Debra A. Guinn
Ronald S. Gibbs
Over the past two decades we have seen a marked increase in survival of very low birth weight infants. This increase in survival has been attributed to increased use of corticosteroids, regionalization of perinatal care, improved methods of mechanical ventilation, availability of exogenous surfactant, and improved nutritional therapy. However, the reduction in mortality has not been accompanied by a reduction in neonatal morbidity or long-term handicaps. It is estimated that 50% of all major neurologic handicaps in children result from premature births.
Despite widespread awareness of the problem and use of therapies believed to be beneficial to prevent preterm births, the rate of preterm delivery is increasing in the United States. The majority of spontaneous premature births occur to women who develop preterm labor or preterm premature rupture of the membranes (PPROM). Cervical incompetence may also result in preterm delivery. Historically, researchers and epidemiologists have approached these conditions as being distinct processes that were mutually exclusive of one another. Recent evidence would suggest that many women have overlapping conditions, which predispose them to deliver preterm. This concept is depicted in Figure 10.1. For example, a women who has preterm delivery secondary to PPROM at 27 weeks gestation, may have had weeks of “silent” or painless contractions or cervical dilation prior to developing ruptured membranes and delivery. Using this broader conceptual framework, this chapter will review the epidemiology, etiology, prevention, and treatment of women with preterm labor.
|
|
|
FIG. 10.1. Overview of spontaneous preterm birth. |
MECHANISMS OF LABOR ONSET
Labor occurs when mechanisms are present that convert the uterus from a state of containment to an environment that attempts to expel the fetus. In humans, the average gestational period is 280 days ± 14 days. Therefore, term labor is defined as labor that occurs between 37 and 42 weeks gestation. Preterm labor is defined as labor that occurs between 20 and 37 weeks gestation. In theory, pathologic activation of the normal parturition process results in preterm labor and delivery.
In both term and preterm labor, following an unknown stimulus, the mechanisms that produce labor override those that maintain the pregnancy. Activation of the parturition process results in membrane activation, cervical ripening, and an increase in myometrial responsiveness to endogenous and exogenous signals. Subsequently, labor progresses along a common pathway that results in uterine contractions that are sufficient to cause progressive cervical dilation to allow for expulsion of the fetus. A number of inciting events have been implicated in premature births. These events include decidual hemorrhage (abruption), mechanical factors (overdistension of the uterus, cervical incompetence), hormonal changes (fetal or maternal stress) or subclinical/clinical infection. Infection is associated with as many as one third of preterm deliveries, particularly those occurring at the earliest gestational ages. The role of infection in preterm labor will be reviewed separately in this chapter.
Animal models have helped in understanding labor. Important findings in animal labor models include an increase in oxytocin receptors present in the myometrium, gap junctions developing between myometrial cells, an increased response to agents capable of producing contractions in the uterus, and physical and biochemical changes of the cervix resulting in a softened consistency. Uterine smooth muscle contractility is produced by the actin–myosin interaction, following myosin light chain phosphorylation, which is controlled by myosin light chain kinase. Myosin light chain kinase is activated by calcium as a calmodulin–calcium complex. Cyclic adenosine monophosphate (cAMP) also regulates kinase by inhibiting phosphorylation. Many factors are involved in this control. Some of the proposed theories of labor will be discussed in the following sections.
Hormonal
Alteration in systemic or local levels of steroid hormones is an initiating factor of labor in some animals. The understanding of their possible role in human labor has been continuously evolving. The withdrawal of the uterine inhibitor hormone progesterone has been shown to play a major role in many animals (e.g., sheep, rats, rabbits). In sheep, this withdrawal seems to be caused by an increased responsiveness of fetal adrenal cells to adrenocorticotropic hormone (ACTH) that results in increased production of cortisol. Through several steps, cortisol redirects placental steroid biosynthesis and decreases progesterone secretion. The decreased circulating progesterone in the sheep permits increased myometrial gap junction formation, an increase in prostaglandin formation, and increased response of the uterus to agents capable of producing contractions. In this sheep model, fetal ACTH secretion has control of the onset of labor.
Major differences exist, however, between sheep hormonal status and that of primates, including humans. In humans, there is no great increase in cortisol from the fetal adrenal gland before labor, nor has a dramatic decrease in progesterone been consistently demonstrated. Progesterone, however, is important in human pregnancy, and numerous studies have examined the role of the progesterone-to-estrogen ratio before the onset of labor. In 1974, investigators demonstrated a significant fall in serum progesterone levels and a rise in estrogen levels in many women before labor. This finding has not been reproduced consistently. Estriol may be a signal from the fetus indicating that it is mature and ready for delivery. Production of estriol increases during the last month of pregnancy. In the large amounts produced, estriol is as active as estradiol in stimulating uterine growth. There are reports of an elevation in the estradiol/progesterone ratio at the end of pregnancy.
Administration of progesterone has not been demonstrated to delay term or preterm labor in primates. The antiprogesterones—RU-486 or mifepristone and ZK-98299 or onapristone—in humans and other primates can enhance the responsiveness of the uterus and induce cervical change within 12 to 48 hours, again suggesting a role for progesterone in preventing labor onset.
Oxytocin
It is well known that oxytocin produces uterine activity when administered to pregnant women. The role of endogenous oxytocin as an initiator of term or preterm labor is less well defined. Some reasons to suspect that oxytocin is a universal initiator of labor are its ability to induce labor when given exogenously, and the increase in blood levels that accompanies labor in most species. Because of the pulsatile manner of oxytocin release and the difficulty in measuring the hormone, its precise role in humans has been difficult to ascertain. Compared with oxytocin levels in nonlaboring patients, levels appear to be significantly increased during the first stage of labor and increase to a greater amount during the second stage of labor. Oxytocin levels are higher in umbilical artery blood than in umbilical vein or maternal blood. This finding suggests that the fetus is a source of oxytocin production and release during labor. It is clear that the uterus becomes more sensitive to oxytocin in the days preceding labor. The number of myometrial cell membrane oxytocin receptors greatly increases as pregnancy advances, with a further increase during labor itself. In humans as well as in other species, the concentration of oxytocin receptors is a major reason for increased contractility of the uterus. The increase in oxytocin receptors is the result of increased estrogen levels.
Prostaglandins
Another important part of the parturition model is the synthesis and release of prostaglandins E2 and F2. This is supported by an increase in prostaglandins or metabolites in the amniotic fluid, endometrium, decidua, myometrium and blood at the time of labor, the administration of prostaglandins inducing labor, and inhibitors to prostaglandin synthesis delaying labor. It is likely that the prostaglandins have a role in parturition originating from the decidua and myometrium. Oxytocin has the ability to stimulate prostaglandin release through the decidual receptors. In addition, infection of the membranes can release prostaglandins and may be an initiating factor in many cases of preterm labor.
Bacterial by-products may be directly responsible for the stimulation of prostaglandin release in the following ways: Bacterial phospholipase releases the precursor arachidonic acid from the amnion, leading to increased prostaglandin synthesis. Gram-negative organisms may also be able to produce prostaglandins through endotoxin stimulation of the decidua or membranes. Gram-positive organisms may also have prostaglandin-stimulating abilities through peptidoglycans. Phospholipase A2 is contained within the lysosome of the fetal membranes. As phospholipase A2 is released from the lysosome, prostaglandin may be synthesized, resulting in uterine contractions.
Cytokines
Cytokines are substances secreted by the immune system in response to infection. There is recent interest in the role of cytokines and growth factors, (e.g., epidermal growth factor, insulin-like growth factors 1 and 2) as potential initiators of labor. The cytokines interleukin 1 (IL-1), IL-6, and tumor necrosis factor (TNF) stimulate the amnion and decidua to produce prostaglandins and increase at time of labor, while transforming growth factor-β (TGF-β) inhibits prostaglandin production by other cytokines and may have antiprogestin properties. Finally, several different cytokines have been found in the amniotic fluid of patients with preterm labor.
Other Factors
Endothelins are potent vasoconstrictors in the sarafotoxin-like family. Some isoforms of endothelins are potent uterotonics. Although endothelin does not appear to increase at time of labor, uterine sensitivity and endothelin-receptor numbers do increase in the pregnant uterus. There is some decrease of endothelin-1 in the amniotic fluid of patients in labor, but this may be a consequence rather than an initiator of labor. Nitric oxide, produced from L-arginine by the enzyme nitric oxide synthase (NOS), mediates relaxation of vascular smooth muscle. It has been shown in various animal tissues, including human, that the NOS enzyme is decreased in myometrial tissue at term. Thus, nitric oxide may have a role in maintaining a quiescent uterus.
It can be hypothesized that parturition is a development of an estrogen environment. This estrogen environment promotes changes in the maternal pituitary with increased oxytocin synthesis and release. Estrogen may also be acting directly on the placenta and cervix. As the antiestrogen progesterone level decreases, estrogen can act to increase oxytocin receptors, prostaglandin production, and gap junction number and size. As the cervix ripens, the underlying membranes and decidua become exposed to the vaginal bacteria, triggering an inflammatory response with release of cytokines and prostaglandins. At this point, the paracrine events take dominance over the endocrine effects. Some conditions, such as infection, can overwhelm the endocrine phase of parturition.
