Antonelli Massimo
Conti Giorgio
Bello Giuseppe
Noninvasive ventilation (NIV) refers to the provision of ventilatory assistance using techniques that do not bypass the upper airway. The theoretical advantages of NIV include avoiding the complications associated with endotracheal intubation, improving patient comfort, and preserving airway defense mechanisms. NIV may be delivered through various devices including negative and positive pressure ventilators. During the first half of the 20th century, negative pressure ventilation was the main means of providing mechanical ventilatory assistance outside the anesthesia suite. Because of several disadvantages relative to negative pressure ventilation, including patient discomfort, restrictions on positioning, lack of airway protection, problems with correct fitting, time-consuming application, and lack of portability, negative pressure ventilators have seen diminishing use in favor of positive pressure assistance modes since the early 1960s. Therefore, only positive pressure support modes are discussed here.
The following sections deal with the history and epidemiology of NIV, as well as currently available equipment and techniques, practical applications, appropriate indications, and possible adverse effects. In this chapter, continuous positive airway pressure delivered noninvasively is referred to as CPAP, and NIV using intermittent positive pressure ventilation (IPPV) with or without positive end-expiratory pressure (PEEP) is referred to as NPPV (noninvasive positive-pressure ventilation). The term NIV is considered to include either CPAP or NPPV.
Background
The first noninvasive report of positive pressure dates back to 1912, when Bunnell (1) used a face mask to maintain lung expansion during thoracic surgery. In 1936, Poulton and Oxon (2) used a vacuum cleaner to generate gas flow and a spring-loaded valve to oppose expiration to treat a patient with cardiogenic pulmonary edema (CPE). A number of studies conducted by Barach et al. (3,4,5) over the 1930s showed that CPAP delivered through a face mask could be useful in the treatment of CPE and other forms of respiratory failure. Noninvasive IPPV administered through a mouthpiece was first described by Motley (6) in the 1940s and was used widely until the early 1980s, either for aerosol delivery in patients with chronic obstructive pulmonary disease (COPD) and asthma, or as a means of ventilatory assistance. The use of noninvasive IPPV declined sharply after the demonstration of lack of benefit in comparison to simple nebulizing treatments (7).
The proliferation of NIV occurred during the 1980s, after the introduction of nasal mask ventilation in the management of obstructive sleep apnea (8). Despite a lack of randomized controlled trials, NIV became the ventilatory mode of first choice for patients with neuromuscular diseases and chest wall deformities (9,10,11,12). In the early 1990s, the encouraging results obtained in the treatment of acute respiratory failure (ARF) by using NPPV (13,14,15) stimulated investigation on various applications in the acute care setting. The desire of avoiding complications of endotracheal intubation (16,17,18,19), potentially lowering morbidity and mortality rates in selected patients with ARF (20,21,22,23), has been the major driving force of the increasing use of NPPV in the acute care setting over the past decade.
In their 28-day international study on patients admitted to 361 ICUs who received mechanical ventilation for more than 12 hours, Esteban et al. (24) found that NPPV through a facial mask was used in 4.9% of overall patients and in 16.9% of patients ventilated because of an exacerbation of COPD. In a prospective 3-week survey of 70 French ICUs performed in 2002, Demoule et al. (25) showed that 23% of patients requiring ventilatory assistance received NPPV as a first-line treatment, a significant increase compared to 1997 (16%) (26); the incidence of NIV for patients admitted to the ICU without intubation was also significantly increased compared to 1997 (52% vs. 35%); furthermore, 3% of patients in 2002 received NPPV before ICU admission compared to none in 1997 (25,26).
Equipment and Techniques
The following paragraphs will discuss various interfaces and ventilatory modes available for administration of NIV. Cough-enhancing techniques will also be described.
Interfaces
Interfaces are devices that connect ventilator tubing to the face, allowing the delivery of pressurized gas into the airway during NIV. Currently available interfaces include nasal and oronasal masks, helmets, and mouthpieces. Selection of a comfortable interface that fits properly is a key issue for the success of NIV.
Nasal Masks
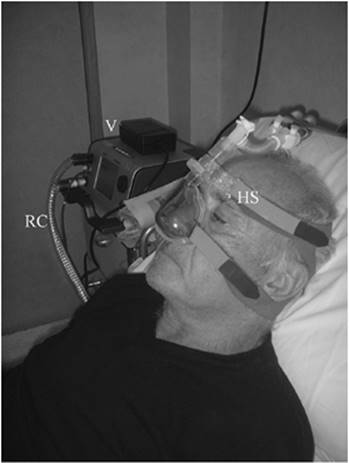
The standard nasal mask is a triangular or cone-shaped clear plastic device that fits over the nose and uses a soft cushion or flange to seal over the skin (Fig. 129.1). Because of the pressure exerted over the bridge of the nose, the mask may cause skin irritation and redness, and occasionally ulceration (Fig. 129.2). For occasional patients who cannot tolerate commercially available masks, custom-molded, individualized masks that conform to facial contours of the patient can be constructed. Several types of strap systems have been used to hold the mask in place. Depending on the interface, straps attach at two or as many as five points on the mask and may be provided with Velcro fasteners. The nasal mask is generally preferred for chronic administration of NIV. In patients with a nasogastric tube, a seal connector in the dome of the mask may be used to avoid air leakage.
|
|
|
Figure 129.1. Noninvasive ventilation delivered through a nasal mask. HS, head straps; RC, respiratory circuit; V, ventilator. (Photograph printed with the permission of the patient.) |
|
|
|
Figure 129.2. Skin lesions caused by a mask. Please note that the point at major risk to develop a skin necrosis is the bridge of the nose. (Photograph printed with the permission of the patient.) |
|
|
|
Figure 129.3. Noninvasive ventilation delivered through nasal pillows. AH, active humidifier; RC, respiratory circuit; V, ventilator. (Photograph printed with the permission of the patient.) |
Nasal Pillows
Nasal pillows or seals consist of soft rubber or silicone plugs that are inserted directly into the nostrils (Fig. 129.3). As they exert no pressure over the bridge of the nose, nasal pillows may be useful in patients who develop irritation or ulceration on the nasal bridge while using nasal or oronasal masks.
Oronasal Masks
Oronasal or face masks cover both the nose and the mouth (Fig. 129.4). The oronasal mask is largely used in patients with copious air leaking through the mouth during nasal mask ventilation. Interference with speech, eating, and expectoration, and the likelihood of claustrophobic reactions, are greater with oronasal than with nasal masks. In the acute setting, however, oronasal masks are preferable to nasal masks because dyspneic patients are mouth breathers, predisposing to greater air leakage during nasal mask ventilation. The oronasal masks, like the nasal mask, may cause skin necrosis over the nasal bridge (27). When the opening pressure of the upper esophageal sphincter (25–30 cm H2O) is overcome, the positioning of a nasogastric tube may protect from gastric distension, even though this is not a common event.
A type of oronasal mask is the “total” face mask (28), which is made of clear plastic and uses a soft silicone flange that seals around the perimeter of the face like a hockey goalie's mask, avoiding direct pressure on facial structures.
Helmet
The helmet (Fig. 129.5) is made of transparent latex-free polyvinyl chloride and is secured by two armpit braces at two hooks (one anterior and the other posterior) of the plastic ring that joins the helmet with a seal connection soft collar adherent to the neck (29,30). The pressure increase during ventilation makes the soft collar sealing comfortable to the neck and shoulders, avoiding air leakage (29). The whole apparatus is connected to an ICU ventilator by a standard respiratory circuit. The two ports of the helmet act as inlet and outlet for inspiratory and expiratory gas flows. The inspiratory and expiratory valves are those of the mechanical ventilator. A specific connector placed in the plastic ring can be used to allow the passage of a nasogastric tube, thus reducing air leaks. The patient is allowed to drink through a straw or to be fed a liquid diet. A new version of the helmet, recently developed, has an antiasphyxia device and two inner inflatable cushions to increase comfort and reduce the internal volume. The main advantages of the helmet include a good tolerability in both adult and pediatric populations (31), with a satisfactory interaction of the patients with the environment; a lower risk of dermal lesions; and, compared with the mask, easier applicability to any patient regardless of the face contour.
|
|
|
Figure 129.4. Noninvasive ventilation delivered through an oronasal mask. HS, head straps; NGT, nasogastric tube; RC, respiratory circuit; SC, seal connection. (Photograph printed with the permission of the patient.) |
|
|
|
Figure 129.5. Noninvasive ventilation delivered through a helmet. AB, armpit braces; IC, inflated cushion; IP, inlet port; NGT, nasogastric tube; OP, outlet port; RC, respiratory circuit; SC, seal connection; SV, security valve; V, ventilator. (Photograph printed with the permission of the patient.) |
Mouthpieces
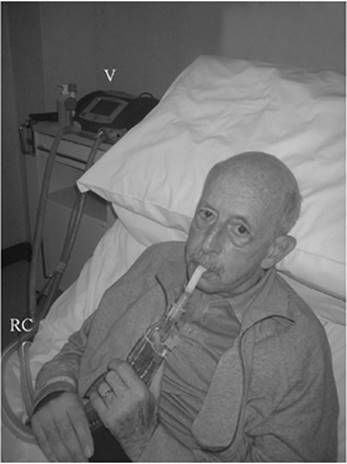
Mouthpieces are simple and inexpensive devices used to provide NPPV for as long as 24 hours a day to patients with chronic respiratory failure (Fig. 129.6). If nasal air leaking reduces efficacy, ventilator tidal volume may be increased or cotton plugs or nose clips may be used for occluding the nostrils. NPPV via mouthpieces has proved to be a valid alternative to tracheostomy in some patients with chronic respiratory muscle insufficiency (32).
|
|
|
Figure 129.6. Noninvasive ventilation delivered through a mouthpiece. RC, respiratory circuit; V, ventilator. (Photograph printed with the permission of the patient.) |
Physiologic Aspects and Patient–Ventilator Interaction during NPPV Delivered by Different Types of Interfaces
The choice of an appropriate interface is one of the crucial issues affecting NIV outcome. Data obtained from physiologic evaluations of NPPV delivered by different types of interfaces have been useful to improve devices and patient–ventilator synchrony.
The study of mask mechanics and air leak dynamics during NPPV may guide mask fit and inspiratory pressure (33). The pressure that fits the mask's cushion against the patient's face is represented by the pressure inside the cushion and is measured by connecting a pressure transducer to the cushion's inflation valve. The mask occlusion pressure is obtained by calculating the gradient between the mask fit pressure and airway pressure.
In a controlled study of a group of stable hypercapnic patients (34), the nasal mask used for delivering NPPV was better tolerated than either nasal pillows or an oronasal mask but was less effective at lowering PaCO2. In another controlled trial of 70 patients with acute respiratory failure (ARF) who randomly received either nasal mask or oronasal NPPV (35), both masks performed similarly with regard to improving vital signs and gas exchange and avoiding intubation, but the nasal mask was significantly less well tolerated than the oronasal mask.
In contrast to NIV via nasal or oronasal masks, with helmet-delivered NIV, patients receive only part of the large volumes administered by the ventilator after inspiratory trigger activation. The rest of the volume is compressed around the head, pressurizing the helmet. It is therefore impossible to measure patient tidal volumes and flows with conventional bedside monitoring. The internal volume surrounding the head varies between 6 and 8 L, but this usually does not represent a problem for rebreathing, provided that sufficient levels of pressure support are delivered (29). When measuring partial pressure of inspired CO2 and end-tidal CO2 in healthy volunteers at 10 cm H2O pressure support, CO2 rebreathing with the helmet is less than 1.5% and is similar to that detected with the oronasal mask (30).
