Mutlu Gökhan M.
Mutlu Ece A.
Acute gastrointestinal (GI) bleeding is a common indication for admission to the intensive care unit (ICU) in the United States, with over 300,000 admissions per year (1). Most (75%) of these arise from the upper GI tract. Despite advances in critical care medicine, the mortality associated with upper GI bleeding has not changed and remains about 10%, likely due to aging of the population and increasing comorbidities (2,3). In this chapter, we will summarize the causes of upper GI bleeding, review the principles of a diagnostic approach, and outline the therapeutic modalities available for management of these patients. Last, we will provide an overview of stress-related mucosal damage.
Epidemiology
The annual incidence of hospital admission for upper GI bleeding in the United States is approximately 100 per 100,000 (1,4). The incidence is twice more common in males than females and increases with age. Patients rarely die from blood loss; rather, death is due to decompensation of other underlying conditions. Mortality for patients younger than 60 years in the absence of malignancy or organ failure is less than 1%.
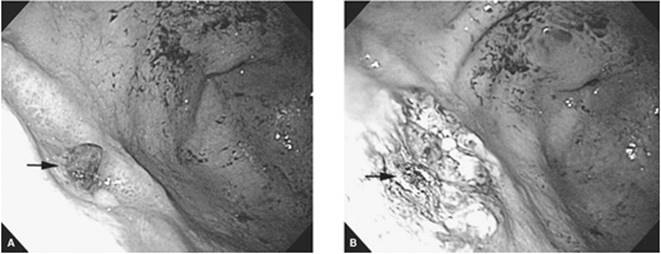
Peptic ulcer disease is the most common cause of upper GI bleeding, accounting for half of cases (5) (Table 152.1). There are four major risk factors for peptic ulcers, including nonsteroidal anti-inflammatory drugs (NSAIDs), Heliobacter pylori infection, stress, and gastric acid (6,7). Among ulcers, those in the duodenum are more common than those found in the stomach (gastric ulcers) (Fig. 152.1). Recent data showed a decline in the proportion of cases caused by peptic ulcer disease—down to 21%—with nonspecific mucosal abnormalities being the most common cause (42%) (8).
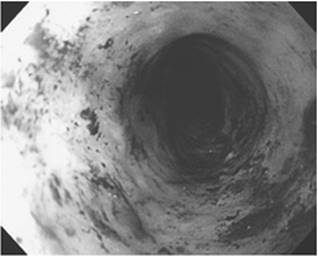
Mallory-Weiss tears account for 5% to 15% of cases, while the proportion of patients bleeding from varices varies widely, depending on the population, from about 5% to 30%. Hemorrhagic or erosive gastropathy (usually from NSAIDs or alcohol) and erosive esophagitis often cause mild upper GI bleeding, but major hemorrhage should not occur from erosions (Fig. 152.2). As the prevalence of H. pylori has decreased in developed countries and the use of NSAIDs has increased, the incidence of bleeding ulcers has decreased, and the proportion of bleeding ulcers due to NSAID—rather than H. pylori—has increased.
Esophagogastric varices are also a common cause of upper GI bleeding and usually develop as a consequence of systemic or segmental portal hypertension (Fig. 152.3). The development of massive bleeding from gastroesophageal varices is indicative of advanced liver disease, and liver transplantation is the only treatment that improves the long-term prognosis in these patients. Isolated gastric varices can occur due to segmental portal hypertension secondary to obstruction of the splenic vein or as a consequence of obliteration of esophageal varices with endoscopic intervention. Active variceal bleeding occurs in about 50% of patients with decompensated cirrhosis, accounting for about one third of all cirrhosis-related deaths. The outcome of an episode of active variceal hemorrhage depends on the control of active bleeding and the avoidance of complications associated with bleeding and its treatment. Establishing the correct diagnosis is also important.
Clinical Presentation
Upper GI bleeding commonly presents with hematemesis and/or melena. The clinical presentation provides clues pointing to the presence of upper GI bleeding. Hematemesis or coffee-ground emesis indicates an upper GI source of bleeding, which is above the ligament of Treitz, at the junction of the duodenum and jejunum. Melena suggests a minimum blood loss of 200 mL. The presence of melena is indicative of blood being present in the digestive tract for at least 12 to 14 hours. Although the more proximal the bleeding site in the upper GI tract, the more likely the patient will have melena, a significant percentage of patients with ascending colon sources of bleeding may also present with melena. Hematochezia is usually a presentation of lower GI bleeding, but an upper GI source that bleeds rapidly may also present with hematochezia (9). Patients with upper GI bleeding who have hematochezia usually have hemodynamic instability and rapidly dropping hemoglobin. Vomiting, retching, or coughing preceding hematemesis—especially in an alcoholic patient—should increase suspicion for a Mallory-Weiss tear. In addition to symptoms, a detailed history should include use of aspirin or other NSAID intake, alcohol consumption, presence of liver disease or variceal bleeding, history of peptic ulcer disease, weight loss, dysphagia, reflux, aortic aneurysm, or abdominal aortic vascular graft.
Diagnostic Evaluation
Gastric Lavage
Nasogastric lavage is important for confirmation of the diagnosis and may be predictive of a high-risk lesion if bright red blood is present in the lavage (10). A nasogastric tube may also decrease the risk of aspiration in patients with active hematemesis. A nonbloody nasogastric aspirate may be seen in up to 16% of patients with upper GI bleeding, usually if bleeding has ceased or if from a duodenal source, particularly if the pylorus is closed (11). Even the presence of bile in the aspirate is often (50%) misleading and does not necessarily rule out a postpyloric source of bleeding (11). Testing stool or emesis for blood during an acute episode of bleeding is not usually helpful (12). Testing of gastric contents can frequently be misleading because of nasogastric tube-related trauma. In addition, the low pH of gastric contents may interfere with the guaiac test's design for occult blood testing in stool, giving false results.
|
Table 152.1 Etiology of Upper Gastrointestinal Bleeding |
|
|
Laboratory evaluation may provide clues to the location of GI bleeding (upper versus lower). An elevated blood urea nitrogen (BUN)-to-creatinine ratio usually indicates an upper GI source as well as major blood loss (13). Patients without renal disease who have a BUN greater than 25 mg/dL have lost a minimum of 1 L of blood. Persistent azotemia (for more than 24 hours) is an indication of hypovolemia because volume loss contributes quantitatively more than the digestion of blood in raising BUN, and is the sole determinant of azotemia 24 hours after cessation of bleeding (14).
