Donald J. Dudley
From 1970 to 1990, the cesarean delivery rate in the United States increased from 5% to 25%. The four primary indications for cesarean delivery include dystocia, elective repeat cesarean delivery, fetal distress, and abnormal fetal presentation. Dystocia, translated, means “difficult birth” and includes all abnormalities that may occur in women during labor. Although the incidence of cesarean delivery in the United States has recently equilibrated at between 20% and 25%, it is generally accepted that this number of abdominal deliveries remains excessively high. Perhaps one reason for the continued high rate of cesarean delivery is a poor understanding of the labor process and the lack of an organized approach to the management of labor. This fundamental lack of understanding often leads to unnecessary induction of labor, which has an a priori risk of cesarean delivery of at least 25%, or to inadequate augmentation of abnormal labor. With fewer inductions of labor and better augmentation of labor, one can expect a decline in the cesarean delivery rate.
Efforts at reducing the cesarean delivery rate have more recently focused on the categories of dystocia and repeat cesarean section. Obviously, the best method to decrease the incidence of repeat cesarean deliveries is not to do one initially. Hence, new efforts are being directed at the diagnosis and management of labor abnormalities in term pregnancies. The purpose of this chapter is to review these labor abnormalities and management options.
KEYS TO THE MANAGEMENT OF NORMAL LABOR
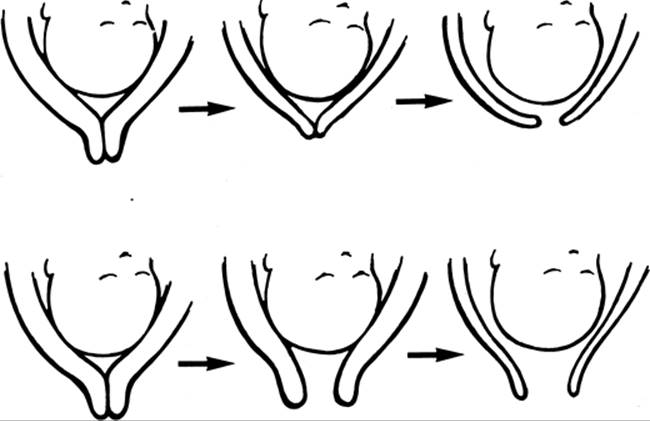
A thorough examination of the management of labor and delivery is available in a comprehensive text edited by Creasy, and the normal labor process is reviewed in Chapter 2 of this text. There are several key points in the management of labor (Table 22.1). The first is that normal labor progresses in a predictable fashion after the diagnosis of labor is made. However, diagnosing labor is more difficult than one might believe. If the diagnosis of labor is made in error, all subsequent actions are incorrect, as one is essentially performing an induction of labor and different management is required. Labor in its simplest terms is defined as cervical change effected by regular, painful uterine contractions. In nulliparous women in their first labor, cervical change is usually manifest by cervical effacement, or thinning, followed by cervical dilation (Fig. 22.1). Conversely, in multiparous women, the initial stage of labor is often characterized by cervical dilation followed by effacement.
|
|
|
TABLE 22.1. Keys to the management of labor |
|
|
|
FIG. 22.1. Cervical effacement and dilation: nulliparas versus multiparas. The upper portion of the figure depicts the cervical changes in early labor of the nulliparous woman. Note that cervical effacement precedes significant dilation. The lower portion depicts the cervical changes of the multiparous woman in early labor. Significant cervical dilation may precede achievement of complete cervical effacement. |
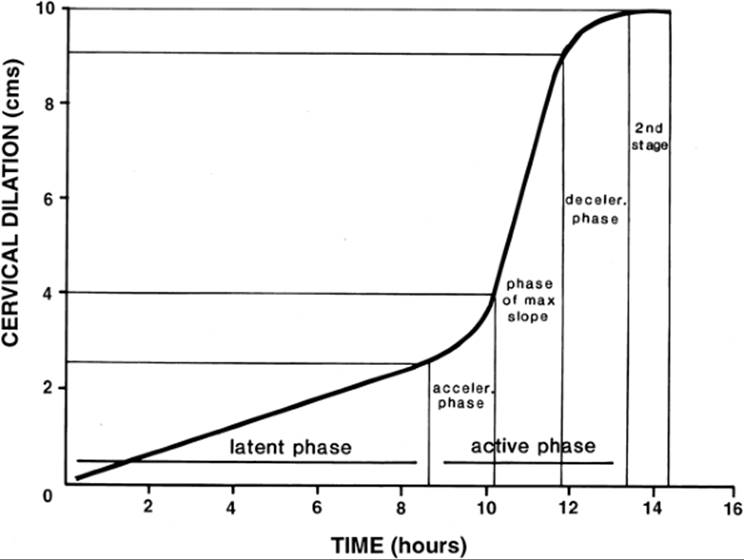
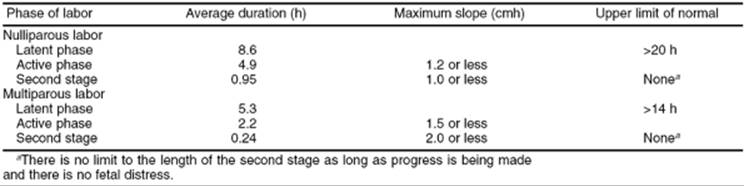
The normal labor curve as defined by Friedman is shown in Figure 22.2. This curve was developed by Emanuel Friedman based on the observation of several thousand laboring women. The first stage of labor is divided into the acceleration phase, active phase, and deceleration phase. The acceleration phase occurs when the active phase of labor starts. The cervix is usually effaced and dilated less than 4 cm. In the active phase, one can anticipate a minimum of 1 cm of dilation per hour (Table 22.2).
The deceleration phase likely is an aberration of the mathematic analysis of Friedman's original data, and as such is likely not a physiologic event. In the second stage of labor, from complete dilation until delivery, one can again anticipate the laboring woman gaining a minimum of 1 cm of station of the fetal head in relation to the maternal pelvis per hour. Cervical examinations should be performed periodically to confirm that progress is being made. Experienced obstetricians often will perform examinations every 2 to 3 hours, depending on the presentation of the patient. After each examination, the progress of labor should be documented graphically on some form of a labor curve, and a plan formulated with regard to future examinations and potential interventions.
|
|
|
FIG. 22.2. The Friedman labor curve. This figure depicts the normal labor curve developed by Emanuel Friedman. Note the different phases of the first stage of labor, including the latent phase, acceleration phase, active phase, and deceleration phase. (Adapted from Friedman EA. Labor: clinical evaluation and management, second ed. New York: Appleton, 1978.) |
|
|
|
TABLE 22.2. Expected length of different phases of labora |
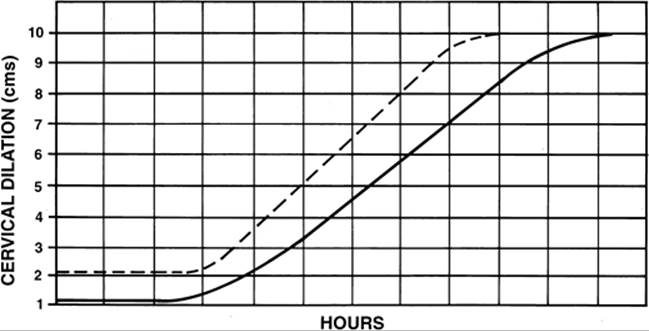
Nulliparous women and multiparous women experience fundamental differences in labor. Figure 22.3 is an example of a labor curve showing the difference in labor patterns expected between nulliparas and multiparas. Labor is the force of uterine contractions overcoming the resistance of the female reproductive tract, including the lower uterine segment, cervix, vagina, and perineum. In nulliparous women, more uterine force is required to overcome resistance in the reproductive tract and the uterus tends to be less effective in maintaining effective uterine contractions. In multiparous women less uterine force is required and the tissues of the reproductive outlet, having been stretched by the previous delivery, have less resistance. As a result, the myometrium of the multipara usually maintains effective contractile activity. Thus, nulliparous women are more likely to develop labor abnormalities that require intervention. Multiparous women usually labor quickly and meet all expected milestones without the need for significant intervention.
|
|
|
FIG. 22.3. Labor curve of nulliparas versus multiparas. Note that different labor slopes are expected between nulliparous (solid line) and multiparous women (dotted line). |
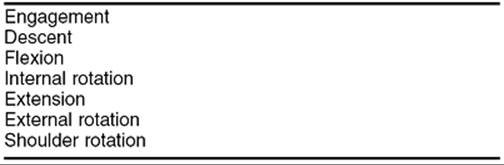
In addition to graphically depicting labor progress, the practitioner should pay close attention to the cardinal movements of labor (Table 22.3). This term refers to the changes that occur in the flexion and position of the fetal head throughout labor. The cardinal movements of labor usually occur in the following sequence: engagement of the fetal head, descent of the fetal head, flexion of the fetal head, internal rotation (assumption of an occiput anterior position), extension (as the fetal head progresses through the birth canal and crowns at the perineum), external rotation (or restitution to the transverse position), and then shoulder rotation after the head has delivered. Abnormalities in the cardinal movements of labor may be reflected by abnormal fetal head position and other specific abnormalities discussed subsequently.
|
|
|
TABLE 22.3. The cardinal movements of labor |
If labor is progressing appropriately a noninterventional approach is indicated, providing for maternal comfort and encouragement. However, if these landmarks are not achieved by the woman in labor, then timely intervention is recommended. Thus, the next important key in the management of labor is prompt intervention when labor progress is inadequate. Ineffective uterine contractions lead to increased tissue acid content in the myometrium, which further contributes to poor contractility. The longer labor continues in a dysfunctional pattern, the less likely the underlying problem can be corrected with medical therapy. Prompt medical therapy for desultory labor is another important key to success in the management of labor.
