![]() BACK PAIN, UROLOGIC CONSIDERATIONS
BACK PAIN, UROLOGIC CONSIDERATIONS
DESCRIPTION The differential diagnosis of back pain includes several potential urologic etiologies:
• Cauda equina syndrome is a surgical emergency. Common findings are bladder dysfunction (especially urinary retention) and saddle anesthesia, in addition to sciatica and weakness
• Endocrine: Adrenal hyperplasia or infarction
• Gynecologic: Neoplasm of uterus or ovary, dysmenorrhea, salpingitis, uterine prolapse
• Infectious: Osteomyelitis, subarachnoid or spinal abscess, tuberculosis, meningitis, basilar pneumonia
• Mechanical: Pregnancy, obesity, fatigue, scoliosis
• Medication: Tadalafil-incidence of back pain and/or myalgia in 9.4% in patients receiving tadalafil 10 mg; 8.3% in patients receiving tadalafil 20 mg, and 3.7% in placebo-treated patients.
• Neoplastic: Myeloma, Hodgkin disease, carcinoma of pancreas or adrenal, metastatic neoplasm from breast, prostate, lung
• Renal: Hydronephrosis, calculus, neoplasm, renal infarction, pyelonephritis
• Trauma: Injury to bone, joint, internal organs, or ligament
REFERENCES
Gerber GS, Brendler CB. Evaluation of the urologic patient: history, physical examination, and urinalysis. In: Wein AJ, et al., eds. Campbell-Walsh Urology. 10th ed. Philadelphia, PA: Saunders, 2012:73–98.
Seftel AD, Farber J, Fletcher J, et al. A three-part study to investigate the incidence and potential etiologies of tadalafil-associated back pain or myalgia. Int J Impot Res. 2005;17(5):455–461.
![]() BALANITIS XEROTICA OBLITERANS/LICHEN SCLEROSIS ET ATROPHICUS
BALANITIS XEROTICA OBLITERANS/LICHEN SCLEROSIS ET ATROPHICUS
DESCRIPTION BXO (Balanitis Xerotica Obliterans) is an inflammatory lesion of the glans and foreskin, now considered to be synonymous with lichen sclerosis et atrophicus (LSA). The term BXO is used when the skin of the genitalia is affected. BXO can cause itching and decreased sensitivity in the head of penis, but the hallmark is urethral meatal stenosis or distal urethral stricture. Differential diagnosis includes leukoplakia, Bowen disease (BD), erythroplasia of Queyrat, or squamous cell carcinoma (SCC) of the glans or preputial skin; biopsy is necessary to confirm the absence of malignancy. (See also Section I: “Penis, Cancer, General Considera-tions” and “Penis, Cutaneous Lesion.”)
TREATMENT
• Local therapy with steroid, estrogen, or testosterone cream
• Surgical therapy with circumcision (when appropriate) and flap reconstruction of fossa navicularis for severe cases; meatal or urethral dilation rarely gives durable response
REFERENCE
Clouston D, Hall A, Lawrentschuk N. Penile lichen sclerosis (balanitis xerotica obliterans). BJU Int. 2011;108(Suppl 2):14–19.
![]() BALANITIS, ZOON (PLASMA CELL BALANITIS)
BALANITIS, ZOON (PLASMA CELL BALANITIS)
DESCRIPTION Also called balanoposthitis chronica circumscripta plasma cellularis and plasma cell balanitis. Can be confused clinically with erythroplasia of Queyrat. Grossly, it appears as a shiny, glazed-red macular erythematous lesion with multiple, pinpoint, bright red “cayenne pepper” spots. Histologically, a subepidermal inflammatory infiltrate of plasma cells and dermal red cell extravasation is present. No malignant transformation is reported. Proposed etiologies include Mycobacterium smegmatis, heat, poor hygiene, or constant friction. Treated by circumcision.
REFERENCE
Weyers W, Ende Y, Schalla W, et al. Balanitis of Zoon: A clinicopathologic study of 45 cases. Am J Dermatopathol. 2002;24(6):459–467.
![]() BALKAN NEPHROPATHY
BALKAN NEPHROPATHY
DESCRIPTION An interstitial nephropathy endemic to the Balkan Republics of Yugoslavia, Bulgaria, and Romania, and that afflicts mainly the middle-aged rural populations. It is slowly progressive, and may eventually end in ESRD. Anemia, proteinuria, and hypertension can be severe. Renal biopsy has no specific markers for the disease. Balkan endemic nephropathy is caused by eating bread that is contaminated with a toxin called aristolochic acid, which comes from a plant called Aristolochia. Balkan endemic nephropathy can occur in multiple family members, but it is not an inherited condition. A strong association with increased incidence of upper tract transitional cell carcinoma (TCC) has been documented, although bladder TCC incidence is normal. Treatment involves aggressive surveillance for TCC and renal replacement therapy, as necessary. (See also Section II: “Aristolochic acid [fang chi].”)
REFERENCE
Stefanovic V, Polenakovic M. Fifty years of research in Balkan endemic nephropathy: Where are we now? Nephron Clin Pract. 2009;112(2):51–56.
![]() BANFF CLASSIFICATION, TRANSPLANT REJECTION
BANFF CLASSIFICATION, TRANSPLANT REJECTION
DESCRIPTION A classification method developed in 1993 for standardization of criteria in the histologic diagnosis of renal allograft rejection. The Banff classification characterizes renal biopsy findings into a scheme that outlines possible clinical approaches to manage the rejection. (See also Section I: “Transplant Rejection, Renal.”)
REFERENCE
Solez K, Racusen LC. The Banff classification revisited. Kidney Int. 2013;83(2):201–206.
![]() BARCAT-REDMAN HYPOSPADIAS REPAIR
BARCAT-REDMAN HYPOSPADIAS REPAIR
DESCRIPTION In a modification of the Mathieu procedure, this repair mobilizes the posterior urethral plate and splits the glans in addition to the parameatal flap. The full-thickness parameatal and urethral plate grafts are tubularized together and laid to rest in the new urethral groove.
REFERENCE
Snodgrass WT. Hypospadias. In: Wein AJ, et al., eds. Campbell-Walsh Urology. 10th ed. Philadelphia, PA: Saunders, 2012:3503–3536.
![]() BARIATRIC SURGERY, UROLOGIC CONSIDERATIONS
BARIATRIC SURGERY, UROLOGIC CONSIDERATIONS
DESCRIPTION Jejunoileal bypass, the 1st bariatric procedure, produced severe hyperoxaluria secondary to steatorrhea. Modern bariatric surgery utilizes gastric restrictive procedures and sometimes bypass of variable amounts of small intestine, such as a Roux-en-Y gastric bypass and biliopancreatic diversion. Modern bariatric surgery is associated with less malabsorption compared to jejunoileal bypass; however, contemporary bariatric bypass patients continue to have hyperoxaluria, hypocitruria, and lower urine volumes, which result in an increased risk of calculus formation.
REFERENCE
Tasca A. Metabolic syndrome and bariatric surgery in stone disease etiology. Curr Opin Urol. 2011;21:129–133.
![]() BARTTER SYNDROME
BARTTER SYNDROME
DESCRIPTION Congenital abnormality that usually presents in childhood with metabolic acidosis, hyperreninemic hyperaldosteronism, and hypokalemia. Presenting symptoms are muscle weakness, polyuria, and sometimes growth retardation. Patients are normotensive. Renal biopsy reveals juxtaglomerular hyperplasia. Defective platelet aggregation and decreased vascular responsiveness to pressors are also noted. Pathophysiology includes decreased sodium transport in the thick ascending loop of Henle; decreased vascular responsiveness and increased prostaglandin secretion may also play a role. This condition is incurable; potassium supplementation, prostaglandin synthesis inhibitors, aldosterone antagonists, and ACE inhibitors can help greatly to ameliorate symptoms.
REFERENCE
Fremont OT, Chan JC. Understanding Bartter syndrome and Gitelman syndrome. World J Pediatr. 2012;8(1):25–30.
![]() BASHFUL BLADDER (PARURESIS, SHY BLADDER SYNDROME, “PEE-SHY”)
BASHFUL BLADDER (PARURESIS, SHY BLADDER SYNDROME, “PEE-SHY”)
DESCRIPTION This is the inability to urinate with others present, such as in a public restroom. It is a relatively common disorder but little is understood about the phobia. According to DSM-IV TR, this disorder is classified as social phobia.
REFERENCE
Hammelstein P, Soifer S. Is “shy bladder syndrome” (paruresis) correctly classified as social phobia? Anxiety Disord. 2006;20(3):296–311.
![]() BCG REFRACTORY TRANSITIONAL CELL CARCINOMA (TCC)
BCG REFRACTORY TRANSITIONAL CELL CARCINOMA (TCC)
DESCRIPTION TCC that recurs after treatment with intravesical BCG treatment. Failure of initial intravesical therapy may be managed by further intravesical therapy or cystectomy, with more aggressive therapy indicated for high-risk patients having superficial invasion (T1), high-grade lesions or concomitant carcinoma in situ (CIS). Patients with high-risk features who fail a 2nd course of BCG have a very high risk of progression to muscle-invasive TCC. In addition, relapses after ≥2 courses of BCG appear to be associated with poor outcomes, despite subsequent aggressive therapy. Several different salvage therapies, including intravesical interferon alone or in combination with BCG, valrubicin, mitomycin C, gemcitabine, and other chemotherapeutic agents, as well as photodynamic therapy, have been described for BCG failures. Salvage therapies have poor response rates, however, and radical cystectomy remains the “gold standard” for the salvage of failed intravesical therapy in high-risk patients. (See Also Section I: “Bladder Cancer, General.”)
REFERENCE
Sengupta S, Blute ML. The management of superficial transitional cell carcinoma of the bladder. Urology. 2006;67(3 Suppl 1):48–54.
![]() BCL-2, UROLOGIC CONSIDERATIONS
BCL-2, UROLOGIC CONSIDERATIONS
DESCRIPTION The protein product of the gene bcl-2 acts as an apoptosis-blocking agent. It appears to be required for normal morphogenesis of the kidney, and may be unimportant as a prognostic factor in RCC. It is seen in higher levels in prostatic intraepithelial hyperplasia but is variable in prostate cancer. Levels increase during XRT. Expression is increased in high-grade bladder tumors.
REFERENCE
King ED, Matteson J, Jacobs SC, et al. Incidence of apoptosis, cell proliferation and bcl-2 expression in transitional cell carcinoma of the bladder: Association with tumor progression. J Urol.1996;155(1):316–320.
![]() BECKWITH–WIEDEMANN SYNDROME
BECKWITH–WIEDEMANN SYNDROME
DESCRIPTION This condition is characterized by macroglossia, abdominal wall defects, adrenal cytomegaly, and neonatal hypoglycemia. Other characteristic features include gigantism, earlobe creases and pits, facial nevus flammeus, and prominent eyes with infraorbital creases. Neonatal hypoglycemia is frequent, of which Wilms tumor, adrenal cortical carcinoma, and hepatoblastoma are most common. Mental retardation is not associated. Most cases are sporadic, but a genetic cause related to mutation or deletion of imprinted genes within the chromosome 11p15.5 region. The mode of inheritance of BWS is complex. Possible patterns include autosomal dominant inheritance with variable expressivity, contiguous gene duplication at 11p15, and genomic imprinting resulting from a defective or absent copy of the maternally derived gene. Several lines of evidence suggest that BWS may be caused by relative overexpression of the maternally imprinted IGF2 gene. Some suggest a slightly increased risk in babies born by assisted reproduction. Close follow-up early in life is recommended for tumor surveillance as 1 of the most ominous findings is the increased risk of neoplasia. In 1 series the majority of tumors were Wilms tumors (67%), followed by hepatoblastomas (11%), rhabdomyosarcomas (5%), and neuroblastomas (4%).
SYNONYM
EMG syndrome (exomphalos, macroglossia, and gigantinism)
REFERENCES
Online Mendelian Inheritance in Man; http://www.omim.org/entry/130650. Accessed March 1, 2014.
