Karen L. Booth
Stephen J. Roth
Pediatric cardiac surgery and postoperative care has undergone significant advancements over the past several decades. The successful collaboration of numerous disciplines including pediatric cardiac surgery, anesthesia, cardiology, and intensive care have led to an increase in the complexity of cardiac lesions repaired with a simultaneous reduction in surgical mortality. There has been a shift away from palliative procedures to primary repair as early as possible, even in the very premature neonate (1,2,3). The heterogeneity of congenital heart disease and the individualized care these patients require has led to the emergence of dedicated pediatric cardiac intensive care units. This chapter focuses on the key principles for successful management of the pediatric cardiac surgical patient including assessment of the preoperative status and operative course, postoperative stabilization, subsequent evaluation of the repair, and support of myocardial function.
Cardiac Intensive Care: A Specialized Environment
The pediatric cardiac intensive care unit (CICU) shares many of the common features of a generalized intensive care unit. Bedside monitors with the ability to display heart rate, arterial blood pressure, central venous pressure, pulse oximetry, and respiratory rate are essential. Additionally, the monitor should be capable of transducing several pressures simultaneously, including right atrial pressure, left atrial pressure, and pulmonary artery or right ventricular pressure, as many pediatric cardiac patients have several intracardiac catheters placed for postoperative hemodynamic monitoring. There should be central monitoring capable of storing at least 24 hours of individual patient hemodynamic data and alarms. This is often important for reconstructing critical events and trending a patient's recovery or deterioration over time.
Ventilators capable of supporting patients of all sizes (from premature neonates through adults) should be readily available. Specialized ventilators such as the oscillator should be also available for patients with coexisting lung disease. Inhaled nitric oxide has become an essential therapy in the treatment of the postoperative cardiac patient with pulmonary hypertension (4,5). There should be several ventilators capable of delivering inhaled nitric oxide, as it is common for more than one patient to be receiving this therapy simultaneously. Bedside blood gas analysis with hand-held point-of-care testing devices is the norm at many institutions. If this is not available, rapid blood gas analysis with a laboratory turnaround time of less than 15 to 30 minutes is necessary.
Many postoperative cardiac patients have dysrhythmias, including tachycardias, bradycardias, and heart block. Thus, the cardiac intensive care unit must be equipped with the equipment to provide temporary cardiac pacing. Most contemporary battery-operated temporary pacemakers also have the ability to deliver rapid atrial pacing, which can terminate tachyarrhythmia including re-entrant supraventricular tachycardia and atrial flutter. A portable electrocardiogram (ECG) machine and defibrillator are essential devices for bedside diagnosis, cardioversion, and emergency defibrillations.
Echocardiography should be accessible for rapid assessment of the postoperative patient for important residual lesions or tamponade. Equipment for emergent bedside sternotomies for tamponade is required. This is accomplished with a mediastinal cart or tray stored in the CICU and stocked with all the necessary instruments. This cart will also facilitate emergency cannulation for extracorporeal membrane oxygenation (ECMO) if mechanical support of the myocardium is necessary.
Postoperative Assessment and Stabilization
The admission of a pediatric patient to the CICU after congenital heart surgery is a complex undertaking. Considerable advanced preparation is required for successful transition of a patient from the operative environment to the intensive care unit. The first several hours after separation from cardiopulmonary bypass (CPB) is the time when patients are the most vulnerable to decompensation as they are physically moved and care is transferred to a new team. Preparations should begin before the patient is admitted to the hospital. Most cardiovascular surgical programs have multidisciplinary conferences to review each patient's history and data. Important components of the preoperative review include the precise anatomic diagnosis, prior operative procedures, coexisting medical conditions, medication regimen, and current preoperative echocardiographic and catheterization findings. In this venue, the surgical approach as well as the initial postoperative care should be planned. For example, if a patient is known to have pulmonary hypertension by preoperative catheterization data, the team can plan to have nitric oxide available in the operating room and/or CICU. If additional studies or subspecialty consultations are required, ample time should be allotted to accomplish a complete preoperative evaluation.
Transition from the Operating Room
As the surgery concludes, a patient report should be formulated by the operating room team and called to the receiving nurse and physician in the CICU. This report includes information on the procedure performed, the hemodynamic status, current vasoactive infusions, and ventilator settings. This allows the CICU sufficient time to prepare the appropriate personnel, equipment, and medications. The patient is transferred to the CICU by the anesthesia and surgical team. Upon arrival the initial goal is to transition from portable monitoring and transport equipment to the bedside CICU monitor and ventilator as efficiently as possible while maintaining gas exchange and patient stability. It is prudent to use the same infusion pumps from the operating room so as to not interrupt any vasoactive infusions. During this critical time, the medical decision making and management of the patient should continue to be provided by the anesthesia and surgical team until a complete exchange of information occurs.
The key operative events are details of the repair, length of CPB including any special techniques used such as deep hypothermic circulatory arrest or low-flow regional perfusion, abnormal rhythms, or significant bleeding after CPB. The initial assessment of the repair typically includes transesophageal or epicardial echocardiography, intraoperative intracardiac saturation measurements to assess for residual shunts, and initial hemodynamic pressure measurements. If a second CPB run is required to correct residual lesions, this can have important effects on myocardial function in the initial postoperative period. If the sternum is left open, it is important to know the exact surgical reason for this decision. For example, was there excessive chest bleeding, poor myocardial function, or difficulty with ventilation (6)? Each would have different implications for management strategies in the first postoperative hours.
The anesthesia team can provide a wealth of information regarding patient course and stability. The key anesthesia events are airway issues such as difficulty with bag-mask ventilation or tracheal intubation, type of anesthesia given including cumulative dose of narcotics and benzodiazepines, current vasoactive and inotropic support, and blood and colloid products administered. The anesthesia team should be able to predict the initial course and readiness for extubation.
After patient transfer and the exchange of information have occurred, the CICU team performs their initial assessment. The physical exam should focus on clinical cardiac output and evidence for residual lesions. Patients often emerge from the operating room hypothermic, and perfusion may be affected by the need to rewarm slowly. Some murmurs are expected (e.g., after a procedure that includes an aortopulmonary shunt). Other patients should have a silent precordial exam, such as repair of a ventricular septal defect (VSD). Patients with cavopulmonary connections such as the bidirectional Glenn or Fontan procedure should also have a quiet precordial exam. Murmurs in these patients may indicate outflow tract obstruction or atrioventricular valve regurgitation, each of which can adversely affect the function of the single ventricle.
Initial laboratory evaluation should include immediate arterial blood gas (ABG) analysis. Ideally, the anesthesia and surgical team should remain in the CICU until the first ABG has been measured to ensure that the patient has adequate gas exchange. Interpretation of the initial ABG requires understanding of the patient's physiology. Patients with two-ventricle physiology are often receiving 100% oxygen (O2) and, in the absence of significant pulmonary pathology, should have a high arterial partial pressure of O2 (PaO2) to reflect this. Patients with large left-to-right shunts preoperatively may have significant alveolar–arterial gradients from pulmonary edema. Patients undergoing right ventriculotomies, as in tetralogy of Fallot repairs, may have right ventricular dysfunction and elevated central venous pressures. This may cause a right-to-left shunt at the atrial level if a patent foramen ovale (PFO) is preserved, and a PaO2 <100 mm Hg regardless of the fraction of inspired oxygen (FIO2) delivered. Single-ventricle patients receive a lower FIO2 to prevent pulmonary overcirculation and systemic undercirculation (see Single Ventricle Physiology). The PaO2 in these patients should be 35 to 45 mm Hg. In general, patients should be ventilated to a normal arterial partial pressure of carbon dioxide (PaCO2), which is 35 to 45 mm Hg. An indication for mildly hyperventilating a patient (PaCO2 30–35 mm Hg) would include pulmonary hypertension to reduce pulmonary vascular resistance (PVR) (7).
Pulmonary overcirculation may be treated with hypoventilation to increase PVR (PaCO2 45–50 mm Hg). Evaluation of a metabolic acidosis with low pH and bicarbonate levels should raise concern for low cardiac output syndrome. This should be treated immediately by providing judicious intravascular volume supplementation, providing increased inotropic support, and maximizing oxygen-carrying capacity with a blood transfusion for anemia. If the cause of the low cardiac syndrome is unclear or is unresponsive to initial measures to improve cardiac output, urgent bedside echocardiography to evaluate the repair and myocardial function and to look for possible tamponade should be performed.
Additional laboratory evaluations to be performed are blood chemistries, complete blood count with platelet count, coagulation studies, and lactate level. Serial postoperative lactate levels after congenital heart surgery have been predictive of outcomes. Higher initial ICU lactate levels (9.4 vs. 5.6 mmol/L) and lactates that continue to rise greater than 0.75 mmol/L/hour are associated with poorer outcome (death or use of ECMO) (8,9). Coagulation parameters including prothrombin time (PT), partial thromboplastin time (PTT), fibrinogen, and platelet count should be normal. Any abnormalities in the setting of excessive chest bleeding should be aggressively corrected. Additional doses of protamine can be given in the CICU if the PTT is prolonged and there is excessive chest bleeding. If all coagulation parameters are corrected and there is still excessive bleeding, an antifibrinolytic such as aprotinin, tranexamic acid, or ε-aminocaproic acid may be considered (10). Aprotinin is currently not available until further studies are done regarding its side effects. Activated factor VIIa has been successfully used for refractory surgical bleeding in the setting of post-CPB ECMO (11). If bleeding remains pronounced despite aggressive pharmacologic and blood product transfusion, it may be a surgical bleed requiring chest exploration. Similarly, brisk chest bleeding that abruptly stops with a concurrent rise in intracardiac pressures is likely due to cardiac tamponade; chest exploration is also typically required in this situation.
An admission chest radiograph should be performed minutes after arrival. This study will verify tracheal tube, nasogastric tube, pacing wire, and intracardiac catheter placement. An assessment of cardiac size and the lungs is essential to rule out a significant pneumothorax or hemothorax, both of which should be evacuated immediately. In some procedures such as unifocalization of aortopulmonary collaterals, there can be alveolar infiltrates from increased blood flow or hemorrhage, and the early use of positive end-expiratory pressure on the ventilator can improve oxygenation. Assessing the placement of intracardiac catheters is important in interpreting pressure and saturation data (see Hemodynamic Monitoring). The right atrial catheter or common atrial catheter typically enters the heart through the right atrial appendage and is directed inferiorly toward the inferior vena cava. The left atrial catheter usually enters the heart through a right pulmonary vein and is directed to the left atrium with a horizontal course. Alternatively, the left atrial catheter may enter the heart through the left atrial appendage and course inferiorly toward the mitral valve. A pulmonary artery catheter enters the heart through the right ventricular outflow tract and is directed superiorly across the pulmonary valve into the main pulmonary artery. A right ventricular catheter enters the heart through the right atrium and crosses the tricuspid valve with the tip in the body of the right ventricle.
A 12- or 15-lead ECG should be performed to assess rhythm and atrioventricular (AV) conduction. Lack of AV synchrony can contribute to a low cardiac output state, so every effort should be made to preserve AV synchrony with temporary pacing if there is AV nodal block or an ectopic junctional rhythm (see Postoperative Rhythm and Pacing). The QRS complex should be compared to baseline to assess for new abnormalities including bundle branch block. Complete right bundle branch block is common after VSD closure for tetralogy of Fallot or truncus arteriosus repairs, but usually it is not of hemodynamic significance. The ST segment should be assessed for signs of ischemia, especially after procedures that include coronary artery reimplantation.
After the initial assessment and stabilization, a plan may be made for weaning both inotropic support and ventilatory support over the subsequent hours to days. Analgesia and sedation will be tailored to this assessment and plan. Older children with short CPB support times, stable hemodynamics, and minimal chest bleeding (e.g., conduit revisions, subaortic membrane resections, septal defect closures) can be extubated almost immediately when they awaken from anesthesia (12). Neonates and younger infants often undergo more complex repairs (e.g., the arterial switch operation, truncus arteriosus repair, AV canal repair, tetralogy of Fallot repair) and will need more gradual weaning of support over 24 to 48 hours. Those undergoing complex neonatal single-ventricle palliation (e.g., stage I palliation for hypoplastic left heart syndrome [HLHS]) often have open sternums; these patients will require several days of stabilization and diuresis before their sternums can be closed.
