Andrew C. Lidral
Katherine W.L. Vig
The role of the orthodontist on a cleft palate team was defined when the cleft palate team approach was recognized as the most appropriate method to manage the care of patients with facial clefts. In the past, individuals with clefts and craniofacial anomalies underwent a succession of evaluations and hospitalizations by their independent caregivers. This individualized delivery of care was considered in the best interest of the patients in spite of additional hospital admissions and general anesthetics. However, this led to the fragmentation of care and higher costs and risks. A team approach for providing care has been developed and is the contemporary standard endorsed by the American Cleft Palate Association, which was established in 1943. In 1972, craniofacial teams became established as an extension to the cleft palate team, and the organization was renamed the American Cleft Palate-Craniofacial Association. This was a natural development to the cleft palate team as clinical geneticists and dysmorphologists became increasingly aware that facial clefts were part of a phenotypic spectrum of craniofacial anomalies (Shprintzen et al., 1985).
The team approach to comprehensive care requires the orthodontist to work in a collaborative way to determine the timing and sequencing of treatment interventions. This patient-centered care by an interactive and evidence-based team of caregivers provides the basis for a rational approach to diagnosis and treatment planning and delivery. Because there are multiple methods and alternative treatment interventions available, the team approach to management requires that patients and their parents be aware of the choices with a risk/cost/benefit appraisal so that they can make an informed decision, understanding the consequences of the different options available, especially in light of emerging technologies and treatment modalities for which long-term outcomes are not available. The “Parameters for evaluation and treatment of patients with cleft lip/palate or other craniofacial anomalies,” which was the product of a consensus conference on recommendations for the care of patients with craniofacial anomalies, serves as a guideline for the clinical management of these anomalies in a patient-oriented manner (American Cleft Palate-Craniofacial Association, 1993).
The purpose of this chapter is to discuss the orthodontic management of the patient with cleft lip and/or palate in the context of a team approach. Orthodontic intervention should be confined to discrete stages in skeletodental development of the craniofacial complex and should not be considered a continuum of treatment from birth to adulthood.
The Team Approach
The timing and sequencing of orthodontic care may conveniently be divided into four distinct developmental periods. These are defined by age and dental development and should be considered time frames for the accomplishment of specific objectives. This avoids the all too common tendency to allow an early phase of treatment intervention to extend through childhood into adolescence and beyond. The timing and sequencing of orthodontic treatment are not carried out in isolation from other members of the team but as a result of collaborative decisions made in a coordinated manner (Fig. 29.1). Several texts provide specific details of treatment intervention, but the overall care of affected infants should rely on team decisions rather than a series of conflicting events sequenced by individual specialists on a team (Surgeon General's Report, 1987). The orthodontist serving on a cleft palate team should consider additional priorities other than malocclusion. The timing and sequencing of treatment should be sensitive to other interventions by specialists on the team, to provide the affected individual with a patientcentered interdisciplinary approach that follows critical pathways (Vig and Turvey, 1985; Turvey et al., 1995). These have been well defined in a document on critical elements of care for children with special health problems, which was developed by the Washington State Department of Health (1997). These guidelines were developed through a consensus process including primary and tertiary care providers, family members, and representatives from a health plan.
|
|
|
FIG. 29.1. Members of a cleft palate-craniofacial team. |
With the understanding that children born with cleft lip and/or palate should be treated by an interdisciplinary team approach, the following four time periods in the child's development will be used as a framework for discussing and recommending defined objectives in the care of this special group of patients.
The Neonate
Presurgical orthopedics or neonatal maxillary orthopedics typically is initiated during the first week following birth unless there are complications due to other congenital anomalies or medical problems (Burston, 1958; McNeil, 1964; Pruzansky, 1964; Jolleys and Robertson, 1972; Hotz et al., 1978; Rosenstein 1982). This treatment is usually carried out by the orthodontist, the pediatric dentist, or the prosthodontist. The goals of presurgical orthopedics are to align both the soft and hard tissues of the cleft segments to approximate the normal neonatal anatomy. This would presumably facilitate closure of the cleft lip and result in fewer postoperative complications such as dehiscence and scarring. In addition, for surgeons advocating primary bone grafting or periosteoplasty, infant orthopedics is a necessity to allow for closure of the alveolar segments. Claims have also been made that restoring the anatomy to normal leads to normalization of future growth. The popularity of infant orthopedics and primary bone grafting was at its height in the 1960s (Long et al., 2000), but reports that primary bone grafting adversely affected the potential growth of the midface and that no long-term benefit was achieved led to a decrease in the use of infant orthopedics by most teams as a routine intervention before surgical lip repair (Pruzansky, 1964; Jolleys and Robertson, 1972; Hotz et al., 1978; Millard 1999). Furthermore, studies comparing various treatment regimens suggested that neonatal maxillary orthopedics produced little effect on developing malocclusions if assessed when the child was 10 years old, especially if treatment had included primary bone grafting to stabilize and prevent maxillary collapse in the infant (Moisted et al., 1993).