Weng EY, Mortier GR, Graham JM Jr. Beckwith-Wiedemann syndrome. An update and review for the primary pediatrician. Clin Pediatr. 1995;34(6):317–326.
![]() BEER NEPHROURETERECTOMY
BEER NEPHROURETERECTOMY
DESCRIPTION Refers to a retroperitoneal 2-incision approach to a nephroureterectomy through a flank and a separate Gibson or a midline Czerny incision.
REFERENCE
Bergman H, Lockhart J. Surgery of the ureteral stump. In: Kaufman JJ, eds. Current Urologic Therapy. Philadelphia, PA: Saunders, 1986:212–214.
![]() BEER POTOMANIA
BEER POTOMANIA
DESCRIPTION A hypo-osmolality syndrome of beer drinkers, usually with hyponatremia. Patients with beer potomania have a history of significant beer drinking, often long term, in conjunction with a poor diet. This may occur because beer has very little sodium and no protein, and the condition is potentially augmented by the possibility of inappropriate antidiuretic hormone (ADH) secretion.
TREATMENT
Fluid restriction, ICU monitoring, and serial serum sodium levels, with slow correction of hyponatremia.
REFERENCE
Sanghvi SR, Kellerman PS, Nanovic L. Beer potomania: An unusual cause of hyponatremia at high risk of complications from rapid correction. Am J Kidney Dis. 2007;50:673–680.
![]() BEHÇET DISEASE
BEHÇET DISEASE
DESCRIPTION This is a multisystem vasculitis that is most active during young adulthood syndrome characterized by oral and genital ulcers (vulvar and penile), uveitis, vascular involvement (venous thrombosis, vasculitis), and nonmucous membrane skin lesions of unknown etiology. Lesions on the genitalia are herpetiform and can be painful. Other genital ulcers, such as syphilis, herpes, and chancroid, must be ruled out 1st. Genital ulcers are treated with local moisture-retaining dressings, topical anesthetics, and steroids. Rebamipide is used to treat aphthous ulcers. For severe mucocutaneous lesions, immunosuppressive systemic agents (corticosteroids, azathioprine, pentoxifylline, dapsone, interferon-alfa, colchicine, and thalidomide) have demonstrated benefit.
REFERENCE
Emmi G, Silvestri E, Squatrito D, et al. Behçet’s syndrome pathophysiology and potential therapeutic targets. Intern Emerg Med. 2014;9(3):257–265.
![]() BELLINI DUCT CARCINOMA (COLLECTING DUCT CARCINOMA)
BELLINI DUCT CARCINOMA (COLLECTING DUCT CARCINOMA)
DESCRIPTION A variant of RCC in which the cell of origin is the collecting duct. Very few cases are reported in literature. Immunohistochemically, the lesion stains with high–molecular-weight keratin and lectin. Histologically, cells demonstrate intracyto-plasmic mucicarminophilic material, which is not seen in RCC. Radical nephrectomy for localized disease is the treatment of choice. Chemotherapy is used (interferon-α–based) for metastatic disease. (See also Section I: “Renal Mass.”) (Image ![]() )
)
REFERENCE
Kassouf W, Binsaleh S, Cohen DD, et al. Bellini duct carcinoma with ovarian metastasis. Can J Urol. 2004;11(6):2461–2462.
![]() BELT PROCEDURE
BELT PROCEDURE
DESCRIPTION Named for Dr. Elmer Belt, who described his technique for performing radical perineal prostatectomy in 1939. Dr. Belt described a new approach to the prostate through the perineum, between the longitudinal fibers of the rectum and the circular fibers of the external anal sphincter. This approach dramatically decreased blood loss. However, Dr. Belt also recommended leaving behind the apex of the prostate to achieve better urinary control, and opening the anterior layer of the Denonvillier fascia during the dissection.
REFERENCE
Belt E, Albert CE, Surber AC Jr. A new anatomic approach in perineal prostatectomy. J Urol. 1939;41:482–497.
![]() BENCHEKROUN ILEAL VALVE
BENCHEKROUN ILEAL VALVE
DESCRIPTION A hydraulic ileal valve is used as the continence mechanism in ileal or ileocecal reservoirs. As the reservoir fills, increased pressure occurs in the valve, which is created by invaginating an ileal segment that then serves as the efferent continent limb.
REFERENCE
McKiernan JM, et al. Continent urinary diversion. In: Wein AJ, et al., eds. Campbell-Walsh Urology. 10th ed. Philadelphia, PA: Saunders, 2012:2450–2478.
![]() BERGER DISEASE (IgA NEPHROPATHY)
BERGER DISEASE (IgA NEPHROPATHY)
DESCRIPTION Sometimes referred to as “idiopathic immunoglobulin A nephropathy,” this condition was 1st described by Berger and Hinglas in 1968. As the most common primary glomerulonephritis, it exhibits a wide variation in manifestation, ranging from a benign, indolent course to rapidly progressive renal failure. Commonly presents with hematuria, proteinuria, and abnormal urine sediment. Diagnosed by renal biopsy demonstrating IgA deposits in the mesangium on immunofluorescence staining.
TREATMENT
• Recent promise seen in corticosteroids, fish oil, and ACE inhibitors
• Renal transplant for cases of renal failure
REFERENCE
Cheng J, Zhang X, Tian J, et al. Combination therapy of ACE inhibitor and an angiotensin receptor blocker for IgA nephropathy: A meta-analysis. Int J Clin Pract. 2012;66(10):917–923.
![]() BERGMAN SIGN
BERGMAN SIGN
DESCRIPTION In urologic radiography, the Bergman sign occurs when the ureter is dilated immediately below a neoplasm, rather than collapsed, as below an obstructing stone, thus showing a chalice shape. Retrograde pyelography demonstrates an irregular ureteral filling defect with complete obstruction and distal ureteral dilation, producing the chalice appearance; a ureteral catheter tends to curl in this segment. The Bergman sign is pathognomonic for neoplasm.
REFERENCE
Bergman H, ed. The Ureter. 2nd ed. New York, NY: Springer-Verlag; 1981.
![]() β-hCG (HUMAN CHORIONIC GONADOTROPIN)
β-hCG (HUMAN CHORIONIC GONADOTROPIN)
DESCRIPTION Glycoprotein with a molecular weight of 38,000 and a half-life of 2 days. It is produced normally by the syncytiotrophoblast cells in pregnancy. hCG is composed of 2 subunits, α and β. The β-subunit is identical to a subunit of LH. Urologic uses include staging and follow-up of testicular cancer (elevated in 100% of choriocarcinoma, 7% of seminoma, 60% of embryonal carcinomas). Has been produced by urothelial tumors and secreting polyembryoma. Therapeutically can be given exogenously to stimulate Leydig cells in secondary hypogonadism and facilitate descent of undescended testicles when administered over several weeks. Typical regimen is 500–2,500 U IM 2 times a week for 4 wk. The hCG test is used to diagnose anorchia in underscended testicles; a failure to increase testosterone after administration suggests anorchia. (See also Section I: “Testis, Cancer, General”; Section I: “Testis, Nonseminomatous Germ Cell Tumors, General.”)
REFERENCE
Bower M, Rustin GJ. Serum tumor markers and their role in monitoring germ cell cancers of the testis. In: Vogelzang NJ, et al., eds. Comprehensive Textbook of Genitourinary Oncology. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2000.
![]() BETHANECHOL SUPERSENSITIVITY TEST
BETHANECHOL SUPERSENSITIVITY TEST
DESCRIPTION A historical variation of urodynamic testing wherein bethanechol was administered subcutaneously 20 min before testing. Usually considered when normal bladder contraction is weak or absent. If positive, a rise in filling pressure of >20 cm of water and a shift in the filling curve to the left are noted. A positive test represents bladder denervation. No change during the test represents myogenic damage.
REFERENCE
Snyder JA, Lipsitz DU. Evaluation of female urinary incontinence. Urol Clin North Am. 1991;18(2):197–209.
![]() BEZOARS (FUNGUS BALLS)
BEZOARS (FUNGUS BALLS)
DESCRIPTION Fungal infections of the kidney occur most commonly in the setting of diabetes, immunosuppression, urinary obstruction, or indwelling urinary catheters or stents. Most commonly Candidaspecies such as C. albicans and tropicalis are involved. Other fungi such as Torulopsis glabrata and Aspergillus may cause renal infections, although less commonly. These infections can cause the formation of fungal balls or bezoars, which can be seen on imaging as a renal pelvic mass or filling defect and may cause obstruction; in the bladder, they may cause irritative voiding symptoms. Urinary tract imaging in the setting of candiduria (funguria) is needed in patients who have persistent candiduria and are at increased risk of bezoars (diabetics or other urologic abnormalities). Urinary tract fungal bezoars are managed with a combination of surgical and medical therapy. (See also Section I: “Fungal Infections, Genitourinary”; Section II: “Funguria.”)
TREATMENT
• Treat medically until endoscopic procedure to remove the bezoar has been accomplished, symptoms have resolved, and cultures are negative
• Candida bezoars: Fluconazole (200–400 mg/d [3–6 mg/kg/d] PO)
• Alternative regimen: Amphotericin B (0.5–0.7 mg/kg/d IV) with or without flucytosine (100 mg/d PO divided into 4 doses)
• Aspergillosis bezoars: Use voriconazole load: 6 mg/kg q12h for 2 doses; then maintenance of 4 mg/kg q12h
• With upper tract involvement, amphotericin B mixed 50 mg/L of sterile water by ureteral catheter, or nephrostomy can be considered
REFERENCE
Pappas PG, Kauffman CA, Andes D, et al. Clinical practice guidelines for the management of candidiasis: 2009 update by the Infectious Diseases Society of America. Clin Infect Dis. 2009;48:503.
![]() BIFID RENAL PELVIS
BIFID RENAL PELVIS
DESCRIPTION A term for incomplete ureteral duplication. Bifid renal pelvis indicates that the confluence of 2 separate pyelocalyceal systems is located at the UPJ. If the confluence is inferior to the UPJ but superior to the entry into the bladder, then this would be termed bifid ureters (Image ![]() ).
).
REFERENCE
Decter R. Renal duplication and fusion anomalies. Pediatric Urol. 1997;44;1323–1341.
![]() BIFID SCROTUM
BIFID SCROTUM
DESCRIPTION A congenital anomaly in which the scrotal folds are completely separate. This is generally seen in conjunction with other anomalies, and may be present in CAH and 5α-reductase deficiency, almost always associated with hypospadias.
REFERENCE
Palmer JS. Genitourinary manifestations in boys and girls associated with genetic diseases. J Men’s Health Gend. 2006;3(1):71–79.
![]() BIOFEEDBACK, UROLOGIC CONSIDERATIONS
BIOFEEDBACK, UROLOGIC CONSIDERATIONS
DESCRIPTION Any method of training the body while receiving feedback on the specific function being trained. Biofeedback ranges from “low tech” (eg, vaginal cones for incontinence) to expensive electronic systems (utilizing EMG or pressure probes). Biofeedback is applied in urology for improvement of urinary incontinence, generally by strengthening pelvic floor muscles, and for treatment of dysfunctional voiding. Biofeedback has also been used to teach patients to stop uninhibited detrusor contractions, teach relaxation of the pelvic floor and promote normal voiding in children.
REFERENCE
Bø K, Kvarstein B, Nygaard I. Lower urinary tract symptoms and pelvic floor muscle exercise adherence after 15 years. Obstet Gynecol. 2005;105:999–1005.
![]() BIOFILM, UROLOGIC CONSIDERATIONS
BIOFILM, UROLOGIC CONSIDERATIONS
DESCRIPTION When microorganisms adhere to the surface of a urologic device (catheter, ureteral stent, implant) and create a matrix of extracellular polymeric substance. Biofilms provide resistance to antimicrobial agents by preventing penetration through the film and thereby limiting access to bacteria. Bacteria protected by a biofilm can also have poor expression of antimicrobial binding proteins and activation of intrinsic resistance genes. Biofilm bacteria can typically withstand 1,000–1,500× the concentration of antimicrobial agents utilized to kill nonfilm bacteria. Numerous strategies to avoid biofilm formation are currently being researched. Options include modifying biomaterial surface properties, antibiotic-impregnated material and frequent changes of foreign bodies when suitable.
