Jonathan E. Davis
URETHRAL CATHETERS
The need to place urinary catheters is common in the emergency department (ED). The reasons for placement vary widely and include the relief of urinary retention, monitoring urinary output for resuscitation efforts, treatment of gross hematuria, and obtaining a urine specimen. Urethral catheter placement is usually a routine and uncomplicated procedure but can sometimes be challenging. As with any other procedure, there are accompanying risks and complications. Emergency physicians should be able to utilize different types of catheters, be able to overcome the common difficulties encountered placing them, and be aware of the acute and chronic complications of urinary catheters.
Urinary catheter placement in the male patient may be complicated by several factors related to the length and path of the urethra. Common pathologic conditions may also make urinary catheter placement difficult (eTable 128.1). Meatal stenosis, either from prior infections, congenital malformation, or previous trauma can be diagnosed when the meatus of the penis is fibrotic and nondistensible. A dilation procedure performed by a urologist may be necessary for catheter placement to be successful. Hypospadias is a congenital condition in which the true urethral lumen is on the ventral aspect of the penis, making catheterization difficult. In a patient with known hypospadias, the glans penis should be inspected to identify a true urethral meatus, as there is often a blind-ended lumen on the glans penis. The conscious patient should be able to state which lumen is functional. Once the lumen is identified, catheterization may proceed in the standard fashion.
eTABLE 128.1
Approach to Difficulties in Male Catheterization
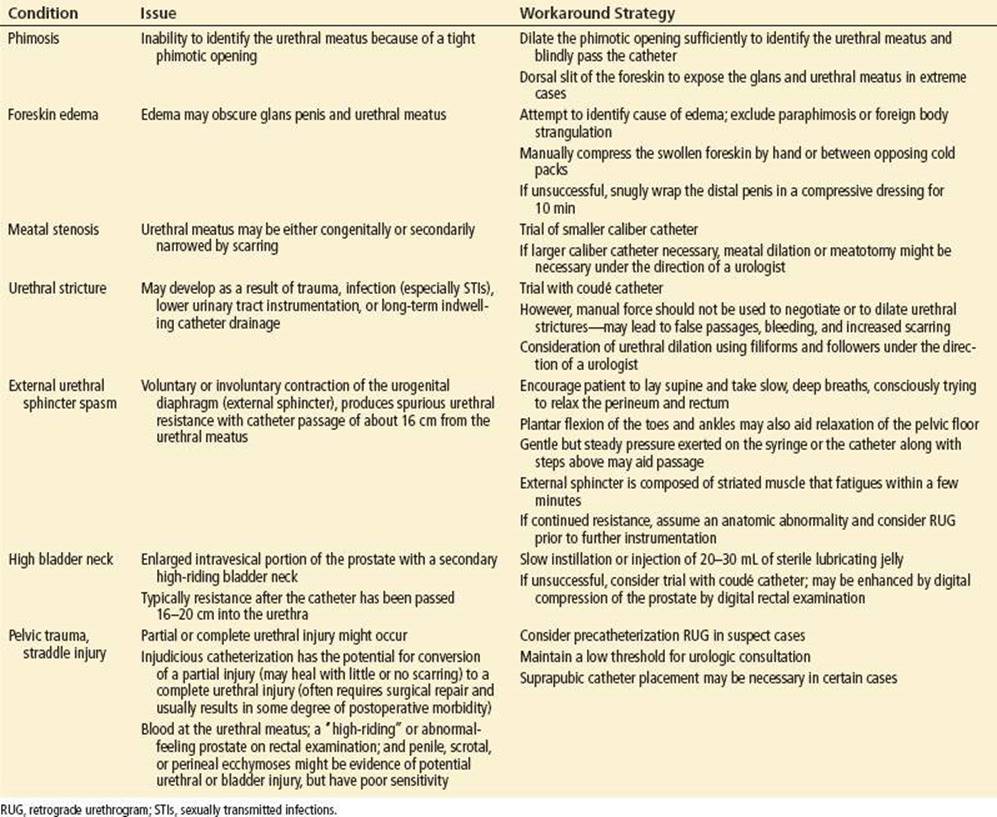
The male urethra is divided into the anterior (penile, bulbous) and posterior (membranous, prostatic) portions (Fig. 128.1). The penile and bulbar urethras are the most common sites of urethral strictures. Strictures are usually noticed when the catheter cannot be advanced more than halfway into the bladder, and the procedure is often accompanied by significant discomfort. There should not be attempts to force the catheter through a stricture. This force may create false passages in the urethra, which can lead to urethral diverticuli, incontinence, infection, and fistula formation. If this situation is encountered, further attempts to place the catheter should be discontinued until a urology consult is obtained. The stricture may require a dilatation procedure or urethroplasty.