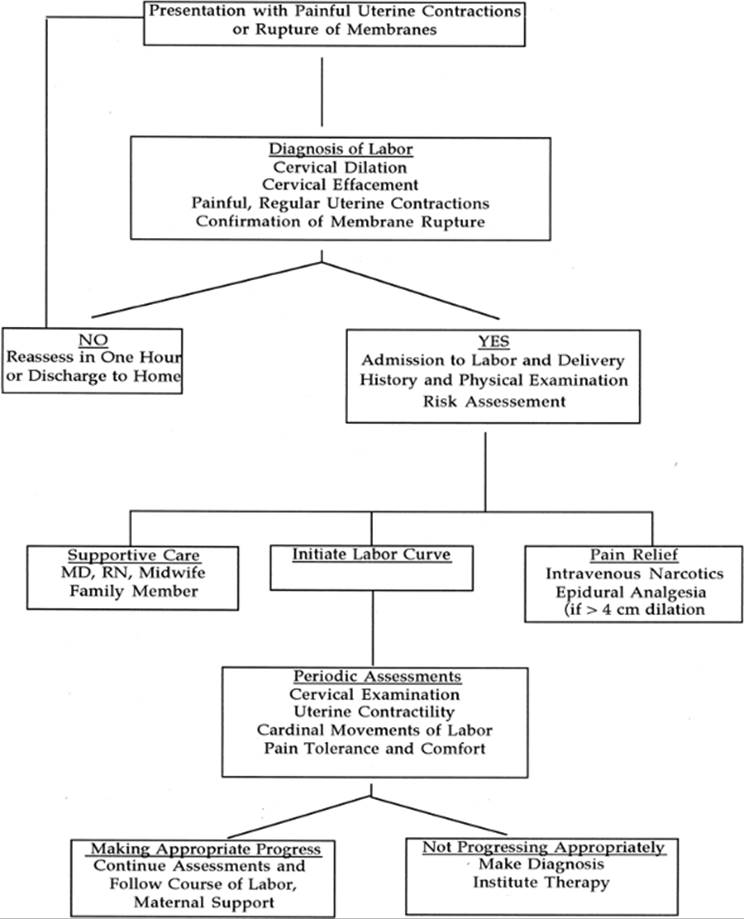
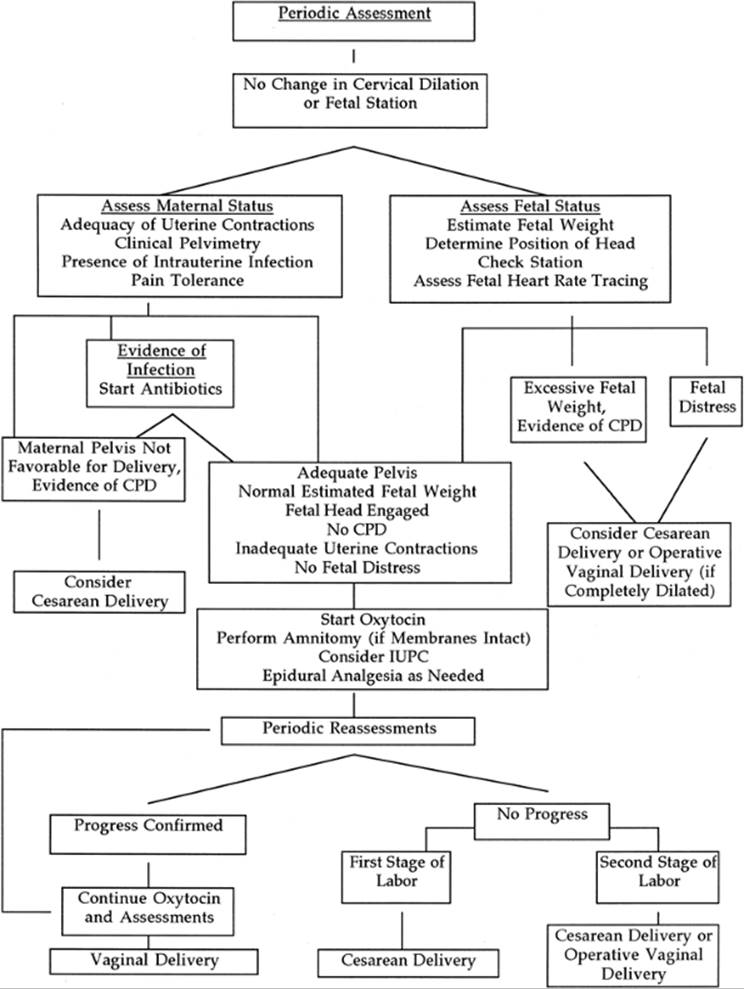
A schematic employing these key components of labor management is shown in Figure 22.4. Normal labor is characterized by coordinated uterine contractions, cervical dilation, gain in station of the fetal head, and normal progress in the cardinal movements of labor. With careful attention to achieving these milestones of normal labor, a successful vaginal delivery is likely. However, should the parturient not achieve these milestones, prompt intervention is more likely to increase the chances for vaginal delivery. Although an aggressive approach with regard to diagnosing labor abnormalities may enhance maternal and fetal outcome, the last important key to the successful management of labor is to use clinical judgment on when to abandon medical therapy in favor of surgical management. If the judgment is made that continuing medical therapy may compromise either mother or fetus, then prompt surgical delivery (cesarean or operative vaginal delivery) should be considered.
|
|
|
FIG. 22.4. Keys to the management of labor. This schematic depicts how the keys to the management of labor can be used to help ensure good maternal and fetal outcomes. |
EPIDEMIOLOGY OF DYSTOCIA
The precise incidence of dystocia is difficult to determine and varies with different populations and different labor and delivery units based on local practice patterns. According to the National Center for Health Statistics, 28% of women who delivered in the United States in 2000 were diagnosed with labor abnormalities, with a primary cesarean delivery rate of 16.1%. Dystocia is more common in nulliparous women than in multiparous women and is more common in the first stage of labor than in the second stage of labor. Labor abnormalities occur in approximately 25% to 30% of nulliparous women and 10% to 15% of multiparous women. Dystocia occurs in the second stage of labor in about 5% to 10% of nulliparous women and is relatively rare in multiparas (<2%).
Abnormal labor is a common indication for cesarean delivery. In the United States in 2000, 22.9% of pregnancies were delivered by cesarean (National Center of Health Statistics), down from the highest incidence of 25% in 1988, but slightly higher than the 20.6% rate in 1996. In 1990, the overall rate was 23.7%, with 7.1% for the indication of “failure to progress” or dystocia and 8.5% for a repeat procedure. Other indications included abnormal presentation (2.6%), fetal distress (2.3%), and other problems (3.2%). Improved management of labor with a decrease in the number of cesarean deliveries for dystocia (and then having less need for repeat procedures) should be the goal of every labor and delivery unit in the United States. While there have been many proposed targets for the overall rate of cesarean delivery, none of these figures are based on scientific evidence.
The American College of Obstetricians and Gynecologists (ACOG) published a monograph focusing on cesarean delivery in the United States. This work was developed by a special ACOG task force to address cesarean delivery rates and published in 2000. The primary conclusions of this report were that efforts to reduce the cesarean delivery rate in the United States should focus on two benchmarks. First, there should be a focus on nulliparous women at term (37 weeks or greater) with singleton fetuses in cephalic presentation. In 1996, the cesarean delivery rate for this group was 17.9%, and the ACOG task force concluded that efforts to achieve a reduction to the 25th percentile, or 15.5%, in this group of women were reasonable and could be accomplished. Second, the task force recommended that efforts be made to reduce the percentage of women attempting vaginal birth after cesarean (VBAC). Of multiparas at 37 weeks gestation or greater with singleton fetuses and vertex presentations with prior low transverse cesarean incisions, 30.3% attempted VBAC in 1996. The task force recommended that a primary goal at the 75th percentile for this year, or 37%, would be reasonable. However, in 2000 the rate of attempted VBAC declined to 20.6%. Clearly, efforts to address the cesarean delivery rate in the United States have been a daunting challenge.
ETIOLOGY OF DYSTOCIA
Traditionally, the causes of abnormal labor have been attributed to the “powers” (uterine contractility), the “passage” (maternal pelvimetry), or the “passenger” (position and size of the fetus). In more scientific terms, these represent a primary dysfunctional labor, cephalopelvic or fetopelvic disproportion, abnormal fetal head position, and asynclitism. This section evaluates each of these potential causes of dystocia. The generic term “failure to progress” is often used as a diagnosis to justify cesarean delivery. This term is more appropriately used as a sign of an underlying problem and does not represent a diagnosis. Hence, the term “failure to progress” is not sufficient to describe the labor problem and should not be used.
Primary Dysfunctional Labor
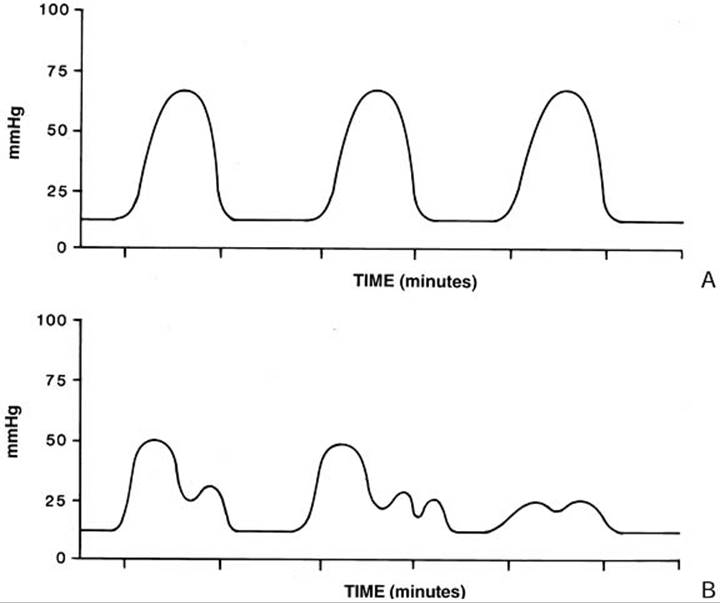
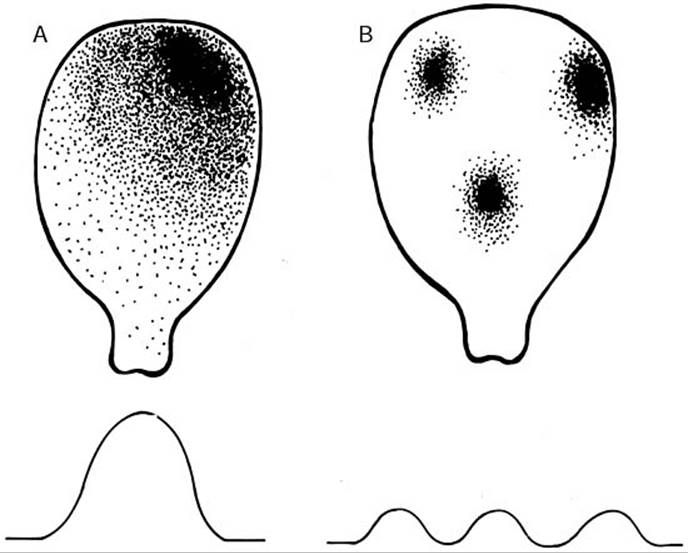
Primary dysfunctional labor refers to inadequate uterine contractility to maintain appropriate progress in labor. In general, an adequate uterine contraction pattern is one in which there are four concerted synchronous contractions every 10 minutes (Fig. 22.5). However, some women contract less frequently and continue to progress adequately in labor such that no intervention or treatment is required. Unlike the cardiac conduction system, the uterus has no defined nervous system for the conduction of electric signals to stimulate muscle contractions. The readiness of the uterus for labor is heralded by the occurrence and widespread distribution of gap junctions throughout the myometrium. Gap junctions allow for the rapid transmission of calcium fluxes through the uterine musculature and, hence, the occurrence of global uterine contractions. The uterus commonly has focal contractions throughout pregnancy (Braxton Hicks contractions) which are not of sufficient strength or duration to effect cervical change and therefore do not constitute labor.
|
|
|
FIG. 22.5. Uterine contraction patterns. Uterine contractions can be depicted using tocodynometry (external monitoring) or direct uterine pressures (using intrauterine pressure catheters). A: Contraction pattern of a normal labor. Significant pressure is obtained with contractions every 2 to 3 minutes. B: Uterine contraction patterns typical of primary dysfunctional labor. Contractions achieve varying degrees of pressure and are often combined (coupling). |
Smooth muscle cells of the uterus are not randomly distributed but are arranged in a specific fashion such that maximal force can be generated to effect vaginal delivery. In women with uterine embryologic abnormalities such as a didelphic uterus or bicornuate uterus, labor is not often successful in achieving vaginal delivery, as global, concerted uterine contractions cannot occur because of the abnormal arrangement of uterine smooth muscle cells. Similar problems may be noted in women exposed to diethylstilbestrol (DES) in utero with uterine anomalies characteristic of this teratogen (e.g., T-shaped uterus).