|
|
|
FIG. 29.2. A: Neonate with complete unilateral cleft lip and palate. B: Neonatal with presurgical orthopedics via lip taping to approximate the segments before cleft lip repair. C: Postsurgical view of definitive lip repair. |
However, as an adjunctive procedure to primary definitive lip repair, the procedure was recognized by plastic surgeons as having benefits and its popularity has recently returned but with objectives different from eliminating orthodontic treatment later in development. Specifically, nasal molding has been advocated as a mechanism to restore normal nasal symmetry and anatomy, while eliminating the need for future nasal revisions. Numerous articles regarding neonatal orthopedics have been published, and the enthusiasm of many clinicians in this field attests to the variety and complexity of the appliances created (Moisted et al., 1993; Winters and Hurwitz, 1995; Grayson et al., 1999). The one feature that all of these appliances have in common is that they adjust the position of the cleft segments into a more ideal relationship prior to definitive surgical repair of the lip (Fig. 29.2). Some are fixed using pins inserted into the maxilla (Millard et al., 1999). This requires at least two general anesthesia procedures, and there is the risk of damaging a developing tooth bud by the inserted pin. This remains a controversial topic, although there are several institutions that continue neonatal maxillary orthopedics and primary bone grafting with substantial benefits reported (Rosenstein et al., 1982; Millard 1999). However, the emerging evidence is only of short-term benefit for presurgical orthopedic appliances, and this needs to be weighed against the increased burden of care due to the multiple number of clinic visits necessary to adjust the appliance during the first year of life (Ross and MacNamera, 1994; Santiago et al., 1998; Severens et al., 1998; Grayson 1999). Long-term outcomes assessing the growth of the midface and both nasal and lip esthetics will be necessary to determine the benefits of presurgical orthopedics and nasal molding.
Although neonatal maxillary orthopedics continues to be practiced in a number of centers in both the United States and Europe, it is not generally considered an essential or desirable routine intervention for treatment of the infant with a cleft. Nonetheless, the molding of segments achieved by these appliances does make definitive lip repair easier for the plastic surgeon, especially in patients with a severely protruding pre- maxilla due to a bilateral cleft lip (Vig and Turvey, 1985).
Surgical lip adhesion in infancy is another technique employed to align the segments, yielding results similar to those obtained with infant orthopedic appliances. When the segments have been aligned following lip adhesion, definitive lip repair, including ensuring muscle continuity, is performed. This early surgical repair of the lip by an adhesion technique has much to commend it as the parents are not required to remove or adjust appliances, the cosmetic appearance is improved with a relatively minor initial surgical procedure, and postoperative care by the parents is minimal. The most serious problem with this approach is the potential of wound dehiscence and the need for an additional surgery (Hotz et al., 1978). Currently, lip adhesion is not universally accepted as a method of realigning the segments before definitive repair of the lip.
Although definitive repair of the lip is usually achieved by the time the infant is 3 to 6 months old, repair of the palate is typically delayed until 12 months to 2 years of age. This is also a controversial issue, and many methods are available for repairing either just the soft palate or both the hard and soft palate simultaneously. The rationale for the timing of palatal repair is related to the speech and language development of the child, which is usually in conflict with the effect of early surgical repair and the constraints of scar tissue on the growth and development of the maxillary complex (Long et al., 2000). Early repair of the palate may have a profound effect on the developing maxilla and dentition. The most common malocclusion of patients who have had repair of a cleft lip or palate is a dental crossbite of anterior and/or posterior teeth, due to maxillary hypoplasia as a result of surgical scaring. The severity of the malocclusion may be associated with certain methods of surgical repair of the palate.
Primary Dentition
At 2 to 3 years of age, the establishment of the primary dentition permits classification of the type of developing malocclusion. This may be part of the diagnostic regime in which the contribution of the skeletal and dental components is specified relative to the etiology of the malocclusion.
The facial soft tissues may mask the underlying skeletal deficiency of the midface in young children (Fig. 29.3). With growth of the intermaxillary space in three dimensions, redistribution of the facial soft tissue changes as the chubby face of infancy takes on the more mature and defined proportions of the child. These facial characteristics reflect the underlying skeletal discrepancy more accurately than in the younger child. The dentition often reflects the skeletal discrepancy, especially if the dentoalveolar component has not compensated for the skeletal relationship and the axial inclination of the teeth reflects the skeletal discrepancy. Typically, dental compensation for maxillary skeletal deficiency results in retroclination of mandibular incisors with proclination of the maxillary incisors to eliminate the anteroposterior discrepancy (Fig. 29.4).
|
|
|
FIG. 29.3. A: Frontal view of a 6-year-old girl with repaired bilateral cleft lip and palate. B: Profile view indicating mild midfacial deficiency in the paranasal and infraorbital regions. |
|
|
|
FIG. 29.4. A: Intraoral view in occlusion of the same child shown Figure 29.3. Note the normal occulsion on the nonaffected side and the anterior crossbite on the affected side. B: Panorex radiograph indicating congenitally absent maxillary lateral incisor associated with the cleft site. C: Lateral skull radiograph in early mixed dentition with superimposed tracing. |
The more upright primary incisors may result in an anterior crossbite and/or posterior crossbite, which may be unilateral or bilateral and with or without a functional shift of the mandible. This shift occurs when the child closes the teeth together. To eliminate mandibular shifts, orthodontic treatment may be indicated to remove the interfering contact by tooth movement. This may involve the maxillary incisors if an anterior crossbite exists or expansion of the posterior segments to eliminate a posterior crossbite (Fig. 29.5). The dental crossbite relationship is a continuing problem once the dentition is established and may be a reflection of the underlying skeletal discrepancy for which growth modification and redirection may be indicated with a facial mask (Fig. 29.6) Many factors need to be considered in determining whether to initiate orthodontic treatment during this stage, including the ability of the child to cooperate, severity of the malocclusion, timing any secondary bone grafts, psychosocial issues, speech considerations, and the need for future orthodontic treatment in either the early mixed or permanent dentition. Given that typically there will be a need for orthodontic treatment in the early mixed and permanent dentitions and there is no evidence for a benefit of treating during the primary dentition, orthodontic treatment may be best deferred until it can be combined with other treatment goals to shorten the overall length of time a patient is in orthodontic treatment.
