Christian M. Neff and Stephen C. Hartsell
The term purpura (Latin meaning “purple”) refers to any skin or mucous membrane eruption resulting from bleeding into the skin. The defining characteristic of purpuric lesions is the absence of blanching, whereas color persists with compression.
Broadly speaking, purpura may result from abnormalities in primary or secondary hemostasis (thrombocytopenia, abnormal platelet function, clotting factor deficiency, abnormal clotting factor function) or disruptions in vascular integrity (trauma, infection, vasculitis, medications, collagen disorders). Deficiencies in platelet number or function are a far more common cause of purpuric skin lesions than are defects or deficiency of a single procoagulant clotting factor (1).
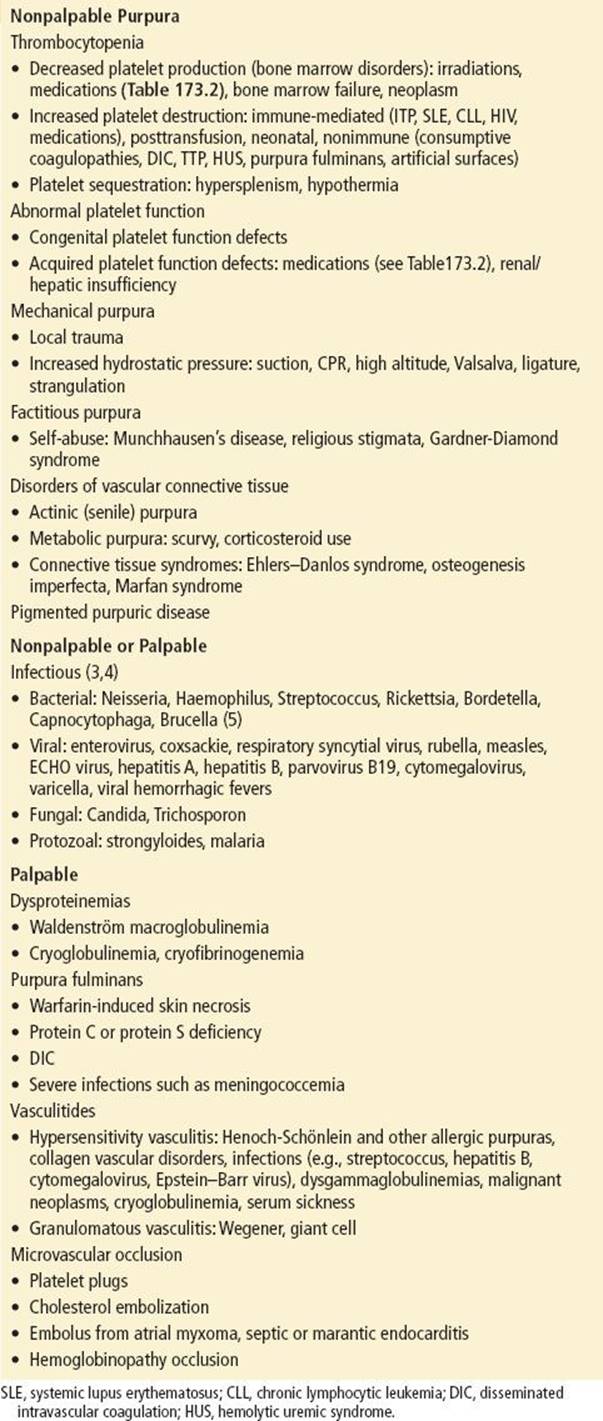
The etiologies of purpura are extensive and range from the trivial (e.g., actinic purpura in the elderly, “bruises” secondary to minor trauma) to the life-threatening (e.g., meningococcemia, thrombotic thrombocytopenic purpura [TTP]) (Table 173.1). Rapid differentiation of benign from potentially serious causes of purpura is essential, as it allows for the initiation of emergent treatments where indicated while minimizing unnecessary evaluation.
