minutes) with a normal increment.
Hashimoto Thyroiditis
A. Pathology
In the early stages of Hashimoto thyroiditis, the gland is diffusely enlarged, firm, rubbery, and nodular. As the disease progresses, the gland becomes smaller. In the late stages, the gland is atrophic and fibrotic, weighing as little as 10–20 g. Microscopically, there is destruction of thyroid follicles and lymphocytic infiltration with lymphoid follicles. The surviving thyroid follicular epithelial cells are large, with abundant pink cytoplasm (Hürthle cells). As the disease progresses, there is an increasing amount of fibrosis.
B. Pathogenesis
The pathogenesis of Hashimoto thyroiditis is unclear. Again, it is possible that a defect in suppressor T lymphocytes allows helper T lymphocytes to interact with specific antigens on the thyroid follicular cell membrane. Once these lymphocytes become sensitized to thyroidal antigens, autoantibodies are formed that react with these antigens. Cytokine release and inflammation then cause glandular destruction. The most important thyroid autoantibodies in Hashimoto thyroiditis are thyroglobulin antibody (Tg Ab), thyroidal peroxidase antibody (TPO Ab) (formerly termed antimicrosomal antibody), and the TSH receptor–blocking antibody (TSH-R [block] Ab). During the early phases, Tg Ab is markedly elevated and TPO Ab only slightly elevated. Later, Tg Ab may disappear, but TPO Ab persists for many years. TSH-R [block] Ab is found in patients with atrophic thyroiditis and myxedema and in mothers who give birth to infants with no detectable thyroid tissue (athyreotic cretins). Serum levels of these antibodies do not correlate with the severity of the hypothyroidism, but their presence is helpful in diagnosis. In general, high antibody titers are diagnostic of Hashimoto thyroiditis; moderate titers are seen in Graves disease, multinodular goiter, and thyroid neoplasm; and low titers are found in the elderly.
Patients with Hashimoto thyroiditis have an increased frequency of the HLA-DR5 histocompatibility antigen, and the disease is associated with a host of other autoimmune diseases (Table 20-3). A polyglandular failure syndromehas been defined in which two or more endocrine disorders mediated by autoimmune mechanisms occur (Chapter 17). Affected patients frequently have circulating organ- and cell-specific autoantibodies that lead to organ hypofunction.
CHECKPOINT
13. What are some drugs that cause hypothyroidism?
14. What are the most useful initial tests of thyroid function in hypothyroidism? What results would you expect compared with normal?
15. What are the key pathophysiologic findings in Hashimoto thyroiditis?
Clinical Manifestations
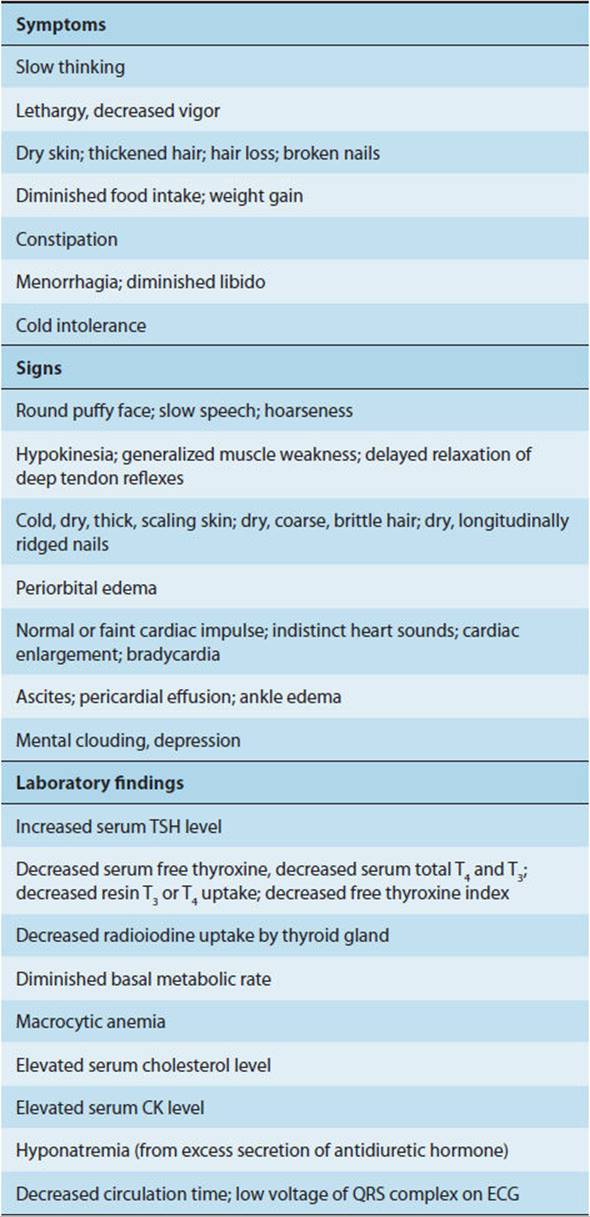
The clinical consequences of thyroid hormone deficiency in the adult are summarized in Table 20-6.
TABLE 20-6 Clinical findings in adult hypothyroidism (myxedema).
Hypothermia is common, and the patient may complain of cold intolerance. The decreased basal metabolic rate leads to weight gain despite reduced food intake.