|
|
|
FIG. 29.5. Palatal expander with bands cemented on the maxillary second premolars and canines with palatal hooks to attach the protraction face mask. |
|
|
|
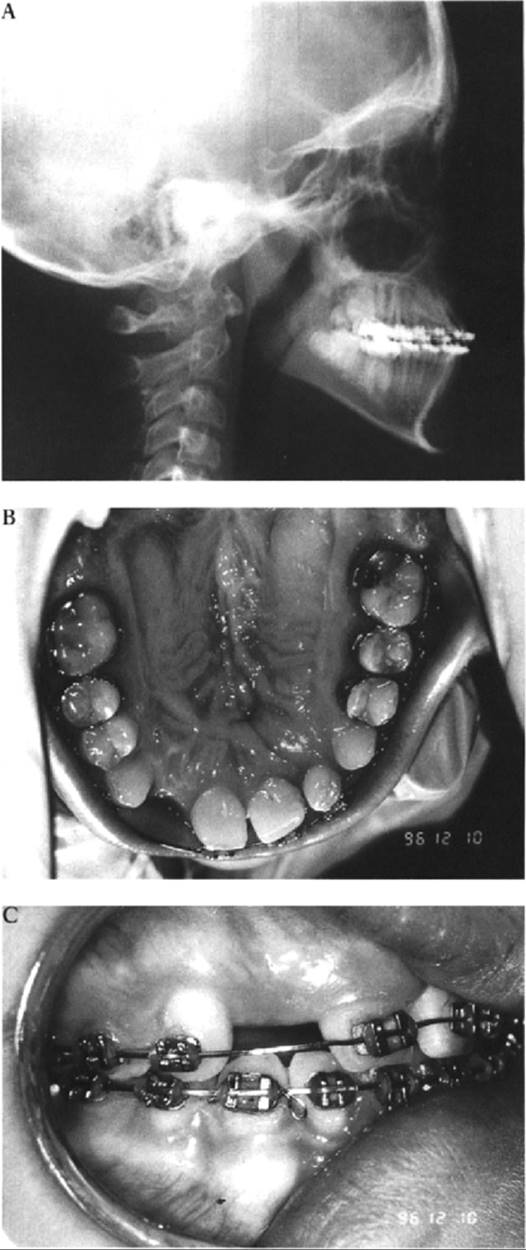
FIG. 29.6. A: Eight-year-old boy with repaired unilateral complete cleft lip and palate with sagittal and transverse maxillary deficiency. B: Lateral skull radiograph of the same boy. Note the 7 mm reverse overjet. C: Protraction face mask with elastics attached to palatal hooks (see Fig. 29.5). D: Lateral and anterior crossbites improving with palatal expansion maxillary dental protraction. |
Severe sagittal skeletal discrepancies in the primary dentition, most commonly caused by maxillary hypoplasia, are a more complex problem. Modification or redirection of growth has been advocated, and use of functional or orthopedic appliances and the forward protraction face mask, as promoted by Delaire, has had some success (Rygh and Tindlund, 1995). More commonly, the “apparent correction” is achieved by a transient change in the position of the teeth only so that, with subsequent growth, the skeletal discrepancy is once again reflected in the re-establishment of the malocclusion. Early treatment procedures, in common with neonatal maxillary orthopedics, require a long-term follow-up period to evaluate the outcome of treatment when the child reaches adolescence (Figs. 29.6,29.7). Excessive changes attributable to therapeutic growth modification are now considered the exception rather than a predictable outcome of this early intervention (Tindlund, 1989, 1994; Ishikawa et al., 2000). Careful consideration must be given to the severity of the skeletal discrepancy, to determine the likelihood of successful growth modification and subsequent long-term results vs. conventional orthognathic surgery at a later stage. It may be more conservative to provide a combined orthodontic/orthognathic surgical treatment plan than to promote long-term growth-modification strategies that may not ultimately be successful.
