Rupali Das, MD, MPH
Melanie Marty, PhD
Marilyn C. Underwood, PhD
BACKGROUND
Many millions of chemical compounds are known today. Of these millions, about 84,000 are on U.S. EPA’s Toxic Substances Control Act (TSCA) inventory of existing commercial chemicals, and approximately 1000–3000 are introduced into the market every year. In the European Union (EU) under the Registration, Evaluation, and Authorization of Chemicals (REACH) program, the registration phase resulted in 143,000 distinct chemicals registered for use in commerce. The processing, use, transport, and disposal of these chemicals present hazards to human health. This was painfully illustrated in 1985 when an accidental release of methyl isocyanate in Bhopal, India, caused death and injury to many thousands of people, resulted in increased public awareness of the effects of chemicals released into the environment. This incident sparked a host of international regulations aimed at preventing the recurrence of a similar tragedy. Routine and accidental releases of hazardous chemicals into air and water, and releases of hazardous waste on land continue to occur. Several recent incidents reveal the critical need for emergency preparedness for intentional releases of hazardous chemical agents. The tsunami off the coast of Japan in 2011, hurricanes that hit the Gulf Coast of North and Central America in 2005, and the “superstorm” that hit the northeastern United States in 2012 caused massive devastation and highlight the need to better plan for chemical releases following natural disasters. Public health and emergency planners now focus on “all-hazards planning,” including chemical, biologic, radiologic, nuclear, and explosions (CBRNE).
The United States and the EU have the most comprehensive and complex environmental laws for the regulation of pollution. Environmental laws have traditionally been grouped according to both environmental media and the nature of pollutants: air pollution, water pollution, noise pollution, hazardous waste, hazardous materials management, remediation of contaminated soil and groundwater, and registration of toxic substances and pesticides.
This chapter discusses health hazards resulting from routine, and accidental releases of hazardous chemicals and waste material into the environment and the laws that are intended to regulate polluting industries and prevent adverse health effects from occurring. This chapter is divided into three sections: routine industrial emissions, accidental releases, and hazardous waste. Each section discusses relevant health-based environmental regulations and the evaluation of potential health effects.
ROUTINE INDUSTRIAL EMISSIONS
In our modern technologic society, industries produce an enormous variety of products using vast amounts of chemicals and numerous physical processes. All industrial processes are associated with emissions of chemicals into the air, water, and/or land. In the 1970s, the United States began to seek information on the impacts of these emissions on human and ecologic health. This section focuses on available information on the extent and public health impacts of emissions into air in the United States.
Industrial emissions include an array of familiar and unfamiliar chemicals, relatively few of which are well characterized toxicologically. While some epidemiologic studies have been useful for characterizing toxicity and the public health impacts of several air pollutants and a number of chemicals in the occupational setting, most information on potential health effects of industrial chemicals comes from animal toxicology studies. Animal studies generally involve exposures of a genetically homogeneous population of rodents to one chemical at a time. Thus little direct knowledge exists about the interactions of chemicals or the consequences of exposure to many chemicals simultaneously in genetically and socially heterogeneous human populations. Sources of airborne emissions are varied and range from large facilities such as oil refineries to small sources such as gas stations, auto body shops, and dry-cleaning operations. Emissions are somewhat characteristic for specific industrial processes and source types.
TYPES OF SOURCES & EMISSIONS TO THE AIR
Air pollutants have been characterized for regulatory purposes into two basic categories: criteria air pollutants (CAPs) and hazardous air pollutants (HAPs) (or toxic air contaminants [TACs] in California programs). The distinction is somewhat arbitrary in that both categories of emissions are toxic. Further, a number of other chemicals can be emitted from industrial facilities that are of concern due to toxicity, but are not on the list of HAPs or TACs.
![]() Criteria Air Pollutants
Criteria Air Pollutants
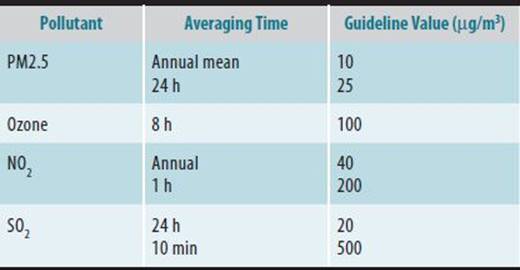
Criteria air pollutants (CAPs) are typical components of smog and were first identified by environmental scientists as posing public health risks in the 1960s. CAPs include chemicals emitted in large quantities and from many sources such as carbon monoxide (CO), sulfur oxides (SOx), nitrogen oxides (NOx), and particulate matter (less than 10 and 2.5 μm in diameter, or PM10 and PM2.5). The descriptor criteriarefers to those chemicals for which there are regulatory standards determined by the U.S. Environmental Protection Agency (EPA) or, in California, by the Air Resources Board (ARB). The standards are air concentrations that are designed to protect public health and which are not to be exceeded for specified durations if an area is to be in compliance with the Clean Air Act. Table 45–1 summarizes the federal ambient air quality standards. Guidelines for general public exposure are also available from the World Health Organization. Table 45–2 summarizes the WHO guidelines for several air pollutants.
Table 45–1. Ambient air quality standards.
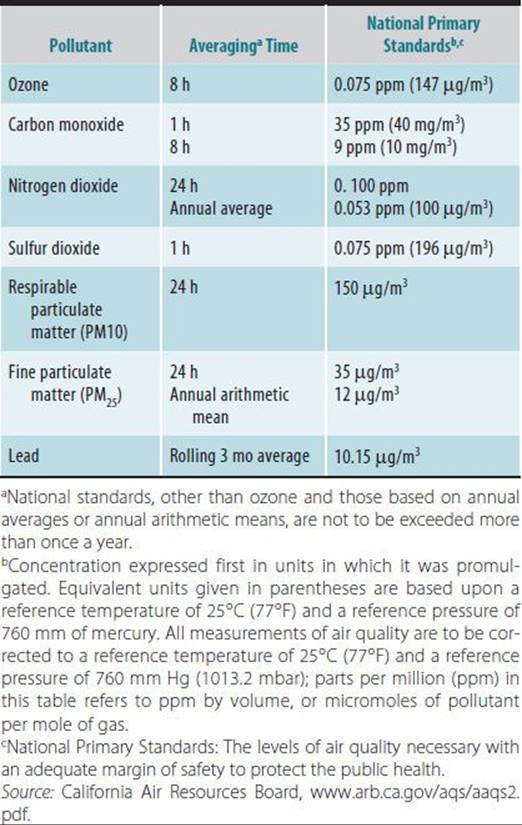
Table 45–2. World Health Organization guidelines for air pollution.
![]() Hazardous Air Pollutants
Hazardous Air Pollutants
Hazardous air pollutants (HAPs) are chemicals emitted into the air that are not CAPs and for which there is some regulatory concern. The U.S. EPA maintains a list of chemicals that have been formally identified as HAPs. Under EPA authority, HAPs are subject to specific regulatory requirements. Similarly, California has listed TACs, which includes all the HAPs as well as other substances, that are subject to stationary and mobile source emissions controls by the ARB.
![]() Types of Sources
Types of Sources
There are a great number of sources of airborne chemicals, which, for regulatory purposes, are divided into mobile sources (primarily cars, trucks, and buses) and stationary sources. Mobile sources are responsible for the majority of emissions of fuel components, and products of incomplete combustion including CAPs. The remainder of this section addresses stationary sources of airborne industrial emissions. Major stationary sources include large industrial complexes such as refineries and aerospace and chemical manufacturing facilities. Major sources usually have large energy requirements and fulfill these demands via combustion of fuels, resulting in significant CAP emissions, including CO, NOx, SOx, and PM2.5. Refineries are some of the largest emitters of CAPs, releasing hundreds of tons per day of SOx and NOx. NOx reacts with hydrocarbons emitted into the air to produce ozone on hot, sunny days. Thus ozone, a major component of photochemical smog, is not emitted directly but represents one reaction product from atmospheric transformation.
Minor stationary sources usually are associated with lower emissions of CAPs than major sources. Yet minor sources can be important emitters of TACs, which are process-dependent. Small dry-cleaning sources emit tetrachloroethylene, a probable human carcinogen. Incinerators, which can be found at both large and small facilities, emit an array of products of incomplete combustion ranging from CO to complex chlorinated compounds such as the carcinogenic 2,3,7,8-tetrachlorodibenzo-p-dioxin (dioxin) and related congeners, as well as metals and acid gases. Polycyclic aromatic hydrocarbons (PAHs), some of which are carcinogens, are high-molecular-weight products of incomplete combustion emitted by incinerators and combustion processes. Metal-finishing operations usually are small sources but may be associated with potentially significant public health impacts. The known human carcinogens hexavalent chromium and nickel are used extensively in metal-finishing operations.
EMISSIONS DATABASES
The EPA maintains the Toxics Release Inventory (TRI), a database of stationary source emissions to air, water, and land, for specified compounds. In addition, the State of California maintains databases of emissions of toxic chemicals to the air from stationary sources. These databases are described below.
![]() National Toxics Release Inventory
National Toxics Release Inventory
In 1986, Congress enacted the Superfund Amendments and Reauthorization Act (SARA) and added Title III, known as the Emergency Planning and Community Right-to-Know Act (EPCRA). Section 313 of SARA Title III created the TRI and gave the EPA authority to collect information quantifying emissions of more than 682 chemicals and chemical classes emitted by industrial sources. A number of hazardous air pollutants are included in the emissions inventories. SARA Title III’s passage was stimulated by the tragedy in Bhopal. Part of the premise for the statute is that citizens have a right to know about toxic materials used, stored, and released into the environment in their communities. The statute also mandates emergency planning for chemical accidents (see following section).
Facilities that need to report emissions to the EPA are generally those that produce, import, or process 25,000 lb or more of a listed substance or use in any manner 10,000 lb or more of a listed substance in a given reporting year. The reporting requirements for persistent bioaccumulative toxic (PBT) chemicals are 0.1 g for dioxins and dioxin-like compounds, and 10–100 lb for other PBTs. Reporting facilities are those with a Standard Industrial Code (SIC) 20–39. These are the SICs for facilities engaged in manufacturing or that fall into one of the following industrial categories: metal mining, coal mining, electric utilities that combust coal and/or oil, chemical wholesale distributors, petroleum terminals and bulk storage facilities, hazardous waste treatment and disposal facilities, and all federal facilities. Reporting facilities have 10 or more full-time employees.
Emissions to air, discharges into surface water, disposal into on-site landfills, injection of liquid wastes into underground wells, transfer of wastes to publicly owned wastewater treatment works, and transfers of chemicals to off-site facilities for treatment, storage, or disposal all must be reported. Both routine releases and accidental spills are covered in the emissions reports. The Pollution Prevention Act of 1990 added further reporting requirements to SARA Title III that result in an ability to compare years by percent change and require the facility to estimate emissions for future years. In addition, the amended act allows information to be gathered regarding on-site or off-site recycling of chemical wastes and source-reduction practices and opportunities.
The TRI database and EPA’s Annual Report are available online at www.epa.gov/tri/ and through the National Library of Medicine’s TOXNET computer system. A mapping function of TRI sources for regional or local areas can be found at http://toxmap.nlm.nih.gov/toxmap/main/index.jsp. EPA’s annual report includes state and county-level data and is available on CD-ROM in public libraries. The EPA provides a search tool, the TRI Explorer, on its Web page that can query the database for emissions information by chemical, including from specific facilities.
TRI data are used for a variety of purposes. The EPA and state and local agencies use the data to identify potential exposures and risks and emissions-reduction opportunities, and to track progress toward pollution reduction. Public interest groups use the data to help educate the public about toxics in their communities, to pressure industry into reducing toxic emissions, and to lobby the government to change policies. Industries use the information to help in pollution-reduction efforts.
In 2011, 20,927 facilities reported under TRI. The total waste produced including that recycled, burned for energy, treated, or released was 22.77 billion pounds. Of this total amount of chemical waste, 4.09 billion pounds were released into the environment for all TRI industries. Of the 26 TRI industry sectors that report chemical releases, metal mining, electric utilities, and chemical manufacturing account for 46%, 15%, and 12% of the total TRI releases, respectively. On-site air emissions totaled 0.8 billion pounds, while on-site water, land, and underground injection totals were 0.22 billion, 2.44 billion, and 0.22 billion pounds, respectively. Some of the chemicals reported under TRI are classified as persistent, bioaccumulative toxicants, or PBTs. These types of chemicals are of concern because they have long environmental half-lives and can accumulate in humans. Approximately 1 million pounds of PBTs were emitted into the air, 0.5% of the total PBT environmental releases. PBT chemicals released into air included 2.9 lb of dioxin and dioxin-like compounds, 89,000 lb of mercury and mercury compounds, 593,000 lb of lead and lead compounds, 322,000 lb of PAHs, and 368 lb of polychlorinated biphenyls (PCBs).
Emissions from facilities reporting to TRI appear to have decreased over time. The U.S. EPA reports an 8% decrease from 2003 to 2011, driven largely by declines in air releases primarily from electric utilities. Notably, mercury emissions have decreased since 2003 by 36% likely due to shifts away from coal and installation of control technologies on coal-fired power plants. The TRI program motivates facilities to decrease their emissions. Poor public relations associated with being an emitter and a desire for more efficient operations and more recovery and recycling of waste have resulted in a decrease in overall emissions to the environment from the manufacturing sector.
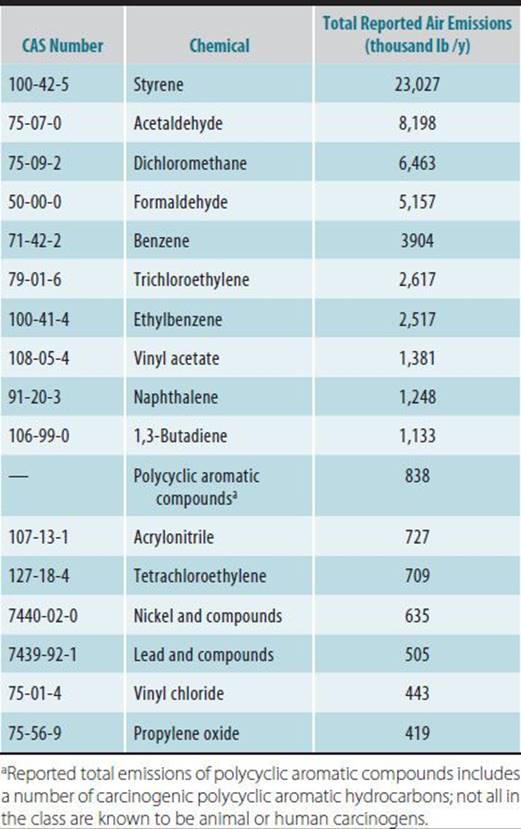
Table 45–3 presents the 15 most common chemicals released into the air from TRI facilities in the United States in 2011. Those carcinogens with reported airborne releases totaling over 400,000 lb are presented in Table 45–4. The most commonly emitted chemicals have toxicity criteria developed by either the EPA or state agencies. These criteria are useful for estimating public health hazards through a risk-assessment process. Of the carcinogens in Table 45–4, benzene, formaldehyde, nickel, trichloroethylene, 1,3-butadiene, and vinyl chloride are classified by the International Agency for Research on Cancer (IARC) as known human carcinogens. In addition, a number of occupations involving high exposure to PAHs are associated with elevated lung cancer risk, and the classification of benzo(a)pyrene was recently updated by IARC to Group 1, known human carcinogen.
Table 45–3. Top 15 TRI chemicals by volume of reported air emissions, 2011.
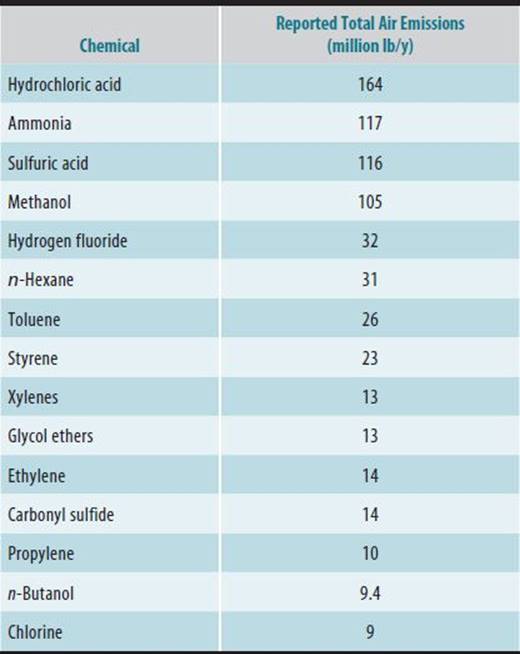
Table 45–4. TRI carcinogens emitted into air in quantities greater than 400,000 lb in 2011.
The TRI data provide useful information on industrial releases into the environment. However, limitations in reporting may result in overall underreporting of total environmental releases, particularly to air, for some chemicals. Small facilities can be major contributors when their emissions are summed. Moreover, many large facilities emit substances into the environment but do not fall into the TRI reporting categories. It should be noted that mobile sources contribute a great deal to airborne toxic chemicals. For example, benzene and 1,3-butadiene emissions reported in TRI represent a small fraction of total emissions into the air of these two chemicals that are emitted primarily from mobile sources. Further, there are many chemicals formed during atmospheric transformation reactions. For example, the majority of airborne formaldehyde results from atmospheric transformation of precursors. Finally, the toxic chemicals released from use of consumer products are not considered in TRI.
