Rebecca R. Roberts and Basem F. Khishfe
Patients in acute distress from mental health causes seek treatment in the emergency department (ED). EDs also provide medical evaluations prior to civil commitment for many patients in psychiatric crisis (1). The purpose is to detect the presence of medical illness complicating or causing psychiatric symptoms. Differentiating between functional (psychiatric) and organic (medical) causes of behavioral abnormalities may seem arbitrary. However, arranging the proper tests, treatments, consultants, and site of care depends on accurately making this differentiation. Several studies have documented high rates of patients receiving treatment for psychiatric illnesses that were really caused by treatable but undetected medical illness (2,3). In addition, patients with functional psychiatric syndromes such as schizophrenia often have comorbidities that go undetected or undertreated, leading to excess mortality (4).
CLINICAL PRESENTATION
The term organic brain syndrome (OBS) covers a range of clinical manifestations. The first two, delirium and dementia, are always presumed to be due to organic causes. Specific changes in cognitive function can help distinguish between delirium and dementia (5) (Table 152.1).
TABLE 152.1
Diagnostic Criteria for Delirium and Dementiaa

Delirium is often due to a life-threatening illness (5–10). In the elderly, it may be one of the most common disease presentations and is associated with high mortality rates (8,9,11). Delirium is defined first by disturbed consciousness. Patients have altered awareness of the environment; difficulty in focusing, sustaining, or shifting their attention; and reduced ability to concentrate (6). Delirious patients may be hyperalert and have inappropriately fearful responses to normal stimuli. They may be hallucinating, hyperactive, or combative. There are also disturbances in at least two of the following: Perception, language, sleep cycles, memory, or psychomotor activity (6). However, the patient’s limited awareness and inability to concentrate often make testing of these functions impossible (10). Delirium is also likely to resolve when the patient recovers from the underlying cause (5,11).
Dementia is now often referred to as a spectrum called neurocognitive disorders (6). It refers to the more gradual development of intellectual impairment sufficient to interfere with social and physical functioning (5,10). The hallmark finding is progressive impairment of memory. Memory deficits can be remarkable in patients who appear to function well otherwise. The diagnosis requires one additional cognitive impairment, such as loss of language, visual–spatial, or abstraction ability; impaired judgment; personality change; or reduced organizational ability (6). In contrast to delirium, consciousness is not clouded and deficits develop slowly over a more prolonged time course (5,10). The maintenance of normal consciousness and self-awareness and the slow progression can result in severe loss of function before family or providers detect the problem. In fact, it is frequently an acute precipitant such as medical illness or a change in living situation that calls attention to the long-term decline.
In addition to delirium and dementia or neurocognitive disorders, all of the major psychiatric diagnostic groups can be closely mimicked by the effects of medications or medical illnesses (7,12). Medical illness can cause clinical manifestations similar to those of psychosis, mania, depression, anxiety disorders, or even personality disorder. In some cases, a neuropsychiatric manifestation is the first symptom prompting treatment (12,13). Finally, medical illness can cause an acute worsening of behavioral symptoms in patients with chronic existing psychiatric diseases that were previously well controlled (14).
DIFFERENTIAL DIAGNOSIS
The first challenge is to distinguish between functional psychiatric illness and OBS (7). One of the most important features in OBS is cognitive dysfunction (7,16). This may be undetectable unless actively sought (17). Most patients with functional disorders, even schizophrenic patients, have normal vital signs, motor and speech function, cognitive function, and memory (12). Thus, abnormalities in these areas cannot be assumed to reflect chronic psychiatric illness. OBS can also be distinguished from functional disorders by comparing the patient’s syndrome to the standard psychiatric definitions (6). The presence of atypical features point to an organic cause (12).
It is useful to note similarities among delirium, dementia, and the more standard psychiatric diagnoses. Delirium shares features with anxiety disorder, acute psychosis, or mania (5,18). Alcohol withdrawal is a form of delirium (19). Dementia can appear similar to depression, chronic schizophrenia, or personality disorder. This same overlap in cause can assist in working through the differential diagnosis.