TABLE 173.1
Causes of Purpura by Morphologic Characteristics
CLINICAL PRESENTATION
Patients with purpura may present to the emergency department due to concern about the rash itself or because of symptoms accompanying the rash. Regardless of the appearance of the rash or associated symptoms and signs, the presence of spontaneous bleeding (“wet” purpura) is a grave sign requiring immediate intervention (2). The cause is usually thrombocytopenia, and the emergent treatment is platelet transfusion. The immediate threat to life is intracranial hemorrhage (2). Severe anemia and shock from blood loss are possible but not common.
Patients without spontaneous bleeding (“dry” purpura) may have extensive petechiae or ecchymoses on the skin but are in less immediate danger. However, spontaneous bleeding may develop at any time, so rapid determination of the cause is still indicated.
Purpuric lesions vary in color, size, consistency, shape, associated erythema, and distribution. These morphologic variations may provide clues to the etiology of the lesions. Purpuric lesions must have a shade of color consistent with hemorrhage. Lesions may be red, blue, purple, yellow-brown, green, or black (1). Lesions are classified by their varying sizes. Lesions <3 mm are termed petechiae, whereas lesions >3 mm are termed purpura (3). Lesions >1 cm in diameter are termed ecchymoses (1). They may be flat and nonpalpable or raised and palpable, with a round or a retiform (branching) shape. Associated erythema may be prominent or absent. The distribution may be localized or generalized. Purpura may appear with a variety of other lesions, depending on the underlying cause and stage of development.
DIFFERENTIAL DIAGNOSIS
The etiologies of purpura are extensive and they encompass hematologic, dermatologic, infectious, traumatic, and rheumatologic entities (see Table 173.1) (1). In addition, purpura may be caused by a variety of drugs, which can cause small-vessel or platelet disorders by direct toxicity, inhibition of function, or immune-mediated mechanisms (Table 173.2) (6,7).
TABLE 173.2
Drugs Causing Purpura

The lesions of purpura are characteristic and difficult to mistake for other types of lesions. Other erythematous rashes, such as viral exanthems and urticaria, can be differentiated from purpura by their light-red color, and in that they blanch with pressure. Similarly, telangiectases and hemangiomata are discrete collections of abnormally dilated blood vessels that appear bright red and usually blanch with pressure. Diascopy, the use of a glass slide to apply pressure over a lesion, is a simple visual method to differentiate lesions due to vascular dilation (which blanch with pressure) from those due to purpura (which do not).
Some lesions are purpuric but do not reflect an underlying illness, and are sometimes classified as mechanical or factitial purpura (3). Purpuric lesions may be created by trauma or increased hydrostatic pressure in normal skin. Examples of mechanisms potentially resulting in purpuric lesions are self-inflicted trauma, forceful or protracted vomiting or sneezing, strangulation, suction, and coining (3,8).
ED EVALUATION
The initial focus of the emergency department evaluation of purpura is to identify and initiate treatment of any life-threatening disorders. Empiric, potentially life-saving treatments (e.g., platelet transfusion or intravenous antibiotics) should be initiated based on the presumptive diagnosis and preliminary laboratory results without awaiting definitive diagnosis. Intracranial hemorrhage should be considered in any patient presenting with purpura associated with neurologic abnormalities, and emergent treatment, usually with platelet transfusion, should be initiated. Meningitis and/or meningococcemia are suggested by purpura associated with fever, altered mental status, headache, neck stiffness, or systemic toxicity, and require emergent resuscitation and treatment with antibiotics. While the initial rash associated with meningococcal infection may be a maculopapular eruption resembling a wide variety of viral exanthems, more than 50% of patients have petechiae or purpura upon presentation (9,10). Active bleeding or wet purpura should likewise be considered a dermatohematologic emergency. Attention should be paid to the presence of bleeding gums, epistaxis, intraocular hemorrhage, guaiac-positive stool, menorrhagia, or hematuria. Marked thrombocytopenia is almost universally the cause of wet purpura, and platelet transfusion should not be delayed while awaiting laboratory confirmation when bleeding is significant.