INFECTION AS A CAUSE OF PRETERM BIRTH
Preterm birth has been linked with symptomatic nongenital infections, such as acute pyelonephritis and pneumonia. In the last 15 years, new information has suggested that subclinical infection may be an important cause of premature labor, especially labors resulting in very early delivery.
The hypothesis linking subclinical infection and premature birth may be summarized as follows: microbes or their products such as endotoxin enter the uterine cavity during pregnancy, most commonly ascending from the lower genital tract. Blood-borne infection from a nongenital focus occurs less commonly. Microbes or their products then interact, most likely with the decidua or possibly with the membranes, producing prostaglandins or directly leading to uterine muscle contraction. This interaction is most likely mediated through a cytokine cascade. As a result, there is cervical dilation, entry of more microbes into the uterus, and continuation of “the viscous cycle” resulting in premature birth.
The first piece of evidence linking subclinical infection to preterm birth is that the prevalence of histologic chorioamnionitis is increased among preterm births. In membranes from preterm deliveries, there is a consistent and very strong association between positive membrane cultures and the likelihood of membrane infiltration. For example, when the birth weight is greater than 3,000 g, the percentage of placentae showing histologic chorioamnionitis is less than 20%; when the birth weight is below 1,500 g, the percentage was fully 60% to 70%. Most cases of histologic chorioamnionitis are caused by infection.
Second, clinically recognized infection is increased in mothers and neonates after preterm birth. This association is also consistent. Sepsis and meningitis are increased three- to ten-fold in preterm infants. Less widely recognized is the increase in maternal infection after preterm birth. These observations suggest that subclinical infection underlies preterm birth and that the infection became clinically evident during or shortly after birth. Alternatively, the preterm infant may be more susceptible to infection that develops after delivery.
Third, there are associations of preterm birth with various maternal lower genital infections or microbes (Table 10.1). Although Ureaplasma urealyticum in the lower genital tract has been associated with low–birth-weight (LBW) infants in earlier studies, a large National Institutes of Health (NIH) study reported no associations of U. urealyticum in the vagina with any adverse pregnancy outcome (preterm birth, PPROM, LBW, or BW <1,500 g). Interestingly, then, U. urealyticum in the lower genital tract is not associated with LBW/preterm pregnancies, even though this organism is one of the most common isolated in the amniotic fluid of women in preterm labor.
Lower genital infection with Chlamydia trachomatis has also not been consistently associated with adverse pregnancy outcome. However, women with active chlamydial infection and with a positive serum antichlamydial immunoglobulin M (IgM) have shown an increase in rates of preterm delivery. Although a consistent association has not been observed between maternal group B streptococci (GBS) colonization and premature birth in several small studies, a large investigation of approximately 13,000 women showed that pregnant women with heavy GBS colonization had a small but significant increase in risk for LBW (odds ratio [OR] = 1.2; 95% confidence interval [CI] = 1.01–1.5). There were no significant increases in other adverse outcomes, including preterm birth, among heavily colonized women. Women with light colonization were not at an increased risk for any adverse outcomes. Results are also contradictory regarding an association between Trichomonas vaginalis and premature birth. Although small, earlier studies had conflicting results, the large Vaginal Infections and Prematurity Study found the presence of T. vaginalis in the vagina at midpregnancy was significantly associated with preterm LBW (7.1% of women with vs. 4.5% without T. vaginalis: OR = 1.6; 95% CI = 1.3–1.9). Considerable data have linked lower genital tract anaerobes with preterm labor. Further, bacterial vaginosis, in which there is a predominance of anaerobes, has been consistently associated with approximately a two- to three-fold increase in spontaneous preterm delivery. Among other infections, untreated pyelonephritis has been associated with a risk of preterm delivery of approximately 30%, and asymptomatic bacteriuria is associated with a 60% higher rate of LBW (95% CI = 1.4–1.9) and a 90% higher rate of preterm delivery (95% CI = 1.3–2.9).
|
|
|
TABLE 10.1. Prenatal infections as a cause of preterm birth (PTB): association and treatment recommendations |
Fourth, positive cultures of the amniotic fluid/membranes/decidua are found in some patients in premature labor. The range of positive amniotic fluid cultures obtained by amniocentesis from asymptomatic women in premature labor is 3% to 24%. When more sensitive testing for detection of bacteria (polymerase chain reaction) is carried out in amniotic fluid from women in preterm labor, bacteria are detected in 30% to 50%. The most widely discussed route of upper genital tract infection in preterm labor is an ascending path through the vagina and cervix. Similarities in organisms isolated from the amniotic fluid and the lower genital tract support this pathogenic route. It is also possible to speculate that bacteria may enter the uterine cavity hematogenously through spread via the placenta, by contamination at the time of instrumentation such as during amniocentesis or chorion villus sampling, or even by spread from the abdominal cavity via the fallopian tubes. Other sources of organisms for hematogenous spread include bacteremia from periodontal disease or procedures. Among women in spontaneous preterm labor with intact membranes, genital mycoplasmas and anaerobic organisms as well as Gardnerella vaginalis (the so-called bacterial vaginosis organisms) are in fact those organisms most commonly found in the amniotic fluid. Sexually transmitted organisms such as Neisseria gonorrhoeae and C. trachomatis are rarely found in the amniotic fluid, and GBS and Escherichia coli are found just occasionally. Patients in preterm labor with the highest likelihood of having a positive culture of the amniotic fluid are those in preterm labor at early gestational ages. It may be speculated that intrauterine infection occurs early in pregnancy (or even has preceded the pregnancy) and may remain without clinical detection for months.
Fifth, biochemical “markers” of infection are often present among women in premature labor. In infection-induced premature labor, the primary site of infection is probably not the amniotic fluid, but the decidua or membranes. More sensitive markers of infection potentially include amniotic fluid glucose concentrations, serum white blood cell counts, C-reactive protein, and amniotic or serum cytokines. Unfortunately, relatively few are clinically useful. Among patients in preterm labor, a low amniotic fluid glucose (<14 mg/dL) correlates well with the likelihood of a positive culture. Among the cytokines, an elevated amniotic fluid IL-6 level is probably the most sensitive marker for infection, but is not yet widely available for clinical use.
Sixth, bacteria or their products induce preterm birth in animal models. The evidence presented here that indicates that infection is a cause of preterm birth in humans is circumstantial. Animal models have provided direct evidence that infection triggers preterm birth in the rabbit, monkey, and mouse.
Seventh, in some clinical circumstances, use of antibiotics has led to a lower rate of preterm birth and to delayed delivery. Antibiotic treatment trials may be classified as one of three designs:
· those conducted prenatally in patients at high risk for preterm delivery
· those conducted among women in preterm labor with intact membranes, as adjuncts to tocolytic therapy
· those conducted among women with PPROM.
Chapter 11 discusses antibiotics in PPROM. Table 10.2 summarizes current practices for use of antibiotics to prevent preterm birth. The discordant results in antibiotic trials raise the question as to why antibiotics have not consistently prevented preterm birth or neonatal morbidity associated with preterm birth. One explanation is that infection is simply not a significant cause of preterm labor, but this seems unlikely in view of all the other evidence. Another explanation is that studies have had too low a power. However, large meta-analyses and the ORACLE trial appear to rule out this possibility. Further, because preterm labor has multiple causes, a true effect of antibiotics may be diluted by those cases of preterm labor not caused by infection. It may also be that only a subset of pregnant women (e.g., perhaps genetically predisposed women) with high cytokine response are at risk for preterm labor after subclinical infection. Another reasonable explanation is that the antibiotics studied in most of the trials were simply the wrong ones (e.g., not including antibiotics with better anaerobic activity) or the antibiotics were given too late or the antibiotic dose or timing were incorrect. It has also been speculated that bacterial lysis as a result of antibiotic therapy may lead to increased exposure to lipopolysaccharide and thus enhance preterm labor. Finally, because infection is more likely to cause very early preterm birth (<32 weeks), trials focusing on women at later gestational ages may not show an effect. For example, the ORACLE I trial enrolled women up to 37 weeks gestation, and only 10% delivered at less than 32 weeks.
|
|
|
TABLE 10.2. Use of antibiotics to prevent preterm birth (PTB) in women with preterm labor and premature rupture of the membranes (PROM) |
EPIDEMIOLOGY OF PRETERM LABOR
Currently, 11.8% of women deliver preterm. The vast majority of preterm deliveries are a result of preterm labor (50%), premature rupture of the membranes (33%), or cervical incompetence. The contributions of preterm labor and premature rupture of the membranes to preterm deliveries vary depending upon a number of factors including socioeconomic status (Fig. 10.2). In a large study from North Carolina, Meis and colleagues found that the most common reason for delivery less than 2,500 g in women who were receiving public assistance was PPROM (34%). In contrast, in women who had private insurance, the most common reason for early delivery was preterm labor (52%). Indicated preterm deliveries accounted for 14% and 18% of preterm deliveries, respectively.
