Maria Suurna
Allen M. Seiden
Otologic Infections
Otitis Externa
Acute otitis externa (AOE) is defined as a diffuse inflammation of the external ear canal, which may also involve the pinna or tympanic membrane (1). This condition is also known as “swimmer's ear” or “tropical ear” due to a higher prevalence in individuals with prolonged water exposure during swimming or who live in warm and humid climates (2). The annual incidence of AOE is about 1:100 to 1:250 within the general population (3).
The external ear comprises the auricle and external ear canal. The medial 60% of the external auditory canal is osseous and contains thin skin densely adherent to the underlying periosteum (Fig. 109.1). The lateral 40% of the external auditory canal is cartilaginous and contains a thin layer of subcutaneous tissue between the skin and cartilage. This subcutaneous layer contains hair follicles and sebaceous and apocrine glands. The skin of the auditory canal has a property of migrating from the tympanic membrane outward, resulting in self-cleansing. Cerumen is formed by glandular secretions and sloughed epithelium and provides both a chemical and mechanical protective barrier to infection. Cerumen is slightly acidic, maintaining a canal pH of 5 to 6.5, which helps inhibit bacterial and fungal growth. The lipid content of cerumen prevents maceration and breakdown of the epithelium. It is the breakdown in this natural defense mechanism that allows for opportunistic infections, giving rise to otitis externa (4).
The risk factors for acute otitis externa are prolonged exposure to water from swimming; dermatologic conditions such as seborrhea, psoriasis, eczema; trauma from ear cleaning, and foreign objects; use of assistive devices such as earplugs or hearing aids; anatomic abnormalities such as exostoses and narrow ear canals; immunocompromising systemic conditions such as diabetes, HIV; concomitant ear diseases such as cholesteatoma, suppurative otitis media; and a history of cancer radiotherapy (1,5).
Symptoms and signs of ear canal inflammation usually have rapid onset. Some of the presenting symptoms may be otalgia, itching, aural fullness, decreased hearing, and pain with chewing. Patients with AOE will often have disproportionately severe pain and will have significant tenderness when pushed on the tragus, or with manipulation of the pinna. Otoscopic exam usually reveals ear canal cellulitis and edema. Depending on the severity of the ear canal swelling, the tympanic membrane may or may not be visualized. The ear canal is often filled with purulent discharge and debris. Inflammation may spread to involve the entire auricle and adjacent skin. Regional lymphadenopathy may be present on the exam (1).
Most cases of AOE are bacterial. Pseudomonas aeruginosa and Staphylococcus species have been found to be the most common pathogens (6). Fungal involvement is uncommon in primary AOE. It is more often seen in chronic otitis externa or as secondary overgrowth following the treatment of bacterial infection.
Initial treatment of otitis externa involves removal of debris from the external ear canal, pain control, use of topical medications, acidification of the ear canal, and control of predisposing factors. Debridement of the external ear canal removes infectious material and allows for better penetration of topical medications. Topical medications can usually be administered directly into the ear canal. However, in many cases marked edema of the ear canal will prevent proper penetration of the medicated drop down into the canal. In this situation, placement of a cotton wick directly into the ear canal for several days will facilitate delivery of the medication (1).
Currently recommended topical preparations consist of antibiotics and steroid combinations. Quinolone antibiotic preparations may have broader microbial coverage and a low risk of contact dermatitis. Caution should be used when treating with neomycin-containing topical preparations due to a potential for neomycin to cause contact sensitivity and in turn lead to worsening of symptoms. Neomycin-containing preparations also have a low risk of causing permanent sensorineural hearing loss and should be used with caution in patients with perforated tympanic membranes. Acetic acid, boric acid, aluminum acetate, and silver nitrate have also been found to be effective. When treating immunocompromised patients, or if otitis externa infection has spread beyond the ear canal, consideration should be given to the use of systemic antibiotics as well. The choice of antibiotics should be based on their antipseudomonal and antistaphylococcal properties (1).
Chronic Otitis Externa
Chronic otitis externa (COE) is a persistent inflammatory disorder of the ear canal usually caused by repeated mechanical debridement or water exposure. Other potential causes are allergic, contact dermatitis, or dermatologic disorders. Chronic inflammation may lead to development of granulation. The treatment of COE involves debridement, avoidance of ear canal manipulation, elimination of the offending agent, and topical corticosteroids. Regular flushing of the ear canal with a mild acidic solution, such as acetic acid or vinegar and distilled water, can help to eradicate infection and keep the canal free of debris (7,8).
|
|
|
Figure 109.1. Anatomic depiction of the external, middle, and inner ear. |
Otomycosis
Otomycosis is a fungal infection of the external ear canal. It constitutes roughly 10% of all cases of otitis externa and is more common in geographic locations with a warm and humid climate, in patients following long-term topical antibiotic therapy, and in patients with diabetes, HIV, or other immunocompromising condition (9). The ear canal will often have cellulitis and edema on otoscopic examination. The canal debris may have a cheeselike or grayish appearance with visualized fungal hyphae. Aspergillus species and Candida species are the most common pathogens (10). Treatment consists of debridement, acidification, and drying of the ear canal. For candidal infections, topical antifungal therapy may also be effective.
Necrotizing Otitis Externa
Malignant or necrotizing otitis externa (MOE) is an aggressive infection that begins as otitis externa but spreads through surrounding tissues toward the skull base. It is seen predominantly in the elderly, diabetic, or immunocompromised patient. Pseudomonas aeruginosa is the most common causative pathogen; however, staphylococcal species are also known to cause the infection (11,12). Fungal causes of MOE are less common, with Aspergillus species the predominating pathogen (13).
MOE initially presents with symptoms and signs of AOE. Subsequently it may progress to temporal bone osteomyelitis and affect adjacent cranial nerves (VII–XII), blood vessels, and soft tissue. If not treated aggressively, the infection can expand intracranially, leading to neurologic symptoms. On otoscopic exam, granulation tissue is classically seen at the bony-cartilaginous junction (11,12,13,14). A raised erythrocyte sedimentation rate and abnormal computed tomography (CT) or magnetic resonance imaging (MRI) scan help to confirm the clinical diagnosis. Other imaging techniques that assist in diagnosis include gallium scan, indium-labeled leukocyte scan, technetium bone scan, and single photon emission tomographs (12,15). Patients will require treatment with systemic antibiotics that cover pseudomonal and staphylococcal infection, including methicillin-resistant Staphylococcus aureus (11,12).
Furunculosis (Ear Canal Abscess)
Furunculosis is a localized infection of the ear canal that is usually caused by an infected hair follicle. It may present with otalgia, otorrhea, and localized tenderness. A tender, often fluctuant nodule within the lateral ear canal can be identified on the exam. The most common pathogen is S. aureus. The treatment includes application of heat, incision and drainage of the infected area, and systemic antibiotic treatment with staphylococcal coverage (16).
Acute Otitis Media
Acute otitis media is an inflammation of the middle ear that is generally characterized by the rapid onset of otalgia, aural fullness, and occasionally fever. In the pediatric patient, more common signs are irritability, sleeplessness, and pulling at the affected ear. On pneumatic otoscopy, the tympanic membrane will have a red, opaque, and bulging appearance with decreased mobility due to the accumulation of purulent fluid in the middle ear space. Erythema of the tympanic membrane may be noted, and if the tympanic membrane is ruptured, patients will present with otorrhea (17,18).
Predominant pathogens in AOM are Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis (19). Observation for 24 to 48 hours in the case of a nonsevere illness in an otherwise healthy individual older than 6 months of age is an initial option. If symptoms persist, antimicrobial therapy should be initiated. Amoxicillin is recommended for initial treatment of acute otitis media, at a recommended dose of 80 to 90 mg/kg per day. In the case of penicillin allergy, azithromycin, clarithromycin, erythromycin-sulfisoxazole or trimethoprim-sulfamethoxazole could be used. Due to the increased incidence of beta-lactamase–producing organisms, the bacterial coverage should be expanded if there is no improvement within 48 to 72 hours. In very rare cases, if pain or fever is excessive, immediate tympanocentesis or myringotomy may be required (18,19).
Otitis media with effusion is the presence of fluid in the middle ear without signs or symptoms of acute ear infection and should be distinguished from acute otitis media. Otitis media with effusion often occurs as a result of eustachian tube dysfunction, or middle ear inflammation following acute infection. It is most common in the pediatric population between the ages of 6 months and 4 years, although it may occur at any age. On pneumatic otoscopy, the tympanic membrane is usually retracted, will have decreased mobility, and an air–fluid level or bubbles are often visualized. Patients often report a decrease in hearing. Otitis media with effusion is often self-limited and is likely to resolve spontaneously within 3 months. If it persists, hearing testing is recommended, particularly in children with language delay, learning problems, or suspicion of significant hearing loss (17,20). In individuals with persistent middle ear effusion leading to hearing loss or structural damage, surgical intervention, such as myringotomy with tympanostomy tube insertion, should be considered. Medical treatment, such as decongestants, has not been shown to be effective in the treatment of middle ear effusion. In an adult presenting with a unilateral middle ear effusion, an examination of the nasopharynx should be performed to rule out the possibility of a nasopharyngeal mass causing obstruction of the eustachian tube.
