The excessive use of antimicrobials (antibiotics) for the treatment of conditions for which these drugs provide little or no benefit (upper respiratory tract infections, bronchitis) has contributed to the emergence of bacterial resistance. It is estimated that 21% of all prescriptions written for antimicrobials are for ambulatory patients seen in physicians’ offices with the diagnosis of upper respiratory tract infections or bronchitis.1
Misuse of antibiotics in the general population is in contrast to the proven benefit of antibiotic prophylaxis for selected surgical procedures, which has been part of a national initiative to enhance compliance, the Surgical Care Improvement Project (SCIP). SCIP, based originally on the Surgical Infection Project (SIP), was designed to combat a perceived national crisis of preventable surgical site infections, identified in the 1990s, which were associated with doubled risk of mortality, 60% higher likelihood of spending time in an intensive care unit, and fivefold risk of readmission.2 The SIP was expanded to the SCIP to include additional perioperative quality measures related to infection control (Table 41-1).3 Each of these measures has been independently associated with a reduction in surgical site infection in clinical trials. The original SCIP goal was a 25% reduction in surgical site infection by 2010. This goal was not met. However, a new goal of 25% reduction was set for 2013 and the latest data analysis suggests that the goal may have been met with 20% reduction achieved in 2012.4

The baseline risk for perioperative infection is highly dependent on factors that require risk adjustment in clinical trials and consideration in clinical care. Patient-related risk factors for surgical site infection include extremes of age (younger than 5 and older than 65 years), poor nutritional status, obesity, diabetes mellitus and perioperative glycemic control, peripheral vascular disease, tobacco use, coexistent infections, altered immune response, corticosteroid therapy, preoperative skin preparation (surgical scrub and hair removal), and length of preoperative hospitalization. Institutional variables include surgical experience and technique (i.e., open vs. laparoscopic), duration of procedure, hospital environments including sterilization of instruments, and maintenance of perioperative normothermia.5,6
Of the aforementioned variables, few are modifiable at the time of surgery. Good perioperative glucose control can reduce infection risk. Perioperative glucose control has been studied predominantly in the cardiothoracic surgery population where it is associated with about a 50% decrease in deep sternal infection.7 Continuous insulin infusion was associated with an additional reduction in surgical site infection compared to intermittent subcutaneous injection.8 These trials are the basis of SCIP measure 4. These findings have been generalized to bowel surgery where patients whose glucose was maintained below 200 mg/dL for 48 hours after surgery compared with those having concentrations greater than 200 mg/dL had significantly fewer surgical site infections (29.7% vs. 14.3%).9 However, intensive insulin regimens designed to keep blood sugar ultralow have shown higher hypoglycemia and mortality compared to conventional treatment.10
Although more difficult to achieve, smoking cessation is a perioperative goal. Perioperative education on smoking cessation by surgeons and anesthesiologists in preoperative evaluation is important. The preoperative period has been called a “teachable moment” and even brief smoking cessation can reduce infection risk. A meta-analysis of four studies that have assessed the effect of 4 to 8 weeks of preoperative smoking cessation demonstrates a risk reduction of approximately 50%.11
The anesthesiologist should contribute to the maintenance of perioperative normothermia. It is logical that hypothermia will result in peripheral vasoconstriction, decreased wound oxygen tension and recruitment of leukocytes, favoring infection and impaired healing. In a meta-analysis of trials comparing intraoperative warming to control, warming was associated with a 64% decrease in surgical site infections.12 Prewarming patients before surgery reduces the peripheral to core temperature gradient and has the added advantage of making placement of intravenous lines easier because of peripheral vasodilation. Active prewarming of volunteers for 2 hours resulted in maintenance of core temperatures above 36°C for 60 minutes of general anesthesia at ambient temperature, whereas core temperatures in unwarmed subjects dropped an average of 1.9°C to below 35°C.
Immunosuppression on the basis of long-term use of corticosteroids has been considered a risk factor for surgical site infection. However, there are surprisingly few studies to support this supposition. In a study of infection after mastectomy, steroid use was not found to be associated with surgical site infection. In contrast, long-term steroid treatment was associated with anastomotic leaks in bowel surgery.13There is clear evidence that a single dose of corticosteroid given to prevent nausea and vomiting and reduce pain does not promote infection. For example, in a study of open abdominal surgery for gynecologic cancer, there were no excess wound infections in patients treated with a single dose of dexamethasone for nausea and vomiting prophylaxis.14
Antimicrobial Prophylaxis for Surgical Procedures
The use of antimicrobial prophylaxis in surgery involves a risk-to-benefit evaluation, which varies depending on the nature of the operative procedure. SCIP measure 1 recommends that prophylactic antimicrobials should be administered intravenously (IV) within 1 hour of surgical incision. The general concept is that tissue concentration of the antibiotic should exceed the minimum inhibitory concentration (MIC) associated with the procedure and or patient characteristics from the time of incision to the completion of surgery. For short-acting antibiotics, this may require redosing (Table 41-2). Antibiotic treatment is not recommended for no longer than 24 hours. This recommendation is based on findings of no benefit to prolonged dosing but rather an increased incidence of drug-resistant organisms.

The antibiotic chosen should be appropriate for the most likely microorganism related to the procedure and patient characteristics (SCIP measure 2). For clean elective surgical procedures such as mastectomy and thyroidectomy in which no tissue (other than the skin) carrying an indigenous flora is penetrated, the risks of routine antimicrobial prophylaxis outweigh the possible benefits. The predominant organisms causing surgical site infections after clean procedures are skin flora (Staphylococcus aureus and Staphylococcus epidermidis). In clean-contaminated procedures, including abdominal procedures and solid organ transplantation, the most common organisms include gram-negative rods and enterococci in addition to skin flora.15 Antibiotic recommendations for specific procedure prophylaxis can be found in Table 41-3.16


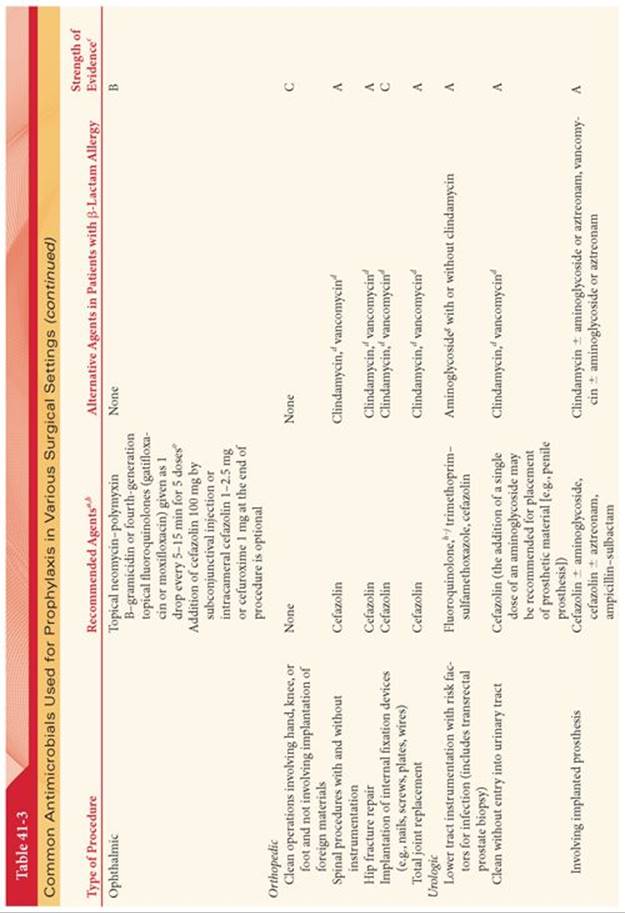


Because of their wide therapeutic index and low incidence of side effects, cephalosporins (most often a cost-effective first-generation cephalosporin such as cefazolin) are the antimicrobials of choice for surgical procedures in which skin flora and normal flora of the gastrointestinal and genitourinary tracts are the most likely pathogens. Patients with documented immunoglobulin E (IgE) reaction to cephalosporins are rare and often mistaken for more common intolerances such as nausea or yeast infection. IgE-mediated anaphylactic reactions to antimicrobials usually occur 30 to 60 minutes after dosing and often include urticaria, bronchospasm, and hemodynamic collapse. This reaction is a life-threatening emergency that precludes subsequent use of the drug. Cephalosporins can safely be used in patients with an allergic reaction to penicillins that is not an IgE-mediated reaction (e.g., anaphylaxis, urticaria, bronchospasm) or exfoliative dermatitis (Stevens-Johnson syndrome, toxic epidermal necrolysis).17Although early reports of cross-reactivity were high due to contaminated drug lots, the actual rate of cross-reactivity is only 1%.17However, the consequences of true anaphylaxis are severe. Patients should be carefully questioned about the nature of any drug allergy.
