H. DAVID REINES
HANI SEOUDI
An acute abdomen is any problem in which the patient's pain or other physical findings originates from an abdominal lesion resulting in serious morbidity or mortality without appropriate therapy.
As sicker patients are admitted to our intensive care units (ICUs), the challenge of diagnosis and treatment of the acute abdomen becomes more important. Patients who are immunocompromised from diseases such as HIV, posttransplant, or chemotherapy frequently present with a nonclassic sign of pain and inflammation. Patients who are post–cardiac surgery have a well-recognized constellation of intra-abdominal catastrophes. Bariatric surgery presents ICU physicians with a whole new set of intra-abdominal problems, which if not recognized early, can lead to death or significant morbidity.
Patients admitted to respiratory care units are subject to various acute abdominal problems. Aranha and Goldberg reported that 32 of 175 (18%) patients on ventilators had acute abdominal problems in the following order of frequency (1): gastrointestinal bleeding, ileus, bowel obstruction, and peritonitis that required operation. Acute abdominal problems are frequent sources of admission and complications in ICUs (2). Early recognition of the acute abdomen and initiation of definitive surgical or medical therapy often determines the outcome. Therefore, knowledge of common abdominal problems and appropriate diagnostic modalities are essential parts of the armamentarium of all ICU physicians. A high index of suspicion that an abdominal problem is causing a patient's critical illness is important to stimulate the necessary diagnostic and therapeutic responses.
Searching for a cause of abdominal signs and symptoms is difficult in the critically ill patient. The patient may not be able to give a lucid history, especially if intubated or sedated. Physical findings may be masked by narcotics, steroids, and other therapy administered.
Anatomy
The peritoneal cavity is a potential space with less than 100 mL of free fluid to lubricate the bowel, liver, and other abdominal organs. Knowledge of the sensory nerve supply of the abdomen is particularly important in evaluating the abdomen in critically ill patients. Deep visceral pain is transmitted via autonomic nerves, both sympathetic and parasympathetic. Visceral pain is poorly localized as pain receptors are much sparser than somatic receptors. The pain is typically unpleasant and is associated with autonomic symptoms such as tachycardia, bradycardia, and diaphoresis. The primary stimulus to visceral pain is stretching of hollow viscera or solid organ capsules. Visceral pain signals share common pathways with somatic pain in the spinothalamic tracts. Visceral pain signals are received in areas of the sensory cortex where somatic structures that originated from the same embryonic segment are represented. This is the reason why visceral pain tends to be referred to remote dermatomes, e.g., shoulder pain caused by diaphragmatic irritation. Abdominal pain becomes more localized when the parietal peritoneum is affected by the underlying inflammatory process. The parietal peritoneum has a rich somatic sensory supply.
Knowledge of the blood supply of the abdomen is also important given the extensive diagnostic and therapeutic applications of angiography in acute abdominal pathology. The foregut (esophagus to duodenum) is supplied by branches of the celiac trunk, the midgut (duodenum to distal transverse colon) is supplied by branches of the superior mesenteric artery (SMA), and the hindgut (descending colon and rectum) is supplied by branches of the inferior mesenteric artery (IMA). The right hepatic artery is replaced (arises from the SMA) in about 10% of the population. An embolus tends to lodge distal to the origins of the most proximal branches of the SMA, namely, the inferior pancreaticoduodenal, the middle colic, and the proximal jejunal branches. The proximal jejunum and the transverse colon are typically spared in acute ischemia due to SMA embolism compared to thrombosis. Collateral circulation exists between branches of the three mesenteric vessels. The marginal artery of Drummond is formed by the anastomosing branches of the SMA and IMA along the mesenteric border of the colon. The arc of Riolan connects the middle colic artery with the ascending branch of the left colic artery. The internal iliac artery contributes to colonic circulation through the anastomosis between the middle and superior rectal arteries.
History
A detailed review of abdominal symptoms should be obtained from either the patient or a family member. The history should include previous surgery, family history, and a list of medications. It should also include allergies, immunosuppressive drugs, and a history of human immunodeficiency virus (HIV), hepatitis, or chemotherapy. As we become more globalized, awareness of infectious disease from emerging countries is necessary for evaluation of disparate symptoms. A complete surgical history is likewise necessary to help focus on the diagnostic and therapeutic interventions. Previous abdominal surgery and hernias are the two most common causes of bowel obstruction. The presence of a percutaneous endoscopic gastrostomy (PEG) or other tubes should alert the physician to the possibility of a problem related to tube misplacement or obstruction. The history should detail any nausea and vomiting, hematemesis, hematochezia, and constipation. Symptoms of biliary disease, especially pain, and jaundice, and a history of ethanol use should be noted. Alcohol abuse and cholelithiasis are the two most common causes of acute pancreatitis.
A careful evaluation of the characteristics of abdominal pain is essential. Its nature, onset, associated symptoms, radiation, and other characteristics are useful in localizing and delineating the cause. Abdominal symptoms can be masked by other disease processes. A diabetic patient who presents with diabetic ketoacidosis may have an underlying abdominal catastrophe as a precipitating factor. Syncope is a symptom that can be caused by ruptured aneurysm, a ruptured spleen, an ectopic pregnancy, or any severe abdominal catastrophe, as well as by neurologic and metabolic problems.
Inferior myocardial infarction, pericarditis, and lower lobe pneumonia may present with upper abdominal pain. Diabetic and immune-suppressed patients, particularly those on steroids, can present with advanced intra-abdominal sepsis before peritoneal signs become obvious. Arthritic patients who are taking steroids or nonsteroidal anti-inflammatory agents and whose conditions suddenly deteriorate must be suspected of harboring an intra-abdominal problem, such as gastrointestinal bleeding or perforation, as a consequence of their medications. Severe bleeding can occur when a posterior ulcer in the first portion of the duodenum erodes into the gastroduodenal artery. Syncope at the onset of abdominal pain may signify a perforated ulcer or intra-abdominal hemorrhage such as from a ruptured aneurysm, spleen, or ectopic pregnancy. Although porphyria and sickle cell crises can mimic abdominal catastrophes, they rarely cause admission to the intensive care unit.
Physical Examination
Abdominal examination in the critically ill patient can be challenging as many patients will be unconscious or intubated. Examination of the abdomen in the critically ill patient who may be combative, comatose, narcotized, or paralyzed is difficult. The standard routine of inspection, palpation, percussion, and auscultation should be followed. Vital signs, including blood pressure (with the patient sitting if possible), pulse, respiratory rate, and rectal or core temperature, should be taken. Too often, oral or axillary temperatures are normal because of peripheral cooling, nasal oxygen administration, or nasogastric (NG) tubes.