Mixed Dentition
The mixed dentition stage starts at approximately 6 years of age with the eruption of the first permanent molars and incisors. Further growth of the craniofacial complex often accentuates a previously mild skeletal discrepancy. As the permanent incisor teeth erupt adjacent to the cleft site, they will typically be rotated, misplaced, or malformed (hypoplastic). In addition, there may be supernumerary, absent, or peg-shaped incisors. This is considered a result of early disruption of the dental lamina at the cleft site, which subsequently affects the developing tooth germs (Figs. 29.8,29.9a). As deficiency of tissue is an inevitable consequence of clefting, not only may there be missing teeth but also the supporting alveolar bone at the cleft site is variable. In the past, rehabilitation of the maxillary dentition was dependent on the expertise of the prosthodontist to replace the missing teeth and alveolus in the cleft defect with a fixed or removable partial denture, or in the most severe cases, an overdenture. This challenge to restore the cleft site was resolved with the advent of secondary alveolar bone grafting in the 1970s (Boyne, 1974; Boyne and Sands, 1976; Abyholm et al., 1981). This provided the orthodontist with one of the most important milestones in managing the cleft site, allowing for the orthodontic movement of teeth across the intact alveolus or the placement of implants for the prosthetic replacement of missing teeth in the cleft site (Fig. 29.9). Elimination of the residual cleft provided a major advance in the contemporary management of the cleft maxilla and is an example of the outcome a coordinated and problem-oriented approach to developing new strategies of treatment (Turvey et al., 1984; Vig et al., 1995; Vig, 1999).
|
|
|
FIG. 29.7. A: Facial profile after 9 months of protraction face mask therapy and palatal expansion (same patient shown in Fig. 29.6). B: Lateral skull radiograph demonstrating anterior crossbite correction. C: Intraoral view with correction of anterior and posterior crossbites. |
|
|
|
FIG. 29.8. A: Facial view of 10-year-old girl with repaired bilateral cleft lip and palate. B: Lateral skull radiograph of mixed dentition with anterior crossbite. C: Intraoral photograph with bilateral posterior and anterior crossbites. |
Alveolar Bone Grafting
The success of alveolar bone grafting requires collaborative treatment planning between the orthodontist, surgeon, and other team members (Troxell et al., 1982; Bergland et al., 1986; Semb, 1991). Secondary alveolar bone grafting offers the following five main benefits:
1. Bone support for unerupted teeth and those teeth adjacent to the cleft. If a bone graft is placed before eruption of teeth adjacent to the cleft, it will improve their periodontal support. If a bone graft is placed after eruption of the canine, the bone will not improve the crestal height of support and will quickly resorb to its original level.
2. Closure of oral-nasal fistulas. By utilizing a threelayered closure technique, with the graft sandwiched between the two soft tissue planes, a high success rate of fistula closure has been observed.
3. Support and elevation of the alar base on the cleft side. This benefit helps to achieve nasal and lip symmetry and provides a stable platform on which the nasal structures are supported. If this procedure is performed alone or combined with alar cartilage revision, satisfactory esthetic changes occur.
4. Construction of a continuous arch form and alveolar ridge. This benefits the orthodontist by moving teeth into the cleft site and the surgeon and prosthodontist by enabling a more esthetic and hygienic prosthesis or implants to be placed when teeth are missing.
5. Stabilization and some repositioning of the premaxilla in the bilateral cleft patient.
Controversies concerning alveolar bone grafting require a rational and evidence-based approach for resolution. These relate to the timing of the alveolar bone graft, the sequencing of orthodontic treatment to correct a transverse discrepancy with palatal expansion, and the sites and types of bone for the graft (Zins and Whittaker, 1979; Vig, 1990, 1999).
Timing of Bone Graft
The timing the bone graft surgery is more dependent on dental development than on chronological age. Ideally, the permanent cuspid root should be approximately one-half to two-thirds formed at the time the graft is placed (Fig. 29.9a). This generally occurs between the ages of 8 and 11 years (Vig, 1992). Rarely is the graft placed prior to this time, although occasionally it may be placed at an earlier age to improve the prognosis of a lateral incisor. Once teeth have erupted into the cleft site, their periodontal support will not improve with a bone graft. Instead, the height of the crest alveolar bone resorbs to its original level. It is for this reason that it essential to perform the graft prior to the eruption of permanent cuspid, or if the lateral incisor will erupt into the cleft, the graft should be placed earlier. Although results from primary bone grafting have indicated a significant adverse effect on maxillary development, performing a secondary bone graft at an age when maxillary growth is almost complete has resulted in no effect on subsequent facial development (Semb et al., 1988).
|
|
|
FIG. 29.9. A: Intraoral radiograph demonstrating successful bone grafting (same patient shown in Fig. 29.8). Note missing permanent lateral incisor on the left with the canine erupting through the graft adjacent to the central incisor and a malformed right lateral incisor, which will be extracted to allow the permanent canine to erupt adjacent to the right central incisor. B: Central incisors moved labially to correct anterior crossbite. Note the mild maxillary deficiency, which has been camouflaged by proclining maxillary incisors. C: Intraoral view following correction of the anterior crossbite. D: Facial appearance following labial movement of the maxillary incisors to correct the crossbite. |
Sequencing of Treatment
Secondary bone grafting has been divided into the categories of early (2-5 years of age), intermediate (6-15 years of and late (16 years to adult). Since the results of an Oslo study, in which 378 consecutive patients who had undergone alveolar bone grafting, were published (Bergland et al., 1986), contemporary opinion supports the intermediate period as the most appropriate time for grafting. This has the greatest benefit and least risk for interfering with midfacial and skeletodental growth and development. This sequencing of procedures, including presurgical orthodontics, requires interdisciplinary communication and cooperation, but the benefit is improved and more predictable patient care.