Amount of Blood Loss
Determination of estimated blood loss is the single, most important aspect of care in patients with upper GI bleeding. This estimation helps with the aggressiveness of volume resuscitation and triage to an appropriate level of care (i.e., transfer to ICU). Most complications associated with blood loss result from the adverse effects of hypovolemia and hemorrhagic shock on organs, and are compounded by the presence of pre-existing atherosclerosis or previous organ damage. Estimation of blood loss is often incorrect and requires an accurate assessment of vital signs, central venous pressure, hemoglobin and hematocrit, and a degree of clinical experience. Most of the indicators of clinically significant blood loss are derived from clinical data, which are summarized in Table 152.2.
Severe hemorrhage is usually defined as greater than 1,000 mL of blood loss. Initial hematocrit may be misleading due to loss of whole blood, which results in equal loss of plasma and erythrocytes. Redistribution of plasma from the extracellular to intravascular space, within 24 to 48 hours of the initial hemorrhage, results in dilution of red cell mass and a fall in hematocrit. The hematocrit fall may occur even more rapidly with volume replacement with crystalloid or nonheme colloid.
Physiologic changes in the cardiovascular system in response to blood loss are helpful in determining the severity of GI bleeding. Acute responses to blood loss represent a spectrum of changes, including resting tachycardia, orthostasis, peripheral vasoconstriction (cold, clammy skin), and acute end-organ dysfunction (mental status changes, oliguria). Chronic blood loss is usually associated with stable hemodynamic responses, retention of hypotonic fluid, and an absence of impaired organ function due to compensatory changes in the cardiovascular system. Many factors may impair or unmask normal responses to blood loss, including drugs, pre-existing dehydration, oxygen desaturation from pulmonary disease, the state of the cardiovascular system (particularly atherosclerotic cerebrovascular disease), abnormal concentration of plasma proteins, and miscellaneous conditions such as spinal cord disease, neuropathy, renal dysfunction, shock, and congestive heart failure.
Diagnostic Workup
Upper GI endoscopy is the diagnostic modality of choice for further evaluation of upper GI bleeding (5,15). Endoscopy helps in localization and identification of the bleeding lesion in the upper GI tract, and can be therapeutic in establishing hemostasis and preventing recurrent bleeding. Upper GI studies with radiocontrast material such as barium are contraindicated in the setting of acute upper GI bleeding due to interference with subsequent endoscopic intervention, angiography, and surgery (5).
Other diagnostic tests for workup of upper GI bleeding include angiography and tagged red blood cell scan (16). Angiographic diagnosis of the source of upper GI bleeding is made by extravasation of contrast material. The bleeding must be brisk, with a rate of about 0.5 to 1 mL/minute. Angiography can be helpful in establishing the diagnosis in 75% of patients; about 85% of bleeding originates from a branch of the left gastric artery (17). Nuclear medicine studies using 99mTc-pertechnetate-labeled red blood cell scan may also aid in localization of the bleeding site and has the ability to detect bleeding at lower rates (less than 0.5 mL/minute) than contrast angiography.
|
|
|
Figure 152.1. Peptic ulcer disease. Endoscopic view of a gastric ulcer with a visible vessel (arrow) before (A) and after (B) endoscopic intervention with gold probe cautery. |
Endoscopy is the diagnostic method of choice for esophagogastric varices. In cases where endoscopy is nondiagnostic and gastric variceal bleeding is suspected, studies such as endoscopic ultrasound, portal venography, or computed tomography (CT) angiography can be used. Cirrhotic patients with upper GI bleeding should be administered a prophylactic antibiotic—usually a fluoroquinolone—preferably prior to endoscopy (18,19).
|
|
|
Figure 152.2. Severe esophagitis. Endoscopic view of severe esophagitis. |
Predictors of Outcome and Risk Stratification
Three clinical parameters that are independent predictors of death and rebleeding are (i) hemodynamic instability, (ii) older age, and (iii) presence of comorbidities (Table 152.3). In addition to clinical features, endoscopic assessment provides further prognostic information and may guide subsequent management decisions.
Upper endoscopy should be performed as soon as possible in patients who present with hemodynamic instability because endoscopic intervention in patients with major bleeding may reveal high-risk findings, such as varices, ulcers with active bleeding, or visible vessel. On the contrary, early endoscopy increases costs without a change in outcomes in patients with low-risk clinical and endoscopic features. Thus, patients with clean-base ulcers, nonbleeding Mallory-Weiss tears, and erosive or hemorrhagic gastropathy who have no hemodynamic or hemoglobin instability and no other medical problems can be considered for discharge to home.
|
|
||
|
Figure 152.3. Esophageal varices. Endoscopic view of a large esophageal varix at the gastroesophageal junction. (Courtesy of Dr. Martin Cohen) |
||
|
Table 152.2 Clinical and Laboratory Determinants of Significant Blood Loss |
||
|
Risk stratification may be useful in that it may allow the identification of low-risk patients who can be managed safely without the need for hospitalization. Risk stratification of patients with upper GI bleeding can be done using clinical and laboratory data, and endoscopic findings (20). Endoscopic risk stratification depends on findings that predict the risk of rebleeding (20) (Table 152.4). Although several scoring systems based on these findings have been proposed, they have not been validated in large studies and, thus, are not routinely used in most centers (21,22,23,24,25,26).
