Danielle Fritze
Michael Mulholland
Presentation
A 58-year-old man presents to the emergency room following several episodes of coffee ground emesis. While awaiting evaluation, he suddenly vomits a large volume of bright red blood. As he is urgently transported to a resuscitation bay, his wife explains that he is generally healthy except for the stomach ulcer he had the previous year. He completed a course of two antibiotics for the ulcer and continues to take omeprazole daily. He has never had an operation and takes no other medications. On exam, the patient is distressed but alert, oriented, and no longer vomiting. Initial vital signs reveal tachycardia with a pulse of 115 and blood pressure of 100/70. He has mild discomfort with deep palpation in the epigastrium, and the remainder of his exam is unremarkable.
Differential Diagnosis
For patients presenting with upper gastrointestinal (GI) bleeding, the source may be located in any portion of the GI tract, from the oropharnyx through the ligament of Trietz (Figure 1). Peptic ulcers are the most common cause of upper GI hemorrhage requiring hospitalization, implicated in nearly half of all cases. Mallory-Weiss tears, esophageal varices, and erosive disease each account for an additional 10%. While neoplasms such as adenocarcinoma or gastrointestinal stromal tumor (GIST) are less common sources, their accurate identification is particularly important for treatment planning. Rare causes of GI hemorrhage include Dieulafoy’s lesions, gastric varices, and hemobilia.

FIGURE 1 • Sources of upper gastrointestinal bleeding.
Although the differential diagnosis for upper GI bleeding is broad, individual patient risk factors may point to a particular source. For example, patients with portal hypertension are at particular risk of variceal bleeding. In anyone who has had an aortic aneurysm repair, aortoenteric fistula must be immediately considered as a potentially lethal source of GI hemorrhage. This patient’s ulcer history makes a recurrent gastric ulcer the most probable source of hematemesis.
Workup
Immediate management of upper GI bleeding is dictated by the patient’s clinical condition. If the airway may be compromised by bleeding or diminished mental status, the patient should be intubated. Adequate intravenous access should be established promptly, with administration of crystalloid or blood products as appropriate for the patient’s vital signs and rate of blood loss. Patients taking warfarin or antiplatelet agents are likely to require reversal of their coagulopathy. Nasogastric (NG) tube placement can be diagnostic of an upper GI bleed if bright red blood is aspirated. NG tube placement also allows for evacuation of gastric contents and a rough estimation of the rate of bleeding.
History and physical exam are rarely diagnostic for a bleeding ulcer but may provide information useful in its management. Most patients with gastric ulcers report symptoms of gnawing or burning epigastric pain with a waxing and waning course. Classically, discomfort from gastric ulcers is exacerbated by oral intake. Slow, chronic blood loss may cause melena and lead to symptoms of anemia. Identification of risk factors for ulcer development such as nonsteroidal anti-inflammatory drug (NSAID) use, smoking, or multiple endocrine neoplasia type I syndrome (MEN I) lends insight into the underlying etiology of the ulcer. Knowledge of any anticoagulant or antiplatelet agents taken by the patient allows for appropriate management of the associated coagulopathy. Physical exam is often unremarkable in ulcer patients, but some will exhibit epigastric tenderness. Peritoneal signs raise concern for perforation that infrequently accompanies hemorrhage. In the acutely bleeding patient, the main utility of physical exam is to identify signs of shock and estimate the degree of blood loss.
In parallel with the initial resuscitation, diagnostic studies are undertaken. Serum hematocrit, coagulation profile, and blood type and screen are obtained; hematocrit is followed serially. Peritoneal signs should prompt an upright chest x-ray to evaluate for pneumoperitoneum. In the absence of peritonitis, no imaging studies are necessary. Esophagogastroduodenoscopy (EGD) is the most effective means of locating the source of upper GI bleeding, with successful identification of the responsible lesion in 95% of patients. In rare cases where the source of bleeding is not located on initial endoscopy, repeat EGD, angiography, or technetium-99m–labeled red blood cell scan may be successful.
