Goran Augustin1, 2
(1)
Department of Surgery Division of Gastrointestinal Surgery, University Hospital Center Zagreb, Zagreb, Croatia
(2)
School of Medicine University of Zagreb, Zagreb, Croatia
Abstract
In James Dowling Trask’s (1821–1883, one of the founders of the American Gynecologic Society) monograph on rupture of the uterus, 303 cases are recorded from 1700 to 1848; of these, only 38 are classified as ruptures during pregnancy, the others being cases of rupture during labor. On a careful examination of the notes in each of these 38 cases, it appears that the number must be considerably reduced – first, elimination of cases where the evidence that they were really cases of rupture of the uterus and not some other condition, for instance, abdominal extrauterine pregnancy and, second, by removing those cases which were really cases of premature labor, the pregnancy having advanced nearly to term. When this reduction has been made, there remain 14 cases [1]. Lustgarten quoted one case in the British and Foreign Medico-Chirurgical Review, one in the Glasgow Medical Journal in 1861, and 17 cases by Lewers in 1887 [2]. Nevertheless, in 1903, Baisch was able to record 37 instances of nontraumatic uterine rupture which occurred in the first 6 months of pregnancy [3].
16.1 History
In James Dowling Trask’s (1821–1883, one of the founders of the American Gynecologic Society) monograph on rupture of the uterus, 303 cases are recorded from 1700 to 1848; of these, only 38 are classified as ruptures during pregnancy, the others being cases of rupture during labor. On a careful examination of the notes in each of these 38 cases, it appears that the number must be considerably reduced – first, elimination of cases where the evidence that they were really cases of rupture of the uterus and not some other condition, for instance, abdominal extrauterine pregnancy and, second, by removing those cases which were really cases of premature labor, the pregnancy having advanced nearly to term. When this reduction has been made, there remain 14 cases [1]. Lustgarten quoted one case in the British and Foreign Medico-Chirurgical Review, one in the Glasgow Medical Journal in 1861, and 17 cases by Lewers in 1887 [2]. Nevertheless, in 1903, Baisch was able to record 37 instances of nontraumatic uterine rupture which occurred in the first 6 months of pregnancy [3].
16.2 Incidence
16.2.1 Developed/Undeveloped Country
Rupture of the uterus of pregnant women is one of the most serious obstetric complications. In spite of the recent advances in modern obstetric practice, it remains a life-threatening complication of pregnancy and labor especially in the developing world [4]. Table 16.1 shows the incidence rate differences between countries:
Table 16.1
(Spontaneous) uterine rupture incidence rates across the world (in decreasing incidence)
|
Country |
Incidence |
|
Ethiopia [5, 6] |
1/38–1/175 |
|
Pakistan [7] |
1/100 |
|
Nigeria (rural) [8] |
1/112 |
|
Yemen [9] |
1/159 |
|
Ibadan [10] |
1/167 |
|
Guinea [11] |
1/199 |
|
Uganda [12, 13] |
1/93–1/200 |
|
Morocco [14] |
1/222 |
|
Sudan [15] |
1/246 |
|
Nigeria [16] |
1/258 |
|
India [17, 18] |
1/357–714 |
|
Lagos [19] |
1/416 |
|
Kenya [20] |
1/425 |
|
Libya [21] |
1/585 |
|
Iraq (Basra) [22] |
1/801 |
|
Turkey [23] |
1/966 |
|
Saudi Arabia [24] |
1/1,011 |
|
Nepal [25] |
1/1,100 |
|
Australia [26] |
1/1,163 |
|
Zimbabwe [27] |
1/1,285 |
|
Republic of South Africa [28] |
1/1,362 |
|
Trinidad [29] |
1/1,500 |
|
Bahrain [30] |
1/2,213 |
|
Tunis [31] |
1/2,581 |
|
Kuwait [32, 33] |
1/1,851–1/3,333 |
|
Canada [34] |
1/3,333 |
|
Taiwan [35] |
1/3,871 |
|
Ireland [36] |
1/4,348 |
|
Qatar [37] |
1/4,968–1/6,843 |
|
Singapore [38] |
1/6,331 |
|
United States [39] |
1/8,000–1/15,000 |
The problem with true incidence rates especially in Africa is that registration of births occurring at home is incomplete, although it is our impression that the number of patients who deliver at home and only seek medical attention when problems occur is decreasing. Also, a number of maternal deaths occur in the rural areas before hospital admission. More importantly, patients are transferred from peripheral hospitals and clinics, where the numbers of deliveries are unknown. Recent reports suggest that the incidence particularly of a spontaneous rupture may be on the increase in industrialized countries [39]. Widespread antenatal care and hospital deliveries made the maternal and fetal morbidity and mortality rather low.
16.2.2 Decade Dependency
Incidence is decade dependent. Incidence of uterine rupture in the United States between 1967 and 1978 was 1/1,000–1/1,500 deliveries, but spontaneous ruptures accounted for 25 % of the total and only 17 % of these occurred before the onset of labor [40]. After two decades, the incidences of spontaneous rupture of the unscarred uterus ranged from 1/8,000 to 1/15,000 deliveries [41]. The incidence is not strictly decade dependent, but due to the rarity of the spontaneous uterine rupture, most studies have a study interval of around a decade to collect enough number of patients sufficient for the analysis and comparison. With the progress of medicine and knowledge of the risk factors, the incidence is decreasing (Fig. 16.1).
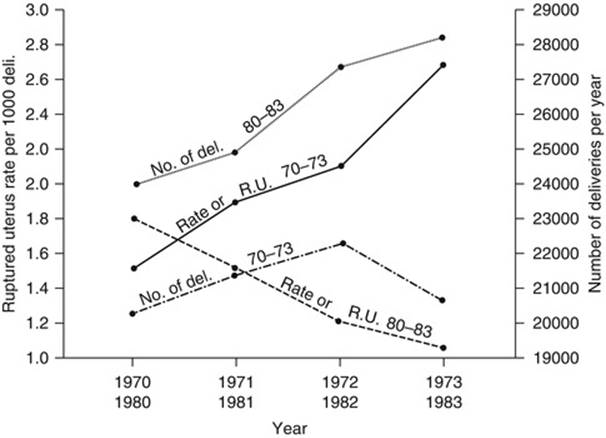
Fig. 16.1
Comparison between the total number of deliveries in 1970–1973 and 1980–1983 in relation to the rate of ruptured uterus per 1,000 deliveries in those years. (The numbers for 1983 are a multiplication of the first 6 months) (R.U. rupture of the uterus) [42]
16.3 Risk Factors
Most cases of spontaneous uterine rupture in undeveloped/developing countries is due to rupture of the unscarred uterus secondary to neglected obstructed labor, while previous Cesarean section scar (scarred uterus) rupture is the most common cause in developed countries [43–45]. On the contrary, in developed countries, rupture of unscarred uterus is severalfold lower than that of scarred uterus involving 1/17,000–1/20,000 deliveries [46]. Schrinsky and Benson in 1978 classified causes of uterine rupture during pregnancy [40] and here is updated and expanded version (Table 16.2):
Table 16.2
Classification of causes of uterine rupture during pregnancy
|
1. Traumatic rupture |
|
A. Instrumental |
|
(i) Uterine sound or curette |
|
(ii) Manual removal of placenta |
|
(iii) Various tool for induction of legal or criminal abortion |
|
B. Violence: direct or indirect |
|
C. Obstetric |
|
(i) Oxytocins, forceps (low, mid, failed), breech extraction |
|
(ii) Intrauterine manipulation: internal version, forceps rotation, shoulder dystocia |
|
(iii) Fundal pressure |
|
(iv) Craniotomy (hydrocephalus) |
|
(v) Neglect: cephalopelvic disproportion, transverse lie |
|
2. Spontaneous (prior to or during labor) rupture |
|
A. Previous uterine surgery |
|
(i) Cesarean section (low segment vs. classical) |
|
(ii) Myomectomy |
|
(iii) Salpingectomy |
|
(iv) Ventrofixation |
|
(v) Curettage or manual removal of the placenta |
|
B. No previous surgery |
|
(i) Congenital uterine abnormality |
|
(ii) Cornual pregnancy |
|
(iii) Hydatidiform mole or chorioadenoma destruens |
|
(iv) Placenta percreta |
|
(v) Genetic susceptibility for rupture (Loeys-Dietz syndrome) |
|
(vi) No apparent cause |
|
3. Combinations |
16.3.1 Scarred Uterus (Previous Cesarean Delivery)
Various reports have shown that previous Cesarean section is the most important predisposing factor for the occurrence of uterine rupture [4, 47, 48], and so-called scarred uterus (uterine scars from any type of operation) is present in up to 65 % of cases [24, 47–49]. The rate of Cesarean delivery has risen from 5 % in 1970 to 26 % in 2003 despite improvement in obstetric procedures such as classic Cesarean section, internal version, total breech exaction, etc. [50]. Relevant to this issue of vaginal birth after Cesarean section (VBAC) is that the overall rate in the United States increased from 3.4 % in 1980 to a peak of 28 % in 1996. Commensurate with this eightfold increase in the VBAC rate, reports of maternal and perinatal morbidity also increased, in particular with reference to uterine rupture. By 2007, the VBAC rate in the United States had fallen to 8.5 %. Not surprisingly, the Cesarean delivery rate also reached an all-time high of 32 % in 2007. In its most recent guidelines pertaining to VBAC in August 2010, the American Congress of Obstetricians and Gynecologists (ACOG) adopted the recommendation not to restrict women’s access to VBAC [51]. This occurred after the National Institutes of Health Consensus Development Conference Panel reviewed the totality of the evidence concerning maternal and neonatal outcomes relating to VBAC in March 2010 [52]. The recurrence rate for uterine rupture is reported to be between 4.8 and 19 % with the highest rates of recurrence seen in women with a history of a ruptured upper uterine segment (classic scar). All studies recommend planned Cesarean delivery [53–55].
16.3.1.1 Previous Classic Cesarean Delivery
Classic Cesarean delivery via vertical midline uterine incision is currently infrequently performed and account for 0.5 % of all births in the United States [56]. There is 11.5 % absolute risk of uterine rupture in women with classic vertical Cesarean scars who underwent an unplanned TOLAC [57]. For women who underwent repeat Cesarean section, the uterine rupture rate for women with prior classical uterine Cesarean scars was 0.64 %. All patients in that study underwent repeat Cesarean delivery, but a high rate of preterm labor resulted in 49 % of the patients being in labor at the time of their Cesarean delivery [56]. Landon et al. reported a 1.9 % absolute uterine rupture rate in women with a previous classic, inverted T, or J incision that either presented in advanced labor or refused repeat Cesarean delivery [58]. These rates of frank uterine rupture in women with classic Cesarean deliveries are in contrast to the higher rates of 4–9 % that the ACOG had historically reported for women with these types of uterine scars [59]. However, there is a 9 % rate of asymptomatic uterine scar dehiscence observed [56]. This result suggests that disruptions of uterine scars might have been misclassified as true ruptures instead of dehiscences in previous studies; this error may explain the bulk of the discrepancy.
16.3.1.2 Previous Low-Vertical Cesarean Delivery
A meta-analysis demonstrated a 1.1 % absolute risk of symptomatic uterine rupture in women undergoing a TOLAC with a low-vertical Cesarean scar [58, 60–63]. Compared to women with low-transverse Cesarean scars, these data suggest no significantly increased risk of uterine rupture or adverse maternal and perinatal outcomes. Interpretation of these studies is hampered by inconsistencies in how high the lower uterine segment could be cut before it was considered a classic incision. Even when the lower uterine segment is already well developed as a result of active labor, a low-vertical incision of adequate length is often impossible to permit fetal delivery. Naef et al. arbitrarily defined a 2 cm extension into the upper segment as a classic extension, and the overall rate of uterine rupture was 0.62 %. This rate could be further divided as 1.15 % for women who underwent a TOLAC compared with no ruptures among women who underwent elective repeat Cesarean delivery [60].
16.3.1.3 Unknown Uterine Scar
In many instances, the type of incision used for a prior Cesarean delivery cannot be confirmed due to unavailability of the operative report. Under these circumstances, the assessment of uterine rupture risk may sometimes be guided by the obstetric history to infer the most probable type of uterine scar. For example, a patient with a history of a preterm Cesarean delivery at 28 weeks’ gestation has a much higher likelihood of having had a vertical uterine incision than a patient who underwent a Cesarean section for an indication of arrest of fetal descent at term. It has been argued that because most Cesarean deliveries in the United States are accomplished via low-transverse uterine incisions, the risk of uterine rupture for patients with an unknown scar is similar to that for women who have previously undergone a low-transverse hysterotomy. This logic depends on the high ratio of low-transverse to vertical incisions performed for Cesarean section, but it ignores the varying probability with which different types of uterine incisions are made under different obstetric circumstances, as well as differences that occur due to varying medical resources and the prevailing local practitioner practices in countries other than the United States (e.g., practices that occur in other countries, such as Mexico or Brazil). An estimated 20,000 African refugees enter the United States each year, 80 % from countries were upper uterine segment Cesarean delivery is not an uncommon practice. Immigration of African refugees to Europe is becoming increasingly common [64]. Nevertheless, the vast majority of Cesarean deliveries performed in the United States are accomplished via low-transverse uterine incisions.
In a small case-control study of 70 patients, no association was found between an unknown uterine scar and the risk of uterine rupture; however, given the rarity of uterine rupture, this study was vastly underpowered to detect such a difference [65]. Two additional, but similarly underpowered, case series have also reported comparable rates of uterine rupture and VBAC success in women with unknown uterine Cesarean delivery scars versus those with documented previous low-transverse hysterotomies [66, 67]. The Maternal-Fetal Medicine Units Network Cesarean Delivery Registry reports a 0.5 % risk of uterine rupture for patients who underwent a TOLAC with an unknown uterine scar [58]. For cases in which there are one or two unknown prior uterine incisions, there is a single small, randomized, controlled trial by Grubb et al. that compared labor augmentation with oxytocin with no intervention in women with prior Cesarean deliveries involving either one or two unknown uterine incisions. Four uterine dehiscences and one uterine rupture occurred, all in the group that underwent labor augmentation [68].
16.3.1.4 Previous Low-Transverse Cesarean Delivery
The risk of uterine rupture after a low-transverse Cesarean delivery varies depending on whether patients undergo a TOLAC or an elective repeat Cesarean delivery and on whether labor is induced or spontaneous, as well as other factors. The vast majority of Cesarean deliveries in the United States are of the low-transverse type. For women who have had one previous Cesarean delivery, examining the various risk factors for uterine rupture is instructive. These absolute risks for uterine rupture are discussed below.
16.3.1.5 Previous Cesarean Delivery Without a Subsequent Trial of Labor
In a large study, the spontaneous uterine rupture rate among women with a single Cesarean delivery scar who underwent scheduled repeat Cesarean delivery without a TOL was 0.16 % [69]. This finding indicates that uteri with Cesarean scars have an intrinsic propensity for rupture that exceeds that of the unscarred organ during pregnancy, which is 0.012 % (OR 12). Therefore, all other uterine rupture rates in women with a previous Cesarean delivery should be referenced to this expected baseline rate.
16.3.1.6 Previous Cesarean Delivery with Subsequent Spontaneous Labor
The uterine rupture rate among women with a single previous Cesarean delivery who labored spontaneously during a subsequent singleton pregnancy is in the range of 0.45–0.72 % [69–71]. This rate of uterine rupture implies an increased relative risk (RR) of three to four for women who labor spontaneously compared with women who undergo elective repeat Cesarean delivery.
16.3.1.7 Previous Cesarean Delivery with Subsequent Augmentation of Labor
Despite the clinical heterogeneity and different VBAC success rates for women undergoing spontaneous labor rather than either labor augmentation or induction, very few studies have stratified their data by labor augmentation versus labor induction, and the data that do exist are conflicting. There is wide variance in the frequency of clinical use of oxytocin as well as in the dose and dosing schedules of oxytocin that are used. As a result, there is a paucity of specific evidence-based clinical guidelines for the use of oxytocin in VBAC trials. In a study by Blanchette et al., the rate of uterine rupture in women who underwent oxytocin augmentation of labor after a previous Cesarean delivery was 1.4 %, compared with 0.34 % in women who underwent a trial of spontaneous labor. This finding suggests a fourfold increased risk of uterine rupture in women who undergo labor augmentation with oxytocin compared with spontaneous labor after a previous Cesarean delivery.
