Kenneth E. Wood
Aaron Joffe
Despite significant advances in prophylaxis, diagnostic approaches, and therapeutic modalities for pulmonary embolism (PE), this disease process still remains an underrecognized and lethal entity. Contemporary estimates suggest that PE affects more than 600,000 patients per year in the United States and reportedly causes or contributes to 50,000 to 200,000 deaths. The incidence of PE causing, contributing to, or accompanying death in hospitalized patients has remained relatively constant at 15% for the past 40 years. Disconcertingly, the antemortem diagnosis of fatal PE has remained fixed at approximately 30% over the same time period. Large contemporary observational studies of PE have reported unexpectedly high mortality rates. In the Management Strategies and Determinants of Outcome in Acute Major PE (MAPPET) series, the overall 3-month mortality in patients with PE was 17% with an in-hospital mortality of 31% when PE was associated with hemodynamic instability. PE-attributable mortality was 45% and 91% in the respective groups (1). In the International Cooperative Pulmonary Embolism Registry (ICOPER), the 90-day mortality was 14.5% in hemodynamically stable PE patients and 51.9% in those with hemodynamic instability. PE-attributable mortality was 34% and 62.5% in the respective groups (2).
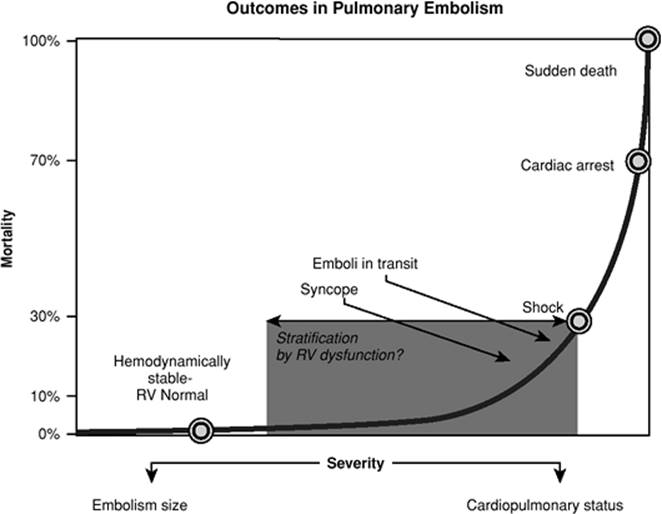
In fatal cases of PE, it has long been appreciated that two thirds of PE deaths will occur within 1 hour of presentation and that anatomically massive PE will account for only one half of the deaths as the remainder can be attributed to smaller submassive or recurrent emboli. There are several important implications of these observations. First, an evidenced-based approach is nearly impossible to define for hemodynamically unstable PE. Second, it is reasonable to propose that outcome from PE is related to the size of the embolism and the underlying cardiopulmonary function. There is a dynamic interaction between the patient's underlying cardiopulmonary status and the embolism size; similar hemodynamic and clinical outcomes will manifest from an anatomically massive PE in a patient with normal cardiopulmonary function and an anatomically submassive embolism in a patient with impaired cardiopulmonary function. Third, an implicit understanding of the physiology of PE will allow for the application of physiologic risk stratification that can be used for diagnostic evaluation and therapeutics. Figure 142.1 represents a proposed risk stratification model defined by the relationship between mortality and severity characterized by the integration of cardiopulmonary status and embolism size. The combination of embolism size and underlying cardiopulmonary status that produces cardiac arrest is associated with a predicted mortality of 70%; this implies that 30% of arrested PE patients will survive and warrants continued use of chest compressions to mechanically fracture the embolism and consideration toward thrombolysis or embolectomy even without a definitive diagnosis when PE is highly suspected. At the opposite extreme, the combination of embolism size and cardiopulmonary status that fails to produce right ventricular (RV) dilatation is associated with a 0% to 1% mortality provided therapeutic anticoagulation is achieved. The combination of embolism size and cardiopulmonary status that produces hemodynamic instability or shock is associated with a 30% mortality rate. Consequently, the presence of shock has traditionally defined the threshold for thrombolysis. As depicted in Figure 142.1, there is likely a broad spectrum of PE patients that are hemodynamically stable with RV dysfunction ranging from those with a minimal embolic burden and a low predicted mortality to patients with incipient shock and a predicted mortality just under 30%. The use of thrombolytics in this heterogeneous group is controversial as the constitutive characteristics of the mortality inflection point remain elusive. Syncope represents an intermediary position between shock and cardiac arrest as failure to recover consciousness results in cardiac arrest, and patients who regain consciousness have a high incidence of hemodynamic instability. The outcomes and mortality associated with emboli in transit and PE patients with a patent foramen ovale (PFO) have not been well reported and likely have severity as depicted in Figure 142.1.
The spectrum of PE most likely to confront the intensivist is predominantly confined to two situations; first, the patient presenting with undifferentiated shock or respiratory failure, and second, an established hospital or ICU patient who develops PE after admission. In either situation, the diagnostics and therapeutics are challenging. Differentiating PE from other life-threatening cardiopulmonary disorders can be exceedingly difficult; logistic constraints can jeopardize definitive diagnostic testing, and hemorrhagic risks in the critically ill can significantly alter the therapeutic approach and compromise the ability to anticoagulate or institute thrombolytic therapy. This chapter will review a structured physiologic approach to diagnostic, resuscitative, and management strategies as well as discuss prophylaxis and ICU-specific PE issues.
Prevention of Venous Thromboembolism
Principles of Prophylaxis
Prophylaxis is defined as any measure “designed to preserve health and prevent the spread of disease.” Insofar as venous thromboembolic disease (VTE) (3) is prevalent among acutely ill hospitalized patients and unprevented VTE may lead to adverse consequences, the use of pharmacologic, mechanical, or vena caval interruption as a means for reducing the occurrence of VTE certainly qualifies as a measure intended to preserve health. In fact, based on strength of evidence, the Agency for Healthcare Research and Quality (AHRQ) has identified “appropriate use of prophylaxis to prevent venous thromboembolism in patients at risk” as the number one opportunity for improvement of patient safety, supporting more widespread implementation (1). The choice of primary prophylaxis is based on the patient's risk of bleeding and thrombosis and is presented in Table 142.1.
|
|
|
Figure 142.1. Outcomes in pulmonary embolism. RV, right ventricle. |
Risk Factors
The Virchow triad of stasis, vessel trauma, and hypercoagulability remain fundamental risk factors for VTE. Furthermore, risk factors can be considered clinical (i.e., multiple trauma or major abdominal surgery, acute myocardial infarction or stroke, need for mechanical ventilation) or patient-related (prior history of VTE, malignancy, inherited coagulopathy).
|
Table 142.1 Venous Thromboembolism Prophylaxis of Critical Care Patient |
||||||||||||||||||
|
||||||||||||||||||
With respect to lower extremity deep venous thrombosis (DVT), observational studies of medical-surgical ICU patients have identified mechanical ventilation, treatment with neuromuscular blockers, and presence of a central venous catheter (CVC) as risk factors for DVT (4). Central venous catheterization, in particular, has been reported to confer an increased relative risk (RR) of 1.04 for each day the catheter was in place (5). Among 261 medical-surgical ICU patients, multivariate regression analysis defined exposure to platelet transfusions and the use of vasopressors to be independent risk factors for ICU-acquired DVT (6).
The two most powerful patient-related risk factors are a prior history of VTE and malignancy. Malignancy is perhaps the most common acquired hypercoagulable state encountered in the ICU and likely will become more prevalent as the general population continues to age. Additionally, end-stage renal disease has been identified as an independent risk factor for ICU-acquired DVT (6). Activated protein C resistance from factor V Leyden (FVL) is the most common hereditary defect predisposition for DVT. In order of descending prevalence among the general population, prothrombin gene mutation 20210A, antithrombin, protein C and S deficiency, elevations in homocysteine, and coagulation factors VIII, IX, and XI may predispose the patient to developing DVT (4). Although uncommon, heparin-induced thrombocytopenia (HIT), an acquired platelet disorder, results in increased risk of both venous and arterial thrombosis (7).
Cancer and the presence of a CVC are the two most powerful risk factors for upper extremity DVT (UEDVT). In the report of Mustafa et al., a CVC at the site of the upper extremity DVT was present in 60% of patients and 46% were diagnosed with cancer. Underscoring the possible additive nature of these two risk factors, 76% of the patients with cancer also had an indwelling CVC (8). In a review of cancer patients who had an indwelling CVC, the reported prevalence of upper extremity DVT, either symptomatic or asymptomatic, ranged from 6.7 to 48% (9). In a prospective registry of 592 patients with upper extremity DVT, the presence of an indwelling CVC was the strongest independent predictor of occurrence (odds ratio, 7.3) (10). It is important to note that nearly 30% of patients will develop an UEDVT with no apparent cause. In these patients, inherited thrombophilia, particularly FVL, prothrombin G20210A mutation, and anticoagulant protein deficiencies may be causative. Evaluated prospectively for a median follow-up of 5.1 years, recurrence of primary UEDVT was reported to be 4.4% in those with inherited thrombophilia compared to 1.6% in those without (11).
Prevalence/Incidence
DVT in the setting of critical illness is underappreciated. Systematic screening has shown 10% of medical-surgical ICU patients to have an existing proximal lower extremity DVT on admission to the ICU. When no form of prophylaxis is used, the incidence of DVT during the ICU stay is variable but high.