In the structurally normal uterus, contractions begin to occur less randomly days to weeks before the initiation of labor. Moreover, there is a distinct diurnal variation of uterine contractility such that, in most women, uterine contractions occur more frequently and labor most often commences at night. These rhythmic variations may be the result of hormonal patterns in which specific and predictable changes in different hormones (e.g., corticotropin-releasing hormone, progesterone, estradiol) allow for more frequent and stronger uterine contractions until the final signal for labor. While the precise nature of this signal in women is not known, cortisol appears to play a key role in the initiation of parturition.
As the normal uterus approaches term and labor commences, different foci for the initiation of a uterine contraction may be present (Fig. 22.6). This phenomenon often leads to the clinical scenario in which some contractions are quite hard and lengthy whereas other contractions are mild and of short duration. Women will have mild contractions interspersed with firmer, more painful contractions because of the lack of a dominant “pacemaker” in the uterine musculature. Eventually, as labor progresses, one of these foci of uterine contractility predominates over other foci, resulting in more concerted and painful uterine contractions. As this occurs, true labor commences with effacement and dilation, and this change is reflected in the uterine tocodynometry patterns (see Fig. 22.5). In a primary dysfunctional labor, uterine activity shifts from the concerted global contractions to more focal and less efficient contractions by allowing the reemergence of other pacemaker foci (see Fig. 22.6). Medical therapy with oxytocin is effective at correcting the underlying pathophysiology and restoring the pattern of global and concerted uterine contractions.
|
|
|
FIG. 22.6. Uterine pacemakers and contractions. A: Normal uterine contraction pattern associated with a single dominant pacemaker focus. B: A uterus with three separate pacemakers, all firing sequentially. Note that the uterine pressure achieved in this situation is less than that shown with a single dominant pacemaker. |
Although usually quite effective, oxytocin therapy may be of little benefit if the woman has intrauterine infection complicating labor. If the parturient has clinical signs of intrauterine infection, then labor progress is often desultory and not remedied with oxytocin augmentation. Clinical signs of intrauterine infection include maternal fever (>38°C), fetal tachycardia (baseline fetal heart rate of >160 beats/min), elevated maternal white cell count, uterine tenderness when the uterus is relaxed, and foul-smelling vaginal discharge. With the diagnosis of intrauterine infection, broad-spectrum antimicrobial agents should be administered and uterine activity stimulated with oxytocin if labor is not progressing adequately.
Cephalopelvic Disproportion
True cephalopelvic disproportion (CPD), or fetopelvic disproportion, is a rare occurrence in the labor and delivery suite. Some authorities believe that CPD occurs in one in 250 pregnancies. CPD occurs when the fetal birth weight or the fetal head is of sufficient size or orientation to preclude entry into the maternal pelvic inlet. This diagnosis if often made in retrospect after the birth weight is known and the positioning of the fetal head has been determined at the time of cesarean delivery. However, in the United States, the term CPD is used to describe almost any unsuccessful attempt at vaginal delivery. Further, the diagnosis of CPD is often used when labor progress is not sufficient and medical therapy is not successful or even not attempted. These cases often reflect inadequate use of oxytocin and are not problems with large fetal size or a small maternal pelvis. CPD is an important diagnosis because it has prognostic information for subsequent pregnancies when VBAC is considered. In women with a prior diagnosis of CPD, success rates of VBAC vary from 50% to 70%. Additionally, they should be managed differently during the VBAC with prompt repeat cesarean if labor does not progress appropriately.
Another important contribution to the fetopelvic relationship is the size of the fetus. Pregnancies with macrosomic fetuses (>4,000 g birth weight) have a greater risk of cesarean delivery for dystocia as a result of true CPD. In a study by Turner and colleagues, fetal macrosomia was associated with longer first and second stages of labor, greater need for oxytocin therapy, and a greater risk for cesarean delivery for CPD refractory to oxytocin. In their patient population, they had an overall incidence of cesarean delivery of 5.2%, but if birth weight was 4,000 to 4,500 g, the incidence of cesarean delivery was 13.8%. Also, forceps delivery was employed in 31.8% of infants with a birth weight of 4,000 to 4,500 g, whereas forceps were used in 13.6% of deliveries overall.
Unfortunately, there are no good predictors of fetal weight to guide management. Sonographic estimates of fetal weight at term are notoriously spurious and can miscalculate birth weight by 500 g or more. The obstetrician employing Leopold maneuvers to estimate fetal weight by palpation of the maternal abdomen can only estimate small, average, or large fetal size. Hence, it is not advisable to induce labor or perform a cesarean delivery for presumed macrosomia unless the obstetrician judges a dangerous situation exists for vaginal delivery (e.g., high risk of shoulder dystocia). Numerous studies of induction of labor for presumed macrosomia consistently show an increase in the cesarean delivery rate with no decrease in neonatal morbidity and poor prediction of macrosomia.
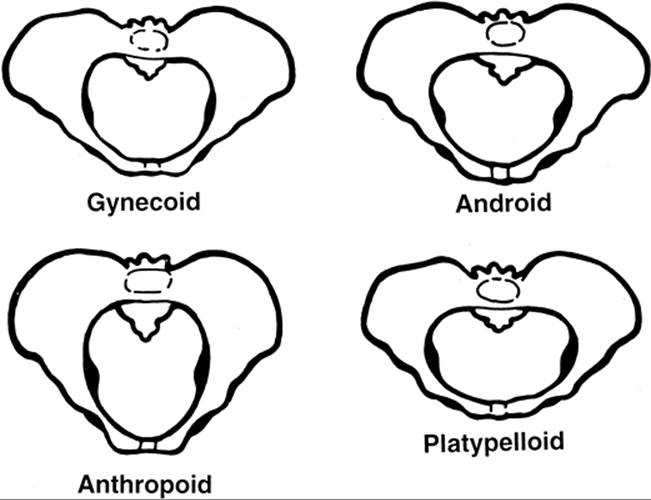
When the diagnosis of a labor abnormality is made, clinical pelvimetry should be performed to assess the dimensions of the maternal pelvis (Fig. 22.7). Only in the rare cases in which the maternal pelvis is markedly small or if there is clear CPD should cesarean delivery be performed without the prior use of oxytocin. For example, labor through a platypelloid pelvis with a normal term-sized fetus is rarely successful because of the markedly shortened anterior–posterior diameter that characterizes this pelvic architecture. After assessment of the pelvic type, approximations of the fetal size should be undertaken. Medical therapy with oxytocin should be instituted unless the fetus appears to be markedly macrosomic (>4,500 g).
|
|
|
FIG. 22.7. Pelvic types. There are four primary pelvic types: gynecoid, android, anthropoid, and platypelloid. Some women may have a mixed pelvic type with features suggestive of different pelvic types and will not fit conveniently into one of these four categories. |
Abnormal Position of the Fetal Head
Abnormal positions of the fetal head include occipital posterior (OP), deep transverse arrest, and deflexion abnormalities such as face and brow presentations and reflect fundamental abnormalities in the cardinal movements of labor. Different positions of the fetal head are depicted in Figure 22.8. An OP position is unfavorable for successful vaginal delivery, particularly if the parturient has an android pelvic structure, as the long diameter of the fetal head negotiates the maternal pelvis at a relatively high station leading to poor descent. Additionally, the fetal heart tracing may have some unusual decelerations that are difficult to interpret, leading to more advanced testing of the fetal acid–base status (e.g., fetal scalp pH determinations). The OP position is a relatively rare cause of dystocia, accounting for about 1 in 250 cesarean deliveries, but it can be corrected with oxytocin therapy. Operative vaginal delivery, either through a Scanzoni maneuver or through a straight OP application with traction, is another option for delivery. A Scanzoni maneuver involves rotating the OP fetus to an occipital anterior (OA) position with forceps and then completing the delivery with forceps from the OA position. A Scanzoni maneuver is associated with a higher incidence of maternal trauma (third- and fourth-degree lacerations of the perineum and sulcus tears of the vagina) and fetal trauma (spinal cord transection). Hence, such deliveries should be performed only by obstetricians skilled in these techniques. Moreover, delivery of the OP fetus with forceps should probably be attempted only if the fetal head has attained at least at +1 to +2 station. At higher stations, cesarean delivery may be the safest alternative. The prudent obstetrician will realize that assigning station in a labor characterized by an OP position is more difficult than in an OA position and often leads to the impression of a lower station than is actually present. Care should be taken to accurately assess the biparietal diameter in relation to the maternal ischial spines.
|
|
|
FIG. 22.8. Position of the fetal head. The sutures of the fetal head should be palpated, and the fetal head position should be recorded to ensure that the normal cardinal movements of labor are being followed. The fetal occiput with the maternal position constitute the reference points. Hence, OA refers to the occiput anterior position; OP, occiput posterior; LOT, left occiput transverse; LOA, left occiput anterior; ROP, right occiput posterior. Any fetal position can occur and should be noted on the labor curve. |
A deep transverse arrest occurs in the second stage of labor where the fetus maintains an occipital transverse (OT) position at a low pelvic station. Deep transverse arrests are often associated with abnormal maternal pelvic architecture and may not be easily delivered via forceps. Keilland forceps were designed to address the problem of the deep transverse arrest. Vacuum delivery should probably be avoided in this circumstance, as excessive traction of the fetus with a deep transverse arrest can result in birth trauma. Cesarean delivery is the prudent option if the fetal station is not sufficiently low for operative vaginal delivery or if excessive traction is required to effect delivery. Operative vaginal delivery for a deep transverse arrest should be performed only by obstetricians skilled in the use of forceps for this problem.
Deflexion abnormalities also cause dystocia. The classic forms of deflexion abnormalities include brow and face presentations. Typically, a brow presentation is characterized by the long axis of the fetal head negotiating the short axis of the midpelvis, precluding vaginal delivery. A fetus in the brow presentation may spontaneously convert to a vertex or face presentation. Whereas fetuses with a brow presentation that do not convert rarely deliver vaginally (except in women with generously sized midpelvic dimensions with a small fetus), face presentations will often deliver vaginally if the mentum, or chin, is positioned anteriorly (mentum anterior). Although these extreme flexion abnormalities are usually easily diagnosed and are relatively rare, other mild flexion abnormalities may not be so readily evident. Flexion abnormalities may be suspected in a prolonged or protracted labor unresponsive to oxytocin. Unfortunately, there are no safe and accepted means to correct flexion abnormalities of the fetal head.
Often, abnormal fetal position may occur as the result of the maternal pelvic type (see Fig. 22.7). For example, android pelvic types often lead to deep transverse arrest or OP position because of the progressive narrowing of the pelvis. Women with an anthropoid pelvis tend to have fetal positions persistently OA or OP, thus interfering with the normal cardinal movements of labor. Finally, women with a true platypelloid pelvis have transverse arrests, assuming the fetal head negotiates the shortened pelvic inlet. Because many women have mixed pelvic types, careful clinical pelvimetry may provide valuable information in the management of dystocia.
