Ronda L. Akins
LEARNING OBJECTIVES
Upon completion of the chapter, the reader will be able to:
1. Differentiate the causes and development of infective endocarditis (IE).
2. Identify the clinical presentation and laboratory evaluation for IE.
3. Assess diagnostic criteria used to evaluate a patient suspected of having IE.
4. Describe the most likely causative organisms of IE, particularly in specific patient populations.
5. Develop appropriate pharmacologic treatment recommendations for patients with IE.
6. Define appropriate patient populations requiring prophylactic treatment, and differentiate appropriate drug regimens.
7. Devise a monitoring plan for patients with IE to determine treatment efficacy and discern any adverse effects.
KEY CONCEPTS
![]() For infective endocarditis (IE) to develop, the occurrence of several factors is required. These factors involve alterations to the endocardial surface which allow bacterial adherence and eventual infection.
For infective endocarditis (IE) to develop, the occurrence of several factors is required. These factors involve alterations to the endocardial surface which allow bacterial adherence and eventual infection.
![]() Persistent fever is the most common symptom present in patients with IE.
Persistent fever is the most common symptom present in patients with IE.
![]() Blood cultures are the essential laboratory test for the diagnosis and treatment of IE. Typically, patients with IE have a low-grade consistent bacteremia. Blood culture results are critical for determining the most appropriate therapy.
Blood cultures are the essential laboratory test for the diagnosis and treatment of IE. Typically, patients with IE have a low-grade consistent bacteremia. Blood culture results are critical for determining the most appropriate therapy.
![]() Echocardiograms are used for detecting the presence of a vegetation. Either a transthoracic echocardiogram (TTE) or a transesophageal echocardiogram (TEE) may be used depending on certain patient characteristics.
Echocardiograms are used for detecting the presence of a vegetation. Either a transthoracic echocardiogram (TTE) or a transesophageal echocardiogram (TEE) may be used depending on certain patient characteristics.
![]() Choosing the appropriate antimicrobial therapy is crucial to achieve adequate organism kill.
Choosing the appropriate antimicrobial therapy is crucial to achieve adequate organism kill.
![]() An extended treatment course of 4 to 6 weeks (in most cases) is required to achieve an adequate cure.
An extended treatment course of 4 to 6 weeks (in most cases) is required to achieve an adequate cure.
![]() The overall goal of therapy is to eradicate the infection and minimize/prevent any complications.
The overall goal of therapy is to eradicate the infection and minimize/prevent any complications.
![]() In an effort to prevent the development of IE, prophylactic treatment generally is considered appropriate for patients with high-risk factors.
In an effort to prevent the development of IE, prophylactic treatment generally is considered appropriate for patients with high-risk factors.
![]() Monitoring the patient’s clinical course is necessary to assess the effectiveness of therapy, detect the potential development of bacterial resistance, and determine outcome.
Monitoring the patient’s clinical course is necessary to assess the effectiveness of therapy, detect the potential development of bacterial resistance, and determine outcome.
Infective endocarditis (IE) is a serious infection affecting the lining and valves of the heart. While this disease is mostly associated with infection of the heart valves, the septal defects may become involved as well. Infections also occur in patients with prosthetic or mechanical devices, such as mechanical heart valves or who are IV drug users (IVDUs). Bacteria is the primary cause of IE; however, fungi and atypical organisms may also be responsible pathogens.
Typically IE is classified into two categories: acute or subacute. The difference between the two categories is based on the progression and severity of the disease. Acute disease is more aggressive, characterized by high fevers, elevated WBC counts, and systemic toxicity, with death occurring within a few days to weeks. This type of IE is often caused by more virulent organisms, particularly Staphylococcus aureus. Subacute disease is typically caused by less virulent organisms, such as viridans streptococci, producing a slower and more subtle presentation. It is characterized by weakness, fatigue, low-grade fever, night sweats, weight loss, and other nonspecific symptoms, with death occurring in several months.
Successful management of patients with IE is based on proper diagnosis, treatment with adequate therapy, and monitoring for complications, adverse events, or development of resistance. The treatment and management of IE are best determined through identification of the causative organism. IE has varied clinical presentations; therefore, patients with this infection may be found in any medical subspecialty (i.e., medicine, surgery, critical care, etc.).
EPIDEMIOLOGY AND ETIOLOGY
Despite IE being a fairly uncommon infection, in the United States, there are about 10,000 to 20,000 new cases annually, and IE accounts for approximately 1 case per 1,000 hospital admissions.1 Although the exact number of cases is often difficult to determine owing to the diagnostic criteria and reporting methods for this disease, it continues to rise. IE is now considered the fourth leading cause of serious infectious disease syndromes following urosepsis, pneumonia, and intra-abdominal sepsis.2 Men are affected more commonly than women at a ratio of 1.7:1. Although IE occurs at any age, more than 50% of cases occur in patients older than 50 years.1 IE in children continues to be uncommon and is mainly associated with underlying structural defects, surgical repair of the defects, or nosocomial catheter-related bacteremia.1 With the increased use of mechanical valves, prosthetic-valve endocarditis (PVE) now accounts for approximately 7% to 25%.3 Patients who are IVDUs are also at an increased risk for IE, with 150 to 2,000 cases per 100,000 persons per year, most being younger adults.3 Additionally, other patients at high risk for IE include patients with any congenital or structural cardiac defects, including valvular disease; long-term hemodialysis; diabetes mellitus; poor oral hygiene; major dental treatment; previous endocarditis; hypertrophic cardiomyopathy; and mitral valve prolapse with regurgitation.4–8
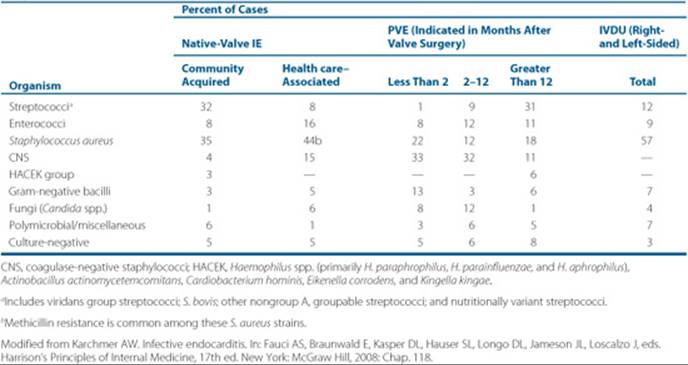
Although almost any type of organism is capable of causing IE, the majority of cases are caused by gram-positive organisms. These consist primarily of streptococci, staphylococci, and enterococci. Consideration of gram-negative, fungal, and other atypical organisms must be taken into account, particularly in certain patient populations. In Table 74–1, approximate percentages are given for each organism based on the type of IE, including native valve (community acquired versus health care-associated), prosthetic valve (grouped by months postsurgery) and IVDUs.
Patient Encounter, Part 1
A 56-year-old man with a history of diabetes and coronary artery disease presents to the emergency department with complaints of weakness, fever, and chills. On interviewing the patient, you determine that he went to the dentist about 3 weeks ago and since that time has lost about 2.3 kg (5 lb). His current weight is 63.6 kg (140 lb). The patient reports that the symptoms began about 1 to 2 weeks ago. He denies any use of alcohol or illicit drugs but admits to smoking about half a pack of cigarettes per day.
What information would make you suspect infective endocarditis (IE)?
Does he have any risk factors for IE?
What additional information would you like to know before deciding on an empirical treatment for this patient?
Table 74–1 Etiologic Organisms of IE
PATHOGENESIS AND PATHOPHYSIOLOGY
![]() For IE to develop, the occurrence of several factors is required. Typically, there must be an alteration of the endothelial surfaces of the heart valves to allow for organism attachment and colonization.These alterations may be produced by an inflammatory process such as rheumatic heart disease or by injury from turbulent blood flow. Platelets and fibrin now deposit on the damaged valves, forming a nonbacterial thrombotic endocarditis (NBTE). At this point, bacteria through hematogenous spread (i.e., bacteremia) adhere to and colonize the nidus, forming a vegetation.8 Further deposits of platelets and fibrin cover the bacteria, providing a protective coating that allows for the development of a suitable environment for continued organism and vegetation progression, often producing an organism density of 109 to 1010 colony-forming units (CFU) per gram. This sequence of events is summarized in Figure 74–1.
For IE to develop, the occurrence of several factors is required. Typically, there must be an alteration of the endothelial surfaces of the heart valves to allow for organism attachment and colonization.These alterations may be produced by an inflammatory process such as rheumatic heart disease or by injury from turbulent blood flow. Platelets and fibrin now deposit on the damaged valves, forming a nonbacterial thrombotic endocarditis (NBTE). At this point, bacteria through hematogenous spread (i.e., bacteremia) adhere to and colonize the nidus, forming a vegetation.8 Further deposits of platelets and fibrin cover the bacteria, providing a protective coating that allows for the development of a suitable environment for continued organism and vegetation progression, often producing an organism density of 109 to 1010 colony-forming units (CFU) per gram. This sequence of events is summarized in Figure 74–1.