In a physiologic study of eight healthy subjects randomized to receive either face mask or helmet CPAP, Patroniti et al. (36) showed that helmet CPAP is as effective as face mask CPAP in increasing end-expiratory lung volume and in minimizing respiratory airway pressure oscillations, without the need of a reservoir bag. In addition, the authors suggested that high gas flow rates should always be considered during helmet-delivered CPAP, to improve CO2 washout and decrease CO2 rebreathing, given the elevated dead space. In a physiologic evaluation of different levels of pressure support ventilation (PSV) during helmet-delivered NPPV (37), the helmet was effective in reducing the inspiratory effort and was efficient in providing ventilation to eight healthy volunteers, without relevant CO2 rebreathing. Furthermore, a low level of PSV (5–10 cm H2O) allowed optimal comfort even at high PEEP (10 cm H2O), whereas a significant discomfort was observed with PSV at 15 cm H2O.
During NPPV, the ventilator must first pressurize the interface and then the respiratory system (38). Some physiologic studies on healthy subjects (38,39) showed that the use of the helmet to deliver PSV increased inspiratory muscle effort and required a longer time to reach the selected level of airway pressure compared with the standard face mask, thus worsening patient–ventilator asynchrony. More recently, Moerer et al. (40) reported a bench study of ventilatory performance by using an in vitro lung model capable of stimulating spontaneous breathing, and compared a helmet and face mask during NPPV at different levels of PSV and PEEP. Measurements included the time delay to activate the ventilatory trigger, the time between the initiation of an inspiratory effort until the preset PEEP level is reached, and the inspiratory pressure–time product (which reflects the inspiratory muscle effort) during these two periods. The helmet, although presenting a significantly longer time delay, caused a lower pressure–time product compared to the face mask. In addition, by increasing the level of PSV or PEEP, the helmet furthermore significantly reduced the delay times and pressure–time product. The investigators suggested that using a minimum PEEP of 6 cm H2O and adding PSV may shorten the delay times and reduce inspiratory muscle effort, and will hardly promote the occurrence of wasted efforts. The longer delay times observed during helmet-delivered NPPV are presumably a consequence of the high compliance of the actual design of the helmet, which needs higher inspiratory volumes than the face mask to reach the same airway pressure. However, the patient can use the large air reservoir within the helmet at the beginning of an inspiration, thus reducing the initial inspiratory muscle effort.
Ventilatory Modes
Continuous Positive Airway Pressure
Continuous positive airway pressure (CPAP) delivers a constant pressure throughout spontaneous inspiration and exhalation without assisting inspiration. Because spontaneous breathing is not assisted, this technique requires an intact respiratory drive and adequate alveolar ventilation. CPAP increases functional residual capacity and opens underventilated alveoli, thus decreasing right-to-left intrapulmonary shunt and improving oxygenation and lung mechanics (41). Moreover, CPAP may reduce the work of breathing and dyspnea in COPD patients by counterbalancing the inspiratory threshold load imposed by intrinsic PEEP (42). Effects on hemodynamics during CPAP have been widely described. By lowering left ventricular transmural pressure in patients with left congestive heart failure, CPAP may reduce left ventricular afterload without compromising cardiac index (43,44). For several years, it was hypothesized that positive airway pressure, by increasing right atrial pressure (45), reduced venous return by decreasing the pressure gradient between mean systemic filling pressure and right atrial pressure (46). However, as demonstrated in experimental (47,48) and human (49) studies, positive airway pressure does not affect the gradient for venous return, because pleural pressure is transmitted to the same extent to both the mean systemic and right atrial pressures. CPAP can be applied by various devices including low flow generators with an inspiratory reservoir, high-flow jet venturi circuits (Fig. 129.7) (both of them with an expiratory mechanical or water valve), and bilevel and critical care ventilators. Continuous positive pressure may be administered using the demand flow (DF) or the gold standard continuous flow (CF) system. With DF CPAP, the patient has to trigger a preset pressure to open the demand valve, whereas with CF CPAP, no valves are present. The work of breathing is significantly greater with the DF system than with the CF one (50,51,52). It is crucial to provide an adequate air flow rate for maintaining a continuous positive pressure, especially in dyspneic patients who breathe at high flow rates.
|
|
|
Figure 129.7. Helmet continuous positive airway pressure (CPAP) delivered by a high-flow jet venturi system. EMV, expiratory mechanical valve; JVS, jet venturi system; RC, respiratory circuit. (Photograph printed with the permission of the patient.) |
Pressure Support Ventilation
Pressure support ventilation (PSV) is a pressure-triggered, pressure-targeted, flow-cycled mode of ventilation. It delivers a preset inspiratory pressure to assist spontaneous breathing, augmenting spontaneous breaths and offsetting the work imposed by the breathing apparatus. A sensitive patient-initiated trigger causes the delivery of inspiratory pressure support that is maintained throughout inspiration, and a reduction in inspiratory flow drives the ventilator to cycle into expiration. Therefore, the patient can control either inspiratory duration or breathing rate. Typical starting pressures are a PEEP of 3 to 5 cm H2O and an inspiratory airway pressure of 8 to 12 cm H2O (Table 129.1).
Bilevel Positive Airway Ventilation
In bilevel positive airway pressure (BiPAP), a valve sets two pressure levels, the expiratory positive airway pressure (EPAP) level, and the inspiratory positive airway pressure (IPAP) level, even in the presence of rapidly changing flows. With this technique, ventilation is produced by the cyclic delta pressure between IPAP and EPAP. EPAP also recruits underventilated lung and offsets eventual intrinsic PEEP.
|
Table 129.1 Proposed Ventilator Settings for Pressure Support Ventilation Mode |
||||||||||||
|
Controlled Mechanical Ventilation
In the mandatory controlled mechanical ventilation (CMV) mode, no patient effort is required, as full ventilatory support is provided. In this mode, ventilator settings include inflation pressure or tidal volume, frequency, and the timing of each breath.
Pressure control ventilation (PCV) delivers time-cycled preset inspiratory and expiratory pressures with adjustable inspiratory-to-expiratory ratios at a controlled rate. The resulting tidal volume is determined by the compliance of the lungs and chest wall, and the resistance to flow of ventilator tubing.
In volume control ventilation (VCV), tidal volume is set and the resulting pressure depends on the thoracic and circuit compliance. VCV can be preferred for those patients with severe chest wall deformity or obesity who may need higher inflation pressures.
Assist/Control Ventilation
In assist/control (A/C) ventilation, the ventilator delivers a breath either when triggered by the patient's inspiratory effort (assist) or independently, if such an effort does not occur within a preselected period (control). When triggering occurs, the ventilator delivers an identical breath to mandatory breaths. Volume-cycled and pressure-limited or pressure-targeted modes are available.
Proportional Assist Ventilation
Proportional assist ventilation (PAV) is an alternative technique in which both flow and volume are independently adjusted. In this technique, the ventilator generates volume and pressure in proportion to the patient's effort, increasing comfort and so improving success and compliance with NPPV (53). Despite the promising concept, there is a substantial lack of large clinical studies.
Ventilatory Mode Selection
All ventilatory modes of NPPV have been used to achieve physiologic or clinical benefit, with theoretical advantages and limitations. Spontaneously breathing patients with respiratory failure of various causes may benefit from CPAP to correct hypoxemia. In acute CPE, mask CPAP can result in early physiologic improvement and reduce the need for intubation (54). In one study (55), BiPAP improved ventilation and vital signs more rapidly in patients with CPE, but it was associated with a higher rate of myocardial infarction compared with CPAP. Conversely, a more recent study (56) found no difference in the risk for developing myocardial infarction during NIV delivered by CPAP or BiPAP modes.
VCV can be useful in patients with changing respiratory impedance. In the presence of elevated peak inspiratory airway pressure, however, this technique is susceptible to air leaks, gastric distention, skin irritation and, consequently, poor patient tolerance.
Pressure-targeted modes maintain delivered tidal volume in patients with air leaking better than volume-targeted modes. Therefore, pressure-targeted ventilators are preferred over volume-targeted ventilators to deliver NPPV in the presence of substantial leaks (57). To best compensate for air leaks, pressure-targeted ventilators should have high and sustained maximal inspiratory flow capabilities (>3 L/second), adjustable I:E ratios and other mechanisms to limit inspiratory duration so that inversion of the I:E ratio is avoided, and adjustable trigger sensitivities or algorithms to prevent autocycling (57). Ventilatory systems for air leak detection, calculation, and compensation are now largely available.
When PSV is used as a noninvasive ventilatory assistance mode, some forms of patient–ventilator asynchrony might be intensified, causing breathing discomfort. During PSV, indeed, brief rapid inhalations may not permit adequate time for the ventilator to cycle into expiration, so that the patient's expiratory effort begins while the unit is still delivering inspiratory pressure (58). Also, eventual air leaks during noninvasive PSV may prevent adequate reduction in inspiratory flow required to open the expiratory valve, thereby prolonging inspiratory flow despite expiratory efforts. When this occurs, a time-cycled expiratory trigger provides a better patient–machine interaction than flow-cycled expiratory trigger (59).
In acute hypercapnic exacerbations of COPD, NPPV performed by different ventilatory modes including PSV, ACV, and PAV is able to provide respiratory muscle rest and improve respiratory physiologic parameters (60,61,62). No difference in clinical outcome or arterial blood gas tensions between patients ventilated in ACV and PSV modes has been found, even though PSV has seemed to be more acceptable to patients and associated with fewer side effects in comparison with ACV (63). As in the intubated mechanically ventilated COPD patients, application of external PEEP is effective in counterbalancing the effects of auto-PEEP and dynamic hyperinflation. The use of noninvasive ventilatory modes in patients with hypoxemic ARF of various causes can improve arterial blood gases, respiratory rate, and dyspnea, and unload the accessory muscles of respiration (20,21,64).
Triggering systems are critical to the success of NPPV in both assist and control modes. During assisted ventilation, flow triggering reduces breathing effort more effectively as compared with pressure triggering, obtaining a better patient–ventilator interaction (65,66,67).
In the absence of evidence favoring a specific ventilatory mode, the choice should be dictated by personal experience, as well as cause and severity of the pathologic process responsible for ARF (68). However, assisted modes (and particularly PSV) are usually best tolerated and can be safely and effectively performed. A modality that provides a backup rate is needed for patients with inadequate ventilatory drive.
Techniques to Assist Cough
The cough mechanism may be severely impaired in neuromuscular diseases when weak expiratory muscles are combined with a markedly reduced vital capacity. An effective cough depends on the ability to generate adequate expiratory airflow, estimated at >160 L/minute (69), which is determined by lung and chest wall elasticity, airway conductance, and expiratory muscle force. Also, an intact glottic function is needed for yielding high peak expiratory cough flows. Manually assisted coughing consists of quick thrusts applied to the abdomen using the palms of the hands, timed to coincide with the patient's cough effort. The maneuver should be applied cautiously after meals and with the patient positioned semiupright to reduce the risk of aspiration of gastric contents.
Manually assisted coughing may enhance expiratory force, but it does not increase inspired volume, so that patients with severely restricted volumes may still achieve insufficient cough flows. Such a limitation may be overcome by using the mechanical insufflator–exsufflator (Fig. 129.8), which delivers a positive inspiratory pressure of 30 to 40 cm H2O via a face mask and then rapidly switches to an equal negative pressure (70). The positive pressure produces an adequate tidal volume, whereas the negative pressure stimulates the high peak expiratory cough flows. Insufflator–exsufflator may be combined with manually assisted coughing to further augment cough effectiveness. Any technique used to assist cough can be performed effectively and frequently by skilled caregivers, with minimal discomfort to the patient.
