Tricia L. C. Kuo1, Nadir Osman2 and Christopher R. Chapple2
(1)
Department of Urology, Singapore General Hospital, Singapore, Singapore
(2)
Department of Urology, Royal Hallamshire Hospital, Sheffield, UK
Christopher R. Chapple
Email: c.r.chapple@sheffield.ac.uk
Introduction
The urethra is a vascular tube that conveys urine out from the bladder. A thorough understanding of basic anatomy and physiological function of the male and female urethra is essential to understand the impact of urethral disorders and their treatment. In this chapter we discuss the clinical anatomy of the male and female urethra as well as urethral disorders commonly encountered in urological practice.
Anatomy
The male and female urethra differ quite significantly in terms of anatomy, physiology and function. As such, the types of pathology that can affect either sex also vary.
The female urethra is approximately 4 cm in length. It is composed of epithelium surrounded by lamina propria and a thin layer of circular smooth muscle. Beneath is a thick longitudinal layer of smooth muscle which runs along the entire length. Striated muscle extends over the distal two-thirds in a horseshoe configuration forming the external urethral sphincter (EUS). The proximal one-third of the female urethra is lined by urothelium and the distal two-thirds by non-keratinised stratified squamous epithelium.
The male urethra may be divided into proximal (posterior) and distal (anterior) segments. The proximal portion consists of the prostatic and membranous segments, and the distal portion consists of the bulbar, pendulous/penile and glandular/navicular fossa segments.
Males have two distinct sphincter mechanisms – the bladder neck mechanism which extends from the internal meatus down to the verumontanum and the distal sphincter which extends up to the verumontanum from the bulbomembranous junction. The two mechanisms are distinct and functionally independent (Fig. 10.1).
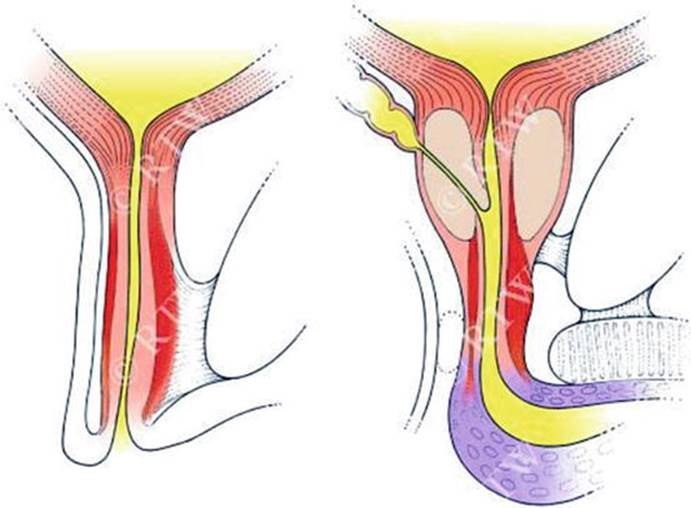
Fig. 10.1
Differences between female and male urethral sphincter mechanisms
Physiology and Function
Sensory innervation of the bladder is conveyed to the spinal cord in the pelvic and hypogastric nerves. This involves sensory nerves in the suburothelial plexus, myelinated (A) and unmyelinated (C) fibres. (A) fibres respond to passive distension and active contraction, whereas C fibres respond to noxious stimuli. The cell bodies are located in the dorsal root ganglia (DRG) at S2–3 and T11–L2 spinal segments. Bladder afferent activity thus ascends from the spinal cord to the pontine micturition centre (PMC) and cerebral cortex.
The motor innervation of the lower urinary tract (LUT) comes from both the parasympathetic and sympathetic branches of the autonomic nervous system. The parasympathetic preganglionic fibres are located in the S2–4 spinal segments, and these synapse with postganglionic cell bodies in the detrusor, bladder neck and urethra. Activation of the parasympathetic fibres causes detrusor contraction and relaxation of the smooth muscle of the bladder neck and urethra. Sympathetic cell bodies are located in T10–12 and L1–2. The preganglionic fibres synapse with postganglionic fibre in the hypogastric plexus. The predominant effect is inhibition of the parasympathetic pathways. The somatic supply to the pelvic floor muscles and external sphincter originates from S2-4 and conveyed by the pudendal nerve.
There are important gender differences with regard to bladder neck sphincter mechanism function. The male bladder neck has a well-developed layer of inner circular smooth muscle along with an outer layer of longitudinal smooth muscle. It has a relatively rich adrenergic innervation (contraction prevents retrograde ejaculation), and its functional competence is considered so reliable as to sufficiently maintain continence in the presence of damage to the EUS. The female bladder neck is less well developed with the predominant orientation of fibres being longitudinal and the principle innervation being cholinergic. Consequently its functional competence is less reliable.
Anatomical/Structural Versus Functional Disorders
A wide variety of pathology can affect the urethra and can be broadly classified in a variety of ways, e.g. congenital or acquired, male or female, anatomical/structural abnormalities or functional abnormalities. A structural and anatomical classification is detailed in Tables 10.1 and 10.2.