Inspection of the abdomen can give many clues. The Gray-Turner sign, flank ecchymosis, was initially described with hemorrhagic pancreatitis but can occur with other causes of retroperitoneal bleeding. The Sister Mary Joseph nodule indicates abdominal or breast malignancy that spread along the round ligament to the umbilicus. Dilated abdominal wall veins indicated advanced portal hypertension. A large abdominal aortic aneurysm may be discerned as a pulsating upper abdominal mass in a thin patient. Absent or hypoactive bowel sounds is a nonspecific sign as many patients will have ileus associated with their critical illness. Bowel sounds are frequently absent in paralyzed patients, despite the fact that muscular paralysis should not eliminate autonomic bowel function. Hyperactive sounds or “rushes” are most common with small bowel obstruction. The presence of bowel sounds, however, does not always correlate with normal bowel function.
The presence of guarding or rigidity indicates peritoneal irritation. Rebound may not be present in a postoperative patient with significant abdominal pathology. It is important to note, however, that patients' response to the presence of blood in the peritoneal cavity is variable. Some patients will have guarding or rigidity whereas others will have a soft abdomen. Assessment of obese patients for abdominal wall rigidity is also unreliable. Obese patients may also have groin or incisional hernias that are not easily discerned. Patients with mesenteric ischemia have pain that is out of proportion to the findings of the physical exam. Rectal and pelvic examinations are frequently avoided in the ICU; however, they are mandatory to discover low pelvic abscesses and masses, prostatic infection, and bloody stools.
The physical examination of the acute abdomen should be performed by an experienced physician on a regular basis. Serial examinations are essential to carefully document any progression of tenderness, muscular rigidity, and the overall trend toward improvement or deterioration. An isolated examination is not nearly as useful as sequential examinations by the same observer. The physician who will ultimately make the decision whether surgical intervention is required should be involved as early as possible.
The presence of abdominal distention in the setting of decreased urine output and increased ventilator pressures should lead to a possible diagnosis of abdominal compartment syndrome and immediately to a measurement of intra-abdominal pressures using bladder pressure manometry.
Laboratory Evaluation
Laboratory tests should be viewed as adjuncts in the evaluation of patients. They often provide useful information but are rarely diagnostic. Depending excessively on laboratory findings is costly and occasionally misleading. A complete hemogram, including hematocrit, hemoglobin, and complete white blood cell (WBC) count, is routine. A decreasing WBC count may give a false sense of improvement, because severe sepsis can cause a leukopenia with a shift to the left that will be missed without a differential count. Urinalysis, including specific gravity and analysis for bacteria, bile, and reducing substances, should be performed. Patients with indwelling Foley catheters often have asymptomatic bacteriuria and mild hematuria. A full workup of “benign bacteriuria” may delay the diagnosis of the true cause of sepsis. The serum amylase concentration, especially fractionated into isoenzymes, is helpful in diagnosing intra-abdominal catastrophe when it is elevated but is not specific. Amylase may be increased in ischemic bowel disease, facial trauma, perforated ulcer, and pancreatitis, or without apparent cause (3). The serum lipase is a more specific marker of acute pancreatitis than amylase and is less influenced by other intra-abdominal problems. Calcium and phosphorus values are also helpful in determining the severity of pancreatitis.
An elevated serum bilirubin level is associated with sepsis, resolving hematoma, hemolysis, and hepatobiliary disease. Likewise, the lactate dehydrogenase concentration may be elevated in numerous disease processes. Liver enzymes, such as serum glutamate oxaloacetic transaminase, serum glutamic pyruvic transaminase, and alkaline phosphatase may be helpful but are rarely diagnostic by themselves.
Laboratory data are most useful in the management and correction of fluids, electrolytes, and acid-base derangements. Persistent acidosis and arterial hypoxemia suggest severe metabolic problems that may be a reflection of unresolved third-space losses from untreated abdominal sepsis or ischemia. These causes are frequently overlooked in the early workup of these problems.
Radiographic Studies
Although plain portable radiographs of the abdomen are obtained on most patients with suspicious abdominal findings, their yield is relatively low and their quality is frequently suboptimal. They are most useful to determine the position of intra-abdominal tubes such as NG and drains. Plain abdominal films are useful to examine abnormal gas patterns intraluminally and extraluminally. The absence of gas may be found with ischemic bowel, whereas small bowel obstruction and colonic volvulus present with massive gaseous distention. An upright abdominal film is desirable; however, many patients in an ICU cannot tolerate this procedure, and therefore, a left lateral decubitus film to discover air-fluid levels and free air above the liver should be obtained. Free air from perforated viscus is best seen in an upright chest radiograph, which is usually possible to obtain in the critically ill patient by sitting the patient up in bed and elevating the head of the bed 75 to 90 degrees.
A retrospective study of 1,000 patients presenting to the emergency room (ER) with acute abdominal pain compared the use of plain films to computed tomography (CT) scans. The majority, 588 of 871 (68%), of abdominal radiographs were interpreted as nonspecific, whereas 83 demonstrated specific diagnostic abnormalities, including bowel obstruction (4%), urolithiasis (2%), ileus (2%), and abnormal foreign bodies (1%) (4). No free air was found. Films were most sensitive for foreign bodies (90%) and bowel obstruction (49%). Only 38 of 188 CT scans were normal. Of these, 120 of 188 had undergone plain films. CT was predictive of bowel obstruction in 75% and pancreatitis in 60%. Of the 120 patients who had both exams, abdominal films were negative in 20%, nonspecific in 76%, and abnormal in 4%. These data could be extrapolated to ICU patients although there are no studies to confirm similar findings.
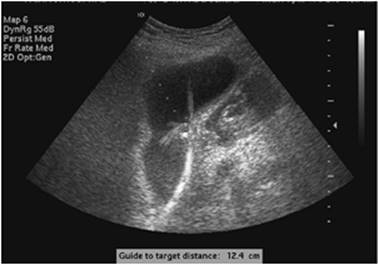
Ultrasonography has emerged as a dependable adjunctive diagnostic tool. It can be brought to the bedside and give data on acalculous cholecystitis, fluid collection, and blood flow. Ultrasound is useful in demonstrating intra-abdominal blood or fluid and to perform percutaneous abscess drainage. It is less invasive and less expensive than CAT scan and does not require transporting patients. However, in patients who have been in an ICU for extended periods, the gallbladder can be expected to be distended with poor contractility, and the ultrasound is not specific for acalculous cholecystitis unless a radionuclide study using a HIDA (hepatobiliary iminodiacetic acid) scan confirms abnormal gallbladder filling. Ultrasound is also difficult to interpret in patients with distended bowel gas. Ultrasound can also be used as a therapeutic tool to help perform procedures such as percutaneous cholecystostomy (Fig. 76.1).
The CT scan has become the most widely used tool to examine the abdomen for abnormalities, and CT scanning is more accurate for diagnosing intra-abdominal fluid collections than any other modality. It is especially useful in liver, splenic, renal, and retroperitoneal abscesses but may not be as useful as ultrasound in the diagnosis of right upper quadrant and pelvic masses.
|
|
|
Figure 76.1. Ultrasound-guided percutaneous cholecystectomy. |
Optimal use of CT scan requires oral contrast, which may be difficult for the critically ill patient to ingest and retain and may be an aspiration risk. It also requires transporting the patient to the scanner accompanied by the nurse, therapist, and physician, and the possibility exists of an untoward event during transport.