Thyroid hormones are required for normal development of the nervous system. In hypothyroid infants, synapses develop abnormally, myelination is defective, and mental retardation occurs. Hypothyroid adults have several reversible neurologic abnormalities, including slowed mentation, forgetfulness, decreased hearing, and ataxia. Some patients have severe mental symptoms, including reversible dementia or overt psychosis (“myxedema madness”). The cerebrospinal fluid protein level is abnormally high. However, total cerebral blood flow and oxygen consumption are normal. Deep tendon reflexes are sluggish, with a slowed (“hung-up”) relaxation phase. Paresthesias are common, often caused by compression neuropathies resulting from accumulation of myxedema (carpal tunnel syndrome and tarsal tunnel syndrome).
Hypothyroidism is associated with muscle weakness, cramps, and stiffness. The serum creatine kinase (CK) level may be elevated. The pathophysiology of the muscle disease in hypothyroidism is poorly understood. Study of the bioenergetic abnormalities in hypothyroid muscle suggests a hormone-dependent, reversible mitochondrial impairment. Changes in energy metabolism are not found in hyperthyroid muscle.
Patients rendered acutely hypothyroid by total thyroidectomy exhibit a decreased cardiac output, decreased stroke volume, decreased diastolic volume at rest, and increased peripheral resistance. However, the pulmonary capillary wedge pressure, right atrial pressure, heart rate, left ventricular ejection fraction, and left ventricular systolic pressure-volume relation (a measure of contractility) are not significantly different from the euthyroid state. Thus, in early hypothyroidism, alterations in cardiac performance are probably primarily related to changes in loading conditions and exercise-related heart rate rather than to changes in myocardial contractility.
In chronic hypothyroidism, echocardiography shows bradycardia and features that suggest cardiomyopathy, including increased thickening of the intraventricular septum and ventricular wall, decreased regional wall motion, and decreased systolic and diastolic global left ventricular function. These changes may be due to deposition of excessive mucopolysaccharides in the interstitium between myocardial fibers, leading to fiber degeneration, decreased contractility, low cardiac output, cardiac enlargement, and heart failure. Pericardial effusion (with high protein content) may lead to findings of decreased electrocardiographic voltage and flattened T waves, but cardiac tamponade is rare.
Hypothyroid patients exhibit decreased ventilatory responses to hypercapnia and hypoxia. There is a high incidence of sleep apnea in untreated hypothyroidism; such patients sometimes demonstrate myopathy of upper airway muscles. Weakness of the diaphragm also occurs frequently and, when severe, can cause chronic alveolar hypoventilation (CO2 retention). Pleural effusions (with high protein content) may occur.
In hypothyroidism, the plasma cholesterol and triglyceride levels increase, related to decreased lipoprotein lipase activity and decreased formation of hepatic LDL receptors. In hypothyroid children, bone growth is slowed and skeletal maturation (closure of epiphyses) is delayed. Pituitary secretion of growth hormone may also be depressed because thyroid hormone is needed for its synthesis. Hypothyroid animals demonstrate decreased width of epiphysial growth plate and articular cartilage and decreased volume of epiphyseal and metaphyseal trabecular bone. These changes are not solely due to lack of pituitary growth hormone, because administering exogenous growth hormone does not restore normal cartilage morphology or bone remodeling, whereas administering T4 does. If unrecognized, prolonged juvenile hypothyroidism results in a permanent height deficit.
A normochromic, normocytic anemia may occur as a result of decreased erythropoiesis. Alternatively, a moderate macrocytic anemia can occur as a result of decreased absorption of cyanocobalamin (vitamin B12) from the intestine and diminished bone marrow metabolism. Frank megaloblastic anemia suggests coexistent pernicious anemia.
Constipation is common and reflects decreased GI motility. Achlorhydria occurs when hypothyroidism is associated with pernicious anemia. Ascitic fluid with high protein content may accumulate.
The skin in hypothyroidism is dry and cool. Normally, the skin contains a variety of proteins complexed with polysaccharides, chondroitin sulfuric acid, and hyaluronic acid. In hypothyroidism, these complexes accumulate, promoting sodium and water retention and producing a characteristic diffuse, nonpitting puffiness of the skin (myxedema). The patient’s face appears puffy, with coarse features (Figure 20-8). Similar accumulation of mucopolysaccharides in the larynx may lead to hoarseness. The hair is brittle and lacking in luster, and there is frequently loss of body hair, particularly over the scalp and lateral eyebrows. If thyroid hormone is administered, the protein complexes are mobilized, a diuresis ensues, and myxedema resolves.
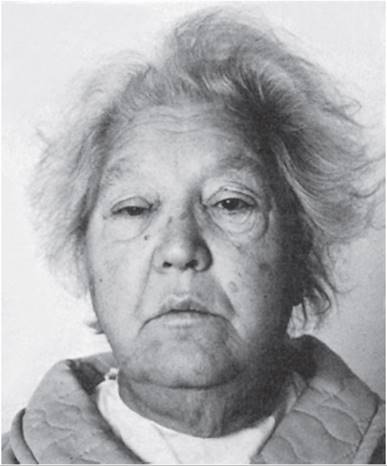
FIGURE 20-8 Myxedema. (Reproduced, with permission, from Greenspan FS et al, eds. Basic and Clinical Endocrinology, 7th ed. McGraw-Hill, 2004.)
Carotenemia (manifested as yellow-orange discoloration of the skin) may occur in hypothyroidism because thyroid hormones are needed for hepatic conversion of carotene to vitamin A. In the absence of sufficient hormone, carotene accumulates in the bloodstream and skin.