|
|
|
FIG. 10.2. Causes of low birth weight births in public and private patients. (Meis P, Ernest J, Moore M. Causes of low birth weight births in public and private patients. Am J Obstet Gynecol 1987;156:1165–1168, with permission). IND, indicated by maternal–fetal condition; PTL, preterm labor; PPROM, preterm premature rupture of membrane; LBWT, low birth weight. |
Several major and minor risk factors are associated with development of preterm labor and premature rupture of the membranes (Table 10.3, Table 10.4). One of the most obvious and important risk factors for prematurity is a prior history of preterm delivery. To better quantify this relationship, Mercer and associates performed a subgroup analysis of data collected during a large population-based observational study evaluating risk factors for preterm delivery. In this study, gravid women with any prior spontaneous preterm birth had a 2.5-fold increased risk of spontaneous preterm delivery in the current pregnancy. This risk increased to 10.6-fold if the spontaneous preterm birth occurred prior to 28 weeks gestation. Interestingly, women with a history of loss between 13 and 22 weeks gestation had rates of prematurity that were similar to women who did not have this history (10.1% vs. 8.8%, P = .69).
|
|
|
TABLE 10.3. Major preterm labor risk factors |
|
|
|
TABLE 10.4. Minor preterm labor risk factors |
Another major risk factor for preterm labor and birth is multiple gestation. The rate of multiple gestations has increased dramatically over the past 15 years. The increase in twins and higher order multiples is largely a reflection of increased use of ovulation induction and assisted reproductive technologies. Fifty percent of twins deliver prematurely with a mean gestational age at delivery of approximately 35 weeks. As expected, the percent of preterm deliveries increases in proportion to the number of fetuses. Triplets and quadruplets deliver on average at 32 weeks and 30 weeks, respectively. Until researchers develop techniques to perform artificial reproductive technologies that minimize the risk of having high order multiples, then these women will continue to be at significant risk for delivering prematurely and suffering the consequences of preterm birth.
African Americans are 1.6 to 2.5 times more likely to deliver prematurely than Caucasian women of similar age and socioeconomic status. Although African Americans have higher rates of prematurity, the rates of neonatal morbidity are lower in African-American neonates when compared to Caucasians born at similar gestational ages. This suggests that the gestational period may be shorter in African-American women. Low socioeconomic status is also strongly associated with prematurity. It is not clear whether this is related to environment, genetic predisposition, infection or access to medical care.
Table 10.4 also lists a number of “minor” risk factors for preterm labor and delivery. Several of these will be discussed in more detail later in this chapter. In general, the minor risk factors can be broken into two categories: those that are potentially modifiable and those that are not. Many of the minor risk factors are common in pregnancy. Individually their contribution to prematurity is small; however, the risk is compounded by addition of other risk factors. The impact of work on preterm birth remains controversial. Prolonged, physically demanding work does appear to independently increase the risk of prematurity and is potentially modifiable.
PREDICTION OF WOMEN AT RISK FOR PRETERM LABOR
Over the past two decades many researchers have focused on identification of women who are at risk for preterm delivery. Theoretically, identification of asymptomatic women at risk for preterm delivery would allow obstetricians to effectively intervene to prevent preterm delivery or to decrease neonatal morbidity and mortality in preterm neonates. In an American College of Obstetricians and Gynecologists' (ACOG) Practice Bulletin titled Assessment of Risk Factors for Preterm Birth, the authors wrote “the ability to predict whether a women is at risk of preterm delivery has value only if an intervention is available that is likely to improve the outcome.” It is believed that identification of women at risk for preterm birth will be beneficial if it allows women to:
· receive a complete course of antenatal corticosteroids prior to delivery
· if necessary, receive tocolytic agents to maximize the probability that antenatal corticosteroids will be given
· be transported to a level III perinatal center.
Another potential benefit of screening is to identify women at low risk for preterm delivery and thereby avoiding administration of potentially dangerous medications or therapies to these women.
Table 10.5 is a review of “ideal” criteria for a screening test. An ideal screening test should have high sensitivity and positive predictive value as well as high specificity and high negative predictive value. Most screening tests do not meet these requirements and trade off sensitivity for specificity. Depending on the clinical scenario where screening tests are used and the consequences of treatment or no treatment, one must decide which test characteristic to stress. For example, one could argue that given the high morbidity associated with preterm birth, the ideal screening test should have a high sensitivity to allow treatment of the majority of women “at risk” and accept a lower specificity rate. On the other hand, one could argue, as ACOG did, that avoidance of treatment with potentially hazardous drugs is beneficial in women with symptoms who are at “low risk” for delivery, thus stressing the importance of the test's specificity and negative predictive value. The following will review available screening tests.
|
|
|
TABLE 10.5. Criteria for screening tests |
Risk Scoring Systems
Risk scoring systems were promoted heavily in the 1980s to identify women at risk for preterm delivery. The risk scoring systems weigh major and minor risk factors for preterm birth as well as current pregnancy complications (see Table 10.3, Table 10.4). The scoring systems work best in multiparous patients and worst in privately insured nulliparas with singleton gestations. Overall, the sensitivity of the screening tool ranges from 3% to 30% and the positive predictive values from 0% to 20% depending on the population studied. While easy to use to identify women who may have modifiable risk factors for preterm delivery, the scoring systems do not reliably identify women at risk. They should not be used alone to institute interventions that may or may not be warranted.
Contraction Monitoring
Contraction monitoring has also been advocated to identify women at risk for preterm birth. Main and associates, in an inner-city clinic in Philadelphia, had low-risk women wear tocometers while waiting in the clinic to be seen between 28 and 32 weeks gestation. Women with 6 or more uterine contractions per hour were more likely to deliver prematurely than women who did not. Using this cutoff, the sensitivity was 75% and the specificity was 79%. As technology became more advanced, this concept was developed further and home uterine activity monitoring (HUAM) became possible. HUAM, as initially promoted, was a combination of telemetric recording of uterine activity and daily contact with perinatal nurses trained to identify signs and symptoms of early preterm labor. The following assumptions were used to establish a role for HUAM:
Women with preterm uterine activity are more likely to deliver prematurely than women who deliver at term.
Women at risk for preterm labor may be unaware of their contractions, thus they present too far along in established labor for treatment to be effective.
Effective treatment for preterm labor is available.
At least 13 randomized clinical trials have evaluated the role of HUAM. These trials differ dramatically depending on the inclusion and exclusion criteria, the use of adjunctive tocolytic agents, and the primary end points. Despite being “randomized clinical trials”, many of the reports were so severely flawed that they were not included into several meta-analyses on the subject. After review of all of the evidence, both ACOG (HUAM: not recommended') and the U.S. Preventive Services (HUAM: devise not effective) discouraged the use of this expensive and unproven therapy. Additional research may be warranted in specific at-risk subgroups.
Salivary Estriol
Salivary estriol has also been promoted as a tool to identify women at risk for preterm birth. The basis for this theory is that estriol, a fetal product, is increased following activation of the fetal hypothalamic–pituitary–adrenal axis prior to spontaneous preterm birth. The estriol can be measured in maternal salivary secretions. Salivary estriol levels have a diurnal variation that peaks at night. Therefore, samples need to be collected in the morning to improve specificity. Using longitudinal sampling with morning collections, the sensitivity of SalEst is 71% and the specificity 77%. The false-positive rate is unacceptably high at 23%. Currently, there are no commercially available salivary estriol kits. Salivary estriol should be considered only as a research tool with limited, if any, clinical indications for use.
Screening for Bacterial Vaginosis
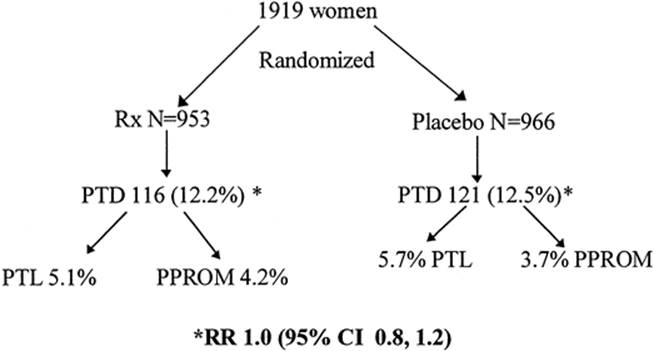
Bacterial vaginosis is a common alteration of normal vaginal flora affecting 10% to 25% of normal women. The majority of infections are asymptomatic. The presence of bacterial vaginosis has been clearly associated with preterm births in both prospective cohort studies and case-control studies. As a result, investigators and clinicians have attempted to eradicate bacterial vaginosis in an effort to reduce the incidence of preterm delivery. Brocklehurst and colleagues evaluated this treatment strategy using meta-analysis. They included five randomized clinical trials. As expected, treatment was highly effective in eradicating bacterial vaginosis (OR = 0.22; 95% CI = 0.17–0.27). The included trials used oral metronidazole, vaginal metronidazole, or vaginal clindamycin. Overall, treatment did not reduce preterm delivery prior to 37 weeks gestation (OR = 0.78; 95% CI = 0.60–1.02), preterm delivery prior to 34 weeks gestation (OR = 0.83; 95% CI = 0.32–2.08), or preterm delivery prior to 32 weeks gestation (OR = 1.51; 95% CI = 0.60–1.61). In a subgroup analysis, no effect was noted with vaginal administration of metronidazole or clindamycin. However, patients with a history of preterm delivery and bacterial vaginosis in the current pregnancy who received active treatment had a significant reduction in preterm delivery rates (OR = 0.37; 95% CI = 0.23–0.60). This meta-analysis has not been updated since the publication of the largest randomized controlled trial to date conducted by the Maternal–Fetal Medicine (MFM)-units network. In this double-blinded, randomized clinical trial, women with bacterial vaginosis were randomized to receive metronidazole 2 g orally for two consecutive days or placebo. Women were re-screened and re-treated, if indicated at 24 to 29 weeks gestation, according to the original treatment assignment. Figure 10.3 summarizes the principal findings of the trial. Overall, there was no reduction in preterm deliveries. This result was confirmed in women who had prior preterm delivery. This study has been widely criticized for using a short course treatment regimen and leaves the question of whether or not it is appropriate to “seek and treat” in high-risk women. In a statement by ACOG, the organization does not endorse routine, universal screening for bacterial vaginosis, but recommends further research on the subject in women with prior preterm delivery.