Hemodynamic Monitoring
Patients undergoing congenital heart surgery will have intravascular or transthoracic intracardiac catheters placed for postoperative hemodynamic monitoring. These catheters are invaluable for the continual assessment of the patient and have a low risk of complications (13,14). Virtually every patient will have an arterial catheter placed for ABG sampling and blood pressure monitoring. Monitoring the central venous pressure is routine as well except for the simplest procedures performed via a thoracotomy (e.g., patent ductus arteriosus ligation or coarctation repair). The most common transthoracic intracardiac catheter placed is a right atrial catheter. This catheter may have more than one lumen, thus allowing for simultaneous central venous pressure measurement and vasoactive medication delivery. Patients may have a second central venous catheter placed by the anesthesiologist to manage the patient in the operating room before CPB is initiated. Often this catheter is inserted into the internal jugular vein with the tip at the superior vena cava–right atrial junction. This catheter may be placed in lieu of a right atrial catheter in older children. Young infants with complex two-ventricle repairs or a mitral valve repair will typically have a transthoracic left atrial intracardiac catheter placed. This catheter is valuable in assessing left ventricular function, mitral valve function, and intravascular volume status.
In single-ventricle patients, a common atrium is either congenitally present or created at the first stage of the procedure. Therefore, transthoracic intra-atrial catheters in these patients are referred to as common atrial catheters. Transthoracic pulmonary artery catheters are placed for selected repairs including truncus arteriosus and tetralogy of Fallot repairs. However, with the increased use of intraoperative transesophageal echocardiography, these catheters are less common and are reserved for procedures where the incidence of postoperative pulmonary hypertension is high, such as repair of obstructed total anomalous pulmonary venous return. More commonly used are transthoracic right ventricular catheters that enter the heart through the right atrial appendage and are positioned with the tip crossing the tricuspid valve. These catheters are useful in assessing right ventricular and pulmonary artery pressures after complex pulmonary artery reconstructions such as in tetralogy of Fallot with pulmonary atresia and aortopulmonary collaterals. In contrast to adults, children rarely have flow-directed pulmonary artery (Swan Ganz) catheters placed for postoperative monitoring. This is due to both small patient size and the need for unobstructed access for intracardiac repairs.
|
Table 81.1 Causes of elevated or reduced right atrial pressure |
||
|
There are multiple causes of abnormal right and left atrial pressures (Tables 81.1 and 81.2). Typically, the mean right atrial pressure ranges from 0 to 8 mm Hg, and the mean left atrial pressure is 1 to 2 mm Hg higher than the right atrial pressure (15). In postoperative patients, these mean pressures are higher due to the effects of CPB on the myocardium and the volume of fluid received in the operating room. In general, mean right and left atrial pressures should not exceed 15 mm Hg; when they are elevated, the etiology should be addressed. In determining the cause of high atrial pressures, the onset is important. Gradually increasing pressures often indicate that a clinical problem such as low cardiac output or tamponade physiology is evolving. A sudden change in the pressure without a change in heart rhythm or other vital signs may indicate a technical problem with the catheter or transducer (e.g., the transducer fell off the bed). Rezeroing a transducer is always indicated if the numbers are not compatible with the clinical status. The morphology of the atrial tracing is also helpful in determining the etiology of a pressure elevation. Large a waves, referred to as cannon a waves, occur when the atrium is contracting against a closed AV valve. This occurs with loss of AV synchrony as in AV block or junctional rhythm. Large v waves occur during ventricular contraction with an incompetent AV valve. Severe AV regurgitation in a low cardiac output state may require surgical consultation and possible reoperation. Low atrial filling pressures in the setting of low arterial blood pressure or cardiac output should be treated with volume expansion. Typically 5 to 10 mL/kg of colloid or crystalloid fluid is the initial dose to restore preload. Chest bleeding with low atrial pressure should prompt correction of any coagulopathy and/or anemia with blood products.
|
Table 81.2 Causes of elevated or reduced left atrial pressure |
||
|
||
|
Table 81.3 Causes of elevated or reduced pulmonary artery pressure |
||
|
Causes of abnormal pulmonary artery or right ventricular pressures are listed in Table 81.3. Normal mean pulmonary artery pressures are 10 to 20 mm Hg (15). There can be considerable variation in the postoperative patient, but the mean should not exceed 25 to 30 mm Hg in repaired patients. The right ventricular systolic pressure is often expressed as a percentage of the systemic systolic pressure, as both may be transiently elevated in response to high catecholamine states such as agitation. The right ventricular pressure should be less than 30% to 50% systemic. Elevated pulmonary pressures are generally not well tolerated for long periods of time. Correcting associated hypocarbia and acidosis, both of which elevate PVR, should be accomplished quickly. Inhaled nitric oxide as a selective pulmonary vasodilator is useful for pulmonary hypertension and low cardiac output (5,16).
Saturation data from intracardiac catheters are also valuable in assessing the postoperative cardiac patient. The causes of abnormal right atrial, left atrial, and pulmonary arterial saturations are listed in Table 81.4. Accurate interpretation of this saturation data relies on precise knowledge of the location of the catheter tip for sampling and the patient's physiology. Right atrial and pulmonary artery saturation data are a useful assessment of the patient's cardiac output and oxygen extraction. Normal superior vena cava, right atrial, and pulmonary arterial saturations in a patient with two-ventricle physiology and no intracardiac shunts are approximately 70% to 80%. If the patient has a normal cardiac output and fully saturated systemic arterial blood, the arteriovenous O2 saturation difference will be normal at approximately 25% to 30% (17). It is common for the right atrial saturation to be in the 60% range after CPB with adequate oxygen delivery and perfusion. Lower right atrial saturations are expected in patients with single-ventricle physiology because of intracardiac right-to-left shunting and systemic O2desaturation. As long as the arteriovenous saturation difference is ≤30%, the cardiac output should be normal. In patients with two-ventricle physiology, the true mixed venous saturation is in the pulmonary arteries where complete mixing of systemic venous blood occurs. An elevation in the pulmonary artery saturation after atrial or ventricular septal defect repair is indicative of a residual left-to-right shunt. An absolute pulmonary artery saturation of >80% while receiving an FIO2 <0.4 is predictive of a residual intracardiac shunt of greater than 1.5:1 (18). The most common causes of decreased left atrial saturation and concurrent systemic desaturation are right-to-left atrial shunting (common after tetralogy of Fallot repair when the PFO is left open) and pulmonary disease.
|
Table 81.4 Causes of abnormal right atrial, left atrial, and pulmonary artery saturation |
|||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||
Transthoracic intracardiac catheters should be maintained in the postoperative period only until the necessary data are obtained. Typically, left atrial and pulmonary artery catheters are removed within the first 48 hours while the patient is still intubated and the chest tubes are in place in case there is bleeding (the coagulation profile should be normal) upon catheter removal. Although significant bleeding is rare, catheters are removed with blood available at the bedside. Right atrial catheters may remain in place up to 2 weeks but should be removed as soon as clinically indicated.
Postoperative Rhythm and Pacing
Arrhythmias are common after congenital heart surgery (19). Postoperative electrolyte imbalances, myocardial stress and dysfunction, and intracardiac incisions and suture lines all play a role in the etiology of new rhythm disturbances. Both bradycardias and tachycardias occur, but fortunately most are self-limited.
The most common bradycardia is sinus bradycardia. Sinus bradycardia is normal in children during sleep and with high vagal tone and is generally benign. Patients returning from the operating room may be hypothermic with core temperatures of 32°C to 34°C; they will remain bradycardic until their temperature rises closer to normal. Patients at risk for sinus bradycardia are those undergoing atrial baffles such as a lateral tunnel-type Fontan for a single-ventricle defect or atrial switch procedures for transposition of the great arteries. Patients with sinus venosus and primum atrial septal defect repairs also commonly have slower sinus rates. Extremely bradycardic patients can be treated with pacing with temporary epicardial wires placed in the operating room, but in the absence of long sinus pauses, sinus bradycardia tends to be well tolerated.
Surgeries near the AV node such as ventricular septal defect repairs, AV canal repairs, resection of subaortic muscle, and tetralogy of Fallot repairs create risk for injury to the conduction system. Usually this is manifest as bundle branch block, most commonly right bundle branch block after tetralogy of Fallot repair. Left bundle branch block can occur with subaortic surgeries. Rarely there is more significant block such as complete heart block. Fortunately, it resolves in the majority of patients (<2% incidence overall, with recovery in two thirds of affected patients) without need for permanent pacemaker placement (20).
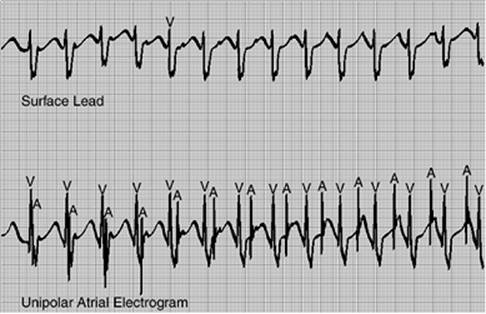
Common tachyarrhythmias include supraventricular tachycardia and junctional tachycardia. Patients with accessory pathways will often first develop a tachyarrhythmia in the postoperative period. Ectopic tachycardias are also common after congenital heart surgery (21). High catecholamine states, intracardiac catheters and suture lines, and electrolyte abnormalities all contribute to the appearance of postoperative tachyarrhythmias in previously asymptomatic patients. The onset of tachycardia may provide useful information regarding its etiology. Tachycardias with a sudden onset that generate a sustained heart rate with minimal variability are likely to be re-entrant in nature. Tachycardias with a gradual increase in heart rate with some beat-to-beat variability are likely to be automatic in nature. Temporary epicardial atrial wires can be used to obtain intracardiac atrial electrograms to examine the relationship of the P waves to the QRS complex to further aid in diagnosis (see Fig. 81.1). Atrial wires can also be used to terminate re-entrant rhythms by overdrive pacing. The indication for treatment is a hemodynamic change causing low cardiac output or blood pressure, as most tachyarrhythmias will improve with time. A summary of common antiarrhythmics used after congenital heart surgery is provided in Table 81.5.
|
|
|
Figure 81.1. The use of an atrial electrocardiogram to diagnose ectopic atrial tachycardia. The surface electrocardiogram (lower tracing) reveals an irregular, narrow complex rhythm. Atrial depolarizations (P waves) are not easily discernible. The unipolar atrial electrocardiogram (upper tracing) reveals a rapid ectopic atrial tachycardia with many blocked atrial premature beats. Atrial depolarization is denoted by “A” and ventricular depolarization is denoted by “V.” |
For re-entrant and ectopic supraventricular tachycardias, β-blockers, such as esmolol, are usually the first-line therapy and are well tolerated. Digoxin can be considered in patients with apparent accessory pathways that are not pre-excited or for rate control in rapid atrial rhythms. Second-line agents include procainamide and amiodarone. Amiodarone should be used with caution, as the incidence of serious side effects including circulatory collapse and proarrhythmia is high (22). Once the tachycardia is controlled and the patient has progressed to extubation, intravenous agents can be transitioned to oral agents (e.g., the β-blocker propranolol can be substituted for esmolol). More refractory supraventricular tachycardias may be treated with the class III agent sotalol, or class IC agents flecainide or propafenone. The length of oral treatment will vary with the nature of the tachycardia, but should be considered for at least 1 to 3 months postoperatively.