In patients with documented IgE-mediated anaphylactic reactions, β-lactam antibiotics can usually be substituted with clindamycin or vancomycin.16 Vancomycin may also be considered when methicillin-resistant S. aureus(MRSA) is considered likely, for example in children or elderly patients known to be colonized with MRSA. Nasal application of mupirocin has been considered as an alternative and has been found to be effective in eliminating MRSA colonization in adults and children. It is U.S. Food and Drug Administration approved for eradication of colonization in adults and health care workers. Treatment with mupirocin is effective in reducing S. aureus infection in documented carriers. Preoperative screening is recommended to identify high-risk patients who would benefit from decolonization and to guide appropriate preoperative antibiotic selection for those with resistant organisms. Routine prophylaxis with vancomycin is not recommended for any patient population in the absence of documented or highly suspected colonization or infection with MRSA (recent hospitalization of nursing home stay and hemodialysis patients) or known IgE-mediated response to β-lactam antibiotics.18 The recommendation against routine prophylaxis with vancomycin is due to concerns about selection of resistant organisms, its risk of inducing hemodynamic instability due to histamine release (red man syndrome; Fig. 41-1) if given rapidly, and evidence that vancomycin is less effective than cephazolin in methicillin-susceptible S. aureus.19,20

Clean-contaminated procedures such as colorectal and abdominal surgeries require additional coverage for gram-negative rods and anaerobes in addition to skin flora. Metronidazole can be added to cefazolin or cefoxitin, cefotetan, ampicillin-sulbactam, ertapenem, or ceftriaxone.
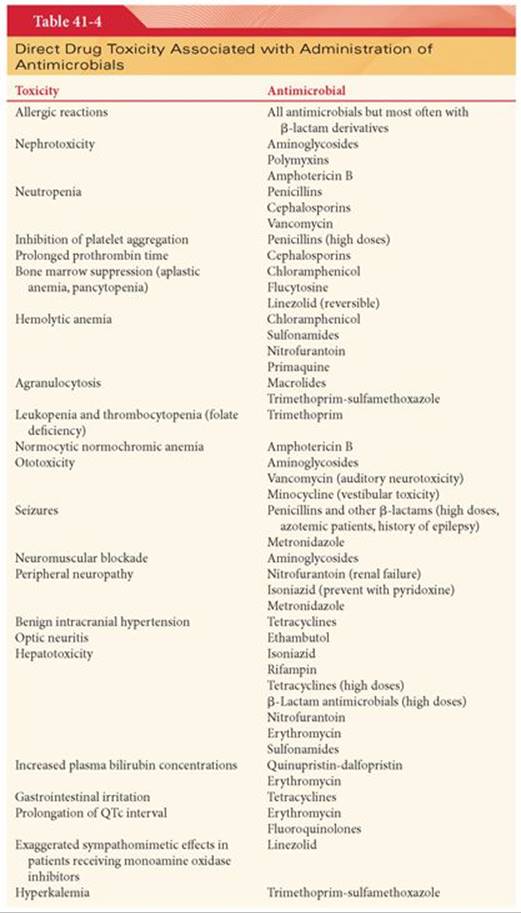
Bowel preparation with oral antimicrobials has been studied as a potentially less costly alternative. Mechanical bowel preparation alone does not reduce infection, but selective decontamination of the digestive tract with oral topical polymyxin, tobramycin, and amphotericin eradicates the colonization gram-negative microorganisms, S. aureus, and yeasts from oral cavity to rectum. Vancomycin would be active against MRSA but is not recommended because gram-positive flora plays an important role in the resistance to colonization.21 In a meta-analysis of eight studies, the combination of oral treatment and perioperative venous prophylaxis was found to be superior to IV prophylaxis alone in preventing surgical site infection and anastomotic leak. However, older studies found that oral antibiotics alone are not a solution. A randomized controlled study was stopped because of higher rate of infection in the oral neomycin and erythromycin group (41%) compared with the single-dose IV metronidazole and ceftriaxone group.22 Another trial of oral metronidazole and kanamycin compared with the same medications given IV found an increased rate of postoperative sepsis and pseudomembranous colitis in the oral group.23Pseudomembranous colitis is the most frequent complication of prophylactic antimicrobials, including the IV cephalosporins. Additional toxicities are covered in Table 41-4.

Antimicrobial Selection
Prompt identification of the causative organism is essential for the selection of appropriate antimicrobial drugs to treat ongoing infection. The efficacy of antimicrobial therapy depends on drug delivery to the site of infection. Transport across the blood–brain barrier varies greatly among antimicrobials. Antimicrobial therapy is more likely to be effective if the infected material (foreign body, prosthesis) is removed. Infections behind obstructing lesions such as pneumonia behind a blocked bronchus will not respond to antimicrobials until the obstruction is relieved.
Nosocomial Infections
Nearly 80% of nosocomial infections occur in three sites (urinary tract, respiratory system, and bloodstream). The incidence of nosocomial infections is highly associated with the use of devices such as ventilators, vascular access catheters, and urinary catheters. Intravascular access catheters are the most common causes of bacteremia or fungemia in hospitalized patients.24 The organism infecting access catheters most commonly comes from the colonized hub or lumen and reflect skin flora (S. aureus and S. epidermidis). Initial therapy of suspected intravascular catheter infection usually includes vancomycin because of the high incidence of MRSA and methicillin-resistant S. epidermidisin the nosocomial environment.
Special Patient Groups
Parturients
Administration of antimicrobials during pregnancy introduces the question of safety for the mother and fetus (Table 41-5). Most antimicrobials cross the placenta and enter maternal milk. The immature fetal liver may lack enzymes necessary to metabolize certain drugs such that pharmacokinetics and toxicities in the fetus are often different from those in older children and adults. Teratogenicity is a concern when any drug is administered during early pregnancy. Increases in maternal blood volume, glomerular filtration rate, and hepatic metabolic activity may decrease plasma antimicrobial concentrations (10% to 50%), especially late in pregnancy and in the early postpartum period. In some parturients, delayed gastric emptying may decrease absorption of orally administered antimicrobials.

Elderly Patients
Physiologic changes that occur with increasing age can alter oral absorption (decreased gastric acidity, reduced gastrointestinal motility), distribution (increased total body fat, decreased plasma albumin concentrations), metabolism (decreased hepatic blood flow), and excretion (decreased glomerular filtration rate) of antimicrobials. Penicillins and cephalosporins, because of their large therapeutic index, obviate the need for significant changes in dosage schedules in elderly patients who have normal serum creatinine concentrations. Conversely, administration of aminoglycosides and vancomycin to elderly patients may require adjustments in dosing regimens. Measurement of plasma concentrations of antimicrobials and monitoring of renal function may be indicated when administering certain antimicrobials to elderly patients.
HIV-Infected Patients
There has been concern about increased risk of postoperative infection in HIV-infected patients based on their increased risk for opportunistic infection in the setting of reduced T4 cell counts. Several recent studies have addressed this issue and produced conflicting results.25–27 Favorable results appear to be related to good preoperative control on an antiretroviral regimen with preserved T4 cell counts.28
Antibacterial Drugs Commonly Used in the Perioperative Period
Penicillins
The basic structure of penicillins is a dicyclic nucleus (aminopenicillanic acid) that consists of a thiazolidine ring connected to a β-lactam ring. The penicillins may be classified into subgroups because of their structure, β-lactamase susceptibility, and spectrum of activity. The bactericidal action of penicillins reflects the ability of these antimicrobials to interfere with the synthesis of peptidoglycan, which is an essential component of cell walls of susceptible bacteria. Penicillins also decrease the availability of an inhibitor of murein hydrolase such that the uninhibited enzyme can then destroy (lyse) the structural integrity of bacterial cell walls. Cell membranes of resistant gram-negative bacteria are in general resistant to penicillins because they prevent access to sites where synthesis of peptidoglycan is taking place.
Clinical Indications
Penicillin is the drug of choice for treatment of pneumococcal, streptococcal, and meningococcal infections. Gonococci have gradually become more resistant to penicillin, requiring higher doses for adequate treatment. Treatment of syphilis with penicillin is highly effective. Penicillin is the drug of choice for treating all forms of actinomycosis and clostridial infections causing gas gangrene.
Prophylactic administration of penicillin is highly effective against streptococcal infections, accounting for its value in patients with rheumatic fever. Transient bacteremia occurs in the majority of patients undergoing dental extractions, emphasizing the importance of prophylactic penicillin in patients with congenital or acquired heart disease or tissue implants undergoing dental procedures. Transient bacteremia may also accompany surgical procedures, such as tonsillectomy and operations on the genitourinary and gastrointestinal tracts, and vaginal delivery.
Administration of high doses of penicillin G IV to patients with renal dysfunction may result in neurotoxicity and hyperkalemia (10 million U of penicillin G contains 16 mEq of potassium). If this amount of potassium introduces a risk to the patient, a sodium salt of penicillin G or a sodium salt of a similar penicillin, such as ampicillin or carbenicillin, can be substituted for the aqueous penicillin G.
