Frank Farrington
Optimum dental health is essential for the total health of the child. The basic dental care needs of children with oral clefts are the same as those for anyone of the same age, with the addition of the special needs resulting from the cleft. Early evaluation and preventive care are extremely important as the primary and developing permanent dentitions provide the basic framework for future dental, orthodontic, and prosthetic treatment. However, parents are often so overwhelmed by other aspects of their children's care that dental needs are given a rather low priority. Emphasizing the fact that their child with an oral cleft needs the same basic dental care as any child the same age brings an element of normalcy to parents' thinking regarding their children's needs. The dental needs of the child can be divided into four stages, based on oral development, preventive needs, and treatment:
1. The infant and toddler need early assessment, and parents need to be oriented toward the prevention of oral disease.
2. The needs of the child during the primary dentition center around the establishment of regular dental care, assessment of the developing dentition, development of a preventive program, and treatment needs related to the cleft.
3. Mixed dentition presents a time of transition as the child becomes more involved in dental care, including the temporary replacement of missing teeth as well as regular dental care.
4. The needs of the adolescent during the development of the young permanent dentition center around the dental needs associated with supporting orthodontic and prosthetic care.
During each of these stages, the management of the child is a prime concern. Management of the child's behavior and attitude toward dental care is as important as the actual dental treatment in the child's overall care. Past dental and medical experience, the age of the child, the extent of care needed, and the child's attitudes and fears must be of major concern in developing a good dental patient. TheAmerican Cleft Palate-Craniofacial Association (1993) provides guidelines for the optimum care of individuals with craniofacial anomalies, regardless of the specific type of disorder. The underlying principle of these guidelines is that patients with craniofacial anomalies are best managed by an interdisciplinary team of specialists.
The Infant and Toddler
The infant should be seen for initial oral evaluation shortly after birth and, preferably, as part of an interdisciplinary team evaluation. Evaluation of factors that may influence surgical management, such as arch form, displacement of the arch segments, and presence of natal or neonatal teeth, needs to be done. Evaluation of airway and feeding problems also needs to be done early. In some programs, the use of an oral appliance is an option as a noninvasive method of management. Dental evaluation and preventive care should begin with this initial team evaluation of the infant. The importance the profession puts on this early evaluation is seen in the American Academy of Pediatric Dentistry (1999) recommendation that all children be seen for a first general dental visit 6 months after the eruption of the first tooth or at 1 year of age, whichever comes first.
The early oral healthcare visit provides the foundation for a lifetime of preventive and corrective dental care and helps to assure optimal oral health during childhood and into adulthood. Oral examination, anticipatory guidance including preventive education, and appropriate therapeutic care are essential during the entire period of oral development, to provide the necessary specialty care needed because of the oral cleft. Following are several recommendations related to infant oral health:
1. Ideally, infant oral healthcare begins with prenatal oral health counseling for parents. An initial oral evaluation should occur within 6 months of the eruption of the first primary tooth and no later than 12 months of age.
2. At the infant oral evaluation visit, the dentist should do the following:
a. Record a thorough medical and dental history, covering the prenatal, perinatal, and postnatal periods
b. Complete a thorough oral examination
c. Assess the patient's risk of developing oral and dental disease and determine an appropriate interval for periodic re-evaluation based on that assessment
d. Discuss and provide anticipatory guidance regarding dental and oral development, fluoride status, nonnutritive oral habits, injury prevention, oral hygiene, and effects of diet on the dentition
3. Dentists who perform such services for infants should be prepared to provide therapy when indicated or should refer the patient to an appropriately trained individual for necessary treatment (American Academy of Pediatric Dentistry, 1999).
The general development of the dentition is the same in children with and without clefts. Abnormal findings are usually isolated to the areas in and adjacent to the cleft itself. Eruption of the dentition occurs at the usual time and in the usual sequence.
