Hao Chih Ho
Mihae Yu
Immediate Concerns
Many critically ill patients require ventilator support for extended periods of time. Maintaining a safe and secure airway for these patients can be challenging, and the choice between continued translaryngeal intubation and tracheostomy is not always easy. Initially, most patients will have an endotracheal tube (ETT) in place. The main consideration for placement of a tracheostomy is the anticipated duration of ventilator support, need for airway access (suctioning), and patient comfort. Predicting the duration of ventilator support is difficult, and the optimal timing of tracheostomy in critically ill patients with acute respiratory failure is controversial. Tracheostomy should be an elective procedure and should not be performed on patients receiving high pressure ventilator support, except on rare occasions when there are mechanical problems with the ETT. With high-volume, low-pressure endotracheal tube cuffs, there is no time interval when conversion to a tracheostomy is mandatory because of potential damage to the trachea from pressure necrosis. The decision to perform a tracheostomy should not be based solely on the duration of endotracheal intubation, especially in patients requiring high pressure ventilator support where the risk of transport to the operating room or loss of airway pressure during percutaneous tracheostomy may cause significant morbidity.
Overview
Tracheostomy is one of the most commonly performed surgical procedures in critically ill patients (1). The modern surgical tracheostomy was first described in 1909 by Chevalier Jackson (2). Ciaglia et al. (3) first described the technique of percutaneous dilational tracheostomy (PDT) in 1985. Bedside PDT is now widely accepted in critical care units.
Indications and Timing
The primary indication for tracheostomy is the requirement for prolonged ventilator support and/or failure to wean from mechanical ventilation for 2 to 3 weeks (4). In 1989, the ACCP Consensus Conference on Artificial Airways in Patients Receiving Mechanical Ventilation recommended tracheostomy for patients whose anticipated need for artificial airway is greater than 21 days (5). Other indications are severe head injury with inability to protect the airway, high spinal cord injuries, laryngeal trauma, upper airway obstruction, and management of pulmonary secretions. The benefits of tracheostomy include sparing the larynx from further direct injury from the translaryngeal tube, improved comfort (6), ability to speak and eat, improved oral care, and possibly earlier transfer from the intensive care unit (ICU) (5). In patients with limited reserve, tracheostomy reduces the work of breathing (shorter length of tubing than the endotracheal tube) and may allow more flexibility in weaning (7,8).
There continues to be debate over the actual impact of tracheostomy on outcome. In two recent studies of patients requiring prolonged mechanical ventilation, Combes et al. (9) found that tracheostomy was associated with lower ICU and in-hospital mortality rates, whereas Clec'h et al. (10) found no reduction in mortality but increased post-ICU mortality if the tracheostomy was left in place.
Another controversial topic is the optimal timing of converting a translaryngeal intubation to a tracheostomy because there is no accurate way to predict the need for prolonged mechanical ventilation in the first few days. A high acuity of illness (Acute Physiology and Chronic Health Evaluation [APACHE] II scores greater than 25) and the presence of shock at the time of ICU admission are two of the best predictors (11,12,13). Pena et al. (14) reviewed 56 cases of subglottic stenosis and found that 86% had a history of tracheal intubation, with a mean duration of 17 days. The ACCP Consensus Conference recommends translaryngeal intubation for an anticipated need of the artificial airway up to ten days and tracheotomy for an anticipated need of the artificial airway for greater than 21 days. The ACCP Consensus Conference also recommends that the decision for tracheostomy be made as early as possible to minimize the duration of translaryngeal intubation (5).
Several studies have provided additional support for early tracheostomy. Rumbak et al. (15) randomized 128 medical patients to either early (within 48 hours) or late (14–16 days) percutaneous tracheostomy and found significantly shorter ICU stays, fewer days on the ventilator, and a lower mortality in the early tracheostomy group. A prospective review of trauma patients by Arabi et al. (16) also found that patients who received early tracheostomy (by day 7 of mechanical ventilation) had shorter ICU stays and fewer days on the ventilator. In a meta-analysis, Griffiths et al. (17) reviewed five clinical trails with a total of 406 patients that compared early (within 7 days) versus late tracheostomy in critically ill adult patients. Mortality and the risk of pneumonia were the same in the two groups, but early tracheostomy significantly reduced the duration of artificial ventilation and length of stay in the ICU.