Table 10.1
Structural/anatomical classification of urethral disorders
|
Disorders of the male urethra |
Disorders of the female urethra |
|
Congenital |
Congenital |
|
Duplication of the urethra |
Distal urethral stenosis in childhood (urethral spasm and dysfunctional voiding) |
|
Urethral stricture (rare) |
|
|
Posterior urethral valves |
|
|
Anterior urethral valves |
|
|
Hypospadias |
|
|
Urethrorectal and vesicorectal fistulas |
|
|
Epispadias |
|
|
Acquired |
Acquired |
|
Urethral stricture |
Urethritis (acute and chronic) |
|
Urethral stenosis |
Urethral caruncle |
|
Urethritis and infections |
Urethrovaginal fistula |
|
Urethral carcinoma |
Urethral diverticulum |
|
Urethral stricture (rare) |
Table 10.2
Functional classification of urethral disorders
|
Functional disorders |
Disorders of sensation |
Hypersensitive sensation or pain due to inflammation |
|
Decreased sensation |
||
|
Disorders of motor function |
||
|
During storage |
Incompetent or underactive/absent |
|
|
During voiding |
Obstruction due to non-relaxation or overactivity, e.g. detrusor-urethral dyssynergia (detrusor bladder neck dyssynergia or detrusor sphincter dyssynergia) |
|
Whilst it is not possible to address all the different urethral pathologies, the common conditions will be discussed in detail in this chapter.
Male Urethral Disorders
Urethral Strictures
Introduction
The term “urethral stricture” refers to an abnormal narrowing of any segment of the urethra surrounded by the corpus spongiosum and implies varying degrees of ischaemic spongiofibrosis. The term “urethral stenosis” is reserved for narrowing of the membranous urethra, the prostatic urethra and the bladder neck as they are not invested by corpus spongiosum (in contrast to the term “urethral distraction defect” as seen with a pelvic fracture urethral injury) [1].
Acquired urethral strictures are more common in men. These can be subcategorised into iatrogenic, traumatic, inflammatory and idiopathic causes [1]. Fenton et al. found that the majority of strictures were idiopathic (34 %) and iatrogenic (32 %) in a review of 175 stricture patients with a total of 194 strictures [2]. Inflammatory and traumatic causes were found in only 20 % and 14 % of patients, respectively. The most commonly involved site was the bulbar urethra (52 %).
Clinical Presentation
Key points in the history include:
· Presenting symptoms – obstructive symptoms (e.g. poor flow, urinary retention), storage symptoms, haematuria, dysuria
· History of trauma, previous instrumentation (e.g. difficult urethral catheterisation) or transurethral procedures
· History of sexually transmitted diseases or urinary infections
· Current status of erectile and ejaculatory function
· Previous treatment, e.g. urethral dilatation or urethrotomy, hypospadias repair, intermittent self-dilatation (ISD)
A directed physical examination should assess the following:
· Difficulties with positioning of patient, i.e. lithotomy position (especially after trauma)
· External genitalia – condition of tissues, previous fibrosis/scarring and lichen sclerosis (LS), previous circumcision, fistula, signs of ongoing infection
· Abdominal examination – suprapubic scars, presence of a suprapubic catheter
· Digital rectal examination
Evaluation and Follow-Up
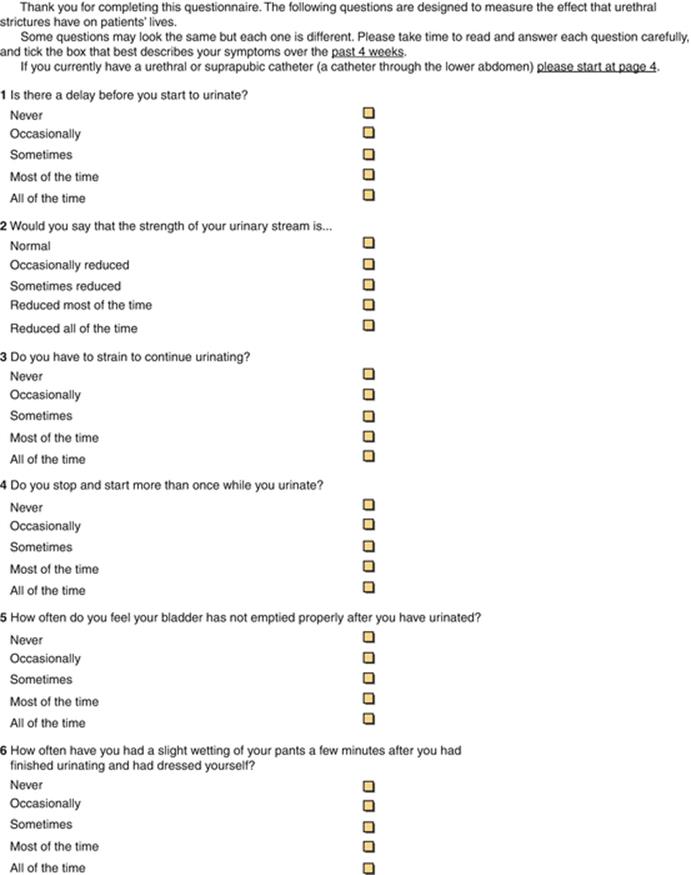
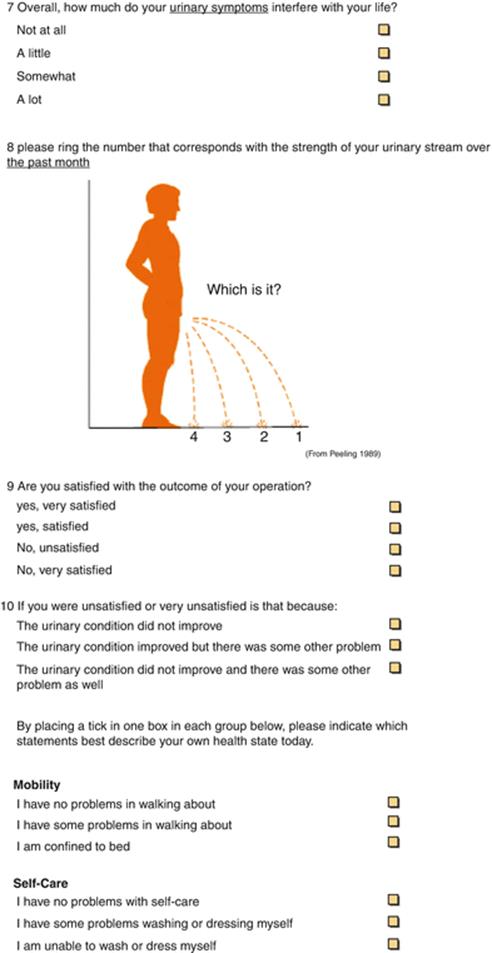
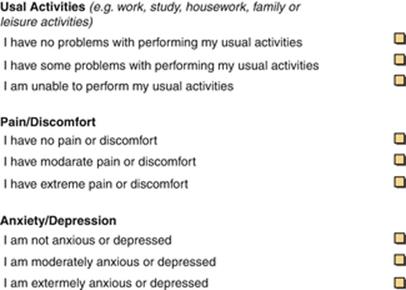
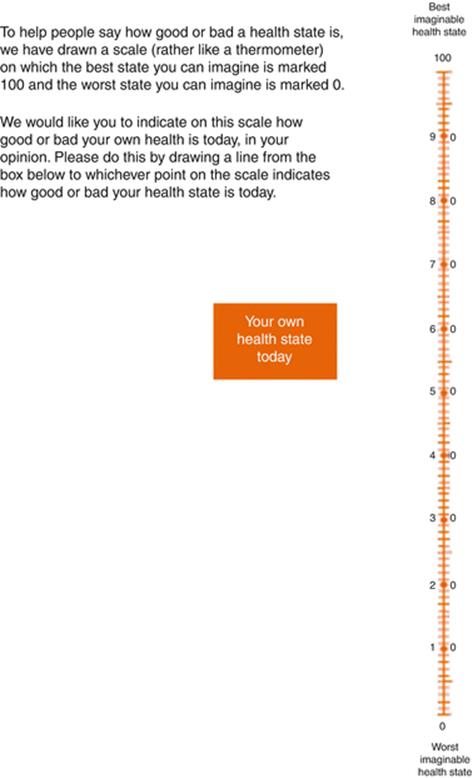