Infant Oral-Facial Orthopedics
The break in the continuity of the alveolar arch may lead to a collapse of the arch segments and the development of anterior and posterior crossbites. Closure of the lip can lead to pressure on the alveolar segments, resulting in remolding of the bony segments and/or collapse of the posterior portions of the arch, creating a unilateral or bilateral crossbite. Depending on the treatment philosophy of the interdisciplinary team and the actual deformity of the alveolar arch, early appliance therapy may be indicated. Use of tape or a combination of tape and orthodontic elastics to close the gap between the anterior and posterior segments of a unilateral cleft allows for less stretching of lip tissue at the time of lip repair. In bilateral clefts, the retraction and centering of the premaxillary segment also makes lip closure easier (Fig. 28.1). To prevent collapse of the arch from the tension of the tape or elastics, a palatal prosthesis, essentially a denture base without teeth, can be used. The appliance is usually tolerated well by infants during the period prior to lip repair. If the appliance is used after the lip repair to stabilize the segments or cover the hard palate defect, the eruption of teeth makes retention of the appliance difficult. Intraoral appliances to stabilize and realign cleft segments have been used for over 50 years. McNeil (1950) used a chewing or feeding plate to realign segments. A model of the cleft arch was progressively modified to reposition the segments. As the infant chewed or nursed, the appliance acted similarly to an orthodontic positioner to move the segments. Removable appliances using expansion screws to slowly expand and reposition the dental arch have been used since the 1960s. To gain more control of the movement of segments, Latham (1980) designed an acrylic palatal appliance containing an elaborate combination of screws and hinges, which was anchored to the maxillary palatal shelves with metal pins. A number of variations of pinned palatal appliances have been developed over the years. A modification developed by Mylin used sliding plastic palatal shelves to keep the hard palate defect sealed during expansion (Farrington, 1998) (Fig. 28.2).
|
|
|
FIG. 28.1. Retraction of the premaxillary segment in a bilateral cleft with tape and elastics. |
Treatment of these crossbites is usually not needed until the child is older. In a few cases, treatment may be advised if there are functional problems associated with the crossbite. The lack of proper anterior development of the maxilla can lead to a pseudo-class III malocclusion. By 2.5 to 3 years of age, the primary dentition should be complete, as it would be in the normal child without a cleft.
|
|
|
FIG. 28.2. Pinned palatal appliance showing sliding shelves to seal palatal cleft during expansion. |
For the child with a cleft, this early evaluation is even more important than for the average child. Erupted natal or neonatal teeth that may be malformed in the area of the cleft need to be identified early. The lateral incisor is located directly in the plane of the suture of the maxillary and premaxillary segments. The primary lateral incisor may be absent or malformed. In some cases, a supernumerary lateral incisor may develop. The tooth may erupt early and can appear anywhere along the cleft line (Figs. 28.3,28.4).
The teeth on either side of the cleft are at increased risk for caries. Their location makes them hard to keep clean and susceptible to plaque accumulation.
Feeding problems related to the cleft and the surgery over the first year increase the risk for early childhood caries. Concerns that the child is well nourished and comfortable, especially after surgery, may keep the child on the bottle past 10 to 12 months, when it is recommended that the child go to a cup. Parents need to be informed of the problems related to prolonged and ad lib. use of the bottle, especially at naptime and at night.
Streptococcus mutans and lactobacilli are important pathogens in the development of dental caries. Usually, S. mutans are not detected before eruption of the primary teeth, and there is a gradual increase in the frequency of S. mutans with age as the number of teeth increases. Seeding of the organism seems to come from the mother, with the time of greatest infectability being around 18 months of age. If the mother has a high Streptococcus count, the child is likely to have a high count as well (Kohler et al., 1979).
|
|
|
FIG. 28.3. Radiography of unilateral cleft showing a wide defect in the area of the lateral incisor, which is shown with no supporting bone on the entire mesial surface. |
Children colonized with 5. mutans before the age of 2 years run a higher risk of developing dental caries than children colonized with the organism at a later age. Almost 50% of children with oral clefts had been colonized with S. mutans and 16% with lactobacilli at the age of 18 months compared to children without clefts, who showed 13% 5. mutans colonization. Kohler et al. (1983) found that 24% of 15-month-old children with mothers who had high levels of S. mutans were colonized with 5. mutans.