Management
The initial evaluation of a patient with upper GI bleeding includes the assessment of hemodynamic stability and need for aggressive resuscitation, if necessary (27). Management of upper GI bleeding can be complex, requiring that additional complications associated with blood loss be considered, particularly if the latter is severe and associated with hemodynamic instability. Table 152.5 summarizes the general principles of management.
|
Table 152.3 Clinical Indicators of Significant Upper GI Bleeding |
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
Table 152.4 Endoscopic Findings That Predict Recurrent Upper GI Bleeding |
||||||||||||||||||||||||
|
||||||||||||||||||||||||
Hemodynamic Resuscitation
The initial management of upper GI bleeding should be directed at restoring blood/volume loss to maintain hemodynamic stability. Hemodynamic stabilization with adequate volume and blood resuscitation prior to endoscopic evaluation also helps to minimize treatment-associated complications (28). Intravenous access with two large-bore (14- to 16-gauge) catheters should be maintained at all times. In cases where peripheral intravenous (IV) catheters cannot be placed, a large-bore central line (9 to 12 French) should be inserted; triple-lumen catheters have one 16- and two 18-gauge ports and are long and should therefore be avoided due to unacceptably high resistance to flow. Hypovolemia and hypotension from GI blood loss should be treated promptly with fluid resuscitation using crystalloid and packed red blood cells (PRBCs).
|
Table 152.5 Principles of Treatment for Upper Gastrointestinal Bleeding |
||
|
All patients with hemodynamic instability or a hematocrit drop of more than 6%, a transfusion requirement greater than two units of PRBCs, or significant active bleeding as evidenced by continued hematemesis with bright red blood from gastric lavage or hematochezia should be admitted to ICU for close observation and resuscitation. High-risk patients, including the elderly or those with severe comorbidities such as ischemic heart disease or congestive heart failure, should be transfused to maintain their hemoglobin greater than 10 g/dL. On the contrary, unnecessary transfusion should be avoided in young, healthy individuals in whom maintenance of hemoglobin above 7 g/dL may be sufficient.
In hemorrhagic shock, close monitoring of end-organ perfusion (coronary, central nervous system, and renal) and preventing ischemic organ injury improves survival. In addition to a baseline electrocardiogram (ECG) and telemetry monitoring, urine output should be monitored continuously. In patients with massive hemorrhage or variceal bleeding, monitoring of preload via a central venous or pulmonary artery catheter may be useful; less invasive monitoring, including those devices using pulse-wave form variability (LidCO, PICCO, Flow Track) to evaluate preload, may also be useful in these situations.
Coagulopathy should be corrected as needed to maintain platelet count greater than 50,000 cells/µL and prothrombin time within 2 seconds of the upper level of normal. After replacement of factors and platelets, recombinant activated factor VII can rapidly correct severe coagulopathy in hepatic failure (29). Elective intubation should be considered in patients with ongoing hematemesis or altered mental status to facilitate endoscopy and decrease the risk of aspiration. Gastroenterology and, in cases of severe bleeding, surgery consultations should be requested (30).
Pharmacologic Treatment
Gastric Acid Suppression
Acid-suppressive therapy with proton pump inhibitors (PPI) is an essential adjunct to therapeutic endoscopy for management of patients with peptic ulcer disease–related upper GI bleeding (31). Acid suppression is beneficial, especially after endoscopic intervention (31,32). Other acid-suppressing agents, including H2-receptor antagonists (H2RA), have not been shown to reduce the rate of rebleeding or transfusion requirement in peptic ulcer disease (31,33,34,35). High-dose proton pump inhibitor infusion following a bolus injection significantly reduces the rate of rebleeding compared to standard therapy in patients with bleeding from peptic ulcer disease (31,36). It is unknown whether oral PPI will provide benefits similar to intravenous PPI. The superiority of PPI over H2RAs has been attributed to better maintenance of gastric pH above 6.0, which may lead to clot stabilization by prevention of fibrinolysis, and thus rebleeding (37). Current recommended doses of IV PPI therapy are lansoprazole, 90- to 120-mg bolus followed by 6 to 9 mg/hour infusion, and pantoprazole, 80 mg bolus followed by 8 mg/hour infusion. The infusion is usually continued for 48 to 72 hours and, if there is no further bleeding, switched to a twice daily dose.
Other Therapies
Splanchnic vasoconstrictors are important adjunct therapies to variceal hemorrhage. The current agent of choice in the United States is the somatostatin analogue, octreotide. Somatostatin and its analogues inhibit the release of vasodilator hormones such as glucagon, thereby indirectly causing splanchnic vasoconstriction and decreased portal inflow. For octreotide, the recommended dose is a 50-µg IV bolus followed by an infusion of 50 µg/hour for 5 days. Additionally, a longer-acting analogue of vasopressin, terlipressin, may also be used. Its efficacy is similar to octreotide and endoscopic sclerotherapy (38). Octreotide may also be considered as an adjunct therapy in the management of nonvariceal bleeding (39).
Cirrhotic patients with upper GI bleeding should be administered a prophylactic antibiotic—usually a fluoroquinolone—preferably prior to endoscopy (18,19). If a vasopressor is needed temporarily for the maintenance of blood pressure, medications that have β2-adrenergic activity, such as dopamine or albuterol, should be avoided due to potential risk of splanchnic vasodilation.
Endoscopic Treatment
Identification and hemostasis of the source of upper GI bleeding is critical in the patient's outcome. In cases for which hemodynamic stability can be established quickly with volume resuscitation, endoscopy can be performed within 24 hours. Emergent endoscopy with therapeutic intervention is needed in patients who remain hemodynamically unstable and continue to bleed (27,40,41).
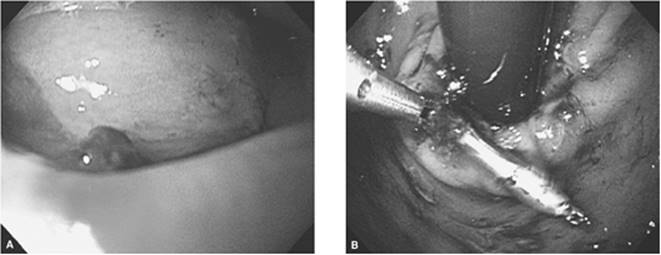
Several endoscopic therapeutic techniques have been developed to achieve hemostasis in nonvariceal upper GI bleeding, including thermal contact devices, bipolar electrocoagulation, heater probe, and injection therapy (epinephrine, alcohol, sclerosing agents such as polidocanol) (Fig. 152.4). The two most commonly used techniques in the United States are injection therapy with epinephrine (1:10,000) and contact thermal devices, which stop bleeding by producing vasoconstriction of bleeding vessels and coagulation, with subsequent destruction of bleeding vessels, respectively (42). Combination therapy with injection and thermal coagulation are superior to monotherapy in patients with major endoscopic stigmata such as active bleeding or adherent clot (43,44). Visible vessels should be treated with thermal coagulation, whereas endoscopic intervention is not required for low-risk lesions such as a clean-base ulcer or a flat spot.