Surgical Technique
The surgical procedure utilizes tissue lining the cleft defect to construct a nasal floor and close the nasal side of the oral-nasal fistula. The cleft lining is elevated in a subperiosteal plane, which leaves bare the osseous margins of the cleft. Cancellous bone taken from the ilium, cranium, or mandibular symphysis is then packed into the cleft defect. Cortical bone is avoided because the cancellous bone revascularizes quickly and is less likely to become infected (Zins and Whittaker, 1979). Once the cleft defect is packed with bone and the margins are overpacked, soft tissue coverage of the graft is required. The donor site is chosen by the surgeon. Traditionally, the iliac crest, ribs, and tibia have been utilized because of their abundant supply of cancellous bone. The morbidity of harvesting bone from these sites results in most patients being hospitalized postsurgically because of complications associated more with the donor site than the oronasal recipient site. The cranium has become an alternative site from which to harvest cancellous bone because of the lack of associated pain and the reduced hospitalization time involved. However, the operating risks are higher and the abundance of cancellous bone reduced. The mandibular symphysis is another donor site that is associated with relatively little pain and allows for early hospital discharge. This site should be utilized only when the permanent mandibular cuspids have been carefully located so as to minimize the chances of injuring these developing teeth.
Orthodontic Considerations Associated with Secondary Bone Grafting
Transverse Dimension
Orthodontic expansion of the posterior segments (Fig. 29.5) preoperatively may improve the occlusion but also may widen an existing fistula. The larger fistula in most cases is favorable because it provides better access at surgery, and closure of the palatal and vestibular fistulas occurs following the cancellous bone graft. Retention of the corrected crossbite with orthodontic appliances postsurgically may be indicated as the bone graft is unlikely to maintain the expansion initially.
Incisor Alignment
Alignment of the incisors adjacent to the cleft will be limited by the available bone into which the roots of the teeth can be moved. Appliances may be placed presurgically but not activated. This permits the initiation of orthodontic tooth movements within 3 to 6 weeks following placement of the bone graft. The early movement of the roots into the grafted bone appears clinically to consolidate the alveolar bone and improve the crestal height.
Canine Eruption
The maxillary canine erupts through the grafted bone following surgery (Fig. 29.9a). With orthodontic movement, enough space is created in the arch to allow the cuspids to erupt successfully. Supernumerary teeth are removed at the time that the bone graft is placed, to create an unobstructed path of eruption for the cuspid. Often, the canine will erupt rapidly once the bone is available, and if the lateral incisors are malformed or absent, especially in patients with bilateral clefts, the canine is encouraged to erupt adjacent to the central incisors. This is an advantage in closing space as it avoids the need for prosthetic replacement of the absent lateral incisors. However, canine substitution needs to be considered in light of the occlusion and the need for orthognathic surgery.
Permanent Dentition
Following eruption of the canines and premolars, the permanent dentition is established. During this time, the adolescent growth spurt and onset of puberty occur. The skeletal discrepancy becomes accentuated, and both facial appearance and occlusal relationships deteriorate (Fig. 29.10). This occurs at a time when the individual is most self-conscious of his or her appearance. Facial scars already detract from the cosmetic appearance, and derogatory comments by peers may have a profound psychological effect. At this time, involution of the adenoidal lymphoid tissue occurs, often with a consequent impairment of speech and hyper-nasality. With a decline in both cosmetic appearance and speech communication, many patients have a special need for early intervention by surgeons, orthodontics, and speech therapists.
Growth Considerations
Unilateral complete clefts of the lip and palate typically become more maxillary-deficient and mandibular-prognathic in appearance. Typically, this is a result of sagittal maxillary deficiency (Kuijpers-Jagtman and Long, 2000; Will, 2000). However, vertical maxillary deficiency may also accentuate the class III tendency, resulting in overclosure of the mandible to achieve occlusion of the teeth. It is important to evaluate clinically the extent of overclosure and to measure the interocclusal clearance at the premolar region with the patient in a resting posture. Alternatively, a class III skeletal relationship can be camouflaged by increasing the vertical dimension to rotate the mandible down and back. Careful consideration must be made to ensure that any camouflage treatment is an acceptable option, depending on the patient's desires, esthetics, occlusion, and biological limits. The class III dental relationship also accentuates the transverse discrepancy. To evaluate the occlusion, study models of the teeth will be necessary so that the relationship of the maxillary to mandibular dentition can be accurately assessed in all three dimensions, taking into account the final sagittal occlusion. Facial growth is the result of the interaction of genetic and environmental factors. Continued growth in early adulthood may enhance or detract from treatment results obtained during childhood and adolescence. These dynamic properties of the face make the management of facial growth both challenging and rewarding (Rygh and Tindlund, 1995; Kuijpers-Jagtman and Long, 2000; Will, 2000). A patient whose orthodontic treatment in the permanent dentition allowed camouflage of the mild skeletal discrepancy and prosthetic replacement of the maxillary right lateral incisor is shown in Figures 29.11-29.13.
