Brian Edwards1 and Veronika Valdova2
(1)
NDA Regulatory Science Ltd, Prime House, Challenge Court, Barnett Wood Lane, Leatherhead, Surrey, KT22 7DE, UK
(2)
ARETE-ZOE, LLC, 1334 E Chandler Blvd #5, Box A-19, Phoenix, 85048, AZ, USA
Brian Edwards (Corresponding author)
Email: brian.edwards@ndareg.com
Veronika Valdova
Email: veronikav@arete-zoe.com
Introduction
Pharmacovigilance systems for regulating and controlling safety of medicines do not differentiate between those exclusively for women and those for men. And yet, the societal circumstances for certain women’s medicines – especially where such medicines affect reproduction – are so obviously different from other medicines, we wished to examine what evidence exists to define how religion, cultural traditions, politics, economics, history and a society’s view of science impacts the safe use of medicines by women. This is a large and complex subject which cannot be covered completely in this one chapter, but we aim to give an overview and to draw on specific examples from around the world to illustrate some of the many interesting issues.
Historic Development of Reproductive Rights for Women
Avoiding pregnancy has been a serious concern for women and men for many years. For example, prior to the nineteenth century, information about human reproduction was widely available to the American public, even though we do not know how well it was understood. However, it was the efforts of Anthony Comstock that drove the manufacture and distribution of a wide range of contraceptive devices underground, due to the 1873 passage of the so-called Comstock Act which outlawed this merchandise in the broad category of ‘obscenities’ (Berger 2010).
As Vancaillie explained, cultural, religious, and political context makes all the difference in reproduction-related decision-making (Vancaillie 2013). Control over one’s own fertility has shifted from secular and religious authorities to the individual. Over the last 50 years ‘Reproductive Rights’, which refer to the right to decide freely and responsibly the number and spacing of children, and to have the information, education and means to do so, have received increased prominence. They were first recognized as a human right at the International Conference on Human Rights in Teheran in 1968 (United Nations 1968). With reference to Paragraph 7.12 of this document, it states that the right to reproductive health now includes the concept that individuals have the right to attain the highest standard of sexual and reproductive health and to make reproductive choices free from coercion. The success of population education and family planning programs in a variety of settings has shown that informed free choice is essential to the long-term success of family planning programs. Any form of coercion has no part to play.
Indeed, the origin of the right to decide on one’s reproductive activity and coercion-free decision-making with regards to reproductive matters dates back to Article 2 of the Convention on the Prevention and Punishment of the Crime of Genocide (Office of the UN Special Adviser on the Prevention of Genocide (OSAPG) 1948) which defines genocide as ‘any of the following acts committed with intent to destroy, in whole or in part, a national, ethnic, racial or religious group, including imposing measures intended to prevent births within the group’ (Office of the UN Special Adviser on the Prevention of Genocide (OSAPG) 1948). As we will see later, discussions about controlling reproduction can quickly be linked to one of the most sensitive issues in human existence.
The 1994 International Conference on Population and Development (ICPD) in Cairo was another milestone in the history of women’s rights (UNFPA 1994; International Conference on Population and Development – ICPD – Programme of Action 1994). ICPD delegates reached a consensus that the equality and empowerment of women was a global priority for stabilizing population growth. A woman’s ability to access reproductive health and rights is central both to this empowerment and is key to sustainable development.
A total of 179 governments signed up to the ICPD Program of Action which set out to:
· Provide universal access to family planning and sexual and reproductive health services and reproductive rights;
· Deliver gender equality, empowerment of women and equal access to education for girls;
· Address the individual, social and economic impact of urbanization and migration;
· Support sustainable development and address environmental issues associated with population changes.
Following on, it was hardly surprising that women’s health was one of the UN Millennium Development Goals (MDG) with a target of 75 % reduction in maternal mortality by 2015 (Oppenheim 2014; UN Department of Public Information 2008).
The 1994 ICPD concluded that the availability of safer methods of modern contraception permitted greater opportunities for individual choices in reproduction matters throughout the world. As of 1994, about 55 % of couples in developing regions were using some method of family planning, a fivefold increase since the 1960s. Although fertility rates in developing world dropped in the same period from six to seven children per woman to three to four, at least 350 million couples worldwide still lacked access to family planning methods. These numbers did not include sexually active unmarried individuals (UNFPA 1994, point 7.13).
Surveys from more than 60 developing countries indicate that more than 100 million women who are not currently using a contraceptive method want to delay the birth of their next child or to stop childbearing altogether (The United Nations Population Fund 1999). Each year during the decade that followed, the number of couples in their reproductive years will increase by about 18 million. Thus the global impact of actions taken in Western countries concerning women’s medicines such as contraception must always be considered (UNFPA 1994).
In an ICPD report in 2010, it was stated that use of any contraceptive methods among currently married women aged 15–49 years was around 75 % in the 15 of the EU Member States and Non-EU advanced countries. Similar high levels were observed in the Russian Federation (80 %) and Turkey (73 %). Low levels were seen in the Balkans, the Caucasus and Central Asia, except Uzbekistan where the proportion was 65 %. In most of these countries, there was a decline in contraceptive use prevalence from 2000 to 2010 (Unmet need for family planning is defined as the proportion of women who have regular sexual intercourse, do not want to get pregnant, and do not use contraceptive methods. The value of this indicator was at about 2–3 % in France (2004/2005), 10–15 % in about a dozen other European countries, Armenia and Georgia, 23 % in Azerbaijan (2006), and 30 % in Bulgaria (Wittich and Philipov 2013, Chapter 1 Section C).
The ICPD Program of Action focuses on population policies at a macro level and addresses demographic situations to achieve sustainable growth and development. Unlike the outcomes of previous World Population Conferences, the Program of Action of the ICPD aims for a holistic approach to reproductive health in context with socio-economic and environmental factors, not just the absence of disease. According to the 2010 ICPD report, fertility changes in Europe and especially countries in transition, encompass several important trends: significant increase in childlessness, drop in overall birth rate, proliferation of non-marital cohabitation, and increase of births out of wedlock (Wittich and Philipov 2013, Chapter 1 Section A). Increase in life-expectancy further worsens the trend of population aging. The ICPD Program of Action clearly linked individual reproductive health to societal and environmental factors, namely delaying of important life decisions such as childbearing because of increased economic uncertainty due to factors such as globalization (Wittich and Philipov 2013).
Against this back drop emphasizing the global importance of contraception for future sustainability of society, are new ways of thinking about health and the place of medicines. The Commission on Social Determinants of Health (CSDH) was set up by the World Health Organization (WHO) to better understand the complexity of health (WHO 2012). They were tasked with summarizing the evidence on how the structure of societies, through myriad social interactions, norms and institutions, are affecting population health, and what governments and public health systems can do about it. Having health framed as a social phenomenon places it more broadly as a topic of social justice. Consequently, health equity (described by the absence of unfair and avoidable or remediable differences in health among social groups) becomes a guiding criterion or principle, and influences the use of all medicines, in particular medicines for the well-woman. Understanding health from a sociocultural perspective is now as important as traditional science.
Medicalization of Women’s Sexuality
Understanding socio-political factors is linked to the phenomenon of ‘medicalization’ which is the process of defining an increasing number of life’s problems as medical problems. This can impact what is regarded as ‘benefit’. Some medicines developed for women are a rich area for medicalization because of the difficulty we have in knowing what is ‘normal’. For example, it has always been difficult to state what constitutes ‘too much’ or ‘too little’ sexual activity. However, researchers have now defined and classified a new medical disorder of ‘female sexual dysfunction’ and commonly cited prevalence estimates indicate that 43 % of women suffer from it (Quasha 2006). This was thought to be causally linked to testosterone deficiency, and a product, Intrinsa (Procter & Gamble), was developed (unsuccessfully) for this indication in surgically oophorectomised women. A E.U. license was refused because of a negative balance of benefit and risk (European Medicines Agency 2010a, b, c; Food and Drug Administration 2004).
Controversy surrounds current attempts to medicalise sexual problems and establish ‘normative data’ for a range of physiological measurements of female sexual response. The regulation of women’s bodies by controlling their sexual expression and reproductive capacity is now conducted through medicine, whereas in the past religion played this role as we discuss further below.
The concerns are that medicalisation has extended to those life events that are natural to women, including menstruation, pregnancy and childbirth, which impacts the meaning of ‘benefit’ when balanced against risks. However, more recently some commentators such as Anita Clayton, the interim chair of the Department of Psychiatry & Neurobehavioral Sciences, University of Virginia School of Medicine, have criticized gender inequality in society when it comes to approval of medications for ‘female sexual dysfunction’, or FSD. She says that although ‘sexual dysfunction is more common in women than in men (43 % vs. 31 %), the FDA has approved 24 treatments for sexual dysfunction in men’, with none for ‘hypoactive sexual desire disorder’, or HSDD, the ‘most common form of FSD’ (Clayton 2014).
Religious Influences on Women’s Health
Managing the risks of female fertility, reproduction, and sexual behavior has a history which has an origin located in many religious doctrines. Some cultures have interfered with female fertility and reproductive medicines through influencing social attitudes and practices. For example, in Judaism at least a sixth of the Oral Tradition’s volume is dedicated to women, with a substantial amount dealing with female health and fertility. It is the earliest source for ethical guidance, of which we are aware, about fertility and contraception, as well as physiology and pathology on the subject. Jewish law is the first which authorized emergency abortion (Chalik 2014, Personal communication; http://www.jogc.com/abstracts/full/200802_womenshealth_1.pdf).
In Judaism, a whole section of Talmud, called Nashim, is dedicated to women, and additional sections, Kiddushin, to the law of marriage, and Gittin, to the law of divorce. Women’s obligations and responsibilities differed from those of men but were considered as important. The equality begins at the highest possible level: in Judaism, unlike Christianity, God is both masculine and feminine. Whilst in Christianity the right to sex is that of man, in Judaism this counts as a woman’s right (The Mamre Institute 2014).
With regards to contraception, any methods that destroy the ‘seed’ or its passage are not permitted for birth control under Jewish law. Thus condoms are not permitted whilst the pill and IUDs are acceptable methods. One of the more mysterious Jewish laws (observed only by orthodox Jews) is the law of Niddah that is a ban on intercourse with a menstruating woman. This period of ‘impurity’ continues another week afterward and extends the “impure” status to 12–14 days. Whilst use of the term ‘impure’ in this context could be disputed the fertility benefits of this practice are relatively consistent with modern because a woman is likely to become pregnant having intercourse on day 14 at the time of typical ovulation.
In another difference from Christianity, under Jewish law a fetus has the status of “potential human life” until it has emerged from mother. That is, fetal life does not have as much value as life in existence, which is the mother’s life. Jewish law not only permits, but requires abortion in circumstances when the mother’s life is in jeopardy (The Mamre Institute 2014).
The position of Catholic Church is encapsulated in the key Catholic text, the ‘catechism’ which does not place a mother’s life before that of a fetus. Moreover, it eliminates the distinction between an unborn child and its mother and in fact prioritizes life of a child because of its innocence (Speake 2012). This position was confirmed by the encyclical letter Humanae Vitae of 1968 and is the basis for the view of the Catholic Church that abortion, even if for therapeutic reasons, is to be absolutely excluded as a ‘licit means of regulating birth’. In addition, it refers to the natural rhythm method as the only acceptable form of contraception. (Paul VI 1968).