Upper GI endoscopy is associated with potential complications, including aspiration, adverse reactions to conscious sedation, viscus perforation, and increased hemorrhage during therapeutic intervention. In patients with recent ischemic cardiac events, the risks of endoscopy may outweigh its benefits, and it should therefore be used judiciously (45). Contraindications to endoscopy include suspected GI perforation, unstable angina, severe coagulopathy, and severe agitation. Complications of endoscopic therapy include mucosal ulceration, motility abnormalities, stricture formation, esophageal perforation, and mediastinitis, as well as portal hypertensive gastropathy due to shunting of blood to the gastric mucosa.
|
|
|
Figure 152.4. Endoscopic management of upper gastrointestinal bleeding. Bleeding Dieulafoy lesion before (A) and after (B) endoscopic intervention (clipping). (Courtesy of Dr. Sri Komanduri) |
Nonvariceal Bleeding
Early therapeutic endoscopic intervention has an important role in achieving hemostasis, reducing rebleeding rates, and improving morbidity and mortality in peptic ulcer–related upper GI bleeding (27,40,46). One third of patients with active bleeding or a nonbleeding visible vessel require urgent surgery; further bleeding is possible if treated conservatively. These patients clearly benefit from endoscopic intervention with reduction in further bleeding, hospital stay, mortality, and costs; newer information suggests that higher-risk patients also benefit from PPI therapy (31). Patients with recurrent bleeding after endoscopic therapy were shown, in a randomized controlled trial, to have benefited from repeat endoscopic therapy. Most patients avoided surgery, and the rate of complication was significantly lower than in the group who underwent surgery (31).
Treatment of adherent clots is controversial. Two small endoscopic trials, which were terminated prematurely, showed better results with endoscopic therapy than conservative therapy (44,47). The control groups had a rebleeding rate of about 35%, whereas patients who were treated endoscopically had rebleeding rates of 0% (44) to 4.8% (47). Double-blind trials of PPI therapy without endoscopic therapy showed extremely low rates of recurrent bleeding (48,49). A recent meta-analysis showed marked heterogeneity among the trials, indicating that aggregating the trials for a summary statistic may not be appropriate. Nonetheless, the summary statistics did not show any significant benefit of endoscopic therapy. Vigorous irrigation to remove the clot may be recommended. If the clot is adherent, perhaps endoscopic therapy is not needed, but the use of a bolus plus a high-dose constant infusion of PPI may be used. Patients with underlying comorbidities may benefit from endoscopic intervention even if the clot is adherent.
A Mallory-Weiss tear is a self-limited disease and therefore does not usually require therapeutic intervention. Bleeding from these tears, which are usually on the gastric side of the gastroesophageal junction, stops spontaneously in 80% to 90% of patients, and recurs only in up to 5% of patients. Endoscopic intervention is effective in actively bleeding Mallory-Weiss tears but is not necessary if active bleeding is not present. Angiographic therapy with intra-arterial infusion of vasopressin or embolization may be useful. Rarely, surgery may be required to repair the tear. Massive bleeding can be seen if the Mallory-Weiss tear occurs in a patient with portal hypertension (50).
Variceal Bleeding
Compared to nonvariceal causes of upper GI bleeding, which stop spontaneously in 90% of cases, variceal bleeding subsides spontaneously in only 50% of patients. The mortality is very high, ranging between 70% and 80% in patients with continued variceal bleeding or rebleeding; each episode of bleeding is associated with a 30% risk of mortality (51). Variceal hemorrhage can predispose patients to hepatic encephalopathy, hepatorenal syndrome, and systemic infection, all of which increase the mortality in these patients. The risk of rebleeding remains high, ranging between 60% and 70%, unless endoscopic intervention is instituted to obliterate the varices. The greatest risk of rebleeding is within the first 48 to 72 hours, although it can occur as late as 6 weeks. Table 152.6 summarizes the risk factors for rebleeding from esophageal varices.
|
Table 152.6 Risk Factors for Early (less than 6 Weeks) Recurrent Variceal Bleeding |
|
|
Esophageal variceal bleeding is usually amenable to endoscopic therapy, which is done to cease blood flow through the venous collateral system in the distal esophageal mucosa and cardia. Cessation of blood flow and obliteration of varices is achieved by either sclerotherapy (induction of thrombosis) or band ligation (direct occlusion). Endoscopic band ligation is the procedure of choice based on the results from a meta-analysis that showed superiority of band ligation over sclerotherapy in initial hemostasis, rate of recurrent bleeding, complications, and mortality (52). Sclerotherapy may be indicated in cases where visualization is poor, but is usually followed by band ligation.
Unlike esophageal varices, endoscopic management of gastric varices is less effective due to deeper localization of varices in the submucosa. Injection of cyanoacrylate tissue glue and thrombin are promising therapies in the endoscopic management of gastric varices (53,54). These patients may usually require nonendoscopic therapies such as balloon tamponade (Sengstaken-Blakemore tube), transjugular portosystemic shunt (TIPS), and surgery. The TIPS procedure is done as salvage therapy to artificially create a portosystemic shunt to decompress the portal venous system and, consequently, variceal vasculature. It is recommended in patients with variceal bleeding refractory to pharmacologic and endoscopic therapy, regardless of the severity of cirrhosis.
Angiographic Treatment
In a few patients with nonvariceal upper GI bleeding, angiographic localization may be necessary, with the option of hemostasis using a vasoconstrictor (i.e., intra-arterial vasopressin) or embolization (i.e., gelatin sponge). Embolization carries the risk of bowel ischemia, infarction, and necrosis, which is seen less in the duodenum than in the stomach due to the dual circulation from celiac and superior mesenteric arteries.
Surgery
Surgical indications for the management of nonvariceal hemorrhage are life-threatening hemorrhage refractory to pharmacologic and endoscopic intervention, failure of medical therapy to resolve or prevent the recurrence of peptic ulcer disease, and related complications such as bleeding. The surgical procedure depends on the location of the ulcer and the clinical status of the patient. Mortality from surgical intervention for peptic ulcer disease can be as high as 30%.