Patients undergoing major general surgery have an event rate of 25% without DVT prophylaxis; 9% of patients will have clinically detectable DVT, and 7% will have proximal DVT. In a study of trauma patients who did not receive prophylaxis, 58% of patients developed a DVT, one third of which were proximal. Similarly, in patients undergoing elective hip surgery and not receiving prophylaxis, the incidence of DVT is 50%, with 23% being clinically detectable and 20% proximal (12). The pooled incidence of detectable DVT in neurosurgical patients is 22%, and the incidence in acute spinal cord injury patients is as high as 90% when prophylaxis is not used (4). The incidence of DVT in critically ill medical patients is reported to be 1% to 15% depending on which screening technique was used. No studies specific to the critically ill have been performed regarding upper extremity DVT, and no prospective studies using systematic screening techniques are available to assess the prevalence or incidence. Nonetheless, there has been an increase over the last several decades attributed to the greater use of transvenous pacemakers and central venous catheters. Symptomatic PE is reported to occur in 7–9% of these patients (13,14), and studies using systematic ventilation/perfusion scanning in those previously diagnosed with upper extremity DVT have reported high-probability scans in 13% (15).
Pharmacologic Prophylaxis
A paucity of data is available regarding anticoagulant prophylaxis in the critical care setting. To date, two published randomized trials of thromboprophylaxis versus placebo in medical-surgical ICU patients are available. In a prospective, double-blind, randomized control trial (RCT) of unfractionated heparin (UFH), 5,000 U administered subcutaneously (SQ) twice daily versus placebo, the rate of objectively confirmed DVT was reduced from 29% to 13% (16). In patients requiring mechanical ventilation ≥48 hours for exacerbations of chronic obstructive pulmonary disease (COPD), treatment with the low-molecular-weight heparin (LMWH) nadroparin once daily versus placebo decreased DVT rates from 29% to 16% (17). Another prospective trial, published in abstract form only, also demonstrated the efficacy of UFH versus placebo as thromboprophylaxis, reducing the DVT rates from 31% to 11% (18).
Despite limited generalizability to the critical care setting, thromboprophylaxis trials of acutely ill hospitalized medical patients and high-risk surgical patients are relevant. A comparison of enoxaparin, 40 mg or 20 mg, with placebo administered once daily for 6 to 14 days (MEDENOX) resulted in fewer DVTs in those receiving the 40-mg dose (19). In a randomized, placebo-controlled trial of dalteparin for the prevention of VTE (PREVENT), dalteparin, 5,000 IU once daily, halved the rate of VTE with a low risk of bleeding (20). Questions have been raised, however, as to whether or not SQ administration of LMWH has sufficient bioavailability to achieve therapeutic plasma levels (≥0.3 IU/mL) in the critically ill. In a prospective, controlled, open-labeled study of enoxaparin, 40 mg once daily, critically ill patients with normal renal function demonstrated significantly lower anti-Xa levels when compared with medical patients in the normal ward (21). This difference does not appear to be associated with vasopressor administration. On the contrary, body weight does seem to have a negative correlation with anti-Xa levels. More recently, a pilot study did not find clinically relevant differences in anti-Xa activity after subcutaneous administration of 2,500 IU dalteparin for venous thromboembolism prophylaxis between ICU patients with and without subcutaneous edema but again demonstrated critically ill patients to have lower anti-Xa activity levels than healthy volunteers (22). These findings call into question whether once-daily dosing is appropriate for the critically ill.
Last, fondaparinux, a synthetic factor Xa inibitor in doses of 2.5 mg SQ daily, has been reported to decrease VTE rates by half versus placebo in older acutely ill medical patients (ARTEMIS) (23); to be more effective than enoxaparin, 30 mg twice daily, for VTE prophylaxis after elective major knee surgery (24); and equivalent to dalteparin, 5,000 IU daily, for the prevention of VTE in high-risk abdominal surgery (PEGASUS) (25). Of note, patients requiring mechanical ventilation and those with severe sepsis and septic shock were excluded from these trials and most were not in the ICU. Nevertheless, the notion that these drugs are superior to placebo in the prevention of VTE is indeed supported.
Mechanical Prophylaxis
Graded compression stockings (GCS), intermittent pneumatic compression devices (IPC), and venous foot pumps (VFP) are attractive insofar as they are without bleeding risk. To date, no RCTs are available to guide their use in medical-surgical ICU patients. In an unblended study of 422 trauma patients, more DVT occurred in patients in whom IPC devices were used than with LMWH (2.7% vs. 0.5%) (26). Only a trend toward significance was found among 2,551 consecutive patients undergoing cardiac surgery treated with either UFH, 5,000 U SQ twice daily, or a combined prophylactic regimen of IPC and UFH; the incidence of objectively confirmed PE decreased from 4% to 1.5% (27). Use of IPC did not appear to have any additional benefit when used with either UFH or LMWH in a randomized pilot trial for VTE prophylaxis in patients undergoing craniotomy (28). IPC was less effective in preventing PE when used in addition to UFH versus LMWH alone in a prospective, randomized, multicenter trial involving acute spinal cord injury patients (29). Additionally, poor fitting GCS may lead to undue constriction and stasis of the limb on which it is applied, increasing risk of subsequent clot. As a preventative measure, most garments are manufactured with a more highly elasticized portion at the upper end as an aid to keeping the hosiery in position. It is important to realize that mechanical prophylaxis in isolation has not been shown to reduce the risk of death or PE. Mechanical VTE prophylaxis alone is not likely to be effective in the ICU and unless bleeding is of great concern, these devices should be deferred in favor of pharmacologic prophylaxis.
IVC Filters
The idea of interrupting the inferior vena cava (IVC) to prevent transit of lower extremity thromboses to the pulmonary circulation is attributed to Trousseau in 1868 (30). Today, IVC interruption is most often carried out by percutaneous insertion of a filter or “umbrella” via the femoral or jugular vein. As a result of technical refinements and ever-increasing expertise in performing the procedure, this one-time surgical technique is performed nearly 50,000 times a year (31). Categorical indications for IVC filter (IVCF) placement include contraindications to anticoagulation (absolute or relative), complications of previously instituted anticoagulation (failure, bleeding, thrombocytopenia, drug reactions), as a prophylactic adjunct to anticoagulation in patients thought to be unable to withstand another embolic event, failure of a previous IVCF, or in association with another procedure (thrombectomy, embolectomy, or thrombolysis). Unfortunately, methodologically sound literature in support of specific indications for filter placement is lacking. This paucity of evidence is highlighted by a systematic MEDLINE search for vena cava filters from 1975–2000, which produced 568 references (32). Only one RCT was identified, and only 15 prospective studies included ≥100 patients. The remainder were retrospective or case reports (65%) or reported on miscellaneous topics (8.1%). This is supported by a more recent Cochrane review (33). Consequently, recommendations for filter placement are largely a matter of opinion.
Decousus et al. (34) reported the first and only RCT of IVCFs for the prevention of PE in patients with documented proximal LEDVT. Patients were followed for 2 years in the initial report, and results of a longer-term follow-up in the same patients were reported after 8 years (35). In the initial report, 400 patients were randomized to receive a filter or no filter in addition to anticoagulation with UFH or LMWH. At 12 days, fewer patients suffered symptomatic or asymptomatic PE in the filter group while bleeding and mortality were unaffected. At 2 years, the number of patients suffering symptomatic PE was no longer significantly different (as a result of more symptomatic PE between years 1 and 2 in the filter group), and the recurrence of DVT was significantly higher in the filter group. Placement of an IVCF had no effect on survival. At 8-year follow-up, patients with filters still had higher DVT rates, but symptomatic PE was lower than in patients without a filter. Mortality was still unaffected. These reports suggest that DVT patients with or without PE may derive limited benefit from an IVCF in addition to anticoagulation alone. Placement of a filter in PE patients who have failed anticoagulation are at higher risk for a decrease in IVC patency or frank occlusion over time when compared to those with other indications for filter placement (36). However, no differences in edema formation, occurrence of varicose veins, trophic disorders, ulcer formation, or postthrombotic syndrome have been shown between those with and without a filter (35). Percutaneous filter placement in the superior vena cava may also be considered for prevention of symptomatic PE due to acute upper extremity DVT in patients in whom therapeutic anticoagulation has failed or is contraindicated. Limited observational data support its safety and efficacy in this setting (37,38).
IVCF use has not been systematically studied in critical care outside the setting of major trauma, where the deployment of retrievable IVCFs (R-IVCF) has been favored. Allen et al. (39) reported that retrievable filters are safe and effective in the prevention of PE in high-risk trauma patients with contraindications to anticoagulation. Interpretation of their findings is hampered by several factors: lack of anticoagulated patients as a comparator, small numbers (53 devices placed in 2,426 patients), and a low overall incidence of thromboembolic events (2.1% with DVT, 0.2% with nonfatal PE, no fatal PE). Others have cautioned that liberal application of these filters in the trauma population does not alter rates of VTE and may lead to a greater incidence of filter and retrieval-related complications (40). Furthermore, two recent studies reported that only about one in five of these devices is, in fact, retrieved, suggesting that they have simply become permanent filters (40,41). A small study of morbidly obese patients undergoing R-IVCF placement prior to gastric bypass surgery reported a 95% success rate when filter retrieval was attempted. Still, 21% developed VTE postoperatively (42).
In sum, no RCT of IVCF for the prevention of PE, generalizable to the critically ill, has yet been published. Currently, their use can only be recommended for those in whom anticoagulation is contraindicated or failed altogether. Consideration may be given to using a R-IVCF in the highest-risk surgical patients with contraindications to anticoagulation, with the emphasis on retrieval and commencement of anticoagulation as soon as is feasible.
