Linda Van Le
The optimal management of the adnexal mass has perplexed clinicians for many years. As long as women have been offered medical care, the adnexal mass has presented a diagnostic as well as therapeutic problem. During the 21st century, we have made many inroads into understanding the development, complications of, and malignant potential of the adnexal mass. Additionally, we have made some advancements in its management: operative laparoscopy has been developed carefully and is approaching appreciable levels of sophistication such that recovery from surgical intervention is at a minimum.
Some considerations of management of the adnexal mass include the following: What is the mass? Should it be followed? How should it be followed? Should a woman have surgery for this? What route of surgery should be undertaken? Should an oncologist assist in the surgical management in the event that the mass is malignant? All of the above questions are timely and ideally should have precise answers such that we may offer optimal care for women. However, many of these issues still are being explored. With the advent of genetic discovery and technical advancement, we hope we will be able to better understand the etiology of the adnexal mass as well as offer management with minimal morbidity.
In this chapter, general background information, modes of diagnosis, ancillary studies, and surgical management of the adnexal mass will be discussed. Our hope is that with the tools available, a rational approach toward the adnexal mass will be presented such that the right choice will be offered for each patient with a minimum of concern for the physician and patient. Efficient diagnostic evaluations should be performed, with the goal of offering the appropriate patient a surgical procedure and expectantly following patients for whom one might predict the mass would resolve, thereby sparing a trip to the operating room. Management of the adnexal mass should be made with confidence and a clear schema and treatment plan. Taken altogether, management of the adnexal mass should be well understood by everyone in clinical gynecologic practice. A triage scheme should be available and understood such that for every patient and every kind of mass a treatment plan is readily available, one that will minimize the chance of malignancy and minimize morbidity should the patient need surgical management.
GENERAL OVERVIEW
In the grand scheme of things ovarian cancer is considered rare; however, it is often fatal. In light of this, management of the adnexal mass is a serious endeavor. Five to ten percent of all women in the United States will undergo surgical evaluation for an adnexal mass and, of these, up to one fifth will have ovarian cancer. Up to 300,000 women are hospitalized each year for evaluation of an adnexal mass and the majority of these patients undergo surgery. The skill then lies in determining which masses will be malignant such that the appropriate surgical preparations will have been undertaken; additionally, masses that may not need exploration then can be followed. Thus, the appropriate evaluation is important and includes a complete history, physical examination, and radiologic studies, as well as serum markers.
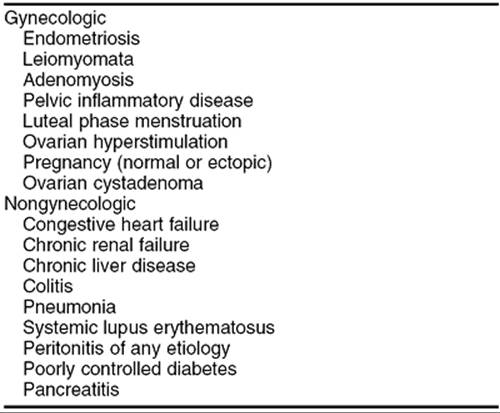
Adnexal mass refers not only to ovarian abnormalities but to masses originating in the fallopian tube, ovary, broad ligament, bowel, as well as uterine masses that lateralize (Table 56.1). Taking a pertinent history is, therefore, important. In addition to ascertaining the quality, severity, and duration of abdominal symptoms, review of menstrual cycle characteristics in premenopausal women, history of pelvic infectious disease, and any gastrointestinal syndromes may guide the diagnosis to one area or another.
|
|
|
TABLE 56.1. Masses occurring in the adnexal region |
Review of the family history, in particular for the occurrence of ovarian cancers, is extremely important. Scientific discoveries within the last decade have determined that specific gene mutations may increase the risk of ovarian cancer in certain subsets of the female population. In the general population, the lifetime risk of ovarian cancer is in 1 in 70 women, approximately 1.7%; however, even without the a specific gene mutation, having one family member with ovarian cancer increases a patient's risk to 5%, and with two relatives with ovarian cancer the risk increases to 7%. Regardless of how alarming it is to identify a family member with the disease, however, less than 10% of ovarian cancer patients will have this significant family history. The most common syndrome associated with familial transmission of ovarian cancer is hereditary breast-ovarian cancer. Of all hereditary cases, this syndrome accounts for the majority of familial ovarian cancers. Many of these cases are associated with germ-line mutations in BRCA1 and BRCA2 genes. BRCA1 is a tumor suppressor gene that, in a “normal” format, controls and regulates abnormal cell growth. In a patient affected by a mutation, this gene does not function to regulate cellular growth and, thus, malignancy evolves. Although advances in science have enabled us to identify many of these mutations, there are other abnormalities in this gene may contribute to not only ovarian cancer but breast cancer. Further investigations are underway to identify these additional gene mutations. BRCA2 is another well-known gene associated with breast-ovarian cancer. In particular, an abnormality in this gene has been found in 1% of the Ashkenazi Jewish population and, presumably, ovarian cancer in this population has been associated with germ-line mutations in BRCA2. If a mutation is found in BRCA1, a lifetime risk of ovarian cancer is estimated between 28% and 44%, and up to 27% in patients with a BRCA2 abnormality. Ovarian cancer also can be part of a constellation of cancers which include colorectal cancer, stomach cancer, endometrial cancer, and ovarian cancer. This is referred to as hereditary nonpolyposis colorectal syndrome. The risk of ovarian cancer is increased to up to 10% of patients who have this syndrome. In the face of germ-line mutations in these genes, ovarian cancer develops at an earlier age, often premenopausally, than in the majority of ovarian cancer cases, which tend to develop postmenopausally. Given the identification of familial risk, registries have been developed to investigate further the association of ovarian cancer in patients and their relatives. For patients with BRCA mutations, increased surveillance is recommended. Monthly breast examinations are encouraged beginning at an early age; some recommend beginning between ages 18 and 21. Additional examinations by a physician are recommended twice a year beginning in the mid-20s. Yearly mammograms are recommended also, beginning at this time. There is some interest in chemoprevention, such as tamoxifen to reduce the risk of breast cancer, and bilateral prophylactic mastectomy is being explored to reduce the risk of incurring breast cancer. Additionally, if a BRCA mutation is present, surveillance for ovarian cancer is recommended. This includes transvaginal ultrasonography and measurement of serum CA-125 beginning in the mid-20s. Bilateral prophylactic oophorectomy may be recommended after a woman has completed her family. Chemotherapeutic prevention of ovarian cancer may be instituted in the form of oral contraceptives. It is well accepted that oral contraceptives reduce the risk of ovarian cancer for women in the general population and may also decrease the risk in women carrying a BRCA mutation.