Children with clefts who took a bottle to bed have shown an increased risk for developing early childhood or nursing bottle caries. In a study by Lin and Tsai (1999), 39% of children reported a bottle-feeding habit. The overall prevalence of baby bottle nursing caries was 15.4%. The decayed-extracted-filled primary teeth (def) scores of bottle-fed children were significantly higher than those of children who were not bottle-fed. Parents and caregivers of bottle-fed babies showed a lack of motivation to perform regular preventive dental home care. Parents of non-bottle-fed children demonstrated significantly better dental care than parents of bottle-fed children regarding brushing frequency and brushing before bed.
Dental treatment of the infant and toddler centers on evaluation, prevention, education of parents, and management of dental problems resulting from the cleft. Prevention of dental disease is a major goal. The fluoride content of the child's water supply needs to be evaluated early. If the water supply has less than the optimum of 0.7 to 1.2 ppm, supplementation needs to be considered at 6 months of age. The level of supplementation is based on the fluoride level of the water and the child's age. A number of families use bottled water for drinking and cooking. If the child's major water intake is from nonfluoridated bottled water, complete or partial supplementation needs to be considered. The bottled water label usually will not indicate if the water is fluoridated. As soon as the first teeth erupt, parents should be instructed to clean them with a cloth when bathing the child.
|
|
|
FIG. 28.4. Unilateral cleft lip and palate showing a malformed tooth erupting ectopically along the cleft margin. |
Anticipatory Guidance
Anticipatory guidance, as used in pediatric health care, is the process of providing practical, developmentally appropriate health information about children to their parents in anticipation of significant physical, emotional, and psychological milestones. This information guides parents by alerting them to impending change, teaching them their role in maximizing their children's developmental potential, and identifying their children's special needs.
Areas of concern in anticipatory guidance in pediatric dentistry are oral development, fluoride adequacy, oral hygiene and diet, habits, nutrition, and injury prevention. Early evaluation and education of the parents as to the dental needs of their child is extremely important if comprehensive dental care is to be provided (Nowak and Casamassimo, 1995).
Special Needs
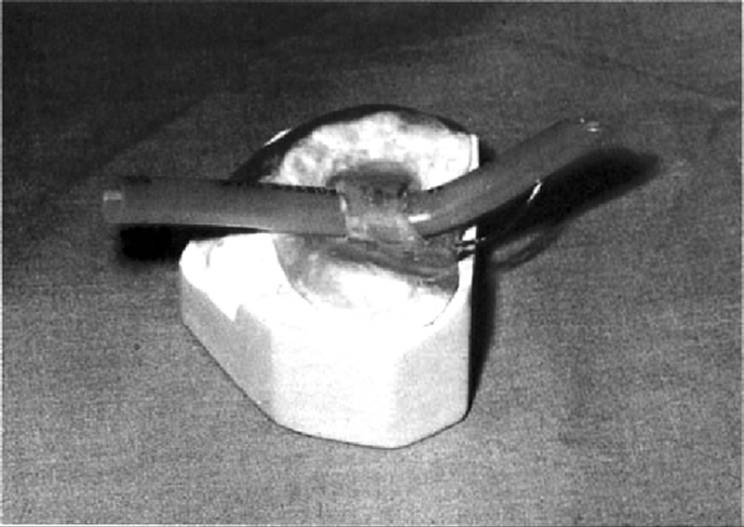
A small number of infants with cleft palate also present with glossoptosis, resulting in difficulty in managing the airway. Usually, this is a transitory problem that resolves itself in a short time as the child grows. Oral appliances to assist in the maintenance of an airway can be used in some cases, thus alleviating the need for other techniques, such as long-term intubation or tracheotomy. Appliances similar to denture bases without teeth have been developed. Impressions can be taken with either alginate or compound. Alginate gives a clearer impression of the cleft defect but runs the risk of material being left in the defect. Compound does not give as detailed an impression but is easier to remove when set. For short-term use, it is usually not necessary to use the undercuts of the defect for retention. With the use of denture adhesive as needed, the appliance does not have to extend into the cleft. The purpose in managing the airway is to use the appliance to hold endotracheal tubes or a wire loop extending posteriorly to hold the tongue forward off the posterior pharyngeal wall. The tube not only holds the tongue forward but also establishes a mechanical airway (Farrington, 1998). Once the basic appliance is complete, a loop of orthodontic wire can be attached with acrylic (Fig. 28.5). The exact length of the wire and amount of curvature will vary in each case. As a starting point, the wire loop should extend posterior to the appliance to a length that is about the same as the anteriorposterior length of the appliance. An endotracheal tube can be attached to the appliance by forming self-cure acrylic around a well-lubricated tube (Fig. 28.6). The tube should be of the same size as one that would be used to intubate that child. The natural curve will help to direct the tube down behind the tongue (Fig. 28.7).
