C. Clay Cothren
Ernest E. Moore
Multiply injured patients admitted to the intensive care unit (ICU) have an array of physiologic derangements that may include metabolic failure and cardiopulmonary embarrassment. In addition to the seeming routine care of the critically ill patient, the intensivist should be able to recognize the inherent differences in care of the postinjury patient. The intensivist should be familiar with the implications of specific injuries including guidelines for nonoperative management, postoperative care, and expected postinjury complications and their sequelae. This chapter will focus on specific issues encountered in the acute resuscitation and overall ICU management of the trauma patient, rather than the initial evaluation of the patient in the emergency department (ED). Initial therapy in the trauma bay, precise indications for operation, and intraoperative decision making for particular injury patterns is beyond the scope of this chapter.
Initial Evaluation in the Intensive Care Unit
Although some patients may arrive in the ICU in extremis necessitating continued resuscitation without a thorough history and physical examination, the majority should undergo a complete assessment promptly, and it should not be assumed that the ED evaluation was comprehensive and accurate. Such an evaluation, often termed the tertiary survey, is a repeated history and physical examination performed in light of imaging studies and pertinent intraoperative findings (1,2). Additionally, the evaluation is more detailed than that performed in the ED, because all the diagnostic results should be available, further information is obtained from family members, and the physician has time for a more meticulous physical examination. Key elements include the patient's past medical history, specifically issues such as cardiopulmonary disease; hypertension including past myocardial infarction; use of β-blockers, steroids, angiotensin-converting enzyme (ACE) inhibitors, and bronchodilators; and other elements that may acutely impact the patient's ongoing care. Discovering minor injuries on the tertiary survey such as subtle extremity injuries overlooked on the initial ED evaluation is common (3,4,5). Documentation of this evaluation, particularly of final imaging results, can be done through a standardized form and facilitates communication among care providers (Fig. 75.1).
The reliability of clinical examination in these patients after ICU admission is often questioned. The clinical exam is important, even in injured patients who are intoxicated or who have sustained a head injury; in addition to external evidence of trauma, the patient's reported pain or discomfort, particularly whether this is increasing or decreasing in nature with time, is paramount. Only in the intubated patient is the clinical examination more limited from a patient response standpoint; specific signs of injury such as ecchymosis, distention, and crepitus are still critical to recognize. Similar to the physician evaluation in the ED, there are clear indications in the ICU for surgeon evaluation for possible laparotomy (Table 75.1).
|
|
|
|
Figure 75.1. A thorough history and physical examination in the intensive care unit including imaging, termed the tertiary survey, can be documented on a standardized form to facilitate communication among care providers. (Continued ) |
|
|
Table 75.1 Indications for surgeon evaluation in the intensive care unit for possible exploratory laparotomy |
|
|
Some patients will require imaging upon arrival to ICU; patients with intracranial or thoracic injury may go emergently to the operating room prior to computed tomography (CT) scanning of the abdomen. These patients, once hemodynamically stable in the ICU, should undergo CT scanning to delineate any associated intra-abdominal injuries. Even in patients who undergo exploratory laparotomy, CT of the abdomen may be necessary to diagnose spine fractures and to evaluate the retroperitoneum. Routine postadmission studies include repeat chest film and laboratory studies. A chest film is important to determine central line catheter, tube thoracostomy, and endotracheal tube positions, as any of these could become dislodged with transport. The chest radiograph may also show interval change in a patient's hemothorax, pneumothorax, or pulmonary contusion. Based upon physical exam findings in the tertiary survey, further imaging of extremities may also be required.
Once the patient has been fully evaluated by the treating ICU physicians and associated imaging and laboratory results obtained, the therapeutic plan is initiated to optimize the patient's cardiopulmonary and metabolic status. In addition to the patient's ongoing cardiopulmonary resuscitation, there is concurrent treatment of known injuries, ongoing evaluation for missed injuries, and monitoring for the sequelae of recognized injuries.
Postinjury Resuscitation
ICU management of the trauma patient, either with direct admission from the ED or following emergent operative intervention, is considered in distinct phases because there are differing goals and priorities. The period of acute resuscitation, typically lasting for the first 12 to 24 hours following injury, combines several principles: optimizing tissue perfusion, ensuring normothermia, and restoring coagulation. There are a multitude of management algorithms aimed at accomplishing these goals—the majority involves goal-directed resuscitation with initial volume loading to attain adequate preload, followed by judicious use of inotropic agents or vasopressors (6). Although the optimal hemoglobin (Hb) level remains debated, during shock resuscitation an Hb >10 g/dL optimizes oxygen delivery (6). A more judicious transfusion trigger of Hb <7 g/dL in the euvolemic patient after the first 24 hours of resuscitation limits adverse inflammatory effects and improves mortality (7,8). The optimum hemoglobin level may vary depending on the patient's underlying cardiac function. The resuscitation of the severely injured trauma patient may require what appears to be an inordinate amount of crystalloid resuscitation. Infusion volumes upwards of 10 liters during the initial 6 to 12 hours may be required to attain an adequate central venous pressure (CVP) above 8 mm Hg. In fact, this is a challenging aspect of early care (i.e., balancing cardiac preload vs. promoting an abdominal compartment syndrome or tissue edema). During this initial treatment period, a low urine output is usually suggestive of a low preload and not an indication for diuretics. Moreover, the use of diuretics during a patient's initial resuscitation should be carefully considered, even if the patient is on such medications as an outpatient.
Invasive monitoring with pulmonary artery catheters may be a critical adjunct in the multiply injured patient (6,9). Not only do such devices allow minute-to-minute monitoring of the patient, but also the added information on the patient's volume status, cardiac function, peripheral vascular tone, and metabolic response to injury permits appropriate therapeutic intervention. With added information on the patient's cardiac function, cardiac indices (CIs) and oxygen delivery (DO2) become important variables in the ongoing ICU management. Resuscitation to values of DO2I >500 mL/minute/m2 and CI >3.8 L/minute/m2 are the goals (6,10,11). Pulmonary artery catheters also enable the physician to monitor response to vasoactive agents. Although norepinephrine is the agent of choice for patients with low systemic vascular resistance (SVR) unable to maintain a mean arterial pressure (MAP) >60 mm Hg (6), patients may have an element of myocardial dysfunction requiring inotropic support. In patients with ongoing need for pressors, one should evaluate for adrenal insufficiency (12,13).
Adequate resuscitation is mandatory, and often determines when the surgeon can safely return the patient to the operating room (OR) after initial operative intervention. Specific goals of resuscitation prior to repeated “semi-elective” transport include a core temperature >35°C, base deficit less negative than 6, and normal coagulation indices. Even those patients who do not require repeat operations should be monitored for resolution of physiologic perturbations; specific indices monitored over time include lactate and base deficit levels as well as temperature. Although correction of base deficit and lactate values is desirable, how quickly this should be accomplished requires careful consideration. Adverse sequelae of aggressive crystalloid resuscitation include increased intracranial pressure, worsening pulmonary edema, and intra-abdominal visceral and retroperitoneal edema resulting in secondary abdominal compartment syndrome (14,15). Therefore, it should be the overall trend of the resuscitation rather than a rapid reduction of the base deficit to less than 5 during the first 4 hours of treatment that is the goal. Exogenous bicarbonate, occasionally given to improve cardiovascular function and response to vasoactive agents if the serum pH is below 7.2, obfuscates the acid-base balance and lactate may be a more reliable indicator of adequate perfusion.