Despite the significant increase in accuracy and decrease in time of the actual scan, recent studies by Hendershot et al. (5) demonstrated that the time for a scan was significantly longer than imagined, because of the efforts to get patients ready, transport patients, transfer them to the table, and then repackage them and return them to the ICU.
The enthusiasm for CT scanning must also be tempered by an evaluation of the efficacy of scans in critically ill patients. In a study by Norwood and Civetta (6), scans were found to be helpful in only 23% of patients, most of whom had been examined because of postoperative sepsis. This study has not been repeated, and therefore it is difficult to determine the efficacy of the CT scan in ICU patients. The CT scan not only has become part of the diagnostic armamentarium, it can be increasingly useful as a therapeutic modality. CT drainage of abscesses, aspiration of pancreatic collections, CT-guided nephrostomy tube insertions, and aspiration of ascites are now easily performed.
A Gastrografin swallow is still an excellent tool to differentiate a gastric leak following gastric bypass surgery or persistent leak from a perforated ulcer.
Diagnostic peritoneal lavage (DPL) has long been a tool to help differentiate abdominal collections from intra-abdominal blood (7). Ultrasonography has largely obviated the need to perform bedside DPL, but the technique is still useful to drain tense ascites and determine the source and infectious nature of the fluid.
Therapy
The treatment of intra-abdominal problems in the acutely ill frequently requires surgical intervention. Surgical consultation should be obtained early in the evaluation. In the preoperative patient, adequate volume resuscitation and electrolyte correction are vital to prepare the patient for surgical repair of the underlying problem. Most fluid losses in preoperative surgical patients are isotonic. Patients who are volume contracted may be hyponatremic, hypochloremic, hypokalemic, and alkalotic because of vomiting, nasogastric suctioning, and third-space losses. These patients require normal saline resuscitation to prevent anesthetic disaster. Only after volume and salt repletion will their chloride-dependent alkalosis resolve. Although hypokalemia may exist, potassium should be administered cautiously until oliguria is resolved.
Acute abdominal catastrophe may be the first event in the precipitous cascade of multiple organ system failure (MOSF). Unrecognized abdominal sepsis is associated with MOSF in 44% of cases (8,9). Early aggressive surgical therapy, vigorous fluid replacement, and appropriate antibiotic regimens are necessary.
The specific management of disease entities should be based on well-established surgical principles. However, the explosion of minimally invasive surgery has lead to a new era in surgical intervention. Many acute abdominal procedures can now be performed either via an open or laparoscopic technique. Most acute cholecystitis can be treated conservatively for 24 to 48 hours. If the signs and symptoms do not improve within 48 hours or if cholangitis appears, an endoscopic retrograde cholangiopancreatography (ERCP) can be performed to drain the common duct. A percutaneous cholecystostomy or a laparoscopic cholecystectomy can then be performed in most cases. Perforated ulcers can now be treated laparoscopically in some surgeons' hands. A true “sea change” in the treatment of ruptured abdominal aneurysm has taken place with the improvements in endovascular aortic repair (EVAR) (10). A significant number of patients can now be treated under local anesthesia with bilateral groin cutdown, avoiding the significant morbidity of open procedures. Although it is too early to determine how much the minimally invasive procedure can affect early and late mortality, initial studies imply that the overall mortality for EVAR, as well as ICU stay and morbidity, may be lower than that of open procedures (11).
Stress ulceration without perforation may be prophylactically treated with antacids, H2 blockers, and sucralfate, although aggressive pH control may lead to an increase in nosocomial pneumonia (12,13,14). Stress ulcer bleeding is rare, but the best treatment is prevention. If bleeding cannot be contained with conservative measures, an operative intervention should be undertaken, which carries with it a high mortality rate of 50% (15,16). Do not wait until multiple transfusions have created dilutional or hypothermic coagulopathies, because mortality rates will approach 100%.
The use of CT scan and ultrasonic-guided drainage and catheter decompression of intra-abdominal abscesses had revolutionized care in some postoperative patients. This procedure results in excellent control of the septic source with a low morbidity (17). It is often preferable to secondary exploratory laparotomy. However, if a patient persists in a downward clinical course, exploration with wide drainage of abscesses may be necessary. In patients with diffuse persistent peritonitis or necrotizing pancreatitis, conversion to an open abdomen with zipper technique may be needed to control the infection (18).
Antibiotics are not panacea for intra-abdominal sepsis, and abscesses will form despite adequate coverage. The use of antibiotics in acute abdominal problems is usually adjunctive to prevent systemic sepsis. The prolonged use of antibiotics for localized abscesses instead of surgical or radiologic drainage can lead to morbidity and increased mortality.
In patients with diffuse peritonitis or necrotizing infected pancreatitis, conversion from a closed abdomen into an open abdomen may be necessary to control the process (19).
Specific Disease States
Any stable patient in an ICU developing sudden shock or sepsis must be examined closely for an intra-abdominal cause. Several conditions that are common causes of abdominal symptoms in critically ill patients are presented in the following sections.
Although appendicitis is the most common abdominal condition requiring surgery, it is rarely seen in the ICU. Pancreatitis and acalculous cholecystitis are more common, especially after open heart surgery. Abdominal distention in elderly patients after orthopedic procedures is frequently caused by ileus and colonic pseudo-obstruction. Patients receiving mechanical ventilation are at high risk for gastrointestinal bleeding, ileus, and unrecognized perforation (2). Stress ulcer perforation and ileus are insidious causes of respiratory failure and sepsis in any patient with a spinal injury (20).
Acquired Immunodeficiency Syndrome (AIDS)
Immunocompromised hosts require special attention when presenting either with abdominal pain or sepsis of unknown origin. Since the advent of antiretroviral medication therapy, the incidence of severe abdominal problems in HIV-positive patients has decreased. Patients presenting with overt AIDS have a constellation of problems that are unique to this population. The frequency of pulmonary, cardiac, gastrointestinal, and renal disease that is not directly related to the underlying HIV has increased (21).
Acute abdominal pain is a complaint in 12% to 45% of patients with HIV infection presenting to the emergency room (22). Earlier studies have noted that cytomegalovirus (CMV), gastroenteritis, followed by lymphoma, Kaposi sarcoma, and mycobacterial disease were frequent causes of abdominal pain in HIV patients. There has been a significant reduction in these opportunistic infections, especially peritonitis secondary to atypical mycobacterium and fungi (23,24).
The clinician must be aware that the HIV patient continues to present with non–HIV-related problems, such as appendicitis, diverticulitis, and pancreatitis. Only 11% of acute abdominal pain in HIV patients is caused by HIV/AIDS, whereas opportunistic infection results in surgery in only 0.9% of patients (25). Surgery should be considered early because of the difficulty in interpreting findings in these patients and the importance of differentiating true surgical from nonsurgical abdominal problems. Earlier studies reported increased morbidity and mortality in patients with AIDS (26), whereas recent data yield 10% to 19% operative mortality for emergency surgery (24).