In another study, the rate of uterine rupture with oxytocin augmentation was 0.9 % versus 0.4 % without oxytocin use [52]. Zelop et al. also found that labor augmentation with oxytocin did not significantly increase the risk for uterine rupture [70]. However, the conclusions to be drawn from this are both limited and suspect because, in general, no proper adjustment has been made for the potential (and very likely) confounding by indication that occurs in the observational studies that attempt to compare the rate of uterine rupture for women receiving treatment with oxytocin versus those who do not (e.g., proper propensity score matching has not been performed). Tahilramaney et al. found that neither the administration nor the duration of oxytocin had an impact on dehiscence or rupture [72]. Phelan found that when oxytocin is used in a judicious manner, there is no increased risk of uterine dehiscence or rupture in the scarred or unscarred uterus [73]. Therefore, the duration of labor and not oxytocin use itself may predispose the patient with or without a uterine scar to rupture. The problem in some studies from developing countries is high percentage of its use; 41.7 % of the respondents were given this drug (all but one had it through intravenous infusion) [9]. Oxytocin was used for augmentation of already prolonged and obstructed labor rather than for active management of labor concluding that the supervision and control over this drug is missing.
In this regard, assessment of the safety of oxytocin use in VBAC trials must consider both the dosage and the time of exposure. These issues were addressed by Cahill et al. in a multicenter, retrospective cohort with at least one prior Cesarean delivery who underwent a TOLAC. At an intravenous oxytocin dosage range of 6–20 mU/min, a more than threefold increased risk of uterine rupture was associated with oxytocin use. At a dosage range of more than 20 mU/min, a nearly fourfold increased risk of uterine rupture was noted. The attributable risk of uterine rupture associated with oxytocin use was 2.9–3.6 % for the maximum oxytocin dose ranges of more than 20 mU/min and more than 30 mU/min, respectively. The authors did not find a significant risk association between time (in terms of both duration of oxytocin exposure and duration of labor) and uterine rupture risk. They suggest an upper limit of 20 mU/min of oxytocin for use in VBAC trials and a judicious approach to the use and monitoring of oxytocin for both labor augmentation and induction.
The benefit of intrauterine pressure catheter (IUPC) monitoring of uterine contractions in VBAC trials is unclear, with only a single small case series failing to detect differences in fetal or maternal morbidity/mortality associated with uterine rupture when an IUPC was used instead of external tocodynamometry. Nevertheless, many institutions have found the IUPC useful in allowing careful titration of oxytocin dosing, especially when maternal habitus poses a limit to the accurate external monitoring of uterine contractions in women undergoing a TOLAC.
16.3.1.8 Previous Cesarean Delivery with Subsequent Induction of Labor
Emerging data indicate that induction of labor after a prior Cesarean delivery appears to be associated with an increased risk of uterine rupture. Zelop et al. found that the rate of uterine rupture that underwent labor induction after a single previous Cesarean delivery was 2.3 % compared with 0.72 % for women who had labored spontaneously [71]. In a study by Ravasia et al., the uterine rupture rate was 1.4 % compared with 0.45 % for women who labored spontaneously [70]. Blanchette et al. found that the uterine rupture rate after previous Cesarean delivery when labor was induced was 4 % compared with 0.34 % for women who labored spontaneously [74]. This last finding suggests a 12-fold increased risk of uterine rupture for women who undergo labor induction after previous Cesarean delivery.
Data on mechanical methods of labor induction for cervical ripening are limited but reassuring. In a small case series, Bujold et al. found no statistically significant difference among the uterine rupture rates of 1.1 % for spontaneous labor, 1.2 % for induction by amniotomy with or without oxytocin, and 1.6 % for induction by transcervical Foley catheter [75]. Conversely, Hoffman et al. reported a 3.67-fold increased risk of uterine rupture with Foley catheter use for preinduction cervical ripening. Importantly, however, many of these patients received concomitant oxytocin together with application of the transcervical Foley catheter [76]. Of particular note is that a recent randomized controlled trial by Pettker et al. found that the addition of oxytocin to the use of a transcervical Foley catheter for labor induction does not shorten the time to delivery and has no effect on either the likelihood of delivery within 24 h or the vaginal delivery rate [77]. In light of these findings, induction of labor with a transcervical Foley catheter alone may be a reasonable option for women undergoing a TOLAC with an unfavorable cervix.
16.3.1.9 Prostaglandins for Cervical Ripening and Induction of Labor After Previous Cesarean Delivery
Current ACOG guidelines discourage the use of prostaglandins to induce labor in most women with a previous Cesarean delivery. This recommendation is based on considerable evidence for an increased risk of uterine rupture associated with prostaglandins. Several studies found a severalfold (3–5 % compared to <1 %) increased risk for uterine rupture when prostaglandins were used in gravidas who underwent a TOLAC [69, 70, 78]. In contrast, two studies did not show significant difference (in both studies, patients with induction of labor had higher percentage of spontaneous uterine perforations) [79, 80]. Landon et al. reported no uterine ruptures among 227 patients who underwent induction with prostaglandins alone. Although the study was underpowered to detect small differences, the particular type of prostaglandin administered did not appear to significantly affect the uterine rupture rate (52 patients received misoprostol; 111, dinoprostone; 60, PGE2 gel; and 4, combined prostaglandins) [58].
16.3.1.10 Previous Cesarean Delivery with Previous Successful Vaginal Delivery
Several studies have shown a protective association of previous vaginal birth on uterine rupture risk in subsequent attempts at vaginal birth after previous Cesarean delivery with around one-fourth to one-fifth of the risk [81–83]. A Maternal-Fetal Medicine Units Network study found that in women with no prior vaginal delivery who underwent a TOLAC, there was an increased risk of uterine rupture with induction versus spontaneous labor (1.5 % vs. 0.8 %, p = 0.02). In contrast, no statistically significant difference was shown for women with a prior vaginal delivery who underwent spontaneous TOLAC compared with labor induction (0.6 % vs. 0.4 %) [84].
16.3.1.11 Previous Cesarean Delivery with Subsequent Successful VBACs
Multiple studies suggest a protective advantage with regard to the uterine rupture rate if a woman has had a prior successful VBAC attempt. Multiple potential explanations exist, but the two most obvious are that a successful prior VBAC attempt assures that (1) the maternal pelvis is tested and that the bony pelvis is adequate to permit passage of the fetus and (2) the integrity of the uterine scar has been tested previously under the stress/strain conditions during labor and delivery that were adequate to result in vaginal delivery without prior uterine rupture. Mercer et al. found that the rate of uterine rupture decreased after the first successful VBAC, but that there was no additional protective effect demonstrated thereafter: the uterine rupture rate was 0.87 % with no prior VBACs, 0.45 % for those with one successful prior VBAC, and 0.43 % for those with two or more successful prior VBACs [85]. Pooled data from five studies indicate an increased uterine rupture rate of 1.4 % (1/73) in failed VBAC attempts that required a repeat Cesarean section in labor [58, 74, 86–88].
16.3.1.12 Interdelivery Interval
Several studies found an interpregnancy interval between Cesarean delivery and a subsequent pregnancy of <6 months that was nearly three to four times as common among patients who had uterine rupture than in control subjects [89, 90]. Shipp et al. similarly found that the risk of symptomatic uterine rupture was increased threefold in women with interdelivery intervals of <18 months when they underwent a TOLAC after one previous Cesarean delivery [91]. The authors controlled for maternal age, public assistance, length of labor, gestational age of 41 weeks, and induction of augmentation of labor with oxytocin. In additional support of this observation, a Canadian study on women who underwent a TOL after a single previous low-transverse Cesarean delivery found that 2.8 % of patients who had an interdelivery interval of ≤24 months had a uterine rupture compared with 0.9 % for those with an interdelivery interval of >24 months (OR 2.65) [92]. In a follow-up study, the same authors examined the risk of uterine rupture between 18 and 24 months. After adjustment for confounding factors, they found that an interdelivery interval shorter than 18 months was associated with a significant increase of uterine rupture (OR 3), whereas an interdelivery interval of 18–24 months was not (OR 1.1). The conclusion is that an interdelivery interval shorter than 18 months but not between 18 and 24 months should be considered as a risk factor for uterine rupture [93].
The authors speculated that a prolonged interpregnancy interval may allow time for the previous Cesarean delivery scar to reach its maximal tensile strength before the scar undergoes the mechanical stress and strain with a subsequent intrauterine pregnancy. Interestingly, the authors also observed that the combination of a short interdelivery interval of ≤24 months and a single-layer hysterotomy closure was associated with a uterine rupture rate of 5.6 %, a rate approximately three times higher than patients without this combination. This is comparable to the rate of uterine rupture for patients undergoing a TOLAC with a previous classic midline Cesarean scar [92]. There were no comparisons of single- or two-layer suture in these studies.
16.3.1.13 One-Layer Versus 2-Layer Hysterotomy Closure
Bujold et al. found a four- to fivefold increased risk of uterine rupture for women who had a previous single-layer uterine low-transverse closure compared with those having a two-layer closure for Cesarean hysterotomy. Uterine rupture occurred in 3.1 % of previous single-layer closure versus 0.5 % of two-layer closure (OR 3.95) [94]. The other studies had similar results with conclusion that single-layer closure should be avoided in women who contemplate future VBAC delivery [95, 96]. One study states that locked but not unlocked single-layer closures were associated with a higher uterine rupture risk than double-layer closure in women attempting a TOL [97].
16.3.2 Multiple Cesarean Deliveries
Most large-scale studies showed that multiple Cesarean sections carry a higher risk for uterine rupture than a previous single Cesarean section. Ten studies published from 1993 to 2010 showed that the risk of uterine rupture in a subsequent pregnancy ranged from 0.9 to 6.0 % (1/17–1/108). This risk is increased 2–16 times compared to women with only a single previous Cesarean delivery [98–100]. A study by Caughey et al. confirmed these results and also found that women with a previous vaginal delivery were about one-fourth as likely to have a uterine rupture as women without a previous vaginal delivery (OR 0.26) [82].
A 2004 ACOG guideline suggested that in women with two previous Cesarean deliveries, only those with a previous vaginal delivery should be considered candidates for a TOLAC [101]. This ACOG recommendation was subsequently revised in an updated 2010 guideline to suggest that women with two previous low-transverse Cesarean deliveries may be considered candidates for TOLAC regardless of their prior vaginal delivery status [51]. The only study with findings contrasting with all these reports where there was no statistically significant difference in uterine rupture between single and multiple previous Cesarean sections was by Landon et al. [102].
16.3.2.1 Previous Uterine Myomectomy
Nearly all uterine ruptures that involve uteri with myomectomy scars have occurred during the third trimester of pregnancy or during labor [103, 104]. Only one case of a spontaneous uterine rupture has been reported before 20 weeks of gestation [105]. Brown et al. reported that among 120 term infants delivered after previous transabdominal myomectomy, no uterine ruptures occurred and 80 % of the infants were delivered vaginally [106]. In contrast, Garnet identified uterine rupture rate of 4 % in women who had scars from a previous myomectomy and who underwent elective Cesarean delivery because of previous myomectomy [107]. Such reports do not often delineate the factors that were deemed important for assessing the risk of subsequent uterine rupture (e.g., number, size, and locations of leiomyomas; number and locations of uterine incisions; entry of the uterine cavity; type of closure technique).
Dubuisson et al. reported a uterine rupture rate of 3 % in patients who underwent previous laparoscopic myomectomy [104]. Only one rupture occurred at the site of the previous myomectomy scar, resulting in the conclusion that the risk of pregnancy-related uterine rupture attributable to laparoscopic myomectomy is 1 %. However, the rarity of spontaneous uterine rupture raises the issue of whether the two uterine ruptures at sites that were not coincident with previous myomectomy scars were attributable to the previous myomectomies. Others reported no pregnancy-related uterine ruptures in women who previously underwent laparoscopic myomectomy [108–111]. However, the number of patients who were allowed to labor was low, and a high percentage of deliveries were by scheduled Cesarean delivery (80, 79, 75, and 65 %, respectively). In a prospective study from Japan, there were no uterine ruptures among 59 patients with a successful vaginal delivery after a prior laparoscopic myomectomy [112]. In a multicenter study in Italy with 386 patients after laparoscopic myomectomy, there was one recorded spontaneous uterine rupture at 33 weeks’ gestation (rupture rate 0.26 %) [113]. Uterine rupture has been reported to occur as late as 8 years after laparoscopic myomectomy [114]. This finding suggests that additional investigations with long-term follow-up are needed.
16.3.2.2 Medical Abortion
Medical abortion was started in the late 1980s, becoming more widely used in the late 1990s with mifepristone and misoprostol being the most used. It came as an alternative for the dilatation and curettage which caused more complications, resulting in 50,000–100,000 maternal deaths every year [115, 116]. In 2006, the total number of abortions for women residing in England and Wales was 193,700 compared with 186,400 in 2005, a rise of 3.9 %. Of these, medical abortions accounted for 30 % of the total compared with 24 % in 2005 [117]. No randomized controlled trial has been powerful enough to properly compare medical and surgical abortions in relation to the possible adverse effects of these two treatments. Misoprostol alone for termination of pregnancy was described for the first time in 1994. It has been used widely in the normal uterus [115, 116].
The absence of previously reported cases of gemeprost-associated uterine rupture may reflect the rarity of this method of pregnancy termination in the second trimester. Fourth case was notable because of the absence of risk factors for uterine rupture. It is unlikely that routine amniocentesis or chorionic villus biopsy would have predisposed this patient to uterine rupture [118]. Initially, higher doses were administered and the conclusion was that smaller doses may lessen the risk of uterine hypertonus and decrease the risk of uterine rupture. There is a case of combined use of oral mifepristone and intravaginal misoprostol (prostaglandin E1 analog) causing uterine rupture [119]. Additional risk factor in such cases is scarred uterus [120–122], but there are cases with this uterine rupture in unscarred uterus [123, 124]. The only systematic review on the subject from 2009 found a seven times higher incidence of uterine rupture of scarred uterus (0.28 %) in comparison with unscarred uterus (0.04 %), but authors found the incidence acceptable to both patients and health-care providers [125]. Rupture in an unscarred uterus is possibly related to the dose, dose interval, gestation, and parity. Based upon pharmacokinetics of misoprostol, a dosage interval of 6 h is common (range 3–12 h) [126]. Uterine rupture occurred in one case with lower accumulated dose of misoprostol (1,200 Ag/30 h) than in some reported regimens (2,400 Ag/24 h) [126]. There is even a case of spontaneous rupture of the unscarred uterus in the first trimester using mifepristone/misoprostol for medical termination of pregnancy [127].
Corticosteroid therapy is listed as a contraindication to mifepristone (but not misoprostol), possibly because of its glucocorticoid antagonistic effect. Whether prolonged corticosteroid therapy can result in a weakened myometrium susceptible to rupture remains to be determined.
The incidence of uterine rupture among women with a prior Cesarean delivery during second trimester pregnancy termination with prostaglandin E2 or oxytocin is 3.8 % [128]. The risk is even higher when oxytocin is used with prostaglandins [129]. The incidence of this complication with misoprostol was difficult to define because of paucity of its use. There was no set regimen protocol for intravaginal misoprostol in second trimester pregnancy termination, and all studies have used a different regimen. Mostly the initial dose was 400 Hg repeated every 4–6 h, up to a maximum of 1,200–1,600 Hg per 24 h. Some studies have augmented misoprostol with either oxytocin or mifepristone [120, 123, 128]. Recently, FIGO has recommended the regimen protocol for second trimester pregnancy termination with 100–200 Hg intravaginal misoprostol, repeated 6 hourly till maximum four doses/24 h [129], and its use should be with care in a previously scarred uterus.
Four cases of rupture of an unscarred uterus in the second trimester following MTOP were found. Only two of these cases used mifepristone and misoprostol [120, 130]. The other women found do not follow the MTOP protocol but contain information relevant to this case. The first was an MTOP using mifepristone and gemeprost. The rupture was found by ultrasound scan the morning after commencing prostaglandins [119]. The second case was a grand multiparous patient [122]. The rupture was found by ultrasound scan following one dose of misoprostol (200 μg) followed by oxytocin 12 h later. Although high doses of prostaglandins is a known risk factor, the above two women were treated for over 24 h, raising the possibility that duration of prostaglandin treatment is a risk factor. Other agents, such as ethacridine lactate, have been linked to uterine rupture, although this is very rare and the case was relating to the second trimester [131].
Cases of uterine rupture have been reported involving small doses of misoprostol. One case involved an endocervical rupture in the second trimester following two doses [132]. Another was a scarred uterus, and the patient was being prepared for surgical management [133]. A similar case to this was of a first trimester rupture following one dose of misoprostol in preparation for surgical termination [134].
