David M. Levi
Joseph Ferreira
Andreas G. Tzakis
Immediate Concerns
Critical care and clinical organ transplantation have developed in parallel over the past several decades. While organ transplantation has emerged as the treatment of choice for an ever-growing number of patients with end-stage organ failure, the intensive care unit (ICU) has become the venue where much of this care is rendered. The modern intensivist plays an important role in the care of the critically ill patient awaiting transplant, the postoperative management of the transplant recipient, and the identification and management of the potential deceased organ donor.
The success of organ transplantation can be attributed to a number of factors. These include better patient selection and preoperative preparation, standardization of surgical techniques, advances in immunosuppression and graft surveillance, and improved postoperative care. This success, in part reflective of advances in critical care medicine, poses a great challenge to the skills of the intensivist and the resources of the ICU. The continuing shortage of organs available for transplantation translates into longer waiting times for recipients, during which their condition may further deteriorate. Additionally, organ allocation algorithms—especially heart, lung, liver, and intestine—in the United States emphasize the “sickest first” philosophy, which states that the highest priority for organs should go to those most in danger of imminent death. Finally, the shortage of organs has forced the transplant community to consider the use of organs from less than ideal donors. The organs from these marginal or “expanded criteria” donors (ECDs), while used with caution, must be considered in order to minimize deaths on the waiting list. The impact on the ICU is clear: more transplants are being performed on critically ill patients with an organ pool that now includes compromised organs.
A prerequisite to the success of organ transplantation is the availability of suitable organs. Deceased organ donors are, and will continue to be in the foreseeable future, our most important organ source. A crucial consideration of the ICU staff should be the timely recognition of the potential organ donor, both those who are brain dead and those for whom death is imminent, and the early involvement of organ procurement organization (OPO) personnel to facilitate the process. The assessment of the potential organ donor, a clear understanding of donation after brain death and cardiac death protocols, and donor management are skills of the intensivist that are fundamental to the organ procurement process and the subsequent transplants performed.
Transplant Activity, Results, and Trends
Organ procurement and transplantation are highly regulated endeavors governed in the United States by the federal Organ Procurement and Transplant Network (OPTN). The OPTN contract is managed by the United Network for Organ Sharing. Each OPO and transplant center (TC) collects and reports data regarding their activity and results. The Scientific Registry of Transplant Recipients (SRTR), administered by the Arbor Research Collaborative for Health with the University of Michigan, analyzes these data and continually evaluates the status of clinical organ transplantation in the United States. This comprehensive analysis is periodically updated and is available to the public through the SRTR Web site (www.ustransplant.org). Data and figures in this chapter regarding transplant activity, results, and trends are from the SRTR (1).
In 2002, in an effort to promote organ donation and procurement, and ultimately increase the number and quality of transplants performed, the U.S. Secretary of Health launched the Health Resources and Services Administration (HRSA) Organ Donation Breakthrough Collaborative. The goal of this nationwide endeavor was to identify the best operational and clinical practices of the most successful OPOs and share these “best practices” with the rest of the health care community. The result of these efforts has been the steady increase, in recent years, in the number of organ donors, the number of organs procured, and the number of transplants performed. As discussed below, the increasing quality of these transplants has manifested as better graft and patient survival.
Kidney
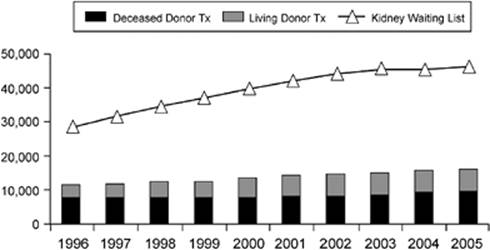
Over 46,000 patients were on the active waiting list for a kidney transplant in 2005. In that year, approximately 16,000 kidney transplants were performed. The total number of kidney transplants has gradually increased, as has the fraction of those kidneys transplanted with other organs. Living donor kidneys accounted for approximately 41% of those transplants, while the remainder of transplanted kidneys originated from deceased donors. Policy changes continue to refine deceased donor kidney allocation to better utilize this scarce resource. Additionally, novel living donor–recipient matching strategies have been developed that offer the prospect of some relief to this shortage (2). As shown in Figure 90.1, the disparity between the number of those waiting for a kidney and those transplanted continues to increase despite increases in both living and deceased organ donation over the past decade.
|
|
|
Figure 90.1. Number of kidney transplants and size of active waiting list per year. TX, transplant. (Source: 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1996–2005. Rockville, MD: Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation, Tables 1.7 and 5.1a. The data and analyses reported in the 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients have been supplied by UNOS and Arbor Research under contract with HHS. The authors alone are responsible for reporting and interpreting these data; the views expressed herein are those of the authors and not necessarily those of the U.S. Government.) |
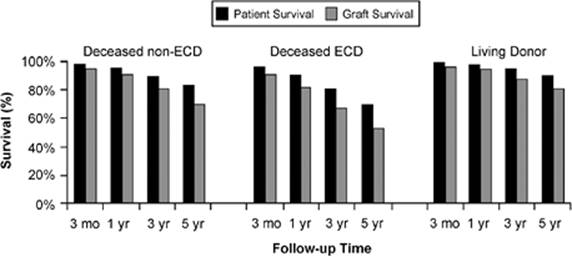
Kidney transplantation confers a clear survival advantage for patients with end-stage renal failure compared to long-term hemodialysis (3). For living donor kidney recipients, 5-year patient and graft survival are 90% and 80%, respectively (Fig. 90.2).