Junctional ectopic tachycardia (JET) is a narrow complex rhythm that arises just below the AV node. It is most common after ventricular septal defect closure in tetralogy of Fallot and AV canal repairs. JET usually occurs in the first 24 to 48 hours postoperatively and is almost always self-limited. The typical electrocardiographic finding is AV dissociation (Fig. 81.2) with a more rapid ventricular rate (typically >180 bpm), but there can be retrograde P waves with a 1:1 relationship. Because of the lack of AV synchrony, this rhythm can lead to elevated atrial pressures and low cardiac output with hypotension. Treatment is directed toward reducing catecholamine states by weaning vasoactive infusions such as dopamine; providing sedation, analgesia, and possibly paralysis; and avoiding hyperthermia with active cooling. Atrial pacing above the junctional rate (if <180 bpm) can restore AV synchrony and improve hemodynamics. The most efficacious pharmacologic therapy includes procainamide in combination with cooling (23). Amiodarone has been reported to be successful in the treatment of JET (24), but it should be used with caution due to acute cardiac side effects such as hypotension and proarrhythmia (22). Because JET is a self-limited tachycardia, once the patient has regained normal sinus rhythm, a gradual reduction in therapy starting with rewarming and removal of deep sedation and/or paralysis can occur. Pharmacologic support should then be weaned over 24 to 48 hours.
Ventricular ectopy after congenital heart surgery can occur, especially in the setting of electrolyte abnormalities. Monomorphic premature ventricular beats or ventricular bigeminy or trigeminy is usually benign and self-limited. Sustained ventricular tachycardia that is rapid and polymorphic is dangerous and concerning for myocardial ischemia. Treatment with lidocaine and cardioversion should be attempted, but an urgent evaluation of myocardial function and perfusion must be pursued or a cardiac arrest may be imminent.
Respiratory and Ventilatory Management
Postoperative ventilation should take into consideration the important cardiopulmonary interactions that occur after congenital heart surgery. Each patient's ventilatory support and weaning plan should be individualized to his or her physiology and hemodynamic status using a set of guiding principles. Frequent reassessment and ventilatory adjustments should be expected.
Positive pressure ventilation has effects on preload. Increasing tidal volumes and positive end-expiratory pressure (PEEP) increase intrathoracic pressure and limit systemic venous return. Increased lung volume and intrathoracic pressure also increase afterload to the right (pulmonary) ventricle (25).
Therefore, in patients with limited right ventricular function, such as patients undergoing tetralogy of Fallot repair with a ventriculotomy, right ventricular output may be compromised by elevated mean airway pressures. This can result in high right-sided filling pressure, poor right ventricular function, hepatomegaly, ascites, and pleural effusions. As the patient becomes fluid overloaded and gas exchange is impaired, the temptation is to increase ventilatory support. However, this may worsen the patient's clinical status. Patients with cavopulmonary connections and passive pulmonary blood flow also have compromised pulmonary blood flow and cardiac output with positive pressure ventilation (26,27). A strategy of a larger tidal volume (15 mL/kg) with a lower ventilatory rate may minimize afterload and give the right ventricle an opportunity to eject or the pulmonary arteries additional filling time during a longer expiratory phase. The patient should be allowed to breathe spontaneously with less mandatory ventilator breaths. Ideally, if the patient will tolerate it, he or she should be extubated as soon as possible after surgery.
|
Table 81.5 Common antiarrhythmic agents used after congenital heart surgery |
||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||||||||||||||||||||||||
|
Figure 81.2. The use of an atrial electrocardiogram to diagnose junctional ectopic tachycardia. The surface electrocardiogram (upper tracing) reveals a regular, narrow complex rhythm with possible atrioventricular (AV) disassociation. The unipolar atrial electrocardiogram (lower tracing) demonstrates AV dissociation with a ventricular rate that is more rapid than the atrial rate. This is junctional ectopic tachycardia. Atrial depolarization is denoted by “A” and ventricular (or junctional) depolarization is denoted by “V.” |
||||||||||||||||||||||||||||||||||||||||||||||||
Positive pressure has the opposite effect on the left (systemic) ventricle. The higher-pressure aorta is not as affected by the lung volumes. The increased intrathoracic pressure decreases left ventricular afterload due to the decreased transmural pressure across the myocardium (28). Therefore, patients with left ventricular dysfunction can improve with the initiation of positive pressure ventilation (29). Patients with ventricular dysfunction also have increased work of breathing due to increased pulmonary edema and decreased lung compliance. Positive pressure ventilation helps these patients by decreasing the work of breathing and oxygen consumption. A judicious amount of PEEP at 3 to 5 cm H2O maintains lung volumes at functional residual capacity. This keeps alveoli recruited and minimizes increases in pulmonary vascular resistance caused by atelectasis.
The mode of ventilation used to support cardiac patients often depends on the experience of the team members in the cardiac intensive care unit. Many units will ventilate in a pressure mode, acknowledging that the lung compliance in most postoperative cardiac patients is normal and not rapidly changing as it is in patients with primary lung disease. Volume ventilation is equally acceptable, and newer ventilators are capable of volume ventilation with deceleration flow patterns, which is more comfortable for spontaneously breathing patients. More novel techniques employing higher airway pressures such as high-frequency oscillatory ventilation and airway pressure release ventilation have been used successfully in pediatric patients with primary lung disease (30,31). These modes of ventilation have limited use after congenital heart surgery due to reductions in cardiac output that occur at higher mean airway pressures in infants (32,33). Fortunately, significant lung disease after cardiac surgery is uncommon. There are selected cases where the degree of lung disease outweighs the cardiac disease and high-frequency oscillatory ventilation has been anecdotally beneficial. Scenarios such as pulmonary hemorrhage after collateral unifocalization procedures, severe pulmonary edema after repair of obstructed total anomalous pulmonary return, and respiratory distress syndrome in premature infants undergoing cardiac surgery are examples.
Timing of extubation is contingent upon several factors. The patient should be evaluated for significant residual cardiac lesions and the adequacy of myocardial function. Hemostasis should be achieved. The patient should be weaned to a low mandatory ventilatory rate (4–6 breaths per minute) or to a pressure support mode with no mandatory breaths and a FIO2 of ≤0.4. The patient should be awake, not tachypneic for age, and able to generate spontaneous tidal volumes of 6 to 8 mL/kg per breath. Problems encountered postextubation include atelectasis, stridor, and diaphragm paresis or paralysis. Atelectasis is most common in neonates, larger but immobile children, or chronically malnourished patients. Chest physiotherapy and occasionally bronchoscopy may be employed to re-expand atelectatic segments of lung. Stridor is usually self-limited and can be treated with nebulized racemic epinephrine and steroids, which reduce mucosal swelling. Persistent stridor or a weak cry can also be a manifestation of a recurrent laryngeal nerve injury with vocal cord paresis or paralysis (34).
Formal assessment of swallowing function to prevent recurrent aspiration of oral feeds may be required if vocal cord injury is identified. Phrenic nerve injury with associated hemidiaphragm dysfunction is challenging to treat. The postextubation chest radiograph typically reveals an elevated hemidiaphragm with collapse of the ipsilateral lung. Fluoroscopy demonstrating decreased (paretic) or paradoxical (paralyzed) movement of the diaphragm will confirm the diagnosis. Ultrasound can also be used to assess diaphragm function, but it is less reliable in distinguishing a paretic from a paralyzed diaphragm, which may impact treatment (35). Usually the injured phrenic nerve will recover with time. Older children can often tolerate the phrenic nerve injury and compensate with the use of accessory muscles of breathing. Neonates and infants may require a hemidiaphragm plication, especially if the diaphragm is paralyzed, to wean successfully from mechanical ventilation (36).
Noninvasive forms of respiratory support are being used more commonly after congenital heart surgery. Continuous positive airway pressure (CPAP) delivered with nasal prongs or a mask and bilevel positive airway pressure (BiPAP) also delivered with nasal or full face masks provides respiratory support using positive pressure without a tracheal tube. In patients who have been extubated but have increased work of breathing or have developed atelectasis, these methods will often avert the need for reintubation. In patients with ventricular dysfunction and marginal hemodynamics, a planned extubation to noninvasive support such as CPAP will provide continued afterload reduction of the systemic ventricle (37). Also, for those patients with prolonged ventilator courses and respiratory muscle deconditioning, a planned extubation directly to CPAP or BiPAP with subsequent weaning can successfully transition a patient to unassisted breathing. Children often require additional sedation to tolerate CPAP and BiPAP masks for longer periods of time.
Sedation, Analgesia, and Neurologic Monitoring
Sedation and analgesia are important components of postoperative care of pediatric cardiac surgical patients. The strategy of sedation and analgesia should be tailored to the age and anatomy of the patient; type of repair and operative course, including rhythm and bleeding concerns; and anticipated postoperative course, including timing of sternal closure (if delayed) and initial hemodynamics. A patient following atrial septal defect closure requires different sedation and analgesia management than a patient following stage 1 palliation who has an open sternum and labile blood pressure. Analgesia is initiated in the operating room, and most agents used are narcotic based. High-dose narcotics have been shown to alleviate the stress response associated with cardiac surgery and CPB (38,39). High-dose fentanyl (up to 25 µg/kg) can be administered to neonates with minimal hemodynamic effect (40). As a continuation of operative anesthesia, patients with marginal hemodynamics and complex repairs or palliations are deeply sedated with continuous fentanyl infusions and usually paralyzed as well for the initial postoperative course to minimize the stress response and oxygen consumption. Interventions in the intensive care unit that may provoke stress such as tracheal tube suctioning should be managed with anticipatory doses of fentanyl (41).
Common muscle relaxants used in the pediatric cardiac intensive care unit are rocuronium, vecuronium, pancuronium, and cisatracurium. Rocuronium has the shortest onset of action and is often used for intubation, but not continuous paralysis. Vecuronium is commonly employed as an infusion for continuous paralysis. Pancuronium is the longest-acting agent and is cleared by the kidneys, so it should be used with caution in patients with renal insufficiency. Cisatracurium is cleared by Hofmann degradation (i.e., independent of renal and hepatic function), so it may be the best choice in patients with multisystem organ failure. The significant side effects of succinylcholine, including severe bradycardia, have limited its routine use in the pediatric cardiac population.
Patients who have achieved hemodynamic stability but may require a longer ventilatory course for diuresis or pulmonary recovery, such as after a unifocalization procedure, benefit from sedation with continuous infusions of a narcotic and benzodiazepine. This provides a more continuous level of sedation and analgesia than intermittent bolus dosing of these agents. As the patient develops tolerance to these agents over several days, doses must be increased to achieve the same effect. The most common narcotic used is morphine, but fentanyl (shorter acting) and hydromorphone can be considered. Caution should be used with bolus dosing of fentanyl because of an idiosyncratic chest wall rigidity reaction that can occur with rapid infusion (42,43). Chest wall rigidity can prevent effective ventilation, and rapid muscle relaxation may be required to treat it.
Midazolam is the most common benzodiazepine used and is desirable due to its amnestic properties. Lorazepam and diazepam are other sedating benzodiazepines employed in the cardiac intensive care unit, but they are administered in bolus doses rather than as infusions. Patients typically develop tolerance to narcotics and benzodiazepine infusions after 5 to 7 days and will need to be transitioned to methadone and lorazepam for a weaning taper after extubation. The advantage to these agents is that they are longer acting and can be administered orally. Therefore, recovered patients can continue narcotic and benzodiazepine tapering as outpatients. Patients who have been successfully extubated can be transitioned to oral agents including acetaminophen, ibuprofen, and oxycodone. Older patients can benefit from the use of narcotic-based patient-controlled analgesia pumps. Short courses of the nonsteroidal anti-inflammatory drug ketorolac (eight doses or less) can be used in patients with normal coagulation and renal function.
Propofol has become a popular sedating agent in adult ICUs (44). It has a rapid onset of action and clearance, and it is an ideal agent in patients for whom rapid awakening is desired. Of note, propofol has no analgesic properties. Because it is a potent vasodilator and negative inotrope, it has limited use in cardiac patients with decreased myocardial function. There also have been reports of myocardial failure and acidosis in children (45). Therefore, propofol has generally been restricted to short-term use in older patients with two-ventricle physiology and normal myocardial function who are anticipated to extubate within 6 to 12 hours.
A promising new agent for sedation in the pediatric population is dexmedetomidine (46). It is an α2 agonist used as a continuous infusion in addition to a narcotic and benzodiazepine. Patients treated with a dexmedetomidine infusion require fewer rescue doses of other agents for sedation. The infusion does not depress respiration, and patients do not develop tolerance. Thus far, this agent appears safe and effective in pediatric cardiac patients, although data are limited to older infants and children (47). Some patients develop bradycardia, which resolves when the infusion is discontinued. A relative contraindication to dexmedetomidine may be high-grade AV nodal block or concurrent administration of medications that slow conduction at the AV node such as digoxin (48).
