Q. You are called by the Gynaecology SpR on call. She is concerned about a patient who had an abdominal hysterectomy 2 days ago. The patient is unwell and complaining of left flank pain and a urological injury is suspected by the gynaecology team. What would you do initially?
A. One must consider this a urological emergency and review the patient without delay. Bear in mind that a urological complication of gynaecological surgery may have occurred, and hence may have future medicolegal implications. On arrival, carefully review all the medical notes, especially the operation note, and speak personally to the gynaecological surgeon who performed the procedure, to establish
Indication for surgery (cancer versus benign aetiology)
Difficulties encountered at time of surgery (prolonged procedure, untoward bleeding, presence of adhesions)
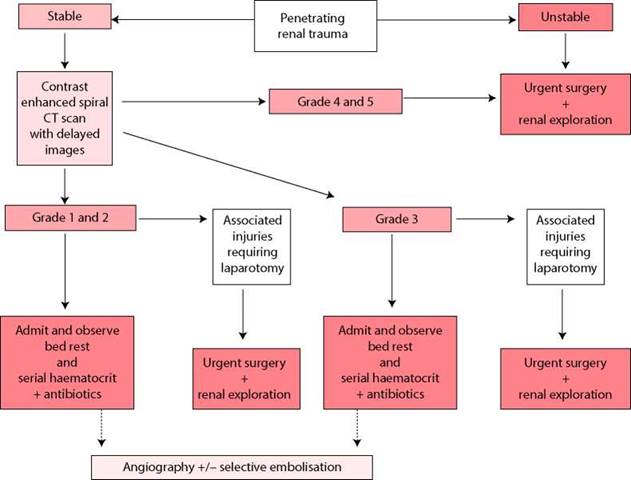
Figure 8.6 Management of penetrating renal trauma in adults (EAU guidelines).
Past medical history, for endometriosis, previous abdominal surgeries and previous radiotherapy treatment
Then take a focussed history, perform a physical examination and carry out necessary investigations.
Q. What features in the history and examination are you interested in?
A. First, characterise the pain (type, location, etc.) and note any previous urological history and the patient’s co-morbidity.
An abdominal examination is necessary looking for scars, full bladder and loin tenderness/mass. Perform a bimanual vaginal examination with a chaperone if the patient can bear it (to look for a vesico-vaginal fistula).
The presence of a pyrexia and tachycardia should be noted as should the patient’s BP. If a drain is present, what is it draining and how much? Is a catheter present? If so, what colour is the urine and how much is the urine output?
Q. Assessment reveals a stable but pyrexial patient with left loin tenderness and excess clear fluid from the drain. What investigations are necessary?
A.
Blood tests - FBC, urea and electrolytes, C-reactive protein and Group & Save (G&S). Urine dipstick and midstream specimen of urine for culture (or catheter specimen urine (CSU) if catheter present).
Drain fluid - Send for biochemical analysis (particularly urea and creatinine - creatinine levels >300 μmol/L will be urine if serum creatinine is normal).
Urgent CT-IVU - To identify the injury and look for another concomitant injury.
A retrograde ureteropyelogram is very sensitive for detecting ureteric injury but may be difficult to arrange in an acute setting (an ultrasound, showing hydronephrosis, has often already been performed but is an insufficient investigation in this scenario).
If a urological injury is suspected the patient should be transferred immediately to a urology ward.
Q. What potential injuries may have occurred?
A. Ureteric (unilateral or bilateral) or bladder or a combination of both.
Q. What does Figure 8.7 show?

Figure 8.7
A. Figure 8.7 is an antegrade nephrostogram demonstrating a left ureteric stricture as a result of iatrogenic injury following gynaecological surgery.
Q. What are the management options? Are you aware of any staging systems for ureteric injury?
A. Management depends on the stage, location and timing of the injury, and the patient’s general condition (Tables 8.2 and 8.3).