Practical application
NIV should be considered early when patients first develop signs of incipient respiratory failure needing ventilatory assistance. It is crucial that caregivers can identify patients who are likely to benefit from NIV and exclude those for whom NIV would be unsafe. Once the decision to institute NIV has been taken, an interface and ventilatory mode must be chosen, and a close monitoring in an appropriate hospital location must be provided. The initial approach should consist in fitting the interface and familiarizing the patient with the apparatus, explaining the purpose of each piece of equipment. Patients should be motivated and reassured by the clinician, instructed to coordinate their breathing with the ventilator, and encouraged to communicate any discomfort or fears. Collaboration among medical practitioners including physicians, respiratory therapists, and nurses is critical to the success of NIV during the early phase of milder respiratory failure and after an initial period to 20 minutes interruption. For patients with more severe failure, NIV application has to be continuous for at least 12 to 24 hours (20), and discontinuation is allowed for short periods only when the clinical situation improves. Aggressive physiotherapy is crucial during the periods of NIV discontinuation. Endotracheal intubation must be rapidly accessible, when indicated (Table 129.2).
|
|
|
Figure 129.8. Mechanical insufflator–exsufflator (MIE). (Photograph printed with the permission of the patient.) |
Patient Selection
The criteria for selecting appropriate patients to receive NIV for ARF include clinical indicators of acute respiratory distress, such as moderate to severe dyspnea, tachypnea, accessory muscle use and paradoxical abdominal breathing, and gas exchange deterioration. Blood gas parameters aid in identifying patients with acute or acute superimposed on chronic CO2 retention. A conscious and cooperative patient is crucial for initiating NIV (Table 129.3), although hypercapnic patients with narcosis who are otherwise good candidates for NIV may represent an exception (71,72).
|
Table 129.2 Criteria for Noninvasive Ventilation Discontinuation and Endotracheal Intubation |
|
|
|
|
Table 129.3 Contraindications to Noninvasive Ventilation |
|
|
During NIV, patients can achieve a level of control and independence totally different from when intubated, and sedation is infrequently required. If benzodiazepines or opiates are administered, caution is advised to prevent undue hypoventilation. NIV should be avoided in patients with hemodynamic instability and in those who are unable to protect the airways (coma, impaired swallowing, and so on) (Table 129.3). Patients with severe hypoxemia (PaO2/FiO2 <100) or morbid obesity (>200% of ideal body weight) should be closely managed only by experienced personnel and with a low threshold for intubation (20,21,73). In the presence of a pneumothorax, NIV can be initiated provided an intercostal drain is inserted. Criteria for NIV discontinuation and endotracheal intubation must be thoroughly considered to avoid dangerous delays (Table 129.2).
Identification of predictors of success or failure may help in recognizing patients who are appropriate candidates for NIV and those in whom NIV is not likely to be effective, thereby avoiding its application and unnecessary delays before invasive ventilation is given. The severity of acidosis at baseline is a logical starting point for identifying patients who might benefit from NPPV. In a retrospective review aimed at identifying patients with COPD who could be treated successfully with NPPV, Ambrosino et al. (74) found that patients in whom NPPV treatment failed were significantly more acidemic at baseline than those successfully treated (mean pH 7.22 versus 7.28). Similarly, Brochard et al. (75), using a priori criteria for the need for intubation, found that success was less likely with a lower starting pH. Also the tolerance of NPPV and the change in arterial blood gas tensions and respiratory rate in the early hours are reasonable predictors of the subsequent outcome in ARF patients with or without hypercapnia (64,74,75,76,77,78,79). NPPV is less likely to be successful if there are associated complications or if the patient's premorbid condition is poor (78,79). Late failure, considered as occurring after 48 hours of successful NPPV, is recognized, with rates reported at 0 to 20%, and has been associated with poor outcomes (78). Patients affected by acute respiratory distress syndrome (ARDS) with a Simplified Acute Physiology Score (SAPS) II >34, and whose PaO2/FiO2 does not improve over 175 after 1 hour of NPPV should be carefully treated, under strict monitoring within the ICU where endotracheal intubation and invasive ventilation are promptly available (64). It is still unclear if the higher mortality observed in patients who failed NPPV and are eventually intubated might be due to a delayed intubation (64).
Machine Settings
Pressures commonly used to administer CPAP in patients with ARF range from 5 to 12 cm H2O. For pressure-cycled ventilation, it is suggested to start at low pressures to facilitate patient tolerance (appropriate initial pressures are a CPAP of 3 to 5 cm H2O and an inspiratory pressure of 8 to 12 cm H2O) and, if necessary, gradually increase pressure settings as tolerated to obtain alleviation of dyspnea, decreased respiratory rate, adequate exhaled tidal volume, and good patient–ventilator interaction (Table 129.1). In the presence of air leaks, adequate inspiratory flows and durations should be set, triggering sensitivity should be adjusted to prevent autocycling, and a mechanism to limit inspiratory time and avoid I:E ratio inversion should be considered when available (57). A backup rate should be applied in patients with inadequate triggering. When VCV is used to deliver NPPV, tidal volume is usually set higher (10–15 mL/kg) to compensate for air leaking. In any case, excessive inflation can cause activation of expiratory muscles during inspiration with consequent patient–ventilator asynchrony. Oxygen supplementation should be provided as needed to keep oxygen saturation above 90% or between 85% and 90% in patients at risk of worsening hypercapnia. When the duration of NIV is expected to be more than a few hours, a heated humidifier may help oronasal dryness and patient's comfort.
Monitoring
In the acute setting, patients can initiate NIV anywhere, at the onset of the acute respiratory distress, but after initiation, they should be transferred to an ICU or a step-down unit for continuous monitoring until they are sufficiently stable to be moved to a medical ward. During transfers, NIV and monitoring should not be discontinued. The early use of NIV for less acutely ill patients with COPD on a medical ward seems to be effective, but if pH is lower than 7.30, admission to an environment with intensive care monitoring is highly recommended (80).
Monitoring of patients undergoing NIV is aimed at determining whether the initial goals are being achieved, including relief of symptoms, reduced work of breathing, improved or stable gas exchange, good patient–ventilator synchrony, and patient comfort (Table 129.4). Gas exchanges are monitored by continuous oximetry and arterial blood gases at baseline, after 1 to 2 hours, and as clinically indicated; physiologic responses are evaluated by continuous electrocardiography, respiratory rate, blood pressure and heart rates; finally, dyspnea, as well as tolerance of the technique, symptoms of impaired sleep, patient–ventilatory asynchrony, and air leaking can be easily assessed through patient queries, bedside observation, and flow, volume, and pressure waveform analysis. If a poor response to NIV occurs and the specific measures used to correct the situation fail to address an adequate improvement within a few hours, NIV should be considered a failure, and invasive ventilation should be promptly considered.
|
Table 129.4 Monitoring of Patients Receiving Noninvasive Ventilation in the Acute Care Setting |
||||||
|
Indications
The following sections will review the available evidence on the efficacy of NIV for various applications in the acute care setting.
Acute Exacerbations of Chronic Obstructive Pulmonary Disease
In patients with ARF resulting from acute exacerbations of COPD, the use of NPPV has been proven to be effective in ameliorating dyspnea (77), improving vital signs and gas exchange (75,77,80,81,82), preventing endotracheal intubation (75,77,80,81), and improving hospital survival (75,80,81). Consequently, there is a general agreement concerning the early use of NPPV in such patients (68,83).
In COPD patients with acute respiratory decompensations, the increased flow resistance and the impossibility to complete the expiration before inspiration determine high levels of dynamic hyperinflation, and substantial shortening of the diaphragm and the inspiratory intercostals and accessory muscles, thereby reducing their mechanical efficiency and endurance. The need to overcome the inspiratory threshold load due to auto-PEEP and to drive the tidal volume against airway resistances increases the respiratory muscle fatigue. During NPPV, the combination of external PEEP and PSV offsets the auto-PEEP level and reduces the work of breathing that the inspiratory muscles must generate to produce the tidal volume (60).
In an early study on the use of face mask NPPV in patients with ARF, Meduri et al. (13) obtained improvements of gas exchanges and avoided endotracheal intubation in a group of COPD patients. Soon thereafter, Brochard et al. (14) described the short-term (45-minute) physiologic effects of inspiratory assistance with a face mask on gas exchange and respiratory-muscle work in 11 patients with COPD and evaluated the therapeutic use of the technique in 13 patients with COPD exacerbations, comparing the results in the latter group with the results of conventional treatment in 13 matched historical-control patients. In the physiologic study, arterial pH rose from 7.31 to 7.38 (p <0.01), PaCO2 fell from 68 to 55 mm Hg (p <0.01) PaO2 rose from 52 to 69 mm Hg (p <0.05), and respiratory rate reduced from 31 to 21 breaths per minute (p <0.01) (14). Only 1 of 13 patients treated with NPPV needed intubation, as compared with 11 of the 13 historical controls (p <0.001). In addition, the NPPV-treated patients were weaned from the ventilator faster and spent less time in the ICU than did the control subjects (14). Subsequently, numerous randomized controlled trials using NPPV in ARF caused by COPD have been published (Table 129.5).
In the first randomized, prospective study on 60 COPD patients, Bott et al. (77) compared NPPV delivered through nasal mask with conventional therapy as a treatment of ARF. Patients receiving NPPV had a significant reduction of PaCO2 and dyspnea score, and 30-day mortality (10% vs. 30%). A multicenter European trial (75) on the efficacy of NPPV in acute exacerbation of COPD randomized 85 COPD patients to receive face mask PSV or conventional treatment (oxygen therapy plus drugs). After 1 hour of NPPV, respiratory rate but not PaCO2 showed a significant decrease. The group of patients treated with NPPV had a significantly lower intubation rate, a lower complication rate (14% vs. 45%), length of hospital stay, and mortality rate. In another randomized study on 23 COPD patients that compared NPPV with conventional treatment, the investigators reported a reduction of intubation rate, with a significant improvement in PaO2, heart rate, and respiratory rate in the NPPV group, even though PaCO2 did not significantly decrease (81). A randomized study on 30 COPD patients with ARF (82) confirmed that early application of NPPV facilitates gas exchange improvement, reduces the need for invasive mechanical ventilation, and decreases the duration of hospitalization. In a randomized trial on 50 COPD patients with acute exacerbation, NPPV reduced weaning time, shortened the length of stay in the ICU, decreased the incidence of nosocomial pneumonia, and improved 60-day survival rates (88). Other and more recent prospective randomized controlled studies on patients with ARF due to COPD exacerbations (89,90) have confirmed the benefit of applying NPPV in improving clinical status and blood gases.
A randomized prospective study by Conti et al. (91) has compared the short- and long-term response to face mask NPPV versus invasive conventional ventilation in COPD patients with ARF failing to sustain the initial improvement with conventional medical therapy in the emergency ward and needing ventilatory assistance. In this study, the intubation rate of 52% in the NPPV group was higher than in other randomized controlled trials, which is not surprising given the higher severity of illness of these patients, as evidenced by the mean pH of 7.2, compared with 7.27 in the study of Brochard et al. (75) and 7.32 in the study of Plant et al. (80). Although the patients who received NPPV were sicker than those reported in previous studies, they showed a trend toward a lower incidence of nosocomial pneumonia during the ICU stay and a better outcome at a 1-year follow-up, as well as no significant differences in ICU and hospital mortality, overall complications, duration of mechanical ventilation and ICU. These findings support early use of NPPV during the course of acute exacerbation of COPD patients. However, also if NPPV is started later, after the failure of medical treatment, it is comparable to invasive mechanical ventilation in terms of survival.
In a matched case-control study conducted in ICU, 64 COPD patients with advanced ARF (pH ≤7.25, PaCO2 ≥70 torr, and respiratory rate ≥35 breaths/minute) prospectively received NPPV and their outcomes were compared with those of a control group of 64 COPD patients (92). NPPV had a high rate of failure (40/64), although mortality rate, duration of mechanical ventilation, and lengths of ICU and post-ICU stay were not different between the two groups, and the NPPV group had fewer complications. In this study, patients who failed NPPV were not harmed by the delayed institution of invasive ventilation, and those who avoided endotracheal intubation had a clear-cut benefit. Based on these results, the authors suggested that in COPD patients with advanced ARF, it might be worthwhile to attempt a trial of NPPV prior to a shift to invasive ventilation with endotracheal intubation.