|
|
|
FIG. 10.3. Metronidazole to prevent preterm delivery in pregnant women with asymptomatic bacterial vaginosis. (Carey J, Klebanoff M, Hauth J, et al. Metronidazole to prevent preterm delivery in pregnant women with asymptomatic bacterial vaginosis. National Institute of Child Health and Human Development Network of Maternal-Fetal Medicine Units. N Engl J Med 2000;8:534–540, with permission.) |
Fetal Fibronectin
Fetal fibronectin has been widely promoted as a tool to identify women at risk for preterm delivery. Fetal fibronectin, a basement membrane protein, is a normal constituent of the extracellular matrix of the maternal–fetal interface. It is present in normal human pregnancies prior to 20 weeks gestation and near term. Its presence between 20 and 34 weeks gestation has been strongly associated with preterm birth, but more importantly, its absence has been associated with low risk of preterm delivery.
Leitich and co-workers performed a comprehensive meta-analysis on the efficacy of fetal fibronectin in identifying women at risk for preterm delivery. They included 27 articles using fetal fibronectin in a variety of settings. Similar to other investigators, they noted that the test's usefulness was a result of its high specificity, and was limited by the low sensitivity in identifying women who would go on to deliver prior to 34 weeks gestation. The sensitivity of the test decreased further in identifying women who would deliver prior to 37 weeks but increased when it was used serially.
In order to maximize fetal fibronectin, its use should be restricted to women with intact membranes, cervical dilation less than 3 cm, and gestational age between 24 and 34 completed weeks gestation, and results should be available within 24 hours. False-positive fetal fibronectins may be obtained in women with recent intercourse or vaginal examinations, or in the presence of bacterial vaginosis and vaginal bleeding.
In general, the sensitivity of fetal fibronectin increases in symptomatic women, women with a cervical length less than 2.5 mm, women with a history of prior preterm delivery, and women with bacterial vaginosis. The negative predictive value in women with preterm contractions ranges from 69% to 92% before 37 weeks gestation. Importantly, a negative fetal fibronectin has a 95% likelihood that delivery will not occur within 14 days of sampling.
Will fetal fibronectin change management and improve outcomes? Fetal fibronectin results have been shown to alter clinical management in certain settings and may be cost-effective. Physicians may use the test to determine who will receive tocolytic therapy and antenatal corticosteroids as well as who is appropriate for a maternal transport. Clearly, this test has potential, yet further work is required to determine what interventions are appropriate and whether the test improves outcomes. An ACOG summary states, “fetal fibronectin may be useful in determining women at high risk for preterm labor. However, their clinical usefulness may rest primarily with their negative predictive value given the lack of proven treatment options to prevent preterm birth.”
Cervical Evaluation
It has long been noted that premature dilation or effacement of the maternal cervix is associated with preterm birth. There has been a great deal of research interest in precisely measuring the uterine cervix with ultrasound to identify women at risk for preterm birth. Several techniques for measuring the cervix have been advocated. In general, it is believed that vaginal measurements are superior to abdominal measurements. Furthermore, several measurements should be obtained and averaged given the variability in cervical lengths for a given individual at a single monitoring session. In order to improve inter-interpreter variability, individuals who are performing the ultrasound should undergo formal training and participate in continuing quality assurance.
Several large prospective cohort studies have been performed which have been useful in establishing cervical nomograms for low-risk and high-risk women. In general, as the cervix becomes progressively shorter or dilates, the risk of preterm delivery increases. Cervical length is also correlated with gestational age (i.e., as gestation advances the cervix matures and shortens). Different cutoff values have been tested. The sensitivity and positive predictive value depend on the prevalence of preterm birth in the population and the gestational age at testing and delivery. A cervical length of ≤30 mm or a dilation of the internal cervical os will identify 80% to 100% of women or 70% to 100% of women who will subsequently have a preterm delivery.
The proponents of cervical ultrasound evaluation stress the benefit in obtaining more precise measurements with vaginal ultrasound than digital evaluation and the improved ability to detect subtle changes. Furthermore, vaginal ultrasound allows one to avoid vaginal examinations. To date, only two published randomized clinical trials have evaluated the use of cervical cerclage in women with premature shortening of the cervix with no evidence of preterm labor. In the first, the cervical incompetence prevention randomized cerclage trial (CIPRACT), women with the following histories were approached:
· a history consistent with cervical incompetence
· PPROM prior to 32 weeks gestation
· history of cold-knife conization
· diethylstilbestrol exposure
· uterine anomaly
Consenting women who met the inclusion criteria and who had a cervical length less than 2.5 cm prior to 27 weeks were randomized to receive a McDonald cerclage and bed rest or bed rest alone. Placement of a cervical cerclage resulted in a significant decrease in preterm delivery prior to 34 weeks gestation (0 of 19 in cerclage group vs. 7 of 16 in the expectant management group, P = .002). The decrease in preterm delivery prior to 34 weeks gestation was also associated with a decrease in composite neonatal outcome (1 of 19 vs. 8 of 16, P = .005). In contrast, Rust et al. randomized women with a shortened cervix detected on routine ultrasound evaluation between 16 and 24 weeks gestation were randomized to receive a cerclage (n = 31) or expectant management (n = 30). The groups were well balanced at randomization for potential confounders. Overall, there was no difference in gestational age at delivery (33.5 ± 6.3 weeks cerclage group vs. 34.7 ± 4.7 weeks in expectant management group, P = .4) or the perinatal death rate (12.9% cerclage group vs. 10.0% in expectant management group, P = .9).
At this time there does not appear to be sufficient evidence to recommend routine ultrasound screening of the uterine cervix since no treatment has been definitively established that will improve neonatal outcome.
Summary of Screening Tests Used to Identify Women at Risk for Preterm Labor
Several screening tests are available to identify women at risk for preterm delivery. All fail to meet the goals of an “ideal screening test”, since no therapy has been proven to be effective in preventing preterm labor and delivery. As a result, these tests should be considered experimental and used as part of randomized clinical trials with sufficient power to evaluate treatments for prevention of preterm birth.
PRETERM LABOR DEFINITION
Preterm labor is defined as labor occurring prior to 37 weeks gestation. Clinically it is difficult to distinguish women with true preterm labor from women who are experiencing preterm uterine contractions. In order to improve the accuracy of the diagnosis, Creasy has proposed using the following criteria: uterine contractions (>4 contractions per 20 minutes) and cervical dilation (≥2 cm in a nullipara and ≥3 cm in a multipara) and cervical effacement (>80%) or uterine contractions and cervical change. Cervical change is the most well-accepted clinical criteria, yet it is the criteria most vulnerable to bias. For example, what constitutes minimal cervical change and over what time period does cervical change need to occur to be acute and warrant intervention? While this definition is more stringent than that proposed by ACOG and others, over 50% of women who fulfill Creasy's criteria will deliver at term with or without treatment. An alternate approach is to await cervical change during a prescribed period of observation. Utter and colleagues defined “minimal” cervical change as dilation of the cervix by at least 1 cm and effacement of at least 1 cm in women less than 3 cm dilated on admission. Is it appropriate to wait for cervical change and will waiting until labor becomes more established affect treatment success? In a retrospective case-control study, Utter et al. compared the outcomes of pregnancies in women who were treated with ritodrine upon admission who had uterine contractions and “minimal” cervical change to women who were observed and treated only when cervical change as defined above was determined. There were no differences in any maternal or neonatal outcomes including the number of days to delivery and “success” rates with tocolysis. Similarly, Guinn and associates randomized women with uterine contractions who were ≤2 cm to one of three therapies: observation alone, subcutaneous terbutaline, or intravenous hydration. Overall, there were no differences in any outcome measures between groups. Approximately 15% of women assigned to each of the groups went on to make cervical change during observation and were treated with parenteral tocolysis. In all cases, parenteral tocolysis was successful in delaying delivery for a minimum of 48 hours to allow treatment with antenatal corticosteroids. This approach avoided administration of tocolytic agents to 85% of women with no increase in morbidity or preterm delivery rates. An alternative strategy to awaiting cervical change is to use the rapid fetal fibronectin test and treat only women with a positive test. However, this strategy remains under investigation.