Patients should undergo comprehensive symptomatic evaluation at presentation and follow-up [3, 4]. The recently published patient-reported outcome measure (PROM) for urethral stricture surgery provides a standardised and validated method of assessing outcomes and consists of a lower urinary tract symptom (LUTS) construct (6 questions), a separate LUTS-specific quality-of-life (QoL) question and Peeling’s voiding picture. The post-operative PROM is supplemented by 2 questions addressing overall patient satisfaction (Appendix A).
Retrograde urethrogram (RUG) is recommended as a reliable, accessible and versatile means to both diagnose and stage urethral stricture. It should be combined with voiding cystourethrography (VCUG) to achieve a synergistic approach to the evaluation of the entire urethra [5]. It remains the standard method to ascertain the location and length of a stricture and any associated urethral pathology, e.g. false passages, fistulae and calculi.
Cystoscopy is recommended by the SIU/ICUD committee as the most specific procedure for the diagnosis of urethral stricture. It is a good adjunct in the staging of anterior urethral stricture, particularly to confirm abnormal or equivocal findings on imaging studies. For pelvic fracture-related urethral distraction defect, cystoscopy is highly recommended for assessment of the bladder neck and posterior urethra [5].
Ultrasonography is another potential adjunctive investigational tool. In addition to ascertaining the length and location, ultrasound can also provide information regarding degree of spongiofibrosis and concomitant pathology, e.g. diverticula, fistulae, stones, false passages and periurethral abscesses [6–8]. Previous retrospective reviews have shown that intraoperative ultrasound changed the surgical approach in 19 % and was integral in deciding between two possible approaches in 26 % of patients [9]. This is suggested as a supplement to the standard approach for most reconstructive surgeons, i.e. an intraoperative decision based on the visual assessment of the anatomy, calibre of the urethra and its vascularity.
The value of uroflowmetry in assessing a stricture preoperatively or for the post-operative follow-up is of limited value. It is the norm to have a patient present with a very tight stricture at the first instance, as they usually have normal bladder function that compensates. In 1968, Smith reported that the effective diameter of the unobstructed male urethra was 11 Fr gauge. Hence, until the stricture narrowed beyond this point, there would be no significant interference with flow, and hence, patients would not be necessarily aware that there was a significant problem [10].
Treatment
In 1974, Sachse introduced direct vision internal urethrotomy (DVIU) to treat urethral strictures by incising with the use of a cold knife [11]. Both urethrotomy and dilatation work by disrupting the stricture, and rely upon adequate tissue vascularity for healing without re-narrowing.
A nationwide survey of practising members of the American Urological Association was performed in 2007 and found that the most commonly used procedures for treatment of urethral strictures were dilatation (used by 92.8 % of surveyed practitioners), optical internal urethrotomy (used by 85.6 %) and endourethral stents (used by 23.4 %). It was noted that for a long bulbar urethral stricture or short bulbar urethral stricture refractory to internal urethrotomy, only 20–29 % of respondents would refer to another urologist, whilst 31–33 % would continue to manage the stricture by minimally invasive means despite predictable failure [12].