Islam does not have organized clergy, or a central authority; and there is no single interpretation of the faith. Different Muslim communities distinguish themselves by schools of Islamic law to which they adhere. Fatwa is a non-binding pronouncement issued by religious jurists or muftis, around which Islamic medical ethics are formulated, including female reproductive rights. Islamic law may coexist with secular states, and variety of interpretations exists, creating significant ambiguity. Fatwa was issued in favor of abortions as well as to support the practice of female genital mutilation in order to contain women’s sexuality and preserve marriageability (Speake 2012).
The issue of female reproductive behavior in the Middle-East and North African region is closely linked to inheritance laws which grant males twice the share of inheritance of females, making them economic assets of the family; while placing the responsibility for family honor on daughters. The most important causes of suicide among unmarried adolescents in Egypt and Iran are loss of virginity and unplanned pregnancy. The resurgence of fundamentalist Islam brings back arguments that women, as the bearers of life, culture, and tradition, belong to society; and control over their behavior including reproductive capacities and choices is essential to preservation of moral authority and values of the society they belong to (Speake 2012).
Iran, the most conservative theocracy in the world, abandoned its family planning program after the Iranian Revolution of 1979, and the Ayatollah Khomeini’s regime became overtly pro-natalist. In 1988, with the end of war with Iraq, a family planning program was reintroduced to slow down rapid population growth. The International Reproductive Rights Research Action Group (IRRRAG) spent 4 years researching women’s reproductive rights in Egypt, in both urban and rural areas (International Reproductive Rights Research Action Group II). Women interviewed often interpreted Islam as fundamentally forbidding the use of contraception (although it specifically does not), and yet they continued to use it, showing much more pragmatism than theologians. Some authors argue that without economic justice and equality Muslim women in the Middle-East and North Africa cannot achieve recognition of their reproductive rights (Speake 2012).
Interpretation of Islamic Beliefs Regarding Contraception
Widespread belief that Islam bans contraception comes from interpretation of officially issued fatwa by local tribal, religious, and community leaders. Due to illiteracy and limited access to these texts, women especially in rural areas have no choice but to trust people around them with regards to legal and religious matters. Although Muslim women in the Middle East and North African region generally hold the same belief – that Islam does not allow contraception – their behavior is often more pragmatic, which may also be due to better informal availability of contraception and better socio-economic status than for those in Afghanistan and Pakistan (Speake 2012).
The impact of the Taliban on women’s health and reproductive rights is an extreme example of the deleterious impact of religious and political dogma on women’s health. This is most notable in Afghanistan and some parts of Pakistan, specifically Federally Administered Tribal Areas (FATA) – the home of the Taliban. The influence campaign builds on a blend of tribal Pashtun values such as independence, personal honor, inviolability of his person, property and women, revenge, hospitality and Islamic creed (Cassidy 2012).
One of the most high profile implications of Taliban rule has been the ban on polio vaccines which they allege will render the next generation impotent. As a result of this campaign, together with the intimidation effect of several dozen health workers, about 4,000 parents refused to have their children vaccinated (Cassidy 2012). The Taliban agenda is prejudiced against women, separating them from men in word and deed. As a result males are not allowed to treat female patients or rescue women even during natural disasters. The interpretation of sharia offered by the Taliban is very narrow and its application is very rigid. Marginalization of educated women has made their contact with western influences difficult. This means that female doctors or other healthcare professionals in areas of Taliban rule would be very rare indeed. However, since 2010, women in Helmand, Jalalabad, and Nangarhar Provinces have been asserting their rights and economic independence with availability of educated professionals to deliver women’s health programs (Ibid).
Socio-political Issues for Women in Former Soviet Union Countries
Countries in Central and Eastern Europe and Asia, which were part of the former Soviet Union, have been in transition at varying pace (DHHS 2003). Services developed specifically for women are often limited to their reproductive needs, especially childbearing. Services addressing other women’s health problems have been underdeveloped, and are non-existent or inaccessible within public health care. Thus, girls, elderly women, the disabled, the unemployed and others with special needs have had limited access to medical services. Women from rural areas throughout the region have particularly limited access to health services. Many rural areas suffer severe shortages of health personnel, medical equipment, and other supplies. Women often must travel long distances to health centers as in the developing world (see Chap. 18).
The inadequacy of health services to meet women’s needs can be observed best with respect to reproductive health. Moreover, the lack of or inadequate access to sex education in schools or other forms of family planning contributes to insufficient contraceptive use. In short, family planning counseling and services usually still do not constitute an integral part of reproductive health services in many countries in this region. Women in most countries have easier access to free abortion services (with the exception of Poland where, with the most stringent medical exceptions, abortion is illegal) while contraceptives, when they are available at all, are usually not reimbursed (WHO 2014).
In Romania, according to the Romanian Reproductive Health Survey published in 2005, only 43 % of women stated that their most recent pregnancy had been planned, whereas 14 % said that the pregnancy was ill-timed and 49 % said it was unwanted. The proportion of women with unwanted pregnancies rose with greater number of living children. Women with low levels of education were more likely to say that their last pregnancy was unwanted (Ministry of Health, Romania 2005).
Romania is a good illustration about how policy impacts use of contraception. There used to be pro-fertility policies from the late 1960s to the 1980s that banned modern contraceptive use. When this policy was reversed, contraception prevalence rates rose for women from 40.5 % in 1993 to nearly 60 % in 2004. Men’s rates of contraception use also rose – from 51 % in 1999 to more than 60 % in 2004. Popularity of condoms increased especially among men who were not married or cohabiting. This was accompanied by marked falls in abortion rates, lower incidence of STDs, and decreased maternal mortality (Ministry of Health, Romania 2005; Horga et al. 2013).
Global Perspective on Reproduction
According to the report of the Guttmacher Institute from 2013, most individuals and couples in the U.S. want to plan the timing and spacing of their childbearing and to avoid unintended pregnancies, for a range of social and economic reasons. In addition, because unintended pregnancy has a significant public health impact, the U.S. Department of Health and Human Services aims to reduce the number of unintended pregnancies (U.S. Department of Health and Human Services 2010). In 2006, the last year for which national-level data are available, 49 % of all pregnancies in the United States were unintended including eight in ten teen pregnancies (Guttmacher 2013). Pregnancy rates for women in the United States continued to decline in 2009, reaching the lowest level in 12 years (102.1 per 1,000 women aged 15–44). This level is 12 % below the 1990 peak (115.8) (Curtin et al. 2013). Increase in illegitimacy is also associated with numerous societal consequences of life without a father, which further worsens prospects of children who already may start life as disadvantaged (Wood and Gell 2014).
The health consequences of illegitimacy for U.S. children are striking: they are three-times more likely to commit suicide and 20–33 times more likely to become victims of child abuse than their peers from low-income households with married parents. The risks to children living outside a two-parent home include higher risk of infanticide (Mac Donald 1998). Thus the consequences of ‘contraceptive failure’ for an unmarried mother can be profound not only for her but also for her child later in life.
The situation can be worse elsewhere in the world. For example, although Muslims must ‘treat orphans with compassion and equity’, Saudi Arabia’s tribal society has tradition of stigmatizing orphans and illegitimate children who may end up abandoned or face life in an orphanage. Even if they are adopted, they are traditionally ‘not marriageable’ and their future is never discussed (Wagner 2011).
Demographic Consequences of Individual Choices
Demography is the statistical study of human populations and their changes (such as the number of births, deaths, marriages, and illnesses) that occur over a period of time especially with reference to size and density, distribution, and vital statistics. Individual choices have effect on demographic trends. In turn, the demographic situation of the environment in which individuals and families live has an impact on maternal health and reproductive decisions, by offering choices or imposing constraints. These circumstances include, among other factors, presence or absence of grandparents or wider family available to provide support to allow woman to continue being economically active; general acceptance of working mothers by employers; presence or absence of healthcare and childcare facilities and logistical networks; and economic and cultural pressure imposed on women in childbearing age. Individual reproductive behavior then translates into trends which can be observed at a population level. Sustainable population growth includes healthy fertility rates. Fertility, together with mortality and immigration, are important demographic drivers.
At the global level, total fertility rates have been falling over the last decades of the twentieth century, largely due to the availability of modern methods of contraception and the choices made by individuals and couples. The average number of children born worldwide fell from 5 in 1950 to 2.7 in 2005: In Africa the total number of children per woman decreased from average 6.7 in 1950 to 5.1 in 2005; in Asia, Latin America, and the Caribbean from 5.9 to 2.5 and 2.6, respectively; and from 3.5 to 2.0 in North America over the same time period. The decline was most marked in Europe where fertility rates have fallen over the last 55 years from 2.7 to 1.4 children per woman. The effect of fertility rates have to be also taken in context of average age at birth which shows generation interval, which determines how long it takes for a daughter to have a child. Currently the highest fertility rates persist in 35 poorest countries in the world. The population of Afghanistan, Nigeria, Uganda, and Yemen, are likely to triple by 2050 (Nugent and Seligman 2008).
The fact that contraception in Eastern Europe is mostly available only with prescription, and is not usually reimbursed, has little effect on overall demographic development which itself ranks as the lowest in the world (Bradatan and Firebaugh 2007). After the end of the Cold War, as a consequence of political, cultural, and economic changes in the region, as well as internal inter-generational tensions, the demographic development in the region took a marked turn downwards. The relationship between demographic trends, reproductive behavior, per-capita income, and economic growth is complex; and the causative factors include shift in values, profound cultural change, inter-generational conflicts, income insecurity, and disintegration of state support system for families (Brainerd 2010; Thornton and Philipov 2007). Thus despite being within the EU, there are distinct demographic differences between Eastern and Western Europe that will impact the environment within which medicines for women will be used.
Socio-political Issues for Women in Russia
In Russia, a tremendous unmet need for family planning exists with abortion still remaining the main method of birth control (Denisov et al. 2013). But Russia’s reproductive troubles do not stop with abortions being used as a method of birth control. By various measures, Russia’s demographic indicators resemble those in many of the world’s poorest and least developed societies (and the figures for males are far worse than those for women). Family formation trends are a further cause for concern. Between 1987 and 1993, the number of births in Russia dropped from 2.5 million to 1.4 million per annum. The all-time low was reached in 1999 when just 1.2 million people were born in Russia. A slight turnaround in 2010 was still below the 27 % replacement level required for long-term population stability (Eberstadt 2011).
In the late 1980s in Russia, births still exceeded deaths by an average of 800,000 births a year. But the collapse of communism brought a series of demographic changes with declining birth rates and rise in deaths. According to Eberstadt’s analysis, this population decline was caused by excess mortality among adults, mainly due to accidents, poisonings including alcohol intoxication, injuries, suicides, homicides, and other unnatural deaths, infectious diseases such as HIV/AIDS and drug-resistant tuberculosis, in combination with an average birth rate of about 1.5 per woman (Eberstadt 2011).