REFERENCE
Tenke P, Köves B, Nagy K, et al. Update on biofilm and infections of the urinary tract. World J Urol. 2012;30:51–57.
![]() BIOTHESIOMETRY, PENILE
BIOTHESIOMETRY, PENILE
DESCRIPTION A simple, inexpensive method of testing the vibratory sensitivity threshold when evaluating neurogenic causes of impotence. It is performed by measuring vibratory thresholds, usually in at least 3 different areas of the body, such as the medial malleolus, fingertips, and glans penis. Probably not as accurate and reproducible as other forms of neurologic testing, such as tibial-evoked potentials, pudendal-evoked potentials, and BCR latency. (See also Section I: “Erectile Dysfunction/Impotence, General.”)
REFERENCE
Bemelmans BL, Hendrikx LB, Koldewijn EL, et al. Comparison of biothesiometry and neuro-urophysiological investigations for the clinical evaluation of patients with erectile dysfunction. J Urol.1995;153(5):1483–1486.
![]() BIRT–HOGG–DUBé SYNDROME
BIRT–HOGG–DUBé SYNDROME
DESCRIPTION Birt–Hogg–Dubé (BHD) syndrome is a rare, autosomal dominant disorder 1st described in 1977. It is caused by germline mutations in the BHD (FLCN) gene that lies within the chromosomal band 17p11.2 and encodes for a tumor-suppressor protein, folliculin. Folliculin is highly expressed in a variety of tissues, including the skin, kidney, and lung (stromal cells and type I pneumocytes). BHD syndrome is the cutaneous triad of fibrofolliculomas (hamartoma of the hair follicle), trichodiscomas, skin tags, and a propensity for renal tumors. The renal tumors are often chromophobe RCC, oncocytoma, or hybrids of these tumors. However, many will develop clear cell tumors as well. These tumors are more likely to be multiple and bilateral. (See also Section I: “Renal Cell Carcinoma, General.”)
REFERENCE
Adley BP, Smith ND, Nayar R, et al. Birt-Hogg-Dubé syndrome: Clinicopathologic findings and genetic alterations. Arch Pathol Lab Med. 2006;130(12):1865–1870.
![]() BITES TO PENIS, ANIMAL, AND HUMAN
BITES TO PENIS, ANIMAL, AND HUMAN
DESCRIPTION Bites to the penis can result in significant morbidity. Of animal bites, the most common is the dog bite. These can be potentially severe, with deep tissue destruction. In the cases of animal bites, patients tend to present early, and usually the wound can be closed after copious irrigation and any necessary debridement is performed. Broad-spectrum antibiotics should be administered for polymicrobial contamination and, in the case of dog bites, penicillin-VK may be given to treat Pasteurella multocida, which may be present in 20–25% of bites. Human bites tend to present later and pose a significant risk for infection. These should be copiously irrigated, broad-spectrum antibiotics should be administered, and wound closure is generally avoided. (See also Section I: “Penis, Trauma.”)
REFERENCES
Cummings JM, Boullier JA. Scrotal dog bites. J Urol. 2000;164:57–58.
Wessells H. Penile and genital injuries. Urol Clin North Am. 2006;33(1):117–126.
![]() BK VIRUS, UROLOGIC CONSIDERATIONS
BK VIRUS, UROLOGIC CONSIDERATIONS
DESCRIPTION A common member of the human polyoma DNA virus, with a seropositivity rate of 60–100% of the general population; it rarely presents any symptoms in immunocompetent hosts, and is not known to cause malignancy. During states of immunosuppression (eg, chemotherapy, AIDS, transplantation), this virus can reactivate and become a significant pathogen. BK virus often affects the urinary tract, with infections of the kidney and bladder being most common due to affinity to urothelial cells. In kidney transplant recipients, it can cause tubulointerstitial nephritis and ureteral stenosis. It has been shown to cause nephropathy in AIDS patients. BK virus has been found in the urine of immunosuppressed patients (viruria) having hemorrhagic cystitis (0.5–5 mo after bone marrow transplantation), causing both life-threatening hematuria and dysuria, as well as asymptomatic infections. Other causes of hemorrhagic cystitis in the differential include cyclophosphamide toxicity and adenovirus infection. The urine cytology–detectable abnormality of polyomavirus-infected cells is an enlarged nucleus with a single large basophilic intranuclear inclusion known as a “decoy cell”; this appears to be the best diagnostic test. Viral urine cultures and PCR are not useful in the diagnosis. It is named after the 1st patient (B.K.) in whom the virus was identified. (See also Section I: “Cystitis, Hemorrhagic [Infectious, Noninfectious, Radiation]” and “Immunocompromised Patients, Urologic Considerations.”)
REFERENCE
Sukov WR, Lewin M, Sethi S, et al. BK virus-associated nephropathy in a patient with AIDS. Am J of Kidney Dis. 2008;51(4):15–18.
![]() BLACK-WATER FEVER
BLACK-WATER FEVER
DESCRIPTION Black-water fever is a clinical entity characterized by acute intravascular hemolysis, classically occurring after the introduction of quinine for treatment of malaria. It is a rare but serious condition, in which hemolysis and anemia produce characteristically dark-colored urine. The condition has become rare since 1950, when quinine was replaced by chloroquine. Currently, it has reemerged from increased reutilization of quinine because of the development of resistance to chloroquine. Treatment of black-water fever is supportive, including stopping the offending drug, blood transfusion for severe anemia, and a short course of steroids. (See Section II: “Malaria, Urologic Considerations.”)
REFERENCE
Tombe M. Images in clinical medicine. Hemoglobinuria with malaria. N Engl J Med. 2008;358(17):1837.
![]() BLADDER AGENESIS
BLADDER AGENESIS
DESCRIPTION Rare and usually lethal congenital abnormality that has been reported in <20 living patients. Associated abnormalities include renal agenesis, retroiliac ureters, crossed fused renal ectopia, malrotation of the gut, colonic duplication, anal atresia, intraperitoneal iliac arteries, and bicornuate uterus. It is caused by a urogenital sinus abnormality during wk 5–7 of development.
TREATMENT
• Separation of urinary and fecal stream
• Other reconstructive surgeries as appropriate
REFERENCE
Kaefer M, Adams MC. Penis and bladder agenesis in a living male neonate. J Urol. 1997;157(4):1439–1440.
![]() BLADDER AUGMENTATION
BLADDER AUGMENTATION
DESCRIPTION Bowel segments are most commonly used to improve bladder capacity and manage poorly compliant bladders. The goal is to protect upper urinary tract drainage and maintain renal function. Augmentation cystoplasty is utilized mainly in patients with disorders of the neurologic system (eg, spinal cord injury [SCI], multiple sclerosis [MS], myelodysplasia). Modifications with bladder neck reconstruction and/or addition of continent channels (Mitrofanoff or Monti channels) can be utilized to facilitate both continence and ease in drainage. Complications associated with bladder augmentation include failure to adequately improve bladder capacity, metabolic disturbances, mucous plugging, urinary tract infections, bladder calculi, vesicoureteral reflux, bladder perforation, and malignancy (usually adenocarcinoma most commonly located at the region of the anastomosis).
REFERENCE
Biers S, Venn SN, Greenwell TJ. The past, present, and future of augmentation cystoplasty. BJU Int. 2011;109:1280–1293.
![]() BLADDER CANCER, INTRAVESICAL AGENTS
BLADDER CANCER, INTRAVESICAL AGENTS
DESCRIPTION Either immunotherapy agents, such as BCG, or chemotherapy agents, such as mitomycin C, are instilled directly into the bladder for the treatment of either carcinoma in situ or high-grade superficial urothelial carcinoma. Adjuvant intravesical chemotherapy regimens have been shown to decrease recurrence rates but no clear improvement in overall progression has been documented. Patients who fail intravesical therapy should be evaluated for extirpative treatment. (See also Section I: “Bladder Cancer, General,” “Bladder Cancer, Nonmuscle-Invasive Bladder Cancer [Ta, T1],” and “Bladder Cancer, Urothelial, Superficial Carcinoma In Situ (CIS) (NMIBC).”)
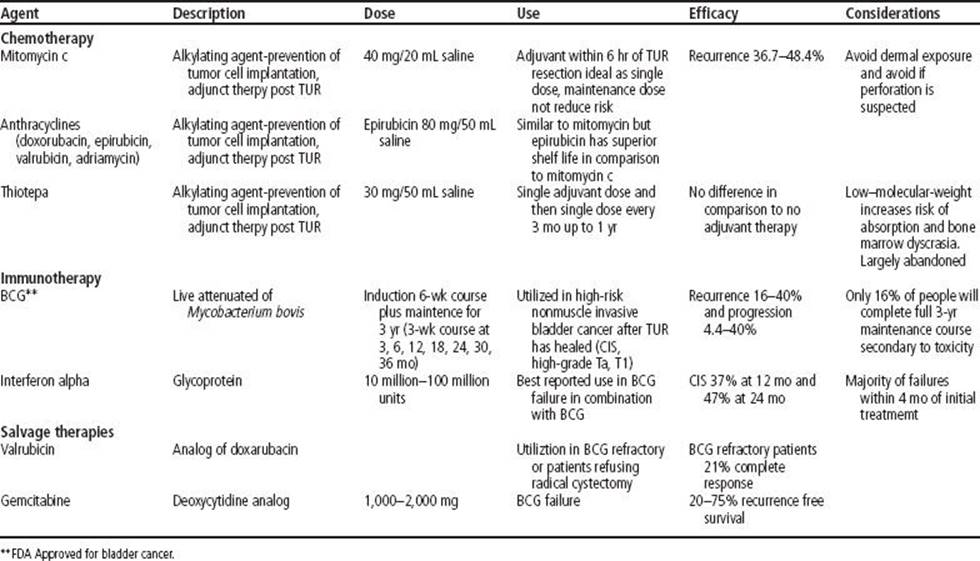
REFERENCE
Logan C, Brown M, Hayne D. Intravesical therapies for bladder cancer-indications and limitations. BJU Int. 2012;110 (Suppl 4):12–21.
![]() BLADDER CANCER, UROTHELIAL, MICROPAPILLARY
BLADDER CANCER, UROTHELIAL, MICROPAPILLARY
DESCRIPTION Micropapillary (MP) bladder cancer is a uncommon variant of urothelial carcinoma, accounting for 0.7–12% of all bladder cancers. This variant has an aggressive profile and is largely resistant to intravesical BCG. The majority of patients, approximately 2/3, have advanced T3/4 staging upon radical cystectomy and 50% have pN+ disease. Median 10-yr survival is 31%, in contrast to 53% for patients with non-MP urothelial carcinoma. Treatment should include early radical cystectomy (Image ![]() ).
).
REFERENCE
Wang J, Boorjian SA, Cheville JC, et al. Outcomes following radical cystectomy for micropapillary bladder cancer versus pure urothelial carcinoma: A matched cohort analysis. World J Urol. 2012;30:801–806.
![]() BLADDER CHORIOCARCINOMA
BLADDER CHORIOCARCINOMA
DESCRIPTION Primary choriocarcinoma of the bladder is exceedingly rare. Only 7 cases are described in the literature. Most cases present with hematuria and may also have gynecomastia. Metastases and β-hCG elevation were seen in the majority of reported cases. A full metastatic workup including scrotal exam and ultrasound are mandatory. 3 of the 7 cases were treated with resection and then chemotherapy, and all 3 showed good response (1 patient died of pulmonary embolus during therapy), the other 4 patients died of the disease. (See also Section I: “Bladder Cancer, General.”)
REFERENCE
Hanna NH, Ulbright TM, Einhorn LH. Primary choriocarcinoma of the bladder with the detection of isochromosome 12p. J Urol. 2002;167(4):1781.
![]() BLADDER CONTRACTILITY INDEX (BCI)
BLADDER CONTRACTILITY INDEX (BCI)
DESCRIPTION A urodynamic variable. BCI = PdetQmax + 5Qmax (Qmax is the maximum flow rate and PdetQmax is the detrusor pressure at maximum flow). Poor detrusor contractility is defined as BCI <100, normal contractility is BCI between 100 and 150, and strong bladder contractility is BCI >150.