In summary, NPPV should be considered the first-line therapeutic option to prevent endotracheal intubation and improve outcome in patients with exacerbations of COPD who have no contraindication to NPPV (Table 129.3).
Asthma
NPPV is considered an option in asthmatic patients at risk for endotracheal intubation. However, mechanical ventilation may be dangerous in patients with asthma, first, by worsening lung hyperinflation with the risk of causing barotrauma, and second, by inducing hemodynamic deterioration by increased intrathoracic pressure. To date, guidelines for NPPV in severe asthma are not supported by strong data. In one study (93), only two of 17 severe asthmatic patients (average initial pH of 7.25 and PaCO2 of 65 mm Hg) required intubation after starting therapy with face mask PSV, and the use of NPPV was associated with a rapid correction of gas exchange abnormalities and improvement in dyspnea. In a retrospective analysis of 33 asthmatic patients treated with NPPV or invasive mechanical ventilation (94), although the NPPV patients were less hypercapnic than the other group, gas exchange and vital signs improved rapidly in the NPPV group, and only three patients eventually required endotracheal intubation. A prospective, randomized, placebo controlled study compared 15 patients with acute asthma who received NPPV plus conventional therapy versus conventional therapy alone, and found an improvement in lung function and decreased hospital admission rate in the NPPV group (95). In contrast, another randomized trial found no significant advantages of NPPV in patients with acute asthma (96), and medical therapy alone can be highly effective in the management of asthmatic patients (97). Therefore, in the absence of clear evidence, no conclusions can be drawn regarding the relative effectiveness of NPPV versus conventional therapy in acute exacerbations of asthma.
Hypoxemic Respiratory Failure
Trials of NPPV in patients with hypoxemic respiratory failure, defined as those with ARF not related to COPD, have yielded conflicting results. In hypoxemic ARF patients, NPPV has been adopted to decrease the amount of work of breathing, correct the rapid shallow breathing, and prevent respiratory muscle fatigue and endotracheal intubation. The studies reviewed in these sections have been conducted on heterogeneous groups of patients with hypoxemic respiratory failure, whereas the analyses of homogeneous patient populations are discussed under each specific topic. Randomized controlled trials using NPPV in hypoxemic ARF patients are shown in Table 129.6.
|
Table 129.5 Randomized Controlled Studies Using Noninvasive Ventilation in Chronic Obstructive Pulmonary Disease |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Meduri et al. (13) in 1989 reported one of the first clinical applications of NPPV in patients with hypoxemic respiratory failure. Subsequently, Pennock et al. (99) reported a 50% success in a large group of patients with ARF of different causes, and similar good results were achieved using NPPV with nasal mask in a second study (100). Wysocki et al. (101) randomized 41 non-COPD patients with ARF to NPPV delivered by face mask versus conventional medical therapy. NPPV reduced the need of endotracheal intubation, the duration of ICU stay, and mortality rate only in those patients with hypercapnia (PaCO2>45 mm Hg), while having no significant advantages in the hypoxemic group without concomitant hypercarbia. On the basis of these results, the investigators concluded that NPPV may not be beneficial in all forms of ARF not related to COPD. In a study conducted by Meduri et al. (102) on the use of NPPV to treat respiratory failure of varied origins, 41 of 158 patients were hypoxemic. These patients required endotracheal intubation in only 34% of cases and showed a mortality rate of 22% compared with a predicted mortality (using the APACHE II score) of 40%. In a pilot study on patients with hematologic malignancies complicated by ARF (103), 15 of 16 individuals showed a significant improvement in blood gases and respiratory rate within the first 24 hours of nasal mask NPPV treatment.
Antonelli et al. (20) conducted a prospective, randomized study comparing NPPV via a face mask to endotracheal intubation with conventional mechanical ventilation in 64 patients with hypoxemic ARF who required ventilatory assistance after failure to improve with aggressive medical therapy. After 1 hour of mechanical ventilation, both groups had a significant improvement in oxygenation. Ten (31%) patients treated with NPPV required endotracheal intubation. Patients randomized to conventional ventilation developed significantly more frequent septic complications such as pneumonia or sinusitis (31% vs. 3%). Among survivors, NPPV patients had a lower duration of mechanical ventilation (p = 0.006) and a shorter ICU stay (p = 0.002). On the basis of these results, this trial suggested that NPPV may lead to more favorable outcomes than conventional ventilation in the management of patients with hypoxemic respiratory failure. Conversely, Wood et al. (104) had a substantially negative evaluation of the use of NPPV when applied to patients with hypoxemic ARF. These investigators randomized 27 patients in the emergency department to receive conventional medical therapy or NPPV for the treatment of hypoxemic respiratory failure. The 16 patients who were randomized to the NPPV group had an intubation rate and duration of ICU stay similar to the 11 patients who received medical treatment alone, but there was a trend toward a greater rate of hospital mortality among the patients in the NPPV group compared to patients in the conventional medical therapy group. Several factors may have influenced these negative results of this study. Among patients requiring endotracheal intubation, those of the NPPV group had a longer delay to intubation (26 vs. 4.8 hours, p = 0.055). In addition, it cannot be excluded that a sicker patient population was randomized to NPPV. Indeed, NPPV patients had a lower PaO2 (60 vs. 71), fewer patients with COPD (12% vs. 36%), and more patients with pneumonia (44% vs. 18%), ARDS (1 vs. 0), and interstitial lung disease (1 vs. 0). Furthermore, they had a higher APACHE II score (18 vs. 16), and more required admission to an ICU (81% vs. 64%).
In a study on 10 hemodynamically stable patients with severe acute lung injury or acute respiratory distress syndrome (ARDS) (105), NPPV had a high success rate (66%) and high hospital survival (70%). Three of the six patients who received NPPV as initial mode of ventilatory assistance were discharged from the ICU within 48 hours. Survival for the 10 patients was 70%, and duration of successful NPPV ranged from 23 to 80 hours. Ferrer et al. (106) have prospectively randomized 105 patients with severe hypoxemic ARF to receive NPPV or high-concentration oxygen. Compared with oxygen therapy, NPPV decreased the need for intubation (13 [25%] vs. 28 [52%]), the incidence of septic shock (6 [12%] vs. 17 [31%]), and the ICU mortality (9 [18%] vs. 21 [39%]), and increased the cumulative 90-day survival (all, p <0.05). Also the improvement of tachypnea and arterial hypoxemia was higher in the NPPV group. In a physiologic study performed by L'Her et al. (107) in patients with acute lung injury, noninvasive PSV combined with PEEP improved dyspnea and gas exchange and lowered neuromuscular drive and inspiratory muscle effort.
In ARDS, transient loss of positive pressure during mechanical ventilation may seriously compromise lung recruitment and gas exchange. For this reason, most NPPV studies have excluded patients with ARDS, and limited data are currently available in the literature. The first application of NIV (via face mask CPAP) in patients with increased permeability pulmonary edema ARDS was reported by Barach et al. in 1938 (4). In 1982, Covelli et al. (108) applied face mask CPAP in 35 patients with ARDS of varied causes, with all patients improving their oxygenation within the first hour of therapy. Only five patients were ultimately intubated, two from mask discomfort and three from a change in mental status and lack of cooperation. In two randomized studies, Antonelli et al. (20,21) reported that among patients with ARDS (n = 31), NPPV avoided intubation in 60%, whereas in their trial including a small number of ARDS patients (n = 7), Ferrer et al. (106) reported an 86% intubation rate. Two NPPV observational studies involving 98 ARDS patients reported an intubation rate of 50% (79,105), which was similar in patients with ARDS of pulmonary or extrapulmonary origin (79). Antonelli et al. (64) prospectively investigated, under close ICU observation, the application of NPPV as first-line intervention in 147 patients with early ARDS. NPPV improved gas exchange and avoided intubation in 54% of treated patients. Avoidance of intubation was associated with less ventilator-associated pneumonia (2% vs. 20%, p <0.001) and a lower ICU mortality rate (6% vs. 53%, p <0.001). SAPS II >34 and a PaO2/FIO2 <175 after 1 hour of NPPV were independently associated with NPPV failure and need for endotracheal intubation.
The above findings are, for the most part, supportive of the use of NPPV to treat hypoxemic patients without hypercapnia. However, an extremely prudent approach is needed, limiting the application of NPPV to hemodynamically stable patients who can be closely monitored in the ICU where endotracheal intubation is promptly available. A decisional flow chart may be adopted in applying NPPV to patients with ARDS (Fig. 129.9).
|
Table 129.6 Randomized Controlled Studies Using Noninvasive Ventilation i\In Nonchronic Obstructive Pulmonary Disease |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Figure 129.9. Decisional flow chart for the application of noninvasive ventilation to acute respiratory distress syndrome (ARDS). ETI, endotracheal intubation; NIV, noninvasive ventilation. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Cardiogenic Pulmonary Edema
Applying positive air pressure has been shown to decrease the work of breathing (41) and left ventricular afterload while maintaining cardiac index (44), thereby benefiting patients with cardiac dysfunction and ARF. The use of mask CPAP in patients with CPE was first described in the 1930s by Poulton and Oxon (2) and Barach et al. (3,4). More recently, several studies have examined responses to NIV of patients with CPE (54,55,56,109,110,111,112,113,114,115,116,117).
A systematic review and meta-analysis performed by Collins et al. (118) suggested that early application of NIV in the emergency department can decrease the relative risk of mortality by 39% and the necessity of endotracheal intubation by 57% when compared with standard medical therapy alone. However, in patients with CPE, NIV should not be viewed as the exclusive therapy, but should be accompanied by the aggressive conventional medical treatment.
In the comparison of NIV modalities, BiPAP has the potential advantage over CPAP of assisting the respiratory muscles during inspiration, which would result in faster alleviation of dyspnea and exhaustion (119). Nevertheless, according to all available data, there is no evidence to suggest superiority of either CPAP or BiPAP in terms of intubation or mortality, even in patients with CPE and hypercapnia (118,120,121). The results of one of the earlier studies showed that BiPAP compared with CPAP might increase the risk for new-onset acute myocardial infarction in patients with CPE (55). A recent study specifically examining myocardial infarction rates with BiPAP compared to CPAP (56) showed no significant difference between groups (CPAP, 3/22; BiPAP, 2/24).
In conclusion, NIV should be strongly considered as a first-line treatment in patients with CPE. Future studies are needed to address the NIV modality of choice and to clarify the actual risk of myocardial infarction.
Pneumonia
The application of NIV to treat pneumonia has yielded no definitive conclusions. In a large controlled trial conducted by Ferrer et al. (106) on patients with severe acute hypoxemic failure, NPPV prevented intubation and improved ICU survival in a subgroup of 34 patients with pneumonia compared with high-concentration oxygen. Confalonieri et al. (86) conducted a prospective, randomized study comparing NPPV delivered through a face mask to standard treatment in 56 patients with severe community-acquired pneumonia and ARF. NPPV was associated with a significant reduction in the rate of endotracheal intubation and duration of ICU stay. However, a post hoc analysis showed that the benefits occurred only in patients with underlying COPD. Jolliet et al. (122) used face mask NPPV in non-COPD patients with severe community-acquired pneumonia. Despite initial improvements in arterial oxygenation and respiratory rate in 22 of 24 patients, the intubation rate was high (66%). Thus, NPPV is indicated in COPD patients with community-acquired pneumonia, but caution should be applied in pneumonia patients without COPD, as the benefit of NPPV in such patients is currently unclear.