In patients presenting with purpura without signs or symptoms of a life-threatening emergency, evaluation should be pursued to elucidate the cause of the purpura. A directed patient history should include recent infections, recent medication or drug ingestion, irradiation or chemical exposure, and systemic symptoms. History of abnormal or spontaneous bleeding (frequent epistaxis, bleeding after dental or other minor procedures, menorrhagia, etc.) should be elicited. Questions relating to hepatic, renal, rheumatologic, or hematologic disease, malignancy, immunosuppression, or human immunodeficiency virus (HIV) infection are also pertinent. A complete list of medications and allergies should be obtained. Except for hereditary coagulation disorders, which rarely present as purpura, and rare hereditary thrombocytopenias, the family history is usually unremarkable. The social history should include questions regarding alcohol and drug use and risk factors for HIV.
Initial physical examination should pay particular attention to markers of serious systemic illness such as fever and other vital sign abnormalities, altered mental status, meningismus, or active bleeding.
Characterization of the purpuric lesions may provide clues to etiology. The distribution of the lesions may suggest specific disease processes. Senile or actinic purpura occurs on sun-exposed areas, usually the forearms, of elderly patients. Vasculitic purpura is usually symmetric and predominates in the lower extremities (e.g., Henoch-Schönlein purpura) (Fig. 173.1). A more generalized distribution of discrete petechiae may be noted when purpura is associated with bacterial illness such as meningococcemia or subacute bacterial endocarditis. Purpuric lesions in thrombocytopenia tend to occur in areas of minor trauma or areas of pressure, such as the belt line or over bony prominences. The purpura of scurvy classically appears as perifollicular petechiae, whereas that of Rocky Mountain spotted fever begins over the distal joints and spreads centrally. The lesions of purpura fulminans are large, symmetric ecchymoses of the lower extremities and buttocks, often with infarcted areas or bullae.

FIGURE 173.1 Henoch-Schönlein purpura. (Courtesy of Dr. Sate Hazma, dermatopathology fellow, University of Birmingham, and Dr. Amy Theos, Assistant Professor, Department of Dermatology, University of Alabama at Birmingham.)
Lesions may be categorized into groups of likely diagnosis based on size, palpability, morphology, and the associated erythema (1,3). Nonpalpable purpuric lesions result primarily from a decrease in the number of functioning platelets or from mechanical insults to the vascular barrier. Nonpalpable purpuric lesions >1 cm may be caused by major trauma or minor trauma coupled with a procoagulant defect or poor dermal vessel support (1). Palpability results from edema, which most commonly results from inflammation, but also may be seen with microvascular occlusion and ischemia (1). Erythema is usually present with inflammation and absent with microvascular occlusion and ischemia.
When bacterial infections cause purpura, the lesions may have a central purulent papule (e.g., disseminated gonococcemia). Immune-mediated vasculitides often have lesions of erythema, bullae, or urticaria in association with palpable purpura. Coumadin-associated vasculopathy may result in necrotizing ecchymoses.
The physical examination may further reveal specific abnormalities in certain causes of purpura. In thrombocytopenia, the optic fundi and mucous membranes may show petechiae. Painful joint effusions may accompany various types of immune-mediated purpura, disseminated gonococcemia, and coagulation disorders. Lymphadenopathy or lesions characteristic of Kaposi sarcoma may be indicators of HIV seropositivity, which may present with purpura in up to 9% of cases (11). Lymphadenopathy may also be found in patients with lymphoma, infectious mononucleosis, and leukemia. Splenomegaly (as well as other forms of hypersplenism) may also be noted in these same illnesses but is absent in most other types of thrombocytopenic purpura (e.g., idiopathic thrombocytopenic purpura) and coagulation defects (1).
All but trivial causes of purpura (e.g., actinic, mechanical, factitial) require laboratory studies to elucidate the underlying cause. As thrombocytopenia is the most common cause of clinically significant purpura, a platelet count is a required component of initial testing. Easy bruising may be noted with platelet counts of 30,000 to 50,000/μL, whereas spontaneous ecchymoses or petechiae usually do not appear until the platelet count is less than 30,000/μL. Internal bleeding, including intracranial hemorrhage, rarely occurs with platelet counts >10,000/μL (12). For example, in a study of patients with thrombocytopenia secondary to immune thrombocytopenia (ITP), minimal bleeding after trauma was uncommon unless the platelet count was less than 60,000/μL, whereas self-limited bleeding, spontaneous bleeding requiring intervention (e.g., nasal packing for epistaxis), and severe life-threatening bleeding did not occur until platelet counts were <40,000, <12,000, and <6,000/μL, respectively (13).