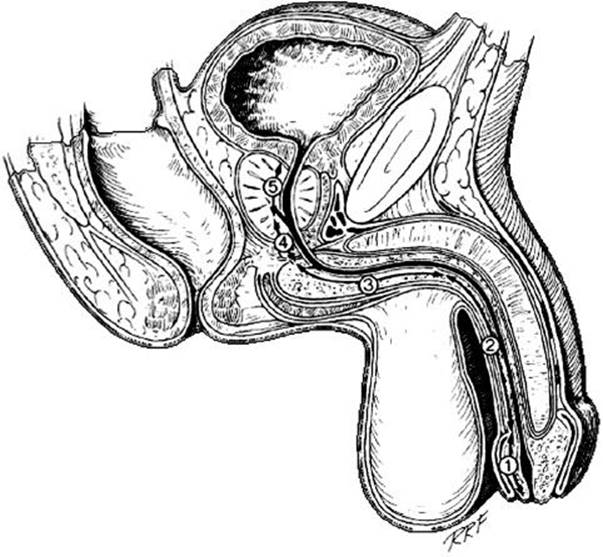
FIGURE 128.1 Anatomy of the male urethra. (1) Fossa navicularis, (2) pendulous urethra, (3) bulbous urethra, (4) membranous urethra, and (5) prostatic urethra. (From Jordan GH, Schellhammer PF. Urethral surgery and stricture disease. In: Droller M, ed. Surgical Management of Urologic Disease. St. Louis, MO: Mosby Year Book; 1992:394.)
The site for the most common problems for placement of male urinary catheters is the prostatic urethra, where the lobes of the prostate create a narrowed lumen. The incidence of benign prostatic hypertrophy (BPH) increases dramatically with advancing age, and the vast majority of men older than 70 years have the anatomical changes, signs, and symptoms of BPH. There are a few basic techniques that can help in passing the tip of the catheter around an enlarged prostate. The use of a coudé catheter is often helpful. This catheter has a firm, upturned end which slips over the enlarged gland (1). Other techniques include placing a finger in the rectum and applying gentle pressure to the prostate as the catheter is passed, or injecting a water-soluble lubricant retrograde into the urethra to decrease friction. Patients who have undergone a radical or simple prostatectomy commonly have bladder neck contractures, and coudé catheters are similarly helpful in these patients. In instances when the ED placement of a catheter has been unsuccessful, urology consultation may be necessary.
Although the vast majority of difficult catheterizations occur in men, occasional difficulties arise in the catheterization of women. Women have short, straight urethras, which are easy to traverse with a standard urethral catheter. At times, however, identifying the urethral meatus can be problematic. Obese women may have redundant labial tissues, which can make visualization of the meatus difficult. Placing the patient in the frog-leg position, using adequate lighting, and having an assistant retract redundant tissue will often aid in the location of the urethral meatus and subsequent placement of the catheter.
Occasionally, prolapse of the pelvic organs (cystocele, enterocele, rectocele, or uterocele) can obscure the view of the female meatus. Simply applying gentle pressure to the offending organ should assist in bringing the meatus into view. Some women have a partially prolapsed urethra called a caruncle, which can distort the normal anatomy. A standard urethral catheter can usually be placed around the caruncle without difficulty.
Complications from the placement of urinary catheters occur uncommonly. If too much pressure is applied to a urethral catheter that is being impeded by a stricture or large prostate, a false passage can be created. This is a result of undermining the urethral mucosa; the consequences may include significant hematuria, stricture formation, and infection. In certain situations involving pelvic trauma, urethral integrity should be assured via a retrograde urethrogram (RUG) prior to the placement of a urinary catheter (Fig. 128.2).
FIGURE 128.2 Anatomy of the male urethra, normal retrograde urethrogram. (1) Fossa navicularis, (2) pendulous urethra, (3) bulbous urethra, (4) membranous urethra, and (5) prosthatic urethra. (Courtesy of Michael Antonis, DO, RDMS.)