Fever and nonspecific abdominal pain are frequently noted although peritoneal signs may be lacking in severely immunocompromised patients (27). Prognosis of patients is somewhat dependent on the CD4 count and viral loads. CD4 counts less than 200 cells/mm3, total lymphocyte count less than 1,000 cells/mm3, and viral loads greater than 75,000 RNA copies/mL are associated with higher morbidity and mortality (24).
Plain films have a low yield compared to CT scan in the diagnoses of processes such as pneumatosis intestinalis. This finding on CT is very suggestive of bowel necrosis. Intraperitoneal collections associated with opportunistic infections can be aspirated under CT guidance (4,28).
Acute appendicitis in AIDS patients may be routine or secondary to opportunistic organisms. Although fever and pain are frequent, white blood cell count may be low or normal (29).
There has been a decrease in bowel perforation secondary to CMV or Kaposi sarcoma since the advent of retroviral therapy. However, diligence is required to ensure perforation has not occurred. Recent data point to lymphoma and disseminated mycobacterial disease as causes for perforation (25). CMV perforations are more common in the ileum and colon secondary to ischemic lesions, which require aggressive surgical therapy and diversion of the fecal stream (23). Acute bowel obstruction suggests disseminated disease and has a poor prognosis if the cause is age related.
Colonic disease, especially toxic megacolon, has been seen with Clostridium difficile colitis, especially in patients with CMV infection. Megacolon can be a significant prognostic indicator in advanced age and may best be treated with colonoscopy for short-term management of the severely ill (30).
Acute hepatobiliary disease secondary to opportunistic disease can present difficult diagnostic problems in patients with CD4 counts less than 100 cells/mm3. Acalculous cholecystitis is more common in HIV/AIDS patients than in the normal population (31,32,33).
Neutropenic patients with cancer also present a diagnosis and therapeutic challenge. In patients who underwent emergency celiotomy for suspected intra-abdominal disease, the most common disease has been reported to be neutropenic enteropathy (61%) with postoperative mortality up to 32% (34).
Biliary Disease
Primary biliary tract disease in critically ill patients appears as calculous or acalculous cholecystitis. Calculous disease may present as acute cholecystitis, cholangitis, or pancreatitis. Acute acalculous biliary disease is a concomitant of critical illness and has been reported in 1% of surgical patients and 0.2% of postoperative cardiac patients (35).
The differentiation of calculous from acalculous disease can be difficult. Several risk factors are associated with the development of acalculous cholecystitis, including use of narcotics for more than 6 days, gastric suction, prolonged ileus with nothing by mouth, ventilatory support longer than 24 hours, multiple recent operations, more than ten blood transfusions, open wound or abscesses, and intravenous hyperalimentation for more than 3 days. The presence of five of these risk factors in a patient with acute abdominal findings should lead to a search for acalculous biliary disease (35,36).
The typical presentation of right upper quadrant pain, a positive Murphy sign, and fever may be absent in critically ill patients. Symptoms of right upper quadrant pain were present in only 30% of patients with acalculous disease, although all exhibited fever. Peritonitis was an inconsistent finding and present in only 24%. Persistent fever was the most consistent finding (37).
The laboratory findings of biliary disease are variable. Leukocytosis is common, although nonspecific. Up to 65% of patients with acalculous cholecystitis have elevated bilirubin; however, a control group of patients receiving multiple transfusions had similar hyperbilirubinemia. Liver enzymes are elevated in less than 50% (35).
Acute cholecystitis can mimic numerous other disease processes in the abdomen. Conversely, the presence of stones in the gallbladder in patients with nonspecific symptoms is not pathognomonic of acute biliary disease. Improved ultrasonography can be supplemented by radionucleotide imaging techniques that can distinguish cystic duct obstruction in acute cholecystitis from other causes of abdominal pain have markedly increased our diagnostic acumen. Derivatives of iminodiacetic acid are rapidly taken up by the hepatocytes and excreted into the bile even in patients with elevations of bilirubin up to 6 g/dL. The test has proved to be 95% accurate in the diagnosis of acute cholecystitis. The presence of fever, mild elevation of bilirubin, sludge on ultrasound, and nonvisualization on HIIDA are accurate indications of acute acalculous cholecystitis in critically ill patients. Caution is urged in patients receiving hyperalimentation, which severely limits the usefulness of the test (38,39). Furthermore, HIDA scan requires moving the critically ill patient to the radiology suite for up to 4 hours, and the risk–benefit ratio requires a high degree of clinical suspicion. The treatment of choice has been surgical drainage, either cholecystostomy or cholecystectomy, if the patient is able to tolerate a major procedure. The use of percutaneous cholecystostomy has been reported in severely ill patients. The mortality rate associated with acalculous cholecystitis is as high as 40% secondary to the multiplicity of the patient's problems (37,40).
Abscess
Intra-abdominal abscesses develop as a complication of secondary peritonitis that is the result of a perforation of a hollow viscus. They usually occur postoperatively, particularly after colonic resection complicated by anastomotic leak (41). This is followed in frequency by diverticular disease, appendicitis, inflammatory bowel disease, and malignancy. Patients undergoing gastric bypass procedures for obesity are also a potential population to develop abscess accompanied by an anastomotic leak. Abscesses can also develop retroperitoneally. This can be the result of retroperitoneal visceral perforation, e.g., cecal perforation or lymphatic and hematogenous spread of bacteria, e.g., infected pancreatic necrosis. Peritonitis and abscess should be suspected in any patient deteriorating following abdominal surgery.
Making the diagnosis of intra-abdominal abscess requires a high index of suspicion as the clinical picture can be vague. Peritonitis is rare, and bowel function may be normal. Physical examination is rarely helpful. Abscesses that have the anterior abdominal wall as part of their walls are associated with a palpable tender mass. Nonspecific manifestations such as fever, chills, malaise, and leukocytosis should raise the suspicion. Hiccup, unexplained pleural effusion, and a raised hemidiaphragm on chest radiograph may indicate subphrenic abscess. Diarrhea and urinary retention may indicate a pelvic abscess. CT scanning, preferably with oral and intravenous contrast, is the standard diagnostic modality. Bedside ultrasonography may be used in patients who are too unstable to move out of the ICU.
The bacterial flora are related to the organ involved, the host defenses, and the duration of the critical illness. The flora of the normal stomach and duodenum is very sparse and is composed mainly of swallowed oral organisms such as microaerophilic streptococci and Streptococcus viridans, lactobacillus, fusiform bacteria, and Candida species. The flora grows and changes remarkably if there is gastric outlet obstruction, achlorhydria, or acid-suppressive therapy. Small bowel flora consists mainly of Enterobacteriaceae, Enterococcus species, and anaerobic species. The flora becomes gradually more dense distally. Colonic flora is extremely dense; it accounts for one sixth of the dry weight of stools and contains both aerobic and anaerobic bacteria with the former much more abundant than the latter. Aerobic bacteria are primarily Gram-negative, e.g., Escherichia coli, Klebsiella species, Enterococcus species, and Proteus species. Anaerobic bacteria include Bacteroides fragilis, Eubacterium species, and Bifidobacterium species. Intra-abdominal abscesses are typically polymicrobial, but anaerobes are difficult to grow on cultures.