Nonoperative Management of Trauma
Blunt Liver and Spleen Injuries
The liver and spleen are the most commonly injured solid organs following trauma, occurring in approximately 10% to 15% of all trauma admissions. The liver's large size makes it the most susceptible organ injured in blunt trauma, and it is frequently involved in upper torso penetrating trauma. Similarly, blunt trauma to the left upper quadrant, often with associated rib fractures, should raise the concern for a splenic injury. Although the liver is more often injured, splenic injuries tend to be more precarious clinically. Nonoperative management of solid organ injuries is pursued in hemodynamically stable patients who do not have overt peritonitis or other indications for laparotomy (16,17,18,19,20,21,22,23,24,25). Since its initial use in the early 1980s, CT scanning has largely supplanted diagnostic peritoneal lavage in the initial evaluation of trauma patients (Fig. 75.2). Key questions when looking at the CT scan include how extensive the injury is by the American Association for the Surgery of Trauma (AAST) solid organ injury grading scale (Table 75.2), how much associated free fluid is within the abdomen, whether there is free contrast extravasation indicating ongoing arterial bleeding, and whether there are pseudoaneurysms of the arteries (Fig. 75.3). High-grade injuries, a large amount of hemoperitoneum, contrast extravasation, and pseudoaneurysms are not absolute contraindications for nonoperative management; however, these patients are at high risk for failure and are more likely to need angioembolization (26,27,28,29). Likewise, there is not an age cutoff for patients for the nonoperative management of solid organ injuries (30,31,32).
|
|
|
Figure 75.2. Representative solid organ injuries; American Association for the Surgery of Trauma grading includes evidence of subcapsular hematomas (A) and parenchymal lacerations (B, C). |
The AAST developed a grading scale to provide a uniform definition of solid organ injuries based upon the magnitude of anatomic disruption (33,34,35). The grading of solid organ injuries permits accurate relay of information between care providers, a predictive value on the incidence of nonoperative failure, and information for appropriate monitoring (Table 75.3). The vast majority of patients with liver or spleen injuries, regardless of grade, can be managed nonoperatively (18,19). Predictors of failure include increasing grade of injury, evidence of blush on CT scan (particularly if this involves free extravasation into the peritoneal cavity rather than pooling within the organ), and a large amount of hemoperitoneum (18,19,27,29,36).
A multidisciplinary approach including angiography with selective angioembolization and endoscopic retrograde cholangiopancreatography (ERCP) with stenting has resulted in decreased nonoperative failure rates and improved survival in liver (37,38) and splenic injuries (39). Splenic angioembolization has been employed since 1995 as an adjunct to nonoperative therapy, with reported salvage rates of 98% (40). Patients with significant hemoperitoneum or overt contrast extravasation who are hemodynamically stable should be considered for possible splenic embolization. Additionally, patients with splenic artery pseudoaneurysms or arteriovenous (AV) fistulae within the spleen are also candidates (41). If a patient is going to fail nonoperative management (Fig. 75.4), the time to failure is different for liver versus spleen injuries. Typically liver injuries rebleed within the first hours of admission, while splenic laceration may have delayed rupture or bleeding weeks following the original injury. General guidelines for operative or angioembolization are noted in Table 75.4. Repeat imaging in patients with complex hepatic injuries can be performed with bedside ultrasound. Patients with evidence of right upper quadrant fluid collections or clinical deterioration (increasing abdominal pain, worsening liver function tests, unexplained fever) should undergo CT scanning (42,43).
|
Table 75.2 American Association for the Surgery of Trauma solid organ injury grading scales |
||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||||||||
|
Figure 75.3. Free contrast extravasation noted on computed tomography scan imaging of the liver (A) and spleen (B). |
||||||||||||||||||||||||||||||||||||||||||
Pancreatic Injuries
Historically, injuries to the pancreas were managed with operative intervention (44). With the recent evolution of nonoperative management for solid organ injuries, a nonresectional management schema has been developed for select pancreatic injuries (45,46). Observation of pancreatic contusions, particularly those in the head of the pancreas that may involve ductal disruption, includes serial exams and monitoring of serum amylase. Patients with pancreatic injuries involving the major ducts, originally a strict indication for operative intervention, may be managed with ERCP and stenting in select patients; durability of this approach is currently under investigation (47).
|
Table 75.3 Appropriate monitoring and nonoperative management failure rates for solid organ injuries by grade |
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
Duodenal Hematomas
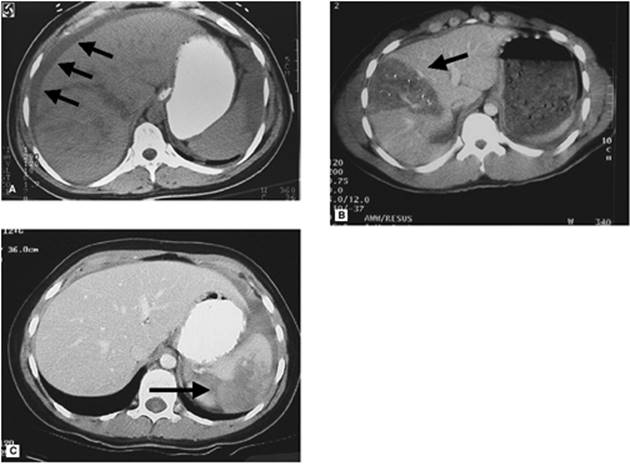
Following blunt trauma, patients may develop hematomas in the duodenal wall that obstruct the lumen. Clinical exam findings include epigastric pain associated with either emesis or high nasogastric tube (NGT) output; CT scan imaging with oral contrast failing to pass into the proximal jejunum is diagnostic (Fig. 75.5). Patients with suspected associated perforation, suggested by clinical deterioration or imaging with retroperitoneal free air or contrast extravasation, should be explored operatively. Nonoperative management includes continuous NGT decompression and nutritional support with total parenteral nutrition (TPN) (48,49). A marked drop in NGT output heralds resolution of the hematoma, which typically occurs within 2 weeks; repeat imaging to document these clinical findings is optional. If the patient does not improve clinically or radiographically within 4 weeks, operative evaluation is warranted.
Penetrating Wounds
Patients with abdominal gunshot wounds (GSWs) violating the peritoneum undergo emergent laparotomy due to an approximate 90% visceral injury rate. Select patients with isolated low-energy GSWs to the right upper quadrant are observed (50,51); CT scan imaging must delineate the tract of the bullet, which should be confined to the parenchyma of the liver, and the patient must be hemodynamically stable with a benign clinical examination. Patients with abdominal stab wounds (SWs) to the back or flank with negative CT imaging or an isolated kidney injury are also managed nonoperatively (52). Similar to patients with right upper quadrant GSWs, individuals with SWs and a CT scan showing the tract of injury confined to the liver are usually observed (53). In some cases, laparoscopy will be done to assess the penetrating liver injury and ensure the viscera are not violated. Regardless of the trauma surgeon's decision for operative versus nonoperative management, it is essential that these patients undergo repeated abdominal examination. Observation for a missed small or large bowel injury is critical; clinical findings in such patients include a rising white blood cell count, fever, tachycardia, and increasing abdominal pain or frank peritonitis. In patients with isolated liver injuries, complications are similar to those for patients with blunt injuries, namely bleeding and bile leaks or biliary sepsis.
|
|
|
Figure 75.4. Rates of nonoperative failure for solid organ injuries. |
Complications of Nonoperative Injury Management
Following hepatic injuries, the most common complication is a bile leak or biloma, occurring in up to 20% of patients (Fig. 75.6) (54,55). Clinical presentation includes abdominal distention, intolerance of enteral feeds, and elevated liver functions tests. CT scanning effectively diagnoses the underlying problem, and the vast majority is treated with percutaneous drainage and ERCP with sphincterotomy. Occasionally, laparoscopy or laparotomy with drainage of biliary ascites is indicated, particularly if the patient fails to resolve his or her ileus and fever (56). Hemobilia, manifested by the triad of right upper quadrant pain, jaundice, and upper gastrointestinal bleeding, is a rare complication. Delayed rupture of a subcapsular hematoma with hemorrhage is another infrequent complication but the diagnosis is usually obvious. Patients undergoing angioembolization for liver trauma must be carefully monitored for hepatic necrosis, and may occasionally require delayed formal hepatic resection (Fig. 75.6). Although some clinicians repeat CT scans on all patients with grade IV and V injuries, typically, only patients with symptoms or persistent altered liver function tests should be reimaged (43).
