Michael J. Murray
Eric L. Bloomfield
Perspective
Anxiety is one of the human emotions that help us anticipate and prepare for real or perceived threats. Anxiety results in the release of endogenous catecholamines with an accompanying increase in heart rate, blood pressure, tremulousness, and so on. In some critically ill patients, anxiety can lead to agitation, i.e., anxiety coupled with confusion and movement and, if the confusion is severe enough, delirium. Increasingly, there is recognition that the spectrum of anxiety, agitation, and delirium may be a manifestation of the effects of the systemic inflammatory response syndrome (SIRS) and multiple organ dysfunction syndrome (MODS), with the brain being the end organ affected. With this recognition of the significance of anxiety has come an increasing attention to monitoring its severity, as well as treatment and assessment of the effects of therapy.
The lung is the most frequently injured organ in patients with MODS, resulting in acute respiratory distress syndrome (ARDS) or acute lung injury (ALI). Patients with ALI and ARDS require intubation and mechanical ventilation, and, with modes of mechanical ventilation adjusted to deliver low tidal volumes with resultant hypercarbia, patients are more likely to become agitated. In such patients in whom sedation is inadequate, neuromuscular blocking agents (NMBAs) may be required. These medications should always be administered cautiously, with daily drug “holidays,” which permit the clinician caring for the patient to determine if the NMBA is still required.
Features
Anxiety
Anxiety is often described as a heightened sense of awareness, apprehension, dread, or anticipation. The latter is an important characteristic, for anxiety is an emotional state; the individual “anticipates” a threat, and anxiety prepares the individual for “fight or flight.” Anxiety has its anatomic construct in the limbic system and is associated with the release of catecholamines, which lead to the tremulousness, sweating, tachycardia, and tachypnea—all the hallmarks of anxiety. In its extreme, an individual may have a “panic attack.”
Oftentimes when clinicians round on patients in the ICU, they find a patient who looks distressed, and blood pressure and heart rate are elevated. We commonly assume that the patient is in pain, and yet frequently, anxiety is the problem. Interestingly, the easiest way to separate these two perceptions is to ask the patient. As part of the daily evaluation of patients in the ICU, they should be asked if they are anxious, if they are in pain, and if they are “getting enough air to breathe?” The latter two complaints are likely to exacerbate anxiety, along with several other experiences that ICU patients may have (Table 63.1). The treatment for pain and anxiety are often the same, but for patients without pain, the treatment algorithm is different (see below). However, anxiety and pain are often a continuum, with the perception of one increasing the perception of the other.
Anxiety may lead to insomnia, a common problem in the ICU, and insomnia (and sleep deprivation) can increase the perception of anxiety (1). Sleep interruption occurs for several reasons, starting with excessive noise levels in many ICUs at night, patient care activities, measurement of vital signs, laboratory tests, radiographs, and so on. Patients who are intubated and mechanically ventilated are even more likely to have interrupted sleep, along with experiencing discomfort from the mode of mechanical ventilation and/or tracheal suctioning, as well as hypercarbia and hypoxia. In surveys of patients discharged from the ICU, patients recall feelings of terror, nervousness, and insomnia (2). Older patients, because they have less organ reserve, are more at risk of developing problems; depending on the extent of chronic health problems, the acute illness, and medications the patients receive, they are more at risk of cognitive dysfunction (3), which increases the risk of developing agitation and delirium (4).
Agitation
In the 2001 Agitation Consensus Conference, agitation was described as “continual movement characterized by constant fidgeting, moving from side to side, pulling at dressings and bed sheets, and attempting to remove catheters or other tubes” (5). Agitation is associated with some degree of cognitive impairment—disorientation, confusion, confabulation, and so on. Agitation is different from anxiety because the agitated patient displays purposeless movement and has some degree of cognitive dysfunction. For the reasons mentioned about removal of invasive devices, agitated patients are at risk of injuring themselves and, in some circumstances, injuring health care providers. Factors associated with agitation (6) include advanced age, neuropsychiatric comorbidities, seriousness of illness, pain, and some drugs that, when given to ICU patients, have unrecognized interactions and side effects. Agitation is associated with an increased length of stay, iatrogenic infections, and self-extubation (6). Many believe that prolonged anxiety, depending on the cause, if left untreated, can lead to agitation (5). Most of the tools to monitor agitation and the effects of therapeutic interventions are listed in Table 63.2 (7,8,9,10,11,12). However, because patient movement is one of the hallmarks of agitation, some clinicians use a variant of the Ramsay Sedation Scale and the Motor Activity Assessment Scale (Table 63.3) to monitor for agitation (13).
|
Table 63.1 Experiences That Increase Patient Anxiety in the Intensive Care Unit |
||||||||||||
|
Delirium
The hallmark of delirium is cognitive dysfunction, most commonly manifested as disorientation in a patient who is critically ill. In the past, such patients were diagnosed as having “ICU syndrome,” a diagnosis of exclusion. Heightened awareness has resulted in several studies that have examined the prevalence (14), types (15), consequences (16), and the diagnosis and management (17) of delirium.
In a coronary care unit, the prevalence of delirium can run as low as 7% (14), whereas in a medical ICU, it may run as high as 70% to 80% (15). Delirious patients may manifest a variety of psychomotor behavior, from hypoactive (listlessness) to hyperactive (combative behavior), with a mixed picture also seen (15). Independent of the motor type, the delirious patient is at risk for developing long-term cognitive impairment (18), a greater length of ICU and hospital stay, and an increased mortality (16). Patients frequently cycle between overly sedated states to hyperactive, agitated states. Management can be difficult, as some medications commonly given to sedate patients have also been associated with an increased incidence of delirium (19).
|
Table 63.2 Sedation Scales |
|||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||
|
Table 63.3 Motor Activity Assessment Scale |
|||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||
Anxiety, agitation, and delirium require recognition (20) and education of health care professionals (17) so we can identify at-risk patients and improve treatment.