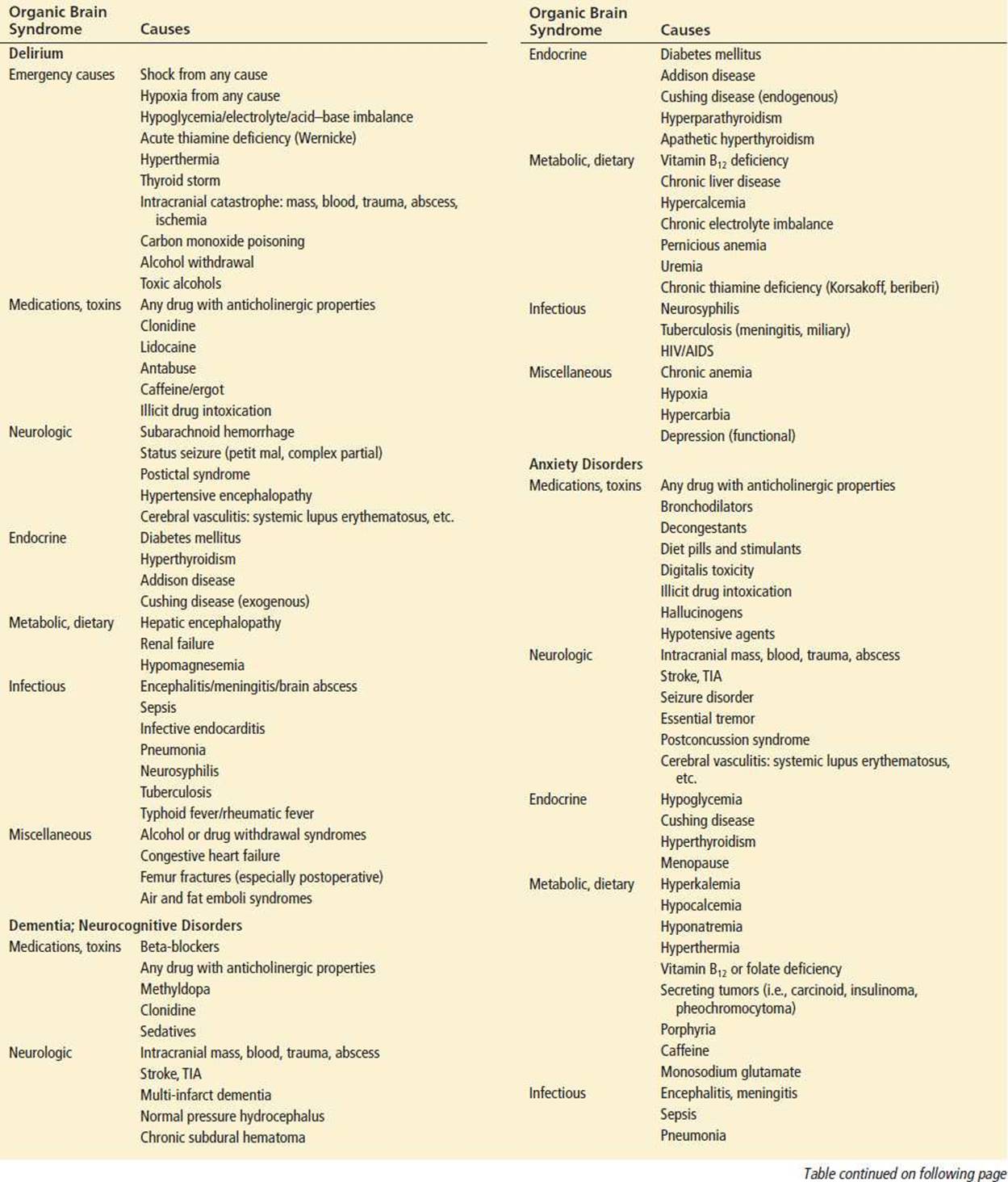
Many medical problems can result in compromised mental functioning and what appear to be manifestations of psychiatric disease (2,7,15,18). Table 152.2 lists the most common causes by clinical syndrome. Medications are by far the most common (7). The major life-threatening causes can be summarized as any profound disruption in blood or nutrient supply to the brain: Shock; hypoxia; sepsis; anemia; hypoglycemia; hypertensive encephalopathy; hyperthermia; fluid, electrolyte, or acid–base imbalance; carbon monoxide; intracranial infection or mass; or stroke (2,7,18). Alcohol withdrawal and Wernicke encephalopathy require emergent recognition and treatment. Infections, both neurologic and systemic, are important causes of OBS. Some infections such as viral encephalitis are seasonal (20,21). Metabolic derangements with behavioral symptoms are common in liver, renal, pulmonary, thyroid, pituitary, and adrenal diseases (2,7,21). Trauma, illicit drugs, and toxins are common in the young (3,22). Patients with HIV infection may present with symptoms of secondary HIV mania as a first sign, and they are also more susceptible to CNS infections (13,23). Altered behavior in patients with cancer, heart disease, collagen vascular disease, or HIV infection should also prompt consideration of organic causes.