|
Table 75.4 General guidelines for operative or interventional radiology intervention during nonoperative management of solid organ injuries |
|
|
|
|
|
|
|
Figure 75.5. Duodenal hematomas are diagnosed radiographically by direct identification of a hematoma (A) or failure to pass oral contrast past the third portion of the duodenum on computed tomography scan (B) or upper gastrointestinal series (C). |
|
|
|
Figure 75.6. Bilomas are the most common complication following hepatic trauma (A), while angioembolization for unremitting postinjury liver hemorrhage may result in partial hepatic necrosis (B). |
|
|
|
Figure 75.7. Splenic implants are autotransplanted into the greater omentum to prevent overwhelming postsplenectomy sepsis (A); follow-up computed tomography scan imaging can differentiate between “normal” implants (B) versus infected implants (C). |
The most common problem in patients with splenic injuries is delayed bleeding, although as noted previously, the majority fails over an established timeframe. Patients undergoing splenic embolization can fail with rebleeding with 13% of patients requiring splenectomy (57). Moreover, those undergoing successful angioembolization typically have significant pain associated with their “splenic infarct,” and up to 20% develop splenic abscesses. In centers that advocate splenic autotransplantation to prevent overwhelming postsplenectomy sepsis (OPSS), recognition of CT scan findings of normal splenic implants versus infected splenic implants is critical in patients with clinical deterioration (Fig. 75.7) (58).
Ongoing Evaluation for Injuries (How to Avoid a Missed Injury)
With the paradigm shift from operative to nonoperative management of trauma, the clinician must have a heightened sense of awareness to avoid missing an occult injury. This is particularly true in multiply injured blunt trauma patients, especially those who are intubated without a reliable abdominal examination. CT scan imaging is not 100% accurate; repeat CT scan imaging, diagnostic peritoneal lavage (DPL), ultrasound, and even laparotomy may be necessary for definitive evaluation.
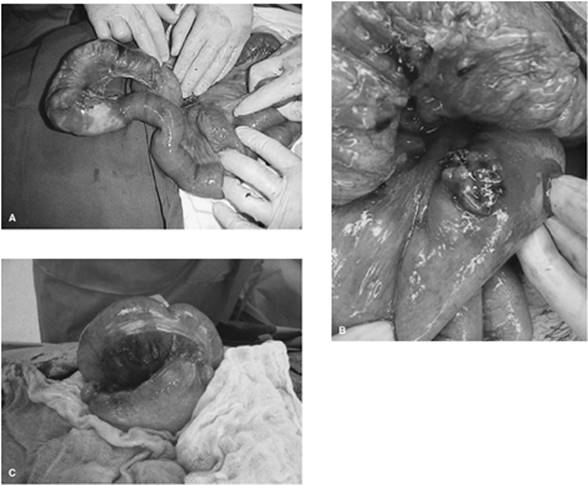
Missed bowel injuries are the most commonly pursued injury, not due to their frequency (less than 5% of blunt trauma) but rather their associated morbidity. Diagnosing a hollow viscus injury is notoriously difficult (59), and even short delays in diagnoses result in increased morbidity (60,61). If a patient's initial CT scan of the abdomen shows free fluid without evidence of a solid organ injury to explain such fluid, evaluation for a bowel injury should be performed (62,63,64). DPL should also be considered in a patient if there is increasing intra-abdominal fluid on bedside ultrasound in patients with a solid organ injury but a stable hematocrit, and/or in patients with unexplained clinical deterioration. Typically, the DPL at the bedside is done, with specific laboratory values indicating need for laparotomy (Table 75.5) (65,66); particular attention should be paid to elevations in bilirubin, alkaline phosphatase, and amylase when pursuing a diagnosis of bowel injury. The specific type of injury may be either bowel perforation due to ischemia from an avulsed mesentery, a direct antimesenteric blowout injury, or a blunt serosal injury (Fig. 75.8). One should not assume that drugs, alcohol, or their associated withdrawal syndromes are the primary source of a patient's clinical deterioration.
|
Table 75.5 A positive diagnostic peritoneal lavage following blunt trauma defined by specific laboratory values |
||||||||||||
|
Missing a rectal injury may be life threatening in patients with pelvic fractures. While some patients have clear findings on physical examination, ranging from hematochezia to overt degloving of the perineum, others may have occult injuries that are missed on initial evaluation in the trauma bay. In fact, the rectal exam may have been omitted in the trauma bay, so the intensivist should ensure that this has been adequately done. Flexible sigmoidoscopy is the easiest diagnostic procedure for the clinician to perform at the bedside in the ICU; endoscopic evaluation should rule out blood within the canal, clear intestinal perforation, or ischemic mucosa (67).
Pancreatic contusions, with or without associated ductal disruption, are difficult to diagnose in patients with blunt abdominal trauma (68). Patients clearly at risk include those with significant mechanisms including high force, a seatbelt sign on physical examination, or a blow to the epigastrium (69). The initial CT scan may show nonspecific stranding of the pancreas. Associated fluid around the pancreas should prompt further invasive studies such as ERCP or magnetic resonance cholangiopancreatography (MRCP) to rule out a biliary or pancreatic duct injury. With a tentative diagnosis of a pancreatic contusion, one may consider following serial determinations of amylase/lipase; although these lab studies do not have a reliable sensitivity (70), increasing values over time combined with an alteration in clinical exam should prompt a repeat CT scan, a duodenal C-loop study, a DPL, or an ERCP depending upon the suspected lesion.
Postoperative Management of Specific Injuries
In addition to the global resuscitation of the trauma patient, ICU oversight must include management of injuries found at operative exploration. Communication between the operating surgeon and the intensivist is critical, and should include intraoperative findings and procedures, any tenuous operative repairs, anticipated problems or complications, the need for repeat operative exploration, and location of drains. The intraoperative estimated blood loss (EBL) and associated blood product transfusion requirements are essential data to anticipate events in the postoperative period. The transfusion information should include whether a massive transfusion protocol was initiated, entailing a 1:1 ratio of packed red blood cells to FFP, or any objective evidence of clinical coagulopathy during operative treatment. Finally, all clinicians caring for the patient should remember that injuries can be missed even with prior operative intervention.
Liver and Spleen Injuries
Although the majority of patients are successfully managed with nonoperative treatment, hemodynamically unstable patients or those with associated injuries may require urgent operative temporization of their solid organ injuries.
Life-threatening bleeding from the liver is most often controlled with perihepatic liver packing or sometimes with additional Foley catheter tamponade of deep lacerations (Fig. 75.9). Immediate concerns in the postoperative period are rebleeding and parenchymal ischemia. Signs of rebleeding are a falling hematocrit, blood clots accumulating under a temporary abdominal closure device, and bloody output from the Jackson-Pratt (JP) drains placed under the temporary abdominal closure covering; the magnitude of hemorrhage is reflected in hemodynamic instability and continued acidosis. Patients with recurrent hemorrhage may be treated with angioembolization or may necessitate repeat operative packing depending on the rate of bleeding (38). Hepatic ischemia is usually due to either a prolonged intraoperative Pringle maneuver or hepatic artery ligation; patients with the former should have an elevation but subsequent resolution of their transaminases while those with the latter may have frank hepatic necrosis. Patients are typically returned to the operating room for pack removal 24 to 48 hours after initial injury. Other long-term sources of morbidity are similar to patients undergoing nonoperative management, and include intra-abdominal abscess, biloma, and hemobilia. Although patients should be evaluated for infectious complications, complex liver trauma patients not infrequently have intermittent “liver fever” for the first 5 postinjury days (71).
|
|
|
Figure 75.8. Bowel injuries following blunt trauma include perforation due to ischemia from an avulsed mesentery (A), a direct antimesenteric blowout injury (B), and a blunt serosal injury (C). |
Operative intervention for splenic injuries includes splenectomy and splenorrhaphy. Postoperative hemorrhage may be due to the splenic hilar vessel tie loosening, a missed short gastric artery, or recurrent bleeding from the spleen if splenic repair was used. An immediate postsplenectomy increase in platelets and white blood cells (WBCs) is normal; however, beyond postoperative day 5 a WBC count above 15,000 should prompt a thorough search for underlying infection (72). Additional sources of morbidity include a concurrent but unrecognized iatrogenic injury to the pancreatic tail during rapid splenectomy resulting in pancreatic ascites or fistula. Patients have an increased incidence of intra-abdominal abscesses in the left upper quadrant following splenectomy with concomitant gastrointestinal injury, but presumptive drainage does not prevent this complication. Routine care also includes immunizations for encapsulated organisms (Streptococcus pneumoniae, Haemophilus influenzae, and Meningococcus) usually just prior to discharge, optimally at 2 to 3 weeks postsplenectomy (73).