Pancreas
Pancreas transplantation offers selected diabetic patients the prospect of glucose control, avoiding—and, in some cases, reversing—the devastating complications of the disease. Most pancreata are transplanted simultaneously with a kidney (SPK), although a significant fraction is transplanted alone (PTA) or at some time after a kidney (PAK) transplant. Deceased donor pancreata remain a relatively underutilized organ resource; only 19% of available deceased donor pancreata are recovered and transplanted. A few percent are procured, processed, and transplanted as islet cell transplants. The reasons for this underutilization are multifactorial, and include regional variation in the number of potential recipients, donor and organ quality, and competition for kidneys with other patients.
|
|
|
Figure 90.2. Kidney transplant patient and graft survival by donor type. ECD, expanded criteria donor. (Source: 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1996–2005. Rockville, MD: Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation, Tables 5.10a, 5.10b, 5.10c, 5.14a, and 5.14b. The data and analyses reported in the 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients have been supplied by UNOS and Arbor Research under contract with HHS. The authors alone are responsible for reporting and interpreting these data; the views expressed herein are those of the authors and not necessarily those of the U.S. Government.) |
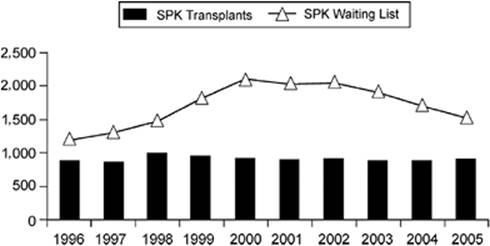
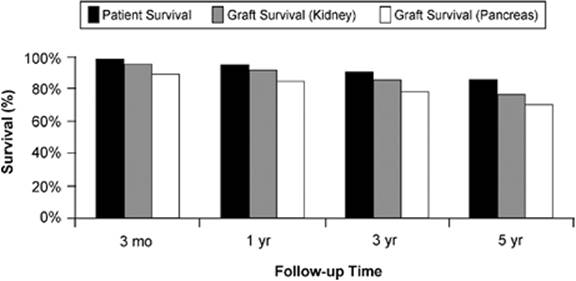
In 2005, 903 SPK transplants, 344 PAK transplants, and 195 PTA transplants were performed. These totals have changed little over the last several years. Figure 90.3 depicts the trend for SPK transplants over the past decade. Similarly, patient and graft survival has improved, with 5-year patient survival approaching 90% (Fig. 90.4).
Liver
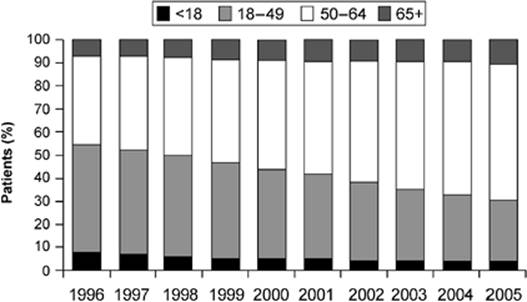
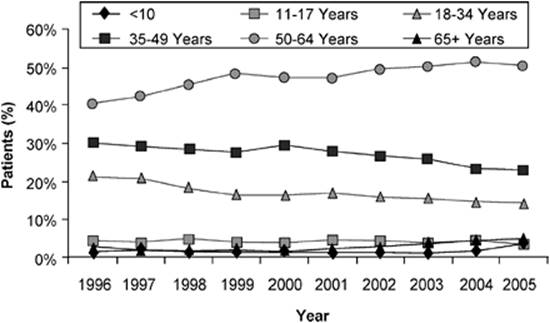
Liver transplantation remains the only therapy for end-stage, chronic liver disease and irreversible, fulminant liver failure. It is increasingly being performed for patients with localized, unresectable hepatocellular carcinoma with promising results (4). Since 2002, the number of patients waiting for liver transplantation has slowly increased to near 13,000. The age distribution of those waiting has changed more dramatically, with ages between 50 and 64 making up the majority (Fig. 90.5).
|
|
|
Figure 90.3. Number of simultaneous pancreas kidney transplants (SPK) and size of active waiting list per year. (Source: 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1996–2005. Rockville, MD: Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation, Tables 1.7 and 8.1a. The data and analyses reported in the 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients have been supplied by UNOS and Arbor Research under contract with HHS. The authors alone are responsible for reporting and interpreting these data; the views expressed herein are those of the authors and not necessarily those of the U.S. Government.) |
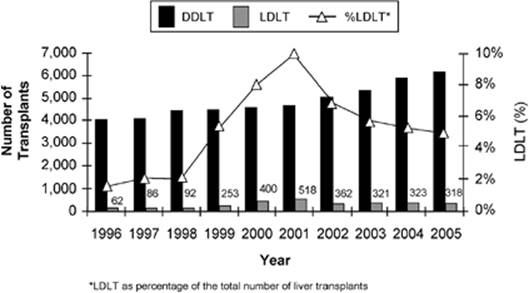
The total number of liver transplants performed has steadily increased over the past decade, with 6,441 transplants in 2005. This increase is due primarily to the increase in deceased donor livers available for transplant. Living donor liver transplantation (LDLT) accounted for 5% of liver transplants performed in 2005, down from a peak of 10% in 2001 (Fig. 90.6). This decrease may be due in part to the increased utilization of ECD livers and concerns about the morbidity and mortality risks associated with living donor liver transplantation.