Diagnosis and Treatment
Once a gastric ulcer is identified, endoscopic therapy is guided by the risk of recurrent hemorrhage and the patient’s clinical stability. Although bleeding frequently resolves spontaneously, specific stigmata of hemorrhage predict continued or recurrent bleeding and the need for intervention (Table 1). Ulcers with evidence of active bleeding or a visible vessel within the lesion (Forrest grade 1a, 1b, and 2a) are at highest risk. Ulcers with an adherent clot and underlying oozing are also prone to recurrent bleeding. Endoscopic intervention is indicated for each of these high-risk lesions. Options include the application of clips, thermal coagulation, or injection of a vasoconstricting or sclerosing agent. When feasible, biopsy of the ulcer is important to identify any associated malignancy. Antral biopsies are used to establish a histologic diagnosis of Helicobacter pylori. For patients with a bleeding ulcer, endoscopic interventions carry a 90% success rate in achieving initial hemostasis. If a patient rebleeds after endoscopic intervention, a second endoscopic attempt at hemostasis is made and has been demonstrated in a randomized trial to be safer than proceeding to surgery. However, for bleeding that cannot be controlled endoscopically (after two attempts), or for patients with hemorrhagic shock, surgery may be lifesaving.
TABLE 1. Forrest Classification of Peptic Ulcers

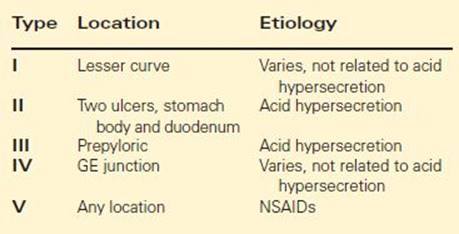
Following initial hemostasis, the etiology of the ulcer must be identified and addressed. H. pylori and NSAIDs are the two most important factors contributing to the development of gastric ulcers (Table 2). Each is implicated in over 50% of cases, with additive effects. Tobacco use is also contributory. Four percent of gastric ulcers harbor an underlying malignancy, most commonly gastric adenocarcinoma. In rare cases, Zollinger-Ellison syndrome, either sporadic or associated with MEN I, may be at fault. Ulcer location may also offer insight into etiology. Prepyloric and duodenal ulcers are typically related to acid hypersecretion, whereas NSAID-induced ulcers may be located anywhere in the stomach (Table 3).
TABLE 2. Etiology of Gastric Ulcer

TABLE 3. Modified Johnson Classification of Gastric Ulcers
Medical therapy directed at ulcer etiology is an important adjunct to endoscopic and surgical interventions. Acid suppression with a proton pump inhibitor (PPI) decreases the risk of rebleeding after endoscopic hemostasis, aids in ulcer healing and prevents ulcer recurrence. NSAIDs should be withheld if medically possible. If NSAIDs are to be continued, concurrent acid suppression or use of misoprostol is imperative. Smoking cessation is strongly encouraged. For patients with H. pylori, eradication of the bacteria results in lower ulcer recurrence rates than acid suppression therapy alone. In over 90% of colonized patients, this can be accomplished with a single course of “triple therapy”—two antibiotics active against H. pylori and a PPI. Confirmed clearance of H. pylori, in combination with a maintenance PPI, is associated with <2% risk of recurrent bleeding in the first year. Endoscopy should be performed after 6 weeks to document ulcer healing. Almost uniformly, recurrence is related to H. pylori reinfection or NSAID use.