Gastrointestinal Injuries
Operative intervention for either penetrating or blunt gastrointestinal injuries entails primary repair, resection with primary anastomosis, or resection with a stoma diversion. Regardless of the type of operation or the type of anastomosis (stapled vs. sewn) (74), one should await resolution of the patient's expected postoperative ileus. Return of bowel function is noted by a decrease in gastrostomy or NGT output and the passing of flatus or stool. If an ileostomy or colostomy was required, one should inspect it daily to ensure it is pink without evidence of necrosis. Postoperative complications include anastomotic leak, prolonged ileus, and bowel obstruction. A leak with intra-abdominal contamination or sepsis presents with increasing abdominal pain, fevers, and respiratory compromise in the extubated patient, or persistent fevers and intolerance of enteral feeding in the intubated patient. CT scan is diagnostic and repeat operation is often required.
|
|
|
Figure 75.9. Perihepatic liver packing or Foley catheter tamponade of deep lacerations is employed to halt hepatic hemorrhage (A); subsequent abdominal imaging shows the radiopaque markers of operatively placed laparotomy pads around the liver (B). |
Important questions for the intensivist following operative intervention for pancreatic injuries include how much of the pancreas was resected, is there a pancreaticoenteric anastomosis, was the pancreatic stump closed with either staples and/or fibrin glue, was the spleen preserved, and where were drains placed (77)? Closed suction drains should remain in place until the patient is tolerating an oral diet or enteral nutrition with the associated drain output being less than 30 mL/day. Postoperative complications include pancreatic fistula, pseudocyst, abscess, pancreaticoenteric leak, and pancreatitis. The most common of these is a pancreatic fistula, occurring in 7% to 20% of patients with isolated pancreatic trauma including the major duct, and in up to 35% of patients with combined pancreatic and duodenal injuries (76). Diagnosis in patients with drains in place is defined as output greater than 30 mL/day with an amylase level three times greater than serum value after postoperative day 5 (77). In patients without drains in place who have persistent abdominal pain, fevers, or intolerance of oral intake, CT scan imaging should be performed to evaluate for an intra-abdominal fluid collection. Drainage by interventional radiology (IR) is performed for fistula diagnosis and control. Pancreatic fistulae following trauma are managed in an identical fashion to those occurring following elective pancreatic resection (77).
Abdominal Vascular Injuries
Vascular injuries can produce rapid exsanguination and threaten extremities, or may be a clinically silent time bomb due to temporary retroperitoneal tamponade. Few result in a delayed diagnosis, particularly with CT scanning, and hence the focus of the intensivist is postoperative management. In general, outcome following vascular injuries is related to the technical success of the operation; the main causes of patient morbidity and mortality are associated soft tissue and nerve injuries once the vascular repair has been accomplished. Therefore, optimizing the patient's hemodynamic status, maintaining euthermia, and correcting coagulopathy are critical points of resuscitation. Prosthetic graft infections are rare complications (78) but preventing bacteremia is imperative; administration of perioperative antibiotics and treatment of secondary infections are indicated. Long-term arterial graft complications such as stenosis or pseudoaneurysms are uncommon, and routine graft surveillance is rarely performed. Consequently, long-term antiplatelet agents or antithrombotics are not routine.
There are specific injuries that require additional care. Abdominal aortic injuries are repaired using either a polytetrafluoroethylene (PTFE) patch or interposition grafting; the patient's systolic blood pressure should not exceed 120 mm Hg for at least the first 72 hours postoperatively. Patients requiring ligation of an inferior vena cava injury often develop marked bilateral lower extremity edema; to limit the associated morbidity the patient's legs should be wrapped with ACE bandages from the toes to the hips and elevated at a 45- to 60-degree angle. For superior mesenteric vein injuries, either ligation or thrombosis following venorrhaphy results in marked bowel edema; fluid resuscitation should be aggressive and abdominal pressure monitoring routine in these patients. In complex hepatic trauma, the right or left hepatic artery, or in urgent situations, the portal vein may be selectively ligated; persistent elevation in liver transaminases indicates secondary liver parenchymal necrosis and may necessitate delayed resection. Of note, if the right hepatic artery is ligated intraoperatively, cholecystectomy is performed concurrently.
Abdominal Wounds
In general, wounds sustained from trauma should be examined daily for progression of healing and signs of infection. Complex soft tissue wounds of the abdomen, such as degloving injuries following blunt trauma (termed Morel-Lavallee lesions), shotgun wounds, and other destructive blast injuries, are particularly difficult to manage. Following initial debridement of devitalized tissue, wound care includes wet-to-dry dressing changes twice daily, or application of the wound vacuum-assisted closure (VAC). One should carefully watch for infection, development of necrotizing fasciitis, subcutaneous abscess, or associated undrained hematoma. Repeated operative débridements may be necessary, and early involvement of the reconstructive surgery service for possible flap coverage is advised.
Midline laparotomy wounds are inspected 48 hours postoperatively by removing the sterile surgical dressing. If the patient develops high-grade fevers, inspection of the wound should be done sooner to exclude an early necrotizing infection. If a wound infection is identified—evidenced by erythema, pain along the wound, or purulent drainage—the wound should be widely opened by removing skin staples. After ensuring that the midline fascia is intact with digital palpation, the wound is managed with wet-to-dry dressing changes.
Damage Control Surgery
Damage control surgery (DCS) is an abbreviated operation whose goals are to control hemorrhage, limit contamination from enteric sources, and enable rapid transport to the ICU for correction of adverse physiology (79,80). There are standard indications for performing the DCS abbreviated laparotomy in patients with unresolved metabolic failure (Table 75.6). Intraoperative techniques of DCS include perihepatic packing, balloon tamponade of deep liver lacerations, segmental stapled bowel resection left in discontinuity, ligation of abdominal venous injuries, shunting of abdominal arterial injuries, and pancreatic drainage.
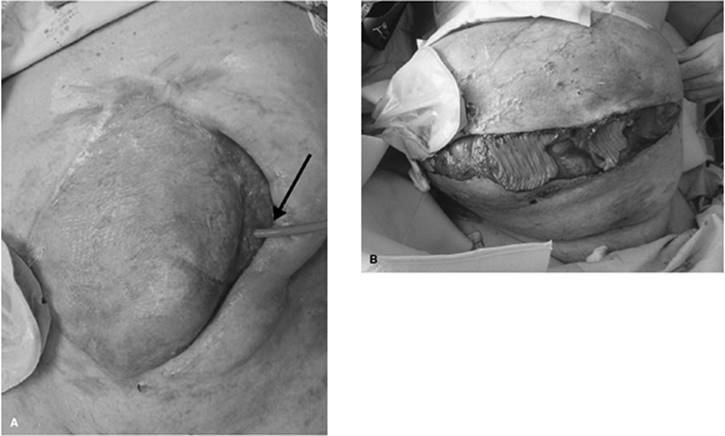
Following DCS, the surgeon will “close” the abdomen with a temporary closure device. Options for temporary closure include Bogotá bag closure (a 3-L Urology irrigation bag), 1010 Steri-Drape (3M Health Care, St. Paul, MN) and Ioban closure, and wound VAC dressing (Fig. 75.10). In the majority of major trauma centers, the patient's abdomen is closed with the 1010 Steri-Drape and Ioban closure after the first operation and with the VAC following additional operative explorations. The temporary abdominal closure allows egress of abdominal contents and contains the edematous bowel while providing excellent decompression. Jackson-Pratt drains are placed under the Ioban covering to control the marked effluent from third spacing during fluid resuscitation.