![]() California’s Air Toxics Hot Spots Inventory
California’s Air Toxics Hot Spots Inventory
The California legislature passed the Air Toxics Hot Spots Information and Assessment Act in 1987 (Health and Safety Code Sections 44300 et seq.), partially in response to the Bhopal tragedy. The act allows the California Air Resources Board (CARB) to generate a comprehensive inventory of emissions of over 400 chemicals, including TACs, from stationary sources in the state and has a community right-to-know provision. The intent of the act is to gather information for cost-effective statewide toxics risk reduction, to provide citizens with information on toxics emitted into the air in their communities, and to require emissions reductions from facilities posing significant public health risks.
Emissions inventories are generated by the facilities and submitted to the local air pollution control district and the CARB. The districts prioritize facilities into categories of high, medium, or low concern based on the amount of pollutant emitted, toxic potency of pollutants, and proximity to populations. Facilities in the high-priority category are required to conduct a quantitative risk assessment of their airborne toxic emissions, which includes air-dispersion modeling and exposure estimates, and a quantitative assessment of the associated individual and population-wide health risks. If the facility is deemed by the district to pose significant risk, the facility must notify the community and engage in risk-reduction activity. The California hot spots program differs from the TRI in that there is a large risk-assessment and public-notification component.
The reporting triggers in the California program are considerably lower than for TRI (other than the TRI PBT chemicals); none is above 100 lb/y. In addition, all types of facilities report their emissions, not just those that fall into the TRI categories. In this respect, the Air Toxics Hot Spots Inventory is quite comprehensive for California. Data are available for emissions from small facilities (eg, dry cleaners and auto body shops) as well as from large complex facilities such as refineries. However, unlike the TRI, the California program focuses only on airborne emissions, and there is no comparable database for land or water emissions in California. In addition, the TRI facilities are required to report yearly, whereas the California program only requires reporting every 4 years.
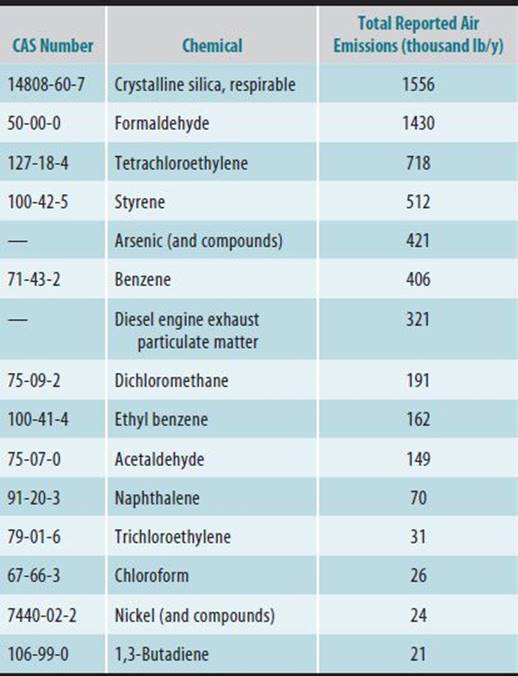
Of over 340 chemicals actually reported as emitted to the air in California in 2011, 80 are emitted in amounts greater than 10,000 lb/y. Table 45–5 summarizes the top 15 chemicals by volume of emissions; Table 45–6 summarizes the top 15 carcinogens emitted by volume. Among these carcinogens, crystalline silica, formaldehyde, arsenic, nickel, benzene, diesel engine particulate matter, trichloroethylene, and 1,3-butadiene are classified by IARC as known human carcinogens. It is interesting to note that the most troublesome chemicals emitted from some sources may not be those with a large volume of emissions. For example, emissions in pounds per year for hexavalent chromium are relatively small (207 lb/y). Yet, because of the high-potency estimates for this known human carcinogen, the near-source cancer-risk estimates can be relatively high. It should be noted that emissions of hexavalent chromium from stationary sources has decreased due to pollution controls. Compared with the California database, tetrachloroethylene emissions to air appear to be grossly underreported in TRI. Tetrachloroethylene emissions from dry cleaners and other sources in California totaled almost 718,463 lb, whereas TRI reports only 709,000 lb for the entire country. This is undoubtedly because many smaller operations use tetrachloroethylene and emit more overall than do those facilities required to report in TRI.
Table 45–5. Top 15 chemicals or chemical mixtures by volume of emissions in California’s 2011 stationary sources inventory.
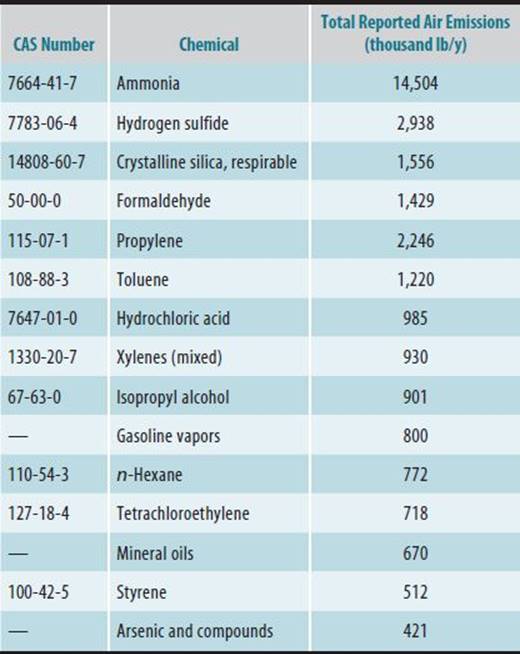
Table 45–6. Top 15 emitted carcinogens by volume in California’s 2011 stationary sources inventory.
Facilities with relatively small emissions may pose high risks to a small number of people if the dispersion characteristics are poor. For example, cancer-risk estimates for dry-cleaning facilities are, in some cases, relatively large for nearby residents because the dry cleaner is located in close proximity to housing and the tetrachloroethylene emissions are poorly dispersed. Measures taken in California to reduce risks from tetrachloroethylene emissions include requiring solvent-recycling equipment and better ventilation and dispersion systems. Regulations adopted in 2007 phase out the use of tetrachloroethylene in dry-cleaning operations by 2023. Emissions reported on both California and the TRI have declined by about half.
Large facilities such as refineries may emit large quantities of material but in some cases have lower cancer-risk estimates than many smaller facilities because residences are located further away, and the materials are emitted from tall stacks, resulting in better dispersion. However, the number of persons exposed to that estimated cancer risk may be considerable. Thus, the population burden of these facilities is larger than smaller facilities impacting few people.
![]() California’s Criteria Air Pollutant Emissions Inventory
California’s Criteria Air Pollutant Emissions Inventory
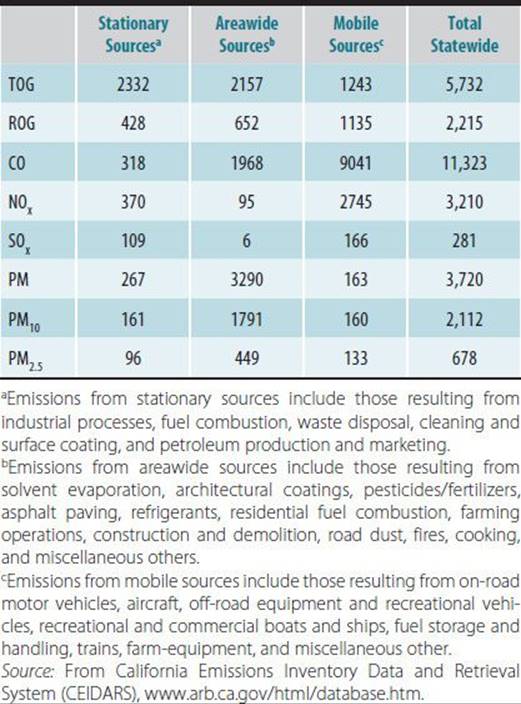
California maintains an inventory of emissions of the criteria air pollutants: CO, NOx, SOx, and particulate matter less than 10 μm (PM10) and less than 2.5 μm (PM2.5) in diameter, as well as emissions of total suspended particulate matter (TSP), reactive organic gases (ROGs), and total organic gases (TOGs). ROGs and NOx combine to form ozone; tracking these two categories of emissions is useful in predicting ozone concentrations. Table 45–7 summarizes the inventory for 2008. The category “Stationary Sources” represents a variety of industrial sources. Industrial emissions account for a significant proportion of total emissions of these pollutants into the air in the state. Emissions listed under “areawide” sources are dominated by consumer products use, architectural coatings, use of pesticides and fertilizers, residential heating, farming operations, and waste burning and disposal. Mobile sources are a major source of all these pollutants because of the combustion of fuels. In addition to tracking emissions of criteria air pollutants, ROGs and TOGs, CARB also maintains a monitoring network to measure ambient air concentrations of these substances. This helps regulators to evaluate air quality, particularly in metropolitan areas of the state, and the effectiveness of pollution-control efforts. Data on air quality are published both quarterly and annually and are available online at www.arb/ca/gov and on CD-ROM from CARB in the publication entitled California Air Quality Data, Air Resources Board, California Environmental Protection Agency.
Table 45–7. Statewide emissions of major components of smog in California in 2008 (tons/day).
IMPORTANCE TO HEALTH CARE PERSONNEL
Epidemiologic studies of adverse health effects of air pollution have focused primarily on the major components of smog, such as ozone, particulate matter, nitrogen oxides, and carbon monoxide. A detailed description of studies is presented in Chapter 46. Recent studies indicate that children growing up in high-pollution areas of the United States (eg, the Los Angeles Basin) suffer from reduced lung function, increased respiratory infections, and induction and exacerbation of asthma. Studies implicate ozone, particulate matter, acid aerosols, and NOx in such respiratory effects. More recent studies suggest traffic-related emissions are causal for asthma in children, and that proximity to major roadways is an important factor for children’s respiratory health. Ozone is a critical component of Los Angeles–type smog and contributes to respiratory and eye irritation. Particulate matter is associated in numerous studies with increased morbidity and mortality from respiratory and cardiac conditions.
To date, there are only a handful of published epidemiologic studies of the association between adverse health effects and exposure to HAPs. In large part, this is a result of the difficulty of such studies, including a lack of exposure data and confounding by other air pollutants. Most of the health impacts of HAPs have been inferred from occupational epidemiologic studies and toxicologic studies in experimental animals. A number of HAPs are carcinogens, while others are respiratory irritants or systemic toxicants. Exposure to HAPs may contribute to respiratory disease, systemic toxicity, and carcinogenicity. There is increasing evidence linking exposure to certain TACs (eg, acrolein, formaldehyde, PAHs, and diesel exhaust particles) to biochemical changes that are characteristic of allergic airways disease, including asthma, such as increases in proinflammatory cytokines and inflammatory cells in bronchiolar epithelium, increased mucin secretion, and elevated antigen-specific immunoglobulin (Ig) E.
Risk assessments conducted for stationary sources in California under the air toxics hot spots program indicate that facility emissions may contribute to cancer and noncancer adverse health effects in surrounding communities. For some industrial processes, risk assessments estimate relatively high (in an environmental context) excess individual cancer risks for people living nearby. Some of the estimated cancer risks from stationary source emissions have been as high as 1 in 1000. There are a large number of causative agents of cancer, and chemical carcinogens emitted into the environment represent one source of these causal agents.
REGULATION OF STATIONARY SOURCES
![]() State Regulations—California
State Regulations—California
The Toxic Air Contaminants Identification and Control Act (1983) created California’s program to reduce health risks from air toxics. This was the first comprehensive state air toxics program to evaluate chemicals in the air and control sources of air toxics. CARB lists about 200 chemicals as TACs. Emissions of TACs from many source types are identified via the air toxics hot spots emissions inventory database and by a program that tests motor vehicle emissions. There are also statewide ambient air monitors that collect data on more than 50 chemicals. After formally identifying a substance as a TAC, CARB investigates the need, feasibility, and cost of reducing emissions of that substance. This process has resulted in air toxics control measures (ATCMs) to reduce emissions from the following sources: gasoline service stations (eg, benzene and other volatiles), chrome plating and anodizing shops (eg, hexavalent chromium), cooling towers (eg, hexavalent chromium), sterilizers and aerators (eg, ethylene oxide), medical waste incinerators (eg, polychlorinated dibenzodioxins and dibenzofurans), serpentine rock in surfacing applications (eg, asbestos), dry cleaning (eg, tetrachloroethylene), metal melting (eg, cadmium, nickel, and arsenic), and low-emission vehicle/clean-fuels regulations (eg, benzene and 1,3-butadiene). A large ongoing effort is reducing emissions dramatically from diesel-fueled engines, both stationary and mobile, resulting in reformulated diesel fuel and a number of ATCMs to curb diesel engine emissions.
Facilities that are subject to the Air Toxics Hot Spots Act and that fall into the high priority category must conduct a risk assessment of their emissions to evaluate public health impacts to the surrounding community. The National Academy of Sciences has defined the health risk assessment for toxicants as four steps: (1) hazard identification, (2) exposure assessment, (3) dose-response assessment, and (4) risk characterization. Risk assessment is described in more detail in Chapter 50. There are comprehensive guidelines for conducting the risk assessments developed by Cal/EPA OEHHA specifically for stationary sources.
In the hazard identification step of risk assessment, the assessor identifies information characterizing the potential toxicity of emitted chemicals, including the toxicological endpoints reported for the chemical. In the Hot Spots program this step involves identifying the emitted chemicals based on the emissions inventories and the hazards associated with exposure to these chemicals.
For the exposure assessment step, the emissions are subject to air dispersion modeling to determine ground-level concentrations in the surrounding communities. The surrounding area is divided into grids and the concentrations modeled for each grid, using information on the emission processes and software developed by the U.S. EPA.
Dose-response assessment involves in-depth evaluation of available human and animal data describing the relationship between exposure or dose and degree of response. There are a number of models that are used to characterize the dose-response relationship. Most recently, the Benchmark Dose approach has been utilized for characterizing the slope of the line for both noncancer toxicological endpoints and carcinogens. Benchmark Dose software is available from U.S. EPA free online at www.epa.gov/ncea/bmds/. USEPA and Cal/EPA have quantified the dose-response relationship for many chemicals. Cancer potency factors generated by the EPA or by OEHHA for carcinogens can be used in risk assessments to estimate the cancer risk posed to the public from exposures to carcinogenic HAPs. The EPA has reference concentrations (RfCs) and the State of California has reference exposure levels (RELs) that are useful in estimating public health impacts for noncancer toxicologic endpoints. Both RfCs and RELs can be viewed as exposure levels at or below which adverse noncancer health impacts are not anticipated. Modeled or measured air concentrations are compared with the RfC or REL to determine the potential hazard. However, there are not enforceable ambient air quality standards for HAPs or TACs. The cancer potency factors, reference exposure levels and reference concentrations, are available from U.S. EPA at http://www.epa.gov/IRIS/ and from California at http://www.oehha.ca.gov/air/hot_spots/index.html.
More than 875 risk assessments conducted by facility operators have been reviewed by the California EPA’s Office of Environmental Health Hazard Assessment. Cancer risks estimated for facilities ranged from 1 in 1 million to 1 in 1000 for lifetime exposures to emitted carcinogens. This program demonstrated that a large number of facilities had risks greater than 10 in 1 million. Typically, regulatory agencies consider an excess individual cancer risk of 1 in 1 million for lifetime exposure to be de minimis. Regulatory activities, such as cleanup of hazardous waste sites or air pollution control requirements, generally are triggered by estimated cancer risk above this level. Initially in the Hot Spots program, about 40% of evaluated facilities posed an estimated cancer risk greater than 10 in 1 million. Key chemicals that drive the cancer risk estimates include benzene, hexavalent chromium, tetrachloroethylene, PAHs, methylene chloride, arsenic, and formaldehyde. Many facilities have taken steps to reduce their emissions and associated risks. Thus the program is a successful motivating force for facilities to reduce emissions partly because of the public-notification provisions.
At the local level, new and modified sources of air pollution are required to obtain operating permits from local air pollution control agencies. The goal is to ensure that new and modified devices are able to meet all air quality standards and not exacerbate air pollution problems in an area. In addition, the air toxics hot spots program risk-reduction provisions for existing facilities are enforced by local air districts and result in enforceable emissions reductions.
![]() Federal Regulations
Federal Regulations
The federal Clean Air Act of 1990 represents a comprehensive statutory framework designed to reduce overall exposure to TACs, protect the stratospheric ozone layer, and reduce deposition of acidic constituents of air pollution (eg, acid rain and acid snow). The Clean Air Act provides for use of market-based principles and other innovative approaches to reducing air pollution. Under Title III of the Clean Air Act, the EPA established a list of 189 HAPs. These HAPs are frequently referred to as air toxics. Technology-based standards have been promulgated by the EPA to control emissions of HAPs from major sources and “area” sources (defined by the EPA as minor sources). Residual risk (cancer and noncancer risks remaining after control devices have been put in place) is being assessed following the implementation of the technology-based standards of air pollution control. Further control measures may be developed if residual risks are considered by the EPA to be unreasonable.