A complete blood count with differential serves as a screen for anemias, bone marrow disorders, various malignancies and infection. The peripheral blood smear screens for abnormal red blood cell and platelet morphology which may be indicative of hemolysis and various platelet abnormalities, respectively. Prothrombin time and activated partial thromboplastin time screen for coagulation or mixed platelet and/or coagulation disorders (14,15). Determination of bleeding time may be of limited use in the emergency department in confirming platelet dysfunction or vascular disorders. The fibrinogen level, along with fibrin–fibrinogen degradation products (FDP, D-dimer), may also be useful (14). Because therapy with blood products is sometimes necessary and their use may confound subsequent diagnosis, extra tubes for type and screen and for other platelet and coagulation assays should be obtained before treatment.
On subsequent (usually inpatient) evaluation, the following tests may be indicated, depending on the suspected etiology: bone marrow aspiration, skin biopsy, bleeding time, autoimmune disease screening tests, clotting factor assays, and platelet function tests (15).
KEY TESTING
• CBC
• PT/INR, PTT
• Peripheral blood smear
• Fibrinogen level, fibrin degradation products
• D-dimer
ED MANAGEMENT
First, life-threatening complications of spontaneous bleeding should be stabilized, and efforts should be made to ascertain the cause of purpura. As described, the history, physical examination, and laboratory studies should allow rapid determination of the category of illness causing the purpura and associated symptoms.
When thrombocytopenia is the cause of purpura, platelet transfusion should be considered only when there is evidence of abnormal bleeding. Generally, each unit of platelets may be expected to raise the platelet count by about 5,000 to 10,000/μL (16). Spontaneous mucous membrane or CNS bleeding can usually be controlled when the platelet count is restored to more than 20,000/μL. Platelet transfusion is relatively contraindicated in disorders caused by intravascular thrombosis such as TTP because platelets may contribute to further thrombosis. In TTP, plasma exchange is the only treatment for which there is firm data on its effectiveness (17). When immune-mediated thrombocytopenia is likely, as in immune thrombocytopenic purpura or posttransfusion purpura, the half-life of transfused platelets is short (hours) compared with that for other disorders (days) (2). In these cases, alternative therapy, such as corticosteroids, immunoglobulins, or splenectomy may eventually be indicated (12,18).
Coagulopathies presenting with spontaneous bleeding may be treated by replacement of specific coagulation factors. In acquired coagulopathies from coumadin or liver disease, vitamin K is indicated. Fresh frozen plasma may be helpful in a variety of coagulopathies and thrombolytic disorders when specific factor replacement is not available or cannot be determined (19).
If purpura is thought to be due to a drug (Table 173.2) regardless of the suspected mechanism, that drug should be discontinued. Anticoagulants or platelet inhibitors (in proper dosages) may be reinstituted, if indicated, when the disorder is controlled.
Specific therapy directed to underlying disorders should be initiated once the etiologic factors have been defined and a diagnosis established.
CRITICAL INTERVENTIONS
• Intervene immediately with the combination of purpura and spontaneous bleeding (wet purpura).
• Intracranial hemorrhage should be considered in patients presenting with purpura and associated neurologic symptoms.
• Meningococcemia and/or meningitis suggested by purpura associated with fever, altered mental status, meningismus, or systemic toxicity represent a life-threatening emergency requiring immediate treatment.
DISPOSITION
Because purpura may reflect hematologic, rheumatologic, traumatic, or infectious disorders, consultation is obtained from appropriate specialists once trivial causes of purpura have been excluded. When the diagnosis is unclear, a dermatology consultation is warranted. Because the underlying disorders that are responsible for purpura often have the potential for progressing to life-threatening emergencies, patients with purpura are often admitted to the hospital for confirmation of the diagnosis and definitive treatment. Patients presenting with spontaneous bleeding or life-threatening complications, such as CNS hemorrhage or septic shock, require immediate hospital admission, usually to an intensive care unit.