Chronic Otitis Media
Chronic otitis media is diagnosed when infection persists for more than 1 to 3 months. It may present as chronic suppurative otitis media (CSOM), which is characterized by persistent bacterial infection and drainage from the ear, or as chronic otitis media with effusion (COME), which results from unresolving inflammation of the middle ear and persistent middle ear secretions with an intact tympanic membrane. Chronic otitis media may be associated with cholesteatoma, which is a keratin cyst that forms from an accumulation of squamous debris in the middle ear with potential for growth and erosion of surrounding structures (21).
Patients with CSOM will present with hearing loss, painless purulent otorrhea, and a chronic tympanic membrane perforation. Evaluation includes visual exam, bacterial culture, and radiographic imaging. Gram-negative and anaerobic organisms are usually seen on cultures with Pseudomonas aeruginosa being a predominant organism. Temporal bone CT scan allows evaluation of the extent of disease and reveals potential complications. Medical treatment of CSOM consists of topical debridement, along with topical and systemic antibiotics. Topical drops often consist of antibiotic and steroid combinations. Ciprofloxacin is recommended for systemic use; however, it cannot be given to children younger than 17 years of age. Surgical treatment is performed for eradication of the infection and reconstruction of the middle ear (21,22).
COME is characterized by persistent hearing loss and a middle ear space filled with thick mucus. Chronic inflammation of the middle ear often begins with obstruction of the eustachian tube. The resulting negative pressure in the middle ear leads to collection of transudate. Secondary to chronic inflammation, the middle ear lining becomes hyperplastic and produces further mucus. On exam the tympanic membrane is intact and has a thickened, opaque appearance. On pneumatic otoscopy, the tympanic membrane does not move. As the disease progresses, the tympanic membrane starts to retract and drape over the ossicles. Nasal obstruction and sinus disease may contribute to eustachian tube insufficiency and lead to middle ear fluid accumulation. Treatment of COME consists of fluid drainage, which is accomplished by myringotomy with ventilation tube insertion. Treating sinus disease and relieving nasal obstruction may improve eustachian tube function (21).
Acute or chronic forms of otitis media, if left untreated, may lead to extracranial or intracranial complications (Table 109.1). Hearing loss, tympanic membrane perforation, atelectasis of the middle ear, mastoiditis, apical petrositis, facial nerve paralysis, labyrinthitis, and ossicular discontinuity are some of the possible intratemporal sequelae of otitis media. Meningitis, extradural abscess, subdural empyema, encephalitis, brain abscess, sigmoid sinus thrombosis, and hydrocephalus are potential intracranial complications. Intracranial complications should be suspected in individuals presenting with changes in mental status (17,23,24,25).
|
Table 109.1 Complications of Otitis Media |
||
|
Labyrinthitis
Labyrinthitis is an inflammation or infection of the vestibular apparatus. Patients typically present with vertigo, nausea, vomiting, and malaise. The cause is most often viral or traumatic but can be bacterial. Bacterial labyrinthitis most often arises as a spread of infection from meningitis or otitis media. It can be serous or suppurative. Viral infections such as mumps, measles, Lassa fever, varicella-zoster, and herpes simplex have been associated with labyrinthitis. Labyrinthitis may or may not be associated with a sensorineural hearing loss, which can be temporary or permanent depending on the cause, patient's age, and severity of the loss (26).
Bell's Palsy
Bell's palsy is defined as an acute unilateral peripheral facial nerve weakness. Diagnosis is made when other causes of facial nerve paralysis such as systemic diseases, infection, trauma, central nervous system disorders, and neoplasm are ruled out. Patients will usually present with abrupt onset of unilateral facial weakness. Other symptoms may include numbness or pain around the ear, decreased taste, and increased sensitivity to sounds (27). Herpes simplex virus is thought to be an etiologic factor for this disease (28). Bell's palsy most commonly occurs in individuals between 10 to 40 years of age. Pregnant women and individuals with diabetes mellitus are at a higher risk of developing Bell's palsy. Most cases spontaneously improve within 6 months. Residual facial nerve weakness may persist in about 15% of affected individuals (27). Recommended treatment consists of the early administration of high-dose prednisone and acyclovir (29). Patients should be educated about using artificial tears and protecting the eye during sleep to prevent corneal abrasion and eye infection. Preferably, treatment should be initiated within 72 hours of the onset of symptoms (27).
Ramsay Hunt Syndrome
Ramsay Hunt syndrome is caused by reactivation of varicella-zoster virus (VZV) in the geniculate ganglion and is associated with eruption of an auricular or oropharyngeal vesicular rash, facial paralysis, and otalgia (30,31). In addition tinnitus, hearing loss, nausea, vomiting, vertigo, and nystagmus can be accompanying symptoms (32). Patients with Ramsay Hunt syndrome present more severe symptoms and have a worse prognosis for recovery of facial nerve function relative to patients with Bell's palsy. The timing between onset of facial paralysis and vesicular eruption may vary. Some patients present with facial paralysis, have a rise in VZV antibody, but never develop cutaneous manifestations. Such cases are termed Ramsay Hunt sine herpete and often are labeled as Bell's palsy (30). Initiation of early treatment with prednisone and acyclovir is currently recommended (33).
Chondritis/Perichondritis
Chondritis/perichondritis of the ear is an infection of auricular cartilage/perichondrium. It is often caused by penetrating injury to the ear, particularly piercing of the pinna. Blunt trauma with auricular hematoma can also lead to infection. Cartilage involvement can also be seen in spreading otitis externa. Due to its relative avascularity, cartilage is more susceptible to infection. Infections are more often reported during warm weather, after exposure to water in pools, lakes, or hot tubs. Patients present with a very tender, erythematous, and indurated auricle. It is generally doughy on palpation and is rarely fluctuant. Pseudomonas aeruginosa has been identified as the most likely cause of the infection (34,35). Treatment consists of removing any foreign body, and drainage of any abscess or hematoma. Patients should be treated aggressively with antibiotics that provide coverage for Pseudomonas. Cartilage necrosis or subperichondrial fibrosis leading to auricular deformity may be seen following the infectious process (34). Recurrent auricular chondritis should raise suspicion for the diagnosis of relapsing polychondritis (36).
Nasal Infections
Septal Abscess
Septal abscess is rare and is defined as a collection of pus between the cartilaginous or bony nasal septum and overlying mucoperichondrium or mucoperiosteum (37). The leading cause is trauma that leads to a septal hematoma. It has also been shown to occur in association with influenza, sinusitis, nasal furuncle, and dental infection. Immunocompromised patients are at a higher risk of dangerous complications. Patients complain of nasal congestion, nasal pain, fever, and headache. On exam there is evidence of an anterior intranasal mass, as the septum will appear swollen and fluctuant. Most common causative organisms are S. aureus and group A beta-hemolytic streptococcus; however, Staphylococcus epidermidis, S. pneumoniae, H. influenzae, and anaerobes are also possible pathogens. Treatment involves antibiotics and surgical drainage. Ischemic necrosis of the septal cartilage may lead to saddle nose deformity or septal perforation. Other complications may involve intracranial infections such as meningitis, brain abscess, and subarachnoid empyema (37,38).
Rhinoscleroma
Rhinoscleroma is a chronic infectious granulomatous disease that originates in the nose but can involve any part of the respiratory tract. It is more common in the Middle East, parts of Latin America, and Eastern Europe, and is often diagnosed in young adults. Three clinical stages are recognized: (i) the catarrhal-atrophic stage, which consists of mucosal congestion and suppurative discharge; (ii) the granulomatous stage, which may present with epistaxis and nasal deformity and is associated with granulomatous nodules and infiltration; and (iii) the sclerotic stage in which fibrosis and stenosis develop (39). Typically patients present with crusting and nodular thickening of the nasal mucosa. Biopsy and culture of the diseased area provides a diagnosis. The presence of Klebsiella rhinoscleromatis is diagnostic of rhinoscleroma. Diagnosis is usually made in the proliferation stage. Biopsy shows an abundance of Mikulicz cells (40). Surgical debridement and prolonged antibiotic therapy is effective against the disease. Streptomycin, tetracycline, rifampin, second- or third-generation cephalosporins, and fluoroquinolones have been found to be effective against Klebsiella rhinoscleromatis. Treatment requires months to years, and relapses are common. Patients require long-term follow-up with repeat cultures and biopsies (39).