Patient Selection
All patients requiring prolonged mechanical ventilation are candidates for tracheostomy. The main contraindications of tracheostomy are hemodynamic instability, uncorrected coagulopathy, active infection over the tracheostomy site, and emergency airway access. Other mitigating circumstances may include risk of infection to adjacent surgical wounds and central line sites (neck and upper chest incisions), and a high fraction of inspired oxygen (FiO2) and/or positive end-expiratory pressure (PEEP) requirement.
Open Versus Percutaneous Tracheostomy
Surgical tracheostomy (ST) is usually performed in the operating room (OR). It can be performed in the ICU, but is not optimal in that setting because of inadequate lighting, suction, and cautery, as well as difficulty in maintaining a sterile field. PDT is usually performed in the ICU, eliminating the need to transport the patient to and from the operating room (OR), as well as the cost of the OR and possibly the cost of anesthesia. In a recent meta-analysis, Delaney et al. identified randomized clinical trials that compared PDT to ST. Seventeen studies involving 1,212 patients were reviewed, and the authors concluded that PDT reduced the incidence of wound infection and may further reduce clinically relevant bleeding and mortality when compared with ST performed in the OR (18). The choice between ST and PDT depends on the operator experience and individual patient issues.
Patient issues favoring surgical tracheostomy include:
1. Coagulation abnormalities—Larger blood vessels are more easily controlled under direct vision during ST, but the smaller wound opening and snug fit of the tracheostomy placed by PDT may help tamponade clinically relevant bleeding from small vessels at the wound edges.
2. High level of oxygenation support with a high FiO2 and/or high PEEP—During PDT, the endotracheal tube is withdrawn until the tip is in the larynx. This often results in a substantial gas leak and possibly hypoxia in these patients. In ST, the endotracheal tube is only withdrawn when the tracheostomy tube is ready to be inserted, minimizing the gas leak and loss of PEEP.
3. Unstable cervical spine—Dilation and tracheostomy tube insertion during PDT requires a significant exertion of force that may result in excessive cervical spine motion which may be avoided with ST.
4. Unusual neck anatomy such as masses, previous surgery, or poor mobility—In these cases, it is safer to perform ST because of the direct visualization of the neck structures.
Techniques
Surgical Tracheostomy
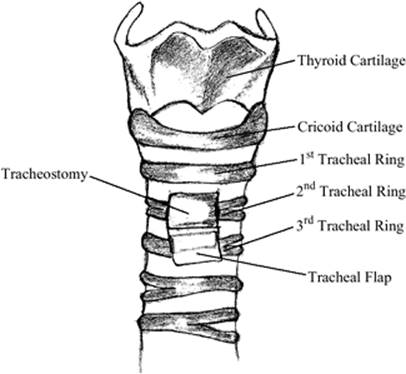
ST can be performed in either the OR or the ICU. The patient usually has an endotracheal tube in place. A shoulder roll is placed to elevate the shoulders and extend the head, which elevates the larynx and exposes more of the upper trachea. The skin from the chin to below the clavicles is prepped. Sterile drapes are used to create an opening from the top of the larynx to the suprasternal notch. The thyroid notch and cricoid cartilage are identified by palpation (Fig. 135.1).
|
|
|
Figure 135.1. Tracheal anatomy and placement of incision. |
Local anesthetic with a vasoconstrictor, such as epinephrine, is then injected into the skin and subcutaneous tissue overlying the second tracheal ring. A 2-cm midline vertical or horizontal incision is then made. The vertical incision extends from the inferior edge of the cricoid cartilage toward the suprasternal notch whereas the horizontal incision is made over the second tracheal ring. Dissection is carried sharply through the platysma muscle. Bleeding is controlled with cautery and/or hemostats and ties. Careful blunt dissection is then used to expose the thyroid isthmus, which is done by palpating the anatomy and using a curved hemostat to gently spread the submuscular tissues parallel to the long axis of the trachea. If the thyroid isthmus overlies the second and third tracheal rings, it may need to be partially or completely transected to expose the trachea.