There is no evidence that pretreatment with mifepristone might increase the chance of uterine rupture. It is thought that the chance might actually be reduced as mifepristone increases cervical compliance; however, as it increases uterine sensitivity to the action of exogenous prostaglandins [119], the risk benefit is not known. Previous Cesarean sections are thought to be a risk factor for uterine rupture. One trial of second trimester abortion using misoprostol in 720 women with one or more previous Cesarean deliveries has been carried out and concluded that the use of misoprostol was not associated with an excess of complications compared with women with unscarred uteri [135].
16.3.3 Unscarred Uterus
An unscarred prelabor primigravid uterus can show a very thin uterine wall, compatible with incomplete uterine rupture, without apparent etiological or risk factors. Walsh and Baxi [136], reviewing the literature over six decades (1946–2006), found 36 primigravid uterine ruptures, and Matsubara et al. have found a further 21 cases [137–141]. Of these 21 cases, 15 were reported in a case series from Nepal [140], with all ruptures occurring after labor of >48 h, and 12 having received no antenatal care. Of 57 (36 + 21) cases previously reported, 55 women had some discernible etiological or risk factors for rupture, including a past history of uterine surgery, congenital uterine anomaly, adherent placenta, labor, or oxytocin and/or prostaglandin use [136–142]. The etiological factors were described as indiscernible in the remaining two cases; one of which was described in a case series and lacked detailed data [143]. In the remaining case – that of a 21-year-old Indian woman – she had stated that she was primigravida, but she had received no antenatal care until rupture, and no further evaluation to identify any underlying condition was performed [144]. Therefore, the data was insufficient to claim “unknown etiology.” There have been no reported cases of primigravid unscarred uterine rupture of unknown etiology, employing its strict definition.
16.3.3.1 Oxytocin
PGE2 is a potent oxytocic agent and rupture of the unscarred uterus has been reported with vaginal and intracervical applications [41, 145–147]. PGE2 should be used with caution particularly in multiparous patients and in combination with oxytocin [39]. Uterine hyperstimulation was not observed and rupture occurred more than 4 h after administration [39].
16.3.3.2 Vacuum-Assisted Vaginal Delivery
One rupture was encountered after vacuum-assisted vaginal delivery. Application of external force in the second stage of labor [148], vacuum forceps, and breech extraction are all possible causes of uterine rupture [41].
16.3.3.3 Parity and Age
High multiparity carries with it certain inherent risks … it can be very unforgiving of any carelessness, incapacity or neglect. John Kevin Feeney, 1935
The high parity observed by John Kevin Feeney (Professor of Gynecology and Obstetrics in University College Dublin and Master of the Coombe Hospital in Dublin) in 1953 is recognized as major risk factor of spontaneous uterine rupture in unscarred uterus in most studies [149, 150]. Some authors have reported that the uterus may have been weakened by thinning and stretching of the muscle fibers during labor, especially with aging and repeated childbearing [39]. There are several studies that show the mean parity at the time of rupture was between 5 and 6 [151–155]. Grand multiparity predisposes to malpresentation and unstable lie, a significant risk factor for ruptured uterus [32, 156]. Grand multiparas attended antenatal clinics sparsely (due to heavy domestic commitments), and consequently, malpresentations were diagnosed late, during labor. However, Beacham et al. [157] and Mennon [158] reported that 56–75.6 % of uterine ruptures occurred in women with a parity of between 1 and 4, while 38 % (69/184) with parity between 5 and 9 had ruptures. Nevertheless, recent evidence suggests that with proper antenatal care, modern obstetrics, and advanced neonatal services there is no difference in outcome between grand multiparous women and women with low parity [159]. Gardeil et al. found only two women with uterine rupture among 39,529 multigravidas who had no previous uterine scar (0.005 %) [160]. Uterine overdistension due to the presence of twin pregnancy was not proven to be the risk factor. Fetal weight in singleton pregnancy is a risk only when it contributes to cephalopelvic disproportion [9].
Age and parity are interrelated risk factors. Women older than 35 and women having their fifth or later birth are at greatest risk for uterine rupture, and the importance of fertility regulation and contraception usage could be clearly concluded [9]. Others state the peak incidence in the 26–35-year age range [157], while one Nigerian study showed peak incidence in 25–29 age group. Probably, it is related to reproductive and life span in developing countries with significantly lower incidence of older parturient women.
Unfortunately, these two factors are prominent features in obstetric practice in Qatar where repeated pregnancies continue into middle age. In their study, 56.9 % cases of uterine rupture were grand multiparous (para 5 or more), and nine patients 39 % were >35 years of age. These findings and review of the literature suggests some additional risk factors that warrant consideration.
Other etiological factors classically recognized as contributing to a rupture of unscarred uterus are as follows: obstetric maneuvers, malpresentations especially transverse fetal position, cephalopelvic disproportion, excessive uterine expressions, abnormal placentation (placenta percreta mainly), trauma due to uterine curettage, and uterine abnormalities [31, 161]. Connective tissue diseases [142] may also induce uterine rupture. In some cases, the rupture of gravid uterus has no obvious cause even before labor [162]. In the series of 40 uterine ruptures, Schrinsky and Benson [40] found ten spontaneous ruptures without any predisposing factors.
16.3.3.4 Congenital Uterine Anomalies
Congenital uterine anomalies affect approximately 1/200 women [163]. In such cases, the walls of the abnormal uteri tend to become abnormally thin as pregnancies advance, and the thickness can be inconsistent over different aspects of the myometrium [164–167]. Ravasia et al. reported an 8 % incidence of uterine rupture in women with congenitally malformed uteri compared with 0.61 % in those with normal uteri who were attempting VBAC [168]. Both cases of uterine rupture in the women with uterine anomalies involved labor induction with prostaglandin E2. In contrast, a study of 165 patients with Müllerian duct anomalies who underwent spontaneous labor after one prior Cesarean delivery reported no cases of uterine rupture [169]. Of note, in this study 36 % had only a minor uterine anomaly (arcuate or septate uterus), and 64 % had a major uterine anomaly (unicornuate, didelphys, or bicornuate uterus). Moreover, only 6 % with Müllerian duct anomalies underwent induction of labor.
For pregnancies that implant in a rudimentary horn of a uterus, a particularly high risk of uterine rupture (≤81 %) is associated with the induction of labor [170]. Importantly, 80 % of ruptures involving these types of rudimentary horn pregnancies occurred before the third trimester, with 67 % occurring during the second trimester.
The decision for induction of labor in women with a congenitally anomalous uterus, especially in cases of a previous Cesarean delivery, must be carefully considered, and given the higher incidence of uterine rupture reported in this patient population. Although the uterine rupture rate for unscarred anomalous uteri during pregnancy is increased relative to that for normal uteri, the precise increase in risk associated with the different types of uterine malformations remains uncertain.
16.3.3.5 Uterine Sacculation
A thin uterine wall, as a result of uterine sacculation [171, 172] or uterine diverticulum [173] may induce uterine rupture. Uterine sacculation is defined as a transitory pouch or saclike structure developing from a portion of the gravid uterus [172]. The typical form of sacculation results from an incarcerated retroverted uterus [171, 172]. A ventrally located cervical ostium and vagina may cause physicians to suspect this diagnosis. Magnetic resonance imaging (MRI) may provide a preoperative diagnosis [171]. In this condition, the anterior uterine wall becomes stretched and thinned. Other conditions, such as previous surgery, a primary myometrial defect, uterine malformation, or placental abnormalities, are listed as possible causes of uterine sacculation [172, 174].
16.3.3.6 Uterine Diverticulum
Uterine diverticulum is frequently misunderstood and reported as uterine sacculation [173]. Uterine diverticulum has a narrow connection with the uterine cavity and a thicker wall than in sacculation [173]. While uterine sacculation is usually observed during pregnancy [172, 174], diverticulum is usually detected in nonpregnant women. Uterine diverticula as complications during pregnancy are rare. Rajiah et al. [173] reported a primigravid woman in whom an MRI revealed uterine diverticulum in the 22nd week of gestation. A Cesarean section was performed in the 31st week. The diverticulum originated from the posterolateral wall of the uterine body and did not contain the fetus. The diverticulum was not excised due to surgical risks. In the postpartum period, the diverticulum was observed via ultrasound. The authors considered that the underlying etiology for the diverticulum may have been congenital because this patient was primigravida with no prior cervical or uterine procedure. Sun et al. [175] reported a case in which the gestational sac implanted in a diverticulum: the pregnancy was terminated at an estimated 7–8 weeks. The authors considered that abnormal development of the paramesonephric duct may cause a congenital uterine deformity, leading to a formation of diverticulum.
Midforceps delivery and breech version extraction have been implicated as potential causes of uterine rupture [176]. Whether or not the manipulation causes the rupture is unclear. Epidural anesthesia has also been linked to uterine rupture; however, in those patients with uterine rupture, the incidence of epidural use is small and ranges from 6 to 21 % [28, 177, 178].
Prelabor uterine rupture in primigravid women was identified in 24 cases up to 2011. In almost half of them, partial wall defect was the principal recognizable risk factor before the onset of labor. It is interesting to note that 52 % of women with specific available information had a history of infertility. A possible explanation could be that infertile patients more frequently undergo diagnostic/operative procedures on their uterus during diagnostic investigation or treatment resulting in a likelihood of iatrogenic damage [179]. It is important that the majority (67 %) of the women did not attend antenatal care [12].
16.3.3.7 Genetic Susceptibility for Rupture
Loeys-Dietz syndrome is a syndrome caused by heterozygous mutations in the genes encoding type 1 or 2 transforming growth factor-β receptor (TGF-βR1/2). The obstetric manifestations are risk of rupture of the gravid uterus and the arteries, either during pregnancy or in the immediate postpartum period, and damage to the vagina, the perineum, and the colon [180].
16.3.3.8 Sexual Intercourse
There are three case reports describing uterine rupture following sexual intercourse [181–183]. The topic for discussion could be is the uterine rupture spontaneous after sexual intercourse of should this mechanism be included in the group of traumatic uterine ruptures. Also it is not known whether intercourse was before cases of other reports of spontaneous uterine rupture.
16.3.3.9 Antenatal Care
The prenatal care in Yemen is very poor. According to the last published data, only 44 % of pregnant women had ever been to any prenatal clinic, with the frequency of visits during a pregnancy ranging from one to four. Women visit antenatal clinic mostly when they encounter a complication and very rarely for a routine antenatal care (13 %). In Yemen, 56 % of pregnant women have never had any antenatal care. Home delivery is still common in Yemen. About 78 % of women deliver at home, 16 % at state hospitals, and about 5 % at private hospitals. The home deliveries are usually attended by midwives with minimal training or relatives who have had some experience of labor. Some of the women will still deliver at home completely alone [9].
16.4 Prevention
The most direct prevention strategy for minimizing the risk of pregnancy-related uterine rupture is to minimize the number of patients who are at highest risk. The salient variable that must be defined in this regard is the threshold for what is considered a tolerable risk. Although this choice is ultimately arbitrary, but safety threshold is chosen as 0.5 % (1/200), therefore the categories of patients that exceed this critical value are those with the following:
· Multiple previous Cesarean deliveries
· Previous classic midline Cesarean delivery
· Previous low-vertical Cesarean delivery
· Previous low-transverse Cesarean delivery with a single-layer hysterotomy closure
· Previous Cesarean delivery with an interdelivery interval of less than 2 years
· Previous low-transverse Cesarean delivery with a congenitally abnormal uterus
· Previous Cesarean delivery without a previous history of a successful vaginal birth
· Previous Cesarean delivery with either labor induction or augmentation
· Previous Cesarean delivery in a woman carrying a macrosomic fetus weighing >4,000 g
· Previous uterine myomectomy accomplished by means of laparoscopy or laparotomy
16.5 Mechanisms and Classification
16.5.1 Definition
Uterine rupture is defined as a disruption of the uterine muscle and visceral peritoneum or a uterine muscle separation with extension to the bladder or broad ligament found at the time of Cesarean delivery or laparotomy following vaginal birth after previous Cesarean section. Rupture can be incomplete or complete.
Incomplete uterine rupture is present when the uterine wall is extremely thinned and the uterine muscular layer is lost but the uterine serosa (parietal peritoneum) is preserved (Fig. 16.2). It is mostly seen with scar dehiscence. Incomplete rupture is also referred to as uterine dehiscence. In contrast to frank uterine rupture, uterine scar dehiscence involves the disruption and separation of a preexisting uterine scar. Uterine scar dehiscence is a more common event than uterine rupture and seldom results in major maternal or fetal complications. Importantly, when the defect in the uterine wall is limited to a scar dehiscence, it does not disrupt the overlying visceral peritoneum, and it does not result in clinically significant bleeding from the edges of the preexisting uterine scar. In addition, in cases of uterine dehiscence (as opposed to uterine rupture), the fetus, placenta, and umbilical cord remain contained within the uterine cavity. If Cesarean delivery is needed, it is for other obstetric indications and not for fetal distress attributable to the uterine disruption.
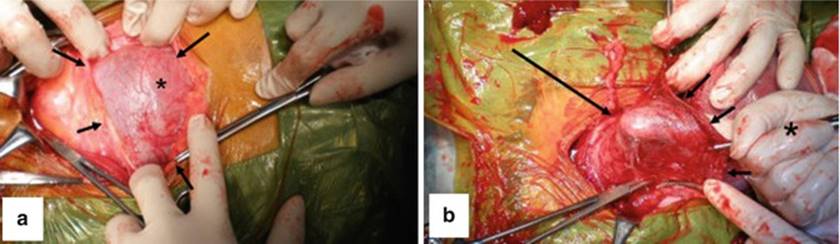
Fig. 16.2
Operative findings during a Cesarean section. (a) The asterisk indicates the thin anterior uterine wall, seen with a bulge caused by fetal parts from the inside. Arrows indicate the peritoneum. The left side of the photograph is the caudal side of the patient. (b) After delivering the fetus and removing the placenta, the thin wall was gently pushed from inside the uterus with a finger. The finger tip (large arrow) is clearly visible through the thin wall. The asterisk indicates the surgeon’s right hand. Small arrows indicate the uterine incision site [184]
Complete uterine rupture is present when rupture occurs through all layers of the uterine wall including serosa with or without accompanying bleeding or hematoma (Fig. 16.3). Therefore, the amniotic cavity directly communicates with the abdominal cavity. In the study by Padhye, 70 % had complete rupture and 25 % incomplete rupture. Seventy percent of scar rupture presented with complete rupture [25].
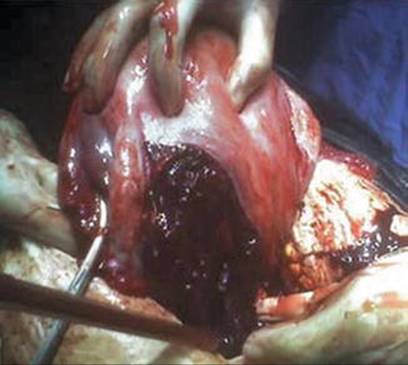
Fig. 16.3
Complete uterine rupture with a large left broad ligament hematoma with multiple small bleeding points from the branches of the uterine artery is seen [148]
16.5.2 Classification
Rickards in 1938 described five types of rupture of the scarred uterus during pregnancy [185]:
· Type I: In this group, the rupture occurs through an old upper segment incision, and the placenta is situated away from the uterine scar. Characteristics include:
· Rupture tends to take place during labor.
· Little or no hemorrhage occurs, and therefore the pulse remains good.
· The pain may become niggling in type after the scar has started to give way.
· The bulging bag of membranes may sometimes be palpated through the abdominal wall.
· Prognosis is good provided that suitable treatment is available.
· Type II: It consists of cases in which the rupture occurs through an upper segment incision and the placenta is situated underneath the old scar. This type of case is more serious and presents a different clinical picture. When the placenta is situated underneath the old scar, a gradual erosion of fibrous tissue by the placental villi occurs [186]. This erosion is an insidious one and may cause marked attenuation of the scar during the latter part of pregnancy. In this type, rupture is more liable to occur before the onset of labor. The eating away of the scar may be associated with vague pains in the lower abdomen [187]. As the process is gradual, hemorrhage is seldom severe. Characteristics include:
· Gradual rupture tends to occur toward the end of pregnancy. This may be accompanied by vague pain in the lower abdomen. Such pain should therefore never be ignored.
· After the onset of labor, hemorrhage occurs and may be of considerable severity.
· Prognosis will not be so favorable as in type I and will depend very largely on the amount of intra-abdominal hemorrhage.
· Type III: The uterine rupture occurs after a previous lower segment Cesarean section. Characteristics include:
· Rupture is said to take place during labor.
· Hemorrhage may occur, due to the extension of the laceration laterally into the uterine arteries.