Acquisition of PVE differs in early stages, where direct inoculation may occur during surgery instead of through hematogenous seeding. The prosthetic valve also has a greater propensity for organism colonization than native valves. However, in late PVE, the process of colonization and vegetation formation is similar to native-valve IE, as described earlier.9
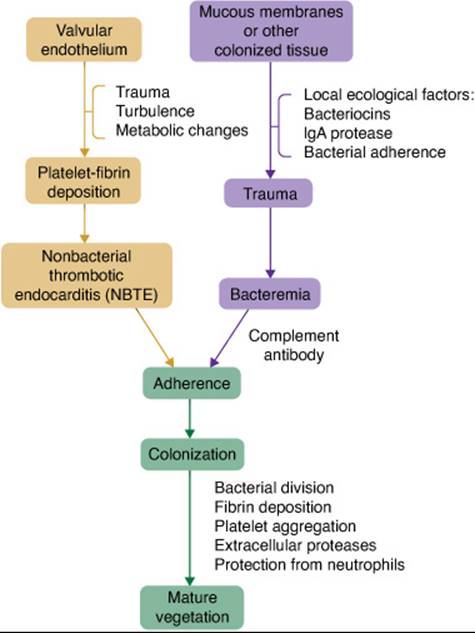
FIGURE 74–1. Pathogenesis of infective endocarditis. (From Ref. 1, Copyright 2005, with permission from Elsevier.)
Classically, vegetations are located on the line along valve closure on the atrial surface of the atrioventricular valves (tricuspid and mitral) or on the ventricular surface of the semilunar valves (pulmonary and aortic) (Fig. 74–2). The vegetations can vary significantly in size ranging from millimeters to several centimeters and may be single or multiple masses. Often, destruction of underlying tissue occurs and may cause perforation of the valve leaflet or rupture of the chordae tendinae, interventricular septum, or papillary muscle. Valve ring abscesses may occur, resulting in fistulas penetrating into the myocardium or pericardial sac, particularly with staphylococcal endocarditis.
Embolic events are also common. Embolization occurs as portions of the friable vegetation break lose and enter the bloodstream. These infected pieces are called septic emboli. Pulmonary abscesses are commonly formed as a result of septic emboli from right-sided IE (tricuspid and pulmonary valves). However, left-sided IE (mitral and aortic valves) is more likely to have an embolus travel to any organ system, especially the kidneys, spleen, and brain. Along with emboli, immune complex deposition may occur in organ systems, causing extracardiac manifestations of the disease. This commonly occurs in the kidneys, producing abscesses, infarction, or glomerulonephritis. Immune complexes or emboli also may produce skin manifestations of the disease, as seen with petechiae, Osler’s nodes, and Janeway’s lesions, or within the eye (e.g., Roth’s spots).
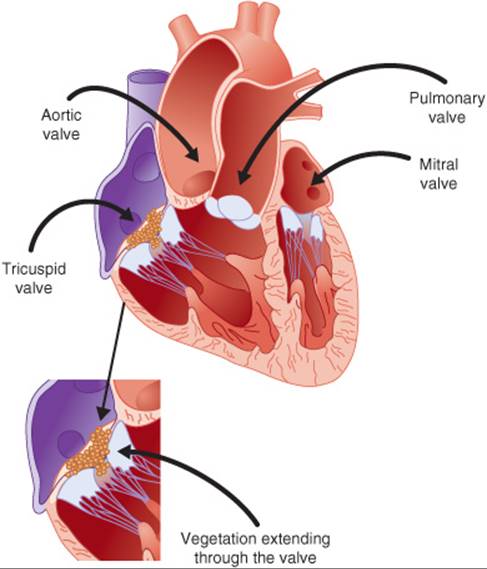
FIGURE 74–2. Diagram of the heart indicating common sites of infection.
Clinical Presentation of IE
General
Patients typically present with nonspecific and variable signs or symptoms.
Symptoms
Complaints from patients may include:
• Fever
• Chills
• Night sweats
• Weakness
• Dyspnea
• Weight loss
• Myalgia or arthralgias
Signs
• Fever is the most common sign of IE
• New or changing heart murmur
• Embolic phenomena (emboli affect the heart, lungs, abdomen, or extremities)
• Skin manifestations (e.g., petechiae, splinter hemorrhages, Osler’s nodes, Janeway’s lesions)
• Splenomegaly
• Clubbing of extremities
Laboratory Tests
• Blood cultures are the most important laboratory assessment for persistent bacteremia, which occurs commonly in IE. A minimum of three blood culture sets should be collected during the initial 24 hours
• Hematologic tests for anemia (normochromic, normocytic)
• WBC count may be elevated in acute disease but could be normal in subacute IE
• Nonspecific findings such as thrombocytopenia, elevated erythrocyte sedimentation rate or C-reactive protein, and abnormal urinalysis (i.e., proteinuria or microscopic hematuria)
Other Diagnostic Tests
An echocardiogram (TTE or TEE) should be performed on any patient with suspected IE to detect the presence of vegetations.
CLINICAL PRESENTATION AND DIAGNOSIS
The clinical presentation for IE is quite variable and often nonspecific. ![]() A fever is the most frequent and persistent symptom in patients but may be blunted with previous antibiotic use, congestive heart failure, chronic liver or renal failure, or infection caused by a less virulent organism (i.e., subacute disease).3 Other signs and symptoms that also may occur are listed in the Clinical Presentation box with some discussed further in detail below.
A fever is the most frequent and persistent symptom in patients but may be blunted with previous antibiotic use, congestive heart failure, chronic liver or renal failure, or infection caused by a less virulent organism (i.e., subacute disease).3 Other signs and symptoms that also may occur are listed in the Clinical Presentation box with some discussed further in detail below.
Heart murmurs are heard frequently on auscultation (over 85% of cases), but a new murmur or change in murmurs is only found in 5% to 10% or 3% to 5%, respectively.1 Additionally, over 90% of patients who have a new murmur will develop congestive heart failure, which is a major cause of morbidity and mortality. Splenomegaly and mycotic aneurysms are also noted in many cases of IE.
This disease is also characterized by the following peripheral manifestations. Some of these clinical findings are found in up to one-half of patients with IE, although recently the prevalence has been decreasing.10
• Skin: Petechiae are very small (usually less than 3 mm) pinpoint flat red spots beneath the skin surface caused by microhemorrhaging. They occur in 20% to 40% of chronic IE, often found on the buccal mucosa, conjunctivae (Fig. 74–3A), and extremities.1 Splinter hemorrhages appear as small dark streaks beneath the finger- or toenails and occur most commonly proximally with IE, typically occurring as a result of local vasculitis or microemboli occurring in about 20% of patients (Fig. 74–3B). Osler’s nodes are small (usually 2–15 mm), painful, tender subcutaneous nodules located on the pads of the fingers and toes (Fig. 74–3D) caused primarily by either septic emboli or vasculitis. These nodes are rare in acute disease but are also nonspecific for IE despite occurring in 10% to 25% of all patients.1 Janeway’s lesions are small, painless hemorrhagic macular plaques on the palms of the hands or soles of the feet due to septic emboli (in approximately 5% of patients) and more commonly associated with acute S. aureus IE (Fig. 74–3E).
• Extremities: Clubbing of the finger tips typically occurs in long-standing illness and is present in approximately 10% to 20% of patients (Fig. 74–3C).1
• Eye: Roth’s spots are rarely occurring (in less than 5% of IE cases), oval-shaped retinal hemorrhages with a pale center near the optic disc (Fig. 74–3F).
Laboratory Studies
![]() Blood cultures are the essential laboratory test for the diagnosis and treatment of IE. Typically, patients with IE have a low-grade consistent bacteremia, with approximately 80% of cases having less than 100 CFU/mL in the bloodstream.1 Blood culture results are critical for determining the most appropriate therapy. Three blood culture sets should be drawn within the initial 24 hours to determine the etiologic agent. Approximately 90% of the first two cultures will yield a positive result. If a positive blood culture is not obtained from a patient with suspected IE, the microbiology laboratory should be notified and cultures requested to be monitored for growth of fastidious organisms for up to 1 month.
Blood cultures are the essential laboratory test for the diagnosis and treatment of IE. Typically, patients with IE have a low-grade consistent bacteremia, with approximately 80% of cases having less than 100 CFU/mL in the bloodstream.1 Blood culture results are critical for determining the most appropriate therapy. Three blood culture sets should be drawn within the initial 24 hours to determine the etiologic agent. Approximately 90% of the first two cultures will yield a positive result. If a positive blood culture is not obtained from a patient with suspected IE, the microbiology laboratory should be notified and cultures requested to be monitored for growth of fastidious organisms for up to 1 month.