TREATMENT OF PRETERM LABOR
Once the diagnosis of preterm labor is made what treatments are available and do they work? Several agents have been used as tocolytic agents to suppress uterine activity in hopes that prolongation of pregnancy would improve neonatal outcomes (Table 10.6). The vast majority of placebo-controlled clinical trials were published during the 1970s and 1980s. Most of the placebo-controlled trials were small and the concurrent use of antenatal corticosteroids was low. Overall, women who received any tocolytic agent had a mean time to delivery of approximately 48 hours. Therefore, it is not surprising that tocolytic therapy has not been associated with improvements in neonatal outcomes. Despite this finding, tocolytic agents are widely prescribed throughout the world. The justification for the continued use of unproven drugs is the supposition that had the drugs been administered along with antenatal corticosteroids that the 48 hours gained in utero would be beneficial to the neonate and result in improved outcomes. This theory remains untested. However, given the current “standard of care” in the United States, it is unlikely that placebo-controlled trials will be performed to confirm the need to administer tocolytic agents in addition to antenatal corticosteroids. The individual agents that are commonly used throughout the world will be reviewed subsequently. The absolute and relative contraindications to administering tocolytic therapy are listed in Table 10.7 and Table 10.8.
|
|
|
TABLE 10.6. Overview of the tocolytic agents |
|
|
|
TABLE 10.7. Absolute contraindications to tocolytic therapy |
|
|
|
TABLE 10.8. Relative contraindications to tocolytic therapy |
Beta-Adrenergic Agonists
The β-mimetics are the most widely prescribed and best-studied tocolytic agents. The two most commonly used β-mimetic agents in the United States are ritodrine and terbutaline. There are a number of treatment protocols for both ritodrine and terbutaline. In the acute setting, the medications can be administered intravenously (ritodrine and terbutaline) or subcutaneously (terbutaline). The dose is increased until uterine quiescence is achieved or maternal side effects develop that prevent the provider from increasing the dose further. Development of tachyphylaxis occurs rapidly. As a result it is common to need to increase the dose of the medication to maintain an acontractile state once steady-state levels are achieved.
The maternal side-effect profile with the β-agonists is of particular concern. None of the β-agonists used for tocolysis are completely β-2 selective. Therefore, mothers can experience side effects from both β-2 and β-1-sensitive tissues. The negative β-2 effects include: maternal hypotension, decreased urinary output, increased glucose secretion, hypokalemia, and pulmonary edema. The negative β-1 effects include: tachycardia, palpitations, constipation, decreased gastric emptying, hypokalemia (decrease 0.6 to 1.5 mEq below pretreatment levels), agitation, and jitteriness. The most severe maternal adverse effects include cardiac arrhythmias, myocardial infarction, pulmonary edema, postpartum cardiomyopathy, and death. These risks can be minimized by judicious use of fluids, close monitoring of intake and output, and avoidance of other tocolytic agents.
Beta-mimetics rapidly cross the placenta. The fetal response is similar to the adult. Cardiovascular effects include tachycardia, increased cardiac output and redistribution of blood flow, increased thickness of the intraventricular septum, neonatal supraventricular tachycardia, myocardial ischemia, myocardial necrosis, hydrops, and hypoglycemia. Long-term follow-up studies demonstrated no overall difference in children exposed to β-mimetics versus control groups that received placebo. However, evidence suggests that the β-mimetics may increase the incidence of intraventricular hemorrhage in preterm neonates. This finding has been noted in a couple of case-control studies performed in large neonatal databases. This finding was not previously noted in the randomized placebo-controlled trials of the β-mimetics. Further studies are necessary to evaluate this potential adverse effect of β-mimetics.
Are the β-mimetics efficacious? The largest placebo-controlled trial of the β-mimetics was performed in Canada and published in 1992. In this trial, 708 women with preterm labor, with or without ruptured membranes, were randomized to receive ritodrine or placebo infusions. Treatment with ritodrine did not reduce perinatal mortality or morbidity, prolong pregnancy, decrease the percent of preterm deliveries, or increase the percentage of women who completed a course of antenatal corticosteroids. The findings of this individual trial are consistent with a previously published meta-analysis of the β-mimetics when used as tocolytic agents. The Canadian study has been widely criticized for including women with PPROM. Tocolytics and antenatal corticosteroids do not appear to be as efficacious in the setting of PPROM, thus potentially diluting any positive effect of the ritodrine.
At this time advocates for the use of the β-mimetic believe that the benefit-to-risk ratio is favorable and that prolonging pregnancy may increase the proportion of women who complete a course of antenatal corticosteroids prior to delivery. As newer agents with less potential for maternal and fetal adverse effects become available, the use of the β-mimetics will continue to decrease in the acute setting.
Magnesium Sulfate
Magnesium sulfate is probably the most widely prescribed tocolytic agent used in the United States. Although the exact mechanism of action is unknown, it likely decreases the free calcium ion concentration in the intracellular compartment of the uterine myometrial myosin light chains, which blocks kinase phosphorylation and therefore decreases the electrical potential of the cell. For acute tocolysis, magnesium sulfate is administered intravenously. A number of protocols for loading the patient and maintenance dosing exist. In general, the magnesium “bolus” is administered in doses that range from 4 to 8 g over a period of 20 minutes to 1 hour. Next, a maintenance infusion (2 to 4 g per hour) is started and adjusted until uterine contraction frequency decreases to less than 4 contractions per hour and no further cervical change is occurring. The infusion is stopped after the patient remains acontractile for 12 to 24 hours. In certain clinical situations (advanced dilation at early gestational ages, women who continue to contract despite high doses of magnesium sulfate, etc.) it may be warranted to continue the infusion for 48 hours to allow for administration of a full course of antenatal corticosteroids.
Magnesium sulfate is primarily cleared by the kidneys and is rapidly excreted in the pregnant woman with normal renal function. It is generally accepted that blood levels of 6 to 8 mg per dL of magnesium sulfate are optimal for tocolysis. However, there is a great deal of variation in the biological response to this agent including the level that is required to achieve uterine quiescence and the level associated with toxicity. For example, in one study investigators used a case-control study design and compared women who did and did not respond to magnesium sulfate tocolysis. Overall, there were no significant differences in serum levels of magnesium sulfate in the women who did and did not respond to tocolysis. This finding is similar to that of a randomized controlled trial comparing a high-dose magnesium protocol (8-g load, then 2–4 g per hour) to a low-dose magnesium protocol (4-g load, then 2–4 g per hour). The high-dose protocol did achieve tocolysis more rapidly than the low-dose protocol. However, there was a corresponding increase in maternal side effects with the high-dose protocol. Overall, there was no difference between the protocols with respect to prolongation of pregnancy or a reduction in neonatal morbidity. Finally, many physicians believe it is necessary to wean patients from magnesium sulfate tocolysis. This practice was evaluated in a randomized trial comparing a weaning protocol to immediate withdrawal of magnesium sulfate. Not surprisingly, weaning prolonged labor and delivery stays by approximately 8 hours. Overall, there was no difference in time gained in utero or differences in neonatal outcomes between the two groups. Women who were weaned had significantly higher rates of recurrent labor in the current admission and in the future.
Maternal side effects are common with magnesium sulfate and are presented in Table 10.9. As blood levels of magnesium increase, so does the potential for severe toxicity. Maternal deaths have occurred with magnesium sulfate as a result of respiratory depression and cardiac arrest. In general, these events should be preventable by following the patient's clinical status carefully. This monitoring should include hourly assessments of intake and output, level of deep tendon reflexes, and oxygen saturation using a pulse oximeter. Careful labeling of all medications as well as strict adherence to concentration should reduce the likelihood of an inadvertent bolus of large amounts of magnesium sulfate. In cases of extreme magnesium toxicity, administration of calcium gluconate may be useful to try and reverse the effects of magnesium sulfate.
|
|
|
TABLE 10.9. Maternal side effects related to MgSO4 |
Finally, long-term magnesium exposure has been associated with significant bone loss and fractures. Therefore, women receiving long-term magnesium therapy should receive supplemental calcium.
Magnesium sulfate also has significant fetal and neonatal effects. Magnesium sulfate crosses the placenta and accumulates in the fetus. As a result, it can affect fetal biophysical parameters (primarily fetal breathing activity) and decrease fetal heart rate variability. Neonates born with cord levels of magnesium sulfate greater than 4 mg per 100 mL may show signs of depression including decreased muscle tone, drowsiness, poor respiratory effort, and low Apgar scores. A case of neonatal osteoporosis with associated fractures has been reported in a woman undergoing long-term tocolysis with magnesium sulfate.