According to the Federal State Statistics Service, over the last 20 years since 1992, Russia became a net mortality society (FSSS 2013). This trend was only reversed in 2012 when the total number of births equaled total mortality (see Fig. 16.1). Part of the population decline in the mid to late 1990s is explained as the consequence of high mortality. The changes in Russian society are so complex it is difficult to identify specific reasons to explain the decline in birth rate. It may be linked to the increased cost of living exceeding income, so that giving birth to a child is perceived as an irrational or irresponsible act. This perception is consistent with a prevailing negative influence of the media in combination with a traditional disregard of Russian culture for women – all of which shape attitudes toward women in childbearing age (Eberstadt 2011).
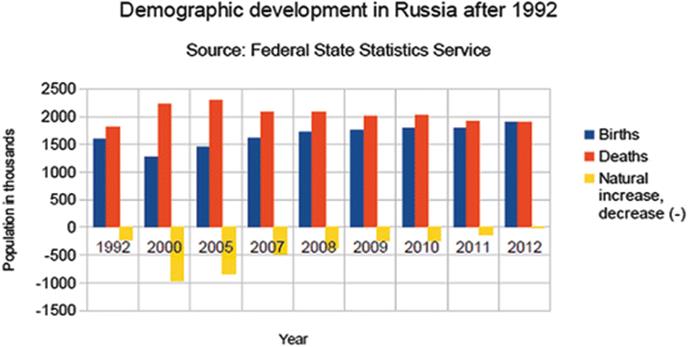
Fig. 16.1
Demographic development in Russia during economic transformation following collapse of the Soviet Union (FSSS 2014)
Cuba
In contrast to other Communist countries and other Latin American countries, Fidel Castro, as the Communist dictator of Cuba, placed a special emphasis on women’s health and well-being because of how he viewed their role in building an egalitarian society. Castro instructed the health department to set up women’s clinics, Sanitary Brigades, and a network of hospitals to specialize in feminine care. Contraception and abortion became widely and readily available to all women and provided for free by the State. In 1965, Castro’s public health department officially decriminalized abortion to reduce maternal morbidity and mortality rates. This action made Cuba’s abortion policy the most liberal policy in the region and most of the world (Croll 1981; Keck and Reed 2012).
Western Europe and the European Union
The birth rate in Western Europe has been in decline since the 1960s and this trend has been only partially reversed in some EU countries because of a higher birth rate among immigrants and more women giving birth later in life.
European Demographic Transition
Clark and Alter (Clark and Alter 2010) explained demographic transition in European societies in the period from 1700 to 1870, and described some phenomena which are still relevant today. By 1870, at the height of the industrial revolution, much of Europe was experiencing economic growth. At that time, fertility levels declined to current levels even in the absence of reliable contraception.
The demographic transition to modern fertility rates only started in the 1870s in England (as shown in Fig. 16.2 below) as in the rest of Europe, and then progressed rapidly. By 2000, the average English woman had fewer than two children over her lifetime. The European Marriage Pattern which kept fertility low was based on delayed marriage, marriage choices and family structure. While fertility within marriage was high, typically about 10–25 % women remained unmarried and therefore excluded from reproduction. At the same time, the illegitimacy rate was low, typically 3–4 % of births, mainly due to social exclusion and limited opportunities and life choices for those affected. This illustrates that individual reproduction behavior is inseparable from cultural, economic, and social environment (Clark and Alter 2010).
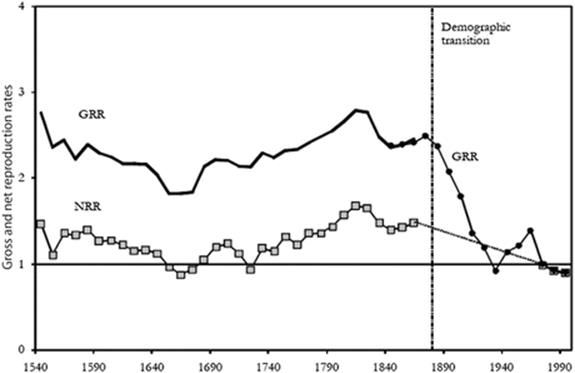
Fig. 16.2
The first demographic transition in England. The Fertility History of England, 1540–2000 (Clark and Alter 2010). Notes: NRR net reproduction rate, GRR gross reproduction rate
“Zero Population Growth”
In 1967, demographer Kingsley Davis introduced the term ‘zero population growth’ by defining the population fertility goal as replacement levels, of about 2.1 child per woman in developed countries and 3.0 in developing countries. This fertility rate was supposed to ensure sustainable development (Population Research Institute, Grimes 1994). The movement became greatly popular in the late 1960s and 1970s.
One of the main supporting arguments was that investment in education, health and family benefits would fall, freeing up resources to be used for improvement of quality of life because of more favorable ratio between economically active individuals and dependents. The early 1970s enthusiasm for economic advantages of zero population growth waned, however; because of long-term adverse consequences of such development. In reality any advantages of zero growth vanish as the population ages due to increased number of dependents who retired from economically active life (Grimes 1994) (Fig. 16.3).
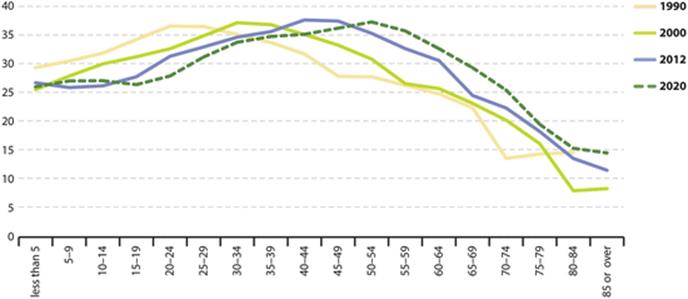
Fig. 16.3
Data from Eurostat showing the EU population is rapidly aging (Eurostat 2013)
The Effects of Zero Population Growth Policies in the Late 1960s on Age Structure of Population in the European Union
Political Influences on Reproductive Behavior in the Czech Republic
The situation in Czechoslovakia illustrates well the effect of policy on reproductive behavior (Fig. 16.4). After the Soviet invasion of 1968, many pro-population measures were implemented to compensate for the decline in birth rates since the 1960s. The era of political ‘normalization’ started with pro-population measures intended to calm down an explosive political situation and ease public unrest. The generation born during this peak was named after then president Gustav Husák – ‘Husák’s children’. People with small children living in confined conditions with their parents only received independent housing from the state if they showed loyalty and gratitude toward the state. The decline in birth rates following the Velvet Revolution in 1989 parallels changes in Russia and other former Warsaw Pact states after the fall of Soviet empire. This has yet to be fully explained because of the enormous complexity of the change. Profound change in economic environment, devaluation of currency combined with sudden surge in prices of property in the early 1990s, coupled with temporary and long-term migration abroad, economic insecurity, in conjunction with lower willingness of parental generation to repeat the experience of multi-generational households with their own children and grandchildren, led to procrastination of starting families, and increased popularity of less formal forms of cohabitation, often considered a ‘temporary solution’ only. Although it is difficult to speculate what role reproductive medicines might have played, it is self-evident that increased availability of contraception meant this generation of women has more control over their own reproduction than their mothers ever had, so that the number of abortions significantly dropped.

Fig. 16.4
Demographic development in Czechoslovakia showing effect of pro-population policies in the early 1970s and drop in birth rate during economic transition after 1989 (Czech Statistical Office 2013)
China’s One Child Policy: A Case Study of Political Impact on Reproductive Behavior
Probably the most extreme case study of policy impact on reproductive behavior of individuals and couples comes from China’s one child policy. Thomas Scharping in his study “Birth Control in China 1949–2000” (Scharping 2003) meticulously researched all aspects of Chinese population policy from 1949. A large number of primary and secondary sources such as national and international statistics, laws, directives, internal documents and conferences were used to compile valid data sets. The political debate around birth control at the Chinese Communist Party (CPP) level is particularly enlightening. After World War Two and takeover of the country by Communists, population growth was seen as essential for national security and defense, especially by Sun Yat-sen and Mao Zedong. But resources required for population growth were obstructing economic development, and scientists and politicians like Zhou Enlai and his wife Deng Yingchao advocated measures which would allow tighter population control already in the mid-1950s. It was not until the late 1970s when the leadership gradually imposed limits on reproduction of the population and implemented its one child policy in response to economic crisis (Allès 2006).
These policy measures greatly accelerated otherwise normal demographic transition toward smaller family size. Because of strong son preference in China the government policies did not always work as intended; and the sex ratio became seriously skewed due to selective abortion practice and female infanticide, reaching 111.8 boys to 100 girls in the census of 1990. Although abortion itself is not illegal in China, and despite little ethical or moral debate about it, prenatal screening and sex selective abortion are still forbidden (Davin 2004).
Between 1979 and 1999, the proportion of women using contraceptive methods in China increased from 60–70 % to 80–90 %, with IUDs and female sterilization being the most widespread methods. Reclassification of nationalities between 1982 and 1990, together with exemptions for some regions, provinces, and minorities, led to major increases in the Mongol, Manchu, and Tijua populations. The author concludes his book by showing the near-impossibility of effectiveness of all these measures, and consequent hiding of illegitimate births from statistics. Scharping’s estimate is that the population under-assessment for the years 1953–1980 is about 11–12 %, and as much as 5–12 % for 2000 (Allès 2006).
Access to Oral Contraceptive Medicines
The requirement for a prescription is an important barrier to access to oral contraceptives, even in developed countries. Over-the-counter access may improve uptake and continuity of protection (Grindlay et al. 2013). Grindlay and colleagues compiled results about contraceptive access from 147 countries between April 2011 and September 2012, and proceeded to analyze regional patterns. About a third of screened countries allowed access to oral contraceptives with prescription only, 8 % required some sort of screening, and 24 % required no prescription at all. In almost 40 % of screened countries oral contraceptives were at the time of this survey available informally without prescription (Grindlay et al. 2013) (Fig. 16.5).
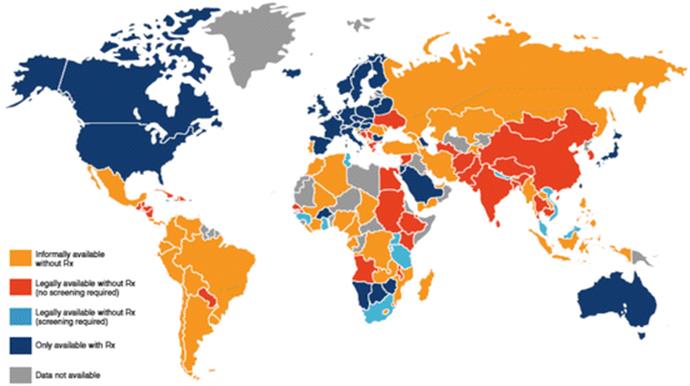
Fig. 16.5
World map of oral contraception availability (Reprinted with permission from Ibis Reproductive Health (Grindlay et al. 2013))
Access to contraceptives is greatly influenced by religious, political, and cultural environments. The primary purpose of contraceptive medicines is not to stop women from having children altogether, but to empower them to better time and space their pregnancies. At a population level, access to contraceptives and their responsible use becomes a public health issue because of direct impact of individual behavior on demographic trends. This is illustrated by the US where about half of pregnancies are reported as unintended, either ill-timed or unwanted. About four out of ten of these unintended pregnancies end in abortion (Guttmacher Institute 2013).