Table 8.2 Staging system and management options for ureteric injury
|
Grade of ureteric injury (AAST) |
Injury |
Management |
|
I |
Haematoma only |
Conservative ± stent |
|
II |
Laceration <50% circumference |
Stent ± suture |
|
III |
Laceration >50% circumference |
Stent ± suture Ureteroureterostomy + stent |
|
IV |
Complete tear <2 cm of devascularisation |
Ureteric reconstruction |
|
V |
Complete tear >2 cm of devascularisation |
Ureteric reconstruction |
Ideally, this patient should be taken back to theatre as soon as possible for cystoscopy (excludes associated bladder injury), bilateral retrograde studies (excludes injury to the contralateral ureter), an attempt at retrograde stenting or alternatively formal repair or reconstruction if necessary.
Table 8.3 Options for ureteric reconstruction
|
Location of injury |
Reconstructive option |
|
Upper ureter |
Ureteroureterostomy Ureterocalycostomy Transureteroureterostomy |
|
Mid ureter |
Ureteroureterostomy Boari flap Transureteroureterostomy |
|
Lower ureter |
Ureteroureterostomy Direct reimplantation Psoas hitch Boari flap |
|
Complete injury (e.g. avulsion) |
Ileal interposition Renal autotransplantation |
Traditionally, it has been suggested that if ureteric injury was diagnosed within a few days then, if open repair/reconstruction is needed, this should ideally be performed immediately. However, if the injury was discovered after approximately 7-14 days, then, if open repair/reconstruction is necessary, this should be delayed for at least 3 months (as this is generally thought to be the time of maximal oedema and inflammation). Currently, it is believed that an earlier repair can still give good results and that the time of diagnosis of the ureteric trauma is not so important.
Delayed repair is certainly essential if the patient is unwell or there are any contraindications for re-operation, e.g. infected urinoma at site of injury. In these cases, nephrostomy drainage should be arranged. A careful attempt at antegrade stenting can be tried in expert centres (Figure 8.8).

Figure 8.8 Antegrade guidewire prior to stenting across iatrogenic ureteric stricture.
Q. What basic principles govern ureteric reconstruction?
A.
1. Mobilization of the ureter preserving the adventitia
2. Debridement of non-viable tissue
3. Spatulation
4. Tension-free mucosa to mucosa anastomosis with fine absorbable sutures (5 or 6 O)
5. An internal ureteric stent and separate drain placed near site of anastomosis
Omental interposition to separate the repair from associated intra-abdominal injuries or suture lines is recommended.
A. bladder catheter should be inserted to limit stent reflux.
Q. How would you manage the patient post-operatively?
A. Remove the bladder catheter 2 days post-operatively. The drain can also be removed at day 2 if output is minimal. The ureteric stent is removed at 6 weeks. A dynamic renogram and IVU are arranged at 3 months (or earlier if the patient has worrying symptoms).
Q. How do missed ureteric injuries present?
A. Missed ureteric injuries are relatively common. They may present with ureteric obstruction (stricturing), urinoma, abscess formation, or fistulation. Ureteric obstruction can result in nephron loss, stones, infection and pain.
Q. What is the likely outcome of ureteric injuries?
A. The outcome of ureteric reconstruction is usually favourable if the principles outlined above are adhered to. Ureteric reflux may result from reconstruction but this is not felt to be an important problem in the adult patient.
Q. What is the role of the interventional radiologist in ureteric injury and reconstruction?
A. The interventional radiologist has several key roles:
Relieving renal obstruction by percutaneous nephrostomy.
Performing nephrostoureterograms which are essential in planning definitive management.
Antegrade stenting with or without retrograde assistance (‘rendezvous procedure’) may be definitive in partial or short ureteric defects although this requires careful follow-up to look for ureteric stricturing.
Balloon dilatation of ureteric strictures may be successful in 50% of cases.
Q. What is the role of ureteroscopy in managing ureteric strictures?
A. Short ureteric strictures can be managed by incision ± balloon dilatation and stenting.
Success rates have been quoted at 75%. Endoscopic treatment of strictures of 2 cm or greater have high failure rates. Longer-term stents are being evaluated and may become established as an option in the future in well-selected patients.
Q. Is there a role for laparoscopy in ureteric reconstruction?
A. Yes, experienced laparoscopists have successfully reconstructed ureteric injuries and this may in the future be the surgical approach of choice.