Steenkamp et al. compared internal urethrotomy to dilation in a randomised controlled trial and found no difference in efficacy between the two methods. Recurrence rates were noted to be higher for strictures of increasing length. They thus recommended dilation or internal urethrotomy (DVIU) for strictures shorter than 2 cm, primary urethroplasty for those longer than 4 cm, and a trial of dilation or urethrotomy for those 2–4 cm in length [13]. Therefore, SIU/ICUD guidelines recommend that primary DVIU/dilation be used as first-line treatment for short (<1–2 cm), single bulbar urethral strictures (Grade A) [14].
Generally, a third DVIU/dilation is not recommended, except if necessitated by patient comorbidities, choice or economic resource (Grade A). This is evidenced by a previous study that showed that after a third dilation or urethrotomy for stricture recurrence at 3 and 6 months, the stricture-free rate at 24 months was 0 (p < 0.0001) [15].
Permanent urethral stenting is not recommended for patients with strictures who are considered to be candidates for urethral reconstruction. There is evidence that subsequent failure of a permanently implanted stent represents a major surgical challenge [16].
Urethroplasty for the anterior urethra consists of a range of operations such as excision and primary anastomosis (EPA) and the different types of substitution urethroplasty. The type of urethral reconstruction depends on several factors. The length, location and aetiology (e.g. lichen sclerosis) and previous interventions all have impact on the final outcome.
A recent analysis of 17 articles comprising a total of 1234 patients over 35 years (1975–2010) found that overall success of EPA was 93.8 %. Reported complications were <5 %, and there was no evidence of persistent loss of sexual function. Other possible complications include fistula, chordee, postmicturation dribbling and recurrence. Thus, EPA should be carried out for patients with short bulbar strictures, especially if expected success rates of other procedures are <90 % [17].
Care needs to be taken in the assessment and subsequently when performing an anastomotic reconstruction of the anterior urethra. In general, only strictures <3 cm were considered for anastomotic procedure. Mobilisation of the urethra and corporal separation allows gain of several more centimetres (Fig 10.2).
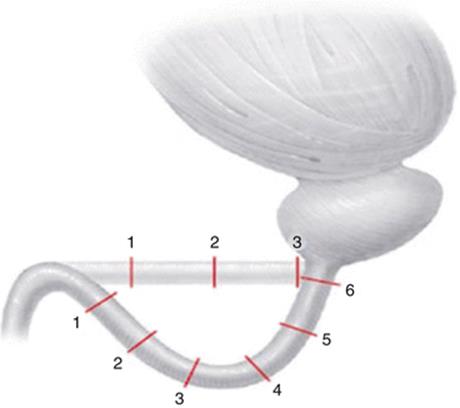
Fig. 10.2
Diagrammatic representation of the additional length (in cm) gained by separation of the corpora cavernosa [18]
Mobilisation of the bulbar urethra should not extend beyond the penoscrotal junction to prevent chordee. In this context, one should perform an augmentation (substitution) if the stricture is too long. Likewise, it is rare to be able to perform an anastomotic urethroplasty for the penile urethra due to the risk of producing a chordee. The exception would be in the case of an acute penile fracture.
Augmentation urethral reconstruction can be either one-stage or two-stage procedure. There are three potential options to a one-stage procedure – an onlay augmentation, an augmented anastomotic or a tube augmentation procedure. Whereas, a two-stage procedure includes excision of the stricture and reconstruction of the roof strip. The second stage tubularisation is carried out at least 3–6 months later, but further evaluation at 2 months is essential to identify what revision, if any, of the first stage is necessary [19].
A systematic review of graft augmentation urethroplasty techniques for treatment of anterior urethral strictures showed there was no significant difference between the average success rates for the dorsal and ventral onlay procedures, 88.4 % and 88.8 % at 42 and 34 months, respectively. The lateral onlay procedure has only been described in 6 patients and is reported to have a success rate of 83 % at 77 months. For penile stricture disease, the success rate for a two-stage procedure was significantly better than the one-stage technique (90.5 % versus 7.5 %, respectively) [20].
Oral mucosa is the most versatile augmentation (substitution) material. Oral mucosa has privileged immunology, with preclinical work showing less fibrosis compared to skin. This mucosa is wet and is unlikely to be affected by lichen sclerosis.
Bioengineered buccal mucosa grafts are likely to have a future role for patients with long and complex strictures. Particularly for redo cases where oral mucosa has already been used, then the supply may be limited. Autologous cell-seeded grafts are not dependent on ingrowth of epithelial cells and show some promise. Tissue-engineered oral mucosa was reported in five men. All patients had complex strictures secondary to lichen sclerosis. Initial graft take was 100 %. However, at 3 years, three patients had intact graft, albeit with the need for instrumentation [21].
Pelvic Fracture Urethral Injuries (PFUI)
Classic signs of blood at the meatus, inability to void and a distended bladder after a traumatic incident are the classic signs but may not always be present. Other signs include a butterfly sign or perineal/scrotal haematoma and a high riding prostate on per rectal examination. It is particularly important to exclude the coexisting rectal injury which is seen in up to 5 % of cases.