Evaluation
Although anxiety is a valid emotional response to hospitalization in an ICU, an overexuberant response to the stressors in the ICU environment can be detrimental. Anxious patients have an increase in the incidence of several disease states/processes (Table 63.4) (21,22,23,24,25).
Patients should be examined on a daily basis, particularly to look for certain signs that increase the likelihood of anxiety (Table 63.5). The laboratory evaluation (Table 63.6) is also helpful in determining if the patient is, indeed, hypercapnic, septic, or has increased or decreased concentrations of electrolytes in the blood that often correlate with an increased risk of neurologic dysfunction.
|
Table 63.4 Anxiety Associated with an Increased Incidence of Several Disease States/Processes |
|
|
|
|
Table 63.5 Physical Examination |
|
|
|
Table 63.6 Laboratory Evaluation |
||
|
||
|
Table 63.7 Nonpharmacologic Therapy for Anxiety-Producing Events |
||
|
|
Table 63.8 Therapy for Anxiety-Producing Events |
|
|
When a patient admits to excessive anxiety, one should first attempt to decrease the anxiety through nonpharmacologic means (Table 63.7) (26,27,28). First and foremost is the recognition that the environment in the ICU must be calm and nurturing, with attention to such details as room temperature, noise levels, and sleep disturbance—the bane of most modern ICUs.
Approximately 60% to 70% of patients who reside in the ICU for greater than 48 hours will require pharmacologic therapy (Table 63.8). Of the possible agents, opioids, benzodiazepines, haloperidol, propofol, and dexmedetomidine are the mainstays of treatment.
Treatment
Nonsteroidal Anti-inflammatory Drugs
Nonsteroidal anti-inflammatory drugs (NSAIDs) do not have sedative properties, but to the extent that they decrease pain, they do decrease pain-associated anxiety. NSAIDs would most likely be contraindicated in ICU patients because of their side effects. However, when cyclo-oxygenase (COX)-2 inhibitors, which have fewer side effects, are coupled with gabapentin or its precursor, pregabalin, they have analgesic and sedative properties if given preoperatively per os to patients who are anticipated to be admitted postoperatively to the ICU. In one study, a combination of 400 mg of celecoxib and 150 mg of pregabalin improved patients' sedation levels by approximately 33% for up to 24 hours postoperatively (29).
Opioids
Because pain or discomfort (from tracheal tube suctioning, nasogastric tubes, or Foley catheters) is a frequent, confounding factor for anxious patients, analgesics are often administered, usually via continuous intravenous infusions. Importantly, opioids have not only analgesic but also anxiolytic properties (30). Morphine has anxiolytic properties, but is not nearly as effective as newer opioids, and, because of the buildup of active metabolites in patients with renal insufficiency, it is not recommended for patients in the ICU. Fentanyl and remifentanil are over 90% effective in providing adequate sedation for intubated and mechanically ventilated patients in the ICU (31). Because of equal efficacy and differences in cost, fentanyl is recommended in most patients, except those with significant renal/hepatic impairment (Table 63.9).
|
Table 63.9 Opioids as Sedative Drugs in the Intensive Care Unit |
||||||||||||
|
||||||||||||
Benzodiazepines
Benzodiazepines, which potentiate the effects of gamma-aminobutyric acid via the benzodiazepine receptor and suppress central nervous system (CNS) activity (32), are administered to provide sedation in the ICU. They were observed to have sedative properties in animals (33), which led to their use because of their hypnotic, muscle-relaxant, anticonvulsive, and antegrade and variable retrograde amnestic properties. The benzodiazepines do not have analgesic properties, but similar to the opioids, they can and do produce respiratory depression in a dose-dependent fashion.
In critically ill patients, many of whom have MODS, because benzodiazepines are metabolized in the liver with the metabolites excreted by the kidneys, the half-lives (t½) are prolonged, and active metabolites may accumulate. Most commonly, benzodiazepines are administered by continuous infusion, so the context-sensitive t½ is more germane but independent of the method of administration because of the potential prolonged effect; a daily “off” period should be established to avoid overdosage (see below). The most commonly used benzodiazepines in the ICU are diazepam, midazolam, and lorazepam (Table 63.10).
Diazepam
Diazepam is an effective sedative-hypnotic with amnestic properties. Because diazepam is irritating when injected intramuscularly or intravenously and due to its long half-life, it is not often administered in the ICU.
Lorazepam
Lorazepam is an intermediate-acting benzodiazepine with a t½ of 10 to 12 hours. Respiratory and cardiovascular effects of lorazepam are no different than those for diazepam and midazolam. Lorazepam is recommended for long-term (greater than 24 hours) administration for patients who are critically ill (34). This may seem surprising because of its t½, but because its metabolites have no clinical activity and there is less intraindividual variability (35), recovery from lorazepam, compared to midazolam, following long-term administration is no different (36) and is associated with pharmacoeconomic benefits (37).
Midazolam
Midazolam is the shortest acting of those benzodiazepines used in the ICU, with a t½ of 1 to 5 hours. Midazolam causes no pain or phlebitis following intravenous administration and is two to four times more potent than diazepam. These characteristics make midazolam an ideal drug for continuous intravenous infusion, as it has rapid onset and relatively rapid offset. It is recommended for short-term use (34); long-term (>24–48 hours) use is problematic because gamma-hydroxy midazolam, the main metabolite, with sedative properties almost identical to the parent compound, accumulates in critically ill patients with decreased albumin levels and decreased renal function, leading to prolonged sedation once the infusion is discontinued. Typically, when administering midazolam for anxiolysis or sedative-hypnotic reasons, 1-mg increments are given intravenously as a bolus, with repeated boluses administered every 5 minutes to effect. A continuous infusion of 0.5 to 5 mg/hour can then be started and continued for as long as necessary.