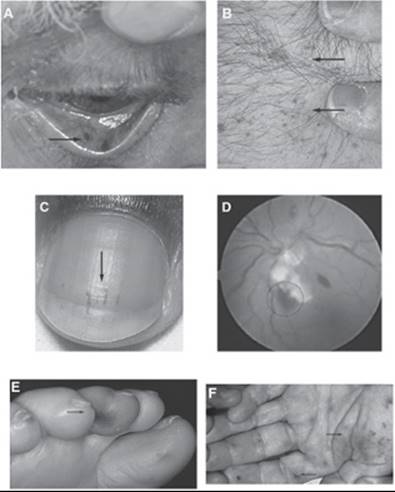
FIGURE 74–3. A. Conjunctival petechiae. (From Wolff K, Johnson RA, Suurmond D. In: Fitzpatrick’s Color Atlas & Synopsis of Clinical Dermatology, 5th ed. New York: McGraw Hill. Copyright 2005.) B. Splinter hemorrhage. (From Collins SP. In: Atlas of Emergency Medicine, 2nd ed. New York: McGraw Hill. Copyright 2002.) C. Clubbing of finger. (From Tosti A, Piraccini BM. In: Fitzpatrick’s Dermatology in General Medicine, 7th ed. New York: McGraw Hill. Copyright 2007.) D. Osler’s nodes. (From Collins SP. In: Atlas of Emergency Medicine, 2nd ed. New York: McGraw Hill. Copyright 2002.) E. Janeway’s lesions. (From Wolff K, Johnson RA, Suurmond D. In: Fitzpatrick’s Color Atlas & Synopsis of Clinical Dermatology, 5th ed. New York: McGraw Hill. Copyright 2005.) F. Roth’s spots (From Effron D, Forcier BC, Wyszynski RE. In: Atlas of Emergency Medicine, 2nd ed. New York: McGraw Hill. Copyright 2002.)
![]() Another important tool aiding in the diagnosis of IE is the echocardiogram. This imaging tool is used to visualize vegetations. Two methods of the echocardiogram are used: the transthoracic echocardiogram (TTE) and the transesophageal echocardiogram (TEE). The TTE has been used since the 1970s; however, it is less sensitive (58–63%) than the TEE (90–100%).10 Despite the TEE being more sensitive, use of the TTE for patients with suspected native-valve IE is usually sufficient.11,12 The TEE may be used as a secondary test for patients whose TTE was negative and in whom a high clinical suspicion of IE exists. Additionally, a TEE is often preferred in patients who have complicated disease, including left-sided IE, prosthetic valves, or perivalvular extension of the vegetation.2,12Echocardiograms also may be employed to assess the need for surgical intervention or to determine the possible source of emboli.11,13
Another important tool aiding in the diagnosis of IE is the echocardiogram. This imaging tool is used to visualize vegetations. Two methods of the echocardiogram are used: the transthoracic echocardiogram (TTE) and the transesophageal echocardiogram (TEE). The TTE has been used since the 1970s; however, it is less sensitive (58–63%) than the TEE (90–100%).10 Despite the TEE being more sensitive, use of the TTE for patients with suspected native-valve IE is usually sufficient.11,12 The TEE may be used as a secondary test for patients whose TTE was negative and in whom a high clinical suspicion of IE exists. Additionally, a TEE is often preferred in patients who have complicated disease, including left-sided IE, prosthetic valves, or perivalvular extension of the vegetation.2,12Echocardiograms also may be employed to assess the need for surgical intervention or to determine the possible source of emboli.11,13
Additional nonspecific tests for IE may be performed. These include hematologic parameters to determine whether the patient is anemic, which occurs in a majority of patients. The WBCs may be elevated, particularly in acute disease. However, in a subacute infection, the WBCs may be normal. An erythrocyte sedimentation rate (ESR) may also be obtained to determine the presence of inflammation, although this test is highly nonspecific and almost always elevated in IE.
DIAGNOSTIC CRITERIA
A definitive diagnosis of IE would consist of a biopsy or culture directly from pathologic specimens from the endocardium. However, this would be a highly invasive test. Therefore, diagnosis of IE relies on clinical presentation as well as laboratory and echocardiogram results. To guide this clinical diagnosis, criteria have been established to assess major and minor criteria for IE14,15 (Table 74–2A). Depending on the number of major or minor criteria a patient demonstrates, he or she will be classified as having a definite, possible, or rejected diagnosis of IE (Table 74–2B).
CAUSATIVE ORGANISMS
Gram-positive bacteria are the most common organisms that produce IE. Streptococci and staphylococci species account for the majority of cases at more than 80%.16 Viridans group streptococci have been considered the primary pathogens in IE. However, staphylococci have been increasing in prevalence as causative organisms and are the dominant causative organisms in some reports (Table 74–1).5,17,18 Other gram-positive, gram-negative, atypical, and fungal organisms are less common but still must be considered in certain patient populations.
Streptococci
Streptococci causing IE are most commonly a group of species called viridans group streptococci. The most common of this group are Streptococcus salivarius, Streptococcus mutans, Streptococcus mitus, and Streptococcus sanguis. This group of bacteria, considered normal flora in the human mouth, is α-hemolytic, and typically, most clinical microbiology laboratories do not differentiate the exact species. These organisms may cause bacteremia after dental procedures, which can lead to the development of IE in at-risk patients. Viridans group streptococci are also the predominant pathogen of IE associated with mitral valve prolapse and native valves and in children.19,20 Another streptococci species that is commonly associated with IE is Streptococcus bovis, classified as group D streptococci, found in the GI tract. However, owing to the similarities of these streptococci, including microbiologic susceptibility, treatment is similar regardless of the species.
Table 74–2 Modified Duke’s Criteria for IE
2A. Definitions of Modified Duke’s Criteria
Major Criteria
Blood culture positive for IE:
Typical microorganisms consistent with IE from two separate blood cultures:
Viridans streptococci, S. bovis, HACEK group, S. aureus, or community-acquired enterococci in the absence of a primary focus, or Microorganisms consistent with IE from persistently positive blood cultures, defined as follows:
At least two positive cultures of blood samples drawn greater than 12 hours apart, or All of three or a majority of four separate cultures of blood (with first and last sample drawn at least 1 hour apart)
Single positive blood culture for C. burnetii or antiphase I IgG antibody titer greater than 1:800
Evidence of endocardial involvement:
Echocardiogram positive for IE (TEE recommended in patients with prosthetic valves, rated at least “possible IE” by clinical criteria, or complicated IE [paravalvular abscess] TTE as first test in other patients), defined as follows:
Oscillating intracardiac mass on valve or supporting structures, in the path of regurgitant, or on implanted material in the absence of an alternative anatomic explanation, or
Abscess, or
New partial dehiscence of prosthetic valve
New valvular regurgitation (worsening or changing of pre-existing murmur not sufficient)
Minor Criteria
Predisposition, predisposing heart condition or injection drug use
Fever, temperature greater than 38°C (100.4°F)
Vascular phenomena, major arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, and Janeway’s lesions
Immunologic phenomena: glomerulonephritis, Osler’s nodes, Roth’s spots, and rheumatoid factor
Microbiological evidence: positive blood culture but does not meet a major criterion as noted abovea or serological evidence of active infection with organism consistent with IE
2B. Modified Duke’s Criteria for the Diagnosis of IE
Definite IE
Pathologic criteria:
(1) Microorganisms demonstrated by culture or histologic examination of a vegetation that has embolized, or an intracardiac abscess specimen, or
(2) Pathologic lesions; vegetation or intracardiac abscess confirmed by histologic examination showing active endocarditis
Clinical criteriab:
(1) Two major criteria, or
(2) One major criterion and three minor criteria, or
(3) Five minor criteria
Possible IE
(1) One major criterion and one minor criterion, or
(2) Three minor criteria
Rejected
(1) Firm alternate diagnosis explaining evidence of IE, or
(2) Resolution of IE syndrome with antibiotic therapy for less than or equal to 4 days, or
(3) No pathologic evidence of IE at surgery or autopsy, with antibiotic therapy for less than or equal to 4 days, or
(4) Does not meet criteria for possible IE, as above
CNS, coagulase-negative staphylococci; TEE, transesophageal echocardiography; TTE, transthoracic echocardiography.
aExcludes single positive cultures for CNS and organisms that do not cause endocarditis.
bSee above for definitions of major and minor criteria.
From Ref. 15, with permission. University of Chicago Press, 2000 by the Infectious Diseases Society of America. All rights reserved.
IE caused by these streptococci typically has a subacute clinical course. The current cure rate is often over 90% unless complications occur, and they do occur in more than 30% of patients.20,21 The majority of viridansstreptococci remain very susceptible to penicillin, with most strains having a minimum inhibitory concentration (MIC) of less than 0.125 mcg/mL.19,22 Organisms with decreased susceptibilities are increasing. Therefore, antibiotic susceptibilities need to be assessed in order to determine the most appropriate treatment regimen.