In women, hypothyroidism may lead to menorrhagia from anovulatory cycles. Alternatively, menses may become scanty or disappear secondary to diminished secretion of gonadotropins. Because thyroid hormone normally has an inhibitory effect on prolactin secretion, hypothyroid patients may exhibit hyperprolactinemia, with galactorrhea and amenorrhea. In men, hypothyroidism can cause infertility and gynecomastia from enhanced release of prolactin. Hyperprolactinemia occurs because TRH stimulates prolactin release.
There is reduced renal blood flow and a decreased glomerular filtration rate. The vasoconstriction may be due to decreased concentrations of plasma ANP. The consequent reduced ability to excrete a water load may cause hyponatremia. However, the serum creatinine level is usually normal.
Long-standing severe untreated hypothyroidism may lead to a state called myxedema coma. Affected patients have typical myxedematous facies and skin, bradycardia, hypothermia, alveolar hypoventilation, and severe obtundation or coma. This condition is usually precipitated by an intercurrent illness such as an infection or stroke or by a medication such as a sedative-hypnotic. The mortality rate approaches 100% unless myxedema coma is recognized and treated promptly.
CHECKPOINT
16. Describe and explain the physiologic consequence of hypothyroidism (as is best known) on the following:
Nervous system
Muscle
Cardiovascular system
Lungs
Liver
Blood
Gl tract
Skin
Reproductive system
Kidney
GOITER
Etiology
Diffuse thyroid enlargement most commonly results from prolonged stimulation by TSH (or a TSH-like agent). Such stimulation may be the result of one of the causes of hypothyroidism (eg, TSH in Hashimoto thyroiditis) or of hyperthyroidism (eg, TSH-R [stim] Ab in Graves disease, hCG in germ cell tumors, or TSH in pituitary adenoma). Alternatively, goiter may occur in a clinically euthyroid patient. Table 20-7 lists the causes and pathogenetic mechanisms.
TABLE 20-7 Goiter: causes and pathogenetic mechanisms.
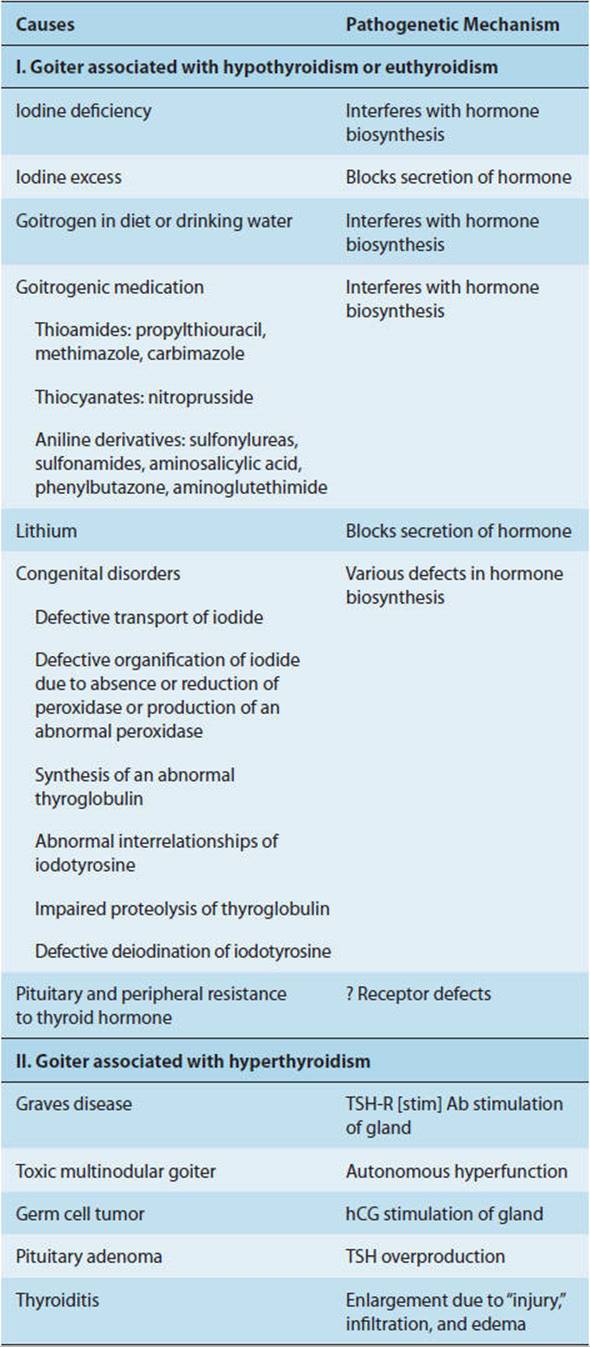
Iodine deficiency is the most common cause of goiter in developing nations. A diet that contains less than 10 μg/d of iodine hinders the synthesis of thyroid hormone, resulting in an elevated TSH level and thyroid hypertrophy. Iodination of salt has eliminated this problem in much of the developed world.
A goiter may also develop from ingestion of goitrogens (factors that block thyroid hormone synthesis) either in food or in medication. Dietary goitrogens are found in vegetables of the Brassicaceae family (eg, rutabagas, cabbage, turnips, cassava). A goitrogenic hydrocarbon has been found in the water supply in some locations. Medications that act as goitrogens include thioamides and thiocyanates (eg, propylthiouracil, methimazole, and nitroprusside), sulfonylureas, and lithium. Lithium inhibits thyroid hormone release and perhaps also iodide organification. Most patients remain clinically euthyroid because TSH production increases.