Rhinosinusitis
Acute Bacterial Rhinosinusitis
Acute bacterial rhinosinusitis most often develops following a viral upper respiratory infection. Some of the presenting diagnostic symptoms include purulent nasal discharge; nasal congestion; maxillary, tooth, or facial pain; and worsening of symptoms following initial improvement. Other symptoms include general malaise and a more generalized headache, although fever is unusual. Predisposing physiologic factors include obstruction of sinus ostia, reduction in number or function of sinus cilia, and a change in the quality of secretions (41). The most common pathogens are S. pneumoniae, H. influenzae, Moraxella catarrhalis, and S. aureus. In immunocompromised patients, in patients with cystic fibrosis, and in patients with sinusitis of nosocomial origin (on mechanical ventilation, with nasal tubing), P. aeruginosa and other aerobic Gram-negative rods are common causative pathogens (42). Anaerobic bacteria are usually associated with sinusitis of dental origin (43). It is often difficult to distinguish between viral and bacterial sinusitis. The diagnosis is usually based on medical history and clinical findings. With bacterial sinusitis symptoms are usually present for >7 days. Sinus puncture with aspiration of sinus contents is the most accurate diagnostic technique; however, since it is invasive, it is not commonly used. Radiographic imaging may help confirm the presence of sinus disease. Plain films can be difficult to interpret and are rarely ordered. CT findings will include thickened mucosa, sinus opacification, or air–fluid levels, and CT is the preferred exam although these findings are nonspecific (Fig. 109.2). A CT is rarely ordered to confirm acute infection unless there is concern about possible complications, such as in the case of frontal or sphenoid sinus infection. Nasal endoscopy will often demonstrate swelling within the middle meatus or sphenoethmoidal recess, with purulent discharge. Antimicrobial treatment of acute sinusitis includes amoxicillin, amoxicillin-clavulanic acid, cephalosporins, trimethoprim-sulfamethoxazole, macrolides, doxycycline, and quinolones. Treatment can be supplemented with nasal saline irrigation, antihistamines, decongestants, and intranasal steroids (41). If not treated, acute bacterial sinusitis may be complicated by development of several orbital and intracranial complications, particularly when the infection involves the ethmoid, frontal, or sphenoid sinuses (44,45) (Table 109.2).
|
|
|
Figure 109.2. A coronal computed tomography (CT) image depicting inflammatory sinus disease. A coronal CT without contrast is the preferred radiographic study to evaluate for the presence and extent of sinus infections. |
Chronic Bacterial Rhinosinusitis
Chronic bacterial rhinosinusitis is diagnosed when symptoms are present for at least 12 weeks. Symptoms are similar to an acute infection, with nasal congestion and purulent discharge predominating, sometimes associated with facial pressure, aural fullness, and anosmia. Nasal endoscopy may reveal nasal polyps, edema, or purulent discharge (46,47). CT findings may reveal mucosal thickening, sinus opacification, polyps, or air–fluid levels (47). Predisposing factors include smoking, inhalant allergies, obstruction of the ostiomeatal complex (Fig. 109.3), immune deficiency, and genetic factors (48). Pathogens are similar to those found in acute infections, with a greater predominance of staphylococcus, Pseudomonas, and possibly anaerobes. The most common anaerobic bacteria include Peptostreptococcus species, Fusobacterium species, Prevotella and Porphyromonas species. In cases of P. aeruginosa, aminoglycosides, fourth-generation cephalosporins, or fluoroquinolones are used (42). A more prolonged course of antibiotic therapy may be required, ranging from 3 to 6 weeks. Adjunctive therapy including decongestants, mucolytics, and steroids may be helpful. If patients do not respond to medical therapy, surgical drainage should be considered (47).
|
Table 109.2 Potential Complications of Sinusitis |
|
|
|
|
|
|
|
Figure 109.3. The ostiomeatal complex, referring to the anterior ethmoid sinus, and the ostia of the maxillary and frontal sinus as they drain into the middle meatus. Most sinus infections begin and persist because of obstruction in this area. The right side depicts these areas swollen; the left demonstrates the postsurgical appearance after the ostiomeatal complex has been opened. Eb, ethmoidal bulla; fr, frontal recess; i, infundibulum; mt, middle turbinate; up, uncinate process. |
Viral Rhinosinusitis
Viral rhinosinusitis is more common than bacterial. The most common pathogens are rhinovirus, influenza viruses, adenoviruses, parainfluenza viruses, and respiratory syncytial virus (RSV). Inflammatory symptoms of viral rhinosinusitis are thought to be due to the host response to the virus. Patients may present with symptoms of the common cold such as nasal congestion, nasal discharge, sneezing, cough, fever, malaise, and muscle ache. Viral rhinosinusitis is usually self-limited. Antiviral therapy may be used for specific viruses. Nasal saline irrigation and various anti-inflammatory medications may aid with symptomatic relief (49).
Fungal Rhinosinusitis
Acute Necrotizing Fungal Rhinosinusitis
Acute necrotizing fungal rhinosinusitis is a fulminant invasive fungal infection that is often life threatening. It usually affects immunocompromised patients, such as diabetics, patients with immunodeficiency disorders, patients undergoing chemotherapy, or patients requiring prolonged stays in the intensive care unit. Patients often present with acute onset of fever, headache, cough, mucosal ulcerations, and epistaxis. On exam, nasal eschar spreading through mucosa, soft tissue, and bone is seen. Histopathologic evaluation of involved tissue reveals necrosis and inflammatory infiltrate with giant cells, lymphocytes, and neutrophils. Gomori methenamine silver or periodic acid-Schiff histologic fungal stains demonstrate tissue and vascular invasion by fungal hyphae. Most common pathogens are Aspergillus, Rhizopus, and Mucor species. Treatment involves emergent surgical debridement, intravenous antifungal drugs such as amphotericin B, and treatment of the underlying immunocompromising disorder. If the disease is not treated, it may lead to rapid dissemination and death (50,51).
|
|
|
Figure 109.4. Magnetic resonance imaging (MRI) of a mycetoma or fungal ball within the sphenoid sinus, demonstrating isodense opacification on T1 images (A), with a ring of enhancement and central attenuation on T2 (B). |
Chronic Invasive Fungal Rhinosinusitis
Chronic invasive fungal rhinosinusitis is a chronic, more indolent, and slowly invasive fungal infection. It too usually affects immunocompromised patients, particularly diabetics and patients requiring prolonged corticosteroid treatment, but has also been reported in otherwise healthy individuals. Patients may present with orbital apex syndrome due to the extension of the infection into the orbit. This will result in decreased vision, ocular immobility, and proptosis. Erosion may also occur into the infratemporal fossa, the anterior cranial fossa, or the premaxillary region. Histopathology reveals a dense accumulation of hyphae, with a chronic inflammatory infiltrate of lymphocytes, giant cells, and necrotizing granulomas. If left untreated, the disease may invade cerebral blood vessels leading to ischemic injury or directly invade the brain. Treatment involves repeated surgical debridement and antifungal drugs (50).
Mycetoma
Mycetoma, also described as a fungal ball, is an accumulation of degenerating fungal hyphae within a sinus cavity. It usually involves one sinus, most often the maxillary sinus. Patients are generally immunocompetent and will present with symptoms of nasal obstruction, postnasal drainage, and localized facial pain. Risk factors include previous sinus surgery, oral-sinus fistula, and chemotherapy treatment. The presence of chronic mucosal inflammation may be noted on nasal endoscopy, along with green-black concretions within the middle meatus. A CT study will reveal sinus opacification, often with areas of calcification. Magnetic resonance imaging (MRI) may be definitive, demonstrating isodense opacification on T1 images, with a ring of enhancement and central attenuation on T2 (Fig. 109.4). This result is from ferromagnetic deposits related to the fungal infection. Aspergillus is the most common organism, although fungal cultures are often found to be negative. Treatment involves surgical removal of the fungal ball with adequate drainage of the affected sinus (51,52).