Staphylococci
Staphylococcal endocarditis is increasing in prevalence, causing a minimum 30% of all cases of IE, with the majority (80–90%) being due to S. aureus (a coagulase-positive stap-hylococci).18,23 This increase in staphylococci has been primarily attributed to expanded use of venous catheters, more frequent valve replacement, and increased IVDU.24 Coagulase-negative staphylococci (CNS) also cause IE; however, these organisms typically infect prosthetic valves or indwelling catheters.25
Historically, S. aureus was considered community acqui-red23; however, now almost half the cases are nosocomial in origin.18 Any patient who is bacteremic with S. aureus is at an increased risk of developing IE. S. aureus also may infect “normal” heart valves (no prior detected valvular disease) in a third of cases.23,24 Therefore, it is imperative to assess these patients adequately for the presence of vegetations. Any heart valve may be affected; however, when the mitral or aortic valve is involved, it often results in extensive systemic infection with a mortality rate of approximately 20% to 65%.16,23When treating S. aureus IE, one must consider whether the isolate displays methicillin resistance, the location of the infection (right or left side), presence of prosthetic valves, and history of IVDU. Despite significant resistance to penicillinase-resistant penicillins (e.g., methicillin and nafcillin), most isolates remain susceptible to vancomycin. However, there is an increasing incidence of S. aureus intermediately resistant or fully resistant to vancomycin.26,27 Fortunately, at this point they are not widespread enough to affect empirical antibiotic selection. Susceptibility reports should be assessed to ensure antibiotic activity.
Over the past decade there has been an increasing emergence of community-acquired methicillin-resistant S. aureus (CA-MRSA) that differs from health care–associated MRSA. This organism tends to be less resistant to many antibiotics with sensitivity to clindamycin, trimethoprim-sulfamethoxazole (TMP-SMX), and minocycline, as well as vancomycin, linezolid, and daptomycin. However, this organism has a virulence gene (Panton-Valentine leukocidin), which produces a toxin causing necrosis. To date this organism primarily causes skin/skin-structure infections or pneumonias (see skin and soft-tissue infections chapter). There have been a limited number of cases of IE caused by CA-MRSA.28 If CA-MRSA is suspected, treatment with vancomycin with or without gentamicin and/or rifampin remains the standard of care.
The predominant coagulase-negative organism causing IE has been S. epidermidis. However, in the past few years, an increase in isolation of another coagulase-negative species (S. lugdunensis) has been noted.29–31 Typically, coagulase-negative staphylococcal IE has a subacute course with numerous complications. Treatment (with or without surgical intervention) is usually successful. On the other hand, S. lugdunensis produces a more virulent infection and, despite similar antibiotic susceptibilities, has a much higher mortality rate.30–32
Enterococci
Enterococci are normal flora of the human GI tract and sometimes found in the anterior urethra. Historically, enterococci were considered part of the streptococci genus but now are separated despite similarities, such as group D classification and causing subacute disease. Frequently affected patients are older males who have undergone genitourinary manipulations or younger females who have had obstetric procedures. Although enterococci are a less common cause of IE, there are two predominant species: Enterococcus faecium and Enterococcus faecalis. E. faecalis is the most common and the more susceptible of the strains. However, enterococci overall are more intrinsically resistant, with enterococcal IE representing one of the most problematic gram-positive infections to treat and cure. Frequently, enterococci display resistance to multiple antibiotics, including penicillins, vancomycin, aminoglycosides, and some of the newer agents (e.g., linezolid or quinupristin/dalfopristin).33
Gram-Negative Organisms
Gram-negative IE is much less common (approximately 2–5%) but is typically much more difficult to treat than gram-positive infections. Fastidious organisms, such as the HACEK group, tend to be seen most commonly, causing 3% of all IE.34 This group consists of Haemophilus spp. (primarily H. paraphrophilus, H. parainfluenzae, and H. aphrophilus), Actinobacillus actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, and Kingella kingae. The clinical presentation of IE by these organisms is subacute, with approximately 50% of patients developing complications. These complications are primarily due to the presence of large, friable vegetations and numerous emboli along with the development of acute congestive heart failure often requiring valve replacement.35,36 It is important to allow cultures sufficient incubation time (often 2–3 weeks) in order to isolate these organisms. Often these organisms may not be isolated on culture and thus present as culture-negative IE.
Other gram-negative organisms, such as Pseudomonas spp., cause IE, especially in IVDUs and patients with prosthetic valves. Additionally, IE may be caused by Salmonella spp., Escherichia coli, Citrobacter spp., Klebsiellaspp., Enterobacter spp., Serratia marcescens, Proteus spp. and Providencia spp.1,37
Gram-negative IE typically has a poor prognosis with high mortality rates (as high as 83%).1 Treatment usually consists of high-dose combination therapy, with valve replacement often a necessity in many patients.
Culture Negative
Negative blood cultures are reported in approximately 5% of confirmed IE cases, often delaying diagnosis and treatment.3,36,38 Sterile cultures may be the result of previous antibiotic use, subacute right-sided disease, slow growth of fastidious organisms, nonbacterial endocarditis (e.g., fungal or intracellular parasitic infections), noninfective endocarditis, or improper collection of blood cultures. If nonbacterial or fastidious organisms are suspected, additional testing is essential. The choice of treatment regimen depends on patient history and risk factors.
Other Organisms
Numerous bacteria, including gram-positive bacilli, unusual gram-negative bacteria, atypical bacteria, and anaerobes, as well as spirochetes, may cause IE, but these infections are rare.34 Some of the more common organisms include Legionella, Coxiella burnetii (Q fever), and Brucella. These rare organisms occur primarily in at-risk patients such as those who have a prosthetic valve or are IVDUs. A comprehensive discussion of these organisms is not feasible for this chapter; for further information, other references sources (particularly references 1–5) should be examined. Treatment of these organisms is difficult, and cure rates are low. Therefore, consulting an infectious diseases specialist is warranted.
Fungi
Fungal endocarditis is quite uncommon but has significant mortality, typically affecting patients who have had cardiovascular surgery, received a prolonged course of broad-spectrum antibiotics, have long-term catheter placement, are immunocompromised, or are IVDUs.10,39 Survival rates have remained poor, at approximately 15%, but improvements (approximately 30%) have been reported owing to advances in diagnosis and treatment.39 The poor prognosis has been attributed to large vegetations, propensity for organism invasion into the myocardium, extensive septic emboli, poor antifungal penetration into the vegetation, and low toxic-to-therapeutic ratio and lack of cidal activity of certain antifungals.39,40 The two most commonly associated organisms are Candida spp. and Aspergillus spp. Lack of clinical studies makes treatment decisions difficult. Typically, combination and/or high-dose therapy in conjunction with surgery is required.
TREATMENT
Therapeutic Considerations
Treatment of IE often is complicated and difficult. Numerous factors involving the vegetation influence the effectiveness of the antimicrobial agents. The vegetation consists of a fibrin matrix (as discussed earlier) that provides an environment where organisms are relatively free to replicate unimpeded, allowing the microbial density to reach very high concentrations (109–1010 CFU/g). Once the organism density has reached this level, the organisms are virtually in a static growth phase. These factors hinder host defenses, as well as the ability of antimicrobials to produce sufficient kill. This is seen often with β-lactams and glycopeptides because their effectiveness can be significantly affected by the bacterial inoculum.
![]() Selection of an appropriate antimicrobial agent must combine characteristics such as the ability to penetrate into the vegetation, the ability to achieve adequate drug concentrations, and the ability to be minimally affected by high bacterial inoculum in order to achieve adequate kill rates.
Selection of an appropriate antimicrobial agent must combine characteristics such as the ability to penetrate into the vegetation, the ability to achieve adequate drug concentrations, and the ability to be minimally affected by high bacterial inoculum in order to achieve adequate kill rates. ![]() To accomplish this, antimicrobials typically have to be given parenterally at high doses with an extended treatment course of 4 to 6 weeks (in most cases). Other desirable drug characteristics include bactericidal and synergistic activity.
To accomplish this, antimicrobials typically have to be given parenterally at high doses with an extended treatment course of 4 to 6 weeks (in most cases). Other desirable drug characteristics include bactericidal and synergistic activity.
Empirical Therapy
![]() The overall goal of therapy is to eradicate the infection and minimize/prevent any complications. Patients with suspected IE should be evaluated for risk factors that may provide some indication as to the most likely organism causing the infection. If no risk factors can be determined, empirical therapy should primarily cover gram-positive organisms. Generally, if streptococci are suspected, empirical treatment should consist of penicillin plus gentamicin. However, if staphylococci or enterococci are suspected, empirical treatment should consist of vancomycin plus gentamicin. It is important to monitor the patient s response to therapy closely until cultures and susceptibilities are determined to ensure adequate treatment.
The overall goal of therapy is to eradicate the infection and minimize/prevent any complications. Patients with suspected IE should be evaluated for risk factors that may provide some indication as to the most likely organism causing the infection. If no risk factors can be determined, empirical therapy should primarily cover gram-positive organisms. Generally, if streptococci are suspected, empirical treatment should consist of penicillin plus gentamicin. However, if staphylococci or enterococci are suspected, empirical treatment should consist of vancomycin plus gentamicin. It is important to monitor the patient s response to therapy closely until cultures and susceptibilities are determined to ensure adequate treatment.
Specific Therapy
The American Heart Association (AHA) has published guidelines for the management of IE, including specific treatment recommendations.5 A summary of these treatments for the most common organisms (streptococci, staphylococci, and enterococci) is provided in Tables 74–3 through 74–6. However, for more detailed information (including dosing, length of treatment, etc.) for these organisms or less common organisms, refer to the complete guidelines.5 These guidelines include primary and alternative regimens, as indicated in the treatment tables under strength of recommendation.