Immunocompromised Patients
Immunocompromised patients in whom respiratory failure develops often require mechanical ventilatory assistance. Endotracheal intubation is associated with numerous complications (16,17,18,19), and in immunosuppressed patients, invasive mechanical ventilation is associated with a significant risk of death (123,124,125). The use of NPPV in immunosuppressed patients has been reported in several studies. Among 11 patients affected by AIDS and opportunistic pneumonia, Meduri et al. (102) reported a 73% NPPV success rate in improving gas exchange. Conti et al. (103) evaluated NPPV delivered via nasal mask in 16 patients affected by ARF complicating hematologic malignancies. Fifteen of the 16 patients showed an early and significant improvement in blood gases and respiratory rate. Five patients died in the ICU following complications independent of the respiratory failure, whereas 11 were discharged from the ICU in stable condition. Antonelli et al. (21) randomized 40 recipients of solid organ transplantation with ARF to NPPV versus conventional therapy. Patients treated with NPPV more often had increases in oxygenation (60% vs. 25%, p = 0.03) and had lower intubation (20% vs. 70%, p = 0.002) and ICU mortality rates (20% vs. 50%, p = 0.05). In addition, the incidence of fatal complications was significantly reduced in the NPPV group. In another study, NPPV via face mask was well tolerated and avoided intubation in 18 of 21 patients developing ARF after bilateral lung transplantation (126). A randomized trial of 52 ARF patients with pneumonia and immunocompromised state of varied origin (127) showed reductions in the need for intubation (46% vs. 77%, p = 0.03) and hospital mortality rate (50% vs. 81%, p = 0.02) in NPPV-treated patients compared with conventionally-treated controls. It is reasonable to consider NPPV as a useful tool to avoid intubation and associated infectious complications in selected patients with immunocompromised states.
Facilitation of Weaning and Extubation
NPPV has been used to permit early extubation in patients who fail to meet standard extubation criteria, thus reducing the complications related to endotracheal tube.
Nava et al. (88) conducted a randomized, controlled trial of 50 patients intubated for ARF because of COPD who failed a T-piece weaning trial after 48 hours of invasive mechanical ventilation. Patients were randomized to undergo early extubation followed by face mask PSV or to remain intubated and undergo routine weaning. Patients receiving NPPV had higher overall weaning rates (88% vs. 68%), shorter durations of mechanical ventilation (10.2 vs. 16.6 days), briefer stays in the ICU (15.1 vs. 24 days), and improved 60-day survival rates (92% vs. 72%) (all p <0.05). Furthermore, none of the patients of the NPPV-treated group developed nosocomial pneumonia, compared with seven of the control group. Girault et al. (98) conducted a prospective, randomized controlled study in 33 patients with acute or chronic respiratory failure who failed a 2-hour T-piece weaning trial, although they met simple criteria for weaning. Sixteen patients initiated conventional invasive PSV, and 17 patients received NPPV immediately after extubation. The NPPV group had a shorter duration of endotracheal intubation (4.6 vs. 7.7 days, p = 0.004), but the total duration of mechanical ventilation was longer in the NPPV group (16.1 vs. 7.7 days, p = 0.0001). In addition, weaning and mortality rates and ICU and hospital lengths of stay were similar between groups. Ferrer et al. (128) investigated the efficacy of earlier extubation with NPPV during persistent weaning failure in 43 mechanically ventilated patients with ARF of varied causes who had failed a spontaneous breathing trial with a T piece for 3 consecutive days. Patients were randomly allocated, either for extubation and NPPV treatment or reconnection to the ventilator and conventional weaning approach consisting of once-daily weaning attempts. Compared with the conventional-weaning group, the NPPV group had shorter periods of invasive ventilation and ICU and hospital stays, less need for tracheotomy to withdraw ventilation, lower incidence of nosocomial pneumonia and septic shock, and increased ICU and 90-day survival (all p <0.05).
Besides weaning facilitation, another potential application of NIV in the weaning process is to avert the need for reintubation in patients with extubation failure, thereby avoiding the risk of increased morbidity and mortality associated with failed extubation (129). Keenan et al. (130) investigated the effectiveness of NPPV compared with standard medical therapy in preventing the need for endotracheal intubation in 81 patients who developed ARF during the first 48 hours after extubation. Comparing the two groups, no significant difference was found in the rate of reintubation or duration of mechanical ventilation, as well as in hospital mortality or ICU or hospital length of stay. Again, in a study conducted by Esteban et al. (131), no benefits from NPPV were found in avoiding reintubation in patients who had developed ARF after extubation, and NPPV was even associated with higher mortality rates as compared with patients treated according to standard treatment. In this study, the time from extubation to reintubation, which is an independent risk factor for increased mortality in reintubated patients (132), was longer in patients who received NPPV. Conversely, positive results were achieved by Ferrer et al. (133) who tested a strategy based on the early use of NPPV to avert reintubation in patients at risk for ARF after extubation. These authors randomized 162 mechanically ventilated patients who tolerated a spontaneous breathing trial but had increased risk for ARF after extubation to receive NPPV for 24 hours versus conventional management with oxygen therapy. In the NPPV group, ARF after extubation was less frequent (p = 0.029) and the ICU mortality was lower (p = 0.015), whereas 90-day survival did not change significantly between groups. Separate analyses of patients without and with hypercapnia (PaCO2 >45 mm Hg) during the spontaneous breathing trial showed that NPPV significantly improved ICU mortality and 90-day survival in hypercapnic patients only.
In summary, further studies are needed to establish the real efficacy of NPPV either in shortening weaning time or to avoid extubation failure, as well as to better define which patient categories are most likely to benefit from NPPV during the weaning process.
Do-Not-Intubate Orders
Applying NPPV has been described in patients with ARF who are poor candidates for endotracheal intubation or who are reluctant to undergo invasive ventilation. In one study of 30 patients, most elderly and COPD, in whom invasive ventilation was “contraindicated or postponed,” 18 patients (60%) were able to be successfully weaned from nasal mask NPPV (134). In a case series of 11 terminally ill patients with ARF who refused endotracheal intubation (135), NPPV delivered via face mask was effective in correcting gas exchange abnormalities in 7 patients, all of whom survived and left the ICU. The authors concluded that even when respiratory failure did not resolve, NPPV offered an effective, comfortable, and dignified method for these patients in providing symptomatic relief of dyspnea and maintaining continuous verbal communication with loved ones. In a trial conducted on 114 patients who declined intubation but accepted NPPV to treat their ARF (136), 49 patients (43%) survived to discharge. Awake patients with congestive heart failure or COPD and those with a more efficient cough mechanism had an increased probability of survival. Another study on 37 COPD patients with do-not-intubate orders who underwent NPPV because of ARF reported a 1-year survival of 30% (137).
A lack of agreement on applying NPPV in do-not-intubate patients does remain, with some authors warning of the potential ethical and economic cost of delaying the inevitable in patients with terminal respiratory failure (138). In patients with the do-not-intubate code, the use of NPPV is justifiable when the acute process responsible for ARF is known to respond well, such as CPE or COPD exacerbation. If NPPV is considered in these terminal patients, the caring clinician should inform the patient or surrogate that NPPV is being used as a form of life support and that it can be stopped at any time if not tolerated.
Postoperative Patients
Thoracic and upper abdominal surgery are associated with a prolonged postoperative gas exchange deterioration and reduction in functional residual capacity, PaO2, and forced vital capacity (139,140). Mask CPAP was initially used by Bunnell (1) in 1912 to maintain lung expansion in patients undergoing thoracic surgery, and by Boothby (141) et al. in 1940 for treating postoperative hypoxemic ARF. Applying mask CPAP or NPPV improves oxygenation and pulmonary function following upper abdominal surgery (139,142,143,144) or coronary artery bypass graft (145,146,147). Squadrone et al. (143) randomized 209 patients who developed severe hypoxemia after major elective abdominal surgery to receive oxygen or oxygen plus CPAP. CPAP-treated patients had a lower intubation rate (1% vs. 10%) and a lower occurrence rate of pneumonia (2% vs. 10%), infection (3% vs. 10%), and sepsis (2% vs. 9%) (all p <0.05) than patients treated with oxygen alone. NPPV improves gas exchange and reduces the need for intubation after lung resection (148,149) or bilateral lung transplantation (126). Thus, accumulating evidence supports the use of NIV to improve gas exchange and avoid reintubation and its attendant complications in selected postoperative patients with respiratory failure.
Obstructive Sleep Apnea
CPAP is recognized to be effective in correcting the respiratory and arousal abnormalities and improving sleep quality in obstructive sleep apnea syndrome (150,151). CPAP is believed to act by pneumatically “splinting” the pharyngeal airway, thus preventing its collapse during sleep (152,153). Also, nasal NPPV has been used in patients with ARF following obstructive sleep apnea syndrome, with improvements in clinical status and arterial blood gas values (154).
Trauma
ARF in trauma patients is generally associated with reduced pulmonary compliance and functional residual capacity, and subsequent restrictive defects (155). In a study of 33 trauma patients with ARF who received face mask CPAP, Hurst et al. (155) found rapid improvements in gas exchange, avoiding intubation in 94% of the cases. In a retrospective survey of 46 trauma patients with ARF who had been given mask NPPV, 33 patients (72%) were successfully weaned to spontaneous breathing (156). In another study (157), NPPV used as first-line treatment in 22 patients with ARF due to blunt chest trauma resulted in rapid improvement in blood gases and respiratory rate, and avoided intubation in 18 patients (82%). In a study of patients with acute hypoxemic respiratory failure needing ventilatory assistance, Antonelli et al. (20) reported that 7 of the 32 patients (22%) randomized to receive NPPV had trauma with pulmonary contusion or atelectasis. NPPV was associated with a rapid improvement in oxygenation, and all seven patients avoided intubation and survived. Despite the favorable results obtained, large randomized studies are needed before definitive recommendations on the use of NIV in posttraumatic ARF can be made.
Restrictive Diseases
NPPV has a role in the treatment of respiratory failure caused by some types of restrictive thoracic diseases. Bach et al. (158) demonstrated that NPPV can prolong survival while decreasing the respiratory morbidity and hospitalization rates in patients with Duchenne muscular dystrophy. Using NPPV prevented intubation in 7 of 11 episodes of ARF in a group of 9 patients with myasthenic crises (159). In ARF due to pulmonary fibrosis, prognosis is poor even when invasive mechanical ventilation is used (160). Aggressive respiratory physiotherapy is crucial in all patients with thoracic restriction.
Bronchoscopy
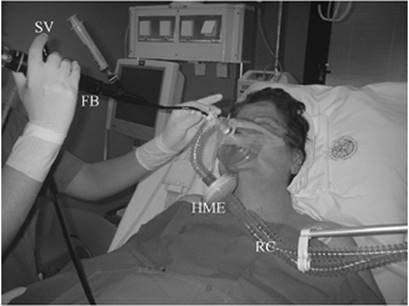
In nonintubated patients, severe hypoxemia is an accepted contraindication to fiberoptic bronchoscopy (FB). Since PaO2 routinely decreases after uncomplicated FB, these patients are at high risk for developing ARF or serious cardiac arrhythmias. Antonelli et al. (161,162) proposed a technique to perform FB with bronchoalveolar lavage in hypoxemic, nonintubated patients by means of facial mask NPPV (Fig. 129.10). The fiberoptic bronchoscope was passed through a T adapter and then advanced transnasally. The technique was safe and effective to avoid gas exchange worsening during FB and to allow an early and accurate diagnosis of pneumonia, preventing undesired intubation, in spontaneously breathing, hypoxemic patients. Similar results were achieved by using the helmet to deliver NPPV, allowing a safe diagnostic FB with bronchoalveolar lavage (163). The specific seal connector placed in the plastic ring of the helmet permitted the passage of the instrument, maintaining assisted ventilation.
|
|
|
Figure 129.10. Fiberoptic bronchoscopy performed during noninvasive ventilation delivered through an oronasal mask. FB, fiberoptic bronchoscope; HME, heat and moisture exchanger; RC, respiratory circuit; SC, seal connection; SV, suction valve. (Photograph printed with the permission of the patient.) |
Adverse effects and complications
Major adverse effects of NIV seldom occur in appropriately selected patients and are minimized when the technique is applied by experienced caregivers (164). The most frequently encountered complications are related to the interface, ventilator airflow or pressure, or patient–ventilator interaction.