Overview of Abortion Laws in the U.S.
The overall U.S. unintended pregnancy rate increased slightly between 1994 and 2008. Although the abortion rate decreased 8 % between 2000 and 2008, there was an 18 % increase among poor women, and 28 % decrease among higher-income women. Some 1.06 million abortions were performed in 2011, down from 1.21 million abortions in 2008, a decline of 13 %. The number of U.S. abortion providers declined from 1,793 in 2008 to 1,720 in 2011. The number of clinics providing abortion services declined from 851 to 839 (Guttmacher Institute n.d.).
Figure 16.6 below shows an overview of abortion laws in the U.S. (Guttmacher Institute 2014a, b). Of the 41 U.S. states which prohibit abortions, exceptions generally apply when it is deemed medically necessary to protect the woman’s life or health (Guttmacher Institute n.d.). According to the Guttmacher Institute, 39 U.S. states require an abortion to be performed by a licensed physician and 20 states require an abortion to be performed in a hospital after a specified point in the pregnancy (Guttmacher Institute 2014a, b).
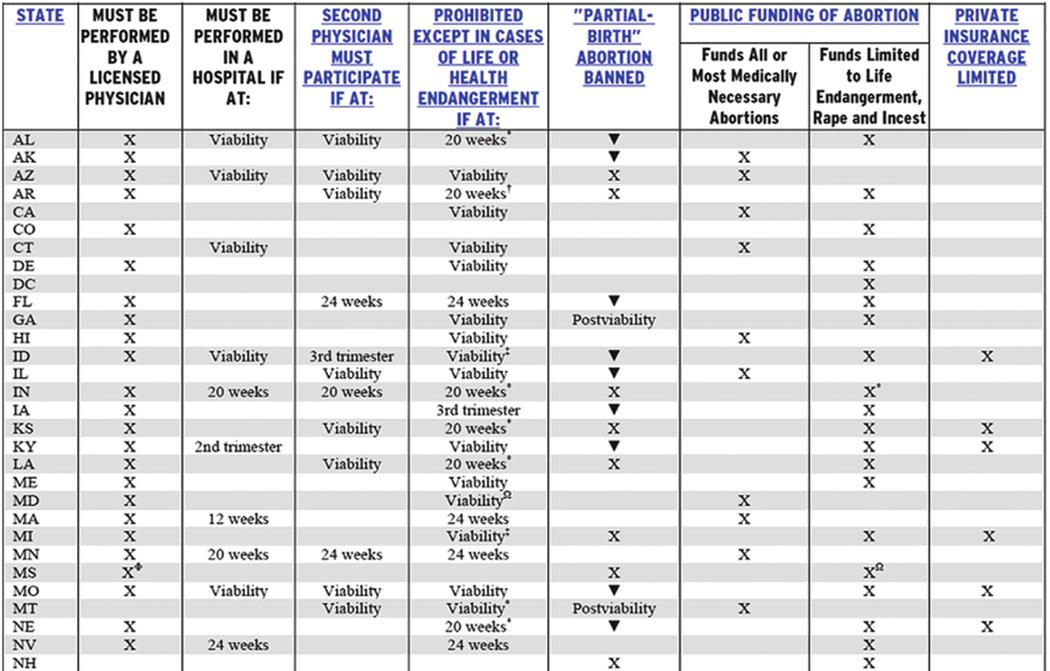
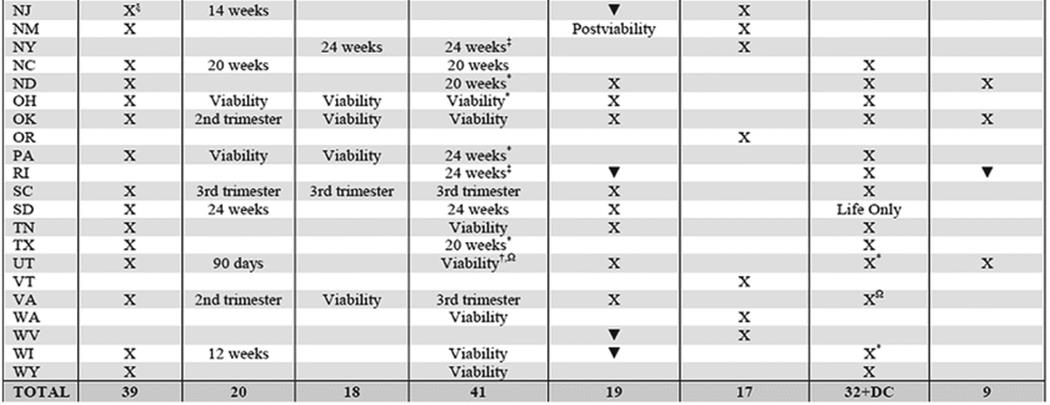
Fig. 16.6
Guttmacher Institute (2014a, b): An overview of US abortion laws
Availability of Hormonal Emergency Contraception in the USA: A Curious Case of Political and Religious Influence
The United States celebrates free markets and yet the competitive forces of medicine and religion have featured in the American social landscape since the nation’s beginnings (Prescott 2011). The complex intertwining of religion, politics and science has been well illustrated by the story surrounding emergency contraception which has been written about at length but will be summarized here.
Emergency contraception (EC) in the form of Plan B has been available by prescription in the United States since 1999. Plan B consists of two 0.75 mg levonorgestrol tablets to be taken 12 h apart as soon as possible and within 72 h after an act of unprotected or inadequately protected intercourse. Efficacy decreases with time so any delay in taking the therapy is critical. In October 2002, three States (Alaska, California and Washington) had made EC over the counter in pharmacies. However, even then many pharmacies were unwilling to advertise this service. Evidence then suggested that 93–97 % of a representative sample of women understood the main purpose of EC (Raymond et al. 2009).
The American College of Obstetrics and Gynecology (ACOG) supported the change to over the counter status (OTC) and provided guidance (American College of Obstetricians and Gynecologists, Committee on Health Care for Underserved Women 2012; American College of Obstetricians and Gynecologists 2010). Opposition came from the National Right to Life Committee some of whose members objected and Pharmacists for Life who claimed EC was an ‘abortifacient’. In response to a submission by a product license holder (Barr Labs), the FDA convened an Advisory panel who voted 23-4 in favor of Plan B being made available without a prescription (Food and Drug Administration 2003).
There was widespread coverage in the main media outlets which was by and large very supportive. However, organizations such as Christian Science Monitor claimed such a decision would lead to more irresponsible sexual behavior and spread sexually transmitted disease. In February 2004, the FDA said it would delay decision until May. The FDA requested further evidence about experience in those aged 16–17 years. A coalition of conservative lawmakers led by Republican Dave Weldon (R-Fla) claimed easier access would increase unsafe sex particularly amongst teenagers. The Catholic Medical Association stated that without medical advice, use of Plan B would be disastrous. The American Life League submitted a petition of 20,000 signatures objecting to Plan B as an abortifacient. In May 2004, the FDA rejected the application on the grounds that girls less than 16 years of age could not use safely Plan B unsupervised. The FDA suggested that OTC status might be granted for women over 16 whereas those younger than 16 would require a prescription. The ACOG (at its 52nd Annual Meeting on May 4th 2004) and Physicians for Reproductive Choice and Health accused FDA of caving into political pressure and disregarding science (Grimes 1994).
Wisconsin introduced an emergency hotline for EC and Plan B was becoming increasingly available through the Internet and social media. A further three states had legislated to permit OTC use: Hawaii, New Mexico and Maine. The FDA repeatedly denied influence from the Bush administration although some external commentators suspected that ‘re-election’ concerns and influence of the right may have been significant. In August 2005, the FDA announced that it had indefinitely deferred Barr’s application for Plan B – a move which was strongly supported by the Secretary of Health Human Services (HHS). Shortly after, Susan Wood, FDA Assistant Commissioner Women’s Health, resigned in protest (Wood et al. 2012). The mainstream media were deeply critical of the FDA position and both the American Medical Association and American Academy of Pediatrics supported OTC Plan B without age limits (Wood et al. 2005).
In February 2011, Teva Women’s Health Inc. (who had taken over Barr Labs) submitted to the FDA a supplemental new drug application for Plan B One-Step, which was the same single dose product and active ingredient as submitted 8 years previously. In December 2011 the FDA inferred that it was ready to grant approval without age restrictions. There then followed an unprecedented intervention by Kathleen Sebelius, Director of HHS, who announced that she believed that the evidence did not conclusively establish that Plan B One-Step should be made available over the counter for all girls of reproductive age (Johnson 2011). Of note, a further Presidential election was due in 2012.
Meanwhile, a legal application to challenge the FDA’s decision had been filed in 2005 by the Center for Reproductive Rights. On April 15th 2013, District Judge Edward Korman overturned the HHS and FDA decision and ordered the FDA to approve the application for Plan B with no age restrictions within 30 days. His argument was based on the premise that age restriction is a barrier to access by those on low income and teenagers, because all would have to show age identification. His ruling was severely critical of the interference by Sebelius in the regulatory process. There were considerable attempts by the US Department of Justice, through the 2nd Circuit Court of Appeals, to delay or even the overthrow the decision (US District Court for the Eastern District of New York 2013).
On June 10, 2013, the FDA notified Judge Korman of its intent to comply with the court’s April 5, 2013 order. To comply, the FDA had asked Teva Women’s Health, to submit a supplemental application seeking approval of the one-pill product to be made available without any restrictions. The FDA fulfilled its commitment to the court by promptly completing its review and approving the supplemental application. The press statement from FDA stated that “over-the-counter access to emergency contraceptive products has the potential to further decrease the rate of unintended pregnancies in the United States (Food and Drug Administration 2013).
This year, in 2014, the FDA expanded access to generic and cheaper versions of Plan B so that these products can now be sold over the counter without age restrictions. Generic versions of the emergency contraceptive were restricted to women ages 17 and older, but those restrictions have now been lifted. The FDA has stated that the only stipulation now is that generic forms of the drug must say they are intended for “women 17 years of age or older,” but no ID check is required. So this ends a decade of wrangling over the accessibility of Plan B in the US (Uhl 2014).
However, this did not mean ready availability of emergency contraception. For example, some hospitals in the U.S. had not been routinely offering emergency contraception to the patients even when they had been victims of sexual assault. Two studies from Illinois and North Carolina found that emergency contraception was offered to victims of sexual assault only in 51 % and 40 %, respectively (Cremer et al. 2010).