|
|
|
FIG. 29.10. Intraoral view of the same patient illustrated at 6 years of age in Figure 29.3. Note anterior crossbite re-establishing as patient undergoes her pubertal growth spurt. |
|
|
|
FIG. 29.11. A: Comprehensive orthodontic treatment with camouflage for stabilized skeletal discrepancy (same patient shown in Figs. 29.3 and 29.10). Note the proclined maxillary incisors and retroclined mandibular incisors. B: Occlusal view showing missing right lateral incisor and left lateral incisor, which is smaller than normal. C: Intraoral lateral view showing class I canine relationship and stable overjet and overbite. |
|
|
|
FIG. 29.12. A: Same patient as illustrated in Figures 29.3,29.10, and 29.11 at age 13 following orthodontic treatment and nose and lip revisions. B: Profile view showing mild midfacial deficiency and paranasal flattening. C: Facial view of patient smiling. Note the symmetry of the upper lip in function. The patient is very satisfied with the facial and dental outcomes. D: Lateral skull radiograph demonstrating class I camouflaged occlusion. E: Panorex radiograph with cleft site successfully bone-grafted and adequate space for implant placement to prosthetically replace the congenitally missing lateral incisor due to the cleft alveolus. F: Class I incisal relationship with some overbite reduction. G: Maxillary occlusal view demonstrating closure of palatal oronasal fistula and adequate bony ridge depth for an implant replacement of the missing lateral incisor. H: Mandibular occlusal view illustrating a well-aligned and symmetrical arch form. |
Skeletal-Facial Considerations
Examination of facial balance and proportions is essential in determining a treatment plan that combines surgery and orthodontics. This clinical evaluation should be carried out with the patient standing so that the overall stature can be taken into consideration. Fullface and profile assessments will provide a database incorporating all three dimensions, and this information should be documented with the patient in a resting position, smiling, animated, and in occlusion. Cephalometric analysis and surgical prediction tracings will provide further information for deciding whether a patient should be treated by orthodontics alone or in combination with a surgical orthognathic procedure. If the skeletal discrepancy is mild and esthetic concerns are minimal, dental compensation by orthodontic treatment alone may be recommended (Figs. 29.9,29.11,29.12,29.13).
Alterations in the axial inclination of teeth may adequately camouflage the skeletal relationship. However, caution should be taken as the individual may outgrow the dental correction so that ultimately skeletal surgery may be necessary to obtain a normal occlusion.
|
|
|
FIG. 29.13. A: Profile of the same patient at age 16 showing stability of the skeletal relationship. B: Smiling view after prosthodontic treatment via an implant for tooth number 7 and esthetic recountouring of tooth number 10. C: Intraoral view of prosthodontic treatment in combination with gingivoplasty to restore the tissue contours and position for an improved tooth display and better gingival symmetry. D: Radiograph showing complete osteointegration of implant prosthesis in the former site of the cleft alveolus. |
If surgery is necessary, the presurgical phase of orthodontic treatment will require decompensation of the dentition so that the maxillary and mandibular teeth are placed in their correct relationship to the underlying skeletal bases. If orthodontic therapy has achieved the ideal relationship of the dentition to their skeletal bases, surgical correction of the skeletal discrepancy will result in normal class I occlusion and a normal skeletal relationship. In the past, using conventional orthognathic surgical techniques for patients with severe maxillary hypoplasia, it was not uncommon to advance the maxilla as much as possible, with the limit being the scar tissue from the lip and palatal repairs. The remaining skeletal discrepancy would then be corrected with a mandibular setback. Essentially, this was a surgical compromise due to the inability to predictably correct the underlying maxillary hypoplasia. With the advent of distraction osteogenesis, it may be possible to correct severe maxillary hypoplasia solely by advancing the maxilla (Cohen et al., 1997; Polley and Figueroa, 1998). This would be accomplished by tissue expansion of the scar tissue at the same time distraction osteogenesis is performed. However, this is an emerging treatment modality that currently has no long-term follow-up results. Questions related to how much to overcorrect the occlusion if utilized on a growing child and the effects of surgery on any remaining growth remain. Also, distraction osteogenesis may not negate the need for a conventional osteotomy to detail the occlusion due to the inability to precisely control the maxilla during distraction. Again, the treatment benefits need to be weighed vs. the burden of care and considered in light of the scientific evidence of positive outcomes (Dalston et al., 1988; Shaw et al., 1995).
Treatment Coordination
The timing and sequencing of orthodontic treatment require close communication with the team. Deciding to delay surgical orthodontic treatment until growth is stabilized may be sound judgment but not always in the patient's best interest, especially when psychosocial development is affected. In some instances, skeletal surgery may be indicated before growth is completed, knowing that a further procedure may be necessary should the patient outgrow the correction. As a general rule, skeletal surgery, orthodontic intervention, and final prosthetic rehabilitation should be completed before soft tissue revision or rhinoplasty is instituted. The outcome of soft tissue surgical procedures when com bined with surgical orthognathic movement of the maxilla and mandible is unpredictable.
Orthodontic Intervention
A coordinated approach to the presurgical phase of orthodontic treatment will be indicated before the surgical procedure. Approximately 12 to 18 months of orthodontics will usually be necessary to align the teeth, correct any midline discrepancy, coordinate arches, and localize space for prosthetic replacement of the teeth. The provision of space for surgical cuts between both the crown and the roots of adjacent teeth is also an important part of the presurgical preparations. Placement of full-sized arch wires with lugs provides a means of intermaxillary fixation at the time of surgery as rigid internal fixation is performed. The goal of the postsurgical phase of orthodontics is to detail the occlusion in coordination with any future prosthodontic treatment, and this should be completed within 4 to 6 months.