Procedural anesthesia in the cardiac intensive care unit for intubations, chest thoracentesis, and catheter placement is commonly required. For many patients, ketamine is an excellent agent for this indication. It is a dissociative anesthetic agent with rapid onset and excellent analgesic properties. Heart rate and blood pressure are preserved through central stimulation and diminished postganglionic reuptake. It has minimal effects on respiratory drive at lower doses, although airway secretions can be increased. A benzodiazepine should be given concurrently for hallucinations in older children. Another effective agent for procedural anesthesia is etomidate. It causes minimal cardiovascular depression and is an ideal agent for tracheal intubation in a hemodynamically compromised patient. Chloral hydrate is a hypnotic agent that can be safely given by mouth or per rectum for nonpainful procedures such as echocardiography.
The practice of neurologic monitoring in postoperative patients is evolving as more information about the neurologic sequelae of cardiac surgery becomes available. The incidence of neurologic abnormalities following CPB surgery is likely to be higher than reported. Postoperative electroencephalographic (EEG) seizures occur in up to 11% to 20% of neonates undergoing contemporary CPB techniques (49,50). The duration of deep hypothermic circulatory arrest appears to have a role in the incidence of seizures (50). Periventricular leukomalacia (as a marker of brain injury) is found on brain magnetic resonance imaging (MRI) in greater than 50% of neonates after congenital heart surgery (51). Most of these lesions appear to resolve over time, but the long-term implications on cognition and development are still being determined (52).
Neurologic surveillance in the cardiac intensive care unit is increasing. Routine EEG monitoring and a brain MRI for every patient are not practical. These tests tend to be reserved for patients with a high clinical suspicion of neurologic injury. The increasing use of near-infrared spectroscopy (NIRS) to monitor transcutaneous cerebral oxygen saturation in the intensive care unit may help identify periods of vulnerability to central nervous system injury. The cerebral oxygen saturation is measured by an oximeter probe placed on the forehead below the hairline. The measured saturation is a combination of mixed venous saturation (approximately 85%) and arterial saturation (approximately 15%). Normal cerebral oxygen saturation varies with cardiac defect but is approximately 70% in acyanotic lesions. A decrease of cerebral oxygen saturation of 20% from baseline was associated with an increased incidence of seizures and coma (53), and prolonged cerebral oxygen desaturation <45% has been associated with an increased incidence of periventricular leukomalacia on brain MRI (54). This technology may be used to monitor cerebral oxygen saturation as a surrogate for cerebral oxygen delivery. Studies demonstrating that interventions that raise the cerebral oxygen saturation lead to a reduction in neurologic injury have not been published to date.
Fluids and Nutrition
The body's inflammatory response to CPB results in significant increases in total body water and edema with diffuse capillary leak. Operative strategies to minimize this process include ultrafiltration on CPB and steroid administration (55). High-risk patients such as neonates and young infants may have peritoneal dialysis catheters placed electively in the operating room. Fluid management and diuretic therapy in the first 24 to 48 hours after cardiac surgery have a significant impact on the patient's hemodynamic status and recovery. During the first 24 hours, many patients are oliguric despite adequate atrial filling pressures. Longer CPB times, increased complexity of the repair, and preoperative renal dysfunction contribute to the duration of oliguria. Intravenous fluids should be restricted to one half of calculated maintenance fluids for at least 24 hours (or longer) if the patient does not have improved urine output. Preload should be maintained with crystalloid or colloid solutions using intermittent boluses of 5 to 10 mL/kg. Albumin (5% solution) priming of CPB circuits results in less requirement for volume expansion and less weight gain during and after CPB when compared to crystalloid solutions (56). This is likely due to increased intravascular oncotic pressure with albumin administration. Anecdotally, neonates benefit from volume expansion with 5% albumin over crystalloid, although there are no controlled trials comparing colloid and crystalloid in the postoperative setting. Older children with less complex repairs can receive normal saline or lactated Ringer solution to avoid blood product exposure.
Electrolytes should be normalized; potassium replacement should be performed cautiously in patients who are oliguric to avoid hyperkalemia. Calcium is a potent inotrope and ionized calcium levels should be maintained at the higher end of the normal range for age (1.2–1.3 mmol/L) (57). This strategy is particularly useful in neonates, patients with 22q11.2 deletions (DiGeorge syndrome) with hypoparathyroidism, and patients with myocardial dysfunction. Calcium can be repleted with bolus dosing (10 mg/kg calcium chloride or 100 mg/kg calcium gluconate) or with a continuous infusion. Magnesium should be repleted to avoid the development of ventricular dysrhythmias, which is more common with hypomagnesemia.
After 12 to 24 hours, diuretics can be introduced as bolus doses or as a continuous infusion. Diuretics can be considered earlier in patients with large left-to-right shunts and pulmonary edema to encourage clearance of excess lung water and weaning from the ventilator. Diuretics should be held longer than 24 hours in hemodynamically unstable patients who need frequent preload repletion with volume boluses. The diuretic initiated first at most institutions is the loop diuretic furosemide; it is administered at a 1 to 2 mg/kg dose intravenously every 6 to 12 hours. A continuous furosemide infusion of 0.1 to 0.3 mg/kg/hour (after an initial loading dose of 1 mg/kg) may be more desirable in hemodynamically fragile patients, or in patients with significant fluid overload (58). If urine output is not adequate, a second agent can be added. Common agents include the thiazide diuretic chlorothiazide, which can be given at a 5 to 10 mg/kg dose intravenously every 6 to 12 hours, and metolazone, which can be given at a 0.1 to 0.4 mg/kg dose enterally once daily. Newer agents including fenoldopam (Table 81.6), a selective dopamine receptor agonist, and nesiritide (Table 81.7), a natriuretic peptide, are additional choices (59,60).
It is common for patients to develop a significant hypochloremic metabolic alkalosis, as well as hypokalemia and hyponatremia, when receiving furosemide and/or chlorothiazide. Chloride can be repleted with arginine chloride, potassium chloride, or sodium chloride (only if hyponatremic from sodium loss and not congestive heart failure). Neonatal patients with shunted single-ventricle physiology can develop high serum bicarbonate levels and a compensatory respiratory acidosis with hypochloremia; their electrolytes should be normalized prior to extubation. Their reduced ventilatory drive and potential for apnea may impact the balance of pulmonary and systemic blood flow if not corrected prior to extubation.
Significant renal dysfunction beyond 72 hours after cardiac surgery is uncommon. Renal replacement therapy should be considered when renal function continues to worsen despite maximizing cardiac output. Often a peritoneal dialysis catheter inserted into the peritoneum and placed to gravity drainage can improve fluid balance without dialysis. Indications for dialysis include life-threatening electrolyte abnormalities including hyperkalemia, persistent metabolic acidosis, severe fluid overload impairing ventilation or sternal closure (if open), and rising blood urea nitrogen levels >100 mg/dL. If required, dialysis can be accomplished with peritoneal exchanges or with continuous venovenous hemofiltration (61). Conventional hemodialysis is usually not well tolerated in postoperative cardiac patients with myocardial dysfunction. Significant ongoing renal dysfunction carries a poor prognosis with >50% mortality in some reports (62,63).
Adequate nutrition after cardiac surgery is required for adequate wound healing and recovery. Unfortunately, nutrition is often compromised for several days due to hemodynamic instability and fluid intake restrictions. Enteral feedings should be restarted as soon as feasible. The use of promotility agents such as metoclopramide and postpyloric feeding tubes can enable enteral feeding in nearly all postoperative cardiac patients. An absolute contraindication for enteral feeding is the presence of necrotizing enterocolitis. Relative contraindications are the presence of an umbilical artery catheter, high-dose vasoconstrictive agents, and paralysis. Patients at increased risk for necrotizing enterocolitis are neonates with left-sided obstructive lesions, aortopulmonary shunts, and cyanotic lesions (64). Enteral feedings can be introduced in these patients but should advance slowly with close observation for signs of feeding intolerance such as emesis and abdominal distention. In patients for whom enteral feedings are not feasible, total parenteral nutrition should be used to avoid a catabolic state. Ranitidine or another histamine-2 antagonist should be routinely prescribed for protection against gastric mucosal bleeding from stress and nasogastric tubes until full-volume enteral feeds are re-established. Extubated patients with nausea should be treated with antiemetics such as ondansetron to encourage oral intake and weaning of intravenous fluids.
|
Table 81.6 Summary of catecholamines and dopaminergic agents |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Infectious Issues
In the first 24 hours following surgery, it is common for patients to have fever. This is presumably related to the inflammatory response after CPB and does not represent infection. Early postoperative fevers should be treated to help minimize oxygen consumption, but the patient may be observed for additional signs of infection prior to starting antibiotic treatment. All patients receive at least three doses of a second-generation cephalosporin (e.g., cefazolin) intravenously in the first 24 hours after surgery as prophylaxis. Treatment is extended in high-risk patients such as those with an open sternum, with immune deficiency, or receiving mechanical circulatory support. Fevers that persist or arise after the first 24 hours should be evaluated with a physical exam focused on the sternal incision, blood cultures obtained from indwelling intravascular catheters, and a urine culture. If tracheal secretions are copious and/or discolored, suggesting a respiratory source for fever, a tracheal aspirate may be obtained for Gram stain and culture. Chronically ventilated patients are often colonized with bacteria in their trachea, so a qualitative change in their secretions or increase in white blood cells on Gram stain may indicate a new respiratory infection. If the clinical suspicion for infection is high, intravenous antibacterial coverage should be broadened while awaiting culture results. Nosocomial infections are a significant cause of morbidity in the ICU (65,66). Every effort should be made to insert intravascular catheters using sterile technique, to enter and manipulate catheters using meticulous care, and to remove intravascular catheters as soon as feasible. Mediastinitis is a serious postoperative infection that occurs in approximately 2% of patients, with Staphylococcus aureus as the most common bacterial agent. Risk factors include prolonged open sternum and need for multiple chest re-explorations (67). Prompt antibiotic treatment with open debridement and use of muscle flaps has decreased the morbidity and mortality from mediastinitis (68).
Low Cardiac Output Syndrome
Low cardiac output syndrome (LCOS) is a common problem after congenital heart surgery with CPB, especially in neonates and young infants (69). Many factors are thought to contribute to decreased cardiac output including myocardial ischemia from aortic cross-clamping and associated reperfusion injury, inflammation from CPB, ventriculotomies (when performed), and the existence of hemodynamically significant residual lesions. There is an expected decrease in cardiac output that occurs over the first 6 to 12 hours after CPB with a nadir of <2 L/minute/m2 in the youngest patients (70). With appropriate recognition, the significant morbidities and occasional mortality related to LCOS can be prevented.
|
Table 81.7 Summary of noncatecholamine vasoactive agents |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||
Recognition of Low Cardiac Output
There are several clinical symptoms and signs of LCOS that should be immediately recognized (Table 81.8). On physical exam, early findings of low cardiac output include tachycardia, cool extremities, delayed capillary refill time, and diminished pulses. Decreased urine output, elevated filling pressures, and low mixed venous oxygen saturation are important signs. Hypotension and metabolic acidosis are later findings; they require immediate attention or a cardiac arrest may be imminent. Evaluation of LCOS should begin with physical exam. For example, auscultation for pathologic murmurs caused by residual obstructions, shunts, or valvar regurgitation is important. Hepatomegaly and ascites may indicate right heart failure, especially in surgeries involving right ventriculotomies. An echocardiogram should be obtained promptly to assess ventricular systolic function and to rule out tamponade. The quality of the repair should be assessed to look for residual lesions that can be corrected by reoperation or catheter-based intervention. Large residual shunts, severe valvular regurgitation, outflow tract obstructions, and venous baffle obstructions are generally poorly tolerated in the postoperative patient. If the patient has an open sternum, or if chest dressings obstruct transthoracic echocardiographic windows, a transesophageal echocardiogram should be performed. Occasionally, the etiology of the low cardiac output is not obvious by echocardiography or needs additional clarification before considering reoperation. There should be a low threshold to progress to cardiac catheterization in these patients. Catheterization in this population can be accomplished safely, even in patients supported with ECMO, and facilitates the diagnosis of important lesions in a majority of the patients (55%–76%) that can be addressed with interventional catheter procedures or reoperation (71,72).
|
Table 81.8 Signs of Low Cardiac Output Syndrome |
|
|
Treatment of Low Cardiac Output Syndrome
Once LCOS is recognized, and concurrent with ruling out correctible residual lesions, immediate therapy should be initiated. The goals of therapy are to maximize oxygen delivery and minimize oxygen consumption of the recovering myocardium. Anemic patients should be transfused with packed red blood cells to increase oxygen-carrying capacity. Cardiac output is a function of preload, contractility, and afterload. Intravascular volume should be repleted either with a colloid solution such as 5% albumin or alternatively with a crystalloid solution. Pharmacologic agents can be used to increase inotropy and decrease afterload (see Tables 81.6 and 81.7). Fevers should be actively prevented (e.g., by cooling the patient) to minimize oxygen consumption. The most unstable patients should receive neuromuscular blockade, deep sedation or anesthesia, and active cooling to minimize oxygen consumption. Continual reassessment of the response to therapy by physical exam focused on perfusion, and monitored parameters such as urine output and acidosis, is required.