The pressure of the mask over the bridge of the nose may induce discomfort, erythema, or ulceration (Fig. 129.2). There are various remedies to ameliorate this complication such as application of a hydrocolloid sheet over the nasal bridge or switching to alternative interfaces.
Air leakage under the mask into the eyes may cause conjunctival irritation, and excessive pressure may be responsible for sinus or ear pain. To minimize these problems, refitting the mask or lowering inspiratory pressure may be useful. Patient–ventilator asynchrony is a common cause of NIV failure and is often related to patient agitation or inability of the ventilator to sense the onset of patient expiration because of excessive air leaking. A judicious use of sedatives may be safe and effective in the treatment of NIV failure due to low tolerance (165), and minimizing air leaks (57,59) may improve patient–ventilator synchrony.
Presumably because of the low inflation pressure used compared with invasive ventilation, NPPV is well tolerated hemodynamically, but it should be avoided in patients with an unstable hemodynamic status, arrhythmias, or uncontrolled ischemia until these problems are stabilized. Gastric insufflation occurs commonly, but it is usually well tolerated. Aspiration pneumonia has been reported in as many as 5% of patients (102). The risk for aspiration is minimized by excluding patients with compromised upper airway function or problems clearing secretions and positioning a nasogastric tube in those with excessive gastric distention, an ileus, or nausea or vomiting. Although pneumothoraces occur very infrequently, inspiratory pressures should be kept at the minimum effective level in patients with bullous lung disease.
Summary
To date, the best-established indication for NIV in the acute care setting is ARF related to exacerbations of COPD. However, evidence has been rapidly accumulating to support application of NIV to treat many other types of ARF in selected patients. Further research should better define indications and patient selection criteria, as well as establish optimal techniques of administration.
Pearls
· NIV has the potential of avoiding the complications associated with endotracheal intubation, improving patient comfort, and preserving speech and airway defense mechanisms.
· Advances in patient–ventilator interfaces and ventilatory modes have fostered the increasing use of NIV in the acute care setting.
· The choice of ventilatory mode should be dictated by personal experience, as well as the patient's respiratory drive, and etiologic factors and severity of the underlying disease causing respiratory failure.
· It is crucial to identify patients who are likely to benefit from NIV and exclude those for whom NIV would be unsafe.
· Several factors are critical to the success of NIV: properly timed initiation, comfortable and well-fitting interface, patient preparation, careful ventilatory mode selection, and respiratory physiotherapy.
· Patients should receive NIV in an intensive care unit or a step-down unit for continuous monitoring until sufficient stabilization.
· NIV can be used to avoid intubation, but not to replace it. Invasive ventilation remains the method of choice for patients with respiratory failure who have contraindications to NIV.
· NIV is indicated as the ventilator mode of first choice in selected patients with COPD exacerbations.
· In acute hypoxemic respiratory failure without hypercapnia, NIV can be used as long as patients are hemodynamically stable and are closely monitored in the intensive care unit to avoid dangerous delays if intubation becomes necessary.
· NIV has a central role in the management of acute respiratory failure of varied causes, improving patient outcome and efficiency of care in the acute setting.
References
1. Bunnel S. The use of nitrous oxide and oxygen to maintain anesthesia and positive pressure for thoracic surgery. JAMA. 1912;58:835.
2. Poulton EP, Oxon DM. Left-sided heart failure with pulmonary edema—its treatment with the “pulmonary plus pressure machine”. Lancet. 1936;231:981.
3. Barach AL, Martin J, Eckman M: Positive-pressure respiration and its application for the treatment of acute pulmonary edema and respiratory obstruction. Proc Am Soc Clin Invest. 1937;16:664.
4. Barach AL, Martin J, Eckman M. Positive-pressure respiration and its application to the treatment of acute pulmonary edema. Ann Intern Med. 1938;12:754.
5. Barach AL, Swenson P. Effect of breathing gases under positive pressure on lumens of small and medium sized bronchi. Arch Intern Med. 1939;63:946.
6. Motley HL, Lang LP, Gordon B. Use of intermittent positive pressure breathing combined with nebulization in pulmonary disease. Am J Med. 1948;5:853.
7. The Intermittent Positive Pressure Breathing Trial Group. Intermittent positive pressure breathing therapy of chronic obstructive pulmonary disease. Ann Intern Med. 1983;99:612.
8. Sullivan CE, Issa FG, Berthon-Jones M, et al. Reversal of obstructive sleep apnea by continuous positive airway pressure applied through the nares. Lancet. 1981;1:862.
9. Rideau Y, Gatin G, Bach J, et al. Prolongation of life in Duchenne's muscular dystrophy. Acta Neurol Belg. 1983;5:118.
10. Kerby GR, Mayer LS, Pingleton SK. Nocturnal positive pressure ventilation via nasal mask. Am Rev Respir Dis. 1987;135:738.
11. Ellis ER, Bye PT, Bruderer JW, et al. Treatment of respiratory failure during sleep in patients with neuromuscular disease: positive-pressure ventilation through a nose mask. Am Rev Respir Dis. 1987;135:148.
12. Bach JR, Alba AS. Management of chronic alveolar hypoventilation by nasal ventilation. Chest. 1990;97:52.
13. Meduri GU, Conoscenti CC, Menashe P, et al. Noninvasive face mask ventilation in patients with acute respiratory failure. Chest. 1989;95:865.
14. Brochard L, Isabey D, Piquet J, et al. Reversal of acute exacerbations of chronic obstructive lung disease by inspiratory assistance with a face mask. N Engl J Med. 1990;95:865.
15. Elliott MW, Steven MH, Phillips GD, et al. Noninvasive mechanical ventilation for acute respiratory failure. BMJ. 1990;300:358.
16. Zwillich CW, Pirson DJ, Creagh CE, et al. Complications of assisted ventilation. Am J Med. 1974;57:161.
17. Stauffer JL, Olson DE, Petty TL. Complications and consequences of endotracheal intubation. Am J Med. 1981;70:65.
18. Craven DE, Kunches LM, Kilinsky V, et al. Risk factors for pneumonia and fatality in patients receiving continuous mechanical ventilation. Am Rev Respir Dis. 1986;113:792.
19. Pingleton SK. Complications of acute respiratory failure. Am Rev Respir Dis. 1988;137:1463.
20. Antonelli M, Conti G, Rocco M, et al. A comparison of noninvasive positive-pressure ventilation and conventional mechanical ventilation in patients with acute respiratory failure. N Engl J Med. 1998;339:429.
21. Antonelli M, Conti C, Bufi M, et al. Noninvasive ventilation for treatment of acute respiratory failure in patients undergoing solid organ transplantation. JAMA. 2000;283:235.
22. Nourdine K, Combes P, Carton MJ, et al. Does noninvasive ventilation reduce the ICU nosocomial infection risk? A prospective clinical survey. Intensive Care Med. 1999;25:567.
23. Girou E, Schortgen F, Delclaux C, et al. Association of noninvasive ventilation with nosocomial infections and survival in critically ill patients. JAMA. 2000;284:2361.
24. Esteban A, Anzueto A, Frutos F, et al. Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day international study. JAMA. 2002;287:345.
25. Demoule A, Girou E, Richard JC, et al. Increased use of noninvasive ventilation in French intensive care units. Intensive Care Med. 2006;32:1747.
26. Carlucci A, Richard JC, Wysocki M, et al. Noninvasive versus conventional mechanical ventilation. An epidemiologic survey. Am J Respir Crit Care Med. 2001;163:874.
27. Antonelli M, Conti G. Noninvasive ventilation in intensive care unit patients. Curr Opin Crit Care. 2000;6:11.
28. Criner GJ, Travaline JM, Brennan KJ, et al. Efficacy of a new full face mask for noninvasive positive pressure. Chest. 1994;106:1109.
29. Antonelli M, Conti G, Pelosi P, et al. New treatment of acute hypoxemic respiratory failure: noninvasive pressure support ventilation delivered by helmet—a pilot controlled trial. Crit Care Med. 2002;30:602.
30. Antonelli M, Pennisi MA, Pelosi P, et al. Noninvasive positive pressure ventilation using a helmet in patients with acute exacerbation of chronic obstructive pulmonary disease: a feasibility study. Anesthesiology. 2004;100:16.
31. Piastra M, Antonelli M, Chiaretti M, et al. Treatment of acute respiratory failure by helmet-delivered non-invasive ventilation in children with acute leukemia: a pilot study. Intensive Care Med. 2004;30:472.
32. Bach JR, Alba AS, Saporito LR. Intermittent positive pressure ventilation via the mouth as an alternative to tracheostomy for 257 ventilator users. Chest. 1993;103:174.
33. Schettino GP, Tucci MR, Sousa R, et al. Mask mechanics and leak dynamics during noninvasive pressure support ventilation: a bench study. Intensive Care Med. 2001;27:1887.
34. Navalesi P, Fanfulla F, Frigeiro P, et al. Physiologic evaluation of noninvasive mechanical ventilation delivered with three types of masks in patients with chronic hypercapnic respiratory failure. Chest. 2000;28:1785.
35. Kwok H, McCormack J, Cece R, et al. Controlled trial of oronasal versus nasal mask ventilation in the treatment of acute respiratory failure. Crit Care Med. 2003;31:468.
36. Patroniti N, Foti G, Manfio A, et al. Head helmet versus face mask for non-invasive continuous positive airway pressure: a physiological study. Intensive Care Med. 2003;29:1680.
37. Costa R, Navalesi P, Antonelli M, et al. Physiologic evaluation of different levels of assistance during noninvasive ventilation delivered through a helmet. Chest. 2005;128:2984.
38. Chiumello D, Pelosi P, Carlesso E, et al. Noninvasive positive pressure ventilation delivered by helmet vs. standard face mask. Intensive Care Med. 2003;29:1671.
39. Racca F, Appendini L, Gregoretti C, et al. Effectiveness of mask and helmet interfaces to deliver noninvasive ventilation in a human model of resistive breathing. J Appl Physiol. 2005;99:1262.
40. Moerer O, Fisher S, Quintel M, et al. Influence of two different interfaces for noninvasive ventilation compared to invasive ventilation on the mechanical properties and performance of a respiratory system: a lung model study. Chest. 2006;129:1424.
41. Katz JA, Marks JD. Inspiratory work with and without continuous positive airway pressure in patients with acute respiratory failure. Anesthesiology. 1985;63:598.
42. Petrof BJ, Legere M, Goldberg P, et al. Continuous positive airway pressure reduced work of breathing and dyspnea during weaning from mechanical ventilation in severe chronic obstructive pulmonary disease. Am Rev Respir Dis. 1990;141:281.
43. Rasanen J, Heikkila J, Downs J, et al. Continuous positive airway pressure by face mask in acute cardiogenic pulmonary edema. Am J Cardiol. 1985;55:296.
44. Naughton MT, Rahman MA, Hara K, et al. Effect of continuous positive airway pressure on intrathoracic and left ventricular transmural pressures in patients with congestive heart failure. Circulation. 1995;91:1725.