REFERENCE
Abrams P. Bladder outlet obstruction index, bladder contractility index and bladder voiding efficiency: three simple indices to define bladder voiding function. BJU Int. 1999:84(1):14–15.
![]() BLADDER DIVERTICULUM
BLADDER DIVERTICULUM
DESCRIPTION A bladder diverticulum is a herniation of the vesical mucosa through the detrusor muscle. Bladder diverticula may be congenital or acquired. Most acquired diverticula are associated with long-standing bladder outlet obstruction (high intravesical pressures) and are most commonly seen in older men with benign prostatic hypertrophy or other forms of bladder outlet resistance; it is rare in women. The condition usually evolves from bladder wall trabeculation, to cellule, and finally a diverticulum, typically located on the lateral wall and rarely at the dome. Since the acquired diverticuli have no muscle wall components, they do not empty well and cause urinary stasis with increased risk of infection, stones, and urothelial carcinoma (intradiverticular tumors have a prevalence of 1–10%). The lack of a muscular wall makes urothelial carcinoma more likely to extend outside the bladder early. Congenital bladder diverticula are uncommon and occur almost exclusively in boys. When next to the ureteral orifice (Hutch diverticula), this can result in vesicoureteric reflux on that side. Treatment usually involves correction of the outlet obstruction to reduce high-pressure voiding. Diverticulectomy (open or laparoscopic) can be performed for recurrent infection or bladder calculi. Treatment for cancers within diverticula may include transurethral resection (can be complicated by narrow ostia and thin diverticular wall), laser ablation, diverticulectomy, partial cystectomy, and radical cystectomy with or without intravesical therapy (Image ![]() ).
).
REFERENCE
Zeman PA, et al. Lower urinary tract symptoms. In: Siroksy MB, et al., eds. Handbook of Urology. 3rd ed. Philadelphia, PA: Lippincott; 2004.
![]() BLADDER EARS
BLADDER EARS
DESCRIPTION Transient bladder outpouchings into the inguinal ring of male infants <6 mo old. This close association of the bladder with the internal ring resolves spontaneously. Inguinal herniorrhaphy in male infants can result in significant bladder damage if bladder ears are present. The condition is differentiated from bladder diverticula by absence of a definable neck.
REFERENCE
Redman JF, Jacks DW, O’Donnell PD. Cystectomy: A catastrophic complication of herniorrhaphy. J Urol. 1985;133(1):97–98.
![]() BLADDER FILLING DEFECTS
BLADDER FILLING DEFECTS
DESCRIPTION Filling defect on a contrast study of the urinary bladder (cystography) may be the result of:
• Air: Artifactual, postinstrumentation, vesicoenteric fistula
• Benign tumor: Prostatic enlargement, inverted papilloma, endometriosis
• Blood clot
• Calculus
• Congenital: Ureterocele
• Extrinsic compression by pelvic organ or mass, pelvic lipomatosis
• Fungus ball (bezoar)
• Infective, inflammatory: Inflammatory edema
• Instruments (catheters), foreign body
• Malignant tumor: Bladder and prostate malignancy, tumors invading urinary bladder from contiguous organs (eg, uterus, colon)
• Radiologic artifact: Fold in nondistended bladder
See also Section I: “Bladder calculi (vesical calculi)” and Section II: “Bladder Mass, Differential Diagnosis.” (Image ![]() )
)
![]() BLADDER HEMANGIOMA
BLADDER HEMANGIOMA
DESCRIPTION A bladder anomaly most often associated with Klippel–Trenaunay syndrome (extensive port wine stains on extremities), bladder hemangioma is a rare, benign tumor. It presents with gross hematuria, at times severe. Bladder hemangiomas may be solitary or multiple.
TREATMENT
• Endoscopic treatment with Nd:YAG laser ablation
• Partial cystectomy can be required for large lesions or uncertainty in diagnosis
REFERENCE
Kato M, Chiba Y, Sakai K, et al. Endoscopic neodymium:yttrium aluminium garnet (Nd:YAG) laser irradiation of a bladder hemangioma associated with Klippel-Weber syndrome. Int J Urol. 2000;7(4):145–148.
![]() BLADDER HERNIA
BLADDER HERNIA
DESCRIPTION Most are found in the inguinal or femoral region and are often associated with bladder outlet obstruction in men. It is estimated that up to 4% of all inguinal hernias can contain some degree of bladder herniation. Rarely, massive herniation may be found, with significant portions on the bladder and distal ureter descending into the scrotum; bladder infarction and obstruction has been reported. In women, herniation of the bladder into the anterior vaginal wall is technically a cystocele. Treatment is repair of inguinal hernia, with reduction of bladder herniation. Bladder outlet obstruction should be identified and treated in males as this may contribute to the original herniation and subsequent recurrences.
SYNONYM
Scrotal cystocele
REFERENCE
Bisharat M, O’Donnell ME, Thompson T, et al. Complications of inguinoscrotal bladder hernias: A case series. Hernia. 2009;13(1):81–84.
![]() BLADDER HYPOPLASIA
BLADDER HYPOPLASIA
DESCRIPTION Lack of urinary bladder development, leading to inadequate function and storage capacity. Hypoplasia is caused either the failure of production or storage of urine, or from complete bypass of the bladder. Causes include urogenital sinus abnormalities, severe epispadias, bilateral renal agenesis, severe renal dysplasia, and bilateral ureteral ectopia. Bladder reconstruction with bowel segments can be attempted.
REFERENCE
Frimberger DC, Kropp BP. Bladder Anomalies in Children. In: Wein AJ, et al., eds. Campbell-Walsh Urology. 10th ed. Philadelphia, PA: Saunders, 2012:3381.
![]() BLADDER, INFLAMMATORY PSEUDOTUMOR
BLADDER, INFLAMMATORY PSEUDOTUMOR
DESCRIPTION A benign spindle cell lesion in patients who have not had surgery (as opposed to postoperative spindle cell nodule). Most patients are from 20–50 yo and present with gross hematuria. The lesion is nodular or pedunculated, but some may be sessile and invade the muscularis propria. This is a benign lesion, but it must be differentiated from myxoid sarcomatoid carcinoma and myxoid leiomyosarcoma. Resection is the treatment.
REFERENCE
Young RH, Eble JN. Non-neoplastic disorders of the urinary bladder. In: Bostwick DG, Eble JN, eds. Urologic Surgical Pathology. 1st ed. St. Louis, MO: Mosby; 1997.
![]() BLADDER LEIOMYOMA
BLADDER LEIOMYOMA
DESCRIPTION Though very rare, it is the most common mesodermal tumor of the bladder, constituting 0.5% of all bladder neoplasms. Usually incidentally discovered, though if large or pedunculated may present with bladder outlet obstruction. Seen more commonly in females. Generally homogeneous and smoothly marginated on ultrasound and CT. MRI better and shows the submucosal origin, usually has low T2 and intermediate T1 signal.
TREATMENT
• Pedunculated lesions are amenable to transurethral resection
• Sessile or large tumors may require partial cystectomy
REFERENCE
Goel R, Thupili CR. Bladder leiomyoma. J Urol. 2013; Epub ahead of print.
![]() BLADDER, LYMPHOMA
BLADDER, LYMPHOMA
DESCRIPTION In lymphoma, involvement of the bladder is usually secondary to systemic disease. Primary lymphoma of the bladder is rare, and carries an excellent prognosis. Most patients are female in the 7th–8th decades. Patients typically present with gross hematuria. The tumors can be single or multiple, sessile or papillary. Most common types are large-cell and small cell lymphocytic lymphoma and further classified as MALT (extranodal marginal zone B-cell lymphoma) lymphomas thought to result from chronic inflammation. Many patients in recent series have chronic cystitis. Radiotherapy has been the treatment of choice for localized lymphoma; otherwise, systemic therapy is undertaken if the bladder is not the primary site.
REFERENCE
Kempton CL, Kurtin PJ, Inwards DJ, et al. Malignant lymphoma of the bladder: Evidence from 36 cases that low-grade lymphoma of the MALT-type is the most common primary bladder lymphoma. Am J Surg Pathol.1997;21(11):1324–1333.
![]() BLADDER MASS, DIFFERENTIAL DIAGNOSIS
BLADDER MASS, DIFFERENTIAL DIAGNOSIS
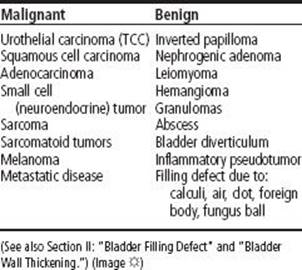
REFERENCE
Abol-Enein H. Nonurothelial cancer of the bladder. Urology. 2007;69(1 Suppl):93–104.
![]() BLADDER, METASTASIS TO
BLADDER, METASTASIS TO
DESCRIPTION The bladder may become involved by tumors by direct extension (most commonly) or metastatic spread. The most common locally invasive are colon, prostate, rectum, and cervix. Distant metastasis to the bladder include stomach, skin, lung, breast, and rarely melanoma. These metastasis are almost always solitary and are often located in the bladder neck or trigone. Lymphoma can be metastatic or primary and secondary involvement by leukemia has been reported.
REFERENCE
Cheng L, et al. Chapter 6. In: Bostwick DG, Cheng L, eds. Neoplasms of the urinary bladder in Urologic Surgical Pathology. 2nd ed. Philadelphia, PA: Mosby Elsevier; 2008.
![]() BLADDER NECK CONTRACTURE
BLADDER NECK CONTRACTURE
DESCRIPTION Scarring and stenosis of the bladder neck occur most commonly as a postoperative complication of transurethral resection of the prostate or radical prostatectomy at the site of vesicourethral anastomosis. Bladder neck contracture may lead to decreased urinary flow, high-pressure voiding, urinary retention, urinary tract infections, and incontinence. Factors associated with this complication include urinary leak at the anastomosis, poor mucosal approximation, suture retraction, ischemia, or foreign bodies such as surgical clips. Postoperative radiation may contribute. Radiation monotherapy can cause contracture with the presentation from 12–36 mo after completion. Management consists of dilation, endoscopic incision (laser, cold cut, electrosurgical) or resection, and, in severe cases, open repair utilizing a Y–V plasty. Occasionally, intermittent self catheterization may be needed to maintain patency.
REFERENCE
Blumenthal KB, Sutherland DE, Wagner KR, et al. Bladder neck contractures related to the use of Hem-o-lok clips in robot assisted laparoscopic radical prostatectomy. Urology. 2008;72(1):158–161.
![]() BLADDER NECK HYPERTROPHY
BLADDER NECK HYPERTROPHY
DESCRIPTION Hypertrophy of the bladder neck is often seen in conjunction with BPH and may lead to obstructive symptoms and dysfunctional high-pressure voiding. Pure bladder neck hypertrophy has also been implicated in chronic pelvic pain syndrome (CPPS) and may respond best to α-adrenergic blockade. (See also Section I: “Bladder Outlet Obstruction [BOO].”)
REFERENCE
Hruz P, Danuser H, Studer UE, et al. Non-inflammatory chronic pelvic pain syndrome can be caused by bladder neck hypertrophy. Eur Urol. 2003;4:106–110.
![]() BLADDER, NEUROFIBROMA
BLADDER, NEUROFIBROMA
DESCRIPTION A rare benign tumor of the nerve sheath from overgrowth of Schwann cells, these lesions originate in the bladder from ganglia in the wall. They can present in childhood as obstruction or voiding symptoms. Malignant degeneration is rare. The condition is sporadic or related to neurofibromatosis. Conservative resection, as needed, is the usual treatment. With severe obstruction or intolerable symptoms, cystectomy may be needed.
REFERENCE
Salvitti M, Celestino F, Gerocarni Nappo S, et al. Diffuse ganglioneuromatosis and plexiform neurofibroma of the urinary bladder: An uncommon cause of severe urological disease in an infant. J Pediatr Urol. 2013;9(3):e131–e133.