Starting with the tube extending about the same length posterior to the appliance as with the wire loop, it can be extended or retracted as needed. The tube should extend back as far as the child will allow. At this point, it should be retracted a few millimeters. In some cases, use of a tube and a wire loop may be considered. The wire loop extends behind the tube and is used to increase the curvature of the tube and to keep it from irritating the posterior pharyngeal wall. The effectiveness of the appliance can be measured using a pulse oxymeter to measure saturation levels with and without the appliance.
|
|
|
FIG. 28.5. Basic palatal appliance with posterior wire loop to hold tongue down. |
|
|
|
FIG. 28.6. Basic palatal appliance with endotracheal tube added to aid in maintaining airway. |
|
|
|
FIG. 28.7. Position of appliance showing the endotracheal tube extending over the tongue to maintain the airway. |
Primary Dentition
As mentioned before, prevention and caries control are the same for the child with a cleft as for other children at the same age and state of development. Hence, more frequent recalls, at 3- to 4-month intervals, may be necessary to monitor oral health. Topical fluoride needs to be professionally applied regularly. In areas without optimal water fluoridation, prescription fluoride supplements should be considered. Use of pit and fissure sealants should be considered in selected cases. Oral hygiene instructions and dietary advice must be checked and reinforced.
Restorative care should be provided before carious lesions become extensive. Loss of a single tooth can complicate the overall treatment. Use of stainless steel crowns on carious primary teeth should be considered, especially if the tooth is to be banded as part of appliance therapy (King and Wei, 1988).
Establishment of a fairly normal occlusion is the overall dental goal. The pure mechanics of treatment must be tempered by the behavioral development and ability of the child to accept treatment and cooperate (Farrington, 1998).
Close supervision is needed because of the added risk the child has for dental disease, especially in the area of the cleft. Parents initially, and the child at the appropriate age, should be instructed in proper oral hygiene techniques. Ectopic eruption of teeth in the area of the cleft and redundant gingival and alveolar tissue make good plaque control difficult (Figs. 28.8,28.9). Children with cleft lip and/or palate have more decayed and filled teeth in the primary dentition than do children without clefts. Almost 50% of children with an oral cleft had S. mutans colonization by 18 months of age. This compares with studies of children without clefts, who had colonization rates of between 13% and 36%. Such early colonization indicates a high risk for dental caries in the primary dentition for children with cleft lip and/or palate (Bokhout et al., 1996).
Eruption of the primary dentition and occlusal development need to be followed closely. A high incidence of natal/neonatal teeth was found in unilateral (2.02%) and bilateral (10.6%) cleft groups. The findings in both groups were higher than the incidence reported in a noncleft group (0.05%) (Machado de Almeida and Gomide, 1996).
|
|
|
FIG. 28.8. Eruption of the lateral incisor into the site of the cleft, resulting in a crossbite; poor plaque control increases the risk of cervical caries. |
|
|
|
FIG. 28.9. The alveolar defect has resulted in the lateral incisor failing to properly erupt into occlusion. |
Dental treatment at this age centers on prevention, caries control, and support for the other disciplines involved. This includes removal of malformed teeth and replacement of teeth that may be needed to help with speech therapy. Occasionally, a child will be seen with an unrepaired hard palate or a hard palate fistula that cannot be closed.