During the physical examination, a full female-oriented examination should be performed including a node survey and breast, abdominal, and pelvic examination. In cases of advanced cancer, nodular masses often are found in the abdomen and pelvis. However, for the most part, this would be quite clear when a patient with ovarian cancer arrives. Thus, in regard to determining whether an adnexal mass is malignant in the early stages, the physical examination may not be helpful. Lastly, the radiologic study and evaluation of a patient with, perhaps, mild symptoms would be of utmost importance.
DISTRIBUTION OF ADNEXAL MASSES BASED ON AGE
One way to approach the adnexal mass is to think of it in regard to the patient's age. The majority of ovarian cancers occur postmenopausally. For the young woman in her late teens and up to mid-20s, the majority of ovarian cysts are, of course, benign. Hemorrhagic corpora lutea and follicular cysts are common. In this age range, however, tubal abnormalities should be strongly considered. They include ectopic pregnancies and sequelae from tubal infections. Of concern in this age group, however, is the solid mass. The germ cell tumors, which for the most part are solid and unilateral, occur rarely but only in this age group. In these cases, preoperative consultation with a gynecologic oncologist may be in order.
In the older yet still reproductive age group, benign masses still prevail. Again, hemorrhagic corpora lutea and follicular cysts are common, as are dermoid cysts. Ultrasonographic characteristics of the ovarian mass in these cases will be helpful. Again, ovarian cancer in this age group is not common. Lastly, the age group for which there is most concern is the postmenopausal group. Albeit infrequent, ovarian cancers predominate, although the majority of masses in the this group are benign.
COMMON EPITHELIAL MASSES
The majority of ovarian masses are benign and, of these, the most common histologic type is epithelial, whether benign or malignant. The epithelial tumors are, for the most part, of the following types: serous, mucinous, endometrioid, clear cell, and transitional cell.
Serous Tumors, Benign and Malignant
Serous tumors are the most common histologic type and account for approximately 50% of all ovarian cancers. The benign counterpart accounts for 50% to 70% of all benign ovarian neoplasms. Although a patient of any age can manifest a benign serous tumor, the average age is 40 years. These tumors appear to be simple on ultrasonographic evaluation in that for the most part, although there may be some small internal echoes, these are purely cystic in appearance. They can be large and are mostly fluid filled. Benign serous tumors are bilateral in 20% of cases.
In contrast, invasive serous ovarian carcinomas account for 50% of all ovarian epithelial cancers. They are often bilateral and occur menopausally. The serous tumor is the prototype for invasive ovarian cancer, the “garden variety” histologic type. As with most ovarian cancers, the tumors are widely disseminated at the time of diagnosis.
Mucinous Tumors, Benign and Malignant
Benign mucinous tumors, mucinous cystadenomas, account for 25% of all benign ovarian neoplasms. They occur at a slightly younger age than serous benign tumors and can occur in young women, as well. They are less often bilateral, with both ovaries involved in only 3% of cases. They tend to be large and can be multiloculated. These are the tumors that have been reported to weigh up to 100 kg. Histologically, the cells are mucin filled and show endocervical or intestinal differentiation. These are the second most common type of ovarian neoplasm. Their invasive counterpart, the mucinous cystadenocarcinoma, represents 15% of invasive ovarian epithelial cancers.
Endometrioid Tumors, Benign and Malignant
The third epithelial type is the endometrioid neoplasm. These neoplasms recapitulate the endometrium and, thus, the epithelial component resembles the endometrial glandular cell. Benign tumors of this histologic type are less common and are associated histologically with changes of adenofibroma or cystadenofibroma. The endometrioid malignant ovarian neoplasm represents up to 25% of ovarian epithelial cancers and is usually moderate in size, ranging up to 20 centimeters. Most ovarian endometrioid neoplasms are malignant. The malignant form tends to be bilateral in 30% of cases. When an endometrioid ovarian invasive cancer is found, up to 25% of patients will have concomitant uterine endometrial cancer or endometrial hyperplasia. Pelvic endometriosis may be found also, and one hypothesis is that these lesions arise from preexisting endometriosis. When an endometrioid invasive cancer is found in the ovary it is the duty of the pathologist to clarify whether this is a metastasis from a primary uterine cancer.
Clear Cell Tumors
The fourth general category of epithelial ovarian neoplasms is the clear cell tumor. Benign clear cell tumors rarely are diagnosed. However, the invasive form of this, the clear cell carcinoma, represents 10% of all ovarian cancers. The clear cell component usually coexists with another epithelial type. The clear cell histology also is associated with endogenous endometriosis in the pelvis in up to 25% of cases.
Transitional Cell Tumors
Lastly, transitional cell tumors, which mimic the epithelium found in the bladder, are rare. The Brenner tumor is a well-known transitional cell tumor and accounts for 2% of all ovarian epithelial tumors. Brenner tumors are considered benign, although a malignant variant has been identified.