The TIPS procedure has decreased the need for surgical shunt, which is indicated for patients with variceal hemorrhage and preserved hepatic synthetic function (55). Distal esophageal transaction, with or without devascularization, is another surgical option in patients with massive, refractory variceal hemorrhage, but is associated with high mortality.
Stress-Related Mucosal Damage
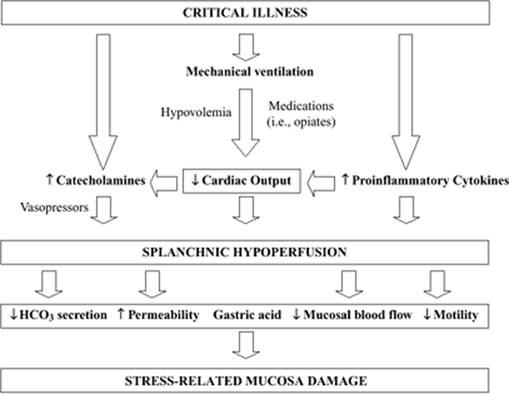
Upper GI bleeding, in addition to being a cause for admission to the ICU, can also develop as a complication of critical illness while the patient is being treated in the ICU. Stress-related mucosa damage (SRMD), also known as stress ulcers, occurs as a consequence of critical illness and is the most common cause of GI bleeding in the ICU (56). The critical care environment is characterized by invasive monitoring and vasoactive and other drugs that affect mesenteric perfusion and oxygen delivery. Additionally, positive pressure ventilation, particularly positive end-expiratory pressure, and conditions such as left heart failure and sepsis can have profound effects on GI epithelial function (56). Impaired splanchnic perfusion plays a pivotal role in the pathogenesis of SRMD (Fig. 152.5). The splanchnic vasculature lacks vasomotor autoregulation, leading to persistent vasoconstriction that continues even after resolution of hemodynamic instability. Gastric acid and pepsin also play a role in the pathogenesis.
Acute respiratory failure requiring mechanical ventilation for longer than 48 hours and coagulopathy are the two strongest independent risk factors for clinically significant GI bleeding due to SRMD (57,58). Mechanically ventilated patients almost invariably develop SRMD and subepithelial hemorrhage within 24 hours of admission to the ICU (59,60). SRMD occurs within a few hours of critical illness and can present as lesions ranging from subepithelial petechiae to superficial erosions that can progress into true ulcers (56). These lesions are usually multiple and occur predominantly in the fundus of the stomach, typically sparing the antrum (60).
Most SRMD lesions are asymptomatic and clinically insignificant, although some patients may develop clinically evident bleeding, presenting with hematemesis, coffee-ground emesis, melena, and hematochezia. Clinically evident bleeding due to SRMD occurs in up to 25% of critically ill patients who do not receive prophylactic therapy, with approximately 20%—corresponding to about 5% of all patients—having clinically significant bleeding, that is, associated with hemodynamic changes or necessitating transfusion (57,60,61). Clinically significant, SRMD-related bleeding is associated with an increased length of ICU stay and morbidity and mortality (62).
Treatment
The treatment of stress ulcer bleeding is supportive. Efforts should be focused on reversing the precipitating factors. Acid suppression with H2RA or PPIs is routinely used as adjunct therapy, given that luminal acidity is an essential factor in the pathogenesis of SRMD (63). Bleeding from SRMD is usually not amenable to endoscopic intervention because the lesions are diffuse. In cases of severe bleeding, endoscopy may be indicated and successful if hemorrhage is from one or several lesions. Since the gastric mucosa has a rich collateral blood supply, angiographic treatment—including embolization or intra-arterial vasopressin—may be considered for bleeding refractory to endoscopic therapy.
Prophylaxis
The incidence of stress ulcer bleeding has been decreasing as a result of more aggressive fluid resuscitation and prophylactic therapy (64). Most deaths in patients with stress ulcer bleeding are not due to GI hemorrhage. Therefore, the contribution of stress ulcer bleeding to overall ICU mortality does not appear to be significant in unselected ICU populations, and, as such, routine prophylaxis in all patients is not warranted. Identification of patients at risk for stress ulcer bleeding is more important than the particular medication used and can reduce unnecessary medication use and cost. Table 152.7 summarizes the risk factors for bleeding from stress ulcers.
|
|
|
Figure 152.5. Mechanisms important in the pathogenesis of stress-related mucosa damage. Splanchnic hypoperfusion leading to diminished mucosal blood flow and other changes in gastrointestinal epithelial function plays a pivotal role in development of stress ulceration. (Adapted from Mutlu GM, Mutlu EA, Factor P. GI complications in patients receiving mechanical ventilation. Chest. 2001;119[4]:1222–1241, with permission.) |
Although gastric acid production is not increased in the most critically ill patients, except those with increased intracranial pressure or severe burns, it is essential in the pathogenesis of SRMD, and thus, therapies targeting gastric acid have been the mainstay of prophylaxis. Medications that suppress gastric acid, such as H2RAs and PPIs, prevent SRMD by raising the gastric fluid pH, ideally above 4.0. Continuous infusion of H2RAs may provide more effective acid suppression compared to intermittent dosing, but the relevance of this practice remains unclear (65). Gastric pH-altering agents, as well as sucralfate, decrease the incidence of clinically significant bleeding by approximately 50%—the absolute rate decreases from about 4% to about 1.7% to 2%—and are effective in preventing clinically evident and significant stress ulcer bleeding (66,67). However, a more recent study showed the superiority of H2RAs over sucralfate in the prevention of SRMD-related bleeding (58).
|
Table 152.7 Risk Factors for Stress Ulcer Bleeding |
|
|
Theoretically, PPIs may provide better prophylaxis due to more consistent pH control; however, their superiority over H2RAs in stress ulcer prophylaxis has not been proven (68,69). In critically ill patients, IV PPI has been shown to achieve and maintain gastric pH greater than or equal to 4 within a few hours of initiation, with a progressive increase within the first 48 hours (70). The continuous administration of IV H2RA was not able to maintain pH control by day 2 despite achieving a gastric pH greater than or equal to 4 initially. However, there have been no large trials specifically investigating the role of IV PPI in SRMD prophylaxis or whether more consistent increases in pH translate into better outcomes. Both H2RAs and PPIs, despite a lack of strong clinical data, are the first-line drugs for stress ulcer prophylaxis, with the route of administration—oral versus IV—determined based on the availability of the GI tract.