Diagnosis of DVT
Validated prediction rules have been published and are useful in patients able to communicate their symptoms. However, many ICU patients will be incapable of effectively communicating any symptoms due to altered mental status, requirement for mechanical ventilation and/or infusions of sedatives, analgesics, or neuromuscular blocking drugs. Physical exam is equally unhelpful. The gold standard for DVT is lower limb venography (43). Adequately performed, it is able to detect all clinically important forms of DVT, including calf thrombosis, thrombosis of the pelvis, and the inferior vena cava. Due to the technical nature of the test, risk of radiocontrast-induced nephrotoxicity, and need to transport the patient from the ICU, it is rarely performed outside research settings. Consequently, compression ultrasound (CUS) is the most commonly reported method of detecting DVT in the ICU setting (44). For symptomatic patients, the reported pooled sensitivity for CUS in excluding a proximal DVT is 97%, but only 62% in asymptomatic patients. Furthermore, CUS lacks sensitivity in the detection of distal DVT, yielding pooled sensitivities of 73% and 53% for symptomatic and asymptomatic patients, respectively (45). Negative serial CUS over a 7- to 10-day period may effectively rule out clinically important DVT, but thus far has only been validated in symptomatic outpatients (43). An alternative to both venography and CUS is computed tomography venography (CTV) of the lower extremities and the pelvic veins as a continuation of CT angiography of the pulmonary arteries. In the setting of diagnostic workup for PE, CTV has a reported sensitivity and specificity of 70% and 96%, respectively, for all DVT, comparable to CUS in one study (46) and was superior to CUS for detection of iliofemoral DVT in a second report, yielding 100% sensitivity and specificity (47). Most recently, the PIOPED investigators reported that CTV and CUS are diagnostically equivalent, reporting a 95.5% concordance between CTV and CUS for diagnosis or exclusion of LEDVT (48). Thus the choice of imaging technique can be made on the basis of safety, expense, and time constraints. Limitations of the test are the same as for those previously mentioned for CT angiography of the pulmonary arteries.
In the case of upper extremity DVT, the first-line diagnostic test is color duplex ultrasound with a three-step protocol involving compression, color, and color Doppler with reported sensitivity and specificity ranging from 78% to 100% and 82% to 100%, respectively (9). In the event of vessel incompressibility but the presence of isolated flow abnormalities in combination with persistent clinical likelihood, contrast venography should be considered. Magnetic resonance venography (MRV) has been studied but with disappointing results. Reported sensitivities are 50% and 71% for MRV with and without gadolinium enhancement, respectively (47).
Treatment of DVT
The mainstay of therapy for all forms of VTE is anticoagulation. The reader is referred to the section for treatment of PE for further details. For larger clot burden involving the iliofemoral system, some suggest administration to thrombolytics. Indeed, a Cochrane review concluded that thrombolysis reduces postthrombotic syndrome and maintains venous patency after DVT when compared to traditional anticoagulation (49). However, the optimum drug, dose, and route of administration have yet to be determined. Endovascular catheter-directed thrombolysis is another promising treatment for acute iliofemoral thrombosis. A more definitive report of any benefits over other therapies will await completion of a recently initiated multicenter RCT for DVT (50).
|
|
|
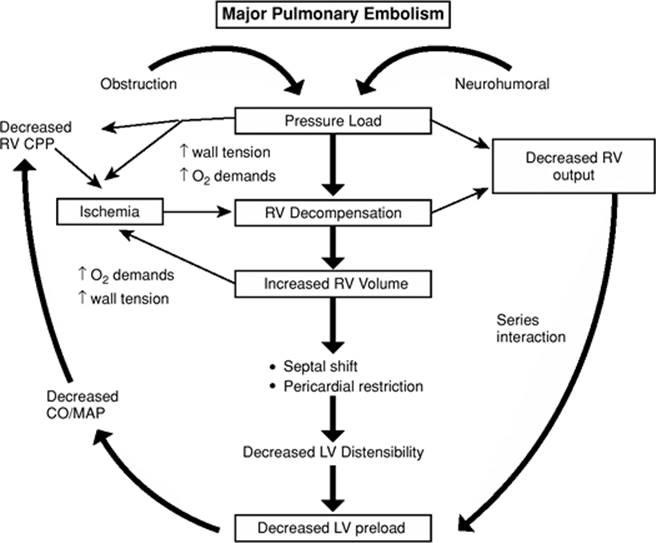
Figure 142.2. Pathophysiology of pulmonary embolism. CO/MAP, cardiac output/mean arterial pressure; CPP, cardiopulmonary pressure; LV, left ventricular; RV, right ventricular. |
Pulmonary Embolism
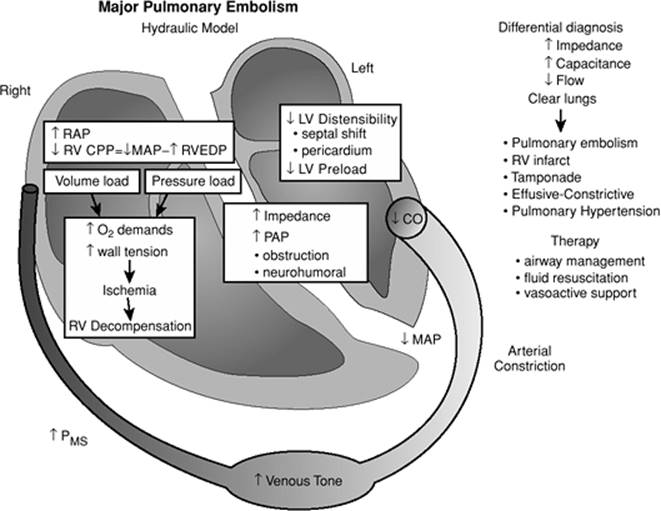
Contemporary risk stratification for the diagnosis, resuscitation, and treatment of PE is predicated on an implicit understanding of the pathophysiology of PE. The vicious pathophysiologic sequence of events related to the impaction of the embolic material on the pulmonary outflow is depicted in Figure 142.2. The combination of mechanical obstruction and neurohumoral factors combined with the patients underlying cardiopulmonary status results in an increase in pulmonary vascular impedance and the induction of pressure load on the right ventricle. Although the impact of the mechanical obstruction is well appreciated, the effect of neurohumoral influence is significantly underappreciated. The release of factors from platelets in the imbedded clot, which include serotonin, adenosine diphosphate (ADP), and thrombin, all precipitate vasoconstriction in the pulmonary artery system (51). The development of a pressure load will precipitate right ventricular decompensation, which decreases right ventricular output. Because the heart is two hydraulic pumps linked in series, diminished output of the right ventricle will result in diminished left ventricular preload. The consequence of diminished left ventricular preload is a decrease in cardiac output and a resultant loss of mean arterial pressure. The perfusion pressure gradient for the right ventricular subendocardium is the difference between the mean arterial pressure and the right ventricular end-diastolic pressure. PE precipitates an increase in right ventricular end-diastolic pressure through the induction of a right ventricular pressure load and the development of right ventricular decompensation. This increases right ventricular myocardial oxygen demands because of the diminished gradient between the mean arterial pressure and the right ventricular subendocardium. This induces further right ventricular decompensation and resultant right ventricular ischemia. The right ventricle compensates through the use of the Starling mechanism and increases right ventricular volume. This results in a left septal shift of the intraventricular septum and further jeopardizing of left ventricular filling. Pericardial restraint, further limits of left ventricular filling, and further impairments of left ventricular distensibility additionally decrease left ventricular preload. This pathophysiologic sequence results in a vicious cycle of ventricular decompensation that manifests as hemodynamic instability and shock. It is important to recognize that PE is a spectrum of presentations and that the most extreme form of PE will result in gross hemodynamic instability and cardiac arrest. Figure 142.3 illustrates a diagrammatic overview of the sequence of events that occur in PE.
|
|
|
Figure 142.3. Pathophysiology and differential diagnosis of pulmonary embolism. CO, cardiac output; CPP, cardiopulmonary pressure; LV, left ventricular; MAP, mean arterial pressure; PMS, PAP, pulmonary artery pressure; RAP, right atrial pressure; RV, right ventricular; RVEDP, RV end-diastolic pressure. |
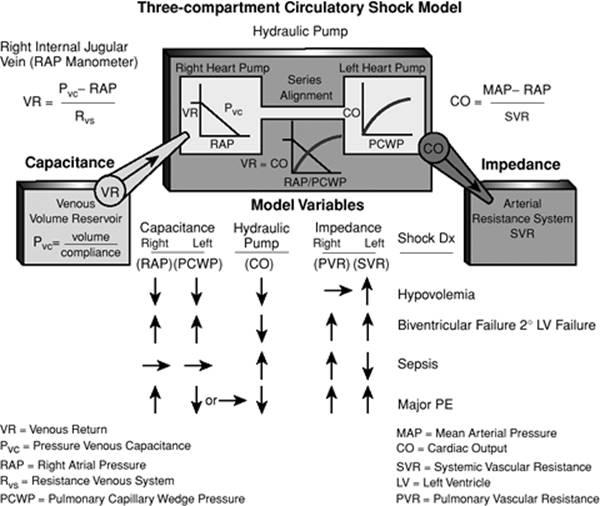
The care of the critically ill patient often proceeds along two parallel pathways; physiologic resuscitation and generation of a differential diagnosis that eventually leads to a definitive diagnosis and treatment. Consequently, the use of a universally applicable model of the circulatory system is of substantial utility in characterizing the physiologic elements for resuscitation and assisting in the differential diagnosis generation. Figure 142.4 represents a three-compartmental model of the circulatory system that is characterized by two hydraulic pumps linked in series. Each hydraulic pump has its own capacitance (volume reservoir) and impedance (resistive element) system. Insofar as the pumps are aligned in series, the output of one pump can never exceed the output of the other. Consequently, hydraulic pumps may be conceptualized as a single hydraulic unit. Using this model, the circulatory system can be viewed as a venous capacitance reservoir that provides volume to a hydraulic pump that generates flow into an impedance bed. Any hemodynamic abnormality, such as hypovolemia, ventricular failure, sepsis, or major PE, may be characterized by defining one or more of the variables in this hydraulic pump. The surrogates for venous capacitance pressure, hydraulic pump function, and impedance are right arterial pressure (RAP), cardiac output (CO), and systemic venous resistance (SVR), respectively. Oftentimes invasive monitoring or echocardiographic assessment is not immediately available on patient presentation in the intensive care unit. Consequently, it is frequently necessary to assess the model elements from physical exam; the venous capacitance reservoir may be estimated from examination the right internal jugular vein, and the pulse character and temperature of extremities maybe relied on to approximate the arterial impedance. Characteristically, a reciprocal relationship between flow and impedance is present in most disease states. Warm flushed extremities with a very wide pulse pressure indicate low vascular impedance and a correspondingly high flow state, whereas cool constricted extremities with a thready narrow pulse pressure suggest a state of high vascular impedance resulting from the compensatory increase in catecholamines to maintain perfusion pressure gradients. Recognizing that flow and impedance are almost uniformly reciprocal, one can exploit this relationship to assist with the differential diagnosis of shock patients. Therefore, the initial assessment of impedance (resistance) allows for the inferential derivation of flow. Cool clamped hypoperfused extremities reflect a catecholamines surge and low flow state. Given the hydraulic pump alignment in series, the presence of an elevated jugular venous pressure against the background of clinical and radiographically clear lungs isolates the hemodynamic lesion to the right ventricle. The differential diagnosis of increased impedance, increased capacitance pressure, and decreased flow against the background of clear lungs is illustrated in Figure 142.3 and includes PE, right ventricular infarct, and pericardial tamponade. Impaired gas exchange in conjunction with the preceding is strongly suggestive of PE. Given the potential likelihood of anticoagulation and thrombolytic therapy in this patient population, invasive monitoring should be selectively used when the circulatory model variables cannot be well characterized from physical exam. A characterization of model variables for various shock states are depicted in Figure 142.4.