Summary
The orthodontist's role on the cleft palate team requires close collaboration with the other team members. The rationale of timing and sequencing orthodontic treatment has been discussed in four periods of development: (1) neonatal or infant maxillary orthopedics, (2) orthodontic considerations in the primary dentition, (3) mixed dentition orthodontics to include presurgical recommendations before an alveolar bone graft and its rationale for use, and (4) final treatment in the permanent dentition using orthodontics alone or orthognathic surgery combining an orthodontic and surgical approach to the correction of dental and skeletal components of malocclusion as well as facilitating any neeessary prosthodontic treatment.
Speech considerations and the communicative skills of the patient with a cleft are important aspects in planning orthognathic surgery for this group of patients. Also, subsequent nose and lip revisions for cosmetic improvement must not be underestimated in the enhancement of the final result following correction of the skeletal and dental discrepancies. Provided the timing and sequencing of appropriate treatment modalities are planned in a closely coordinated, problemoriented approach by the team members, patients with clefts should have optimal functional and esthetic results. Outcome measures for reporting the results of surgical interventions require that valid and reliable measures be identified and implemented (Dalston et al., 1988; Shaw et al., 1995). The ultimate outcome of team-based care is to have a fully rehabilitated patient who is satisfied with the treatment outcomes in terms of speech, hearing, occlusion, facial, and dental esthetics such that he or she needs only conventional dental and medical preventive therapies typical of any adult and possesses optimal self-esteem to develop his or her full potential.
Acknowledgements
We are indebted to Dr. Jack Lude for permission publish Figure 29.2 and to the patients and their families for agreeing to participate in this publication. In addition, we extend gratitude to the orthodontic residents and to the members of the cleft palate team at Children's Hospital of Columbus, Ohio, including Drs. Robert Ruberg, Peter Larsen, Brent Buchele, Rafael Villolobos, Ron Berggren, James Ferraro, Gregory Wiet, Michael Martyn, Darryl Willett, Lisa Knobloch, Christine Halket, and Annemarie Sommer as well Ms. Leslie Justice, CPNP; Ms. Christina Ferguson, MS, CCC-SLP; Nancy Neal, RN, BSN, CPN, and Ms. Katy Nash Krahn, MS, CGC for their cooperative management of the patients illustrated in this chapter.
References
Abyholm, FE, Bergland, O, Semb, G (1981). Secondary bone grafting of alveolar clefts. Scand J Plast Reconstr Surg 15: 127–140.
American Cleft Palate-Craniofacial Association (1993). Parameters for the evaluation and treatment of patients with cleft lip/palate or other craniofacial anomalies. Cleft Palate Craniofac J 30 (Suppl 1): 4.
Bergland, O, Semb, G, Abyholm, FE (1986). Elimination of the residual alveolar cleft by secondary bone grafting and subsequent orthodontic treatment. Cleft Palate J 23: 175–205.
Boyne, PJ (1974). Use of marrow-cancellous bone grafts in maxillary alveolar and palatal clefts. J Dent Res 53: 821.
Boyne, PJ, Sands, NR (1976). Combined orthodontic-surgical management of residual palato-alveolar cleft defect. Am J Orthod 70: 20.
Burston, WR (1958). The early treatment of cleft palate conditions. Dent Pract 9: 41–52.
Cohen, SR, Burstein, FD, Stewart, MB, Rathburn, MA (1997). Maxillary-midface distraction in children with cleft lip and palate: a preliminary report. Plast Reconstr Surg 9: 1421–1428.
Dalston, RM, Marsh, JL, Vig, KWL, et al. (1988). Minimal standards for reporting the results of surgery on patients with cleft lip, palate or both. A proposal. Cleft Palate J 25: 3–7.
Grayson, BH, Santiago, PE, Brecht, LE, Cutting, CB (1999). Presurgical nasoalveolar molding in infants with cleft lip and palate. Cleft Palate Craniofac J 36: 486–98.
Hotz, MM, Gnoinski, WM, Nussbaumer, H, Kistler, E (1978). Early maxillary orthopedics in cleft lip and palate cases: guidelines for surgery. Cleft Palate J 15: 405–411.
Ishikawa, H, Kitazawa, S, Iwasaki, Nakamura, S (2000). Effects of maxillary protraction combined with chin-cap therapy in unilateral cleft lip and palate patients. Cleft Palate Craniofac J 37: 92–97.
Jolleys, A, Robertson, NRE (1972). A study of the effects of early bone grafting in complete clefts of the lip and palate—five year study. Br J Plast Surg 25: 229–237.
Kuijpers-Jagtman, AM, Long, RE, Jr (2000). The influence of surgery and orthopedic treatment on maxillofacial growth and maxillary arch development in patients treated for orofacial clefts. Cleft Palate Craniofac J 37: 527.
Long, RE, Jr, Semb, G, Shaw, WC (2000). Orthodontic treatment of the patient with complete clefts of lip, alveolus, and palate: lessons of the last 60 years. Cleft Palate Craniofac J 37: 533.
McNeil, CK (1964). Orthopedic principles in the treatment of lip and palate clefts. In: International Symposium on Early Treatment of Cleft Lip and Palate, edited by RP Hotz. Berne: Hans Huber.
Millard, DR, Latham, R, Huifen, X, et al. (1999). Cleft lip and palate treated by presurgical orthopedics, gingivoperiosteoplasty, and lip adhesion (POPLA) compared with previous lip adhesion method: a preliminary study of serial dental casts. Plast Reconstr Surg 103: 1630–1644.