Asynclitism
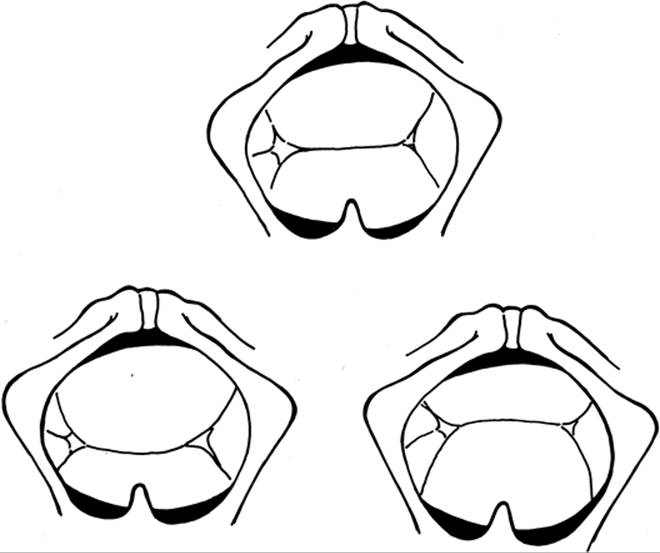
When asynclitism of the fetal head occurs, the sagittal suture of the head is either deviated posteriorly or anteriorly in relation to the maternal outlet (Fig. 22.9). As with other situations involving abnormal positioning of the fetal head, a larger diameter of the fetal head is expected to negotiate the bony pelvis of the mother. In these situations, the second stage of labor is often prolonged and arrest of descent is common, leading to an increased need for operative vaginal delivery. An important aspect of performing operative vaginal delivery involves correction of the asynclitism of the fetal head. This correction can often be accomplished with forceps that have a sliding lock or through vacuum extraction of the fetus, where the precise attitude and positioning of the fetus is of less importance.
|
|
|
FIG. 22.9. Synclitism. The term synclitism refers to the relative orientation of the fetal sagittal suture with the maternal bony pelvis. Top: Normal synclitism of a fetus in left occiput transverse position, with the sagittal suture equidistant between the anterior and posterior segments of the maternal pelvis. Lower Left: Posterior asynclitism, where the sagittal suture is closer to the posterior bony pelvis, and more of the right parietal bone is palpated.Lower Right: Anterior asynclitism in which the sagittal suture is more anteriorly located, and the left parietal bone is more readily evident. |
Fetal Abnormalities
Specific fetal abnormalities may contribute to the etiology of dystocia. Fetuses with neuromuscular disease, and particularly those that have suffered an in utero demise, may have flexion abnormalities. Also, fetal conditions such as hydrocephalus, hydrops fetalis, and tumors of the head or sacrum can lead to mechanical obstruction of the birth canal and hence cause dystocia, which is usually not remedied except by cesarean delivery.
SPECIFIC LABOR ABNORMALITIES
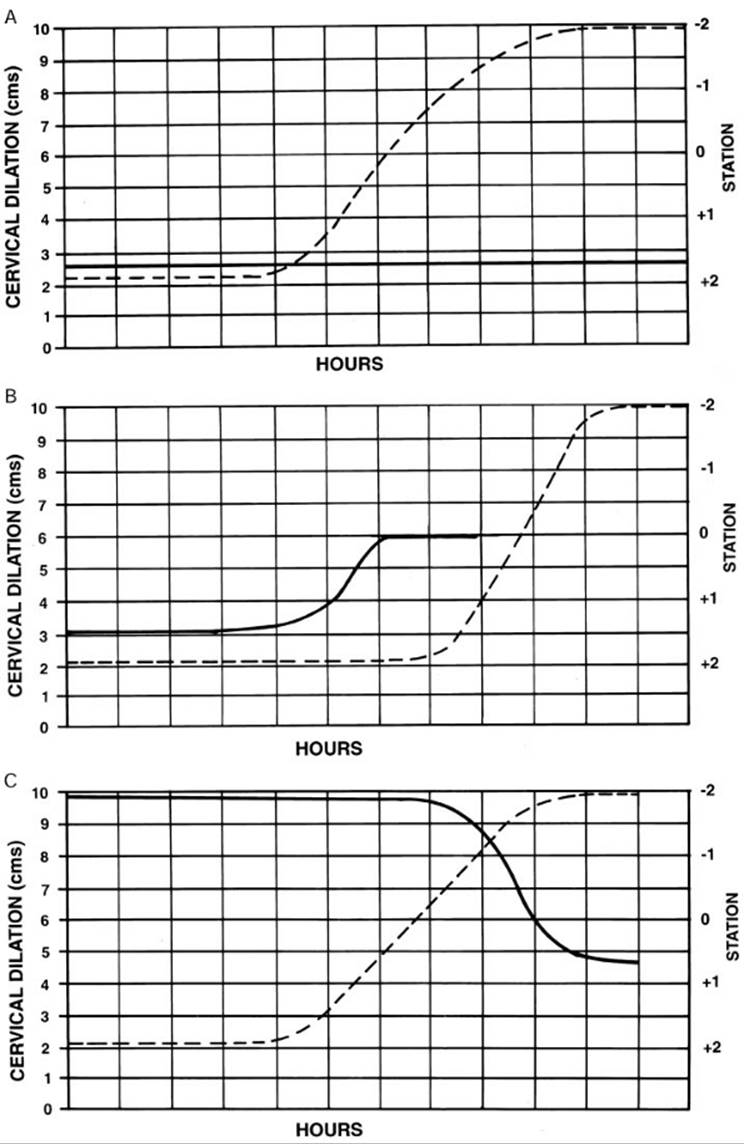
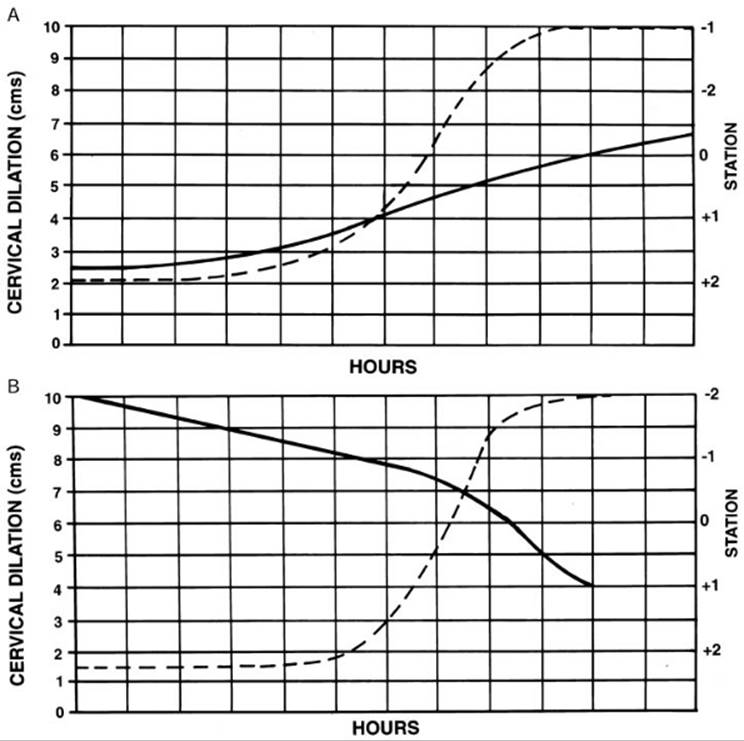
Only if the progress of labor is closely monitored can labor abnormalities be diagnosed. Moreover, the timely diagnosis of these labor abnormalities, with prompt medical therapy, should improve the chances of achieving a vaginal delivery. These labor abnormalities can be classified as either arrest disorders (Fig. 22.10) or protraction disorders (Fig. 22.11). Table 22.2 provides parameters for abnormal labor.
|
|
|
FIG. 22.10. Arrest disorders. These figures depict examples of different arrest disorders. A: Prolonged latent phase. Although one might say that a prolonged latent phase is not strictly an arrest disorder, it reflects an abnormality in the normal progress of labor in which the change into the active phase is arrested. B: Arrest of dilation, in which the cervix achieves 6 cm of dilation but then does not change for 2 hours. C: Example of an arrest of descent. The fetal head moves from a -2 station to a 0 to -1 station but then makes no further progress. |
|
|
|
FIG. 22.11. Protraction disorders. These examples of protraction disorders are exaggerated to depict each abnormality. In each case, these abnormalities should be detected early, and appropriate therapy instituted. A: Protracted active phase. Note that the average slope is much less than 1.5 cm per hour. B: Prolonged and neglected second stage. Intervention should occur sooner than indicated on this partogram. |
Prolonged Latent Phase
A prolonged latent phase (see Fig. 22.10A) occurs when regular painful uterine contractions are present for an extended period of time without entering the active phase of labor. Although a prolonged latent phase is not generally classified as an arrest disorder, some authorities believe that the latent phase is an example of a primary dysfunctional labor. In nulliparous women, the definition of a prolonged latent phase is a period of uterine activity without cervical change for more than 20 hours; in multiparas this time period is 14 hours. The cervix may be dilated up to 4 cm and completely effaced. The precise etiology is not clear but likely reflects ineffective uterine contractions without a dominant myometrial pacemaker. The management of a prolonged latent phase is controversial, and in general there are two possible approaches. Some obstetricians believe that a prolonged latent phase reflects an underlying labor abnormality that should be managed aggressively with amniotomy and oxytocin. The other approach is to provide supportive measures including intravenous hydration and narcotic pain relief. Studies comparing these approaches have not shown either to be a clearly superior choice, so either treatment plan is acceptable as long as the patient understands the plan and risks. The more aggressive approach in some cases may be an induction of labor with the attendant higher risk of cesarean delivery, whereas the more conservative approach runs the risk of prolonging a potentially dysfunctional labor. Either option is acceptable. Deciding which course to take requires obstetric judgment and a motivated, informed patient.
Arrest of Dilation
An arrest of dilation occurs when there is no cervical change after 2 hours in the active phase of labor despite uterine activity (see Fig. 22.10B). In most cases, arrest of dilation occurs as a result of ineffective uterine contractions. Uterine contractions may become dysfunctional and lose their synchronous, rhythmic nature. Figure 22.5 shows an example of the loss of a dominant myometrial pacemaker with the expression of two pacemakers firing independently and without coordinated uterine contractions. In any case, prompt medical therapy with oxytocin usually corrects the underlying problem. In those rare cases where CPD is evident on evaluation of the patient, prompt cesarean delivery is indicated.
Arrest of Descent
After complete dilation is achieved, the primary goal of the second stage of labor is to gain station of the fetal head through the maternal pelvis with eventual delivery. If the patient does not gain station of 1 cm after an hour of adequate pushing efforts, an arrest of descent is diagnosed (see Fig. 22.10C). The cause of this arrest disorder may be one or a combination of several underlying abnormalities, including inadequate uterine contractions, CPD, abnormal fetal position, and asynclitism. If an arrest of descent is diagnosed, the obstetrician has several options, including the use of oxytocin, operative vaginal delivery, or cesarean delivery. The choices for therapy should be guided by the fetal status, station of the fetal head, maternal status, and operator experience.