Other Common Benign Tumors
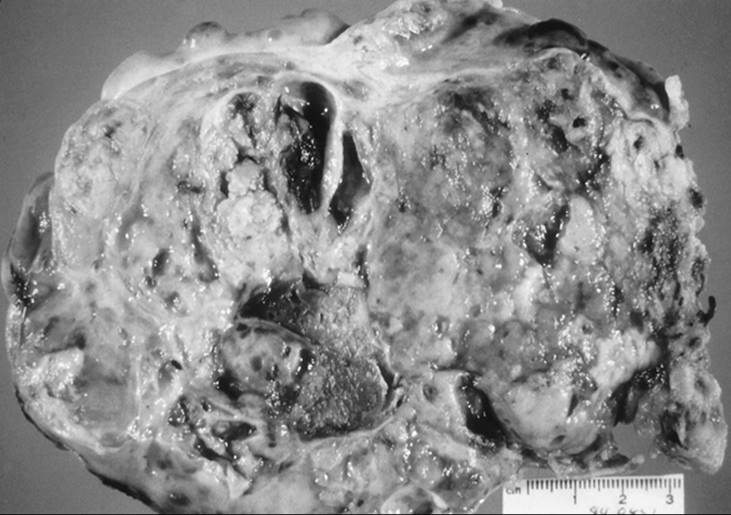
The dermoid cyst is a common benign tumor found in all ages. This tumor is comprised of three germ cell layers, which explains the term teratoma. The three germ layers include the ectoderm, mesoderm, and endoderm. It is the most common type of ovarian germ cell neoplasm and occurs frequently. This teratoma accounts for 25% of all ovarian neoplasms and is most commonly found in the reproductive age group; however, it can be found in younger women and in postmenopausal women. The mature teratoma can grow to quite a large size before a patient has pain or notices abdominal swelling. Up to 15% of cases are bilateral and these tumors can grow to a large size, weighing several kilograms (Fig. 56.1). These tumors are well known for their smooth, glistening, pearly white surface. Either cystectomy or adnexectomy can be performed to treat these neoplasms effectively. These tumors are interesting because of a radiologic finding of teeth or bone or cartilage on plain film. Additionally, they have a characteristic finding on ultrasonography and computed tomography (CT) scan. Within the cyst wall is a protuberance called Rokitansky protuberance. These neoplasms are well known for the greasy sebaceous material associated with hair, bone, or teeth found within the cyst. Thyroid tissue, salivary gland tissue, and gastrointestinal and bronchial epithelium can be found, associated with bone, cartilage, and smooth muscle. Other ectodermal tissues, including brain, neural, retina, and choroid plexus, are also found. Clinical complications associated with the presence of these neoplasms include torsion rupture and infection. More uncommonly, hemolytic anemia and malignant transformation may also occur.
|
|
|
FIG. 56.1. Removal of a large dermoid cyst. |
Endometriomas of the ovary involve bilateral ovaries in up to 50% of cases. These cysts often are associated with dense adhesions to the broad ligament or cul-de-sac and are difficult to excise. The contents are usually chocolate colored and thickened. Cystectomy can be performed successfully in many cases. The presence of endometriomas indicates advanced endometriosis, and usually other pelvic sites are involved, such as the cul-de-sac or other peritoneal structures. Bilateral salpingo-oophorectomy is curative, if clinically appropriate, in that estrogen drives the growth of these cysts. Ovarian endometrioid carcinoma can be associated with these benign neoplasms.
Physiologic cysts can appear as adnexal masses. These include follicular cysts and corpus luteal cysts, which are most common in the reproductive age group and range from small to moderate in size. Follicular cysts are unilocular, and the ultrasonographic image should be that of a simple cyst; however, if there is a region of clotted blood this area will appear as cystic or solid. The interpretation of this is dependent upon the ultrasonographer. However, given that these benign physiologic cysts prevail in the reproductive age group, a laparoscopic approach could be offered should surgical evaluation be necessary.
RADIOLOGIC EVALUATION OF THE ADNEXAL MASS
Whether suspicion of an adnexal mass arises as a result of a patient's symptoms or suspicious findings during a pelvic examination, radiologic imaging is usually the next step in the diagnostic evaluation. For gynecologic problems, fortunately, transvaginal ultrasonography gives the best visualization of the adnexal region. Previously, transabdominal ultrasonography was used routinely to visualize the adnexa. However, the transvaginal approach, by virtue of the proximity of the probe to the adnexa, gives startlingly clear characterization of the adnexal region.
Description of an adnexal mass should include qualitative modifiers. If the mass is cystic, comments such as whether the cyst is simple (indicating that there are no internal echoes or populations of suspicion) or complex should be made. The size and whether there has been interval growth should be noted.
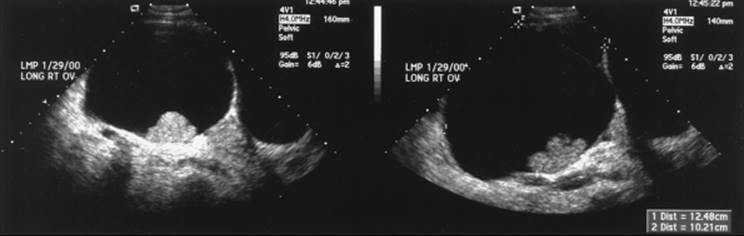
Additionally, solid components are important, because malignant masses often will have solid sections. Several studies have indicated that the incidence of malignancy increases when masses are multiloculated and contain solid areas. Other reports indicate that the most suggestive finding of malignancy is inner wall abnormalities, such papillations, or a solid area. Other important features found on ultrasonography actually can be reassuring, such as calcium found next to fat as noted in dermoid tumors. Thus, adnexal masses that have solid components, inner wall papillations, or nodularity should not be observed further and surgical evaluation would be in order (Fig. 56.2).