Occasionally a urethral catheter cannot be removed from a patient because the balloon will not deflate. The easiest maneuver is to cut the valve off the end of the catheter, which may facilitate removal. If this technique fails to relieve the obstruction, a guidewire can be introduced into the balloon lumen of the catheter to attempt to relieve a balloon port obstruction preventing egress of balloon contents. If this method fails and the catheter needs to be removed emergently, a urologist may have to perform invasive maneuvers to better facilitate catheter removal.
A catheter may be forcibly pulled out of the bladder in patients with altered sensorium or other issues. Replacing the catheter is usually not difficult, but consideration should be given to any resulting injuries. Repeatedly pulling out a urinary catheter puts the patient at risk for developing incontinence secondary to external sphincter damage, and may also lead to hematuria with significant blood loss. If a urethral catheter that has been removed traumatically cannot be replaced easily, urology consultation should be obtained, and performance of a RUG should be considered.
Urinary tract infection is a complication of a long-term urethral catheter. The duration of catheterization is the most important risk factor for the development of catheter associated bacteriuria (2). The incidence of bacteriuria with indwelling catheterization is 3% to 8% per day. The rate might be considerably higher in hospitalized, elderly, debilitated, or postpartum patients. By 1 month, nearly all patients with an indwelling catheter will have bacteriuria. Urinary catheterization is the leading cause of nosocomial infection (2). Other less frequent complications of long-term indwelling urethral catheterization include bladder stones, recurring bladder spasm, periurethral abscesses, urethral stricture formation, bladder perforation (3), and urethral erosion (4).
When a catheterized patient presents with a urinary tract infection, the catheter should be changed. Patients with long-term need for catheterization should have them changed monthly. Antibiotic treatment is usually not indicated for asymptomatic patients, and may in fact select for antibacterial resistance. Many studies have documented the overuse of urethral catheters, and the best strategy for preventing catheter-related infections is the more judicious use (5).
Other problems from long-term indwelling catheters include local infections (epididymitis, balanitis, and prostatitis), erosive hypospadias, and bladder stone formation (6). In general, urethral catheters are not the treatment of choice for debilitated or incontinent patients, and their indications should be carefully considered. Other options include intermittent catheterization, condom catheters, and suprapubic catheters.
THREE-WAY IRRIGATION CATHETERS
Placement of a three-way irrigation catheter may be required in ED patients complaining of gross hematuria and exhibiting symptoms of bladder obstruction. Gross hematuria is often complicated by obstruction secondary to the formation of blood clots. Significant bleeding should be treated aggressively with three-way catheter placement and bladder irrigation to maintain patency of the urethra and to accurately monitor the amount of bleeding. If gross hematuria persists or copious blood clots are encountered, continuous bladder irrigation can be therapeutic.
A three-way irrigating catheter is needed in patients who require continuous bladder irrigation. Three-way catheters have three ports, one providing standard access to urinary drainage, a second to instill irrigating solution, and a third to control the inflation of the balloon. Sterile saline or water may be infused passively through the irrigation port using a reservoir (Kelly) bag placed above the level of the bladder. There are several types of three-way catheters, ranging from a soft plastic coudé type to others with large holes at the distal end to facilitate the passage of large clots. When there is significant bleeding and clot formation, the three-way catheter with the largest tolerated diameter should be used.
SUPRAPUBIC CATHETERS
Suprapubic catheters are placed in patients for a variety of reasons revolving around a need for alternative bladder drainage. Suprapubic catheters that have been in place for longer than a month form a mature fistulous tract and therefore can be removed and changed without fear of losing tract patency. Changing the catheter over a guidewire facilitates this procedure. Before replacing a suprapubic catheter, the bladder should be filled with saline or water to facilitate the correct placement of the new catheter into the bladder.
Suprapubic catheters may also become obstructed with mucous or debris. The catheter should be flushed to attempt to relieve the obstruction, which is similar to the procedure used with a standard urinary catheter. Suprapubic catheters should be replaced every 4 to 6 weeks or when they are suspected to be the nidus of an infection.