|
|
|
Figure 142.4. Three-compartment circulatory shock model. |
The gas exchange abnormalities in PE are exceedingly complex and a function of the size and character of the embolic material, the magnitude of the occlusion against the background of the patients underlying cardiopulmonary status, and the interval time since the embolic event (52). The multiple causes of hypoxia have been attributed to an increase in alveolar dead space, ventilation perfusion abnormalities, right-to-left shunting, and in the case of cardiogenic shock, a low mixed venous O2. Although seemingly counterintuitive, the multiple inert gas technique suggests that a low V/Q relationship develops and precipitates hypoxia in PE consequent to the redistribution of blood flow away from the embolized area, resulting in excessive perfusion in the unembolized lung regions and subsequent reperfusion through the atelectatic area of the previous clot.
It is especially instructive to exam the clinical manifestation of PE patients without underlying cardiac pulmonary disease because it permits the assessment of the effects of the embolic event and specific compensatory responses. In this particular population, the clinical and physiologic implications of PE are directly correlated to the size of embolism (53,54,55). In these studies, there is significant correlation observed between the magnitude of the angiographic obstruction and the mean pulmonary artery pressure (mPAP) RAP, PaO2, and pulse. It has been suggested that a pulmonary vascular resistance (PVR) of greater than 500 dyne.s.cm-5 is correlative with a degree of obstruction exceeding 50% (56). It is interesting to note that depression in oxygen saturation is common and may occur with as little as 13% angiographic obstruction and commonly is the only clinical manifestation when the obstruction is less than 25% (55). When the extent of pulmonary vascular obstruction is 25% to 30%, pulmonary hypertension begins to develop (normal mPAP, 20 mmHg). It is important to recognize that this represents an increase in excess to similarly described nonembolic experimental obstruction, which further illustrates the relative contribution of the neurohumoral mechanism to pulmonary vascular impedance. Patients without underlying cardiopulmonary disease are unable to generate a mean pulmonary artery pressure in excess of 40 mm Hg, which is reported to be the maximal pressure that a healthy ventricle can generate. In patients without an underlying cardiopulmonary disease, either a large single embolus or the cumulative incremental effects of multiple recurrent emboli generating obstructions over 50% are needed to precipitate right ventricular failure. Consequently, mean pulmonary artery pressure in excess of 40 mm Hg represents either significant underlying cardiopulmonary disease or the effects of multiple embolic events that have occurred over a prolonged time period enabling the development of the right ventricular hypertrophy. It is important to recognize that the relationship between pulmonary vascular resistance and the extent of anatomic obstruction is hyperbolic and not linear. Direct increases in pulmonary vascular resistance occur when anatomic obstruction exceeds 60% (57). In the population with no underlying cardiopulmonary disease, an increase in right arterial pressure and setting of PE is almost uniformly indicative of severe pulmonary vascular obstruction. The right arterial pressure is characteristically related to the mean pulmonary artery pressure but is generally not elevated until the mean pulmonary artery pressure exceeds 30 mm Hg and anatomic obstruction exceeds 35% to 40%. Right arterial pressure can be elevated without a decrease in cardiac output in patients with PE. However, a decrease in cardiac output without an increase in right arterial pressure should suggest an alternative non–PE-related diagnosis.
In contrast to patients without an underlying cardiopulmonary disease, patients with previous cardiopulmonary disease characteristically will manifest a significantly greater degree of cardiovascular impairment with less anatomic vascular obstruction (58). This is perhaps best exemplified in the European Pulmonary Embolism Trial where 90% of the patients who presented in shock had prior cardiopulmonary disease and 56% of those with prior cardiopulmonary disease presented in shock compared to only 2% of patients without cardiopulmonary disease (59). In this population of patients with prior cardiac disease, the level of mean pulmonary artery pressure is disproportionately elevated compared to that of anatomic obstruction, which strongly suggests that underlying cardiopulmonary hemodynamics dominates the presentation process. With a mean angiographic obstruction of only 23%, significant elevations in mean pulmonary artery pressure were reported in a population with previous cardiopulmonary disease, and the increment in the mean pulmonary artery pressure was directly related to the pulmonary capillary wedge pressure (PCWP) (58). This level of anatomic obstruction would be below the threshold to elicit an increase in mean pulmonary artery pressure in patients without cardiopulmonary disease. In patients with prior cardiopulmonary disease, the right arterial pressure was reported to be an unreliable indicator of the magnitude of the embolic event and limited its usefulness in the assessment of extensive vascular obstruction and life-threatening disease. Therefore, it appears that there is no consistent relationship between the extent of embolic obstruction and right ventricular impairment in patients with previous cardiopulmonary disease. Hemodynamic and right ventricular function can be misleading as measurements of the effect of the embolic event, which clearly underscores that the assessment of the severity is predicated on the pre-embolic status of the patient as illustrated in Figure 142.1.
Readily Available Diagnostic Studies
The development of a differential diagnosis in the case of the undifferentiated shock patient or existing patients in the critical care unit is usually predicated on elements derived from the history, physical findings, and readily available diagnostic studies to include a chest x-ray (CXR) study, arterial blood gas (ABG), and electrocardiogram (ECG). It is important to recognize the physiologic footprint that PE makes on these readily available studies to ensure that PE is hierarchically incorporated into the differential diagnosis of the unstable patient. Generating this differential diagnosis is often difficult in the critical care environment given the inability to obtain a current history from the patient, multiple comorbidities masking physical findings, and coexistent disease that already compromises existing laboratory variables. Although multiple risk factors are additive, admission to an intensive care unit by itself denotes a significant risk factor for venous thromboembolism. In patients presenting to the intensive care unit with undifferentiated shock or respiratory failure, it is imperative to review each specific case for risk factors that may contribute to the development of PE. The previously defined hydraulic model of the circulation allows for a physiologic characterization of the differential diagnosis. The constellation of right arterial pressure elevation with cool clamped extremities indicative of low flow against the background of relatively clear lungs and CXR isolates the hydraulic lesion to the right ventricle with a very limited differential diagnosis as illustrated in Figure 142.3. Occasionally, invasive hemodynamic measurements will be available, which should reflect an increase in the right arterial pressure, a low cardiac output state in the shock population, associated with a low pulmonary capillary wedge pressure and a high SVR.
Electrocardiogram
Since the sentinel description in 1935 by McGinn and White (60) of the S1Q3T3 pattern in a limited number of patients with PE-induced cor pulmonale, a plethora of ECG manifestation have been reported. However, several important points from large series regarding the ECG findings for PE may be helpful: First, a normal ECG is distinctly unusual and it is reported in only in a minority of patients in the UPET Trial without cardiopulmonary disease (14%) (61) and was similarly appreciated in only 30% of patients in the PIOPED Trial (62). Rhythm disturbances are uncommon, and the incidence of atrial fibrillation and flutter as a presenting component of PE is exceedingly small as are first-, second-, or third-degree heart blocks. The most common ECG findings are related to abnormalities in the ST-T wave segment. In UPET (61) and PIOPED (62), these changes occurred in 42% and 49% of patients, respectively. Recently, it has been shown that the anterior T-wave inversion pattern is the most common abnormality in PE, occurring in 68% of patients. It was the ECG sign that was most correlative with the severity of the underlying embolic event as 90% of the patients with anterior T-wave inversion had a Miller Score exceeding 50% (mean 60%), and 81% of those had a mean pulmonary artery pressure elevation exceeding 30 mm Hg (54). The early appearance of the T-wave inversion was reported to be an even stronger marker of the severity of the event and similarly correlative with the efficacy of thrombolytic therapy given the T-wave normalization that occurred in patients who had successful thrombolytic therapy (63).
Chest Radiograph
Although the chest radiograph cannot be effectively used to include and exclude PE, it is helpful in contributing to the diagnostic assessment by excluding other diseases that may mimic PE and defining abnormalities that necessitate further evaluation, and it may provide a crude assessment of severity (64). Similar to the ECG, a normal chest radiograph in patients with angiographic-proven PE is unusual and occurred in only 16% and 34% of patients in the PIOPED (62) and UPET (61), respectively, who did not have cardiopulmonary disease. In PIOPED, there appeared to be an association between severity of the thromboembolic event and the radiographic findings defined by the relationships between pulmonary artery pressure (PAP), oxygen saturation, and CXR findings when normal chest x-ray views were compared to those with parenchymal and vascular abnormalities (64). Vascular abnormalities including relative oligemia in the area of embolic event were correlative with the severity of PE. Other findings on CXR suggestive of PE include abrupt cutoff of the pulmonary artery, relative or focal oligemia, and distention of the proximal portion of the pulmonary artery.