Other drugs should not be mixed with penicillin as the combination may inactivate the antimicrobial. Intrathecal administration of penicillins is not recommended because these drugs are potent convulsants when administered by this route. Furthermore, arachnoiditis and encephalopathy may follow intrathecal penicillin administration.
Excretion
Renal excretion of penicillin is rapid (60% to 90% of an intramuscular [IM] dose is excreted in the first hour), such that the plasma concentration decreases to 50% of its peak value within 1 hour after injection. Approximately 10% is eliminated by glomerular filtration, and 90% is eliminated by renal tubular secretion. Anuria increases the elimination half-time of penicillin G approximately 10-fold.
Duration of Action
Methods to prolong the duration of action of penicillin include the simultaneous administration of probenecid, which blocks the renal tubular secretion of penicillin. Alternatively, the IM injection of poorly soluble salts of penicillin, such as procaine or benzathine, delays absorption and thus prolongs the duration of action. Procaine penicillin contains 120 mg of the local anesthetic for every 300,000 U of the antimicrobial. Possible hypersensitivity to procaine must be considered when selecting this form of the antimicrobial for administration.
Penicillinase-Resistant Penicillins
The major mechanism of resistance to the penicillins is bacterial production of β-lactamase enzymes that hydrolyze the β-lactam ring, rendering the antimicrobial molecule inactive. Methicillin (dimethoxybenzylpenicillin), oxacillin, nafcillin, cloxacillin, and dicloxacillin are not susceptible to hydrolysis by staphylococcal penicillinases that would otherwise hydrolyze the cyclic amide bond of the β-lactam ring and render the antimicrobial inactive. Specific indications for these drugs are infections caused by staphylococci known to produce this enzyme. Penetration of nafcillin into the central nervous system (CNS) is sufficient to treat staphylococcal meningitis. Parenteral methicillin has largely been superseded by oxacillin and nafcillin. Hemorrhagic cystitis and an allergic interstitial nephritis (hematuria, proteinuria) may accompany administration of methicillin. Hepatitis has been associated with high-dose oxacillin therapy. Renal excretion of methicillin, oxacillin, and cloxacillin is extensive. More than 80% of an IV dose of nafcillin is excreted in the bile, which may be an advantage when high-dose therapy is necessary in a patient with impaired renal function.
Oxacillin and nafcillin, unlike methicillin, are relatively stable in an acidic medium, resulting in adequate systemic absorption after oral administration. Nevertheless, variable absorption from the gastrointestinal tract often dictates a parenteral route of administration for treatment of serious infections caused by penicillinase-producing staphylococci. Cloxacillin and dicloxacillin are available only as oral preparations and may be preferable because they produce higher blood levels than do oxacillin and nafcillin.
Penicillinase-Susceptible Broad-Spectrum Penicillins (Second-Generation Penicillins)
Broad-spectrum penicillins, such as ampicillin, amoxicillin, and carbenicillin, have a wider range of activity than other penicillins, being bactericidal against gram-positive and gram-negative bacteria. They are, nevertheless, all inactivated by penicillinase produced by certain gram-negative and gram-positive bacteria. Therefore, these drugs are not effective against most staphylococcal infections.
Ampicillin
Ampicillin (α-aminobenzylpenicillin) has a broader range of activity than penicillin G. Its spectrum encompasses not only pneumococci, meningococci, gonococci, and various streptococci but also a number of gram-negative bacilli, such as Haemophilus influenzae and Escherichia coli. Ampicillin is stable in acid and thus is well absorbed after oral administration, although peak plasma concentrations are lower than those achieved after administration of penicillin V. Approximately 50% of an oral dose of ampicillin is excreted unchanged by the kidneys in the first 6 hours, emphasizing that renal function greatly influences the duration of action of this antimicrobial. Ampicillin also appears in the bile and undergoes enterohepatic circulation. Among the penicillins, ampicillin is associated with the highest incidence of skin rash (9%), which typically appears 7 to 10 days after initiation of therapy. Many of these rashes are due to protein impurities in the commercial preparation of the drug and do not represent true allergic reactions.
Amoxicillin
Amoxicillin is chemically identical to ampicillin except for an −OH substituent instead of an −H on the side chain. Its spectrum of activity is identical to that of ampicillin, but it is more efficiently absorbed from the gastrointestinal tract than ampicillin, and effective concentrations are present in the circulation for twice as long.
Extended-Spectrum Carboxypenicillins (Third-Generation Penicillins)
Carbenicillin
Carbenicillin (α-carboxybenzylpenicillin) results from the change from an amino to carboxy substituent on the side chain of ampicillin. The principal advantage of carbenicillin is its effectiveness in the treatment of infections caused by Pseudomonas aeruginosa and certain Proteus strains that are resistant to ampicillin. This antimicrobial is penicillinase susceptible and therefore ineffective against most strains of S. aureus. Carbenicillin is not absorbed from the gastrointestinal tract; therefore, it must be administered parenterally. The elimination half-time is approximately 1 hour and is prolonged to approximately 2 hours when there is hepatic or renal dysfunction. Approximately 85% of the unchanged drug is recovered in urine over 9 hours. Probenecid, by delaying renal excretion of the drug, increases the plasma concentration of carbenicillin by approximately 50%.
The sodium load administered with a large dose of carbenicillin (30 to 40 g) is considerable because greater than 10% of carbenicillin is sodium (about 5 mEq/g). Congestive heart failure may develop in susceptible patients in response to this acute drug-produced sodium load. Hypokalemia and metabolic alkalosis may occur because of obligatory excretion of potassium with the large amount of nonreabsorbable carbenicillin. Carbenicillin interferes with normal platelet aggregation such that bleeding time is prolonged but platelet count remains normal.
Extended-Spectrum Acylaminopenicillins (Fourth-Generation Penicillins)
The acylaminopenicillins (mezlocillin, piperacillin, azlocillin) have the broadest spectrum of activity of all the penicillins. Like the carboxypenicillins, the acylaminopenicillins are derivatives of ampicillin. These drugs are ineffective against penicillinase-producing strains of S. aureus. The acylaminopenicillins have lower sodium content than the carboxypenicillins but otherwise the side effects are similar. Clinical studies have not demonstrated that these antimicrobials are superior to the carboxypenicillins.
Penicillin β-Lactamase Inhibitor Combinations
Clavulanic acid, sulbactam, and tazobactam are β-lactam compounds that have little intrinsic antimicrobial activity. However, these compounds bind irreversibly to the β-lactamase enzymes, which are produced by many bacteria, thus inactivating these enzymes and rendering the organisms sensitive to β-lactamase–susceptible penicillins. Clavulanic acid is available with oral amoxicillin and parenteral ampicillin preparations have been combined with sulbactam.
Cephalosporins
Cephalosporins, like the penicillins, are bactericidal antimicrobials that inhibit bacterial cell wall synthesis and have a low intrinsic toxicity. These antimicrobials are derived from 7-aminocephalosporanic acid. Resistance to the cephalosporins, as to the penicillins, may be due to an inability of the antimicrobial to penetrate to its site of action. Bacteria can also produce cephalosporinases (β-lactamases), which disrupt the β-lactam structure of cephalosporins and thus inhibit their antimicrobial activity. Like the newer penicillins, the new cephalosporins have an extraordinarily broad spectrum of antimicrobial action but are expensive.
Individual cephalosporins differ significantly with respect to the extent of absorption after oral ingestion, severity of pain produced by IM injection, and protein binding. IV administration of any of the cephalosporins can cause thrombophlebitis. Diacetyl metabolites of cephalosporins can occur and are associated with decreased antimicrobial activity.
A positive Coombs’ reaction frequently occurs in patients who receive large doses of cephalosporins. Hemolysis, however, is rarely associated with this response. Nephrotoxicity owing to cephalosporins, with the exception of cephaloridine, is less frequent than after administration of aminoglycosides or polymyxins.
The incidence of allergic reactions in patients being treated with cephalosporins ranges from 1% to 10%. The majority of the allergic reactions consist of cutaneous manifestations, which occur 24 hours after drug exposure. Life-threatening anaphylaxis is estimated to occur in 0.02% of treated patients.29 Because the cephalosporins share immunologic cross-reactivity, patients who are allergic to one cephalosporin are likely to be allergic to others. The possibility of cross-reactivity between cephalosporins and penicillins seems to be very infrequent, and cephalosporins are often selected as alternative antimicrobials in patients with a history of penicillin allergy.29
Cephalosporins and Allergy to Penicillins
Hypersensitivity is the most common adverse reaction to β-lactam antimicrobials. Allergic reactions are noted in 1% to 10% of patients treated with penicillins, making these antimicrobials the most allergenic of all drugs.30 Most often, the allergic response is a delayed reaction characterized by a maculopapular rash and/or fever. Less often but more serious is immediate hypersensitivity that is mediated by IgE antibodies. Manifestations of immediate hypersensitivity may include laryngeal edema, bronchospasm, and cardiovascular collapse. Allergic reactions may occur in the absence of previous known exposure to any of the penicillins. This may reflect prior unrecognized exposure to penicillin, presumably in ingested foods. Allergic reactions can occur with any dose or route of administration, although severe anaphylactic reactions are more often associated with parenteral than with oral administration. Some patients who experience cutaneous reactions may continue to receive the offending penicillin or receive the same penicillin in the future without experiencing a similar response.