![]() BLADDER OUTLET OBSTRUCTION INDEX (BOOI)
BLADDER OUTLET OBSTRUCTION INDEX (BOOI)
DESCRIPTION Based on the International Continence Society (ICS) nomogram for identifying bladder outlet obstruction during urodymamic evaluation. The ICS nomogram categorizes patients with LUTS into obstructed, equivocal (or slightly obstructed) or unobstructed based on the maximum detrusor pressure during voiding versus the maximum flow rate.
BOOI = PdetQmax – 2Qmax
PdetQmax is the maximum detrusor pressure at peak flow and Qmax is the maximum flow rate.
Patients are obstructed if the BOOI is >40, equivocal if the BOOI is 20–40, and unobstructed if the BOOI is <20.
REFERENCES
Abrams P. Bladder outlet obstruction index, bladder contractility index and bladder voiding efficiency: Three simple indices to define bladder voiding fuction. BJU Intl. 1999;84(1):14–15.
Rom M, Waldert M, Klingler HC, et al. Bladder outlet obstruction in men with acute urinary retention: an urodynamic study. World J Urol. 2013;31(5):1045–1050.
![]() BLADDER PAIN/INTERSTITIAL CYSTITIS SYMPTOM SCORE (BPIC-SS)
BLADDER PAIN/INTERSTITIAL CYSTITIS SYMPTOM SCORE (BPIC-SS)
DESCRIPTION BPIC-SS is a questionnaire to select bladder pain syndrome/interstitial cystitis patients for clinical trials. It may have a role in clinical practice in the future. It consists of 8 questions divided into broad areas: Urge to urinate, urinary frequency, and bladder pain and pressure. For the scoring, a single score is created by summing all 8 items to create a total score ranging from 0–38.
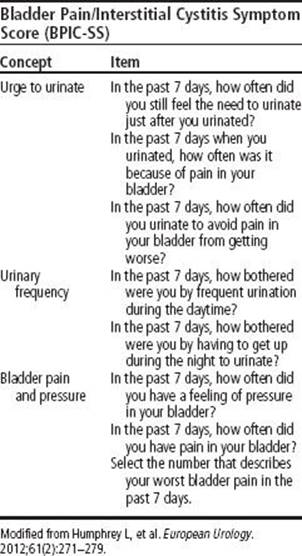
REFERENCE
Humphrey L, Arbuckle R, Moldwin R. et al. The Bladder Pain/Interstitial Cystitis Symptom Score: Development, Validation, and Identification of a Cut Score European Urology, Volume 61, Issue 2, 2012; Pages 271–279.
![]() BLADDER, PARAGANGLIOMA
BLADDER, PARAGANGLIOMA
DESCRIPTION Exceedingly rare tumor, with 15% being malignant. Accounts for 10% of extra-adrenal pheochromocytomas. Catecholamine release is sometimes triggered by voiding, bladder distention, defecation, or intercourse. Typical symptoms are those of a pheochromocytoma (diaphoresis, paroxysmal hypertension, palpitations, headaches, syncope). The lesion may arise from embryonic nests of chromaffin cells in the sympathetic plexus of the detrusor muscle. Cystoscopy should be accompanied by adrenergic blockade; routine biopsy should be avoided. Transurethral resection is considered inadequate, since most lesions involve the entire thickness of the bladder wall. Treatment for smaller lesions consists of partial cystectomy with pelvic lymph node dissection. Radical cystectomy is recommended with large tumors or if lymphatic involvement is present.
REFERENCE
Dahm P, Gschwend JE. Malignant non-urothelial neoplasms of the urinary bladder: A review. Eur Urol. 2003;44(6):672.
![]() BLADDER, PHEOCHROMOCYTOMA
BLADDER, PHEOCHROMOCYTOMA
DESCRIPTION Similar to pheochromocytomas in other areas of body; 10% are malignant. They are thought to arise from paraganglionic cells in bladder, usually around the trigone. Most are hormonally active and can present with hypertension during bladder emptying and filling. Can appear as a submucosal tumor on cystoscopy. Late metastasis can occur, so long-term follow-up is warranted.
TREATMENT
• Partial cystectomy is the treatment of choice
• TUR may cause a hypertensive crisis
REFERENCE
Beilan J, Lawton A, Hajdenberg J, et al. Pheochromocytoma of the urinary bladder: A systematic review of the contemporary literature. BMC Urol. 2013;13(1):22.
![]() BLADDER SARCOMA (LEIOMYOSARCOMA/RHABDOMYOSARCOMA)
BLADDER SARCOMA (LEIOMYOSARCOMA/RHABDOMYOSARCOMA)
DESCRIPTION Types of sarcoma that have been described in the bladder include angiosarcoma, leiomyosarcoma, rhabdomyosarcoma, liposarcoma, chondrosarcoma, and osteosarcoma. These, combined, account for <1% of all malignant tumors of the bladder. They usually present with hematuria or voiding symptoms. Sarcomas of the bladder are rare aggressive malignancies. Leiomyosarcoma is the most common malignant mesenchymal tumor that arises in the bladder of adults. It occurs more frequently in men. On histology, parallel bundles of spindle cells are seen. The mainstay of treatment is aggressive excision (4–5 cm margins), but even with such treatment the 5-yr disease-specific survival is 62%. Rhabdomyosarcomas are most common in young children. Embryonal rhabdomyosarcomas in children characteristically produce polypoid lesions in the base of the bladder, and is known as sarcoma botryoides. For pediatric rhabdomyosarcoma, a multimodal approach utilizing surgery, radiation, and chemotherapy is employed, with improving rates of bladder preservation and improving prognosis. Metastatic disease treatment consists of resection, radiation, and chemotherapy with single-agent (doxorubicin or ifosfamide). (See also Section I: “Bladder Cancer, General”; Section I: “Rhabdomyosarcoma, Pediatric [Sarcoma Botryoides].”)
REFERENCES
Rosser CT, Slaton JW, Izawa JI, et al. Clinical presentation and outcome of high-grade urinary bladder leiomyosarcoma in adults. Urology. 2003;61:1151–1155.
Stevens MC. Treatment for childhood rhabdomyosarcoma: The cost of cure. Lancet Oncol. 2005;6(2):77–84.
![]() BLADDER SMALL CELL CARCINOMA (OAT CELL, SIGNET RING)
BLADDER SMALL CELL CARCINOMA (OAT CELL, SIGNET RING)
DESCRIPTION Neuroendocrine or small cell carcinoma is an aggressive malignancy derived from either neuroendocrine or pluripotent cells. This tumor most commonly arises in the lung, but may occur in multiple locations including the bladder and less frequently the prostate. Neuroendocrine tumor of the bladder is rare, with ∼286 cases reported in the English literature. It can be seen alone or in combination with other tumor types, most frequently TCC. Small cell carcinoma of the bladder presents as any other bladder tumor, most frequently with hematuria. The diagnosis is made pathologically. The tumor usually presents as muscle-invasive disease (94% in 1 series), and often with metastatic disease (67% in same series). Most common sites of metastases are to lymph nodes, liver, bone, lung, and brain. Due to the high rate of early dissemination, chemotherapy is the mainstay of treatment, with radical cystectomy often performed afterward. The tumor also appears responsive to combined chemotherapy and radiation. Prognosis is generally worse than for urothelial carcinoma. (See also Section I: “Bladder Cancer, General.”) (Image ![]() )
)
SYNONYMS
• Small cell carcinoma
• Neuroendocrine tumor
• Oat cell carcinoma
TREATMENT
• Partial or radical cystectomy
• Platinum-based chemotherapy has achieved partial regression
REFERENCE
Koga F, Yokoyama M, Fukushima H. Small cell carcinoma of the urinary bladder: A contemporary review with a special focus on bladder-sparing treatments. Expert Rev Anticancer Ther. 2013;13(11):1269–1279.
![]() BLADDER, TEARDROP
BLADDER, TEARDROP
DESCRIPTION Diffuse pelvic pathology can compress the bladder into a teardrop configuration on various imaging studies, such as excretory urography or cystogram. Causes include pelvic lipomatosis, pelvic hematoma, pelvic adenopathy, and enlarged pelvic vasculature (usually caused by vena cava obstruction). Occasionally, a muscular patient with a hypertrophied iliopsoas muscle can exhibit this finding.
REFERENCE
Amis ES, Newhouse JH, eds. Essentials of Uroradiology. 1st ed. Boston: Little, Brown; 1991:287–288.
![]() BLADDER TRABECULATION AND CELLULES
BLADDER TRABECULATION AND CELLULES
DESCRIPTION Trabeculation is a cystoscopic description of hypertrophy of smooth muscle bundles in the muscularis propria layer of the bladder wall, which occurs over time due to high-pressure voiding in the setting of bladder outlet obstruction. The obstruction may be due to anatomic obstruction such as benign prostatic hyperplasia (BPH) in the adult or posterior urethral valves in the child, or to neurogenic dysfunction such as detrusor sphincter dyssynergia. It is a manifestation of increased collagen deposition in the bladder wall. More extreme degrees of trabeculation are termed “cellules.” These small pockets are caused when the bladder mucosa is pushed between the collagen and muscle fibers of the bladder wall. Cellules may progress to form an acquired bladder diverticulum. (See also Section II: “Bladder Diverticulum.”) (Image ![]() )
)
REFERENCES
Bai SW, Park SH, Chung DJ, et al. The significance of bladder trabeculation in the female lower urinary system: An objective evaluation by urodynamic studies. Yonsei Med J. 2005;46(5):673–678.
Sirosky MB, Babyan RK. Lower urinary tract symptoms. In: Siroksy MB, et al., eds. Handbook of Urology. 3rd ed. Philadelphia, PA: Lippincott; 2004.
![]() BLADDER, VILLOUS ADENOMA
BLADDER, VILLOUS ADENOMA
DESCRIPTION This tumor has a histologic appearance identical to villous adenoma of the colon. It can also be seen in the urachus. Cystoscopically, it appears exophytic and papillary. Histologically, a mucous-secreting epithelium with goblet cells is seen. It is treated by transurethral resection with possible cystectomy, if invasion is suspected.
REFERENCE
Channer JL, Williams JL, Henry L. Villous adenoma of the bladder. J Clin Pathol. 1993;46(5):450–452.
![]() BLADDER WALL CALCIFICATION, DIFFERENTIAL DIAGNOSIS
BLADDER WALL CALCIFICATION, DIFFERENTIAL DIAGNOSIS
DESCRIPTION Bladder wall calcification is a relatively uncommon finding. The differential includes:
• Amyloidosis
• Bilharzia (urinary schistosomiasis)
• Cyclophosphamide-induced cystitis
• Encrusted cystitis
• Mitomycin C intravesical treatment
• Tuberculosis
• Urothelial carcinoma
REFERENCE
Pollack HM, Banner MP, Martinez LO, et al. Diagnostic considerations in urinary bladder wall calcification. AJR Am J Roentgenol. 1981;136(4):791–797.
![]() BLADDER WALL THICKENING, DIFFERENTIAL DIAGNOSIS
BLADDER WALL THICKENING, DIFFERENTIAL DIAGNOSIS
DESCRIPTION Bladder wall thickening can be seen on US, CT, or MRI. The differential includes:
• Bacterial/viral cystitis
• Bilharzial infection (urinary schistosomiasis)
• Bladder cancer (urothelial carcinoma, nonurothelial carcinoma)
• Bladder fistula (Crohn disease, diverticulitis)
• Hemorrhagic cystitis
• High-pressure storage/voiding (eg, bladder outlet obstruction, neurogenic bladder)
• Systemic lupus erythematosus
• Tuberculosis (Image ![]() )
)
REFERENCE
Wong-You-Cheong JJ, Woodward PJ, Manning MA, et al. Inflammatory and nonneoplastic bladder masses: Radiologic-pathologic correlation. Radiographics. 2006;26(6):1847–1868.