Once the trachea is dissected free of the overlying tissues, the second ring is identified. An incision is made in the trachea between the first and second ring and extended laterally through the second ring (Fig. 135.1). This results in a tracheal flap (Fig. 135.2) that can be sutured to the inferior edge of the skin incision, creating a stoma. The endotracheal tube is withdrawn, and the tracheostomy tube is inserted into the trachea under direct vision. The creation of a stoma may facilitate reinsertion of the dislodged tube in the first few days when the fistula tract may not have stabilized. Another technique is to make a criss-cross incision on the trachea and simply insert the tracheostomy under direct vision after lifting the edges with a tracheal hook. Suturing the tracheostomy tube in place may help decrease the risk of accidental decannulation.
|
|
|
Figure 135.2. Tracheal flap created in open tracheostomy. |
Percutaneous Dilational Tracheostomy
The most common technique for performing PDT is that of Ciaglia. Originally, the technique used sequential dilators (3), but it has since been simplified to using a single tapered dilator. This dilator has a hydrophilic coating that is activated by immersing it in sterile water or saline. This procedure can be performed blindly, although many clinicians use fiberoptic bronchoscopy to observe the placement, as well as to prevent inadvertent injury to the posterior wall of the trachea and/or misplacement of the tracheostomy (19,20).
The patient is positioned, and the neck is prepped and draped as described for the surgical technique. The neck is palpated to identify the thyroid notch and cricoid cartilage. Local anesthetic with a vasoconstrictor is then injected into the skin and subcutaneous tissue inferior to the cricoid cartilage, followed by a 1.5-cm incision made either horizontally or downward from the inferior edge of the cricoid cartilage. A curved hemostat is then used to dissect gently down to the anterior trachea. A fingertip is used to palpate the cricoid cartilage through the incision and to bluntly dissect any tissue overlying the trachea. The endotracheal tube is withdrawn until the upper tracheal rings are visualized with a bronchoscope. Additional local anesthetic is then injected into the tracheal wall. The trachea air column is located by directing the needle posterior and caudally in the midline. Entry into the trachea is visualized with the bronchoscope, and 1 mL of local anesthetic is injected into the lumen of the trachea. Thereafter, the partially filled local anesthetic syringe is attached to the sheathed introducer needle. Once again, the tracheal air column is found and verified with the bronchoscope. The goal is to place the needle between the first and second or the second and third tracheal rings (Fig. 135.1). Once free flow of air is obtained, the outer sheath is advanced slightly, and the inner needle is removed. The J-wire is then advanced through the sheath into the trachea, and the sheath is removed. The 14 French introducing dilator is advanced over the guidewire and is used to dilate the access site. Following the initial dilation, the large tapered dilator is used to dilate the track. Finally, the tracheostomy tube with a guide (the largest one that will fit inside the tracheostomy tube) is threaded over the sheath and guidewire, and then into the trachea. The dilation and tracheostomy tube insertion requires significant force, and visualization of the process with the bronchoscope is invaluable in minimizing the risk of an unidentified injury to the posterior wall of the trachea. After placement of the tracheostomy tube, the ETT is removed, and the bronchoscope is inserted into the fresh tracheostomy to confirm placement and remove blood and secretions. Fresh blood clots can cause acute airway obstruction; the bronchoscope allows direct visualization and removal of the clot.
