T. Flint Porter
James R. Scott
Cesarean section is a term commonly used in obstetrics to describe the delivery of a viable fetus through an incision in the abdominal wall (laparotomy) and the uterus (hysterotomy). However, the words cesarean and section used together are redundant, because both imply incision. Cesarean birth and cesarean delivery are preferable terms and are used interchangeably in this chapter.
Cesarean delivery has played a major role in lowering both maternal and perinatal morbidity and mortality rates during the past century. The initial purpose of the surgery was to preserve the life of the mother with obstructed labor, but indications have expanded over the years to include delivery for a variety of more subtle dangers to the mother or the fetus. Contributing to its more frequent use is its increased safety, which is largely a result of better surgical technique, improved anesthesia, effective antibiotics, and availability of blood transfusions. Nevertheless, there has been increasing concern over what is considered by many to be an excessive cesarean rate in contemporary obstetrics.
The percentage of babies in the United States delivered by cesarean dramatically increased from less than 5% in 1965 to 25% in 1990. The reasons for this striking increase are multiple. During the 1970s and 1980s, it was assumed that cesarean delivery would be the solution to numerous obstetric problems. Facing increasing medical-legal pressures, obstetricians gradually abandoned most vaginal breech and forceps deliveries, broadened the definition of intrapartum fetal distress, and liberalized the diagnosis of dystocia. Also, a greater number of older women and older primigravidae, whose primary cesarean rates are higher, were having children. Finally, the escalation in primary cesareans increased the overall cesarean rate, because in most subsequent pregnancies, babies were delivered by repeat cesarean.
Although perinatal outcome in the United States improved during the period when the cesarean rate increased, it also improved in other countries where cesarean rates remained low. Moreover, the incidence of cerebral palsy has not declined during the past 20 years because perinatal morbidity and mortality are more often a function of antepartum events, abnormal fetal growth, congenital anomalies, and premature birth. Delivery by cesarean usually is associated with an increased cost for the health care system and the patient when compared with vaginal birth. These factors have led to efforts to reduce the rate of cesarean delivery. Most emphasis has been placed on decreasing the number of repeat cesareans by encouraging vaginal birth after cesarean (VBAC). Accordingly, the percentage of women attempting VBAC increased from less than 10% in 1988 to about 30% in 1996. During this same period, the percentage undergoing cesarean declined to about 20%. Unfortunately, initial enthusiasm for VBAC has been dampened by the results from several studies showing adverse maternal and perinatal outcomes in some women who attempted it. In turn, this has led to a steady decline in the number of women attempting VBAC and an increase in the overall cesarean rate to about 24%.
INDICATIONS
Cesarean birth is necessary whenever labor is unsafe for either mother or fetus, when labor cannot be induced, when dystocia or fetal problems present significant risks with vaginal delivery, and when an emergency mandates immediate delivery. It is not practical to list all potential indications for cesarean delivery or to discuss the numerous changes in obstetric management that have influenced these over the years (Table 24.1). Many indications are well accepted, a number are subjective or selectively applied in individual patients, and others are more controversial. The majority of cesareans are performed for fetal indications, a few are solely for maternal reasons, and some benefit both fetus and mother. Repeat cesarean accounts for approximately 30% of cesarean deliveries in the United States, dystocia is the indication for up to 30%, and fetal distress, breech, and other conditions are responsible for the remaining cases.
|
|
|
TABLE 24.1. Common indications for cesarean delivery |
Labor Contraindicated
Uterine contractions can be hazardous to the mother under certain circumstances. These include central placenta previa, previous classic uterine incision, myomectomy transecting the uterine wall, or uterine reconstruction. In these situations, labor and vaginal delivery may result in uterine rupture and hemorrhage, endangering the life or future health of the mother. Conditions in which labor is dangerous to the fetus include placenta previa, velamentous insertion of the cord or other forms of vasa previa, and cord presentation. More recent indications include treatable fetal anomalies such as meningomyelocele and certain degrees of hydrocephaly.
Failed Induction
Conditions such as alloimmunization, diabetes mellitus, intrauterine growth retardation, and hypertensive disorders constitute a threat to the mother or fetus and often require delivery when the cervix is unfavorable for induction. If attempts to induce labor are inappropriate or unsuccessful, cesarean birth is the only alternative. This is especially true in nulliparous women. More effective methods of softening the cervix before inducing labor preterm may reduce the need for cesarean.
Dystocia
Mechanical problems of the uterus, fetus, or birth canal or ineffective uterine contractions that result in unsuccessful progress of labor and vaginal delivery are referred to collectively as dystocia. This term encompasses a variety of commonly used clinical terms, such as failure to progress, cephalopelvic disproportion (CPD), and dysfunctional labor. However, CPD is a relative term. Although fetal macrosomia sometimes causes CPD, most cesarean births for abnormal labor involve a normal-sized infant. Dystocia occasionally is also caused by soft tissue tumors and abnormal fetal presentations.
Intrapartum Fetal Heart Rate Abnormalities
Electronic fetal monitoring improves the chance of detecting fetal compromise, but its inaccuracy (false-positive rate) has also contributed to the increased number of cesarean births. Nonreassuring fetal heart rate patterns and the diagnosis of fetal distress are discussed elsewhere. Many clinicians have replaced vaginal breech deliveries with cesarean delivery to avoid the risk of intrapartum asphyxia or delivery-related trauma from head entrapment and umbilical cord prolapse. An increase in adverse perinatal outcome with singleton vaginal breech delivery was confirmed in one large randomized controlled trial.