As regards the use of U.S. EPA TRI information, the EPA promotes pollution reduction and provides information on its Web site of best practices to reduce pollution using examples of voluntary efforts by industry to reduce their TRI emissions. While not regulatory, these actions by industry, which include process changes, leak prevention, and raw material changes, make a difference in overall environmental releases. In 2011, about 2300 facilities reported initiating release reduction activities in the United States.
WORLDWIDE PERSPECTIVE
U.S. EPA’s TRI attracted the attention of other countries, and many countries now have a Pollutant Release and Transfer Register (PRTR). The Canadian government established a National Pollutant Release Inventory (NPRI) in 1990, with many similarities to the TRI. This registry reports releases to air, water, and land, and transfers for treatment and disposal of over 300 pollutants and includes about 8000 facilities. Canada’s NPRI has provided information on long-term trends. From 1990 to 2011 large reductions in emissions to the air of heavy metals, SOx, and dioxins have occurred due primarily to pollution control regulatory actions. Data from the NPRI is available on the Environment Canada Web site. Similarly, Mexico has established a PRTR. The three-country Commission for Environmental Cooperation publishes a periodic report compiling information on pollutant releases in North America using data from U.S. EPA’s TRI, Canada’s NPRI and Mexico’s PRTR. Although the chemicals and industrial processes reporting in the three countries are not identical, the report provides a comparison across the three countries emphasizing the similarities in the systems and providing a continental view of pollutant releases. The most recent European Union registry (E-PRTR) includes reporting from 27 member states, Lichtenstein, Iceland, Norway, Serbia, and Switzerland. In this release register, about 28,000 facilities in 9 industrial sectors report their releases of 91 chemicals. The reports are updated on an annual basis. The latest report covers information on environmental releases in 2010 and is available at http://prtr.ec.europa.eu/Home.aspx. Such developments on the international level, which have occurred in 50 countries, facilitate pollution-control efforts on a global scale.
ACCIDENTAL RELEASES
Health care providers, first responders, and public health agencies may be called upon in the event of any large-scale accident. As health care providers gather information that is critical for assessing the public health effects of the release during their evaluation of potentially exposed persons, it is essential for them to be familiar with the health consequences of releases, reporting requirements, relevant regulations, and the steps involved in the public health assessment of chemical releases.
![]() Accidental Chemical Releases & the Role of Health Care Providers
Accidental Chemical Releases & the Role of Health Care Providers
Accidental chemical releases may cause a variety of health effects. However, it may be difficult to relate exposure from a release to alleged injury because preexposure health status information and exposure data may be unavailable. Much of the available information about the public health effects of chemical spills is based on reviews of medical records from initial clinic visits or medical consultations. In addition to providing immediate and continuing medical care, the information gathered can help to improve knowledge about long-term effects of chemicals released into the environment. When a victim of a hazardous substance exposure is evaluated, the following information should be recorded in the medical record:
• Subjective complaints
• General medical history, including the presence of preexisting medical conditions such as asthma, and a history of smoking
• Occupational history, including potential workplace exposures unrelated to the release that might contribute to health complaints
• Exposure history
• Geographic and physical location of the individual relative to the site of the release
• During the incident, the estimated length of time spent at any given location relative to the release
• Activities that may affect the exposure dose of chemical, such as strenuous exercise in the area of the chemical release or consumption of contaminated water or food
• Timing of onset of symptoms relative to potential exposure to accidentally released chemicals
• Identity of the substance(s) released
• Whether fires or explosions occurred as a result of the accident, which could involve exposure to combustion or pyrolysis products
• Physical examination
• Results of specific laboratory tests, such as spirometry, if relevant
Health care providers may play multiple roles following accidental releases of hazardous substances. In order to adequately respond, health care providers should:
• Be prepared with an “all-hazards” approach, relying on general principles of emergency management that can be applied to any natural or man-made incident.
• Be familiar with chemical, biological, radiologic, nuclear, and explosive (CBRNE) agents that have greatest potential for harm.
• Be aware of required reporting of syndromes or illnesses to health agencies.
• Develop and drill disaster response plans.
![]() Accident Statistics
Accident Statistics
A. Prevalence and Causes of Accidental Releases
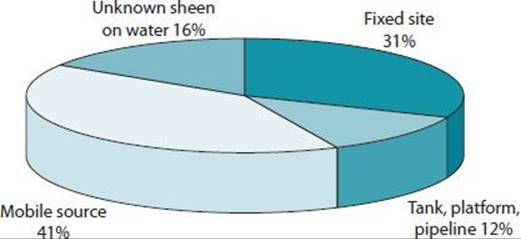
The storage and transportation patterns of hazardous chemicals contribute to the high potential for accidental releases. Both in the United States and worldwide, chemical production continues to rise. Billions of pounds of hazardous chemicals are stored at manufacturing plants around the United States. More than a billion tons of hazardous chemicals are transported annually in the United States by trucks or railroad tank cars. The materials most often transported by rail are liquefied petroleum gas, chlorine, and anhydrous ammonia. Figure 45–1 depicts the source of accidental releases.
![]() Figure 45–1. Source of hazardous substance and oil releases reported to the Emergency Release Notification System, 2012 (32,551 incidents reported). (Reproduced with permission from RTKNet.org, a project of the Center for Effective Government, Washington, DC. http://www.rtknet.org/db/erns.)
Figure 45–1. Source of hazardous substance and oil releases reported to the Emergency Release Notification System, 2012 (32,551 incidents reported). (Reproduced with permission from RTKNet.org, a project of the Center for Effective Government, Washington, DC. http://www.rtknet.org/db/erns.)
For the 10 years, from 2002 to 2012, more than 370,000 incidents involving hazardous substances, including intentional chemical releases, were reported to the National Response Center. In 2012 alone, more than 32,000 incidents were reported.
B. Public Health Consequences of Releases
The Agency for Toxic Substances and Disease Registry (ATSDR) maintains the National Toxic Substance Incidents Program (NTSIP), which collaborates with the Department of Transportation to track transportation and fixed-facility chemical incidents. From 2002 to 2012, NTSIP recorded more than 117,000 stationary facility and 68,000 transportation chemical incidents. NTSIP works with several state partners to track and respond to chemical releases and offers tools and resources to respond to releases of toxic substances.
From 1990 to 2009, ATSDR maintained the Hazardous Substances Emergency Event Surveillance (HSEES) system to track public health outcomes of accidental releases in the United States. Ammonia is the most commonly produced and released substance in the United States (Table 45–8). The most frequent cause of injury due to accidental releases is chlorine, which accounts for a small proportion of accidents and is responsible for a disproportionately large number of injuries, indicating its high acute toxicity. Respiratory irritation is most common type of health effect reported following chemical releases (Table 45–9). Trauma is more common in transportation-related incidents and is generally caused by mechanical events, not the hazardous substance released. Most victims of hazardous materials incidents are transported to a hospital and treated on an outpatient basis or treated at the scene of an incident. One in 10 individuals with illness or injury related to chemical releases is admitted to a hospital. Hazardous materials releases may result in fatalities among both employees and members of the public. Death is often the result of burns or transportation-related trauma. Table 45–10 depicts the numbers of victims and deaths resulting from chemical incidents.
Table 45–8. Ten most frequently released hazardous substances.a
Ammonia
Paint, NOSb
Carbon monoxide
Hydrochloric acid
Sulfur dioxide
Sodium hydroxide
Sulfuric acid
Mercury
Volatile organic compounds, NOSb
Benzene
aBased on incidents reported to the Hazardous Substances Emergency Events Surveillance system 2007–2008. http://www.atsdr.cdc.gov/HS/hsees/annual2008.html.
bNOS = Not otherwise specified.
Table 45–9. Types of health effects reported following accidental releases of hazardous substances.a
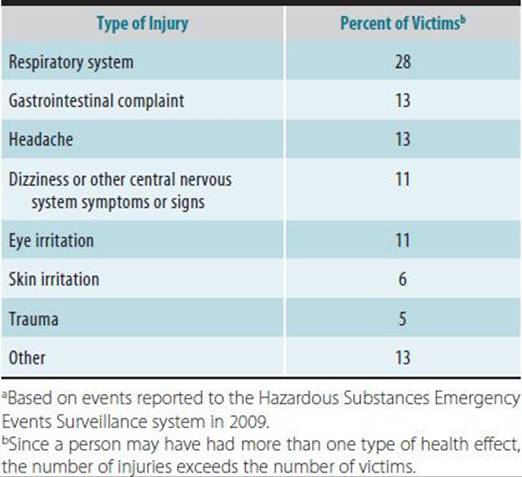
Table 45–10. Numbers of victims and fatalities reported by the National Toxic Substance Incidents Program, 2005–2013.a

Following accidental releases of hazardous materials, workers, including emergency response personnel (such as firefighters and police) are injured most frequently, followed by the general public. In most cases, emergency responders are injured less frequently than other workers, partly because they wear more protective equipment than other workers at the scene of a release. Most nonemergency response employees (eg, cleanup and construction workers) and many emergency responders who are injured do not wear any personal protective equipment. Emergency responders are more often injured in transportation-related events than in fixed facility releases, while nonemergency response workers are more often injured in fixed facility incidents.
![]() Response to Accidental Releases
Response to Accidental Releases
Professionals essential in the response to accidental releases include health care providers, hospital staff, and emergency responders.
A. Health Care Provider Role
In addition to providing medical information during a release and treating exposed victims, health care providers can act as reliable spokespersons on the potential health threat of toxic chemicals being used or stored at facilities in the community. Providing reliable toxicity information to first responders and the community in a timely manner should be one of the main goals of health professionals responding to a release.
When evaluating individuals for potential exposure to accidentally released chemicals, health care personnel must first identify the compound, consider decontaminating the individual, and decide on appropriate treatment measures. Online resources, material safety data sheets, and regional poison control centers should be consulted for substance identification and medical treatment options. If these sources do not have appropriate toxicity information, it may be necessary to contact the manufacturer directly. Manufacturers are allowed to withhold trade secrets about hazardous chemicals from the public, but they are required to provide this information to physicians or nurses who require it for the purpose of treating victims of exposure. Specific proprietary information can be legally obtained in order to render appropriate medical care, but the person receiving this information must agree to maintain this information confidential.
B. Hospital Role
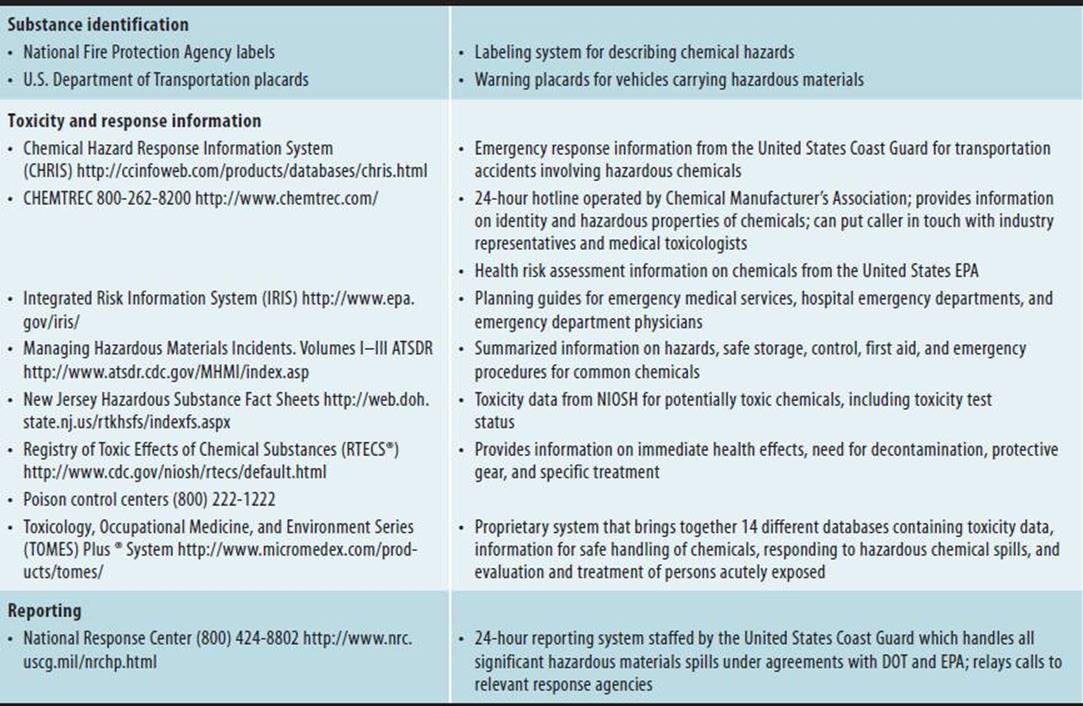
Following major chemical incidents, local hospitals may be overwhelmed by the volume of patients seeking acute care. To optimize response to these emergencies, hospitals should plan for response to accidental releases and establish policies specifying the scope and conduct of patient care to be provided at the facility. This includes determining methods to triage patients into mild, moderate, and severe injury categories; establishing treatment protocols; specifying decontamination methods to be used in treatment areas; and coordinating with other area hospitals, and local and state agencies. Current toxicologic reference materials, including online databases and telephone numbers of the regional poison control center should be readily available (Table 45–11). Information on referral and consultation services should be regularly updated.
Table 45–11. Resources for planning and response to accidental releases of hazardous materials.
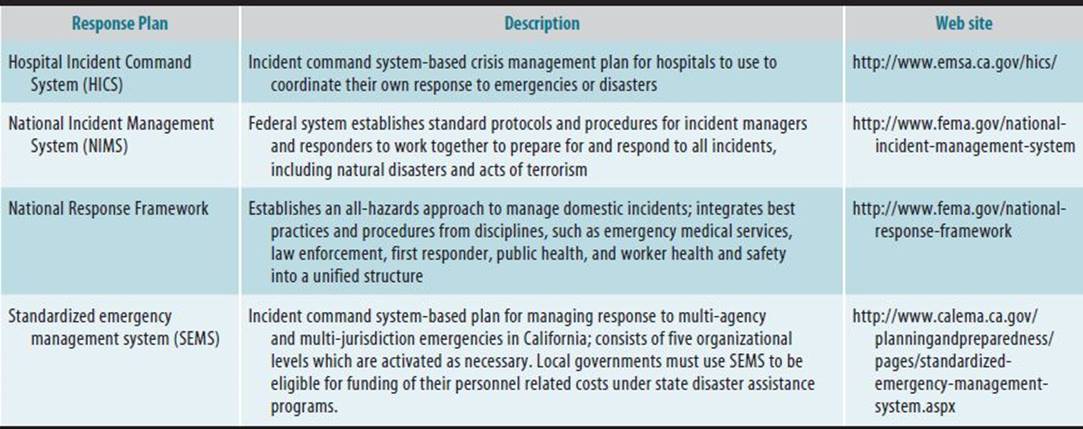
Hospitals and other health care providers are part of a statewide emergency medical care system that coordinates patient distribution to hospitals and monitors medical resources during incidents (Table 45–12). The emergency medical care system also assists in planning and training, as well as certifying certain response personnel, such as paramedics. Hospitals and emergency responders should coordinate drills and simulations to ensure optimal response during a large-scale emergency.
Table 45–12. Guidance for emergency response.
C. Emergency Responder Role
Firefighters and emergency medical technicians are usually the first on the scene of an accident. By establishing protocols for decontamination, evacuating or sheltering in place, emergency responders assist the injured, control the spread of chemicals, and minimize the impact on the surrounding community. Individual health care providers and hospitals should ensure that emergency responders are included in response plans as well as in drills.
D. Treatment
Following most cases of accidental exposure, symptomatic treatment will suffice. This entails choosing supportive or palliative treatment based on signs and symptoms and the route of exposure. Attempts should be made to distinguish symptoms caused by anxiety (worried well) from those caused by direct chemical effects. For some chemicals, clinical effects may not be immediately obvious, and delayed toxicity may need to be considered. For example, following phosgene inhalation exposures, patients should be monitored for 24 hours for onset of pulmonary edema (see Chapters 22 and 23 for more detailed information on acute upper airway and pulmonary injury). Only rarely are chemical-specific medications or antidotes available. For example, following inhalation or dermal exposure to hydrofluoric acid, treatment options may include nebulized or subcutaneous calcium gluconate in addition to corticosteroids; the oxime class of chemicals are antidotes for organophosphate poisoning.
E. Decontamination
To minimize contamination of response personnel and most efficiently treat exposed individuals, the incident commander at a hazardous materials incident typically establishes a command post and creates hazard zones (Figure 45–2). The hot zone, also known as the “exclusion” zone, is closest to the spill and only responders wearing personal protective equipment should be allowed to enter. Entry and exit is controlled through an entry point and a separate point of exit. Only rudimentary first aid is provided in this area. The warm zone provides a systematic way to lessen the exposure to the chemical hazard for those who have been in the hot zone and also serves to control the spread of contamination into the cold zone.
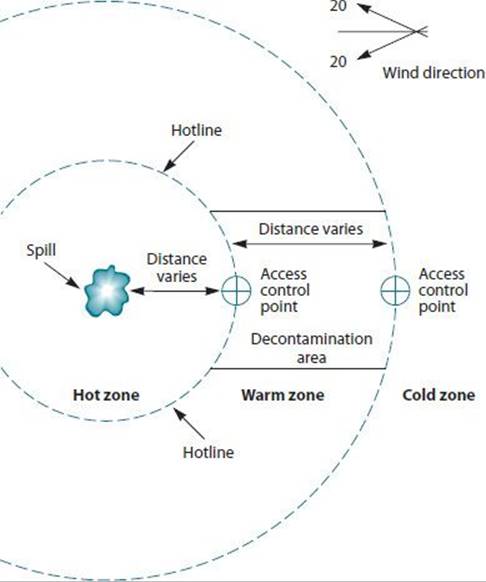
![]() Figure 45–2. Schematic of hot, warm, and cold zones at a hazardous materials spill site.