The major concern about using pH-altering medications is their association with gastric colonization with the Enterobacteriaceae due to an increased gastric pH and subsequent retrograde gastro-oropharyngeal contamination resulting in an increased risk of ventilator-associated pneumonia (71,72,73). Based on available data, the risk of pneumonia attributable to pH-altering drugs can be minimized via the implementation of preventive measures such as maintenance of the semirecumbent position, avoidance of high gastric residuals, and the administration of tube feeds into the small bowel whenever possible (74,75).
Enteral feeding also decreases the risk of clinically evident GI bleeding (62,76,77). The beneficial effects of enteral feeding are probably multifactorial, including dilutional alkalinization of gastric fluid and mucosal cytoprotection through the restoration of gastric epithelial energy stores (62,78). However, due to limited data, the use of enteral nutrition as the sole “therapy” for stress ulcer prophylaxis should be discouraged. Initiation and discontinuation of pharmacologic prophylaxis should be independent of enteral nutrition.
Pearls
· Peptic ulcer disease is the most common cause of upper GI bleeding.
· Most (greater than 90%) nonvariceal upper GI bleeding subsides spontaneously.
· Hemodynamic resuscitation is critical for management of upper GI bleeding.
· Three clinical characteristics that are independent predictors of death and rebleeding of upper GI bleeding are hemodynamic instability, older age, and the presence of comorbidities.
· Endoscopy is the diagnostic modality of choice for further evaluation of upper GI bleeding.
· Early therapeutic endoscopic intervention plays an important role in achieving hemostasis, reducing the rebleeding rate, and improving morbidity and mortality in peptic ulcer–related upper GI bleeding.
· A high-dose infusion of proton pump inhibitor following a bolus injection significantly reduces the rate of rebleeding compared to standard therapy in patients with bleeding from peptic ulcer disease.
· Variceal bleeding subsides spontaneously in only 50% of patients.
· Mortality is very high—between 70% and 80%—in patients with continued variceal bleeding or rebleeding.
· The greatest risk of rebleeding is within the first 48 to 72 hours, although it can occur as late as 6 weeks.
· Splanchnic hypoperfusion plays a pivotal role in the pathogenesis of stress-related mucosal damage.
· Stress-related mucosal damage may occur in most critically ill patients within 24 hours of admission to the intensive care unit.
· Mechanical ventilation and coagulopathy are the most important risk factors for stress ulcer bleeding.
· Use of prophylaxis against stress-related mucosal damage should be restricted to critically ill patients with risk factors.
· The treatment of stress ulcer bleeding is supportive.
References
1. Zimmerman HM, Curfman K. Acute gastrointestinal bleeding. AACN Clin Issues. 1997;8(3):449–458.
2. Pitcher JL. Therapeutic endoscopy and bleeding ulcers: historical overview. Gastrointest Endosc. 1990;36(5 Suppl):S2–S7.
3. Farrell JJ, Friedman LS. Gastrointestinal bleeding in older people. Gastroenterol Clin North Am. 2000;29(1):1–36, v.
4. Longstreth GF. Epidemiology of hospitalization for acute upper gastrointestinal hemorrhage: a population-based study. Am J Gastroenterol. 1995;90(2):206–210.
5. Jutabha R, Jensen DM. Management of upper gastrointestinal bleeding in the patient with chronic liver disease. Med Clin North Am. 1996;80(5):1035–1068.
6. Hunt RH, Malfertheiner P, Yeomans ND, et al. Critical issues in the pathophysiology and management of peptic ulcer disease. Eur J Gastroenterol Hepatol. 1995;7(7):685–699.
7. Hallas J, Lauritsen J, Villadsen HD, Gram LF. Nonsteroidal anti-inflammatory drugs and upper gastrointestinal bleeding, identifying high-risk groups by excess risk estimates. Scand J Gastroenterol. 1995;30(5):438–444.
8. Boonpongmanee S, Fleischer DE, Pezzullo JC, et al. The frequency of peptic ulcer as a cause of upper-GI bleeding is exaggerated. Gastrointest Endosc. 2004;59(7):788–794.
9. Jensen DM, Machicado GA. Diagnosis and treatment of severe hematochezia. The role of urgent colonoscopy after purge. Gastroenterology. 1988;95(6):1569–1574.
10. Aljebreen AM, Fallone CA, Barkun AN. Nasogastric aspirate predicts high-risk endoscopic lesions in patients with acute upper-GI bleeding. Gastrointest Endosc. 2004;59(2):172–178.
11. Cuellar RE, Gavaler JS, Alexander JA, et al. Gastrointestinal tract hemorrhage. The value of a nasogastric aspirate. Arch Intern Med. 1990;150(7):1381–1384.
12. Schaffner J. Acute gastrointestinal bleeding. Med Clin North Am. 1986;70(5):1055–1066.
13. Felber S, Rosenthal P, Henton D. The BUN/creatinine ratio in localizing gastrointestinal bleeding in pediatric patients. J Pediatr Gastroenterol Nutr. 1988;7(5):685–687.
14. Stellato T, Rhodes RS, McDougal WS. Azotemia in upper gastrointestinal hemorrhage. A review. Am J Gastroenterol. 1980;73(6):486–489.
15. Adang RP, Vismans JF, Talmon JL, et al. Appropriateness of indications for diagnostic upper gastrointestinal endoscopy: association with relevant endoscopic disease. Gastrointest Endosc. 1995;42(5):390–397.
16. Barth KH. Radiological intervention in upper and lower gastrointestinal bleeding. Baillieres Clin Gastroenterol. 1995;9(1):53–69.
17. Irving JD, Northfield TC. Emergency arteriography in acute gastrointestinal bleeding. Br Med J. 1976;1(6015):929–931.