Streptococci
Most isolates are highly susceptible to penicillin; therefore, penicillin G remains the regimen of choice. However, ceftriaxone may be used as an alternative agent if the patient is allergic or resistance is suspected to penicillin. Typically, the length of treatment is 4 weeks and remains the most common regimen. However, a shorter course (i.e., 2 weeks) may be employed for a patient with uncomplicated IE due to highly penicillin-susceptible strains with no extracardiac infection or whose creatinine clearance is greater than 20 mL/min. If the shorter length of therapy is chosen, gentamicin should be added to the previous regimens for the entire course (i.e., 2 weeks). Recommended therapies for highly penicillin-susceptible viridans streptococci are summarized in Table 74–3.
Patient Encounter, Part 2: Medical History, Physical Examination, and Diagnostic Tests
PMH: Type II diabetes mellitus since age 48; admits that his diet prevents his diabetes from being well controlled; coronary artery disease; cardiac pacemaker since 1998
FH: Father had a history of diabetes and died at age 72 with end-stage renal disease; mother died at age 75 from complications of a broken hip
SH: Smokes about half a pack of cigarettes per day. Initially denied use of alcohol of illicit drugs—now states that he has used illicit IV drugs in the past
Meds: Metformin 850 mg orally three times daily; sotalol 80 mg orally twice daily
Allergies: NKDA
ROS: Recent weight loss of 2. 3 kg (5 lb), decreased appetite, significant fatigue × 2 weeks
PE:
VS: BP 168/89 mm Hg, P 88 bpm, RR 19 breaths per minute, T 38.5°C (101.3°F)
CV: Slight tachycardia, positive murmur
Abd: Obese, soft, nontender, nondistended; (+) bowel sounds
Labs: Within normal limits, except WBC = 16.4 × 103/mm3
(16.4 × 109/L)
Four sets of blood cultures were drawn. Two sets were drawn on admission and two sets were drawn about 12 hours later when the patient spiked a fever. Results are pending.
Diagnostic Tests
A transthoracic echocardiogram (TTE) has been ordered.
Results are pending.
Given this additional information, what is your assessment of the patient’s condition?
Identify your empirical treatment recommendations for this patient.
What other information would be beneficial to obtain?
As penicillin MICs increase (greater than 0.12 mcg/mL but less than or equal to 0.5 mcg/mL) for viridans group streptococci, treatment doses are increased, and 4 weeks of treatment is suggested. In addition, combination therapy with gentamicin is recommended during the first 2 weeks. In patients who are allergic or intolerant to either of the β-lactams, vancomycin is an alternative treatment option. Additionally, in patients with resistant strains of viridansgroup streptococci (MIC greater than 0.5 mcg/mL), treatment should employ antimicrobial agents for enterococcal IE (precise agents determined by the susceptibility report).
Patient Encounter, Part 3: Additional Laboratory and Diagnostic Tests
Blood Cultures: All cultures are positive for viridans group streptococci.
Labs: Within normal limits
Echo: 3-mm vegetation on the tricuspid valve
Given this additional information, are there any changes in your assessment of the patient?
How would you tailor your treatment based on these new data?
What would be your treatment goals, including length of treatment?
What other information would be beneficial to have?
Patients with PVE caused by penicillin-susceptible strains of viridans streptococci require treatment for 6 weeks with penicillin G or ceftriaxone with or without gentamicin during the initial 2 weeks of therapy. However, if the organism demonstrates less susceptibility to penicillin (MIC greater than 0.12 mcg/mL), a combination therapy with penicillin G or ceftriaxone plus gentamicin should be given for the entire 6 weeks. Vancomycin remains the primary alternative if the patient is allergic to β-lactams (e.g., penicillins, cephalosporins, etc.).
Staphylococci
It is important to determine (a) whether the isolate is methicillin-susceptible or methicillin-resistant and (b) whether the patient has a prosthetic valve. For patients with no prosthetic material, methicillin-susceptible staphylococci treatment should consist of a penicillinase-resistant penicillin (e.g., nafcillin or oxacillin) with or without gentamicin, and for methicillin-resistant strains, therapy should consist of vancomycin (see Table 74–4). Combination therapy with aminoglycosides, when used in these patients, typically is given only during the first 3 to 5 days of therapy. In the absence of prosthetic material, some treatment guidelines do not recommend combination therapy against MRSA. However, many clinicians may combine either gentamicin or rifampin with vancomycin if the patient is unresponsive to monotherapy.
Increasing resistance of staphylococci necessitates the expanded use of alternative therapies. A recent clinical study demonstrated similar activity for daptomycin compared to standard therapy (i.e., penicillinase-resistant penicillin for methicillin-sensitive S. aureus (MSSA) or vancomycin for MRSA) in staphylococcal IE.41 The FDA, based on this study, has approved an indication of daptomycin for the treatment of right-sided IE or bacteremia caused by S. aureus. Recommended dosing for these indications are 6 mg/kg/day (unless renal adjustments are necessary).41 This study along with another retrospective study reported daptomycin safe and well tolerated.41,42 Additionally, other antibiotics, such as linezolid and quinupristin/dalfopristin, have been used in patients who were unresponsive to standard therapy, although they have had variable response rates.43–45 These therapies often are reserved for patients who have been unresponsive to traditional therapy (e.g., β-lactams or vancomycin) or for organisms that remain susceptible to these agents when resistant to traditional therapy.
Table 74–3 Therapy of Native-Valve Endocarditis Caused by Highly Penicillin-Susceptible Viridans Group Streptococci and S. bovis
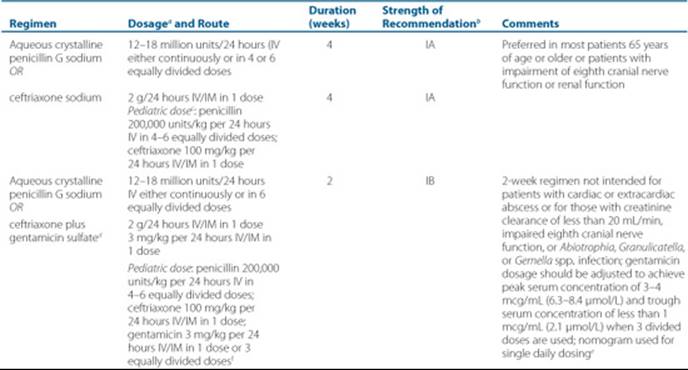
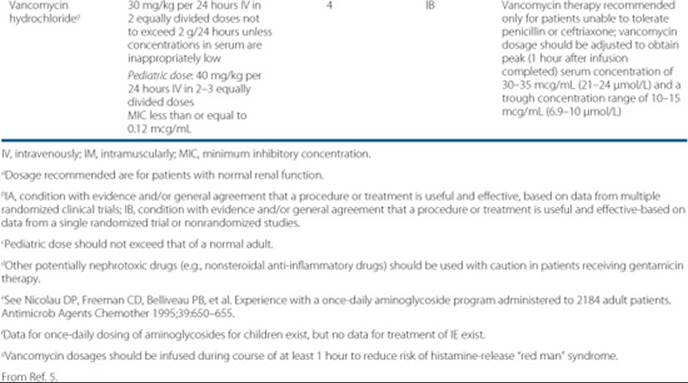
Table 74–4 Therapy for Endocarditis Caused by Staphylococci in the Absence of Prosthetic Materials
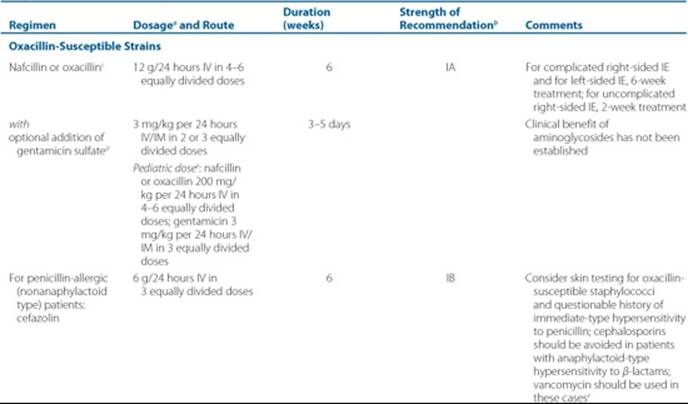
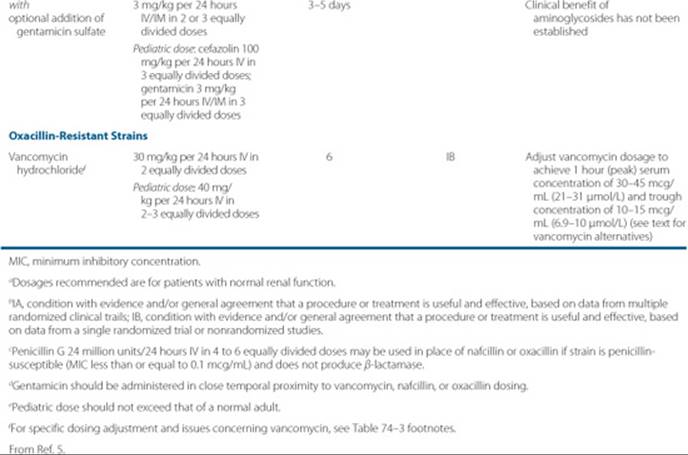
Table 74–5 Therapy for PVE Caused by Staphylococci
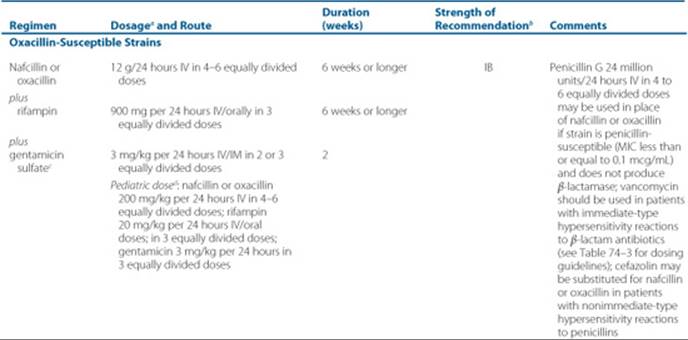
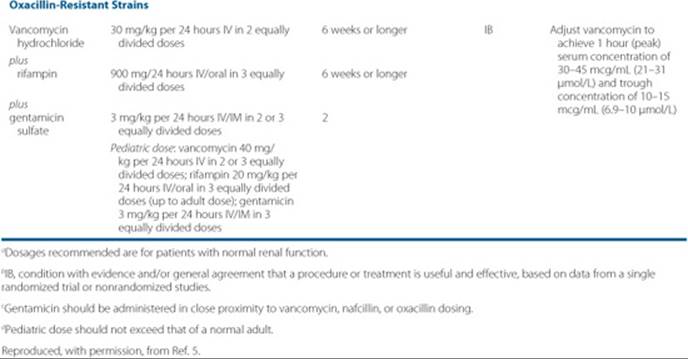
For staphylococcal PVE, treatment length increases significantly, typically requiring a minimum of 6 weeks (see Table 74–5). For MSSA, a penicillinase-resistant penicillin is still employed, as well as vancomycin for MRSA. However, with either regimen, the addition of both gentamicin for first 2 weeks and rifampin for the entire length of treatment is recommended.