A major concern should be patient management. The small child does not always distinguish between the examination and treatment of the various team members. To the young child, there is no difference between dental treatment and other care that involves the face and oral cavity. This is of special concern when the child needs restorative or oral surgical care. If the child needs extensive restorative care, consideration should be given to combining the dental care with some other surgical care, such as ear, nose, and throat surgery. In treating any young child where behavior is an issue, consideration should be given to restoration with stainless steel crowns on primary molars rather than alloys or composites. The goal in the restoration of any primary tooth should be that, with proper oral hygiene, a tooth should have to be restored only once.
Mixed Dentition
With the eruption of the first permanent molars, caries of the occlusal surfaces and morphological defects that require restoration or sealing may be expected (McDonald et al., 2000). Gray et al. (1991)found that the best predictor of dental caries in the first permanent molars of 7-year-olds was caries in three or more primary molars by 5 years of age.
Eruption of the permanent dentition during the elementary school years must be carefully observed. In boys with unilateral cleft lip and palate, eruption of the permanent maxillary lateral incisors and the permanent maxillary second molar is retarded on the cleft side. In boys with bilateral cleft lip and palate, the highest retardation of eruption was found in the permanent maxillary lateral incisor and the permanent maxillary first molar (Peterka et al., 1996). Ectopic eruption of both primary and permanent incisors is common. Lateral incisors may erupt in the cleft defect without periodontal support. These teeth are usually very unstable, are lost prematurely, or have to be extracted (Fig. 28.10).
Dental treatment centers on caries control, temporary replacement of missing teeth, general dental care, and support for the other services involved in the child's care. Preventive care centers on the expanded use of fluorides and occlusal sealants. Plaque control in the areas of the cleft can be difficult, and following surgery or grafts, the child and parents may be reluctant to adequately clean the areas. Prevention at this age is marked by acceptance of increasing responsibility by children for their own oral health. Parental involvement is still needed; however, the parents' role moves from one of performing the child's oral hygiene to that of active supervision. By the start of middle school, most children can provide their own basic oral hygiene. Parents do need to actively inspect the results of their children's oral hygiene practices. As the child gets older, home-applied fluoride gels and rinses need to be considered, especially in children with poor plaque control and a history of caries. The child must be able to follow instructions and properly expectorate before home-applied gels and rinses should be introduced. Fluoride rinses have been shown to be very effective when orthodontic and prosthetic appliances are used and plaque control is difficult (McDonald et al., 2000).
|
|
|
FIG. 28.10. The alveolar defect has resulted in the lateral incisor erupting into the arch without periodontal support. Note the rotation of the central incisor and the scar tissue from the lip repair. |
Alveolar grafts are usually carried out as the permanent maxillary canines begin their initial eruption. The graft provides a bed of bone into which the canine on the cleft side can erupt. Prior to grafting, expansion of the maxillary arch to correct crossbites and to align the alveolar segments is usually completed. Appliances to stabilize the arch, such as a transpalatal arch, may be placed for retention. It is critically important that oral hygiene and home care be excellent to reduce caries risk factors. Use of sealants on teeth being banded, especially molars, and frequent checking for loose bands are essential in caries prevention.
As the child grows older, appearance and replacement of missing teeth become more important to the child and parents. Removable and fixed appliances each have drawbacks. Removable appliance use for longterm tooth replacement has problems of compliance and proper care by the preteen child. Loss of appliances, when removed for eating and sports at school, is common. The frequently changing dentition at this age affects the fit and comfort of removable appliances. Fixed appliances, such as the lingual arch to hold replacement teeth, work well at this age (Figs. 28.11,28.12). Compliance issues are removed, but oral hygiene and increased caries risk become concerns. Banding permanent molars increases caries risk and makes oral hygiene more difficult; however, if the risk is recognized and a sound preventive program established, these appliances are very effective. When possible, consideration should be given to banding second primary molars instead of permanent molars. Although the caries and hygiene problems still exist, the long-term risk is reduced.
|
|
|
FIG. 28.11. Maxillary lingual arch with prosthetic teeth attached. |
|
|
|
FIG. 28.12. Maxillary lingual arch in place. Note the partial-eruption appearance of the lateral incisor to match the contralateral side. |
Young Permanent Dentition
The dental needs of the adolescent with a cleft are similar to the needs of children of the same age without a cleft except for the additional facial and oral problems caused by the cleft. Care mainly centers on the repair of malformed teeth and the replacement of missing teeth. Many children in this age group undergo orthodontic treatment. Incorporation of prosthetic teeth is an easy way to temporarily replace teeth and give the child an appearance similar to that of his or her peers (Figs. 28.13,28.14 and 28.15).