18. Soriano G, Guarner C, Tomas A, et al. Norfloxacin prevents bacterial infection in cirrhotics with gastrointestinal hemorrhage. Gastroenterology. 1992;103(4):1267–1272.
19. Hou MC, Lin HC, Liu TT, et al. Antibiotic prophylaxis after endoscopic therapy prevents rebleeding in acute variceal hemorrhage: a randomized trial. Hepatology. 2004;39(3):746–753.
20. Katschinski B, Logan R, Davies J, et al. Prognostic factors in upper gastrointestinal bleeding. Dig Dis Sci. 1994;39(4):706–712.
21. Rockall TA, Logan RF, Devlin HB, et al. Risk assessment after acute upper gastrointestinal haemorrhage. Gut. 1996;38(3):316–321.
22. Rockall TA, Logan RF, Devlin HB, et al. Selection of patients for early discharge or outpatient care after acute upper gastrointestinal haemorrhage. National Audit of Acute Upper Gastrointestinal Haemorrhage. Lancet. 1996;347(9009):1138–1140.
23. Kollef MH, O'Brien JD, Zuckerman GR, et al. BLEED: a classification tool to predict outcomes in patients with acute upper and lower gastrointestinal hemorrhage. Crit Care Med. 1997;25(7):1125–1132.
24. Corley DA, Stefan AM, Wolf M, et al. Early indicators of prognosis in upper gastrointestinal hemorrhage. Am J Gastroenterol. 1998;93(3):336–340.
25. Church NI, Dallal HJ, Masson J, et al. Validity of the Rockall scoring system after endoscopic therapy for bleeding peptic ulcer: a prospective cohort study. Gastrointest Endosc. 2006;63(4):606–612.
26. Bjorkman DJ, Zaman A, Fennerty MB, et al. Urgent vs. elective endoscopy for acute non-variceal upper-GI bleeding: an effectiveness study. Gastrointest Endosc. 2004;60(1):1–8.
27. Barkun A, Bardou M, Marshall JK. Consensus recommendations for managing patients with nonvariceal upper gastrointestinal bleeding. Ann Intern Med. 2003;139(10):843–857.
28. Baradarian R, Ramdhaney S, Chapalamadugu R, et al. Early intensive resuscitation of patients with upper gastrointestinal bleeding decreases mortality. Am J Gastroenterol. 2004;99(4):619–622.
29. Ejlersen E, Melsen T, Ingerslev J, et al. Recombinant activated factor VII (rFVIIa) acutely normalizes prothrombin time in patients with cirrhosis during bleeding from oesophageal varices. Scand J Gastroenterol. 2001;36(10):1081–1085.
30. Kolkman JJ, Meuwissen SG. A review on treatment of bleeding peptic ulcer: a collaborative task of gastroenterologist and surgeon. Scand J Gastroenterol. 1996;218(Suppl):16–25.
31. Lau JY, Sung JJ, Lee KK, et al. Effect of intravenous omeprazole on recurrent bleeding after endoscopic treatment of bleeding peptic ulcers. N Engl J Med. 2000;343(5):310–316.
32. Jensen DM, Cheng S, Kovacs TO, et al. A controlled study of ranitidine for the prevention of recurrent hemorrhage from duodenal ulcer. N Engl J Med. 1994;330(6):382–386.
33. Gisbert JP, Gonzalez L, Calvet X, et al. Proton pump inhibitors versus H2-antagonists: a meta-analysis of their efficacy in treating bleeding peptic ulcer. Aliment Pharmacol Ther. 2001;15(7):917–926.
34. Kaviani MJ, Hashemi MR, Kazemifar AR, et al. Effect of oral omeprazole in reducing re-bleeding in bleeding peptic ulcers: a prospective, double-blind, randomized, clinical trial. Aliment Pharmacol Ther. 2003;17(2):211–216.
35. Collins R, Langman M. Treatment with histamine H2 antagonists in acute upper gastrointestinal hemorrhage. Implications of randomized trials. N Engl J Med. 1985;313(11):660–666.
36. Lin HJ, Lo WC, Lee FY, et al. A prospective randomized comparative trial showing that omeprazole prevents rebleeding in patients with bleeding peptic ulcer after successful endoscopic therapy. Arch Intern Med. 1998;158(1):54–58.
37. Green FW, Kaplan MM, Curtis LE, et al. Effect of acid and pepsin on blood coagulation and platelet aggregation. A possible contributor prolonged gastroduodenal mucosal hemorrhage. Gastroenterology. 1978;74(1):38–43.
38. Escorsell A, Ruiz del Arbol L, Planas R, et al. Multicenter randomized controlled trial of terlipressin versus sclerotherapy in the treatment of acute variceal bleeding: the TEST study. Hepatology. 2000;32(3):471–476.
39. Imperiale TF, Birgisson S. Somatostatin or octreotide compared with H2 antagonists and placebo in the management of acute nonvariceal upper gastrointestinal hemorrhage: a meta-analysis. Ann Intern Med. 1997;127(12):1062–1071.
40. Rollhauser C, Fleischer DE. Ulcers and nonvariceal bleeding. Endoscopy. 1999;31(1):17–25.
41. ASGE Standards of Practice Committee. An annotated algorithmic approach to upper gastrointestinal bleeding. Gastrointest Endosc. 2001;53:853–858.
42. ASGE Technology Status Evaluation Report: Endoscopic hemostatic devices. Gastrointest Endosc. 2001;54:833–840.
43. Chung SS, Lau JY, Sung JJ, et al. Randomised comparison between adrenaline injection alone and adrenaline injection plus heat probe treatment for actively bleeding ulcers. BMJ. 1997;314(7090):1307–1311.
44. Jensen DM, Kovacs TO, Jutabha R, et al. Randomized trial of medical or endoscopic therapy to prevent recurrent ulcer hemorrhage in patients with adherent clots. Gastroenterology. 2002;123(2):407–413.
45. Cappell MS, Iacovone FM Jr. Safety and efficacy of esophagogastroduodenoscopy after myocardial infarction. Am J Med. 1999;106(1):29–35.
46. Laine L, Peterson WL. Bleeding peptic ulcer. N Engl J Med. 1994;331(11):717–727.
47. Bleau BL, Gostout CJ, Sherman KE, et al. Recurrent bleeding from peptic ulcer associated with adherent clot: a randomized study comparing endoscopic treatment with medical therapy. Gastrointest Endosc. 2002;56(1):1–6.