· The bladder may be involved (rarely), giving rise to hematuria.
· Type IV: The rupture is complete, through an upper segment incision, and the child, within its bag of membranes, is expelled into the abdominal cavity, the placenta remaining in situ. The uterine scar gives way along its entire length, the contractions persist, and the child is extruded into the abdominal cavity. The fetal heart sounds almost invariably disappear and fetal movements cease. The physical signs are characteristic. The uterus is felt to be pushed over to one side, and the child, floating in the abdominal cavity, is very easily palpable. Characteristics include:
· Fetal heart sounds cease as a rule.
· Fetal movements usually stop.
· The uterus is pushed over to one side.
· The fetus, lying free in the abdominal cavity, is easily palpable.
· Type V: The rupture is complete, through an upper segment incision, and the child, with its placenta, is extruded completely into the abdominal cavity. Characteristics include:
· Often associated with severe intra-abdominal hemorrhage.
· Fetal heart sounds are absent.
· Fetal movements are absent.
· The uterus is pushed over to one side.
· The fetus, lying free in the abdominal cavity, is easily palpable.
16.5.3 Pathophysiology
16.5.3.1 Scarred Uterus
Patients who had a previous uterine scar were more likely to rupture in the hospital as a result of attempted trial of scar and the poor monitoring of labor [12]. In scarred uteri, the vast majority of uterine dehiscence and ruptures will occur via the uterine scar. The atrophic, inelastic nature of the scar renders it less adaptive to forces in labor, predisposing to scar rupture. However, a particularly rigid anterior lower segment may cause abnormal distribution of force. During retraction, the posterior wall may be excessively shortened and thinned due to the rigid anterior uterine scar, catalyzing atypical uterine rupture via healthy tissue. Any factor compromising uterine structural integrity or causing abnormal distribution of force can precipitate uterine rupture. The site of uterine rupture is unpredictable and may be atypical. The most common location is lower anterior uterine segment.
There are only six cases of posterior uterine rupture complicating vaginal birth after Cesarean section in the period 1997–2011 [147, 188–192]. Fetal malposition with an occipitoposterior position has previously contributed to posterior uterine ruptures (Fig. 16.4), as has malpresentation with a transverse lie and dead fetus [190–192]. Malposition alters the distribution of contractile force and increases labor dystocia; certain malpresentations cause uterine hyperdistension, which may also precipitate atypical uterine rupture.
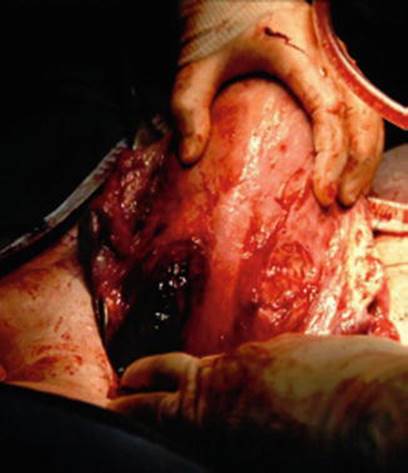
Fig. 16.4
Vertical posterior rupture of scarred uterus due to occipitoposterior position of the fetus [191]
Prostaglandins generating excessive uterine activity have been assumed to be the cause of uterine rupture. Buhimschi et al. suggested that prostaglandins induce local biochemical modifications that weaken the scar, predisposing it to rupture [193]. Figueroa et al. [189] proposed that prostaglandins might have caused excessive uterine activity that resulted in a posterior wall sacculation in the face of a strong anterior scar. During the second stage of labor, with the fetus undergoing cardinal movements, uterine rupture occurred through the weakened posterior wall. But in the five instances of rupture through posterior uterine wall in the presence of anterior scar, only in two cases was labor induced by prostaglandin, suggesting other factors may play a role. The presence of an inelastic scar comprised of fibrous tissue on the anterior wall prevents even distribution of forces of contraction. As uterine muscle undergoes retraction during active phase of labor, the healthy posterior wall may undergo excessive shortening and thinning compared to inelastic anterior wall, which could have predisposed to rupture.
The lower segment uterine rupture is the most common (60 %) site of rupture [46, 194–196] with anterior transverse location being the most common [16]. The second most common location is extension to broad ligament, and other locations have an incidence of around 5 % [16]. The study did not differentiate between rupture caused by obstructed labor and scarred uterus. Rupture is complete in around 73 % cases and incomplete in 27 % [46, 194, 196, 197].
16.5.3.2 Unscarred Uterus
Obstruction as a cause of uterine rupture and the delay in accessing qualified care is found in developing counties with patients without antenatal care. The causes of rupture during labor may briefly be described as follows: some obstruction exists opposing the advance of the child; whether the obstruction is pelvic contraction, unusual size of the child, or malpresentation does not matter – the uterus continuing to contract, thickening of the upper part of the uterus occurs, while its lower segment becomes thinned. If assistance is not given, the lower segment becomes more and more thinned and finally ruptures. It is to be noted that rupture of the uterus during labor almost always begins in the lower segment. These may be complete or incomplete, according as they involve the entire thickness of the organ, or only extend to the peritoneal covering; they may extend to the vagina.
It is the most common cause of spontaneous rupture during pregnancy and labor ranging from 68.5 to 73.2 % [5, 12] in developing countries. In developed countries, it is significantly lower starting from 13 % [159].
16.6 Clinical Presentation
16.6.1 Symptoms and Signs
The signs and symptoms of uterine rupture largely depend on the timing, site, type, and extent of the uterine defect. Classical signs and symptoms of uterine rupture have been reported by many authors ranging back to 1881 [198]. Sudden, severe, shearing abdominal pain with the absence of fetal heart sounds and cessation of uterine contractions in conjunction with vaginal bleeding and shock is classical presentation. Overall, only 45 % of cases reviewed had the classical signs and symptoms of uterine rupture [8, 13, 21, 158, 176, 199–202]. Commonly reported signs and symptoms related to uterine rupture are abdominal pain and tenderness, shock, vaginal bleeding, undetectable fetal heart beat, palpable fetal body parts, cessation of contractions, and signs of intraperitoneal bleeding. One study showed that severe abdominal pain was present in 13.4 % of patients with uterine rupture, shock in 21.3 %, bleeding in 16.8 %, disappearance of fetal heart sounds in 8.9 %, and cessation of contractions in 5.6 % [201]. Less commonly associated with uterine rupture are epigastric pain, shoulder pain (right sided or bilateral), abdominal distention and paralytic ileus, hematuria, hypertonic uterus, altered uterine contour, and fluid thrill. Fetal distress, manifested by fetal bradycardia and absence of fetal movement, is also reported.
16.6.1.1 Labor
Rupture of the uterus during labor is also associated with cessation of labor pain, recession of presenting fetal body parts, cervical lacerations, and vaginally palpable uterine defect. The most common sign is the sudden appearance of fetal distress during labor. One series reported that 81 % of patients with uterine rupture during labor have evidence of fetal distress prior to the onset of bleeding or abdominal pain [178], while in another study the most common manifestation of uterine rupture were fetal heart abnormalities present in 43.5 % [24]. The observation of sudden fetal heart irregularity in laboring women should be taken as a potential sign of danger [37].
16.6.1.2 Scarred Uterus
The signs and symptoms of uterine rupture in patients with a previously scarred uterus differ from patients without a uterine scar [200]. Uterine rupture at the site of a previous uterine scar is typically less violent and less dramatic than a spontaneous or traumatic rupture because of their relatively reduced vascularity. The most common sign in women with previous uterine scar is lower abdominal tenderness. In women without a scar, shock is the most common sign, followed by uterine bleeding, severe abdominal pain, and easily palpable fetal parts. Severe abdominal pain is common to both groups of women with and without a uterine scar.
16.6.1.3 Incomplete and Silent Rupture
In incomplete rupture, the symptoms can be minimal and so obscured as to lead us to almost inevitable diagnostic errors. Silent antepartum rupture of the uterus is usually associated with a previous uterine scar, produced by Cesarean section, myomectomy, or perforation of the uterus at the time of curettage. Spontaneous silent rupture of the intact uterus is exceptionally rare in the antenatal period, and if it occurs the rupture usually involves the uterine fundus in patients of high parity. In one study, 4.5 % of patients in this study had no signs and symptoms and were incidentally found to have a ruptured uterus [201].
16.6.1.4 Delayed Presentation
Delayed presentation is possible if uterine perforation is “covered.” The rupture may be covered by small intestine, therefore preventing acute massive bleeding. Therefore, vital signs and laboratory data could be stable. Covering by the small intestine may also prevent amniotic rupture or amniotic cavity protrusion, which may explain the initial absence of a fetal heart rate pattern indicative of cord troubles (Fig. 16.5). In this case, the pouch of Douglas was closed, possibly due to the previous laparotomy, prohibiting blood retention [203].
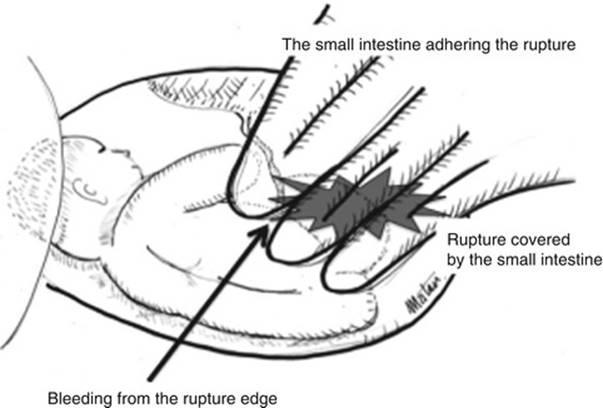
Fig. 16.5
Schematic diagram of the laparotomy findings. The uterine rupture was not initially discernible. Bleeding was observed from the rupture edge (arrow). The small intestine tightly adhered to the anterior uterine wall over the uterine rupture. After separating the small intestine, uterine rupture became evident. Amniotic membrane beneath the rupture site remained intact [203]
One article described uterine rupture occluded by “fetal legs.” Blihovde et al. [204] described a prelabor primiparous uterine rupture at the 32nd week of gestation, with the ruptured site being occluded by the fetal legs. There was abdominal pain but without vaginal bleeding, hemodynamic instability, or fetal compromise. CT revealed the uterine rupture occluded by the protruding fetal legs from the ruptured site, which was confirmed by laparotomy. The fetal legs, protruding through the rupture and occluding it, masked the symptoms and signs of the rupture, delaying the diagnosis.
16.6.1.5 Spinal Anesthesia
There have been concerns that the use of epidural analgesia may mask clinical symptoms (mostly abdominal pain) causing delayed diagnosis of uterine rupture [188]. The most common sign of uterine rupture is non-reassuring fetal heart rate pattern with variable deceleration [205]. Other findings are more variable and include abdominal pain, vaginal bleeding, and hypovolemia. Epidural analgesia rarely masks the signs and symptoms of uterine rupture, and in fact sudden development of “breakthrough pain” under epidural analgesia may improve the specificity of abdominal pain as a symptom of uterine rupture in patients attempting vaginal birth after previous uterine surgery [205].
16.6.2 Physical Examination
A physical examination reveals tenderness in the middle of lower abdomen with or without guarding. Vaginal bleeding can be present. Blood pressure depends on the rate of uterine bleeding, and the patient can be hypotensive with increased pulse rate. There is recommendation that clinicians should consider the diagnosis of uterine rupture when a patient presents with abdominal pain, even without evidence of hypovolemia, vaginal bleeding, contractions, or fetal compromise [203, 204].
Shoulder pain (Kehr’s sign) is a valuable sign of intraperitoneal blood in subdiaphragmatic region. Even a small amount can cause this symptom, but it is important to realize that it may be 24 h or longer after the bleeding has occurred before blood will track up under the diaphragm, and some cases of acute massive intraperitoneal bleeding may not initially have shoulder pain. Sooner or later, however, shoulder pain will usually appear, and it is in the doubtful cases with a slow leak of blood into the peritoneal cavity over a period of 2 or 3 days that such referred pain is of great diagnostic value.
If there is sufficient cervical dilatation, the vaginal examination may reveal intestinal loops or parts of the greater omentum in the uterine cavity. There is also considerable abdominal distension with dyspnea, caused by the compression of the thoracic cavity.
Postpartum fever ≥38 °C after Cesarean delivery is associated with an increased risk of uterine rupture during a subsequent trial of labor [206].
Antepartum hemorrhage (APH), often indicates uterine rupture [192] and may occur in association with shoulder tip pain due to hemoperitoneum. APH was documented in 33 % (2/6) of posterior uterine ruptures [191]. With posterior uterine rupture, bleeding may be concealed, as described in two earlier cases where signs of hypovolemia developed, each with a large concealed hemoperitoneum [147, 188]. It should be kept in mind that maternal pulse and blood pressure remained could remain within normal limits despite massive uterine rupture, demonstrating the potentially misleading capacity for compensation in an otherwise fit patient. In 33 % (2/6) of posterior uterine ruptures, women reported persistent abdominal pain [147, 191].
If the fetus is partly or completely outside the ruptured uterus, especially if the rupture is on the anterior wall, hard mass can be palpated [184].
16.7 Diagnosis
Around 30 % of patients are diagnosed with uterine rupture preoperatively [37, 157]. Laboratory findings should include hemoglobin which is lowered, and the exact value and dynamics of its decrease depend on the intensity of uterine wall bleeding. Since fetal heart abnormalities are one of the most common features in patients during labor [24], measurement of possible fetal heart abnormalities in laboring patients should be taken as a potential sign of danger [178].
16.7.1 Transvaginal/Transabdominal Ultrasound
A transvaginal and transabdominal ultrasound should be performed to search direct and indirect findings of suspected uterine rupture. Direct signs are thinned wall with bulging of fetal parts (Fig. 16.6) or for visualization of the rupture. The fetus can be partly or completely out of the uterus (Fig. 16.7). Indirect signs are free peritoneal fluid (blood) especially in the pouch of Douglas, extraperitoneal hematoma, intrauterine blood, empty uterus, gestational sac above the uterus (Fig. 16.8), and large uterine mass with gas bubbles [183, 184, 207].

Fig. 16.6
An abdominal ultrasound image of the uterine wall and the fetal minor part. Small arrow indicates a thin uterine wall, which is slightly bulging. Beneath the thin uterine wall, a fetal minor part (large arrow) is visible, which was palpated as a hard mass through the abdomen [184]

Fig. 16.7
Ultrasound image demonstrating contracted uterus (lower) with fetal extremities and amniotic sac outside the uterus [183]

Fig. 16.8
Ultrasound image demonstrating contracted uterus, endometrial stripe, and no intrauterine gestation, with the placental tissue above and bladder to the right [183]
16.7.2 Abdominal CT
Abdominal CT scan should be done in unequivocal cases such as intestinal adhesions over uterine rupture delaying diagnosis. It is seen as focal disruption of the myometrium along with hemoperitoneum (Fig. 16.9). Other signs (see direct and indirect signs) such as fetal parts or hemoperitoneum outside of the uterus can be seen (Figs. 16.10, 16.11 and 16.12).
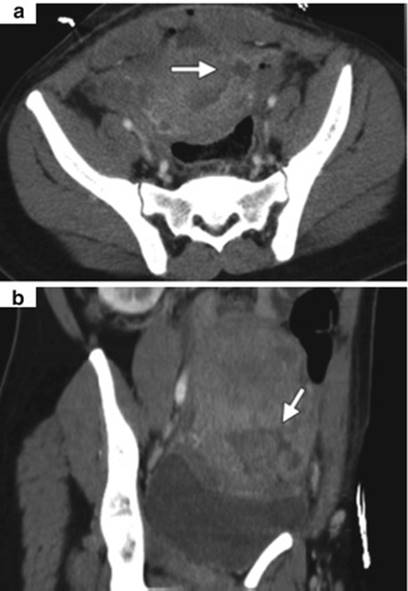
Fig. 16.9
Partial uterine rupture in a 29-year-old woman. Axial (a) and coronal oblique (b) contrast-enhanced CT images obtained 4 days after Cesarean delivery show disruption of the myometrium (arrow) in the left side of the lower uterine segment, a finding depicted as a hypoattenuating band in the myometrium connecting the uterine cavity with a fluid collection in the left broad ligament and pelvis [208]

Fig. 16.10
Contrast CT scan of abdomen and pelvis of another patient showing a defect in the anterior wall of the uterus (arrow) and fluid collection with wall enhancement and adjacent fluid collection 2 weeks after elective Cesarean section with normal postoperative course [209]

Fig. 16.11
Axial CT scan of abdomen (the same patient as in Fig. 16.10) showing the measurement of fluid collection anterior to the uterus (arrow) [209]

Fig. 16.12
A 34-year-old woman with seven previous Cesarean deliveries and a history of scant prenatal care presented at 32 weeks. The CT scan revealed a fetal hand protruding through the lower uterine segment (arrow) [210]
16.7.3 Magnetic Resonance Imaging
The MRI appearance consists of a focal myometrial defect which may be filled with hematoma and an associated hemoperitoneum (Fig. 16.13). Uterine rupture is a surgical emergency, and MRI should only be considered when the diagnosis is inconclusive and the patient is hemodynamically stable [212].