|
Table 75.6 Intraoperative indications to perform damage control surgery |
||||||||||
|
||||||||||
Upon transfer to the ICU, aggressive resuscitation of the patient is performed to reverse metabolic failure (81). This includes vigorous rewarming through heating the room, infusion of fluids and blood products through a warming device, and use of a warming device such as the Bair Hugger (Augustine Medical, Inc., Eden Prairie, MN); more aggressive measures may include warm saline irrigation of the stomach, chest, and abdominal cavities via an NGT, thoracostomy tubes, and DPL catheters. Continuous arteriovenous rewarming may be warranted for refractive temperatures <34°C. Restoration of a normal cardiovascular state is attained by infusion of fluids and blood products, as well as judicious use of vasopressor agents. Finally, the patient's coagulopathy must be reversed with appropriate blood products including fresh frozen plasma, cryoprecipitate, and platelets. Occasionally recombinant activated factor VII (rFVIIa; NovoSeven, NovoNordisk, Denmark) is needed. Ideally, physiologic correction should occur within 12 to 24 hours of admission to the ICU, with planned return to the operating room for definitive repair.
There are several specific management points of the patient with an open abdomen that deserve mention. Despite a widely open abdomen, patients can develop abdominal compartment syndrome (ACS) (82); therefore, bladder pressures should be monitored every 4 hours, with significant increases in pressures alerting the clinician to the possible need for repeat operative intervention and abdominal decompression. Patients with an open abdomen lose between 500 and 2,500 mL/day of abdominal effluent. Appropriate volume compensation for this albumin-rich fluid remains controversial, both in the amount administered (replacement based on clinical indices vs. routine 1/2-mL replacement for every milliliter lost) as well as the type of replacement (crystalloid vs. colloid/blood products). Patients with abdominal packing in place, particularly for liver lacerations, may rebleed from such injuries. In these situations, the patient may begin to exsanguinate from the abdomen through the JP drains placed under the Ioban covering. Rapid clamping of the abdominal JP drains with blood product resuscitation may provide enough intra-abdominal pressure and subsequent tamponade to stabilize the patient for reoperation. Alternatively, bedside laparotomy with repacking of the liver is an option. In patients suffering cardiac arrest from hemorrhage, removing the temporary abdominal closure dressing at the bedside with aortic and portal triad clamping is warranted.
|
|
|
Figure 75.10. Methods of temporary abdominal closure following damage control surgery or operative decompression for abdominal compartment syndrome: Bogotá bag closure (A), 1010 Steri-Drape and Ioban closure (B), and vacuum-assisted closure dressing (C). |
Abdominal Compartment Syndrome
The abdominal compartment syndrome is typified by intra-abdominal hypertension due to either intra-abdominal injury (primary) or following massive resuscitation (secondary) (83,84,85,86,87). Secondary ACS may be due to any etiology requiring such a resuscitation, including extremity trauma, isolated head injury, chest trauma, or even following postinjury related sepsis (88). The large volumes of crystalloid required to manage multiply injured patients results in resuscitation-associated bowel edema, retroperitoneal edema, or large quantities of ascitic fluid. A diagnosis of intra-abdominal hypertension cannot be definitively made by physical examination, but is obtained by measuring bladder pressures. To measure a patient's bladder pressure, 50 mL of saline is instilled into the bladder via the aspiration port of the Foley catheter with the drainage tube clamped; a three-way stopcock and water manometer is placed at the level of the pubic symphysis (89). Bladder pressures are then measured on the manometer in centimeters of water (Table 75.7) and correlate with the physiologic impact of ACS. Conditions in which the bladder pressure is unreliable include bladder rupture, external compression from pelvic packing, neurogenic bladder, and adhesive disease.
|
Table 75.7 Abdominal compartment syndrome grading system based upon bladder pressure measurements |
||||||||||
|
|
|
|
Figure 75.11. Physiologic derangements associated with intra-abdominal hypertension leading to abdominal compartment syndrome. ICP, intracranial pressure; UOP, urine output; CO, cardiac output; VEDV, ventricular end-diastolic volume; SV, stroke volume; SVR, systemic vascular resistance; PA, pulmonary artery; CVP, central venous pressure. |
Increased abdominal pressure affects multiple organ systems (Fig. 75.11). The ACS, however, is defined by intra-abdominal hypertension causing such end organ sequelae as decreased urine output, increased pulmonary pressures, decreased preload and subsequent cardiac dysfunction, and even elevated intracranial pressure (ICP) (83). As any of these clinical manifestations of ACS may be attributed to the primary injury, a heightened awareness of this entity must be maintained. Organ failure can occur over a wide range of recorded bladder pressures; there is not a single measurement of bladder pressure that prompts therapeutic intervention, except >35 cm H2O. Rather, emergent decompression is warranted in the patient with intra-abdominal hypertension with end organ dysfunction. Mortality is directly affected by decompression, with 64% mortality in patients undergoing presumptive decompression, 70% mortality in patients with a delay in decompression, and 89% mortality in those without decompression (90).
Decompression is typically performed operatively either at the bedside in the ICU if the patient is hemodynamically unstable, or in the operating room. Bedside laparotomy is easily accomplished, precludes transport in hemodynamically compromised patients, and requires minimal equipment (scalpel, suction, cautery, and abdominal temporary closure dressings). Patients with significant intra-abdominal fluid as the primary component of their ACS, rather than bowel or retroperitoneal edema, may be candidates for decompression via a percutaneous drain (91,92). Differentiation of those amenable to such drainage is determined by bedside ultrasound, hence obviating a trip to the operating room for a critically ill patient (Fig. 75.12).
|
|
|
Figure 75.12. Bedside ultrasound of the abdomen demonstrates resuscitation-induced ascites (A, B); placement of a pigtail drain (C) over the liver may evacuate enough fluid to reduce the intra-abdominal pressure and associated abdominal compartment syndrome organ failure. |
|
|
|
Figure 75.13. Complications of the open abdomen include intra-abdominal abscess, bile leaks, enteric fistula (A), and bowel perforations (B). |
With morbidity and mortality rates exceeding 50% (82,86,93), patients at risk for development of ACS, particularly those receiving large amounts of crystalloid and blood products during shock resuscitation, should be evaluated closely. Development of secondary ACS is a particularly indolent process; decreasing urine output and increasing peak airway pressures may herald the onset of intra-abdominal hypertension. Moreover, despite prior decompression with temporary abdominal closure, patients may develop recurrent ACS, which impacts overall morbidity and mortality (82). Some clinicians have queried aggressive intervention to prevent the development of ACS, such as the role of limiting unnecessary volume resuscitation and the use of alternative fluids such as colloids (15); however, the choice of albumin for fluid resuscitation in the intensive care unit has always been questioned (94). Supranormal trauma resuscitation has been shown to require more crystalloid administration and to cause more cases of ACS (86); therefore, goal-directed therapy should aim for an oxygen delivery index of ≥500 mL/minute/m2 (10). Although perhaps counterintuitive in the acute resuscitation of patients, early administration of vasoactive agents to reduce the volume of crystalloid administered might be a therapeutic alternative in these patients at risk for ACS. In patients with acute renal failure, with minimal to no urine output, judicious fluid administration, early use of pressors, and institution of renal replacement therapy prior to fluid overload may also be warranted.
Damage control surgery and the recognition of the abdominal compartment syndrome have improved patient outcomes but at the cost of an open abdomen. Over 20% of patients with an open abdomen suffer a significant number of gastrointestinal complications that prolong their hospital course. Reported complications include intra-abdominal abscess, bile leaks, enteric fistula, and bowel perforations (Fig. 75.13) (95). Management includes operative or percutaneous drainage of abscesses, ERCP and drainage of bilomas, and control of fistulae and nutritional support for bowel complications. Current research is under way to develop techniques to minimize complications and reduce morbidity in patients with these devastating injuries.