|
Table 63.10 Benzodiazepines Used for Anxiolysis in the Intensive Care Unit |
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
Additional Cautions and Recommendations Regarding Benzodiazepine Use
The United States Food and Drug Administration (FDA) has administered black box warnings for benzodiazepines to the effect that anyone administering these respiratory depressants must be skilled in airway management and resuscitation. Similarly, one must have the benzodiazepine antagonist flumazenil—a drug that reverses all known CNS effects of benzodiazepines—available in the ICU. Flumazenil has maximum effect within 5 to 10 minutes after intravenous administration and has a mean t½ of approximately 1 hour. Typically, it is given in 0.1- to 0.2-mg increments, repeated every 5 to 10 minutes, to a total dose of 1 mg. Because of the active metabolites of diazepam and midazolam, these benzodiazepines should be used with extra caution in patients with renal insufficiency, as the active metabolites will accumulate. Furthermore, although these medications are often given as intravenous infusions, because of the increasing emphasis on cost efficacy in our ICUs, patients who are able to take medications per os should, when feasible, have their intravenous medication discontinued and an oral benzodiazepine started (38).
Furthermore, despite the guidelines that have previously been established (34), not all studies have shown a benefit of lorazepam compared to midazolam for long-term administration; Barr et al. (39) found in 24 patients that those who received midazolam for greater than 72 hours had emergence times from their drug-induced hypnotic state that were shorter than those patients who received lorazepam. Additional research in this area of finding the best short-term and long-term sedative agents is recommended (40).
It is further recommended and supported by clinical studies that patients who are on long-term (greater than 24 hours) infusions of benzodiazepines benefit from a daily drug “holiday” (41), i.e., infusion stopped typically every morning around 7:00 or 8:00 a.m., and the infusion remains off until the patient exhibits symptoms or signs that warrant restarting the infusion. The possibility of overdosing is decreased if patients are assessed on a regular basis for their degree of sedation. There are several tools that can be used to monitor the adequacy of sedation, beginning with the Ramsey Sedation Scale (Table 63.11) (9), although there are several others that may be more comprehensive (Table 63.2) (7,8,9,10,11,12).
|
|
|
Table 63.11 Ramsey Sedation Scale |
The team that manages patients in the ICU who require intravenous administration of benzodiazepines should follow a protocol for the administration of these drugs and use a tool with which they are familiar to monitor the degree of sedation. As a final caveat, once these medications are completely discontinued, up to one third of the patients will exhibit signs of withdrawal (42). In these patients, it is common practice to discontinue the benzodiazepines slowly over several days, treating the side effects of withdrawal—tachycardia and hypertension—with a beta-blocker or an alternative drug, including chronic low doses of benzodiazepines in those patients in whom beta-blockers are contraindicated.
Propofol
Propofol (di-isopropylphenol) is a highly lipophilic compound formulated in an isotonic oil in water emulsion (Intralipid) that is unrelated to other sedative/anesthetic agents (43). Because it is formulated in lipid emulsion, side effects include hypertriglyceridemia and bacterial contamination of infusions. The addition of ethylenediaminetetraacetic acid (EDTA) or bisulfite as preservatives decreases the incidence of bacterial overgrowth. A rare side effect is the propofol infusion syndrome (44), metabolic acidosis, and ventricular fibrillation in children and in young adults with neurologic injury receiving greater than 100 µg/kg per minute of propofol for greater than 12 to 24 hours. Propofol is now probably the most commonly used intravenous anesthesia induction agent, and is being advocated by some for use in moderate sedation (endoscopy suite) protocols (45). Because of its rapid onset and offset, few residual aftereffects, and low side-effect profile, it is often used for short-term sedation in the ICU. As the cost of the product has decreased, it is more commonly administered for long-term sedation in the ICU. Propofol has no analgesic properties, so for patients with pain, an analgesic drug should be coadministered. Propofol has also been used to treat status epilepticus (46) and to induce sleep in the ICU (47).
Dexmedetomidine
Alpha-2 (α2) agonists, such as methyldopa and clonidine, have long been known to have sedative properties; in fact, clonidine is administered epidurally for its antinociceptive effects in the spinal cord. Dexmedetomidine is an α2 agonist that acts by binding to α2 receptors in the locus ceruleus with a high α2/α1 ratio of approximately 1,620:1, approximately seven times more avidly than clonidine. Binding to the α2 receptor releases norepinephrine and decreases sympathetic activity; the net effect is sedation, analgesia, and amnesia. Dexmedetomidine is unique compared to the other anxiolytic drugs because patients are not only calm but appear to be sleeping (48). It is commonly used to sedate patients following cardiac surgery (49) and after neurosurgical procedures (50). Whether it is superior to propofol for these patients has not been determined (51). Patients who abuse alcohol, cocaine, and marijuana may benefit the most because dexmedetomidine treats many of the symptoms and signs of withdrawal (52). Many clinicians prefer dexmedetomidine to opioids or benzodiazepines because it is not associated with respiratory depression. However, because of its central alpha agonist, hypotension can and does occur. Fortunately, low-dose dexmedetomidine (6 µg/kg per hour for 10 minutes followed by an infusion of 0.2 µg/kg per hour) is as effective as higher doses (0.6 µg/kg per hour), with fewer side effects (48,53). There is concern that if dexmedetomidine is used for greater than 24 hours and discontinued abruptly, that a hyperdynamic state will ensue similar to the one that develops when clonidine is stopped abruptly following long-term use; but cases of cardiac arrest, though reported, are uncommon. Dexmedetomidine has been approved by the FDA for 24-hour use (54), although many clinicians are using it for longer than 24 hours. Of the currently used anxiolytic medications, dexmedetomidine is the most expensive.
Butyrophenones
Butyrophenones are neuroleptic drugs that are also known as antipsychotic drugs or major tranquilizers. They induce apathy, a state of mental detachment in patients with psychoses or delirium. By inhibiting dopamine-mediated neurotransmissions in the CNS, they decrease the frequency of hallucinations, delusions, and other abnormal thoughts. Patients become so detached from their environment that they develop a characteristic flat affect. Butyrophenones are active in the chemoreceptor trigger zone in the brainstem and thus are effective antiemetics; they are also used to treat hiccups and are used as synergistic anxiolytic drugs when used with benzodiazepines.