Pharmacologic Therapy
Catecholamines (Table 81.6) have been the first-choice pharmacologic agents for increasing cardiac output. Almost all patients who undergo congenital heart surgery receive dopamine immediately after CPB. Dopamine stimulates β receptors in the heart and increases contractility; typical initial dosing is 3 to 7 µg/kg/minute via continuous infusion. Higher doses (>10 µg/kg/minute) will also stimulate α receptors in the peripheral vasculature and cause vasoconstriction. Epinephrine is another commonly used catecholamine. Low to moderate doses of epinephrine (0.02–0.1 µg/kg/minute) increase contractility and cause mild peripheral vasoconstriction, both of which tend to increase blood pressure. Dobutamine primarily stimulates β receptors in the heart. Higher doses have been associated with arrhythmias and tachycardia. This synthetic catecholamine is most often used in pediatric patients with chronic congestive heart failure (e.g., dilated cardiomyopathy) rather than in the postoperative setting. Isoproterenol stimulates β receptors in the heart and is both an inotrope and chronotrope. Because it causes tachycardia, which increases oxygen consumption, and peripheral vasodilation, which can lower blood pressure, it is not commonly used to treat LCOS. Norepinephrine and phenylephrine (pure α agonist) are predominantly α-receptor agonists; norepinephrine possesses reduced inotropic activity compared to dopamine and epinephrine, and their use is limited to patients with profound hypotension. Arginine vasopressin is a noncatecholamine vasoconstrictor that increases blood pressure by promoting vascular smooth muscle constriction without causing tachycardia. Its use has been described in patients with vasodilatory shock, but its role in cardiogenic shock is unclear and it has not improved outcomes in pediatric patients with poor myocardial function (73,74,75). Patients requiring continued high doses of these potent vasoconstricting agents to support systemic blood pressure should be considered for mechanical circulatory support. Catecholamines should also be used judiciously in postoperative neonates. While these agents do increase cardiac output, the relatively noncompliant neonatal myocardium may be more susceptible to catecholamine-driven increases in tachycardia, afterload, and oxygen consumption. Animal data show actual necrosis of neonatal piglet myocardium exposed to high-dose epinephrine (76). Fortunately, alternative pharmacologic options are available.
Afterload reduction is increasingly recognized as the principal form of pharmacologic support for the myocardium after CPB. The type III phosphodiesterase inhibitors milrinone and amrinone inhibit the breakdown of cyclic adenosine monophosphate (AMP), thus increasing the intracellular Ca2+ concentration, which enhances myocyte contractility, peripheral vasodilation, and diastolic relaxation (77). Milrinone has a shorter half-life than amrinone and less antiplatelet side effects, thus making it the more desirable alternative. Milrinone is tolerated well by postoperative neonates, and it promotes increased cardiac output, lower atrial pressures, and decreased pulmonary and systemic vascular resistance (78). A large, multicenter trial of milrinone after congenital heart surgery investigated the prophylactic use of milrinone in preventing LCOS. Patients treated with 0.75 µg/kg/minute of milrinone had a relative risk reduction of 55% for LCOS compared to patients treated with placebo (79). Based on these data and anecdotal experience, milrinone combined with dopamine is currently the combination therapy most commonly used to prevent and treat LCOS after congenital heart surgery. The vasodilators nitroprusside and nitroglycerine, both of which are nitric oxide donors, can decrease afterload and improve cardiac output, but they have no direct inotropic effects on the heart.
Other agents used to treat LCOS include thyroid hormone, B-type natriuretic peptide (BNP), and glucocorticoids. All patients exposed to CPB develop low thyroid hormone levels in the blood approximately 24 hours after bypass; this typically recovers by 5 to 7 days. Data are mixed, but there is some evidence that replacing tri-iodothyronine, the biologically active form of thyroid hormone, after congenital heart surgery increases cardiac output, blood pressure, and time to negative fluid balance and extubation (80,81,82). The natriuretic hormone system is important in regulating fluid balance and is normally activated in response to atrial stretch receptors. Data from adult patients with heart failure suggest that infusions of nesiritide, a synthetic form of BNP, decreases atrial pressures and systemic vascular resistance, and improves cardiac output (83). Preliminary pediatric data are less convincing for improved cardiac output, although diuresis was enhanced (60). Lastly, glucocorticoids in the form of hydrocortisone have been shown to decrease the inotrope requirements in neonates and infants receiving high-dose catecholamines (>0.15 µg/kg/minute epinephrine) after congenital heart surgery (84). The mechanism of the effect is not clear, but may be due to increased expression of β receptors on myocytes. Inflammation after CPB may produce relative adrenal insufficiency and vasodilation that is partially reversed with additional steroids in the postoperative course. However, many of the patients studied did not have cortisol levels measured prior to glucocorticoid administration.
Extracorporeal Membrane Oxygenation
When all interventions to maximize oxygen delivery are performed but the patient remains in a low cardiac output state with metabolic acidosis and end organ dysfunction, mechanical circulatory support should be considered. The principal mode of mechanical circulatory support in the postoperative pediatric cardiac patient is venoarterial (cardiac) ECMO. The overall goal of ECMO is to provide myocardial rest that allows for recovery. The indications for cardiac ECMO are listed in Table 81.9. Ideally, the patient should be placed on ECMO before the development of severe end organ dysfunction or cardiac arrest. In the event of an unexpected cardiac arrest, a patient can be supported using a crystalloid-primed circuit following rapid arterial and venous cannulation. Survival to hospital discharge as high as 64% has been reported for such patients (85). Cannulation can be initiated via an open sternum with direct atrial and aortic cannulation when the patient fails to wean from CPB or suffers a postoperative cardiac arrest. Alternatively, the neck or groin vessels can be accessed if there is more time for cannulation.
The expected course of myocardial recovery after CPB is 3 to 5 days (86,87). If the patient is unable to wean from ECMO after this time, and there are no residual cardiac lesions to be corrected, the possibility of cardiac transplantation should be explored, since most patients cannot be supported with ECMO for longer than 2 to 4 weeks due to complications. Smaller ventricular assist devices are becoming available to bridge infants and young children to transplant when indicated (88). Patient populations with poor outcomes are those who fail to wean from CPB, those with cavopulmonary connections, and adult congenital patients (89,90). The results of cardiac ECMO for all indications through July 2006 as reported to the international registry of the Extracorporeal Life Support Organization (ELSO) were 60% survival through decannulation and 42% survival to discharge (89).
|
Table 81.9 Indications for Venoarterial Extracorporeal Membrane Oxygenation |
|
|
Support of the Myocardium after Cardiac Transplantation
Pediatric cardiac transplant recipients are a unique population in the postoperative period because both donor and recipient considerations are relevant to outcomes. Myocardial function of the donated heart will depend on donor factors including the circumstances leading to donor status, the level of vasoactive support preharvest, and the ischemic time. Recipient factors include preoperative pulmonary vascular resistance and its impact on donor right heart function, end organ function, and the overall condition of the patient. Patients with congenital heart disease often have pre-existing adhesions and variant anatomy that may complicate and lengthen transplant surgery. Because the transplanted heart is denervated and tends to be bradycardic in the immediate postoperative period, pacing wires should be placed to allow control of the heart rate. If pacing wires do not exist or do not capture, isoproterenol can be used as a chronotrope. This is less desirable because isoproterenol increases oxygen consumption and can cause arrhythmias and systemic hypotension at higher doses. All cardiac transplant patients should have both right and left heart atrial pressures monitored. In infants and young children, this will necessitate the placement of an intracardiac left atrial catheter. Monitoring both right and left heart filling pressures is critical in differentiating right heart failure caused by elevated PVR (only right atrial pressures elevated) from biventricular failure due to graft ischemia or acute rejection (both right and left atrial pressures elevated). Right heart failure is an important cause of morbidity and mortality after cardiac transplantation and should be treated aggressively (see next section) (91).
Pulmonary Hypertension and Right Heart Failure
Primary right heart failure and pulmonary hypertension leading to secondary right heart failure are significant causes of morbidity in postoperative pediatric cardiac patients. Primary right heart failure should be anticipated in patients undergoing right ventriculotomies for right ventricular outflow tract reconstruction (e.g., tetralogy of Fallot repair) or conduit placement (e.g., truncus arteriosus repair). Those at risk for pulmonary hypertension and secondary right heart failure include patients with pulmonary venous or pulmonary arterial obstruction, heart transplant recipients with elevated PVR from preoperative left atrial hypertension, and patients with preoperative pulmonary hypertension from large left-to-right shunts (16). Anticipatory postoperative care and early recognition of right ventricular dysfunction will optimize recovery.
Patients who are expected to have a reactive pulmonary vascular bed should have a transthoracic pulmonary artery or right ventricular catheter placed intraoperatively for monitoring in the ICU. In the absence of direct measurement of pulmonary artery pressures, signs of pulmonary hypertension include elevated right-sided filling pressures with normal or low left-sided filling pressures and tachycardia. Patients with right-to-left shunts can become more cyanotic. As the right heart fails, physical exam will reveal poor perfusion, hepatomegaly, and possibly a loud tricuspid regurgitation murmur. In a pulmonary hypertensive crisis, signs of poor left heart filling occur and include systemic hypotension and bradycardia. In the immediate postoperative period, a patient with pulmonary hypertension should be evaluated for residual anatomic problems. Residual pulmonary venous obstruction, pulmonary artery stenosis, or significant left-to-right shunts can all cause pulmonary hypertension and may not be responsive to medical therapies.
Patients who undergo an extensive right ventriculotomy or who are anticipated to have pulmonary hypertension can benefit from an intraoperative strategy that allows right-to-left shunting at the atrial level. Typically, these are patients with tetralogy of Fallot or truncus arteriosus who have hypertrophied and noncompliant right ventricles. With an incision as part of the repair, the right ventricle may develop both systolic and diastolic dysfunction (92). If a transannular patch across the right ventricular outflow tract is required to relieve obstruction, pulmonary regurgitation creates a volume load on the struggling right ventricle as well. It is helpful to leave the foramen ovale patent, or even to create a new atrial level communication, to allow the right ventricle to decompress with a right-to-left shunt. In this physiology, systemic cardiac output will be preserved at the expense of mild cyanosis, which is usually well tolerated and transient (93).