The penicillin molecule itself is probably unable to form a complete antigen, but instead the ring structure of penicillin is opened to form a hapten metabolite, penicilloyl. Approximately 95% of patients allergic to penicillin form this penicilloyl-protein conjugate (the major antigenic determinant); the remaining allergic patients form 6-aminopenicillic acid and benzylpenamaldic acid (minor antigenic determinants). Skin testing with a polyvalent skin test antigen, penicilloyl-polylysine, makes it possible to detect most patients who would develop a life-threatening allergic reaction if treated with a penicillin antimicrobial. Nevertheless, minor antigenic determinants that would not be detected by skin testing may produce severe allergic reactions.
Cross-Reactivity
The presence of a common nucleus (β-lactam ring) in the structure of all penicillins means that allergy to one penicillin increases the likelihood of an allergic reaction to another penicillin. Furthermore, there would seem to be the potential for cross-reactivity between penicillins and cephalosporins as they both share a common β-lactam ring. However, actual cross-reactivity is rare.17,29
Classification
Cephalosporins are classified as first-, second-, and third-generation because of their antimicrobial spectrum. In general, activity against gram-positive cocci decreases, and activity against gram-negative cocci increases from the first- to third-generation cephalosporins. First-generation cephalosporins are inexpensive, exhibit low toxicity, and are as active as second- and third-generation cephalosporins against staphylococci and nonenterococcal streptococci. For these reasons, first-generation cephalosporins have been commonly selected for antimicrobial prophylaxis in patients undergoing cardiovascular, orthopedic, biliary, pelvic, and intraabdominal surgery (see the section “Antimicrobial Prophylaxis for Surgical Procedures”). All cephalosporins can penetrate into joints and can readily cross the placenta.
First-Generation Cephalosporins
Cephalothin is the prototype of first-generation cephalosporins. Like most other cephalosporins, cephalothin is excreted largely unaltered by the kidneys, emphasizing the need to decrease the dose in the presence of renal dysfunction. Oral absorption is poor and IM injection is painful, accounting for its common administration by the IV route. Although cephalothin is present in many tissues and fluids, it does not enter the cerebrospinal fluid in significant amounts and is not recommended for treatment of meningitis. Cefazolin has essentially the same antimicrobial spectrum as cephalothin but has the advantage of achieving higher blood levels, presumably due to slower renal elimination. In this regard, cefazolin is viewed as the drug of choice for antimicrobial prophylaxis for many surgeries. This drug is well tolerated after IM or IV injection.
Second-Generation Cephalosporins
Cefoxitin and cefamandole are examples of second-generation cephalosporins with extended activity against gram-negative bacteria. Cefoxitin is resistant to cephalosporinases produced by gram-negative bacteria. Cefamandole is pharmacologically similar to cefoxitin, but its methylthiotetrazole side chain poses a risk of bleeding and disulfiram-like reactions with concurrent use of alcohol. Both drugs are excreted predominantly unchanged by the kidneys. Cefuroxime is more effective than cefamandole against H. influenzae and is the only second-generation cephalosporin effective in the treatment of meningitis.
Third-Generation Cephalosporins
Third-generation cephalosporins have an enhanced ability to resist hydrolysis by the β-lactamases of many gram-negative bacilli including E. coli, Klebsiella, Proteus, and H. influenzae. Unlike older cephalosporins, the third-generation cephalosporins achieve therapeutic levels in the cerebrospinal fluid and can be used to treat meningitis. The third-generation cephalosporins seem to have the same relatively low toxicities as the older cephalosporins.
Cefotaxime was the first third-generation cephalosporin and has been effective in a broad range of infections, including meningitis caused by gram-negative bacilli other than Pseudomonas. The elimination half-time of this antimicrobial is approximately 1 hour, with clearance via the kidneys and hepatic metabolism. An adjustment in dosage or dosing interval is indicated in patients with renal dysfunction who are being treated with this drug. Approximately 30% of cefotaxime is excreted as a desacetyl derivative that has antibacterial activity and is synergistic with the parent compound. Ceftriaxone has the longest elimination half-time of any third-generation cephalosporin and is highly effective against gram-negative bacilli, especially Neisseria and Haemophilus. Cefixime is an orally effective third-generation cephalosporin that is as active as other cephalosporins against pneumococci, group A streptococci, and H. influenzae but less active against S. aureus and not active against anaerobes such as Pseudomonas. The spectrum of activity of cefixime and a single daily dose make it attractive for upper respiratory tract infections, but less expensive alternatives are available.
Other β-Lactam Antimicrobials
Aztreonam
Aztreonam is a monobactam antimicrobial that lacks the thiazolidine ring present in penicillins and the dihydrothiazine ring found in cephalosporins. The antimicrobial activity of this drug is limited to gram-negative bacteria. Aztreonam is not absorbed from the gastrointestinal tract, but therapeutic blood levels are achieved after IM or IV administration in most body tissues and fluids, including cerebrospinal fluid. The elimination half-time is about 1.5 hours, and clearance is principally by glomerular filtration. Neither nephrotoxicity nor bleeding disorders have been reported. A unique advantage is the absence of any cross-reactivity between aztreonam and circulating antibodies of penicillin- or cephalosporin-allergic patients.31 Because aztreonam combines the activity of the aminoglycosides with the low toxicity of the β-lactam antimicrobials, it can replace aminoglycosides in the treatment of many gram-negative infections. A potential disadvantage of aztreonam is the development of enterococcal superinfections. This antimicrobial is significantly more expensive than aminoglycosides.
Aminoglycoside Antimicrobials
Aminoglycosides are poorly lipid-soluble antimicrobials that are rapidly bactericidal for aerobic gram-negative bacteria. As would be predicted with the poor lipid solubility of these drugs, less than 1% of an orally administered aminoglycoside is absorbed into the systemic circulation. Aminoglycosides have a volume of distribution similar to the extracellular fluid volume and undergo extensive renal excretion due almost exclusively to glomerular filtration. There is a linear relationship between the plasma creatinine concentration and the elimination half-time of aminoglycosides. In the presence of normal renal function, the elimination half-time of aminoglycosides is 2 to 3 hours and is prolonged 20- to 40-fold in the presence of renal failure. Determination of the plasma concentration of aminoglycosides is an essential guide to the safe administration of these antimicrobials in the setting of renal dysfunction. The role of aminoglycosides is influenced by their toxicity (see the section “Side Effects”) and cost-effectiveness relative to other antibiotics with broad gram-negative coverage.
Streptomycin was the first parenterally administered antimicrobial that was active against many gram-negative bacilli and Mycobacterium tuberculosis. Current use of this drug is limited because of the rapid emergence of resistant organisms, the frequent occurrence of vestibular damage during prolonged treatment, and the availability of less toxic antimicrobials.
Gentamicin is active against P. aeruginosa as well as the gram-negative bacilli. Gentamicin penetrates pleural, ascitic, and synovial fluids in the presence of inflammation. Monitoring plasma concentrations of gentamicin is the best approach for recognizing potentially toxic levels (>9 µg/mL). If plasma concentrations of gentamicin cannot be monitored, the dose can be adjusted based on the plasma creatinine concentration.
Amikacin is a semisynthetic derivative of kanamycin that has the advantage of not being associated with the development of resistance. The principal use of amikacin is in the treatment of infections caused by gentamicin- or tobramycin-resistant gram-negative bacilli. Unlike other aminoglycosides, this drug should not be administered in combination with penicillin, which may result in antagonism of the bactericidal actions of penicillin against some strains of Enterococcus faecalis. The incidence of nephrotoxicity and ototoxicity is similar to that produced by gentamicin.
Neomycin is commonly used for topical application to treat infections of the skin (as after burn injury), cornea, and mucous membranes. Allergic reactions occur in 6% to 8% of patients treated with topical neomycin. Oral neomycin does not undergo systemic absorption and is thus administered to decrease bacterial flora in the intestine before gastrointestinal surgery and as an adjunct to the therapy of hepatic coma (decreases blood ammonia concentrations).
Side Effects
The side effects of aminoglycosides that limit their clinical usefulness include ototoxicity, nephrotoxicity, skeletal muscle weakness, and potentiation of nondepolarizing neuromuscular blocking drugs. These side effects parallel the plasma concentration of the aminoglycoside, emphasizing the need to decrease the dose of these drugs in patients with renal dysfunction.