Allergic Fungal Sinusitis
Allergic fungal sinusitis (AFS) is a form of chronic hypertrophic sinus disease and not really a true infection. The cause of AFS is thought to be in part an allergic response to the presence of noninvasive fungi in the sinus cavity and has been likened to allergic bronchopulmonary aspergillosis (51). Patients will commonly present with hypertrophic sinus disease and nasal polyps. Symptoms of headache, paranasal fullness, and nasal discharge are often reported. Sinus CT often reveals the presence of chronic sinusitis with hyperattenuation present in the opacified sinus, creating an inhomogeneous appearance often with areas of calcification (Fig. 109.5). Serum IgE levels are often elevated. Histologic evaluation reveals the presence of allergic mucin, containing fungal hyphae and elevated eosinophils. There is no evidence of mucosal invasion. Intraorbital and intracranial expansion may occur secondary to pressure resorption of surrounding bone. The most common causative agents are Bipolaris spicifera and Curvularia lunata. Other causative agents are Exserohilum rostratum, Alternaria species, and Aspergillus species. Treatment consists of sinus surgery to remove the diseased mucosa and allergic mucin, although recurrence is common. Once AFS is diagnosed, if there are no contraindications, treatment with corticosteroids should be initiated (52,53).
|
|
|
Figure 109.5. Computed tomography (CT) of the sinuses in a patient with allergic fungal sinusitis, demonstrating an inhomogeneous appearance with areas of calcification. |
Oral Cavity
Gingivitis
Gingivitis affects 50% to 90% of the adult population. It has an infectious etiology caused by oral microflora in the accumulating dental plaque and usually contains both aerobic and anaerobic bacteria. Gingivitis is a reversible disease. Chronic gingivitis often leads to bleeding of the gums during tooth brushing (54). Gingivitis may progress to periodontitis, which involves inflammation of deeper tissues leading to the loss of supporting connective tissue and alveolar bone. This disease is nonreversible and may lead to loss of involved teeth (55,56). Treatment involves primarily good oral hygiene along with the mechanical removal of plaque and calculus (55).
Acute Necrotizing Ulcerative Gingivitis (Trench Mouth)
Acute necrotizing ulcerative gingivitis (trench mouth, Vincent stomatitis) is a rare periodontal disease characterized by gingival necrosis, ulceration, pain, and bleeding (57). Disease is most commonly seen in young adults. Patients will often present with sudden onset of gingival inflammation. Gingival lacerations covered with gray membranes and gingival bleeding are noted on the exam. The causative organisms are fusospirochetal bacteria, which become pathogenic during periods of compromised immune system function. Bacteroides and Selenomonas species have also been implicated in the disease (57). Diagnosis is based on clinical findings. Risk factors include dental crowding, physical fatigue, increased stress, low socioeconomic status, immunosuppression, smoking, and poor oral hygiene (58). Treatment includes eliminating precipitating factors, treatment of underlying immunosuppression, oral hygiene, mechanical debridement of affected areas, and antibiotics. Penicillin or metronidazole is recommended for antibiotic treatment (57).
Herpetic Gingival Stomatitis
Herpetic gingivostomatitis is an infection due to herpes simplex virus. Primary infection most commonly manifests in children between the ages of 2 and 5 years. Patients may present with fever and irritability. Oropharyngeal pain, mucosal edema and erythema are often present. Vesicular lesions appear on mobile or nonkeratinized mucosal surfaces (buccal, labial) and attached or keratinized surfaces (gingiva, hard palate). These usually rupture within 24 hours, leaving small ulcers with an elevated margin. Diagnosis is confirmed by viral studies and biopsy. Treatment is usually supportive, although acyclovir may help to shorten the severity and duration of the infection. Once the primary infection resolves, infection remains dormant, the reservoir usually being the trigeminal ganglion. Periodic reactivation of infection may occur. In most cases, individuals must have an active lesion to be able to transmit the virus (59,60).
Herpangina
Herpangina is a disease that commonly occurs in children (61). Coxsackie A virus is the most common causative organism (62). Patients will present with fever, malaise, and sore throat. On exam patients are noted to have oropharyngeal erythema. Vesicles and small ulcers are present on the posterior pharynx, often on the uvula and soft palate. The course is usually self-limiting (61).
Candidiasis
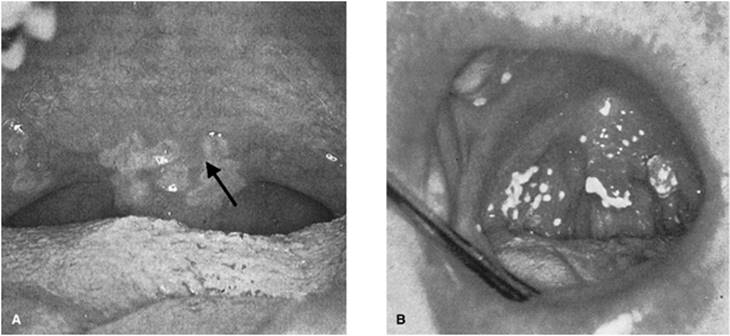
Candidiasis is caused by overgrowth of Candida albicans. Often the patient is predisposed, with a history of immunosuppression, radiation, or altered microflora following long-term broad-spectrum antibiotic use. In the pseudomembranous form, yellow-white plaques are present that have been likened to milk curds (Fig. 109.6A), whereas in the erythematous form, these plaques have disappeared (Fig. 109.6B). Clinical diagnosis may be confirmed with potassium hydroxide staining revealing fungal hyphae. Initial therapy usually consists of oral hygiene and topical treatment. Some of the available agents include oral nystatin preparations, amphotericin lozenges, and clotrimazole troches. Ketoconazole, fluconazole, and itraconazole can be used for systemic treatment if indicated (63).
Odontogenic Infections
Odontogenic infections often originate from infected pulp and may spread to the fascial spaces of the head and neck where an abscess may form (Fig. 109.7). The potential spaces are found around the face—masticator, buccal, canine, and parotid; in the suprahyoid area—submandibular, sublingual, and parapharyngeal; and in the infrahyoid area—retropharyngeal and paratracheal. The most common causative organisms are S. aureus, group A streptococci, and anaerobic bacteria. Treatment with broad-spectrum antibiotics is recommended (64,65).
Ludwig's Angina
Ludwig's angina is an infection that involves the left and right sublingual and submandibular spaces, generally spreading rapidly through fascial planes. It occurs most often in adults with poor dentition, usually from an infection involving the second or third molar. Other sources may include inflammation of the tongue or floor of mouth, and lingual tonsillitis (65,66).
Patients will often present with submandibular swelling but not fluctuance, and swelling of the floor of the mouth that pushes the tongue upward and backward toward the palate. In the case of advanced disease, patients may present in acute distress with fever, difficulty handling secretions, and dyspnea that favors a seated and head forward position. Infection can be rapidly progressive, leading to airway compromise. Anaerobic organisms and streptococci are the most common cause of Ludwig angina. Treatment requires close airway monitoring with prophylactic tracheotomy in most cases for airway protection, administration of antibiotics, and surgical drainage (66,67).
|
|
|
Figure 109.6. Oropharyngeal infection by Candida albicans (thrush). These photos demonstrate the pseudomembranous form (A) associated with yellow-white plaques, and the erythematous form (B). (From Walner DL, Shott SR. Infectious and inflammatory disorders. In: Seiden AM, Tami TA, Pensak ML, et al., eds. Otolaryngology: The Essentials. New York, NY: Thieme Medical Publishers; 2001:188, with permission.) |
Pharynx
Tonsillitis/Pharyngitis
Tonsillopharyngitis is a common disease characterized by infection of the nasopharynx and oropharynx and associated lymphoid tissue. Acute tonsillopharyngitis may be caused by viral or bacterial infection, a virus being most common. It is often difficult to distinguish between a bacterial and viral cause based on clinical exam. Patients present with fever, malaise, odynophagia, and lymphadenitis. On exam tonsillar enlargement, erythema, and exudate may be present. Upper respiratory viruses such as rhinovirus, coronavirus, and adenovirus are the most common causes of viral infection (68). The most common cause of bacterial tonsillopharyngitis is a group A beta-hemolytic streptococci (GABHS). It can be diagnosed by performing a group A Streptococcus test. Other pathogens have also been associated with the disease such as M. catarrhalis, H. influenzae, S. aureus, and S. pneumoniae (69). Diphtheria and gonococcal infections should also be considered. If GABHS infection is suspected, antibiotic treatment should be initiated. Penicillin, amoxicillin, erythromycin, and first-generation cephalosporins are recommended for treatment. It is recommended to perform a group A Streptococcus test prior to initiation of antibiotic treatment (68,70). If not treated, bacterial tonsillopharyngitis may lead to complications that can be suppurative and nonsuppurative. The nonsuppurative complications include scarlet fever, acute rheumatic fever, and poststreptococcal glomerulonephritis. Suppurative complications include peritonsillar, parapharyngeal, and retropharyngeal cellulites and/or abscess (71). In cases of recurrent streptococcal tonsillopharyngitis or infections unresponsive to antimicrobial therapy, tonsillectomy might be indicated (72).