![]() BLASTOMYCOSIS, GENITOURINARY
BLASTOMYCOSIS, GENITOURINARY
DESCRIPTION Blastomyces dermatitidis is endemic in the Ohio, Mississippi, and Missouri river basins. It is an opportunistic infection in immunocompromised patients, particularly associated with prolonged steroid use (>2 mo), HIV, solid tumors treated with radiation or chemotherapy, and end-stage renal and hepatic disease. GU blastomycosis tends to involve the prostate and epididymis, and produces voiding complaints. Genitourinary disease may be seen in 20–30% of disseminated infections. Prostatic abscess can be seen. Up to 30% can have epididymal involvement. GU blastomycosis is a manifestation of systemic disease; it has been reported to be transmitted by sexual relations to the GU system of the partner. Diagnosis may be made by isolation of fungus from the urine, semen, or tissue. Detection of blastomyces A antigen by immunodiffusion may be helpful in diagnosis. Other serologic testing with enzymeimmnoassay and radioimmunoassay have high sensitivity (85–88%) and specificity (100%).
TREATMENT
• Standard therapy for disseminated infection is long-term amphotericin B
• Long-term ketoconazole (12 mo) at 400 mg/d may be effective for prostatitis/epididymitis
• Itraconazole may be effective in focal uncomplicated infections
REFERENCES
Wise GJ, Freyle J. Changing patterns in genitourinary fungal infections. AUA Update, Vol. XVI, Lesson 1, 1997.
Wise GJ, Talluri GS, Marella VK. Fungal infections of the genitourinary system: Manifestations, diagnosis, and treatment. Urol Clin North Am. 1999;26(4):701–718.
![]() BLEOMYCIN TOXICITY
BLEOMYCIN TOXICITY
DESCRIPTION Used in combination chemotherapy for testicular cancer as well as cervical, ovarian, SCC, and lymphoma, induces single- and double-strand breaks in DNA called scission. Pulmonary fibrosis (fibrosing alveolitis) is a potentially lethal toxicity; it can develop 1–6 mo after treatment and has been reported to occur beyond 6 mo. Bleomycin may also cause hypersensitivity pneumonitis and nodular pulmonary densities. Skin changes, alopecia, and stomatitis are common. Vascular toxicity, anaphylaxis, and Raynaud phenomenon have been reported. Clinical indications of pulmonary toxicity may include any of the following: Cough (nonproductive), dyspnea, pleuritic chest pain, fever, tachypnea, rales, lung restriction, and hypoxemia. Renal insufficiency is a risk factor for bleomycin toxicity (80% eliminated by the kidney).
TREATMENT
• Discontinue drug with suspected bleomycin-induced injury; steroids may help some cases.
• Attention to minimizing oxygen concentration and hydration status during surgery is essential.
REFERENCE
Fyfe AJ, McKay P. Toxicities associated with bleomycin. J R Coll Physicians Edinb. 2010;40(3):213–215.
![]() BLUE DIAPER SYNDROME
BLUE DIAPER SYNDROME
DESCRIPTION Defect in tryptophan absorption in which the urine contains indoles, giving it a blue color. Similar to Hartnup disease, a chronic course is usual. Hypoplasia of the optic disc and abnormal eye movements have also been reported.
SYNONYMS
• Familial hypercalcemia with nephrocalcinosis and indicanuria
• Tryptophan malabsorption
TREATMENT
Low-tryptophan diet; no treatment known for underlying defect
REFERENCE
Chen Y, Wu L, Xiong Q. The ocular abnormalities of blue diaper syndrome. Metab Pediatr Systemic Ophthalmol. 1991;14(3–4):73–75.
![]() BLUE DOT SIGN
BLUE DOT SIGN
DESCRIPTION A blue discoloration seen through the scrotal wall when the testes are tented against the skin. Indicates the presence of torsion of appendix testes or appendix epididymis. Should be assessed during the evaluation of scrotal pain or swelling. The torsed appendix may swell to the size of the testicle itself. If torsion of the cord can be ruled out by palpation of the unequivocally normal testicle, appendiceal torsion can be observed. (See also Section I: “Torsion, Testis or Testicular/Epididymal Appendages.”)
REFERENCE
Dresner ML. Torsed appendage. Diagnosis and management: Blue dot sign. Urology. 1973;1(1):63–66.
![]() BLUE NEVUS (MELANOSIS), UROLOGIC CONSIDERATIONS
BLUE NEVUS (MELANOSIS), UROLOGIC CONSIDERATIONS
DESCRIPTION Benign melanotic lesion of the prostate that must be differentiated from malignant melanoma. It is usually an incidental finding after TURP. In prostate, the term blue nevus has been used when melanin is confined to ovoid or elongated melanocytes in the stroma, whereas the term melanosis has been used for those prostatic lesions that have melanin in both the stromal melanocytes and glandular epithelium. It has been reported in lesions with adenocarcinoma.
REFERENCE
Muzaffar S, Aijaz F, Pervez S, et al. Melanosis of the prostate: A rare benign morphological entity. Br J Urol. 1995;76(2):265–266.
![]() BOARI-OCKERBLAD FLAP
BOARI-OCKERBLAD FLAP
DESCRIPTION After appropriate bladder mobilization, a tonguelike flap of bladder based on the ipsilateral superior vesicle artery is incised. The base of the flap should be at least 4 cm, while the tip should be at least 3 cm. The tubularized flap is then anchored to the psoas minor tendon, and either direct or tunneled anastomosis with the ureter is then performed. Useful to reimplant the ureter when there is loss of the distal ureter.
REFERENCE
Nakada SY, Hsu T. Management of Upper Urinary Tract Obstruction. In: Wein AJ, et al., eds. Campbell-Walsh Urology. 10th ed. Philadelphia, PA: Saunders; 2012:1122–1168.
![]() BODY MASS INDEX (BMI), UROLOGIC CONSIDERATIONS
BODY MASS INDEX (BMI), UROLOGIC CONSIDERATIONS
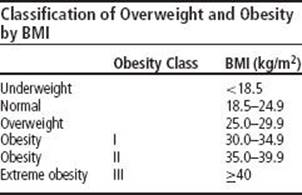
DESCRIPTION The BMI is defined as the weight (in kilograms) divided by the height (in meters2). BMI is used to categorize obesity (see table). Higher BMI carries many increased health risks, including diabetes and coronary artery disease. Obesity and elevated BMI have many detrimental effects and associations in urology. Elevated BMI has been shown to be an independent risk factor for incontinence in females and for adverse outcomes in prostate cancer. BMI has been clearly correlated with incidence and risk of formation of renal calculi in both men and women. It has been implicated in ED, with reduction of BMI correlating with increased IIEF score. Increased BMI as a marker of obesity implies increased difficulty in many open, laparoscopic, and percutaneous procedures. A BMI calculator from the NIH is available online at: http://www.nhlbisupport.com/bmi/. (See also Section II: "Obesity, Urologic Considerations.”)
REFERENCES
Esposito K, Giugliano F, Di Palo C, et al. Effect of lifestyle changes on erectile dysfunction in obese men: A randomized controlled trial. JAMA. 2004;291:2978–2984.
Taylor EN, Stampfer MJ, Curhan GC, et al. Obesity, weight gain, and the risk of kidney stones. JAMA. 2005;293:455–462.
![]() BONE MARROW/STEM CELL TRANSPLANTATION, UROLOGIC CONSIDERATIONS
BONE MARROW/STEM CELL TRANSPLANTATION, UROLOGIC CONSIDERATIONS
DESCRIPTION High-dose chemotherapy regimens used for bone marrow transplantation and stem cell transplantation are accompanied by multiple toxic side effects. The most common urologic complication is hemorrhagic cystitic (HC), with an incidence ranging from 7–68%. HC is commonly seen in a dose dependent manner after the administration of cyclophosphamide and ifosfamide. Both medications have the same metabolite, acrolein. HC can further be caused by busulfan, pelvic irradiation, thrombocytopenia, and the presence of a urinary viral infection (adenovirus, BK virus, cytomegalovirus [CMV], polyoma virus). Early onset HC tends to be due to acrolein exposure, late HC is associated with viral etiologies. Other possible urologic sequelae of high-dose chemotherapy exposures include bladder fibrosis, fistula, bladder contracture, chronic urinary tract infections, pyuria, and secondary malignancies. A preventative measure for HC is premedication with 2-mercaptoethane sodium sulfonate (Mesna) and hydration. Catheter drainage and continuous bladder irrigation may limit acrolein exposure to bladder urothelium. Tumor lysis syndrome and uric acid stone development are also possible.
REFERENCE
Monarch PA, Arnold LM, Merkel PA. Incidence and prevention of bladder toxicity from cyclophosphamide in the treatment of rheumatic diseases: A data-driven review. Arthritis Rheum. 2010;62(8):9–21.
![]() BONE METASTASIS, UROLOGIC CONSIDERATIONS
BONE METASTASIS, UROLOGIC CONSIDERATIONS
DESCRIPTION Bone metastasis is a common problem in urologic malignancies. Prostate cancer has a predilection to metastasize to bone but bone metastasis from renal cell carcinoma, urothelial carcinoma, and adrenocortical carcinoma is also seen. An elevated alkaline phosphatase suggests bone lesions. The diagnosis often involves a radionucleotide bone scan with confirmatory imaging study and possibly a biopsy. Bone metastases are associated with pain (which may be severe), pathologic fractures, and possible spinal compression (often referred to as skelet al-related events or SRE). These lesions often require treatment independently from the primary tumor. Options for treatment include chemotherapy, surgery, and external beam radiation. Radiation therapy is often highly successful at controlling local bony symptoms and radioisotopes such as strontium-89 are useful for palliation of more extensive bone metastasis. Radium 223 (Xofigo) an α-emitter has been approved for bony metastatic prostate cancer and can improve quality of life and extend survival in metastatic castrate resistant prostate cancer. In prostate cancer in particular, bisphosphonate therapy such as zolendronic acid, and osteoclast targeting agents such as denosumab are used to prevent progression and skelet al-related complications and may be effective at preventing occurrence of bone metastases (Image ![]() ).
).
REFERENCES
Bishr M, Saad F. Preventing bone complications in prostate cancer. Curr Opin Support Palliat Care. 2012:6(3):299–303.
Coleman RE. Clinical features of metastatic bone disease and risk of skelet al morbidity. Clin Cancer Res. 2006;15;12(20 Pt 2):6243s–6249s.
![]() BONE MINERAL DENSITY, UROLOGIC CONSIDERATIONS
BONE MINERAL DENSITY, UROLOGIC CONSIDERATIONS
DESCRIPTION Prolonged ADT for prostate cancer is associated with decreased bone mineral density (BMD) and osteoporosis, leading to disabling skelet al fractures. Bisphosphonate therapy (zoledronic acid, alendronate, others), smoking cessation, weight-bearing exercise, and vitamin D and calcium supplementation can help improve BMD during androgen ablation therapy. (See also Section II: “Osteoporosis and Osteopenia, Urologic Considerations.”) Some recommend that BMD should be monitored during androgen-deprivation therapy using BMD scans (dual-energy x-ray absorptiometry or DEXA):
• T-score: The number of standard deviations (SDs) by which the patient’s bone mass falls above or below the mean peak bone mass for a 30-yr-old healthy adult. For every 1 SD decrease in T-score, relative risk of fracture increases ∼1.5–2.5-fold
• WHO interpretation of T-scores: Normal: ≥–1; Osteopenia: –1 to –2.5; Osteoporosis ≤–2.5; Severe osteoporosis: ≤–2.5 and ≥1 fracture
REFERENCE
Ryan CW, Huo D, Stallings JW, et al. Lifestyle factors and duration of androgen deprivation affect bone mineral density of patients with prostate cancer during 1st year of therapy. Urology. 2007;70(1):122–126.
![]() BONE SCAN, UROLOGIC CONSIDERATIONS
BONE SCAN, UROLOGIC CONSIDERATIONS
DESCRIPTION The radionucleotide bone scan is a sensitive test for bone metastases and is obtained during the initial staging or in the setting of recurrent or metastatic disease in urologic malignancies (prostate, urothelial, renal, and adrenocortical carcinomas). A standard bone scan is generally performed by acquiring multiple images of the skeleton 3–4 hr after IV injection of 99mtechnetium-labeled methylene-diphosphonate (MDA). Due to low specificity, if a lesion is identified, particularly when solitary, further investigation is necessary using confirmatory testing. This may be done with plain radiographs, CT, or MRI. Bone scans are extensively used in prostate cancer to detect and follow bone metastases. In prostate cancer patients with extensive bony metastasis, the bone scan may have a “super scan” appearance, in which the focal lesions coalesce to produce diffusely increased uptake. An increase in the contrast between bone and background soft tissue and faint or absent renal images are the typical appearances seen on a “super scan.” (Image ![]() )
)
REFERENCE
Coleman R, Rubens R. Radionucleotide bone scan. In: Abeloff, ed. Clinical Oncology. 3rd ed. New York, NY: Churchill Livingstone; 2004.