Of the butyrophenones, haloperidol is the drug used most often to treat delirium in the ICU. Haloperidol has a wide therapeutic margin but has important side effects including hypotension, extrapyramidal symptoms, anticholinergic effects (tachycardia, urinary retention, ileus), neuroleptic malignant syndrome, and seizures. These side effects are rare. Hypotension following a dose of haloperidol is almost always seen in patients who are hypovolemic. Extrapyramidal symptoms are more often seen in younger patients and in patients with depleted dopamine stores, e.g., patients with Parkinson disease.
The initial dose of haloperidol is usually 0.5 to 2 mg administered parenterally, although depending on the patient's size, age, and degree of agitation/delirium, 5 mg can be given. Haloperidol has a slow onset, so peak effects may not be seen for 15 to 30 minutes. Repeat doses then should be administered at 30- to 60-minute intervals. Recurrence of agitation or an increase in delirium is an indication for repeat doses, which may be increased if the initial dose was inadequate. Tardive dyskinesia or neuroleptic malignant syndrome can occur even during the short duration of therapy used in the ICU.
Haloperidol, because of its anticholinergic effects, may prolong the QT in a dose-dependent fashion, resulting in arrhythmias and torsades de pointes. Patients receiving haloperidol should have their electrocardiogram monitored.
A recent retrospective study of 989 patients who were mechanically ventilated in the ICU found that those patients who received haloperidol had significantly lower mortality than those who did not (55). Although not an indication for increased use of haloperidol, the results should be reassuring to those who have concerns about its use.
Other Agents
Several anesthetic agents have been tried to sedate patients in the ICU, with unanticipated results. When nitrous oxide was used, anemia developed and led to the realization that nitrous oxide interfered with vitamin B12 metabolism. Similarly, when etomidate was used for sedation, patients developed adrenocortical insufficiency because we now know that etomidate interferes with cortisol metabolism. However, a few anesthetic agents have withstood the test of time with respect to their use in the ICU.
Barbiturates
Barbiturates have pronounced effects on the CNS, lowering intracranial pressure and raising the seizure threshold. They have been used in the past to induce a “barbiturate coma” in patients with increased intracranial pressure and terminate seizures. Barbiturates administered by intravenous bolus produce hypotension and because of their lipid solubility, if given by continuous infusion, accumulate in fat stores and, therefore, have a duration of action that can be significantly long, i.e., days to weeks. In current practice, they are infrequently administered by continuous infusion for long-term use.
Ketamine
Ketamine is a phencyclidine derivative that is a nonbarbiturate, rapid-acting, general anesthetic that is administered parenterally to induce anesthesia. Ketamine induces “dissociative anesthesia” because it interrupts association pathways of the brain before blocking sensory pathways—patients may perceive pain, but it does not bother them. However, because it is a phencyclidine derivative, 10% to 20% of adult patients may have psychologic sequelae including hallucinations.
Ketamine is used as a general anesthetic because it raises cardiac output, pulse rate, and arterial and venous pressures. Ketamine maintains pharyngeal and laryngeal reflexes without suppressing respiration. Ketamine is also a bronchodilator and has been advocated as the anesthetic agent of choice in patients with reactive airways disease. Twenty to 30 years ago, it was commonly used. Because of the increasing incidence of reactive airways disease, there is renewed interest in ketamine for sedation of patients with lung disease. A 1-mg/kg bolus of ketamine can be administered, followed by an infusion of 1.0 mg/kg per hour, titrated up to 4.5 mg/kg per hour; many administer a benzodiazepine to reduce the frequency of psychologic sequelae. Ketamine is contraindicated in patients with cardiac ischemia or raised intracranial pressure.
Neuromuscular Blockade
Despite what should be effective doses of anxiolytic drugs, some patients remain delirious and agitated, and a further increase in the dose of anxiolytic drugs is proscribed because of side effects. Such patients, along with those with closed-head injuries, tetanus, and ALI, may require other therapeutic modalities. If the patient is tracheally intubated, mechanically ventilated, and receiving adequate sedation, chemical paralysis with a NMBA is an option (Table 63.12).
Patients with ARDS are often difficult to ventilate and are commonly agitated, hemodynamically unstable, and have a decreased mixed venous oxygen saturation that is life threatening. Additional sedative drugs will only worsen hemodynamics, so NMBAs may be the only (life-saving) alternative that have been shown to improve gas exchange (56).
|
Table 63.12 Indications for the Management of Patients with Neuromuscular Blocking Agents |
|
|
|
|
|
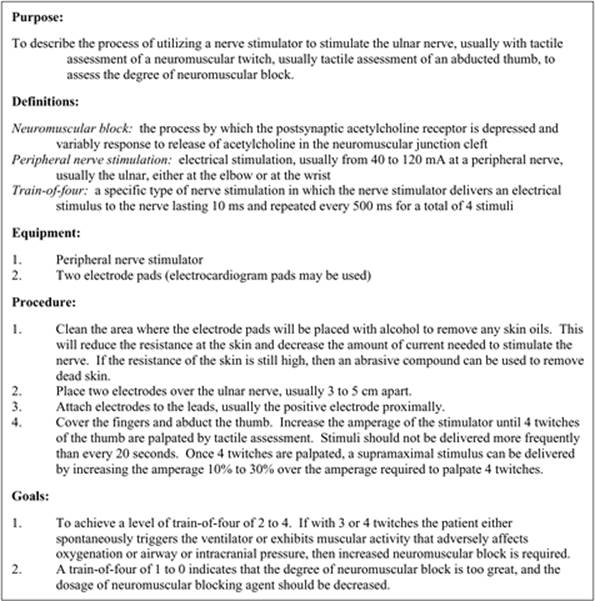
Figure 63.1. Protocol for monitoring degree of neuromuscular block using a nerve stimulator and assessment of the train-of-four twitch. (Reproduced from Murray MJ, Oyen L, Bazzell CM. Use of sedatives, analgesics, and neuromuscular blockers. In: Parillo JE, Dellinger RP, eds. Critical Care Medicine: Principles of Diagnosis and Management. 2nd ed. St. Louis, MO: Mosby; 2001:296–311, with permission.) |
Monitoring
Before administering NMBAs to patients, certain requirements must be met. Patients must be mechanically ventilated, sedated, and monitored.