Protracted Active Phase
When cervical change continues with adequate uterine contractions in the active phase of labor, but over a longer time period than anticipated, then a prolonged active phase is the diagnosis (see Fig. 22.11A). In nulliparous patients, cervical change is less than 1.2 cm per hour, whereas in multiparous patients cervical change is occurring at less than 1.5 cm per hour. A prolonged active phase may be the result of inadequate uterine contractility, but often both the timing and strength of uterine contractions appear to be normal and cervix dilation occurs slowly despite oxytocin therapy. The underlying problem may be true CPD or an undiagnosed flexion abnormality. Oxytocin therapy often is not successful in accelerating labor, and an arrest of dilation or descent may be inevitable regardless of the therapies employed. Should a protracted active phase lead to an arrest of labor despite oxytocin therapy, cesarean delivery is the best therapeutic course.
Prolonged Second Stage
An exaggerated example of a prolonged second stage is shown in Fig. 22.11B. A prolonged second stage is diagnosed when the fetal head descends less than 1 cm per hour. A second stage lasting longer than 2 hours has traditionally been considered abnormal and is an indication for operative vaginal delivery or cesarean delivery. However, more contemporary management allows for more flexibility in the management of the second stage of labor. If the fetus is tolerating the stresses of the second stage well and some gain in station is being made, then there is no indication for terminating the second stage solely on the basis of time in the second stage. Because epidural analgesia may increase the length of the second stage, there is no reason for intervention on the obstetrician's part if the fetal heart rate tracing is acceptable and the mother is comfortable. However, maternal exhaustion will often occur and result in the need for operative intervention. As with the other labor abnormalities, an attentive obstetrician with a plan of management for any contingency should improve both maternal and fetal outcome in abnormal second stages of labor.
In summary, several specific labor abnormalities may occur and can easily be diagnosed. With a rational plan of management, the need for cesarean delivery can be avoided and salutary maternal and fetal outcomes accomplished. The term “failure to progress” thus is not sufficient for a diagnosis. For example, a woman may have “arrest of dilation” followed by treatment with oxytocin. Should this be unsuccessful, then she may require cesarean delivery for “arrest of dilation refractory to oxytocin therapy.” Addressing labor abnormalities in more specific terms enables more rational treatment strategies to be used in the current and future pregnancies, regardless of the outcome.
EPIDURAL ANALGESIA AND LABOR PROGRESS
The impact of epidural analgesia on the occurrence of dystocia and the cesarean delivery rate has been controversial. Epidural analgesia is an excellent form of pain relief for the laboring woman, and in some labor and delivery units, the majority of laboring women opt for this therapy (see Chapter 3). Epidural analgesia is a vital part of the obstetrician's and anesthesiologist's armament to provide pain relief during labor, and both the ACOG and the American Society of Anesthesiologists endorse the use of epidural analgesia for pain management in labor.
However, epidural analgesia may have contributed significantly to the cesarean delivery epidemic of the past two decades. A meta-analysis by Morton and colleagues in 1994 of epidural use in the laboring woman cites an increased risk of 10% for cesarean delivery. Studies have supported this finding. Traynor and associates in 2000 reported that epidural analgesia was associated with a four-fold increased risk for cesarean delivery (12.2% in women with epidural vs. 3.3% in women without epidural), and that the risk for cesarean delivery increased progressively with higher station, less dilation, and less effacement at the time of catheter placement. Similarly, in 2000, Sizer and Nirmal found that epidural analgesia was associated with an increased incidence of OP presentation, leading to a three-fold increase in the risk for cesarean delivery (13.7% for OA presentation, 41.7% for OP presentation) and for operative vaginal delivery (24.4% for OA presentation, 43.7% for OP presentation).
Conversely, other studies contradict these reports and note that epidural use was not associated with an increase in the incidence of OP presentations. Clark and colleagues published a prospective randomized trial in 1998 comparing epidural analgesia with intravenous opioids for pain relief. The cesarean delivery rates were no different in the two groups (13.6% in the opioid group, 9.6% in the epidural group). Imprey and co-workers, in a retrospective review of 1,000 nulliparas, found that an increase in the epidural use from 10% to 57% over the course of 7 years did not result in an increase in the cesarean delivery rate of 3.8% to 5%. Zhang and colleagues, in a summary of studies regarding the use of epidural analgesia and labor outcome, concluded that clinical trials of epidural use of low-dose bupivacaine did not increase the risk of cesarean delivery. Notably, however, observational studies do indicate an increase risk for cesarean and instrumental deliveries, suggesting that selection bias may skew these results. These data depict the exceptional difficulty of studying this clinical issue, given the complexity of the labor process and the multitude of factors that may impact on labor outcomes.
The key to the rational use of epidural analgesia is the approximation of fetal station and cervical dilation. In a 1999 study, Holt and colleagues reported that the strongest risk factor for needing cesarean delivery with epidural analgesia was station at the time of epidural placement. The higher the station at the time of epidural, particularly if -1 or higher, the greater the risk for cesarean delivery. Based on these studies, it seems prudent to recommend that epidural placement be delayed until fetal station has reached the midpelvis. Importantly, women in labor should not be denied epidural analgesia when clinically reasonable and safe.
OPTIONS FOR THE MANAGEMENT OF DYSTOCIA
Once dystocia is diagnosed and a specific abnormality identified, the obstetrician has a number of therapeutic options that can lead to vaginal delivery rather than immediate cesarean delivery. Oxytocin should be administered first unless there is a clear contraindication to this medication, as this is an effective and safe therapy in experienced hands and can correct most labor abnormalities. A schematic depicting an example of one method to manage abnormal labor is shown in Figure 22.12.
|
|
|
FIG. 22.12. Therapeutic options in the management of dystocia. This schematic provides one algorithm for the management of dystocia. The primary goal is to effect vaginal delivery with good maternal and neonatal outcomes. |
Mapping the Progress of Labor
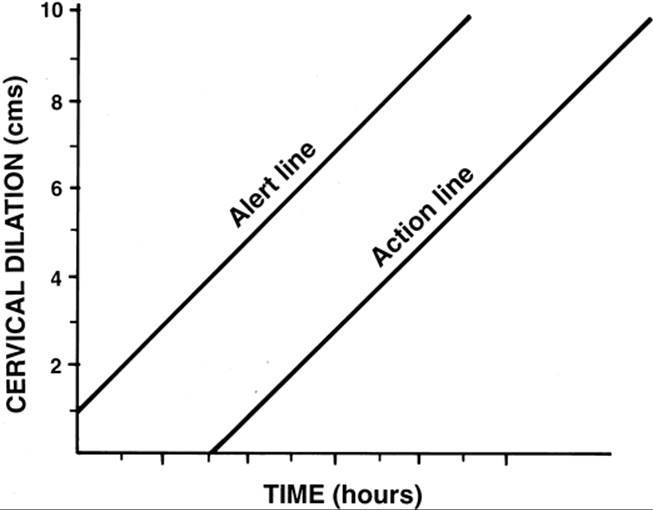
A key adjunct to the management of labor is the use of some form of a labor curve. Several different labor curves have been developed, and no one is better than any other. Several reports have shown that the graphic analysis of labor progress improves maternal and fetal outcomes while lowering cesarean delivery rates, including sites in underdeveloped countries. Many labor and delivery units use the concept of “alert” and “action” lines (Fig. 22.13). In this type of partogram (or labor curve), crossing an alert line merely means that labor progress is slowing, while crossing the action line indicates that a specific action must be taken. Mapping labor progress allows for the timely diagnosis of dysfunctional labor and the prompt institution of medical therapy. Therefore, most contemporary labor and delivery suites have incorporated the use of labor curves into the routine management of laboring women.
|
|
|
FIG. 22.13. Action and alert lines in the management of labor. This figure depicts the alert and action lines graphically. This type of labor curve has been used successfully to manage labor in many different settings. With this curve, slowing of the labor curve is first marked by an alert that labor is not progressing normally. Then, with further lack of progress, the action line is crossed, mandating that some form of action (medical or surgical therapy) be instituted. (Adapted from Philpott RH, Castle WM. Cervicographs in the management of labor in primigravidae: II. The action line and treatment of abnormal labor. J Obstet Gynecol Br Commonw 1972;79:599–602, with permission.) |
Amniotomy
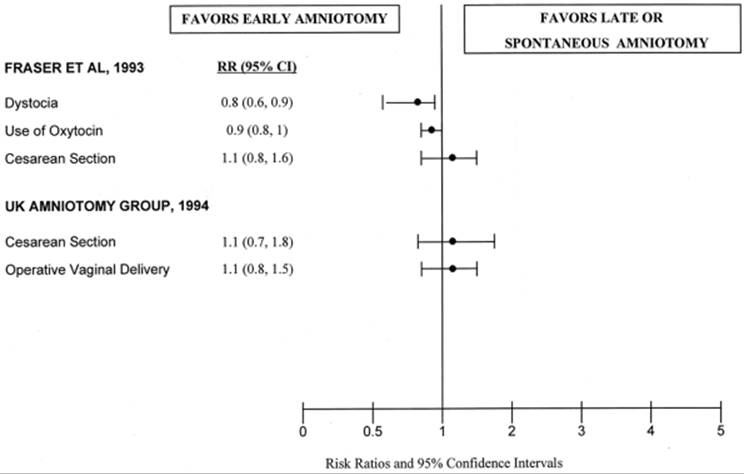
Artificial rupture of membranes has been used in the management of slow or desultory labor for decades. This intervention has been deplored by some obstetricians as needless intervention and recommended by others as a useful adjunct. Retrospective studies with relatively small sample sizes suggest that amniotomy could speed normal labor and stimulate abnormal labor to again meet normal milestones. However, large-scale prospective randomized studies do not support the routine use of amniotomy in the management of dystocia (Fig. 22.14). Although normal labor is accelerated modestly, particularly in multiparous women, women in whom amniotomy was routinely used did not have lower rates of cesarean delivery. Additionally, there is a modest increase in the rate of intrauterine infection in women who underwent amniotomy early in the course of labor (e.g., <4 cm dilation). Rupture of the membranes is also associated with variable decelerations of the fetal heart rate as a result of umbilical cord constriction. This problem can, in some cases, be remedied with amnioinfusion of warm saline into the uterine cavity through an intrauterine pressure catheter (IUPC). In such situations, the obstetrician uses one measure to improve outcome (amniotomy) which unfortunately leads to further interventions that otherwise could have been avoided.
|
|
|
FIG. 22.14. Odds ratio of the effect of amniotomy on labor dystocia. Amniotomy has little effect on the course of labor, the incidence of dystocia, or the incidence of cesarean delivery. |
Conversely, there are reasonable indications for amniotomy. Amniotomy is an excellent method for labor induction if the cervix is favorable and the fetal head well applied to the cervix. The judicious use of amniotomy after 5 cm does accelerate labor in the multiparous woman, but less so in the nullipara. Also, oxytocin tends to work more efficiently if the membranes have been ruptured. Disruption of the membranes is required for internal monitoring of the fetal heart rate tracing or of uterine activity. Rupturing of the membranes will detect meconium staining of the amniotic fluid and alert the obstetrician and pediatrician to be prepared for a potentially high-risk circumstance regarding care of the newborn and the prevention of meconium aspiration.