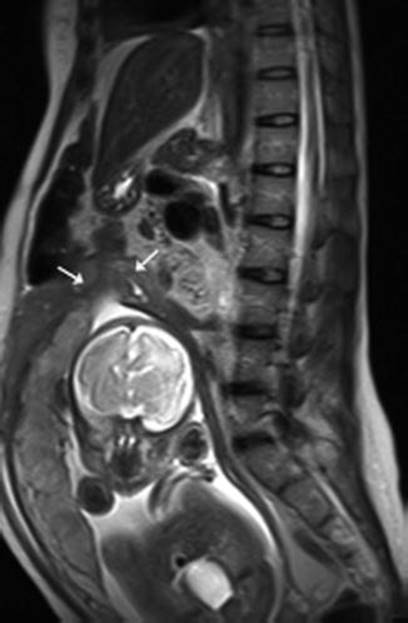
Fig. 16.13
A 35-year-old female patient in her third trimester with lower abdominal pain and with prior history of Cesarean delivery. Sagittal T2-weighted image shows a focal disruption at the fundus of the uterus (arrows) with associated hematoma. No part of the fetus protruded into the abdominal cavity [211]
Scar dehiscence is a separation that involves only a portion of the uterine scar in the lower uterine segment after Cesarean delivery; in these cases, an extensive fluid collection with air bubbles in the bladder flap as a sign of local infection can be seen. The differential diagnosis should consider bladder flap hematoma, endometritis, and normal Cesarean delivery incision changes, which are better depicted with MR imaging.
16.7.4 Uterine Tone Monitoring
Uterine tone monitoring is mandatory in patients with clinical presentation described. External monitoring (external tocodynamometer) demonstrate the classic sign of complete loss of uterine tone. In contrast, internal monitoring (internal pressure transducer) demonstrated an increase in uterine resting tone. Both techniques reveal a stepwise gradual decrease in contraction amplitude followed by a sudden onset of profound and prolonged fetal bradycardia in patients with rupture of an unscarred uterus at term – so-called staircase sign (Fig. 16.14) [213]. When internal monitoring was used, the intrauterine pressure catheter did not show a complete loss of resting tone (Fig. 16.15). In general, internal monitoring has better sensitivity for the detection of both fetal heart rate and uterine contraction, consistent with the published reports of the persistence of uterine contraction and increased resting tone in cases of rupture monitored by intrauterine catheter – findings that were not observed with external monitoring [39, 178]. However, few papers in the literature actually documented the type of uterine monitoring used. Furthermore, the uterine contraction pattern may differ depending upon the presence or absence of a uterine scar, or with the site and direction of rupture.

Fig. 16.14
Uterine contraction pattern during rupture of an unscarred uterus at term. External cardiotocogram was used for the tracing. Black arrows show the gradual decrease of the amplitude of uterine contractions (staircase sign). Black arrowhead with dashed body shows prolonged fetal bradycardia [213]
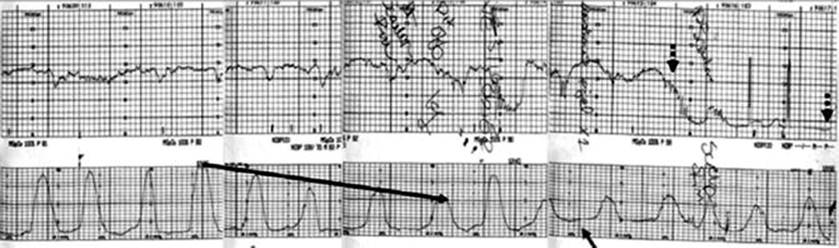
Fig. 16.15
Uterine contraction pattern of another case during term rupture of an unscarred uterus. Intrauterine pressure catheter was used for the tracing. Black arrow shows the gradual decrease of the amplitude of uterine contractions (staircase sign). Black arrowheads with dashed body show prolonged fetal bradycardia. Gray arrow shows increased resting tone [213]
Bradycardia is the most common fetal heart rate abnormality seen in cases of uterine rupture [178, 214–216] and may occur as a result of cord compression within the uterine rupture, loss of uterine perfusion, or placental abruption. This staircase pattern appears to be a unique combination of fetal heart rate pattern and uterine contraction pattern that may be of value in diagnosing uterine rupture. Fetal bradycardia starts right after or several minutes after staircase sign [213]. CTG abnormalities are associated with 55–87 % of uterine ruptures [217]. Other recognized signs of uterine rupture include loss of station of presenting part and new inefficient contractility [218].
16.8 Treatment
16.8.1 Perioperative Management
Once a diagnosis of uterine rupture is established, the immediate stabilization of the mother and the delivery of the fetus are imperative. After securing the airway and adequately ventilating the patient with oxygen, careful and immediate attention must be paid to correct hypovolemia. Patients should have multiple, preferably large-bore, intravenous catheters placed with vigorous fluid resuscitation and blood product replacement. In a study from Yemen, antibiotics were used in 100 %, 32.4 % received prophylaxis against gas gangrene, and 32.4 % received antitetanic serum [9].
The use of prophylactic antibiotics is controversial; Schrinsky and Benson state that they have no value [40], while others recommend their use because 30 patients (23 %) in one series (19 with an unscarred uterus and 11 with a previously scarred uterus) had intraperitoneal sepsis at the time of laparotomy [42]. More importantly, Gaffin et al. state that hypovolemic shock may lead to invasion of gram-negative bacteria from the ischemic bowel mucosa to the bloodstream, complicating the picture with endotoxemia and septic shock [219].
16.8.2 Operative Treatment
In 1932, Mahfouz urged conservative treatment whenever possible [220], but nowadays the key to successful treatment is early surgical intervention.
The time available for successful intervention after frank uterine rupture and before the onset of major fetal morbidity is only 10–37 min [49, 74, 216, 221, 222].
After the fetus is successfully delivered, the type of surgical treatment for the mother should depend on the following factors:
· Type of uterine rupture
· Extent of uterine rupture
· Degree of hemorrhage
· General condition of the mother
· Future childbearing
16.8.2.1 Suture Repair
Uterine bleeding is typically most profuse when the uterine tear is longitudinal rather than transverse. Conservative surgical management involving uterine suture repair (Figs. 16.16 and 16.17) should be reserved for women who have the following findings:

Fig. 16.16
The ruptured and contracted uterus found during emergent exploration [183]

Fig. 16.17
The line of uterine rupture, extending inferiorly from the left side of the previous lower segment scar [183]
· Desire for future childbearing [223]
· Low-transverse uterine rupture
· No extension of the tear to the broad ligament, cervix, or paracolpos
· Easily controllable uterine hemorrhage
· Good general condition
· No clinical or laboratory evidence of an evolving coagulopathy
Repair of a ruptured uterus is achieved in 13–74 % of cases [4, 28, 177, 178, 224]. Suture repair in general carries a recurrence risk of uterine rupture of 4–19 % at a subsequent pregnancy [31, 225, 226]. Therefore, it is recommended that women with a previous suture repair of uterine rupture undergo an elective Cesarean delivery as soon as fetal lung maturity can be demonstrated [227–230]. There are cases where pregnancy was undisturbed until 37 weeks and then Cesarean section performed [231]. Recommendations are not strong because there are no prospective studies. The type of rupture dictates the type of uterine repair. In one study, the percentage of patients with simple repair of the uterus was significantly higher in the previously scarred uterus group (90.2 %) when compared to the previously unscarred uterus group (57.5 %). Hysterectomy was performed in 25 % of the patients with previously unscarred uterus, which was significantly higher than the 9.8 % in patients with previously scarred uterus [33].
16.8.2.2 Hysterectomy
Hysterectomy should be considered the treatment of choice in several indications:
· Intractable uterine bleeding
· Uterine rupture sites – multiple, longitudinal, or low lying
· Placenta percreta
· Irremediable uterine atony/accreta
· Probability of cervical cancer
Total Abdominal Hysterectomy
Total abdominal hysterectomy is definitive procedure unless cardiovascular decompensation necessitates subtotal abdominal hysterectomy or simple suture repair with/without bilateral tubal ligation [232–234]. Previous studies support total hysterectomy because of the probability of cervical cancer in the cervical stump and increased rate of bleeding and discharge [235, 236]. The cervical malignancy rate was 0.39–1.9 %. Their rate has currently decreased to 0.1–0.15 % due to cytological surgery [237]. It was also found that although the difference was not statistically significant, the amount of blood loss, duration of operation, and rate of maternal deaths, ABO need for blood transfusion and reoperation were higher in the total hysterectomy group [237]. Hysterectomy rate differs significantly in the range of 6–83 % [4, 28, 74, 143, 177, 178, 224, 238, 239]. In a study by Leung et al., 19 % of patients required hysterectomy. Sixty-eight percent of hysterectomies were performed because the uterus was not deemed repairable, 21 % for irremediable uterine atony, and 5 % because of placenta accreta [49].
Placenta percreta is additional therapeutic problem if present during spontaneous uterine rupture. Up to 1966, there were 33 cases published [240], and in the period from 1966 to 2000, there were only 40 cases reported worldwide [241]. In cases of spontaneous rupture of the uterus due to placenta percreta, partial manual removal and hysterectomy showed 20 % mortality, while hysterectomy with no attempt at manual removal resulted in 100 % survival. When the adherent placenta was left in situ, 67 % succumbed. Clearly, the treatment of choice is total abdominal hysterectomy with no attempt at manual removal [240, 242–245].
Subtotal Hysterectomy
Subtotal hysterectomy is the preferred operation when shorter operation is indicated, as in hemodynamic instability or cardiovascular decompensation to minimize mortality and morbidity [237]. In this study by Özden et al., this recommendation was for general emergency hysterectomies, not only spontaneous uterine ruptures which represented 10 % of cases [237]. In patients with spontaneous uterine rupture, studies show that total abdominal hysterectomy was done in 14 % women, subtotal hysterectomy in 5–22 %, uterine repair with bilateral tubal ligation in 25–45 %, and uterine repair without bilateral tubal ligation in 39 % of patients [9, 12].
During operation, the placenta should be examined and evacuated. It can be found in the abdominal cavity or placed intrauterine. The amniotic sac can be intact (Fig. 16.18) [223, 246] or disrupted.

Fig. 16.18
Intraoperative photograph showing the uterus (lower part of operative field), the gestational sac (on the left), and the placenta (upper right) after opening the abdomen [246]
16.8.2.3 First Trimester
Case reports on the management of uterine rupture in the first trimester are limited. Often, the clinical condition of the patients requires an emergency hysterectomy. However, there have been reports with conservation of the uterus. A midgestational uterine rupture was repaired using fibrin-coated collagen fleece, allowing the successful continuation of the pregnancy [247].
16.8.2.4 Elective Cesarean Section
A recurrent uterine rupture rate of 4–19 % has been noted in patients with a prior repair [28, 54, 248, 249]. For this reason, it has been recommended that women with a previous uterine rupture undergo an elective Cesarean delivery as soon as fetal lung maturity can be demonstrated [224, 250]. All studies recommend planned Cesarean delivery [64, 156, 228, 251]. Delivery between 37 and 38 weeks is recommended for patients with a history of ruptured lower uterine scar, while those with a history of ruptured classical scar or previous uterine rupture, the opinion varies as to the time of delivery. Some surgeons deliver at 35 weeks, while others recommend admission to the hospital 1 week prior to the gestational age at which labor started in the previous pregnancy [54, 55].
On the contrary, a case series described 18 pregnancies, occurring in 15 patients in whom a simple repair of a ruptured gravid uterus had been previously performed. Seventeen of these pregnancies had a successful outcome, and there were no cases of recurrent rupture [252]. Therefore, there is evidence that a patient with previous uterine rupture can carry another pregnancy. This chance appears to increase if the uterus is closed with a double-layer suture [94]. It is also important to note that Weingold et al. in 1966 found that 29 % (2/7) of patients who underwent repair of a ruptured uterus later presented with another rupture in a subsequent pregnancy [199]. In the last 50 years, there is a significant improvement in diagnostic accuracy due to modern imaging modalities and diagnostic laparoscopy; therefore, this outcome should be analyzed cautiously.
16.9 Prognosis
Maternal and perinatal mortality vary significantly between developed and developing countries. Also these rates are highly variable in the same country especially between cities and rural areas. Due to the rarity of the disease and improvement in diagnostic and therapeutic modalities, the mortality was also decade dependent.
16.9.1 Maternal Outcome
16.9.1.1 Maternal Morbidity
The maternal morbidity rate ranges from 11.8 to 46.2 % [40, 202, 253]. Commonly reported maternal morbidity includes hemorrhage and shock, overall 46 %; infection (wound infection, 13.8 %; peritonitis, 10.2 %; tubo-ovarian abscess or urinary tract infection, 19.8 %; pelvic inflammatory disease, 4.3 %; respiratory infections including pneumonia, 2.2 %; and tetanus, 2 %); vesicovaginal fistula, 6.6 %; pelvic hematoma (mostly in the broad ligament), 19.2 %; fever, 21.7 %; and paralytic ileus, 18.9 %.
Complications of surgery such as injury to the bladder and ureter, dehiscence, and hernia have been described. Less commonly, hematuria, renal failure, disseminated intravascular coagulation (DIC), atelectasis, thrombophlebitis, pulmonary and cerebral embolism, and intestinal obstruction are reported as complications of uterine rupture.
In a series reported by Eden et al., 58 % of patients with uterine rupture required five or more units of blood [4]. In the study by Weingold et al. in 1966, 29 % (2/7) of patients who underwent repair of a ruptured uterus later presented with another rupture in a subsequent pregnancy and one of these women died [199].
16.9.1.2 Maternal Mortality
Maternal mortality as a consequence of uterine rupture occurs at a rate of 0–1 % [90] in developed countries, but the mortality rates in developing countries are 2–8 % [8, 12, 194, 196, 233, 254–257] and even 11 % reported in one Ethiopian study from 2002 [258]. The availability of modern medical facilities in developed nations is likely to account for this difference in maternal outcomes.
Maternal mortality depends on several other factors. In a South African study from 1976, with the mortality rate 8.5 % due to the rupture of an unscarred uterus, deaths could be further subdivided into mortality for women with longitudinal uterine tears (8.2 %), transverse tears (4 %), posterior wall tears (13 %), and multiple uterine tears (25 %). Golan et al. reported no deaths among 32 mothers who experienced rupture of a scarred uterus compared with 15 % (9/61) of women with an intact uterus [28]. Mokgokong and Marivate noted that the maternal mortality rate associated with uterine rupture largely depends on whether the diagnosis is established before (4.5 %) or after delivery (10.4 %) [238].
16.9.2 Fetal Outcome
16.9.2.1 Fetal Morbidity
It has been shown that significant neonatal morbidity occurred in women with uterine rupture when more than 18 min elapsed between the onset of prolonged decelerations and delivery [49]. Others claim that the time available for successful intervention after frank uterine rupture and before the onset of major fetal morbidity is 10–37 min [49, 74, 216, 221, 222].
Fetal Hypoxia or Anoxia
Leung et al. found that 5 % of neonates born to women who had uterine ruptures developed neonatal asphyxia (defined as umbilical-artery pH <7 with seizures and multiorgan dysfunction). No neonate had clinically significant perinatal morbidity when delivery was accomplished within 17 min of an isolated and prolonged deceleration of fetal heart rate. If severe late decelerations preceded prolonged deceleration, perinatal asphyxia was observed as soon as 10 min from the onset of the prolonged deceleration to delivery [49]. In a study by Menihan, 55 % (6/11) of fetuses born after uterine rupture had bradycardias between 18 and 37 min prior to delivery. Although the rate of fetal acidosis was high (91 %), no permanent neurological injuries or neonatal deaths occurred [216]. Bujold and Gauthier found that, even with rapid (<18 min) intervention between prolonged deceleration in fetal heart rate and delivery, 10 % (1/10) of neonates developed hypoxic-ischemic encephalopathies with impaired motor development. They concluded that, though rapid intervention did not always prevent severe metabolic acidosis and serious neonatal disease, it probably did limit the occurrence of neonatal death [92]. The incidence of hypoxic-ischemic encephalopathy associated with uterine rupture in another study was 5 % (1/20) [58].