TABLE 152.2
Causes of Organic Brain Syndrome by Manifestationa

ED EVALUATION
Any patient with neuropsychiatric symptoms should receive a thorough history, physical and mental status examination (3,16,17). Often, the history must be obtained from family or paramedics. Sometimes family members can articulate only that the patient has changed or worsened in some indefinite way. A frequent complaint in the elderly is a sudden refusal or inability to eat (1). The history should include information on medications, alcohol and drug use (including over-the-counter and herbal preparations), recent hospitalizations, surgeries, or trauma (5,12,19,24,25). Past psychiatric, endocrine, pulmonary, cardiac, renal, hepatic, malignant, and collagen vascular diseases and potential exposure to medications or toxins and risk factors for HIV infection are important history questions (2,7,13,17,23,26). Complaints such as headache, focal neurologic deficits, abdominal pain, dyspnea, fever, incontinence, nonauditory hallucinations, weight loss, cough, vomiting, or diarrhea also point to organic causes (1).
The patient’s normal level of functioning and the pattern and rate of behavioral change must be ascertained. A recent abrupt change in a previously normal patient or new additional psychiatric manifestations in patients with chronic illness, are key signs of organic cause (7,8,11,27). Visual hallucinations, distortions, or illusions are also important clues to an organic etiology (12). Beware of missing new delirium occurring in a patient with chronic dementia. For example, acute worsening of chronic dementia can occur with a new stroke, pneumonia, sepsis, myocardial infarction, new medications, or metabolic, endocrine, or rheumatologic derangements. Sometimes it is not clear what precipitated the ED visit of a patient with chronic dementia. Sensitive questioning can reveal that family members no longer feel able to safely care for the patient and desire help or even nursing home placement. In other cases, the patient has had a catastrophic anger reaction that the family did not mention because they did not recognize it as a classic manifestation of dementia.
Physical examination findings indicative of an organic cause include abnormal vital signs, diaphoresis, jaundice, or pallor. Any motor disturbance such as tremor or partial complex seizure activity should be noted (12); either increased or decreased psychomotor activity levels may be seen (15). Signs of thyroid or adrenal disease should be sought. A complete neurologic examination, including gait and tests of cognitive function, is required (7,15,16). Certain findings on mental status examination indicate an organic cause for behavioral changes. A neat, well-groomed appearance in a patient who is now disorganized indicates a very abrupt onset (17). Altered awareness of the environment, anxiety, labile mood, or rapid changes in mental status are associated with OBS, as are language abnormalities, altered speech, or disordered visual–spatial abilities. The new onset of mania in a patient older than the age of 30, or psychosis in patients older than 40, is highly unusual and should prompt testing for organic causes.
When ordering tests to detect the cause of OBS, it helps to categorize those causes as medication-related, toxicologic, neurologic, endocrine, metabolic, dietary, infectious, hepatic, renal, cardiac, or pulmonary. The specific evaluation should be guided by findings in the history, physical, and mental status examinations (7). Glucose, electrolytes, complete blood count, and renal function tests should be obtained (12). Additional useful testing may include electrocardiography, liver and thyroid function tests, toxicology, and arterial blood gases for hypoxia, CO2 retention, and carbon monoxide exposure. A chest x-ray, urinalysis, and blood and urine cultures should be done when infection is suspected. Most patients warrant computed tomography of the head and lumbar puncture with cerebrospinal fluid cultures, including tests for tuberculosis and viral encephalitis (12). In patients with dementia, additional testing for correctable causes should include vitamin B12, folate, thyroid, and syphilis testing (28).