Thus, amniotomy can be a useful adjunct in the management of labor, but only if used wisely and in appropriate circumstances. As long as the parturient is making adequate progress in labor and the fetal heart rate tracing is normal, there is no indication for amniotomy. Spontaneous rupture of the membranes usually occurs at between 7 and 9 cm dilation. Cervical examinations should be minimized after the membranes have been ruptured to decrease the chance of infection because the number of cervical examinations correlates well with the risk of intrauterine infection.
Intrauterine Pressure Catheters
An IUPC is often introduced into the amniotic cavity to help determine the strength of uterine contractions. Application of the catheter requires that the fetal membranes are ruptured, either through spontaneous or artificial rupture of the membranes. Some IUPC require a pressure transducer at the bedside which requires calibration to obtain reliable pressure measurements. More recent devices have the pressure transducer in the tip of the catheter, presumably yielding more reliable pressure measurements. Unfortunately, these pressure readings may be spurious, but more importantly there is a wide range of variation in the duration, strength, and frequency of contractions in normal labor. Thus, quantification of labor using IUPC and applying one standard to all women in labor seems unlikely to lead to favorable maternal outcomes.
Many different quantitative approaches to uterine contractility have been proposed using IUPC technology. For example, the Montevideo unit is the average intensity of the uterine contractions multiplied by the number of contractions over a 10-minute period (expressed as mm Hg/10 min). A total of 200 Montevideo units indicates that there is adequate uterine contractility to effect labor progress. Past studies have suggested that if this level of uterine activity was achieved and no labor progress resulted, then one could state that an adequate trial of labor had been completed and justify cesarean delivery. Other studies have found that IUPCs increase the rate of intrauterine infection with no definable benefit. No study to date has shown that the use of IUPC technology improves maternal or perinatal outcome. Therefore, there is no compelling reason to use IUPC in the management of labor. Perhaps the best application for IUPCs is in assisting nursing personnel with the use of oxytocin so that the precise timing of uterine contractions can be determined.
Oxytocin
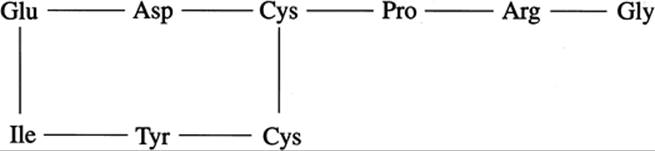
Oxytocin is a nine–amino-acid peptide (Fig. 22.15) normally produced in the hypothalamus and secreted by the posterior pituitary in a spurting or pulsatile fashion. During normal pregnancy, serum oxytocin concentrations remain essentially unchanged throughout gestation, and there is only modest increase in total serum concentrations before labor. However, with labor, plasma levels increase and then peak in the second stage. Oxytocin receptor expression increases in the decidua in the weeks preceding the onset of labor, and increases sharply just before labor. Oxytocin receptors are expressed primarily in decidua, myometrium, and breast tissue. Myometrial sensitivity to oxytocin parallels expression of oxytocin receptors such that responsiveness begins at about 20 weeks of gestation and then dramatically increases at about 30 weeks of gestation. Oxytocin is cleared from peripheral blood by the liver and kidney and is also significantly metabolized by oxytocinase, an enzyme produced in abundant quantities by the placenta and gestational tissues.
|
|
|
FIG. 22.15. The amino acid structure of oxytocin. Oxytocin is a nine–amino-acid peptide with two disulfide bonds. |
Oxytocin may be administered intravenously, subcutaneously, intramuscularly, and buccally. With intravenous administration, there is a concentration-dependent increase in its serum levels but with wide individual variation in responsiveness to the drug. Intravenous administration of oxytocin has effects only on tissues expressing receptors and thus has an excellent therapeutic index. Oxytocin administration results in an increase in the frequency, duration, and strength of uterine contractions. The myometrial response to oxytocin is highly variable, and uterine hyperstimulation may occur at any dose of administered oxytocin depending on the individual patient. Uterine hyperstimulation necessitating discontinuation of the drug or a decrease in the dose being used is the most common side effect of the medication. The only known side effects of oxytocin not related to uterine activity include disturbances in water homeostasis and electrolytes. Oxytocin has approximately 1% the antidiuretic effect of vasopressin, and these side effects are usually seen only at high concentrations of oxytocin infusion (e.g., 40–50 total units administered). Also, intravenous boluses of oxytocin can lead to hypotension and tachycardia as a result of a paradoxical relaxation of vascular smooth muscle.
From the first clinically described use of oxytocin in the 1940s, there has been controversy as to the best and most appropriate regimen for oxytocin use. Table 22.4 summarizes some different acceptable oxytocin protocols currently used. Historically, early regimens of oxytocin administration were highly individualized by physician preference, ranging from relatively low doses to extremely high doses. For example, Seitchik and Castillo found that the most important determinant of the maximum oxytocin dose and the frequency of hyperstimulation was dose-incrementation interval. Those patients who received lower dose increments (every 30–40 min) by 1.0 mU per minute had lower oxytocin doses and less hyperstimulation with good outcomes.
|
|
|
TABLE 22.4. Acceptable oxytocin protocols |
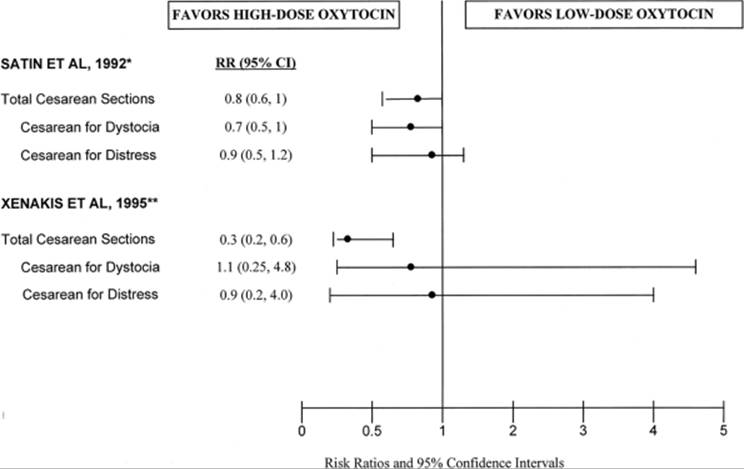
However, more recent studies have shown that low-dose protocols may result in higher cesarean delivery rates when compared to higher-dose oxytocin protocols. Satin and colleagues used two different methods of oxytocin administration. In one 5-month period, they used a low-dose regimen in 1,251 women where the starting dose of 1 mU per minute was increased by 1 mU per minute every 20 minutes until 8 mU per minute was reached, and then the incremental increase was by 2 mU per minute every 20 minutes up to a maximum of 20 mU per minute. For the next 5-month period (1,537 women), they studied the higher-dose regimen advocated by O'Driscoll in which the starting dose of 6 mU per minute was increased by 6 mU per minute every 20 minutes up to a maximum of 42 mU per minute. Among those patients being augmented, the average maximum oxytocin dose was greater in the high-dose protocol (14.7 mU/min vs. 6.6 mU/min), as was the incidence of uterine hyperstimulation (52% vs. 39%). Notably, there was a significant decrease in the cesarean section rate for dystocia (9% vs. 12%), the use of forceps (12% vs. 16%), rates of neonatal sepsis (8% vs. 12%), and a shorter time from admission to delivery (10.1 h vs. 13.4 h).
In a following study, Satin and colleagues compared two incremental dosing intervals of high-dose oxytocin, comparing a 20-minute dosing interval versus a 40-minute dosing interval. In those women receiving oxytocin for labor augmentation, 603 were in the 20-minute interval group and 564 were in the 40-minute interval group. The results of this study showed that the maximum oxytocin dose, the time from admission to delivery, and the incidence of uterine hyperstimulation were similar in each group. However, women receiving incremental increases in oxytocin at 20-minute intervals had a significantly lower cesarean section rate for dystocia (8% vs. 12%).
A randomized study by Xenakis and associates compared the low-dose protocol of Seitchik and Castillo to a higher-dose protocol in which oxytocin was commenced at 4 mU per minute and increased by 4 mU per minute every 15 minutes. They found a significantly greater number of cesarean deliveries in women receiving the lower-dose regimen (25.7% vs. 10.4%). There were no differences in maternal or neonatal outcome or in the incidence of hyperstimulation. The average maximal dose of oxytocin in the high-dose regimen was only 9 mU per minute, suggesting that achieving a more rapid response with higher doses does not require excessive amounts of oxytocin and that prompt correction of the labor abnormality is critical for success.
These studies suggest that a higher dose of oxytocin will stimulate a higher proportion of patients earlier, resulting in more timely correction of dysfunctional labor and in a lower risk for cesarean delivery (Fig. 22.16). There are numerous factors that can account for the wide variation in responsiveness to oxytocin infusions, including differences in oxytocin receptor expression, differences in oxytocin plasma concentrations, and differences in oxytocinase concentrations and activity.
|
|
|
FIG. 22.16. Odds ratio of low-dose oxytocin versus high-dose oxytocin. High-dose oxytocin results in lower overall cesarean delivery rates. |
An important unanswered question relates to the safest maximum dose of oxytocin. While some authorities advocate a maximal dose of 42 mU per minute, there are few data upon which to base this recommendation. In a prospective randomized double-masked trial of oxytocin dosage in labor induction and augmentation by Merrill and Zlatnik, two different doses were used. A low- dose regimen of 1.5 mU per minute increasing by 1.5 mU per minute every 30 minutes was compared with a higher-dose regimen of 4.5 mU per minute increasing by 4.5 mU per minute every 30 minutes. Higher-dose oxytocin was associated with a significant shortening of labor, but with no significant differences in cesarean delivery rates. The highest oxytocin dose administered was 117 mU per minute and there were no differences in neonatal outcomes. Hence, no solid recommendations based on data can be made regarding the maximal safe dose of oxytocin.
Regardless of the choice of protocols, clinical judgment should be used when oxytocin therapy is prescribed. There should be no evidence of fetopelvic disproportion based on clinical pelvimetry and estimated fetal weight. If the pelvis is not adequate, or the fetus is large, then the dysfunctional labor may be a sign that vaginal delivery is not safe, and cesarean delivery would be the more appropriate therapy. Additionally, oxytocin should not be used in women with prior classic cesarean section scars because the risk of uterine rupture is high (5%–10%). Care should be taken when women with prior low transverse cesarean sections are being augmented with oxytocin. Although the studies regarding the use of oxytocin and the risk of scar dehiscence are mixed, one should know the total dose given and follow the course of labor carefully. Vaginal birth after cesarean section is addressed more fully in Chapter 24. Oxytocin is an extremely effective drug when used appropriately but can be dangerous for mother and fetus if used inappropriately. Therefore, clinical judgment is required whenever oxytocin is used in the management of dystocia.
Obstetric Patience
Traditional management of labor has been challenged by some new concepts based on scientific data rather than expert opinion. These new ideas rely on the obstetrician's patience and willingness to allow time for the patient to progress at a somewhat slower rate than has previously been felt to be acceptable. In this regard, these concepts are based on the use of fetal monitoring to ensure that the fetus is tolerating labor well.