Ancillary Care Issues
Tubes and Drains
Following operative or nonoperative management of abdominal injuries, patients may have a variety of tubes and drains. Intra-abdominal drains are typically closed suction drains such as JP or Blake drains; the amount from the drain should be quantified every 8-hour shift, and the character of the output (bilious, succus, bloody, etc.) from the drains should be monitored daily. Although general guidelines for drain removal are <30 to 50 mL/day, one should consult with the surgeon prior to removal. Patients with rectal injuries may have presacral drains placed, which consist of Penrose drains exiting next to the rectum; these are passive drains, and should be covered with ABD pads for appropriate coverage. Patients with open abdomens and temporary abdominal closure will often have drains of some type; again, quantity and quality of the effluent may guide treatment options such as intravenous fluid replacement and need for return to the operating room.
Enteral access for nutrition is acquired through multiple techniques. NGTs, placed for gastric decompression, can be used for enteral nutrition once NGT output drops off. Gastrostomy tubes, either percutaneously or operatively placed, exit the abdominal cavity in the left upper quadrant. These should be placed to gravity for 24 hours after initial insertion. Jejunal feeding tubes are operatively placed; surgeons may choose to use needle catheter jejunostomy (NCJ) tubes or red rubber catheters. The primary issues with jejunal feeding tubes are those encountered with NCJs. Due to the small caliber of the feeding tube, there is the propensity for clogging. The NCJ should be flushed every 6 hours with saline, and only NCJ compatible enteral formulas should be used. Additionally, no medications should be placed down the NCJ. Nasojejunal tubes, often called nasobiliary feeding tubes, may be placed in the ICU using upper endoscopy.
Nutrition
Although the topic of nutrition could encompass an entire textbook, a few issues warrant mention (96). Multiple studies have illustrated the importance of early total enteral nutrition (TEN) in the trauma population, particularly its impact in reducing septic complications (97,98,99,100). The route of enteral feedings, stomach versus small bowel, tends to be less important as gut tolerance appears equivalent unless there is upper gastrointestinal pathology (101,102). Although early enteral nutrition is the goal, one should be cognizant of any bowel anastomoses; typically, evidence of bowel function should be present prior to advancing to goal tube feeds. Overzealous jejunal feeding can lead to small necrosis, a devastating complication (103). Patients undergoing monitoring for nonoperative management of solid organ injuries should remain NPO in the first 24 to 48 hours in case they require an operation. There is some residual concern about TEN in patients with an open abdomen; tube feeding, by any route, may be started within 24 hours of abdominal closure, as over 90% of patients will tolerate TEN (104,105). Moreover, in patients relegated to an open abdomen, TEN should be started. The role of trophic tube feeds (10–20 mL/hour) while actively attempting to close fascia remains controversial.
Prophylaxis
A critical component of the overall care of the multiply injured patient in the ICU includes prevention of secondary complications, such as deep venous thrombosis (DVT) and stress gastritis. Administration of heparinoids for the prevention of DVT following trauma or surgical intervention is the current standard of care (106). Issues following abdominal trauma include timing of such administration in patients with either active bleeding from traumatic injury or those with solid organ injuries. Typically, heparin products are held until patients have resolved their hemorrhagic diathesis or until 24 hours after their hemoglobin has stabilized. Carafate is the current drug of choice for the prevention of stress gastritis (107,108). In patients who have had specific gastric surgery, H2 blockers may be used as an alternative.
References
1. Janjua KJ, Sugrue M, Deane SA. Prospective evaluation of early missed injuries and the role of tertiary trauma survey. J Trauma. 1998;44:1000–1006; discussion 1006–1007.
2. Biffl WL, Harrington DT, Cioffi WG. Implementation of a tertiary trauma survey decreases missed injuries. J Trauma. 2003;54:38–43; discussion 43–44.
3. Enderson BL, Reath DB, Meadors J, et al. The tertiary trauma survey: a prospective study of missed injury. J Trauma. 1990;30:666–669; discussion 669–670.
4. Brooks A, Holroyd B, Riley B. Missed injury in major trauma patients. Injury. 2004;35:407–410.
5. Buduhan G, McRitchie DI. Missed injuries in patients with multiple trauma. J Trauma. 2000;49:600–605.
6. Moore FA, McKinley BA, Moore EE, et al. Inflammation and the Host Response to Injury, a large-scale collaborative project: patient-oriented research core—standard operating procedures for clinical care. III. Guidelines for shock resuscitation. J Trauma. 2006;61:82–89.
7. Herbert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled trial of transfusion requirements in critical care. N Engl J Med. 1999;340:409–417.
8. Moore FA, Moore EE, Sauaia A. Blood transfusion. An independent risk factor for postinjury multiple organ failure. Arch Surg. 1997;132:620–624; discussion 624–625.
9. Abou-Khalil B, Scalea TM, Trooskin SZ, et al. Hemodynamic responses to shock in young trauma patients: need for invasive monitoring. Crit Care Med. 1994;22:633–639.
10. McKinley BA, Kozar RA, Cocanour CS, et al. Normal versus supranormal oxygen delivery goals in shock resuscitation: the response is the same. J Trauma. 2002;53:825–832.
11. Velmahos GC, Demetriades D, Shoemaker WC, et al. Endpoints of resuscitation of critically injured patients: normal or supranormal? A prospective randomized trial. Ann Surg. 2000;232:409–418.
12. Cooper MS, Stewart PM. Corticosteroid insufficiency in acutely ill patients. N Engl J Med. 2003;348:727–734.
13. Offner PJ, Moore EE, Ciesla D. The adrenal response after severe trauma. Am J Surg. 2002;184:649–653.
14. Balogh Z, McKinley BA, Holcomb JB, et al. Both primary and secondary abdominal compartment syndrome can be predicted early and are harbingers of multiple organ failure. J Trauma. 2003;54:848–859.
15. Balogh Z, McKinley BA, Cocanour CS, et al. Secondary abdominal compartment syndrome is an elusive early complication of traumatic shock resuscitation. Am J Surg. 2002;184:538–543.
16. Carrillo EH, Wohltmann C, Richardson JD, et al. Evolution in the treatment of complex blunt liver injuries. Curr Probl Surg. 2001;38:1–60.
17. Hurtuk M, Reed RL, Espositio TJ, et al. Trauma surgeons practice what they preach: the NTDB story on solid organ injury management. J Trauma. 2006;61:243–255.
18. Peitzman AB, Heil B, Rivera L, et al. Blunt splenic injury in adults: multi-institutional study of the Eastern Association for the Surgery of Trauma. J Trauma. 2000;49:177–187.
19. Richardson DJ, Franklin GA, Lukan JK, et al. Evolution in the management of hepatic trauma: a 25-year perspective. Ann Surg. 2000;232:324–330.
20. Velmahos GC, Toutouzas KG, Radin R, et al. Nonoperative treatment of blunt injury to solid abdominal organs: a prospective study. Arch Surg. 2003;138:844–851.
21. Malhotra AK, Fabian TC, Croce MA, et al. Blunt hepatic injury: a paradigm shift from operative to nonoperative management in the 1990s. Ann Surg. 2000;231:804–813.
22. Pachter HL, Guth AA, Hofstett SR, et al. Changing patterns in the management of splenic trauma: the impact of nonoperative trauma. Ann Surg. 1998;227:708–717; discussion 717–719.
23. Christmas AB, Wilson AK, Manning B, et al. Selective management of blunt hepatic injuries including nonoperative management is a safe and effective strategy. Surgery. 2005;138:606–610.
24. Velmahos GC, Toutousas K, Radin R, et al. High success with nonoperative management of blunt hepatic trauma: the liver is a sturdy organ. Arch Surg. 2003;138:475–480; discussion 480–481.