Controversy exists over the long-term effects of magnesium sulfate. A number of cohort and case-control studies have suggested that magnesium sulfate exposure at birth may reduce rates of cerebral palsy in preterm infants. The data are compelling enough that several investigators are now testing this hypothesis in randomized trials. The MagNet trial was the first trial published that formally evaluated this hypothesis. The MagNet trial randomized women with preterm labor and intact membranes to receive magnesium sulfate or other tocolytics if ≤4 cm dilated on admission or magnesium sulfate or placebo if more than 4 cm dilated. The trial was stopped at the first planned interim analysis because there were 7 pediatric deaths (n = 46) in the magnesium arm compared to no pediatric deaths (n = 47) in the tocolytic/placebo arm (OR = 15.2; 95% CI = 4.8–25.6). The groups were well balanced at randomization for potential confounders. Thus, there was no obvious explanation for the excess deaths in the magnesium arms of the trial other than magnesium sulfate exposure. The dramatic findings from this small trial have not been previously noted in large neonatal databases or in placebo-controlled trials. Ultimately, we will need to await the results of ongoing trials to either confirm or refute the findings of the MagNet trial.
Is magnesium sulfate efficacious? Only three small placebo-controlled trials have evaluated the efficacy of magnesium sulfate as a tocolytic agent. In the placebo-controlled trials, magnesium sulfate did not significantly prolong pregnancy or decrease neonatal morbidity. However, the majority of trials with magnesium sulfate compare it to the β-mimetic agents. In these larger trials magnesium sulfate does appear to be equally “efficacious” to the β-mimetics in prolonging pregnancy with a superior maternal side-effect profile. As a result, magnesium sulfate is generally used throughout the United States as a first-line tocolytic agent.
Calcium Channel Blockers
The calcium channel blockers are promising tocolytic agents. Calcium channel blockers or calcium antagonists are nonspecific smooth muscle relaxants. They prevent the influx of extracellular calcium ions into the myometrial cell. The effects are not specific to the uterus.
Numerous protocols for nifedipine exist. In general, 10 mg nifedipine is administered orally. If contractions persist the dose can be repeated every 20 minutes for a total of 30 mg in 1 hour. Maternal hypotension is relatively common. If hypotension develops, additional doses of nifedipine must be held. Once contractions decrease, the patient may receive 10 mg every 6 hours of nifedipine orally or receive 30 to 60 mg of the sustained-release nifedipine per day. Nicardipine, a potent uterine relaxant, may be administered as a 40-mg loading dose followed in 2 hours by a 20-mg dose to a maximum dose of 80 mg if uterine contractions do not abate. This can be followed by sustained-release nicardipine 45 mg every 12 hours.
The calcium channel blockers produce vasodilation and decrease peripheral vascular resistance. Maternal hypotension defined as either a 25% decrease in mean arterial pressure or symptomatic hypotension is relatively common. Many patients experience transient facial flushing or develop nausea and headache. Maternal side effects appear to be less common than in women treated with the β-sympathomimetics but severe complications have been reported. For example, there has been a case of maternal myocardial infarction associated with high-dose nifedipine therapy following ritodrine treatment in women in preterm labor. We have had a similar case using a low dose of nifedipine following magnesium sulfate tocolysis. Nifedipine potentiates the toxicity of magnesium sulfate by causing neuromuscular blockade. There have been reports of profound hypotension, neuromuscular blockade, and maternal death resulting from the combination of magnesium sulfate therapy and calcium channel blockers. This complication may not be as frequent as initially believed. However, there are no protocols that establish the safety of using these medications together. Therefore, they should not be used concurrently.
In general, the calcium channel blockers appear to be well tolerated by the fetus and neonate. There has been one case of neonatal heart block associated with their use. Concerns remain that the calcium channel blockers may have adverse effects on the fetal and placental circulation resulting in growth restriction, acidosis, and stillbirths. These concerns do not appear to be supported by the literature.
Prostaglandin Synthetase Inhibitors
Prostaglandins are integrally involved in cervical ripening and labor. Therefore, it would make sense that inhibiting prostaglandin synthesis should prevent preterm labor and delivery. Nonsteroidal antiinflammatory drugs (NSAIDs) inhibit cyclooxygenase, thus preventing the conversion of arachidonic acid to prostaglandin. The effects are not limited to the uterus. Indomethacin is the most widely studied prostaglandin synthetase inhibitor used for treatment of women in preterm labor.
Our protocol for indomethacin tocolysis involves the administration of a 100-mg loading dose given as a suppository per rectum. If regular uterine contractions persist 1 to 2 hours after the initial 100-mg suppository, an additional 50 to 100 mg may be given. Oral therapy is then instituted at 50 mg every 6 hours for 48 hours while betamethasone is dispensed. The absorption of indomethacin is excellent from both the rectal and oral routes. Therefore, if rectal suppositories are not available, the oral formulation can be effectively substituted. Fetal echocardiography is not considered necessary when administering indomethacin as outlined above. Fetal contraindications to the use of indomethacin include growth restriction, renal anomalies, chorioamnionitis, oligohydramnios, ductal dependent cardiac lesions, and twin–twin transfusion syndrome.
Indomethacin is very well tolerated in the gravida in comparison to other tocolytic agents. Serious maternal side-effects are rare when the agent is used in a brief course of tocolysis. As with any NSAID, mild gastrointestinal upset may occur. More serious potential complications include gastrointestinal bleeding, alterations in coagulation, thrombocytopenia, and asthma in aspirin-sensitive patients.
Prolonged treatment can lead to renal injury, especially when nephrotoxic drugs such as aminoglycosides are employed. Drugs of this class are antipyretic agents and may obscure a clinically significant fever. Maternal contraindications to indomethacin include renal or hepatic disease, active peptic ulcer disease, poorly controlled hypertension, asthma, and coagulation disorders.
In contrast to the generally favorable maternal side-effect profile, the potential for fetal and neonatal complications of indomethacin tocolysis is worrisome. In actuality, serious complications are rare when limiting treatment to short courses and adhering to established protocols.
The principal side effects of indomethacin tocolysis have been constriction of the ductus arteriosus, oligohydramnios, and neonatal pulmonary hypertension. The ductal constriction occurs because formation of prostacyclin and prostaglandin E2, which maintain ductal vasodilation, is inhibited by indomethacin. Moise and colleagues reported Doppler evidence of ductal constriction in 7 of 14 fetuses exposed to indomethacin between 27 and 31 weeks of gestation. Tricuspid regurgitation occurred in three fetuses. All ductal abnormalities resolved within 24 hours of discontinuation of indomethacin and none of the neonates had pulmonary hypertension. The Moise group later reported on the effect of advancing gestational age on ductal constriction in association with indomethacin and stated that “a dramatic increase in constriction was noted at 32 weeks gestation when the rate of compromise approached 50%.” However, ductal constriction was noted as early as 24 weeks, and occurred in 11 of the 23 fetuses prior to 30 weeks. This was a retrospective analysis of echocardiograms performed on 44 patients with premature labor or hydramnios treated with indomethacin. Although never clearly stated, these patients appeared to be on courses of therapy for greater than 48 hours. Indomethacin was the “third-line agent” in premature labor unresponsive to terbutaline or magnesium sulfate.
Oligohydramnios associated with indomethacin tocolysis is common, dose-related, and reversible. The oligohydramnios is a consequence of reduced fetal urine production due in turn to reduction by indomethacin of the normal prostaglandin inhibition of antidiuretic hormone and by direct effects on the renal blood flow. Indomethacin can be an effective therapy for hydramnios, especially when complicated by preterm labor.
Primary pulmonary hypertension in the neonate is a serious condition that has also been reported with prolonged (more than 48 hours) indomethacin therapy. This complication has not been reported when therapy was restricted to 24 to 48 hours, however, the incidence may be as high as 5% to 10% with long-term therapy.
Necrotizing enterocolitis and intraventricular hemorrhage have been observed in the LBW neonate exposed to indomethacin in utero when it was used outside of standardized protocols that did not limit the duration of treatment, or was the second or third agent added to recalcitrant preterm labor. Since such patients have an increased risk of subclinical intraamniotic infection, and since intraamniotic infection is associated with a greater risk of such complications, it is not clear that indomethacin incurs independent risk for these morbidities. Subsequently, two larger studies have not confirmed this finding or demonstrated any association between indomethacin exposure and any adverse neonatal outcome. Follow-up studies of children treated in utero with indomethacin have not found significant long-term effects although they did not specifically target the LBW neonate.
Indomethacin has been reported to be effective in two small randomized, placebo-controlled trials. The first found indomethacin was superior to placebo in delaying delivery for 48 hours (80% vs. 33%). The second demonstrated a sustained delay in delivery for patients treated with indomethacin (95% at 48 hours and 83% at 7 days) compared with placebo (23% at 48 hours and 16% at 7 days). Additional prospective, randomized trials have found indomethacin to be comparable to ritodrine and magnesium sulfate and superior to nylidrin for tocolysis. There are additional reports that describe indomethacin tocolysis favorably, but many used other tocolytic agents simultaneously or sequentially.
Indomethacin appears to be an effective tocolytic agent that is well tolerated by the mother, and appears to be tolerated by the fetus when used appropriately. Exposure should be limited to 48 consecutive hours to allow for administration of antenatal corticosteroids and should be restricted to gestational ages less than 32 weeks.