Dental caries continue to be the major dental infectious disease problem for adolescents. A rise in the caries attack rate continues with the eruption of the second permanent molars and premolars. Adolescents are still prone to tooth decay. Immature permanent teeth, an increase in susceptible tooth surfaces, and factors such as diet, independence in seeking or avoiding care, poor oral hygiene practices, and failure to comply with preventive recommendations contribute to dental and periodontal disease.
|
|
|
FIG. 28.13. During orthodontic treatment, a large space has been created due to missing teeth in the area of the cleft. |
|
|
|
FIG. 28.14. Prosthetic teeth to be incorporated into an orthodontic appliance. The acrylic ridge overlap and lingual wires prevent the teeth from rotating on the arch wire. |
The adolescent can still benefit from fluoride throughout the teenage years. Although the systemic benefit of fluoride for developing enamel is not considered necessary after the age of 16, the topical benefits of remineralization and antimicrobial activity still can be obtained through water fluoridation, professionally applied or prescribed fluoride, and fluoridated toothpaste.
|
|
|
FIG. 28.15. Prosthetic teeth wired into place in the orthodontic appliance. |
The American Academy of Pediatric Dentistry (1999) recommends that the adolescent benefit from a preventive dental program consisting of the following:
1. Fluorides
a. Systemic fluoride intake via optimal fluoridation of drinking water or professionally prescribed supplements to age 16 years or eruption of the second permanent molars is needed.
b. A fluoride dentifrice is recommended, to provide continuous topical fluoride benefit.
c. Regular professionally applied fluoride treatments through adolescence should be based on the individual patient's caries pattern and fluoride status of the community water.
d. Topical supplementation by home-applied fluoride is indicated by an individual's dental caries pattern or caries risk.
2. Oral Hygiene and Diet Management
a. Adolescents should be educated and motivated to maintain personal oral hygiene through daily plaque removal, including flossing. Professional cleaning and calculus removal is recommended, with a frequency determined by the dentist.
b. Dietary analysis and management should consider dental disease patterns, overall nutrient and energy needs, psychological aspects of adolescent nutrition, dietary carbohydrate intake, and wellness.
3. Sealants
Pit and fissure sealants can be of significant benefit. The occlusal surfaces of second permanent molars are highly prone to caries. Sealants are an effective decay-preventing measure that should be used on an individual basis.
Periodontal Disease
Adolescence seems to be a critical period in periodontal health. Data suggest that irreversible periodontal damage begins in late adolescence and early adulthood. Pubertal changes characteristically affect the periodontium with an increase in inflammation, which in most cases is managed by oral hygiene and professional care. Periodontal disease in patients with cleft palate is similar in extent to the general population. Patients with cleft lip, palate, and alveolus had a predisposition to deep periodontal destruction of teeth adjacent to the cleft (Schultes et al, 1999).
Crowded or malpositioned teeth, hypertrophic gingiva, orthodontic appliances, and prosthetic replacements can impede proper plaque removal and thus perpetuate periodontal disease. It is important to incorporate periodontal treatment into the comprehensive treatment as early as possible.
Missing Teeth
A significant concern in the dental care of the adolescent with a craniofacial cleft is missing teeth. As part of the team evaluation, the permanent replacement of missing teeth must be considered. As the permanent dentition is complete, decisions as to how to replace missing teeth must be made. Temporary replacement of anterior teeth, usually maxillary lateral incisors, may continue to be needed during orthodontic care or during the period of alveolar and periodontal grafting, to establish the continuity of the dental arch. Pontics may be incorporated into orthodontic appliances, and teeth may be replaced with removable or fixed appliances, such as acid etch bridges. Use of dental implants is becoming a standard of care for single tooth replacement. Although implants have been placed in the early teen years, this treatment is usually delayed until late adolescence, when growth and development, surgical treatment, and orthodontic care are complete.