Peritonsillar Abscess
Peritonsillar abscess is the most common deep infection of the head and neck. It usually occurs as a complication of bacterial tonsillitis or less frequently in cases of infectious mononucleosis. Infection may spread through the tonsillar capsule into the space between the tonsil and superior constrictor muscle and sequentially develop into an abscess. Peritonsillar abscess is most commonly diagnosed in adults or adolescents. Patients will present with increasing pharyngeal pain, dysphagia, trismus, dysarthria, drooling, and a muffled voice. The clinical exam reveals trismus, peritonsillar bulging that displaces the soft palate medially, and uvular deviation toward the opposite side. Patients will often have tonsillar exudates and tender cervical lymphadenopathy (65). A peritonsillar abscess is usually polymicrobial, with Group A streptococci and anaerobes the most common pathogens (73). The diagnosis is usually made on physical exam. A CT scan may help if the diagnosis is uncertain. Treatment involves aspiration or incision and drainage of the abscess along with antibiotic therapy (74). If the peritonsillar abscess becomes recurrent, a tonsillectomy would be indicated (75). A peritonsillar space infection has the potential for spreading to the parapharyngeal space, the manifestations of which may be delayed (65).
|
|
|
Figure 109.7. Schematic representation of the deep fascial spaces of the head and neck. (From Portugal LG, Padhya TA, Gluckman JL. Anatomy and Physiology. In: Seiden AM, Tami TA, Pensak ML, et al., eds. Otolaryngology: The Essentials. New York, NY: Thieme Medical Publishers; 2001:477, with permission.) |
Lemierre Syndrome
Lemierre syndrome is described as the presence of oropharyngeal infection, sepsis, internal jugular vein thrombosis, and septic emboli caused by Fusobacterium necrophorum (76). This is a Gram-negative anaerobic organism that can be part of the normal human oropharyngeal, gastrointestinal, or genitourinary flora. In the present time disease is rather uncommon due to the availability of antibiotics. Most often Lemierre syndrome affects young adults with a recent history of oropharyngeal, tonsillar, or peritonsillar infection. Patients will often present with tenderness and swelling of the lateral neck, secondary to thrombophlebitis of the internal jugular vein. Septic emboli may spread and affect other organs, especially the lungs. The disease requires immediate antibiotic treatment with agents such as clindamycin, metronidazole, ampicillin-sulbactam, or ticarcillin-clavulanate for a period of at least 6 weeks (76,77). In the case of abscess formation, surgical drainage might be required. In rare cases of refractory disease, ligation or excision of the jugular vein might be indicated (77,78).
Infectious Mononucleosis
Infectious mononucleosis is a systemic disease caused by Epstein-Barr virus (EBV). It most commonly occurs in teenagers and young adults. The virus is transmitted through saliva. Patients will present with fever, fatigue, malaise, sore throat, and generalized nontender lymphadenopathy. On exam patients will have inflamed tonsils with exudate. Hepatosplenomegaly may also be present. Diagnosis is confirmed by the presence of atypical lymphocytes on peripheral smear, a positive monospot test, and positive EBV titers. Treatment of mononucleosis is supportive (79,80). Corticosteroids are used to decrease inflammation, particularly in cases where airway obstruction is a concern due to marked tonsillar enlargement. In severe cases of airway obstruction, establishing a secure airway might be indicated. Patients will develop a rash if treated with amoxicillin for presumed bacterial tonsillitis; thus administration of amoxicillin should be avoided (79).
Larynx/Airway
Supraglottitis/Epiglottitis
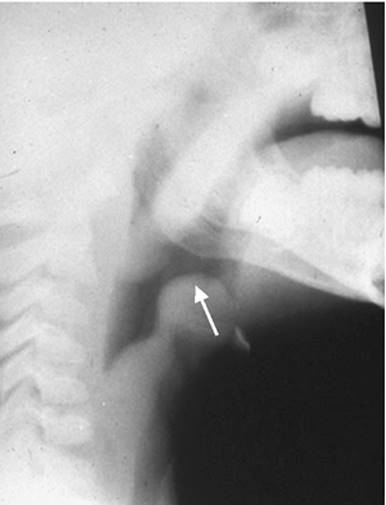
Epiglottitis is an infectious disease of the epiglottis and supraglottis, most commonly bacterial in origin. It usually has a sudden onset, with patients developing high fever, pain with swallowing, drooling due to difficulty handling secretions, and respiratory distress. On presentation the patient is often found sitting in a hunched-forward position with an extended neck and open mouth (sniffing position) (81). On a lateral neck film, edema of the epiglottis and a ballooning of the hypopharynx (thumb sign) will be noted (Fig. 109.8). On direct visualization the epiglottis will appear erythematous (cherry-red) and swollen. Care should be taken with airway manipulation as it may quickly precipitate complete airway obstruction. H. influenzae type b used to be the most common causative agent; however, with the introduction of the vaccine the incidence of H. influenzae–related epiglottitis has significantly decreased (82). Currently S. pneumoniae group A beta-hemolytic streptococci are the most common causative agents (82,83). Epiglottitis is considered an emergency as it has a potential for rapid complete airway obstruction, particularly in children. When epiglottitis is diagnosed, in most cases a secure airway should be established via endotracheal intubation or tracheostomy. The decision to extubate or decannulate is based on clinical improvement. Treatment with intravenous antibiotics (ceftriaxone or ampicillin/sulbactam) and steroids is initiated (81,82). Adults may sometimes present with supraglottitis where the epiglottitis is not involved. In these cases, the airway can often be managed more conservatively, although close in-hospital observation is required.
|
|
|
Figure 109.8. Lateral plain neck radiograph demonstrating edema of the epiglottis associated with epiglottitis. |
Laryngitis
Acute laryngitis most often occurs as part of an upper respiratory infection and therefore is usually caused by rhinovirus (84). Laryngoscopy reveals diffuse laryngeal erythema and edema, often producing a cough and hoarseness. The treatment is often supportive, including voice rest, humidification, and occasionally anti-inflammatory medications.
Croup
Croup is an inflammatory disease of the subglottic airway. Almost always it is associated with a viral infection, most commonly caused by parainfluenza and influenza viruses. It most commonly occurs in the pediatric population between the ages of 1 and 3 years. Patients usually present with fever, tachypnea, inspiratory stridor, hoarseness, and a barking cough. The history often includes a preceding upper respiratory infection. Radiographic studies reveal subglottic narrowing, the so-called steeple sign (Fig. 109.9). Depending on the severity of the symptoms, patients might require close observation and establishment of a secure airway. Administration of glucocorticoids is recommended to decrease airway inflammation, and racemic epinephrine treatments are often helpful. When croup is recurrent, an airway evaluation with laryngoscopy and bronchoscopy is recommended to assess for anatomic abnormalities (85).
|
|
|
Figure 109.9. Subglottic edema causing narrowing and the so-called steeple sign associated with croup. (From Stern Y, Myer CM. Infectious and inflammatory disorders. In: Seiden AM, Tami TA, Pensak ML, et al., eds. Otolaryngology: The Essentials. New York, NY: Thieme Medical Publisher; 2001:304, with permission.) |
Diphtheria
Diphtheria is an infectious disease of the upper airway. It is caused by Corynebacterium diphtheriae and is rather rare due to widespread immunization. Patients will present with fever and malaise. Bloody nasal discharge and pseudomembranes in the nose, oropharynx, and larynx may be noted on exam. The presence of membranes may lead to airway obstruction and respiratory failure. Exotoxins produced by the bacteria may affect the heart, liver, kidney, and brain. Clinical diagnosis is confirmed by bacterial smear and cultures on Löffler or tellurite media. The treatment consists of ensuring a secure airway, administration of antitoxin, and antibiotics. Penicillin or erythromycin is recommended for treatment (68,86).
Bacterial Tracheitis
Bacterial tracheitis is a rare, potentially life-threatening respiratory infection. It is characterized by the presence of thick membranous tracheal secretions that do not readily clear with coughing and may lead to occlusion of the airway. Patients will present with fever, cough, stridor, and generalized malaise. Patients do not respond to racemic epinephrine treatment. Radiographic findings often reveal irregular tracheal margins with a normal-appearing epiglottis. Diagnosis is made with direct visualization of thick membranous tracheal secretions or the presence of purulent tracheal secretions in the glottis and subglottis (87,88). The most commonly isolated pathogen is S. aureus. Other causative bacterial pathogens include H. influenzae, S. pneumoniae, Streptococcus pyogenes, M. catarrhalis, Klebsiella, and Pseudomonas species (87,88,89). If the diagnosis of bacterial tracheitis is made, treatment consists of securing the airway, endoscopically removing tracheal membranes, and administration of antibiotics (87).
Neck
Salivary Gland Infections
Viral Infections
Mumps
Mumps is a viral infection caused by paramyxovirus and is the most common viral infection that involves the salivary glands. Infected patients display signs of fever and malaise. Painful parotid swelling occurs within 24 hours and is often bilateral. Ten percent of patients have submandibular gland involvement. Patients may experience pain with salivation. Twenty-five percent of affected adolescent or adult males will develop orchitis, and 5% of females may present with oophoritis. Mastitis, pancreatitis, and central nervous system involvement may also occur in affected individuals. Mumps infection can also lead to sensorineural hearing loss. The treatment is usually supportive. In children the disease has a less severe course than in adults (90).
Other potential viruses that may infect the salivary glands include coxsackie A, echovirus, choriomeningitis, parainfluenza type 1 and 3, and cytomegalovirus (90,91).