A congenital goiter associated with hypothyroidism (sporadic cretinism) may occur as a result of a defect in any of the steps of thyroid hormone synthesis (Table 20-5). All of these defects are rare.
Goiter with hyperthyroidism is usually due to Graves disease. In Graves disease, the gland is diffusely enlarged because of stimulation by TSH-R [stim] Ab and other antibodies rather than by TSH.
Pathogenesis & Pathology
In goiter resulting from impaired thyroid hormone synthesis, there is a progressive fall in serum T4 and a progressive rise in serum TSH. As the TSH increases, iodine turnover by the gland is accelerated and the ratio of T3 secretion relative to T4 secretion is increased. Consequently, the serum T3 may be normal or increased, and the patient may remain clinically euthyroid. If there is more marked impairment of hormone synthesis, goiter formation is associated with a low T4, low T3, and elevated TSH, and the patient becomes clinically hypothyroid.
In the early stages of goiter, there is diffuse enlargement of the gland, with cellular hyperplasia caused by the TSH stimulation. Later, there are enlarged follicles with flattened follicular epithelial cells and accumulation of thyroglobulin. This accumulation occurs particularly in iodine deficiency goiter, perhaps because poorly iodinated thyroglobulin is less easily digested by proteases. As TSH stimulation continues, multiple nodules may develop in some areas and atrophy and fibrosis in others, producing a multinodular goiter (Figure 20-9).
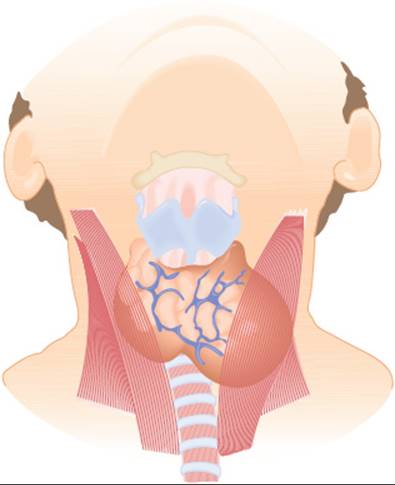
FIGURE 20-9 Multinodular goiter. (Redrawn, with permission, from Gardner DG et al, eds. Greenspan’s Basic and Clinical Endocrinology, 9th ed. McGraw-Hill, 2011.)
In patients with severe iodine deficiency or inherited metabolic defects, a nontoxic goiter develops because impaired hormone secretion leads to an increase in TSH secretion. The elevation in serum TSH level results in diffuse thyroid hyperplasia. If TSH stimulation is prolonged, the diffuse hyperplasia is followed by focal hyperplasia with necrosis, hemorrhage, and formation of nodules. These nodules often vary from “hot” nodules that can trap iodine and synthesize thyroglobulin to “cold” ones that cannot. In early goiters, the hyperplasia is TSH dependent, but in later stages the nodules become TSH-independent autonomous nodules. Thus, over a period of time there may be a transition from a nontoxic, TSH-dependent, diffuse hyperplasia to a toxic or nontoxic, TSH-independent, multinodular goiter.
The exact mechanism underlying this transition to autonomous growth and function is unknown. However, mutations of the gsp oncogene have been found in nodules from many patients with multinodular goiter. Such mutations presumably occur during TSH-induced cell division. The gsp oncogene is responsible for activation of regulatory GTP-binding (Gs) protein in the follicular cell membrane. Chronic activation of this protein and its effector, adenylyl cyclase, is postulated to result in thyroid cell proliferation, hyperfunction, and independence from TSH.
Clinical Manifestations
With decades of TSH stimulation, enormous hypertrophy and enlargement of the gland can occur. The enlarged gland may weigh 1–5 kg and may produce respiratory difficulties secondary to obstruction of the trachea or dysphagia secondary to obstruction of the esophagus. More modest enlargements pose cosmetic problems.
Some patients with multinodular goiter also develop hyperthyroidism late in life (Plummer disease), particularly after administration of iodide or iodine-containing drugs.
THYROID NODULES & NEOPLASMS
Tumors of the thyroid usually present as a solitary mass in the neck. The most common neoplasm, accounting for 30% of all solitary thyroid nodules, is the follicular adenoma. It is a solitary, firm, gray or red nodule, up to 5 cm in diameter, completely surrounded by a fibrous capsule. The surrounding normal thyroid tissue is compressed by the adenoma. Microscopically, the adenoma consists of normal-appearing follicles of varying size, sometimes associated with hemorrhage, fibrosis, calcification, and cystic degeneration. Occasionally, only ribbons of follicular cells are present, without true follicles. Malignant change probably occurs in less than 10% of follicular adenomas.
Thyroid cancers are not common. Most are derived from the follicular epithelium and, depending on their microscopic appearance, are classified as papillary or follicular carcinoma. The major risk factor predisposing to epithelial thyroid carcinoma is exposure to radiation, but genetic factors have also been recognized. Most papillary and follicular cancers pursue a prolonged clinical course (15–20 years). Papillary carcinoma typically metastasizes to regional lymph nodes in the neck, whereas follicular cancer tends to spread via the bloodstream to distant sites such as bone or lung. Medullary carcinoma is an uncommon neoplasm of the C cells (parafollicular cells) of the thyroid that produce calcitonin (see Chapter 17). Approximately 30% of all medullary thyroid carcinomas are a manifestation of multiple endocrine neoplasia type 2 (MEN-2), inherited in an autosomal dominant fashion.