Moisted, K, Dahl, E, Skovgaard, LT, et al. (1993). A multicentre comparison of treatment regimens for unilateral cleft lip and palate using a multiple regression model. Scand J Plast Reconstr Surg Hand Surg 27: 277–284.
Polley, JW, Figueroa, AA (1998). Rigid external distraction: its application in cleft maxillary deformities. Plast Reconstr Surg 102: 1360–1372.
Pruzansky, S (1964). Pre-surgical orthopedics and bone grafting for infants with cleft lip and palate: a dissent. Cleft Palate J 1: 164–182.
Rosenstein, SW, Monroe, CW, Kernahan, DA, et al. (1982). The case for early bone grafting in cleft lip and cleft palate. J Oral Surg 70: 297–309.
Ross, RB, MacNamera, MC (1994). Effect of presurgical infant orthopedics on facial esthetics in complete bilateral cleft lip and palate. Palate Craniofac J 31: 68–73.
Rygh, P, Tindlund, RS (1995). Early considerations in the orthodontic management of skeletodental discrepancies. In: Facial Clefts and Craniosynostosis. Principles and Management, edited by TA Turvey, KWL Vig, and RJ Fonseca. Philadelphia: WB Saunders, pp. 234–319.
Santiago, PE, Grayson, BH, Cutting, CB, et al. (1998). Reduced need for alveolar bone grafting by presurgical orthopedics and primary gingivoperiosteoplasty. Cleft Palate Craniofac J 35: 77–80.
Semb, G (1988). Effect of alveolar bone grafting on maxillary growth in unilateral cleft lip and palate patients. Cleft Palate J 25: 288–295.
Semb, G (1991). Analysis of the Oslo Cleft Lip and Palate Archive. Long Term Dentofacial Development. Oslo: Univ. of Oslo. Dissertation.
Severens, JL, Prahl, C, Kuijpers-Jagtman, AM, Prahl-Andersen, B (1998). Short-term cost-effectiveness analysis of presurgical orthpedic treatment in children with complete unilateral cleft lip and palate. Cleft Palate Craniofac J 35: 222–226.
Shaw, WC, Roberts, CT, Semb, G (1995). Evaluating treatment alternatives: measurement and design. In: Facial Clefts and Craniosynostosis. Principles and Management, edited by TA Turvey, KWL Vig, and RJ Fonseca. Philadelphia: WB Saunders. pp. 756–766.
Shprintzen, RJ, Siegel-Sadewitz, VL, Amatp, A, Goldberg, RB (1985). Anomalies associated with cleft lip, cleft palate or both. Am J Med Genet 20: 585–595.
Surgeon General's Report (1987). Children with Special Health Care Needs. Washington, DC; Government Printing Office.
Tindlund, RS (1989). Orthopaedic protraction of the midface in the deciduous dentition. Results covering 3 years out of treatment. J Craniomaxillofac Surg 17 (Suppl 1): 17–19.
Tindlund, RS (1994). Skeletal response to maxillary protraction in patients with cleft lip and palate before age 10 years. Cleft Palate Craniofac J 31: 295–308.
Troxell, J, Fonseca, R, Osbon, D (1982). A retrospective study of alveolar cleft grafting. J Oral Maxillofac Surg 40: 721–725.
Turvey, T, Vig, K, Moriarty, J, Hoke, J (1984). Delayed bone grafting in the cleft maxilla and palate: a retrospective multidisciplinary analysis. Am J Orthod 86: 244–256.
Turvey, TA, Vig, KWL, Fonseca, R (1995). Facial Clefts and Craniosynostosis. Philadelphia: WB Saunders.
Vig, KWL (1990). Orthodontic considerations applied to craniofacial dysmorphology. Cleft Palate J 27: 141–145.
Vig, KWL (1992). Timing of alveolar bone grafting: an orthodontist's viewpoint. In: Problems in Plastic and Reconstructive Surgery, edited by JA Lehman and D Serafin. Philadelphia: JB Lippincott, pp. 58–72.
Vig, KWL (1999). Alveolar bone grafts: the surgical/orthdontic management of the cleft maxilla. Ann Acad Med Singapore 28: 721–727.
Vig, KWL, Turvey, TA (1985). Orthodontic, surgical interaction in the management of cleft lip and palate. Clin Plast Surg 12: 735–748.
Vig, KWL, Turvey, TA, Fonseca, RJ (1995). Orthodontic and surgical considerations in bone grafting the cleft maxilla and palate. In: Facial Clefts and Craniosynostosis. Principles and Management, edited by TA Turvey, KWL Vig, and RJ Fonseca. Philadelphia: WB Saunders.
Washington State Department of Health (1997). Cleft Lip and Palate: Critical Elements of Care. Seattle: Division of Family and Community Services, Office for Children with Special Health Care Needs.
Will, LA (2000). Growth and development in patients with untreated clefts. Cleft Palate Craniofac J 37: 523–526.
Winters, JC, Hurwitz, DJ (1995). Presurgical orthopedics in the surgical management of unilateral cleft lip and palate. Plast Reconstr Surg 95: 755–764.
Zins, JE, Whittaker, LA (1979). Membranous vs. endochondral bone autografts: implications for craniofacial reconstruction. Surg Forum 30: 521.