Postoperative care should focus on minimizing the reactivity of the pulmonary vascular bed. The post-CPB inflammatory response, pulmonary arterial endothelial dysfunction, and alveolar hypoxia from edema and atelectasis all contribute to pulmonary hypertension (16). These should be time-limited processes as the patient recovers. The strategies for medical treatments are outlined in Table 81.10. The initial approach is to minimize the factors that increase PVR. Acidosis, agitation, and hypoxia all increase PVR and can provoke a pulmonary hypertensive crisis. Therefore, patients with pulmonary hypertension should be pain free, deeply sedated, and possibly paralyzed. They should be maintained with a mild alkalosis using either mild hyperventilation or sodium bicarbonate administration. Oxygen is a pulmonary vasodilator, so patients should receive supplemental oxygen and not be weaned to room air even if the arterial oxygen saturation is normal. Patients not responding to these initial maneuvers should be treated with vasodilators.
|
Table 81.10 Treatment of postoperative pulmonary hypertension |
|
|
Nitric oxide (NO) is a selective pulmonary vasodilator when inhaled. It crosses the alveolar wall where it acts on vascular smooth muscle by increasing levels of cyclic guanosine monophosphate (cGMP) to cause relaxation. It is usually delivered via a tracheal tube but can also be delivered via a face mask or nasal cannula. A reduction in pulmonary artery pressure is usually seen at doses of up to 40 parts per million; higher doses may increase toxicity (from methemoglobinemia) without any additional reduction in the pulmonary pressure (94). The uses of inhaled nitric oxide (iNO) in the treatment of pulmonary hypertension after congenital heart surgery are extensive (95,96). Its selective pulmonary vasodilation occurs without significant systemic hemodynamic effects, which is desirable in tenuous postoperative patients. The most responsive patients appear to be those who have relief of pulmonary venous obstruction such as with repair of obstructed total anomalous pulmonary venous return or congenital mitral stenosis (97). iNO is also an ideal agent to prevent right ventricular failure in a transplanted heart not accustomed to elevated PVR (91,98).
After the patient's pulmonary artery pressures have normalized and diuresis has been achieved, iNO can be slowly weaned off. If the dose of iNO is decreased too rapidly (e.g., dose lowered at intervals <4 to 6 hours), and especially below doses of 5 parts per million, pulmonary hypertension can recur. This is called “rebound” pulmonary hypertension (99). If the patient fails to wean off due to rebound, he or she can be transitioned to sildenafil (a phosphodiesterase type V inhibitor, which reduces the degradation of cGMP) to mitigate this phenomenon and as a transition to oral therapy (100,101). Caution should be used in administering iNO to patients with pulmonary hypertension caused by severe left ventricular dysfunction. Pulmonary vasodilation can increase pulmonary blood flow and left atrial pressures, which may volume overload the left ventricle, causing further dysfunction (102).
Intravenous vasodilators are not selective for the pulmonary vasculature, but some agents still have a role in treating pulmonary hypertension and right ventricular dysfunction. Milrinone (a phosphodiesterase type III inhibitor) is used to afterload reduce the right ventricle and provide inotropic support and diastolic relaxation. Prostaglandin derivatives such as prostacyclin, delivered either nebulized or as an intravenous infusion, can be beneficial but are dose limited by their systemic vasodilatory side effects. Prostacyclin is now commonly prescribed as a long-term outpatient therapy for pulmonary hypertension associated with congenital heart disease in children (103). Given the extensive literature supporting the benefits of iNO, the nonspecific vasodilators such as nitroprusside, tolazoline (an α-receptor agonist), and isoproterenol should be used infrequently for the treatment of postoperative pulmonary hypertension (104). Oral therapies for adults with chronic primary pulmonary hypertension, including calcium channel blockers and endothelin receptor blockers, have not been adequately studied in children in the postoperative setting, but may have a future role.
Single-ventricle Physiology
Patients with single-ventricle physiology are among the most challenging to care for in the pediatric cardiac intensive care unit. There are many variations of single-ventricle anatomy, but the defects can be broadly divided into those with a single left ventricle and obstruction to pulmonary blood flow, such as tricuspid or pulmonary atresia, and those with a single right ventricle and obstruction to systemic blood flow, such as HLHS. Most neonates with single-ventricle anatomy require prostaglandin E1 to maintain adequate pulmonary or systemic blood flow via the ductus arteriosus. The single ventricle's output occurs in parallel to the lungs and body, rather than in series as in normal (two-ventricle) physiology. The output to the systemic and pulmonary circulations is dependent on the vascular resistance in each circulation. The single ventricle's workload is the sum of the outputs to these two circulations, so that the single ventricle does the work of two ventricles. During the postnatal transition, PVR falls rapidly, so these patients often develop excessive pulmonary blood flow and compromised systemic flow within a few days of birth. This is commonly referred to as pulmonary overcirculation.
Most neonates with single-ventricle anatomy will need a palliative operation. This will be either an aortopulmonary shunt when pulmonary flow is obstructed or a stage I (Norwood) operation with aortic arch reconstruction and an aortopulmonary shunt or right ventricle–pulmonary artery conduit when systemic flow is obstructed. Occasionally, a single-ventricle patient will have unobstructed pulmonary and systemic blood flow through two well-developed outflow tracts. These patients usually require a pulmonary artery band shortly after birth to limit pulmonary blood flow as their first-stage palliation.
Shunted Single-ventricle Physiology
Irrespective of whether a stage I palliation, aortopulmonary shunt alone, or pulmonary artery band is the first palliative operation, the principles of balancing the systemic and pulmonary circulations are the same in the postoperative period. The operation does not alter the basic physiology of parallel circulations. An acceptable balance of pulmonary-to-systemic blood flow can be defined as sufficient pulmonary blood flow to provide adequate systemic oxygenation without pulmonary overcirculation. The newer modification of the stage I palliation that includes a right ventricle–to–pulmonary artery conduit is less likely to create overcirculation compared to an aortopulmonary shunt, since pulmonary blood flow occurs only in systole (105). However, depending on the size of the patient and the conduit, overcirculation from a right ventricle–to–pulmonary artery conduit can still occur. Assuming normal pulmonary venous saturations of 100% and normal oxygen extraction with a mixed venous saturation of 60%, a systemic and pulmonary artery saturation of 80% would result in a pulmonary blood flow (Qp)–to–systemic blood flow (Qs) ratio of 1:1, which represents balanced circulations (106). This would correlate with an arterial PaO2 of approximately 40 mm Hg. Typically, the Qp:Qs ratio is higher than this, and as it progresses toward 2:1, the single ventricle becomes volume overloaded. A Qp:Qs ratio of greater than 2:1 may be associated with low systemic output, hypotension, and acidosis.
The ability to monitor Qp:Qs accurately at the bedside is limited. Arterial saturations and mixed venous saturations (using superior vena caval saturation as a representative value) can be measured, but pulmonary venous saturations are assumed (107). Since the degree of postoperative lung disease is highly variable, assuming that pulmonary venous saturations are normal can erroneously underestimate pulmonary blood flow and the degree of overcirculation in patients with low systemic oxygen saturations (108). In patients with complete cardiac mixing, high systemic saturations are likely to represent pulmonary overcirculation. A patient with high systemic saturations (>90%) and high arterial PaO2 (>50 mm Hg) with low blood pressure and metabolic acidosis should be treated for pulmonary overcirculation.
Strategies to treat pulmonary overcirculation focus on increasing PVR and decreasing pulmonary blood flow. Transfusing the patient to a hematocrit of 45% to 50% will increase blood viscosity and PVR. Minimizing inspired oxygen to a room air level and/or even lower (e.g., FIO2 of 17%–19%) with the addition of nitrogen also increases PVR. Allowing the PaCO2 to rise (e.g., to 45–50 mm Hg with a pH <7.34) with hypoventilation or by the addition of carbon dioxide to the ventilator circuit has a similar effect (7). A cross-over trial comparing hypoxic gas mixtures to inhaled carbon dioxide in preoperative neonates with HLHS for increasing PVR was performed (109). Both methods increased the resistance and decreased the pulmonary blood flow, but carbon dioxide administration increased oxygen delivery to the brain as measured by increased mixed venous saturations in the superior vena cava and decreased arteriovenous saturation difference. In addition, high systemic vascular resistance should be avoided, as it increases pulmonary blood flow and the afterload on the single ventricle (110). High upper extremity blood pressures and oxygen saturations should raise the suspicion of residual coarctation of the aorta in single-ventricle patients and aortic arch obstruction. Large-dose catecholamines should be avoided, and afterload reduction with milrinone should be optimized. If a patient remains in a low cardiac output state despite ventilatory and pharmacologic strategies to limit pulmonary blood flow, surgical options such as narrowing the pulmonary conduit or aortopulmonary shunt with clips should be considered.
Excessive cyanosis is less common after patients are palliated with an aortopulmonary shunt, but it does occur. Possible etiologies include lung disease, elevated PVR, obstruction to pulmonary blood flow, and low mixed venous saturation from increased oxygen consumption or low cardiac output. Lung disease should be detectible by chest radiograph, and interventions can be performed in an effort to improve gas exchange. Elevated PVR is less common but may be seen in a patient with HLHS who has an intact or highly restrictive atrial septum and pulmonary venous hypertension before surgery (111). Despite decompression of atrial hypertension by opening the atrial septum, PVR can remain elevated postoperatively; it may respond to a brief course of iNO, similar to other patients who undergo relief of left atrial hypertension (16). The mortality rate of patients with HLHS and intact atrial septum is high despite strategies for emergent decompression and operation (112). When a shunt-dependent postoperative patient suddenly develops oxygen desaturation and bradycardia, it should raise the suspicion of acute shunt thrombosis. These patients need emergent cannulation for ECMO and shunt revision. Many patients with shunted single-ventricle physiology have labile hemodynamics for the first several postoperative hours to days. Delayed sternal closure is an accepted strategy that provides rapid access for additional procedures such as clipping of the shunt and emergent ECMO cannulation, if needed (6).
Cavopulmonary Connections
The transition to a superior vena cava–to–pulmonary artery connection, which is called a bidirectional Glenn shunt (BDG), is typically performed when a single-ventricle patient is 3 to 6 months old. The BDG is the first of a two-stage conversion to a total cavopulmonary circulation with separation of pulmonary and systemic blood flow (Fontan circulation). The advantage of a BDG is a reduced volume load and work for the single ventricle. The patient usually undergoes a cardiac catheterization to assess the pulmonary artery anatomy and measure PVR prior to the BDG. A PVR of less than approximately 3 to 4 Woods units is considered optimal. This operation is usually well tolerated by patients. It is common to observe systemic hypertension after the BDG; this may be secondary to intracranial hypertension from elevated superior vena cava pressures. Patients are often irritable in the first postoperative days, perhaps due to headache. Mild hypertension should be tolerated, as this preserves cerebral blood flow during the transition to passive pulmonary blood flow through the BDG. Systemic hypertension associated with bleeding or marked hypertension (>120 mm Hg systolic blood pressure) should be treated.
Cyanosis associated with elevated superior vena cava pressure occasionally occurs after BDG. If there is a low transpulmonary gradient with elevated atrial pressures, ventricular function should be optimized with inotropes. If the atrial pressures are low and the transpulmonary gradient is greater than 10 mm Hg, this suggests either anatomic obstruction to pulmonary blood flow or elevated PVR. The role of carbon dioxide and its effects on PVR and pulmonary blood flow is complex in BDG patients. Modest hypoventilation with elevated carbon dioxide increases arterial PaO2, presumably by increasing pulmonary blood flow via greater cerebral blood flow from cerebral autoregulation (113). The vasodilatory role of carbon dioxide in the brain predominates over any increase in PVR from hypoventilation and lower blood pH (114). The data for use of nitric oxide in these patients are mixed. In one study it appeared to lower superior vena cava pressures and improve oxygenation (115). However, in another study, it had no impact on oxygenation (116). Positive pressure ventilation and increased intrathoracic pressures may play a role in limiting passive pulmonary blood flow, so early extubation is advocated (117). A superior vena cava pressure of >20 mm Hg that is unresponsive to medical therapies is concerning for the successful transition to BDG physiology. Postoperative cardiac catheterization to assess for reversible causes and consideration of possible takedown of the BDG should be pursued.