Complications
The important complications of tracheostomy include infection, bleeding, inadvertent extubation, paratracheal placement, esophageal perforation, subcutaneous emphysema, pneumothorax, tracheal stenosis, tracheoinnominate fistula, tracheoesophageal fistula, tracheocutaneous fistula after decannulation, cardiopulmonary arrest, and death. In a meta-analysis of 1,212 patients, the most common clinically relevant complications noted were wound infections (6.6%) and bleeding (5.7%) (18). Inadvertent postoperative decannulation with inability to recannulate the trachea due to the absence of a formed tract may occur. Immediate endotracheal intubation is mandatory rather than attempting to push the tracheostomy tube back into a semioccluded orifice.
A specific complication of surgical tracheostomy is the risk of airway fire. This can occur when a spark from the electrocautery ignites the oxygen leaking from the opened trachea. This can be prevented by meticulous hemostasis during the pretracheal dissection, and avoiding the use of electrocautery to make the trachea incision and after the trachea is opened. Complications specific to PDT include extraluminal placement of the tracheostomy tube. Perforation of the esophagus or the pharynx has been described when a bronchoscope was not used. Cannulation of the mediastinum may result in catastrophe since the patient cannot be oxygenated or ventilated with acute asphyxiation. There is a learning curve using PDT, and it has been reported that complications are higher in the earlier cases of the operator (21). Using bronchoscopy to guide PDT should prevent extraluminal placement, and suturing the tracheostomy tube in place may decrease the risk of inadvertent decannulation of a freshly placed tube (21).
Obesity is associated with higher rates of complications in PDT, including posterior tracheal wall injury, malpositioning, and accidental decannulation (21,22); however, this technique may be safely used in experienced hands (23). The use of bronchoscopy and an extra-long tracheostomy may help minimize the incidence of these complications (21,24).
Summary
Many tracheostomy procedures are performed in critically ill patients in the ICU. A high severity of injury and shock on admission are predictors of prolonged mechanical ventilation. If these patients do not show evidence of improvement in the first few days, the option of tracheostomy should be considered and discussed with the patient and/or medical decision makers. The choice between ST and PDT depends on local operator expertise and patient-specific issues. Bedside PDT is performed as safely as ST in the OR and may be associated with more efficient use of health care resources.
Pearls
· There may be brisk bleeding from the skin edges or anterior jugular veins. Have sutures ready to ligate or oversew these sites.
· Make sure the bronchoscope and ET tube are withdrawn adequately to avoid impaling them with the needle. Place the end of the bronchoscope so that it remains in the ET tube, but leave the tip of the ET tube just visible. Withdraw the bronchoscope and ET tube as a unit until the upper tracheal rings are visualized. When they are withdrawn adequately, the light from the bronchoscope can be visualized through the neck incision, and pressure on the anterior trachea with a finger or hemostat at the anticipated tracheostomy site will result in an indentation that can be seen with the bronchoscope.
· Although seemingly easy, finding the airway with the needle is the most important and most difficult part of the procedure. Stabilize the trachea with the nondominant hand, and insert the needle perpendicular to the airway while carefully aspirating for air.
· Placing a finger on the tracheal opening between dilatation and tracheostomy tube insertion will minimize the gas leak and loss of PEEP.
· The track may require dilation with the curved hemostat to facilitate the insertion of the tracheostomy tube. A single-cannula tracheostomy tube has a smaller outer diameter and is easier to insert; the disadvantage is the lack of an inner cannula that can be removed and cleaned.
· For large necks, a longer tracheostomy tube—such as the Shiley XLT—may be necessary. Make sure the appropriate supplies are available before the procedure.
· Insert the bronchoscope into the newly placed tracheostomy tube to ensure placement and evacuate any blood from the procedure.
· Losing an airway can be life threatening. Any procedure of the airway should include personnel who are skilled at intubating and managing the airway emergently.
· Get a chest radiograph to make sure there is no pneumothorax and to document the tracheostomy tube placement.
References
1. Durbin GC Jr. Questions answered about tracheostomy timing? Crit Care Med. 1999;27:2024.
2. Jackson C. Tracheostomy. Laryngoscope. 1909;19:285.
3. Ciaglia P, Firsching R, Syniec C. Elective percutaneous dilational tracheostomy: a new simple bedside procedure; preliminary report. Chest. 1985;87:715.