|
|
|
FIG. 56.2. Ultrasonographic image of an ovary with internal wall papillations. The final pathology of this ovarian cyst was clear cell adenocarcinoma. |
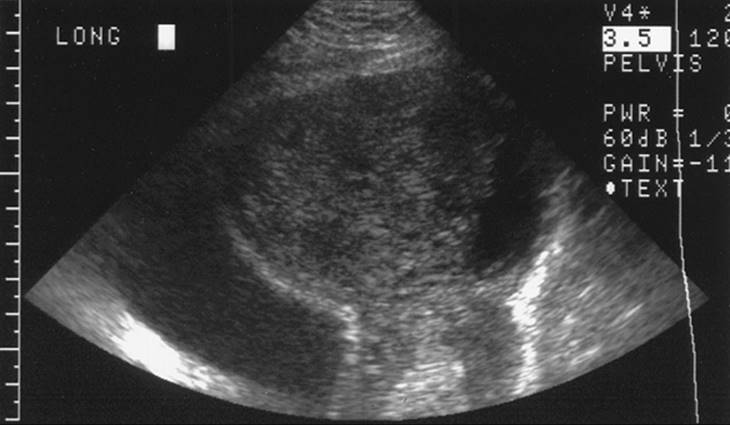
An ultrasonographic evaluation can clarify the etiology of the mass. Although not definitive, suggestions that the masses may arise from the tube, such as the form of hydrosalpinges or tuboovarian abscesses, can be helpful. This is operator dependent and, as such, obtaining an ultrasonographic examination from a quality center would be of utmost importance in managing patients with adnexal masses (Fig. 56.3 and Fig. 56.4).
|
|
|
FIG. 56.3. Ultrasonographic image of a tuboovarian abscess. |
|
|
|
FIG. 56.4. Ultrasonographic image of a cystadenofibroma. |
Most ovarian malignancies occur in the postmenopausal group. In addition to the abnormal findings noted above for which surgery is recommended, growth of a mass in any age group is most likely an indication for surgical evaluation. It has been suggested, however, that in the postmenopausal population, a cystic mass that is simply cystic, that is has no nodularity, papillations, nor solid areas, may be managed conservatively. In a study of over 7,000 postmenopausal women, unilocular ovarian cysts measuring less than 10 centimeters in diameter in asymptomatic women were infrequently malignant. The patients in whom unilocular cysts were detected were observed, and 50% of the masses resolved within 60 days. Of the residual patients, all the masses were found to be benign when evaluated during surgery. Thus, these findings should be reassuring for the postmenopausal patient with unilocular cysts, in particular if the cysts are stable over several ultrasonographic examinations.
In addition to ultrasonographic findings, Doppler sonography may add some information. Doppler ultrasonography allows an evaluation of ovarian blood flow. With emission of a sound wave from a stationary source, reflection of the sound wave from a moving target is relative to its velocity. The strategy of using Doppler ultrasonography in ovarian masses would be to detect abnormal blood flow associated with neoangiogenesis often associated with ovarian malignancy. Thus, several indices have been developed for standardization of the study of ovarian blood flow. These include systolic-to-diastolic ratio, resistance index, and pulsatility index. Doppler analysis of flow is performed at multiple points, then color coded according to the direction of blood flow and superimposed on the anatomic location. A Doppler study can be performed quickly and is felt to add to the sonographic diagnosis. In a normal ovary, pulsatility and resistance indices are low. These indices also show changes relative to phases of the menstrual cycle. In contrast, in ovarian tumors, are associated with development of new blood vessels required to support growth of the aberrant tissue, the newly formed vessels have no smooth muscle vasculature, and thus the Doppler signalling is abnormal.
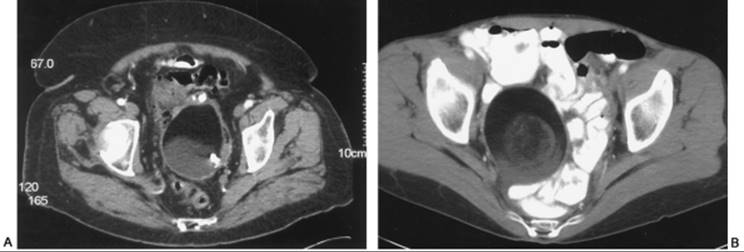
In the event that ultrasonographic findings are uncertain or more information is needed before surgical evaluation is undertaken, CT can be helpful. The conventional CT scan obtains images one slice at a time. Slice thickness is usually 8 to 10 millimeters, and patient immobilization is critical for obtaining clear views. Each slice is then reconstructed by the computer to result in a full image of the pelvis. Usually radiopaque oral agents are used to opacify the gastrointestinal tract. Intravenous contrast can be administered to visualize vascular and genitourinary structures. Ovarian nodularity, septations, and fat can be characterized well by CT scan. Additionally, if there is a concern that ultrasonographic findings may be reflecting a loop of bowel, CT can clarify this by using contrast. CT scans are fairly accurate for diagnosing a dermoid cyst given the combination of fat and calcification in these neoplasms (Fig. 56.5). If there is some concern that an adnexal mass may be uterine, such as in the case of myomas, CT can clarify this. Lastly, if an abdominal and pelvic CT scan is ordered, information regarding the rest of the lower abdomen and upper abdomen can be obtained.
|
|
|
FIG. 56.5. Computed tomography image of dermoid cysts. A: Internal calcification. |
Magnetic resonance imaging (MRI) uses magnetic fields and radio waves. As compared with CT scan, which uses x-ray attenuation, multiple tissue characteristics are analyzed by MRI. One of the advantages is that no ionizing radiation is used for MRI. Patients with electrical pumps or implants such as pacemakers cannot undergo MRI evaluation. Gadolinium is used as intravenous contrast to better visualize organs and abnormalities. Compared with MRI, the CT scan is less expensive and usually more readily available. When evaluating disease, MRI may provide additional information but, for the most part, similar information is gained from either modality when evaluating the adnexal mass.
A new modality, positron emission tomography (PET), is undergoing investigation for clinical use in the evaluation of gynecologic malignancies. This radiologic test is based on the uptake of 18F-fluoro-2-dioxyglucose. This scan differs greatly from previous scans, which measure the differences between normal tissue and cancerous tissue; it is hypothesized that cancer tissues process this glucose analog differentially such that when a PET scan is performed, the emission of images is different in abnormal tissues. Theoretically, then, this technique is potentially more sensitive than classic imagining methods for detecting metastatic disease. The glucose analog is given intravenously, then the scan is performed and images are displayed for interpretation. This study usually is performed in the nuclear medicine department. Some investigators have suggested that the PET scan is more sensitive than CT or MRI for detecting the recurrence of ovarian cancer. Other investigators differ and note that the false-negative and false-positive result rates are quite high. The PET scan is an experimental modality; its use may increase with more experience. We have yet to understand fully its use in the evaluation of gynecologic malignancies, and insurance reimbursement issues still exist.