Bacterial Infections
Bacterial infections of the salivary glands often develop following salivary stasis, secondary to ductal obstruction by a stone or mass, or a decrease of salivary flow secondary to dehydration. Any sort of intraoral trauma, such as extensive dental work, may also cause an inflammatory obstruction of the duct. The most common causative pathogens are S. aureus and Streptococcus viridans. The parotid gland is affected more often, likely due to lower bacteriostatic activity of saliva from this gland as compared to the submandibular or sublingual glands. Patients will present with pain, swelling, and erythema in the region of the salivary gland, exacerbated by eating. Patients may also have fever, malaise, and an elevated white count. Treatment involves hydration to increase salivary flow, massaging of the affected gland, sialogogues, and administration of antistaphylococcal antibiotics. In cases of chronic or recurrent sialadenitis, removal of the obstructing stone or excision of the gland might be recommended (91,92).
Lymphadenitis
Lymphadenitis is an inflammatory process involving lymph nodes. The pediatric group is more commonly affected. Upper respiratory viral infections are the most common cause of cervical lymphadenopathy. This condition is self-limited and usually does not require treatment. Bacterial lymphadenitis usually occurs as a complication of skin or respiratory infection. The most common causative organisms are S. aureus and group A streptococci. Patients may present with tender lymphadenopathy, which may progress to formation of an abscess. If bacterial lymphadenitis is suspected, treatment with beta-lactamase–resistant antibiotics is recommended. In case of progression to abscess formation, incision and drainage are indicated (93,94).
Catscratch Disease
This disease usually presents with subacute solitary or regional lymphadenopathy in patients with a previous contact with a kitten or cat. It is primarily caused by Bartonella henselae; however, cases of Bartonella clarridgeiae and Bartonella elizabethae have been reported. Lymphadenopathy occurs 1 to 3 weeks after a scratch, bite, or other contact with an infected kitten or cat. Small red-brown nontender papules may develop at the site of inoculation 3 to 30 days after contact. The lymph nodes draining the affected site gradually enlarge and are moderately tender, with the overlying skin appearing warm and erythematous. Up to 10% of lesions may require surgical drainage. Histologic examination reveals granulomas with multiple microabscesses. The indirect fluorescent antibody test and enzyme immunoassay are used for detection of specific serum antibody to B. henselae (95).
Mycobacterium
Nontuberculous mycobacterial infection is a rare cause of lymphadenitis. It presents as a slowly enlarging, nontender cervical mass. The infection can affect adults; however, it is most commonly found in children younger than 5 years of age. It is often diagnosed after failure to respond to treatment with antibiotics.
The most common causative pathogen is Mycobacterium avium-intracellulare. Other reported pathogens are M. scrofulaceum, M. kanasasaii, M. fortuitum, and M. malmoense (96). Nontuberculous mycobacteria are found ubiquitously in the environment—in soil, food, water, animals, and so on. It is usually acquired from the environment, and there is no evidence of person-to-person transmission. An intradermal PPD test (purified protein derivative of tuberculin) aids in the diagnosis of nontuberculous lymphadenitis. However, positive cultures will be more definitive (97). Complete surgical resection of infected tissues has been the gold standard for the treatment of nontuberculous mycobacterial infections. Treatment with antituberculous medications, such as macrolides (clarithromycin), has also been shown to be effective in some cases. Recent studies have suggested an antibiotic therapeutic trial prior to surgical excision or as an adjunct to surgical excision (98).
Actinomycosis
Actinomycosis is an infection caused by Actinomyces israelii, a Gram-positive anaerobic bacterium. The disease has multiple presentations and is often misdiagnosed. Most of these infections occur in the head and neck region (>50%), most often entering the tissue through an area of prior trauma. As the infection develops, patients will be noted to have a woody induration that eventually leads to central abscess formation. This abscess will generally track to a mucosal surface or externally to the skin, forming a sinus or fistulous tract. The suppurative drainage will contain so-called sulfur granules, yellow flecks containing the bacterial colonies. The diagnosis is best made by culture, but as anaerobic cultures can be unreliable, diagnosis may have to rely on the clinical picture and histology. The organisms stain best with Gram and Gomori methenamine silver stains. Treatment consists of drainage and debridement of the infected area with administration of penicillin (99).
Deep Neck Space Infections
Retropharyngeal Space Abscess
The retropharyngeal space is defined by the prevertebral fascia posteriorly, the posterior layer of the deep cervical fascia anteriorly, the skull base superiorly, and the posterior mediastinum inferiorly (Fig. 109.7). Infection usually develops from infected retropharyngeal lymph nodes, which receive lymphatic drainage from the paranasal sinuses, nasopharynx, and middle ear, and are more common in children. Trauma is another common cause. Patients commonly present with fever, pain with swallowing, decreased oral intake, drooling, malaise, and torticollis. Trismus and neck swelling are often present. The most common causative organisms are S. pyogenes and anaerobic bacteria (73). Lateral radiographic images of the neck in extension reveal thickened prevertebral soft tissue. Computed tomography aids in determining the presence of an abscess. Therapy involves the administration of intravenous antibiotics and drainage of the abscess. Transoral drainage is recommended unless there is extension lateral to the great vessels, i.e., the carotid artery (100). If left untreated, spontaneous rupture of the abscess may lead to aspiration of infectious material. Infection may spread to the parapharyngeal and prevertebral spaces, and lead to mediastinitis, or involve the great vessels (65).
Parapharyngeal Space Abscess
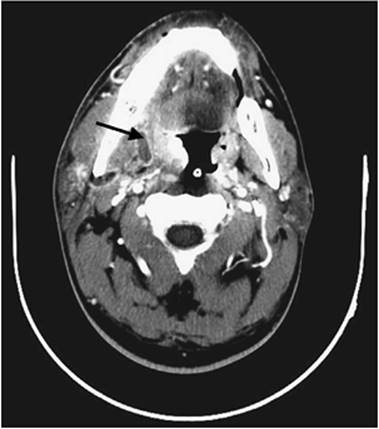
The parapharyngeal space is a potential space that extends from the skull base to the greater cornu of the hyoid bone (Fig. 109.7). The pharynx and superior constrictor muscle are the medial boundaries; the internal pterygoid muscle, parotid gland, and mandible are lateral structures; the prevertebral fascia lies posteriorly; and the pterygomandibular ligament is an anterior structure that surrounds the parapharyngeal space. The styloid process divides the space into an anterior and posterior division. Pharyngeal infections, molar tooth infections, gingivitis, and even mastoiditis may spread to the parapharyngeal space. If untreated, infection has the potential to spread to the retropharyngeal space, to the mediastinum, and to involve the great vessels causing internal jugular thrombosis and erosion of the internal carotid artery. Airway compromise may occur. Patients typically present with a prior history of a sore throat or tooth infection. Initial symptoms are fever and pain with swallowing. Tender, erythematous swelling at the angle of the mandible and parotid is typically found on clinical exam, but it will not appear fluctuant even if an abscess is present. Examination of the pharyngeal will often reveal medial displacement of the ipsilateral tonsil. Trismus may develop secondary to inflammation of the medial pterygoid muscle. Torticollis toward the opposite side often results from inflammation of lymph nodes under the sternocleidomastoid muscle. Patients may also complain of otalgia (65,101,102). The most common causative pathogens are S. aureus, S. pyogenes, and anaerobic bacteria (73). Computed tomography aids in evaluation of the site and the extent of infection, distinguishing between cellulitis and abscess (Fig. 109.10). Parapharyngeal space infections require immediate treatment with intravenous antibiotics and surgical drainage if an abscess is present. This is usually done through an external approach. Transoral drainage is not recommended (65,102).
|
|
|
Figure 109.10. Computed tomography (CT) of the neck demonstrating a parapharyngeal space abscess. |
Tips and Pearls
Infections of the head and neck may be an occult source of sepsis in critically ill patients, especially since nasopharyngeal and oropharyngeal tubes may cause obstruction and mucosal breakdown.
· In a patient presenting with an ear infection, pushing on the tragus will elicit pain if it is an outer or external ear infection, but not if it is a middle ear infection.
· Oral antibiotics are rarely helpful in the treatment of external otitis, a condition that is more effectively treated with topical preparations.
· Otomycosis caused by aspergillus usually presents with grayish black or yellow dots (fungal conidiophores) surrounded by a cottonlike material (fungal hyphae) that is easily visible when examining the ear canal.
· Otitis externa with granulation tissue in a diabetic patient should be considered diagnostic of necrotizing otitis externa and treated aggressively.
· In an adult presenting with a unilateral middle ear effusion, it is essential to evaluate the nasopharynx to rule out the presence of a nasopharyngeal mass obstructing the eustachian tube.
· Auricular perichondritis should be treated early and aggressively to prevent the sequela of auricular deformity.