Ototoxicity
Ototoxicity manifests as vestibular dysfunction, auditory dysfunction, or both and parallels the accumulation of aminoglycosides in the perilymph of the inner ear. There is drug-induced destruction of vestibular or cochlear sensory hairs that is dose-dependent and most likely occurs with chronic therapy, especially in elderly patients, in whom renal dysfunction is more likely. Furosemide, mannitol, and probably other diuretics seem to accentuate the ototoxic effects of aminoglycosides. Vestibular toxicity manifests as nystagmus, vertigo, nausea, and the acute onset of Ménière’s syndrome. Auditory dysfunction manifests as tinnitus or a sensation of pressure or fullness in the ears. Deafness may develop suddenly.
Nephrotoxicity
Aminoglycosides accumulate in the renal cortex and can produce acute tubular necrosis that initially manifests as an inability to concentrate urine and the appearance of proteinuria and red blood cell casts. These changes are usually reversible if the drug is discontinued. Neomycin is the most nephrotoxic of the aminoglycosides and therefore is not administered by the parenteral route.
Skeletal Muscle Weakness
Skeletal muscle weakness can occur with the intrapleural or intraperitoneal institution of large doses of aminoglycosides. This effect is most likely because of the ability of aminoglycosides to inhibit the prejunctional release of acetylcholine while also decreasing postsynaptic sensitivity to the neurotransmitter. IV administration of calcium overcomes the effect of aminoglycosides at the neuromuscular junction. Patients with myasthenia gravis are uniquely susceptible to skeletal muscle weakness if treated with an aminoglycoside. Administration of a single dose of an aminoglycoside is unlikely to produce skeletal muscle weakness in an otherwise healthy patient.
Macrolides
Macrolides are stable in the presence of acidic gastric fluid, and as a result, these antimicrobials are well absorbed from the gastrointestinal tract. Structurally, these antimicrobials are characterized by 14 to 16 carbon atoms joined together in a complex, central molecule that is linked to various side chains.
Erythromycin
Erythromycin has a spectrum of activity, which includes most gram-positive bacteria, Streptococcus pneumoniae, S. aureus, Moraxella catarrhalis, H. influenzae, Mycoplasma, Chlamydia pneumoniae, and Corynebacterium diphtheriae. In patients who cannot tolerate penicillins or cephalosporins, erythromycin or clindamycin are an effective alternative for the treatment of streptococcal pharyngitis, bronchitis, and pneumonia. Gastrointestinal intolerance is the most common side effect which severely limits its use. IV preparations are available for treatment of severe infections, but prolonged use by this route of administration is limited by the common occurrence of thrombophlebitis at the injection site and development of tinnitus or hearing loss in many patients. Severe nausea and vomiting may accompany infusion of erythromycin. Erythromycin is excreted largely in bile and only to a minor degree in urine. The dosage need not be altered in the presence of renal failure.
Effects on QTc
Oral erythromycin prolongs cardiac repolarization and is associated with reports of torsades de pointes.32 Because erythromycin is extensively metabolized by cytochrome P-450 3A (CYP3A) isozymes, commonly used medications that inhibit the effects of CYP3A may increase plasma erythromycin concentrations thus increasing the risk of ventricular dysrhythmias and sudden death. The concurrent use of erythromycin and strong inhibitors of CYP3A such as ketoconazole is not recommended.
Azithromycin
Azithromycin resembles erythromycin in its antimicrobial spectrum, but an extraordinarily prolonged elimination half-time (68 hours) permits once-a-day dosing for 5 days (500 mg on day 1 and 250 mg on days 2 to 5). Tissue levels of azithromycin can be expected to remain at therapeutic levels for 4 to 7 days after a 5-day treatment course. Unlike clarithromycin, bioavailability of azithromycin is decreased by food such that the drug should be administered 1 hour before or 2 hours after meals.
Clindamycin
Clindamycin resembles erythromycin in antimicrobial activity, but it is more active against many anaerobes. Because severe pseudomembranous colitis can be a complication of clindamycin therapy, this drug should be used only to treat infections that cannot be adequately treated by less toxic antimicrobials. Significant diarrhea in patients treated with clindamycin is an indication to discontinue this drug and initiate evaluation for pseudomembranous colitis. However, clindamycin is indicated in the treatment of or prophylaxis for serious infections caused by susceptible anaerobes, particularly those originating in the gastrointestinal tract and female genital tract.
Only about 10% of administered clindamycin is excreted in an active form in urine; the remainder is changed into inactive metabolites. In patients with renal dysfunction, the elimination half-time of clindamycin is only slightly prolonged, and little change in dosage is required. In patients with severe liver disease, the dose of clindamycin may need to be decreased.
Side Effects
Clindamycin produces prejunctional and postjunctional effects at the neuromuscular junction, and these effects cannot be readily antagonized with calcium or anticholinesterase drugs. Large doses of clindamycin can induce profound and long-lasting neuromuscular blockade in the absence of nondepolarizing muscle relaxants and after full recovery from the effects of succinylcholine has occurred.33 Skin rashes occur in about 10% of patients treated with clindamycin.
Vancomycin
Vancomycin is a bactericidal glycopeptide antimicrobial that impairs cell wall synthesis of gram-positive bacteria. The oral route of administration is used only for the treatment of staphylococcal enterocolitis and antimicrobial-associated pseudomembranous enterocolitis, taking advantage of the fact that vancomycin is poorly absorbed from the gastrointestinal tract. Vancomycin is administered IV for the treatment of severe staphylococcal infections or streptococcal or enterococcal endocarditis in patients who are allergic to penicillins or cephalosporins. Concomitant administration of an aminoglycoside is often necessary when vancomycin is used in the treatment of enterococcal endocarditis. Vancomycin is the drug of choice in the treatment of infections caused by MRSA. Vancomycin can be useful in the therapy of prosthetic heart valve endocarditis caused by S. epidermidis. In this setting, vancomycin is often administered in combination with gentamicin or rifampin. Vancomycin is also used for prophylaxis against endocarditis in penicillin- and cephalosporin-allergic patients who have valvular heart disease and are undergoing dental procedures.
When vancomycin is administered IV, the recommendation is to infuse the calculated dose (10 to 15 mg/kg) over 60 minutes to minimize the occurrence of drug-induced histamine release and hypotension. As such it can be begun 2 hours prior to surgery for prophylaxis. Infusion over 60 minutes produces sustained plasma concentrations for up to 12 hours. Vancomycin is principally excreted by the kidneys, with 90% of a dose being recovered unchanged in urine. The elimination half-time is approximately 6 hours and may be greatly prolonged (as long as 9 days) in the presence of renal failure. Determination of plasma vancomycin levels is an important guide to dosage (20 to 30 µg/mL is considered ideal) when this antimicrobial must be administered in the presence of renal dysfunction.
Side Effects
Rapid infusion (<30 minutes) of vancomycin has been associated with profound hypotension and even cardiac arrest.34–37 Hypotension is often accompanied by signs of histamine release characterized by intense facial and truncal erythema (“red man syndrome”). The red man syndrome may occur even with slow infusion of vancomycin and is not always associated with hypotension.38 Cardiovascular side effects most likely reflect nonimmunologic histamine release induced by vancomycin.39 Although drug-induced histamine release initially causes increases in myocardial contractility, this effect is promptly followed by venodilation, a sudden decrease in left ventricular filling, and decreased contractility. Histamine produces hypotension in humans by directly dilating peripheral blood vessels. Direct myocardial depression produced by vancomycin does not seem to be important in causing hypotension in humans.39 Vancomycin may also produce allergic reactions characterized as anaphylactoid with associated hypotension, erythema, and occasionally bronchospasm.37 Plasma tryptase concentrations are not increased following vancomycin-induced anaphylactoid reactions thus permitting a method to distinguish anaphylactic from anaphylactoid reactions.40 Arterial hypoxemia manifesting as an unexpected decrease in the Spo2 may occur in association with vancomycin administration, perhaps reflecting drug-induced vasodilation in the lungs leading to an increase in ventilation to perfusion mismatching.41 Oral H1 (diphenhydramine 1 mg/kg) and H2 (cimetidine 4 mg/kg) receptor antagonists administered 1 hour before induction of anesthesia decreased histamine-related side effects of rapid vancomycin infusion (1 g over 10 minutes).42 In ambulatory anesthesia settings, as for orthopedic procedures, the time available for vancomycin administration before surgical incision or tourniquet inflation is often limited and may result in inadequate levels of antibiotic in blood and tissues if vancomycin cannot be administered more rapidly than 10 to 15 mg/kg over 60 minutes.