Arterial Blood Gas
It is important to recognize that hypoxia in PE is not uniform as PaO2 readings greater than 80 mm Hg were seen in approximately 12% of UPET patients and 19% of PIOPED patients (65,66). It is similarly important to recognize that a normal PaO2 does not exclude PE and occurred in approximately 14% of patients in the PIOPED Trial (62,67). In patients without underlying cardiopulmonary disease, it is likely that these small changes in oxygen saturation reflect low levels of severity in PE. In contrast to the almost linear relationship between PE severity and arterial oxygen saturation levels in patients without cardiopulmonary disease, there appears to be no correlation between the arterial oxygen saturation or PaO2 and magnitude of the embolic event in patients with cardiopulmonary disease. Given that many patients in intensive care units have significant gas impairment and are maintained on mechanical ventilation, it is the change in the oxygen saturation or the requirement of escalating levels of inspired oxygen that should prompt the consideration toward evaluation for PE. In intensive care units that are capable of measuring dead space (Vd/Vt) or end-tidal CO2, these should similarly be used given the physiologic imprint of increased dead space with PE.
Diagnostic Therapeutic Approach
Risk Stratification
The contemporary approach to physiologic risk stratification is depicted in Figure 142.1. The combination underlying cardiopulmonary status and embolic size that precipitates cardiac arrest is surprisingly associated with a mortality of only 70% in reported series. This underscores the necessity of aggressively pursuing patients with suspected underlying PE presenting with cardiac arrest because approximately 30% of those patients with PE and cardiac arrest will survive. At the other extreme, it is equally underappreciated that the predicted mortality of patients with hemodynamically stable PE and normal right ventricle is very low when treated with appropriate anticoagulation. The combination of embolic size and cardiopulmonary status that precipitates decompensation resulting in shock is associated with a 30% mortality. Although not well reported, syncope and emboli in transit have predicted mortalities just below that of a shock patient. Echocardiography is frequently used to risk-stratify patients with PE who are hemodynamically stable. However, it is important to recognize that the vast overwhelming majority of patients with right ventricular dysfunction and hemodynamic stability will do well with anticoagulation alone. As is evident in Figure 142.1, there is a spectrum of presentations related to hemodynamically stable patients with PE that may include patients with incipient shock and those with insignificant dilatation of the right heart. It is important to recognize that an anatomic obstruction of approximately 30% is necessary to provoke elevations in pulmonary artery pressure. Similarly literature related to echocardiography reveals that an obstruction of 30% is needed to precipitate right ventricular dilatation.
The presence of hemodynamic deterioration or shock in a patient with PE represents the failure of both compensatory mechanisms to maintain forward flow and is associated with significant increases in mortality. Consequently, the presence of shock has traditionally been used as a discriminator to define the likelihood of survivorship from PE. The presence of shock in patients with PE is associated with a threefold to sevenfold increase in mortality (68,69). It is underappreciated that the vast majority of patients with anatomically massive PE do not present in shock. Case series have reported a majority of patients without underlying cardiopulmonary disease and associated anatomically massive PE present with a normal cardiac output (70). Similarly, it is important to recognize that hemodynamically stable patients who are not in shock, who have experienced submassive or massive PE, have similar mortality rates (68,69). An anatomically massive PE, unless accompanied by physiologic decompensation resulting in shock and hemodynamic instability, does not appear to be associated with increased mortality.
Figure 142.5 represents a diagnostic/therapeutic algorithm based on the presence or absent of shock. In all patients presenting with PE, therapeutic anticoagulation should be undertaken on presentation provided there are no contradictions to anticoagulation. The therapeutic effect of heparin is related to the ability to prevent further clot propagation and the prevention of recurrent of PE. Insofar as the risk of recurrent thromboembolic event is highest in the period immediately after PE, and because recurrent thromboembolic events are the most common cause of death in hemodynamic stable patients, it is pivotal to adequately and appropriately achieve a therapeutic level of anticoagulation as soon as feasible. Given the risks of bleeding associated with critical illness, unfractionated intravenous heparin is recommended because of the short half-life and the ability to reverse the therapeutic effect of heparin with protamine. Low-molecular-weight heparin, although appealing in the outpatient treatment of DVT and stable PE patients cannot be readily reversed.
|
|
|
Figure 142.5. Diagnostic therapeutic approach to pulmonary embolism. AMI, acute mesenteric ischemia; CT, computed tomography; DVT, deep vein thrombus; LV, left ventricle; RV, right ventricle; TEE, transesophageal echocardiography; TTE, transthoracic echocardiography; US, ultrasound; V/Q, ventilation/perfusion. |
In patients without evidence of hemodynamic stability, spiral CT scanning has supplanted ventilation perfusion scanning as a diagnostic modality of choice in PE. In patients with elevated creatinine or inability to tolerate a CT scan, Ventilation/ perfusion (V/Q) scanning represents a reasonable alternative given the overwhelming experience using this technique. Pretest probability characterizations are pivotal in the diagnosis of PE whether CT scanning or ventilation/perfusion scanning is used. Pretest probability can be characterized by the use of scoring systems or based on clinical judgment. The combination of a high pretest probability with a high-probability V/Q scan confirms the diagnosis of PE. Similarly, a low-probability V/Q scan in conjunction with a low clinical pretest probability effectively excludes PE. Any other combination of pretest probability and scan probability requires further testing to include and exclude PE. Similarly, it is imperative to characterize a pretest probability for PE using CT scanning as a diagnostic modality. In patients with a high pretest probability and a negative spiral CT scan, further diagnostic studies should be undertaken. Although spiral CT scanning has been used to either exclude or confirm PE, there is an evolving literature that suggests spiral CT scanning can be used to define the severity of PE. Recent reports have been able to characterize the extent of pulmonary artery obstruction (71,72). Similar to the Miller and Walsh scores, which defined the extent of anatomic obstruction, there has been variability in reports of outcome related to the extent of obstruction. Measurements that are available from the CT scan include the calculation of the RV/LV axis ratio, the diameter of the right ventricular chamber, assessment of pulmonary artery diameter, and reflux of contrast material into the inferior vena cava (73). Although there are no prospective studies that have been conducted to assess the utility of spiral CT scanning as a predictor for severity stratification, it has been reported that the probability of death is significantly correlative with the RV/LV ratio. It appears that spiral CT scanning is evolving as the modality of choice for the diagnosis of PE and will be used to define severity stratification (73).
Further risk stratification of hemodynamically stable patients with PE may be undertaken using brain natriuretic peptide (BNP) and troponin levels. In patients with hemodynamic stability and confirmed PE that presents with a normal BNP and troponin levels, the predicted outcomes are excellent, and many of these patients may be treated as outpatient in the future. The presence of elevation in BNP and troponin define a high-risk population of patients with hemodynamic stability and warrant admission and close observation. The approach to this population will be discussed subsequently in this chapter.
In contrast to the patient presenting without hemodynamic instability, patients with suspected PE and hemodynamic instability are at high risk for rapid deterioration and sudden death. This demands an expeditions approach to the diagnosis, resuscitation, and therapy of this population. Echocardiography is an ideal first assessment of the hemodynamically unstable patient because it is becoming readily available, an integral part of critical care medicine, repeatable, and useful in recognition and differentiation of PE along with assessing the severity of the embolic event and the patient's response to therapy (74,75,76). Characteristic findings suggestive of PE include right-sided thrombi, right ventricular dilatation, hypokinesis, tricuspid regurgitation, and paradoxical shifting of the ventricular septum. Similarly, the echocardiographic findings of acute myocardial infarction, tamponade, aortic dissection, or valvular disease may be equally useful in confirming the diagnosis and excluding PE. In patients without underlying cardiopulmonary disease, the magnitude of the abnormalities seen on echocardiogram correlate with the degree of pulmonary artery outflow obstruction (77). Similar to the original data related to angiographic measurement of pressure generation with PE, it appears that an obstruction of 30% is necessary to produce right ventricular dilatation. Degrees of obstruction less than 30% will not characteristically present with right ventricular dilatation. Consequently, right ventricular dilatation has been used for severity stratification as the outcome of patients who do not have right ventricular dysfunction is excellent with therapeutic anticoagulation. It is crucial to recognize that the presence of right ventricular function is not specific for PE. Patients with previous cardiopulmonary disease may have evidence of right ventricular dysfunction at baseline. In this setting, right ventricular function might be a representative of a spectrum of diseases that range from RV infarct with cardiomyopathy to cor pulmonale and antecedent pulmonary hypertension. Several echocardiographic findings have been reported to be useful in differentiating PE from non-PE events. Patients with baseline cor pulmonale or recurrent PE characteristically have evidence of hypertrophy in the right ventricle with a thickness measuring greater than 5 mm (76,78) and a minimal septal shift, whereas acute right ventricular failure secondary to PE should not be associated with right ventricular hypertrophy nor accompanied by a septal shift (77,79). In patients with pre-existing cardiopulmonary disease, it is imperative to establish the diagnosis of PE, which may be undertaken with diagnostic studies previously discussed in a nonshock patient. Spiral CT scanning has supplanted V/Q scans in the critically ill population. In patients with evidence of PE that is confirmed on the diagnostic studies, candidacy for either medical thrombectomy with thrombolytic therapy or surgical embolectomy should be undertaken. It is crucial to recognize that the absence of right ventricular pressure overload in the unstable patient in whom PE is being considered effectively excludes PE as a culprit cause of the hemodynamic instability. Occasionally, and in the appropriate clinical context, patients without underlying cardiopulmonary disease in extremis and with anticipated arrest with evidence of right ventricular dilatation and high pretest probability for PE may be considered as candidates for medical embolectomy with thrombolytic therapy or surgical embolectomy, given the time necessary to perform confirmatory studies, which may jeopardize effective treatment.