Figure 45–2. Schematic of hot, warm, and cold zones at a hazardous materials spill site.
Decontamination takes place in the warm zone and may extend into the cold zone. The cold zone is also termed the support zone; this area is theoretically safe from the chemical hazard and is usually set up a considerable distance upwind of the spill. Command and control activities, first aid, and planning take place in the cold zone. Plume modeling may be used to map expected chemical concentrations to determine the different zones.
Many local jurisdictions have developed hazardous materials (HAZMAT) teams, trained to identify and respond to hazardous materials incidents. Decontamination in the field is most likely to be performed by these teams. Guidelines exist for the decontamination of potentially exposed emergency responders. The Occupational Safety and Health Administration (OSHA) has issued requirements for emergency medical technicians and any other health care providers who may be required to respond to a hazardous materials spill. OSHA also requires that employers provide the necessary protective equipment and training to any employee who may encounter a situation involving hazardous materials. Guidelines for decontamination of the public also exist, but no uniform procedure is recommended by all agencies. Because the level of exposure is often unknown, it is considered good management to decontaminate at or near the site of the release.
Following exposure to a hazardous substance in liquid form, decontamination generally involves removing clothes and copiously rinsing the skin and eyes with water to remove chemical contaminants. Spills involving oily materials such as petroleum products may require the use of soap. Runoff water should be contained, if possible, to prevent the contamination of water sources. Decontamination with water may be harmful in some cases. For example, in the presence of water, metal phosphides such as aluminum, zinc, and magnesium phosphides hydrolyze to produce the toxic gas phosphine. If dermal exposure to a metal powder is suspected, the skin should be brushed off and clothes should be aerated in a ventilated area. Clothes should then be laundered and the contaminated bare skin should be thoroughly washed with soap and water.
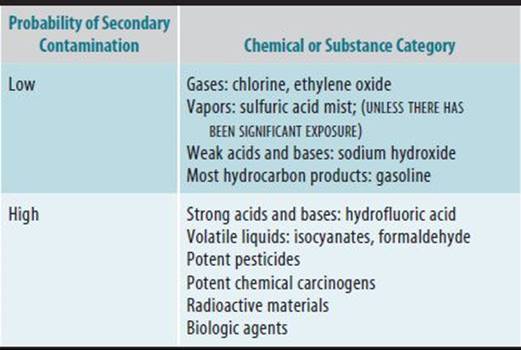
An additional issue of occasional concern is that of secondary contamination of health care facilities and workers with toxic materials on the skin or clothes of accident victims or from toxic vomitus, in the case of ingestion. An example of a substance that is of low risk for toxicity from secondary contamination is a gas, such as chlorine. Substances of high risk for toxicity for secondary contamination require protection of both treatment facilities and medical personnel and include concentrated acids and bases and potent chemical carcinogens (Table 45–13).
Table 45–13. Probability for secondary contamination of health care facilities and providers.
F. Sheltering in Place versus Evacuation
In general, a decision to institute protective actions immediately following a spill is made by the emergency response incident commander, such as a fire chief, police officer, or coast guard officer, in conjunction with local health personnel and elected officials. Few options are available for the protection of community residents after accidental releases. In the case of a release into water, residents may be cautioned to avoid contact with or consumption of the contaminated source. Following releases into air, the two alternatives for protective action are sheltering-in-place or evacuation. The decision to evacuate or shelter-in-place involves weighing many factors. For example, the characteristics of the chemical, the estimated concentration as a function of time, the source, size, and duration of the release, meteorological conditions and the intactness and infiltration rates of the structures used for protection must all be considered. Finally, the proximity of institutions that might require special attention during both evacuation and sheltering-in-place, such as schools, hospitals, and prisons, should be considered.
In-place protection is nearly always better than evacuation. It is of greatest benefit when the chemical’s peak concentration, rather than its cumulative dose, presents the greater toxicity. Sheltering-in-place should be the initial response while any situation is being assessed. Buildings with ventilation systems turned off and with intact doors and windows closed may reduce exposure to half compared to unprotected outdoor exposures. Evacuation may be the preferred choice when there is the threat of a release, though none has yet occurred, or when the release may create an explosion or fire hazard. Evacuation is usually a time-consuming and confusing process and is the safest alternative only when it can be completed prior to the time when a toxic cloud reaches a populated area.
Both in-place protection and evacuation are most effective in protecting individuals from toxic exposure when the local population has received prior education about the proper procedures to follow in the event of an accidental release. Public education about toxic incidents should be coordinated with instruction on response planning for other natural and intentional disasters. Educational sessions should be held with the full participation of all agencies that might respond to an actual event. Chemical emergency planning is most effective when industry, government, the medical community, local community organizations, and public interest groups have established working relationships and coordinate their efforts to mitigate the effects of an accident.
![]() Public Response After Accidental Releases
Public Response After Accidental Releases
A. The Four Steps of Risk Assessment
During an actual release of a hazardous material, the health care provider must be prepared to assess the attendant risks and assist with the response. The National Academy of Sciences has defined the health risk assessment for toxicants as four steps: (1) hazard identification, (2) exposure assessment, (3) toxicologic and dose-response evaluation, and (4) risk characterization. Health risk assessment is discussed in greater detail in Chapter 50. In theory, risk assessment is separated from risk management decisions made during an accidental release. In practice, however, because time constraints are imposed by the emergent nature of accidental releases, there is no clear separation of these four steps and risk assessors may play a part in influencing management decisions based on the incomplete data available. Public health officials may act as either risk assessors or as risk managers, and multidisciplinary and interagency involvement is customary, even during small-scale chemical accidents. A large-scale accident may involve physicians, toxicologists, epidemiologists, emergency responders, and other staff from local, state, and federal agencies. The following sections examine the four steps of risk assessment as they apply to an accidental release.
1. Hazard identification—Hazard identification involves describing the released chemicals and determining their relative hazards in order to ascertain the immediate, delayed, and longer-term health risks posed by the release. The parent compound, as well as the breakdown products and other major ingredients in the formulation, must be identified, which can be done by using online government and chemical manufacturer databases. Identification of the spilled compound may not always be easy as rail tank car placards may be missing or inadequate toxicity testing may lead to failure to accurately categorize a chemical as hazardous. For new chemicals, health effects data may not be readily accessible. Information on breakdown products, chemical interactions, and nontoxicologic hazards, such as flammability, should be sought. In addition to causing thermal injury, explosions or fires may result in the release of a variety of toxic products of incomplete combustion, such as benzene, phosgene, or sulfur dioxide.
When more than one substance has spilled, information regarding potential chemical interactions should be assessed to the extent possible.
2. Exposure assessment—Exposure assessment entails the characterization of the source and location of the release, the potential pathways of human exposure, the population at risk, and the level of exposure. Exposures must be evaluated immediately following the release and levels predicted until the source is contained. In most cases, public health officials will need to rely on emergency responders for information on the exact location of the release, the time of the accident, whether the release has been contained, and the total amount spilled. The route of exposure to a hazardous substance often determines the types of health effects observed following its accidental release. Although routes of exposure are often obvious, as when inhalation exposure follows a massive release into the air, this may not always be the case. For any particular spill, multiple routes of exposure may need to be considered.
Geographic information systems that take into account terrain, weather, and residential locations may be used to map spills and to predict the path of the chemical plume to better characterize potential exposures and identify the population at risk. Often, however, in the confusion that follows an accidental release, geographic information systems do not provide accurate, timely information to guide risk management decisions. Environmental monitoring of the released chemical and its breakdown products or other de novo toxicants is important to accurately determine the level of exposure; monitoring is essential in the case of a dynamic exposure source. The population at risk of exposure includes employees of the facility or transport mode responsible for the release; people at nearby facilities, residences, and businesses; and people in transit in their vehicles in the area of the release or in the path of the chemical plume. Although emergency responders are more likely to wear personal protective equipment than other workers or the general public, they are usually at greatest risk of exposure and adverse health effects.
3. Dose-response evaluation—Toxicologic and dose-response evaluation involves characterizing the relationship between the exposure dose and the adverse health effects. Both animal and human data should be consulted, as human testing is often inadequate. The results of acute, subchronic, chronic, carcinogenicity, and reproductive toxicity testing should be obtained. When quantitative human data are unavailable, animal data are related to an equivalent human dose on a body weight or surface area basis.
4. Risk characterization and risk management—Risk characterization involves identification of health effects that may be expected from the release and of individuals or institutions at greatest risk of adverse health effects. Risk management involves instituting emergency-response action levels to protect individuals from further exposure or to prevent injury.
A. HEALTH EFFECTS—Health effects following accidental releases may be categorized into immediate, delayed, and carcinogenic. Table 45–9 lists the immediate health effects most commonly reported as a result of spills. While most health care providers evaluate and treat exposed persons for immediate effects, persistent or delayed conditions following exposure to accidentally released compounds may occur. For example, various reports exist in which reactive airway dysfunction syndrome has been described in police officers following a single exposure during transportation accidents. For the majority of hazardous substances releases, however, inadequate information is available on the long-term effects of acute exposures.
After a short-term exposure (up to 2 weeks), a quantitative evaluation can be made of certain potential long-term effects such as cancer, based on the inherent toxicity of the compound, the exposure level, and the dose-response assessment. For most compounds, a short-term exposure would result in a negligible risk of cancer. If an accidental release results in chronic environmental or occupational exposures to relatively low levels of a contaminant, however, it is prudent to estimate risks of cancer or other long-term effects to guide surveillance, cleanup, and other response measures.
In addition to physical consequences of accidental chemical exposure, the psychological impact of accidental releases is an important factor to consider. Depression, anger, and anxiety are common in communities immediately following, and as prolonged consequences of, accidental releases. Health care providers and public health officials should recognize that exposed persons may need evaluation for and treatment of psychological problems. Additionally, anxiety about the possible effects of released chemicals may increase health care utilization by the “worried well,” as well as by individuals considering litigation.
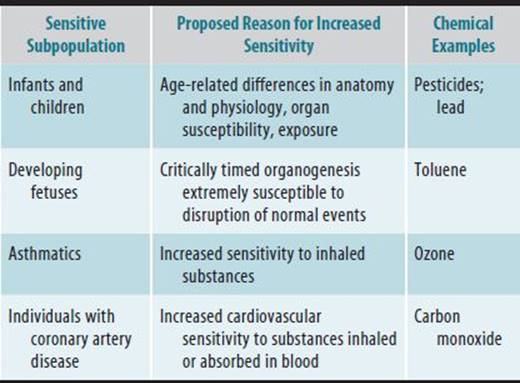
Persons who may be predisposed to adverse effects following exposure to accidentally released chemicals are termed “sensitive individuals,” some of whom are identified in Table 45–14. Institutions housing such individuals, such as schools, hospitals, or elderly care facilities that are in the vicinity of an accidental release may warrant special mitigation measures. Public health officials may need to notify the public that certain sensitive subpopulations may be at an increased risk of specified health consequences.
Table 45–14. Examples of “sensitive individuals” with conditions predisposing toward adverse health effects following exposure to chemicals.
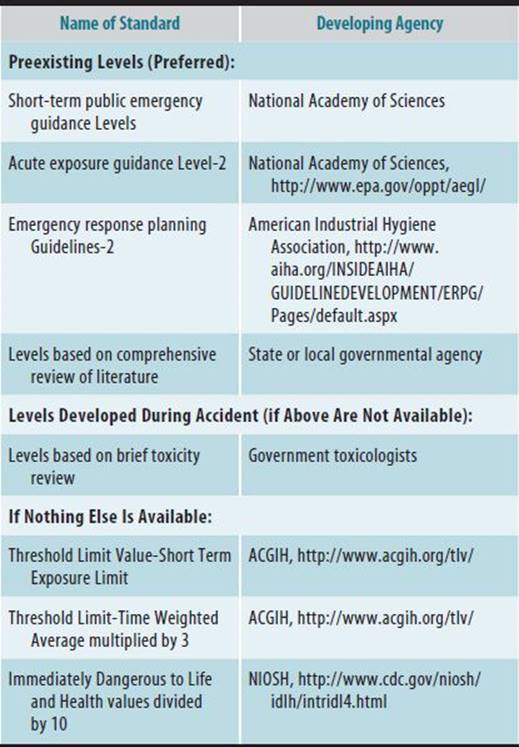
B. EMERGENCY RESPONSE STANDARDS—Emergency response action levels are used to guide shelter-in-place or evacuation decisions; if evacuation has occurred, these levels may be used to determine when it is safe for community members to reenter the area. It is important to note that these levels are not used to predict health effects in a potentially exposed population. In general, a level defines the concentration and duration to which most individuals may be exposed without suffering from a designated health effect (eg, mild, severe, or life-threatening). To derive an emergency response level, the highest exposure dose that does not result in the health effect of interest (the no adverse or lowest adverse effect level) should be divided by uncertainty factors ranging from 1 to 10 to account for inadequacies in the database, incomplete scientific knowledge, and protection of sensitive subpopulations. The use of uncertainty factors offers a margin of safety for officials to consider when recommending responses to accidental releases. In the event of an accidental release, a variety of exposure reference levels may be used. These standards vary considerably in their use of accurate scientific methods and intent to protect public health (Table 45–15).
B. Coordination of Multiagency Response
Several governmental agencies and professional specialties will likely be involved in the response to any major incident. Responses may be confusing, frustrating, and duplicative. To streamline response to major incidents, agencies should coordinate efforts to establish joint plans. Several levels of response may be activated as needed to deliver effective aid to multiagency and multijurisdiction emergencies. These levels are (1) field, (2) local government, (3) county, (4) region, (5) state, and (6) federal. Joint emergency management teams may operate under all kinds of emergencies, including intentional releases of hazardous substances and natural disasters. The National Response Framework builds on the existing National Incident Management System (NIMS) and the Incident Command System (ICS) and presents guiding principles that enable all response partners to prepare for and provide a unified national response to disasters and emergencies, regardless of the size (see Table 45–12).
Table 45–15. Hierarchy of emergency response (1-hour) action standards for guiding actions during and after accidental releases.
![]() Regulations
Regulations
Health care providers involved in the planning for or response to accidental releases should be aware of the complex regulations governing this area of environmental health and the sources of data for hazardous substance releases.
A. Definition of Hazardous Materials
Hazardous materials are defined as materials or substances in forms or quantities that, if released, might pose an unreasonable risk to health and safety or property. Chemicals listed under the Comprehensive Environmental Response, Compensation, and Liability Act of 1980 (CERCLA), also known as Superfund, are considered to be hazardous substances. Approximately 2400 materials are listed and are classified broadly into categories such as explosives, flammables, corrosives, combustibles, poisons, oxidizers, biological agents, and radioactive materials. The transport of hazardous materials is regulated by the Department of Transportation (DOT) under the Hazardous Materials Transportation Act of 1975.
1. Stationary Source Accidents: Federal Regulations—In general, stationary source accidental release planning and response falls under the jurisdiction of EPA and transportation accidents under DOT. Mandatory emergency planning and reporting requirements for the manufacture, storage, and transportation of hazardous materials are determined by four major federal regulations: CERCLA and EPCRA, the Hazardous Material Transportation Act of 1975 (HMTA) as amended, the Clean Air Act Amendments of 1990 (CAAA), and the Clean Water Act (CWA).
CERCLA (42 Code of Federal Regulations Chapter 103) requires that for each hazardous substance, the EPA establish a reportable quantity (RQ) based on the substance’s physical, chemical, and toxicological properties, including aquatic and mammalian toxicity, ignitability, and reactivity, among other factors. Hazardous substance releases equal to or in excess of the RQ must be reported immediately to the National Response Center (NRC) as well as to state and local emergency response officials. This notification is required for transportation incidents and releases from vessels as well as stationary source emergencies. Failure to report accidental releases can include civil and criminal penalties, including monetary fines, imprisonment, or both. There is no requirement to report non-CERCLA substances. The latter category includes chemicals for which there is inadequate toxicity information for characterization as hazardous materials. EPCRA (40 Code of Federal Regulations Part 355.40), or SARA Title III, requires that the release of an RQ or more of a hazardous substance that results in exposure of people outside the facility boundary be reported to state and local authorities. EPCRA also requires states to establish statewide and local emergency planning groups to develop chemical emergency response plans for each community and requires facilities to provide material safety data sheets (MSDSs) or a list of hazardous materials on site to states, local planners, and fire departments, and through them, the public. EPCRA builds the foundation of the community emergency response plan and public/industry dialog on accidental release risk and risk reduction. EPCRA also requires facility operators to notify the state emergency response commission (or its equivalent) of the type and quantity of hazardous materials stored in quantities equal to or in excess of the RQ. These regulations have resulted in increased notification of local, state, and federal governments about hazardous materials stored at facilities and improved knowledge of the patterns of accidental releases from both fixed and mobile sources. However, increased concerns for security as a consequence of actual and threatened terrorist events have resulted in reduced public availability of much of this information. In addition, requirements to notify local agencies about the transportation of these substances through their jurisdictions varies considerably from state to state.
