Carla Kohoyda-Inglis
Stewart C. Wang
Presentation
A 32-year-old man with no significant past medical history presents as the unrestrained driver of an older, midsized, four-door sedan involved in a severe head-on motor vehicle crash with a large tree (Figure 1). Bystanders found the man unresponsive and pulled him from the vehicle. On arrival of Emergency Medical Services (EMS), the man was responsive only to painful stimuli, had labored respirations, and was bleeding from the mouth. On EMS examination, the patient’s abdomen was firm, but not distended, with positive bowel sounds.

FIGURE 1 • Vehicle damage from frontal crash into large tree.
Differential Diagnosis
Care of injured patients begins with assessment at the scene by emergency responders to get the right patient to the right place in the right amount of time. This patient met Field Triage Decision Scheme step 1 (Physiologic) criteria with decreased level of consciousness (Glasgow Coma Scale (GCS) ≤ 13) and was appropriately transported to a high-level trauma center.
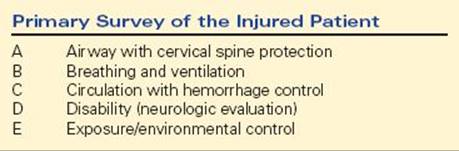
Unlike penetrating trauma, blunt trauma such as motor vehicle crashes may cause internal injuries in multiple body compartments with little external evidence. Initial evaluation (primary survey) of the patient in the emergency room focuses on quickly identifying and treating life-threatening injuries that affect Airway, Breathing, Circulation, Disability (neurologic) (Table 1).
TABLE 1. Primary Survey of the Injured Patient
On arrival to the trauma center, EMS reported a large amount of damage to the steering wheel and that the patient had been restrained by an automatic shoulder belt but had not used the available lap belt. There was 13 inches of intrusion in the toepan area (Figure 2). Passenger compartment intrusion >12 inches at the occupant site or 18 inches anywhere in the vehicle is associated with a high risk of severe injury (Injury Severity Score (ISS) > 15) to that occupant and is part of step 3 of the Guidelines for the Field Triage of Injured Patients.