Traditionally, an arrest of the active phase of labor with oxytocin augmentation for more than 2 hours was an indication for cesarean delivery. However, studies by Rouse and colleagues question this 2-hour time limit. In their initial study, the Rouse group found that extending the time period of active-phase arrest while on oxytocin from 2 hours to 4 hours was both safe and effective. In their original cohort of 542 normal women presenting with arrest of term labor, 126 demonstrated no labor progress after 2 hours of oxytocin augmentation. However, 101 of these 126 delivered vaginally, decreasing the overall cesarean delivery from 26% (if the 2-hour limit was used) to 8% for the entire study. In those women with presumed adequate labor on the basis of Montevideo units, 32 of 52 delivered vaginally simply by waiting for 4 hours rather than moving to cesarean after 2 hours. These women did have a higher incidence of intrauterine infection, but without increased neonatal morbidity.
In a following study, Rouse and colleagues observed 501 women with a similar protocol. Of these women, 38 had sustained adequate labor for 2 hours based on Montevideo units and no progress in labor. By merely waiting another 2 hours, 23 (or 61%) delivered vaginally and avoided an otherwise indicated cesarean delivery based on traditional criteria. Again, there were no adverse neonatal effects of continuing oxytocin for 4 hours, and there was a higher incidence of intrauterine infection in those women who labored further. Additionally, they found that achievement and maintenance of 200 Montevideo units, the value traditionally noted to represent “adequate” labor, was not predictive of delivery route.
While patient numbers are as yet insufficient to change traditional recommendations on the management of labor arrest, these studies, if confirmed, strongly suggest that allowing more time for oxytocin augmentation is reasonable, effective, and safe. A key issue again is that one management plan should not necessarily apply to all women in labor, as there is considerable individual variation in labor progress and responsiveness to oxytocin.
Two studies have explored different strategies of managing the second stage of labor. These studies have compared two groups of women in the second stage, in which one group of women was encouraged to push promptly with the diagnosis of complete dilation while the other group was encouraged to rest for 1 to 2 hours (or more) before starting pushing efforts. In the study by Fraser and associates, nulliparous women in the delayed pushing group were encouraged to wait at least 2 or more hours prior to pushing. Over 900 women were enrolled in each group. When compared to the early pushing group, women who delayed pushing had a lower incidence of “difficult delivery” (17.8% vs. 22.5%). Difficult delivery was defined as the need for midpelvic delivery, low-pelvic delivery with rotation, any manual rotational delivery, or second stage cesarean delivery. The primary difference was in the incidence of midpelvic delivery (9.3% vs. 13%), while cesarean delivery rates were similar (5.0% vs. 5.7%). Maternal morbidity and neonatal outcomes were similar between the two groups.
The other study of delayed pushing, by Hansen and colleagues, was also a randomized prospective trial comparing immediate versus delayed pushing efforts in over 250 women. In those women randomized to delayed pushing, nulliparas were rested for 120 minutes while multiparas rested for 60 minutes. The investigators found that there were no statistically significant differences in instrumental delivery rate, neonatal outcome, and rates of perineal injury. Women who rested had a longer second stage of labor, but decreased total time pushing, fewer decelerations, and less fatigue. Only three cesarean deliveries were performed, all in the control group. The authors concluded that delayed pushing, up to 4.9 hours, was safe and may be useful in selected patients.
The studies described in this section underscore the value of obstetric patience. While there are average times for the first and second stages of labor, these studies show that traditional and arbitrary time limits may be extended safely in selected patients, with improved maternal outcomes and continued good neonatal outcomes.
Operative Vaginal Delivery
Operative vaginal delivery should only be performed if the following criteria are met: complete cervical dilation, engagement of the fetal head filling the hollow of the sacrum, known position of the fetal head, and sufficient operator experience. Forceps- or vacuum-assisted vaginal delivery should be performed only on behalf of the mother or fetus and not for the convenience of the obstetrician. In the context of dystocia, the primary reason for moving to assisted vaginal delivery is an arrest of descent of the fetal head. This arrest may be due to inadequate uterine contractions, insufficient maternal pushing efforts, abnormal position of the fetal head (OP or deep transverse arrest), or asynclitism of the fetal head. In these situations, the mother often has pushed for 2 hours or more and may be unable to continue with effective pushing efforts because of exhaustion.
Appropriate forceps use or indications for vacuum extraction are dependent on the experience of the obstetrician. Experienced obstetricians skilled in the use of forceps have the judgment to use the appropriate instruments and traction for a successful and safe vaginal delivery. Less experienced providers may find vacuum extraction more successful but vacuum-assisted delivery still requires judgment and skill for a safe delivery. Even with vacuum extraction, prudent use in specific situations will decrease the incidence of maternal and fetal complications. An all too common occurrence is the inappropriate use of operative vaginal delivery with adverse obstetric and neonatal outcomes, usually due to inappropriate application at a higher than expected station. In experienced hands, there are no differences in neonatal outcome in infants delivered by normal vaginal delivery or by outlet forceps.
Cesarean Delivery
If all the previously outlined measures are not successful, then cesarean delivery is likely needed to obtain a good maternal and neonatal outcome. Although one should not move to cesarean delivery before all options are considered, similarly one should not hesitate to operate if a successful vaginal delivery is not possible without potential serious risk or harm to the fetus and neonate. Delay in moving to cesarean delivery when indicated can potentially lead to adverse maternal and neonatal outcomes such as postpartum hemorrhage, uterine rupture, and birth injury. Cesarean section is discussed in detail in Chapter 24.
ACTIVE MANAGEMENT OF LABOR
Since the mid-1960s, an organized approach known as the active management of labor (AMOL) has been developed and advocated by the obstetric staff at the National Maternity Hospital in Dublin, Ireland. Initially conceived by Kieran O'Driscoll, this approach has been modified over the years. The advocates of AMOL cite a continuing low cesarean delivery rate (approximately 10%) with excellent outcomes for mother and infant. The primary goal of AMOL is to prevent prolonged labor. Women are guaranteed that they will either be delivered, or close to delivery, within 12 hours of admission to the labor and delivery unit. The style and content of this labor management have generated much controversy and misunderstanding in the United States. For example, many obstetricians believe that the active part of AMOL is aggressive intervention in the laboring woman or high oxytocin doses, but in fact it refers to the fact that an obstetrician (usually the head of the department) reviews the labor progress of each patient to ensure that optimal outcomes are achieved.
Basic Concepts of AMOL
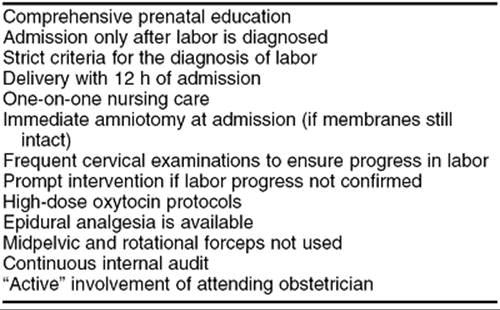
Table 22.5 lists the primary components of AMOL. Perhaps the hallmark feature of AMOL is that no patients are admitted to the labor and delivery unit unless the diagnosis of labor has been made. Labor is defined as painful, regular uterine contractions with complete cervical effacement, regardless of cervical dilation. The average dilation of the cervix at the time of admission is 2 to 3 cm. AMOL applies only to the nulliparous patient, as multiparous women who have had previous vaginal delivery usually do not have prolonged labor and have a higher risk of uterine rupture with oxytocin administration. After the diagnosis of labor has been made, amniotomy is performed at the time of admission regardless of cervical dilation. The diagnosis of labor is key. If this diagnosis is incorrect, then an induction of labor is being initiated with the attendant increased risk for cesarean delivery.
|
|
|
TABLE 22.5. Key concepts of active management of labor |
On admission, a nurse-midwife or student midwife is assigned to the patient who stays with only this patient throughout her entire labor. There are no provisions for change of nursing shifts. Also, these patients receive detailed instructions on expectations during labor in prenatal birthing classes. One-on-one nursing care, with a clear vision of the ensuing labor, alleviates maternal anxiety and is perhaps the most distinguishing feature of AMOL over other styles of labor management as practiced in the United States.
Cervical examinations to corroborate labor progress are performed by the midwives every 1 to 2 hours. If the patient does not make adequate progress in labor, oxytocin administration is promptly initiated at 6 mU per minute and increased by 6 mU per minute every 15 minutes until 7 to 8 contractions occur every 15 minutes (see Table 22.4). During labor, the patient is never left unattended by the midwife assigned to her care and uterine activity is palpated by the midwife. The midwife assigned to the parturient will then perform the delivery with the head midwife in attendance. The attending obstetrician is asked to intervene only when there is need for an obstetric operation, such as episiotomy, forceps delivery, or cesarean delivery. Midforceps delivery and rotational forceps are not performed.
With AMOL at the National Maternity Hospital, cesarean delivery rates for dystocia are less than 10%. Oxytocin is used in 50% to 60% of nulliparas and only 10% to 15% of multiparas (who are not managed with this program). Delivery occurs in less than 12 hours in 98% of women. Cerebral palsy rates approximate that of the United States, or about 2 per 1,000 births, and birth trauma is rare. Epidural analgesia is allowed and does not impact significantly on the cesarean delivery rate. Clearly, AMOL suits the population served at this hospital well.
Lessons from AMOL
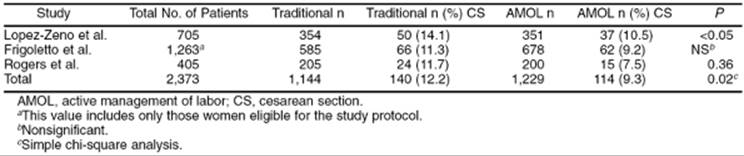
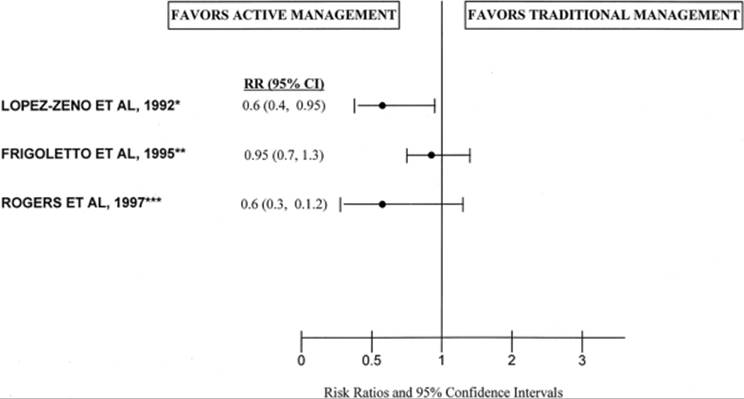
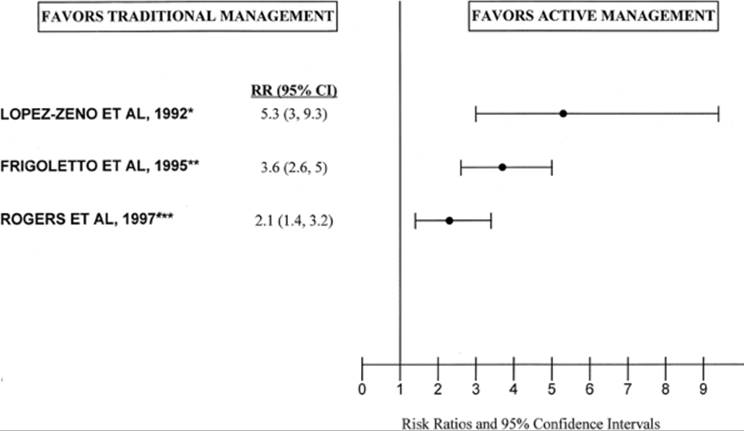
Three prospective randomized trials of AMOL have been conducted in the United States (Table 22.6). Lopez-Zeno and colleagues found a significant decrease in the cesarean delivery rate in nulliparous patients in the AMOL arm of the studies, from 14.1% to 10.5%. Frigoletto and associates randomized over 1,200 to AMOL or traditional management and found no decrease in the cesarean delivery rate but were able to show a modest decrease in the duration of labor in the AMOL arm. In the third study, Rogers and colleagues also found no significant decrease in cesarean delivery rate but confirmed a decrease in the length of labor. These discrepancies may be because AMOL may not significantly reduce the cesarean delivery rate if the baseline rate is 11% or less. In other nonrandomized studies, AMOL has been shown to decrease the primary cesarean delivery rate by 25% to 50%, and a recent meta-analysis by Glantz and McNanley showed that the risk of cesarean delivery for dystocia was decreased on average by 34%. In an analysis of these three randomized trials, AMOL resulted in a lower risk for cesarean delivery (Table 22.6, Fig. 22.17) and a greater incidence of delivery within 12 hours of labor (Fig. 22.18). A prospective randomized study performed at the National Maternity Hospital in New Zealand by Sadler and co-workers found that the cesarean delivery rate was similar in their conventionally managed and actively managed women (9.4% vs. 9.7%), but that women in the AMOL had shorter labors and a lower relative risk for prolonged labor.