![]() BONNEY TEST (MARSHALL TEST)
BONNEY TEST (MARSHALL TEST)
DESCRIPTION A clinical test used for >50 yr for the diagnosis of stress incontinence and for the selection of patients for incontinence surgery. As originally described, the test consists of 2 parts:
• The patient coughs with a full bladder, and simultaneous urine loss from the urethra is visually confirmed.
• The examiner elevates the bladder neck with a finger on either side of the urethra while the patient coughs again.
• If the patient is then continent, the test is considered positive and the patient is thought to have an anatomic defect correctable by surgical elevation of the bladder neck. Bonney cautioned that the fingers must be carefully placed to avoid compressing the urethra in the midline.
The contemporary clinical utility of the test has been questioned by many clinicians.
REFERENCE
Miyazaki FS. The Bonney test: A reassessment. Am J Obstet Gynecol. 1997;177(6):1322–1328; discussion 1328–1329.
![]() BORS-COMARR CLASSIFICATION OF VOIDING DYSFUNCTION
BORS-COMARR CLASSIFICATION OF VOIDING DYSFUNCTION
DESCRIPTION Based on observations noted with spinal cord injury patients. The system takes into account 3 main factors:
• Anatomic location of the lesion (upper motor neuron, lower motor neuron)
• Completeness of the lesion (partial vs. complete SCI)
• Presence of residual urine, which would mean “unbalanced,” according to the definition
• Best applied to patients with a complete neurologic lesion after spinal shock has resolved
REFERENCE
Pryse-Phillips W, Pryse-Phillips W. Companion to Clinical Neurology. 2nd ed. New York, NY: Oxford; 2003.
![]() BOSNIAK CLASSIFICATION OF RENAL CYSTS
BOSNIAK CLASSIFICATION OF RENAL CYSTS
DESCRIPTION Classification system to differentiate renal cystic masses visualized on CT as benign or malignant. Cysts are graded on scale from I–IV, with grade I having typical appearance of benign simple cyst, and grade IV having appearance of RCC. Classification is based on homogeneity and complexity of cystic fluid, presence or absence of septations, calcifications, or solid components; and the density of cystic fluid as determined by Hounsfield units. (See also Section II: “Renal Cysts,” Section II: “Renal Mass.”)
• Category I: Benign simple cysts; thin walls without septa, calcifications, or solid components; water density and no contrast enhancement. No further imaging needed.
• Category II: Benign cysts with a few thin septa; the wall or septa may contain fine calcification and sharp margins, are nonenhancing, and usually measure <3 cm.
• Category IIF: Well-marginated and may have thin septa or minimal smooth thickening of the septa or wall, which may contain calcification that may also be thick and nodular; no contrast enhancement. Includes totally intrarenal nonenhancing lesions >3 cm. These require follow-up (designated by the “F” designation).
• Category III: Indeterminate cysts with thickened irregular or smooth walls or septa; enhancement present. 40–60% are malignant (cystic RCC and multiloculated cystic RCC). Other class III lesions are benign and include hemorrhagic cysts, infected cysts, and multiloculated cystic nephroma. Surgery is recommended, although additional imaging by MRI or with biopsy is supported by some clinicians.
• Category IV: Risk of malignancy is 85–100%. Characteristics of category III cysts plus they contain contrast-enhancing soft tissue components that are adjacent to and independent of the wall or septum. Surgery is recommended (Image ![]() ).
).
REFERENCE
Israel GM, Bosniak MA. Urology. 2005;66(3):484–488.
![]() BOURNE TEST
BOURNE TEST
DESCRIPTION A diagnostic test for the detection of enterovesical or colovesical fistulas. Radiographs are taken of centrifuged urine samples, which are obtained immediately after a barium enema. In 1 series of 10 patients, in 7 of the 10, the Bourne test was the only positive evidence of an otherwise occult colovesical fistula later proven at surgery.
REFERENCE
Lawrence C, Shaffer HA Jr, Bickston SJ. Image of the month. Bourne test, enterovesical fistulas. Gastroenterology. 2003;125(2):291, 641.
![]() BOWENOID PAPULOSIS
BOWENOID PAPULOSIS
DESCRIPTION Bowenoid papulosis is an uncommon skin lesion affecting the genitals, groin, and perianal areas of young, sexually active adult men and women. The histology appearance resembles Bowen disease. BP is rarely invasive and may even regress spontaneously, thus conservative treatments are often adequate. The natural history of the disease is unknown, but the lesions usually follow a benign clinical course, and spontaneous regression is observed. Evolution of the lesions to invasive carcinoma is rare. The papules are asymptomatic, discrete, small (averaging 4 mm in diameter), flat, reddish violaceous or brown, often coalescent, and usually have a smooth, velvety surface. Many patients have a history of genital infection with viral warts or herpes simplex. Genital warts are primarily caused by HPV types 6 and 11. Treatment should be conservative. Individual lesions can be adequately treated by excision, cautery, cryoablation, or laser surgery, much as ordinary warts, without the need for wide surgical margins. Alternatively, lesions may be treated for 3–5 wk with 5% 5-fluorouracil cream or imiquimod cream QOD.
REFERENCE
Campione, E, Centonze C, Diluvio L, et al. Bowenoid Papulosis and Invasive Bowen’s Disease: A multidisciplinary approach. Acta Derm Venereol. 2013;93(2):228–229.
![]() BOYARSKY GUIDELINES FOR BPH
BOYARSKY GUIDELINES FOR BPH
DESCRIPTION To provide reproducible guidelines for the severity of symptoms of prostatism, BPH, and LUTS, scored questionnaire formats have been developed. Traditional assessment tools include the Madsen–Iversen Point System and the Boyarsky Guidelines. These have been generally replaced by the AUA or I-PSS questionnaires, but are used in several ongoing follow-up studies of BPH therapies.
REFERENCE
Boyarsky S, Jones G, Paulson DF, et al. A new look at bladder neck obstruction by the Food and Drug Administration regulators: Guidelines for investigation of benign prostatic hypertrophy. Trans Am Assoc Genitourinary Surg. 1976;68:29–32.
![]() BOYCE NEPHROTOMY (ANATROPHIC NEPHROLITHOTOMY)
BOYCE NEPHROTOMY (ANATROPHIC NEPHROLITHOTOMY)
DESCRIPTION The longitudinal anatrophic nephrotomy takes advantage of a nearly avascular plane in the kidney (Brödel white line), which can be used to remove staghorn calculi (Boyce anatrophic nephrolithotomy). The incision site in the lateral posterior surface of the kidney can be accurately identified by injecting indigo carmine in the posterior renal artery branch. Once the capsule is incised, the parenchyma is divided with the blunt end of the knife in the proper plain. Traditionally used for staghorn calculi.
REFERENCE
Straffon RA. Anatrophic nephrolithotomy. In: Novick AC, Streem BS, Pontes JE, et al., eds. Stewart’s Operative Urology. Baltimore, MD: Williams & Wilkins; 1989:191–197.
![]() BRACHYTHERAPY SEED EMBOLUS
BRACHYTHERAPY SEED EMBOLUS
DESCRIPTION Brachytherapy is used to treat prostate cancer via image-guided implantation of radioactive seeds of iodine125 or palladium103. These seeds, when placed into periprostatic tissue, have been noted to migrate, at times entering the prominent periprostatic veins and traveling centrally. Multiple investigations have yielded varying rates of seed displacement and embolization ranging from 0.7–55% of all cases. The most common target organ is the lung, but reports of coronary artery and hepatic emboli exist through a patent foramen ovale. The iodine125 seed measures 4.5 mm in length and 0.8 mm in diameter and, due to its small size, is more frequently involved in embolization. Because of their size, these emboli are often asymptomatic and are diagnosed incidentally on imaging studies. 2 concerns regarding this process are possible injury to the end organ, especially in cases of patent foramen ovale, and diminution of the radiation dose to the prostate.
REFERENCE
Nguyen BD. Cardiac and hepatic seed implant embolization after prostate brachytherapy. Urology. 2006;68(3):673.
![]() BRAIN METASTASIS, UROLOGIC CONSIDERATIONS
BRAIN METASTASIS, UROLOGIC CONSIDERATIONS
DESCRIPTION Brain metastatic disease can be seen with several urologic malignancies, most commonly with renal cell carcinoma and germ cell tumors (GCT). They generally are poor prognostic indicators. Patients may be asymptomatic with occult disease or display neurologic symptoms such as headache, nausea, and vomiting, mental status changes, seizures, or focal signs. Patients presenting with urologic tumors and neurologic signs should be worked up for brain metastases. CT scan is generally quick and readily available, but MRI has higher sensitivity and is better at distinguishing metastases from other intracranial processes. Due to their high impact on quality of life, these often require prompt treatment usually via radiation therapy or surgical removal.
REFERENCE
Nguyen TD. Brain metastasis. Neurol Clin. 2007;25(4):1173–1192.
![]() BRENNER TUMORS
BRENNER TUMORS
DESCRIPTION These are tumors of variable malignant potential of the ovary. Extraovarian and testicular origins have been reported, and they usually present as an ovarian mass. Light microscopy demonstrates distinctive nests of transitional cells indistinguishable from urothelium. Classified as typical, metaplastic, proliferating, or malignant, these lesions usually stain for carcinoembryonic antigen (CEA). Theorized origin is from a metaplastic process of coelomic epithelium. Usually, surgical removal is used to assess malignant potential.
REFERENCE
Caccamo D, Socias M, Truchet C. Malignant Brenner tumor of the testes and epididymis. Arch Pathol Lab Med. 1991;115(5):524–527.
![]() BRICKER URETERAL ANASTOMOSIS
BRICKER URETERAL ANASTOMOSIS
DESCRIPTION A direct ureteral-to-small bowel end-to-side refluxing anastomosis incorporating full-thickness ureteral and intestinal wall. It is used in ileal conduit construction.
REFERENCE
Dahl DM, McDougal WS. Use of intestinal segments in urinary diversion. In: Wein AJ, et al., eds. Campbell-Walsh Urology. 10th ed. Philadelphia, PA: Saunders; 2012:2411–2449.
![]() BRIGHAM SLING (URETHROPEXY)
BRIGHAM SLING (URETHROPEXY)
DESCRIPTION Used to treat stress incontinence in women. A combined endoscopic needle sling procedure that utilizes a rectus fascial strip placed at the bladder neck through a vaginal incision. The fascial sling is held in place with needles placed through the anterior abdominal wall, similar to the Stamey and Raz suspension needle procedures. (See also Section I: “Incontinence, Urinary, Adult Female.”)
REFERENCE
Loughlin KR. The Brigham sling. Contemp Urol. 1998;10:69–75.
![]() BRINK SCORE
BRINK SCORE
DESCRIPTION A digital test of pelvic muscle strength for evaluation of a pelvic muscle exercise program. Factors of perceived pressure, alteration of the vertical plane, and time were combined to form a 7-point scale. Currently used in pelvic floor physical therapy regimens.
REFERENCE
Brink CA, Wells TJ, Sampselle CM, et al. A digital test for pelvic muscle strength in women with urinary incontinence. Nurs Res. 1994;43:352–356.
![]() BRITISH TESTICULAR TUMOR CLASSIFICATION
BRITISH TESTICULAR TUMOR CLASSIFICATION
DESCRIPTION Used mainly in Great Britain, and based on the concept that all nonseminomatous tumors represent displaced, nonorganized embryonic blastomeres and are therefore teratomas. Disparate lesions are classified under a common category. The World Health Organization classification is used in most of the rest of the world.