HMTA (49 Code of Federal Regulations Part 171.15) requires that the release of a hazardous material during transportation be reported to the NRC under certain circumstances such as death, injury, significant property damage, evacuation, or highway closure.
Section 112r of the CAAA contains regulations aimed at preventing accidental releases of regulated materials and other extremely hazardous substances to the air and minimizing the consequences of releases by focusing preventive measures on those chemicals that pose the greatest risk. It requires facilities to identify hazards resulting from releases, to design and maintain safe facilities, and to minimize the consequences of releases when they occur. In addition, the CAAA is unique among environmental regulations in that it requires the protection of not only the environment and the health of the public, but the health and safety of workers, as well. To protect workers, OSHA has promulgated a chemical process safety standard to protect workers from chemical accidents at facilities using highly toxic, reactive, flammable, or explosive substances (29 Code of Federal Regulations 1910.119). To protect the public, EPA established a rule governing Risk Management Programs for Accidental Release Prevention (40 Code of Federal Regulations Part 68). This rule requires facilities to prepare hazard assessments evaluating potential effects of an accidental release of any regulated substance. Based on these hazard assessments, facilities must develop programs aimed at prevention of and emergency response to accidental releases.
CWA (40 Code of Federal Regulations Part 110.10, Part 300.300) requires that the oil releases reported to the NRC if the release (1) violates applicable water quality standards; (2) causes a film, sheen, or discoloration of the water or adjoining shoreline; or (3) causes a sludge or an emulsion to be deposited beneath the surface of the water or upon the adjoining shorelines.
![]() International Perspective
International Perspective
Although both major and minor chemical accidents occur internationally, an accurate tally of these incidents is not available because reporting requirements and record-keeping vary widely between countries. Moreover, lack of public disclosure and the absence of functioning right-to-know laws severely limit the information that is available for many countries.
![]() Europe
Europe
The European Union (EU) has one of the most coordinated approaches to tracking chemical incidents outside the United States. The 1982 Seveso Directive provided guidelines on risk management and emergency planning for the prevention of chemical accidents for the EU. The legislation’s purpose is twofold: (1) to incorporate control and safety measures into the design of a plant or process and to prepare emergency plans; and (2) to inform the general public about hazardous substances on site and recommendations for actions to be taken in the event of an incident. In addition, it provides for notification of authorities if dangerous materials are stored, transported, used in operations, or released in an accident. The legislation has been modified over the years and now requires active provision of information to the public on a “right-to-know” basis as well as safety reports, accident prevention, and emergency response plans.
The Major Accident Reporting System database is maintained by the Major-Accident Hazards Bureau in Italy and contains reports of accidental releases from all EU states. Member nations are required to report major accidents, but enforcement is variable and the information is incomplete. Non-EU member nations, including those of the Organization for Economic Cooperation and Development (OECD) may report on a voluntary basis.
![]() Coordinated Programs
Coordinated Programs
The United Nations Environment Program (UNEP) and its partners have developed Awareness and Preparedness for Emergencies at Local Level (APELL) to prevent accidents and minimize their impacts. While initially intended for accidental releases of hazardous substances from stationary facilities, the program has expanded its applications to transportation incidents and natural disasters. To complement the APELL program, the OECD Chemical Accidents Program, in cooperation with the International Labor Organization, UNEP, the World Health Organization, and the World Bank prepared voluntary guidelines, “Guiding Principles for Chemical Accident Prevention,” to provide a foundation to prevent, prepare for, and respond to chemical accidents throughout the world. The document describes the roles of industry, public authorities, employees, the public, and organizations to prevent and mitigate the effects of hazardous materials accidents. It is suggested that safety programs be aimed toward completely preventing harm to human health, environment, and property (“zero-risk”), while recognizing that accidents will still occur. The “Guiding Principles” state that industries from OECD countries should operate with these same guidelines in their plants located in non-OECD (developing) nations.
NUCLEAR ACCIDENTS
Nuclear accidents may occur anywhere radioactive materials are in use but may be more likely in countries with covert nuclear programs, where safety and early warning systems may be inadequately tested or nonexistent. In 2011, the flooding of the Fukushima Daiichi nuclear facility in Japan resulted from the Tōhoku earthquake and tsunami. The nuclear meltdown and release of radioactive materials was the largest nuclear disaster since the Chernobyl disaster of 1986. Radiation is still leaking from the facility, with long-term environmental and public health consequences yet to be ascertained. While large-scale accidents are well publicized, numerous small accidental exposures, including military and hospital overexposures, may not be reported publicly for several years after their occurrence. Unlike the multiple reporting systems for accidental chemical releases, reporting systems for radiologic accidents in the United States are not standardized or easily accessible.
![]() Nuclear Regulation in the United States
Nuclear Regulation in the United States
A. Agencies Involved in Accident Response
Accidental exposure to radiologic material may be a result of situations as varied as nuclear reactor or nuclear power plant accidents, transport incidents involving radioactive material, spacecraft reentry, or fallout from atmospheric testing of nuclear devices. In the event of a radiologic accident, various federal agencies coordinate their efforts at the accident scene under the umbrella of the Federal Radiological Emergency Response Plan. The Federal Emergency Management Agency (FEMA) coordinates federal and state activities. The Nuclear Regulatory Commission (NRC) is the lead federal agency in an emergency at a licensed nuclear facility. The Department of Energy (DOE) is the lead agency in an emergency at one of its nuclear facilities or in a transportation accident involving radiologic material in its custody. The EPA is the lead agency in an emergency involving radioactivity originating in a foreign country or in a domestic accident involving unregulated radioactive material. State and local governments are responsible for the health and welfare of the general public during an emergency.
The EPA has developed a system of protective action guides (PAGs) to help officials make critical decisions. These guidelines identify the radiation levels at which state and local officials should take actions to safeguard human health during an accident and direct the development of emergency response plans. The PAGs identify three phases of an emergency: early, intermediate, and late. In the early phase, which usually lasts from several hours to several days, evacuation and sheltering are the principal actions to insulate the public from exposure to direct radiation and inhalation of airborne radioactive material. In the intermediate phase, which can last from weeks to months, actions may include limiting food and water consumption to decrease ingestion of radioactive material and relocating people to minimize radiation exposure. Administration of stable iodine also may be considered in the early to intermediate phases. In the late phase, which can last from months to years, the PAGs address the decontamination of property. In an actual emergency, protective actions in addition to those addressed by the PAGs may be needed.
B. Nuclear Reactor Accidents
There are currently more than 100 licensed reactors in the United States, and formal approval of emergency response plans is a condition for obtaining and maintaining operating licenses of these facilities. The NRC coordinates all off-site radiologic emergency preparedness efforts and evaluates state and local plans. Current regulations require that emergency planning be conducted at the facility with provisions for off-site emergency response, including arrangements for medical services for injured or radiologically contaminated individuals and training for those who may be called on to assist in an emergency.
The NRC has a nuclear plant emergency preparedness goal that sets health objectives in terms of probability of occurrence compared with other events. For example, the goal for severe accident prevention is a frequency of occurrence of less than 1 in 1 million per reactor per year; the risk to an average individual in the vicinity of a nuclear power plant of prompt fatalities that might result from reactor accidents should not exceed 0.1% of the sum of prompt fatality risks resulting from other accidents; and the risk to the population in the area near a nuclear power plant of cancer fatalities that might result from nuclear power plant operation should not exceed 0.1% of the sum of cancer fatality risks resulting from all other causes.
![]() International Coordination
International Coordination
There are some efforts to institute international safety standards for nuclear reactors. OECD member countries account for approximately 85% of the world’s installed nuclear capacity, and nuclear energy represents nearly a quarter of the electricity supply for these countries. Accident management activities exist in OECD countries, although there is significant variation among member countries as to what should be classified as severe accident management. The Nuclear Energy Agency, a panel of the OECD, has outlined existing programs in member countries and has encouraged further efforts at consistent emergency preparedness. However, among other issues, the lack of uniformity found in older reactors poses problems in the international safety regulatory arena.
There are separate regulations for emergency response planning for transport accidents involving radioactive material. It is estimated that more than 40 million shipments of packages containing radioactive material are made each year throughout the world, although there have been no reported transport accidents with serious radiologic consequences to date. The International Atomic Energy Agency has issued guidelines that have served for years as the basis for regulating the safe transport of radiologic materials worldwide. These universal recommendations are implemented by local authorities, taking into account the specific legislative structures and actual shipments.
HAZARDOUS WASTE
Concern about hazardous waste typically ranks at the top of the list when the public is polled about environmental concerns. The public is increasingly turning to physicians for advice and answers. A physician should have a working understanding of the health risks created by hazardous waste and be able to take an exposure history. The ability to recognize when an exposure may be occurring is critical because environmental medicine, like occupational medicine, is prevention oriented.
The following material on hazardous waste includes an overview of the nature and magnitude of the problem, the use of exposure assessment and health studies for studying the impact of hazardous waste facilities, and a synopsis of hazardous waste regulation and management. The focus is on chemical waste; however, of particular interest to the health care community, pharmaceutical, radioactive waste, and regulated medical waste (biohazardous) are also addressed. The last part provides a glimpse into hazardous waste issues at the international level.
DEFINING THE PROBLEM
The term hazardous waste is ambiguous. It more accurately should refer to hazardous chemicals because it is unclear when a hazardous chemical becomes a hazardous waste. For the most part, in US regulation there is control over the storage, treatment, and disposal of hazardous waste, not hazardous chemicals. The single exception is the regulation of underground storage tanks. There are as many possible types of hazardous wastes as there are possible combinations of hazardous and toxic chemicals. These are the by-products of industry, home, agriculture, or the environment. Only a tiny fraction of chemicals in use have adequate toxicologic data. Data on interactions between different chemicals are even sparser.
Hazardous waste, as defined by US legislation, is a subset of solid waste and can include solids, sludges, liquids, and containerized gases. These broad definitions have a myriad of exceptions, many being a result of the political influence of those who create the waste. Because the following materials are not considered solid waste, they are not listed as hazardous waste: domestic sewage, certain nuclear waste, in situ mining waste, and pulping liquors used in the production of paper in the kraft paper process. Hazardous waste exclusions include agricultural wastes used as fertilizers; mining overburden; discarded wood treated with arsenic; chromium wastes; petroleum-contaminated media from tank cleanup; specific ore-processing wastes; specific utility wastes; oil and gas exploration, development, and production waste; and cement kiln waste.
Most household chemicals are also excluded from hazardous waste categorization, although there are many toxic chemicals in today’s commercial products. Universal waste is a special category of hazardous waste found in household and different types of businesses waste, that are not allowed to put into municipal solid waste. Universal waste as defined by the federal government includes batteries, mercurycontaining equipment, pesticides, mercury containing lamps, and pesticides. States can add additional items to the list. Universal waste must collected separately, thus making it easier to send them for recycling or proper disposal. There is interest in certain pharmaceutical waste being added to the universal waste list.
It is important to note that hazardous waste also excludes chemicals discharged directly into the air or water (ie, releases allowed by permits under other federal pollution-control statutes such as the Clean Air Act and the CWA). Firms that generate small quantities of hazardous wastes can escape management requirements. Hazardous wastes mixed with fuel oils can be burned and released into the environment without adequate controls.
Americans are the largest producers of hazardous waste per capita; however, it should be noted that despite all the exceptions mentioned earlier, the definition of hazardous waste in the United States encompasses much more than that of any other country. In 2011, 16,447 large-quantity generators produced 34 million tons of hazardous waste, which is about 1 ton per 9 people. Chemical and petroleum/coal products manufacturing companies were responsible for most of the hazardous waste generation. Wastewater treatment and disposal accounted for the next most. The states generating the most hazardous waste were Texas and Louisiana, which accounted for 58% of the national total quantity generated.
It is estimated that as many as 425,000 abandoned hazardous waste sites exist in the United States, although the EPA has inventoried only 46,000. As of March 2013, 1312 sites were on the EPA’s National Priorities List (NPL). The EPA proposes sites for the NPL by applying a hazard-ranking system, which is an assessment of the relative public health, environmental, and ecologic threat posed by a given site. There are more than 156 sites owned by the federal government, primarily the DOE and the Department of Defense, on the NPL. These federal sites pose significant concern because of their large geographic areas and the complex mixture of waste that is contaminating them.
![]() Pharmaceutical Waste
Pharmaceutical Waste
Pharmaceutical waste is generated at hospitals and other health care facilities and dispensed for home use, encompasses both prescription and nonprescription drugs. It has been estimated that hospitals and long-term care facilities waste at least 125 million pounds of pharmaceuticals per year. Pharmaceuticals that are not used are often flushed down the toilet or poured down the drain. Pharmaceuticals disposed of in this manner are released directly to environment after passing through wastewater treatment plants, which are often not designed to remove pharmaceuticals from the effluent. Though not typically measured for in surface water monitoring, special studies have shown both nonprescription and prescription pharmaceuticals in US streams.
![]() Regulated Medical Waste
Regulated Medical Waste
Regulated medical waste is often called “biohazardous” as it refers to infectious, or potentially infectious, waste. Regulated medical waste is generated or produced as a result of any of the following: diagnosis, treatment, or immunization of human beings or animals; research dealing with infectious agents; serums, vaccines, antigens, and antitoxins; waste that is biohazardous; or “sharps”—devices having acute rigid corners, edges, or protuberances capable of cutting or piercing, including hypodermic needles, blades, needles, and broken glass. Regulated medical waste is generated by physician and dentist offices; by clinics, hospitals, skilled nursing facilities, research facilities, research laboratories, clinical laboratories, and other health care facilities; by illicit drug users; and by diabetics and others who depend on injections for health reasons.
Hospitals in the United States generate more than 2 million tons of regulated medical waste each year. Only 20% of the waste is considered infectious, yet in the past, all waste was commingled. Similar practices were followed in other health care settings; however, hospitals, which comprise only 2% of the total number of generators, produce approximately 77% of the total infectious waste. As there has been increasing dependence in the medical community on disposable items, there has been an increase in the amount of regulated medical waste being produced.
![]() Radioactive Waste
Radioactive Waste
The production of nuclear power and weapons creates hazardous waste from remnants left from uranium mining and routine radioactive waste at nuclear power facilities, weapons-production facilities, nuclear bomb testing locations, and cleanup at decommissioned nuclear power plants and military sites. Low-level radioactive waste (approximately 0.5 Ci/yd3) results from radiologic uses at more than 20,000 facilities nationwide, such as hospitals, universities, biomedical research, pharmaceutical development, and other industrial sources. Civilian nuclear waste also arises from the 104 nuclear power plants in the United States. A large nuclear power plant produces 460 tons of low-level waste (approximately 1 Ci/yd3) that includes contaminated trash, sludges and resins from the reactor, and irradiated reactor parts. Spent fuel from a power plant (approximately 27 tons per year) has a high level of radioactivity (689,999 Ci/yd3 of waste). In addition, there are 12 nuclear reactors that are currently in shutdown mode and are being decommissioned. The decommissioning of these facilities produces spent fuel and low-level waste (approximately 76 Ci/yd3).
The other major source of radioactive waste is from the production of nuclear weapons by the DOE for the Department of Defense. Defense waste is divided into low-level waste (1 Ci/yd3), transuranic waste (4 Ci/yd3), and high-level waste (approximately 780 Ci/yd3).
In 1993, about 800,000 yd3 of civilian low-level radioactive waste and 10,000,000 yd3 of military low-level radioactive waste were produced. Approximately 3346000 ft3 of low-level radioactive waste was disposed of in 2000. By 2005, there were approximately 52,000 tons of spent nuclear fuel stored at commercial power reactors. That same year, commercial nuclear reactors produced 28,000 metric tons of high-level waste (spent fuel) that accounted for 96% of the total radioactivity of all nuclear waste generated. The military produced 1,500,000 ft3 of high-level and 1,110,000 yd3 of transuranic waste. In addition to these wastes produced as a result of typical operating practices, the decommissioning of civilian reactors and military bases resulted in an additional amount of nuclear waste, primarily low-level waste.
EXPOSURE ASSESSMENT
Exposure assessment is the process of identifying all individuals or population subgroups that have been exposed to a chemical or chemicals. Based on demographic data available in the 1980s, the EPA estimated that approximately 41 million people live within a 4-mi radius of the 1134 NPL sites. Of course, residence near a hazardous waste site or a facility that handles hazardous waste does not necessarily translate to actual exposure to substances released from the site. For instance, completed exposure pathways were identified at only 45% of the NPL hazardous waste sites. A completed exposure pathway consists of the following five elements: a source of contamination, an environmental medium, a point of exposure, route(s) of exposure, and a receptor population. Table 45–16 lists some of the exposure pathways that should be considered.
Table 45–16. Top 20 hazardous substances at CERCLA sites.