25. Rojani RR, Claridge JA, Yowler CJ, et al. Improved outcome of adult blunt splenic injury: a cohort analysis. Surgery. 2006;140:625–631; discussion 631–632.
26. Goan YG, Huang MS, Lin JM. Nonoperative management for extensive hepatic and splenic injuries with significant hemoperitoneum in adults. J Trauma. 1998;45:360–364; discussion 365.
27. Nwomeh BC, Nadler EP, Meza MP, et al. Contrast extravasation predicts the need for operative intervention in children with blunt splenic trauma. J Trauma. 2004;56:537–541.
28. Malhotra AK, Latifi R, Fabian TC, et al. Multiplicity of solid organ injury: influence on management and outcomes after blunt abdominal trauma. J Trauma. 2003;54:925–929.
29. Schurr MJ, Fabian TC, Gavant M, et al. Management of blunt splenic trauma: computed tomographic contrast blush predicts failure of nonoperative management. J Trauma. 1995;39:507–512; discussion 512–513.
30. Falimirski ME, Provost D. Nonsurgical management of solid abdominal organ injury in patients over 55 years of age. Am Surg. 2000;66:631–635.
31. Myers JG, Dent DL, Stewart RM, et al. Blunt splenic injuries: dedicated trauma surgeons can achieve a high rate of nonoperative success in patients of all ages. J Trauma. 2000;48:801–805; discussion 805–806.
32. Harbrecht BG, Peitzman AB, Rivera L, et al. Contribution of age and gender to outcome of blunt splenic injury in adults: multicenter study of the Eastern Association for the Surgery of Trauma. J Trauma. 2001;51:887–895.
33. Moore EE, Cogbill TH, Jurkovich GJ, et al. Organ injury scaling: spleen and liver (1994 revision). J Trauma. 1995;38:323–324.
34. Moore EE, Cogbill TH, Malangoni MA, et al. Organ injury scaling. Surg Clin North Am. 1995;75:293–303.
35. Moore EE, Cogbill TH, Malangoni MA, et al. Organ injury scaling, II: pancreas, duodenum, small bowel, colon, and rectum. J Trauma. 1990;30:1427–1429.
36. Watson GA, Rosengart MR, Zenati MS, et al. Nonoperative management of severe blunt splenic injury: are we getting better? J Trauma. 2006;61:1113–1118.
37. Johnson JW, Gracias VH, Gupta R, et al. Hepatic angiography in patients undergoing damage control laparotomy. J Trauma. 2002;52:1102–1106.
38. Denton JR, Moore EE, Coldwell DM. Multimodality treatment for grade V hepatic injuries: perihepatic packing, arterial embolization, and venous stenting. J Trauma. 1997;42:964–967.
39. Haan JM, Biffl WL, Knudson MM, et al. Splenic embolization revisited: a multicenter review. J Trauma. 2004;56:542–547.
40. Dent D, Alsabrook G, Erickson BA, et al. Blunt splenic injuries: high nonoperative management rate can be achieved with selective embolization. J Trauma. 2004;56:1063–1067.
41. Davis KA, Fabian ATC, Croce MA, et al. Improved success in nonoperative management of blunt splenic injuries: embolization of splenic artery pseudoaneurysms. J Trauma. 1998;44:1008–1013; discussion 1013–1015.
42. Lyass S, Sela T, Lebensart PD, et al. Follow-up imaging studies of blunt splenic injury: do they influence management? Isr Med Assoc. 2001;10:731–733.
43. Cox JC, Fabian TC, Maish GO 3rd, et al. Routine follow-up imaging is unnecessary in the management of blunt hepatic injury. J Trauma. 2005;59:1175–1178; discussion 1178–1180.
44. Patton JH Jr, Lyden SP, Croce MA, et al. Pancreatic trauma: a simplified management guideline. J Trauma. 1997;43:234–239; discussion 239–241.
45. Wales PW, Shuckett B, Kim PC. Long-term outcome after nonoperative management of complete traumatic pancreatic transection in children. J Pediatr Surg. 2001;36:823–827.
46. Jobst MA, Canty TG, Lynch FP. Management of pancreatic injury in pediatric blunt abdominal trauma. J Pediatr Surg. 1999;34:818–823.
47. Lin BC, Liu NJ, Fang JF, et al. Long-term results of endoscopic stent in the management of blunt major pancreatic duct injury. Surg Endosc. 2006;20:1551–1555.
48. Cogbill TH, Moore EE, Feliciano DV. Conservative management of duodenal trauma: a multicenter perspective. J Trauma. 1990;30:1469–1475.
49. Huerta S, Bui T, Porral D, et al. Predictors of morbidity and mortality in patients with traumatic duodenal injuries. Am Surg. 2005;71:763–767.
50. Demetriades D, Gomez H, Chahwan S, et al. Gunshot injuries to the liver: the role of selective nonoperative management. J Am Coll Surg. 1999;188:343–348.
51. Moore EE. When is nonoperative management of a gunshot wound to the liver appropriate? J Am Coll Surg. 1999;188:427–428.
52. Chiu WC, Shanmuganathan K, Mirvis SE, et al. Determining the need for laparotomy in penetrating torso trauma: a prospective study using triple-contrast enhanced abdominopelvic computed tomography. J Trauma. 2001;51:860–868; discussion 868–869.
53. Demetriades D, Hadjizacharia P, Constantinou C, et al. Selective nonoperative management of penetrating abdominal solid organ injuries. Ann Surg. 2006;244:620–628.
54. Kozar RA, Moore FA, Cothren CC, et al. Risk factors for hepatic morbidity following nonoperative management: multicenter study. Arch Surg. 2006;141:451–459.
55. Giss SR, Dobrilovic N, Brown RL, et al. Complications of nonoperative management of pediatric blunt hepatic injury: diagnosis, management, and outcomes. J Trauma. 2006;61:334–339.
56. Goldman R, Zilkowski M, Mullins R, et al. Delayed celiotomy for the treatment of bile leak, compartment syndrome, and other hazards of nonoperative management of blunt liver injury. Am J Surg. 2003;185:492–497.
57. Cocanour CS, Moore FA, Ware DN, et al. Delayed complications of nonoperative management of blunt adult splenic trauma. Arch Surg. 1998;133:619–624; discussion 624–625.
58. Cothren CC, Biffl WL, Moore EE, et al. Characteristic radiographic findings of post-injury splenic autotransplantation: avoiding a diagnostic dilemma. J Trauma. 2004;57(3):537–541.
59. Fakhry SM, Watts DD, Luchette FA; EAST Multi-Institutional Hollow Viscus Injury Research Group. Current diagnostic approaches lack sensitivity in the diagnosis of perforated blunt small bowel injury: analysis from 275,557 trauma admissions from the EAST multi-institutional HVI trial. J Trauma. 2003;54:295–306.
60. Fakhry SM, Brownstein M, Watts DD, et al. Relatively short diagnostic delays (<8 hours) produce morbidity and mortality in blunt small bowel injury: an analysis of time to operative intervention in 198 patients from a multicenter experience. J Trauma. 2000;48:408–414.
61. Niederee MJ, Byrnes MC, Helmer SD, et al. Delay in diagnosis of hollow viscus injuries: effect on outcome. Am Surg. 2003;69:293–298.
62. Ng AK, Simons RK, Torreggiani WC, et al. Intra-abdominal free fluid without solid organ injury in blunt abdominal trauma: an indication for laparotomy. J Trauma. 2002;52:1134–1140.
63. Miller PR, Croce MA, Bee TK, et al. Associated injuries in blunt solid organ trauma: implications for missed injury in nonoperative management. J Trauma. 2002;53:238–242.
64. Rodriguez C, Barone JE, Wilbanks TO, et al. Isolated free fluid on computed tomographic scan in blunt abdominal trauma: a systematic review of incidence and management. J Trauma. 2002;53:79–85.
65. McAnena OJ, Marx JA, Moore EE. Peritoneal lavage enzyme determinations following blunt and penetrating abdominal trauma. J Trauma. 1991;31:1161–1164.