4. Heffner JE. The role of tracheotomy in weaning. Chest. 2001;120(Suppl 6):477.
5. Plummer AL, Gracey DR. Consensus conference on artificial airways in patients requiring mechanical ventilation. Chest. 1989;96:178.
6. Nieszkowska A, Combes A, Luyt CE, et al. Impact of tracheotomy on sedative administration, sedation level, and comfort of mechanically ventilated intensive care unit patients. Crit Care Med. 2005;33:2527–2533.
7. Davis K Jr, Campbell RS, Johannigman JA, et al. Changes in respiratory mechanics after tracheostomy. Arch Surg. 1999;134:59.
8. Diehl JL, El Atrous S, Touchard D, et al. Changes in the work of breathing induced by tracheotomy in ventilator dependent patients. Am J Respir Crit Care Med. 1999;159:383.
9. Combes A, Luyt C, Nieszkowska A, et al. Is tracheostomy associated with better outcomes for patients requiring long-term mechanical ventilation? Crit Care Med. 2007;35:802–807.
10. Clec'h C, Alberti C, Vincent F, et al. Tracheostomy does not improve the outcome of patients requiring prolonged mechanical ventilation: a propensity analysis. Crit Care Med. 2007;35:132–138.
11. Heffner JE, Zamora CA. Clinical predictors of prolonged translaryngeal intubation in patients with the adult respiratory distress syndrome. Chest. 1990;97:447.
12. Estenssoro E, Gonzalez F, Laffaire E, et al. Shock on admission day is the best predictor of prolonged mechanical ventilation in the ICU. Chest. 2005;127:598.
13. Afessa B, Hogans L, Murphy R. Predicting 3-day and 7-day outcomes of weaning from mechanical ventilation. Chest. 1999;116:456.
14. Pena J, Cicero R, Marin J, et al. Laryngotracheal reconstruction in subglottic stenosis: an ancient problem still present. Otolaryngol Head Neck Surg. 2001;125:397.
15. Rumbak MJ, Newton M, Truncale T, et al. A prospective, randomized, study comparing early percutaneous dilational tracheotomy to prolonged translaryngeal intubation (delayed tracheotomy) in critically ill medical patients. Crit Care Med. 2004;32:1689.
16. Arabi Y, Haddad S, Shirawa N, et al. Early tracheostomy in intensive care trauma patients improves resource utilization: a cohort study and literature review. Crit Care. 2004;8:R347.
17. Griffiths J, Barber VS, Morgan L. Systematic review and meta-analysis of studies of the timing of tracheostomy in adult patients undergoing artificial ventilation. BMJ. 2005;330:1243.
18. Delaney A, Bagshaw SM, Nalos M. Percutaneous dilational tracheostomy versus surgical tracheostomy in critically ill patients: a systematic review and meta-analysis. Crit Care. 2006;10:R55.
19. Oberwalder M, Weis H, Nehoda H, et al. Videobronchoscopic guidance makes percutaneous dilational tracheostomy safer. Surg Endosc. 2004;18:839.
20. Fernandez L, Norwood S, Roettger R, et al. Bedside percutaneous tracheostomy with bronchoscopic guidance in critically ill patients. Arch Surg. 1996;131:129.
21. Kost K. Endoscopic percutaneous dilatational tracheotomy: a prospective evaluation of 500 consecutive cases. Laryngoscope. 2005;115(10 Pt 2):1–30.
22. Byhahn C, Lischke V, Meininger D, et al. Peri-operative complications during percutaneous tracheostomy in obese patients. Anaesthesia. 2005;60:12–15.
23. Heyrosa M, Melniczek D, Rovito P, et al. Percutaneous tracheostomy: a safe procedure in the morbidly obese. J Am Coll Surg. 2006;202:618–622.
24. Blankenship D, Kulbersh B, Gourin C, et al. High-risk tracheostomy: exploring the limits of the percutaneous tracheostomy. Laryngoscope. 2005;115:987–989.