ABNORMAL THYROID FUNCTION TESTS IN CLINICALLY EUTHYROID INDIVIDUALS
Increases & Decreases in Hormone-Binding Proteins
Sustained increases or decreases in the concentration of TBG and other thyroid-binding proteins in the plasma are produced by several normal and disordered physiologic states and by medications. These are summarized in Table 20-8. For example, TBG levels are elevated during pregnancy and by estrogen and oral contraceptive therapy. TBG levels are depressed in the nephrotic syndrome and by glucocorticoid or androgen therapy.
TABLE 20-8 Effects of normal and disordered physiologic states and medications on plasma thyroid-binding proteins and thyroid hormone levels.
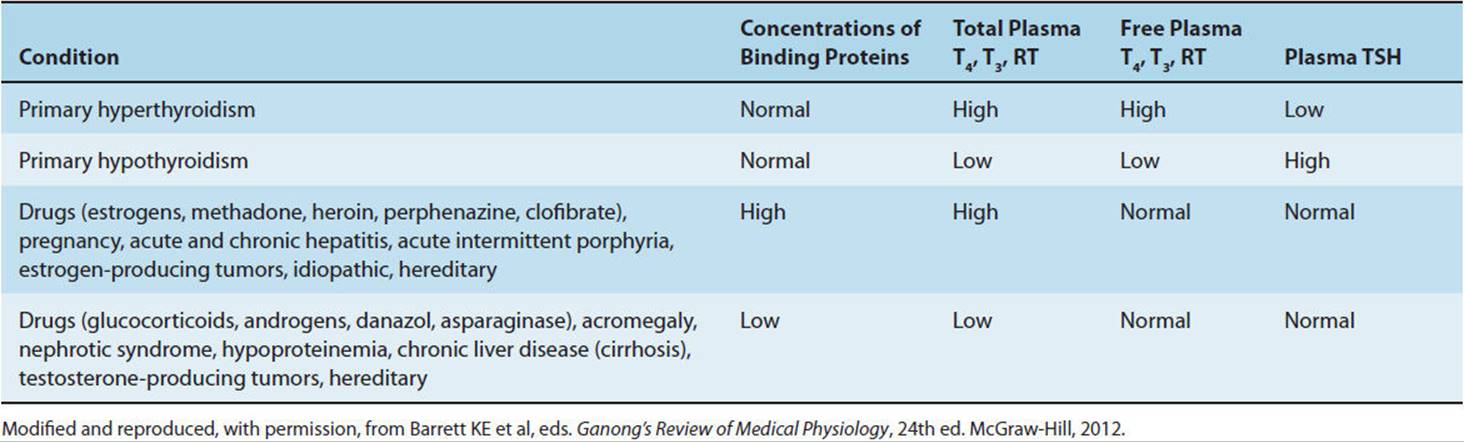
When a sustained increase in the concentration of TBG and other binding proteins occurs, the concentration of free thyroid hormones falls temporarily. This fall stimulates TSH secretion, which then results in an increase in the production of free hormone. Eventually, a new equilibrium is reached in which the levels of total plasma T4 and T3 are elevated, but the concentrations of free hormones, the rate of hormone degradation, and the rate of TSH secretion are normal. Therefore, individuals manifesting sustained increases in TBG and other binding proteins remain euthyroid. When a sustained decrease in the concentration of TBG and other binding proteins occurs, equivalent changes occur in the opposite direction, and again the individuals remain euthyroid.
Abnormal Hormone-Binding Proteins
Changes in serum concentrations of the hormone-binding proteins transthyretin or albumin alone usually do not cause significant changes in thyroid hormone levels. However, several unusual syndromes of familial euthyroid hyperthyroxinemia have been described. In the first, a familial syndrome called euthyroid dysalbuminemic hyperthyroxinemia, there is abnormal binding of T4 (but not T3) to albumin. In the second, there is an increased serum level of transthyretin. In the third, there are alterations in transthyretin, a tetrameric protein that transports 15–20% of circulating T4. The alterations in transthyretin structure produced by different point mutations can markedly increase its affinity for T4. In some families, these mutations in transthyretin are transmitted by autosomal dominant inheritance. In all three of these syndromes, total T4 is elevated, but free T4 is normal and the patients are euthyroid. A fourth syndrome has also been described in which there is both pituitary and peripheral resistance to thyroid hormone. As noted, this condition may be due to point mutations in the human thyroid receptor (hTR-β1) gene, resulting in abnormal nuclear T3 receptors.
Effects of Nonthyroidal Illness & Drugs
Several nonthyroidal illnesses and various drugs inhibit the 5′-deiodinase that converts T4 to T3, resulting in a fall in plasma T3. Illnesses that depress 5′-deiodinase include severe burns or trauma, surgery, advanced cancer, cirrhosis, renal failure, myocardial infarction, prolonged fever, caloric deprivation (fasting, anorexia nervosa, malnutrition), and selenium deficiency. The decreased serum T3 in nonthyroidal illnesses is thought to be an adaptive physiologic change, enabling the sick patient to conserve energy and protein. Drugs that depress 5′-deiodinase include glucocorticoids, propranolol, amiodarone, propylthiouracil, and cholecystography dyes (eg, ipodate, iopanoic acid).