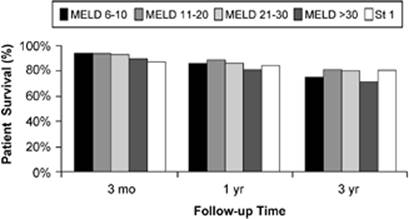
Liver allocation for adults depends primarily on disease severity as determined by the Model for End-Stage Liver Disease (MELD). The MELD formula uses easily obtained laboratory data—total bilirubin, serum creatinine, and international normalized ratio—and is highly predictive of death on the waiting list (5). Important exceptions are made for selected patients with hepatocellular carcinoma and other groups of patients for whom the MELD score does not reflect disease severity. Despite performing transplants in more older patients, utilizing more ECD livers, and employing an allocation system that gives priority to the sickest patients, the results of liver transplantation continue to be encouraging (Fig. 90.7).
|
|
|
Figure 90.4. Patient and graft survival for simultaneous pancreas kidney transplantation. (Source: 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1996–2005. Rockville, MD: Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation, Tables 8.10 and 8.14. The data and analyses reported in the 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients have been supplied by UNOS and Arbor Research under contract with HHS. The authors alone are responsible for reporting and interpreting these data; the views expressed herein are those of the authors and not necessarily those of the U.S. Government.) |
Heart
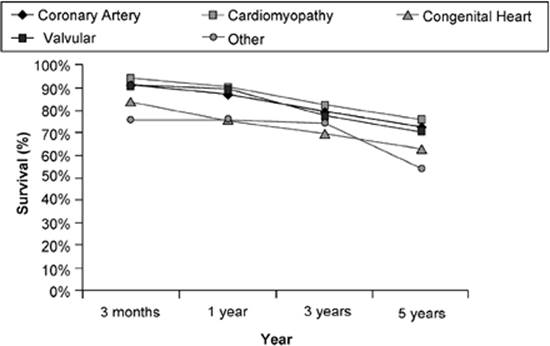
The number of patients on the waiting list for a heart and the number of transplants performed has decreased significantly over the past decade (Table 90.1). Over the same time, deaths on the waiting list have declined and survival results after heart transplantation remain high (Fig. 90.8). These data reflect the improvements in transplantation, better medical management of interventional techniques for patients with heart disease, and the development of more effective mechanical support devices.
Limitations to heart preservation require that geographic location be a significant factor in the heart allocation system. Also, determining the urgency remains difficult because it is based on qualitative factors, including the “need” for hospitalization, inotropes, and mechanical support by the potential recipient.
|
|
|
Figure 90.5. Age distribution of patients listed for liver transplant per year. (Source: 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1996–2005. Rockville, MD: Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation. The data and analyses reported in the 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients have been supplied by UNOS and Arbor Research under contract with HHS. The authors alone are responsible for reporting and interpreting these data; the views expressed herein are those of the authors and not necessarily those of the U.S. Government.) |
Lung
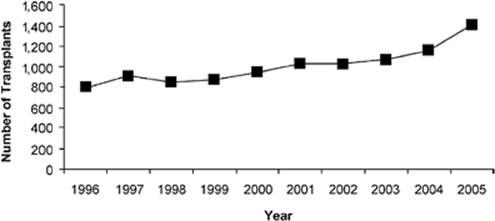
There were more than 3,000 patients awaiting lung transplants at the end of 2005. The past decade has seen a steady increase in the percentage of older patients on the waiting list (Fig. 90.9). Over the past several years, the average waiting time to transplant has decreased, the number of deaths on the list has decreased, and the number of transplants has increased, with a peak of 1,407 lung transplants in 2005 (Fig. 90.10). These data are the product of changes in lung allocation policy, better patient management while on the list, and the efforts of OPOs and hospitals to recognize and optimize potential lung donors. Of note, the number of combined heart–lung transplants has declined, with just 45 performed in 2005.
The typical recipient is an adult 50 to 64 years of age, with a diagnosis of emphysema or idiopathic pulmonary fibrosis. The median waiting time to transplant is nearly 7 months. Survival rates after lung transplant have gradually improved, the main determinants of outcome including recipient age, diagnosis, history of prior transplant, and severity of illness at the time of transplant. Adjusted survival rates at 1, 3, and 5 years are currently 85%, 66%, and 51%, respectively.
Intestine
Intestinal transplantation has emerged as an accepted therapy for complicated intestinal failure. Standardization of surgical techniques, better management of the intestinal failure patient, improvements in immunosuppression, and advances in graft surveillance have led to better patient and graft survival (6). Survivors are almost always able to be completely tapered from parenteral nutrition.
|
|
|
Figure 90.6. Number of liver transplants performed by donor type per year. DDLT, deceased donor liver transplant; LDLT, living donor liver transplant. (Source: 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1996–2005. Rockville, MD: Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation. The data and analyses reported in the 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients have been supplied by UNOS and Arbor Research under contract with HHS. The authors alone are responsible for reporting and interpreting these data; the views expressed herein are those of the authors and not necessarily those of the U.S. Government.) |
The intestine can be transplanted as an isolated organ or as part of a composite graft depending on the needs of the patient. The multivisceral graft includes, en bloc, the stomach, liver, duodenum, pancreas, and small intestine. This graft can be modified to include or exclude the liver, spleen, colon, or a kidney. Each modification has critical care implications, especially when the recipient requires a liver as part of the transplant.