Maternal or Fetal Emergency
Certain maternal or fetal conditions require immediate delivery of the baby because vaginal delivery is either impossible or inappropriate. Such circumstances include severe placental abruption, hemorrhage from placenta previa, prolapse of the umbilical cord, active genital herpes, and impending maternal death.
COMPLICATIONS
A variety of postpartum complications—including unexplained fever, endometritis, wound infection, hemorrhage, aspiration, atelectasis, urinary tract infection, and venous thromboembolism—occur in up to 25% of women who undergo cesarean delivery. The frequency of cesarean-related maternal death varies with the institution and with the condition necessitating the procedure. However, rates are less than 1 per 1,000 operations, and many deaths are related to an underlying maternal illness or anesthetic complications.
Late maternal complications of cesarean delivery include intestinal obstruction from adhesions, dehiscence of the uterine incision in subsequent pregnancies, and abnormal myometrial invasion of the placenta (accreta, increta, percreta) in subsequent pregnancies. Both intestinal obstruction and scar dehiscence are more common with the classic incision than with a lower uterine segment incision. The incidence of abnormal myometrial invasion by the placenta (accreta, increta, percreta) increases with each cesarean and can result in severe and intractable hemorrhage at delivery, often requiring cesarean hysterectomy. This should be suspected in all women with a placenta previa and a history of cesarean.
TYPES OF CESAREAN OPERATIONS
Almost all contemporary cesareans are performed using a transperitoneal approach to reach the uterine wall. An extraperitoneal technique was sometimes used in the past in patients with an infected uterus in an attempt to reduce the chance of peritonitis. More effective antibiotics have now made this approach unnecessary.
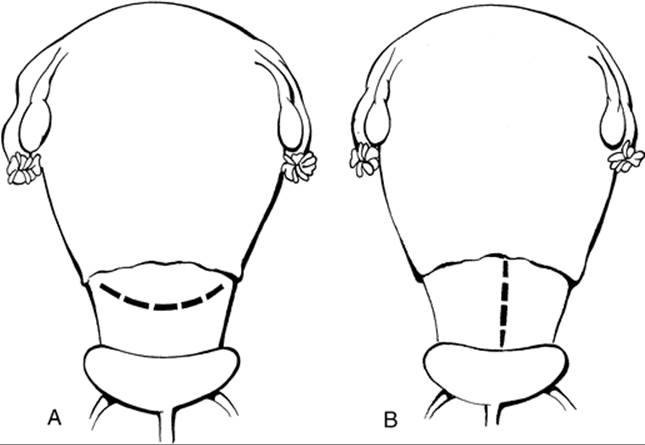
The two major types of cesarean operations are classified by the location and direction of the uterine incision. The first are those incisions made in the upper segment of the uterus (Fig. 24.1). The vertical incision usually made in the anterior fundus is referred to as a classic incision. It is used primarily when it is difficult to deliver the infant through a low uterine segment incision. The second type is characterized by incisions made in the lower portion of the uterus after the bladder has been displaced downward (Fig. 24.2). The preferred and most frequently used is the low transverse incision. A vertical incision may also be made in this area, but it usually involves the upper uterine segment unless the lower segment is quite elongated by labor.
|
|
|
FIG. 24.1. Classic cesarean incision in the upper segment of the uterus. |
|
|
|
FIG. 24.2. Incisions in lower uterine segment. A: Low transverse incision. B: Low vertical incision. |
Occasionally, variations are used because of unanticipated difficulty (Fig. 24.3). These incisions are best avoided by careful assessment and planning. A J-shaped incision is made when the obstetrician begins a transverse lower uterine segment incision and finds the lower uterine segment to be too narrow. It often is not realized that the incision is inadequate until delivery is attempted. A vertical extension from one end is necessary to avoid extension into the broad ligament. The T-shaped incision is made for similar reasons.
|
|
|
FIG. 24.3. Undesirable variations of uterine incisions. A: J-shaped incision. B: T-shaped incision. |
ANESTHESIA
The choice of anesthetic technique and agents is dictated by a number of factors, as discussed elsewhere in Chapter 3. Most patients requiring immediate delivery because of fetal distress, hemorrhage, or shock are not candidates for spinal or epidural anesthetic techniques. The same is true for women with previous injury or surgery to the spine, skin infections of the lower back, or coagulopathy. Conversely, patients with active pulmonary disease, such as pneumonia or tuberculosis, or in whom intubation is judged difficult, are not good candidates for inhalation anesthesia.
The choice between regional block and inhalation anesthesia should be discussed among the patient, anesthesiologist, and obstetrician and should be based on the urgency of delivery, patient choice, and skill of the anesthesiologist.