Occasionally there is a need to emergently place a suprapubic catheter in the setting of urinary retention when standard catheterization has failed, or in the setting of a traumatic urethral disruption. This should be performed by a consulting urologist when one is available, though the procedure is straightforward. Several techniques are described, the most common involving a percutaneous Seldinger technique, threading the catheter over a guidewire placed into the bladder via a suprapubic needle puncture. Patients who are significantly obese, have had prior abdominal or genitourinary surgery, or have had multiple prior suprapubic catheters are suboptimal candidates for percutaneous suprapubic tubes and usually require an open procedure in a more controlled operative setting to reduce the risk of complications.
URETERAL STENTS
The placement of ureteral stents is a common practice in urology to facilitate adequate urine flow through the ureter. The most common reason is for stone disease. A ureteral stent may be placed after a large kidney stone is treated. The most common stents are double-J stents that can be identified on plain films by the curls that are in both the bladder and the renal pelvis. Emergency physicians should be aware of their indications, complications, and side effects.
Stents are placed to allow the unimpeded passage of urine and to aid in the passage of stones into the bladder. Patients who have signs and symptoms of infected urine and also have signs of urinary obstruction (e.g., by stones or strictures) often have stents placed emergently to allow adequate drainage of urine and to prevent septic complications (see also nephrostomy tubes below).
Pain is the most common complication associated with urethral stents. The pain usually results from irritation of the mucosa of the renal pelvis or the bladder. Patients commonly complain of flank pain, dysuria, frequency, gross hematuria, and urgency. The symptoms usually abate in time but may require the use of narcotic pain medications. Symptoms may also be alleviated by oral anticholinergic agents, which may be started in consultation with a urologist. Other complications include infection, migration, obstruction, and encrustation. Bacterial colonization of ureteral stents is common. Patients with a urinary stent in place who exhibit signs or symptoms of urinary infection should be promptly treated with antibiotics, including adequate coverage for Pseudomonas species (7). Urology consultation is prudent in this situation.
Large obstructing ureteral calculi (e.g., greater than 10 mm in diameter) may impede the retrograde passage of a ureteral stent. Occasionally, a patient’s anatomy does not allow perfect alignment of the ureteral stent in either the bladder or the renal pelvis, leading to stent migration. The stent can move proximally in the ureter or distally toward the bladder and often fails to function correctly. A one-view abdominal radiography (kidneys, ureters, and bladder [KUB]) is helpful in assessing stent location (Fig. 128.3).

FIGURE 128.3 A kidneys, ureter, and bladder view showing a stent in proper placement.
Stent encrustation (stone formation around a stent) and obstruction may occur when ureteral stents are not removed or changed for long periods of time. Patients can develop hydronephrosis or renal failure as a result. Urgent consultation for stent removal or replacement is often necessary.
NEPHROSTOMY TUBES
The primary urgent indication for percutaneous nephrostomy (PCN) catheter placement is to relieve an obstructed, infected renal collecting system (pyonephrosis). Pyonephrosis represents infection (pus) that is under pressure (obstructed collecting system). Pyonephrosis is associated with significant morbidity and mortality if not treated swiftly and aggressively. Relief of obstruction remains the cornerstone of treatment, with appropriate broad-spectrum intravenous antimicrobials playing an important adjunctive role.
Retrograde ureteral stents and PCN catheters have been demonstrated to be equally effective in relieving obstruction, with similar complication rates (8). The advantages of PCN catheters include: wide variety of available catheter sizes, ability to irrigate the catheter to avoid or alleviate clogging, direct measurement of urinary output from the affected kidney, and minimizing ureteral manipulation as to decrease the risk of precipitating sepsis or ureteral rupture. In addition, the procedure can typically be performed under local anesthesia with procedural sedation. Depending on institutional capabilities and local protocol, the procedure can be performed by an interventional radiologist. Advantages of cystoscopic ureteral stenting over PCN include decreased bleeding risk by avoiding puncture of the highly vascular renal capsule, lack of an external catheter exiting the flank, and often less postprocedural patient discomfort.
Emergent PCN is also utilized in the treatment of obstructive uropathy from a variety of causes associated with acute renal failure. Another general indication for PCN catheter placement is access to the renal collecting system for diagnostic or therapeutic procedures. PCN catheter placement may also be utilized as a secondary procedure if initial ureteral stent placement is unsuccessful, or fails to alleviate signs or symptoms of pyonephrosis. Major complications of PCN include sepsis, hemorrhage, vascular injury, bowl injury, or pleural complications. Complications occur in 2% to 6% of procedures, and have a higher frequency when PCN is performed after-hours likely owing to the overall higher risk profile of patients necessitating emergency intervention (Fig. 128.1) (9).