Because T3 is the major active thyroid hormone at the tissue level, it is surprising that patients with mild-to-moderate nonthyroidal illness exhibit normal TSH levels despite low T3 levels and do not appear hypothyroid. However, such patients retain the ability to respond to a further reduction (or to an increase) in serum T3 by increasing (or decreasing) pituitary TSH secretion. Patients with severe illnesses (eg, those undergoing bone marrow transplantation for leukemia) may manifest impaired TSH secretion.
Most patients with nonthyroidal illnesses have low serum T3 levels related to the decreased peripheral conversion of T4 to T3. However, in some patients, the primary cause of the low serum T3 is reduced secretion of T4 by the gland. In others, the binding of T4 and T3 by serum thyroid-binding proteins is impaired because of the decreased concentrations of thyroid-binding proteins (Table 20-8) and the presence of circulating inhibitors of binding.
The low T3 state generally disappears with recovery from the illness or cessation of the drug. Among critically ill patients with low T3 levels, clinical trials have not demonstrated benefit from T3 replacement. Because low T3 levels are difficult to interpret during acute illness, the diagnostic approach should be based primarily on serum TSH levels.
Subclinical Thyroid Dysfunction
With the development of more sensitive laboratory tests of thyroid function, it is increasingly recognized that some clinically euthyroid individuals have subclinical thyroid dysfunction, defined by low or high TSH levels but normal circulating T4 and T3 levels. Many individuals with subclinical thyroid disease have abnormal TRH stimulation tests, but the clinical significance of these biochemical abnormalities continues to be debated. Subclinical hypothyroidism is defined as an elevated TSH (>4.5 mU/L) but normal circulating thyroid hormone levels. Subclinical hypothyroidism is more common among women and among the individuals older than 65 years where the prevalence is as high as 10–12%. Importantly, the typical symptoms and signs of overt hypothyroidism, including weight gain, fatigue, and cold intolerance, are not consistently associated with subclinical dysfunction. The underlining causes of subclinical hypothyroidism are similar to those associated with overt hypothyroidism, particularly Hashimoto thyroiditis, but a substantial proportion have no obvious etiology. In the presence of circulating thyroid (anti-TPO) autoantibodies, approximately 5% of individuals with subclinical hypothyroidism progress to overt hypothyroidism each year, compared with 2% per year or less among those without thyroid autoantibodies.
Pooled analyses of individual level data from multiple prospective studies suggest that subclinical hypothyroidism is associated with an increased risk of atherosclerotic heart disease and heart failure, particularly when the TSH levels are greater than 10 mU/L. Other studies suggest the risk of cardiovascular complications may be limited to younger individuals (those younger than 55 years). Some, but not all, studies suggest subtle neurocognitive abnormalities, particularly related to executive functions.
Unfortunately, there are no large randomized trials of treatment of subclinical hypothyroidism with clinical endpoints such as heart disease or heart failure. Some individuals report improved exercise tolerance and an improved sense of well-being when given sufficient thyroxine to normalize serum TSH, but there is insufficient evidence to recommend routine treatment of individuals with persistent subclinical hypothyroidism that does not progress to overt hypothyroidism. A large multicenter placebo-controlled trial in Europe (TRUST) has been designed to address this issue, but results are not expected for several years.
Subclinical hyperthyroidism is defined as a low TSH (<0.5 mU/L) but normal circulating thyroid hormone levels. Autonomous thyroid nodules or early Graves disease is believed to account for the majority of cases. The prevalence of subclinical hyperthyroidism is considerably lower than that for subclinical hypothyroidism at 1–3% and also increases with age. The classic symptoms and signs of hyperthyroidism are typically absent among individuals with subclinical hyperthyroidism. The natural history of subclinical hyperthyroidism is not well known, but one study of postmenopausal women with endogenous subclinical hyperthyroidism found that more than 50% had normal TSH levels after 1 year of follow-up.
Prospective studies have demonstrated subtle abnormalities of cardiac contractility in individuals with subclinical hyperthyroidism, and one prospective study found that individuals older than 65 years with TSH of less than 0.1 mU/L had a threefold greater risk of developing atrial fibrillation than those with normal TSH levels. Subclinical hyperthyroidism may also be associated with bone loss and fracture in postmenopausal women. In a prospective study of women older than 65 years, the risks of hip and spine fracture were two to three times higher among those with TSH of less than 0.1 mU/L (mostly from over-replacement with thyroid hormone) compared with those with normal TSH levels.
CHECKPOINT
17. What is a goiter?
18. What are the causes and mechanisms of goiter formation?
19. What is the basis for transition from nontoxic, TSH-dependent diffuse hyperplasia to a toxic or nontoxic TSH-independent multinodular goiter?
20. How large can the thyroid gland become with decades of stimulation?
21. What are the different types of thyroid cancer and their characteristics?
22. What are some physiologic and pathophysiologic conditions in which thyroid metabolism is altered? How and with what effects?
23. What is the overall thyroid status of a patient with a sustained decrease in thyroid-binding globulin?
24. What are some of the factors which depress 5′-deiodinase activity?
25. How does nonthyroidal illness typically affect thyroid hormone levels?
CASE STUDIES
Yeong Kwok, MD
(See Chapter 25, p. 734 for Answers)
CASE 99
A 25-year-old African American woman presents with a complaint of rapid weight loss despite a voracious appetite. Physical examination reveals tachycardia (pulse rate 110 bpm at rest), fine moist skin, symmetrically enlarged thyroid, mild bilateral quadriceps muscle weakness, and fine tremor. These findings strongly suggest hyperthyroidism.