TUMOR MARKERS
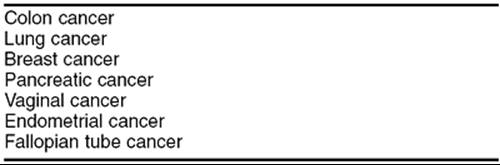
The purpose for using tumor markers is two-fold as follows: (a) to measure these preoperatively to try to predict the malignant nature of the mass in question so that surgical preparations may be undertaken and (b) to follow disease once established. Traditionally, the most important tumor marker for epithelial ovarian cancers is CA-125. This antigen is expressed epithelially when a CA-125 level is ordered, and the amount of expression is measured by antibody assay using OC-125. CA-125 is relevant in particular to epithelial ovarian cancers, for which a cutoff of 35 U/mL has been determined to divide normal from abnormal levels. This has been accepted as the standard for clinical practice in the United States. Numerous studies have shown CA-125, drawn preoperatively, to be unreliable as a predictor of the malignant nature of a mass. During early stages of cancer, such as stage I disease, only 50% of patients will have elevated levels. Additionally, many other adnexal masses and disease processes may express elevated levels of CA-125 (Table 56.2 and Table 56.3). For screening purposes, many investigators have moved on to a combination of CA-125 with other tumor markers or with ultrasonographic findings. To date, there have been no successful screening protocols using serum and ultrasonographic preoperative data to accurately predict adnexal malignancy. Lastly, in the event of an ovarian epithelial neoplasm, preoperative CA-125 levels have been found to be controversial in regard to final outcome.
|
|
|
TABLE 56.2. Benign conditions associated with elevated CA-125 |
|
|
|
TABLE 56.3. Other malignancies associated with elevated CA-125 |
For following disease progression and regression, however, CA-125 levels have been invaluable. For monitoring responses to treatment, elevated levels accurately reflect progression or regression of disease in over 90% of patients. Thus, CA-125 is useful preoperatively as a baseline for ovarian cancer and is one of the main methods of following disease progression, in combination with radiologic imaging and clinical examination.
CA-125 levels can be elevated postoperatively because of surgical manipulations of the abdominal organs. If a preoperative CA-125 level was not drawn and a diagnosis of cancer is made intraoperatively, a postoperative CA-125 level should be measured, taking into consideration that elevated levels may be seen due to surgery. The elevation may not be so important, because it will be the rate of decline and actual resolution of elevated levels that would be most indicative of disease prognosis. Of note, the half-life of CA-125 is 20 days.
Numerous other markers have been studied to attempt to predict ovarian malignancy preoperatively and to follow cancer should it be diagnosed. Other tumor antigens include CA-15-3, CA-72-4 (TAG-72), CA-130, and CA-19-9. However, only CA-125 is in common use, and our clinical protocols include this antigen for following disease. The other tumor markers have not been as successful, in that their accuracy is less than that of CA-125 and many assays may not be readily available. A new tumor marker, lysophosphatidic acid (LPA), has been studied and may be promising in ovarian cancer. This lipid mediator can be assayed in serum and has been found to be elevated in patients with cancer.
SURGICAL EVALUATION
Once it has been decided that a mass requires surgical evaluation, the patient is scheduled for surgery and the surgeon must decide which approach to attempt. Gynecologists have been trained to make essentially two kinds of incisions when using an open approach. The most common transverse incision is the Pfannenstiel incision, also known as the bikini incision. Usually performed at the superior aspect of the pubic hair region for cosmetic reasons, its exposure is limited. When space is not a consideration for node dissection or removal of a large mass, the Pfannenstiel is useful in that it heals well, is reportedly less painful, and is associated with a lower incidence of wound dehiscence as compared to vertical incisions. Other transverse approaches include the Cherney and Maylard incisions. To perform a Cherney incision, a transverse skin incision is made, and the rectus muscles are identified at the insertion into the pubic synthesis and divided, commonly using electrocautery. With the rectus muscle out of the way, pelvic exposure is greatly enhanced and, thus, this incision is very useful when additional pelvic exposure is needed, yet the cosmetic aspects of a transverse incision are preserved. Closure of this incision is straightforward. The rectus tendons should be reapproximated to the inferior tendon of the rectus sheath using permanent sutures. Thus, in this incision, the rectus muscles are preserved. Alternatively, another space-endowing incision is the Maylard. Again using the transverse skin incision, once the rectus muscles are identified, the inferior epigastric vessels which reside in the lateral aspect of the rectus muscles are identified and ligated. The rectus muscles are divided using electrocautery. If approached cautiously and slowly, division of the rectus muscles is not complicated by bleeding. As with the Cherney incision, the Maylard incision affords greater exposure to the pelvic region than does a Pfannenstiel.
Alternatively, when a malignancy is suspected and surgical staging may be required, a vertical incision is used because of accessibility to the upper abdomen should this be needed; clearly, transverse skin incisions are limiting for exploration and management of disease found in the upper abdomen. There are two major vertical incisions, the paramedian incision and midline vertical incision. In performing a paramedian incision, the skin incision is just lateral to midline. Some consider these incisions stronger because of the displacement of the skin defect over the rectus muscle defect. The incidence of incisional hernia formation is decreased. However, the midline incision is used most commonly. With the need for upper abdominal exposure, the midline incision is ideal because of the ability to extend the incision superiorly.
Exposure is usually ideal with the midline incision, although in many cases the Cherney and Maylard incisions offer better exposure of the pelvis. Because the midline facial area is less vascular, the entry in the midline can be performed quickly, with minimal damage to rectus muscles and nerves. Also, blood loss is decreased with a midline incision. However, this is considered one of the weaker incisions and hernias, dehiscence, and eviscerations occur more readily with this incision than with others.