Obviously, if patients are going to be paralyzed, they must be mechanically ventilated. Similarly, they must be sufficiently sedated that they will have no recall of the experience; most patients who are not adequately sedated will have terrifying dreams/recall (57). Most practitioners will first implement sedation therapy to the point that the patient is unconscious before initiating NMBA therapy. Finally, the use of NMBAs is associated with many adverse side effects. Monitoring the depth of blockade and the necessity of blockade is essential in minimizing these side effects.
Assessing the degree of blockade by measuring the amount of block of the neuromuscular receptor with a twitch monitor is the preferred technique. An electrical stimulus is applied to a peripheral motor nerve, and the effects of the stimulus on the motor group supplied by that nerve are observed (Fig. 63.1). This is most often performed using a twitch stimulator that generates a stimulus of up to 160 mA intensity that lasts 10 ms and is repeated every 500 ms so that four stimuli (train-of-four [TOF]) are delivered (Fig. 63.2). The effects can be visualized, but the preferred technique is for the observer to palpate the response. In the ICU, it is probably easiest to measure the TOF response by stimulating the ulnar nerve at the wrist. The goal of therapy is to provide a sufficient amount of drug so that the patient has only one to two twitches, as opposed to none (overblocked) or three to four (possibly underblocked) twitches.
|
|
|
Figure 63.2. Train-of-four monitoring. A: With the twitch stimulator at 40 to 10 mA, four twitches are measured. B: As the neuromuscular blocking agent (NMBA) takes effect, the second, third, and fourth twitches are weaker/fade. C: The goal with additional time or drug is to have one to two twitches. |
Complications of NMBA
One of the most feared complications of neuromuscular block is accidental extubation. Should a paralyzed patient become accidentally extubated, time is of the essence, especially in patients with ARDS. Ventilation must begin immediately with a mask and anesthesia bag using 100% oxygen while steps are taken to reintubate the patient.
Another feared complication is profound weakness once the drug is discontinued. This may seem counterintuitive—the NMBA is administered to produce profound weakness. This is true, but when the NMBA is discontinued, we anticipate that the patient will recover normal neuromuscular function within hours. One study of two of the longest-lasting NMBAs (pancuronium and doxacurium) in which 40 critically ill patients were paralyzed an average of two to three days found that once doxacurium was discontinued, patients recovered their strength within 4 hours; the patients receiving pancuronium recovered their strength within 24 hours (58).
Though not seen in this study, approximately 10% of patients who receive NMBAs will develop a myopathy from which it takes days or weeks to recover (59). Weakness is a common problem in the ICU and, when secondary to muscle weakness per se, is known as CIM (critical illness myopathy). The cause of CIM in the ICU is multifactorial (60), but most studies indicate that prolonged use of NMBAs in the ICU is one of the causative factors (59). Because corticosteroids are also known to produce myopathy, many intensivists are very cautious when infusing NMBAs in patients who are also receiving corticosteroids (61), a common scenario. Caution is appropriate and should be the norm when infusing NMBAs in patients who are critically ill. Daily assessments must be made to determine if NMBA use is justified, and the TOF should be maintained at one to two twitches.
Treatment
Aminosteroidal Compounds (Fig. 63.3)
Pancuronium
Pancuronium is a long-acting, nondepolarizing, aminosteroidal compound that produces effective block for up to 90 minutes after a bolus dose of 0.06 to 0.08 mg/kg. Intermittent boluses are often administered, but it can be used as a continuous infusion, titrating the dose to one or two twitches by TOF monitor. Pancuronium induces vagolysis, limiting its use in patients who cannot tolerate an increase in heart rate. In patients with renal or liver failure, pancuronium's effects are prolonged because of the increased elimination half-life of pancuronium and its 3-hydroxypancuronium metabolite, which has one third to one half the activity of pancuronium.
Vecuronium
With the deletion of the methyl group at one of pancuronium's two N-methyl-piperidine moieties (leaving vecuronium with a single [monoquaternary] piperidine group at the R-2 position), scientists were able to produce an intermediate-acting NMBA without the vagolytic properties of pancuronium. An intravenous bolus dose of 0.08 to 0.10 mg/kg produces block within 2½ to 3 minutes that typically lasts 35 to 45 minutes. After a bolus dose, it can be given as a continuous infusion of 0.8 to 1.4 µg/kg per minute, titrating the rate to the degree of block desired. The 3-desacetylvecuronium metabolite has 50% of the pharmacologic activity of the parent compound (62) so that patients with hepatic dysfunction may have increased plasma concentrations of both the parent compound and the active metabolite, causing prolonged block. Renal dysfunction also prolongs the duration of block. Vecuronium is associated with CIM, especially in patients receiving corticosteroids. Vecuronium is being used with decreased frequency in ICU patients.
Rocuronium
Rocuronium is a newer aminosteroidal NMBA, with an intermediate duration of action and a rapid onset that has been tested in the ICU (63). When given as a bolus of 0.6 to 0.1 mg/kg, block is almost always achieved within 2 minutes, with maximum block occurring within 3 minutes; continuous infusions are administered at 8 to 10 µg/kg per minute (64) and usually produce a fairly dense block. Rocuronium's metabolite, 17-desacetylrocuronium, has approximately only 5% to 10% activity compared to the parent compound. Renal failure should not have an effect on duration of action, but hepatic failure may prolong rocuronium's duration of action.