Table 74–6 Therapy for Native-Valve or Prosthetic-Valve Enterococcal Endocarditis Caused by Strains Susceptible to Penicillin, Gentamicin, and Vancomycin
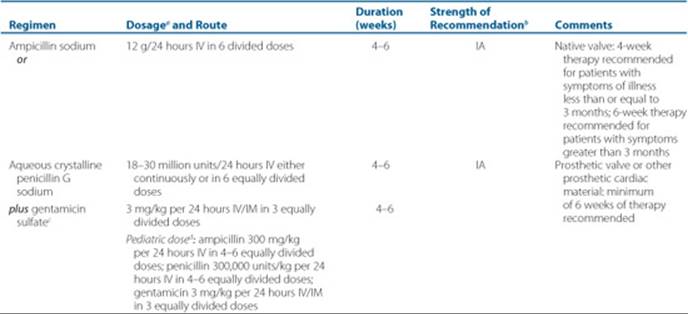
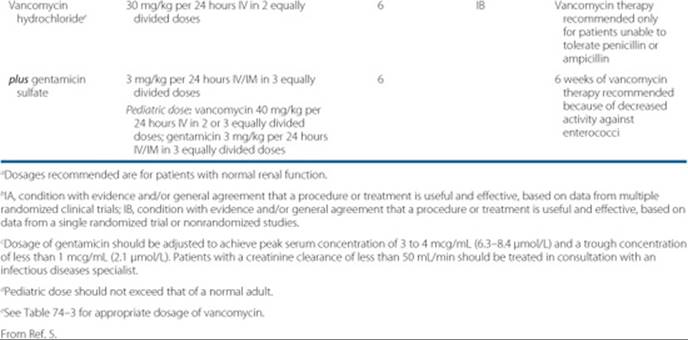
Enterococci
For enterococci, it is imperative to determine species and antibiotic susceptibilities. If the organism is susceptible to penicillin and vancomycin, treatment may consist of highdose penicillin G, ampicillin, or vancomycin plus gentamicin (see Table 74–6). Treatment length is usually 4 to 6 weeks, with the aminoglycoside used over the entire course. As resistance develops to penicillin, ampicillin and vancomycin remain treatment options. Once the isolate becomes resistant to ampicillin, vancomycin is considered the treatment of choice.
If the isolate is determined to be vancomycin-resistant, it is most important to know the exact species because some of the treatment options, such as quinupristin/dalfopristin, are not active against E. faecalis. Currently, the treatment options for vancomycin-resistant enterococci (VRE) are not well established by clinical studies or patient experience. The treatment recommendations for vancomycin-resistant E. faecium include linezolid or quinupristin/dalfopristin for a minimum of 8 weeks. However, newer agents, such as daptomycin, may provide another option for treatment for either enterococci species (E. faecium and E. faecalis). Additionally, guidelines suggest the use of imipenem-cilistatin plus ampicillin or ceftriaxone plus ampicillin for the treatment of E. faecalis with a minimum of 8 weeks of therapy. Consultation with an infectious diseases specialist is recommended.
Gram-Negative Organisms
Identification of the exact isolate is crucial in gram-negative IE because treatment decisions depend on which organism is isolated. Therapy is usually targeted to the most susceptible antibiotics. Combination therapy (usually the addition of an aminoglycoside) is commonly used. For example, Pseudomonas spp. are treated with an antipseudomonal (e.g., piperacillin, cefepime, imipenem, etc.) plus high-dose aminoglycoside (typically tobramycin 8 mg/kg/day). However, exact dosing of antibiotics depends on the organism isolated. Length of treatment is usually a minimum of 6 weeks.
HACEK Group
The HACEK group is difficult to isolate, often taking weeks for identification. If one of these organisms is suspected (e.g., subacute disease, embolism, large vegetations, etc.), it is important to initiate appropriate empirical treatment. The preferred regimen is ceftriaxone (or another third- or fourth-generation cephalosporin), followed by ampicillin-sulbactam. However, for patients who are intolerant of these treatments, ciprofloxacin may be used. The length of treatment typically is 4 weeks for these organisms.
Culture-Negative
Treatment for culture-negative IE presents a significant dilemma. Therapeutic regimens are guided by specific isolated organisms. When cultures fail to identify a specific organism, decisions regarding treatment should cover the most common causative organisms. If the patient is unresponsive to this initial treatment, then additional coverage for less common organisms is warranted. An infectious diseases specialist should be consulted for managing a patient with this type of infection.
Fungi
Treatment of fungal IE is exceptionally difficult. There is a significant lack of studies to identify and recommend the most appropriate therapy. Currently, amphotericin B is the most common treatment. However, valve replacement surgery is often considered an adjunct therapy. IV antifungal therapy requires high doses for a minimum of 8 weeks of treatment. Oral azoles (e.g., fluconazole) are used as long-term suppressive therapy to prevent relapse. The exact role of some of the newer antifungals (e.g., voriconazole and caspofungin) is unknown, but they should provide a viable option.46,47
Surgery
Surgical intervention has become an integral therapy in combination with pharmacologic management of IE. Valve replacement is the predominant intervention, and it is used in a minimum of 25% for all cases of IE.1 Surgery may be indicated if the patient has unresolved infection, ineffective antimicrobial therapy (often associated with fungal IE), more than one episode of serious emboli, refractory congestive heart failure, significant valvular dysfunction, a mycotic aneurysm requiring resection, local complications (perivalvular or myocardial abscesses), or a prosthetic-valve infection associated with a pathogen that demonstrates higher antimicrobial resistance (e.g., staphylococci, gram-negative organisms, and fungi).40,48,49 Often a patient’s hemodynamic status (i.e., blood pressure, heart rate, pulmonary artery pressure, etc.) is used to determine when surgical intervention is warranted.50 Despite appropriate medical management and cure, a significant number of people who develop native-valve endocarditis require valve replacement surgery. Involvement of the aorta is considered an indication for surgery in over 70% of patients with PVE.50
Dosing Considerations
The majority of antibiotic and antifungal agents used for the treatment of IE require dosing modifications based on renal or hepatic function. However, the most closely monitored is vancomycin and aminoglycosides. This is due in part because (a) therapeutic levels are normally monitored, and (b) the increased likelihood of developing toxicities (i.e., nephrotoxicity) if the level is too high or adverse outcomes (i.e., clinical failure or resistance development) if level is too low. General dosing considerations are included in Table 74–7 for the most commonly used drugs for treating IE. However, specific dosing adjustments for individual patients should be determined by referring to an appropriate drug dosing reference.
Patient Encounter, Part 4: Additional Laboratory
Susceptibility Report

Given this additional information, are there any changes in your assessment of the patient?
Do you need to adjust your treatment regimen based on these data?
Would your treatment goals, particularly length of treatment, change?