Posterior urethral injuries associated with pelvic fracture are best considered as pelvic fracture urethral distraction injury (PFUDD). This term was introduced by Turner-Warwick [22]. However, a large percentage of such injuries are partial and do not necessarily result in “distraction” or “separation”. Therefore, the terminology of PFUI has replaced PFUDD.
Some types of pelvic fracture are associated with a higher risk of posterior urethral injury. The highest risk of urethral injury was found in cases with straddle fracture when combined with diastasis of the sacroiliac (SI) joint (24 times more than the rest of the pelvic fractures); this was followed by straddle fracture alone (3.85 times) and Malgaigne’s fracture (3.4 times) [23].
Ideally a retrograde urethrogram should be performed in all patients suspected of having a PFUI. The urethrogram should be performed with 45° oblique views with the downside leg externally rotated and flexed at the knee. The downward obturator fossa should be completely closed on the scout film to confirm appropriate positioning. This is followed by the injection of 15–20 ml of contrast under fluoroscopic guidance. However, in polytrauma patients, this may be logistically difficult. In addition, extravagated contrast can confuse later CT findings.
There are two accepted treatment methods in the acute setting. Early closed realignment over a catheter can be done using blind or endoscopic techniques. The second and safest approach recommended for the majority of cases is the placement of a suprapubic catheter and an interval perineal urethroplasty 3–6 months later. It is well established that immediate open retropubic urethroplasty and open catheter realignment result in significantly higher incontinence and impotence rates and hence are not recommended (Grade A) [24].
The progressive perineal approach is the means to which an end-to-end bulbomembranous anastomosis (BMA) can be achieved in stepwise fashion. These are:
1.
2.
3.
4.
When adequate access to the membranous urethra and the bladder neck cannot be accomplished with the above four steps, an abdominoperineal approach could be used, with or without transpubic exposure.
The success rate of uncomplicated bulbomembranous anastomosis (BMA) is quoted at 90–98 % [25–29]. However, this very much depends on the competence of the surgeon, experience of the tertiary unit and severity of the surgery. Surgical complications include erectile dysfunction and incontinence.
Female Urethral Disorders
Urethral Diverticulum
Introduction
Urethral diverticula (UD) are outpouchings of the urethral wall which occur almost exclusively in women between the ages of 30 and 60. The actual prevalence is unknown but is estimated to be around 1–6 % in the general populace, increasing to as much as 40 % in women with lower urinary tract symptoms (LUTS) [30, 31].
Most UD are postulated to arise after infection of the paraurethral glands [30]. Other possible causes may be trauma, childbirth or iatrogenic injury. Paraurethral glands have ducts draining into the urethra and are located in the posterolateral position along the whole urethral length. Their main function is the secretion of mucin which acts as a mucosal sealant. Infection of urethral gland leads to obstruction of the ducts and abscess formation. These abscesses then point and often rupture into the urethral lumen, after which the tract epithelialises and a diverticulum forms. The connection between the diverticulum and the urethra is termed the ostium.
UD are usually distributed along the 3 or 9 o’clock positions of the urethra [32]. They can have simple or complex configurations whereby the sac wraps partially or completely around the urethra [33]. Ostia typically open into the urethral lumen at the 6 o’clock position. Untreated UD can result in stone formation and benign or malignant neoplasms (although associated malignancy is extremely rare).
Clinical Presentation
UD present a major diagnostic challenge due to the non-specificity of the presenting symptoms [34]. These symptoms typically comprise storage LUTS, dysuria, urethral pain, pelvic pain and dyspareunia. In addition patients may complain of stress or urgency urinary incontinence, voiding difficulties or retention of urine and urethral discharge or bleeding. The classically described triad of dysuria, dyspareunia and dribbling is actually uncommon. Due to the non-specificity of symptoms, there is often a delay in diagnosis [35]. Confusable conditions include bladder pain syndrome and recurrent urinary tract infection, which can coexist along with UD and is usually attributed to stagnation of urine.
Vaginal examination may reveal a periurethral swelling or be entirely normal particularly if the diverticulum is anteriorly placed. Examination during an acute infective exacerbation may demonstrate significant tenderness. Milking the sac may produce urine or discharge per urethra. Hardness of the swelling may indicate a stone or malignancy. Identification of stress urinary incontinence, urogenital prolapse and urethral hypermobility is important as their presence may influence the surgical approach.
Evaluation
Routine urinalysis (± urine microscopy and culture) is essential to assess for infection or haematuria. Urethroscopic examination may allow visualisation of the ostium in up to 60 % of cases [36]. A zero degree lens will provide the best visualisation of the whole lumen.
We advise the use of urodynamics preoperatively in all patients to assess baseline urinary tract function. Voiding cystourethrography during a videourodynamic study was previously considered the study of choice for diagnosis of UD but has now been superseded by newer imaging modalities. It has low diagnostic accuracy (around 65 %), as the ostium may be stenotic or the flow down the urethra may be too weak to allow the sack to fill with contrast.
Ultrasound can be performed transvaginally, transabdominally and less commonly transurethrally, to demonstrate a UD. Transvaginal and transurethral ultrasound provides better detail although are more invasive. Although very rapid and inexpensive, ultrasound for the identification of UD is user dependent and requires a high degree of expertise to identify the relevant surgical anatomy.
In contrast to ultrasound, post-micturition magnetic resonance imaging (MRI) is easier to perform and interpret. It is currently considered the best investigation for identifying and defining UD [37]. Surface or endoluminal coils (placed in the rectum or vagina) can be used, the advantage of the latter is the superior signal to noise ratio and better image resolution [38]. T2-weighted images provide the best mode of identifying UD. Both sagittal and coronal views are needed for surgical planning. It is also essential that images are taken post-voiding.