Regional anesthesia has the potential to adversely affect maternal and fetal hemodynamics. In the dorsal recumbent position, the gravid uterus compresses the inferior vena cava, resulting in decreased venous return and maternal cardiac output and, eventually, hypotension and reduced uterine perfusion. This is referred to as the inferior vena cava syndrome. The weight of the pregnant uterus progressively compresses the aorta as the mean arterial pressure falls, thus also reducing blood flow to the pelvis. Hypotension produced by regional anesthetic techniques compounds this problem. Devices attached to the operating table, inflatable wedges or towels placed under the patient, or tilting the table can be used to displace the uterus to the patient's left in preparation for cesarean delivery. Rapid intravenous infusion of physiologic solution containing sodium immediately before the initiation of regional anesthesia also reduces the incidence of hypotension.
The status of the fetus worsens as the time of exposure to anesthesia lengthens. Progressive fetal depression as induction-to-delivery time is prolonged makes it important to avoid unnecessary delay before and during surgery. The abdomen should be fully prepped, draped, and ready for the incision before general anesthesia is induced. On the other hand, reckless surgical techniques for rapid delivery of the fetus are unwise. An induction-to-delivery time of 5 to 15 minutes is reasonable if maternal oxygenation, blood pressure, and displacement of the uterus are monitored and maintained.
OPERATIVE PROCEDURE
Preparation
Cesarean delivery requires the same preoperative care as any major surgery plus additional consideration for the status of the fetus. A patient who is dehydrated from prolonged labor needs volume correction with intravenous fluids. Because anemia is relatively common in pregnancy, a hemoglobin or hematocrit level should be checked preoperatively. Blood is typed and screened to be available for immediate transfusion. Routine preparation of autologous blood is not cost effective for most cesarean patients, because few are transfused. However, autologous blood can be prepared during the antepartum period if the patient is at high risk for hemorrhage as with placenta previa or accreta. Because the bladder will be in the operative field, it is necessary to place an indwelling catheter before beginning surgery. The patient and her partner should be given an explanation of the details of the operation, the reason it is necessary, and the risks involved. Informed written permission for the procedure, anesthetic, administration of blood, and possible hysterectomy, if necessary, is then signed by the patient.
With elective repeat cesarean delivery, it is the obligation of the physician to obtain evidence of fetal maturity. Documentation by noninvasive techniques is outlined in Table 24.2. If the criteria confirm gestational age assessment on the basis of menstrual dates in a patient with normal menstrual cycles and no immediately antecedent use of oral contraceptives, delivery can be scheduled after 39 weeks by menstrual dates. Ultrasonography is considered confirmatory of menstrual dates if there is gestational age agreement within 1 week by crown-rump measurement obtained at 6 to 11 weeks, or within 10 days by the average of multiple measurements obtained at 12 to 20 weeks. When the fetal gestational age remains uncertain, amniocentesis for amniotic fluid studies should be employed to ensure fetal maturity. Awaiting the onset of spontaneous labor is another option.
|
|
|
TABLE 24.2. Fetal maturity assessment before elective repeat cesarean delivery |
Aspiration of the acidic contents of the stomach, a known risk of general anesthesia in pregnant women, can be avoided by pretreatment with any of several medications. Prophylactic antibiotics are administered to reduce the risk of postpartum infection, which is increased with prolonged labor, prolonged rupture of the membranes, and numerous cervical examinations. A single dose of a broad-spectrum antibiotic, such as 1 g of a cephalosporin, usually is given after the umbilical cord has been clamped. However, if an intrapartum infection is apparent preoperatively, therapeutic antibiotics should be given before surgery and continued postoperatively. Preparation of the abdomen includes scrubbing the skin with soap and an antiseptic agent such as nonorganic iodide. The abdomen is then draped, leaving the area for the incision exposed. Personnel trained in neonatal resuscitation should be available.
Surgical Technique
A lower abdominal midline vertical incision and the transverse Pfannenstiel incision are used most commonly for cesarean deliveries. The vertical incision minimizes blood loss and allows extension above the umbilicus, if necessary. It also allows for rapid access to the abdominal cavity because of diastasis of the rectus muscles, common in late pregnancy. Nevertheless, the transverse Pfannenstiel incision is used more frequently because of the cosmetic result preferred by most women. Entry through this incision is relatively rapid in experienced hands, visualization of the pelvis is adequate, and there may be less risk of subsequent herniation.
The abdomen is opened in layers, and any large bleeding vessels are clamped. Meticulous hemostasis is postponed if it will unduly delay delivery of the fetus. The abdominal cavity is inspected briefly, and the direction and degree of rotation of the uterus are noted. Retractors are placed in the abdominal incision for better visualization. The bladder is dissected carefully away from the serosa of the uterus and a small transverse incision is made in the midline of the uterus, a few centimeters below the peritoneal incision (Fig. 24.4A, Fig. 24.4B, Fig. 24.4C, Fig. 24.4D and Fig. 24.4E). Care should be taken to keep the fetal membranes intact. Under direct vision, the incision is extended laterally with bandage scissors in a gentle upward curve using the operator's fingers as a guide (Fig. 24.4F).