Surgical Approach
While surgery remains the primary means of managing anatomic complications of ulcer disease, the development of effective pharmacotherapy for acid suppression and H. pylori clearance has reduced the role of surgery in addressing the underlying etiology. When treating anatomic complications, the operation should be carefully tailored to the patient’s clinical scenario. The appropriate surgical procedure for a bleeding gastric ulcer is also dependent upon the patient’s condition (Figure 2). For unstable patients, midline laparotomy is followed by anterior gastrotomy. Once the lesion is identified, the ulcer is oversewn, biopsied (if possible) and the gastrotomy repaired. For stable patients with a history of refractory ulcer disease, an antisecretory procedure such as truncal vagotomy or distal gastrectomy should be considered.

FIGURE 2 • Algorithm for management of bleeding gastric ulcer.
Truncal Vagotomy
In patients with bleeding gastric ulcers, truncal vagotomy is indicated for those who have failed previous medical therapy. These patients usually have a long-standing history of ulcer disease and have proven refractory to (or serially noncompliant with) PPIs and H. pylori eradication. Vagotomy markedly reduces cholinergic stimulation of gastric acid secretion. Because vagotomy also results in pyloric denervation, a concurrent procedure such as pyloroplasty or antrectomy is thus necessary to ensure gastric drainage.
To perform a truncal vagotomy, the left hepatic lobe is retracted cephalad and laterally with division of the triangular ligament as needed to expose the hiatus. The overlying peritoneum is incised and the esophagus dissected circumferentially for several centimeters about the gastroesophageal (GE) junction. Anteriorly, the vagal trunk is found closely applied to the esophageal wall. In contrast, the posterior vagus may reside 1 cm or more posterolateral to the esophagus. Palpation may aid in initial identification of the nerves. Once both trunks are located, proximal and distal clips are placed to allow for resection of a 2-cm intervening segment of nerve. These specimens are sent to pathology for histologic confirmation. There may be several divisions of each vagal trunk, so the area of the GE junction is carefully inspected to determine that all vagal fibers have been divided. Prior to closure, cruroplasty may be required to prevent development of a hiatal hernia.
Distal Gastrectomy
If a patient with bleeding gastric ulcer is stable, there are a few scenarios in which a distal gastrectomy can be considered. As with truncal vagotomy, patients are usually only considered candidates for distal gastrectomy if they have a history of failed medical management, especially patients with large antral ulcers that cannot be easily oversewn or patients with ulcers suspicious for cancer. Risks of operative death and complications are much higher for distal gastrectomy than simple oversewing or vagotomy, so this procedure should only be undertaken when clear indications exist.
To perform distal gastrectomy, a vertical incision in the supraumbilical midline affords adequate exposure in most cases. Following exploration of the abdomen, a Kocher maneuver is performed to mobilize the duodenum. Mobilization of the distal stomach begins with division of the gastrocolic ligament. Entry into the lesser sac permits examination of the posterior gastric wall. The omentum is then divided along the greater curvature, from the duodenum halfway to the GE junction. The right gastroepiploic vessels are ligated and divided near the gastroduodenal artery (GDA). The gastrohepatic ligament is then incised. The right gastric artery is identified, ligated, and divided near the superior border of the duodenum. Branches of the left gastric artery are divided along the lesser curve in preparation for resection and anastomosis. An area of healthy proximal duodenum is chosen and transected with a stapling device. The proximal extent of the resection is determined by the location of the ulcer and the condition of the gastric wall. The stomach is also divided with a stapling device and all staple lines are oversewn. Continuity of the GI tract can be reestablished via either Billroth I or II reconstruction, depending upon the length and health of the duodenal stump.
Special Intraoperative Considerations
Type IV gastric ulcers can be particularly challenging to manage due to their proximity to the GE junction. In most cases, the ulcer can be resected as part of the distal gastrectomy with an extension along the lesser curve. Traditional Billroth I or II reconstruction is avoided as it is likely to result in narrowing of the GE junction. Instead, roux-en-Y gastrojejunostomy permits construction of a wide anastomosis, incorporating the distal GE junction and the entirety of the gastrotomy. In rare circumstances, the ulcer may be oversewn and left in situ. A concurrent antisecretory procedure with H. pylori eradication, PPI, and cessation of NSAIDs results in satisfactory ulcer healing in most patients.