Resuscitation and Stabilization
Throughout the diagnostic evaluation, patients with suspected PE often require aggressive resuscitation and attempts at stabilization. In these patients, marginal hemodynamic stability is often maintained by intense catecholamine release. Frequently, escalating oxygen requirements necessitate intubation and mechanical ventilation. Intubation may precipitate cardiovascular collapse in patients with major PE for several reasons: sedative hypnotics that are used for intubation can mitigate the catecholamine surge on which the patient is dependent and similarly produce vasodilatation, which impairs the perfusion pressure gradient to the right ventricular subendocardium, provoking further ischemia and cardiac decompensation. Excessive lung ventilation on initial intubation may create air trapping and diminish venous return. Initiation of mechanical ventilation can increase the pulmonary vascular resistance and further jeopardize right ventricular function. Consequently, intubation should be carefully undertaken, weighing the risk and benefits of a conscience awake technique with topical or local anesthesia in conjunction with a rapid-sequence approach using neuromuscular blockade and/or fiberoptic intubation. Etomidate is an ideal sedative hypnotic insofar as it preserves hemodynamic status.
Conventionally, volume expansion with 1 to 2 L of crystalloid solution is initial treatment for hypotension in patients with undifferentiated shock. However, in patients with PE-related shock, increases in right ventricular pressure and volume generate significant increases in systolic wall stress, provoking myocardial ischemia. Excessive fluid resuscitation further dilates the right ventricle and produces increased wall stress, resulting in further right ventricular decompensation. In patients with anatomically massive PE and low cardiac output who were normotensive and required vasopressors on presentation, Mercat et al. (80) reported increases in cardiac output with a 500-mL fluid challenge. The authors reported that the increase in cardiac output was consistently proportional to the baseline right ventricular and diastolic volume index. Therefore, fluid may be used judicially in normotensive patients without evidence of significant right ventricular dysfunction. In patients with echocardiographic evidence of severe right ventricular dysfunction, fluid resuscitation may provoke increased wall stress, ischemia, and right ventricular dysfunction. When measured right ventricular pressure are high or there is evidence of severe right ventricular dysfunction, early consideration should be given to vasopressor therapy.
Although there are no controlled human trials related to vasoactive support in PE, extrapolation from animal models suggests that norepinephrine improves right ventricular dysfunction through vasoconstriction that augments mean arterial pressure and enhances perfusion pressure gradients to the right ventricular subendocardium. In addition, norepinephrine possesses modest inotropic properties that have been shown to provide complementary enhancement of right ventricular function (81,82). Given the previously described vasoconstrictive effects of the neurohumoral response to PE, it may be reasonable to consider the use of inhaled nitric oxide to decrease pulmonary vascular afterload in patients with evidence of severe right ventricular dysfunction who are pressor dependent. Small reports have suggested that inhaled prostacyclin and nitric oxide will increase cardiac output, decrease pulmonary artery pressures, and improve gas exchange in cases of shock-related PE (83,84).
The presence of shock or hemodynamic decompensation in patients with proven PE is an indication for either medical embolectomy with thrombolytic therapy or surgical embolectomy. Although the use of thrombolytic therapy is controversial in patients who are hemodynamically stable, it is acknowledged as the therapeutic choice in hemodynamically unstable patients in whom there is no contraindication to thrombolytic therapy. The PIOPED investigators considered thrombolytic therapy the standard of care for patients with “shock or major disability” and considered it unethical to treat patients with hemodynamic stability with heparin alone in the research trial (85). Several points regarding the use of thrombolytic therapy in PE patients should be emphasized. First, in virtually all studies, there is greater rapidity in the rate of resolution when comparing heparin to thrombolytic therapy in terms of the percent resolution detected by perfusion scanning and angiography. Second, no reported clinical trial has defined any difference in the degree of embolic resolution after day 7. This is perhaps best illustrated in the original UPET Trial conducted in 1970 (68). In this landmark publication related to the use of thrombolytic therapy and PE, the baseline angiographic defect in the heparin group was 25% and 26% in the urokinase group. Within the first 24 hours, the percent of angiographic resolution in the heparin group was 8.1% and 22.1% in the urokinase-treated group. However, by day 5, the extent of the degree of angiographic resolution in the heparin and urokinase groups was equivalent at 36% and 40%, respectively. By 1 year, the extent of angiographic resolution was 77% in the heparin group and 78% in the urokinase group (Table 142.2). A comparison of clinical trials conducted comparing lytic therapy to heparin reveals similar findings as there is no reported difference in any physiologic or imaging modality after day 5 when comparing the two therapeutic options (Table 142.3). However appealing the rapidity of resolution may be, only one small trial (86) has demonstrated a mortality benefit. This small trial consisted of only eight patients with benefit confined only to those who received thrombolytic therapy. It is important to note that the patients randomized to heparin had previously been treated with heparin and experienced recurrent PE and were subsequently randomized to the heparin treatment. Third, there does not appear to be any difference related to the effectiveness of thrombolytic agents provided that they are given in equivalent doses over a similar time frame (70,87). This is best exemplified in trials that compared rT-PA given over 2 hours and urokinase given in the same time interval (70). Fourth, bleeding complications from thrombolytic therapy remain a substantial concern with major hemorrhage report occurring in approximately 12% of patients and fatal hemorrhage occurring in 1% to 2% of patients (88). Intracranial hemorrhage rates have been reported from 1.2% to 2.1% (89) and is fatal in at least half of the cases (90). Last, there does not appear to be a difference between intrapulmonary thrombolytic therapy and peripheral IV thrombolytic therapy (91).
|
Table 142.2 Rate and Extent of Perfusion Scan Resolution in Urokinase Pulmonary Embolism Trial (UPET) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Table 142.3 Randomized Trials—Lysis versus Heparin |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Assessing the efficacy of thrombolytic therapy can be difficult in the first several hours. Echocardiographic studies undertaken prior to the use of thrombolytic therapy have suggested that there are two types of morphologic characteristics of PE that may assist in defining the efficacy of therapy. Thrombi that are long, mobile, and hypoechoic/heterogeneous seem to be more susceptible to thrombolytic therapy. In contrast, echocardiographically defined emboli that are immobile and hyperechoic/homogeneous seem less susceptible to thrombolytic therapy. In a small case report series of patients who received thrombolytic therapy and had the previous characterizations made by echocardiography, long mobile hypoechoic emboli had higher cardiac outputs, lower central venous pressures, and diminished peripheral vascular resistance compared to the group with echocardiographically defined immobile embolism after the use of thrombolytic therapy. It is important to note that the mortality in the group that underwent successful embolectomy was 0% compared to a 30% mortality in the group that failed to respond to thrombolytic therapy (92). Monitoring the efficacy of thrombolytic therapy can similarly be challenging as continuous echocardiography and imaging studies are not available. Monitoring of end-tidal CO2 has been proposed to monitor the efficacy of thrombolytic therapy. End-tidal CO2 was found to significantly increase in patients who survived with thrombolytic therapy compared to those with no appreciable change in end-tidal CO2 measurements in patients who did not survive. This would suggest that continuous monitoring of end-tidal CO2 enables assessment of the efficacy of thrombolytic therapy and may be used as a barometer to define the need of subsequent thrombolytic or embolectomy in cases of failed thrombolytic therapy (93). Unsuccessful thrombolysis is reported to occur in approximately 8% of patients undergoing therapy. This may be defined as persistent clinical instability or significant residual echocardiographic dysfunction. In the limited literature that compares repeat thrombolysis to surgical thromboembolectomy, there appears to be significant survival benefit in undertaking surgical embolectomy. The mortality in patients undergoing surgical embolectomy after failed thrombolytic therapy was reported to be 7% compared to 38% of patients who underwent repeat thrombolysis. Recurrent PE was significantly higher in patients who underwent repeat thrombolysis and was the cause of death in a significant number of patients. It should be noted that patients who underwent surgical thromboembolectomy also had the placement of vena cava filters (94).
Thrombolytic therapy in hemodynamically stable patients remains a continuing and controversial topic. Multiple reviews and meta-analyses are available to assist with the use of thrombolytic therapy (95,96,97) (Cochrane Collaboration 2006, issue 3). The long-term outcome of patients with thrombolytic therapy is not well described but it appears that most patients undergo an uneventful course, the mortality is approximately 8%, and major bleeding is reported to occur in 9.6% with recurrent PE reported in 7.6%. The mean vascular obstruction diminished from 64% to 29% within 48 hours, and right ventricular function was reversible within 48 hours in 80% of the patients, while lung scan improved 45% within 6 to 8 days of therapy. This contemporary review of thrombolytic therapy similarly reported that predictive indicators of a poor hospital course in patients receiving thrombolytic therapy were an initial pulmonary vascular obstruction greater than 70% and hemodynamic instability at presentation associated with persistence of paradoxical septal motion on echocardiography. Long-term mortality was related to older age, persistence of vascular obstruction more than 30% after thrombolytic therapy, and cancer (98).
Surgical embolectomy is indicated for patients presenting in shock or cardiopulmonary instability and an inability to tolerate thrombolytic therapy. Ideally, these emboli are large and located centrally and consideration of embolectomy is undertaken prior to cardiac arrest. This requires preoperative localization via CT documentation and ideally echocardiographic of right heart function (99). In the era of modern surgical embolectomy, outstanding results have been reported by multiple investigators. In a study that undertook surgical embolectomy with most patients having a contraindication to thrombolytic therapy and significant right ventricular dysfunction, there was a 6% operative mortality and only 12% late deaths from disease other than PE (100). The overall improvement in operative mortality related to surgical thromboembolectomy most likely relates to preop selection of patients who had not experienced cardiac arrest and the use of cardiopulmonary bypass (99).
The approach to hemodynamically stable patients with PE and right ventricular dysfunction remains a controversial and contentious topic. Recently, the use of BNP, which is indicative of right ventricular stress, and troponin levels, which are indicative of myocardial ischemia, have been used in the stratification of this population. These biomarkers have been reported to allow for severity characterization of patients with PE. In instances where there is an absence of an elevation in BNP or troponin levels, the predicted outcome is excellent and these patients do not warrant intensive care evaluation. In contrast, elevations in BNP and troponin levels are associated with a higher mortality and are evolving as discriminators for the use of thrombolytic therapy in patients with PE.
