Timing and Duration
The objectives of presurgical orthodontic treatment are to enable maximal surgical correction of the deformity, to facilitate any segmental surgical procedures and to enable the production of an ideal stable occlusion. An essential feature of the treatment plan is to decompensate the dento-alveolar results of the jaw deformity and as such is very different from the “compensatory” approach of the pure orthodontic management of the case. Hence the need for careful consideration by the patient and clinicians as to the desired choice of treatment. The majority of orthodontic treatment is undertaken prior to surgery, although some prefer to undertake minimal orthodontic treatment prior to surgery leaving the major proportion to the postoperative phase. Both of these approaches have advantages and disadvantages. Extensive presurgical preparation is usually better accepted by the patient giving maximum compliance. However, the dental movements may be hindered by the underlying skeletal and soft tissue discrepancy. Conversely, although the orthodontic changes may be easier once a normal skeletal and soft tissue relationship has become established, prolonged postoperative orthodontics may not be tolerated by the patient and leads to poor patient satisfaction.
Presurgical Orthodontics
Presurgical preparation usually takes 18-24 months, whilst postsurgical refinement should be completed within 6 months of the operation.
The goals of presurgical orthodontics are to facilitate the surgery by:
· Alignment of the dentition.
· Levelling of the occlusal plane, either as a continuous arch or segmentally prior to surgical levelling.
· Incisor decompensation.
· Buccal segment decompensation.
· Coordination of the upper and lower arches.
· Providing a means of fixation.
Alignment of the Dentition — The Technology
Dental arch alignment requires 3-dimensional control of tooth position. Most use a pre-adjusted Edgewise appliance system with a slot dimension of .022” × .028” or variants upon this. The term preadjusted appliance refers to the bracket design such that adjustments are incorporated into the brackets to create a final position of the teeth with the correct mesiodistal angulation (tip), buccopalatal or buccolingual inclination (torque) and horizontal positions (in/out) relative to each other. Individual teeth within the dental arch therefore have specific adjustments built into their appropriate bracket (Figure 4.1). A variety of pre-adjusted systems are available each with minor variations in the tip and torque values. This is referred to as the bracket prescription. Segmental surgery requires the added facility of a double tube on the mandibular molars and/or a triple tube on the maxillary molars. The Tip-EdgeTM appliance system is equally applicable to presurgical alignment although individual operators will have their preferred bracket prescription.
It is worthwhile considering the variations in bracket tip and torque required in specific cases. In an ideal occlusion, the crown of the lower incisor lies labial to the apex for ideal tooth inclination. In Class II cases where proclined lower incisor require decompensation, the use of MBTTM brackets with the 60 of additional lingual crown torque can aid the mechanics. Conversely, Super-torqueTMbrackets, with additional palatal root torque to the upper incisors, can be useful in correcting severely retroclined incisors in Class II division 2 cases. Mesiodistal tooth angulation (tip) becomes important when considering the preparation of a case for segmental surgery as it is important to facilitate the surgery (see below) by ensuring the roots adjacent to the osteotomy site are either parallel or slightly divergent. Again in an ideal functioning occlusion, the crown of the canine should lie mesial to the apex. Where the osteotomy cuts are to be made distal to the canines, the use of the canine bracket of the opposite side ensures that the tip incorporated into the bracket keeps the apices forward and out of the way of the surgical cuts.

Figure 4.1 Pre-adjusted Edgewise appliances with individual brackets designed for specific teeth.
The choice of archwire material and sequence is to a large extent, driven by operator preference. The use of modern “superelastic” nickel titanium wires is frequently beneficial for initial alignment. However, where the interbracket span is minimal, for example with mutually rotated lower incisors or premolars, the efficiency of these wires is reduced. In this situation, archwires with loops for flexibility may be preferable, for example .014” or .016” stainless steel or Titanium/Molybdenum (TMA) wires. Ultimately, heavy rectangular stainless steel archwires should be placed at the time of surgery (.019” × .028” or .022” × .028”) for maximal tooth control and with the addition of hooks to facilitate fixation.
Arch Levelling
The decision as to whether to fully level the arches is very much dependent on the patient's facial height and the upper lip/incisor relationship. In Class II corrections, where the facial height is reduced, it is preferable to preserve a Curve of Spee in the lower arch so that when the mandible is advanced, the lower incisors slide down the cingulum plateau of the upper incisors thereby increasing the lower facial height (Figure 4.2). Although this may occur in some Class II division 1 cases, it is especially common in patients with Class II division 2 incisor relationships where the presurgical orthodontic preparation converts the incisors into a Class II division 1 pattern.
Following surgery this results in buccal segment lateral open bites with occlusal contact in only the incisor and terminal molar regions. This tripod of contacts is referred to as a “3-point landing”. The lateral open bites (Figure 4.3)require closure as part of the postsurgical orthodontic phase of treatment (see Chapter 10).
In Class II cases where the intention is to avoid increasing the facial height, the lower arch should be levelled as part of the presurgical orthodontic preparation, or by segmental surgical procedures. With a shallow curve of Spee (approximately 2 mm), it may be possible to level the arches orthodontically through a combination of buccal segment extrusion, incisor intrusion and/or incisor proclination (Figure 4.4). Levelling the Curve of Spee without space will procline the lower incisors, and reduce the potential for mandibular advancement. If the intention is to maintain anteroposterior arch length, then premolar extractions will be required, especially if there is any crowding present (Figure 4.5).