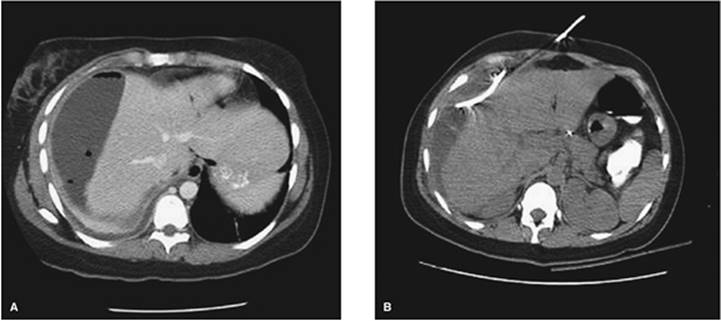
Whenever possible the source of infection should be dealt with surgically, e.g., appendectomy or resection of necrotic or perforated intestine. Open surgical management is not always possible or necessary. Surgical consultation should be obtained, and the decision to operate is based on individual patient conditions. Open surgical drainage does not always entail a celiotomy. Drainage of subphrenic abscess can be performed through the bed of the 12th rib, and extra peritoneal drainage of lower quadrant abscesses may be done. The efficacy of CT-guided percutaneous drainage of intra-abdominal abscesses (Fig. 76.2) has long been established (17,42,43). This minimally invasive technique is quite helpful, particularly when operative intervention carries a high risk of morbidity as in the case of Crohn disease (44). In a retrospective study of 38 patients with intra-abdominal abscesses due to colorectal disease both postoperative and primary, the overall success rate of percutaneous drainage was 89% (45). Antibiotic therapy is based on empiric coverage of bacteria that is normally present within the gut rather than culture results. Antibiotics are adjunctive in treating intra-abdominal sepsis. The antibiotic regimen should cover Gram-positive, Gram-negative, and anaerobic bacteria. Antifungal agents are not given even if fungi are seen on cultures unless the patient is immunosuppressed or has recurrent intra-abdominal infection. Guidelines for the use of antimicrobial agents are published by several medical societies (46).
Mortality from intra-abdominal sepsis ranges from 7.5% for single abscess to 43% for patients with multiple abscesses and peritonitis (47). Overall mortality from intra-abdominal infection is 24%. Mortality correlates directly with acute physiology score, malnutrition, age, and shock. Only early recognition, appropriate use of antibiotics, and prompt drainage can improve on these data.
Pneumoperitoneum
The most common cause of pneumoperitoneum is laparotomy or laparoscopy. After abdominal surgery, free air may persist for weeks, although air from laparoscopy is frequently absent at 48 hours.
|
|
|
Figure 76.2. Right subphrenic abscess is drained percutaneously under computed tomography guidance. |
Pneumoperitoneum in a patient who does not have a recent history of laparotomy or laparoscopy should be presumed to be due to a perforated viscus until proven otherwise. Perforation of the stomach or duodenum due to peptic ulcer disease is more likely to cause an obvious pneumoperitoneum than perforation of the colon due to diverticular disease. Other conditions that may cause pneumoperitoneum are a recent percutaneous endoscopic gastrostomy and barotrauma to the lung (48,49). The latter, however, occurs much less frequently with today's lung-protective strategies whereby peak airway pressures are not allowed to exceed 40 cm H2O. Patients who suffer severe chest trauma with pneumothorax and pneumomediastinum can also have pneumoperitoneum.
Pneumoperitoneum has been observed in up to 10% of patients who have demonstrated other evidence of extra alveolar air. Macklin and Macklin (49) postulated that air first ruptures though distended alveoli and dissects toward the mediastinum. From there, it dissects down the mediastinum and ruptures into the peritoneal cavity. The diagnosis of perforated viscus may be difficult in paralyzed, mechanically ventilated patients who cannot complain of tenderness and who will have a soft abdomen and absent bowel sounds.
Pneumoperitoneum should be evaluated in the context of the patient's overall condition. In unconscious or paralyzed septic patients with no obvious source of sepsis, pneumoperitoneum should prompt an exploratory laparotomy. Diagnostic peritoneal lavage may be considered if the risk of operative exploration is too high or the index of suspicion is low. The presence of bacteria, bile, more than 500 WBCs/mm3 can be inferred to indicate an acute abdominal process requiring immediate laparotomy.
Pseudo-Obstruction Of The Colon
Isolated colonic ileus without mechanical obstruction was first described by Ogilvie (50). Patients at risk are the elderly and those requiring bed rest, prolonged narcotic use, and mechanical ventilation. Massive colonic distention presents a perplexing dilemma in the ICU. The cause is unknown, but the condition typically occurs in patients with associated illness who are bedridden for a long time. The most common risk factors are old age, multiple trauma, abdominal and pelvic operations, orthopedic operations, and spinal cord injuries (50,51). Hyponatremia and hypokalemia may play a role in the development of this condition. The abdomen is distended and tympanitic without signs of peritonitis, fever, or leukocytosis.
On radiograph the colon appears diffusely distended, including the rectum, and the small bowel is usually not seen. The cecum, being the widest segment of the colon, is at risk for necrosis and perforation if the diameter reaches 12 cm. Mechanical obstruction should be ruled out with a Hypaque enema. This is a hyperosmolar water-soluble enema that helps to cleanse the colon and, unlike barium, does not interfere with a subsequent colonoscopy.
Initial management consists of decompressing the stomach and colon with nasogastric and rectal tubes. Electrolyte abnormalities, especially hypokalemia, should be promptly corrected. If there is no response to these measures, neostigmine, a parasympathomimetic, should be given to stimulate colonic motility (52). Neostigmine is given in a dose of 1 to 2 mg intravenously and can be repeated in 3 hours. This should be done under cardiac monitoring as it may result in severe bradycardia. Neostigmine should not be given if the patient's baseline heart rate is less than 60 beats per minute, the systolic blood pressure is less than 90 mm Hg, or if there is a significant heart block or bronchospasm. The next step in management, if the previous measures fail, is colonoscopic decompression. This is associated with a higher-than-normal risk of perforation and therefore should be used gently and with the goal of decompression only. It is not necessary to advance the colonoscope all the way to the cecum. Recurrence is seen in up to 40% of patients, and colonoscopy can be repeated. Surgery is reserved for patients who fail all other measures and those with complications or impending cecal rupture, i.e., diameter more than 12 cm. The operation of choice is right hemicolectomy with primary ileocolic anastomosis if there is no evidence of necrosis or perforation, in which case an ileostomy with mucus fistula should be performed.