Meanwhile, levonorgestrel emergency contraception had become available over-the-counter in Norway (2000), Sweden (2001), The Netherlands (2004), India (2005), Canada (2008), and Spain (2009). Another 45 countries now allow access from a pharmacist without a prescription. The regulatory review in general is that the physical and medical risks are few and the main concern is awareness, availability, and privacy. Formal availability does not mean the medication will be accessible though. In Italy, many doctors refuse to prescribe it, and many pharmacists refuse to sell it, arguing with their right for professional self-determination and conscience. Given the very low risks of harm, it has been suggested that availability without prescription at general sales outlets, such as supermarkets, would remove the legal duty of physician and pharmacists to provide the medication and relieve them of moral dilemmas leaving provision to market forces and personal choice (Ceva and Moratti 2013). Thus it is unlikely that we will have heard the last of how best to manage the benefits and risks of emergency contraception.
The Impact of Religion
Religion may impact on the use of women’s medicines, especially contraception by either creating barriers or facilitating use. Unfortunately, studies of such questions are hampered by methodological limitations such as cross-sectional approach to data collection, non-representative samples and limited measures of religion.
Religion affects the formation of sexual attitudes, behaviors, and ethics of teenage sexuality. Mark Regnerus, a professor of sociology at the University of Texas, in his book Forbidden Fruit explored the relationship between religious discourse and sexual behaviors of American teenagers (Regnerus 2007). The research was based on several outstanding national data sets. About 97 % Americans believe in God, about 80 % claim that religion is fairly important to them, and more than half regularly participate in religious services. The vast majority of youth also participate in some sort of sexual activity. Prior to this book, research concerning religiosity and sexual behavior of American teenagers was considerably limited. The topics had indeed been studied but always separately from each other. Regnerus delivered a comprehensive presentation of religion’s effects on teen sexual behaviors, perceptions of risk, motivations, and attitudes. Religiosity, more than religious affiliation, influences adolescent decision-making. The core message religious parents tend to communicate to their children is more related to morality and values rather than sexuality.
The attitudes of Christian youth, especially those who declare themselves as Protestants, are rather conservative, and the pledge of abstinence does have delaying effect on start of sexual activity. Regnerus’s findings suggest that teen sexual life is nowhere near as rampant as presented by the media. The use of contraception by teens is unreliable not because of religious attitudes but because of their flawed risk perception, reliance on unproven techniques and lack of planning (Davidson 2011). This is discussed further in Chap. 3 (Prescribing Medicines to Adolescent Women, p. 69).
Issues Influencing Use of Women’s Medicines in Developing Countries
Perspectives on women’s medicines in developing countries are discussed in some detail in the following chapter (Chap. 18, p. 531) but we would also like to comment here on issues in these countries, particularly in relation to political and religious influences.
We know that in some cultures when it comes to contraceptive use and family planning, women lack decision-making power to negotiate about sex, childbearing and contraception, as husbands assume sexual access and control. While a husband can, and often does, refuse to use contraceptives despite his persistent sexual demands, women find themselves caught in their conflicting roles as solely responsible for family planning, and at the same time to be sexually available to their husbands.
In some developing countries, ill women still need their husbands’ approval before they can go out to seek medical treatment or health care. Or, when they do arrive at the hospital, there are numerous medical procedures that require their husbands’ signatures. Thus, in such countries gender roles and male-female power relations have a more important role in influencing how women’s medicines will be used compared with traditional medical practice.
Although, as we mentioned earlier, since 1994 some governments have been obliged to provide access to means of control over one’s own reproduction, some countries still have a long way to go. Rashid conducted research among adolescent married women in urban slums of Bangladesh (Rashid 2011). She described and contrasted in detail the irrelevancy of international agreement on human rights when young women are intimidated by the patronage structure of local gangs who fill the vacuum created by the failure of government involvement to providing essential women’s health services (Rashid et al. 2011).
Not all people think that having fewer children is a blessing and some get deeply suspicious about genocidal agendas of ‘birth control missionaries’. Family planning was introduced in Malawi in the 1960s but was banned shortly afterwards and it took 20 years of dialogue to reintroduce a child spacing program as part of the country’s population management. The people of Malawi were extremely unhappy about the whole idea of contraception and understood it as a post-colonial conspiracy to wipe out the black population. Policy guidelines were first introduced in Malawi in 1992 and amended in 1996 to remove barriers such as spousal consent, age, and parity. Total fertility declined only slowly from 6.7 children per woman in 1992 to 6.0 in 2004 and about 5.6 in 2010. African society is constructed in such a way that high fertility and a large surviving family is economically and socially rewarding. This is in stark contrast to western societies where many women who want to have a family postpone their children till later or limit the size of a family below what they actually want because of socio-economic pressure (Palamuleni 2013).
The situation was similar in other African nations, too. After gaining independence in 1980, Zimbabwe received worldwide recognition for its effective family planning programs. But, Zimbabweans took a hostile position to the idea because of concerns over conspiracy to control the black population. Pro-birth tribal politics in Kenya in combination with religious concerns shaped fierce opposition against governmental family planning efforts to slow down population growth in the 1960s and 1970s. Governmental involvement in family planning programs, especially in low-income countries generates deep suspicions over genocidal efforts among the population, especially when funded from high income countries. Sentiments and clashes over family planning may be so powerful that they can bring down entire governments.
Shiffman and Quissel (2012) make a good case for full consideration of political and religious objections in newly reintroduced family planning policies in low-income countries. A report in the Lancet arising from the London Family Planning Summit in July 2012 indicates that the efforts to provide men and women in low-income countries methods to control their own fertility are gaining momentum once again (Shiffman and Quissell 2012).
In Pakistan (which is discussed in some detail in Chap. 18), as many as 60 % women believe that family size is determined by God (Farid-ul-Hasnain et al. 2013). The frequency varies between rural and urban areas. Religious figures are both spiritual and community leaders so their influence is ubiquitous and hard to evade. Premarital and extramarital sex is forbidden by both religion and culture, marriage follows only a few years after the onset of puberty and illiteracy and limited access to information excludes any possibility of informed autonomous decision-making. Most young women learn about sex on their wedding night and only learn that sex leads to pregnancy when they learn they are pregnant (Ibid).
About 32 % of Pakistani students believed use of oral contraceptives was against Islamic philosophy (Ajmal et al. 2011). Illiteracy rates remain high especially in rural areas and access to healthcare is very difficult as described in Chap. 18. In 2006–2007, less than a quarter of Pakistani married women use contraception, up from 9 % in 1999. In a survey conducted in 2006–2007, 96 % of ever-married and currently married women age 15–49 knew of at least one method of family planning. This had increased from about 62 % in 1984–1985 (National Institute of Population Studies, Islamabad, Pakistan, and Macro International Inc., Calverton, Maryland USA 2008). However, there are significant barriers to contraceptive use in Pakistani society, due to numerous cultural factors such as son preference and high prevalence of misinformation and misconceptions about contraceptive products and their side effects (Farid-ul-Hasnain et al. 2013). In the 2006-6 survey, 28 % of married non-users attributed single causes for non-use as “up to God” and 10 % because their husband opposed use (National Institute of Population Studies, Islamabad, Pakistan, and Macro International Inc., Calverton, Maryland USA 2008).
Religious, Moral and Ethical Objections to Provision of Women’s Medicines
Based on the Ethical and Religious Directives for Catholic Health Care Services (ERD), Catholic hospitals have refused to provide emergency contraception, perform abortions and sterilization procedures, as well as in vitro fertilization (IVF) treatment.
The Catholic argument is that IVF goes against natural conception, and that infertility is God’s will. Another argument relates to the number of created embryos to give the couple best chance of pregnancy, and the consequent discarding of embryos which were not used, among other reasons for their poor quality and low chances of survival. Disposal of non-viable embryos is thus seen in the same light as abortion. Objections can come from secular quarters, too, where the main resistance is against unwed and same-sex couples. The treatment is typically not reimbursed so the poor are excluded by default.
Religious issues have profound impact on access of vulnerable populations to reproductive medicines in the developed world as well. This can be illustrated by the history of a long religious battle over a healthcare facility in Austin, Texas. In May 1965, Seton Medical Center entered into an agreement with the city manager of Austin, the then owner of the Brackenridge hospital. Seton was a Catholic facility owned and operated by the Daughters of Charity of St. Vincent DePaul which would take full management and control of the public hospital, Brackenridge. The declared purpose was to continue essential health care services including women’s reproductive, children’, and trauma, for all citizens of the Austin and Travis County, regardless of their financial means. This public/private partnership was not unusual.
The main complication of the deal was Seton’s requirement to adhere to the Ethical and Religious Directives for Catholic Health Care Services developed by the U.S. Conference of Catholic Bishops (USCCB) in 1994 which banned the facility from direct involvement in reproductive services such as contraception, sterilization, abortion, and fertility services, namely in vitro fertilization and insemination to which the Catholic Church morally objected. The directives did permit an indirect role in the delivery of some of these services should a Catholic institution affiliate with a non-Catholic institution.
The conflict which followed lasted 7 years, involved all the aspects of national debate, including intense discussion over the provision of emergency contraception. The Catholic Church is a major stakeholder in the health care field in the U.S. and exerts enormous influence over the provision of health care services. More than 600 Catholic hospitals function in 47 states with 1 in 6 patients being taken care of by a Catholic Church health care facility. The Daughters of Charity National Health System had an excellent record in nursing and managing successful hospitals throughout the nation. The restrictions from Rome; however, and increasing secularization of society, created new challenges for them. The Second Vatican Council, which met through 1962–1965, emphasized social justice and human dignity. The Daughters redefined their governance and ministry and renewed their commitment to the poor and the oppressed. The mission was redefined from ‘bringing students and patients into the nuns’ world’ to ‘nurses entering the patients’ world’, to share their experience.
Secular influences at Seton grew through the 1970s due to appointment of lay administrators, nursing supervisors, and trustees who played a significant role in negotiations with Brackenridge. In cases where a Catholic facility sought affiliation with a non-Catholic institution, it had to ask the local bishop for approval. The bishop in Austin was not normally involved in hospital policy decisions, but it was his responsibility to communicate directly with the Vatican’s Congregation for the Doctrine of the Faith, which was responsible for ensuring that Catholic teachings were implemented in all church facilities. The National Conference of Catholic Bishops, a church policy-making body in the U.S., got involved in the debate on issues of abortion and reproductive services (Wall 2010).
In 1968 the Catholic Church through its Encyclica ‘Humanae Vitae’ (Paul VI 1968) came up with an answer to all this turmoil, which was as much a religious stance as it was political one: it confirmed its position that abstinence is the only acceptable contraception method. With some regional variations, the Church insists on this stance to this day. The 1968 Encyclical Humanae Vitae caused a serious divide between Church hierarchy and laity and caused a split among Catholic clergy. Particularly controversial was the exclusion of reproductive services including family planning from Catholic hospitals which merged with non-Catholic institutions.
The partnership was vital for Brackenridge for several reasons. A significant number of uninsured patients were denied access to healthcare, not only in Austin but nationwide. Brackenridge employees and management were worried that removal of the institution from public scrutiny would allow decision-making behind closed doors. Austin’s bishop John McCarthy, one of the country’s moderates, aggressively supported the deal between Seton and Brackenridge and in July 1995 he wrote a letter to Vatican with background information on the proposed lease. The bishop signed the lease in October 1995, assuming Vatican’s consent. The Vatican responded in March 1996 and again in 1997, with a request that all reproductive services should be ceased. Any breach of contract with the city regarding reproductive services would subject Seton to a multimillion dollar fine.