· The presence of a nasal septal hematoma or abscess requires immediate drainage to prevent secondary necrosis of the septal cartilage and the subsequent development of a saddle nose deformity.
· A bacterial rather than viral sinus infection should be suspected when symptoms have been present for >7 to 10 days or symptoms are worsening after 5 days.
· Primary herpes can be distinguished from aphthous ulceration by the fact that aphthous ulcers appear only on mobile or unattached mucosal surfaces, whereas herpetic lesions appear on both mobile and attached mucosa.
· Ludwig's angina can be rapidly progressive and should be considered an airway emergency, with a prophylactic tracheotomy recommended in most cases.
· Due to its potential for rapid airway compromise, epiglottitis should be considered an airway emergency.
· Due to its deep location, a parapharyngeal space abscess will cause tender induration of the upper neck, but not fluctuance.
References
1. Rosenfeld RM, Brown L, Cannon CR, et al. American Academy of Otolaryngology–Head and Neck Surgery Foundation. Clinical practice guideline: acute otitis externa. Otolaryngol Head Neck Surg. 2006;134(4 Suppl):S4–23.
2. Russell JD, Donnelly M, McShane DP, et al. What causes acute otitis externa? J Laryngol Otol. 1993;107:898–901.
3. Guthrie RM. Diagnosis and treatment of acute otitis externa: an interdisciplinary update. Ann Otol Rhinol Laryngol. 1999;17:2–23.
4. Kelly KE, Mohs DC. The external auditory canal. Anatomy and physiology. Otolaryngol Clin North Am. 1996;29:725–739.
5. Rutka J. Acute otitis externa: treatment perspectives. Ear Nose Throat J. 2004;83(9 Suppl 4):20–21.
6. Clark WB, Brook I, Bianki D, et al. Microbiology of otitis externa. Otolaryngol Head Neck Surg. 1997;116:23–25.
7. Osguthorpe JD, Nielsen DR. Otitis externa: review and clinical update. Am Fam Physician. 2006;74(9):1510–1516.
8. Schapowal A. Otitis externa: a clinical overview. Ear Nose Throat J. 2002;81(8 suppl 1):21–22.
9. Kaur R, Mittal N, Kakkar M, et al. Otomycosis: a clinicomycologic study. Ear Nose Throat J. 2000;79:606–609.
10. Lucente FE. Fungal infections of external ear. Otolaryngol Clin North Am. 1993;26:995–1006.
11. Amorosa L, Modugno GC, Pirodda A. Malignant external otitis: review and personal experience. Acta Otolaryngol Suppl. 1996;521:3–16.
12. Slattery WH, Brackmann DE. Skull base osteomyelitis: malignant external otitis. Otolaryngol Clin North Am. 1996;29:795–806.
13. Kountakis SE, Kemper JV, Chang CYJ, et al. Osteomyelitis of the base of the skull secondary to Aspergillus. Am J Otolaryngol. 1997;18:19–22.
14. Chandler JR. Malignant external otitis. Laryngoscope. 1968;78:1257–1294
15. Okpala NC, Siraj QH, Nilssen E, et al. Radiological and radionuclide investigation of malignant otitis externa. J Laryngol Otol. 2005;119(1):71–75.
16. Bojarb DI, Bruderly T, Abdulrazzak Y. Otitis externa. Otolaryngol Clin North Am. 1996;29:761–782.
17. Bluestone CD, Gates GA, Klein JO, et al. Definitions, terminology, and classification of otitis media. Ann Otol Rhinol Laryngol. 2002;111: 8–18.
18. Lieberthal AS, Ganiats TG, Cox EO, et al. American Academy of Pediatrics Subcommittee on Management of Acute Otitis Media. Diagnosis and management of acute otitis media. Pediatrics. 2004;113(5):1451–1465.
19. Hoberman A, Marchant CD, Kaplan SL, et al. Treatment of acute otitis media consensus recommendations. Clin Pediatr. 2002;41:373–390.
20. Rosenfeld RM, Culpepper L, Doyle KJ, et al. American Academy of Pediatrics Subcommittee on Otitis Media with Effusion; American Academy of Family Physicians; American Academy of Otolaryngology—Head and Neck Surgery. Clinical practice guideline: Otitis media with effusion. Otolaryngol Head Neck Surg. 2004;130(5 Suppl):S95–118.
21. Jahn AF. Chronic otitis media: diagnosis and treatment. Med Clin North Am. 1991;75(6):1277–1291
22. Kenna MA. Treatment of chronic suppurative otitis media. Otolaryngol Clin North Am. 1994;27(3):457–472.
23. Leskinen K, Jero J. Acute complications of otitis media in adults. Clin Otolaryngol. 2005;30:511–516.
24. Penido NO, Borin A, Iha L, et al. Intracranial complications of otitis media: 15 years of experience in 33 patients. Otolaryngol Head Neck Surg. 2005;132:37–42.
25. Osma U, Cureoglu S, Hosoglu S. The complications of chronic otitis media: report of 93 cases. J Laryngol Otol. 2000;114:97–100.
26. Hyden D, Akerlind B, Peebo M. Inner ear and facial nerve complications of acute otitis media with focus on bacteriology and virology. Acta Otolaryngol. 2006;126(5):460–466.
27. Ahmed A. When is facial paralysis Bell palsy? Current diagnosis and treatment. Cleve Clin J Med. 2005;72(5):398–401, 405.
28. Jackler RK, Furuta Y. Reactivation of herpes simplex virus type 1 in patients with Bell's palsy. Am J Otol. 1998;19:236–245.
29. Abour KK, Ruboylanes JM, Von Doersten PG, et al. Bell's palsy treatment with acyclovir and prednisone compared with prednisone alone: a double blind, randomized, controlled trial. Ann Otol Rhinol Laryngol. 1996;105:307–378.
30. Sweeney CJ, Cilden DH. Ramsay Hunt syndrome. J Neurol Neurosurg Psychiatry. 2001;71:149–154.
31. Murakami S, Nakashiro Y, Mizobuchi M, et al. Varicella-zoster virus distribution in Ramsay Hunt syndrome revealed by polymerase chain reaction. Acta Otolaryngol. 1998;118:145–149.
32. Kuhweide R, Van de Steene V, Vlaminck S, et al. Ramsay Hunt syndrome: pathophysiology of cochleovestibular symptoms. J Laryngol Otol. 2002;116(10):844–848
33. Murakami S, Hato N, Horiuch J, et al. Treatment of Ramsay Hunt syndrome with acyclovir-prednisone: significance of early diagnosis and treatment. Ann Neurol. 1997;41:353–357.
34. More DR, Seidel JS, Beyan PA. Ear-piercing techniques as a cause of auricular chondritis. Pediatr Emerg Care. 1999;15:189–192
35. Keene WE, Markum AC, Samadpour M. Outbreak of Pseudomonas aeruginosa infections caused by commercial piercing of upper ear cartilage. JAMA. 2004;291(8):981–985.
36. Bachor E, Blevins NH, Karmody C, et al. Otologic manifestations of relapsing polychondritis. Review of literature and report of nine cases. Auris Nasus Larynx. 2006;33(2):135–141.
37. Ambrus PS, Eavey RD, Baker AS, et al. Management of nasal septal abscess. Laryngoscope. 1981;91:575–582.
38. Canty PA, Berkowitz RG. Hematoma and abscess of the nasal septum in children. Arch Otolaryngol Head Neck Surg. 1996;122:1373–1376.
39. Andraca R, Edson RS, Kern EB. Rhinoscleroma: a growing concern in the United States? Mayo Clinic experience. Mayo Clin Proc. 1993;68(12):1151–1157.
40. Stiernberg CM, Clark WD. Rhinoscleroma—a diagnostic challenge. Laryngoscope. 1983;93(7):866–870.
41. Marple BF, Brunton S, Ferguson BJ. Acute bacterial rhinosinusitis: a review of U.S. treatment guidelines. Otolaryngol Head Neck Surg. 2006;135(3):341–348.
42. Brook I. Microbiology and antimicrobial management of sinusitis. Otolaryngol Clin North Am. 2004;37(2):253–266.
43. Brook I. Sinusitis of odontogenic origin. Otolaryngol Head Neck Surg. 2006;135(3):349–355.
44. Younis RT, Lazar RH, Anand VK. Intracranial complications of sinusitis: a 15-year review of 39 cases. Ear Nose Throat J. 2002;81(9):636-8, 640-2, 644.
45. Jackson LL, Kountakis SE. Classification and management of rhinosinusitis and its complications. Otolaryngol Clin North Am. 2005;38(6):1143–1153.
46. Benninger MS, Ferguson BJ, Hadley JA, et al. Adult chronic rhinosinusitis: definitions, diagnosis, epidemiology, and pathophysiology. Otolaryngol Head Neck Surg. 2003;129(3 Suppl):S1–32.