In summary, PE remains a common and lethal problem that usually confronts the intensivist in the form of undifferentiated respiratory failure and shock. Diagnosis is difficult and challenging in the intensive care unit because of the patient complexity and coexistent illnesses. The use of spiral CT scans and echocardiography is evolving to define severity stratification in the ICU population and facilitate the timely diagnosis of PE. It is imperative to incorporate PE into the differential diagnosis of patients with undifferentiated shock, and the use of a structure model for shock diagnosis and therapy is helpful to ensure that PE is expeditiously diagnosed and optimal treatment is undertaken. Thrombolytic therapy is recognized as the treatment of choice for hemodynamically unstable patients, and the optimal approach to the hemodynamically stable patient with right ventricular dysfunction remains to be defined.
References
1. Kasper W, Konstantinides S, Geibel A, et al. Management strategies and determinants of outcome in acute major pulmonary embolism: results of a multicenter registry. J Am Coll Cardiol. 1997;30:1165–1171.
2. Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the international cooperative pulmonary embolism registry (icoper). Lancet. 1999;353:1386–1389.
3. Quality AfHRa. Making health care safer: a critical analysis of patient safety practices. April 28, 2008.
4. Cook DJ, Crowther MA, Meade MO, et al. Prevalence, incidence, and risk factors for venous thromboembolism in medical-surgical intensive care unit patients. J Crit Care. 2005;20:309–313.
5. Ibrahim EH, Iregui M, Prentice D, et al. Deep vein thrombosis during prolonged mechanical ventilation despite prophylaxis. Crit Care Med. 2002;30:771–774.
6. Cook D, Crowther M, Meade M, et al. Deep venous thrombosis in medical-surgical critically ill patients: prevalence, incidence, and risk factors. Crit Care Med. 2005;33:1565–1571.
7. Warkentin TE, Greinacher A. Heparin-induced thrombocytopenia and cardiac surgery. Ann Thor Surg. 2003;76:638–648.
8. Mustafa S, Stein PD, Patel KC, et al. Upper extremity deep venous thrombosis. Chest. 2003;123:1953–1956.
9. Gaitini D, Beck-Razi N, Haim N, et al. Prevalence of upper extremity deep venous thrombosis diagnosed by color Doppler duplex sonography in cancer patients with central venous catheters. J Ultrasound Med. 2006; 25:1297–1303.
10. Joffe HV, Kucher N, Tapson VF, et al. Upper-extremity deep vein thrombosis: a prospective registry of 592 patients. Circulation. 2004;110:1605–1611.
11. Martinelli I, Battaglioli T, Bucciarelli P, et al. Risk factors and recurrence rate of primary deep vein thrombosis of the upper extremities. Circulation. 2004;110:566–570.
12. Murray MT, Coursin DB, Pearl RG, et al., eds. Critical Care Medicine: Perioperative Management. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002.
13. Becker DM, Philbrick JT, Walker FB 4th. Axillary and subclavian venous thrombosis. Prognosis and treatment. Arch Intern Med. 1991;151:1934–1943.
14. Hingorani A, Ascher E, Lorenson E, et al. Upper extremity deep venous thrombosis and its impact on morbidity and mortality rates in a hospital-based population. J Vasc Surg. 1997;26:853–860.
15. Monreal M, Lafoz E, Ruiz J, et al. Upper-extremity deep venous thrombosis and pulmonary embolism. A prospective study. Chest. 1991;99:280– 283.
16. Fraisse F, Holzapfel L, Couland JM, et al. Nadroparin in the prevention of deep vein thrombosis in acute decompensated COPD. The association of non-university affiliated intensive care specialist physicians of France. Am J Resp Crit Care Med. 2000;161:1109–1114.
17. Cade JF. High risk of the critically ill for venous thromboembolism. Crit Care Med. 1982;10:448–450.
18. Kappor M KY, Tessler S. Subcutaneous heparin prophylaxis significantly reduces the incidence of venous thromboembolic events in the critically ill. Crit Care Med. 1999;27:A69.
19. Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. Prophylaxis in medical patients with enoxaparin study group. N Engl J Med. 1999;341:793–800.
20. Leizorovicz A, Cohen AT, Turpie AG, et al. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation. 2004;110:874–879.
21. Priglinger U, Delle Karth G, Geppert A, et al. Prophylactic anticoagulation with enoxaparin: is the subcutaneous route appropriate in the critically ill? Crit Care Med. 2003;31:1405–1409.
22. Rommers MK, Van der Lely N, Egberts TC, et al. Anti-xa activity after subcutaneous administration of dalteparin in ICU patients with and without subcutaneous oedema: a pilot study. Crit Care (London, England.) 2006;10:R93.
23. Cohen AT, Davidson BL, Gallus AS, et al. Efficacy and safety of fondaparinux for the prevention of venous thromboembolism in older acute medical patients: Randomised placebo controlled trial. BMJ. 2006;332:325–329.
24. Bauer KA, Eriksson BI, Lassen MR, et al. Fondaparinux compared with enoxaparin for the prevention of venous thromboembolism after elective major knee surgery. N Engl J Med. 2001;345:1305–1310.
25. Agnelli G, Bergqvist D, Cohen AT, et al. Randomized clinical trial of postoperative fondaparinux versus perioperative dalteparin for prevention of venous thromboembolism in high-risk abdominal surgery. Br J Surg. 2005;92:1212–1220.
26. Ginzburg E, Cohn SM, Lopez J, et al. Randomized clinical trial of intermittent pneumatic compression and low molecular weight heparin in trauma. Br J Surg. 2003;90:1338–1344.
27. Ramos R, Salem BI, De Pawlikowski MP, et al. The efficacy of pneumatic compression stockings in the prevention of pulmonary embolism after cardiac surgery. Chest. 1996;109:82–85.
28. Macdonald RL, Amidei C, Baron J, et al. Randomized, pilot study of intermittent pneumatic compression devices plus dalteparin versus intermittent pneumatic compression devices plus heparin for prevention of venous thromboembolism in patients undergoing craniotomy. Surg Neurol. 2003;59:363–372; discussion 372–364.
29. Prevention of venous thromboembolism in the acute treatment phase after spinal cord injury: a randomized, multicenter trial comparing low-dose heparin plus intermittent pneumatic compression with enoxaparin. J Trauma. 2003;54:1116–1124; discussion 1125–1116.
30. Trousseau A. Phlegmatia alba dolens: Clinique medicale de l'hotel-dieu de paris. JB Baillere et Fils. 1868:652–695.
31. Ansell J. Vena cava filters: do we know all that we need to know? Circulation. 2005;112:298–299.
32. Girard P, Stern JB, Parent F. Medical literature and vena cava filters: so far so weak. Chest. 2002;122:963–967.
33. Young T, Tang H, Aukes J, et al. Vena caval filters for the prevention of pulmonary embolism. Cochrane Database Syst Rev. 2007 Oct 17;(4): CD006212.
34. Decousus H, Leizorovicz A, Parent F, et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. Prévention du Risque d'Embolie Pulmonaire par Interruption Cave Study Group. N Engl J Med. 1998;338:409–415.
35. PREPIC Study Group. Eight-year follow-up of patients with permanent vena cava filters in the prevention of pulmonary embolism: the PREPIC (Prévention du Risque d'Embolie Pulmonaire par Interruption Cave) Randomized Study. Circulation. 2005;112:416–422.
36. Crochet DP, Stora O, Ferry D, et al. Vena Tech-LGM filter: long-term results of a prospective study. Radiology. 1993;188:857–860.
37. Ascher E, Hingorani A, Tsemekhin B, et al. Lessons learned from a 6-year clinical experience with superior vena cava Greenfield filters. J Vasc Surg. 2000;32:881–887.
38. Spence LD, Gironta MG, Malde HM, et al. Acute upper extremity deep venous thrombosis: safety and effectiveness of superior vena caval filters. Radiology. 1999;210:53–58.
39. Allen TL, Carter JL, Morris BJ, et al. Retrievable vena cava filters in trauma patients for high-risk prophylaxis and prevention of pulmonary embolism. Am J Surg. 2005;189:656–661.
40. Antevil JL, Sise MJ, Sack DI, et al. Retrievable vena cava filters for preventing pulmonary embolism in trauma patients: a cautionary tale. J Trauma. 2006;60:35–40.
41. Karmy-Jones R, Jurkovich GJ, Velmahos GC, et al. Practice patterns and outcomes of retrievable vena cava filters in trauma patients: an AAST multicenter study. J Trauma. 2007;62:17–24; discussion 24–15.
42. Schuster R, Hagedorn JC, Curet MJ, et al. Retrievable inferior vena cava filters may be safely applied in gastric bypass surgery. Surg Endosc. 2007;21:2277–2279.
43. Cook D, Douketis J, Crowther MA, et al. The diagnosis of deep venous thrombosis and pulmonary embolism in medical-surgical intensive care unit patients. J Crit Care. 2005;20:314–319.
44. Cook D, McMullin J, Hodder R, et al. Prevention and diagnosis of venous thromboembolism in critically ill patients: a Canadian survey. Crit Care (London, England). 2001;5:336–342.
45. Kearon C, Gent M, Hirsh J, et al. A comparison of three months of anticoagulation with extended anticoagulation for a first episode of idiopathic venous thromboembolism. N Engl J Med. 1999;340:901–907.
46. Taffoni MJ, Ravenel JG, Ackerman SJ. Prospective comparison of indirect CT venography versus venous sonography in ICU patients. AJR Am J Roentgenol. 2005;185:457–462.
47. Lim KE, Hsu WC, Hsu YY, et al. Deep venous thrombosis: comparison of indirect multidetector CT venography and sonography of lower extremities in 26 patients. Clin Imag. 2004;28:439–444.
48. Goodman LR, Stein PD, Beemath A, et al. CT venography for deep venous thrombosis: continuous images versus reformatted discontinuous images using PIOPED II data. AJR Am J Roentgenol. 2007;189:409–412.