The final stage in the single-ventricle palliation is the completion of the cavopulmonary connection with a Fontan operation. This can be performed with either a lateral tunnel baffle through the common atrium or an extracardiac conduit, usually when the patient is 2 to 3 years old and weighs 10 to 15 kg. Patients again undergo a preoperative cardiac catheterization to assess pulmonary artery anatomy and PVR. It is common at this catheterization to discover both aortopulmonary collaterals and decompressing venovenous collaterals from systemic to pulmonary veins. Large aortopulmonary collaterals are typically eliminated (by coil embolization) to lower pulmonary artery pressure, and venovenous collaterals are occluded to increase pulmonary blood flow from systemic veins into the pulmonary arteries (118,119). Postoperative concerns after a Fontan are usually focused on PVR and cardiac output. An ideal Fontan baffle pressure is 10 to 15 mm Hg with a transpulmonary gradient of <10 mm Hg. A Fontan baffle pressure >20 mm Hg is worrisome. Elevated Fontan baffle and atrial pressures indicate low cardiac output or tamponade physiology. An elevated Fontan baffle pressure with a low atrial pressure indicates either high PVR or obstruction in the Fontan pathway; these patients should be promptly investigated and treated. Low Fontan baffle and atrial pressures indicate inadequate intravascular volume status (106). The passive pulmonary blood flow of the Fontan circulation is preload dependent, so hypovolemia will quickly lead to low cardiac output and hypotension. Patients undergoing Fontan operations often have sinus node dysfunction with junctional rhythm. AV synchrony should be preserved with mechanical pacing to maximize cardiac output. Surgical fenestration of the Fontan baffle has a positive impact on the early recovery Fontan patients. In the immediate postoperative hours, the fenestration allows for a right-to-left shunt. This shunt decompresses the Fontan baffle and causes mild oxygen desaturation; however, it preserves cardiac output by increasing preload to the ventricle. The PVR is transiently elevated due to the inflammatory response after CPB. The Fontan circulation is highly sensitive to elevations in PVR, so acidosis, alveolar hypoxia, and atelectasis should be avoided. As the patient diureses and is extubated from positive pressure ventilation, PVR decreases and the arterial oxygen saturation improves as less blood is shunted right to left. The duration of pleural effusions, which are common after the Fontan operation, is also reduced by the fenestration (120). The fenestration may be electively closed with an occluder device during cardiac catheterization at a later time with good intermediate functional outcomes (121).
Pediatric cardiac surgery patients can be challenging. With specialized care, vigilant monitoring, and good communication between teams, outcomes may be rewarding.
References
1. Jonas RA. Comprehensive Surgical Management of Congenital Heart Disease. New York: Oxford University Press; 2004:3–10.
2. Tweddell JS, Spray TL. Newborn heart surgery: reasonable expectations and outcomes. Pediatr Clin North Am. 2004;51(6):1611–1623, ix.
3. Wernovsky G, Rubenstein SD, Spray TL. Cardiac surgery in the low-birth weight neonate. New approaches. Clin Perinatol. 2001;28(1):249–264.
4. Curran RD, et al. Inhaled nitric oxide for children with congenital heart disease and pulmonary hypertension. Ann Thorac Surg. 1995;60(6):1765–1771.
5. Wessel DL. Inhaled nitric oxide for the treatment of pulmonary hypertension before and after cardiopulmonary bypass. Crit Care Med. 1993;21(9 Suppl):S344–345.
6. Tabbutt S, et al. Delayed sternal closure after cardiac operations in a pediatric population. J Thorac Cardiovasc Surg. 1997;113(5):886–893.
7. Chang AC, et al. Pulmonary vascular resistance in infants after cardiac surgery: role of carbon dioxide and hydrogen ion. Crit Care Med. 1995;23(3):568–574.
P.1235
8. Charpie JR, et al. Serial blood lactate measurements predict early outcome after neonatal repair or palliation for complex congenital heart disease. J Thorac Cardiovasc Surg. 2000;120(1):73–80.
9. Munoz R, et al. Changes in whole blood lactate levels during cardiopulmonary bypass for surgery for congenital cardiac disease: an early indicator of morbidity and mortality. J Thorac Cardiovasc Surg. 2000;119(1):155–162.
10. Jonas RA. Comprehensive Surgical Management of Congenital Heart Disease. New York: Oxford University Press; 2004:61–62.
11. Dominguez TE, et al. Use of recombinant factor VIIa for refractory hemorrhage during extracorporeal membrane oxygenation. Pediatr Crit Care Med. 2005;6(3):348–351.
12. Marianeschi SM, et al. Fast-track congenital heart operations: a less invasive technique and early extubation. Ann Thorac Surg. 2000;69(3):872–876.
13. Flori HR, et al. Transthoracic intracardiac catheters in pediatric patients recovering from congenital heart defect surgery: associated complications and outcomes. Crit Care Med. 2000;28(8):2997–3001.
14. Gold JP, et al. Transthoracic intracardiac monitoring lines in pediatric surgical patients: a ten-year experience. Ann Thorac Surg. 1986;42(2):185–191.
15. Lock JE. Hemodynamic evaluation of congenital heart disease. In: Lock JE, Keane JF, Perry SB, eds. Diagnostic and Interventional Catheterization in Congenital Heart Disease. 2nd ed. Boston: Kluwer Academic Publishers; 2000:37–72.
16. Wessel DL. Current and future strategies in the treatment of childhood pulmonary hypertension. Prog Pediatr Cardiol. 2001;12(3):289–318.
17. Barratt-Boyes BG, Wood EH. The oxygen saturation of blood in the venae cavae, right-heart chambers, and pulmonary vessels of healthy subjects. J Lab Clin Med. 1957;50(1):93–106.
18. Lang P, et al. Early assessment of hemodynamic status after repair of tetralogy of Fallot: a comparison of 24 hour (intensive care unit) and 1 year postoperative data in 98 patients. Am J Cardiol. 1982;50(4):795–799.
19. Lan YT, Lee JC, Wetzel G. Postoperative arrhythmia. Curr Opin Cardiol. 2003;18(2):73–78.
20. Weindling SN, et al. Duration of complete atrioventricular block after congenital heart disease surgery. Am J Cardiol. 1998;82(4):525–527.
21. Rosales AM, et al. Postoperative ectopic atrial tachycardia in children with congenital heart disease. Am J Cardiol. 2001;88(10):1169–1172.
22. Saul JP, et al. Intravenous amiodarone for incessant tachyarrhythmias in children: a randomized, double-blind, antiarrhythmic drug trial. Circulation. 2005;112(22):3470–3477.
23. Walsh EP, et al. Evaluation of a staged treatment protocol for rapid automatic junctional tachycardia after operation for congenital heart disease. J Am Coll Cardiol. 1997;29(5):1046–1053.
24. Perry JC, et al. Pediatric use of intravenous amiodarone: efficacy and safety in critically ill patients from a multicenter protocol. J Am Coll Cardiol. 1996;27(5):1246–1250.
25. Shekerdemian L, Bohn D. Cardiovascular effects of mechanical ventilation. Arch Dis Child. 1999;80(5):475–480.
26. Penny DJ, Hayek Z, Redington AN. The effects of positive and negative extrathoracic pressure ventilation on pulmonary blood flow after the total cavopulmonary shunt procedure. Int J Cardiol. 1991;30(1):128–130.
27. Shekerdemian LS, et al. Cardiopulmonary interactions after Fontan operations: augmentation of cardiac output using negative pressure ventilation. Circulation. 1997;96(11):3934–3942.
28. Pinsky MR, et al. Augmentation of cardiac function by elevation of intrathoracic pressure. J Appl Physiol. 1983;54(4):950–955.
29. Grace MP, Greenbaum DM. Cardiac performance in response to PEEP in patients with cardiac dysfunction. Crit Care Med. 1982;10(6):358–360.
30. Arnold JH, et al. High-frequency oscillatory ventilation in pediatric respiratory failure: a multicenter experience. Crit Care Med. 2000;28(12):3913–3919.
31. Courtney SE, et al. High-frequency oscillatory ventilation versus conventional mechanical ventilation for very-low-birth-weight infants. N Engl J Med. 2002;347(9):643–652.
32. Gullberg N, Winberg P, Sellden H. Changes in mean airway pressure during HFOV influences cardiac output in neonates and infants. Acta Anaesthesiol Scand. 2004;48(2):218–223.
33. Simma B, et al. Conventional ventilation versus high-frequency oscillation: hemodynamic effects in newborn babies. Crit Care Med. 2000;28(1):227–231.
34. Khariwala SS, Lee WT, Koltai PJ. Laryngotracheal consequences of pediatric cardiac surgery. Arch Otolaryngol Head Neck Surg. 2005;131(4):336–339.
35. Miller SG, Brook MM, Tacy TA. Reliability of two-dimensional echocardiography in the assessment of clinically significant abnormal hemidiaphragm motion in pediatric cardiothoracic patients: comparison with fluoroscopy. Pediatr Crit Care Med. 2006;7(5):441–444.
36. Joho-Arreola AL, et al. Incidence and treatment of diaphragmatic paralysis after cardiac surgery in children. Eur J Cardiothorac Surg. 2005;27(1):53–57.
37. Midelton GT, Frishman WH, Passo SS. Congestive heart failure and continuous positive airway pressure therapy: support of a new modality for improving the prognosis and survival of patients with advanced congestive heart failure. Heart Dis. 2002;4(2):102–109.
38. Anand KJ, Hansen DD, Hickey PR, Hormonal-metabolic stress responses in neonates undergoing cardiac surgery. Anesthesiology. 1990;73(4):661–670.
39. Anand KJ, Hickey PR. Halothane-morphine compared with high-dose sufentanil for anesthesia and postoperative analgesia in neonatal cardiac surgery. N Engl J Med. 1992;326(1):1–9.
40. Hickey PR, et al. Pulmonary and systemic hemodynamic responses to fentanyl in infants. Anesth Analg. 1985;64(5):483–486.
41. Hickey PR, et al. Blunting of stress responses in the pulmonary circulation of infants by fentanyl. Anesth Analg. 1985;64(12):1137–1142.
42. Muller P, Vogtmann C. Three cases with different presentation of fentanyl-induced muscle rigidity—a rare problem in intensive care of neonates. Am J Perinatol. 2000;17(1):23–26.
43. Fahnenstich H, et al. Fentanyl-induced chest wall rigidity and laryngospasm in preterm and term infants. Crit Care Med. 2000;28(3):836–839.
44. McKeage K, Perry CM. Propofol: a review of its use in intensive care sedation of adults. CNS Drugs. 2003;17(4):235–272.
45. Bray RJ. Propofol infusion syndrome in children. Paediatr Anaesth. 1998;8(6):491–499.
46. Tobias JD, Berkenbosch JW. Initial experience with dexmedetomidine in paediatric-aged patients. Paediatr Anaesth. 2002;12(2):171–175.
47. Chrysostomou C, et al. Use of dexmedetomidine in children after cardiac and thoracic surgery. Pediatr Crit Care Med. 2006;7(2):126–131.
48. Berkenbosch JW, Tobias JD. Development of bradycardia during sedation with dexmedetomidine in an infant concurrently receiving digoxin. Pediatr Crit Care Med. 2003;4(2):203–205.
49. Helmers SL, et al. Perioperative electroencephalographic seizures in infants undergoing repair of complex congenital cardiac defects. Electroencephalogr Clin Neurophysiol. 1997;102(1):27–36.
50. Gaynor JW, et al. Increasing duration of deep hypothermic circulatory arrest is associated with an increased incidence of postoperative electroencephalographic seizures. J Thorac Cardiovasc Surg. 2005;130(5):1278–1286.
51. Mahle WT, et al. An MRI study of neurological injury before and after congenital heart surgery. Circulation. 2002;106(12 Suppl 1):I109–114.
52. Gaynor JW, et al. The relationship of postoperative electrographic seizures to neurodevelopmental outcome at 1 year of age after neonatal and infant cardiac surgery. J Thorac Cardiovasc Surg. 2006;131(1):181–189.
53. Austin EH 3rd, et al. Benefit of neurophysiologic monitoring for pediatric cardiac surgery. J Thorac Cardiovasc Surg. 1997;114(5):707–715, 717; discussion 715–716.
54. Dent CL, et al. Brain magnetic resonance imaging abnormalities after the Norwood procedure using regional cerebral perfusion. J Thorac Cardiovasc Surg. 2005;130(6):1523–1530.
55. Gaynor JW. The effect of modified ultrafiltration on the postoperative course in patients with congenital heart disease. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2003;6:128–139.