Other Tocolytic Agents
Several other tocolytic agents have been proposed for use. These include the oxytocin analogs, nitroglycerin, cyclooxygenase 2 (COX-2) inhibitors, ketorolac, progestins, and nitric-oxide inhibitors. The oxytocin analogs have been the most widely tested. These agents appear promising in delaying delivery and have acceptable maternal side-effect profiles. However, use of these agents did not appear to improve neonatal outcome. Therefore, the Food and Drug Administration (FDA) did not approve Antosiban for use in women with preterm labor. As a result of the failure to bring an “effective” drug to market, it is doubtful that any of the pharmaceutical companies will invest the capital necessary to develop new tocolytic agents in the near future.
MAINTENANCE TOCOLYIS FOLLOWING ARREST OF PRETERM LABOR
If preterm labor is arrested, the patient remains at high risk for a recurrent episode of preterm labor and preterm birth. Maintenance tocolytic therapy may decrease chances for delivery in some cases. Several agents including the β-mimetics (ritodrine and terbutaline), magnesium sulfate, prostaglandin synthetase inhibitors, and the calcium channel blockers have been tested in randomized trials.
Efficacy of Oral Tocolysis with Beta-Mimetics
We have been able to identify eight randomized placebo-controlled trials of oral β-mimetic maintenance therapy to prevent recurrent preterm labor and preterm delivery. A total of 915 patients were randomized in these eight trials. In six of the eight trials there was no decrease in the preterm delivery rate or a prolongation of pregnancy with maintenance tocolytic therapy when compared to controls receiving no treatment. Seven of the eight trials reported on the number of women treated for recurrent preterm labor. Overall, for women receiving a β-mimetic, the rate of recurrent preterm labor was 32.5% (range, 2%–59%) and for patients receiving placebo or no therapy 28.3% (range, 12.9%–63%). Despite obvious differences in the trials, Sanchez-Ramos and colleagues combined these data using meta-analysis (Table 10.10). When they restricted the analysis to trials comparing β-mimetics to placebo or no therapy, there was no benefit of treatment for prevention of preterm birth (OR = 1.08; 95% CI = 0.82–1.43) or risk of recurrent preterm labor (OR = 0.90; 95% CI = 0.63–1.28). One could argue that it is not appropriate to combine trials when there is no consistency between the trials in inclusion criteria and definitions of preterm labor and recurrent preterm labor. Regardless, whether the trials are evaluated individually, cumulatively as a review, or using meta-analysis, there does not appear to be any benefit of oral β-mimetic tocolysis.
|
|
|
TABLE 10.10. Impact of maintenance tocolysis on preterm delivery |
Several potential explanations can be offered as to why oral β-mimetic therapy appears to be ineffective. Oral administration of terbutaline results in inconstant drug levels, characterized by peaks and troughs. The need to take the drug every 2 to 4 hours throughout the day, including awakening at regular intervals throughout the night, may decrease compliance. Finally, long-term exposure to β-mimetic agents results in desensitization of the β-adrenergic receptors in the myometrium. Development of tolerance is related to both the duration of therapy and the total dose of the β-mimetics. As a result the drugs may lose effectiveness over time.
Efficacy of Continuous Subcutaneous Administration of Terbutaline
Terbutaline may be administered by a continuous portable subcutaneous pump for maintenance therapy. Its theoretical advantages over oral maintenance therapy are continuous low maintenance drug levels and the ability to bolus the drug if uterine contractions develop, thus preventing or decreasing the development of tolerance of the β-receptors to the β-agonist terbutaline.
A number of descriptive studies of terbutaline pump therapy for prevention of preterm birth have been published in peer review journals. It was not until 1997 that the first randomized, placebo-controlled trial of the terbutaline pump was published. In this study women with preterm labor were assigned to receive terbutaline pump therapy (n = 15), placebo pump therapy (n = 12), or oral terbutaline (n = 15). If women developed recurrent preterm labor, the blind was broken and women receiving placebo were crossed-over to terbutaline. Although conclusions were limited by the small number of patients in each group and the crossover design, there were no differences in the mean delay to delivery or in neonatal morbidity.
In 1998, Guinn and associates reported their randomized double-blind trial of terbutaline pump therapy. Preterm labor was defined prospectively as the presence of uterine contractions and ≥1 cm cervical dilation, ≥80% effacement or cervical change. Women received magnesium sulfate with or without indomethacin therapy for acute preterm labor. Women with singleton gestations and intact membranes between 22 and 336/7 weeks gestation were eligible. Consenting women were randomized to receive terbutaline pump (n = 24) or placebo pump therapy (n = 28). Pump therapy was initiated by the research nurse using a standard protocol. In addition to their programmed infusion, patients were allowed to administer up to two additional boluses (either 0.25 mg terbutaline or 0.25 cc saline depending on the treatment group) for uterine contractions. At randomization, the groups were well balanced with respect to parity, prior preterm delivery, gestational age, and cervical examination. Overall there was a 1-day difference in mean time to delivery between the groups (terbutaline 29 days and placebo 28 days, P = .78). There were no differences in the rates of preterm delivery at less than 34 and less than 37 weeks gestation, recurrent preterm labor (terbutaline 38% and placebo 37%, P = .89), or rates of neonatal morbidity.
Despite very limited information regarding terbutaline pump therapy, its use has been widely promoted by several home health care corporations that target the majority of their services to the obstetric patient. Terbutaline pump therapy whether used alone or in conjunction with HUAM programs is extremely expensive, averaging over $200 per day, when compared to oral therapy or no therapy. As its use has increased, so have reports of complications related to therapy. As a result, the FDA issued an alert regarding the potential dangers associated with terbutaline pump therapy and the lack of data supporting the efficacy of this treatment.
Risks Associated with Oral or Subcutaneous Beta-Mimetic Therapy
Frequent unwanted effects of β-mimetic therapy include palpitations, tremor, nausea, vomiting, headache, thirst, nervousness, and restlessness. Complications of the oral β-mimetics and the subcutaneous administration of terbutaline include sudden death, pulmonary edema, cardiac arrhythmias, hepatitis, glucose intolerance, and gestational diabetes. There has also been one case of neonatal myocardial necrosis in a woman receiving high doses of subcutaneous terbutaline.
Summary of Beta-Mimetics for Maintenance Therapy
There is no compelling evidence from the randomized controlled trials to support the use of β-mimetics for maintenance therapy. Given the potential risks associated with the β-mimetics, there is no justification for its continued use as a chronically administered therapy.
Other Maintenance Tocolytic Agents
Compared to the β-mimetics, there have been relatively few trials exploring options for maintenance therapy. Magnesium sulfate has been administered on a chronic basis intravenously and orally. Long-term magnesium exposure can result in significant osteopenia, especially when used in conjunction with multiple doses of corticosteroids and bed rest. There have been reports of both mothers and neonates developing significant osteopenia following prolonged magnesium exposure. In the randomized trials that compare oral magnesium to placebo, no apparent benefits were noted in time to delivery or neonatal outcomes.
Long-term tocolysis with the prostaglandin synthetase inhibitors is contraindicated. The fetal risk is far in excess of any potential benefits. It is possible that more selective COX-2 inhibitors will be useful for maintenance therapy. The calcium channel blockers appear to be gaining popularity to reduce recurrent preterm labor. Two trials have compared nifedipine to β-sympathomimetics agents. These investigations were equivalent or superior to the β-mimetics for prolonging pregnancy, with lessened maternal side effects. Carr and colleagues published the only randomized trial of nifedipine compared to no therapy. They randomized 74 women to receive oral nifedipine (20 mg every 4 to 6 hours) or no treatment. The groups were well balanced at randomization for potential confounders. There were no differences in the time gained from initiation of therapy until delivery in the two groups (37 days nifedipine and 32 days no therapy) or gestational age at delivery (35.4 weeks nifedipine and 35.3 weeks no therapy). Oral nifedipine following successful tocolysis with magnesium sulfate did not improve pregnancy outcome. While this study did not report any significant complications of therapy, there has been a report of a myocardial infarction following treatment with nifedipine for maintenance tocolysis.
Conclusions Regarding Maintenance Tocolysis
At this time there is no evidence that any of the available maintenance tocolytic agents are effective in prolonging gestation, reducing preterm births, or improving neonatal outcome. Each of the therapies has been associated with significant complications. Therefore, we cannot recommend that any of these agents be used outside of properly designed randomized trials.
ANCILLARY THERAPY FOR WOMEN IN PRETERM LABOR
Several investigators have studied the impact of adjunctive antibiotic therapy in women with preterm labor and intact membranes. These studies have included women across the spectrum of gestational ages and cervical dilations and have used a variety of antibiotic regimens. This subject was reviewed by King and Flenady in the Cochrane Database. Beneficial effects of antibiotics included a significant prolongation of pregnancy (5.4 days), reduction in maternal infectious morbidity, and a trend toward reduction in neonatal sepsis. However, this was coupled with an increase in perinatal mortality (OR = 3.36; 95% CI = 1.21–9.32). The largest study published to date was ORACLE II. This study included women in preterm labor between 20 and 37 weeks gestation. In this trial, 6,295 women were enrolled, and data from 6,241 women was available for analysis. Overall, use of antibiotics was not associated with a reduction in neonatal morbidity or mortality or prolongation of pregnancy. The only exception was decreased use of postpartum antibiotic prescription in women who had received antibiotics. Based on the results of this trial and the Cochrane Database review, at this time, adjunctive antibiotic therapy for women in preterm labor is not indicated. GBS prophylaxis should be administered following the 2002 Centers for Disease Control and Prevention (CDC)/ACOG guidelines.