|
|
|
FIG. 24.4. Cesarean delivery. A: Reflection of peritoneum from the serosa of the uterus to the bladder is identified. B: Peritoneal reflection between the uterus and bladder is elevated and incised. C: The bladder is displaced away from the lower uterine segment. D: The bladder is retracted, and the incision is planned to be 2 to 3 cm below the peritoneal incision. E: A small incision is made through the uterine wall to the fetal membranes. F: A uterine incision is made in a curvilinear shape, using bandage scissors. G: The fetal head is elevated through the uterine incision by the operator's hand. |
An alternative method of opening the uterus in a woman with an adequately developed lower uterine segment is to make a shallow curvilinear incision through the pubocervical fascia to the fetal membranes. Inserting both index fingers into the opening, the operator pulls laterally, bluntly opening the uterus. The operator ruptures membranes and inserts one hand beneath the lower edge of the uterine incision to feel the presenting fetal part. If vertex, the occiput is identified, and the head is flexed and brought into the uterine incision (Fig. 24.4G). The assistant or operator exerts fundal pressure to deliver the fetal head gently through the incision, after which an assistant suctions the mouth and nares with a bulb syringe while the operator continues to deliver the shoulders gently in a manner similar to that of a vaginal delivery. Specially designed forceps or a vectis also can be used to deliver the head through the uterine incision.
After delivery, the umbilical cord is clamped and divided, and the infant is handed off the operative field. Although spontaneous delivery of the placenta is preferable, it may be removed manually by blunt separation from the uterine wall. The uterine cavity is inspected for any structural abnormality, and retained placental tissue and membranes are removed. Dilation of the endocervical canal from above is usually unnecessary. Following delivery of the placenta, oxytocin should be administered to stimulate uterine contractions and reduce bleeding.
The cut edges of the uterine incision may be grasped with ring forceps or other noncrushing clamps for traction and to control bleeding. The uterine incision may be closed with a one-layer or two-layer technique (Fig. 24.5A and Fig. 24.5B). With the exception of a shorter operating time using the one-layer technique, neither has been found superior to the other. Persistent bleeding in the incision line may be controlled with interrupted figure-of-eight sutures or electrocautery. Inspection of the uterine incision and surrounding organs should be followed by removal of abdominal packs and lavage and suctioning to remove any residual blood, amniotic fluid, or meconium. If desired, surgical sterilization via tubal ligation may be performed at this point. It adds little time or morbidity to cesarean delivery and does not significantly prolong postpartum recovery. The Pomeroy method is the simplest sterilization technique and gives satisfactory results.
|
|
|
FIG. 24.5. Wound closure. A: First layer of closure. B: Second layer of closure. |
The abdominal incision is closed most commonly with a delayed-absorbable synthetic suture, although a nonabsorbable suture is also acceptable in high-risk groups. A mass-layer closure should be considered for vertical incisions, especially in patients at high risk of disruption.
Postoperative management is similar to that of any patient who has had major surgery, including removal of the urinary catheter on the first postoperative day, oral feedings advanced as tolerated, and early ambulation to avoid thromboembolism. Most women are ready for discharge on the third postoperative day, although hospitalization should be continued if clinically indicated and documented by the physician in the patient's record.
Closure of the Classic Incision
The thickness of the upper uterine wall sometimes requires a three-layer closure to and including the serosa. Continuous suture techniques may be used, but interrupted sutures frequently give a more exact closure. The first layer should include about half the thickness of the wall and can be continuous or figures-of-eight. A second continuous layer is placed to avoid leaving a space between the layers. The third layer should close the serosa in a manner that minimizes exposed raw surfaces using continuous, unlocked absorbable suture. Each bite of the needle should begin on the raw surface of the wound and exit through the serosa a few millimeters from the cut edge. With this technique, sometimes referred to as a baseball stitch, the cut edge is infolded, and the serosa is on the surface.
Techniques for Difficult Cesarean Deliveries
After a prolonged obstructed labor, the fetal head often is impacted in the midpelvis. Manipulation of an impacted fetal head may result in damage to a thinned and elongated lower uterine segment, with extension of the incision into the cervix or broad ligament and laceration of uterine vessels. The vaginally placed hand of an assistant pushing upward can facilitate dislodgement of the fetal head.
Most malpresentations can be delivered safely through a low transverse uterine incision extended widely to deliver the aftercoming head. However, this may impossible with a preterm malpresentation or other circumstances such as placenta previa. If the lower uterine segment is too narrow to accommodate a transverse incision, a vertical incision should be performed, even if it extends into the uterine corpus.
Incision of the uterus through the maternal surface of the placenta can result in considerable hemorrhage. The operator should continue quickly to extend the incision for delivery of the fetus but not cut or fracture the placenta, because disruption of chorionic vessels may result in fetal hemorrhage. Instead, the placenta should be separated from the uterine wall to allow access to the fetal membranes so that rupture may occur and the fetus may be delivered. Occasionally, an internal podalic version and breech extraction are necessary.
POSTMORTEM CESAREAN DELIVERY
Most obstetricians will never be forced to decide whether or not postmortem cesarean is necessary. Nevertheless, all should be familiar with the general principles. First, the certainty of maternal death must be clinically established quickly and preferably confirmed by electrocardiographic or electroencephalographic findings. Documentation of fetal well-being before deciding on delivery may give erroneous information, because the time from apparent fetal death to actual fetal death or serious damage is unknown. Second, the abdomen and uterus should be opened rapidly, ignoring aseptic precautions. Third, the fetus must be delivered quickly, given immediate resuscitation, and transferred to an intensive care nursery. Finally, the placenta should be removed and the uterus and abdomen closed.