Fetal Acidosis
In 99 cases of uterine rupture, Leung et al. found that 43 % had an umbilical-artery pH <7, and 58 % of these newborns had a pH <6.8. In association with these pH levels, 39 % had 5-min Apgar scores of <7, and 12 % of whom had 5-min Apgar scores of <3 [49]. Menihan found that 91 % who were born after uterine rupture had an umbilical-artery cord pH level <7.0, and 45 % had 5-min Apgar scores <7. The most important factor for the development of fetal acidosis was complete extrusion of the fetus and placenta into the maternal abdomen [216].
16.9.2.2 Fetal Mortality
Fetal mortality is reported in the range of 54.3–81.7 % [9, 40, 194, 196, 233, 257], and 91–93 % found in Pakistan and Uganda [7, 12]. In the study by Al Salem et al., the perinatal mortality rate was two times lower (157/1,000) in the scarred uterus group, which is significantly lower than the perinatal mortality (372/1,000) in the unscarred uterus group [33]. Smith et al. found that the overall risk of perinatal death due to uterine rupture was 1/2,100 and uterine rupture was three times more likely to result in death of the infant if the delivery took place in a hospital with <3,000 births a year (1/1,300) compared to 1/4,700 in hospitals with >3,000 births a year [259].
Fetal distress and neonatal demise resulting from uterine rupture is related to placental abruption and hypovolemia resulting in placental hypoperfusion, which develops rapidly as is evident from previous instances of posterior rupture. Prompt delivery resulted in fetal salvage before fetal compromise could develop.
References
1.
Trask JD. A statistical inquiry into the causes, symptoms, pathology, and treatment of rupture of the uterus. Am J Med Sci. 1848;15:383–418.
2.
Lewers AH. Rupture of the uterus during pregnancy, with notes of a case. Br Med J. 1887;1:58–60.PubMedCentralPubMed
3.
Baisch D. Beitr z Geburtsh v Gynäk. 1903;7:249.
4.
Eden RD, Parker RT, Gall SG. Rupture of the gravid uterus: a 53-year review. Obstet Gynecol. 1986;68:671–4.PubMed
5.
Deneke F. Ruptured uterus in Ethiopia. Int J Gynaecol Obstet. 1996;54:175–6.PubMed
6.
Chamiso B. Rupture of pregnant uterus in Shashemene General Hospital, south Shoa, Ethiopia (a three year study of 57 cases). Ethiop Med J. 1995;33:251–7.PubMed
7.
Khan S, Parveen Z, Begum S, Alam I. Uterine rupture: a review of 34 cases at Ayub Teaching Hospital Abbottabad. J Ayub Med Coll Abbottabad. 2003;15:50–2.PubMed
8.
Groen GP. Uterine rupture in rural Nigeria: review of 144 cases. Obstet Gynecol. 1974;44:682–7.PubMed
9.
Dhaifalah I, Santavy J, Fingerova H. Uterine rupture during pregnancy and delivery among women attending the Al-Tthawra Hospital in Sana’a City Yemen Republic. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2006;150:279–83.PubMed
10.
Konje JC, Odukoya AA, Ladipo OA. Ruptured uterus in Ibadan, a twelve year review. Int J Gynaecol Obstet. 1990;32:207–13.PubMed
11.
Balde MD, Breitabach GP, Bastert G. Uterine rupture - an analysis of 81 cases in Conakry, Guinea. Int J Gynecol Obstet. 1990;322:223–7.
12.
Kadowa I. Ruptured uterus in rural Uganda: prevalence, predisposing factors and outcomes. Singapore Med J. 2010;51:35–8.PubMed
13.
Rendle-Short CW. Rupture of the gravid uterus in Uganda. Am J Obstet Gynecol. 1960;79:1114–20.PubMed
14.
El Mansouri A. Accouchements sur uterus cicatriciel. Apropos de 150 cas. Rev Fr Gyencol Obstet. 1994;89:606–12.
15.
Ahmed SM, Daffalla SE. Incidence of uterine rupture in a teaching hospital, Sudan. Saudi Med J. 2001;22:757–61.PubMed
16.
Nyengidiki TK, Allagoa DO. Rupture of the gravid uterus in a tertiary health facility in the Niger delta region of Nigeria: a 5-year review. Niger Med J. 2011;52:230–4.PubMedCentralPubMed
17.
Veena P, Habeebullah S, Chaturvedula L. A review of 93 cases of ruptured uterus over a period of 2 years in a tertiary care hospital in South India. J Obstet Gynaecol. 2012;32:260–3.PubMed
18.
Ibha K, Poonam G, Sehgal A, Kamala D. Rupture of gravid uterus: experience at an Urban Medical Centre in Northern India. J Obstet Gynaecol India. 2003;53:558–62.
19.
Agboola A. Rupture of the uterus. Niger Med J. 1977;12:19–20.
20.
Lema VM, Ojwang SB, Wanjala SH. Rupture of the gravid uterus: a review. East Afr Med J. 1991;68:430–41.PubMed
21.
Rahman J, Al-Sibai MH, Rahman MS. Rupture of the uterus in labor. A review of 96 cases. Acta Obstet Gynecol Scand. 1985;64:311–5.PubMed
22.
Al-Rubaei S. A 10 years review of rupture pregnant uterus in Basra maternity and child hospital. Al-Qadisiah Med J. 2011;7:9–20.
23.
Vedat A, Hasan B, Ismail A. Rupture of the uterus in labor: a review of 150 cases. Isr J Med Sci. 1993;29:639–43.PubMed
24.
Rouzi AA, Hawaswi AA, Aboalazm M, et al. Uterine rupture incidence, risk factors, and outcome. Saudi Med J. 2003;24:37–9.PubMed
25.
Padhye SM. Rupture of the pregnant uterus – a 20 year review. Kathmandu Univ Med J. 2005;3:234–8.
26.
Lynch JC, Pardy JP. Uterine rupture and scar dehiscence. A five year survey. Anaesth Intensive Care. 1996;24:699–704.PubMed
27.
Mohamed K. A 5 year review of rupture of the pregnant uterus in Harare, Zimbabwe. J Obstet Gynaecol. 1987;7:192–6.
28.
Golan A, Sandbank O, Robin A. Rupture of the pregnant uterus. Obstet Gynecol. 1980;56:549–54.PubMed
29.
Roopnarinesingh S, Suratsingh J. Rupture of the gravid uterus in Trinidad. West Indian Med J. 1980;29:53–6.PubMed
30.
Al-Jufairi ZA, Sandhu AK, Al-Durazi KA. Risk factors of uterine rupture. Saudi Med J. 2001;22:702–4.PubMed
31.
Ahmadi S, Nouira M, Bibi M, et al. Uterine rupture of the unscarred uterus. About 28 cases. Gynecol Obstet Fertil. 2003;31:713–7.PubMed
32.
Chibber R, El-Saleh E, Al Fadhli R, et al. Uterine rupture and subsequent pregnancy outcome–how safe is it? A 25-year study. J Matern Fetal Neonatal Med. 2010;23:421–4.PubMed
33.
Al Salem MH, Makhseed M, Ahmed MA, Gupta M. Rupture of the gravid uterus: experience of the Maternity Hospital, Kuwait. Med Princ Pract. 2000;9:97–105.
34.
Fedorkow DM, Nimrod CA, Taylor PJ. Ruptured uterus in pregnancy: a Canadian hospital’s experience. Can Med Assoc J. 1987;137:27–9.
35.
Chen KC, Hsieh TT. Rupture of gravid uterus: a eight-year clinical analysis and review of the literature. Changgeng Yi Xue Za Zhi. 1992;15:15–22.PubMed
36.
Gardiel F, Daly S, Turner MJ. Uterine rupture in pregnancy reviewed. Eur J Obstet Gynecol Rep Biol. 1994;56:107–10.
37.
Al Sakka M, Hamsho A, Khan L. Rupture of the pregnant uterus - a 21-year review. Int J Gynaecol Obstet. 1998;63:105–8.PubMed
38.
Chen LH, Tan KH, Yeo GS. A ten-year review of uterine rupture in modern obstetric practice. Ann Acad Med Singapore. 1995;24:830–5.PubMed
39.
Sweeten KM, Graves WK, Athanassiou A. Spontaneous rupture of the unscarred uterus. Am J Obstet Gynecol. 1995;172:1851–6.PubMed
40.
Schrinsky DC, Benson RC. Rupture of the pregnant uterus: a review. Obstet Gynecol Surv. 1978;33:217–32.PubMed
41.
Miller DA, Goodwin TM, Gherman RB, Paul RH. Intrapartum rupture of the unscarred uterus. Obstet Gynecol. 1997;89:671–3.PubMed
42.
Lachman E, Moodley J, Pitsoe SB, Philpott RH. Rupture of the gravid uterus. S Afr Med J. 1985;67:333–5.PubMed
43.
Ola ER, Olamijulo JA. Rupture of the uterus at the Lagos University Teaching Hospital, Lagos, Nigeria. West Afr J Med. 1998;17:188–93.PubMed
44.
Iloki LH, Okongo D, Ekoundzola JR. Uterine rupture in an African environment. 59 cases at the University Hospital Center in Brazzaville. J Gynecol Obstet Biol Reprod (Paris). 1994;23:922–5.
45.
Padyne SM. Rupture of the pregnant uterus – a 20 year review. Kathmandu Univ Med J. 2005;3:234–8.
46.
Ofir K, Sheiner E, Levy A, Katz M, Mazor M. Uterine rupture: differences between a scarred and an unscarred uterus. Am J Obstet Gynecol. 2004;191:425–9.PubMed
47.
Chazotte C, Cohen WR. Catastrophic complications of previous caesarean section. Am J Obstet Gynecol. 1990;163:738–42.PubMed
48.
Flamm BL, Newman LA, Thomas SJ, et al. Vaginal birth after caesarean delivery: results of a 5 year multicenter collaborative study. Obstet Gynecol. 1990;76:750–3.PubMed
49.
Leung AS, Leung EK, Paul RH. Uterine rupture after previous Cesarean delivery: maternal & fetal consequences. Am J Obstet Gynecol. 1993;169:945–50.PubMed
50.
Hamilton BE, Martin JA, Stton PD. Births in preliminary data for 2002. Nat Vital Stat Rep. 2003;51:1–20.
51.
American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 115: vaginal birth after previous Cesarean delivery. Obstet Gynecol. 2010;116(2 Pt 1):450–63.
52.
National Institutes of Health Consensus Development Conference Panel. National Institutes of Health Consensus Development conference statement: vaginal birth after Cesarean: new insights March 8–10, 2010. Obstet Gynecol. 2010;115:1279–95.
53.
Cowan RK, Kinch RA, Ellis B, Anderson R. Trial of labor following Cesarean delivery. Obstet Gynecol. 1994;83:933–6.PubMed
54.
Sheth SS. Results of treatment of rupture of the uterus by suturing. J Obstet Gynaecol Br Commonw. 1968;75:55–8.PubMed
55.
Lim AC, Lau WC, Fung HYM. Pregnancy after uterine rupture: a report of 5 cases and a review of the literature. Obstet Gynecol Surv. 2005;60:613–7.PubMed
56.
Chauhan SP, Magann EF, Wiggs CD, et al. Pregnancy after classic Cesarean delivery. Obstet Gynecol. 2002;100(5 Pt 1):946–50.PubMed
57.
Rosen MG, Dickinson JC, Westhoff CL. Vaginal birth after Cesarean: a metaanalysis of morbidity and mortality. Obstet Gynecol. 1991;77:465–70.PubMed
58.
Landon MB, Hauth JC, Leveno KJ, et al. Maternal and perinatal outcomes associated with a trial of labor after prior Cesarean delivery. N Engl J Med. 2004;351:2581–9.PubMed
59.
American College of Obstetricians and Gynecologists. ACOG practice bulletin no 5. Vaginal birth after previous Cesarean delivery. Clinical management guidelines for obstetrician-gynecologists. Int J Gynaecol Obstet. 1999;66:197–204.
60.
Naef 3rd RW, Ray MA, Chauhan SP, et al. Trial of labor after Cesarean delivery with a lower-segment, vertical uterine incision: is it safe? Am J Obstet Gynecol. 1995;172:1666–74.PubMed
61.
Adair CD, Sanchez-Ramos L, Whitaker D, et al. Trial of labor in patients with a previous lower uterine vertical Cesarean section. Am J Obstet Gynecol. 1996;174:966–70.PubMed
62.
Martin JN, Perry KG, Roberts WE, Meydrech EF. The case for trial of labor in the patient with a prior low-segment vertical Cesarean incision. Am J Obstet Gynecol. 1997;177:144–8.PubMed
63.
Shipp TD, Zelop CM, Repke JT, et al. Intrapartum uterine rupture and dehiscence in patients with prior lower uterine segment vertical and transverse incisions. Obstet Gynecol. 1999;94(5 Pt 1):735–40.PubMed
64.
William BG, Llyod-Smith JO, Gouws D, et al. The potential impact of classical Cesarean scar in Sub-Saharan Africa. PLoS Med. 2006;3:e262.
65.
Leung AS, Farmer RM, Leung EK, et al. Risk factors associated with uterine rupture during trial of labor after Cesarean delivery: a case-control study. Am J Obstet Gynecol. 1993;168:1358–63.PubMed
66.
Pruett KM, Kirshon B, Cotton DB. Unknown uterine scar and trial of labor. Am J Obstet Gynecol. 1988;159:807–10.PubMed
67.
Beall M, Eglinton GS, Clark SL, Phelan JP. Vaginal delivery after Cesarean section in women with unknown types of uterine scar. J Reprod Med. 1984;29:31–5.PubMed
68.
Grubb DK, Kjos SL, Paul RH. Latent labor with an unknown uterine scar. Obstet Gynecol. 1996;88:351–5.PubMed
69.
Lydon-Rochelle M, Holt VL, Easterling TR, Martin DP. Risk of uterine rupture during labor among women with a prior Cesarean delivery. N Engl J Med. 2001;345:3–8.PubMed
70.
Ravasia DJ, Wood SL, Pollard JK. Uterine rupture during induced trial of labor among women with previous Cesarean delivery. Am J Obstet Gynecol. 2000;183:1176–9.PubMed
71.
Zelop CM, Shipp TD, Repke JT, et al. Uterine rupture during induced or augmented labor in gravid women with one prior Cesarean delivery. Am J Obstet Gynecol. 1999;181:882–6.PubMed
72.
Tahilramaney MP, Boucher M, Eglinton GS, et al. Previous Cesarean section and trial of labor: factors related to uterine dehiscence. J Reprod Med. 1984;29:17–21.PubMed
73.
Phelan JP, Clark SL, Diaz F, Paul RH. Vaginal birth after Cesarean. Am J Obstet Gynecol. 1987;157:1510–5.PubMed
74.
Blanchette H, Blanchette M, McCabe J, Vincent S. Is vaginal birth after Cesarean safe? Experience at a community hospital. Am J Obstet Gynecol. 2001;184:1478–87.PubMed
75.
Bujold E, Blackwell SC, Gauthier RJ. Cervical ripening with transcervical foley catheter and the risk of uterine rupture. Obstet Gynecol. 2004;103:18–23.PubMed
76.
Hoffman MK, Sciscione A, Srinivasana M, et al. Uterine rupture in patients with a prior Cesarean delivery: the impact of cervical ripening. Am J Perinatol. 2004;21:217–22.PubMed
77.
Pettker CM, Pocock SB, Smok DP, et al. Transcervical foley catheter with and without oxytocin for cervical ripening: a randomized controlled trial. Obstet Gynecol. 2008;111:1320–6.PubMed
78.
Taylor DR, Doughty AS, Kaufman H, et al. Uterine rupture with the use of PGE2 vaginal inserts for labor induction in women with previous Cesarean sections. J Reprod Med. 2002;47:549–54.PubMed
79.
Flamm BL, Anton D, Goings JR, Newman J. Prostaglandin E2 for cervical ripening: a multicenter study of patients with prior Cesarean delivery. Am J Perinatol. 1997;14:157–60.PubMed
80.
Delaney T, Young DC. Spontaneous versus induced labor after a previous Cesarean delivery. Obstet Gynecol. 2003;102:39–44.PubMed
81.
Zelop CM, Shipp TD, Repke JT, et al. Effect of previous vaginal delivery on the risk of uterine rupture during a subsequent trial of labor. Am J Obstet Gynecol. 2000;183:1184–6.PubMed
82.