|
|
|
Figure 90.7. Patient survival after deceased donor liver transplant over time by decrease severity. St 1 represents status 1 patients—these patients have the highest priority. The Model for End-Stage Liver Disease (MELD) ranges from 6 to 40. A higher MELD reflects a greater disease severity and a higher place on the waiting list. (Source: 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1996–2005. Rockville, MD: Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation. The data and analyses reported in the 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients have been supplied by UNOS and Arbor Research under contract with HHS. The authors alone are responsible for reporting and interpreting these data; the views expressed herein are those of the authors and not necessarily those of the U.S. Government.) |
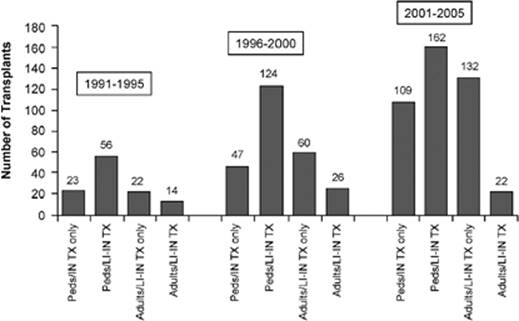
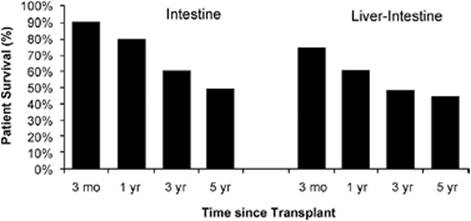
The number of intestinal transplants has been increasing, as illustrated in Figure 90.11. Many variables affect outcome, and, in recent years, patient and graft survival have been improving. Patient survival from data over the past 15 years is shown in Figure 90.12.
Donor Recognition and Assessment
Transplantation depends on organ donation. OPOs are charged with the responsibility of deceased organ donor recognition and assessment. Medical professionals are required to cooperate with OPO personnel to ensure that all potential organ and tissue donors are identified and afforded the opportunity to donate (7,8). It is recommended that OPO and hospital staff collaborate by establishing criteria as to when it is the earliest appropriate time to consult the OPO.
|
Table 90.1 Number of patients on heart waiting list by year |
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
|
||||||||||||||||||||||||
|
Figure 90.8. Patient survival after heart transplant by diagnosis. (Source: 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1996–2005. Rockville, MD: Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation. The data and analyses reported in the 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients have been supplied by UNOS and Arbor Research under contract with HHS. The authors alone are responsible for reporting and interpreting these data; the views expressed herein are those of the authors and not necessarily those of the U.S. Government.) |
||||||||||||||||||||||||
The critical care physician's first priority is to provide excellent patient care. Additionally, he or she should recognize, when brain death is imminent or when withdrawal of support measures are considered, that there is an opportunity through organ donation to help other patients. Timing is critical: approaching a family too early is inappropriate and too late threatens the potential for organ donation.
|
|
|
Figure 90.9. Age distribution of active lung waiting list by year. (Source: 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1996–2005. Rockville, MD: Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation. The data and analyses reported in the 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients have been supplied by UNOS and Arbor Research under contract with HHS. The authors alone are responsible for reporting and interpreting these data; the views expressed herein are those of the authors and not necessarily those of the U.S. Government.) |
To assist in defining the appropriate time to consider OPO involvement, UNOS has devised the term imminent neurologic death. This term describes the patient with an irreversible brain injury who may fit the general criteria of a potential organ donor but has not been legally declared brain dead. It is appropriate to notify the OPO when a patient meets this definition and displays an absence of at least three of the following neurologic functions as a result of the brain injury (not pharmacologic sedation or other confounding variables):
· Pupillary reaction
· Response to cold calorics
· Gag reflex
· Cough reflex
· Corneal reflex
· Doll's eyes reflex
· Response to painful stimuli
· Spontaneous breathing
In short, when the diagnosis of brain death is being considered, and the clinical assessment has begun to confirm that diagnosis, the OPO should be notified.
|
|
|
Figure 90.10. Number of deceased donor lung transplants per year. (Source: 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1996–2005. Rockville, MD: Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation. The data and analyses reported in the 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients have been supplied by UNOS and Arbor Research under contract with HHS. The authors alone are responsible for reporting and interpreting these data; the views expressed herein are those of the authors and not necessarily those of the U.S. Government.) |
There are two important implications of the above statement that warrant clarification. First, OPO personnel are permitted access to patients' medical records per an exemption in the Health Insurance Portability and Accountability Act (HIPAA) (9). Second, the critical care provider is not required to notify the patient's family that the OPO has been consulted. If they wish, critical care providers can inform the family and/or introduce the idea of organ donation. It is not recommended that they discuss the process and options in detail. That task should be left to OPO personnel who are specially trained to approach grieving families and are qualified to obtain informed consent for organ and tissue donation.