Classification System
A comprehensive classification system, termed the LNSC3 system, for UD was proposed by Leach et al. It describes the following aspects of UD: location, number, size, site of connection with urethra, configuration and continence state [39] (Table 10.3).
Table 10.3
LNSC3 classification system
|
L |
Location |
Distal, middle or proximal urethra |
|
+ or − extension behind bladder neck |
||
|
N |
Number |
Single or multiple |
|
S |
Size |
Centimetres |
|
C1 |
Configuration |
Single, multiloculated or saddle shaped |
|
C2 |
Communication |
Site of communication with urethra: distal, mid or proximal |
|
C3 |
Continence |
Is stress incontinence present or not |
Treatment
Conservative management is indicated for asymptomatic patients, those who are minimally symptomatic and those not wanting to undergo surgery. The mainstay of conservative treatment is urethral antibiotic prophylaxis as necessary.
If surgery is being considered, a videourodynamic study is recommended preoperatively to provide an objective assessment of bladder and urethral function as patients often have coexistent problems such as stress incontinence and detrusor overactivity [40]. Surgery for UD is challenging due to its extension through part of the urethral sphincter mechanism, which makes incontinence a significant risk. The tissues around the UD are often inflamed and fibrosed due to recurrent infection leading to a lack of clear planes. Surgery is best deferred until any infective flare-ups have been adequately treated. The best surgical approach is a transvaginal excision with urethral sphincter reconstruction which should only be performed in experienced hands. The procedure is usually performed in the lithotomy position although with more complex and proximal diverticula, the prone position provides optimal access [41]. Apart from de novo or worsening stress incontinence, other risks of surgery include urethrovaginal fistula and dyspareunia. A Martius flap can be used to reduce the risk of fistula formation and to facilitate any subsequent incontinence surgery which may be needed. We would not advise the use of techniques such as marsupialisation of a UD or incision of the ostium as both are associated with high morbidity.
Urethrovaginal Fistula
Urethrovaginal fistula is rare. In developed nations, they usually arise as a result of iatrogenic injury (e.g. surgery for stress incontinence, prolapse and urethral diverticula). In developing nations, the most common cause by far is obstructed labour. Less frequent causes include vaginal cancer, radiation therapy and pelvic fracture. Recently with the increasing use of synthetic mesh in incontinence surgery, mesh erosion has emerged as a new cause of fistulae.
Clinical Presentation
Clinical presentation is dependent on the size and location of the fistula [42]. The patient may be continent if the fistula is in the distal urethra, but usually patients with a fistula complain of urine passing involuntarily out per vagina. Fistula located proximally or in the mid urethra may lead to leakage intermittently or in certain positions.
Evaluation
It is important to document the number and location of fistulae. This is best done via a combination of examination under an anaesthetic (EUA) and cystoscopy. Imaging may be helpful.
Treatment
If diagnosed within the first 2–3 weeks following iatrogenic trauma, operative repair is recommended. After this window of opportunity, if the patient is dry with a urethral catheter in situ, then there is a chance that drainage alone may lead to spontaneous healing. Should the fistula tract fail to close after a period of 30 days, it is unlikely to close spontaneously [43].
Surgical management is associated with a significant risk of stress urinary incontinence, as the sphincter mechanism is usually damaged due to the injury that caused the fistula. The traditional approach is transvaginal. Utmost care must be taken to avoid too much dissection around the fistulous tract, which may further damage the urethral sphincter mechanism. Martius flap interposition between the urethral and vaginal closure is recommended to reduce the risk of recurrence and facilitates future placement of an autologous fascial sling should the patient develop post-operative stress incontinence.
Female Urethral Stricture
Introduction
Urethral stricture in females is rare, representing 4–13 % of the causes of bladder outlet obstruction in women [44]. Obstruction in women is in itself an uncommon urodynamic finding in women presenting with urinary tract symptoms (2.7–8 %) [45]. The pathogenesis of female urethral strictures is poorly understood, and the postulated aetiological factors include trauma, infection and prior instrumentation. There are currently no accepted standardized definitions or diagnostic criteria.
Clinical Presentation
Patients typically complain of voiding lower urinary tract symptoms (LUTS) but may also have storage LUTS and a feeling of incomplete bladder emptying, particularly if post-void residuals are elevated.
Evaluation
First-line investigations include uroflowmetry and measurement of post-void residual volumes (PVR). Some authors make the diagnosis using urethral calibration placing the threshold in terms of a diagnostic calibre anywhere in the range of 14 Fr to 20 Fr. On urodynamic testing, stricture would be suggested by a high-pressure, low-flow pattern along with radiological evidence on urethrography of a narrowed urethral segment and ballooning of the proximal non-strictured urethra. An MRI scan may demonstrate an associated diverticulum or fistula.
Treatment
First-line management is usually urethral dilatation which can be considered to have a mean success rate of around 47 % at mean follow-up of 43 months [46]. Urethrotomy is not recommended in women due to the significant risk of damage to the urethral sphincter mechanism. Recently there has been increased interest in reconstructive surgery for female urethral strictures. Urethral reconstruction can be undertaken through dorsal, ventral or a circumferential approach using grafts (e.g. vaginal or buccal mucosa) or using labial flaps. The available literature suggest that reported success rates in excess of 80 % can be achieved using these approaches with a low risk of stress incontinence in expert hands [46]. The low risk of stress incontinence can probably be explained by the fact that most strictures are located distally where the sphincter mechanism is at its thinnest.