Caughey AB, Shipp TD, Repke JT, et al. Rate of uterine rupture during a trial of labor in women with one or two prior Cesarean deliveries. Am J Obstet Gynecol. 1999;181:872–6.PubMed
83.
Kayani SI, Alfirevic Z. Uterine rupture after induction of labour in women with previous caesarean section. Br J Obstet Gynaecol. 2005;112:451–5.
84.
Grobman WA, Gilbert S, Landon MB, et al. Outcomes of induction of labor after one prior Cesarean. Obstet Gynecol. 2007;109(2 Pt 1):262–9.PubMed
85.
Mercer BM, Gilbert S, Landon MB, et al. Labor outcomes with increasing number of prior vaginal births after Cesarean delivery. Obstet Gynecol. 2008;111(2 Pt 1):285–91.PubMed
86.
Gregory KD, Korst LM, Cane P, et al. Vaginal birth after Cesarean and uterine rupture rates in California. Obstet Gynecol. 1999;94:985–9.PubMed
87.
McMahon MJ, Luther ER, Bowes Jr WA, Olshan AF. Comparison of a trial of labor with an elective second Cesarean section. N Engl J Med. 1996;335:689–95.PubMed
88.
Rageth JC, Juzi C, Grossenbacher H. Delivery after previous Cesarean: a risk evaluation. Swiss Working Group of Obstetric and Gynecologic Institutions. Obstet Gynecol. 1999;93:332–7.PubMed
89.
Esposito MA, Menihan CA, Malee MP. Association of interpregnancy interval with uterine scar failure in labor: a case-control study. Am J Obstet Gynecol. 2000;183:1180–3.PubMed
90.
Stamilio DM, DeFranco E, Paré E, et al. Short interpregnancy interval: risk of uterine rupture and complications of vaginal birth after Cesarean delivery. Obstet Gynecol. 2007;110:1075–82.PubMed
91.
Shipp TD, Zelop CM, Repke JT, et al. Interdelivery interval and risk of symptomatic uterine rupture. Obstet Gynecol. 2001;97:175–7.PubMed
92.
Bujold E, Mehta SH, Bujold C, Gauthier RJ. Interdelivery interval and uterine rupture. Am J Obstet Gynecol. 2002;187:1199–202.PubMed
93.
Bujold E, Gauthier RJ. Risk of uterine rupture associated with an interdelivery interval between 18 and 24 months. Obstet Gynecol. 2010;115:1003–6.PubMed
94.
Bujold E, Bujold C, Hamilton EF, et al. The impact of a single-layer or double-layer closure on uterine rupture. Am J Obstet Gynecol. 2002;186:1326–30.PubMed
95.
Bujold E, Goyet M, Marcoux S, et al. The role of uterine closure in the risk of uterine rupture. Obstet Gynecol. 2010;116:43–50.PubMed
96.
Gyamfi C, Juhasz G, Gyamfi P, et al. Single- versus double-layer uterine incision closure and uterine rupture. J Matern Fetal Neonatal Med. 2006;19:639–43.PubMed
97.
Roberge S, Chaillet N, Boutin A, et al. Single- versus double-layer closure of the hysterotomy incision during Cesarean delivery and risk of uterine rupture. Int J Gynaecol Obstet. 2011;115:5–10.PubMed
98.
Miller DA, Diaz FG, Paul RH. Vaginal birth after Cesarean: a 10-year experience. Obstet Gynecol. 1994;84:255–8.PubMed
99.
Macones GA, Cahill A, Pare E, et al. Obstetric outcomes in women with two prior Cesarean deliveries: is vaginal birth after Cesarean delivery a viable option? Am J Obstet Gynecol. 2005;192:1223–9.PubMed
100.
Tahseen S, Griffiths M. Vaginal birth after two caesarean sections (VBAC-2)-a systematic review with meta-analysis of success rate and adverse outcomes of VBAC-2 versus VBAC-1 and repeat (third) caesarean sections. Br J Obstet Gynaecol. 2010;117:5–19.
101.
American College of Obstetricians and Gynecologists. ACOG practice bulletin no 54: vaginal birth after previous Cesarean. Obstet Gynecol. 2004;104:203–12.
102.
Landon MB, Spong CY, Thom E, et al. Risk of uterine rupture with a trial of labor in women with multiple and single prior Cesarean delivery. Obstet Gynecol. 2006;108:12–20.PubMed
103.
Morimatsu Y, Matsubara S, Higashiyama N, et al. Spontaneous uterine rupture during pregnancy soon after a laparoscopic adenomyomectomy. Reprod Med Biol. 2007;6:175–7.
104.
Dubuisson JB, Fauconnier A, Deffarges JV, et al. Pregnancy outcome and deliveries following laparoscopic myomectomy. Hum Reprod. 2000;15:869–73.PubMed
105.
Golan D, Aharoni A, Gonen R, et al. Early spontaneous rupture of the post myomectomy gravid uterus. Int J Gynaecol Obstet. 1990;31:167–70.PubMed
106.
Brown AB, Chamberlain R, Te Linde RW. Myomectomy. Am J Obstet Gynecol. 1956;71:759–63.PubMed
107.
Garnet JD. Uterine rupture during pregnancy. An analysis of 133 patients. Obstet Gynecol. 1964;23:898–905.PubMed
108.
Seinera P, Farina C, Todros T. Laparoscopic myomectomy and subsequent pregnancy: results in 54 patients. Hum Reprod. 2000;15:1993–6.PubMed
109.
Nezhat CH, Nezhat F, Roemisch M, et al. Pregnancy following laparoscopic myomectomy: preliminary results. Hum Reprod. 1999;14:1219–21.PubMed
110.
Seracchioli R, Rossi S, Govoni F, et al. Fertility and obstetric outcome after laparoscopic myomectomy of large myomata: a randomized comparison with abdominal myomectomy. Hum Reprod. 2000;15:2663–8.PubMed
111.
Seracchioli R, Manuzzi L, Vianello F, et al. Obstetric and delivery outcome of pregnancies achieved after laparoscopic myomectomy. Fertil Steril. 2006;86:159–65.PubMed
112.
Kumakiri J, Takeuchi H, Itoh S, et al. Prospective evaluation for the feasibility and safety of vaginal birth after laparoscopic myomectomy. J Minim Invasive Gynecol. 2008;15:420–4.PubMed
113.
Sizzi O, Rossetti A, Malzoni M, et al. Italian multicenter study on complications of laparoscopic myomectomy. J Minim Invasive Gynecol. 2007;14:453–62.PubMed
114.
Oktem O, Gokaslan H, Durmusoglu F. Spontaneous uterine rupture in pregnancy 8 years after laparoscopic myomectomy. J Am Assoc Gynecol Laparosc. 2001;8:618–21.PubMed
115.
Daponte A, Nzewenga G, Dimopoulos KD, Guidozzi F. The use of vaginal misoprostol for second-trimester pregnancy termination in women with previous single Cesarean section. Contraception. 2006;74:324–7.PubMed
116.
Daponte A, Nzewenga G, Dimopoulos KD, Guidozzi F. Pregnancy termination using vaginal misoprostol in women with more than one caesarean section. J Obstet Gynaecol. 2007;27:597–600.PubMed
117.
Department of Health. www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsStatistics/DH_075697.
118.
Byrne P, Onyekwuluje T. Uterine rupture after termination of pregnancy with gemeprost. Br Med J. 1991;302:852.
119.
Norman JE. Uterine rupture during therapeutic abortion in the second trimester using mifepristone and prostaglandin. Br J Obstet Gynaecol. 1995;102:332–3.PubMed
120.
Phillips K, Berry C, Mothers AM. Uterine rupture during second trimester termination of pregnancy using mifepristone and a prostaglandin. Eur J Obstet Gynecol Reprod Biol. 1996;65:175–6.PubMed
121.
Letourneur B, Parant O, Tofani V, Berrebi A. Uterine rupture on unscarred uterus following labor induction for 2nd trimester termination of pregnancy with oral misoprostol: conservative management. J Gynecol Obstet Biol Reprod (Paris). 2002;31:371–3.
122.
Al-Hussaini TK. Uterine rupture in second trimester abortion in a grand multiparous woman. A complication of misoprostol and oxytocin. Eur J Obstet Gynecol Reprod Biol. 2001;96:218–9.PubMed
123.
Syed S, Noreen H, Kahloon LE, Chaudhri R. Uterine rupture associated with the use of intra-vaginal misoprostol during second-trimester pregnancy termination. J Pak Med Assoc. 2011;61:399–401.PubMed
124.
Khabbaz AY, Usta IM, El-Hajj MI, et al. Rupture of an unscarred uterus with misoprostol induction: case report and review of the literature. J Matern Fetal Med. 2001;10:141–5.PubMed
125.
Goyal V. Uterine rupture in second-trimester misoprostol-induced abortion after Cesarean delivery: a systematic review. Obstet Gynecol. 2009;113:1117–23.PubMed
126.
Pongsatha S, Tongsong T. Misoprostol for second trimester termination of pregnancies with prior low transverse Cesarean section. Int J Gynaecol Obstet. 2003;80:61–2.PubMed
127.
Willmott FJ, Scherf C, Ford SM, Lim K. Rupture of uterus in the first trimester during medical termination of pregnancy for exomphalos using mifepristone/misoprostol. Br J Obstet Gynaecol. 2008;115:1575–7.
128.
Daskalakis G, Papantoniou N, Mesogitis S, et al. Sonographic findings and surgical management of a uterine rupture associated with the use of misoprostol during second-trimester abortion. J Ultrasound Med. 2005;24:1565–8.PubMed
129.
Weeks A, Faundes A. Misoprostol in obstetrics and gynaecology. Int J Gynaecol Obstet. 2007;99:S156–9.PubMed
130.
Bagga R, Chaudhary N, Kalra J. Rupture in an unscarred uterus during second trimester pregnancy termination with mifepristone and misoprostol. Int J Gynecol Obstet. 2004;87:42–3.
131.
Malhotra N, Chanana C. Silent rupture of unscarred uterus: an unusual presentation at second trimester abortion. Arch Gynecol Obstet. 2007;275:283–5.PubMed
132.
Lee SL, Su JM, Shen WL, Chang FM. Unscarred uterine cervical rupture during second-trimester termination using misoprostol. Taiwan J Obstet Gynecol. 2007;46:445–7.PubMed
133.
Berghahn L, Christensen D, Droste S. Uterine rupture during second trimester abortion associated with misoprostol. Obstet Gynecol. 2001;98:976–7.PubMed
134.
Kim JO, Han JY, Choi JS, et al. Oral misoprostol and uterine rupture in the first trimester of pregnancy: a case report. Reprod Toxicol. 2005;20:575–7.PubMed
135.
Dickinson JE. Misoprostol for second-trimester pregnancy termination in women with a prior caesarean delivery. Obstet Gynecol. 2005;105:352–6.PubMed
136.
Walsh CA, Baxi LV. Rupture of the primigravid uterus: a review of the literature. Obstet Gynecol Surv. 2007;62:327–34.PubMed
137.
Dow M, Wax JR, Pinette MG, et al. Third-trimester uterine rupture without previous Cesarean: a case series and review of the literature. Am J Perinatol. 2009;26:739–44.PubMed
138.
Wada S, Kudo M, Minakami H. Spontaneous uterine rupture of a twin pregnancy after laparoscopic adenomyomectomy: a case report. J Minim Invasive Gynecol. 2006;13:166–8.PubMed
139.
Villa G, Mabrouk M, Guerrini M, et al. Uterine rupture in a primigravida with adenomyosis recently subjected to laparoscopic resection of rectovaginal endometriosis: case report. J Minim Invasive Gynecol. 2008;15:360–1.PubMed
140.
Padhye SM. Rupture uterus in primigravida: morbidity and mortality. Kathmandu Univ Med J. 2007;5:492–6.
141.
Banas T, Klimek M, Fugiel A, Skotniczny K. Spontaneous uterine rupture at 35 weeks’ gestation, 3 years after laparoscopic myomectomy, without signs of fetal distress. J Obstet Gynaecol Res. 2005;31:527–30.PubMed
142.
Walsh CA, Reardon W, Foley ME. Unexplained prelabor uterine rupture in a term primigravida. Obstet Gynecol. 2007;109:455.PubMed
143.
Kieser KE, Baskett TF. A 10-year population-based study of uterine rupture. Obstet Gynecol. 2002;100:749–53.PubMed
144.
Abbi M, Misra R. Rupture of uterus in a primigravida prior to onset of labor. Int J Fertil Womens Med. 1997;42:418–20.PubMed
145.
Azem F, Jaffa A, Lessing JB, Peyser MR. Uterine rupture with the use of a low-dose vaginal PGE2 tablet. Acta Obstet Gynecol Scand. 1993;73:316–7.
146.
Heckel S, Ohl J, Dellenbach P. Rupture of an unscarred uterus at full term after an intracervical application of dinoprostone (Prepidil) gel. Rev Fr Gynecol Obstet. 1993;88:162–4.PubMed
147.
Hawe JA, Olha KS. Posterior uterine rupture in a patient with a lower segment caesarean section scar complicating prostaglandin induction of labour. Br J Obstet Gynaecol. 1997;104:857–8.PubMed
148.
Kurdoglu M, Kolusari A, Yildizhan R, et al. Delayed diagnosis of an atypical rupture of an unscarred uterus due to assisted fundal pressure: a case report. Cases J. 2009;2:7966.PubMedCentralPubMed
149.
Feeney JK. Complications associated with high multiparity; a clinical study of 518 cases. J Ir Med Assoc. 1953;32:36–55.PubMed
150.
Suner S, Jagminas L, Peipert JF, Linakis J. Fatal spontaneous rupture of a gravid uterus: case report and literature review of uterine rupture. J Emerg Med. 1996;14:181–5.PubMed
151.
Marguilies D, Crapanzano JT. Rupture of the intact uterus. Obstet Gynecol. 1966;27:863–8.
152.
Yussman MH, Haynes DM. Rupture of the gravid uterus. A 12-year study. Obstet Gynecol. 1970;36(1):15–20.
153.
Aboyeji AP, Ijaiya MD, Yahaya UR. Ruptured uterus: a study of 100 consecutive cases in Ilorin, Nigeria. J Obstet Gynaecol Res. 2001;27:341–8.PubMed
154.
Okogbenin SA, Gharoro EP, Otoide VO, Okonta PI. Obstetric hysterectomy: fifteen years’ experience in a Nigerian tertiary centre. J Obstet Gynaecol. 2003;23:356–9.PubMed
155.
Olatunji AO, Sule-Odu AO, Adefuye PO. Ruptured uterus at Sagamu, Nigeria. Niger Postgrad Med J. 2002;9:235–9.PubMed
156.
Ofir K, Sheiner E, Levy A, et al. Uterine rupture: risk factors and pregnancy outcome. Am J Obstet Gynecol. 2003;189:1042–6.PubMed
157.
Beacham WD, Beacham DW, Webster HD, Fielding SL. Rupture of the uterus at New Orleans Charity Hospital. A report of 101 cases and comparison with the previously reported 96 cases. Am J Obstet Gynecol. 1970;106:1083–91.PubMed
158.
Menon KMK. Rupture of the uterus a review of 164 cases. J Obstet Gynecol Brit Comm. 1962;69:18–28.
159.
Yamani TY, Rouzi AA. Induction of labor with vaginal prostaglandin-E2 in grand multiparous women. Int J Gynecol Obstet. 1998;62:255–9.
160.
Gardeil F, Daly S, Turner MJ. Uterine rupture in pregnancy reviewed. Eur J Obstet Gynecol Reprod Biol. 1994;56:107–10.PubMed
161.
Leung F, Courtois L, Aouar Z, et al. Spontaneous rupture of the unscarred uterus during labor. Case report. Gynecol Obstet Fertil. 2009;37:342–5.PubMed
162.
Walsh CA, O’Sullivan RJ, Foley ME. Unexplained prelabor uterine rupture in a term primigravida. Obstet Gynecol. 2006;108(3 Pt 2):725–7.PubMed
163.
Nahum GG. Uterine anomalies. How common are they, and what is their distribution among subtypes? J Reprod Med. 1998;43:877–87.PubMed
164.
Gordon CA. Ruptured pregnancy in the closed rudimentary horn of a bicornuate uterus. Am J Obstet Gynecol. 1935;29:279–82.
165.
Tien DSP. Pregnancy in the rudimentary horn of the uterus. Review of the literature and report of one case. Chin Med J. 1949;67:485–8.
166.
Schauffler GC. Double uterus with pregnancy. J Am Med Assoc. 1941;117:1516–20.
167.
Nahum GG. Rudimentary uterine horn pregnancy. A case report on surviving twins delivered eight days apart. J Reprod Med. 1997;42:525–32.PubMed
168.