Figure 4.2 (a) and (c) Class II deep overbite cases, with an increased curve of Spee, facilitates an increase in anterior face height as the mandible is advanced (b) and (d). The resulting contact between the upper and lower incisors and the terminal molars of each side of the arch is referred to as a “3-point landing”. Note the significant increase in lower facial height accompanying the advancement.
Segmental Levelling
a) In cases of reduced vertical dimension
In cases with a severe overbite the so-called “3-point landing” may produce lateral open bites which are too large to close by orthodontic extrusion of the premolars and canines. Many operators consider 2 mm of extrusion from each arch as the absolute maximum that can be achieved and remain stable without rebound. Beyond this, levelling should be achieved through surgery, usually through a set-down of the lower labial segment with a mandibulotomy (see Chapter 9). Where there is a reverse Curve of Spee in the upper arch, as in some Class II division 2 cases, it may be necessary to undertake segmental surgery to both the upper and lower labial segments.

Figure 4.3 Following mandibular advancement the resulting lateral open bites can (a) be closed in the postoperative orthodontic phase (b) or may even close spontaneously (c) and (d).See also Figure 4.16.

Figure 4.4 Orthodontic levelling of an increased curve of Spee can be achieved as a combination of premolar/molar extrusion, incisor intrusion or incisor proclination.

Figure 4.5 (a) Levelling the curve of Spee orthodontically will lead to (b) incisor proclination and an increase in arch length unless space is created through extractions.
With all segmental surgery cases, the presurgical orthodontics should facilitate the alveolar section by diverging the canine and premolar roots. The mesiodistal tip incorporated into the canine brackets is such that the root apex will align distal to the crown encroaching into the site of the surgical cuts. When planning cases for segmental surgery it may be desirable to use the right canine bracket on the left canine and vice versa in order to keep the roots away from the osteotomy site. The brackets can then be replaced with those of the correct side in the postsurgical period.
Segmental orthodontic levelling is designed to place the buccal segments at one level and the incisor segments at a different level. This can be achieved by three segmental archwires, two running in the buccal segments from premolar to molar on each side together with a third segment for the canine and incisors. This approach tends to produce a lack of control of the tooth positions and therefore a continuous arch is preferred, from molar to molar but with an anterior step for the canines and incisors.
In the latter case, the surgeon will cut the archwire across the osteotomy site at the time of surgery. Although the segments are immobilised using rigid internal fixation, it is essential to provide additional fixation at the occlusal level. This can be done with a prefabricated continuous archwire bent to the planned postoperative segments. However, insertion of this wire intraoperatively can be extremely time-consuming. It is preferable to use a rigid prefabricated horseshoe shaped 1.0 mm steel supplemental arch wire, engaged passively into double or triple tubes on the molars and secured by ligatures to the three archwire segments (Figure 4.6). Ultimately, the sectional arches can be replaced with a continuous archwire once the patient has recovered.

Figure 4.6 To control the occlusal relationship after segmental surgery the segmented arch (upper) is fixed at the occlusal level using a heavy 1mm stainless steel archwire. This is engaged passively into a headgear tube on the molar bands. Auxillary steel ligatures lash the segmented orthodontic archwire in the anterior and buccal segments to the heavy buccal arch.
b) In cases of increased vertical dimension
In anterior open bite cases, the presurgical orthodontics must not be allowed to extrude the incisors as this is potentially unstable and will jeopardise the surgical correction. The presurgical orthodontics should accentuate the open bite through intrusion of the labial segments and extrusion of the buccal segments. In this way maximal surgical correction can be achieved and any postsurgical incisor change will ensure closure of the anterior open bite (Figures 4.7a and 4.7b).
Incisor Decompensation
In the majority of cases of severe antero-posterior disproportion, the soft tissues of the lips and tongue produce a secondary deformity of incisor inclination. In skeletal Class III cases, so-called compensation presents with proclined upper incisors and retroclined lower incisors (Figure 4.8). Presurgical preparation (decompensation) corrects the axial inclinations to maximise the mandibular setback (Figure 4.9). Although dictated by the amount of crowding, it is common for the lower arch to be treated nonextraction, aligning the labial segment by proclination. Care should be taken not to breach the labial alveolar plate, destroying the periodontal attachment, producing a dehiscence of the gingival margin. Periodontal grafting should be considered.