Prophylaxis
![]() Certain conditions have been associated more commonly with IE due to pre-existing cardiac disease in the presence of a transient bacteremia. In an effort to prevent the development of IE, prophylactic treatment generally is considered appropriate for these at-risk patients. Although there are no well-controlled clinical studies of these recommendations, it is thought that if antibiotics are given just prior to a procedure, the number of bacteria may be decreased in the bloodstream and prevent the bacteria from adhering to the valves.
Certain conditions have been associated more commonly with IE due to pre-existing cardiac disease in the presence of a transient bacteremia. In an effort to prevent the development of IE, prophylactic treatment generally is considered appropriate for these at-risk patients. Although there are no well-controlled clinical studies of these recommendations, it is thought that if antibiotics are given just prior to a procedure, the number of bacteria may be decreased in the bloodstream and prevent the bacteria from adhering to the valves.
Patient Encounter, Part 5: Create a Care Plan
Based on this patient’s information, create a care plan for the management of his IE. Be sure to include
(a) a statement regarding treatment requirements and/or possible problems, (b) goals of therapy, (c) a patient-specific plan, including preventive plans, and (d) a follow-up plan to assess whether the goals have been met and to determine whether the patient experienced any adverse effects.
Cardiac conditions in which prophylaxis is reasonable include presence of prosthetic valves or material, prior IE, congenital cardiac disease (specific forms only), cardiac transplant patients with cardiac valvulopathy (Table 74–8).7 While many patients have other cardiac dysfunction, only patients with these conditions are considered to be at a high risk of developing IE. No prophylaxis is advised in other patients.
Transient bacteria may occur due to many types of dental and surgical procedures. However, the AHA has recently published new guidelines significantly limiting the types of procedures where prophylaxis is appropriate. Only dental procedures involving manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa are considered to increase the likelihood that high-risk patients will develop IE.7 Viridans group streptococci are the primary bacteria targeted for prophylaxis in this circumstance. On the other hand, prophylaxis for GI or genitourinary surgeries primarily targets enterococci.
Table 74–7 Dosage Considerations for Standard Antibiotics for Treatment of IEa
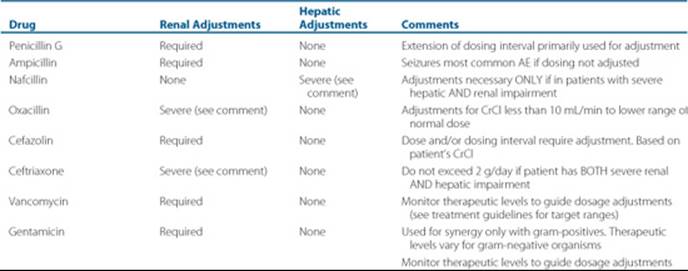
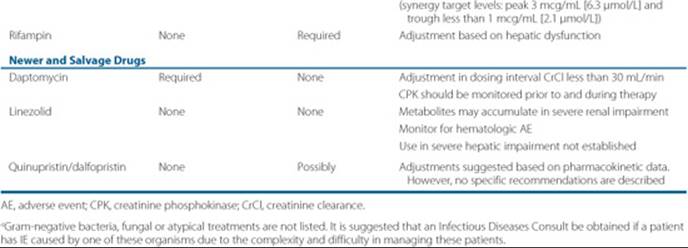
Table 74–8 Cardiac Conditions Associated With the Highest Risk of Adverse Outcome From Endocarditis for Which Prophylaxis With Dental Procedures Is Reasonablea
Prosthetic cardiac valve or prosthetic material used for cardiac-valve repair
Previous IE
CHDb
Unrepaired cyanotic CHD, including palliative shunts and conduits
Completely repaired congenital heart defect with prosthetic material or device, whether placed by surgery or by catheter intervention, during the first 6 months after the procedurec
Repaired CHD with residual defects at the site or adjacent to the site of a prosthetic patch or prosthetic device (which inhibit endothelialization)
Cardiac transplantation recipients who develop cardiac valvulopathy
CHD, congenital heart disease.
aAll dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa is reasonable to give prophylaxis in the patient conditions listed above.
bExcept for the conditions listed above, antibiotic prophylaxis is no longer recommended for any other form of CHD.
cProphylaxis is reasonable because endothelialization of prosthetic material occurs within 6 months after the procedure.
From Ref. 7. Copyright 2007, American Heart Association. All rights reserved.
Table 74–9 Prophylactic Regimens for Denta Procedure
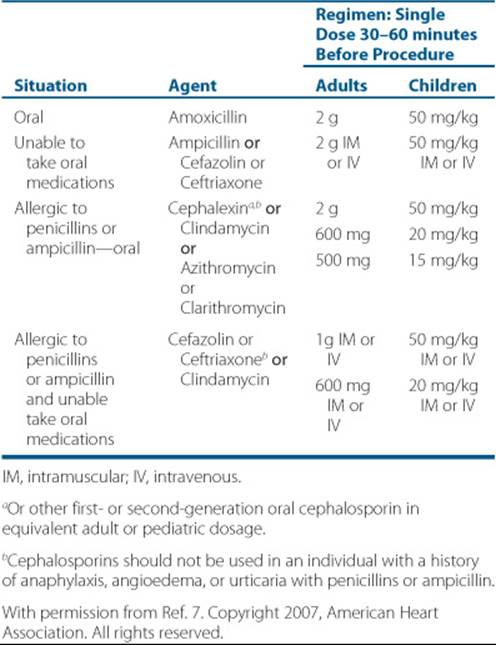
The AHA guidelines include suggested antibiotic regimens for dental procedures where prophylaxis is warranted.7 Recommended regimens for dental procedures are listed in Table 74–9. These guidelines recommend a single oral or intramuscular/IV dose initiated shortly before the procedure. The regimen for dental procedures consists primarily of a penicillin as first choice, with a cephalosporin for nonanaphylactic penicillin-allergic patients and clindamycin or a macrolide for penicillin-allergic patients. A second prophylactic dose is not recommended. However, if an infection develops at the procedure site, additional antibiotics (i.e., a therapeutic course) may be required.
OUTCOME EVALUATION
Monitoring for successful therapy is critical in this serious infection to prevent complications, prevent resistance development, and decrease mortality. Routine assessment of clinical signs and symptoms, as well as laboratory tests (i.e., repeat blood cultures), microbiologic testing, and serum drug concentrations (if appropriate), must be performed.
Resolution of signs and symptoms typically occurs within a few days to a week in most cases. Monitor the patient daily for febrile episodes, as well as other vital signs, with expected normal values within 2 to 3 days of initiating antimicrobial therapy.3 Persistent signs or symptoms could be indicative of inadequate treatment or development of resistance.
Blood cultures are the primary laboratory evaluation to assess response to therapy. Typically, with appropriate treatment, they should become negative within 3 to 7 days. Use subsequent blood cultures if the patient appears not to be responding to therapy or on completing treatment to confirm eradication of infection. Evaluate all susceptibility reports to assess antimicrobial therapy.
Additionally, the patient needs to be counseled on the necessity of prophylactic antibiotics prior to major dental treatments (in appropriate patients) in order to prevent recurrent infections. This is critical in patients with risk factors that predispose them to developing IE, such as prosthetic heart valves, other valvular defects, or previous IE.
Develop a follow-up plan to determine whether the patient has achieved a cure, which includes a clinical evaluation of signs/symptoms, repeat blood cultures, and possibly a repeat echocardiogram. The patient should also be assessed for any adverse events. This should be performed usually within a few weeks after the completion of therapy.
![]() Patient Care and Monitoring
Patient Care and Monitoring
1. Assess the patient’s symptoms and/or laboratory results to determine if the empirical therapy is effective. Is the patient’s fever resolving? Is the patient’s WBC decreasing?
2. Review available microbiologic cultures and sensitivity to assess whether the initial antimicrobial regimen needs to be tailored?
3. Review any additional diagnostic tests to determine if treatment may be needed to prevent/minimize complications (e.g., emboli, congestive heart failure).
4. Evaluate therapeutic serum drug concentrations as appropriate (e.g., vancomycin and gentamicin).
5. Monitor serum creatinine in order to make appropriate renal adjustments of the antimicrobials as necessary.
6. Assess any repeat blood cultures and vital signs to determine continued treatment effectiveness.
7. Evaluate the patient for occurrence of any adverse drug reactions and possible drug allergies and/or drug interactions.
8. Develop a plan if the patient is going to continue therapy at home. Once defervescence has occurred, the patient may complete therapy outside the hospital by receiving the antimicrobials from an outpatient infusion center or through a home health agency.
9. Develop a follow-up plan to assess the resolution of infection once the patient has completed therapy. Assessment of any adverse events also should be conducted at this time.
10. Educate high-risk patients on the importance of taking prophylactic antibiotics prior to having certain dental procedures in an effort to prevent the future development of another infection. Stress the potential complications as well as the morbidity and mortality that are associated with IE and that taking precautions can minimize or prevent them.
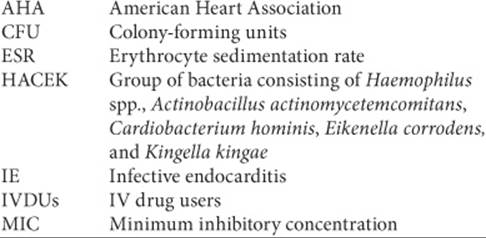
Abbreviations Introduced in This Chapter
 Self-assessment questions and answers are available at http://www.mhpharmacotherapy.com/pp.html.