ED MANAGEMENT
ED management generally depends on the underlying cause of OBS. The physician’s first task is to rapidly identify and treat life-threats and then to take action to prevent injury (e.g., from falling out of bed or wandering away). As unsuspected alcoholism is common and the diagnosis of Wernicke encephalopathy or withdrawal can be difficult, thiamine should be given empirically and the glucose level checked early and followed up as necessary (12). Unless it is obvious that the patient is suffering from severe alcohol withdrawal, extra caution is appropriate when initiating sedatives for behavioral control, as another condition may be causing global brain dysfunction, and there may be increased sensitivity to sedatives (11,15). Frequent reassessment is especially critical in patients with delirium, as the underlying causes are so serious and the condition can deteriorate rapidly. One-to-one observation, sedatives, or even restraints, may be necessary to ensure the patient’s safety during evaluation and treatment (9,11,15).
CRITICAL INTERVENTIONS
• Rapidly search for and treat life threatening conditions.
• Distinguish between functional psychiatric illness and organic disease.
• Search for new medical illness superimposed upon a chronic dementia that can cause an acute but reversible decline or change.
DISPOSITION
Nearly all patients suffering from acute OBS need to be hospitalized for continued diagnostic evaluation and treatment or for the assurance of their physical safety (5). An exception is the patient with chronic dementia who has not had an acute decline in function but who is brought to the ED for evaluation of a long-term problem. Any medical illness superimposed upon a chronic dementia can cause an acute but reversible decline, so those with chronic dementia and acute worsening need admission. Another exception is the patient who is suffering from recreational drug or alcohol intoxication that clears in the ED. If these patients are discharged, they must go home with responsible family or friends.
Families caring for patients with progressive dementia need to be warned about the dangers of driving, cooking, or starting fires and to know that patients can wander away or can occasionally exhibit catastrophic anger reactions if they are under stress. It helps families to understand that these reactions can be a normal consequence of dementia. Good follow-up must be ensured. Social services will be helpful in arranging home nursing care.
Psychiatric consultation may assist in the assessment of competency when the patient’s judgment is in question. Some patients may try to leave the hospital once they are admitted; a recorded psychiatric competence evaluation is extremely helpful to hospital staff (9,11). Patients with acute impairment of judgment or consciousness or with cognitive deficits do not have sufficient decision-making capacity to sign themselves out of the hospital against medical advice (30). There is growing use of empiric symptom severity scores, such as the Organic Brain Syndrome Score for assessing OBS, and there are inpatient intervention programs that show promise for improvement in diagnosis and management (9,11,25,27).
Common Pitfalls
• Failing to do a complete history, physical, and mental status examination in all patients with psychiatric symptoms (3,7,16).
• Failing to note abnormal vital signs as an indicator of possible organic causes.
• Assuming that apparent psychiatric symptoms are due to functional psychiatric disorders (3,7).
• Assuming that physical complaints in a psychiatric patient are due to functional causes (1).
• Failing to detect a mild early cognitive deficit or assuming that it is due to chronic functional illness.
• Missing acute delirium that occurs in a patient with chronic dementia.
• Becoming distracted by combative or abnormal behavior and thus failing to follow through in performing a complete evaluation and frequent reassessments.
REFERENCES
1. Korn CS, Currier GW, Henderson SO. “Medical clearance” of psychiatric patients without medical complaints in the emergency department. J Emerg Med. 2000;18(2):173–176.
2. Koranyi EK. Undiagnosed physical illness in psychiatric patients. Ann Rev Med. 1982;33:309–316.
3. Reeves RR, Pendarvis EJ, Kimble R. Unrecognized medical emergencies admitted to psychiatric units. Am J Emerg Med. 2000;18(4):390–393.
4. Mitchell AJ, Malone D. Physical health and schizophrenia. Curr Opin Psychiatry. 2006;19:432–437.
5. Murphy BA. Delirium. Emerg Med Clin North Am. 2000;18(2):243–252.
6. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorder, DSM-5. 5th ed. Arlington, VA: American Psychiatric Association; 2013.
7. Dorsey ST, Bazarian JJ. Medical conditions that mimic psychiatric approach for evaluation of patients who present with psychiatric symptomatology. Emerg Med Rep. 2002;23(20):233–243.
8. Edlund A, Lundstrom M, Karlsson S, et al. Delirium in older patients admitted to general internal medicine. J Geriatr Psychiatry Neurol. 2006;19:83–90.
9. Lundstrom M, Edlund A, Karlsson S, et al. A multifactorial intervention program reduces the duration of delirium, length of hospitalization and mortality in delirious patients. J Am Geriatr Soc.2005;53:622–628.