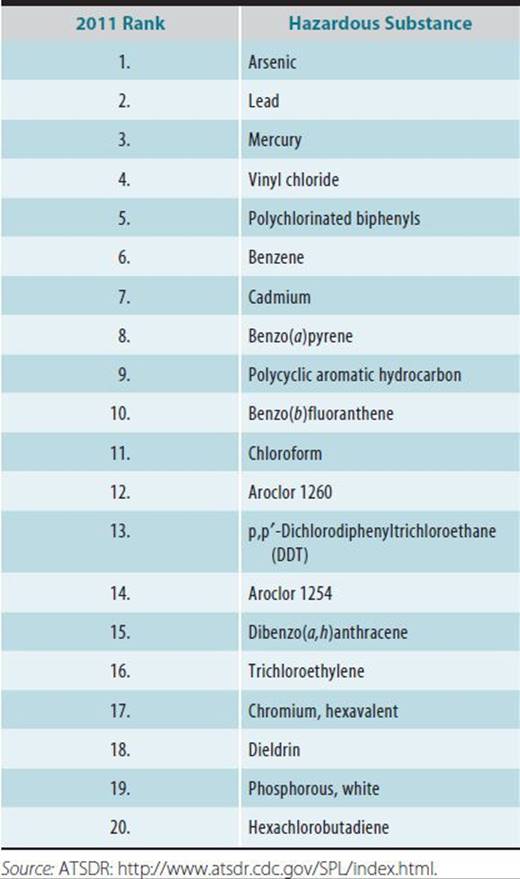
At 91% of the NPL hazardous waste sites with completed exposure pathways, the exposure occurred through contaminated groundwater; at 46% of the sites, exposure occurred from contaminated soil; at 14% of the sites, exposure was via contaminated biota. However, these data need to be understood in the context of how they are collected by regulatory agencies. When hazardous waste sites are evaluated, the soil and groundwater almost always are sampled; however, air monitoring and sampling of biota are not usually conducted. Additionally, most environmental data are collected from the land immediately comprising the site and not from the surrounding neighborhood where potential exposed populations may be living. It is typical that community exposure is evaluated using models to estimate the fate and transport of chemicals from on-site to the neighborhood.
There are more than 600 unique substances found at waste sites in the United States; Table 45–16 lists the top 20 substances. The prioritization of the substances is based on three criteria: frequency of occurrence of a toxic substance at NPL sites, the substance’s toxicity, and the potential for human exposure. Most hazardous waste sites are contaminated with a mixture of chemicals rather than a single chemical, and very little toxicologic information is known about mixtures.
People in communities are very suspicious of the modeled exposure and risk estimates used to assess the health impact. Communities that live around hazardous waste sites are increasingly asking for biologic monitoring investigations to ascertain their exposure.
Biologic monitoring measures exposure by monitoring body fluids (typically blood or urine) for the chemicals of interest. Biologic monitoring provides the best evidence of exposure and avoids many of the exposure assumptions and animal-to-human extrapolations that are used in traditional exposure/risk assessment. However, depending on the pharmacokinetics of the chemical, biologic monitoring may not provide the needed information about chronic exposure to chemicals from a hazardous waste site. For instance, volatile organic compounds such as vinyl chloride have very short half-lives (2–4 hours) in the blood, and thus a discrete blood sample analyzed for vinyl chloride may not reflect chronic, residential exposure. Unlike public health standards for allowable concentrations of a chemical in drinking water or soil, there are no accepted guidelines for the interpretation of biologic monitoring levels. Laboratories that conduct this type of testing define “normal,” but these numbers have not been rigorously reviewed and typically are abstracted from one published study or from a straw poll of laboratory workers. Finally, if the chemical is detected above “normal,” interpretation of the results to the community member or patient as a short- or long-term health impact is a huge unknown at this time.
Interpretation of biologic monitoring for individuals or communities surrounding a hazardous waste facility is greatly facilitated by the availability of large databases on the levels of chemicals in the “population,” essentially “historical controls.” The CDC publishes these data as a part of the National Health and Nutrition Examination Survey (NHANES), an ongoing survey of the general US population. Over 450 chemicals are now measured in the blood or urine in a random sample of about 10,000 individuals examined every 2 years, the most recent data that is available is from 2009 to 2010 sampling. This national reference information was useful in finding that blood concentrations of three perfluorochemicals were 2–4 times higher in individuals living near several perfluorochemical manufacturers than average levels found in the national reference (NHANES). The elevated concentrations were deemed to be associated with drinking contaminated well water or public drinking water.
HEALTH IMPACT OF HAZARDOUS WASTE
In general, little is known about long-term exposure to low levels of contamination in the environment. Various techniques have been used and are being used to study the health impact. However, the world of small-area epidemiology has all the usual problems of an uncontrolled or multivariable study, as well as several more. For instance, misclassification of exposure owing to inadequate exposure assessment can predetermine the findings of a null study. This aspect of hazardous waste has not been funded adequately. For example, approximately $4.2 billion is spent each year on hazardous waste sites in the United States, yet less than 1% has been devoted to the study of health risks at these sites.
Reviewing existing health outcome data often is the first step taken at a site. Data may be drawn from morbidity and mortality databases, birth statistics, medical records, tumor and disease registries, and surveillance databases. Reviewing such information for the small population around one site could not discriminate the risk from an environmental exposure unless the relative risk is high, for instance, similar to the relative risk for smoking causing lung cancer. However, reviewing available data sources over a larger area (called an ecologic study) has found significant effects from hazardous waste sources: increased hospitalization for coronary heart disease in areas near hazardous waste sites and increased risk of low birth weight and maternal residency near a polychlorinated biphenyl (PCB)–contaminated hazardous waste site in New York State.
Many disease- and symptom-prevalence studies have been conducted in response to community concerns about living next to hazardous waste sites. Many of these studies do not show statistically significant increases in adverse health effects. However, these studies often are plagued by inadequate study sample size, insufficient information about the level of exposure, and bias in self-reporting. Several investigations at specific sites have documented a variety of symptoms of ill-health in exposed persons, including low birth weight, cardiac anomalies, headache, fatigue, and respiratory and a constellation of neurobehavioral problems. It is more difficult to find an association with exposure and disease for health outcomes that are delayed in appearance, especially cancer.
Biomarkers of effect may be used to make comparisons of preclinical events rather than frank disease. This is an improvement over long-term, equivocal cancer-cluster or other endpoint studies. Biologic markers of effect are indicators of change or variation in cellular or biochemical components or processes, structures, or functions that are measurable in humans and, depending on the magnitude, are recognized as an established or potential health impairment or disease. A major limitation of the usefulness of bio-markers of effect to ascertain the health impact of hazardous waste sites exposures is that they are often not substance-specific; therefore, the adverse effect might be caused by factors other than the exposure of concern.
An assessment of 7307 individuals living in the Superfund site of Libby, Montana, found radiographic abnormalities greatest in former workers at the asbestos-containing vermiculite mines. Those individuals who lived with a former worker and may have been exposed to asbestos from take-home exposure also had increased association with pleural abnormalities. Playing in asbestos-containing piles of mine waste and longer duration of residency in Libby were associated with pleural abnormalities, even after controlling for occupational and take-home exposure.
Lack of good exposure information is common to most health studies of hazardous waste sites. This flaw reflects historical tendencies to collect data to conform to remediation efforts rather than health impact concerns. Site investigations historically have determined the extent of soil and ground-water contamination on the hazardous waste site only. Community exposure information then may be modeled, or surrogates for exposure may be used. In ecologic studies, exposure may equate to residency within a census tract or ZIP code. In symptom-prevalence studies, distance from the site or self-reported odor detection may be used. Exposure from groundwater contamination probably has been the most quantifiable, although this information is also based on several assumptions. The Massachusetts Department of Public Health constructed a water-distribution model to recreate exposure from trichloroethylene contamination in two of the eight municipal drinking water wells in Woburn and found a nonstatistical association with contaminated water exposure during maternal pregnancy and leukemia diagnosis for 21 children, whereas the child’s exposure to contaminated drinking water from birth to age of diagnosis showed no association with leukemia risk.
Most hazardous waste site studies are restricted by the small size of the exposed community, which does not allow for an adequate study size. For the general population the scientific explanation why or why not health studies are appropriate in certain situations is very difficult to understand. A helpful tool for communities is the Web site: www.communityhealthstudies.org, which is aimed at lay audiences and provides background information and a study size calculator that illustrates the difficulties in designing a study.
Adequate study size may be addressed by using meta-analyses to pool similar studies or the creation of exposure registries. Meta-analysis is a quantitative review and pooling of similar studies. The combination of studies of small populations into meta-analyses might generate sufficient power to reach conclusions, provided that the basic measures involved are comparable and that sound methods are used in all separate studies. The interpretation of meta-analyses is tempered by the awareness that reporting and publication biases can distort the sample of studies available for pooling. Meta-analyses have not yet been used for hazardous waste epidemiology as they have for clinical trials, but they may be useful in the future if there is consistency in environmental studies.
ATSDR was established, in part, to create registries of populations exposed to hazardous wastes and follow these populations over time to observe associated health effects. ATSDR has developed several specialized registries to study the long-term health effects of exposure to specific chemicals at hazardous waste sites, with the intention of combining data from several sites where similar exposures have occurred to achieve populations large enough that the associated health effects can be detected. Four hazardous substances have been selected for the chemical-specific registries: trichloroethylene (TCE), 2,3,7,8-tetrachlorodibenzo-p-dioxin (dioxin), benzene, and trichloroethane. ATSDR also has established two additional registries: individuals living in Libby, Montana (exposure from asbestos-containing vermiculite) and individuals most directly affected by the World Trade Center collapse.
An emerging condition reported from communities living next to hazardous waste sites is sensitivity to chemicals. This condition, frequently called multiple chemical sensitivity (MCS), is characterized by a wide variety of symptoms in response to extremely low levels of chemically unrelated, everyday substances. The most common symptoms appear to be fatigue, mood changes, and memory and concentration difficulties, followed by various muscular, airway, headache-related, and eye-irritation complaints. More than 120 substances, ranging from barbecue smoke and public restroom deodorizers to detergents, newspaper print, and marking pens, have been said to trigger these symptoms. There are no generally recognized physical signs or laboratory tests to describe this condition, thus MCS as a medical diagnosis is very controversial (see Chapter 49).
Psychological health effects are some of the most important effects observed in those living next to a hazardous waste site or a large facility that handles hazardous waste. While there has been some effort to scientifically study the physical health effects from living next to hazardous waste facilities, the psychological effects are unquantified and unsubstantiated except for anecdotal description. Research on the psychological impact of human-created disasters such as the effects of the Exxon Valdez disaster has shown that members of the high-exposure group were 3.6 times more likely to have generalized anxiety disorder and 2.9 times more likely to have posttraumatic stress disorder (PTSD). This acute environmental incident resembles a natural disaster more than the long-term stress impact from living next to a permanent potential or real health problem of an abandoned hazardous waste site.
Communities that experience chronic stress from living near a hazardous waste site suffer even more uncertainty than those involved in an acute disaster because there are so many more unknowns about how health will be affected in the future. There is also the feeling of a complete loss of control over the environment and their homes that once were a haven and subsequently are felt to be unsafe. In addition, unlike with a natural disaster, these communities are seen as hyper-sensitive because the outside world cannot see the devastation that natural or synthetic acute disasters incur. Documentation of the chronic psychosocial effects of living near a hazardous waste site is not yet available. Therefore, these communities are overlooked. Rather than joining as a community to react to an acute disaster, these communities tend to fragment, and individuals who are not directly affected view those who are suffering symptoms as overreacting. Built-in community support systems often break down in these situations.
Federal and most state laws do not provide a mechanism for compensating individuals who have developed illnesses from environmental exposures to hazardous waste sites. Instead, individuals must bring personal injury actions against “responsible parties” shown to have caused disposal of the waste and must prove that a particular waste caused the illness. Despite the fact that these suits are difficult to win, thousands of plaintiffs are pressing such claims in the United States and in many other countries.
![]() Pharmaceutical Waste
Pharmaceutical Waste
Drinking water contaminated with pharmaceuticals is thought to be the primary route of exposure of concern, after improper disposal into the toilet or down the drain. This may be occurring as most water treatment plants are not designed to treat pharmaceutical waste and if the discharge occurs to a surface water body that is used as drinking water, there are no testing requirements or safety limits for pharmaceuticals in drinking water.
Health risks from pharmaceutical-contaminated drinking water include increased risk of developing cancer (chemotherapeutic drugs or hormones), reproductive impairment (hormones), and the selection and development of antibiotic-resistant bacteria. Some would argue that the low concentrations of pharmaceuticals in surface water/drinking water would pose no appreciable risk when evaluated on a pharmaceutical by pharmaceutical basis. However, a mixture of pharmaceuticals may together pose a health risk. If animals are to be sentinels of human health impacts, the effects of estrogenic compounds have been linked in several studies to intersex characteristics being found in fish from various waterbodies.
![]() Regulated Medical Waste
Regulated Medical Waste
The primary health risks associated with infectious health care wastes are a result of occupational exposure for those who handle it, not for the general population. Treated health care wastes disposed of in a landfill pose some of the same potential impacts as solid waste if the landfill is not maintained properly. Contamination of the air can arise from incinerators burning health care waste. The EPA’s 1995 dioxin emissions inventory estimated that health care waste incineration was the nation’s third largest dioxin and furan source. The prevalence of chlorine-containing polyvinyl chloride (PVC) plastic products in health care waste is largely responsible.
The spread of hepatitis B virus (HBV) and the human immunodeficiency virus (HIV) through health care waste has become a public fear. Because of the extremely limited viability of HIV outside a living host, the potential for developing HIV infection from health care waste is remote. HBV has a more lengthy viability in the environment and therefore presents a slightly higher risk of infection from health care waste. Sharp objects pose the greatest concern because of their ability to puncture the skin and provide a portal of entry for disease transmission.
![]() Radioactive Waste
Radioactive Waste
For communities living next to nuclear waste facilities involved in nuclear power, disposal, or weapons production, the primary routes of exposure come as a result of using contaminated water for drinking, showering, or recreation; eating fish harvested as food habituating in the contaminated water; or consuming edible plants that were irrigated with the contaminated water and absorbed some of the radioactive substances. Additionally, there are low releases of radioactivity in the air emissions from most nuclear waste–generating facilities.
The main health effect associated with radiation exposure is cancer. In general, tissues with a high rate of turnover are more susceptible to the effects of ionizing radiation. Thus the thyroid, lung, breast, stomach, colon, and bone marrow have high sensitivity.
Another group of fast-growing cells susceptible to ionizing radiation is germ cells. There is some evidence showing that parental exposure to ionizing radiation may result in increased cancer for offspring. In utero exposure to ionizing radiation also has been associated with spontaneous abortion, growth retardation, and congenital defects.
HAZARDOUS WASTE REGULATION
The recognition of environmental problems in the United States historically has been a reactionary process. Reaction to the hospitalization of several people in 1972 in Minnesota resulting from drinking well water that had been contaminated with arsenic wastes resulted in the first legislation to address hazardous waste: the Resource Conservation and Recovery Act of 1976 (RCRA). RCRA requires that hazardous waste be identified and tracked as it is generated, ensures that it is contained and transported properly, and regulates the storage, disposal, and/or treatment of hazardous waste. This has been termed cradle-to-grave hazardous waste tracking.
In 1999, 1575 treatment, storage, or disposal facilities subject to RCRA permitting standards managed 26.3 million tons of hazardous waste. Land disposal accounted for 69% of the management total. Nationwide, 16 million tons of hazardous wastes were disposed of in underground injection wells, 1.4 million tons were disposed of in landfills, 705,000 tons were managed in surface impoundments, and 30,000 tons were managed by land treatment (land farming). Recovery (recycling) operations, including waste oil, solvent, and metals recovery, accounted for 8% of the national management total, and thermal treatment accounted for 11% of the national management total.
As a result of the discovery of the Love Canal dump-site in 1975, the public became concerned about the past mismanagement of hazardous waste. Public pressure came to bear on the federal government to take regulatory action to protect public health. Health authorities and public health professionals were pressured to identify the actual and potential health problems that were associated with abandoned hazardous waste sites. CERCLA (Superfund) was created in 1980 to address inactive or abandoned waste sites. The Superfund derives its name from a large federal trust fund capitalized with a special tax on chemical and petroleum feedstocks, federal appropriations, penalties collected from firms found responsible for contamination, and interest earned on the fund balance. The provision to collect this tax ended in 1995 and no funds remain in the Superfund. USEPA’s cleanup costs are paid from the general fund until costs can be recovered from the responsible parties.
While RCRA is a regulatory program that addresses current hazardous waste storage, treatment, and disposal, CERCLA deals with abandoned hazardous waste sites. The bulk of the CERCLA program requires private parties to remediate existing waste sites. CERCLA also causes hazardous waste producers to exercise great care in disposing of hazardous wastes to avoid the creation of a future Superfund site.
Many states have developed their own superfund programs, frequently by creating new environmental protection agencies. State hazardous waste site programs were largely modeled after the Superfund program.
![]() Pharmaceutical Waste
Pharmaceutical Waste
The discovery of a variety of pharmaceuticals in surface, ground, and drinking waters around the country is raising concerns about the potentially adverse environmental consequences of these contaminants. Minute concentrations of chemicals known as endocrine disrupters, some of which are pharmaceuticals, are having detrimental effects on aquatic species and possibly on human health and development. The consistent increase in the use of potent pharmaceuticals, driven by both drug development and the aging population, is creating a corresponding increase in the amount of pharmaceutical waste generated. Some pharmaceutical waste is explicitly listed or qualifies based on its characteristics as hazardous waste under RCRA. Specific health care diagnostics and chemotherapeutic agents need to be handled as radioactive waste (see below). While there is growing concern that other pharmaceutical waste also needs to be regulated, at this time there is very little legislation. Some communities have voluntary takeback programs to try to reduce the amount of pharmaceuticals that are being put down the toilet. Alameda County, one of the San Francisco Bay Area counties has passed an ordinance to create a county-wide takeback program, to be financed by the pharmaceutical corporations, however it has yet to be implemented due to legal challenge by the pharmaceutical industry.