Benzylisoquinolinium Compounds
Atracurium
Atracurium is an intermediate-acting NMBA with minimal cardiovascular side effects but is associated with histamine release at higher doses. Atracurium has a unique metabolism (ester hydrolysis and Hofmann elimination) so that renal or hepatic dysfunction does not affect its duration of block. Atracurium has been associated with persistent neuromuscular weakness as has been reported with other NMBAs.
Cisatracurium
Cisatracurium, one of atracurium's 16 isomers, is an intermediate-acting benzylisoquinolinium NMBA that is increasingly used in lieu of atracurium. It produces few, if any, cardiovascular effects and has fewer tendencies to produce mast cell degranulation than does atracurium. Bolus doses with a 0.10 to 0.2 mg/kg result in paralysis in an average of 2.5 minutes, and recovery begins at approximately 25 minutes; maintenance infusion rates should be started at 2.5 to 3.0 µg/kg per minute. Cisatracurium is also metabolized by ester hydrolysis and Hofmann elimination, so duration of block should not be affected by MODS. There have not yet been reports of significantly prolonged recovery associated with cisatracurium. The mean peak plasma laudanosine concentrations are lower in patients receiving cisatracurium compared to patients receiving clinically equivalent doses of atracurium. Laudanosine at high doses produces seizures in animals; a case of seizures in a human receiving atracurium or cisatracurium has not been reported.
|
|
|
Figure 63.3. Chemical structures of neuromuscular blocking agents. Cisatracurium is the 1R-cis 1′R-cis isomer, one of the 10 isomers found in atracurium. |
Recovery
Patients receiving an NMBA should have daily drug holidays. If the NMBA is no longer required, it is discontinued. It is anticipated that with all the NMBAs, the TOF should normalize (four twitches) within 3 to 4 hours. If not, the patient may have a CIM associated with the NMBA (with an increased incidence in patients receiving corticosteroids and patients with sepsis, etc.). If, after 24 hours, the patient has inadequate strength, additional studies should be done to include an assessment of the antibiotics the patient is receiving, electrolytes (calcium, magnesium, phosphorus), and temperature (hypothermia prolongs neuromuscular block). If no comorbid condition accounts for the degree of neuromuscular block, a neurology consult should be considered. In this context, an electromyography is typically performed (to rule out critical illness polyneuropathy) and, in some circumstances, a muscle biopsy is obtained. Patients with CIM secondary to the neuromuscular blockade will have loss of myosin. Treatment is supportive with maintenance of sedation, mechanical ventilation, physical therapy, skin care, eye care, and so on.
Summary
Over the past 30 years, there is increased recognition that patients in the ICU are anxious, and as patients become older, have more comorbid conditions, and are more critically ill, they will increasingly exhibit agitation and delirium. These factors increase morbidity and mortality, prolonging the length of stay and worsening the outcome. Even patients who survive have memories that are disturbing and, in some circumstances, lead to the equivalent of a posttraumatic stress syndrome. Practitioners in an ICU must recognize when their patients become anxious, agitated, and delirious; identify contributing factors; and treat the disorders with anxiolytic medications. The effects of therapy must be monitored with the use of a standard scale, one that is used throughout the institution's ICUs. In some patients in whom the sedation is inadequate, NMBAs may be indicated. Appropriate sedation, monitoring, securing of the airway, and monitoring the adequacy of mechanical ventilation must be ensured. Patients receiving any of these medications are at risk for side effects, which must be monitored as well. An effective sedation and paralysis protocol will improve patient outcome and patient satisfaction.
Stress Points
1. Anxiety and pain are different emotional states, and most patients who are oriented can differentiate between anxiety and pain.
2. Before relying on pharmacologic interventions to treat pain or anxiety, first assess possible confounding factors such as a distended bladder in a patient who does not have a Foley catheter; hypercapnia in someone with impending respiratory failure; or someone who is becoming septic, which is manifested by encephalopathy.
3. Anxiety can lead to agitation, which in turn can result in self-injury and injury to care providers.
4. Delirium is an increasingly recognized problem in the intensive care unit (ICU), which can result in long-term cognitive impairment.
5. Physiologic derangements must first be ruled out before treating anxiety, agitation, or delirium.
6. Opioids and benzodiazepines are the pharmacologic mainstays of treating anxiety.
7. Midazolam, propofol, or dexmedetomidine are the preferred short-term (24–48 hours) treatments of anxiety.
8. Lorazepam and fentanyl are the preferred long-term anxiolytic agents.
9. Haloperidol is an effective therapy for older patients with delirium.
10. Mechanically ventilated patients who remain agitated despite adequate anxiolytic therapy are candidates for an NMBA.
11. Patients must be adequately sedated before an NMBA is administered.
12. Patients receiving NMBAs must be mechanically ventilated, with precautions taken to ensure that the tracheal tube or tracheostomy tube is protected.
13. The primary NMBAs used for mechanically ventilated patients are the aminosteroidal compounds (pancuronium or rocuronium) and the benzylisoquinolinium compounds (atracurium or cisatracurium).
14. Daily drug “holidays” should be implemented when using anxiolytic drugs or NMBAs.
15. Patients who have received anxiolytic drugs for greater than 3 to 7 days are at risk of becoming dependent and may exhibit signs of withdrawal when the drug(s) is/are discontinued.
16. Patients who have received NMBAs for greater than 12 to 24 hours are at increased risk of developing critical illness myopathy (CIM) when the NMBA is discontinued.
References
1. Treggiari-Venzi M, Borgeat A, Fuchs-Buder T, et al. Overnight sedation with midazolam or propofol in the ICU: effects on sleep quality, anxiety and depression. Intensive Care Med. 1996;22:1186–1190.
2. Rotondi A, Lakshmipathi C, Sirio C, et al. Patients' recollections of stressful experiences while receiving prolonged mechanical ventilation in an intensive care unit. Crit Care Med. 2002;30:746–752.