Management of the Open Abdomen in the Icu
The abdominal compartment syndrome (ACS) is a condition in which the intra-abdominal pressure rises to a point that impairs respiratory, renal, and cardiovascular function (53). The condition is described mainly in the trauma population but can occur in any patient who receives a massive resuscitation for a profound shock state. The abdomen is not necessarily the site where the original pathology occurs, e.g., severe burns (54). This is sometimes described as secondary ACS. It is believed that severe edema of the abdominal wall, bowel wall, and the retroperitoneum occurs as a result of massive fluid shifts associated with the severe systemic inflammation that accompanies reperfusion of tissues after shock states. The diagnosis of ACS is made when there is abdominal distention associated with high ventilator pressures, oliguria, and elevated urinary bladder pressures (>25–30 cm H2O). Treatment consists of abdominal decompression using a midline celiotomy and keeping the abdomen open using various dressing mechanisms over the bowel. For a detailed discussion of the ACS, see the section on abdominal trauma.
The treatment principles in trauma patients have been extrapolated to general surgery patients. More abdomens are now kept open if fascial closure is expected to increase abdominal pressure. By keeping the abdomen open, renal and pulmonary functions are not compromised and the integrity of fascial edges is preserved. The open abdomen also gives the opportunity for frequent bedside washouts and debridements such as with infected pancreatic necrosis. Once the swelling has resolved, the abdomen should be closed as soon as possible either by primary fascial closure or using one of the commercially available biologic or synthetic grafts. Prolongation of the open abdomen management is associated with increased risk of fistula formation.
Bariatric Surgery
It is estimated that over 130,000 bariatric procedures will be performed in the United States each year (55). Many of these patients have sleep apnea, hypoventilation, or other physiologic abnormalities that require ICU care in the immediate postoperative period. Since anastomotic leaks following gastric bypass and duodenal switch are potentially fatal, rapid recognition, diagnosis, and treatment are necessary to minimize patient risk. Likewise, acute gastric dilatation requires immediate treatment. The hallmarks of dilatation and leak are persistent tachycardia, tachypnea, fever, anxiety, and hiccups, usually accompanied by a mild leukocytosis with or without fever (56). Because this is also found in patients with pulmonary emboli, it is vital that the diagnosis of leak be made early.
Abdominal pain is frequently not a major symptom, although shoulder (referred) pain may be present. In the absence of hypoxemia in the first 48 hours, the above symptoms should suggest leak and immediate Gastrografin swallow with adequate volume of contrast should be performed. The presence of a large gastric bubble without leak requires immediate decompression via either a percutaneous or surgical therapy (56). This will prevent gastric perforation or an anastomotic disruption from pressure. A leak must be addressed immediately with drainage either percutaneously for small and contained leaks, or operative intervention to attempt to repair and drain the area of concern.
Acute Mesenteric Ischemia
Numerous causes exist for acute intestinal ischemia. Embolus (50%–60%) or thrombus (25%–35%) of the superior mesenteric artery (SMA) must be differentiated from nonmesenteric thrombosis (10%–20%) and acute mesenteric venous occlusions (5%) (57,58,59,60). Colonic and rectal ischemias have been reported after abdominal aortic aneurysmectomy in which the inferior mesenteric artery was ligated (61).
A characteristic of gut ischemia is the disparity between the patient's pain and abdominal findings. Pain is found in 75% to 90% of patients. Nausea and vomiting are present in 50% to 60% of patients, whereas upper gastrointestinal bleeding is less common (62,63). Abdominal distention is present in 56% to 80%, peritoneal signs in 60%, ileus in 50%, and shock and fever in 30% of patients. Leukocytosis (WBC count of 20,000/mm3) is seen in less than 50% of patients. A mild elevation in amylase is common (59,64).
The presence of physical signs indicating peritoneal irritation is extremely important because they portend impending or progressive gangrene and are associated with significant mortality. Leukocytosis out of proportion to the physical findings, elevated hematocrit, unexplained acidosis, and blood-tinged fluid on peritoneal lavage are all signs of advancing intestinal necrosis (62).
Plain radiographs are useful to exclude the other processes that can stimulate the symptoms. Signs of intestinal ischemia on plain radiographs is a grave prognosticator with 90% mortality (62).
Patients at highest risk are those older than 50 years of age with either valvular or atherosclerotic heart disease, congestive heart failure (especially if there is poor control with digitalis and diuretics), hypovolemia, hypotension of any cause, recent myocardial infarction or cardiogenic shock, or cardiac arrhythmias (58,59,62). Dialysis patients seem to be at added risk for right colon ischemia. The use of sigmoid tonometry also has been suggested to detect colonic ischemia (65).
|
|
|
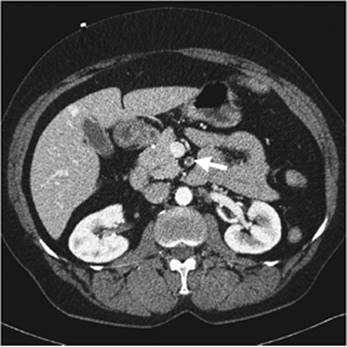
Figure 76.3. Superior mesenteric artery embolus (white arrow). |
|
|
|
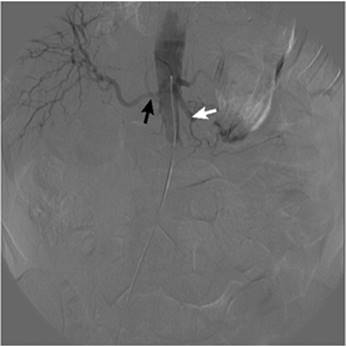
Figure 76.4. Superior mesenteric artery angiogram showing an embolus distal to the proximal jejunal branches (white arrow) and a replaced right hepatic artery (black arrow). |
Once the diagnosis is suspected, vigorous fluid resuscitation is necessary to maintain adequate blood flow and pressure head in the mesenteric vessels. Gastrointestinal decompression with a NG tube and proper hemodynamic monitoring are necessary to adequately resuscitate these precarious patients. Early heparinization should be used if immediate surgery is not undertaken.
CAT scans have improved in both availability and reliability and may demonstrate clot or ischemia (Fig. 76.3). Emergency selective arteriography is still the keystone of the diagnostic and therapeutic approach to acute mesenteric ischemia (Fig. 76.4). Arteriography can differentiate occlusive from nonocclusive disease. Although there are reports of successful thrombolysis of clot in the SMA (66), acute occlusion is best treated by immediate surgical restoration of circulation by embolectomy or aortosuperior mesenteric artery bypass. Examination of the bowel for ischemia, which will require resection, is essential to avoid unnecessary morbidity and mortality.
Nonocclusive mesenteric ischemia is diagnosed when mesenteric vasoconstriction on angiogram is seen in the patient with a clinical picture suggestive of intestinal ischemia. Shock and vasopressors make interpretation of the arteriogram difficult. Treatment of this disease is begun in the radiology suite by the administration of papaverine (30–60 mg/hour) through a catheter placed selectively in the SMA. If peritoneal signs are present and abdominal exploration is necessary to examine the viability of the bowel, vasodilators and local anesthetics can be injected directly into the base of the mesentery.
When papaverine is the primary treatment for nonocclusive ischemia, it is continued for 24 hours and an arteriogram is repeated. Heparin may be used concomitantly.
Maintaining adequate plasma volume and blood pressure is essential to maintain perfusion of the splanchnic vessels. Occasionally, dextran has been used to expand plasma and to decrease sludging. Digitalis should be used cautiously.