Donation Consent Request
Informed consent is required for organ donation. Signed organ donor cards, living wills, and driver's license organ donor designation are recognized as legal “first-person consent” documents. More often, informed consent is obtained by trained OPO personnel from the potential donor's legal next-of-kin or designated health care surrogate. Before the family is approached for consent, it is appropriate that the ICU team inform the family as to the patient's condition and prognosis. Once brain death has been declared and confirmed or, alternatively, once care efforts have been deemed futile and a decision has been made to withdraw support, OPO personnel can approach the family for a discussion about organ donation. The HRSA Organ Donation Breakthrough Collaborative stresses that “effective requesting” requires planning and communication between OPO and ICU personnel so that the family is approached with sensitivity and compassion (10).
|
|
|
Figure 90.11. Number of intestinal transplants by age group and era. TX, transplant; LI, liver; IN, intestine; Peds, pediatric patients. (Source: 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1996–2005. Rockville, MD: Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation. The data and analyses reported in the 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients have been supplied by UNOS and Arbor Research under contract with HHS. The authors alone are responsible for reporting and interpreting these data; the views expressed herein are those of the authors and not necessarily those of the U.S. Government.) |
Organ Donation Process
There are fundamentally two types of potential donors that can be considered from the critical care population: ventilator-dependent patients who will be withdrawn from life-sustaining measures and patients who are declared clinically brain dead. In the former circumstance, it is possible to offer the option of organ donation after cardiac death (DCD), provided certain criteria are met. In the latter, donation may occur in the presence of circulation after the patient has been declared clinically brain dead. This is termed organ donation after brain death (DBD). As guidelines, UNOS has published the Critical Pathway for the Organ Donor and the Critical Pathway for Donation After Cardiac Death (11).
Brain Death
History and Legislation
For centuries, the timing of death coincided with the cessation of circulation. Advances in cardiopulmonary resuscitation and techniques such as hypothermic total circulatory arrest demand a re-examination of this definition. Death, by definition, is permanent. Also, the advent of prolonged mechanical ventilation showed that respiration and circulation could be supported even in cases of complete, irreversible cessation of brain function. Medical advancements over the past century have required that the definition and timing of death be reconsidered. It is out of this milieu that the concept of brain death has emerged and evolved.
|
|
|
Figure 90.12. Patient survival after intestinal transplant, 1991–2005. (Source: 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1996–2005. Rockville, MD: Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation. The data and analyses reported in the 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients have been supplied by UNOS and Arbor Research under contract with HHS. The authors alone are responsible for reporting and interpreting these data; the views expressed herein are those of the authors and not necessarily those of the U.S. Government.) |
In 1956, Löfstedt and Von Reis described six mechanically ventilated patients with lethal brain injuries. On examination, all were unarousable and unresponsive, flaccid, areflexic, and apneic. Spontaneous respiratory effort had ceased abruptly. Cerebral angiography demonstrated no blood flow to the brain. Autopsy revealed cerebral necrosis (12). In 1959, Wertheimer et al. described “the death of the nervous system,” which they concluded should be regarded in the same accord as death by cardiopulmonary arrest (13). In the same year, Mollaret and Goulon introduced the term coma dépassé (beyond coma), an irreversible condition of coma and apnea (14). These observations, as well as those by others over the next decade, culminated in the well-known review of the Harvard Committee, which, in 1968, described brain death as being characterized by “unresponsiveness and lack of receptivity, the absence of movement and breathing, the absence of brainstem reflexes, and coma whose cause has been identified” (15).
In the years that followed, the criteria were revised to exclude the need for a 24-hour period between brain death evaluations and that an electroencephalogram (EEG) is useful in the diagnosis but not required (16). In 1971, Mohandas and Chou specifically identified damage to the brain stem as a critical component of brain death. This point remains key in both clinical and legal brain death definitions (17).
Key legislation was introduced in 1980 with the Uniform Determination of Death Act (UDDA), which met the approval of the National Conference of Commissioners on Uniform State Laws in cooperation with the American Medical Association, the American Bar Association, and the President's Commission on Medical Ethics. This law has served as the medical and legal communities' foundation for the determination of brain death in all situations (18). In the United States, the most recent appraisal and comprehensive guide to assist clinicians in the evaluation of brain death was published by the American Academy of Neurology in 1995, which provided evidence-based practice measures along with a very practical version of apnea testing (19).
Brain Death Determination
Brain death is fundamentally a clinical diagnosis based on key physical examination features in the context of a specific history and in the absence of confounding factors. Important considerations in a precise brain death evaluation include a history of an acute, irreversible catastrophic event involving the cerebral hemispheres and brain stem, ruling out any conditions that may confound the determination. Confounding factors that prohibit a diagnosis of brain death include acid-base, electrolyte, or endocrine disturbances; severe hypothermia; hypotension; drug intoxication; poisoning; or the presence of neuromuscular blocking agents.
The clinical physical examination remains the gold standard for brain death evaluation. The key examination features include no motor response to pain, no pupillary response to light, absent oculocephalic reflex, absent corneal reflex, absent cough and gag reflex, and apnea (20). If the patient does not exhibit any of these neural reflexes, the clinician may document the diagnosis of clinical brain death in accordance with state law. Each state specifies who is qualified to make the determination of brain death. A given hospital may have a policy stating who can determine brain death and whether a time interval or second exam is needed to verify the diagnosis.