Ototoxicity is likely when persistent high plasma concentrations (>30 µg/mL) are present. The incidence of nephrotoxicity in association with vancomycin treatment is low. Particular attention to ototoxicity and nephrotoxicity is required when vancomycin is administered with an aminoglycoside. The administration of vancomycin to a patient recovering from succinylcholine-induced neuromuscular blockade has resulted in a return of neuromuscular blockade.43
Bacitracins
Bacitracins are a group of polypeptide antibiotics effective against a variety of gram-positive bacteria. Use of these antimicrobials is limited to topical application in ophthalmologic and dermatologic ointments. Despite a perception that topical application of bacitracin rarely results in allergic reactions, there are reports of anaphylactic reactions following bacitracin nasal packing and mediastinal irrigation.44,45 Established topical uses of bacitracin include treatment of furunculosis, carbuncle, impetigo, suppurative conjunctivitis, and infected corneal ulcer.
Metronidazole
Metronidazole is bactericidal against most anaerobic gram-negative bacilli and Clostridium species. If administered orally, the drug is well absorbed and widely distributed in body tissues, including the CNS. As such, this antimicrobial has been useful in treating a variety of CNS, bone and joint infections, abdominal and pelvic sepsis, and endocarditis. Administered orally, metronidazole is useful for treating pseudomembranous colitis. Metronidazole is a useful part of preoperative prophylactic regimens for elective colorectal surgery. For serious anaerobic infections, the drug is administered IV.
Side effects of metronidazole include dry mouth (metallic taste) and nausea. Concurrent ingestion of alcohol may cause a reaction similar to that produced when alcohol is ingested by patients taking disulfiram. Neuropathy and pancreatitis are infrequent.
Fluoroquinolones
The fluoroquinolones are broad-spectrum antimicrobials that are bactericidal against most enteric gram-negative bacilli.46 They are rapidly absorbed from the gastrointestinal tract, and penetration into body fluids and tissues is excellent. Their elimination half-time is prolonged (3 to 8 hours), and the principal route of excretion is via the kidneys, including glomerular filtration and renal tubular secretion. The dose of the fluoroquinolones should be decreased in the presence of renal dysfunction. Side effects are minimal, with mild gastrointestinal disturbances (nausea, vomiting) and CNS disturbances (dizziness, insomnia) occurring in less than 10% of treated patients. Fluoroquinolones have been useful clinically in the treatment of genitourinary and gastrointestinal infections, but soft tissue and bone infections have not responded to these drugs. Fluoroquinolones are bactericidal against most mycobacteria and are useful as part of multidrug regimens.47 Fluoroquinolones are associated with an increased risk of tendinitis and tendon rupture that is enhanced in patients older than 60 years of age, taking corticosteroid drugs, and in patients with kidney, heart, or lung transplants. In addition, fluoroquinolones may exacerbate muscle weakness in patients with myasthenia gravis.
Ciprofloxacin
Ciprofloxacin is highly effective in the treatment of urinary and genital tract infections, including prostatitis, and gastrointestinal infections. The major advantage of ciprofloxacin is its greatly enhanced serum concentration and its availability as an IV preparation. Because of high blood levels and good tissue penetration, ciprofloxacin has been useful in the treatment of a variety of systemic infections, including upper and lower respiratory tract infections, skin and soft tissue infections, and bone and joint infections. Most strains of M. tuberculosis are susceptible to ciprofloxacin.
Moxifloxacin
Moxifloxacin is long acting for the treatment of acute bacterial sinusitis, acute bacterial exacerbation of chronic bronchitis, community-acquired pneumonia, skin infections, and complicated intraabdominal infections. Because of serious adverse effects including peripheral neuropathy, syndrome of inappropriate secretion of antidiuretic hormone, tendonitis, acute liver failure, QTc prolongation, toxic epidermal necrolysis, psychotic reactions, and Stevens-Johnson syndrome, use is recommended only when less toxic options are not available.
Antiseptic and Disinfectant Prophylaxis for Surgical Procedures
Contamination of the surgical site is a requirement for surgical site infection. Decontamination of the skin with antiseptic preparations reduces the burden of skin flora but the effect on the incidence of surgical site infection is not clear.48 Centers for Disease Control and Prevention guidelines recommend showering or bathing with an antiseptic solution before surgery and the clinical practice guidelines from the National Institute for Health and Care Excellence recommend bathing or showering with soap, use of an iodine-impregnated drape, and immediate preparation with an antiseptic solution. Neither set of guidelines puts forth a preference of type of antiseptic solution. The main types of disinfectants are alcohols, chlorhexidine, and iodine-containing preparations which can be used alone or in combination.
Topical Antiseptics
Alcohols
Alcohols are applied topically to decrease local cutaneous bacterial flora (quick drying and antisepsis) before penetration of the skin with needles. Their antiseptic action can be enhanced by prior mechanical cleansing of the skin with water and a detergent and gentle rubbing with sterile gauze during application.
Ethyl alcohol is an antiseptic of low potency but moderate efficacy, being bactericidal to many bacteria. On the skin, 70% ethyl alcohol kills nearly 90% of the cutaneous bacteria within 2 minutes, provided the area is kept moist. Greater than a 75% decrease in cutaneous bacterial count is unlikely with a single wipe of an ethyl alcohol–soaked sponge followed by evaporation of the residual solution. Isopropyl alcohol has a slightly greater bactericidal activity than ethyl alcohol. Alcohols reduce bacterial contamination and are not fungicidal or virucidal.
Fire Risks
It is important to recognize that alcohol-based preparations are flammable until all the liquid has evaporated.49,50 Alcohol-based surgical solutions can create a fire hazard (flash fire) especially if the solution is allowed to pool (for example in the umbilicus) or the patient is draped before the solution is completely dry resulting in trapped alcohol vapors being channeled to the surgical site where a heat source may be used. Sterile towels may be used to absorb excess alcohol-based solutions.
Chlorhexidine
Chlorhexidine is a colorless chlorophenol biguanide solution that disrupts cell membranes of the bacterial cells and is effective against both gram-positive and gram-negative bacteria. It persists on the skin to provide continued antibacterial protection. As a hand wash or surgical scrub, 2% chlorhexidine causes a greater initial decrease in the number of normal cutaneous bacteria than does povidone-iodine or hexachlorophene, and it has a persistent effect equal to or greater than that of hexachlorophene. Chlorhexidine is mainly used for the preoperative reduction of cutaneous flora for the surgeon and patient. It is also used to treat superficial infections caused by gram-positive bacteria and to disinfect wounds. As an antiseptic, chlorhexidine is rapid acting, has considerable residual adherence to the skin, has a low potential for producing contact sensitivity and photosensitivity, and is poorly absorbed even after many daily hand washings. Chlorhexidine solutions in an alcohol base are not appropriate for instillation into the eye (corneal injury) or middle ear (deafness).
Iodine
Iodine is a rapid-acting antiseptic that, in the absence of organic material, kills bacteria, viruses, and spores. For example, on the skin, 1% tincture of iodine will kill 90% of the bacteria in 90 seconds, whereas a 5% solution achieves this response in 60 seconds. In the presence of organic matter, some iodine is bound covalently, diminishing the immediate but not eventual effect. Nevertheless, commercial preparations contain iodine in such excess that minimal organic matter does not adversely influence immediate efficacy. The local toxicity of iodine is low, with cutaneous burns occurring only with concentrations of greater than 7%. In rare instances, an individual may be allergic to iodine and react to topical application. An allergic reaction usually manifests as fever and generalized skin eruption.
The most important use of iodine is disinfection of the skin. For this use, it is best used in the form of a tincture of iodine because the alcohol vehicle facilitates spreading and skin penetration. Iodine may also be used in the treatment of wounds and abrasions. Applied to abraded tissue, 0.5% to 1.0% iodine aqueous solutions are less irritating than the tinctures.
Iodophors
An iodophor is a loose complex of elemental iodine with an organic carrier that not only increases the solubility of iodine but also provides a reservoir for sustained release. The most widely used iodophor is povidone-iodine, in which the carrier molecule is polyvinylpyrrolidone. A 10% solution contains 1% available iodine, but the free iodine concentration is less than 1 ppm. This is sufficiently low that little, if any, staining of the skin occurs. Because of the low concentrations, the immediate bactericidal action is only moderate compared with that of iodine solutions.