3. Fong HK, Sands LP, Leung JM. The role of postoperative analgesia in delirium and cognitive decline in elderly patients: a systematic review. Anesth Analg. 2006;102:1255–1266.
4. Vaurio L, Sands LP, Wang Y, et al. Postoperative delirium: the importance of pain and pain management. Anesth Analg. 2006;102:1267–1273.
5. Anonymous. Management of the agitated intensive care unit patient. Crit Care Med. 2002;30:S97–S123.
6. Jaber S, Chanques G, Altairac C, et al. A prospective study of agitation in a medical-surgical ICU. Incidence, risk factors, and outcomes. Chest. 2005;128:2749–2757.
7. De Jonghe B, Cook D, Griffith L, et al. Adaptation to the Intensive Care Environment (ATICE): development and validation of a new sedation assessment instrument. Crit Care Med. 2003;31:2344–2354.
8. Weinert C, McFarland L. The state of intubated ICU patients: development of a two-dimensional sedation rating scale for critically ill adults. Chest. 2004;126:1727–1730.
9. Ramsay MAE, Savege TM, Simpson BRJ, et al. Controlled sedation with alphaxalone-alphadolone. Br Med J. 1974;2:656–659.
10. Sessler CN, Gosnell MS, Grap MJ, et al. The Richmond Agitation-sedation Scale. Validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. 2002;166:1338–1344.
11. Riker RR, Graser GL, Cox PM; Continuous infusion of haloperidol controls agitation in critically ill patients. Crit Care Med. 1994;22:433–440.
12. de Lemos J, Tweeddale M, Chittock D. Measuring quality of sedation in adult mechanically ventilated critically ill patients. The Vancouver Interaction and Calmness Scale. Sedation Focus Group. J Clin Epidemiol. 2000;53:908–919.
13. Devlin JW, Boleski G, Mlynarek M, et al. Motor Activity Assessment Scale: a valid and reliable sedation scale for use with mechanically ventilated patients in an adult surgical intensive care unit. Crit Care Med. 1999;27:1271–1275.
14. Rincon HG, Granados M, Unutzer J, et al. Prevalence, detection and treatment of anxiety, depression, and delirium in the adult critical care unit. Psychosomatics. 2001;42:391–396.
15. Peterson JF, Pun BT, Dittus RS, et al. Delirium and its motoric subtypes: a study of 614 critically ill patients. J Am Geriatr Soc. 2006;54:479–484.
16. Thomason JWW, Shintani A, Peterson JF, et al. Intensive care unit delirium is an independent predictor of longer hospital stay: a prospective analysis of 261 non-ventilated patients. Crit Care. 2005;9:R375–R381.
17. Ely EW, Stephens RK, Jackson JC, et al. Current opinions regarding the importance, diagnosis, and management of delirium in the intensive care unit: a survey of 912 healthcare professionals. Crit Care Med. 2004;32:106–112.
18. Miller RR III, Ely EW. Delirium and cognitive dysfunction in the intensive care unit. Semin Respir Crit Care Med. 2006;27:210–220.
19. Pandharipande P, Ely EW. Sedative and analgesic medications: risk factors for delirium and sleep disturbances in the critically ill. Crit Care Clin. 2006;22:313–327.
20. McNicoll L, Pisani MA, Ely EW, et al. Detection of delirium in the intensive care unit: comparison of confusion assessment method for the intensive care unit with confusion assessment method ratings. J Am Geriatr Soc. 2005;53:495–500.
21. Rosengren A, Hawken S, Ôunpuu S, et al. Association of psychosocial risk factors with risk of acute myocardial infarction in 11119 cases and 13648 controls from 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364:953–962.
22. Rosenkranz MA, Busse WW, Johnstone T, et al. Neural circuitry underlying the interaction between emotion and asthma symptom exacerbation. Proc Natl Acad Sci U S A. 2005;102:13319–13324.
23. Ploghaus A, Narain C, Beckmann C, et al. Exacerbation of pain by anxiety is associated with activity in a hippocampal network. J Neurosci. 2001;21:9896–9903.
24. Crippen D. Agitation in the ICU: part one. Anatomical and physiologic basis for the agitated state. Crit Care. 1999;3R35–R46.
25. Kain ZN, Caldwell-Andrews AA, Maranets I, et al. Preoperative anxiety and emergence delirium and postoperative maladaptive behaviors. Anesth Analg. 2004;99:1648–1654.
26. Fumagalli S, Boncinelli L, Lo Nostro A, et al. Reduced cardiocirculatory complications with unrestrictive visiting policy in an intensive care unit. Circulation. 2006;113:946–952.
27. Baker CF. Sensory overload and noise in the ICU: sources of environmental stress. Crit Care Q. 1984;6:66–80.
28. Parthasarathy S. Sleep in the intensive care unit: sleepy doctors and restless patients. Clin Intensive Care. 2005;16:129–136.
29. Reuben SS, Buvanendran A, Kroin JS, et al. The analgesic efficacy of celecoxib, pregabalin, and their combination for spinal fusion surgery. Anesth Analg. 2006;103:1271–1777.
30. Park G, Lane M, Rogers S, et al. A comparison of hypnotic and analgesic based sedation in a general intensive care unit. Br J Anaesth. 2007;98:76–82.
31. Muellejans B, López A, Cross MH, et al. Remifentanil versus fentanyl for analgesia based sedation to provide patient comfort in the intensive care unit: a randomized, double-blind controlled trial [ISRCTN43755713]. Crit Care 2004;8:R1–R11.
32. Haefely W. The biological basis of benzodiazepine actions. J Psychoactive Drugs. 1983;15:19–39.
33. Zbinden G, Randall LO. Pharmacology of benzodiazepines: laboratory and clinical correlations. Adv Pharmacol. 1967;5:213–291.