The Texas Family Planning Association was very uneasy about the whole situation because they were not allowed to be involved. In 2000 the situation dramatically changed after McCarthy’s retirement and appointment of more conservative bishop Gregory Aymond, a supporter of Vatican teachings, by John Paul II. Aymond was the representative to the USCCB 2001 meeting when the bishops developed new Ethical and Religious Directives and agreed to especially focus on Part Six ‘Forming New Partnerships with Health Care Organizations and Providers’. After considering several options, the city proposed to create a hospital within a hospital, which would handle all contraception and sterilization services and emergency contraception for women after a sexual assault. The Daughters of Charity resolved the conflict by offering an innovative compromise. In many ways, the resolution of this conflict serves as an example of strong and competent leadership focused on key goals, which were to maintain essential services for all people of Austin, including the poor (Wall 2010).
In the U.S. most states have ‘conscientious objection’ in their legislation which allows physicians to opt out from performing abortions. Meyers and Woods argue that physicians have an obligation to perform all socially sanctioned medical services, including abortions. The case study presented by Meyers and Woods outlines conflicting legal obligations between a state-mandated obligation to provide abortion services for two population groups – inmates from local penal facility and those deemed incompetent to make their own medical decisions – and the right of physicians to opt-out from providing abortion services. Of eight physicians qualified to perform the procedure only one was willing to perform elective abortions. As a result of this opt-out clause, as of 1991, 83 % of US counties had no abortion provider (Meyers and Woods 1996) compared to 89 % in 2011 (Guttmacher Institute n.d.).
Religious Beliefs About Blood Transfusion
A patient’s refusal of blood transfusion on religious grounds is one of the most controversial examples of conflict between medical ethics and religion. Jehovah’s Witnesses consider refusal of blood transfusions fundamental because acceptance of blood which is sacred would prevent them from entering Paradise. Members of the Church are required to observe this rule under threat of expulsion from the community. No other religion is so extreme in their view. Jehovah’s Witnesses who accept blood and in this way revoke their membership in the organization are then ostracized by the community to the point that they are completely blanked by their lifelong friends and family members who are still part of the Church, and essentially treated as outcasts.
The Watchtower Society introduced the policy of refusal of blood transfusion in 1945. Since 1961 it enforced zero tolerance towards those who wilfully accept blood transfusion. In 2001, Dr. Carl Saphier conducted a study with the purpose of determining the rates of obstetric haemorrhage and maternal mortality in women Jehovah’s Witnesses. Death rate of 521 deaths per 100,000 live births among Jehovah’s Witnesses constitutes a number approximately 44 times higher than the general US population. According to Dr Reed, former Witness and currently a widely recognised authority on the sect, the number of deaths worldwide caused by refusal of blood transfusion on religious grounds is estimated around 9,000 a year (Radomyski 2011).
Otherwise, Jehovah’s Witnesses accept most medical treatments, surgical and anaesthetic procedures, devices and techniques, as well as haemostatic and therapeutic agents that do not contain blood, for example non-blood fluids such as crystalloids and colloids, erythropoiesis stimulating agents (ESAs), desmopressin, vasoconstrictors and recombinant clotting factors (Royal United Hospital Bath NHS Trust 2013).
Conscientious Objection to the Provision of Emergency Contraception
Wicclair argues that the refusal to provide emergency contraception to the victims of sexual assault based on conscience is unjustified, because an institution “cannot have a conscience”, an attribute, as well as ethical and moral objections can only be expressed by human beings (Wicclair 2011). However, in some instances the hospital mission can be considered an analogue to the conscience of a physician, nurse or pharmacist. One way to explore moral identity of an institution is to explore its mission statement. Although it is disputable why staff of such an institution should be required not to make an exception on offering emergency contraception for rape victims, there are several reasons for enabling hospitals to maintain their identity and integrity by exempting them from general institutional obligations. First, it may be important to staff to work in institution which shares a commitment to a core set of goals, values, and principles, and violation of these values may at the very least to moral distress. The same principle applies to patients who seek care in such an institution (Wicclair 2011).
Human Papillomavirus Vaccine: A Case Study of the Issues Associated with Mandatory Vaccination in Michigan, USA
Compulsory vaccination against Human Papilloma Virus (HPV) became a hot political issue in the U.S. The vaccine (Gardasil) was first approved by the FDA in September 2006 (the HPV vaccine is discussed further in Chap. 9). Gardasil protects against four strains of HPV, the most common sexually transmitted disease in the U.S., including the strains which are linked to higher incidence of cervical cancer. Because the vaccine has the greatest benefit before a person becomes sexually active, the Advisory Committee on Immunization Practices recommended its application to girls between 11 and 12 years of age (Centrum for Disease Control and Prevention 2013).
Three months after approval was granted the vaccination became compulsory for all girls entering sixth grade in Michigan. Making vaccination mandatory in this way caused a furious political debate. Although Advocacy groups such as Focus on the Family did not object to availability of the vaccine, they certainly objected to its mandatory use. In their view, such a requirement by a secular state constitutes intervention which may be irreconcilable with the child’s family’s religious values and beliefs.
Groups which are recommending mandatory HPV vaccination have drawn an analogy with the success of breast cancer screening procedures which has saved many women’s lives by enabling them to receive treatment earlier. A critical question is whether achieving a higher level of coverage justifies the infringement of parental autonomy that compulsory vaccination inevitably entails. Different ethical frameworks that accord varying weights to communitarian and individualistic values will lead to contrasting answers to this question. Ethical and epidemiological analyses are essential to decisions about mandating a medicine such as the HPV vaccine, as are political calculations and the possibility that additional mandates may inflame grassroots opposition, be it religious, philosophical, or ideological (Zimmerman 2006; Colgrove 2006).
Female Subjects in Clinical Research Studies
Following the guidance arising from Declaration of Helsinki in 1964, the restriction on participation of vulnerable subjects in clinical research originally referred only to pregnant women. It was later extended by the FDA in 1977 to all premenopausal women of childbearing age as the most effective way of minimizing this risk (FDA 1977; National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research 1979). This was understandable following the thalidomide and diethylstilbestrol (DES) disasters. The former disaster is very well known, whereas the latter was relatively more recent and its consequences are still ongoing with concerns about adverse effects in the grandchildren of DES women.
Diethylstilbestrol (DES) is a synthetic form of oestrogen that was prescribed to pregnant women between 1940 and 1971 to prevent miscarriage. In the early 1950s research was conducted to assess the efficacy of this treatment and no benefit was found to substantiate its use. Despite this, DES continued to be prescribed. According to the CDC DES Update: Consumers 2014; only in the 1970s did it come to light that daughters of women who were taking this medication during pregnancy had a higher risk of clear cell adenocarcinoma of the vagina and cervix (Herbst et al. 1971). In 1971, the FDA advised that use in pregnancy was contraindicated (Editorial, Western J Med, 1971). In some European countries such as France, Netherlands and the UK the drug continued to be prescribed in pregnancy until 1977 under the name Distilbène®. However, it was not until 2000 that approval for use in humans was completely withdrawn by FDA in the US. There is a modestly increased risk of breast cancer and cervical cancer among women who had been taking DES during pregnancy (National Cancer Institute at the National Institutes of Health 2011).
Women make up over half over the world population but their health needs (except for reproductive concerns), as well as involvement in clinical research has lagged behind. Therefore, realization set in that not including women in developmental programs was becoming a significant safety concern in its own right because of the missing information about benefit-risk at the time of approval. The policy not to include women in research started to change in the US around 1986–1987 after the NIH issued guidelines urging inclusion of women for the first time in NIH Grants and Contracts (National Institutes of Health (NIH) 2003; National Institute of Health Office for Extramural Research 2014a, b). In 1990 the Women’s Health Equity Act was passed and the Center for Disease Control and Prevention (CDC) established the National Breast and Cervical Cancer Prevention Program (Mikulski 1990).
In June 1993, the National Institute of Health (NIH) Revitalization Act (An Act To amend the Public Health Service Act to revise and extend the programs of the National Institutes of Health, and for other purposes, 1993) included the following key points:
· reauthorized certain expiring authorities of the NIH,
· mandated establishment of the Office of Research Integrity,
· lifted the moratorium on human fetal tissue transplantation research
· mandated inclusion of women and minorities in clinical research protocols
· created the Office of Research on Women’s Health,
· created the National Center for Human Genome Research,
· mandated establishment of an intramural laboratory and clinical research program on obstetrics and gynaecology within The Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD).
The law stirred much political controversy. This was particularly because the moratorium on research on human embryos from IVFs had been terminated by creation of the Human Embryo Panel. Until then, all IVF grant proposals had to be approved first by an Ethics Advisory Board and yet no such board had been reconstituted (S.1 – National Institutes of Health Revitalization Act of 1993 – Subtitle B – Clinical Research Equity Regarding Women and Minorities, n.d., p. 1).
In the Consolidated Appropriations Act of 2008, Congress provided the Department of Health of Human Services Office on Women’s Health (OWH) with funds for the Institute of Medicine (IOM) to conduct a comprehensive review of the status of women’s health research, summarize what has been learned about how diseases specifically affect women, and report to the Congress on suggestions for the direction of future research.
The committee focused on conditions that are specific to women, are more common or more serious in women, have distinct causes or manifestations in women, have different treatments and outcomes in women, or have high morbidity or mortality in women. The Committee identified breast cancer, cardiovascular disease and cervical cancer as conditions in which the research contributed to major progress (National Research Council 2010).
Regulation of Women’s Medicines and Risk Management Plans
Current regulatory practice for maintaining a satisfactory balance of benefit and risk of medicines and ensuring proper use depends on a risk management plan involving all stakeholders. This is primarily governed by medicines legislation targeted to the pharmaceutical industry and regulatory agencies based on guidelines developed by The International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH) (“ICH E2E” 2004). A medicines regulatory perspective on women’s medicines is covered in Chap. 16 of this book and will therefore not be covered in detail here.
Call for a More Holistic Approach
From our review of the place of women’s medicines, especially those for controlling reproduction, we suggest that a more holistic view of managing the risks of these medicines is needed. This should involve taking into account social, religious and political views, and long-term demographic consequences for the community and nation in case overall birth rate declines below replacement level, or exceeds limitations imposed by the community’s resources.
This harks back to 1999 when the FDA produced a risk management framework for all medicines in the USA. The FDA had convened a Task Force which subsequently recommended that FDA take the opportunity to engage all stakeholders to re-examine the current system for managing the risks associated with the use of medical products. They encouraged public policy discussion that focused on defining more clearly the roles and responsibilities of all participants of the risk management system.
An activity often lacking in risk management models is risk confrontation: community-based problem solving that actively involves relevant stakeholders in the decision-making process (U.S. Department of Health and Human Services and Food and Drug Administration 1999). Even as far back as 1989, The National Research Council wrote that determining the acceptable level of risk should occur in a larger context. So even for medicines in general, social and community values are at least as important as the technical judgments of professionals and should be included in the determination of acceptable risk (National Research Council 1989).