Clinical Uses
The iodophors have a broad antimicrobial spectrum and are widely used as hand washes, including surgical scrubs; preparation of the skin before surgery or needle puncture; and treatment of minor cuts, abrasions, and burns. A standard surgical scrub with 10% povidone-iodine solutions (Betadine) will decrease the usual cutaneous bacterial population by greater than 90%, with a return to normal in about 6 to 8 hours. Compared with povidone-iodine, a disinfectant that contains an iodophor in isopropyl alcohol (DuraPrep) is more effective than povidone-iodine in decreasing the number of positive skin cultures immediately after disinfection as well as in bacterial regrowth and colonization of epidural catheters.51 As vaginal disinfectants, iodophors may be absorbed, introducing the risk of fetal hypothyroidism if used in a parturient.52
Corneal Toxicity
Chemical burns to the cornea may follow exposure (accidental splashes) to a variety of disinfectant solutions (chlorhexidine, hexachlorophene, iodine, alcohol, detergents containing iodine-based solutions). Povidone-iodine solution without detergent appears to be least toxic to the cornea.53
Preference for Chlorhexidine or Iodine for Skin Disinfection
Central vascular catheters are a common site of hospital-acquired infection. The superiority of chlorhexidine compared to iodine-based solutions has been examined in several studies. A meta-analysis of eight studies concluded that the incidence of bloodstream infections was significantly less when central vascular lines were inserted after skin preparation with chlorhexidine gluconate compared to povidone-iodine.54 In contrast, no difference was detected in catheter colonization when skin was prepared with iodine or chlorhexidine before epidural catheter insertion.55 An iodophor in isopropyl alcohol solution was found to be superior to povidone-iodine, decreasing the number of positive skin cultures immediately after disinfection as well as in bacterial regrowth and colonization of epidural catheters51 and chlorhexidine-impregnated split dressing may reduce colonization of epidural catheters.56 However, concerns have been raised about potential neurotoxicity of chlorhexidine, which is inadvertently introduced into the neuraxial space.57
Quaternary Ammonium Compounds
Quaternary ammonium compounds are bactericidal in vitro to a wide variety of gram-positive and gram-negative bacteria. Many fungi and viruses are also susceptible. M. tuberculosis, however, is relatively resistant. Alcohol enhances the germicidal activity of quaternary ammonium compounds so that tinctures are more effective than aqueous solutions. The major site of action of quaternary ammonium compounds appears to be the cell membrane, where these solutions cause a change in permeability.
Benzalkonium and cetylpyridinium (mouthwash) are examples of quaternary ammonium compounds. These compounds may be used preoperatively to decrease the number of microorganisms on intact skin. There is a rapid onset of action, but the availability of more efficacious solutions has decreased their frequency of use. Quaternary ammonium compounds have been widely used for the sterilization of instruments. Endoscopes and other instruments made of polyethylene or polypropylene, however, absorb quaternary ammonium compounds, which may decrease the concentration of the active ingredient to below a bactericidal concentration.
Hexachlorophene
Hexachlorophene (pHisoHex) is a polychlorinated bisphenol that exhibits bacteriostatic activity against gram-positive but not gram-negative organisms. Immediately after a hand scrub with hexachlorophene, the cutaneous bacterial population may be decreased by only 30% to 50% compared with greater than 90% following use of an iodophor. Nevertheless, 60 minutes later, the bacterial population surviving a hexachlorophene scrub will have decreased further to about 4%, whereas with the iodophor scrub, the bacterial population will have recovered to about 16% of normal.
Because most of the potentially pathogenic bacteria on the skin are gram-positive, 3% hexachlorophene is commonly used by physicians and nurses to decrease the spread of contaminants from caregivers’ hands. This antiseptic is also used to cleanse the skin of patients scheduled for certain surgical procedures. Hexachlorophene may be absorbed through intact skin in sufficient amounts to produce neurotoxic effects, including cerebral irritability.
Methods for Sterilization of Instruments
Formaldehyde
Formaldehyde is a volatile, wide-spectrum disinfectant that kills bacteria, fungi, and viruses by precipitating proteins. A 0.5% concentration requires 6 to 12 hours to kill bacteria and 2 to 4 days to kill spores. A 2% to 8% concentration is used to disinfect inanimate objects such as surgical instruments. Formaldehyde can be toxic, allergenic, and was named a known carcinogen by the U.S. National Toxicology Program in 2011. Most exposure is through volatilization and use under with fume hoods is recommended.
Glutaraldehyde
Glutaraldehyde is superior to formaldehyde as a disinfectant because it is rapidly effective against all microorganisms, including viruses and spores. This disinfectant also possesses tuberculocidal activity. Glutaraldehyde is less volatile than formaldehyde and hence causes minimal odor and irritant fumes. A period of 10 hours is necessary to sterilize dried spores, whereas an acid-stabilized solution kills dried spores in 20 minutes. Neither alkaline nor acidic solutions are damaging to most surgical instruments and endoscopes. As a sterilizing solution for endoscopes, glutaraldehyde is superior to iodophors and hexachlorophene.
Pasteurization
Pasteurization (hot water disinfection) is a process that destroys microorganisms in a liquid medium by application of heat. Pasteurizing water temperatures in the range of 55°C to 75°C will destroy all vegetative bacteria of significance in human disease, as well as many fungi and viruses. Pasteurization kills bacteria by coagulating cell proteins, and water acts as a very effective medium for transferring the heat required to destroy organisms. This is the rationale for maximizing direct water contact with surfaces to be disinfected. Water temperatures of greater than 75°C may cause some plastic parts to deform. Equipment (respiratory therapy breathing circuits, anesthesia breathing circuits) should be submerged in water at 68°C for a minimum of 30 minutes. With respect to breathing circuits, pasteurization is effective against gram-negative rods, M. tuberculosis, and most fungi and viruses. Pasteurization may be a cost-effective alternative to potentially toxic disinfecting solutions such as glutaraldehyde and formaldehyde.
Cresol
Cresol is bactericidal against common pathogenic organisms including M. tuberculosis. It is widely used for disinfecting inanimate objects. Cresol should not be used to disinfect materials that can absorb this solution because burns could result from subsequent tissue contact.
Silver Nitrate
Silver nitrate is used as a caustic, antiseptic, and astringent. A solid form is used for cauterizing wounds and removing granulation tissue. It is conveniently dispensed in pencils that should be moistened before use. Solutions of silver nitrate are strongly bactericidal, especially for gonococci, accounting for its frequent use as prophylaxis for ophthalmia neonatorum.
Silver sulfadiazine or nitrate is used in the treatment of burns. With this use, hypochloremia may occur, reflecting the combination of silver ions with chloride. Hyponatremia also may result because the sodium ions are attracted by chloride ions into the exudate. Furthermore, absorbed nitrate can cause methemoglobinemia.
Ethylene Oxide
Ethylene oxide is a readily diffusible gas that is noncorrosive and antimicrobial to all organisms at room temperature. This gaseous alkylating material is widely used as an alternative to heat sterilization. It reacts with chloride and water to produce two additional active germicides, ethylene chlorohydrin and ethylene glycol. Special sterilizing chambers are required because the gas must remain in contact with the objects for several hours. Adequate airing of sterilized materials, such as tracheal tubes, is essential to ensure removal of residual ethylene oxide and thus minimize tissue irritation. Ethylene oxide sensitization has been described in children with spina bifida experiencing preoperative anaphylactic reactions, always in association with latex sensitization.58
References
1. Gonzales R, Steiner JF, Sande MA. Antibiotic prescribing for adults with colds, upper respiratory tract infections, and bronchitis by ambulatory care physicians. JAMA. 1997;278:901–904.
2. Kirkland KB, Briggs JP, Trivette SL, et al. The impact of surgical-site infections in the 1990s: attributable mortality, excess length of hospitalization, and extra costs. Infect Contr Hosp Epidemiol. 1999;20:725–730.
3. Rosenberger LH, Politano AD, Sawyer RD. The surgical care improvement project and prevention of post-operative infection, including surgical site infection. Surg Infect. 2011;12:163–168.
4. U.S. Department of Health and Human Services. National action plan to prevent health care-associated infections: road map to elimination. Health.gov Web site. http://www.health.gov/hai/prevent_hai.asp#table1. Accessed February 2, 2014.
5. Anderson DJ, Kaye KS, Classen D, et al. Strategies to prevent surgical site infections in acute care hospitals. Infect Control Hosp Epidemiol. 2008;29(suppl 1):S51–S61.
6. Mangram AJ, Horan TC, Pearson ML, et al. Guideline for prevention of surgical site infection. Infect Control Hosp Epidemiol. 1999;20:250–278.
7. Zerr KJ, Furnary AP, Grunkemeier GL, et al. Glucose control lowers the risk of wound infection in diabetics after open heart operations. Ann Thorac Surg. 1997;63:356–361.
8. Furnary AP, Zerr KJ, Grunkemeier GL, et al. Continuous intravenous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical procedures. Ann Thorac Surg. 1999;67:352–360.
9. McConnell YJ, Johnson PM, Porter GA. Surgical site infections following colorectal surgery in patients with diabetes: association with postoperative hyperglycemia. J Gastrointest Surg. 2009;13:508–515.
10. NICE-SUGAR Study Investigators; Finfer S, Chittock DR, Su SY, et al. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360(13):1283–1297.
11. Sorensen LT. Wound healing and infection in surgery. The clinical impact of smoking and smoking cessation: a systematic review and meta-analysis. Arch Surg. 2012;147(4):373–383.