Summary
Urethral disorders have a varied pathophysiology and clinical presentation. A key to diagnosis is having a high degree of clinical suspicion and utilisation of appropriate specialised investigations. The treatment depends on the patient presentation, disease pathophysiology and the resources available. In view of their relative rarity, complex cases should be treated at high-volume tertiary centres.
Points of Interest
· Urethral disorders have a varied pathophysiology and clinical presentation.
· Assessment of urethral pathology often requires specialised investigations and recently includes patient-reported outcome measures (PROM) particularly for urethral strictures.
· Determinants of type of procedure for treatment of urethral stricture depend on stricture location, length, degree of spongiofibrosis, previous intervention and surgeon experience.
· Urethral diverticula present a diagnostic challenge. Surgery is recommended for symptomatic patients.
· Majority of urethral diverticula can be approached via a transvaginal approach, with the patient in a prone position. A Martius flap reduces the risk of fistulation.
· Female urethral strictures are rare and can be treated first with urethral dilatation, with consideration for urethral reconstruction if recalcitrant.
Appendix A
References
1.
Latini JM, McAninch JW, Brandes SB, Chung JY, Rosenstein D. SIU/ICUD consultation on urethral strictures: epidemiology, etiology, anatomy, and nomenclature of urethral stenosis, strictures and pelvic fracture urethral disruption injuries. Urology. 2014;83(3 Suppl):S1–7.CrossRefPubMed
2.
Fenton AS, Morey AF, Aviles R, et al. Anterior urethral strictures: etiology and characteristics. Urology. 2005;65(6):1055–8.CrossRefPubMed
3.
Jackson MJ, Chaudhury I, Mangera A, Brett A, Watkin N, Chapple CR, Andrich DE, Pickard RS, Mundy AR. A prospective patient-centred evaluation of urethroplasty for anterior urethral stricture using a validated patient-reported outcome measure. Eur Urol. 2013;64(5):777–82.CrossRefPubMed
4.
Jackson MJ, Sciberras J, Mangera A, Brett A, Watkin N, N’Dow J, Chapple CR, Andrich DE, Pickard RS, Mundy AR. Defining a patient-reported outcome measure for urethral stricture disease. Eur Urol. 2011;60(1):60–8.CrossRefPubMed
5.
Angermeier KW, Rourke KF, Dubey D, Forsyth RJ, Gonzalez CM. SIU/ICUD consultation on urethral strictures: evaluation and follow-up. Urology. 2014;83(3 Suppl):S8–17.CrossRefPubMed
6.
Morey AF, McAninch JW. Sonographic staging of anterior urethral strictures. J Urol. 2000;163:1070–5.CrossRefPubMed
7.
Gupta N, Dubey D, Mandhani A, Srivastava A, Kapoor R, Kumar A. Urethral stricture assessment: a prospective study evaluating urethral ultrasonography and conventional radiological studies. BJU Int. 2006;98:149–53.CrossRefPubMed
8.
Heidenreich A, Derschum W, Bonfig R, Wilbert DM. Ultrasound in the evaluation of urethral stricture disease: a prospective study in 175 patients. Br J Urol. 1994;74:93–8.CrossRefPubMed
9.
Buckley JC, Wu AK, McAninch JW. Impact of urethral ultrasonography on decision-making in anterior urethroplasty. BJU Int. 2011;109:438–42.CrossRefPubMed
10.
Smith JC. Urethral resistance to micturition. Br J Urol. 1968;40:125–56.CrossRefPubMed
11.
Sachse H. Treatment of urethral stricture: transurethral slit in view using sharp section. Fortschr Med. 1974;92(1):12–5.PubMed
12.
Bullock TL, Brandes SB. Adult anterior urethral strictures: a national practice patterns survey of board certified urologists in the United States. J Urol. 2007;177(2):685–90.CrossRefPubMed
13.
Steenkamp JW, Heyns CF, de Kock ML. Internal urethrotomy versus dilation as treatment for male urethral strictures: a prospective, randomized comparison. J Urol. 1997;157(1):96–101.CrossRef
14.
Buckley JC, Heyns C, Gilling P, Carney J. SIU/ICUD consultation on urethral strictures: dilation, internal urethrotomy and stenting of male anterior urethral strictures. Urology. 2014;83(3 Suppl):S18–22.CrossRefPubMed
15.
Heyns CF, Steenkamp JW, De Kock ML, Whitaker P. Treatment of male urethral strictures: is repeated dilation or internal urethrotomy useful? J Urol. 1998;160(2):356–8.CrossRefPubMed
16.
Chapple CR, Bhargava S. Management of the failure of a permanently implanted urethral stent – a therapeutic challenge. Eur Urol. 2008;54:665–70.CrossRefPubMed
17.
Morey A, Watkin N, Shenfield O, et al. SIU/ICUD consultation on urethral strictures: anterior urethra – primary anastomosis. Urology. 2014;83(3 Suppl):S23–6.CrossRefPubMed
18.
Mundy AR. Anastomotic urethroplasty. BJU Int. 2005;96:921–44.CrossRefPubMed
19.
Chapple C, Andrich D, Atala A, Barbagli G, Cavalcanti A, Kulkarni S, Mangera A, Nakajima Y. SIU/ICUD consultation on urethral strictures: the management of anterior urethral stricture disease using substitution urethroplasty. Urology. 2014;83(3 Suppl):S31–47.CrossRefPubMed
20.