FIGURE 2 • Interior damage with >12 in of toepan intrusion into the driver’s space. This meets step 3 (Mechanism of Injury) criteria for field triage and is associated with significant risk of severe injury.
On primary survey, he was awake and alert, but complaining of right lower chest and right upper abdominal pain. His vital signs were BP 110/80, RR 12, HR 95, T36.7. Physical examination revealed decreased breath sounds in the right chest and tenderness on palpation on the right lower chest wall and the right upper abdomen without peritoneal signs. Focused abdominal sonography for trauma (FAST) ultrasound exam showed fluid at the right hepatorenal fossa with right-kidney irregularity. Portable chest x-ray (CXR) showed fluid in the right chest; pelvis x-ray was normal. A chest tube was placed for the right hemothorax with 900-mL initial output and slow subsequent output.
Workup
In the absence of indication for immediate surgical exploration (e.g., hemodynamic instability with positive FAST or high chest tube output), 3-D imaging to detect occult internal injuries from blunt trauma is the next priority. CT scans in this patient showed the following:
(1) A large complex liver laceration extending completely through the medial segment of the left lobe and into the lateral segment of the left lobe and the right lobe (Figure 3A).
(2) Poorly perfused right kidney, narrowing of the right renal artery with extravasation of intravenously administered contrast material from the right renal artery, and a large right perinephric hematoma (Figure 3B).
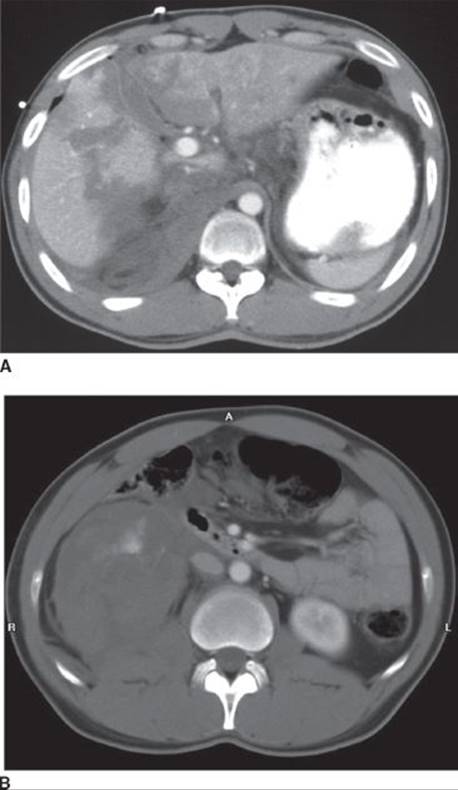
FIGURE 3 • CT scan images from the patient in the scenario demonstrating (A) large complex liver laceration and (B) large perinephric hematoma with contrast extravasation.
Initial Management
Surgical management of the multiply injured patient involves the principles of quick stabilization and resuscitation followed by prioritized treatment of individual injuries. With control of the airway and ability to ventilate the patient, the highest priority is to control hemorrhage, especially arterial bleeding. The presence of active contrast extravasation (arterial bleeding) from the right kidney on abdominal CT mandates immediate intervention. Experience over the past few decades has shown that many solid abdominal organ injuries can be managed without open abdominal exploration and also that hemorrhage control with interventional radiologic techniques provides better organ salvage rates than open operations, which frequently result in organ removal (e.g., nephrectomy, splenectomy) rather than repair to control bleeding. Since there were no immediate hard indications for open exploration (hemodynamic instability, hollow organ injury, penetrating mechanism), this patient underwent radiologically guided embolization of the right kidney and liver with successful control of the bleeding (Figures 4 and 5). The patient was then admitted to the ICU for supportive care.
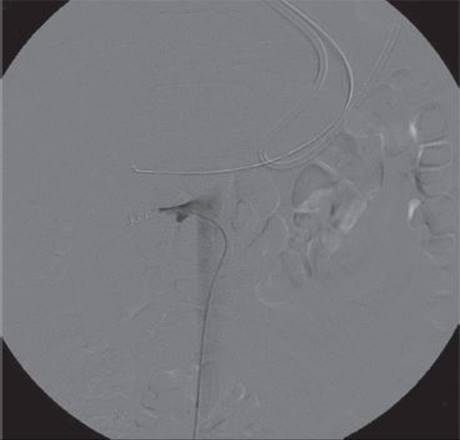
FIGURE 4 • Bleeding from the right renal artery was controlled after placement of 5- and 8-mm coils.
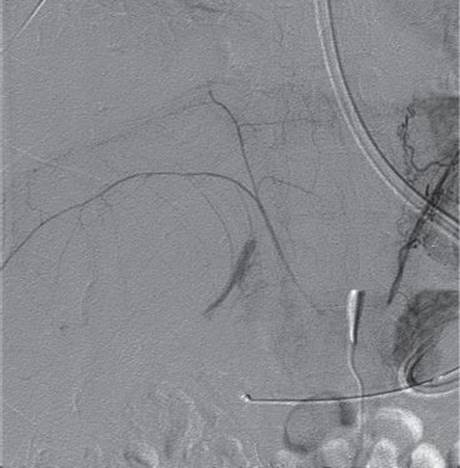
FIGURE 5 • Extravasation from a descending branch of the right hepatic artery. This was subsequently controlled with injection of Gelfoam.
While hemorrhage control is paramount as indication for surgical intervention in the initial postinjury period, the sequelae of organ injury in the days following may also require intervention. It is also important to reassess the patient for injuries missed during the initial assessment. Bile leak is common following large liver injuries and must be controlled (washout and drain placement, often laparoscopic) to avoid bile peritonitis. A HIDA scan is a sensitive test for bile leakage. In this patient, screening HIDA scan on post injury day 3 showed bile extravasation from the liver with drainage into the right chest tube via the pleural cavity. A clinical diagnosis of right diaphragmatic injury was made. Right-sided diaphragm injuries from blunt trauma are much less common than injuries to the left side. Small isolated right diaphragm injuries may not require operative repair since they are much less likely to develop complications such as organ herniation due to the large liver buttressing it underneath. However, due to the interval development of increased liver elevation on CXR as well as the complication of bile leak into the pleural cavity, operative repair was indicated in this case.
Operative Management
The patient was explored through a midline abdominal incision. The liver was found to be partially herniated into the right chest (Figure 6). In order to safely reduce the fractured liver back into the abdominal cavity, the midline abdominal incision was extended into the right chest (thoracoabdominal incision) to allow the liver to be pushed down from above. The large diaphragm tear was easily repaired with pledgeted sutures (Figure 7). The thin, pliable nature of the diaphragm can result in significant disorientation of torn edges, and optimal repair is facilitated by alignment of the edges with tags, stay sutures, or clamps during the repair. The right pleural cavity was irrigated and drainage maintained with a chest tube. Source control and drainage is an important surgical principle when tissues have been damaged and contents contaminate body cavities. The gallbladder was found to be partially avulsed in the line of the liver laceration and was resected. Multiple drains were placed to drain the leak from bile ducts too small to control individually. The abdominal cavity volume was insufficient to allow primary fascial closure following the reduction of the liver due to the intestinal swelling induced by injury and operation. Closure of the fascia with resultant increased abdominal compartment pressures would have compromised renal as well as pulmonary function in this patient with significant injuries to both of those organ systems and also increased the chances for incisional dehiscence. The fascia was bridged with a temporary dressing and closed at a subsequent operation. Temporary closure techniques (e.g., V.A.C., ABThera) have simplified the management of complex trauma patients requiring abdominal operations for damage control.

FIGURE 6 • Large liver laceration found on abdominal exploration.

FIGURE 7 • Repair of diaphragm with pledgeted sutures.
TAKE HOME POINTS
· The ABCDs take top priority: Airway, Breathing, Circulation, Disability.
· Indications for urgent laparotomy following blunt trauma include
o Hemoperitoneum in the setting of hemodynamic instability
o Perforation of hollow viscus or peritonitis
· At urgent laparotomy, the primary objective is damage control of bleeding and peritoneal soilage. It is better to do a partial operation for damage control than to complete a large complex operation on a sick, unstable, multiply injured patients.
· Most solid organ injuries can be managed without open operation; advances in 3-D medical imaging and interventional radiologic techniques have markedly decreased the need for open abdominal exploration.
· Not all clinically important injuries will be immediately diagnosable, even with extensive 3-D scanning. Follow-up evaluations and a high index of suspicion are essential.
SUGGESTED READINGS
Demetriades D, Velmahos GC. Indications for and techniques of laparotomy. In: David Feliciano, Kenneth Mattox, Ernest Moore, eds. Trauma. 6th ed. New York, NY: McGraw-Hill Professional, 2007:607–622.
Franklin GA, Casós SR. Current advances in the surgical approach to abdominal trauma. Injury. 2006;37(12):1143–1156.
Lee JC, Peitzman AB. Damage-control laparotomy. Curr Opin Crit Care. 2006;12(4):346–350.
Sasser SM, Hunt RC, Sullivent EE, et al. National Expert Panel on Field Triage, Centers for Disease Control and Prevention (CDC). Guidelines for field triage of injured patients. Recommendations of the National Expert Panel on Field Triage. MMWR Recomm Rep. 2009;58(RR-1):1–35.