Figure 4.7 (a) and (b) Segmental orthodontic levelling of the Curve of Spee with a continuous archwire. The step in the archwire is designed to accentuate the anterior open bite by incisor intrusion and buccal segment extrusion. Any postsurgical rebound of the teeth will help maintain closure of the open bite.

Figure 4.8 The secondary dental deformity of a prognathous mandible is the so called “compensation” with proclination of the maxillary incisors and retroclination of the mandibular incisor teeth.
Severely crowded cases may need extractions to provide the space for arch alignment. With simultaneous decompensation of the lower incisors, the extractions of choice are the lower second premolars, assuming all teeth to be of good prognosis. This also adds to the anchorage balance in the lower arch through the incorporation of eight teeth in the anterior segment.
When using the pre-adjusted Edgewise brackets the orthodontist can take advantage of the mesiodistal tip incorporated into the canine bracket slot to aid lower incisor decompensation. During the alignment phase, the tip in the bracket would tend to throw the canine crown anteriorly, which in turn leads to proclination of the incisors (Figure 4.10a). Therefore the technique of “laceback” ligatures to the lower canine crown should be avoided (Figure 4.10b).

Figure 4.9 Dental “compensation” in a Class III case with proclination of the maxillary incisors and retroclination of the mandibular incisor teeth (continuous outline), compared with the ideal incisor inclination (broken outline) as seen on a lateral skull radiograph. The correction of the incisor angulation is termed decompensation.
The upper incisors generally need to be retracted, a procedure, which may necessitate premolar extractions. In moderately crowded cases these will be the upper first premolars to aid the anchorage balance. In very mildly crowded cases, some would opt to move the upper arch distally using anchorage-reinforcing devices. In order to avoid the undesirable effects of the tip incorporated into the brackets, laceback ligatures should be employed during the aligning phase. The clinician may also use Class II directed interarch elastics to aid mutual decompensation of upper and lower arches.

Figure 4.10 Once engaged with an initial aligning archwire, the mesiodistal tip incorporated into the mandibular canine bracket tends to throw the crown anteriorly (a) so aiding lower incisor decompensation in Class III cases. The technique of tying the crown back to the molar through the use of a “laceback” ligature (b) should be avoided in these cases.
Most cases with an anterior open bite, require a differential posterior impaction of the maxilla. The posterior maxilla is impacted by a greater amount than the anterior segment. The effect of this surgery is to retrocline the incisors (Figure 4.11). Hence when undertaking orthodontics in this situation, the presurgical preparation may intentionally leave the upper incisors slightly proclined.
Decompensation in Class II Cases
The soft tissue influence in Class II cases is variable nevertheless the goal is to place the incisor segments at the correct inclination to the dental bases. In the lower arch, the incisors may be proclined (“compensated”), in which case decompensation by retraction is indicated and usually involves premolar extractions (Figure 4.12). As in the upper arch in Class III cases, laceback ligatures will aid decompensation.

Figure 4.11 Impacting the maxilla posteriorly (dotted outline) has the effect of retroclining the maxillary incisors, and so presurgical orthodontics may intentionally leave the incisors proclined.
In the maxillary arch, especially in patients with a low vertical dimension, the lower lip may become trapped palatal to the upper incisors which become proclined. Presurgical preparation will involve retraction of the upper incisors back to a normal inclination. If the proclined maxillary incisors are naturally spaced, retraction may be undertaken without the need to resort to extractions. However in many cases, especially where there is crowding, the loss of premolars is indicated.
Arch Coordination
Anteroposterior changes in skeletal relationships frequently require an alteration in the transverse widths of the arches for coordination, especially expansion of the upper arch. Whether this can be achieved by orthodontics alone, or through a combination of orthodontics and surgery depends upon:

Figure 4.12 Decompensation in Class II cases will depend on the position of the incisors, which in most cases require retroclining in both upper and lower arches. Here shown as moving from the continuous to the broken outlines.
· the amount of expansion required;
· the initial inclination of the buccal segment dentition;
· the relative degree of expansion required throughout the buccal segments.
Orthodontic expansion is achieved by tipping movement. Where the teeth are initially tipped palatally, uprighting will allow a good dental interdigitation, which is important for stability. Where the buccal teeth are either upright or even already flared buccally, further expansion will not produce a satisfactory stable occlusion. In such cases surgical expansion is required (see Chapter 9)
Methods of Orthodontic Arch Expansion
Quadhelix
The quadhelix appliance is the most frequently used appliance for expanding the maxillary dentition (Figure 4.13a). Although producing an overall tipping movement, it has the advantage of enabling differential expansion within the buccal segments.