Self-assessment questions and answers are available at http://www.mhpharmacotherapy.com/pp.html.
REFERENCES
1. Fowler VG Jr, Scheld WM, Bayer AS. Endocarditis and intravascular infections. In: Mandell GL, Bennett JE, Dolin R, eds. Principles and Practice of Infectious Diseases, 6th ed. Philadelphia: Elsevier, 2005:975–1022.
2. Bayer AS, Bolger AF, Taubert KA, et al. Diagnosis and management of infective endocarditis and its complications. Circulation 1998;98: 2936–2948.
3. Mylonakis E, Calderwood SB. Infective endocarditis in adults. N Engl J Med 2001;345:1318–1320.
4. Habib B. Management of infective endocarditis. Heart 2006;92: 124–130.
5. Baddour LM, Wilson WR, Bayer AS, et al. American Heart Association Scientific Statement. Infective endocarditis: Diagnosis, antimicrobial therapy, and management of complications. Circulation 2005;111: e394–e433.
6. Millar BC, Moore JE. Emerging issues in infective endocarditis. Emerg Infect Dis 2004;10:110–116.
7. Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: Guidelines from the American Heart Association. Circulation 2007;116:1736–1754.
8. Moreillon P, Que Y. Infective endocarditis. Lancet 2004;363:139–149.
9. Baddour LM, Wilson WR. Infections of prosthetic valves and other cardiovascular devices. In: Mandell GL, Bennett JE, Dolin R, eds. Principles and Practice of Infectious Diseases, 6th ed. Philadelphia: Elsevier, 2005:1022–1044.
10. Karchmer AW. Infective endocarditis. In: Braunwald E, ed. Heart Disease: A Textbook of Cardiovascular Medicine, 6th ed. Philadelphia: Saunders, 2001:1723–1748.
11. Cecchi E, Imazio M, Trinchero R. Infective endocarditis: Diagnostic issues and practical clinical approach based on echocardiography. J Cardiovasc Med 2008;9:414–418.
12. Sachdev M, Peterson GE, Jollis JG. Imaging techniques for diagnosis of infective endocarditis. Cardiol Clin 2003;21:185–195.
13. Di Salvo G, Habib G, Pergola V, et al. Echocardiography predicts embolic events in infective endocarditis. J Am Coll Cardiol 2001;37:1069–1076.
14. Durack DT, Lukes AS, Bright DK Duke Endocarditis Service. New criteria for diagnosis of infective endocarditis: Utilization of specific echocardiographic findings. Am J Med 1994;96:200–209.
15. Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis 2000;30:633–638.
16. Bridger A. Infective endocarditis: New strategies for diagnosis and prophylaxis. JAAPA 2001;14:35–47.
17. Cabell CH, Jollis JG, Peterson GE, et al. Changing patient characteristics and the effect on mortality in endocarditis. Arch Intern Med 2002;162:90–94.
18. Fowler VG Jr., Miro JM, Hoen B, et al. Staphylococcus aureus endocarditis: A consequence of medical progress. JAMA 2005;293:3012–3021.
19. Hoen B. Special issues in the management of infective endocarditis caused by gram-positive cocci. Infect Dis Clin North Am 2002;16:437–452.
20. Ferrieri P, Gewitz MH, Gerber MA, et al. Unique features of infective endocarditis in childhood. Circulation 2002;105:2115–2127.
21. Knoll B, Tleyjeh IM, Steckelberg JM, et al. Infective endocarditis due to penicillin-resistant viridans group streptococci. Clin Infect Dis 2007;44:1585–1592.
22. Upton A, Drinkovic D, Pottumarthy S, et al. Culture results of heart valves resected because of streptococcal endocarditis: Insights into duration of treatment to achieve valve sterilization. J Antimicrob Chemother 2005;55:234–239.
23. Murray RJ. Staphylococcus aureus infective endocarditis: Diagnosis and management guidelines. Intern Med J 2005;35:S25–S44.
24. Petti CA, Fowler VG Jr. Staphylococcus aureus bacteremia and endocarditis. Cardiol Clin 2003;21:219–233.
25. Miele PS, Kogulan PK, Levy CS, et al. Seven cases of surgical native valve endocarditis caused by coagulase-negative staphylococci: An underappreciated disease. Am Heart J 2001;142:571–576.
26. Woods CW, Cheng AC, Fowler VG Jr, et al. Endocarditis caused by Staphylococcus aureus with reduced susceptibility to vancomycin. Clin Infect Dis 2004;38:1188–1191.
27. Centers for Disease Control. Staphylococcus aureus resistant to vancomycin—United States, 2002. MMWR 2002;51:565–567.
28. Millar BC, Prendergast BD, Moore JE. Community-associated MRSA (CA-MRSA): An emerging pathogen in infective endocarditis. J Antimicrob Chemother 2008;61:1–7.
29. Anguera I, Del Rio A, Miro JM, et al. Staphylococcus lugdunensis infective endocarditis: Description of 10 cases and analysis of native valve, prosthetic valve, and pacemaker lead endocarditis clinical profiles. Heart 2005;91:e10.
30. Van Hoovels L, De Munter P, Colaert J, et al. Three cases of destructive native valve endocarditis caused by Staphylococcus lugdunensis. Eur J Clin Microbiol Infect Dis 2005;24:149–152.
31. Frank KL, Luiz del Pozo J, Patel R. From clinical microbiology to infection pathogenesis: How daring to be different works for Staphylococcus lugdunensis. Clin Microbiol Rev 2008;21:111–133.
32. Burgert SJ. Destructive native valve endocarditis caused by Staphylococcus lugdunensis. South Med J 1999;92:812–814.
33. Linden PK. Optimizing therapy for vancomycin-resistant enterococci (VRE). Semin Respir Crit Care Med 2007;28:632–645.
34. Brouqui P, Raoult D. Endocarditis due to rare and fastidious bacteria. Clin Microbiol Rev 2001;14:177–207.
35. Feder HM Jr., Roberts JC, Salazar JC, et al. HACEK endocarditis in infants and children: Two cases and a literature review. Pediatr Infect Dis J 2003;22:557–562.
36. Naber CK, Erbel R. Diagnosis of culture negative endocarditis: Novel strategies to prove the suspect guilty. Heart 2003;89:241–243.
37. Morpeth S, Murdoch D, Cabell CH, et al. Non-HACEK gram-negative bacillus endocarditis. Ann Intern Med 2007;147:829–835.
38. Houpikian P, Raoult D. Blood culture-negative endocarditis in a reference center: Etiologic diagnosis of 348 cases. Medicine 2005;84:162–173.
39. Ellis ME, Al-Abdely H, Sandridge A, et al. Fungal endocarditis: Evidence in the world literature, 1965–1995. Clin Infect Dis 2001;32:50–62.
40. Pierrotti LC, Baddour LM. Fungal endocarditis, 1995–2000. Chest 2002;122:302–310.
41. Fowler V, Boucher HW, Corey GR, et al. Daptomycin versus standard therapy for bacteremia and infective endocarditis caused by Staphylococcus aureus. N Engl J Med 2006;355:653–665.
42. Segreti JA, Crank CW, Finney MS. Daptomycin for the treatment of gram-positive bacteremia and infective endocarditis: A retrospective case series of 31 patients. Pharmacotherapy 2006;26:347–352.
43. Nathani N, Iles P, Elliott TSJ. Successful treatment of MRSA native valve endocarditis with oral linezolid therapy: A case report. J Infect 2005;51:e213–e215.
44. Corne P, Marchandin H, Macia J-C, Jonquet O. Treatment failure of methicillin-resistant Staphylococcus aureus endocarditis with linezolid. Scand J Infect Dis 2005;37:946–949.
45. Drew RH, Perfect JR, Srinath L, et al. Treatment of methicillin-resistant Staphylococcus aureus infections with quinupristin/dalfopristin in patients intolerant of/or failing prior therapy: For the Synercid Emergency-Use Study Group. J Antimicrob Chemother 2000;46:775–784.
46. Rajendram R, Alp NJ, Mitchell AR, et al. Candida prosthetic valve endocarditis cured by caspofungin therapy without valve replacement. Clin Infect Dis 2005;40:e72–e74.
47. Reis LJ, Barton TD, Pochettino A, et al. Successful treatment of Aspergillus prosthetic valve endocarditis with oral voriconazole. Clin Infect Dis 2005;41:752–753.
48. Sohail MR, Martin KR, Wilson WR, et al. Medical versus surgical management of Staphylococcus aureus prosthetic valve endocarditis. Am J Med 2006;119:147–154.
49. Rivas P, Alonso J, Moya J, et al. The impact of hospital-acquired infections on the microbial etiology and prognosis of late-onset prosthetic valve endocarditis. Chest 2005;128:764–771.
50. Akowuah EF, Davies W, Oliver S. Prosthetic valve endocarditis: Early and late outcome following medical or surgical treatment. Heart 2003;89:269–272.