Questions
A. What other features of the history should be elicited?
B. What other physical findings should be sought?
C. Serum TSH and free thyroxine level are ordered. What results should be anticipated?
D. What are the possible causes of this patient’s condition?
E. What is the most common cause of this patient’s condition, and what is the pathogenesis of this disorder?
F. What is the pathogenesis of this patient’s tachycardia, weight loss, skin changes, goiter, and muscle weakness?
CASE 100
A 45-year-old woman presents complaining of fatigue, 30 pounds of weight gain despite dieting, constipation, and menorrhagia. On physical examination, the thyroid is not palpable; the skin is cool, dry, and rough; the heart sounds are quiet; and the pulse rate is 50 bpm. The rectal and pelvic examinations show no abnormalities, and the stool is negative for occult blood. The clinical findings suggest hypothyroidism.
Questions
A. What other features of the history should be elicited? What other findings should be sought on physical examination?
B. What is the pathogenesis of this patient’s symptoms?
C. What laboratory tests should be ordered, and what results should be anticipated?
D. What are the possible causes of this patient’s condition? Which is most likely?
E. What other conditions may be associated with this disorder?
CASE 101
A 40-year-old woman who has recently emigrated from Afghanistan comes to a practice office to establish medical care. She complains only of mild fatigue and depression. Physical examination reveals a prominent, symmetrically enlarged thyroid about twice normal size. The remainder of the examination is unremarkable.
Questions
A. What other features of the history should be elicited?
B. What is the most likely cause of the patient’s thyroid enlargement? What is the pathogenetic mechanism of goiter formation in this disease?
C. What laboratory tests should be ordered and why?
CASE 102
A 47-year-old man presents complaining of nervousness, difficulty concentrating, restlessness, and insomnia. He has lost 25 pounds over the past 6 weeks and complains of heat intolerance. Physical examination reveals a 1-cm nodule in the left lobe of the thyroid gland.
Questions
A. What is the most likely explanation for the patient’s condition?
B. What laboratory tests should be ordered to confirm the diagnosis? What would you expect the results to be?
C. What further evaluation of the nodule could be undertaken?
D. If a biopsy is done, what can be expected in the pathologist’s report?
CASE 103
A 28-year-old woman returns for follow-up after routine laboratory tests show a markedly elevated total T4 level. The patient is totally asymptomatic, and the physical examination is unremarkable.
Questions
A. What conditions and medications could be responsible for this presentation?
B. What further laboratory tests should be ordered?
C. If the patient is pregnant, how can the elevated total plasma T4 level be explained?
D. If several asymptomatic family members have been told of similar laboratory test results, what is the most likely explanation of the patient’s disorder?
REFERENCES
General
Bianco AC. Minireview: cracking the metabolic code for thyroid hormone signaling. Endocrinology. 2011 Sep;152(9):3306–11. [PMID: 21712363]
Chiamolera MI et al. Minireview: thyrotropin-releasing hormone and the thyroid hormone feedback mechanism. Endocrinology. 2009 Mar;150(3):1091–6. [PMID: 19179434]
Cooper DS et al. The thyroid gland. Chapter 7. In: Gardner DG et al, eds. Greenspan’s Basic and Clinical Endocrinology, 9th ed. McGraw-Hill, 2011.
Danzi S et al. Thyroid hormone and the cardiovascular system. Med Clin North Am. 2012 Mar;96(2):257–68. [PMID: 22443974]
Heuer H et al. Minireview: pathophysiological importance of thyroid hormone transporters. Endocrinology. 2009 Mar;150(3):1078–83. [PMID: 19179441]
St Germain DL et al. Minireview: defining the roles of the iodothyronine deiodinases: current concepts and challenges. Endocrinology. 2009 Mar;150(3):1097–107. [PMID: 19179439]
Hyperthyroidism
Bahn RS. Autoimmunity and Graves’ disease. Clin Pharmacol Ther. 2012 Apr;91(4):577–9. [PMID: 22434030]
Bahn RS. Graves’ ophthalmopathy. N Engl J Med. 2010 Feb 25;362(8): 726–38. [PMID: 20181974]
Bartalena L et al. Clinical practice. Graves ophthalmopathy. N Engl J Med. 2009 Mar 5;360(10):994–1001. [PMID: 19264688]
Cooper DS et al. Subclinical thyroid disease. Lancet. 2012 Mar 24;379(9821):1142–54. [PMID: 22273398]
Franklyn JA et al. Thyrotoxicosis. Lancet. 2012 Mar 24;379(9821): 1155–66. [PMID: 22394559]
Klubo-Gwiezdzinska J et al. Thyroid emergencies. Med Clin North Am. 2012 Mar;96(2):385–403. [PMID: 22443982]
Seigel SC et al. Thyrotoxicosis. Med Clin North Am. 2012 Mar;96(2): 175–201. [PMID: 22443970]
Stan MN et al. The evaluation and treatment of Graves ophthalmopathy. Med Clin North Am. 2012 Mar;96(2):311–28. [PMID: 22443978]