48. Sung JJ, Chan FK, Lau JY, et al. The effect of endoscopic therapy in patients receiving omeprazole for bleeding ulcers with nonbleeding visible vessels or adherent clots: a randomized comparison. Ann Intern Med. 2003;139(4):237–243.
49. Khuroo MS, Yattoo GN, Javid G, et al. A comparison of omeprazole and placebo for bleeding peptic ulcer. N Engl J Med. 1997;336(15):1054–1058.
50. Schuman BM, Threadgill ST. The influence of liver disease and portal hypertension on bleeding in Mallory-Weiss syndrome. J Clin Gastroenterol. 1994;18(1):10–12.
51. Smith JL, Graham DY. Variceal hemorrhage: a critical evaluation of survival analysis. Gastroenterology. 1982;82(5 Pt 1):968–973.
52. Laine L, Cook D. Endoscopic ligation compared with sclerotherapy for treatment of esophageal variceal bleeding. A meta-analysis. Ann Intern Med. 1995;123(4):280–287.
53. Lo GH, Lai KH, Cheng JS, et al. A prospective, randomized trial of butyl cyanoacrylate injection versus band ligation in the management of bleeding gastric varices. Hepatology. 2001;33(5):1060–1064.
54. Yang WL, Tripathi D, Therapondos G, et al. Endoscopic use of human thrombin in bleeding gastric varices. Am J Gastroenterol. 2002;97(6):1381–1385.
55. Henderson JM, Nagle A, Curtas S, et al. Surgical shunts and TIPS for variceal decompression in the 1990s. Surgery. 200;128(4):540–547.
56. Mutlu GM, Mutlu EA, Factor P. GI complications in patients receiving mechanical ventilation. Chest. 2001;119(4):1222–1241.
57. Schuster DP, Rowley H, Feinstein S, et al. Prospective evaluation of the risk of upper gastrointestinal bleeding after admission to a medical intensive care unit. Am J Med. 1984;76(4):623–630.
58. Cook D, Guyatt G, Marshall J, et al. A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. N Engl J Med. 1998;338(12):791–797.
59. Lucas CE, Sugawa C, Riddle J, et al. Natural history and surgical dilemma of “stress” gastric bleeding. Arch Surg. 1971;102(4):266–273.
60. Peura DA, Johnson LF. Cimetidine for prevention and treatment of gastroduodenal mucosal lesions in patients in an intensive care unit. Ann Intern Med. 1985;103(2):173–177.
61. Gurman G, Samri M, Sarov B, et al. The rate of gastrointestinal bleeding in a general ICU population: a retrospective study. Intensive Care Med. 1990;16(1):4449.
62. Cook D, Heyland D, Griffith L, et al. Risk factors for clinically important upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. Crit Care Med. 1999;27(12):2812–2817.
63. Skillman JJ, Gould SA, Chung RS, et al. The gastric mucosal barrier: clinical and experimental studies in critically ill and normal man, and in the rabbit. Ann Surg. 1970;172(4):564–584.
64. Haglund U. Stress ulcers. Scand J Gastroenterol Suppl. 1990;175:27–33.
65. Baghaie AA, Mojtahedzadeh M, Levine RL, et al. Comparison of the effect of intermittent administration and continuous infusion of famotidine on gastric pH in critically ill patients: results of a prospective, randomized, crossover study. Crit Care Med. 1995;23(4):687–691.
66. Cook DJ, Witt LG, Cook RJ, et al. Stress ulcer prophylaxis in the critically ill: a meta-analysis. Am J Med. 1991;91(5):519–527.
67. Cook DJ, Reeve BK, Guyatt GH, et al. Stress ulcer prophylaxis in critically ill patients. Resolving discordant meta-analyses. JAMA. 1996;275(4):308–314.
68. Levy MJ, Seelig CB, Robinson NJ, et al. Comparison of omeprazole and ranitidine for stress ulcer prophylaxis. Dig Dis Sci. 1997;42(6):1255–1259.
69. Kantorova I, Svoboda P, Scheer P, et al. Stress ulcer prophylaxis in critically ill patients: a randomized controlled trial. Hepatogastroenterology. 2004;51(57):757–761.
70. Morris JA, Karlstadt R, Blatcher D, et al. Intermittent intravenous pantoprazole rapidly achieves and maintains gastric pH ≥4 compared with continuous infusion H2-receptor antagonist in intensive care unit. Crit Care Med 31st Annual congress of the Society of Critical Care Medicine (SSCM) 26-30 January, 2002, San Diego, CA. 30:Abstract 143.
71. Heyland D, Mandell LA. Gastric colonization by Gram-negative bacilli and nosocomial pneumonia in the intensive care unit patient. Evidence for causation. Chest. 1992;101(1):187–193.
72. du Moulin GC, Paterson DG, Hedley-Whyte J, et al. 1982. Aspiration of gastric bacteria in antacid-treated patients: a frequent cause of postoperative colonisation of the airway. Lancet. 1982;1(8266):242–245.
73. Craven DE, Steger KA, Barat LM, et al. Nosocomial pneumonia: epidemiology and infection control. Intensive Care Med. 1992;18(Suppl 1):S3–S9.
74. Kollef MH. Ventilator-associated pneumonia. A multivariate analysis. JAMA. 1993;270(16):1965–1970.
75. Drakulovic MB, Torres A, Bauer TT, et al. 1999. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial. Lancet. 1999;354(9193):1851–1858.
76. Pingleton SK, Hadzima SK. Enteral alimentation and gastrointestinal bleeding in mechanically ventilated patients. Crit Care Med. 1983;11(1):13–16.
77. Raff T, Germann G, Hartmann B. The value of early enteral nutrition in the prophylaxis of stress ulceration in the severely burned patient. Burns. 1997;23(4):313–318.
78. Ruiz-Santana S, Ortiz E, Gonzalez B, et al. Stress-induced gastroduodenal lesions and total parenteral nutrition in critically ill patients: frequency, complications, and the value of prophylactic treatment. A prospective, randomized study. Crit Care Med. 1991;19(7):887–891.