Systemic antibiotics are indicated because of the high incidence of positive blood cultures resulting from compromised bowel. Antibiotics may mask peritoneal signs. Decompression by NG suction can decrease bowel distention.
The mortality rate for acute mesenteric ischemia has remained at 70% to 80% (59,63). Embolus in the SMA is still associated with a 44% to 90% mortality rate whereas nonocclusive ischemia without peritoneal signs has a more favorable outcome. Peritonitis is associated with mortality rates of 60% to 90% (59,62). Logistic regression yields an odds ratio of 22 for peritonitis and 14.9 for hypotension as independent predictors of mortality (59).
The early workup of a suspicion of ischemia followed by aggressive and rapid diagnostic workup seems to be the only method for improving this abysmal mortality rate (63). Death occurs from MSOF secondary to ischemia (65%), sepsis (25%), pulmonary failure (8%), and stroke (2%) (59). Although second-look operations are frequently used at 24 to 48 hours to determine viability of remaining bowel, survival is not necessarily improved by this technique (67).
Summary
Acute abdominal problems are frequent among ICU patients. The physician must maintain a high level of suspicion that an abdominal problem is present when faced with a deteriorating critically ill patient. History and physical examination must be used to guide the use of more invasive and expensive tests. Laboratory tests are usually adjunctive and rarely diagnostic. Radiographic procedures, especially ultrasound and CT scans, when appropriately used, can be helpful. Surgical consultation should be obtained early in a patient's course, because treatment frequently requires surgical intervention. Only by maintaining constant vigilance can critical care practitioners guide their patients through the multiple perturbations created by acute abdominal problems.
Pearls
· Patients admitted to an ICU with abdominal pain, fever, evidence of multiorgan failure, unexplained acidosis, or jaundice should have an acute abdominal source ruled out early in their course.
· The absence of obvious signs and symptoms in an acutely ill patient does not rule out an acute abdominal problem.
· Resuscitation of acute abdominal problems frequently requires large volumes of isotonic crystalloid fluids and broad-spectrum antibiotics.
· Common postoperative abdominal problems include abscess, leak from anastomoses or perforated bowel, acalculous cholecystitis, and ileus.
· Acute abdominal pain in an immunocompromised patient requires a high index of suspicion and rapid diagnosis of uncommon infectious causes.
· The diagnostic approach to acute abdominal symptoms includes radiologic examinations—ultrasound or CT scan (with oral contrast when indicated) early in the workup.
· Abdominal distension associated with low urine output and high ventilatory pressures should prompt measurement of abdominal compartment pressures and surgical consult.
· Acute mesenteric embolus is the most common cause for intestinal ischemia (50%–60%). It may present as severe pain out of proportion to the physical signs and requires immediate diagnosis and surgical treatment to prevent significant morbidity/mortality.
References
1. Aranha GV, Goldberg NB. Surgical problems in patients on ventilators. Crit Care Med. 1981;9:478.
2. Brewer RJ, Golden GT, Hitch DD, et al. Abdominal pain: an analysis of 1,000 consecutive cases in a university hospital emergency room. Am J Surg. 1976;131:219.
3. Weaver DW, Busuito MJ, Bouwman DL, et al. Interpretation of serum amylase levels in the critically ill patient. Crit Care Med. 1985;13:532.
4. Ahn SH, Mayo-Smith WW, Murphy BL, et al. Acute nontraumatic abdominal pain in adult patients: abdominal radiography compared with CT evaluation. Radiology. 2002;225:159.
5. Hendershot KM, Fakhry SM, Haikman H, et al. Duration and safety of computed tomography in severely injured blunt trauma patients. Paper presented at: 56th Annual Meeting of the Association for the Surgery of Trauma; September 28–30, 2006; New Orleans, LA.
6. Norwood SH, Civetta JM. Abdominal CT scanning in critically ill surgical patients. Ann Surg. 1985;202:166.
7. Larson FA, Haller C, Delcore R, et al. Diagnostic peritoneal lavage in acute peritonitis. Am Surg. 1992;164:449.
8. Fry DE, Pearlstein L, Fulton RL, et al. Multiple system organ failure: the role of uncontrolled infection. Arch Surg. 1980;115:136.
9. Knaus WA, Draper EA, Wagner DP, et al. Prognosis in acute organ-system failure. Ann Surg. 1985;202:685.
10. Lifeline Registry of EVAR Committee. Lifeline registry of endovascular aneurysm repair: long-term primary outcome measures. J Vasc Surg. 2005;42:1.
11. EVAR Trial Participants. Endovascular aneurysm repair versus repair in patients with abdominal aortic aneurysm (EVAR trial 1): randomized controlled trial. Lancet. 2005;365:2179.
12. Hastings PR, Skillman JJ, Bushnell LS, et al. Antacid titration in the prevention of acute gastrointestinal bleeding: a controlled, randomized trail in 100 critically ill patients. N Engl J Med. 1978;298:1041.
13. Shuman RN, Schoster DP, Zuckerman GR. Prophylactic therapy for stress ulcer feeding: a reappraisal. Ann Intern Med. 1987;106:562.
14. Tryba M. Risk of acute stress bleeding and nosocomial pneumonia in ventilated intensive care unit patients: sucralfate vs. antacids. Am J Med. 1987;83:117.
15. Cook DJ, Fullder HD, Guyatt, et al. Risk factors for gastrointestinal bleeding in critically ill patients. N Engl J Med. 1994;330:377.
16. Hubert JP, Kiernan PD, Weld JS, et al. The surgical management of bleeding stress ulcers. Ann Surg. 1980;191:672.
17. Levison MA. Percutaneous versus open operative drainage of intra-abdominal abscesses. Infect Dis Clin North Am. 1992;6:25.
18. Mismatsu K, Oida T, Kanou H, et al. Open abdomen management after massive bowel resection for superior mesenteric arterial occlusion. Surg Today. 2006;36:241.
19. Ashley SW, Perez A, Pierce EA, et al. Necrotizing pancreatitis: contemporary analysis of 99 consecutive cases. Ann Surg. 2001;234:572.
20. Reines HD, Harris RC. Pulmonary complications of acute spinal cord injuries. Neurosurgery. 1987;21:193.
21. Huang l, Quartin A, Jones D, et al. Intensive care of patient with HIV Infection. N Engl J Med. 2006;355:173.
22. Barone JE, Gingold BS, Arvanitis ML, et al. Abdominal pain in patients with acquired immune deficiency syndrome. Ann Surg. 1986;204:619.
23. Saltzman DJ, Williams RA, Gelfand DV, et al. The surgeon and AIDS. Arch Surg. 2005;140: 961.
24. Tran HS, Moncure M, Tarnoff M, et al. Predictors of operative outcome in patients with human immunodeficiency virus infection and acquired immunodeficiency syndrome. Am J Surg. 2000;180:228.
25. Yoshida D, Caruso JM. Abdominal pain in the HIV infected patient. J Emerg Med. 2002;23:111.
26. Davidson T, Allen-Mersh TG, Miles AJ, et al. Emergency laparotomy in patients with AIDS. Br J Surg. 1991;78:924.
27. Lowy AM, Barie PS. Laparotomy in patients infected with human immunodeficiency virus: indications and outcome. Br J Surg. 1994;81:942.