47. Devaiah AK. Adult chronic rhinosinusitis: diagnosis and dilemmas. Otolaryngol Clin North Am. 2004;37(2):243–252.
48. Kennedy DW. Pathogenesis of chronic rhinosinusitis. Ann Otol Rhinol Laryngol Suppl. 2004;193:6–9.
49. Winther B, Gwaltney JM Jr, Mygind N, et al. Viral-induced rhinitis. Am J Rhinol. 1998;12(1):17–20.
50. DeShazo RD, Chapin K, Swain RE. Fungal sinusitis. N Engl J Med. 1997;337:254–259.
51. DeShazo RD, Swain RE. Diagnostic criteria for allergic fungal sinusitis. J Allergy Clin Immunol. 1995;96:24–35.
52. Schubert MS. Allergic fungal sinusitis. Otolaryngol Clin North Am. 2004;37(2):301–326.
53. DeShazo RD, O'Brien M, Chapin K, et al. Criteria for the diagnosis of sinus mycetoma. J Allergy Clin Immunol. 1997;99475–99485.
54. Pihlstrom BL, Michalowicz BS, Johnson NW. Periodontal diseases. Lancet. 2005;306:1809–1820.
55. Preshaw PM, Seymour RA, Heasman PA. Current concepts in periodontal pathogenesis. Dent Update. 2004;31:570–578.
56. Tatakis DN, Kumar PS. Etiology and pathogenesis of periodontal diseases. Dent Clin North Am. 2005;49:491–516.
57. Johnson BD, Engel D. Acute necrotizing ulcerative gingivitis. A review of diagnosis, etiology and treatment. J Periodontol. 1986;57(3):141–150.
58. Rowland RW. Necrotizing ulcerative gingivitis. Ann Periodontol. 1999;4:65–73.
59. Amir J. Clinical aspects and antiviral therapy in primary herpetic gingivostomatitis. Paediatr Drugs. 2001;3(8):593–597.
60. Ajar AH, Chauvin PJ. Acute herpetic gingivostomatitis in adults: a review of 13 cases, including diagnosis and management. J Can Dent Assoc. 2002;68(4):247–251.
61. Cherry JD, Jahn CL. Herpangina: the etiologic spectrum. Pediatrics. 1965;36(4):632–634.
62. Zavate O, Avram G, Pavlov E. Coxsackie A virus-associated herpetiform angina. Virologie. 1984;35(1):49–53.
63. Greenspan D, Greenspan JS. HIV-related oral disease. Lancet. 1996;348(9029):729–733.
64. Flynn TR. The swollen face. Severe odontogenic infections. Emerg Med Clin North Am. 2000;18(3):481–519.
65. Baker AS, Montgomery WW. Oropharyngeal space infections. Curr Clin Top Infect Dis. 1987;8:227–265.
66. Busch RF, Shah D. Ludwig's angina: improved treatment. Otolaryngol Head Neck Surg. 1997;117:5172–5175.
67. Baqain ZH, Newman L, Hyde N. How serious are oral infections? J Laryngol Otol. 2004;118:561–565.
68. Bisno AL. Acute pharyngitis. N Engl J Med. 2001;344(3):205–211.
69. Brook I, Gober AE. Increased recovery of Moraxella catarrhalis and Haemophilus influenzae in association with group A beta-haemolytic streptococci in healthy children and those with pharyngo-tonsillitis. J Med Microbiol. 2006;55(Pt 8):989–992.
70. Rufener JB, Yaremchuk KL, Payne SC. Evaluation of culture and antibiotic use in patients with pharyngitis. Laryngoscope. 2006;116:1727–1729.
71. Tewfik TL, Al Garni M. Tonsillopharyngitis: clinical highlights. J Otolaryngol. 2005;34(Suppl 1):S45–49.
72. Darrow DH, Siemens C. Indications for tonsillectomy and adenoidectomy. Laryngoscope. 2002;112:6–10.
73. Brook I. Microbiology and management of peritonsillar, retropharyngeal, and parapharyngeal abscess. J Oral Maxillofac Surg. 2004;62:1545–1550.
74. Herbild O, Bonding P. Peritonsillar abscess. Arch Otolaryngol. 1981;107(9):540–542.
75. Kronenberg J, Wolf M, Leventon G. Peritonsillar abscess: recurrence rate and the indication for tonsillectomy. Am J Otolaryngol. 1987 Mar–Apr;8(2):82–84.
76. Moreno S, Garcia Altozano J, Pinilla B, et al. Lemierre's disease: postanginal bacteremia and pulmonary involvement caused by Fusobacterium necrophorum. Rev Infect Dis. 1989;11:319–324.
77. Brook I. Microbiology and management of deep facial infections and Lemierre syndrome. ORL J Otorhinolaryngol Related Spec. 2003;65:117–120.
78. Nadkarni MD, Verchick J, O'Neill JC. Lemierre syndrome. J Emerg Med. 2005;28:297–299.
79. Ebell MH. Epstein-Barr virus infectious mononucleosis. Am Fam Physician. 2004;70(7):1279–1287.
80. Rea TD, Russo JE, Katon W, et al. Prospective study of the natural history of infectious mononucleosis caused by Epstein-Barr virus. J Am Board Fam Pract. 2001;14(4):234–242.
81. Carey MJ. Epiglottitis in adults. Am J Emerg Med. 1996;14(4):421–424.
82. Shah RK, Roberson DW, Jones DT. Epiglottitis in the Haemophilus influenzae type B vaccine era: changing trends. Laryngoscope. 2004;114:557–560.
83. Trollfors B, Nylen O, Carenfelt C, et al. Aetiology of acute epiglottitis in adults. Scand J Infect Dis. 1998;30(1):49–51.
84. Monto AS. Epidemiology of viral respiratory infections. Am J Med. 2002;112(Suppl 6A):4S–12S.
85. Stroud RH, Friedman NR. An update on inflammatory disorders of the pediatric airway: epiglottitis, croup, and tracheitis. Am J Otolaryngol. 2001;22(4):268–275.
86. Hadfield TL, McEvoy P, Polotsky Y, et al. The pathology of diphtheria. J Infect Dis. 2000;181(Suppl 1):S116–120.
87. Friedman EM, Jorgensen K, Healy GB, et al. Bacterial tracheitis–two-year experience. Laryngoscope. 1985;95(1):9–11.
88. Mahajan A, Alvear D, Chang C, et al. Bacterial tracheitis, diagnosis and treatment. Int J Pediatr Otorhinolaryngol. 1985;10(3):271–7.
89. Salamone FN, Bobbitt DB, Myer CM, et al. Bacterial tracheitis reexamined: is there a less severe manifestation? Otolaryngol Head Neck Surg. 2004;131(6):871–876.
90. Johnson A. Inflammatory conditions of the major salivary glands. Ear Nose Throat J. 1989;68(2):94–102.
91. Blitzer A. Inflammatory and obstructive disorders of salivary glands. J Dent Res. 1987;66:675–679.
92. Travis LW, Hecht DW. Acute and chronic inflammatory diseases of the salivary glands: diagnosis and management. Otolaryngol Clin North Am. 1977;10:329–38
93. Gosche JR, Vick L. Acute, subacute, and chronic cervical lymphadenitis in children. Semin Pediatr Surg. 2006;15(2):99–106.
94. Leung AK, Robson WL. Childhood cervical lymphadenopathy. J Pediatr Health Care. 2004;18:3–7.
95. Massei F, Gori L, Macchia P, et al. The expanded spectrum of bartonellosis in children. Infect Dis Clin North Am. 2005;19:691–711.
96. Flint D, Mahadevan M, Barber C, et al. Cervical lymphadenitis due to non-tuberculous mycobacteria: surgical treatment and review. Int J Pediatr Otorhinolaryngol. 2000;53(3):187–194.
97. Danielides V, Patrikakos G, Moerman M, et al. Diagnosis, management and surgical treatment of non-tuberculous mycobacterial head and neck infection in children. ORL J Otorhinolaryngol Related Spec. 2002;64:284–289.
98. Luong A, McClay JE, Jafri HS, et al. Antibiotic therapy for nontuberculous mycobacterial cervicofacial lymphadenitis. Laryngoscope. 2005;115:1746–1751.
99. Richtsmeier WJ, Johns ME. Actinomycosis of the head and neck. CRC Crit Rev Clin Lab Sci. 1979;11(2):175–202.
100. Kirse DJ, Roberson DW. Surgical management of retropharyngeal space infections in children. Laryngoscope. 2001;111:1413–1422.
101. Sethi DS, Stanley RE. Parapharyngeal abscesses. J Laryngol Otol. 1991;105(12):1025–1030.
102. Boscolo-Rizzo P, Marchiori C, Zanetti F, et al. Conservative management of deep neck abscesses in adults: the importance of CECT findings. Otolaryngol Head Neck Surg. 2006;135(6):894–899.