49. Watson LI, Armon MP. Thrombolysis for acute deep vein thrombosis. Cochrane Database Syst Rev. 2004 Oct 18;(4):CD002783.
50. Enden T, Sandvik L, Klow NE, et al. Catheter-directed Venous Thrombolysis in acute iliofemoral vein thrombosis–the CaVenT study: rationale and design of a multicenter, randomized, controlled, clinical trial (nct00251771). Am Heart J. 2007;154:808–814.
51. Stratmann G, Gregory GA. Neurogenic and humoral vasoconstriction in acute pulmonary thromboembolism. Anesth Analg. 2003;97:341– 354.
52. D'Alonzo GE, Dantzker DR. Gas exchange alterations following pulmonary thromboembolism. Clin Chest Med. 1984;5:411–419.
53. Dalen JE, Banas JS Jr., Brooks HL, et al. Resolution rate of acute pulmonary embolism in man. N Engl J Med. 1969;280:1194–1199.
54. McDonald IG, Hirsh J, Hale GS, et al. Major pulmonary embolism, a correlation of clinical findings, haemodynamics, pulmonary angiography, and pathological physiology. Br Heart J. 1972;34:356–364.
55. McIntyre KM, Sasahara AA. The hemodynamic response to pulmonary embolism in patients without prior cardiopulmonary disease. Am J Cardiol. 1971;28:288–294.
56. Dalen JE, Grossman W. Profiles in pulmonary embolism: cardiac catheterization and angiography. Philadelphia, PA: Lea & Febiger; 1980.
57. Petitpretz P, Simmoneau G, Cerrina J, et al. Effects of a single bolus of urokinase in patients with life-threatening pulmonary emboli: a descriptive trial. Circulation. 1984;70:861–866.
58. McIntyre KM, Sasahara AA. Determinants of right ventricular function and hemodynamics after pulmonary embolism. Chest. 1974;65:534–543.
59. The UKEP study: multicentre clinical trial on two local regimens of urokinase in massive pulmonary embolism. The UKEP Study Research Group. Eur Heart J. 1987;8:2–10.
60. McGinn S, White P. Acute cor pulmonale resulting from pulmonary embolism. JAMA. 1935;104:1473–1480.
61. Stein PD, Dalen JE, McIntyre KM, et al. The electrocardiogram in acute pulmonary embolism. Progr Cardiovasc Dis. 1975;17:247–257.
62. Stein PD, Terrin ML, Hales CA, et al. Clinical, laboratory, roentgenographic, and electrocardiographic findings in patients with acute pulmonary embolism and no pre-existing cardiac or pulmonary disease. Chest. 1991;100:598–603.
63. Ferrari E IA, Darcourt J. No scintigraphic evidence of myocardial abnormality in severe pulmonary embolism with electrocardiographic signs of anterior ischemia Eur Heart J. 1995;16(Suppl):269 abstract.
64. Stein PD, Athanasoulis C, Greenspan RH, et al. Relation of plain chest radiographic findings to pulmonary arterial pressure and arterial blood oxygen levels in patients with acute pulmonary embolism. Am J Cardiol. 1992;69:394–396.
65. Urokinase pulmonary embolism trial. Circulation. 1973;47(Suppl):1–108.
66. Stein PD, Goldhaber SZ, Henry JW, et al. Arterial blood gas analysis in the assessment of suspected acute pulmonary embolism. Chest. 1996;109:78–81.
67. Stein PD, Goldhaber SZ, Henry JW. Alveolar-arterial oxygen gradient in the assessment of acute pulmonary embolism. Chest. 1995;107:139–143.
68. Urokinase pulmonary embolism trial. Phase 1 results: a cooperative study. JAMA. 1970;214:2163–2172.
69. Alpert JS, Smith R, Carlson J, et al. Mortality in patients treated for pulmonary embolism. JAMA. 1976;236:1477–1480.
70. Meneveau N, Schiele F, Metz D, et al. Comparative efficacy of a two-hour regimen of streptokinase versus alteplase in acute massive pulmonary embolism: immediate clinical and hemodynamic outcome and one-year follow-up. J Am Coll Cardiol. 1998;31:1057–1063.
71. Mastora I, Remy-Jardin M, Masson P, et al. Severity of acute pulmonary embolism: evaluation of a new spiral CT angiographic score in correlation with echocardiographic data. Eur Radiol 2003;13:29–35.
72. Qanadli SD, El Hajjam M, Vieillard-Baron A, et al. New CT index to quantify arterial obstruction in pulmonary embolism: comparison with angiographic index and echocardiography. AJR Am J Roentgenol. 2001;176:1415–1420.
73. Ghaye B, Ghuysen A, Willems V, et al. Severe pulmonary embolism: pulmonary artery clot load scores and cardiovascular parameters as predictors of mortality. Radiology. 2006;239:884–891.
74. Come PC. Echocardiographic evaluation of pulmonary embolism and its response to therapeutic interventions. Chest. 1992;101 (Suppl):151S–162S.
75. Konstantinides S GA, Kasper W. Role of cardiac ultrasound in the detection of pulmonary embolism. Semin Respir Crit Care Med. 1996;17:39–49.
76. Torbicki A, Tramarin R, Morpurgo M. Role of echo/Doppler in the diagnosis of pulmonary embolism. Clin Cardiol. 1992;15:805–810.
77. Jardin F, Dubourg O, Bourdarias JP. Echocardiographic pattern of acute cor pulmonale. Chest. 1997;111:209–217.
78. Kasper W, Geibel A, Tiede N, et al. Distinguishing between acute and subacute massive pulmonary embolism by conventional and Doppler echocardiography. Br Heart J. 1993;70:352–356.
79. Kasper W, Geibel A, Tiede N, et al. Echocardiography in the diagnosis of lung embolism [in German]. Herz. 1989;14:82–101.
80. Mercat A, Diehl JL, Meyer G, et al. Hemodynamic effects of fluid loading in acute massive pulmonary embolism. Crit Care Med. 1999;27:540–544.
81. Angle MR, Molloy DW, Penner B, et al. The cardiopulmonary and renal hemodynamic effects of norepinephrine in canine pulmonary embolism. Chest. 1989;95:1333–1337.
82. Hirsch LJ, Rooney MW, Wat SS, et al. Norepinephrine and phenylephrine effects on right ventricular function in experimental canine pulmonary embolism. Chest. 1991;100:796–801.
83. Capellier G, Jacques T, Balvay P, et al. Inhaled nitric oxide in patients with pulmonary embolism. Intens Care Med. 1997;23:1089–1092.
84. Webb SA, Stott S, van Heerden PV. The use of inhaled aerosolized prostacyclin (IAP) in the treatment of pulmonary hypertension secondary to pulmonary embolism. Intens Care Med. 1996;22:353–355.
85. Tissue plasminogen activator for the treatment of acute pulmonary embolism. A collaborative study by the PIOPED investigators. Chest. 1990;97:528–533.
86. Jerjes-Sanchez C, Ramirez-Rivera A, de Lourdes Garcia M, et al. Streptokinase and heparin versus heparin alone in massive pulmonary embolism: a randomized controlled trial. J Thromb Thrombol. 1995;2:227–229.
87. Goldhaber SZ, Kessler CM, Heit JA, et al. Recombinant tissue-type plasminogen activator versus a novel dosing regimen of urokinase in acute pulmonary embolism: a randomized controlled multicenter trial. J Am Coll Cardiol. 1992;20:24–30.
88. Levine MN. Thrombolytic therapy for venous thromboembolism. Complications and contraindications. Clin Chest Med. 1995;16:321–328.
89. Dalen JE, Alpert JS, Hirsh J. Thrombolytic therapy for pulmonary embolism: is it effective? Is it safe? When is it indicated? Arch Int Med. 1997;157:2550–2556.
90. Arcasoy SM, Kreit JW. Thrombolytic therapy of pulmonary embolism: a comprehensive review of current evidence. Chest. 1999;115:1695–1707.
91. Verstraete M, Miller GA, Bounameaux H, et al. Intravenous and intrapulmonary recombinant tissue-type plasminogen activator in the treatment of acute massive pulmonary embolism. Circulation. 1988;77:353–360.
92. Podbregar M, Krivec B, Voga G. Impact of morphologic characteristics of central pulmonary thromboemboli in massive pulmonary embolism. Chest. 2002;122(3):973–979.
93. Wiegand UK, Kurowski V, Giannitsis E, et al. Effectiveness of end-tidal carbon dioxide tension for monitoring thrombolytic therapy in acute pulmonary embolism. Crit Care Med. 2000;28:3588–3592.
94. Meneveau N, Seronde MF, Blonde MC, et al. Management of unsuccessful thrombolysis in acute massive pulmonary embolism. Chest. 2006;129:1043–1050.
95. Agnelli G, Becattini C, Kirschstein T. Thrombolysis vs heparin in the treatment of pulmonary embolism: a clinical outcome-based meta-analysis. Arch Int Med. 2002;162:2537–2541.
96. Thabut G, Thabut D, Myers RP, et al. Thrombolytic therapy of pulmonary embolism: a meta-analysis. J Am Coll Cardiol. 2002;40:1660–1667.
97. Wan S, Quinlan DJ, Agnelli G, et al. Thrombolysis compared with heparin for the initial treatment of pulmonary embolism: a meta-analysis of the randomized controlled trials. Circulation. 2004;110:744–749.
98. Meneveau N, Ming LP, Seronde MF, et al. In-hospital and long-term outcome after sub-massive and massive pulmonary embolism submitted to thrombolytic therapy. Eur Heart J. 2003;24:1447–1454.
99. Aklog L. Emergency surgical pulmonary embolectomy. Semin Vasc Med. 2001;1:235–246.
100. Leacche M, Unic D, Goldhaber SZ, et al. Modern surgical treatment of massive pulmonary embolism: results in 47 consecutive patients after rapid diagnosis and aggressive surgical approach. J Thor Cardiovasc Surg. 2005;129:1018–1023.