45. Scharf SM, Caldini P, Ingram RH. Cardiovascular effects of increasing airway pressure in the dog. Am J Physiol. 1977;232:H35.
46. Braunwald E, Binion JT, WL Morgan, et al. Alterations in central blood volume and cardiac output induced by positive pressure breathing counteracted by metaraminol (Aramine). Circ Res. 1957;5:670.
47. Fessler H, Brower R, Wise R, et al. Effects of positive end-expiratory pressure on the gradient for venous return. Am Rev Respir Dis. 1991;143:19.
48. Nanas S, Magder S. Adaptation of the peripheral circulation to PEEP. Am Rev Respir Dis. 1992;146:688.
49. Jellinek H, Krenn H, Oczenski W, et al. Influence of positive airway pressure on the pressure gradient for venous return in humans. J Appl Physiol. 2000;88:926.
50. Gibney RT, Wilson RS, Pontoppidan H. Comparison of work of breathing on high gas flow and demand valve continuous positive airway pressure systems. Chest. 1982;82:692.
51. Beydon L, Chasse M, Harf A, et al. Inspiratory work of breathing during spontaneous ventilation using demand valves and continuous flow systems. Am Rev Respir Dis. 1988;138:300.
52. Sassoon CSH, Lodia R, Rheeman CH, et al. Inspiratory muscle work of breathing during flow-by, demand-flow and continuous-flow systems in patients with chronic obstructive pulmonary disease. Am Rev Respir Dis. 1992;145:1219.
53. Younes M, Puddy A, Roberts D, et al. Proportional assist ventilation: results of an initial clinical trial. Am Rev Respir Dis. 1992;145:121.
54. Bersten AD, Holt AW, Vedig AE, et al. Treatment of severe cardiogenic pulmonary edema with continuous positive airway pressure delivered by face mask. N Engl J Med. 1991;325:1825.
55. Mehta S, Jay GD, Woolard RH, et al. Randomized prospective trial of bilevel versus continuous positive airway pressure in acute pulmonary edema. Crit Care Med. 1997;25:620.
56. Bellone A, Monari A, Cortellaro F, et al. Myocardial infarction rate in acute pulmonary edema. Crit Care Med. 2004;32:1860.
57. Mehta S, McCool FD, Hill NS. Leak compensation in positive pressure ventilators: a lung model study. Eur Respir J. 2001;17:259.
58. Jubran A, Van de Graffe WB, Tobin MJ. Variability of patient–ventilator interaction with pressure support ventilation in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1995;152:129.
59. Calderini E, Confalonieri M, Puccio PG, et al. Patient–ventilator asynchrony during noninvasive ventilation: the role of expiratory trigger. Intensive Care Med. 1999;25:662.
60. Appendini L, Palessio A, Zanaboni S, et al. Physiologic effects of positive end-expiratory pressure and mask pressure support during exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1994;149:1069.
61. Vitacca M, Clini E, Pagani M, et al. Physiologic effects of early administered mask proportional assist ventilation in patients with chronic obstructive pulmonary disease and acute respiratory failure. Crit Care Med. 2000;28:1791.
62. Girault C, Richard JC, Chevron V, et al. Comparative physiologic effects of noninvasive assist-control and pressure support ventilation in acute hypercapnic respiratory failure. Chest. 1997;111:1639.
63. Vitacca M, Rubini F, Foglio K, et al. Non-invasive modalities of positive pressure ventilation improve the outcome of acute exacerbations in COLD patients. Intensive Care Med. 1993;19:450.
64. Antonelli M, Conti G, Esquinas A, et al. A multiple-center survey on the use in clinical practice of noninvasive ventilation as a first-line intervention for acute respiratory distress sindrome. Crit Care Med. 2007;35:18–25.
65. Aslanian P, El Atrous S, Isabey D, et al. Effects of flow triggering on breathing effort during partial ventilatory support. Am J Respir Crit Care Med. 1998 Jan;157(1):135.
66. Giuliani R, Mascia L, Recchia F, et al. Patient–ventilator interaction during synchronized intermittent mandatory ventilation. Effects of flow triggering. Am J Respir Crit Care Med. 1995;151:1.
67. Nava S, Ambrosino N, Bruschi C, et al. Physiological effects of flow and pressure triggering during non-invasive mechanical ventilation in patients with chronic obstructive pulmonary disease. Thorax. 1997;52:249.
68. Organized jointly by the American Thoracic Society, the European Respiratory Society, the European Society of Intensive Care Medicine, and the Societe de Reanimation de Langue Francaise, and approved by ATS Board of Directors, December 2000. International Consensus Conferences in Intensive Care Medicine: noninvasive positive pressure ventilation in acute respiratory failure. Am J Respir Crit Care Med. 2001;163:283.
69. Bach JR, Saporito LR. Criteria for extubation and tracheostomy tube removal for patients with ventilatory failure: a different approach to weaning. Chest. 1996;110:1566.
70. Bach JR, Mechanical insufflation-exsufflation: comparison of peak expiratory flows and manually assisted and unassisted coughing techniques. Chest. 1993;104:1553.
71. Diaz GG, Alcaraz AC, Talavera JC, et al. Noninvasive positive-pressure ventilation to treat hypercapnic coma secondary to respiratory failure. Chest. 2005;127:952.
72. Scala R, Naldi M, Archinucci I, et al. Noninvasive positive pressure ventilation in patients with acute exacerbations of COPD and varying levels of consciousness. Chest. 2005;128:1657.
73. Pankow W, Hijjeh N, Schuttler F, et al. Influence of noninvasive positive pressure ventilation on inspiratory muscle activity in obese subjects. Eur Respir J. 1997;10:2847.
74. Ambrosino N, Foglio K, Rubini F, et al. Non-invasive mechanical ventilation in acute respiratory failure due to chronic obstructive pulmonary disease: correlates for success. Thorax. 1995;50:755.
75. Brochard L, Mancebo J, Wysocki M, et al. Noninvasive ventilation for acute exacerbations of chronic obstructive pulmonary disease. N Engl J Med. 1995;333:817.
76. Soo Hoo GW, Santiago S, Williams J. Nasal mechanical ventilation for hypercapnic respiratory failure in chronic obstructive pulmonary disease: determinants of success and failure. Crit Care Med. 1994;27:417.
77. Bott J, Carroll MP, Conway JH, et al. Randomized controlled trial of nasal ventilation in acute ventilatory failure due to chronic obstructive airways disease. Lancet. 1993;341:1555.
78. Moretti M, Cilione C, Tampieri A, et al. Incidence and causes of non-invasive mechanical ventilation failure after initial success. Thorax. 2000;55:819.
79. Antonelli M, Conti G, Moro ML, et al. Predictors of failure of noninvasive positive pressure ventilation in patients with acute hypoxemic respiratory failure: a multi-center study. Intensive Care Med. 2001;27:1718.
80. Plant PK, Owen JL, Elliott MW. Early use of noninvasive ventilation for acute exacerbations of chronic obstructive pulmonary disease on general respiratory wards: a multicenter randomized controlled trial. Lancet. 2000;355:1931.
81. Kramer N, Meyer TJ, Meharg J, et al. Randomized, prospective trial of noninvasive positive pressure ventilation in acute respiratory failure. Am J Respir Crit Care Med. 1995;151:1799.
82. Celikel T, Sungur M, Ceyhan B, et al. Comparison of noninvasive positive pressure ventilation with standard medical therapy in hypercapnic acute respiratory failure. Chest. 1998;114:1636.
83. Mehta S, Hill NS. Noninvasive ventilation. Am J Respir Crit Care Med. 2001;163:540.
84. Barbé F, Togores B, Rubi M, et al. Noninvasive ventilatory support does not facilitate recovery from acute respiratory failure in chronic obstructive pulmonary disease. Eur Respir J. 1996;9:1240.
85. Angus RM, Ahmed AA, Fenwick LJ, et al. Comparison of the acute effects on gas exchange of nasal ventilation and doxapram in exacerbations of chronic obstructive pulmonary disease. Thorax. 1996;51:1048.
86. Confalonieri M, Potena A, Carbone G, et al. Acute respiratory failure in patients with severe community-acquired pneumonia. A prospective randomized evaluation of noninvasive ventilation. Am J Respir Crit Care Med. 1999;160:1585.
87. Martin TJ, Hovis JD, Constantino JP, et al. A randomized prospective evaluation of noninvasive ventilation for acute respiratory failure. Am J Respir Crit Care Med. 2000;161:807.
88. Nava S, Ambrosino N, Clini E, et al. Noninvasive mechanical ventilation in the weaning of patients with respiratory failure due to chronic obstructive pulmonary disease. A randomized, controlled trial. Ann Intern Med. 1998;128:721.
89. Thys F, Roeseler J, Reynaert M, et al. Noninvasive ventilation for acute respiratory failure: a prospective randomised placebo-controlled trial. Eur Respir J. 2002;20:545.
90. Dikensoy O, Ikidag B, Filiz A, et al. Comparison of non-invasive ventilation and standard medical therapy in acute hypercapnic respiratory failure: a randomised controlled study at a tertiary health centre in SE Turkey. Int J Clin Pract. 2002;56:85.
91. Conti G, Antonelli M, Navalesi P, et al. Noninvasive vs. conventional mechanical ventilation in patients with chronic obstructive pulmonary disease after failure of medical treatment in the ward: a randomized trial. Intensive Care Med. 2002;28:1701.
92. Squadrone E, Frigerio P, Fogliati C, et al. Noninvasive vs. invasive ventilation in COPD patients with severe acute respiratory failure deemed to require ventilatory assistance. Intensive Care Med. 2004;30:1303.
93. Meduri GU, Cook TR, Turner RE, et al. Noninvasive positive pressure ventilation in status asthmaticus. Chest. 1996;110:767.
94. Fernandez MM, Villagra A, Blanch L, et al. Non-invasive mechanical ventilation in status asthmaticus. Intensive Care Med. 2001;27:486.
95. Soroksky A, Stav D, Shpirer I. A pilot prospective, randomized, placebo-controlled trial of bilevel positive airway pressure in acute asthmatic attack. Chest. 2003;123:1018.
96. Holley MT, Morrissey TK, Seaberg DC, et al. Ethical dilemmas in a randomized trial of asthma treatment: can Bayesian statistical analysis explain the results? Acad Emerg Med. 2001;8:1128.
97. Levy BD, Kitch B, Fanta CH. Medical and ventilatory management of status asthmaticus. Intensive Care Med. 1998;24:105.
98. Girault C, Daudenthun I, Chevron V, et al. Noninvasive ventilation as a systematic extubation and weaning technique in acute-on-chronic respiratory failure: a prospective, randomized controlled study. Am J Respir Crit Care Med. 1999;160:86.
99. Pennock BE, Crawshaw L, Kaplan PD. Noninvasive nasal mask ventilation for acute respiratory failure. Chest. 1994;105:441.
100. Lapinsky SE, Mount DNB, Mackey D, et al. Management of acute respiratory failure due to pulmonary edema with nasal positive pressure support. Chest. 1994;105:229.
101. Wysocki M, Tric L, Wolff MA, et al. Noninvasive pressure support ventilation in patients with acute respiratory failure. Chest. 1993;103:907.
102. Meduri GU, Turner RE, Abou-Shala N, et al. Noninvasive positive pressure ventilation via face mask. Chest. 1996;109:179.
103. Conti G, Marino P, Cogliati A, et al. Noninvasive ventilation for the treatment of acute respiratory failure in patients with hematologic malignancies: a pilot study. Intensive Care Med. 1998;24:1283.
104. Wood KA, Lewis L, Von Harz B, et al. The use of noninvasive positive pressure ventilation in the emergency department. Chest. 1998;113:1339.
105. Rocker GM, Mackensie M-G, Willilams B, et al. Noninvasive positive pressure ventilation: successful outcome in patients with acute lung injury/ARDS. Chest. 1999;115:173.