TABLE 4. Key Technical Steps in Distal Gastrectomy and Truncal Vagotomy

Postoperative Management
Following surgery for a bleeding gastric ulcer, patients remain on bowel rest with NG decompression. These measures may be discontinued as gastric emptying resumes. Patients should be observed for potential postoperative complications such as surgical site infection (SSI), hemorrhage, or anastomotic leak. For those with a Billroth II reconstruction, duodenal stump leak is a particularly morbid complication.
With initiation of oral intake, patients who undergo gastrectomy should also be monitored for postgastrectomy dumping syndrome. This is characterized by postprandial GI and vasomotor symptoms, such as nausea, abdominal pain, dizziness, and even syncope. In most patients, these symptoms are temporary, and easily managed with frequent small meals. In a small minority of patients, however, dumping symptoms can become debilitating. Octreotide may be helpful in this circumstance. At discharge, all patients are counseled to avoid tobacco and NSAIDs as well as to continue PPI therapy. Those colonized with H. pylori receive triple therapy and eradication is confirmed at follow-up.
Case Conclusion
The patient’s immediate management included placement of two large-bore ivs, crystalloid resuscitation, and a pantoprazole infusion. His initial hematocrit was 28%, with normal coagulation studies. Endoscopy performed while the patient was still in the emergency room revealed a 2-cm gastric ulcer in the prepyloric region (type III) with a nonbleeding visible vessel. Clips were applied and biopsies performed endoscopically. He was then admitted to the hospital for observation. The following day, he had another episode of hematemesis. Endoscopy was again attempted, but unsuccessful in controlling the bleeding. He required two units of packed red blood cells but remained hemodynamically stable. He was taken to the operating room emergently for surgical intervention. Given the history of recurrent type III gastric ulcer following H. pylori eradication and long-term acid suppression, an antisecretory procedure was deemed appropriate. Truncal vagotomy was performed in conjunction with distal gastrectomy. The patient tolerated the procedure well, and recovered without recurrent bleeding or serious complication. Final surgical pathology confirmed a benign gastric ulcer.
TAKE HOME POINTS
· Although decreasing in incidence, peptic ulcer remains the most common cause of upper GI bleeding, with significant associated mortality.
· H. pylori infection and NSAID use are the most frequent inciting factors in bleeding gastric ulcers.
· Endoscopy is the first-line diagnostic intervention and is therapeutically effective in a majority of patients.
· Surgery is indicated in patients with massive bleeding, failure of endoscopic therapy, recurrent hemorrhage, or neoplasm.
· Anterior gastrotomy, ulcer oversewing, and biopsy is the procedure of choice for patients without a history of refractory ulcer disease.
· Truncal vagotomy is indicated only for patients with ulcers refractory to adequate PPI therapy and H. pylori eradication.
· Distal gastrectomy with inclusion of the ulcer in the specimen is the procedure of choice in stable patients with refractory ulcer disease who have large antral ulcers.
· Acid suppression and clearance of H. pylori decrease the risk of recurrent bleeding gastric ulcer.
SUGGESTED READINGS
Enestvedt BK, Gralnek IM, Mattek N, et al. An evaluation of endoscopic indications and findings related to nonvariceal upper-GI hemorrhage in a large multicenter consortium. Gastrointest Endosc. 2008;67(3):422–429.
Gisbert JP, Khorrami S, Carballo F, et al. H. pylori eradication therapy vs. antisecretory non-eradication therapy (with or without long-term maintenance antisecretory therapy) for the prevention of recurrent bleeding from peptic ulcer. Cochrane Database Syst Rev. 2004(2):CD004062.
Gralnek IM, Barkun AN, Bardou M. Management of acute bleeding from a peptic ulcer. N Engl J Med. 2008;359(9):928–937.