The outlook for the infant is improved if delivery occurs before maternal death, and survival continues to be possible if delivery is accomplished within 10 minutes of maternal death. Unfortunately, the degree of damage from cerebral hypoxia is difficult to predict and the prognosis for the fetus is usually ominous. Uncommonly, a mother who opposes fetal intervention dies before giving birth, thereby presenting the obstetrician with an ethical dilemma.
PRIMARY ELECTIVE CESAREAN
Performing a cesarean delivery solely because the patient desires to avoid labor would have seemed unthinkable 20 years ago. However, in recent years a growing number of patients and physicians have supported the notion that women have the right to choose elective cesarean rather than go through the rigors of labor, regardless of any obstetric or medical indication. Proponents reason that women have the right to choose their method of delivery because of the inconveniences of unscheduled labor and the possibility that vaginal delivery may result in pelvic support disorders. The practice of performing primary cesarean delivery for these reasons has gained wide acceptance in some parts of the world among women of higher socioeconomic status.
Although cesarean delivery in modern obstetrics is considered a safe procedure, recovery time and the risk of thromboembolic episodes and infections are still higher with cesarean birth than with vaginal birth. Furthermore, although most elective surgeries are done only once, a primary cesarean often is followed by repeat cesarean deliveries, with morbidity increasing with each birth. The risks of complications such as uterine rupture, placenta previa, and placenta accreta increase proportionately with the number of cesareans performed. All may result in severe hemorrhage, postpartum hysterectomy, urologic and bowel injury, and even maternal death.
The controversy surrounding primary elective cesarean delivery will not be resolved unless adequate controlled studies are performed. Until that time, the decision to perform cesarean delivery on demand should be made only after careful consideration of all of the risks involved.
VAGINAL BIRTH AFTER PREVIOUS CESAREAN
The rising number of women undergoing elective repeat cesarean has been one of the principal reasons for the steady increase in the cesarean delivery rate in the United States during the last 30 years. Not surprisingly, several governmental and professional organizations have advocated a trial of labor (TOL) in all women with a prior cesarean. Based on the results of early studies comparing VBAC with repeat cesarean, VBAC appeared to be successful in 60% to 80% of women undergoing TOL. Uterine rupture, the most serious potential complication of attempted VBAC, appeared to be a rare event with few consequences. However, the results of more recent prospective trials indicate that a decision to undergo a TOL after previous cesarean is not as straightforward as it once seemed.
Safety
Most of the emerging body of literature comparing VBAC with repeat cesarean suggests that a TOL should be offered to thoughtfully selected candidates. Contraindications include a classic scar, a low vertical scar that extends into the upper segment of the uterus, previous uterine rupture, and a T-shaped scar. Other factors that may increase the likelihood of uterine rupture include two or more prior cesarean deliveries, macrosomia, induction of labor, the presence of müllerian anomalies, and postdatism. The patient should be aware that problems could arise during her pregnancy that could necessitate repeat cesarean delivery.
Some minor complications may be more common in women who undergo repeat cesarean. However, the most recent meta-analysis of retrospective and prospective series comparing VBAC with repeat cesarean has showed that most major complications are more likely for women who attempt VBAC (Fig. 24.6). Most complications occur in women with a failed TOL, especially if an emergency cesarean is necessary.
|
|
|
FIG. 24.6. Odds ratio graph comparing morbidity of trial of labor versus elective repeat cesarean delivery. |
The degree of perinatal morbidity and mortality after a failed TOL, especially in cases of uterine rupture, has been under-appreciated until recently (see Fig. 24.6). In theory, fetal damage is minimized if delivery can be accomplished expeditiously. However, fetal damage can occur even if delivery occurs less than 18 minutes after uterine rupture. Furthermore, immediate delivery requires around-the-clock in-hospital obstetric and anesthesia coverage, typically available only in large university or tertiary level centers. In one survey, anesthesiologists were available in-hospital on nights and weekends in only 26% of hospitals with 500 to 1,499 births per year, and in only 3% of those with fewer than 500 births per year. Although the absolute risk of perinatal death associated with VBAC is low (12.9 per 10,000), it is significantly greater than with elective cesarean, especially if uterine rupture occurs.
Success of Labor
In most published series, 60% to 80% of women who attempt VBAC have successful vaginal births. However, many of these studies have included only women who meet strict inclusion criteria, excluding those who otherwise would be considered VBAC candidates in clinical practice. Based on the available evidence, the probability of successful VBAC for women whose first cesarean was done for a nonrecurring indication is similar to the probability of vaginal delivery in all laboring patients. Moreover, their probability of success is improved if they also have had a previous vaginal delivery, regardless of whether or not it was before their first cesarean birth or was a successful VBAC. In contrast, successful VBAC is less likely for women whose primary cesareans were performed for labor dystocia (50%–70%).