106. Ferrer M, Esquinas A, Leon M, et al. Noninvasive ventilation in severe hypoxemic respiratory failure: a randomized clinical trial. Am J Respir Crit Care Med. 2003;168:1438.
107. L'Her E, Deye N, Lellouche F, et al. Physiologic effects of noninvasive ventilation during acute lung injury. Am J Respir Crit Care Med. 2005;172:1112.
108. Covelli HD, Weled BJ, Beekman JF. Efficacy of continuous positive airway pressure administered by face mask. Chest. 1982;81:147.
109. Masip J, Betbese AJ, Paez J, et al. Non-invasive pressure support ventilation versus conventional oxygen therapy in acute cardiogenic pulmonary edema: a randomized study. Lancet. 2000;356:2126.
110. Levitt MA. A prospective, randomized trial of BIPAP in severe acute congestive heart failure. J Emerg Med. 2001;21:363.
111. Kelly CA, Newby DE, McDonagh TA, et al. Randomised controlled trial of continuous positive airway pressure and standard oxygen therapy in acute pulmonary oedema. Eur Heart J. 2002;23:1379.
112. Nava S, Carbone G, Dibatista N, et al. Noninvasive ventilation in cardiogenic pulmonary edema. Am J Respir Crit Care Med. 2003;168:1432.
113. Cross AM, Cameron P, Kierce M, et al. Non-invasive ventilation in acute respiratory failure. Emerg Med J. 2003;20:531.
114. L'Her E, Duquesne F, Girou E, et al. Noninvasive continuous positive airway pressure in elderly cardiogenic pulmonary edema patients. Intensive Care Med. 2004;30:882.
115. Park M, Sangean MC, Volpe MC, et al. Randomized, prospective trial of oxygen, continuous positive airway pressure, and bilevel positive airway pressure by face mask in acute cardiogenic pulmonary edema. Crit Care Med. 2004;32:2407.
116. Crane SD, Elliott MW, Gilligan P, et al. Randomised controlled comparison of continuous positive airways pressure, bilevel non-invasive ventilation, and standard treatment in emergency department in patients with acute cardiogenic pulmonary oedema. Emerg Med J. 2004;21:155.
117. Bellone A, Vettorello M, Monari A, et al. Noninvasive pressure support ventilation vs. continuous positive airway pressure in acute hypercapnic pulmonary edema. Intensive Care Med. 2005;31:807.
118. Collins SP, Mielniczuk LM, Whittingham HA, et al The use of noninvasive ventilation in emergency department patients with acute cardiogenic pulmonary edema: a systematic review. Ann Emerg Med. 2006;48:260.
119. Wysocki M. Noninvasive ventilation in acute cardiogenic pulmonary edema: better than continuous positive airway pressure? Intensive Care Med. 1999;25:1.
120. Masip J, Roque M, Sanchez B, et al. Noninvasive ventilation in acute cardiogenic pulmonary edema: systematic review and meta-analysis. JAMA. 2005;294:3124.
121. Ho KM, Wong K. A comparison of continuous and bi-level positive airway pressure non-invasive ventilation in patients with acute cardiogenic pulmonary oedema: a meta-analysis. Crit Care. 2006;10:R49.
122. Jolliet P, Abajo B, Pasquina P, et al. Non-invasive pressure support ventilation in severe community-acquired pneumonia. Intensive Care Med. 2001;27:812.
123. Estopa R, Torres-Marti A, Kastanos N, et al. Acute respiratory failure in severe hematologic disorders. Crit Care Med. 1984;12:26.
124. Blot F, Guignet M, Nitenberg G, et al. Prognostic factors for neutropenic patients in an intensive care unit: respective roles of underlying malignancies and acute organ failures. Eur J Cancer. 1997;33:1031.
125. Ewig S, Torres A, Riquelme R, et al. Pulmonary complications in patients with haematological malignancies treated at a respiratory ICU. Eur Respir J. 1998;12:116.
126. Rocco M, Conti G, Antonelli M, et al. Non-invasive pressure support ventilation in patients with acute respiratory failure after bilateral lung transplantation. Intensive Care Med. 2001;27:1622.
127. Hilbert G, Gruson D, Vargas F, et al. Noninvasive ventilation in immunosuppressed patients with pulmonary infiltrates, fever, and acute respiratory failure. N Engl J Med. 2001;344:481.
128. Ferrer M, Esquinas A, Arancibia F, et al. Noninvasive ventilation during persistent weaning failure: a randomized controlled trial. Am J Respir Crit Care Med. 2003;168:70.
129. Epstein SK, Ciubotaru RL, Wong JB. Effect of failed extubation on the outcome of mechanical ventilation. Chest. 1997;112:186.
130. Keenan SP, Powers C, McCormack DG, et al. Noninvasive positive-pressure ventilation for postextubation respiratory distress: a randomized controlled trial. JAMA. 2002;287:3238.
131. Esteban A, Frutos-Vivar F, Ferguson ND, et al. Noninvasive positive-pressure ventilation for respiratory failure after extubation. N Engl J Med. 2004;350:2452.
132. Epstein SK, Ciubotaru RL. Independent effects of etiology of failure and time to reintubation on outcome for patients failing extubation. Am J Respir Crit Care Med. 1998;158:489.
133. Ferrer M, Valencia M, Nicolas JM, et al. Early noninvasive ventilation averts extubation failure in patients at risk: a randomized trial. Am J Respir Crit Care Med. 2006;173:164.
134. Benhamou D, Girault C, Faure C, et al. Nasal mask ventilation in acute respiratory failure. Experience in elderly patients. Chest. 1992;102:912.
135. Meduri GU, Fox RC, Abou-Shala N, et al. Noninvasive mechanical ventilation via face mask in patients with acute respiratory failure who refused endotracheal intubation. Crit Care Med. 1994;22:1584.
136. Levy M, Tanios MA, Nelson D, et al. Outcomes of patients with do-not-intubate orders treated with noninvasive ventilation. Crit Care Med. 2004;32:2002.
137. Chu CM, Chan VL, Wong IW, et al. Noninvasive ventilation in patients with acute hypercapnic exacerbation of chronic obstructive pulmonary disease who refused endotracheal intubation. Crit Care Med. 2004;32:372.
138. Clarke DE, Vaughan L, Raffin TA. Noninvasive positive pressure ventilation for patients with terminal respiratory failure: the ethical and economic costs of delaying the inevitable are too great. Am J Crit Care. 1994;3:4.
139. Craig DB. Postoperative recovery of pulmonary function. Anesth Analg. 1981;60:46.
140. Linder KH, Lotz P, Ahnefeld FW. Continuous positive airway pressure effect on functional residual capacity, vital capacity and its subdivisions. Chest. 1987;92:66.
141. Boothby WM, Mayo Cw, Lovelace WR, II. The use of oxygen and oxygen-helium, with special reference to surgery. Surg Clin North Am. 1940;20:1107.
142. Joris JL, Sottiaux TM, Chiche JD, et al. Effect of bi-level positive airway pressure (BiPAP) nasal ventilation on the postoperative pulmonary restrictive syndrome in obese patients undergoing gastroplasty. Chest. 1997;111:665.
143. Squadrone V, Coha M, Cerutti E, et al. Continuous positive airway pressure for treatment of postoperative hypoxemia: a randomized controlled trial. JAMA. 2005;293:589.
144. Jaber S, Chanques G, Sebbane M et al. Non-invasive positive pressure ventilation in patients with respiratory failure due to severe acute pancreatitis. Respiration. 2006;73:166.
145. Pinilla J, Oleniuk FH, Tan L, et al. Use of a nasal continuous positive airway pressure mask in the treatment of postoperative atelectasis in aortocoronary bypass surgery. Crit Care Med. 1990;18:836.
146. Pennock BE, Kaplan PD, Carlin BW, et al. Pressure support ventilation with a simplified ventilatory support system administered with a nasal mask in patients with respiratory failure. Chest. 1991;100:1371.
147. Matte P, Jacquet L, Van Dyck M, et al. Effects of conventional physiotherapy, continuous positive airway pressure and non-invasive ventilatory support with bilevel positive airway pressure after coronary artery bypass grafting. Acta Anaesthesiol Scand. 2000;44:75.
148. Aguilo R, Togores B, Pons S, et al. Noninvasive ventilatory support after lung resectional surgery. Chest. 1997;112:117.
149. Auriant I, Jallot A, Hervè O, et al. Non-invasive ventilation reduces mortality in acute respiratory failure following lung resection. Am J Respir Crit Care Med. 2001;164:1231.
150. Jenkinson C, Davies RJ, Mullins R, et al. Comparison of therapeutic and subtherapeutic nasal continuous positive airway pressure for obstructive sleep apnoea: a randomised prospective parallel trial. Lancet. 1999;353:2100.
151. Loredo JS, Ancoli-Israel S, Kim EJ, et al. Effect of continuous positive airway pressure versus supplemental oxygen on sleep quality in obstructive sleep apnea: a placebo-CPAP-controlled study. Sleep. 2006;29:564.
152. Abbey NC, Block AJ, Green D, et al. Measurement of pharyngeal volume by digitized magnetic resonance imaging. Effect of nasal continuous positive airway pressure. Am Rev Respir Dis. 1989;140:717.
153. Schwab RJ, Pack AI, Gupta KB, et al. Upper airway and soft tissue structural changes induced by CPAP in normal subjects. Am J Respir Crit Care Med. 1996;154:1106.
154. Sturani C, Galavotti V, Scarduelli C, et al. Acute respiratory failure, due to severe obstructive sleep apnoea syndrome, managed with nasal positive pressure ventilation. Monaldi Arch Chest Dis. 1994;49:558.
155. Hurst JM, DeHaven CB, Branson RD. Use of CPAP mask as the sole mode of ventilatory support in trauma patients with mild to moderate respiratory insufficiency. J Trauma. 1985;25:1065.
156. Beltrame F, Lucangelo U, Gregori D, et al. Noninvasive positive pressure ventilation in trauma patients with acute respiratory failure. Monaldi Arch Chest Dis. 1999;54:109.
157. Xirouchaki N, Kondoudaki E, Anastasaki M, et al. Noninvasive bilevel positive pressure ventilation in patients with blunt thoracic trauma. Respiration. 2005;72:517.
158. Bach JR, Ishikawa Y, Kim H. Prevention of pulmonary morbidity for patients with Duchenne muscular dystrophy. Chest. 1997;112:1024.
159. Rabinstein A, Wijdicks EF. BiPAP in acute respiratory failure due to myasthenic crisis may prevent intubation. Neurology. 2002;59:1647.
160. Fumeaux T, Rothmeier C, Jolliet P. Outcome of mechanical ventilation for acute respiratory failure in patients with pulmonary fibrosis. Intensive Care Med. 2001;27:1868.
161. Antonelli M, Conti G, Riccioni L, et al. Noninvasive positive-pressure ventilation via face mask during bronchoscopy with BAL in high-risk hypoxemic patients. Chest. 1996;110:724.
162. Antonelli M, Conti G, Rocco M, et al. Noninvasive positive-pressure ventilation vs. conventional oxygen supplementation in hypoxemic patients undergoing diagnostic bronchoscopy. Chest. 2002;121:1149.
163. Antonelli M, Pennisi MA, Conti G, et al. Fiberoptic bronchoscopy during noninvasive positive pressure ventilation delivered by helmet. Intensive Care Med. 2003;29:126.
164. Hill NS. Complications of noninvasive positive pressure ventilation. Respir Care. 1997;42:432.
165. Constantin JM, Schneider E, Cayot-Constantin S, et al. Remifentanil-based sedation to treat noninvasive ventilation failure: a preliminary study. Intensive Care Med. 2006;33(1):82–87.