Caring for the adolescent patient with a cleft is a rewarding endeavor. Science is unable to provide a decisive answer to many of the questions that guide treatment, so it becomes obligatory to let the patient have an expanded role in determining the course of treatment. This may require spending time listening to a patient who may not want to tell us anything at the time we want to hear it. With more time and more patience, a course can usually be plotted which will get both the practitioner and the patient to a desired destination (Canady, 1995).
Periodontal therapy should be an integral part of the total restoration of the function and esthetics of the cleft palate patient. Periodontal treatment should begin early and continue as supportive therapy.
The amount of periodontal destruction is more pronounced in the cleft lip and palate patient than in noncleft patients. Bacterial plaque accumulation is enhanced due to irregularly positioned teeth or displaced teeth, difficulty in closing the lips, mouth breathing, and inadequate personal oral hygiene care. It is important to appreciate the etiology of periodontal disturbances in cleft lip and palate patients so that periodontal disease can be diagnosed early and treatment initiated and maintained before, during, and after surgical, orthodontic, and prosthetic treatments (Santi et al., 1995).
In prosthetic treatment of cleft lip and palate patients, it is imperative to prevent regression and collapse of the alveolar segments and teeth after surgical and orthodontic correction, but it is also important that the treatment provide equal functional loading capabilities for the upper and lower jaws. Accordingly, some of the teeth in the upper jaw must be splinted across the cleft, to increase the functional loading capability and to prevent regression. Use of multiple-unit fixed prostheses, however, may create a number of problems, including extensive loss of sound tooth structure and increased difficulty with oral hygiene. It is desirable to include as few teeth as possible in the fixed prosthesis (Suzuki et al., 1995). Single tooth implants can be considered when esthetically and functionally restoring the dental arch. Cosmetically, the single tooth replacement is more acceptable than a multiunit bridge. Tooth structure is spared on healthy adjacent teeth, and the problem presented by large pulp chambers on abutment teeth in teenage patients is circumvented. A possible disadvantage is the necessity of adequate graft height and width to support the implant. In the case of placement of implants in grafted sites, it seems likely that the success of osseointegration would approach that of implants in nongrafted areas. Early failure of the implant should be evident in the first year after implantation (Verdi et al., 1991).
Once the permanent dentition has erupted and facial growth is complete, treatment of the adolescent is directed at prosthetic care to permanently replace missing teeth. The reason teeth are missing is not as important at this stage as the design and construction of the prosthesis.
Family Support
There are a number of excellent resources available to the family that provide information on the management of the child's oral health needs. The American Academy of Pediatric Dentistry web site provides information to parents, children, and professionals regarding proper oral health care for children of all ages. The American Dental Association also has an extensive array of information for the lay public and professionals on all aspects of oral healthcare, new products, and research. The American Dental Association can be contacted by phone, mail, or through its web site. The information available from these organizations addresses children with special needs but is basically directed at the needs of the average child. There are two organizations providing programs and support specifically related to individuals with cleft defects and other facial differences: (1) AboutFace in Canada (http://www.interlog.com/~abtface/aface.html) and AboutFace U.S.A. (http://www.interlog.com/~abtface/AUSA.html) and (2) the American Cleft Palate-Craniofacial Association (http://www.cleftline.org). The goal of the foundation is to provide information to parents of newborns with clefts and other craniofacial birth defects and to healthcare professionals. Both organizations provide a wealth of information through published material, web sites, and chapters throughout the United States and Canada. A major service these organizations offer parents and families is the opportunity to interact with parents of other children with similar problems. Chances for new parents to talk or correspond with others who “have been there” can help. The opportunity to see children who have been through the various levels of surgery and the results that may seem impossible to achieve when the newborn is first seen can help parents and other family members adjust to the initial trauma of this unexpected problem.
Regardless of the interaction an individual has in the oral healthcare of a child with a craniofacial defect, the goal of all those involved is to provide the general and specialty care needed for the child to pass through the various stages of oral development as easily and normally as possible.