Vaginal Birth After Cesarean in Obstetric Practice
Counseling Potential Candidates for VBAC
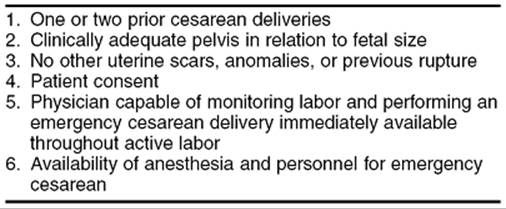
Only women who meet specific criteria and who can deliver in appropriate facilities should be offered VBAC (Table 24.3). Initial evaluation includes a search for contraindications to VBAC and review of medical records if the type of previous incision is unknown (Table 24.4). Once this evaluation is complete, thorough, impartial, and factual counseling should be given and reviewed at intervals during pregnancy. Notably, the probability of achieving a successful VBAC and the magnitude of the maternal and perinatal risks associated with a failed TOL should be discussed with each potential candidate and documented in the prenatal record. Support and encouragement should be given regardless of the decision made. Global mandates for TOL after previous cesarean are inappropriate, because individual risk factors are not considered.
|
|
|
TABLE 24.3. Criteria for vaginal birth after cesarean |
|
|
|
TABLE 24.4. Contraindications to vaginal birth after cesarean |
Intrapartum Management
A TOL after previous cesarean should be conducted in facilities where anesthesia, obstetric, and blood bank personnel are immediately available. Each hospital should develop a protocol for management of VBAC (Fig. 24.7). One reasonable approach to the initial evaluation of a woman attempting VBAC includes the following measures:
|
|
|
FIG. 24.7. Flow sheet showing one management scheme for vaginal birth after cesarean. |
· Intravenous access on admission
· Blood count, type and screen
· Nothing by mouth
· Continuous electronic fetal monitoring
· Alert anesthesia, obstetric, and neonatal personnel
Once labor has begun, women attempting VBAC should be frequently evaluated and monitored. Most authorities recommend continuous electronic fetal heart rate monitoring during labor. Personnel who are familiar with the potential complications of VBAC should be present to watch closely for fetal distress and inadequate progress of labor.
Induction and Augmentation
Spontaneous labor is preferable to labor induction and augmentation in any woman who is attempting a TOL after a previous cesarean delivery. Several series have documented increased rates of failure, as well as uterine rupture, in women who have had a previous cesarean and who are undergoing labor induction or augmentation, especially if prostaglandin preparations are employed as cervical ripening agents. The use of misoprostol is of particular concern.
Analgesia
There are few contraindications to epidural anesthesia, and adequate pain relief may encourage a greater number of women to choose TOL over repeat cesarean. Epidural analgesia rarely masks the signs and symptoms of uterine rupture, and success rates for VBAC are similar to those experienced by women who receive other types of pain relief.
Uterine Rupture
Uterine rupture, the most serious complication of VBAC, is often life threatening for both mother and baby. Incomplete or partial rupture refers to an opening of the previous scar but not the overlying peritoneum. This includes extrusion of intrauterine contents into the broad ligament. A complete rupture is a separation of the previous scar and overlying peritoneum with extrusion of intrauterine contents into the abdominal cavity. Scar dehiscence is defined as an opening of the previous scar with intact overlying visceral peritoneum and no expulsion of intrauterine contents (also termed a window).
Intrapartum uterine ruptures requiring emergency treatment occur in approximately 0.5% of patients with a transverse low-segment scar. The rupture usually involves the old scar and lower uterine segment but may be stellate and extend intraperitoneally or retroperitoneally. Contributing factors include induction with oxytocin or prostaglandin preparations, dysfunctional labor, more than one prior cesarean delivery, high parity, and even previous perforation of the nonpregnant uterus by curettage, hysteroscopy, metroplasty, and myomectomy.
Diagnosis
The signs and symptoms of uterine rupture may be surprisingly subtle. However, the diagnosis soon becomes apparent as the maternal or fetal condition, or both, deteriorate. Fetal heart rate pattern abnormalities are identified with uterine rupture most consistently, although none is specific. A common scenario involves variable decelerations that evolve rapidly into late decelerations, bradycardia, and undetectable fetal heart tones (Fig. 24.8). Hence, all fetal heart rate pattern abnormalities exhibited by women attempting VBAC should be investigated thoroughly.
|
|
|
FIG. 24.8. Fetal heart rate tracing shows changes in pattern during uterine rupture. |
Other clinical findings of uterine rupture include uterine or abdominal pain, which usually occurs in the area of the previous incision, may range from mild to severe, and sometimes is described as a tearing sensation. Uterine contractions often diminish in intensity and frequency, although no rupture-specific pattern has been identified. Vaginal or intraabdominal bleeding is associated with anxiety, restlessness, weakness, dizziness, gross hematuria, shoulder pain, and shock. Loss of station of the presenting part is diagnostic but not essential for the diagnosis.
Management
Women who are suspected of having uterine rupture should undergo immediate exploratory laparotomy and cesarean delivery. Perinatal outcome is dependent on the severity of the rupture and its relationship to the placenta and umbilical cord. Damage to the placenta or umbilical cord may lead quickly to hypoxemia, permanent end-organ dysfunction, and fetal death. Fetal extrusion into the abdominal cavity is particularly detrimental. Once delivery has been accomplished, repair of the uterine defect is possible in many cases and may be considered if it appears technically feasible, if the patient wants to retain fertility, or if her condition is not jeopardized by continued hemorrhage. The wound edge should be debrided before reapproximation followed by closure similar to that used for cesarean delivery. Hysterectomy is required if there has been extension into the broad ligament vessels, extensive damage to the uterine myometrium, or in the presence of placenta accreta.