![]() Regulated Medical Waste
Regulated Medical Waste
In the late summer of 1987, a 30- to 40-mi stretch of beaches on Long Island and New Jersey was affected by trash washing ashore. The appearance of syringes and other health care wastes on the shore caused great alarm and resulted in the closure of some beaches. The Medical Waste Tracking Act of 1988 was passed by Congress and set up a 2-year demonstration project including a tracking system for health care waste and with voluntary state participation. Thought the regulatory aspects of the Medical Waste Tracking Act expired in 1999, health care waste disposal is regulated under each state’s authority.
![]() Radioactive Waste
Radioactive Waste
Following the Three Mile Island accident in 1979, the public became very concerned about radioactivity. Nuclear waste disposal became a liability for the few states that had been accepting waste from other states. In late 1979, two of the three low-level waste facilities in the United States announced their intention to close their doors to nuclear waste from other states. In response to the impending nuclear waste backlog, the Low-Level Radioactive Waste Act, a federal mandate that defined the states’ responsibility for the low-level wastes produced within their borders, was passed by Congress in 1980. The Low-Level Radioactive Waste Amendment Act of 1985 placed the states in regional compacts for the purpose of sharing the burden of disposal and set milestones for the construction of regional repositories. There are 10 compacts composed of 44 states. Six states and the District of Columbia and Puerto Rico are not affiliated with a compact. In theory, within each compact, there must be at least one site developed for disposal of low-level waste. At this time, there are only four active licensed low-level disposal sites: Barnwell, South Carolina, Hanford, Washington, Clive, Utah, and Andrews County, Texas. Opened in 2012, the Andrews County, Texas site is the first commercially owned disposal site.
The Nuclear Waste Policy Act of 1982 specifies a detailed approach for high-level radioactive waste disposal, with the DOE having operational responsibility and the NRC having regulatory responsibility for the transportation, storage, and geologic disposal of the waste. This legislation requires that the health and environmental impact of a high-level disposal site be acceptable for thousands of years. The waste site must be in a solid form in a licensed deep, stable geologic structure. The Nuclear Waste Policy Amendments Act of 1987 designated a candidate site for a high-level waste repository at Yucca Mountain, Nevada. The DOE found the site viable and recommended to the president that the site be developed. In 2002, the Congress approved moving forward with Yucca Mountain.
In June 2008 the Department of Energy filed for a license application with the Nuclear Regulatory Commission for a permanent geologic repository at Yucca Mountain NV.
In March 2010 the DOE withdrew the application. However, in June 2010 a Nuclear Regulatory Commission panel of Administrative judges ruled that DOE’s motion to withdraw its application to construct a high-level nuclear waste repository at Yucca Mountain is denied. DOE is expected to appeal the decision which will be heard in the DC circuit.
HAZARDOUS WASTE & PUBLIC HEALTH
Toxicologic animal studies that examine the mechanism, pharmacokinetics, and cell and organ impact of hazardous waste typically have been carried out within academic research institutions usually funded by the National Institute for Environmental Health Sciences (NIEHS) or the EPA. On the other hand, human-based studies of hazardous waste are carried out in the public health arena, historically by state health departments. The roles of the various public health levels of government in responding to the concern over the impact of hazardous waste on the health of the citizenry will be described in this section. Hazardous waste epidemiologic research also is now being conducted by environmental and occupational health clinics within academic institutions.
Local health departments are on the front line, along with physicians, in responding to environmental and public health concerns raised by citizens. The environmental and public health response at the local level is multifaceted, with hazardous waste issues being one aspect. Addressing the underground storage issues, tracking health care, and permitting and inspecting RCRA facilities are some of the responsibilities that generally are mandated for local health departments to regulate. Additionally, these same organizations often must be not only regulators but also public health officials. For questions and problems beyond its expertise or funding abilities, the local health department staff then refers issues to the state health department.
Many state health departments have specialized staff to deal with hazardous waste issues such as environmental toxicologists, epidemiologists, health educators, community coordinators, and physicians. State health departments play a supportive role for local health departments in addition to investigating alleged cancer and other disease clusters around hazardous waste sites.
Since 1987, the ATSDR has supported staff within the states to provide public health oversight at hazardous waste sites, primarily the Superfund sites, in those states. This funding has greatly enhanced state ability and effectiveness to address the health issues that confront them at Superfund sites or other releases of hazardous wastes.
At the federal government level, there are several groups that are concerned with the health effects of hazardous waste. These include the NIEHS, the National Center for Environmental Health (NCEH), and ATSDR. Superfund legislation (CERCLA) created ATSDR to address the health issues of hazardous waste to complement the regulatory mandate given to the EPA for overseeing cleanup. This pairing of a nonregulatory, scientific, fact-finding agency with a regulatory agency had been done previously with the pairing of National Institute of Occupational Health and Safety (NIOSH) and OSHA.
ATSDR’s multipronged approach to dealing with hazardous waste sites includes reviewing and assessing the real health impact of each site, conducting or sponsoring epidemiologic and health studies of exposed communities, educating the community and health care providers about hazardous waste exposure and potential health impact, and reviewing the literature and identifying gaps in the toxicologic information about hazardous waste chemicals.
DATA SOURCES
Information sources concerned with hazardous waste usually fall into two categories: those that deal with facilities or sites and those that deal with chemicals considered hazardous (see Table 45–17). To evaluate whether a site may be causing health effects in an individual living near a facility, it is necessary first to establish what chemicals may be stored, treated, or released from the site and whether there is the possibility that these chemicals have migrated off-site. Site exposure information may be obtained from databases generated from government reporting systems that are available to the public. These databases include the TRI, the Biennial Reporting System, the Comprehensive Environmental Response, Compensation, and Liability Information System (CERCLIS) list, and the Nuclear Reactor List. Once exposure to chemicals of concern has been established, it may be necessary to research the toxicologic information about those chemicals. While basic toxicologic information may be found using Medline or by reading medical journals, there are several information sources that have compiled toxicologic and other chemical-specific information into a readily accessible and well-organized format. These toxicologic databases include the Hazardous Substance Release Effects Database and the Hazardous Substances Database (Table 45–17).
Table 45–17. Hazardous waste databases.
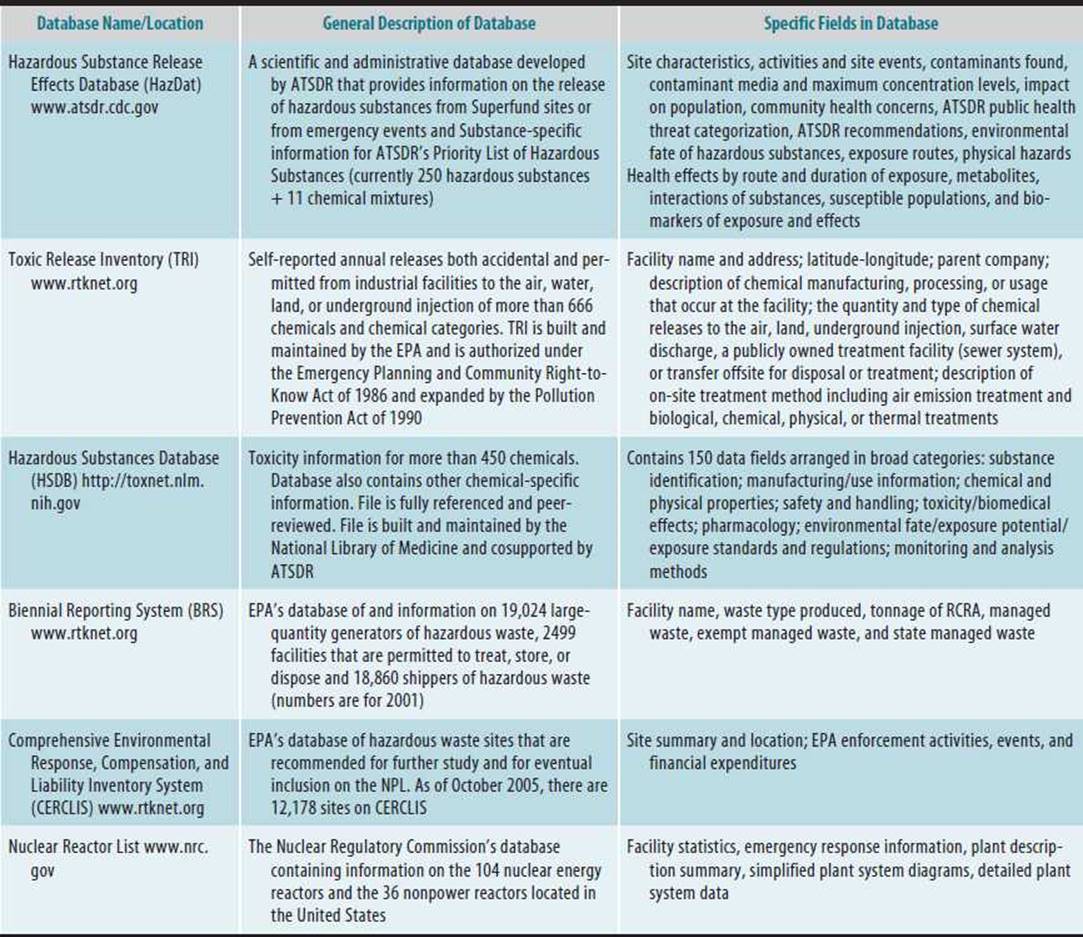
HAZARDOUS WASTE MANAGEMENT PRACTICES
Hazardous waste management is an attempt to achieve a balance between minimizing the environmental and health impact and costs of an industrial society and the economic and social costs involved in achieving these objectives. Management of hazardous waste involves recycling, treating the waste to reduce its volume or hazardous level, and disposal. All these activities are regulated, but there still may be some potential health risk posed. In addition, there is still the continued disposal mismanagement or accidental release by a few hazardous waste users.
Hazardous waste laws are based on the legal concept that generators of hazardous waste are liable for the long-term impact of their waste management practices, including their past practices. As a result, there has been an impetus for change in the waste management arena. One estimate puts the cost of cleaning up a hazardous waste site at 10–100 times greater than the cost of originally treating the wastes in the most efficient fashion. Now, most generators endeavor to minimize waste, and many manufacturers even factor waste management into the life cycle of their products (from research through manufacturing to use by the consumer and eventually ultimate disposition).
Reduction, reusing, and recycling of industrial waste are being actively pursued by many companies. This holistic approach to hazardous waste management is termed industrial ecology. Industrial ecology moves our industrial and economic systems toward a relationship with the interrelatedness of Earth’s natural systems. Industrial ecology is an organizing umbrella that encompasses a number of different approaches, including terms such as pollution prevention, waste minimization, and green chemistry. Green Chemistry focuses on the invention, design, and application of chemical products and processes to reduce or to eliminate the use and generation of hazardous substances. It focuses on the intrinsic hazard properties of the chemical products and transformations. The USEPA promotes the concept of “Green Chemistry” as a way to design processes and products that prevents or minimize the generation of hazardous wastes http://www.epa.gov/greenchemistry/. For instance, when Pfizer was gearing up to produce Viagra, Pfizer’s chemists designed a new reaction strategy that racially reduced the amount of solvent required, cut out the reagents tin chloride, an environmental pollutant, and hydrogen peroxide, which is a fire and transportation hazard, and produced just a quarter of the waste of the original process.
Waste reduction requires changes such as product formulation, process modification, equipment redesign, recovery of waste materials for reuse, and waste separation for exchange or resale. Waste reduction may involve material substitution, process modification, equipment modification, or retraining personnel to get rid of wasteful habits and other housekeeping practices. Recycling consists of recovering and treating waste, and reuse means the recovery, without additional treatment, of hazardous waste that then can be used by the industry generating the waste or by another industry. Recycling of wastewater, solvents, and used oil is commonplace now. As the costs of raw materials, waste treatment, and disposal rise, so has the popularity of industrial ecology. Waste exchanges, regional clearinghouses that facilitate the effective use of waste between various industries, began appearing in the late 1980s.
![]() Treatment of Hazardous Waste
Treatment of Hazardous Waste
Treatment of hazardous waste that cannot be reused or recycled and remediation of contaminated hazardous waste sites involve a variety of methods: physical, chemical, biologic, and thermal treatment. Physical treatment does not reduce the toxicity of the waste but does transfer the waste into another medium or prevents the waste from migrating. Air stripping is one of the most common physical processes used for remediating groundwater contaminated with volatile organic compounds. Air stripping is a mass-transfer process that enhances the volatilization of compounds from water by passing air through water to improve the transfer between the air and water phases. The vapor may be released without treatment or may be passed through activated carbon before release. Similarly, contaminated soils may be cleaned using soil vapor extraction. Soil vapor extraction consists of passing an air stream through soil contaminated with volatile organic compounds, thereby transferring the contaminants from the soil matrix to the air stream.
Chemical treatment is used to alter the chemical structure of the waste constituents, thereby reducing the material’s toxicity. The simplest example of this is the neutralization of an acidic or alkaline waste stream. Chemical oxidation using ozone, hydrogen peroxide, and chlorine is capable of destroying a wide range of organic molecules, including volatile organic compounds, mercaptans, phenols, and inorganics such as cyanide. Other chemical treatment methods include precipitation, ion exchange, and chemical dechlorination.
Stabilization, solidification, and fixation are physiochemical methods used to stabilize waste prior to disposal so that it is easier to handle and also as a remedy at abandoned hazardous waste sites that primarily keeps the material from migrating and decreases the permeability, thereby reducing leaching.
Biologic treatment is the degradation of organic waste by the action of microorganisms with the aim of changing the molecular structure to create less toxic metabolites or completely breaking down the molecule to carbon dioxide, water, and inert inorganic residuals. Biologic treatment of almost any organic material can be accomplished because virtually all organic compounds can be degraded if the proper microbial communities are established, maintained, and controlled. Biologic treatment has been used for many years with municipal and industrial waste streams. In situ bioremediation means that biologic treatment is used to clean up contaminated groundwater and subsurface contaminants where they are found without excavating the overlying soil. Natural attenuation refers to using naturally occurring bacteria for the remediation, whereas enhanced bioremediation refers to the addition of nutrients or specifically chosen or genetically modified bacteria to the soil or water. Natural attenuation is often the choice for cleanup of low-level petroleum-contaminated groundwater.
Thermal methods such as incineration and thermal desorption involve the use of heat to clean up contaminated soil. Incineration uses very high temperatures (870–1370°C [1600–2500°F]) to alter the molecular structure to ideally reduce the toxicity. The soil typically becomes an ash. Incineration changes hydrocarbon molecules into carbon dioxide and water vapor. The combustion of wastes containing sulfur produces sulfur dioxide and sulfur trioxide. Halogen-containing wastes produce the corresponding acid halogen gas (eg, hydrogen chloride or hydrogen bromide). Metals cannot be destroyed and are oxidized. The volatility of oxidized arsenic, antimony, cadmium, and mercury can create problems in the flue gas. Because of the tight regulations on incineration air emissions and concern from communities, on-site incinerators rarely are chosen as a remedy at hazardous waste sites.
Thermal desorption uses temperatures between 93.3°C and 537.8°C (200°F and 1000°F) to drive low-volatile compounds from contaminated soil. The compounds are then trapped, cooled, and recovered for proper disposal. Unlike incineration, the soil remains intact with thermal desorption.
DISPOSAL OF HAZARDOUS WASTE
Disposal means long-term storage in landfills, underground injection wells, or ocean dumping. Surface impoundments such as pits, ponds, and lagoons are storage facilities, not land disposal facilities.
In the past, it was cheap and simple to dig a hole in the ground, fill it with untreated waste, and cover the waste with clay to keep the rain out. However, chemicals in the waste leached from the fill, resulting in the contamination of groundwater and drinking water throughout the United States. Landfills still are the most popular method for disposal, but there are now strict guidelines for their construction. Federal regulation requires hazardous waste landfills to be double-lined, a leachate collection system to collect the inevitable migration of liquid through the liner and a ground-water monitoring system to check for failure of the leachate collection system. Additionally, waste may be disposed of in a landfill if it meets certain criteria related to corrosivity, reactivity, flammability, and toxicity. Thus waste often may be treated prior to its deposit in a landfill. The treatment method also may generate a by-product that must be disposed of as hazardous waste (eg, incineration dust). As a result, even though landfilling of hazardous waste is discouraged, there always will be the need for some hazardous waste landfills.
Injection of waste into deep underground wells is also used for disposal of hazardous waste. Injection usually occurs below the deepest drinking-water aquifer, 1000–10,000 ft (304.8–3048 m) down. Modern deep wells use such safety features as double or triple casings and leak-detection systems. However, even if a leak is detected, remedying the problem may be impossible.
Ocean dumping has been a method of choice for disposal of dredge spoils, industrial waste, sludge from wastewater treatment plants, and radioactive waste but currently is being discouraged because of concern for ecologic damage and contamination of marine food chains.