Ravasia DJ, Brain PH, Pollard JK. Incidence of uterine rupture among women with mullerian duct anomalies who attempt vaginal birth after Cesarean delivery. Am J Obstet Gynecol. 1999;181:877–81.PubMed
169.
Erez O, Dukler D, Novack L, et al. Trial of labor and vaginal birth after Cesarean section in patients with uterine Müllerian anomalies: a population-based study. Am J Obstet Gynecol. 2007;196:537.e1–11.
170.
Nahum GG. Uterine anomalies, induction of labor, and uterine rupture. Obstet Gynecol. 2005;106:1150–2.PubMed
171.
Gottschalk EM, Siedentopf JP, Schoenborn I, et al. Prenatal sonographic and MRI findings in a pregnancy complicated by uterine sacculation: case report and review of the literature. Ultrasound Obstet Gynecol. 2008;32:582–6.PubMed
172.
Frei KA, Duwe DG, Bonel HM, et al. Posterior sacculation of the uterus in a patient presenting with flank pain at 29 weeks of gestation. Obstet Gynecol. 2005;105:639–41.PubMed
173.
Rajiah P, Eastwood KL, Gunn ML, Dighe M. Uterine diverticulum. Obstet Gynecol. 2009;113:525–7.PubMed
174.
Friedman A, DeFazio J, DeCherney A. Severe obstetric complications after aggressive treatment of Asherman syndrome. Obstet Gynecol. 1986;67:864–7.PubMed
175.
Sun X, Xue M, Xiao S, et al. Uterine diverticulum complicating pregnancy diagnosed by ultrasound and uteroscopy. Int J Gynaecol Obstet. 2010;109:247–8.PubMed
176.
Phelan JP. Uterine rupture. Clin Obstet Gynecol. 1990;33:432–7.PubMed
177.
Plauché W, Von Almen W, Muller R. Catastrophic uterine rupture. Obstet Gynecol. 1984;64:792–7.PubMed
178.
Rodriguez MH, Masaki DI, Phelan JP, Diaz FG. Uterine rupture: are intrauterine pressure catheters useful in the diagnosis? Am J Obstet Gynecol. 1989;161:666–9.PubMed
179.
Uccella S, Cromi A, Bogani G, et al. Spontaneous prelabor uterine rupture in a primigravida: a case report and review of the literature. Am J Obstet Gynecol. 2011;205:e6–8.PubMed
180.
Gutman G, Baris HN, Hirsch R, et al. Loeys-Dietz syndrome in pregnancy: a case description and report of a novel mutation. Fetal Diagn Ther. 2009;26:35–7.PubMed
181.
Nassar A, Usta I, Finianos A, Kaspar H. Spontaneous uterine rupture following intercourse. Acta Obstet Gynecol Scand. 2004;83:114–5.PubMed
182.
Tan TL, Kolhe S, Shafik A. Spontaneous uterine rupture following intercourse in a scarred uterus. J Obstet Gynaecol. 2005;25:392.PubMed
183.
Albrecht K, Lam G. Preterm spontaneous uterine rupture in a non-labouring grand multipara: a case report. J Obstet Gynaecol Can. 2008;30:586–9.PubMed
184.
Matsubara S, Shimada K, Kuwata T, et al. Thin anterior uterine wall with incomplete uterine rupture in a primigravida detected by palpation and ultrasound: a case report. J Med Case Rep. 2011;5:14.PubMedCentralPubMed
185.
Rickards CE. Uterine rupture following Caesarean section. Br Med J. 1938;1:1359–61.PubMedCentralPubMed
186.
Hornung R. Z Gebutrtsh Gynak. 1929;95:580.
187.
Potter IW, Am J. Obstet Gynecol. 1930;19:289.
188.
Wang PH, Yuan CC, Chao HT, et al. Posterior uterine wall rupture during labour. Hum Reprod. 2000;15:1198–9.PubMed
189.
Figueroa R, Garry D, Mackenzie AP. Posterior uterine rupture in a woman with a previous Cesarean delivery. J Matern Fetal Neonatal Med. 2003;14:130–1.PubMed
190.
Singhal SR, Agarwal U, Sangwan K, et al. Intrapartum posterior uterine wall rupture in lower segment Cesarean section scarred uterus. Acta Obstet Gynecol Scand. 2005;84:196–7.PubMed
191.
Majumdar S, Warren R, Ifaturoti O. Fetal survival following posterior uterine wall rupture during labour with intact previous caesarean section scar. Arch Gynecol Obstet. 2007;276:537–40.PubMed
192.
Navaratnam K, Ulaganathan P, Akhtar MA, et al. Posterior uterine rupture causing fetal expulsion into the abdominal cavity: a rare case of neonatal survival. Case Rep Obstet Gynecol. 2011;2011:426127.PubMedCentralPubMed
193.
Buhimschi CS, Buhimschi IA, Patel S, et al. Rupture of the uterine scar during term labour: contractility or biochemistry? Br J Obstet Gynaecol. 2005;112:38–42.
194.
Malik HS. Frequency, predisposing factors and fetomaternal outcome in uterine rupture. J Coll Physicians Surg Pak. 2006;16:472–5.PubMed
195.
Fatima N. Rupture of uterus at term. J Coll Physicians Surg Pak. 1998;8:137–9.
196.
Rizwan N, Abbasi RM, Uddin SF. Uterine rupture, frequency of cases and fetomaternal outcome. J Pak Med Assoc. 2011;61:322–4.PubMed
197.
Ezegwui HU, Nwogu-Ikojo EE. Trends in uterine rupture in Enugu, Nigeria. J Obstet Gynaecol. 2005;25:260–2.PubMed
198.
Ricci JV. Rupture of the gravid uterus. In: Ricci JV (ed). Genealogy of gynecology. Philadelphia: Blakistan; 1950.
199.
Weingold AB, Sanford S, Sherman DH. Rupture of the gravid uterus. Surg Gynecol Obstet. 1966;125:1233–8.
200.
Van der Merwe JV, Ombelet WU. Rupture of the uterus: a changing picture. Arch Gynecol. 1987;240:159–71.PubMed
201.
Skelly HR, Duthie AM, Philpott RH. Rupture of the uterus: the preventable factors. S Afr Med J. 1976;50:505–9.PubMed
202.
Deaton JL, Maier D, Andreoli J. Spontaneous uterine rupture during pregnancy after treatment of Asherman’s syndrome. Am J Obstet Gynecol. 1989;160:1053–4.PubMed
203.
Kuwata T, Matsubara S, Usu R, et al. Intestinal adhesion due to previous uterine surgery as a risk factor for delayed diagnosis of uterine rupture: a case report. J Med Case Reports. 2011;5:523.PubMedCentral
204.
Blihovde L, Tawfik J, Hill DA. Prelabor third-trimester uterine rupture in an unscarred uterus with occlusion by fetal small parts: a case report. J Reprod Med. 2010;55:437–40.PubMed
205.
ACOG. Vaginal birth after previous Cesarean delivery. ACOG Pract Bull. 1999;5:558–65.
206.
Shipp TD, Zelop C, Cohen A, et al. Post-Cesarean delivery fever and uterine rupture in a subsequent trial of labor. Obstet Gynecol. 2003;101:136–9.PubMed
207.
Omers R, Ulbrich R, Schauer A, Kuhn W. Sonographic detection of an asymptomatic rupture of the uterus due to necrosis during the third trimester. Int J Gynecol Obstet. 1988;26:279–84.
208.
Sierra A, Burrel M, Sebastia C, et al. Utility of multidetector CT in severe postpartum hemorrhage. Radiographics. 2012;32:1463–81.PubMed
209.
Waseem M, Cunningham-Deshong H, Gernsheimer J. Abdominal pain in a postpartum patient. J Emerg Med. 2011;41:261–4.PubMed
210.
Eller AG, Fisher B. Images in clinical medicine. Diagnosis of uterine rupture on CT. N Engl J Med. 2009;360:170.PubMed
211.
Beddy P, Keogan MT, Sala E, Griffin N. Magnetic resonance imaging for the evaluation of acute abdominal pain in pregnancy. Semin Ultrasound CT MR. 2010;31:433–41.PubMed
212.
Vadnais M, Awtrey C, Pedrosa I. Breaking point: magnetic resonance imaging evaluation of an obstetric emergency. Am J Obstet Gynecol. 2009;200:e1–3.PubMed
213.
Matsuo K, Scanlon JT, Atlas RO, Kopelman JN. Staircase sign: a newly described uterine contraction pattern seen in rupture of unscarred gravid uterus. J Obstet Gynaecol Res. 2008;34:100–4.PubMed
214.
Sheiner E, Levy A, Ofir K, et al. Changes in fetal heart rate and uterine patterns associated with uterine rupture. J Reprod Med. 2004;49:373–8.PubMed
215.
Ridgeway JJ, Weyrich DL, Benedetti TJ. Fetal heart rate changes associated with uterine rupture. Obstet Gynecol. 2004;103:506–12.PubMed
216.
Menihan CA. Uterine rupture in women attempting a vaginal birth following prior Cesarean birth. J Perinatol. 1998;18(6 Pt 1):440–3.PubMed
217.
Guise JM, McDonagh MS, Osterweil P, et al. Systematic review of the incidence and consequences of uterine rupture in women with previous caesarean section. Br Med J. 2004;329:19–23.
218.
RCOG. Birth after previous Caesarean section, Green Top 45. Royal College of Obstetricians and Gynaecologists; 2007.
219.
Gaffin SL, Grinberg Z, Abraham C, et al. Protection against hemorrhagic shock in the cat by human plasma containing endotoxin specific antibodies. Surg Res. 1981;31:18–21.
220.
Mahfouz N. J Obstet Gynaecol Br Emp. 1932;39:743.
221.
Yap OW, Kim ES, Laros Jr RK. Maternal and neonatal outcomes after uterine rupture in labor. Am J Obstet Gynecol. 2001;184:1576–81.PubMed
222.
Bujold E, Gauthier RJ. Neonatal morbidity associated with uterine rupture: what are the risk factors? Am J Obstet Gynecol. 2002;186:311–4.PubMed
223.
Rana R, Puri M. Pre-labor silent rupture of unscarred uterus at 32 weeks with intact amniotic sac extrusion: a case report. Cases J. 2009;2:7095.PubMedCentralPubMed
224.
Spaulding LB, Gallup DC. Current concepts for management of rupture of the gravid uterus. Obstet Gynecol. 1979;54:437–41.PubMed
225.
Lazarevid V. Zlb Gynäk. 1932;56:1291.
226.
Wenner R. Zur Frage der spontanen Uterusruptur. Gynaecologia. 1949;128:38–41.PubMed
227.
Conturso R, Redaelli L, Pasini A, Tenore A. Spontaneous uterine rupture with amniotic sac protrusion at 28 weeks subsequent to previous hysteroscopic metroplasty. Eur J Obstet Gynecol Reprod Biol. 2003;107:98–100.PubMed
228.
Soltan MH, Khashoggi T, Adelusi B. Pregnancy following rupture of the pregnant uterus. Int J Gynecol Obstet. 1996;52:37–42.
229.
Ritchie EH. Pregnancy after rupture of the pregnant uterus. J Obstet Gynaecol Br Commonw. 1971;78:642–8.PubMed
230.
Klungsoyr P, Kiserud T. Rupture of the uterus treated with suture. Acta Obstet Gynecol Scand. 1990;69:93–4.PubMed
231.
Chen FP. Term delivery after repair of a uterine rupture during the second trimester in a previously unscarred uterus: a case report. J Reprod Med. 2007;52:981–3.PubMed
232.
Gupta U, Ganesh K. Emergency hysterectomy in obstetrics: review of 15 years. Asia-Oceania J Obstet Gynaecol. 1994;20:1–5.PubMed
233.
Kafkas S, Taner CE. Ruptured uterus. Int J Gynecol Obstet. 1991;34:41–4.
234.
Nagarkatti SRS, Ambiye VR, Vaidya PR. Ruptured uterus: changing trends in etiology and management. J Postgrad Med. 1991;37:136–9.PubMed
235.
Lau WC, Fung HYM, Roger MS. Ten years experience of Cesarean and postpartum hysterectomy in a teaching hospital in Hongkong. Obstet Gynecol Surv. 1997;74:133–7.
236.
Al Sakka M, Dawdah W, Al HS. Case series of uterine rupture and subsequent pregnancy outcome. Int J Fertil. 1999;44:293–300.
237.
Özden S, Vildirim G, Basarun T, et al. Analysis of 59 cases of emergent peripartum hysterectomies during a 13-year-period. Arch Gynecol Obstet. 2005;271:363–7.PubMed
238.
Mokgokong ET, Marivate M. Treatment of the ruptured uterus. S Afr Med J. 1976;50:1621–4.PubMed
239.
Flamm BL, Goings JR, Liu Y. Elective repeat Cesarean delivery versus trial of labor: a prospective multicenter study. Obstet Gynecol. 1994;83:927–32.PubMed
240.
Sumawong V, Nondasuta A, Thanapath S, Budthimedhee V. Placenta accreta. A review of the literature and a summary of 10 cases. Obstet Gynecol. 1966;27:511–6.PubMed
241.
Nagy PS. Spontaneous rupture of the uterus caused by placenta percreta at 28 weeks of twin pregnancy. Eur J Obstet Gynecol Reprod Biol. 2003;111:207–9.PubMed
242.
Bakanow. Zbl Gynaek. 1928;52:2159.
243.
Malkasian GD, Welch JS. Placenta previa percreta. Obstet Gynecol. 1964;24:298–300.PubMed
244.
Hassim AM, Lucas C, Elkabbani SA. Spontaneous uterine rupture caused by placenta percreta. Br Med J. 1968;2:97–8.PubMedCentralPubMed
245.
Callender CG, King EL. Spontaneous rupture of a normal uterus associated with placenta accreta forming a central placenta previa. Am J Obstet Gynecol. 1949;57:1020–2.PubMed
246.
Guèye M, Mbaye M, Ndiaye-Guèye MD, et al. Spontaneous uterine rupture of an unscarred uterus before labour. Case Rep Obstet Gynecol. 2012;2012:598356.PubMedCentralPubMed
247.
Shirata I, Fujiwaki R, Takubo K, et al. Successful continuation of pregnancy after repair of a midgestational uterine rupture with the use of a fibrin-coated collagen fleece (TachoComb) in a primigravid woman with no known risk factors. Am J Obstet Gynecol. 2007;197:e7–9.PubMed
248.
Agüero O, Kizer S. Obstetric prognosis of the repair of uterine rupture. Surg Gynecol Obstet. 1968;127:528–30.PubMed
249.
Astet B. Rupture of the uterus in Swedish departments of obstetrics, 1956–1961. Acta Obstet Gynecol Scand. 1967;46:168–82.
250.
Richie EH. Pregnancy after rupture of the pregnant uterus. J Obstet Gynaecol Br Commonw. 1971;78:642–8.
251.
Engelson BE, Albrechtsen S, Iversen OE. Peripartum hysterectomy- incidents and maternal mortality. Acta Obstet Gynecol Scand. 2001;80:409–12.
252.
O’Connor RA, Gaughan B. Pregnancy following simple repair of the ruptured gravid uterus. Br J Obstet Gynaecol. 1989;96:942–4.PubMed
253.
Kulkarni NP, Kendre BV. Ruptured uterus-experience at a rural medical college. J Obstet Gynaecol. 1990;40:75–9.
254.
Ezechi OC, Mabayoje P, Obiesie LO. Ruptured uterus in South Western Nigeria: a reappraisal. Singapore Med J. 2004;45:113–6.PubMed
255.
Ekpo EE. Uterine rupture as seen in the University of Calaber Teaching Hospital, Nigeria: a five-year review. J Obstet Gynaecol. 2000;20:154–6.PubMed
256.
Ogunnnowo T, Oylayemi O, Aimakhu CO. Uterine rupture: UCH, Ibadan experience. West Afr J Med. 2003;22:236–9.
257.
Adanu RM, Obed SA. Ruptured uterus; a seven-year review of cases form Accra, Ghana. J Obstet Gynecol Can. 2003;25:225–30.
258.
Gessessew A, Melese MM. Ruptured uterus – eight year retrospective analysis of causes and management outcome in Adigrat Hospital, Tigray Region, Ethiopia. Ethiop J Health Dev. 2002;16:241–5.
259.
Smith GCSS, Pell JP, Pasupathy D, Dobbie R. Factors predisposing to perinatal death related to uterine rupture during attempted vaginal birth after caesarean section: retrospective cohort study. Br Med J. 2004;329:375.