Pregnancies After Uterine Rupture
If the site of the ruptured scar is confined to the lower segment, the rate of repeat rupture or dehiscence in labor is 6%. In contrast, if the upper segment is involved, the rate jumps to 32%. Therefore, women with prior uterine rupture are best delivered by repeat cesarean as soon as the fetus is mature or at 36 to 37 weeks of gestation, before the onset of labor.
CESAREAN HYSTERECTOMY
Indications
Occasionally, hysterectomy must be performed immediately after cesarean or vaginal delivery. A useful classification is based on emergency indications (e.g., uterine rupture, uncontrollable uterine hemorrhage, placenta accreta, uterine infection) and nonemergency indications (e.g., for significant uterine pathology such as carcinoma in situ or uterine leiomyomas).
Emergency Indications
Uncontrollable uterine hemorrhage may result from uterine rupture, uterine atony, placenta accreta, placental site sinusoids after placenta previa, or a coagulation defect. When surgery is indicated to control hemorrhage of uterine origin, the patient's desire to preserve childbearing capacity and the current danger are assessed. Nonsurgical management is indicated in such circumstances as uterine atony and coagulation defect. Bimanual uterine massage, oxytocin, prostaglandin administration, and blood replacement should be used before surgical intervention is considered. Hemorrhage from lower uterine segment venous sinuses associated with placenta previa sometimes can be controlled with mattress or figure-of-eight 2-0 to 0 absorbable sutures. With uterine atony, surgical interruption of the arterial flow to the uterus may be tried as the first measure of control. The operator may proceed to bilateral ligation of the hypogastric or the uterine arteries. If this is not efficacious, hysterectomy may be necessary.
Hysterectomy can also be lifesaving as treatment of severe uterine infection. The patient who has experienced a second-trimester septic abortion with septic shock, peritonitis, or uterine perforation may be saved by prompt hysterectomy. Clostridial infection, dehiscence of a classic incision with uterine infection, or a severe uterine infection unresponsive to antibiotics should also be treated by hysterectomy.
Nonemergency Indications
The risks and benefits of hysterectomy for nonemergency indications are much less certain than for emergency conditions. Hysterectomy performed at term is associated with hemorrhage, infection, thromboembolism, and injury to contiguous organs. The declining use of hysterectomy despite an increase in the incidence of cesarean delivery reflects a generally accepted conservative approach in most situations. Tubal ligation is a safer operation at term than is hysterectomy. When carcinoma in situ must be treated, removal of the cervix at the time of hysterectomy is much more certain and technically less complicated in the nonpregnant state. The decision to perform a nonemergency hysterectomy requires good judgment, which is based on existing skills, facilities, and the needs of the individual patient.
Procedure
The technique for hysterectomy is described elsewhere, but some points are especially pertinent to its performance immediately after cesarean or vaginal delivery. In general, blood is conserved if the uterine wound for cesarean delivery is closed rapidly before beginning the hysterectomy. Normal ovaries should be preserved, and the operator should be aware that the relative shortening of the uteroovarian ligament at term necessitates extra care in the placement of clamps and sutures in this area. The increased vascularity of the pregnant uterus requires considerable care in the correct placement of clamps and sutures.
In the uterus at term, palpation of the portio of the cervix is often difficult, and portions of the cervix may be left behind inadvertently at the time of hysterectomy. This may be avoided by vaginal placement of easily palpated clips or clamps on the cervix prior to surgery. Alternatively, a vertical incision can be made in the lower uterine segment and extended caudad until the limits of the cervix are identified. Drainage of the pelvic cavity may be necessary, depending on the adequacy of hemostasis. In emergent situations or when the patient is unstable, a supracervical hysterectomy is simpler and quicker and may be preferable to total hysterectomy.
SUMMARY POINTS
· Cesarean delivery has played a major role in lowering both maternal and perinatal morbidity and mortality.
· Cesarean birth is necessary whenever labor is unsafe for either mother or fetus, when labor cannot be induced, when dystocia or fetal problems present significant risks with vaginal delivery, and when an emergency mandates immediate delivery.
· A variety of postpartum complications—including unexplained fever, endometritis, wound infection, hemorrhage, aspiration, atelectasis, urinary tract infection, and venous thromboembolism—occur in up to 25% of women who undergo cesarean delivery.
· The risk of late complications of cesarean, including uterine rupture, placenta previa, and placenta accreta, is directly proportional to the number of previous cesarean deliveries.
· The preferred and most frequently used is the low transverse incision.
· The decision to perform cesarean delivery on demand should be made only after careful consideration of all of the risks involved.
· A TOL after cesarean is safest in patients with only previous low transverse incisions.
· A TOL after cesarean preferably is undertaken in facilities where an immediate emergent cesarean can be performed.
· Women whose primary cesarean was performed for a nonrecurring condition have a better chance of success than women whose primary cesarean was performed for labor dystocia.
· Major complications occur more often in women who have a failed TOL after cesarean than in those who have an elective repeat cesarean.
· The most devastating complication of VBAC is uterine rupture, occurring in 0.5% of all women who attempt a TOL after cesarean.
· Uterine rupture during a TOL after cesarean often results in fetal damage or death, even if delivery is accomplished quickly.
SUGGESTED READINGS
1. American College of Obstetricians and Gynecologists. Vaginal delivery after previous cesarean birth. ACOG Practice Bulletin No. 5, Washington, DC: ACOG, 1999:1.