Risk confrontation is not in ICH E2E and is not routinely part of the RMPs required by ICH agencies. Interesting, as of December 2013, there is no FDA published Risk Evaluation and Mitigation Strategies for contraceptive medicines. Given the important interaction between religious, political and social factors, we recommend for policy holders that a more robust approach is taken to managing the risks of reproductive medicines, taking all stakeholders – in particular women themselves – into account. A transparent approach to examining all concerns and sources of evidence is required. This means that concerns that were expressed about emergency contraception, as an example, could be captured as ‘missing information’ in a RMP. We should examine the root causes behind such a safety concern as they may need to be addressed.
Conclusions
Women with their specific needs and inevitably dependent status in certain stages of life are much more vulnerable to the effects of the political and religious environment which surrounds them. Religious beliefs of the society which surrounds them may affect their sexual and reproductive behavior at least to the same level as their own beliefs and values; and political and socio-economic environment determines choices they have with regards to reproductive behavior.
Any methods designed to control the level of human reproduction are a sensitive political as well as religious matter and a public health issue. The reproductive health of a nation is of key importance to public health. Therefore, risks associated with the use and misuse of women’s medicines that control fertility and reproduction affect the health and well-being of the individual as well as long-term health of society and its sustainability.
Political decisions, socio-economic environment, culture, administrative measures, religious influences, and public policies profoundly affect decision-making of individuals and couples when and how they start a family, how many children they wish to have, how many children they do have; and spacing and timing of pregnancies. Thus we need to adapt our approach to risk management by adapting planning to social, religious and cultural variation. This will have implications for advising women about how to use medicines and for the design of educational programs about safe use of medicines for the advancement of women’s well-being and health.
Take Home Messages
· Public health agencies need to understand how reproductive health of women is central to sustainable development.
· Healthy choices need to be made available to all women, including those who wish to pursue their education and career and have a family.
· Contraceptive medicines are intended to empower women to time their pregnancies better and are not intended to prevent pregnancy altogether.
· Although knowledge about contraception is expanding, as its use, there are still parts of the world where ignorance prevails.
· Even within the European Union, the social fabric of some Member States will mean that a risk management plan for a contraceptive or a plan that involves fertility control will vary. Indeed, the ability of some women to report suspected adverse reactions or other problems with women’s medicines may be severely impaired.
· Risk management must adapt according to the prevailing social and religious attitudes and opinions of the time
· Clinicians/pharmacists need to understand how medicines for controlling reproduction are very different in that their benefit/risk depends on the political policies, social and religious beliefs and values within a society at any given time.
· Access to contraception and acceptability of methods depend on the cultural background of the women concerned and her set of beliefs.
· Treatments that control fertility can be an extremely delicate matter because individual circumstances even within a religious group may vary widely.
· In some political, religious or other environments safety issues may not be readily discussed or revealed and so must be sought using sensitivity and respect for an individual’s cultural values.
References
Ajmal F, Agha A, Karim MS (2011) Knowledge, attitudes and practices (KAP) regarding sexuality, sexual behaviors and contraceptives among college/university students in Karachi, Pakistan. J Coll Physicians Surg Pak 21(3):164–168PubMed
Allès É (2006) Thomas Scharping, birth control in China, 1949–2000. Population policy and demographic development. China Perspect [Online] 59 (no. May–June 2005). http://chinaperspectives.revues.org/484
American College of Obstetricians and Gynecologists (2010) ACOG practice bulletin no. 112: emergency contraception. Obstet Gynecol 115(5):1100–1109. doi:10.1097/AOG.0b013e3181deff2aCrossRef
American College of Obstetricians and Gynecologists, Committee on Health Care for Underserved Women (2012) Access to emergency contraception, committee opinio no 542. Obstet Gynecol 120:1250–1253
Berger MW (2010) Virtue, vice, and contraband: a history of contraception in America. Bull Hist Med 84(2):281–282CrossRef
Berkman JA (2012) The morning after: a history of emergency contraception in the United States. Bull Hist Med 86(2):296–297CrossRef
Bliley T (1999) An act to amend the Controlled Substances Act to direct the emergency scheduling of gamma hydroxybutyric acid, to provide for a national awareness campaign, and for other purposes. https://www.govtrack.us/congress/bills/106/hr2130
Bradatan C, Firebaugh G (2007) History, population policies, and fertility decline in Eastern Europe: a case study. J Fam Hist 32(2):179–192. doi:10.1177/0363199006297732CrossRef
Brainerd E (2010) Human development in Eastern Europe and the CIS since 1990. Human development research paper 2010/16, United Nations Development Programme, United Nations. http://hdr.undp.org/sites/default/files/hdrp_2010_16.pdf
Brown K (2011) The day embassy Kabul forever changed: remembering the 1979 assassination of Adolph ‘Spike’ dubs and the dismantling of the American Civilian Mission in Afghanistan. Small Wars J. http://smallwarsjournal.com/jrnl/art/the-day-embassy-kabul-forever-changed
Buckley M (2013) Of human bonds: between sex work and trafficking. Fair Observer, 9 Sept 2013. http://www.fairobserver.com/article/human-trafficking-and-out-russia
Cassidy RM (2012) War, will, and warlords – counterinsurgency in Afghanistan and Pakistan 2001–2011. Marine Corps University Press, Quantico. http://www.marines.mil/Portals/59/Publications/War,%20Will,%20and%20Warlords.pdf
Centrum for Disease Control and Prevention (2013) HPV vaccines. Centrum for Disease Control and Prevention, 5 Feb 2013. http://www.cdc.gov/hpv/vaccine.html
Ceva E, Moratti S (2013) Whose self-determination? Barriers to access emergency contraception in Italy. Kennedy Inst Ethics J 23(2):139–167PubMedCrossRef
Chalik G (2014) Book chapter, 3 Apr 2014
Clark G, Alter G (2010) The demographic transition and human capital, 1700–1870. In: The Cambridge economic history of modern Europe, Vol. 2010. Volume 1, 1700–1870. Cambridge University Press. http://dev3.cepr.org/meets/wkcn/1/1679/papers/Alter-Clark_Chapter.pdf
Clayton A (2014) The FDA, sexual dysfunction and gender inequality. Huffington Post, 7 Feb 2014. http://www.huffingtonpost.com/anita-h-clayton-md/the-fda-sexual-dysfunctio_b_4724459.html
Colgrove J (2006) The ethics and politics of compulsory HPV vaccination. N Engl J Med 355:2389–2391PubMedCrossRef
Cremer ML, Nichols S, Masch RJ (2010) Breaking the barriers to emergency contraception access in the USA: the time has come. Expert Rev Obstet Gynecol 5(2):195–201CrossRef
Croll E (1981) Women in rural production and reproduction in the Soviet Union, China, Cuba, and Tanzania: socialist development experiences. Development and the Sexual Division of Labor 7(2):361–374
Curtin SC, Abma JC, Ventura SJ, Henshaw SK (2013) Pregnancy rates for U.S. women continue to drop. NCHS data brief, no. 136. National Center for Health Statistics, Hyattsville, 136:1–8.
Davidson S (2011) Forbidden fruit: sex & religion in the lives of American teenagers. J Youth Adolesc 40(6):752–755CrossRef
Davin D (2004) Book review: birth control in China, 1949–2000: population policy and demographic development. Med Hist 48(1):130–131PubMedCentralCrossRef
Denisov B, Sakevich V, Jasilioniene A (2013) Divergent trends in abortion and birth control practices in Belarus, Russia and Ukraine. PLoS One 7(11):1–10. doi:10.1371/journal.pone.0049986
DHHS, The National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research (1979) The Belmont report. Ethical principles and guidelines for the protection of human subjects of research. U.S. Department for Health, Education, and Welfare
DHHS (2003) Reproductive, maternal, and child health in Eastern Europe and Eurasia: a comparative report division of reproductive health centers for disease control and prevention. DHHS, Apr 2003. http://dhsprogram.com/pubs/pdf/od28/00frontmatter.pdf
Eberstadt N (2011) The dying bear – Russia’s demographic disaster. Foreign Affairs, Dec 2011
European Medicines Agency (2010a) EPAR summary for the public Intrinsa testosterone. EMA/369753/2010, EMEA/H/C/634. European Medicines Agency. http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/000634/human_med_000845.jsp&mid=WC0b01ac058001d124
European Medicines Agency (2010b) Press release Warner Chilcott UK Ltd withdraws its application for an extension of indication for Intrinsa. European Medicines Agency. http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/000634/wapp/Post-authorisation/human_wapp_000102.jsp&mid=WC0b01ac058001d128
European Medicines Agency (2010c) Withdrawal assessment report for Intrinsa. EMA, London, Oct 2010. http://www.ema.europa.eu/docs/en_GB/document_library/Application_withdrawal_assessment_report/2010/10/WC500098424.pdf
Eurostat (2013) Demographic profile of EU-27 population, 1990, 2000, 2012, 2020 (million persons). Eurostat, July 2013. http://epp.eurostat.ec.europa.eu/statistics_explained/index.php/Europe_2020_indicators_-_employment
Farid-ul-Hasnain S, Johansson A, Gulzar S, Krantz G (2013) Need for multilevel strategies and enhanced acceptance of contraceptive use in order to combat the spread of HIV/AIDS in a Muslim society: a qualitative study of young adults in Urban Karachi, Pakistan. Glob J Health Sci 5(5):57–66. doi:10.5539/gjhs.v5n5p57PubMed
Food and Drug Administration (1977) General consideration for the clinical evaluation of drugs. U.S. Department for Health, Education, and Welfare
Food and Drug Administration (2003) Joint session of the nonprescription drugs advisory committee and the advisory committee for reproductive health drugs. Food and Drug Administration, 16 Dec 2003
Food and Drug Administration (2004) FDA Intrinsa Advisory Committee background document overview. Food and Drug Administration. http://www.fda.gov/ohrms/dockets/ac/04/briefing/2004–4082b1_02_a-fda-intrinsa-overview.htm
Food and Drug Administration (2013) FDA approves plan B one-step emergency contraceptive for use without a prescription for all women of child-bearing potential. FDA Newsroom, 20 June 2013. http://www.fda.gov/newsevents/newsroom/pressannouncements/ucm358082.htm
FSSS (2013) Vital statistics. Population: main indicators. Russian Federation Federal State Statistics Service, Moscow. http://www.gks.ru/bgd/regl/b13_12/IssWWW.exe/stg/d01/5–05.htm