REFERENCE
Ulbright TM. Neoplasms of the testes. In: Bostwick D, ed. Urologic Surgical Pathology. 1st ed. St. Louis, MO: Mosby; 1997.
![]() BRONCHOGENIC CYST, RETROPERITONEAL
BRONCHOGENIC CYST, RETROPERITONEAL
DESCRIPTION Bronchogenic cysts are congenital abnormalities arising from remnants of the primitive foregut, which gives rise to the respiratory diverticulum. Generally asymptomatic and benign, these lesions are often incidentally discovered. The true prevalence is unknown due to their asymptomatic nature. Retroperitoneal location is exceedingly rare with only approximately 60 cases reported in the literature. Most retroperitoneal bronchogenic cysts are located near the left adrenal gland or peripancreatic. Anatomopathologic criteria include pseudostratified, ciliated columnar epithelium with cartilage, smooth muscle or seromucous glands. May become larger over time due to continued epithelial secretion. Infection, perforation, hemorrhage, and malignant degeneration are possible and surgical extirpation is recommended. Definitive diagnosis can only be made histopathologically. (See also Section I: “Retroperitoneal Masses, Fluid, and Cysts.”)
REFERENCE
Govaerts K, Van Eyken P, Verswijvel G, et al. A bronochognic cyst, presenting as a retroperitoneal cystic mass. Rare Tumors. 2012;4(1):e13.
![]() BRUNN BUDS AND NESTS (VON BRUNN NESTS)
BRUNN BUDS AND NESTS (VON BRUNN NESTS)
DESCRIPTION Variant of bladder epithelium, noted in 80–90% of normal bladders. Brunn buds are an invagination of surface epithelium into the lamina propria. Brunn nests represent a further invagination within the lamina propria and are a more progressed form of a Brunn bud. Cystitis cystica is thought to result from a Brunn nest that closes over on itself, forming a cyst. May become involved with urothelial carcinoma; controversy exists as to whether radical or conservative therapy is indicated if these lesions are involved by TCC.
REFERENCE
Dinney CP, Ramirez EI, Swanson DA, et al. Management of transitional cell carcinoma involving von Brunn’s nests. J Urol. 1995;153:944–949.
![]() BRUSHITE (CALCIUM MONOHYDROGEN PHOSPHATE)
BRUSHITE (CALCIUM MONOHYDROGEN PHOSPHATE)
DESCRIPTION A type of calcium phosphate calculus of the kidney. Brushite stones are particularly dense and are 2nd only to cysteine stones in their resistance to fragmentation. Calcium phosphate is the most common type of stone seen in distal renal tubular acidosis (type 1). On metabolic evaluation, primary calcium phosphate stone formers tend to have higher urine volumes, and higher calcium and lower citrate excretion than do idiopathic calcium oxalate formers. (See also Section I: “Urolithiasis, Adult, General”; Section II: “Urolithiasis, Calcium Oxylate/Phosphate.”)
REFERENCE
Evan AP, Lingeman JE, Coe FL, et al. Crystal-associated nephropathy in patients with brushite nephrolithiasis. Kidney Int. 2005;67(2):576–591.
![]() BTA TESTING (BTA AND BTA STAT URINE TEST)
BTA TESTING (BTA AND BTA STAT URINE TEST)
DESCRIPTION The BTA test (Bard; Redmond, Washington) is a latex agglutination assay. It qualitatively detects high–molecular-weight basement membrane complexes, present when tumor cells become invasive and undergo proteolytic degradation. A comparison of BTA with bladder wash cytology reported a higher sensitivity of BTA (54% vs. 23%); however, BTA was associated with a high false-positive rate (specificity 9%). A multicenter trial demonstrated sensitivities of 40% and 16% for BTA and urine cytology, respectively.
The initial BTA test had 2 limitations: It was a latex agglutination test, and it yielded high false-positive rates. Consequently, the new BTA stat test was developed; it is a monoclonal antibody immunoassay that detects the presence of newly identified human complement factor H-related protein (hCFhrp). A study of BTA stat reported higher sensitivity compared with cytology. BTA stat has also had higher sensitivity compared with the BTA test (58% vs. 44%). The specificity of BTA stat was reported as 72% for benign genitourinary disease and 95% in healthy volunteers. The main advantage of the BTA test is that it can simply be performed in an office setting and provides rapid results.
REFERENCE
Leyh H, Hall R, Mazeman E, et al. Comparison of the Bard BTA test with voided urine and bladder wash cytology in the diagnosis and management of cancer of the bladder. Urology. 1997;50:49–53.
![]() BULBOCAVERNOSUS REFLEX
BULBOCAVERNOSUS REFLEX
DESCRIPTION Used as a means of evaluating sacral neurologic integrity. The reflex is commonly elicited by touching the labium minus lateral to the clitoris or squeezing the glans penis and observing for anal contraction. Afferent limb of reflex arc is the pudendal nerve, efferent limb is via the inferior hemorrhoidal branch of the pudendal nerve. Reflex is integrated at the S2–S4 cord level. Relevant urologically for its innervation of the bladder outlet and in erectile function and ejaculation.
REFERENCE
Wester C, Fitzgerald MP, Brubaker L, et al. Validation of the clinical bulbocavernosus reflex. Neurourol Urodyn. 2003;22(6):589–591.
![]() BULKING AGENTS, INJECTABLE
BULKING AGENTS, INJECTABLE
DESCRIPTION Injections of various agents (synthetic and natural) have been used in urology to treat conditions such as vesicoureteral reflux, intrinsic sphincter deficiency (ISD), and stress urinary incontinence (SUI). Some products that have been used in the United States are listed here. Collagen is no longer available but is included in the table due to its widespread use in the past. A recent study in elderly patients with SUI noted improvement in incontinence after bulking therapy. In contrast to earlier reports, side effects due to injections were few and mild. Coaptite, macroplastique, and durasphere are actively used for SUI in the United States. Only Deflux is still used for VUR in the United States. (See also Section I: “Incontinence, Urinary, Adult Male”; Section I: “Incontinence, Urinary, Adult Female”; Section I: “Vesicoureteral Reflux, Pediatric”; and Section II: “STING Procedure.”)
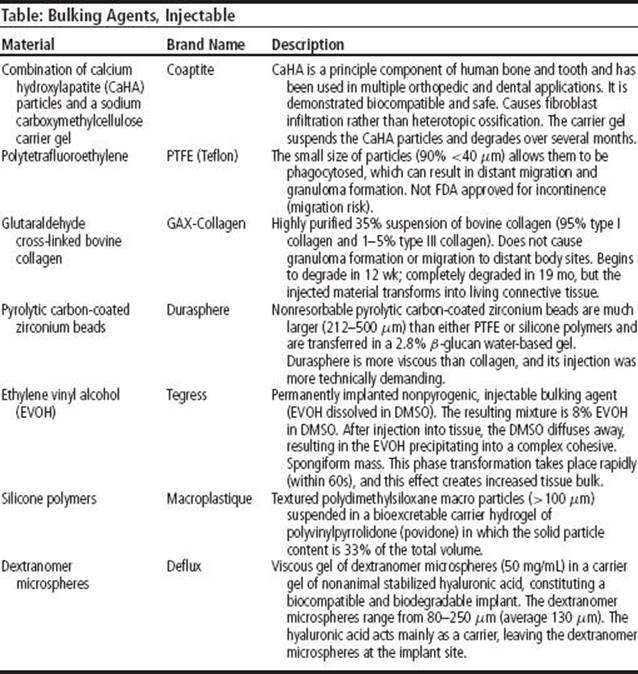
REFERENCES
Mayer RD, Dmochowski RR, Appell RA, et al. Multicenter prospective randomized 52-week trial of calcium hydroxylapatite versus bovine dermal collagen for treatment of stress urinary incontinence. Urology. 2007;69(5):876–880.
Mohr S, Siegenthaler M, Mueller MD, et al. Bulking agents: an analysis of 500 cases and review of the literature. Int Urogynecol J. 2013;24(2):241–247.
Wilson TS, Lemack GE, Zimmern PE. Management of intrinsic sphincteric deficiency in women. J Urol. 2003;169(5):1662–1669.
![]() BULLOUS PEMPHIGOID
BULLOUS PEMPHIGOID
DESCRIPTION A dermatologic condition thought to be autoimmune related. The condition is more common in men and in patients >60 yr of age. Although variable in clinical presentation, a preliminary nonbullous phase is usually characterized by severe pruritus and nonspecific skin changes, followed by formation of confluencing vesicles and marked erythema of the skin. Immunohistochemical evaluation of the skin biopsy shows IgG deposition along the skin basement membrane. Commonly used medications are anti-inflammatory agents (eg, corticosteroids, tetracyclines, dapsone) and immunosuppressants (eg, azathioprine, methotrexate, mycophenolate mofetil, cyclophosphamide). Most patients require therapy for 6–60 mo.
REFERENCE
Gual A, Iranzo P, Mascaró JM Jr. Treatment of bullous pemphigoid with low-dose oral cyclophosphamide: A case series of 20 patients. J Eur Acad Dermatol Venereol. 2014;28(6):814–818.
![]() BUN (BLOOD UREA NITROGEN), INCREASED/DECREASED
BUN (BLOOD UREA NITROGEN), INCREASED/DECREASED
DESCRIPTION Blood urea nitrogen (BUN) is a product of dietary protein metabolism. It is produced in the liver and cleared by the kidneys. The serum BUN level depends on both the rate of production and the rate of renal clearance. In renal failure, BUN and creatinine levels generally increase. Factors that might increase BUN include drugs (lithium, diuretics, aminoglycosides, corticosteroids), GI bleeding, prerenal azotemia, renal disease (diabetic nephropathy, pyelonephritis, glomerulonephritis), and obstructive nephropathy. Factors that lower BUN include liver disease, malnutrition and low-protein diets, 3rd-trimester pregnancy, celiac disease, and acromegaly. BUN along with sodium is thought to be responsible for the solute diuresis (postobstructive diuresis) that results after relief of renal obstruction.
REFERENCE
Aronson D, Mittleman MA, Burger AJ. Elevated blood urea nitrogen as a predictor of mortality in patients admitted for decompensated heart failure. Am J Med. 2004;116(7):466–473.
![]() BURCH COLPOSUSPENSION
BURCH COLPOSUSPENSION
DESCRIPTION The pubocervical fascia at the level of the bladder neck is fixed to Cooper’s ligament bilaterally, usually through a Pfannenstiel incision and a retropubic exposure. It is used in treatment of stress incontinence in women.
REFERENCE
Burch JC. Urethrovaginal fixation to Cooper’s ligament for correction of stress incontinence, cystocele, and prolapse. Am J Obstet Gynecol. 1961;81281–81290.
![]() BUSCHKE-LOWENSTEIN TUMOR
BUSCHKE-LOWENSTEIN TUMOR
DESCRIPTION Nonmalignant penile or perineal lesion, which may be large and exophytic. May cause urethral erosion and fistulas. Can be very locally invasive and mistaken grossly for SCC. Microscopically, broad rete pegs, filled with benign squamous cells and surrounded by a layer of inflammatory cells, are noted. A possible role of HPV 6 and 11 in the development is theorized. Treatment is by local excision after proven diagnosis. (See also Section I: “Condylomata Acuminata (Venereal Warts)”and “Penis, Lesion.”)
SYNONYMS
• Verrucous carcinoma
• Giant condyloma acuminata
REFERENCE
Chu QD, Vezeridis MP, Libbey NP, et al. Giant condyloma acuminata (Buschke-Lowenstein tumor) of the anorectal and perianal regions. Analysis of 42 cases. Dis Colon Rectum. 1994;37(9):950–957.
![]() BYAR FLAPS
BYAR FLAPS
DESCRIPTION The penile prepuce is split dorsally and transferred ventrally, yielding redundant ventral skin (Byars flaps) to be used in 2nd-stage hypospadias repair.
REFERENCE
Snodgrass WT. Hypospadias. In: Wein AJ, et al., eds. Campbell-Walsh Urology. 10th ed. Philadelphia, PA: Saunders; 2012:3503–3536.