12. Mahoney CB, Odom J. Maintaining intraoperative normothermia: a meta-analysis of outcomes with costs. AANA J. 1999;67(2): 155–163.
13. Suding P, Jensen E, Abramson MA, et al. Definitive risk factors for anastomotic leaks in elective open colorectal resection. Arch Surg. 2008;143:907–912.
14. Bolac CS, Wallace AH, Broadwater G, et al. The impact of postoperative nausea and vomiting prophylaxis with dexamethasone on postoperative wound complications in patients undergoing laparotomy for endometrial cancer. Anesth Analg. 2013;116(5):1041–1047.
15. Hidron AI, Edwards JR, Patel J, et al; National Healthcare Safety Network Team and participating National Healthcare Safety Network facilities. Antimicrobial-resistant pathogens associated with healthcare-associated infections: annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006–2007. Infect Control Hosp Epidemiol. 2008;29:996–1011.
16. Bratzler DW, Dellinger, EP, Olsen KM, et al; American Society of Health-System Pharmacists; Infectious Diseases Society of America; Surgical Infection Society; Society for Healthcare Epidemiology of America. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am J Health Syst Pharm. 2013;70(3):195–283. http://www.ashp.org/surgical-guidelines. Accessed February 24, 2014.
17. Frumin J, Gallagher JC. Allergic cross-sensitivity between penicillin, carbapenem, and monobactam antibiotics: what are the chances? Ann Pharmacother. 2009;43:304–315.
18. Gould FK, Brindle R, Chadwick PR, et al. Guidelines (2008) for the prophylaxis and treatment of methicillin-resistant Staphylococcus aureus (MRSA) infections in the United Kingdom. J Antimicrob Chemother. 2009;63:849–861.
19. Bull AL, Worth LJ, Richards MJ. Impact of vancomycin surgical prophylaxis on the development of methicillin-sensitive Staphylococcus aureus surgical site infections: report from Australian surveillance data (VICNISS). Ann Surg. 2012;256(6):1089–1092.
20. Finkelstein R, Rabino G, Mashiah T, et al. Vancomycin versus cefazolin prophylaxis for cardiac surgery in the setting of a high prevalence of methicillin-resistant staphylococcal infections. Thorac Cardiovasc Surg. 2002;123:326–332.
21. van der Waaij D, MansonWL, Arends JP, et al. Clinical use of selective decontamination: the concept. Intens Care Med. 1990;16(suppl 3): S212–S216.
22. Weaver M, Burdon DW, Youngs DJ, et al. Oral neomycin and erythromycin compared with single-dose systemic metronidazole and ceftriaxone prophylaxis in elective colorectal surgery. Am J Surg. 1986;151:437–442.
23. Keighley MR, Arabi Y, Alexander-Williams J, et al. Comparison between systemic and oral antimicrobial prophylaxis in colorectal surgery. Lancet. 1979;1:894–897.
24. Wenzel RP, Edmond MB. The evolving technology of venous access. N Engl J Med. 1999;340:48–50.
25. Harbell J, Fung J, Nissen N, et al; HIV-TR Investigators. Surgical complications in 275 HIV-infected liver and/or kidney transplantation recipients. Surgery. 2012;152(3):376–381.
26. Muchuweti D, Jönsson KU. Abdominal surgical site infections: a prospective study of determinant factors in Harare, Zimbabwe [published online ahead of print September 19, 2013]. Int Wound J.
27. Coleman J, Green I, Scheib S, et al. Surgical site infections after hysterectomy among HIV-infected women in the HAART era: a single institution’s experience from 1999–2012. Am J Obstet Gynecol. 2014;210(2):117.e1–117.e7.
28. Kigera JW, Straetemans M, Vuhaka SK, et al. Is there an increased risk of post-operative surgical site infection after orthopaedic surgery in HIV patients? A systematic review and meta-analysis. PLoS One. 2012;7(8):e42254.
29. Annè S, Reisman RE. Risk of administering cephalosporin antibiotics to patients with histories of penicillin allergy. Ann Allergy Asthma Immunol. 1995;74(2):167–170.
30. Pallasch TJ. Principles of pharmacotherapy: III. Drug allergy. Anesth Prog. 1988;35:178–189.
31. Adkinson NF. Immunogenicity and cross-allergenicity of aztreonam. Am J Med. 1990;88:12S–15S.
32. Ray WA, Murray KT, Meredith S, et al. Oral erythromycin and the risk of sudden death from cardiac causes. N Engl J Med. 2004;351(11):1089–1096.
33. Ahdal OA, Bevan DR. Clindamycin-induced neuromuscular blockade. Can J Anaesth. 1995;42:614–617.
34. Lyon GD, Bruce DL. Diphenhydramine reversal of vancomycin-induced hypotension. Anesth Analg. 1988;67:1109–1110.
35. Mayhew JF, Deutsch S. Cardiac arrest following administration of vancomycin. Can Anaesth Soc J. 1985;32:65–66.
36. Southorn PA, Plevak DJ, Wilson WR. Adverse effects of vancomycin administered in the perioperative period. Mayo Clin Proc. 1986;61:721–724.
37. Symons NLP, Hobbes AFT, Leaver HK. Anaphylactoid reactions to vancomycin. Can Anaesth Soc J. 1985;32:65–66.
38. Davis RL, Smith AL, Koup JR. The “red-man’s syndrome” and slow infusion of vancomycin. N Engl J Med. 1985;313:756–757.
39. Levy JH, Kettlekamp N, Goertz P, et al. Histamine release by vancomycin. A mechanism for hypotension in man. Anesthesiology. 1987;67:122–125.
40. Renz CL, Thurn JD, Finn HA, et al. Oral antihistamines reduce the side effects from rapid vancomycin infusion. Anesth Analg. 1998;87:681–685.
41. Gopalan K, Dhandha SK. Hypoxia following perioperative administration of vancomycin. Anesth Analg. 1993;76:200–201.
42. Renz CL, Laroche D, Thurn JD, et al. Tryptase levels are not increased during vancomycin-induced anaphylactoid reactions. Anesthesiology. 1998;89:620–625.
43. Albrecht RF, Lanier WL. Potentiation of succinylcholine-induced phase II block by vancomycin. Anesth Analg. 1993;77:1300–1302.
44. Blas M, Briesacher K, Lobato E. Bacitracin irrigation: a cause of anaphylaxis in the operating room. Anesth Analg. 2000;91:1027–1028.
45. Gail R, Blakley B, Warrington R, et al. Intraoperative anaphylactic shock from bacitracin nasal packing after septorhinoplasty. Anesthesiology. 1999;91:1545–1547.
46. Hooper DC, Wolfson JS. Fluoroquinolone antimicrobial agents. N Engl J Med. 1991;324:384–394.
47. Alangaden GJ, Lerner SA. The clinical use of fluoroquinolones for the treatment of mycobacterial diseases. Clin Infect Dis. 1997;25:1213–1218.
48. Kamel C, McGahan L, Polisena J, et al. Preoperative skin antiseptic preparations for preventing surgical site infections: a systematic review. Infect Control Hosp Epidemiol. 2012;33:608–617.
49. Barker SJ, Polson JS. Fire in the operating room: a case report and laboratory study. Anesth Analg. 2001;93:960–965.
50. Improper use of alcohol-based skin preps can cause surgical fires. Health Devices. 2003;32:441–443.
51. Birnbach DJ, Meadows W, Stein DJ, et al. Comparison of povidone iodine and DuraPrep, an iodophor-in-isopropyl alcohol solution, for skin disinfection prior to epidural catheter insertion in parturients. Anesthesiology. 2003;98:164–169.
52. Vorherr H, Vorherr UF, Mehta P, et al. Vaginal absorption of povidone-iodine. JAMA. 1980;244:2628–2629.
53. Rae SCC, Brown B, Edelhauser HF. The corneal toxicity of presurgical skin antiseptics. Am J Ophthalmol. 1984;97:221–232.
54. Chaiyakunapruk N, Veenstra DL, Lipsky BA, et al. Chlorhexidine compared with povidone-iodine solution for vascular catheter–site care: a meta-analysis. Ann Intern Med. 2002;136:792–801.
55. Kasuda H, Fukuda H, Togashi H, et al. Skin disinfection before epidural catheterization: comparative study of povidone-iodine versus chlorhexidine ethanol. Dermatology. 2002;204(suppl 1): 42–46.
56. Kinirons B, Mimoz O, Lafendi L, et al. Chlorhexidine versus povidone iodine in preventing colonization of continuous epidural catheters in children. Anesthesiology. 2001;94:239–244.
57. Milstone AM, Bamford P, Aucott SW, et al. Chlorhexidine inhibits L1 cell adhesion molecule-mediated neurite outgrowth in vitro. Pediatr Res. 2014;75:8–13.
58. Porri F, Pradal M, Lemiere C, et al. Association between latex sensitization and repeated latex exposure in children. Anesthesiology. 1997;86:599–602.