Confirmatory tests can serve a complementary role in the determination of brain death, but are not routinely required; though at times helpful, their availability and utility vary from institution to institution. Commonly used diagnostic tests to confirm brain death include cerebral angiography, cerebral nuclear imaging with contrast, and EEG. These tools can be especially useful in pediatric patients or those patients in whom the neurologic examination findings may be difficult to assess. Examples of the latter include the patient with severe facial trauma or spinal cord injury. Cerebral angiography and nuclear imaging serve to assess intracranial perfusion. The absence of perfusion supports the diagnosis of brain death but, alone, is not sufficient to make the diagnosis. The use of the EEG can also be complementary, but must be used with caution. It is used often because of its wide availability relative to other confirmatory studies, but is subject to artifact and interference in the ICU environment.
Although the same principles for the evaluation and diagnosis of brain death are used in the pediatric patient, the clinical examination may be difficult because of the patient's size, developmental differences, and course of treatment. In 1987, a group composed of several prominent medical societies convened and published guidelines for the determination of brain death in children. The group concluded that although the specifics of the clinical exam and the pertinent findings that determine brain death are essentially the same, in the pediatric population, repeat assessments by different observers and a more liberal use of confirmatory tests are recommended (21).
Donor Management
In many ways, management of the organ donor resembles that of the critically ill patient, with an important distinction. The goal for the critically ill patient is recovery, prolonging life, and improving its quality. The goal of donor management is maximization of the number and quality of transplantable organs (22). Once brain death has been determined, OPO personnel play an instrumental role in donor management. Brain death is associated with grossly impaired body temperature regulation, profound hypernatremia due to diabetes insipidus, impaired blood pressure regulation, coagulopathy, endocrine dysfunction, and electrolyte and acid-base disturbances. Physiologic derangement may have been the manifestation of the inciting injury or insult; this is often worse at the time of cerebral edema, herniation, and brain death (23,24,25,26,27,28).
Monitoring and Maintenance
Donor maintenance has become more sophisticated in recent years. Each OPO has detailed protocols and care pathways for organ donor optimization. Each has a medical director and/or critical care physician as a consultant or as an active participant in the process. The OPO community under the direction of the HRSA has developed its “best practices” for donor monitoring and maintenance. Fluids administered, urine output, and any other fluid losses are measured. Monitoring routinely includes the use of arterial catheters for blood pressure monitoring, central venous pressure monitoring, and sometimes pulmonary artery (PA) catheter placement. Arterial oxygenation is monitored via continuous pulse oximetry.
Fluid warmers and other warming devices are utilized as needed to maintain normothermia. Mechanical ventilation modalities geared toward maintaining oxygenation and ventilation while minimizing pulmonary injury are utilized. Hemodynamic derangement is addressed with fluids (crystalloid, colloid, and blood products) and the administration of vasopressors, inotropes, or antihypertensives as indicated. A standardized battery of laboratory tests is obtained, and detected abnormalities are corrected, if possible. Acid-base abnormalities are corrected, and hypernatremia and hyperglycemia are treated. Antibiotics, corticosteroids, endocrine replacement, and other medications are given to the donor in accordance with detailed management protocols. Cultures, viral serologies, blood type, and human leukocyte antigen studies are performed to assess donor and recipient compatibility.
Assessment
Coincident with monitoring and correction of physiologic derangement, the donor organs are evaluated for transplantation. A thorough history is obtained and the medical record reviewed. Emphasis is placed on detection of infection, presence or a history of malignancy, and comorbid conditions that can affect organ viability.
Each organ is considered individually, and specific tests are available to measure function or detect impairment (29). The heart is evaluated by an assessment of the donor's hemodynamic status, sometimes with the aid of a PA catheter, need for vasopressors or inotropic drugs, transthoracic echocardiography, and, in selected cases, coronary angiography. Lung assessment includes serial arterial blood gas measurement, chest radiography, and flexible bronchoscopy. The kidneys are evaluated by urine output, serum creatinine measurement, and, for some OPOs, a calculation of the glomerular filtration rate. After procurement, a renal cortical biopsy can yield important information regarding organ quality. Some OPOs and TCs preserve kidneys with a pulsatile perfusion machine. Some transplant surgeons use the performance parameters of the kidney(s) on the pump as an adjunct measure of quality. There are few specific indicators of pancreas viability and quality. Euglycemia without the need for significant amounts of exogenous insulin is preferable. Elevated serum amylase may raise concern that the gland is not suitable because of pancreatitis. The liver is assessed by transaminase and bilirubin measurements. Serum albumin and coagulation studies are measures of liver function. A liver biopsy obtained percutaneously before procurement, or in the operating room at the time of organ recovery, can be useful for detecting inflammation, necrosis, fibrosis, or steatosis. There are no specific standardized methods for the evaluation of the donor intestine.
While organ evaluation has improved, nothing has approached the judgment of the experienced transplant surgeon visually inspecting the organs at the time of organ recovery. It is this important evaluation, in conjunction with the donor's history and physiologic condition and the results of organ-specific studies, that is ultimately used to decide whether an organ is suitable for transplant.
Organ Recovery and Preservation
Like donor maintenance and assessment, the surgical recovery and preservation of organs for transplant has become a highly orchestrated process directed by the OPO. The procurement procedure often occurs at a hospital with otherwise little contact with transplant procedures or patients. The procedure is usually added to an already busy operating room schedule and is often given little priority. Yet, procurement is a time in which multiple surgeons—sometimes from multiple institutions—convene to assess, remove, and preserve those organs suitable for transplantation. While the procurement takes place, specialized OPO personnel support a grieving family, and critically ill patients are being mobilized and prepared for transplant surgery. The procurement is a time-sensitive, highly orchestrated procedure.