28. Wiesner W, Mortele KJ, Glickman JN, et al. Pneumatosis intestinalis and portomesenteric venous gas in intestinal ischemia: correlation of CT findings with severity of ischemia and clinical outcome. AJR Am J Roentgenol. 2001;177:1319.
29. Binderow SR, Shaked AA. Acute appendicitis in patients with AIDS/HIV infection. Am J Surg. 1991;162:9.
30. Beaugerie L, Ngo Y, Goujard F, et al. Etiology and management of toxic megacolon in patients with human immunodeficiency virus infection. Gastroenterology. 1994;107:858.
31. French AL, Beaudet LM, Benator DA, et al. Cholecystectomy in patients with AIDS: clinicopathologic correlations in 107 cases. Clin Infect Dis. 1995;21:852.
32. Flum DR, Wallack MK. Cholecystectomy and AIDS. J Am Coll Surg. 1997:184:669.
33. LaRaja RD, Rothenberg RE, Odom JW, et al. The incidence of intra-abdominal surgery in acquired immunodeficiency syndrome: a statistical review of 904 patients. Surgery. 1989;105:175.
34. Glenn J, Funkhouser WK, Schneider PS. Acute illnesses necessitating urgent abdominal surgery of neutropenic cancer patients: description of 14 cases and review of the literature. Surgery. 1989;105:778.
35. Savino JA, Scalea TM, Del Guercio LRM: Factors encouraging laparotomy in acalculous cholecystitis. Crit Care Med. 1985;13:377.
36. Petersen SR, Sheldon GF. Acute acalculous cholecystitis: a complications of hyperalimentation. Am J Surg. 1979;138:814.
37. Long TN, Heimbach DM, Carrico CJ. Acalculous cholecystitis in critically ill patients. Am J Surg. 1978;136:31.
38. Shuman WP, Gibbs P, Rudd TG, et al. PIPIDA scintigraphy for cholecystitis: false positives in alcoholism and total parenteral nutrition. Am J Radiol. 1982;138:1.
39. Kalff V, Froelich JW, Lloyd R, et al. Predictive value of an abdominal hepatobiliary scan in patients with severe intercurrent illness. Radiology. 1983;146:191.
40. Longmaid HE, Bassett JG, Gottlieb H. Management of gallbladder perforation by percutaneous cholecystostomy. Crit Care Med. 1985;13:686.
41. Deveney CW, Lurie K, Deveny KE. Improved treatment of intra-abdominal abscess. Arch Surg. 1988;123:1126.
42. Wright HK, Dunn E, MacArthur JD, et al. Specific but limited role of new imaging techniques in decision-making intra-abdominal abscesses. Am J Surg. 1982;143:456.
43. Montgomery RS, Wilson SE. Intra-abdominal abscesses: image-guided diagnosis and therapy. Clin Infect Dis. 1996;23:8.
44. Sahai A, Belair M, Fianfelice D, et al. Percutaneous drainage of intra-abdominal abscesses in Crohn's disease: short and long term outcome. Am J Gastroenterol. 1997;92:75.
45. Eng M, Hyman N, Osler T. The role of computed tomography-guided percutaneous drainage of intraabdominal abscesses in colon and rectal disease. J Pelvic Surg. 2002;8(3):163.
46. Solomkin JS, Mazuski JE, Baron EJ, et al. Guidelines for the selection of anti-infective agents for complicated intra-abdominal infections. Clin Infect Dis. 2003;37:99.
47. Dellinger EP, Wertz MJ, Meakins JL, et al. Surgical infection stratification system for intra-abdominal infection: multicenter trial. Arch Surg. 1985:120:21.
48. Hillman KM. Pneumoperitoneum: a review. Crit Care Med. 1982;10:476.
49. Macklin MT, Macklin CC. Malignant interstitial emphysema of the lungs and mediastinum as an important occult complication in many respiratory diseases and other conditions: an interpretation of the clinical literature in the light of laboratory experiment. Medicine. 1944;23:281.
50. Ogilvie H. Large intestine colic due to sympathetic deprivation: a new clinical syndrome. Br J Med. 1948;2:671.
51. Jetmore AB, Timmcke AE, Gathright JB, et al. Ogilvie's syndrome: colonoscopic decompression and analysis of predisposing factors. Dis Colon Rectum. 1992;35:1135.
52. Ponec RJ, Saunders MD, Kimmey MB. Neostigmine for the treatment of acute colonic pseudo-obstruction. N Engl J Med. 1999;341:137.
53. Burch JM, Moore EE, Moore FA, et al. The abdominal compartment syndrome. Surg Clin North Am. 1996;76:88.
54. Ivy ME, Atweh NA, Palmer J, et al. Intra-abdominal hypertension and abdominal compartment syndrome in burn patients. J Trauma. 2000;49:387.
55. Santry HP, Gillen DL, Lauderdale DS. Trends in bariatric surgical procedures. JAMA. 2005;294:1909–1917.
56. DeMaria E. Morbid obesity. In: Mulholland MW, ed. Greenfield's Surgery. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006:741.
57. Stoney RJ, Cunningham CG. Acute mesenteric ischemia. Surgery. 1993;114:489.
58. Safioleas MC, Moulakakis KG, Papavassiliou VG, et al. Acute mesenteric ischaemia, a highly lethal disease with a devastating outcome. Vasa. 2003;35:106.
59. Edwards MS, Cherr GS, Craven TE, et al. Acute occlusive mesenteric ischemia: surgical management and outcomes. Ann Vasc Surg. 2003;17:72.
60. Endean ED, Barnes SL, Kwolek CJ, et al. Surgical management of thrombotic acute intestinal ischemia. Ann Surg. 2001;233:801.
61. Birnabaum W, Rudy L, Wylie EJ. Colonic and rectal ischemia following abdominal aneurysmectomy. Dis Colon Rectum. 1964;7:293.
62. Boley SJ, Brandt LJ, Veith FJ. Ischemic disorders of the intestine. Curr Probl Surg. 1978;15:1.
63. Birnabaum W, Rudy L, Wylie EJ. Colonic and rectal ischemia following abdominal aneurysmectomy. Dis Colon Rectum. 1964;7:293.
64. Ottinger LW. The surgical management of acute occlusion of the superior mesenteric artery. Ann Surg. 1978;188:721.
65. Montgomery A, Hartmann M, Jonsson K, et al. Intramucosal pH measurements with tonometers for detecting gastrointestinal ischemia in porcine hemorrhage shock. Circ Shock. 1989;29:319.
66. Nishida A, Fukui K. Transcatheter treatment of thromboembolism in the superior mesenteric artery. N Engl J Med. 2005;353:4.
67. Kaminsky O, Yampolski I, Aranovich D, et al. Does a second-look operation improve survival in patients with peritonitis due to acute mesenteric ischemia? A five-year retrospective experience. World J Sur. 2005;29:645.