|
|
|
TABLE 22.6. Cesarean delivery incidence in randomized studies of active management of labor |
|
|
|
FIG. 22.17. Odds ratio of the effect of active management of labor on cesarean delivery rate. Active management of labor is associated with a lower risk of cesarean delivery in one study but with equivocal results in two studies. |
|
|
|
FIG. 22.18. Odds ratio of the effect of active management of labor on delivery within 12 hours. Active management of labor is associated with delivery within 12 hours of presentation to the labor and delivery units in each study depicted. |
Many lessons can be derived from the AMOL protocol. First, AMOL is a regimented integrated approach to the management of labor in all nulliparous women admitted to the hospital. In many ways, this philosophy runs counter to the concept of individualizing patient care according to each woman's specific situation. However, application of protocols in some situations, as in clinical practice guidelines, leads to more standardized application of appropriate therapies with concomitant improved outcomes. Whereas much has been made of the use of early amniotomy and the relatively high doses of oxytocin employed in AMOL protocols, a detailed analysis by Thorton and Lilford indicates that the most important component of AMOL in achieving a low cesarean birth rate is one-on-one nursing. And perhaps the most important aspect of nursing care in this setting is the alleviation of maternal anxiety and the prompt diagnosis and treatment of dystocia.
AMOL is an excellent example of how an organized approach to labor management can lead to improved outcomes. Although AMOL cannot be adopted in its entirety in all labor and delivery units in the United States, the principles of AMOL can be adapted in many situations. First, normal women at term with uterine contractions should be admitted only when they are in active labor. Obviously, there are exceptions to this concept, but premature admission with interventions usually implies that an induction of labor is being performed for no clear indication. Second, dysfunctional labor should be promptly diagnosed and treated with appropriate medical therapy. Third, efforts to alleviate maternal anxiety through prenatal education and attentive, sympathetic caregivers should be maximized. Unfortunately, labor and delivery units in the United States would find it impossible to provide one-on-one nursing care throughout labor with the current staffing policies of most units. However, more personal interactions with all caregivers, from nurses to obstetricians, should be encouraged. And last, there is little delay in making the decision to move to cesarean delivery, improving both maternal and neonatal outcomes. Although critics of AMOL cite perceived excessive intervention (based on the use and doses of oxytocin), proponents of AMOL counter that a cesarean delivery rate of 20% to 25% versus less than 10% is the greater intervention.
SUMMARY POINTS
· Dystocia is common, particularly in the nulliparous woman, and is a common indication for cesarean delivery.
· Early amniotomy does not improve labor outcomes. However, amniotomy after 5 cm of dilation can shorten the time of labor but at the expense of a modest increase in infectious morbidity.
· Early application of epidural analgesia can contribute to labor abnormalities, particularly in the second stage, and can lead to an increased need for operative vaginal delivery.
· Active management of labor (AMOL) protocols can decrease the cesarean delivery rate in some populations.
· Oxytocin protocols using higher doses (3–6 mU/min and increasing concentrations every 15–20 min) decrease the need for cesarean delivery for dystocia with adequate safety for mother and fetus.
· All authorities agree that the primary goal in managing women in labor is to obtain healthy babies with minimal maternal morbidity. However, the methods used to achieve these goals elicit a great deal of controversy among obstetricians. Nevertheless, following the principles of labor management as outlined in this chapter should ensure good maternal and fetal outcomes.
SUGGESTED READINGS
Keys to the Management of Labor
Creasy RK, ed. Management of labor and delivery. Maulden, MA: Blackwell Science, 1997.
Friedman EA. Labor: clinical evaluation and management, second ed. New York: Appleton, 1978.
Epidemiology of Dystocia
American College of Obstetricians and Gynecologists Task Force on Cesarean Delivery Rates. Evaluation of cesarean delivery. Washington, DC: American College of Obstetricians and Gynecologists, 2000.
Martin JA, Hamilton BE, Ventura SJ, et al. Births: final data for 2000. Hyattsville, MD: National Center for Health Statistics, 2002. National Vital Statistics Reports, Vol. 50, No. 5.
Etiology of Dystocia
Challis JRG. Mechanism of parturition and preterm labor. Obstet Gynecol Surv 2000;55:650–660.
Duff P, Sanders R, Gibbs RS. The course of labor in term patients with chorioamnionitis. Am J Obstet Gynecol 1983;147:391–395.
Moore TM, Iams JD, Creasy RK, et al. Diurnal and gestational patterns of uterine activity in normal human pregnancy. Obstet Gynecol 1994;83:517–523.
O'Driscoll K, Meagher D, Boylan P. Active management of labor: the Dublin experience, third ed. London: Mosby-Yearbook, 1993.
Turner MJ, Rasmussen MJ, Turner JE, et al. The influence of birthweight on labor in nulliparas. Obstet Gynecol 1990;76:159–163.
Epidural Analgesia and Labor Progress
Clark A, Carr D, Loyd G, et al. The influence of epidural analgesia on cesarean delivery rates: a randomized, prospective clinical trial. Am J Obstet Gynecol1998;179:1527–1533.
Holt RO, Diehl SJ, Wright JW. Station and cervical dilation at epidural placement in predicting cesarean risk. Obstet Gynecol 1999;93:281–284.
Impey L, MacQuillan K, Robson M. Epidural analgesia need not increase operative delivery rates. Am J Obstet Gynecol 2000;182:358–363.
Morton SC, Williams MS, Keeler EB, et al. Effect of epidural analgesia for labor on the cesarean delivery rate. Obstet Gynecol 1994;83:1045–1052.
Sizer AR, Nirmal DM. Occipitoposterior position: associated factors and obstetric outcome in nulliparas. Obstet Gynecol 2000;96:749–752.
Traynor JD, Dooley SL, Seyb S, et al. Is the management of epidural analgesia associated with an increased risk for cesarean delivery? Am J Obstet Gynecol2000;182:1058–1062.
Zhang J, Klebanoff MA, DerSimonian R. Epidural analgesia in association with duration of labor and mode of delivery: a quantitative review. Am J Obstet Gynecol 1999;180:970–977.
Options for the Management of Dystocia
Dujardin B, De Schampheleire I, Sene H, et al. Value of the alert and action lines on the partogram. Lancet 1992;339:1336–1338.
Fraser WD, Marcoux S, Krauss I, et al, for the Pushing Early or Pushing Late with Epidural Study Group. Multicenter, randomized, controlled trial of delayed pushing for nulliparous women in the second stage of labor with continuous epidural analgesia. Am J Obstet Gynecol 2000;182:1165–1172.
Fraser WD, Marcoux S, Moutquin JM, et al. Effect of early amniotomy on the risk of dystocia in nulliparous women. N Engl J Med 1993;328:1145–1149.
Hansen SL, Clark SL, Foster JC. Active pushing versus passive fetal descent in the second stage of labor: a randomized controlled trial. Obstet Gynecol2002;99:29–34.
Lucidi RS, Chez RA, Creasy RK. The clinical use of intrauterine pressure catheters. J Maternal-Fetal Med 2001;10:420–422.
Merrill DC, Zlatnik FJ. Randomized, double-masked comparison of oxytocin dosage in induction and augmentation of labor. Obstet Gynecol 1999;94:455–463.
Philpott RH, Castle WM. Cervicographs in the management of labor in primigravidae: II. The action line and treatment of abnormal labor. J Obstet Gynecol Br Commonw 1972;79:599–602.
Rouse DJ, Owen J, Hauth JC. Active-phase labor arrest: oxytocin augmentation for at least 4 hours. Obstet Gynecol 1999;93:323–328.
Rouse DJ, Owen J, Savage KG, et al. Active phase labor arrest: revisiting the 2-hour minimum. Obstet Gynecol 2001;98:550–554.
Satin AJ, Leveno KJ, Sherman ML, et al. High- versus low-dose oxytocin for labor stimulation. Obstet Gynecol 1992;80:111–116.
Satin AJ, Leveno KJ, Sherman ML, et al. High-dose oxytocin: 20- versus 40-minute dosage interval. Obstet Gynecol 1994;83:234–238.
Seitchik J, Castillo M. Oxytocin augmentation of dysfunctional labor. I. Clinical data. Am J Obstet Gynecol 1982;144:899–905.
U.K Amniotomy Group. A multicenter randomized trial of amniotomy in spontaneous first labor at term. Br J Obstet Gynecol 1994;101:307–309.
Xenakis EMJ, Langer O, Piper JM, et al. Low-dose versus high-dose oxytocin augmentation of labor—a randomized trial. Am J Obstet Gynecol1995;173:1874–1878.
Active Management of Labor
Frigoletto RD, Leiberman E, Lang JM, et al. A clinical trial of active management of labor. N Engl J Med 1995;333:495–490.
Glantz JC, McNanley TJ. Active management of labor: a meta-analysis of cesarean delivery rates for dystocia in nulliparas. Obstet Gynecol Surv1997;52:497–505.
Lopez-Zeno J, Peaceman AM, Adashek JA, et al. A controlled trial of a program for the active management of labor. N Engl J Med 1992;326:450–454.
Rogers R, Gibson GJ, Miller AC, et al. Active management of labor: does it make a difference? Am J Obstet Gynecol 1997;177:599–605.
Sadler LC, Davison T, McCowan LME. A randomized controlled trial and meta-analysis of active management of labor. BJOG 2000;107:909–915.
Thorton JG, Lilford RJ. Active management of labor: current knowledge and research issues. Br Med J 1994;309:366–369.