56. Russell JA, Navickis RJ, Wilkes MM. Albumin versus crystalloid for pump priming in cardiac surgery: meta-analysis of controlled trials. J Cardiothorac Vasc Anesth. 2004;18(4):429–437.
57. Langer GA. Role of sarcolemmal-bound calcium in regulation of myocardial contractile force. J Am Coll Cardiol. 1986;8(1 Suppl A):65A–68A.
58. Singh NC, et al. Comparison of continuous versus intermittent furosemide administration in postoperative pediatric cardiac patients. Crit Care Med. 1992;20(1):17–21.
59. Costello JM, et al. Fenoldapam after pediatric cardiac surgery: what is conventional diuretic therapy? Pediatr Crit Care Med. 2006;7(4):399– 400.
60. Mahle WT, et al. Nesiritide in infants and children with congestive heart failure. Pediatr Crit Care Med. 2005;6(5):543–546.
61. Fleming F, et al. Renal replacement therapy after repair of congenital heart disease in children. A comparison of hemofiltration and peritoneal dialysis. J Thorac Cardiovasc Surg. 1995;109(2):322–331.
62. Giuffre RM, et al. Acute renal failure complicating pediatric cardiac surgery: a comparison of survivors and nonsurvivors following acute peritoneal dialysis. Pediatr Cardiol. 1992;13(4):208–213.
63. Shaw NJ, et al. Long-term outcome for children with acute renal failure following cardiac surgery. Int J Cardiol. 1991;31(2):161–165.
64. McElhinney DB, et al. Necrotizing enterocolitis in neonates with congenital heart disease: risk factors and outcomes. Pediatrics. 2000;106(5):1080–1087.
65. Stover BH, et al. Nosocomial infection rates in US children's hospitals' neonatal and pediatric intensive care units. Am J Infect Control. 2001;29(3):152–157.
66. Slonim AD, et al. The costs associated with nosocomial bloodstream infections in the pediatric intensive care unit. Pediatr Crit Care Med. 2001;2(2):170–174.
67. Huddleston CB. Mediastinal wound infections following pediatric cardiac surgery. Semin Thorac Cardiovasc Surg. 2004;16(1):108–112.
68. Tortoriello TA, et al. Mediastinitis after pediatric cardiac surgery: a 15-year experience at a single institution. Ann Thorac Surg. 2003;76(5):1655–1660.
69. Wessel DL. Managing low cardiac output syndrome after congenital heart surgery. Crit Care Med. 2001;29(10 Suppl):S220–230.
70. Wernovsky G, et al. Postoperative course and hemodynamic profile after the arterial switch operation in neonates and infants. A comparison of low-flow cardiopulmonary bypass and circulatory arrest. Circulation. 1995;92(8):2226–2235.
71. Booth KL, et al. Cardiac catheterization of patients supported by extracorporeal membrane oxygenation. J Am Coll Cardiol. 2002;40(9):1681–1686.
72. Zahn EM, et al. Interventional catheterization performed in the early postoperative period after congenital heart surgery in children. J Am Coll Cardiol. 2004;43(7):1264–1269.
73. Dunser MW, et al. Cardiac performance during vasopressin infusion in postcardiotomy shock. Intensive Care Med. 2002;28(6):746–751.
74. Rosenzweig EB, et al. Intravenous arginine-vasopressin in children with vasodilatory shock after cardiac surgery. Circulation. 1999;100(19 Suppl):II182–186.
75. Rozenfeld V, Cheng JW. The role of vasopressin in the treatment of vasodilation in shock states. Ann Pharmacother. 2000;34(2):250–254.
76. Caspi J, et al. Age-related response to epinephrine-induced myocardial stress. A functional and ultrastructural study. Circulation. 1991;84(5 Suppl):III394–399.
77. Young RA, Ward A. Milrinone. A preliminary review of its pharmacological properties and therapeutic use. Drugs. 1988;36(2):158–192.
78. Chang AC, et al. Milrinone: systemic and pulmonary hemodynamic effects in neonates after cardiac surgery. Crit Care Med. 1995;23(11):1907–1914.
79. Hoffman TM, et al. Efficacy and safety of milrinone in preventing low cardiac output syndrome in infants and children after corrective surgery for congenital heart disease. Circulation. 2003;107(7):996–1002.
80. Bettendorf M, et al. Tri-iodothyronine treatment in children after cardiac surgery: a double-blind, randomised, placebo-controlled study. Lancet. 2000;356(9229):529–534.
81. Chowdhury D, et al. Usefulness of triiodothyronine (T3) treatment after surgery for complex congenital heart disease in infants and children. Am J Cardiol. 1999;84(9):1107–1109, A10.
82. Mackie AS, et al. A randomized, double-blind, placebo-controlled pilot trial of triiodothyronine in neonatal heart surgery. J Thorac Cardiovasc Surg. 2005;130(3):810–816.
83. Mills RM, et al. Sustained hemodynamic effects of an infusion of nesiritide (human b-type natriuretic peptide) in heart failure: a randomized, double-blind, placebo-controlled clinical trial. Natrecor Study Group. J Am Coll Cardiol. 1999;34(1):155–162.
84. Shore S, et al. Usefulness of corticosteroid therapy in decreasing epinephrine requirements in critically ill infants with congenital heart disease. Am J Cardiol. 2001;88(5):591–594.
85. Duncan BW, et al. Use of rapid-deployment extracorporeal membrane oxygenation for the resuscitation of pediatric patients with heart disease after cardiac arrest. J Thorac Cardiovasc Surg. 1998;116(2):305–311.
86. Black MD, et al. Determinants of success in pediatric cardiac patients undergoing extracorporeal membrane oxygenation. Ann Thorac Surg. 1995;60(1):133–138.
87. Duncan BW, et al. Mechanical circulatory support in children with cardiac disease. J Thorac Cardiovasc Surg. 1999;117(3):529–542.
88. Hetzer R, et al. Mechanical cardiac support in the young with the Berlin Heart EXCOR pulsatile ventricular assist device: 15 years' experience. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2006:99–108.
89. ECLS Registry Report. Ann Arbor, MI: Extracorporeal Life Support Organization.
90. Booth KL, et al. Extracorporeal membrane oxygenation support of the Fontan and bidirectional Glenn circulations. Ann Thorac Surg. 2004;77(4):1341–1348.
91. Stobierska-Dzierzek B, Awad H, Michler RE. The evolving management of acute right-sided heart failure in cardiac transplant recipients. J Am Coll Cardiol. 2001;38(4):923–931.
92. Cullen S, Shore D, Redington A. Characterization of right ventricular diastolic performance after complete repair of tetralogy of Fallot. Restrictive physiology predicts slow postoperative recovery. Circulation. 1995;91(6):1782–1789.
93. Laudito A, et al. Complete repair of conotruncal defects with an interatrial communication: oxygenation, hemodynamic status, and early outcome. Ann Thorac Surg. 2006;82(4):1286–1291; discussion 1291.
94. Journois D, et al. Inhaled nitric oxide as a therapy for pulmonary hypertension after operations for congenital heart defects. J Thorac Cardiovasc Surg. 1994;107(4):1129–1135.
95. Adatia I, et al. Diagnostic use of inhaled nitric oxide after neonatal cardiac operations. J Thorac Cardiovasc Surg. 1996;112(5):1403–1405.
96. Russell IA, et al. The effects of inhaled nitric oxide on postoperative pulmonary hypertension in infants and children undergoing surgical repair of congenital heart disease. Anesth Analg. 1998;87(1):46–51.
97. Atz AM, et al. Inhaled nitric oxide in children with pulmonary hypertension and congenital mitral stenosis. Am J Cardiol. 1996;77(4):316–319.
98. Auler Junior JO, et al. Low doses of inhaled nitric oxide in heart transplant recipients. J Heart Lung Transplant. 1996;15(5):443–450.
99. Atz AM, Adatia I, Wessel DL. Rebound pulmonary hypertension after inhalation of nitric oxide. Ann Thorac Surg. 1996;62(6):1759–1764.
100. Atz AM, Wessel DL. Sildenafil ameliorates effects of inhaled nitric oxide withdrawal. Anesthesiology. 1999;91(1):307–310.
101. Knoderer CA, Ebenroth ES, Brown JW. Chronic outpatient sildenafil therapy for pulmonary hypertension in a child after cardiac surgery. Pediatr Cardiol. 2005;26(6):859–861.
102. Loh E, et al. Cardiovascular effects of inhaled nitric oxide in patients with left ventricular dysfunction. Circulation. 1994;90(6):2780–275.
103. Rosenzweig EB, Kerstein D, Barst RJ. Long-term prostacyclin for pulmonary hypertension with associated congenital heart defects. Circulation. 1999;99(14):1858–1865.
104. Drummond WH, Lock JE. Neonatal ‘pulmonary vasodilator’ drugs. Current status. Dev Pharmacol Ther. 1984;7(1):1–20.
105. Cua CL, et al. Early postoperative outcomes in a series of infants with hypoplastic left heart syndrome undergoing stage I palliation operation with either modified Blalock-Taussig shunt or right ventricle to pulmonary artery conduit. Pediatr Crit Care Med. 2006;7(3):238–244.
106. Wernovsky G, Bove E. Single ventricle lesions. In: Chang AC, Hanley FL, Wernovsky G, et al., eds. Pediatric Cardiac Intensive Care. Baltimore: Williams & Wilkins; 1998:271–287.
107. Rossi AF, et al. Usefulness of intermittent monitoring of mixed venous oxygen saturation after stage I palliation for hypoplastic left heart syndrome. Am J Cardiol. 1994;73(15):1118–1123.
108. Taeed R, et al. Unrecognized pulmonary venous desaturation early after Norwood palliation confounds Gp:Gs assessment and compromises oxygen delivery. Circulation. 2001;103(22):2699–2704.
109. Tabbutt S, et al. Impact of inspired gas mixtures on preoperative infants with hypoplastic left heart syndrome during controlled ventilation. Circulation. 2001;104(12 Suppl 1):I159–164.
110. Wright GE, et al. High systemic vascular resistance and sudden cardiovascular collapse in recovering Norwood patients. Ann Thorac Surg. 2004;77(1):48–52.
111. Atz AM, et al. Preoperative management of pulmonary venous hypertension in hypoplastic left heart syndrome with restrictive atrial septal defect. Am J Cardiol. 1999;83(8):1224–1228.
112. Vlahos AP, et al. Hypoplastic left heart syndrome with intact or highly restrictive atrial septum: outcome after neonatal transcatheter atrial septostomy. Circulation. 2004;109(19):2326–2330.
113. Bradley SM, Simsic JM, Mulvihill DM. Hypoventilation improves oxygenation after bidirectional superior cavopulmonary connection. J Thorac Cardiovasc Surg. 2003;126(4):1033–1039.
114. Fogel MA, et al. Brain versus lung: hierarchy of feedback loops in single-ventricle patients with superior cavopulmonary connection. Circulation. 2004;110(11 Suppl 1):II147–152.
115. Agarwal HS, et al. Inhaled nitric oxide use in bidirectional Glenn anastomosis for elevated Glenn pressures. Ann Thorac Surg. 2006;81(4):1429– 1434.
116. Adatia I, Atz AM, Wessel DL. Inhaled nitric oxide does not improve systemic oxygenation after bidirectional superior cavopulmonary anastomosis. J Thorac Cardiovasc Surg. 2005;129(1):217–219.
117. Tabbutt S. Systemic oxygenation in patients with a bilateral cavopulmonary anastomosis. Pediatr Crit Care Med. 2006;7(4):396–397.
118. Spicer RL, et al. Aortopulmonary collateral vessels and prolonged pleural effusions after modified Fontan procedures. Am Heart J. 1996;131(6): 1164–1168.
119. Sugiyama H, et al. Characterization and treatment of systemic venous to pulmonary venous collaterals seen after the Fontan operation. Cardiol Young. 2003;13(5):424–430.
120. Bridges ND, et al. Effect of baffle fenestration on outcome of the modified Fontan operation. Circulation. 1992;86(6):1762–1769.
121. Goff DA, et al. Clinical outcome of fenestrated Fontan patients after closure: the first 10 years. Circulation. 2000;102(17):2094–2099.