Figure 4.13 Examples of arch expansion methods: (a) quadhelix, (b) hyrax screw, and (c) auxillary expansion arch engaged in headgear tubes on molar bands.
Hyrax Screw
The hyrax screw (Figure 4.13b) is principally used for expansion prior to the fusion of the mid-palatal suture. The age at which this occurs may vary but it is usually complete by 21 years. Some suggest that the mechanism of expansion is more bodily movement rather than tipping in nature although this has been questioned.
Expansion Arch
Minor degrees of tooth movement can be achieved through expansion with a rectangular orthodontic archwire (usually of .018 × .025 minimum size). Use of a rectangular wire enables active buccal root torque to be placed in the buccal segments of the wire in order to achieve a positive overbite of the buccal cusps. Occasionally, the rectangular archwire can be used in conjunction with a 1mm rigid and expanded stainless steel arch fitted into the headgear tubes of the upper molars (Figure 4.13c).
Alternative Arch Expanders
The development of Nickel/Titanium materials has led to the marketing of an array of expansion devices which incorporate the shape/ memory and superelasticity properties of these materials.
Monitoring Arch Coordination During Treatment
When preparing the arches for correction of Class II problems, testing of arch co-ordination in the transverse dimension can be achieved by simple forward posturing of the mandible. In Class III corrections the use of an acrylic template of the occlusal surfaces of the lower arch is invaluable. The template can be prepared by taking an alginate impression of the aligned lower arch and pouring cold cure acrylic resin into the occlusal portion of the impression. At successive visits, the template of the lower arch can then be occluded with the upper arch to check compatibility and avoid the need for repeated study models (Figure 4.14).

Figure 4.14. An acrylic template of the aligned lower arch can be used to check coordination with the upper arch expansion at successive visits.
Facilitating Surgical Correction
Towards the end of the presurgical phase, upper and lower rectangular archwires should be in position and surgical hooks or soldered brass wires are added in the midline and throughout the buccal segments (Figure 4.15). These provide a means of attaching temporary intermaxillary fixation during surgery. They can also be used to attach seating elastics or intermaxillary elastics during the immediate postoperative period.
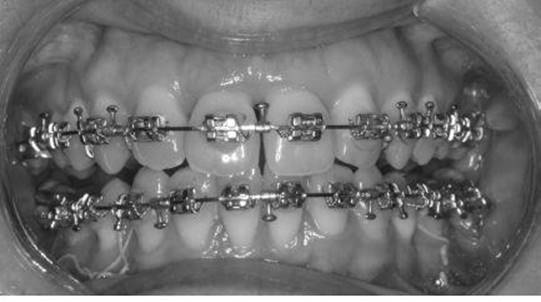
Figure 4.15 Rectangular archwires with surgical hooks. Note the archwires are engaged in the brackets using stainless steel ligatures.
Postsurgical Orthodontics
The goals of postsurgical orthodontics are to refine the occlusion, ensure a balanced occlusion and to plan the retention regime.
In cases of segmental surgery, where canine brackets have been reversed preoperatively, it is necessary to re-bond the canine brackets, placing brackets of the correct side in order to produce a normal canine angulation.
Postsurgical settling of a “3-point landing” usually involves a combination of flexible archwires together with vertical intra-oral seating elastics between the upper and lower arches (Figures 4.16a and 4.16b). Where the maxillary arch is level, a rigid upper rectangular archwire is maintained whereas a flexible wire, for example a braided steel wire, can be placed in the lower arch. When both arches need extrusion, the rectangular wires can be sectioned and seating elastics applied between the segments.

Figure 4.16 Closure of a lateral open-bite using postoperative intraoral elastics.
Retention
As in routine orthodontics, the tooth movements undertaken as part of orthognathic surgery require a period of retention following removal of the fixed appliances. This is to allow the alveolar bone and periodontal tissues to consolidate. Where there has been correction of incisor rotations or closure of large spaces, a permanent fixed bonded lingual or palatal retainer is employed. In other cases, a removable retainer of varying designs may be used. In general, it is good practice to avoid any retainer wirework passing through embrasures where extraction spaces have been closed (Figure 4.17).

Figure 4.17 A removable retainer designed to avoid wirework passing through previously closed extraction sites.