Emergency transfer of patients with life-threatening complications of purpuric illness is indicated when the needed blood products, specialty consultation, or level of care are not available. Stabilization with intravenous fluids and emergently indicated blood products (when available) should be accomplished before transfer, after consultation with the accepting physician. Patients whose illness may progress rapidly should be considered for air ambulance transfer when ground transport times would be prolonged.
Common Pitfalls
• Failure to recognize the signs and symptoms of emergent conditions associated with purpura, such as intracranial hemorrhage and serious bacterial infections, may result in devastating delays in treatment.
• Failure to consider the trivial causes of purpura may result in unnecessary time and expense spent in pursuing a diagnostic workup.
• Drugs are a common cause of purpura and, unless an adequate history of drug exposure is obtained, the causal agent may initially be missed.
• Dismissing associated mucous membrane or spontaneous bleeding (wet purpura) may result in delay in therapy (usually platelet transfusion) and increased risk of life-threatening hemorrhage.
• Premature administration of drugs or blood products may delay laboratory diagnosis, and in some cases, may worsen the disease process responsible for the purpura.
REFERENCES
1. Piette WW. Hematologic diseases. In: Freedeberg IM, Eisen AZ, Wolff K, et al., eds. Dermatology in General Medicine, 6th ed. New York, NY: McGraw-Hill; 2003:1523.
2. Crosby WH. Wet purpura, dry purpura. JAMA. 1975;232:744–745.
3. Key NS, Phillips MD, Levy ML. Vascular purpura and diseases of blood vessels. In: Loscalzo J, Schafer A, eds. Thrombosis and Hemorrhage, 2nd ed. Baltimore, BA: Lippincott Williams & Wilkins; 1998:763.
4. Young NS, Brown KE. Parvovirus B19. NEJM. 2004;350:586–597.
5. Massasso D, Gibson K. Brucellosis mimicking Henoch-Schonlein purpura. Med J Aust. 2007;186:602–603.
6. Aster RH, Bougie DW. Drug-induced immune thrombocytopenia. NEJM. 2007;357:580–587.
7. Visentin GP, Liu CY. Drug-induced thrombocytopenia. Hematol Oncol Clin North Am. 2007;21(4):685–696.
8. Friedman-Kien AE, Laurenstein LJ, Rubinstein P, et al. Disseminated Kaposi’s sarcoma in homosexual men. Ann Intern Med. 1982;96:693–700.
9. Wolf RE, Birbara CA. Meningococcal infections at an army training center. Am J Med. 1968;44(2):243–455.
10. Carpenter RR, Petersdorf RG. The clinical spectrum of bacterial meningitis. Am J Med. 1962;33:262–275.
11. Ratner L. Human immunodeficiency virus–associated autoimmune thrombocytopenic purpura: A review. Am J Med. 1989;86:194–198.
12. Cines DB, Blanchette VS. Immune thrombocytopenic purpura. NEJM. 2002;346:995–1008.
13. Lacey JV, Penner JA. Management of idiopathic thrombocytopenic purpura in the adult. Semin Thromb Hemost. 1977;3:160–174.
14. Rogers GM, Bithell TC. The diagnostic approach to the bleeding disorders. In: Lee GR, Foerster J, Lukens J, et al., eds. Wintrobe’s Clinical Hematology, 10th ed. Baltimore, BA: Williams & Wilkins; 1999:1557.
15. Taylor RE, Blatt PM. Clinical evaluation of the patient with bruising and bleeding. J Am Acad Dermatol. 1981;4:348–368.
16. Schafer AI. Acquired disorders of platelet function. In: Loscalzo J, Schafer A, eds. Thrombosis and Hemorrhage, 2nd ed. Baltimore, BA: Williams & Wilkins; 1998:707.
17. George JN. Thrombotic thrombocytopenic purpura. NEJM. 2006;354:1927–1935.
18. Psaila B, Bussel JB. Immune thrombocytopenic purpura. Hematol Oncol Clin North Am. 2007;21:743–759.
19. Cohen H. Avoiding the misuse of fresh frozen plasma. BMJ. 1993;307:395–396.