2. Caughey AB, Shipp TD, Repke JT, et al. Trial of labor after cesarean delivery: the effect of previous vaginal delivery. Am J Obstet Gynecol 1998;179:938–941.
3. Caughey AB, Shipp TD, Repke JT, et al. Rate of uterine rupture during a trial of labor in women with one or two prior cesarean deliveries. Am J Obstet Gynecol 1999;181:872–876.
4. Choy-Hee L, Raynor BD. Misoprostol induction of labor among women with a history of cesarean delivery. Am J Obstet Gynecol 2001;184:1115–1117.
5. Duff P. Prophylactic antibiotics for cesarean delivery: a simple cost-effective strategy for prevention of postoperative morbidity. Am J Obstet Gynecol1987;157:794.
6. Enkin MW, Wilkinson C. Single versus two layer suturing for closing the uterine incision at caesarean section (Cochrane Review). In: Cochrane Database of Systemic Reviews. The Cochrane Library; Issue 2. Oxford: Update Software; 2002.
7. Gilliam M, Rosenberg D, Davis F. The likelihood of placenta previa with greater number of cesarean deliveries and higher parity. Obstet Gynecol2002;99:976–980.
8. Hannah ME, Hannah WJ, Hewson SA, et al. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial. Term Breech Trial Collaborative Group. Lancet 2000;356:1375–1383.
9. Hook B, Kiwi B, Amini SB, et al. Neonatal morbidity after elective repeat cesarean section and trial of labor. Pediatrics 1997;100:348.
10. Kastner ES, Figueroa R, Garry D, et al. Emergency peripartum hysterectomy: experience at a community teaching hospital. Obstet Gynecol2002;99:971–975.
11. Katz VL, Dotters DJ, Droegemueller W. Perimortem cesarean delivery. Obstet Gynecol 1986;68:571.
12. Leung AS, Leung EK, Paul RH. Uterine rupture after previous cesarean delivery: maternal and fetal consequences. Am J Obstet Gynecol 1993;169:945–950.
13. Lydon-Rochelle M, Holt VL, Easterling TR, et al. Risk of uterine rupture during labor among women with a prior cesarean delivery. N Engl J Med2001;345:3–8.
14. McMahon MJ, Luther ER, Bowes WA, et al. Comparison of a trial of labor with an elective second cesarean section. N Engl J Med 1996;335:689.
15. Mozurkewich EL, Hutton EK. Elective repeat cesarean delivery versus trial of labor: a meta-analysis of the literature from 1989 to 1999. Am J Obstet Gynecol 2000;183:1187–1197.
16. Phelan JP, Korst LM, Settles DK. Uterine activity patterns in uterine rupture: a case-control study. Obstet Gynecol 1998;92:394–397.
17. Rageth JC, Juzi C, Grossenbacher H. Delivery after previous cesarean: a risk evaluation. Swiss Working Group of Obstetric and Gynecologic Institutions. Obstet Gynecol 1999;93:332–337.
18. Ravasia DJ, Wood SL, Pollard JK. Uterine rupture during induced trial of labor among women with previous cesarean delivery. Am J Obstet Gynecol2000;183:1176–1179.
19. Reddy UM, DiVito MM, Armstrong JC, et al. Population adjustment of the definition of the vaginal birth after cesarean rate. Am J Obstet Gynecol2000;183:1166–1169.
20. Reyes-Ceja L, Cabrera R, Insfran E, et al. Pregnancy following previous uterine rupture. Obstet Gynecol 1969;34:387.
21. Scott JR. Mandatory trial of labor after cesarean delivery: an alternative viewpoint. Obstet Gynecol 1991;77:811.
22. Scott JR. Putting elective cesarean into perspective. Obstet Gynecol 2002;99:967–969.
23. Sims EJ, Newman RB, Hulsey TC. Vaginal birth after cesarean: to induce or not to induce. Am J Obstet Gynecol 2001;184:1122–1124.
24. Smith GC, Pell JP, Cameron AD, et al. Risk of perinatal death associated with labor after previous cesarean delivery in uncomplicated term pregnancies. JAMA 2002;287:2684–2690.
25. Vinueza CA, Chauhan SP, Barker L, et al. Predicting the success of a trial of labor with a simple scoring system. J Reprod Med 2000;45:332–336.
26. Yap OW, Kim ES, Laros RK Jr. Maternal and neonatal outcomes after uterine rupture in labor. Am J Obstet Gynecol 2001;184:1576–1581.
27. Yeast JD, Jones A, Poskin M. Induction of labor and the relationship to cesarean delivery: a review of 7001 consecutive inductions. Am J Obstet Gynecol1999;180(3 Pt 1):628–633.
28. Zelop CM, Shipp TD, Cohen A, et al. Trial of labor after 40 weeks' gestation in women with prior cesarean. Obstet Gynecol 2001;97:391–393.
29. Zelop CM, Shipp TD, Repke JT, et al. Uterine rupture during induced or augmented labor in gravid women with one prior cesarean delivery. Am J Obstet Gynecol 1999;181:882–886.
30. Zelop CM, Shipp TD, Repke JT, et al. Outcomes of trial of labor following previous cesarean delivery among women with fetuses weighing >4000 g. Am J Obstet Gynecol 2001;185:903–905.