66. Heneman PL, Marx JA, Moore EE, et al. Diagnostic peritoneal lavage: accuracy in predicting necessary laparotomy following blunt and penetrating trauma. J Trauma. 1990;30:1345–1355.
67. Velmahos GC, Gomez H, Falabella A, et al. Operative management of civilian rectal gunshot wounds: simpler is better. World J Surg. 2000;24:114–118.
68. Leppaniemi AK, Haapiainen RK. Risk factors of delayed diagnosis of pancreatic trauma. Eur J Surg. 1999;165:1134–1137.
69. Arkovitz MS, Johnson N, Garcia VF. Pancreatic trauma in children: mechanisms of injury. J Trauma. 1997;42:49–53.
70. Takishima T, Sugimoto K, Hirata M, et al. Serum amylase level on admission in the diagnosis of blunt injury to the pancreas: its significance and limitations. Ann Surg. 1997;226:70–76.
71. Cogbill TH, Moore EE, Feliciano DV, et al. Hepatic enzyme response and hyperpyrexia after severe liver injury. Am Surg. 1992;58:395–399.
72. Weng J, Brown CVR, Rhee P, et al. White blood cell and platelet counts can be used to differentiate between infection and the normal response after splenectomy for trauma: prospective validation. J Trauma. 2005;59:1076–1080.
73. Howdieshell TR, Heffernan D, Dipiro JT. Therapeutic Agents Committee of the Surgical Infection Society. Surgical infection society guidelines for vaccination after traumatic injury. Surg Infect. 2006;7:275–303.
74. Demetriades D, Murray JA, Chan L, et al. Penetrating colon injuries requiring resection: diversion or primary anastomosis? An AAST prospective multicenter study. J Trauma. 2001;50:765–775.
75. Conlon KC, Labow D, Leung D, et al. Prospective randomized clinical trial of the value of intraperitoneal drainage after pancreatic resection. Ann Surg. 2001;234:487–493; discussion 493–494.
76. Ridgeway MG, Stabile BE. Surgical management and treatment of pancreatic fistulas. Surg Clin North Am. 1996;76:1159–1173.
77. Howard TJ, Stonerock CE, Sarkar J, et al. Contemporary treatment strategies for external pancreatic fistulas. Surgery. 1998;124:627–632.
78. Wolford HY, Cothren CC, Moore EE. Postinjury abdominal aortic graft infection: documentation and successful management. J Trauma. 2006;61:1274–1276.
79. Moore EE, Burch JM, Franciose RJ, et al. Staged physiologic restoration and damage control surgery. World J Surg. 1998;22:1184–1190; discussion 1190–1191.
80. Hirshberg A, Walden R. Damage control for abdominal trauma. Surg Clin North Am. 1997;77:813–820.
81. Sagraves SG, Toschlog EA, Rotondo MF. Damage control surgery—the intensivist's role. J Intensive Care Med. 2006;21:5–16.
82. Raeburn CD, Moore EE, Biffl WL, et al. The abdominal compartment syndrome is a morbid complication of postinjury damage control surgery. Am J Surg. 2001;182:542–546.
83. Burch JM, Moore EE, Moore FA, et al. The abdominal compartment syndrome. Surg Clin North Am. 1996;76:833–842.
84. Meldrum DR, Moore FA, Moore EE, et al. Prospective characterization and selective management of the abdominal compartment syndrome. Am J Surg. 1997;174:667–672.
85. Ivatury RR, Porter JM, Simon RJ, et al. Intra-abdominal hypertension after life-threatening penetrating abdominal trauma: prophylaxis, incidence, and clinical relevance to gastric mucosal pH and abdominal compartment syndrome. J Trauma. 1998;44:1016–1021.
86. Balogh Z, McKinley BA, Cox Jr CS, et al. Abdominal compartment syndrome: the cause or effect of postinjury multiple organ failure. Shock. 2003;20:483–492.
87. Maxwell RA, Fabian TC, Croce MA, et al. Secondary ACS: an underappreciated manifestation of severe hemorrhagic shock. J Trauma. 1999;47:995–999.
88. McNelis J, Marini CP, Jurkiewicz A, et al. Predictive factors associated with the development of abdominal compartment syndrome in the surgical intensive care unit. Arch Surg. 2002;137:133–136.
89. Kron IL. A simple technique to accurately determine intra-abdominal pressure. Crit Care Med. 1989;17:714–715.
90. Cheatham ML, White MW, Sagraves SG, et al. Abdominal perfusion pressure: a superior parameter in the assessment of intra-abdominal hypertension. J Trauma. 2000;49:621–626.
91. Corcos AC, Sherman HF. Percutaneous treatment of secondary abdominal compartment syndrome. J Trauma. 2001;51:1062–1064.
92. Latenser BA, Kowal-Vern A, Kimball D, et al. A pilot study comparing percutaneous decompression with decompressive laparotomy for acute abdominal compartment syndrome in thermal injury. J Burn Care Rehabil. 2002;23:190–195.
93. Biffl WL, Moore EE, Burch JM, et al. Secondary abdominal compartment syndrome is a highly lethal event. Am J Surg. 2001;182:645–648.
94. Finfer S, Norton R, Bellomo R, et al. The SAFE study: saline vs. albumin for fluid resuscitation in the critically ill. Vox Sang. 2004;87(Suppl 2):123–131.
95. Miller RS, Morris JA Jr, Diaz JJ Jr, et al. Complications after 344 damage-control open celiotomies. J Trauma. 2005;59:1365–1371.
96. Jacobs DG, Jacobs DO, Kudsk KA, et al. Practice management guidelines for nutritional support of the trauma patient. J Trauma. 2004;57:660–678.
97. Moore FA, Moore EE, Jones TN, et al. TEN versus TPN following major abdominal trauma—reduced septic morbidity. J Trauma. 1989;29:916–922.
98. Moore FA, Feliciano DV, Andrassy RJ, et al. Early enteral feeding, compared with parenteral, reduces postoperative septic complications. The results of a meta-analysis. Ann Surg. 1992;216:172–183.
99. Moore FA, Moore EE, Haenel JB. Clinical benefits of early post-injury enteral feeding. Clin Intensive Care. 1995;6:21–27.
100. Hasenboehler E, Williams A, Leinhase I, et al. Metabolic changes after polytrauma: an imperative for early nutritional support. World J Emerg Surg. 2006;1:29.
101. Neumann DA, DeLegge MH. Gastric versus small-bowel tube feeding in the intensive care unit: a prospective comparison of efficacy. Crit Care Med. 2002;30:1436–1438.
102. Reignier J, Bensaid S, Perrin-Gachadoat D, et al. Erythromycin and early enteral nutrition in mechanically ventilated patients. Crit Care Med. 2002;30:1237–1241.
103. Melis M, Fichera A, Ferguson MK. Bowel necrosis associated with early jejunal tube feeding: a complication of postoperative enteral nutrition. Arch Surg. 2006;141:701–704.
104. Cothren CC, Moore EE, Ciesla DJ, et al. Post-injury abdominal compartment syndrome does not preclude early enteral feeding following definitive closure. Am J Surg. 2004;188:653–658.
105. Kozar RA, McQuiggan MM, Moore EE, et al. Postinjury enteral tolerance is reliably achieved by a standardized protocol. J Surg Res. 2002;104:70–75.
106. Rogers FB, Cipolle MD, Velmahos G, et al. Practice management guidelines for the prevention of venous thromboembolism in trauma patients: the EAST practice management guidelines work group. J Trauma. 2002;53:142–164.
107. Maier RV, Mitchell D, Gentilello L. Optimal therapy for stress gastritis. Ann Surg. 1994;220:353–360.
108. Eddleston JM, Vohra A, Scott P, et al. A comparison of the frequency of stress ulceration and secondary pneumonia in sucralfate- or ranitidine-treated intensive care unit patients. Crit Care Med. 1991;19:1491–1496.