In summary, several incisions are available to gynecologists. Choice of incision is critical to successful evaluation of the gynecologic problem at hand. If malignancy is suspected, then the midline incision is recommended. However, suspicion of malignancy is based on a thorough knowledge of the risks, taking into consideration the radiologic characteristics of the mass and the patient's age. Thus, by a “best guess” scenario of the malignant potential of the adnexal mass being evaluated, the incision should be chosen.
Once the abdomen is open, it is recommended that washings be obtained before manipulation of the pelvic organs, so that a true assessment of cytologic spread can be undertaken. This can be performed in many ways. Simply, a large syringe can be used to inject the pelvis with fluid, and then the fluid is withdrawn using the empty syringe. Alternatively, various suction devices are available for use in the operating room to efficiently remove pelvic washings. The solution recommended for pelvic washings is isotonic so that lysis of cells does not occur. Plasmalyte warmed to body temperature is recommended. When obtaining washings, it is helpful to cup one's hand in the abdomen and aspirate the collective washings from this so as to not to aspirate epiploica. A small amount of heparin is added to the collection, which is then transported to the cytology department for evaluation.
After washings are obtained, a thorough exploration of the upper and lower abdomen is in order. In the upper abdomen, the diaphragm and omentum should be palpated for possible metastatic sites. Also, by reaching under the omentum for the root of the mesentery, the periaortic region should be palpated for adenopathy. Because the intent is to pack away bowel so that pelvic visualization is optimized, lysis of adhesions may be necessary to release small bowel loops that may be adherent in the pelvis. After doing so, using laparotomy sponges to collect the bowel, a retractor can be placed. Care should be taken in thin patients not to compress the psoas muscle and cause femoral nerve damage. Then the adnexal mass of interest is examined. If the pelvic mass is an ovarian cyst, either a cystectomy or an oophorectomy can be performed, depending upon the preoperative discussion with the patient and the index of suspicion for malignancy. For most postmenopausal women, an oophorectomy is planned. If there is any question as to whether the mass is truly malignant and the patient desires preservation of her ovaries, a cystectomy can be performed; if malignancy is suggested by frozen section, completion of the oophorectomy can be performed later during the surgery. In a quality hospital, frozen section analysis should have high correlation, upwards of 90%, with the final pathology findings.
Classically, when a malignancy is found in a postmenopausal woman, complete surgical staging, including total hysterectomy and bilateral salpingo-oophorectomy, is performed. Washings from the pelvis, both gutters, and diaphragm should be obtained. Bilateral pelvic sidewall, paracolic gutter, cul-de-sac, and anterior vesical biopsy samples should be obtained. These can be obtained by lifting a small portion of peritoneum and excising sharply. If there is bleeding at the biopsy site, the area can be cauterized for hemostasis. In lieu of obtaining a diaphragm biopsy, which can be performed using a cervical biopsy forceps, a scraping of this area can be performed. The right side of the diaphragm is scraped with a Pap smear spatula. The dominant hand is extended into the right upper quadrant and the diaphragm scraped. Cells are smeared from the spatula onto a slide and fixed with traditional preservative or submerged in liquid cytology media. When only an ovary(ies) is(are) affected without evidence of extraovarian spread, pelvic lymph node and periaortic node sampling should be performed, as well as omental biopsy. Lymph node dissection is not commonly performed by the general gynecologist so will not be described here; however, several excellent references describe the technique. Possible resources for the gynecologist who does not often perform lymph node dissection ideally include consultation with a gynecologic oncologist. However, if one is not available, a surgical oncologist or a urologic oncologist may be of assistance.
After ascertaining that all sites are hemostatic and sponge and instrument counts are correct, the abdomen is closed. For vertical incisions, two running sutures meeting in the midline should be sufficient for a fascial closure. If there is any concern that this closure would not be durable, as in patients who are malnourished or are on steroids or other immunosuppressive agents, interrupted closure with a permanent suture may be undertaken. Successful closure of the abdomen often is taken for granted but is a very important part of any surgical procedure. Wound infection and skin separations are unpleasant for the patient; however, serious complications such as fascial dehiscence can result. Although the Smead-Jones closure traditionally has been felt to be the most secure, it is very time consuming and may not afford any extra advantage for the patient when compared with mass abdominal wall closure. When using the Smead-Jones closure, monofilament permanent suture often is used. Alternatively, single interrupted sutures encompassing the entire abdominal wall can be used. However, using two sutures and running the fascia from the opposite poles to the midline is equally effective. This, of course, shortens operating room time and the amount of time the patient is under anesthesia.
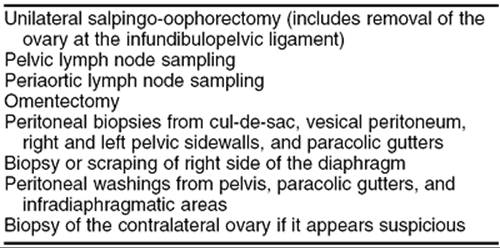
There are many compelling reasons to stage an ovarian cancer. First of all, the extent of tumor is clearly described within our staging system, thus making communication among physicians and the clinical implications quite clear. Given a certain stage of disease, a patient may obtain appropriate therapeutic or adjuvant chemotherapy or radiation therapy. Staging in ovarian cancer is particularly important, because microscopic metastases are serious implications for postoperative treatment. In a classic study, up to 30% of patients thought to have stage I ovarian cancer based on incomplete surgical staging were upgraded to a more advanced stage when microscopic metastases were discovered during a later surgery. Therefore, if full staging, which includes pelvic and periaortic lymph node dissection, had not been included, these patients would have been treated incorrectly. Unfortunately, despite the availability of gynecologic oncologists in this country, full staging still is not offered to all patients. Not only are node dissections omitted, full palpation of the upper abdomen and omental biopsies are omitted. Although the missing staging procedures sometimes can be attributed to a skill issue such as lymph node dissection, failure to evaluate the diaphragm or perform straightforward peritoneal biopsies usually reflects the surgeon's lack of understanding of the necessity of full staging for ovarian malignancies. Complete staging is described in Table 56.4.