10. Meyers J, Stein S. The psychiatric interview in the emergency department. Emerg Med Clin North Am. 2000;18(2):173–183.
11. Grace JB, Holmes J. The management of behavioural and psychiatric symptoms in delirium. Expert Opin Pharmacother. 2006;7:555–561.
12. Talbot-Stern JK, Green T, Royle TJ. Psychiatric manifestations of systemic illness. Emerg Med Clin North Am. 2000;18(2):199–209.
13. Nakimuli-Mpungu E, Musisi S, Kiwuwa Mpungu S, et al. Primary mania versus HIV-related secondary mania in Uganda. Am J Psychiatry. 2006;163:1349–1354.
14. Sokolski KN, Denson TF. Exacerbation of mania secondary to right temporal lobe astrocytoma in a bipolar patient previously stabilized on valproate. Cogn Behav Neurol. 2003;16:234–238.
15. Samuels SC, Evers MM. Delirium. Pragmatic guidance for managing a common, confounding, and sometimes lethal condition.Geriatrics. 2002;57(6):33–38.
16. Irons MJ, Farace E, Brady WJ, et al. Mental status screening of emergency department patients: Normative study of the quick confusion scale. Acad Emerg Med. 2002;9(10):989–994.
17. Williams ER, Shepherd SM. Medical clearance of psychiatric patients. Emerg Med Clin North Am. 2000;18(2):185–198.
18. Arora M, Daughton J. Mania in the medically ill. Curr Psychiatr Rep. 2007;9:232–235.
19. Olmedo R, Hoffman RS. Withdrawal syndromes. Emerg Med Clin North Am. 2000;18(2):273–288.
20. Griffin DE. Encephalitis, myelitis, neuritis. In: Mandell GL, Bennett JC, Dolin R, eds. Mandell, Douglas, and Bennett’s: Principles and Practice of Infectious Disease. Vol 1. 6th ed. Philadelphia, PA: Elsevier; 2005:1143–1149.
21. Monnet FP. Behavioural disturbances following Japanese B encephalitis. Eur Psychiatry. 2003;18:269–273.
22. Horwath E. Psychiatric and neuropsychiatric manifestations of HIV infection. J Int Assoc Phys AIDS Care. 2002;1(suppl 1):S1–S15.
23. Trevisani VFM, Castro AA, Neves Neto JF, et al. Cyclophosphamide versus methylprednisolone for treating neuropsychiatric involvement in systemic lupus erythematosus (review). Cochrane Database Syst Rev. 2006;2:115.
24. Lundstrom M, Edlund A, Bucht G, et al. Dementia after delirium in patients with femoral neck fractures. J Am Geriatr Soc. 2003;51:1002–1006.
25. Lundstrom M, Olofsson B, Stenvall M, et al. Postoperative delirium in old patients with femoral neck fracture: A randomized intervention study. Aging Clin Exp Res. 2007;19:178–186.
26. Kato T, Shiratori K, Kobashigawa T, et al. Systemic lupus erythematosus with organic brain syndrome: Serial electroencephalograms accurately evaluate therapeutic efficacy. Intern Med. 2006;45:95–99.
27. Bjorkelund KB, Larsson S, Gustafson L, et al. The Organic Brain Syndrome (OBS) Scale: A systematic review. Int J Geriatr Psychiatry. 2006;21:210–222.
28. Carluccio A, Sundaram N, Yanagisawa R, et al. Apathetic thyrotoxicosis secondary to atypical subacute thyroiditis. Case report. Endocr Pract. 2012;18:5.
29. Drugs that may cause psychiatric symptoms. Med Lett Drugs Ther. 2002;44(1134):59–62.
30. Miller SS, Marin DB. Assessing capacity. Emerg Med Clin North Am. 2000;18(2):233–242.
31. Petz L. Neurological manifestations of systemic lupus erythematous and thrombotic thrombocytopenic purpura. Stroke. 1977;8:719–722.
32. Renoir T. Selective serotonin reuptake inhibitor antidepressant treatment discontinuation syndrome: A review of the clinical evidence and the possible mechanisms involved. Front Pharmacol. 2013;4:45.
33. Wall C. Myxedema coma: Diagnosis and treatment. Am Fam Physician. 2000;62(11):2485–2490.