Mangera A, Patterson JM, Chapple CR. A systematic review of graft augmentation urethroplasty techniques for the treatment of anterior urethral strictures. Eur Urol. 2011;59(5):797–814.CrossRefPubMed
21.
Bhargava S, Patterson JM, Inman RD, MacNeil S, Chapple CR. Tissue-engineered buccal mucosa urethroplasty – clinical outcomes. Eur Urol. 2008;53(6):1263–9.CrossRefPubMed
22.
Turner-Warwick RT. Principles of urethral reconstruction. In: Webster GD, Kirby RS, King L, et al., editors. Reconstructive urology. Oxford: Blackwell Scientific Publications; 1993. p. 609–42.
23.
Koraitim MM, Marzouk ME, Atta MA, Orabi SS. Risk factors and mechanism of urethral injury in pelvic fractures. Br J Urol. 1996;77(6):876–80.CrossRefPubMed
24.
Gomez RG, Mundy T, Dubey D, El-Kassaby AW, Firdaoessaleh, Kodoma R, Santucci R. SIU/ICUD consultation on urethral strictures: pelvic fracture urethral injuries. Urology. 2014;83(3 Suppl):S48–58.CrossRefPubMed
25.
Salchipour M, Khezri A, Askari R, et al. Primary realignment of posterior urethral rupture. J Urol. 2005;2:211–5.
26.
Morey AF, McAninch JW. Reconstruction of the posterior urethral disruption injuries: outcome analysis in 82 patients. J Urol. 1997;157:506–10.CrossRefPubMed
27.
Koraitim MM. Assessment and management of an open bladder neck at posterior urethroplasty. Urology. 2010;76:476–9.CrossRefPubMed
28.
Kizer WS, Armenakas NA, Brandes SB, et al. Simplified reconstruction of the posterior urethral disruption defects: limited role with supracrural rerouting. J Urol. 2007;177:1378–81.CrossRefPubMed
29.
Lumen N, Hoebeke P, Troyer BD, et al. Perineal anastomotic urethroplasty for posttraumatic urethral stricture with or without previous urethral manipulations: a review of 61 cases with long term followup. J Urol. 2009;181:1196–200.CrossRefPubMed
30.
Anderson MJ. The incidence of diverticula in the female urethra. J Urol. 1967;98(1):96–8.
31.
Stewart M, Bretland PM, Stidolph NE. Urethral diverticula in the adult female. Br J Urol. 1981;53(4):353–9.CrossRefPubMed
32.
Rovner ES. Urethral diverticula: a review and an update. Neurourol Urodyn. 2007;26(7):972–7.CrossRefPubMed
33.
Handel LN, Leach GE. Current evaluation and management of female urethral diverticula. Curr Urol Rep. 2008;9(5):383–8.CrossRefPubMed
34.
Patel AK, Chapple CR. Female urethral diverticula. Curr Opin Urol. 2006;16(4):248–54.CrossRefPubMed
35.
Rufford J, Cardozo L. Urethral diverticula: a diagnostic dilemma. BJU Int. 2004;94(7):1044–7.CrossRefPubMed
36.
Saito S. Usefulness of diagnosis by the urethroscopy under anesthesia and effect of transurethral electrocoagulation in symptomatic female urethral diverticula. J Endourol. 2000;14(5):455–7.CrossRefPubMed
37.
Neitlich JD, Foster Jr HE, Glickman MG, et al. Detection of urethral diverticula in women: comparison of a high resolution fast spin echo technique with double balloon urethrography. J Urol. 1998;159(2):408–10.CrossRefPubMed
38.
Daneshgari F, Zimmern PE, Jacomides L. Magnetic resonance imaging detection of symptomatic noncommunicating intraurethral wall diverticula in women. J Urol. 1999;161(4):1259–61.CrossRefPubMed
39.
Leach GE, Sirls LT, Ganabathi K, et al. L N S C3: a proposed classification system for female urethral diverticula. Neurourol Urodyn. 1993;12(6):523–31.CrossRefPubMed
40.
Kuo HC. Videourodynamic characteristics and lower urinary tract symptoms of female bladder outlet obstruction. Urology. 2005;66(5):1005–9.CrossRefPubMed
41.
Reeves FA, Inman RD, Chapple CR. Management of symptomatic urethral diverticula in women: a single-centre experience. Eur Urol. 2014;66(1):164–72.CrossRefPubMed
42.
Pushkar DY, Dyakov VV, Kosko JW, et al. Management of urethrovaginal fistulas. Eur Urol. 2006;50(5):1000–5.CrossRefPubMed
43.
Zimmern PE, Hadley HR, Staskin D, et al. Genitourinary fistulas: vaginal approach for repair of vesicovaginal fistulas. Clin Obstet Gynaecol. 1985;12(2):403–13.PubMed
44.
Groutz A, Blaivas JG, Chaikin DC. Bladder outlet obstruction in women: definition and characteristics. Neurourol Urodyn. 2000;19(3):213–20.CrossRefPubMed
45.
Carr LK, Webster GD. Bladder outlet obstruction in women. Urol Clin North Am. 1996;23(3):385–91.CrossRefPubMed
46.
Osman NI, Mangera A, Chapple CR. A systematic review of surgical techniques used in the treatment of female urethral stricture. Eur Urol. 2013;64(6):965–73.CrossRefPubMed