34. Jacobi J, Fraser GL, Coursin DB, et al. Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med. 2002;30:119–141.
35. Swart EL, van Schijndel RJ, van Loenen AC, et al. Continuous infusion of lorazepam versus midazolam in patients in the intensive care unit: sedation with lorazepam is easier to manage and is more cost-effective. Crit Care Med. 1999;27:1461–1465.
36. Swart EL, Zuideveld KP, de Jongh J, et al. Comparative population pharmacokinetics of lorazepam and midazolam during long-term continuous infusion in critically ill patients. Br J Clin Pharmacol. 2004;57:135–145.
37. MacLaren R, Sullivan PW. Pharmacoeconomic modeling of lorazepam, midazolam, and propofol for continuous sedation in critically ill patients. Pharmacotherap.y 2005;25:1319–1328.
38. Cigada M, Pezzi A, Di Mauro P, et al. Sedation in the critically ill ventilated patient: possible role of enteral drugs. Intensive Care Med. 2005;31:482–486.
39. Barr J, Zomorodi K, Bertaccini EJ, et al. A double-blind, randomized comparison of i.v. lorazepam versus midazolam for sedation of ICU patients via a pharmacologic model. Anesthesiology. 2001;95:286–298.
40. Izurieta R, Rabatin JT. Sedation during mechanical ventilation: a systematic review. Crit Care Med. 2002;30:2644–2648.
41. Schweickert WD, Gehlbach BK, Pohlman AS, et al. Daily interruption of sedative infusions and complications of critical illness in mechanically ventilated patients. Crit Care Med. 2004;32:1272–1276.
42. Cammarano WB, Pittet J-F, Weitz S, et al. Acute withdrawal syndrome related to the administration of analgesic and sedative medications in adult intensive care unit patients. Crit Care Med. 1998;26:676–684.
43. Barr J. Propofol: a new drug for sedation in the intensive care unit. Int Anesthesiol Clin. 1995;33:131–154.
44. Fudickar A, Bein B, Tonner PH. Propofol infusion syndrome in anaesthesia and intensive care medicine. Curr Opin Anaesthesiol. 2006;19:404–410.
45. Riphaus A, Gstettenbauer T, Frenz MB, et al. Quality of psychomotor recovery after propofol sedation for routine endoscopy: a randomized and controlled study. Endoscopy. 2006;38:677–683.
46. Brown LA, Levin GM. Role of propofol in refractory status epilepticus. Ann Pharmacothe.r 1998;32:1053–1059.
47. Kelly DF, Goodale DB, Williams J, et al. Propofol in the treatment of moderate and severe head injury: a randomized, prospective double-blinded pilot trial. J Neurosurg. 1999;1042–1052.
48. Hall JE, Uhrich TD, Barney JA, et al. Sedative, amnestic, and analgesic properties of small-dose dexmedetomidine infusions. Anesth Analg. 2000;90:699–705.
49. Herr DL, Sum-Ping STJ, England M. ICU sedation after coronary artery bypass graft surgery: dexmedetomidine-based versus propofol-based sedation regimens. J Cardiothorac Vasc Anesth. 2003;17:576–584.
50. Bekker A, Sturaitis MK. Dexmedetomidine for neurological surgery. Neurosurgery. 2005;57(1 Suppl):1–10; discussion 1–10.
51. Corbett SM, Rebuck JA, Greene CM, et al. Dexmedetomidine does not improve patient satisfaction when compared with propofol during mechanical ventilation. Crit Care Med. 2005;33:940–945.
52. Steadman JL, Birnbach DJ. Patients on party drugs undergoing anesthesia. Curr Opin Anaesthesiol. 2003;16:147–152.
53. Ingersoll-Weng E, Manecke GR Jr, Thistlethwaite PA. Dexmedetomidine and cardiac arrest. Anesthesiology. 2004;100:738–739.
54. Chang NS, Simone AF, Schultheis LW. From the FDA: what's in a label? A guide for the anesthesia practitioner. Anesthesiology. 2005;103:179–185.
55. Milbrandt EB, Kersten A, Kong K, et al. Haloperidol use is associated with lower hospital mortality in mechanically ventilated patients. Crit Care Med. 2005;33:226–229.
56. Gainnier M, Roch A, Forel J-M, et al. Effect of neuromuscular blocking agents on gas exchange in patients presenting with acute respiratory distress syndrome. Crit Care Med. 2004;32:113–119.
57. Ballard N, Robley L, Barrett D, et al. Patients' recollections of therapeutic paralysis in the intensive care unit. Am J Crit Care. 2006;16:86–95.
58. Murray MJ, Coursin DB, Scuderi PE, et al. Double-blind, randomized, multicenter study of doxacurium vs. pancuronium in intensive care unit patients who require neuromuscular-blocking agents. Crit Care Med. 1995;23:450–458.
59. Murray MJ, Brull SJ, Bolton CF. Brief review: nondepolarizing neuromuscular blocking drugs and critical illness myopathy. Can J Anaesth. 2006;53:1148–1156.
60. Bolton CF. Neuromuscular manifestations of critical illness. Muscle Nerve. 2005;32:140–163.
61. Larsson L, Xiapeng L, Edström L, et al. Acute quadriplegia and loss of muscle myosin in patients treated with nondepolarizing neuromuscular blocking agents and corticosteroids: mechanisms at the cellular and molecular levels. Crit Care Med. 2000;28:34–45.
62. Segredo V, Caldwell JE, Matthay MA, et al. Persistent paralysis in critically ill patients after long-term administration of vecuronium. N Engl J Med. 1992;327:524–528.
63. Stene J, Murray M, DeRuyter M, et al. Selective rocuronium pharmacodynamics and kinetics during ICU infusion. Anesthesiology. 1998;89:477A.
64. Khuenl-Brady KS, Sparr H, Pühringer F, et al. Rocuronium bromide in the ICU: dose finding and pharmacokinetics. Eur J Anesthesiol Suppl. 1995;11:79–80.