References
Ameican Academy of Pediatric Dentistry (2001). American Academy of Pediatric Dentistry Reference Manual 2000–01. Pediatr Dent 22. Guidelines for Dental Health of the Adolescent, pp. 52–54.
American Cleft Palate-Craniofacial Association (1993). Parameters for Evaluation and Treatment of Patients with Cleft Lip/Palate or Other Craniofacial Anomalies. Pittsburgh: American Cleft Palate-Craniofacial Association.
Bokhout, B, van Loveren, C, Xavier, F, et al. (1996). Prevalence of Streptococcus mutans and lactobacilli in 18-month-old children with cleft lip and/or palate. Cleft Palate Craniofac J 33: 5, pp. 424–428.
Canady, J (1995). Emotional effects of plastic surgery on the adolescent with a cleft. Cleft Palate Craniofac J 32: 2, pp. 120–124.
Farrington, FH (1998). Management of the child with cleft lip and palate. In: Clinical Dentistry, Vol. 2, edited by J Clark. St. Louis: Mosby, Chapter 14, pp. 1–18.
Gray, MM, Marchment, MD, Anderson, RJ (1991). The relationship between caries experience in the deciduous molars at 5 years and in first molars of the same child at 7 years. Community Dent Health 8: 3–7.
King, NM, Wei, SH (1988). The management of children with cleft lip and palate. In: Pediatric Dentistry—Total Patient Care, edited by SH Wei. Philadelphia: Lea and Febiger, pp. 374–387.
Kohler, B, Bratthall, D, Krasse, B (1979). Intrafamilial levels of Strep, mutans and some aspects of the bacterial transmission. Scand J Dent Res 86: 35–42.
Kohler, B, Bratthall, D, Krasse, B (1983). Preventive measures in mothers influence the establishment of the bacterium Streptococcus mutans in their infants. Arch Oral Biol 28: 225–231.
Latham, RA (1980). Orthopedic advancement of the cleft maxillary segment: a preliminary report. Cleft Palate J 17: 227–233.
Lin, YJ, Tsai, C (1999). Caries prevalence and bottle-feeding practices in 2-year-old children with cleft lips, cleft palate, or both in Taiwan. Cleft Palate Craniofac J 36: 622–626.
Machado de Almeida, C, Gomide, MR (1996). Prevalence of natal/neonatal teeth in cleft lip and palate infants. Cleft Palate Craniofac J 33: 4. pp. 397–399.
McDonald, RE, Avery, DR, Stookey, GK (2000). Dental caries in the child and adolescent. In: Dentistry for the child and adolescent, edited by RE McDonald and DR Avery. St. Louis: Mosby, pp. 209–246.
McNeil, CK (1950). Orthopedic procedures in the treatment of congenital cleft palate. Dent Rec 70: 126–132.
Nowak, AJ, Casamasssimo, PS (1995). Using anticipatory guidance to provide early dental intervention. J Am Dent Assoc 126: 1156–1163.
Peterka, M, Peterlpva, R, Likovsky, Z (1996). Timing of exchange of the maxillary deciduous and permanent teeth in boys with three types of orofacial clefts. Cleft Palate Craniofac J 33: 4, pp. 318–323.
Santi, E, Weinberg, MA, Abitol, TE (1995). Periodontal and prosthetic treatment of a cleft lip and palate patient: a case report. Cleft Palate Craniofac J 32: 4, pp. 346–349.
Schultes, G, Gaggl, A, Karcher, H (1999). Comparison of periodontal disease in patients with clefts of palate and patients with unilateral clefts of lip, palate, and alveolus. Cleft Palate Craniofac J 36: 4, pp. 322–327.
Suzuki, R, Taniguchi, H, Ohyama, T (1995). Prosthodontic abutment in four patients with unilateral cleft lip and palate. Cleft Palate Craniofac J 32: 5, pp. 346–349.
Verdi, FJ, Lanzi, GL, Cohen, SR, Powell, R (1991). Use of the Branemark implant in the cleft palate patient. Cleft Palate Craniofac J 28: 3, pp. 301–304.