![]() Pharmaceutical Waste
Pharmaceutical Waste
Pharmaceutical waste that is covered under RCRA must be disposed of as a official hazardous waste. Typically, this waste stream is incinerated and the ash disposed of at a hazardous waste landfill. Many other pharmaceuticals should be treated similarly but since they are not officially considered a hazardous waste they are often disposed in the drain or with solid waste and landfilled. Takeback programs as well as a reduction in the number of and size of prescriptions can help reduce the amount of pharmaceuticals being improperly disposed. Pharmaceuticals received in takeback programs are incinerated.
![]() Health Care Waste
Health Care Waste
Previously, every hospital had an incinerator in which it burned the infectious and noninfectious waste that was generated within the hospital. However, these incinerators had only rudimentary air pollution control devices, and heavy metals, acid gases, and dioxins release may have resulted. With the advent of stricter air pollution laws, many hospital incinerators were shut down. It is estimated that there were 6200 health care incinerators in 1988, and in 2003, there were around 100.
Many health care waste generators are using steam sterilization for certain health care waste. Steam sterilization does not create particulate emissions but does generate significant odors. Furthermore, it cannot be used to treat mixed waste, that is, infectious and radiologic and chemical. Since 1999, there has been a significant increase in the use of alternative technologies to treat health care waste: heat waste with microwaves and radio-waves; expose the waste to chemicals, bleach, or chlorine dioxide; subject the waste to heated chemicals; or expose the waste to irradiation sources.
![]() Radioactive Waste
Radioactive Waste
Radioactive wastes do not respond sufficiently to stabilization by chemical, physical, or biologic processes. Only time can render radioactive wastes inactive. At present, storage appears to be the only means of successfully solving the disposal problem.
Spent fuel from nuclear reactors can be reprocessed. This involves extracting the uranium and the plutonium, but this method results in concentrated fission process product wastes that also require disposal. In addition, because of the concern that plutonium, a by-product of reprocessing, could be diverted to produce nuclear weapons, reprocessing of nuclear fuel elements has been discontinued in the United States.
Radioactive wastes require confinement for shorter or longer periods of time depending on the characteristics of the radionuclides contained within them. The radioactivity of low-level waste will decline to safe levels in approximately 200–300 years, whereas intermediate-level waste will need safe containment for thousands of years. High-level waste, with half-lives of millions of years, requires special treatment.
Low-level waste disposal typically involves near-surface disposal facilities. Near-surface disposal facilities are required to be topped with an impermeable cover that will not allow air emissions and will keep rainwater from filtering through the waste. Still, the most likely mechanism for the release of radionuclides to the environment is transport in groundwater.
There are not yet any high-level or spent-fuel storage facility for the United States or worldwide. The quantities produced so far are being stored temporarily where they have been generated. A number of options have been proposed for storage of high-level waste; currently, the United States is reviewing its options for handling high-level radioactive waste as the proposed repository at Yucca Mountain is being shut down.
INTERNATIONAL PERSPECTIVES
All countries are dealing with hazardous waste issues. The kind and size of each country’s response to these concerns varies according to the social, political, and economic policies of the nation’s government and people. Examining each country’s approach to hazardous waste is beyond the scope of this chapter; however, the responses may be crudely reviewed according to developed, democratized countries, developing central and eastern European countries, and other developing countries.
The status quo of hazardous waste regulation and public health protection for these country groupings is likely to change tremendously in the coming years with globalization of the commercial enterprise and trade liberalization. There is concern that trade liberalization may encourage countries to set low levels of environmental protection, standards, and enforcement to reduce production costs and encourage foreign investment. In essence, lax regulations could be viewed as a production subsidy. Others see health and environmental protection as nontariff barriers.
![]() Developed Nations
Developed Nations
Most industrialized nations have established a national regulatory program that is aimed at protecting human health and the environment from the mismanagement of hazardous waste. The major elements in a national control system for hazardous waste management are:
• Developing an administrative definition for identifying and classifying hazardous waste to the particular level of detail necessary to support its legal procedures
• Defining the responsibilities placed on the waste generator
• Registering or licensing those involved in collection, transport, intermediate storage, treatment, and disposal of hazardous wastes
• Controlling transport, including importing and exporting, using a cradle-to-grave theory involving a manifest system
• Permitting of treatment or disposal facilities
• Developing a national strategy or plan for establishing facilities
• Addressing old or abandoned sites
In most developed countries, the responsibility for managing the national control system is shared among the national, regional, and local governments. While the details differ from country to country, the national government generally is responsible for establishing national standards, guidelines, or codes of practice. Regional and local governments often are responsible for enforcement and licensing activities.
Although most industrialized/developed nations have created hazardous waste management systems that include the elements just mentioned, there are differences in how these elements are implemented. Without examining each country’s system in detail, the essence of the various differences can be represented by listing examples.
Every national system differs in the detailed method for defining hazardous waste and in the breadth of waste included. For instance, specifically controlled waste is the term used for hazardous waste in Japan. Japan classifies fewer items as hazardous waste than any other developed country.
• The European Union has taken bold steps to address the human health and environmental impacts of all chemicals. Under legislation passed by the EU in 2006, the REACH (Registration, Evaluation, Authorization, and Registration of Chemical Substances) requires companies to register chemicals they with a new agency based in Finland. Through REACH, the EU will encourage sustainability.
• Cleaner production is a term introduced by the United Nations Environmental Program (UNEP) in 1989, it is analogous to the pollution prevention concept in the United States.
• It is extremely difficult to compare quantities of industrial or hazardous waste in different countries not only because of the various definitions but also because of inconsistent collection of statistics. For instance, sewage sludge is specifically excluded in some countries’ hazardous waste definition (for example in the United States) but not in others.
• In most developed countries, collection and transport of hazardous waste are carried out by private industry. In Sweden, collection and transportation of hazardous waste are handled through local utility companies run by the municipality.
• In most developed countries, hazardous waste may move freely across internal boundaries within the country. In Germany, a special permit is required before a shipment of hazardous waste is allowed to cross state boundaries.
• The United Kingdom is well known for its advocacy of codisposal of hazardous waste in municipal waste landfill sites.
• The Netherlands has an almost total absence of suitable sites for landfilling; thus landfilling of hazardous waste is prohibited unless specific exemption is granted.
• In Japan, vacant land is scare, so incinerating municipal and hazardous waste is a common means (78% of wastes) of disposal.
• In most developed countries, the primary means of encouraging waste avoidance or recycling is imposition of strict controls on hazardous waste disposal, accompanied by the charging of a stiff fee.
• Most countries have developed a national inventory and cleanup program of old or abandoned hazardous waste sites. One exception is Japan, where there is no general law governing the identification, assessment, and cleanup of contaminated soil, although many cases of such pollution have been identified.
![]() Developing Countries
Developing Countries
It is estimated that developing countries generate 20 million tons per year of hazardous waste. Of this amount, roughly 15 million tons are produced by the central and eastern European countries. Three primary sources of hazardous waste in developing countries are wastes generated by foreign-owned, state-owned, or joint-venture firms; wastes generated by small entrepreneurs, farmers, and householders; and wastes imported from other, usually more developed, countries. On the whole, major corporations have assumed responsibility for their own wastes. However, in cases where the industries are small or locally owned, adequate responsibility for treatment and disposal has not been assumed. Developing countries do not have resources to deal effectively with any of these sources.
Training, technical expertise, facility development, legislation, and the necessary governmental institutions, all in varying degrees, are inadequate in developing countries. Multinational companies may be expected to help, but they have a vested interest that would be expected to interfere with their dealing effectively with the full problem. Much assistance will need to be provided by developed countries.
To begin to fill the organizational void in these countries, information exchanges have been created by developed nations and international organizations. For instance, the UNEP has developed an International Register of Potentially Toxic Chemicals to identify all chemicals that have been banned or severely restricted by five or more countries and is currently preparing guidelines to assist countries in developing environmental protection legislation.
Democratization and the end of one-party rule in most of eastern Europe are considered to have an important impact on hazardous waste issues in these developing countries. Most of the former socialized countries have well-developed occupational health services and rather poorly developed environmental health services and hazardous waste management programs. The ideology of the previous Communist governments may explain this pattern: Worker well-being was valued more than environmental quality, and most of the industry was owned and operated by the national governments. Toxicology, clinical occupational medicine, and some aspects of industrial hygiene have been relatively strong in many eastern European countries, whereas epidemiology, environmental engineering, risk assessment, and risk communication have not.
Unlike in the industrialized, developing countries of eastern Europe, hazardous waste concerns are a relatively new phenomena in the developing countries of Africa, Asia, and Central and South America. However, this is changing primarily as a result of exportation of hazardous waste and the transfer of hazardous industries from developed countries to the developing world. Environmental exposure to hazardous chemicals is increasing in developing countries. In many of the world’s countries, there are no environmental regulations for hazardous waste, or if they do exist, there is little or no enforcement. The daily struggles for survival are the primary focus. Political agreements between developing and industrialized countries are critical to ensure that environmental and human health protection takes place in developing countries. Efforts at the international level have centered on controlling hazardous industries and hazardous wastes.
Thousands of tons of hazardous waste are shipped internationally each year. In 1989, 35 countries and the EC agreed to the Basel Convention, the first step toward regulating international transportation of hazardous waste. Currently, 163 countries have ratified the Basel Convention. The United States has signed but not ratified the Basel Convention. This treaty requires notification of intent of international hazardous waste transport and prior informed consent (PIC) by the receiving country. The original convention allowed hazardous waste transport to continue. A March 1994 addition to the Basel Convention immediately banned exporting hazardous wastes to developing countries for incineration or burial, and exporting of hazardous wastes for “recycling” was banned as of December 31, 1997.
The Lome IV Convention also banned hazardous waste export among more than 80 countries in Africa, the Caribbean, Europe, and the Pacific. Such international cooperation may be elusive. Various reports of countries redefining hazardous waste in order to avoid complying with the Basel Agreement are already surfacing. This is another reason that efforts such as those underway by the OECD to harmonize hazardous waste definitions into an international standard are so critical.
The transfer of hazardous waste technologies to developing countries is a consequence of stringent industrial and environmental regulations and increasing labor costs in the industrialized world. Alternatively, developing countries are attractive because of cheap labor and lack of (or poor implementation of) labor, environmental, and industrial regulations. Efforts to affect ethical behavior in the exporting of hazardous technologies to developing countries also have been attempted by international organizations: the OCED’s Guidelines for Multinational Enterprises, the United Nations’ Code of Conduct on Transnational Corporations, and the International Labor Organization’s Tripartite Declaration of Principles Concerning Multinational Enterprises and Social Policy. Efforts to deal with transboundary hazardous waste and other pollution have been spearheaded by the United Nations, the WHO, the ILO, the European Economic Community, and the OECD.
![]() Health Care Waste
Health Care Waste
Concern about air contamination coming from incineration of health care waste is a concern in other developed nations. In fact, it was research in Germany that showed that the levels of dioxins and furans in the fly ash collected from health care waste incinerators could be two orders of magnitude higher than the levels found in the fly ash of municipal waste incinerators. It was thought that health care waste may contain a greater percentage of plastic (∼30%) than municipal waste (∼7%) or that the municipal waste incinerators were equipped with better air pollution control and operated by better-trained professionals. In 2000, stricter emission limits for health care waste incinerators were introduced in the EU, resulting in the closing of many incinerators. Although alternative treatment technologies are increasing in number, incineration is still the prevailing method.
In developing countries, there are additional concerns, namely, exposure to untreated health care waste by landfill scavengers and waste pickers. The WHO indicates that there are many reports of needlestick injuries to waste workers and scavengers in dumpsites. Recently, children playing in garbage bins near a health center in Russia found discarded small pox vaccine ampules, and became infected with the live-vaccine strain of the virus. Treatment of health care waste prior to disposal is needed to eliminate such risks.
![]() Radioactive Waste
Radioactive Waste
According to the International Atomic Energy Agency, about 10,000 m3 of high-level radioactive waste accumulates each year in 25 countries with 437 nuclear reactors. This massive amount of radioactive material has no permanent home. Not a single country has implemented a long-term plan for its disposal; each relies on interim measures. Most countries are hoping to dispose of the high-level waste deep underground in geologically stable areas; eight countries are currently in the site-characterization phase of developing an underground storage facility. Other considerations for high-level radioactive waste disposal include permanent subterranean storage, entombment under the sea, and nuclear transmutation. Russia used ocean dumping extensively in the past and is responsible for most of the radioactive locations in the world’s oceans. Although Russia is not officially dumping it now, it has imported and stockpiled large quantities of high-level waste that it is not capable of handling.
Historically, the primary mechanism of disposing of low-level radioactive waste by other countries had been sea dumping. However, the practice was discontinued in 1983 in part because of widespread public opposition and a non-binding resolution passed by the signatories to the London Dumping Convention, which placed a de facto moratorium on sea dumping.
REFERENCES
Agency for Toxic Substances and Disease Registry: National Toxic Substance Incidents Program. http://www.atsdr.cdc.gov/ntsip/.
American Industrial Hygiene Association. Emergency Response Planning Guidelines. http://www.aiha.org/INSIDEAIHA/GUIDE-LINEDEVELOPMENT/ERPG/Pages/default.aspx.
Centers for Disease Control and Prevention. Fact Sheets on Specific Chemical Agents. http://www.bt.cdc.gov/chemical/factsheets.asp.
Commission for Environmental Cooperation. Taking Stock—North American Pollutant Releases and Transfers, 2012. www.cec.org.
Lim SR: Priority screening of toxic chemicals and industry sectors in the U.S. Toxics Release Inventory. J Environ Manage 2011;92:2235 [PMID: 21561706].
Organization for Economic Cooperation and Development. Risk Management of Installations and Chemicals. The Chemicals Accidents Program. http://www.oecd.org/chemicalsafety/risk-management/thechemicalaccidentsprogramme.htm.
The Right to Know Network. Spills and Accidents Database. http://www.rtknet.org/db/erns.
United Nations Environment Program—Awareness and Preparedness for Emergencies at the Local Level. http://www.unep.org/resourceefficiency/Business/CleanerSaferProduction/SaferProduction/APELL/APELLProgramme/tabid/78883/Default.aspx.
U.S. Environmental Protection Agency. Acute exposure guideline levels (AEGLs). http://www.epa.gov/oppt/aegl/.
U.S. Environmental Protection Agency: TRI National Analysis Dataset, 2011. http://www.epa.gov/tri/tridata/tri11/nationalanalysis/index.htm.
U.S. National Library of Medicine. Toxicology Network. Toxic Release Inventory. http://toxnet.nlm.nih.gov/cgi-bin/sis/htmlgen?TRI.
![]() SELF-ASSESSMENT QUESTIONS
SELF-ASSESSMENT QUESTIONS
Select the one correct answer to each question.
Question 1: Criteria air pollutants (CAPs)
a. make up all the components of smog
b. pose few public health risks
c. include carbon monoxide (CO), sulfur oxides (SOx), and nitrogen oxides (NOx)
d. are chemicals for which there are no regulatory standards
Question 2: Hazardous air pollutants (HAPs)
a. are CAPs emitted into the air
b. are chemicals for which there is no regulatory concern
c. are formally identified by the EPA
d. circumvent specific regulatory requirements
Question 3: Superfund Amendments and Reauthorization Act (SARA)
a. replaced the Emergency Planning and Community Right-to-Know Act (EPCRA)
b. gave states the authority above that of the EPA
c. authorizes citizens to block the use of toxic materials in their communities
d. mandates emergency planning for chemical accidents
Question 4: Health impacts of HAPs
a. cannot be inferred from occupational epidemiologic studies
b. cannot be inferred from toxicologic studies in experimental animals
c. do not involve respiratory irritants or systemic toxicants
d. include respiratory disease, systemic toxicity, and carcinogenicity
Question 5: The federal Clean Air Act of 1990
a. fails to reduce overall exposure to toxic air pollutants
b. ignores the stratospheric ozone layer
c. places a cap on the deposition of acidic constituents of air pollution
d. provides for use of market-based principles and other innovative approaches to reducing air pollution
Question 6: Hazardous materials (HAZMAT) teams
a. are licensed by OSHA
b. respond to hazardous materials incidents
c. prefer to perform decontamination in hospitals
d. first remove clothing and rinse the skin with water
Question 7: Emergency response action levels
a. are used to guide shelter-in-place or evacuation decisions
b. determine when it is safe for HAZMAT teams to enter the area
c. define the fatal doses to which individuals are exposed
d. offer absolute safety for officials in charge
Question 8: Protective action guides (PAGs)
a. help officials make critical decisions following a nuclear accident
b. designate the state and local officials who will take actions to safeguard human health during a nuclear accident
c. establish EPA authority in the event of nuclear accident
d. discourage protective actions other than those addressed by the PAGs
Question 9: Hazardous waste
a. is internationally defined to include solids, sludges, liquids, and containerized gases
b. includes domestic sewage, certain nuclear waste, and in situ mining waste
c. exclusions include agricultural wastes used as fertilizers
d. includes most household chemicals
Question 10: Agency for Toxic Substances Disease Registry (ATSDR)
a. was established to reimburse populations exposed to hazardous wastes for their associated health effects
b. has developed several specialized registries to study the long-term health effects of exposure to specific chemicals at hazardous waste sites
c. has selected four hazardous substances for the chemical-specific registries: trichloroethylene, dioxin, benzene, and PCBs
d. has established registries to monitor miners living in Montana and individuals most directly affected by the Love Canal chemical contamination