|
|
|
TABLE 56.4. Complete staging for ovarian cancer |
SPECIAL CLINICAL SITUATIONS
Ovarian cancer is usually a disease of postmenopausal women. Thus, when faced with surgical evaluation of an adnexal mass, should a total hysterectomy and bilateral removal of adnexa be required, the implications are not as striking. However, in the case of a young woman with an incidental malignancy found during surgery, there is the added dilemma of how to address the unaffected organs after removal of the adnexa. For the young woman in whom a malignancy is suspected, conservative treatment is recommended (Table 56.5). Conservative surgery may be considered in women who are nulliparous with only suspected stage I disease (cancer confined to an ovary). After conservative surgery, should more advanced disease be diagnosed after pathologic evaluation of resected specimens, additional surgery may be undertaken as needed after consultation with an oncologist.
|
|
|
TABLE 56.5. Surgical staging for ovarian cancer in young women |
For young patients who wish for preservation of fertility options, all efforts should be made to perform a cystectomy. Samples can be sent for frozen section to determine if the ovarian mass is benign or malignant. If there is a question of malignancy, staging should be performed. Care should be taken to understand the patient's wishes for reproduction before performing surgical staging. In these cases it is clearly best to discuss all possible options preoperatively with the patient; in general, masses in premenopausal women are benign. However, in the event that a malignancy is found, if the contralateral ovary appears to be normal the uterus and ovary can be preserved, and the rest of the staging is as for the postmenopausal woman. That is, pelvic and periaortic node dissection, peritoneal and omental biopsies, and washings should be obtained. In the young patient, if there are bilateral masses and it is suspected that both ovaries are involved, thought should be given to preserving the uterus, given the advances made in assisted reproductive technology. Egg donation and other services may be available for this patient should removal of both ovaries be indicated.
Another special scenario is management of the mass with borderline histology, also known as tumors of low malignant potential. Ovarian low malignant tumors have been described for all of corresponding invasive epithelial ovarian neoplasms. Serous and mucinous histologies make up the largest proportion of these tumors. Histologically, low malignant tumors differ from truly invasive lesions in that invasion into ovarian stroma is not detected; the epithelial lining is multilayered, and only mild nuclear atypia is present. These tumors account for up to 16% of ovarian malignancies. As compared with truly invasive ovarian cancers, the majority of tumors of low malignant potential are early stage and confined to one ovary. Once resected, regardless of stage, the role of adjuvant or therapeutic chemotherapy is unclear (unlike that for invasive epithelial ovarian cancers); this disease is felt to not benefit from adjuvant chemotherapy and remains a surgically treated disease. CA-125 levels are elevated in some patients with tumors of low malignant potential. In these cases, monitoring this marker for the recurrence of disease may be useful.
In the postmenopausal population, management is straightforward. At the minimum, unilateral salpingo-oophorectomy is performed and, more frequently, a bilateral salpingo-oophorectomy and often hysterectomy are performed. Again, the majority of tumors of low malignant potential are of early stage and prognosis is good. In the young population, a cystectomy is a possibility. Although recurrence rates may be higher after cystectomy, mortality rates from recurrent disease appears to be unchanged. When cystectomies are performed in these cases, women desiring children may be able to gain a few years and complete a family before undergoing or requiring more definitive surgery.
Adnexal masses in the young women may also be of germ cell origin. This is a special clinical scenario in that these neoplasms occur exclusively in young women. The main complaints include abdominal pain, with a pelvic mass found during examination. Some patients have acute abdominal pain resulting from torsion or rupture and hemorrhage of these masses. When evaluating a patient whose condition is not acute, the radiologic image usually reflects a solid mass with some cystic changes. The most common germ cell ovarian tumor is a dysgerminoma (Fig. 56.6). This is also the most common ovarian malignancy for young and pregnant women. This germ cell tumor is unusual in that it has a high incidence of bilaterality. Should a solid tumor be found and a germ cell tumor suspected, α-fetoprotein, human chorionic gonadotropin, and LBH levels may be drawn preoperatively, although none of these is necessarily predictive of finding a germ cell tumor. During surgery, given that most of these patients have not completed childbearing and that germ cells tumors most often are confined to the ovary, a conservative approach such as unilateral adnexectomy can be performed. Routine biopsy of the contralateral ovary in the case of a dysgerminoma is not recommended, even though the bilaterality rate is higher than with other germ cell tumors.
|
|
|
FIG. 56.6. Dysgerminoma in a 17-year-old girl. |
Another germ cell neoplasm that occurs in young women is the endodermal sinus tumor. This tumor is classically associated with elevated α-fetoprotein and may be found in conjunction with a dysgerminoma. These tumors confer a worse prognosis. The malignant counterpart of the dermoid cyst, a malignant teratoma, may also be found in this population. These tumors are uncommon. In summary, if a germ cell tumor is diagnosed in a young person, a unilateral procedure may be performed if there is no suspicion of metastatic disease to the contralateral ovary or pelvis. If in doubt, a conservative approach would be best, with preservation of other reproductive organs and the possibility of returning for another laparotomy should this be indicated.