The organ recovery operation has become standardized. The procedure is performed in the operating room using a standard sterile technique. The donor's identity, informed consent, blood type, brain death certification, and medical record are again reviewed. The chest and abdomen are opened. The donor is inspected for malignancy or occult disease. The organs to be procured are visually inspected. Some dissection is done to mobilize the organs. The donor is heparinized, followed by the insertion of cannulas for the administration of cold preservation fluid. The time is recorded, and the aorta is clamped, initiating the start of cold ischemia. The donor organs are flushed with specialized preservation solutions to exsanguinate the organs and instill preservation fluid. Three commonly used solutions are the University of Wisconsin (UW) solution, histidine-tryptophan-ketoglutarate (HTK) solution, and Celsior solution. The organs are removed sequentially, with the thoracic organs being removed first, followed by the abdominal organs, then the kidneys. Finally, various vessels are taken for vascular conduits if needed, and lymph nodes and the spleen are taken for immunologic studies.
Our ability to preserve organs for transplant is rather limited. Optimally, the cold ischemia time for transplanted organs should be less than 4 hours for hearts and lungs, less than 10 hours for the abdominal viscera, and less than 24 hours for kidneys. Certainly, organs have been successfully transplanted with many more hours of ischemia, but the risk of delayed graft function and graft nonfunction rises rapidly as time elapses.
The brain-dead organ donor remains the preferred donor type, since circulation and supportive interventions continue until the moment hypothermic preservation is initiated. This type of donor is relatively controlled, and allows time for confirmation of death, informed consent, optimization, assessment, organ allocation, and coordinating the recovery. Finally, the quantity and quality of the organs recovered from this donor type are typically greater than that obtained from DCD donors.
In the DCD donor, there is a time interval between the withdrawal of support from the patient, cardiopulmonary arrest, determination and pronouncement of death, the start of the recovery procedure, and initiation of cold preservation. The amount of time this takes is difficult to predict, but certainly adds to the ischemic injury to the organs, and limits the surgeon's ability to assess the organs for transplant (30). Logistically, the process is more difficult than that for the brain-dead organ donor. The process is emotionally sensitive and must be handled with the utmost sensitivity and care (31).
The DCD donor concept is simple: some patients with lethal insults or injuries for whom supportive measures are to be withdrawn are candidates for organ donation if the organ recovery can take place within minutes of the cessation of circulation. The logistics of the process are complex. OPO personnel must be consulted prior to the withdrawal of support, but they do not participate in the withdrawal process or pronouncement of death (32). The task of the OPO personnel is to explain the options regarding organ donation to the patient's family or designee, obtain informed consent, and coordinate the assembling of a surgical recovery team to be present and immediately available at the time of death.
The withdrawal of support usually takes place in, or near, the operating suite. The family may be present, but must be willing to leave immediately upon declaration of death. It is preferred that the patient be heparinized prior to cessation of circulation. The physician authorized and designated to assess and pronounce death is present. This physician must not be affiliated with the OPO, the transplant team, or potential recipient(s). The surgical recovery team prepares to begin, but waits in an adjacent room beyond view for two reasons: (a) in deference to any family members present and (b) to ensure that they in no way influence the protocol for the withdrawal of life support, nor the physician's assessment and determination of death. Once death has been declared, the recovery must begin after 2 minutes but before 5 minutes have elapsed. If the patient does not expire in 30 to 60 minutes, he or she is brought back to the ICU, and the procurement is cancelled. This possibility should be explained when consent is obtained. Recently, the issue of DCD organ donation has been addressed separately by a consensus conference of experts in transplantation, the Institute of Medicine, and UNOS (33,34,35).
Future Expectations
The past several years have generated dramatic advances in transplantation, and the future promises much more. The transplant community will continue to investigate methods for expanding the pool of organs available for transplantation. Multiple modalities, ranging from public education to increasing organ donation awareness to the use of living donors and ECDs, will continue. The problems related to the long-term use of immunosuppressive drugs, disease recurrence, and organ donor disease transmission will pose important challenges in the years to come. The development of comprehensive centers designed to treat the spectrum of patients with end-stage organ failure, and not just those patients who are potentially transplant recipients, will likely continue. Strategies are evolving that may take us closer to the lofty goal of immunologic tolerance. Finally, advances in tissue engineering and cell transplantation give us a glimpse of a future where organs can be repaired or produced in the laboratory to the recipient's exact specifications.
References
1. 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients: Transplant Data 1996. Rockville, MD: Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation. (The data and analyses reported in the 2006 Annual Report of the U.S. Organ Procurement and Transplantation Network and the Scientific Registry of Transplant Recipients have been supplied by UNOS and Arbor Research under contract with HHS. The authors alone are responsible for reporting and interpreting these data; the views expressed herein are those of the authors and not necessarily those of the U.S. Government.)
2. Segev DL, Gentry SE, Warren DS, et al. Kidney paired donation and optimizing the use of live donor organs. JAMA. 2005;293:1883.
3. Wolfe RA, Ashby VA, Milford EL, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341:1725.
4. Kim RD, Reed AI, Fujita S, et al. Consensus and controversy in the management of hepatocellular carcinoma. J Am Coll Surg. 2007;205:108.