Grimes S (1994) Fertility decline in Western Europe. Population Research Institute. http://www.pop.org/content/fertility-decline-in-western-europe-1727
Grindlay K, Burns B, Grossman D (2013) Prescription requirements and over-the-counter access to oral contraceptives: a global review. Contraception 88(1):91–96. doi:10.1016/j.contraception.2012.11.021PubMedCrossRef
Guttmacher Institute (2013) Unintended pregnancy in the United States, Dec 2013. http://www.guttmacher.org/pubs/FB-Unintended-Pregnancy-US.html
Guttmacher Institute (2014a) Abortion in the United States. Advancing Sexual and Reproductive Health Worldwide through Research, Policy Analysis, and Public Education, 1 May 2014. http://www.guttmacher.org/media/presskits/abortion-US/statsandfacts.html
Guttmacher Institute (2014b) An overview of abortion laws. State policies in brief. Guttmacher Institute, 1 Apr 2014. http://www.guttmacher.org/statecenter/spibs/spib_OAL.pdf
Herbst AL, Ulfelder H, Poskanzer DC (1971) Adenocarcinoma of the vagina. Association of maternal stilbestrol therapy with tumor appearance in young women. N Engl J Med 284:878–881PubMedCrossRef
Horga M, Gerdts C, Potts M (2013) The remarkable story of Romanian women’s struggle to manage their fertility. J Fam Plann Reprod Health Care 39:2–4. doi:10.1136/jfprhc-2012-100498PubMedCrossRef
International Conference on Population and Development – ICPD – Programme of Action (1994) Report of the international conference on population and development. International Conference on Population and Development – ICPD – Programme of Action, Cairo, 5 Sept 1994. http://www.unfpa.org/public/home/publications/pid/1973
Johnson C (2011) U.S. Dept of Health & Human Services Secretary Kathleen Sebelius – a statement on plan B one-step (December 7, 2011). RapGenius, 7 Dec 2011. http://news.rapgenius.com/Us-dept-of-health-and-human-services-secretary-kathleen-sebelius-prepared-testimony-before-house-energy-and-commerce-committee-annotated#note-2375178
Keck CW, Reed GA (2012) The curious case of Cuba. Am J Public Health 102(8):E13–E22PubMedCentralPubMedCrossRef
Mac Donald H (1998) The real welfare problem is illegitimacy. City J. http://www.city-journal.org/html/8_1_a1.html
Meyers C, Woods RD (1996) An obligation to provide abortion services: what happens when physicians refuse? J Med Ethics 22:115–120PubMedCentralPubMedCrossRef
Mikulski B (1990) S.2961 – Women’s Health Equity Act of 1990. http://beta.congress.gov/bill/101st-congress/senate-bill/2961
Ministry of Health, Romania (2005) Reproductive health survey Romania 2004 summary report 2005. Summary report, Ministry of Health, May 2005. http://www.unece.org/fileadmin/DAM/stats/gender/vaw/surveys/Romania/Romania_Publication.pdf
National Research Council (2010) Women’s health research: progress, pitfalls, and promise. The National Academies Press, Washington, DC, p 42. http://www.nap.edu/catalog.php?record_id=12908
National Cancer Institute at the National Institutes of Health (2011) Diethylstilbestrol (DES) and cancer. http://www.cancer.gov/cancertopics/factsheet/Risk/DES
National Institute of Health Office for Extramural Research (2014a) Inclusion of women and minorities as participants in research involving human subjects. National Institute of Health Office for Extramural Research, 12 Mar 2014. http://grants.nih.gov/podcasts/All_About_Grants/episodes/Inclusion_April_2011.mp3
National Institute of Health Office for Extramural Research (2014b) Policy implementation page: inclusion of women and minorities as participants in research involving human subjects – policy implementation page. National Institute of Health Office for Extramural Research, 12 Mar 2014. http://grants1.nih.gov/grants/funding/women_min/women_min.htm
National Institute of Population Studies, Islamabad, Pakistan, and Macro International Inc., Calverton, Maryland USA (2008) Pakistan Demographic and Health Survey 2006–07. National Institute of Population Studies and Macro International Inc., Islamabad, June 2008. http://dhsprogram.com/pubs/pdf/FR200/FR200.pdf
National Institutes of Health (NIH) (2003) Guidelines for inclusion of women, minorities, and persons with disabilities in NIH-supported conference grants. NOT-OD-03–066. http://grants1.nih.gov/grants/guide/notice-files/NOT-OD-03–066.html
National Research Council (1989) Improving risk communication. The National Academies Press, Washington, DC. http://www.nap.edu/openbook.php?record_id=1189
Nugent R, Seligman B (2008) How demographic change affects development. Technical background paper. Demographics and development in the 21st century initiative. Center for Global Development. http://www.cgdev.org/doc/Demographic_and_Development/DD_background_12_10_08.PDF
Office of the UN Special Adviser on the Prevention of Genocide (OSAPG) (1948) Convention on the prevention and punishment of the crime of genocide. Office of the UN Special Adviser on the Prevention of Genocide (OSAPG), 9 Dec 1948. http://www.un.org/ga/search/view_doc.asp?symbol=a/res/260(III)
Oppenheim K (2014) VIII. Contribution of the ICPD programme of action to gender equality and the empowerment of women. The World Bank. https://www.un.org/esa/population/publications/PopAspectsMDG/07_OPPENHEIMMASON.pdf
Palamuleni ME (2013) Socio-economic and demographic factors affecting contraceptive use in Malawi. Afr J Reprod Health 17(3):91–104PubMed
Paul VI (1968) Encyclical letter Humanae Vitae of the Supreme Pontiff Paul VI to his venerable brothers the patriarchs, archbishops, bishops, and other local ordinaries in peace and communion with the Apostolic See to the clergy and faithful of the whole Catholic world, and to all men of good will on the regulation of birth. Acta Apostolicae Sedis 60:481–503. http://www.vatican.va/holy_father/paul_vi/encyclicals/documents/hf_p-vi_enc_25071968_humanae-vitae_en.html
Prescott H (2011) The morning after: a history of emergency contraception in the United States. Critical issues in health and medicine. Rutgers University Press. http://rutgerspress.rutgers.edu/product/Morning-After,4650.aspx
Quasha DR (2006) Intrinsa: an inquiry into female sexual dysfunction and testosterone”. Third-year written work requirement, Harvard Law School. http://dash.harvard.edu/bitstream/handle/1/10015296/Quasha06.pdf
Radomyski M (2011) Medical oaths: when religion and ethics collide. Amst Law Forum 3(1):68–80
Rashid SF (2011) Human rights and reproductive health: political realities and pragmatic choices for married adolescent women living in urban slums, Bangladesh. BMC Int Health Hum Rights 11(Suppl 3):S3PubMedCentralPubMedCrossRef
Rashid SF, Akram O, Standing H (2011) The sexual and reproductive health care market in Bangladesh: where do poor women go?”. Reprod Health Matters 19(37):21–31. doi:10.1016/S0968-8080(11)37551-9PubMedCrossRef
Raymond EG, L’Engle KL, Tolley EE, Ricciotti N, Arnold MV, Park S (2009) Comprehension of a prototype emergency contraception package label by female adolescents. Contraception 3(79):199–205CrossRef
Regnerus M (2007) Forbidden fruit: sex and religion in the lives of American teenagers. Oxford University Press, New YorkCrossRef
Royal United Hospital Bath NHS Trust (2013) Jehovah’s witnesses and other patients who refuse blood components. Bath: Royal United Hospital Bath, National Health Service, Apr 2013. http://www.ruh.nhs.uk/about/policies/documents/clinical_policies/blue_clinical/Blue_783_Clinical_Management_of_Jehovahs_Witnesses_and_Other_Patients_who_refuse_blood_components.pdf
Scharping T (2003) Birth control in China 1949–2000. Population policy and demographic development. London/New York, RoutledgeCurzon, xvi+406 p
Shiffman J, Quissell K (2012) Family planning: a political issue. Lancet 380(9837):181–185PubMedCrossRef
Speake B (2012) What is the role of Islam in relation to women’s reproductive and sexual rights in the Middle East and North Africa Region? University of Leeds. http://www.e-ir.info/2012/09/11/islam-and-womens-reproductive-and-sexual-rights-in-the-mena-region/
The Mamre Institute (2014) The role of women. Machon Mamre, 20 Apr 2014. http://www.mechon-mamre.org/jewfaq/women.htm
Thornton, Arland, and Dimiter Philipov (2007) Developmental idealism and family and demographic change in Central and Eastern Europe, vol 2007. Budapest. http://www.oeaw.ac.at/vid/download/edrp_3_07.pdf
Uhl K (2014) Levonorgestrel tablet, 1.5 Mg approval for women 17 Years of age and above. Department of Health and Human Services, Mar 2014. http://www.hpm.com/pdf/blog/PLAN%20B%20-%20FDA%20Exclusivity%20&%20Carve-Out%20Determination.pdf
UN Department of Public Information (2008) GOAL 5: improve maternal health. UN Department of Public Information, Sept 2008. https://www.un.org/millenniumgoals/2008highlevel/pdf/newsroom/Goal%205%20FINAL.pdf
UNFPA (1994) ICPD – international conference on population and development: master plans for development. UNFPA. http://www.unfpa.org/public/home/sitemap/icpd/international-conference-on-population-and-development
United Nations (1968) Final act of the international conference on human rights Teheran. United Nations, New York, 22 May 1968. http://legal.un.org/avl/pdf/ha/fatchr/Final_Act_of_TehranConf.pdf
U.S. Department of Health and Human Services and Food and Drug Administration (1999) Creating a risk management framework report to the FDA commissioner from the task force on risk management. Food and Drug Administration. http://www.fda.gov/downloads/safety/safetyofspecificproducts/ucm180520.pdf
US District Court for the Eastern District of New York (2013) Tummino et al. vs. Hamburg et al., (US District Court for the Eastern District of New York)
Vancaillie T (2013) Emerging trends in female permanent contraception. Expert Rev Obstet Gynecol 8(3):285–294CrossRef
Wagner RL (2011) A life alone for Saudis born out of wedlock. The Jerusalem Post, 29 Dec 2011. http://www.jpost.com/Middle-East/A-life-alone-for-Saudis-born-out-of-wedlock
Wall BM (2010) Conflict and compromise: catholic and public hospital partnerships. Nurs Hist Rev 18:100–117PubMedCentralPubMedCrossRef
WHO (2012) Social determinants of health. Report by the Secretariat. 132nd session: WHO, Executive Board, 23 Nov 2012. http://www.who.int/social_determinants/B_132_14-en.pdf?ua=1
WHO (2014) Facts and figures about abortion in the European Region. WHO, 9 Mar 2014
Wicclair MR (2011) Conscientious refusals by hospitals and emergency contraception. Camb Q Healthc Ethics 20(1):130–138PubMedCrossRef
Wittich VG, Philipov D (2013) UNECE regional report: ICPD beyond 2014: the UNECE region’s perspective (prepublication version). UNECE regional report. United Nations, United Nations Economic Commission for Europe, Geneva, June 2013. http://www.unece.org/fileadmin/DAM/pau/icpd/Conference/Other_documents/Report_ICPD_beyond_2014.pdf
Wood AJJ, Drazen JM, Greene MF (2005) A sad day for science at FDA. N Engl J Med 353(12):1197–1199PubMedCrossRef
Wood AJJ, Drazen JM, Greene MF (2012) The politics of emergency contraception. N Engl J Med 366(2):101–102PubMedCrossRef
Wood B, Gell J (2014) Effects of fatherlessness on children – social consequences. ANCPR: Children’s Legal Foundation, 20 Apr 2014. http://www.ancpr.com/effects_of_fatherlessness_on_chi.htm
Zimmerman RK (2006) Ethical analysis of HPV vaccine policy options. Vaccine 24:4812–4820PubMedCrossRef