LAPAROSCOPIC APPROACH TO THE ADNEXAL MASSES
The role of laparoscopy in the management of the adnexal mass has advanced tremendously over the last decade. Laparoscopic technique has been developed and equipment is available such that laparoscopic surgery has never been easier. The advantages of a laparoscopic approach to management of the mass include shorter hospital stay, less pain, shorter recovery time, less expensive process by virtue of fewer days of hospitalization, and the potential to minimize the development of adhesions. Alternatively, the risks and complications of a laparoscopic approach differ from those associated with laparotomy. Although striking when reported and laparoscopic complications such as puncture of a vessel can be severe, altogether they are uncommon. Minimal requirements for a laparoscopic approach to the adnexal mass include adequate surgical skill to perform competently either a cystectomy or adnexectomy, accurate and prompt frozen section services, and the availability of staging in a timely fashion should rupture or advanced disease be diagnosed (Table 56.6). With the laparoscopic approach, once the mass is removed frozen section is completed as usual. Should the mass be malignant, staging should be undertaken as usual, either laparoscopically if the surgeon is skilled or by proceeding to laparotomy. If rupture of the mass occurs and the frozen section confirms malignancy, in general it is recommended that staging be performed promptly. However, should there be spill of ovarian contents inadvertently or in the process of performing a cystectomy, although the stage is upgraded to stage Ic ovarian cancer, it is unclear that the prognosis is much worse; however, in many cases the patient would be committed to adjuvant chemotherapy.
|
|
|
TABLE 56.6. Criteria for laparoscopic removal of adnexal mass |
A unique complication associated with the laparoscopic approach to the mass with malignant potential is the occurrence of port-site implants. Studies have reported port-site dissemination and metastasis in 20% to 50% of patients. The mechanism for metastasis to these sites is direct tracking of tumor cells through port sites. Suggestions for decreasing the risk of port site metastasis in the event ovarian cancer is found at laparoscopy include resection of the port site or copious irrigation at the time of removal of instruments through the port site.
The key to successful laparoscopic management of an adnexal mass then returns to the main issue, selection of the appropriate patient given a best guess scenario of whether a mass is benign or malignant. A postmenopausal woman with a complex mass has a higher chance of malignancy and, therefore, the surgeon planning a laparoscopic approach should absolutely have a contingency plan should malignancy be discovered. Alternatively, because the chance of malignancy is less frequent in the premenopausal group, laparoscopic approach usually is appropriate in this age group. Until we can predict absolutely which masses are malignant, a combination of age and radiologic appearance, in particular ultrasonographic findings, should be integrated to determine the best approach for each patient.
SUMMARY POINTS
· Inroads have been made into the management of the adnexal mass. These include conservative management of the simple cyst in the postmenopausal woman and offering a laparoscopic approach to adnexal masses.
· An ideal method for determining preoperatively whether a mass is benign or malignant has not been discovered. Should we be able to predict this, plans and preparations could be made accordingly.
· All surgeons managing the adnexal mass should know the appropriate cancer staging procedures for the postmenopausal woman and the young woman desiring preservation of fertility. Even if the surgeon is not technically equipped to perform the actual node dissection, assistance frequently can be arranged. In the event a malignancy is diagnosed, appropriate staging is imperative to save the patient another surgical procedure and to determine the extent of the disease so that adjuvant therapy can be prescribed.
· New tumor markers and radiologic approaches are being pursued fervently such that soon we may be able to more accurately distinguish malignant from benign adnexal masses. In the meanwhile, appropriate medical and surgical management of the adnexal mass is the responsibility of all gynecologic surgeons.
SUGGESTED READINGS
Radiologic Evaluation of the Adnexal Mass
Bailey CL, Ueland FR, Land GL, et al. The malignant potential of small cystic ovarian tumors in women over 50 years of age. Gynecol Oncol 1998;69:3–7.
Soper JT. Radiographic imaging in gynecologic oncology. Clin Obstet Gynecol 2001;44:485–494.
Van Nagell JR, Ueland FR. Ultrasound evaluation of pelvic masses: predictors of malignancy for the general gynecologist. Curr Opin Obstet Gynecol1999;11:45–49.
Yen R, Sun S, Shen Y, et al. Whole body positron emission tomography with 18F-fluoro-2-deoxyglucose for the detection of recurrent ovarian cancer. Anticancer Res 2001;21:3691–3694.
Surgical Evaluation
Chan JK, Manetta A. Prevention of femoral nerve injuries in gynecologic surgery. Am J Obstet Gynecol 2002;186:1–7.
Young RC, Decker DG, Wharton JT, et al. Staging laparotomy in early ovarian cancer. JAMA 1983;260:3072–3076.
Tumor Markers
Jeyarajah AR, Ind TEJ, Skates S, et al. Serum CA125 elevation and risk of clinical detection of cancer in asymptomatic postmenopausal women. Cancer1999;85:2068–2072.
Mol BW, Boll D, De Kanter M, et al. Distinguishing the benign and malignant adnexal mass: an external validation of prognostic models. Gynecol Oncol2001;80:162–167.
Xu Y, Shen, Z, Wiper DW, et al. Lysophosphatidic acid as a potential biomarker for ovarian and other gynecologic cancers. JAMA 1998;280:719–723.
Special Clinical Situations
Boruta D, Van Le L. Ovarian tumors of low malignant potential: current understanding and controversy. Curr Probl Obstet Gynecol Fertil 2002;25:45–57.
Duska LR, Change Y, Flynn CE, et al. Epithelial ovarian carcinoma in the reproductive age group. Cancer 1999;85:2623–2629.
Morice P, Camatte S, El Hassan J, et al. Clinical outcomes and fertility after conservative treatment of ovarian borderline tumors. Fertil Steril 2001;75:92–96.
Morice P, Wicart-Poque F, Rey A, et al. Results of conservative treatment in epithelial ovarian carcinoma. Cancer 2001;92:2412–2418.
Laparoscopic Approach to the Adnexal Mass
Hopkins MP, von Gruenigen V, Gaich S. Laparoscopic port site implantation with ovarian cancer. Am J Obstet Gynecol 2000;182:735–736.
Manolitsas TP, Fowler JM. Role of laparoscopy in the management of the adnexal mass and staging of gynecologic cancers. Clin Obstet Gynecol2001;44:495–521.
Mettler L. The cystic adnexal mass: patient selection, surgical techniques and long-term follow-up. Curr Opin Obstet Gynecol 2001;13:389–397.
Morice P, Viala J, Pautier P, et al. Port-site metastasis after laparoscopic surgery for gynecologic cancer. A report of six cases. J Reprod Med 2000;45:837–840.