Hydration therapy, either oral or intravenously, is widely used as adjunctive therapy for women with preterm contractions and preterm labor. This practice was popularized during the 1980s when the β-mimetics were being widely prescribed. Prior to administration of the β-mimetics, women were hydrated to prevent hypotension. In many cases, as women were receiving their hydration therapy, their contractions reduced in frequency, thus obviating the need for parenteral tocolysis. Guinn and associates published a randomized trial comparing two commonly used therapies for preterm contractions to observation only. Women were included who had cervical dilation less than 2 cm, effacement less than 80%, gestational age 24 to 33 completed weeks gestation, and regular uterine contractions. Women were randomly assigned to receive intravenous hydration, one dose of subcutaneous terbutaline (0.25 mg), or observation only. There were no differences between the groups with time gained in utero, the proportion of women who delivered preterm, or the proportion of women who developed cervical change and received parenteral treatment with tocolytic agents. Intravenous hydration was associated with the highest hospital costs and charges and has the highest potential for adverse effects. Intravenous hydration should be reserved only for women who are obviously dehydrated.
Bed rest has also been widely prescribed for women in preterm labor. There is little if any data that suggests that bed rest is efficacious in women with threatened preterm labor or arrested preterm labor. There are significant costs associated with bed rest including hospital days, lost wages, and lost domestic productivity. It should not be routinely prescribed to women at risk for preterm labor or delivery.
Two therapies are extremely beneficial to women with preterm labor. The first is antenatal corticosteroids. There have been 15 randomized, placebo-controlled trials that tested the efficacy of antenatal corticosteroids in women at risk for preterm birth. Exposure to a complete course of antenatal corticosteroids (betamethasone 12 mg i.m. q24h ×2 doses or dexamethasone 6 mg i.m. q12h ×4 doses) significantly improves neonatal outcomes including a reduction in respiratory distress syndrome, intraventricular hemorrhage, and death. The data are so compelling that the ACOG and the NIH recommend that all women at risk for preterm birth prior to 34 weeks gestation receive antenatal corticosteroids. Repeat courses of antenatal corticosteroids are not recommended as they may reduce respiratory morbidity while increasing the potential for intraventricular hemorrhage and chorioamnionitis. Long-term follow-up studies are underway which will help to define the long-term risks and benefits of repeat courses of antenatal corticosteroids.
The other therapy that appears to be highly efficacious in improving neonatal outcomes is the administration of GBS prophylaxis to women at risk for preterm birth. The attack rates for preterm neonates colonized with GBS are significantly higher than in term infants. As a result, prophylaxis has been demonstrated to be highly beneficial in preventing invasive GBS and its sequelae in preterm neonates.
CONCLUSIONS
Prevention of preterm birth remains an elusive goal. Despite widespread recognition and interest in the problem, the rate of preterm delivery is increasing in the United States. Clearly continued research efforts are necessary to better elucidate the biology of parturition and abnormal parturition to allow us to develop more effective therapies. In the mean time, it is premature to incorporate screening tests to identify women at risk for preterm labor outside of randomized treatment trials since no treatment has been proven to prevent preterm delivery. In women with an acute episode of preterm labor, tocolysis can be administered with antenatal corticosteroids. All of the tocolytic agents are potentially dangerous and should be used with caution in a supervised setting. Currently, there is no data to support the use of maintenance tocolysis in women whose preterm labor is successfully arrested. All women in spontaneous preterm labor should receive a single course of antenatal corticosteroids and GBS prophylaxis following the 2002 CDC/ACOG guidelines.
SUMMARY POINTS
· The rate of preterm birth is increasing in the United States.
· Subclinical infection is an important cause of preterm labor and delivery.
· Risk factor screening misses the majority of women who deliver preterm.
· Fibronectin and vaginal ultrasound of the cervix are promising technologies to identify women at low and high risk for preterm delivery.
· Universal screening for bacterial vaginosis is not warranted.
· Management of women with asymptomatic shortening of the uterine cervix is controversial.
· The diagnosis of preterm labor should be made using objective and reproducible criteria to avoid over and under treatment of women at risk for delivery.
· Tocolytic therapy has not been associated with improvements in neonatal outcome.
· All tocolytic agents have the potential to adversely affect the mother and the neonate and should only be administered in a supervised setting.
· Currently, there is no data to support the use of maintenance tocolytic therapy.
· Tocolytic therapy should not be administered without concurrent administration of antenatal corticosteroids.
· Weekly courses of antenatal corticosteroids should not be routinely prescribed.
SUGGESTED READINGS
American College of Obstetricians and Gynecologists. Assessment of risk factors for preterm birth. ACOG Practice Bulletin No. 31, 2001.
Althuisius S, Dekker G, Hummel P, et al. Final results of the Cervical Incompetence Prevention Randomized Cerclage Trial (CIPRACT): therapeutic cerclage with bed rest versus bed rest alone. Am J Obstet Gynecol 2001;185:1106–1112.
Brocklehurst P, Hannah M, McDonald H. Interventions for treating bacterial vaginosis in pregnancy. Cochrane Database of Systematic Reviews 2002;1:28.
Carey J, Klebanoff M, Hauth J, et al. Metronidazole to prevent preterm delivery in pregnant women with asymptomatic bacterial vaginosis. National Institute of Child Health and Human Development Network of Maternal-Fetal Medicine Units. N Engl J Med 2000;8:534–540.
Carr D, Clark A, Kernek K, et al. Maintenance oral nifedipine for preterm labor: a randomized clinical trial. Am J Obstet Gynecol 1999;181:822–827.
Creasy R. Preterm birth prevention: where are we? Am J Obstet Gynecol 1993;168:1223–1230.
Group TCPLI. Treatment of preterm labor with the beta-adrenergic agonist ritodrine. N Engl J Med 1992;327:308–312.
Guinn D, Goepfert A, Owen J, et al. Management options in women with preterm uterine contractions: a randomized clinical trial. Am J Obstet Gynecol1997;177:814–818.
Guinn D, Goepfert A, Owen J, et al. Terbutaline pump maintenance therapy for prevention of preterm delivery: a double-blind trial. Am J Obstet Gynecol1998;179:874–878.
Guinn D, Atkinson M, Sullivan L, et al. Single versus weekly courses of antenatal corticosteroids for women at risk for preterm delivery: a multicenter randomized controlled trial. JAMA 2001;286:1581–1587.
Kenyon S, Taylor D, Tarnow-Mordi W. Broad-spectrum antibiotics for preterm, prelabour rupture of fetal membranes: the ORACLE II randomized trial. Lancet2001;357:979–988.
King J, Flenady V. Prophylactic antibiotics for inhibiting preterm labor with intact membranes. Cochrane Database of Systematic Reviews 2003;1.
Klebanoff M, Regan J, Rao A, et al. Outcome of the Vaginal Infections and Prematurity Study: results of a clinical trail of erythromycin among pregnant women colonized with group B streptococci. Am J Obstet Gynecol 1995;5:1540–1545.
Leitich H, Ergarter C, Kaider A, et al. Cervicovaginal fetal fibronectin as a marker for preterm delivery: a meta-analysis. Am J Obstet Gynecol1999;180:1169–1176.
Lewis D, Bergstedt S, Edwards M, et al. Successful magnesium sulfate tocolysis: is “weaning” the drug necessary? Am J Obstet Gynecol 1997;177:742–745.
Main D, Katz M, Chiu G, et al. Intermittent weekly contraction monitoring to predict preterm labor in low-risk women: a blinded study. Obstet Gynecol1988;75:757–761.
Meis P, Ernest J, Moore M. Causes of low birth weight births in public and private patients. Am J Obstet Gynecol 1987;156:1165–1168.
Mercer B, Goldenberg R, Moawad A, et al. The preterm prediction study: effect of gestational age and cause of preterm birth on subsequent obstetric outcome. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Am J Obstet Gynecol 1999;181:1216–1221.
Mittendorf R, Covert R, Boman J, et al. Is tocolytic magnesium sulphate associated with increased total pediatric mortality. Lancet 1997;250:1517–1518.
Moise KJ, Huhta JC, Sharif DS. Indomethacin in the treatment of premature labor: effects on the fetal ductus arteriosus. N Engl J Med 1988;319:327–331.
National Institutes of Health Consensus Development Conference Statement. Effects of corticosteroid for fetal maturation on perinatal outcomes. Am J Obstet Gynecol 1996;173:246–252.
Rust O, Jones K, Benham B, et al. A randomized trial of cerclage versus no cerclage among patients with ultrasonographically detected second-trimester preterm dilatation of the internal os. Am J Obstet Gynecol 2000;183:830–835.
Sanchez-Ramos L, Kaunitz A, et al. Efficacy of maintenance therapy after acute tocolysis: A meta-analysis. Am J Obstet Gynecol 1999;181:484–490.
Utter G, Dooley S, Tamura R, et al. Awaiting cervical change for the diagnosis of preterm labor does not compromise the efficacy of ritodrine tocolysis. Am J Obstet Gynecol 1990;163:882–886.