5. Kamath PS, Kim WR. The model for end-stage liver disease (MELD). Hepatology. 2007;45:797.
6. Ruiz P, Kato T, Tzakis AG. Current status of transplantation of the small intestine. Transplantation. 2007;83:1.
7. Department of Health and Human Services, Centers for Medicare and Medicaid Services Conditions of Participation CFR 42, Parts 405, 482, 488, 498, Volume 72:61, March 30, 2007, Rules and Regulations.
8. United Network for Organ Sharing (UNOS). Policies and Procedures 7.0. http://www.unos.org/PoliciesandBylaws2/policies/docs/policy_23.doc. Accessed February 10, 2007.
9. Joint Commission on Accreditation of Health Care Organizations. Healthcare at the Crossroads: Strategies for Narrowing the Organ Donation Gap and Protecting Patients. Federal Register § 164.512(h), December 28, 2000.
10. U.S. Department of Health and Human Services, Health Resources and Services Administration, Office of Special Programs, Division of Transplantation. The Organ Donation Breakthrough Collaborative: Best Practices Final Report. Washington, DC: U.S. Department of Health and Human Services; 2003. Contract: 240–94-0037, Task Order No. 12.
11. United Network for Organ Sharing (UNOS). Critical Pathway for the Organ Donor and the Critical Pathway for Donation After Cardiac Death. http://www.unos.org/resources/donorManagement.asp?index=2. Accessed February 10, 2007.
12. Löfstedt S, Von Reis G. Intracranial lesions with abolished passage of x-ray contrast through the internal carotid arteries. Opuscula Med. 1956;8:199.
13. Wertheimer P, Jouvet M, Descotes J. A propos du diagnostic de la mort du système nerveux dans les comas avec arrêt respiratoire traites par respiration artficielle. Presse Med. 1959;67:87.
14. Mollaret P, Goulon M. Le coma dépassé. Rev Neurol. 1959;101:3.
15. A definition of irreversible coma. Report of the Ad Hoc Committee of the Harvard Medical School to examine the definition of brain death. JAMA. 1968;205:337.
16. Beecher HK. After the definition of irreversible coma. N Engl J Med. 1969;281:1070.
17. Mohandas A, Chou SN. Brain death: a clinical and pathological study. J Neurosurg. 1971;35:211.
18. Uniform Determination of Death Act, 12 Uniform Laws Annotated (U.L.A.) 589 (West 1993 and West Supp. 1997).
19. The Quality Standards Subcommittee of the American Academy of Neurology. Practice parameters for determining brain death in adults (summary statement). Neurology. 1995;45:1012.
20. Wijdicks EFM. The diagnosis of brain death. N Engl J Med. 2001;344:1215.
21. Guidelines for the determination of brain death in children. American Academy of Pediatrics Task Force on Brain Death in Children. Pediatrics. 1987;80:298.
22. Rudow DL, Ohler L, Shafer T. A Clinician's Guide to Donation and Transplantation. Lenexa, KS: Applied Measurement Professionals Inc; 2006.
23. Grossman MD, Reilly PM, McMahon DJ, et al. Loss of potential solid organ donors due to medical failure. Crit Care Med. 1996;24:A76.
24. Powner D, Darby J. Management of variations in blood pressure during care of organ donors. Prog Transplant. 2000;10:25.
25. Powner D, Kellum J, Darby J. Abnormalities in fluids, electrolytes, and metabolism of organ donors. Prog Transplant. 2000;10:88.
26. Powner D, Kellum J. Maintaining acid-base balance in organ donors. Prog Transplant. 2000;10:98.
27. Powner D, Reich H. Regulation of coagulation abnormalities and temperature in organ donors. Prog Transplant. 2000;10:146.
28. Powner D, Darby J, Stuart S. Recommendations for mechanical ventilation during donor care. Prog Transplant. 2000;10:33.
29. United Network for Organ Sharing (UNOS). Policies and Procedures 2.0. http://www.unos.org/PoliciesandBylaws2/policies/docs/policy-2.doc. Accessed February 10, 2007.
30. Lewis J, Peltier J, Nelson H, et al. Development of the University of Wisconsin donation after cardiac death evaluation tool. Prog Transplant. 2003;13:265.
31. McVearry-Kelso C, Lyckholm LJ, Coyne PJ, et al. Palliative care consultation in the process of organ donation after cardiac death. J Palliative Med. 2007;10:118.
32. United Network for Organ Sharing (UNOS). OPTN Bylaws, Appendix B, Attachment III-1 of the OPTN bylaws. Model elements for controlled DCD recovery protocols. http://www.unos.org/policiesandBylaws2/bylaws/UNO- SByLaws/DOCs/bylaw_145.doc. Accessed July 1, 2007.
33. Bernat JL, D'Alessandro AM, Port FK, et al. Report of a national conference on donation after cardiac death. Am J Transplant. 2006;6:281.
34. Institute of Medicine, National Academy of Sciences. Non-Heart Beating Organ Transplantation: Medical and Ethical Issues in Procurement. Washington, DC: National Academy Press; 1997.
35. Institute of Medicine, National Academy of Sciences. Non-Heart Beating Organ Transplantation: Practice and Protocols. Washington, DC: National Academy Press; 1997.