The decision regarding cystoscopy with ureteral stent versus PCN catheter placement for the treatment of pyonephrosis is multifactorial, and typically guided by a urologist in conjunction with an interventional radiologist if necessary. In general, however, emergent PCN catheter decompression is the treatment of choice in septic or otherwise unstable patients given anesthetic risks. In less extreme circumstances, a trial of cystoscopic ureteral stent placement is typically advocated as the first line in treatment.
URINARY CONDUITS
Bowel is sometimes used to serve as a surgically created conduit for urine; for example, this may be done after radical cystectomy for invasive bladder cancer. The most common form of urinary conduit is an ileal conduit formed by a small piece of ileum that has been removed and attached to the ureters. The distal end is then made into a stoma at the abdominal wall, and the urine is collected in an external urostomy bag. Other procedures include formation of a neobladder that is orthotopically placed, allowing the patient to void in the normal fashion. Another option is the formation of a stoma that may be catheterized through the umbilicus using a straight catheter.
As with any large abdominal and pelvic operation with bowel manipulation, patients may later develop a small bowel obstruction. Hernias can develop around the stoma (parastomal) or at the surgical site (incisional). Because the ureter is sutured to the bowel, a stricture can develop at the anastomosis, potentially causing hydronephrosis, insidious renal failure, pyelonephritis, or urosepsis. Because the ureteroileal anastomosis allows the free reflux of urine, pyelonephritis is common in these patients. Because conduits are chronically colonized with fecal flora, positive urine cultures should typically be treated only if the patient is symptomatic.
CRITICAL INTERVENTIONS
• Quickly place a urinary catheter to relieve acute urinary retention.
• Use a coudé-tip catheter for difficult placement of the catheter if the prostate or bladder neck is the area of obstruction.
• Place a three-way irrigating catheter for treatment of gross hematuria with clots.
• Urinary obstruction with associated infection (pyonephrosis) is an emergency, necessitating prompt decompression of the collecting system by cystoscopy with ureteral stent or by placement of a PCN tube.
• Perform a RUG prior to attempts at urinary catheterization if there is any question about urethral integrity.
Common Pitfalls
• Overzealous attempts by staff to place a urinary catheter leading to the formation of a false passage.
• Failure to consult urology after unsuccessful attempts at catheter placement.
• Overuse of antibiotics in the asymptomatic patient with a chronic, colonized catheter.
• Failure to treat pyonephrosis promptly by decompression of the urinary collecting system.
ACKNOWLEDGMENT
We wish to acknowledge the work of Dr. Paul E. Pamphrus on the previous edition of this chapter.
REFERENCES
1. Bregenzer T, Frei R, Widmer AF, et al. Low risk of bacteremia during catheter replacement in patients with long-term urinary catheters. Arch Intern Med. 1997;157(5):521–525.
2. Hooton TM, Bradley SF, Cardenas DD, et al. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin Infect Dis. 2010;50(5):625–663.
3. Farraye MJ, Seaberg D. Indwelling Foley catheter causing extraperitoneal bladder perforation. Am J Emerg Med. 2000;18:497–500.
4. Steidle CP, Mulcahy JJ. Erosion of penile prostheses: A complication of urethral catheterization. J Urol. 1989;142:736–739.
5. Saint S, Lipsky B. Preventing catheter-related bacteriuria: Should we? Can we? How? Arch Intern Med. 1999;159(8):800–808.
6. McDowell G, Hayden L, Wise H. Penile necrosis secondary to an indwelling Foley catheter. J Urology. 1987;138:1243–1244.
7. Farsi HM, Mosli HA, Al-Zemaity MF, et al. Bacteriuria and colonization of double-pigtail ureteral stents: Long-term experience with 237 patients. J Endourology. 1995;9(6):469–472.
8. Pearle MS, Pierce HL, Miller GL, et al. Optimal method of urgent decompression of the collecting system for obstruction and infection due to ureteral calculi. J Urol. 1998;160:1260–1264.
9. Lewis S, Patel U. Major complications after percutaneous nephrostomy: Lessons from a department audit. Clin Radiol. 2004;59:171–179.