Stiebel-Kalish H et al. Treatment modalities for Graves’ ophthalmopathy: systematic review and metaanalysis. J Clin Endocrinol Metab. 2009 Aug;94(8):2708–16. [PMID: 19491222]
Wiersinga WM. Autoimmunity in Graves’ ophthalmopathy: the result of an unfortunate marriage between TSH receptors and IGF-1 receptors? J Clin Endocrinol Metab. 2011 Aug;96(8):2386–94. [PMID: 21677036]
Hypothyroidism
GyamfiC et al. Thyroid dysfunction in pregnancy: the basic science and clinical evidence surrounding the controversy in management. Obstet Gynecol. 2009 Mar;113(3):702–7. [PMID: 19300337]
Hennessey JV. Clinical review: Riedel’s thyroiditis: a clinical review. J Clin Endocrinol Metab. 2011 Oct;96(10):3031–41. [PMID: 21832114]
Michels AW et al. Immunologic endocrine disorders. J Allergy Clin Immunol. 2010 Feb;125(2 Suppl 2):S226–37. [PMID: 20176260]
Parle J et al. A randomized controlled trial of the effect of thyroxine replacement on cognitive function in community-living elderly subjects with subclinical hypothyroidism: the Birmingham Elderly Thyroid study. J Clin Endocrinol Metab. 2010 Aug;95(8):3623–32. [PMID: 20501682]
Pearce EN. Update in lipid alterations in subclinical hypothyroidism. J Clin Endocrinol Metab. 2012 Feb;97(2):326–33. [PMID: 22205712]
Goiter
Bahn RS et al. Approach to the patient with nontoxic multinodular goiter. J Clin Endocrinol Metab. 2011 May;96(5):1202–12. [PMID: 21543434]
Medeiros-Neto G et al. Approach to and treatment of goiters. Med Clin North Am. 2012 Mar;96(2):351–68. [PMID: 22443980]
Thyroid Nodules & Neoplasms
Miller MC. The patient with a thyroid nodule. Med Clin North Am. 2010 Sep;94(5):1003–15. [PMID: 20736109]
Pacini F et al. Approach to and treatment of differentiated thyroid carcinoma. Med Clin North Am. 2012 Mar;96(2):369–83. [PMID: 22443981]
Papaleontiou M et al. Approach to and treatment of thyroid disorders in the elderly. Med Clin North Am. 2012 Mar;96(2):297–310. [PMID: 22443977]
Abnormal Thyroid Function Tests in Clinically Euthyroid Individuals, Subclinical Hypothyroidism, & Subclinical Hyperthyroidism
Biondi B. How could we improve the increased cardiovascular mortality in patients with overt and subclinical hyperthyroidism? Eur J Endocrinol. 2012 Sep;167(3):295–9. [PMID: 22802423]
Biondi B. Natural history, diagnosis and management of subclinical thyroid dysfunction. Best Pract Res Clin Endocrinol Metab. 2012 Aug;26(4):431–46. [PMID: 22863386]
Carpi A et al. Subclinical hyperthyroidism and cardiovascular manifestations: a reevaluation of the association. Intern Emerg Med. 2013 Apr;8(Suppl 1):S75–7 [PMID: 23462890]
Collet TH et al; Thyroid Studies Collaboration. Subclinical hyperthyroidism and the risk of coronary heart disease and mortality. Arch Intern Med. 2012 May 28;172(10):799–809. [PMID: 22529182]
Cooper DS et al. Subclinical thyroid disease. Lancet. 2012 Mar 24;379(9821):1142–54. [PMID: 22273398]
Donangelo I et al. Update on subclinical hyperthyroidism. Am Fam Physician. 2011 Apr 15;83(8):933–8. [PMID: 21524033]
Fatourechi V. Subclinical hypothyroidism: an update for primary care physicians. Mayo Clin Proc. 2009;84(1):65–71. [PMID: 19121255]
Ferrara AM. Homozygous thyroid hormone receptor β-gene mutations in resistance to thyroid hormone: three new cases and review of the literature. J Clin Endocrinol Metab. 2012 Apr;97(4):1328–36. [PMID: 22319036]
Goichot B et al. Subclinical hyperthyroidism: considerations in defining the lower limit of the thyrotropin reference interval. Clin Chem. 2009 Mar;55(3):420–4. [PMID: 19147733]
Gyamfi Bannerman C. Basic science and clinical evidence regarding treatment of subclinical hypothyroidism during pregnancy. Clin Obstet Gynecol. 2011 Sep;54(3):488–92. [PMID: 21857179]
Jones DD et al. Subclinical thyroid disease. Am J Med. 2010 Jun;123(6):502–4. [PMID: 20569751]
Monzani A et al. Endocrine disorders in childhood and adolescence. Natural history of subclinical hypothyroidism in children and adolescents and potential effects of replacement therapy: a review. Eur J Endocrinol. 2012 Dec 10;168(1):R1–R11. [PMID: 22989466]
Mooradian AD. Subclinical hypothyroidism in the elderly: to treat or not to treat? Am J Ther. 2011 Nov;18(6):477–86. [PMID: 20634685]
Ngumezi C et al. When does treatment of subclinical hypothyroidism reduce cardiovascular risk? JAAPA. 2012 Feb;25(2):57–8. [PMID: 22416557]
Thvilum M et al. A review of the evidence for and against increased mortality in hypothyroidism. Nat Rev Endocrinol. 2012 Mar 6; 8(7):417–24. [PMID: 22392154]
Weiss IA et al. Subclinical hypothyroidism and cardiovascular risk: recommendations for treatment. Cardiol Rev. 2011 Nov–Dec;19(6):291–9. [PMID: 21983317]
Wiersinga WM. Should we treat mild subclinical/mild hyperthyroidism? Yes. Eur J Intern Med. 2011 Aug;22(4):324–9. [PMID: 21767746]